course handouts - university of houston
TRANSCRIPT

Course Handouts
INTERCONTINENTAL HOTEL 15201 Dallas Parkway Addison, Texas 75001

CE in the Southwest hosted by
PROGRAM LOCATION
INTERCONTINENTAL HOTEL 15201 Dallas Parkway Addison, Texas 75001
PROGRAM AGENDA
Saturday, March 22, 2014
7:00 am to 8:00 am Registration/Continental Breakfast/Visit Exhibits
Lectures presented Peter Kehoe, OD, DOS, FAAO:
8:00 am to 9:45 am Primary Care Electrodiagnostics COPE ID #36509-GO
9:45 am to 10:15 am Break/Visit Exhibits
10:15 am to 11:05 am Excellence in Optometric Patient Care COPE ID #34316-GO
11:05 am to 12:00 pm Prescribing Sports Specific Sunwear COPE ID #40708-GO
12:00 pm to 1:00 pm Lunch provided by UHCO and UIW
Lecture presented by Jennifer Deakins, OD:
1:00 pm to 2:45 pm Neuroimaging in Optometry COPE ID #40448-NO
2:45 pm to 3:15 pm Break/Visit Exhibits
Lecture presented by Bruce Onofrey, OD, RPH, FAAO, FOGS:
3:15 pm to 5:00 pm My Doc told me to get an eye exam because..... COPE ID #37212-PH CEE Available
Sunday, March 23, 2014
7:00 am to 8:00 am Registration/Continental Breakfast/Visit Exhibits
Lecture presented by Bruce Onofrey, OD, RPH, FAAO, FOGS:
8:00 am to 9:45 am GLC-Not Just IOP, Think DPP, OMG! COPE ID #37209-GL CEE Available
9:45 am to 10:15 am Break/Visit Exhibits
Lecture presented by Richard Sharp, OD:
10:15 am to 12:00 am Adult Acute Binocular Diplopia COPE ID #40698-SD
12:00 pm to 1:00 pm Lunch provided by UHCO and UIW
1:00 pm to 2:45 pm Diagnosis and Management of Secondary Glaucomas COPE ID #40699-GL
2:45 pm to 3:15 pm Break/Visit Exhibits
Lecture presented by Jennifer Deakins, OD and Jenny Terrell, OD:
3:15 pm to 4:05 pm Community-Based Eye Care: Optometry's Role in Public Health
COPE ID #40472-GO
Lecture presented by Jenny Terrell, OD:
4:05 pm to 5:00 pm Professional Responsibility COPE ID #40651-EJ

Primary Care Electrodiagnostics Peter H. Kehoe, OD, DOS, FAAO
Diplomate – American Board of Optometry 2-Hour General Optometry
COPE Course ID: 36509-GO
Neuro-Physiology of Vision o Phototransduction o Visual Pathway
Visual Evoked Potential (VEP) Electric signal registered at the occipital region in response to a visual stimuli.
o VEP Visual – patient observes a visual stimulus Evoked – generates electrical energy at the retina Potential – measure the electrical activity in the visual cortex
o Measure the function of the entire vision system; no patient response required
VEP – Previous Limitations
VEP – Current In-Office Technologies
VEP Stimulus o Flash o Pattern
Contrast Sensitivity Visual Acuity Color
VEP Components o Repolarization o Depolarization o Amplitude o Latency o High Contrast o Low Contrast
International Society for Clinical Electrophysiology of Vision o http://www.iscev.org/standards/proceduresguide.html
American Academy of Ophthalmology Preferred Practice Patterns
American Optometric Association Clinical Practice Guidelines
VEP and Other Ophthalmic Diagnostic Tests
Psychophysics of Vision o Visual Acuity o Contrast Sensitivity o Visual Field Test
Diopsys NOVA-TR o User-Defined Protocol o Customize testing parameters specific to each patient and pathology o Pattern Type & Size, Contrast level, Eye o Testing times are flexible and depend upon the customized settings
Diopsys NOVA-TR o Different Spatial Frequencies o Building Protocols o Building Option Sets o Multiple Sclerosis o Amblyopia – Vision Therapy o Neuro – Rehab - TBI
Prescribing and Response to Treatment
Diopsys NOVA-LX o Fixed Protocol
Pattern Type and Size are pre-determined o Normative Database for Glaucoma o Easy to interpret results for doctor and patient
VEP and Glaucoma – Well Defined Science o The Visual Evoked Potential in Glaucoma and Ocular Hypertension: Effects of Check
Size, Field Size, and Stimulation Rate Invest Ophthalmology Vis Science 24:175-183, 1983
o “The finding that is of clinical importance is the presence of abnormally long VEP latencies in some patients with ocular hypertension.
o The abnormal prolongation of VEP latency in these eyes may reflect subclinical optic nerve lesions that have not been uncovered with other techniques.”
Why VEP? o VEP is an objective, functional test that can help discriminate between healthy and
glaucomatous eyes2
How We Test o Low Contrast
Demonstrates degradation of magnocellular pathways
An early indication of glaucoma o High Contrast
Demonstrates degradation of parvocellular pathways
An early indicator of central vision loss and issues caused by problems before signal reaches optic nerve
Running Tests o Simple, automated protocol guides technician through the test o Operator friendly - anyone in the office can be trained to run the test1 o Patient set-up to printable results in as little as 4-6 minutes

Reading the Results o Quickly interpret results to enhance medical decision making and treatment
planning o Easy-to-read reports allow clinician to demonstrate therapeutic results and monitor
disease progression Normal or Abnormal – Red – Yellow - Green
Incorporating VEP in a Comprehensive Optometric Practice o Incorporating Any Technology in an Office
Does it do something our other technology doesn’t? Will it provide clinical information that will impact the treatment of our
patients? Can it be incorporated into our office? Space – Patient Flow - Staff Is it “standard of care” or “leading edge”? Is it “patient friendly”? Will it be profitable and/or Practice Builder?
Efficiency – Billable - Referrals
Clinical Example #1 – 11 year old Female o Complicated History o Normal VEP
Successful Vision Therapy Outcome
Clinical Example #2 – 63 year old Female o Unusual OCT and VF o Abnormal VEP leads to early treatment decision
Clinical Example – pERG #1
Clinical Example – pERG #2
Incorporating VEP in Our Practice o Space o Patient Flow o Staff o InfantSEE® Exams
Our Glaucoma Protocol including VEP o Annual Exam o 3-4 months later: gonio, IOP + VEP o 3-4 months later: HRT, HVF and OCT
Profitability of VEP o Comparison with other procedures o 95930 Reimbursement and limitations o Diagnosis codes associated with 95930
Referrals and Marketing due to VEP

Diopsys NOVA-PERG (Pattern ERG) o Available Fourth Quarter 2012
Test takes less than 2 minutes Allows simultaneous display of VEP and PERG Can help distinguish between retinal and cortical pathway issues Will display retinocortical timing
o Clinical Protocol o Profitability
Potentially TWO codes performed simultaneously
Summary – VEP + ERG o Good for The Patient o Patients accept and understand the technology o Objective data with no patient stress o Good for The Practice o Valuable clinical data for a variety of diagnoses o Easily incorporated into practice flow o A source of professional and patient referrals o One of the highest reimbursed procedures in the practice
Questions

Excellence in Optometric Patient Care Peter H. Kehoe, OD, DOS, FAAO
Diplomate – American Board of Optometry Cope: Applied
Course Description: You will learn the fundamentals of Excellence in Optometric Patient Care. Patient Expectations, office set up, staff, equipment, a review of clinical guidelines for specific disease states, and coding and billing will be discussed. An action plan will be provided to participants depending on the goals of the practitioner. Course Objectives: 1. You will learn the challenges and opportunities of Excellence in Optometric Patient Care,
regardless of the practice setting or modality. 2. The incidence and clinical practice guidelines for several common eye and systemic diseases
that are routinely discovered and managed in an optometric practice will be the basis of describing the infrastructure and staffing necessary to successfully provide Excellence in Optometric Patient Care in a corporate or traditional optometric practice including office layout and equipment.
3. Clinical Practice Guidelines with be the framework to outline a plan of action for certain ocular and systemic disease states and discuss where to learn proper coding and billing concepts, specifically the challenges of medical insurance versus vision insurance.
Introduction
Patient Expectations a. What Patients Expect from their Eye Doctor
The commitment necessary by the doctor and Staff Doctor and Practice Goals
Revenue
Patient Diversification
Introducing Medical Optometry
Primary Care Optometry
Total Patient Care
Philosophy
Optometry is THE primary eye care provider
Vision is our history but medical eye care is our future
The commitment necessary from the doctor
The commitment necessary from the staff
Meeting the total patient care needs – and expectations – of ALL your patients

Excellence in Optometric Patient Care and Doctor Driven Dispensing are closely linked.
Healthy Eyes - Healthy People – Healthy Practice
Incidence and Clinical Practice Guidelines for Common Conditions in an Optometric Practice
Review – Vision Problems in the U.S. – Prevalence of Adult Vision Impairment and Age-Related Eye Disease in America
o Cataracts o Age-Related Macular Degeneration o Glaucoma o Ocular Allergies o Dry Eye o Ocular Side-Effects of Systemic Disease
Diabetes Hypertension Cancers Emotional Disorders
Review – Children’s Vision and ocular health statistics o Refractive Error o Binocular Vision Issues o 3-D Vision
Review AOA Clinical Practice Guidelines for a Variety of Common Eye Conditions that can be managed in an optometric practice
o Dry Eyes o Red Eyes o Glaucoma o Macular Degeneration o Diabetic Patients
Necessary Office Infrastructure
Physical Plant Layout o Rooms and Patient Flow
Paperwork needs – health history, insurance information o Documentation for Medical Records and Medical – Legal o Patient Education
Staffing Needs o Patient Flow o Training Opportunities
Instrumentation o Disease Specific o Patient Education Opportunities o Getting Started with the Basics o Advanced instruments for advanced practices

Staffing
Phone Contact – triage versus information gathering – setting patient expectations
Understanding and Communicating the Concept to patients throughout the encounter
Mining for patient needs, wants and desires
The role of staff and need for additional training – Certified Paraoptometrics
The Optometrist(s)
Training is adequate – but is the commitment and desire equal to the training? o Where/How to gain additional confidence
Throughout the exam – extending the history and understanding the needs of patients.
Gaining or refreshing additional expertise – where, how and in what order
Skills necessary – always within the comfort zone!
Communicating the conditions and offering the provision of services
Setting the expectation that the optometrist is THEIR eye doctor for ALL eye conditions The Concept of Prescribing
Doctor Driven Dispensing Basics for vision needs of your patients
Prescribing special testing o Disease Specific o Based on Clinical Practice Guidelines
Prescribing the follow-up examination o Disease Specific o Based on Clinical Practice Guidelines
Coding and Billing in a Total Patient Care Mode
Discuss the philosophy and challenges of vision versus medical insurance and how to communicate with patients.
Discuss the concepts of proper billing and coding for common medical eye conditions
Review resources for learning the proper coding and billing procedures, including AOA and other sources
Summary
Review Concepts Excellence in Optometric Patient Care
Develop an Action Plan of implementing Excellence in Optometric Patient Care in an optometric practice

Prescribing Sports Specific Sunglasses
Course Description: A thorough and up-to-date review of sunglass options for the weekend and elite athlete will allow the
prescriber to offer patients research and medically recommended eyewear, both prescription and non-
prescription for protection and vision enhancement. The major sunglass manufacturers/brands that are
typically found in an optometric or optical practice will be shared with prescribing guidelines, marketing
messages, and competitive comparisons for golf, fishing, boating, cycling and many other popular
sports.
Course Objectives: 1. A discussion on the potential market for Sports Specific Sunglass prescribing based on US sports
participation will be the framework for the course. 2. Peer reviewed research on specific tints and lens/frame materials will be reviewed both for lenses
and frames. 3. Attendee will gain a thorough understanding of available sunglass options for a variety of sports. 4. A basic understanding of specific prescribing recommendations from sports vision organizations will
be shared 5. Inventory, internal and external marketing and point of purchase recommendations will be
discussed. 6. Participants will leave with a road map for incorporating Sports Specific Sunglass prescribing into
their practice.
1. A discussion on the potential market for Sports Specific Sunglass prescribing based on US sports
participation will be the framework for the course. 15 minutes
2. Peer reviewed research on specific tints and lens/frame materials will be reviewed both for
lenses and frames. 15 minutes
3. Attendee will gain a thorough understanding of available sunglass options for a variety of sports.
30 minutes
4. A basic understanding of specific prescribing recommendations from sports vision organizations
will be shared 15 minutes
5. Inventory, internal and external marketing and point of purchase recommendations will be
discussed. 15 minutes
6. Participants will leave with a road map for incorporating Sports Specific Sunglass prescribing into
their practice. 10 minutes

Neuroimaging in Optometry
Jennifer Deakins, O.D.
Community Eye Clinic, Fort Worth, Texas
• Bio
• UHCO class of 2010
• Residency in Ocular Disease, Bridge Builders Eye Clinic
• Current associate at Eagle Mountain Family Eye Care, Lake Worth (formerly 1st Eye Care)
• You never know what’s going to walk in the door…
• Overview
• Neuroimaging role in eye care
• Importance of coordination with neuroradiologist, neurologist, and/or neuro-ophthalmologist
• Relevant Imaging
• X-ray
• Computed Tomography (CT)
• Magnetic Resonance Imaging (MRI)
• Magnetic Resonance Angiography/venography (MRA/MRV)
• Computed Tomography Angiography (CTA)
• Indications for Imaging
• Ordering
• Case Reports
• What is the role of Neuroimaging in Eye Care?
• Coordinated Care
• The Radiologic Technologist
• 2 yrs Associates degree or 4 yr Bachelor of Science

• Coordinated Care - Referrals
• Neurologist
• Pediatric Neurologist
• John Honeycutt, MD
• Hayden Head, MD (Ped Neuroradiologist)
• Neuro-Ophthalmologist (4 in the DFW area)
• John McHenry, MD
• Sam Abdul-Rahim, MD
• Terminology Review
• X-ray
• Electromagnetic waves pass through tissue soft tissue, are absorbed by denser tissue. Image is
developed onto film.
• Skull x-ray to pre-screen for metallic FB prior to MRI
• CT
• Based on standard x-ray attenuation by tissues of various densities
• Rapid rotation of x-ray tube around patients
• Denser material (like bone) blocks/attenuates the x-ray beam and is “brighter” while less dense
material (like air) allows the beam to pass through and is “darker”
• Radiation exposure = 115 chest x-rays or 1 yr of background radiation
• CT with contrast or without
• Contrast material - Iodinated
• Contraindications - prior allergic rxn or renal failure
• Improved sensitivity and specificity
• Should be used for most ophthalmic imaging
• Exception:
• Thyroid eye disease*

• CT with and without contrast
• CT of the orbit, head or both
• Orbital:
• Images obtained at a different angle using thinner slices (0.7mm vs 3-
4mm)
• Can be reconstructed to any slice thickness (usually 2mm)
• Most common planes are axial and coronal, sagittal views can be
reconstructed
• Coronal views show relationship btwn EOMs, optic nerve, and
surrounding bone structures
• Note - 3-D reconstructions popular but can “smooth” over abnormalities and 2-D images should
always be viewed as well
• Indications for CT
ACUTE conditions
ie. trauma, HA, papilledema, vision/visual field loss, diplopia
If there contraindications to MRI - claustrophobia, severe obesity, cochlear implant, ferromagnetic
aneursym clip, pacemaker or other metallic FB
• The ABC’s of CT
A Acute study needed (bleeding, trauma, hydrocephalus, emergent case)
B Bone (fracture, sinus dz)
C Calcification (meningioma, craniopharyngioma,
retinoblastoma)
• Calcified Lesions
• Thyroid Eye Disease
• MRI
• Based on detecting signal from resonance within a large magnetic field
• MR signal generated from interaction of hydrogen protons within the powerful magnetic field
Just how powerful you ask?

Fun fact…Tesla (T) is the unit that measures
the magnetic field created by the MRI
• Contraindications to MRI
• Absolute - cardiac pacemaker* and any retained or implanted metallic foreign body (in critical
location)
• Difficult patients - movement disorders, children, claustrophobia
• 15-20 minutes per study, typically 8-10 studies
• MRI
• Signal intensity
• Hyperintense, isointense, hypointense
• 2 most common pulse sequences T1 and T2 - weighted images
• Normal anatomy - T1
• Intracranial or other pathology - T2
• Both typically acquired as part of MRI of orbit and brain
• Most important tissue appearances on MRI
• FAT - bright/hyperintense on T1
• CSF - bright/hyperintense on T2
• Pathology on MRI
• Most impt T1 hyperintense substances
• Subacute hemorrhage
• Proteinaceous fluid
• Melanin (very hyperintense T1 and very hypotintense T2) very useful in
imaging choroidal melanomas or intracranial melanoma metastases.
• Pathology on MRI
• Hyperintense T2 pathologies
• Demyelinating lesions

• Ischemia
• Inflammatory dz
• Toxic or metabolic disorders
• Neoplasms
• Optic Neuritis (example)
• What is fat suppression?
• Allows better visualization
• Hyperintense fat signal can block contrast enhancement
• Can show content of fat-containing lesions ie orbital dermoid cysts and lipomas
• Should always use for post-contrast orbital T1 - evaluating optic nerve sheath menigioma or
optic neuritis
• Usually, post-contrast fat suppression is standard (no need to order separately)
• FLAIR - Fluid attenuation inversion recovery
• FLAIR sequences show pathological hyperintensity on T2 better
• Should order when looking for demyelinating disease
• Hyperintense T2 signal of CSF can mask pathology
• GRE - Gradient Echo Sequence
• Shows blood very well, even trace amounts
• When used with T1 and T2, age of hemorrhage can be determined
• Good for looking at hemes associate with AV malformations and traumatic brain injury
• Gadolinium Contrast in MRI
• Should be used for all neuro-ophthalmic imaging (unless CI)
• Minimal side effects - skin rash, sweating itching
• Previously thought safe for kidney dz, beware nephrogenic systemic fibrosis (NSF)
• MRI with contrast is no longer “no risk” for renal dz patients
• Contrast in MRI
• 2 is often better than 1
• CT and MRI together may provide a more complete picture
• Especially in lesions that affect soft tissue AND bone
• Assessing Vascular Lesions
• MRA and CTA has reduced need for invasive catheter angiography
• Iodinated contrast-filled vessels can be seen without interference from background tissue
• 3-D rotational images
• MRA
• 2 types
• Time-of-flight (TOF) MRA *preferred for ophthalmic imaging
• Phase-contrast (PC) MRA
• MRA advantages over CTA
• No iodine contrast
• Less nephrotoxic
• Increased signal-to-noise ratio
• Easier post-processing techniques
• CTA advantages over MRA
• Increased spatial resolution
• Technically easier, faster to study
• Less motion artifacts
• Third Nerve Palsy
• Pupil involvement?
• For partial/complete EOM involvement WITH pupil involvement
• Traditional method - invasive catheter angiography
• MRA or CTA

• Usually MRI/MRA
• Third Nerve Palsy
• Third Nerve Palsy
• Vasculopathic patients with complete external WITHOUT pupil involvement
• Can be observed - likely ischemic
• Without vasculopathic risk factors or vasculopathic patients that don’t improve or progress over
several months - imaging indicated**
• MRA and CTA - up to 98% sensitivity in identifying aneurysm leading to third nerve palsy
• MRA and CTA - other uses
• AV malformations
• MRA and CTA - other uses
• Dural or carotid-cavernous fistula
• MRA and CTA - other uses
• Supected carotid artery disease
• MRV and CTV
• MRV/CTV used to exclude dural venous sinus thrombosis in cases of papilledema from increased
ICP
• Cerebral venous sinus thrombosis (CVST) can have same symptoms of
idiopathic intracranial HTN (CVST is a rare stroke involving thrombosis of
dural venous sinuses that drain blood from the brain)
• Indications - Vision Loss
• Unilateral or bilateral vision loss
• Unilateral or bilateral optic neuropathy
• Junctional scotoma
• Bitemporal hemianopsia
• Homonymous hemianopsia
• Cortical blindness

• Indications - Pupillary Defects
• Efferent pupillary defects
• Anisocoria due to Horner’s syndrome or 3rd nerve palsy
• Afferent pupillary defects
• RAPD
• Light near dissociation
• Indications - Orbit
• Thyroid eye disease
• Orbital tumors
• Idiopathic orbital inflammation
• Orbital cellulitis
• Carotid-cavernous fistula
• Indications - Lid Abnormalities
• Lid retraction
• Lid lag
• Ptosis
• Orbital lid lesions
• Indications - Fundus Abnormalities
• Papilledema
• Optic atrophy
• Optic nerve hypoplasia
• Optic disc drusen
• Choroidal folds
• Ordering Imaging
• Relevant clinical findings

• Suspected lesion location
• Differential diagnoses
• Urgency of imaging request
• Where to send
• Private imaging centers
• Radiology Associates www.radntx.com
• Preferred Imaging www.preferredmri.com
• Hospitals
• OD privileges
• Wait time
• Form
• Reasons for Imaging in Eye Care
32 per 10,000 cases imaging was ordered (ophthalmic services in hospital)
1. Suspected compressive lesions in anterior visual pathway
2. Acquired ocular motility disturbance
3. Orbital lesion
4. Cerebrovascular event
5. Headache
6. Sinusitis
• Case Reports
1. Severely asymmetric glaucoma
2. CN 6 Palsy and Temporal Arteritis
3. Pseudotumor cerebri (presumed)
4. Bilateral Papilledema
5. Thyroid eye disease

6. Ocular Ischemic Sydrome
• Asymmetric Glaucoma
• 68 Hispanic Female
• Presented to BB diagnosed with POAG (since 2007) treated in Mexico with Kryptan
(brimonidine, timolol, dorzolamide) and Xalatan
• LPI OU performed in Mexico
• Asymmetric Glaucoma
Clinical Findings
• BCVA OD 20/30 OS 20/25
• Mild/Mod DES and MGD
• LPI’s superior OU
• NS and cortical cataracts OU
• Gonio - open to CB, no pigment, very slight anterior bowing
• POAG OD>>OS
• Referred for CT
• Optic Nerve
• Visual Field
• OCT
• CT Results
• CN 6 Palsy and Temporal Arteritis
• 60 yo WF, slightly elevated cholesterol (diet and exercise)
• Sudden onset diplopia, after visit to chiropractor
• HA and tenderness on left side of head x 10 days
• BVCA OD 20/20 OS 20/20
• EOMs…primary gaze appeared to be left exotropia. (Pt was fixating on deviated image). True
findings: esotropia OD 15 pd, 3+ restriction of abduction OD
• Normal posterior/fundus findings, (-) AION
• Right CN6 palsy, suspected temporal arteritis
• Immediate MRI for motility disturbance
• CBC/Sed rate/CRP for temporal arteritis
• MRI Results
• Neurologist report
• Pseudotumor Cerebri (presumed)
• 37 black female
• Moderately overweight, hypertensive
• Reports ‘tension HA’ in the evening
• Hx of breast cancer surgery 2003
• Meds: Diltiazem, HCTZ, tylenol prn
• Clinical Findings
• BCVA 20/20 OD, OS 20/20
• IOP 20, 20
• 2 old corneal scars OD
• Mild HTN retinopathy
• Optic Nerve
• OCT
• MRI Results
• Pseudotumor - diagnosed
• 20 yo white female
• Reports HA (diagnosed with migraines). 2-3 times per week, variable location.
• Thyroid disroder, seasonal allergies, anxiety
• Amitriptyline HCL, cetirizine, synthroid, tri-sprintec, tylenol 3

• BCVA OD 20/20, OS 20/20
• IOP OD 20, OS 21 mmHg
• Normal anterior findings
• Normal peripheral retina/vasculature
• Bilateral optic nerve edema OD>OS
• MRI ordered – orbits and brain, with and without contrast
• No compressive lesions. Fluid intensity lesion left lateral aspect of the sella, likely a Rathke cyst.
Follow up MRI of pituitary in 6mo.
• Questionable mild prominence of CSF in ON sheaths bilaterally. May be within normal limits, of
uncertain significance.
• Referred to neuro OMD, lumbar puncture performed. High opening CSF.
• Pt was treated with diamox, clinical improvement in HA symptoms
• Limited communication = difficulty in follow cases
• Bilateral Papilledema
• 12 yo WF
• Requests CL exam
• 20/20 OD, OS
• Bilateral elevated rim tissue and NFL
• HA symptoms revealed upon further questioning
• CT
• MRI
• Thyroid Eye Disease
• 68 Black Female
• Previously dx’d with HTN, hyperthyroid, age-related arthritis
• Meds: Synthroid, Clonidine, Lisinopril, Diltiazem, Premarin
• Reported OS more prominent than OD x 2 yrs, stable

• (-) dip, (-) pain with eye mvmt
• Clinical findings
• BCVA 20/20 OD 20/25 OS
• Asymmetric proptosis OS>OD, (-) EOM restrictions
• Mild bulbar hyperemia, no significant DES
• 3+ cortical and 2+ NS cataract OU
• Normal ONH, macula, and fundus
• MRI without contrast of brain and orbit
• Refer for cat sx
• MRI Report
Impression:
Bilateral, symmetrical proptosis. Mild symmetric emlargement of EOMs, lateral rectus spared.
Suggestive of thryoid eye disease. No evidence of compression of ONH.
• Ocular Ischemic Syndrome
• Pt referred by fellow OD for retinal evaluation
• Hx of squamous cell carcinoma of the base of the tongue, prior neck sx and radiation
• DM type 2, HTN, RA, carotid artery dz
• 20/30 OD, 20/25 OS. Normal IOP
• Normal anterior structures, no NV of angle
• Glaucoma?
• 67 Hispanic male
• 20/25 OD, 20/30 OS
• Mild cataracts
• CVF – restriction in left field
• IOP 28 OD, 31 OS
• Glaucoma?

• Glaucoma?
• Glaucoma?
• References
• Lee, Andrew G et al. Imaging for neuro-ophthalmic and orbital disease - a review. Clinical and
Experimental Ophthalmology 2009; 37: 30-53.
• Mathews, JP et al. Can ophthalmic requests for neuroimaging be improved? Eye, 2004; 18: 290-
292.
• Lee, Andrew G. Ten Pearls for improving your use of neuro-imaging in neuro-ophthalmology.
Pearls in Ophthalomolgy, 2009.
• Bose, Swaraj. Principles of Imaging in Neuro-Ophthalmology. Ophthlamology, 2nd Ed. Ed by
Yanoff, M. and Duker J. 1241- 1248. Mosby, 2004.












































2/20/2014
1
ADULT ACQUIRED
DIPLOPIA
Rick Sharp, O.D. Assistant Professor, Rosenberg School of Optometry
Adjunct Assistant Professor, University of Houston College of Optometry
ADULT ACQUIRED
DIPLOPIA
Rick Sharp, O.D. Assistant Professor, Rosenberg School of Optometry
Adjunct Assistant Professor, University of Houston College of Optometry
ADULT ACQUIRED
DIPLOPIA
Rick Sharp, O.D. Assistant Professor, Rosenberg School of Optometry
Adjunct Assistant Professor, University of Houston College of Optometry
Diplopia cases at the VA in Baltimore
• Resident at Baltimore VAMC • Told preceptor I liked neuro • So, all diplopias given to me • Didn’t have a strategy at first • Felt stressed • Hospital inpatients • Walk ins
• I didn’t have a strategy to evaluate diplopia • So, I developed a strategy • Learned to like diplopias
• And to this day I like diplopias …….OK…not this well…..
“It’s a huge differential diagnosis,” said Nurhan Torun, MD, director of the neuro-ophthalmology service at Beth Israel Deaconess Medical Center and an instructor of ophthalmology at Harvard Medical School in Boston. “Diplopia tends to be intimidating for many practitioners.” Intimidation may even turn to dread. “When most ophthalmologists see a patient with a chief complaint of diplopia, they hate it,” said Michael S. Lee, MD, associate professor of ophthalmology, neurology and neurosurgery at the University of Minnesota in Minneapolis. “They often don’t know what to do with the patient.” What they do know, of course, is that the proper workup will take longer than a standard office visit. Well…………….good to know I was not the only one feeling this way initially.
The Baby Boomers are not coming….THEY ARE HERE!!!
• 2 years ago saw NP on Wed PM, was 6 now 11, all turned 65
• They get vascular TNP, SNP, FNP and decompensated heterophorias
You must know the common presentations but be ready for the
uncommon ones
• Non-isolated CN palsies (e.g., a TNP combined with a SNP, etc.)
• Thyroid eye disease causing diplopia
• Myasthenia gravis
• Internuclear ophthalmoplegias (i.e, brainstem origin)
• We will review these, uncommon but must be aware none-the-less

2/20/2014
2
The usual presentation with patients 65 and older…….
• A vascular (hypertensive or diabetic) TNP, SNP, or FNP
• A decompensated heterophoria (age, significant glasses change with cataract formation, or onset with a new oral medication). Usually age and Rx change.
• (Just make sure you are
stronger than your patients)
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
You walk into the exam room………
• If it’s a IIIn. Palsy • Easiest diagnosis • Ptosis • Eye is “down and
out” • Pupil involved or
not involved • Should take about
10 seconds after you walk in
Down because IV (superior oblique) is working Out because VI (lateral rectus) is working
Superior oblique
You walk into the exam room………
• It’s a Vin. Palsy
• You see it’s not a IIIrd
• Do quick lateral versions….there it is
• Should take about 10 seconds
• This is a LEFT sixth nerve palsy • Don’t get fooled by this presentation • Fixating with paretic eye (we will go further in detail about this)
You walk into the exam room………
• It’s a IVn. Palsy
• Ok, this is the tricky one
• Not a III or VI
• Maddox rod testing (this is the key)
• Diagnosis in about 3 minutes
We will discuss this diagnosis in detail
(note head tilt with this Left FNP)
OK, you’ve ruled out III, IV, VI……..
• So now you want to know if there’s comitance
• If so, decomp heterophoria • You will prescribe prism • Maddox rod comes in handy
here • If not comitant……..this is
where the real fun starts • But usually…it’s either III, IV,
VI or decomp phoria
• Any non-isolated CN palsy or pupil involvement
• Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM),
other signs • ….and more….

2/20/2014
3
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
Binocular or Monocular?
• Cover each eye individually and look evaluate their symptoms
• If you have monocular diplopia or triplopia or polyplopia you most likely have: – Uncorrected astigmatism – Pre-retinal membrane – Cataract with large vacuoles – ..combination of above
• Of course you can have monocular diplopia WITH a binocular diplopia (patients with pre-retinal membranes can have decompensation of their heterophorias too)
• You have to sort this out first • Usually you can do this in several seconds
MONOCULAR or BINOCULAR?
• First make sure they have their glasses on – If they have uncorrected astigmatism, they may
see two images with each eye or one eye
• Cover OD and ask, cover OS and ask
• With both eyes open ask
• If you don’t do this: – You may be on a “wild goose chase”
– Waste time
– Be angry with yourself at the end
Causes Monocular Diplopia
• Uncorrected asigmatism (ghost overlap – most common, esp. with new spectacle prescription)
• Pre-retinal membrane (metamorphopsia – fairly common)
• Dry or Wed ARMD (metamorphopsia)
• Looking through edge of bifocal (amazing but true)
• Dislocated IOL (rare)
• Monocular diplopia…………..but you mistakenly think it’s binocular diplopia
First is there a III, IV, or VI nerve palsy
• IIIn. Palsy – easy
– Don’t get tricked by an INO
– Make sure isolated
• Vin. Palsy – easy
– Don’t get tricked by fixation with paretic eye
– Make sure isolated
• IVn. Palsy – this is where most of trouble is
– Avoid mnemonic schemes, you may forget them

2/20/2014
4
The Usual Situations
• An isolated III, IV, or VI
– Either follow or order blood and imaging tests
• A decompensated heterophoria
– Rx glasses with prism
Will discuss INO’s later
I know, you can’t wait for that
o Bilateral pinhole – could keep trial frame with bilateral pinholes available o To grab anytime you have a diplopia case o Just pull it out and ask patient if they still have diplopia o PH will resolve:
• Uncorrected astigmatism • Pre-retinal membrane
What patients may report as “double vision”
D D Uncorrected astigmatism
Metamorphopsia
EOM Functional Anatomy
• Medial rectus (IIIn) – no problem
• Lateral rectus (VIn) – no problem
• Superior and Inferior recti (IIIn) – no problem
• Inferior oblique (IIIn) – maybe a problem
• The Superior oblique (IVn) this is where
most of the problem lies
• If the superior oblique is paralysed (an intorter and a depressor) then:
The inferior oblique will extort eye The superior rectus will elevate eye (hyper)
Patient sees this with extorsion

2/20/2014
5
Ludwig Edinger 1833-1890 1855-1918
Karl Friedrich Otto Westphal
I was taught……. This structure coordinated all the EOM movements. But now….
The EW nucleus actually only controls autonomic functions of the pupil – constriction and accommodation but NOT IIIn. EOM coordination. That’s done by IIIn. Nucleus.
YOUR LIBRARY
• No. 1 Neuro Book
• Paperback
• 30th edition available
• Not on Kindle yet
• F.J. Bajandas was a neuro-ophthal at UTHSC in San Antonio, killed in car accident 1981 who initially wrote this book
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
STEP 1 - R/O a THIRD NERVE PALSY
• This would be difficult to miss • Ptosis – many times a complete ptosis with no diplopia • The eye is down and out
– Down: nerve IV is still active and pulls eye down – Out: nerve VI is still active and abducts
• Double check for IV = the IIIn eye will intort with attempted infraduction (fun to watch while at the slit lamp)
• Doubt you will miss this • Do not confuse with:
– Internuclear ophthalmoplegia (INO)
• Pupil sparing – if older, HBP or DM, may not arrange imaging – How is the pupil spared in a TNP? (Pupilomotor fibers in the nerve
periphery, oculomotor nerves in the core of the nerve)
• Pupil involved - imaging • This diagnosis should take about 5 seconds
Third Nerve Levator
Superior rectus
Medial rectus
Inferior Oblique the only EOM with origin from within the orbit
Inferior rectus Superior oblique is CN IV
Lateral rectus is CN VI

2/20/2014
6
Third Nerve Palsy
• Ptosis (lid held up here). (There may be no c/o diplopia because of this) • “Down and out” – OS lateral rectus working (CN VI) out OS superior oblique working (CN IV) down • Pupil dilated (in some cases) – dilator unopposed by sphincter, dilation
Q: How does on evaluate the superior oblique during a IIIn. palsy?
A: At slit lamp visualize the 12 oclock position of corneal limbus and ask the
patient to look down
The eye will intort with attempted downgaze, then you know for sure No. 4 is
OS
There are ISOLATED nerve palsies and not ISOLATED ones
• The not isolated and not so good friends are: – Bilateral ptosis (sign of a nuclear
TNP)
– Cerebellar ataxia
– Hemitremor
– Hemiparesis
– Altered consciousness
• So look/ask for these signs as well as another CN palsy
Isolated III, IV, and VI are the best ones to have
Nuclear TNP (extremely rare) Bilateral ptosis (both levators innervated by central caudal Nucleus)
Fascicle TNP – with ataxia
or hemitremor Usually ishemic, infiltrative (tumor), rarely inflammatory
Uncal herniation syndrome Dilated pupil (Hutchinson pupil) with altered consciousness, Then MR, IO, SO, IR
Posterior communicating artery Aneurysm Most common cause of nontraumatic IIIn. palsy with pupil involvement
Cavernous sinus syndrome May see TNP with IV, V, and VI TNPs tend to be partial Pupillary fibers are sometimes spared
Orbital syndrome TN spilts before entering orbital fissue Superior: Superior rectus & levator Inferior: IR, MR, IO, iris, ciliary musc Usually some orbit pathology (e.g. orbital cellulitis)
Pupil Sparing Isolated IIIn • Pupillomotor fibers of III travel in outer layers of nerve closer to nutrient blood supply surrounding the nerve as opposed to the nerve core blood supply • Diabetes, hypertension, athero- sclerosis
1 2
3 4
5
6
7
So why is the pupil fixed and dilated before the other ocular signs? • Pupillomotor fibers are in the nerve periphery • EOM motor fibers in the core This also explains pupil sparing with a vascular TNP, closer to nutrient blood supply
Uncal Herniation Syndrome

2/20/2014
7
Posterior Communicating artery aneurysm
• Third nerve is adherent to aneurysmal sac • A hemorrhage of the aneurysm may push blood into the substance of the nerve • Pupil may be spared, on occasion, as aneurysm compresses the nerve • Follow patient carefully for initial 5-7 days initially
About pupil sparing IIIrds
• Pupil spared in 80% of vascular TNP, not spared in 20%
• Pupil involved in 95% of compressive TNP
• So you manage: imaging or no imaging
• E.g.: 80yo with DM and HBP, isolated – I will follow, no imaging
• E.g.: with ANY pupil involvement I will get imaging
Q: What imaging and when?
A: Very soon, like the same day or next day if possible
• MRI (Magnietic Resonance Imaging) of brain with and without contrast
• MRA (Magnetic Resonance Angiography)
Should an OD be ordering imaging?
• It’s up to you and how comfortable you are
• They want your business
• Can go through the primary care provider
• Some insurances require go through PCP
Case in Point
• Female with Left pupil involved IIIn. palsy, thought to be isolated diagnosed by physician
• After about one week finally sent to eye doctor
• Eye doctor ordered MRI and MRA for next day after examination.
• Called imaging facility for results next day, patient expired before tests done. Ruptured aneurysm of posterior communicating artery

2/20/2014
8
Case in Point
• 80yoF with pupil involved IIIn palsy
• Diabetic and hypertensive
• Called PCP for blood work and imaging
• My staff called patient following week: appointment made to see local OMD in 3 months
• Called PCP back, he responded
• Sent letter to PCP
• Never saw patient again (a fee for service patient)
The Pupil will drive some of your decision making:
• 80yo diabetic with HBP and isolated TNP with pupil sparing – may decide no imaging, just follow. Three month resolution.
The Pupil will drive some of your decision making:
• 80yo diabetic with HBP and isolated TNP with pupil involved
• MRI and MRA
I got Burned!!!!
(well…….not really)
Interesting IIIn Presentation
• About year 1989 • Saw 40yo F, diabetic with intermittant diplopia • Had large exophoria, pupils normal, no ptosis • Dilated Fundus Exam: florid neovascularization of disk and
elsewhere OD and OS • Arranged to see retina next day for immediate PRP • Retinal specialist called next day saying “this patient has a
third nerve palsy, why was she sent to me” (BURNED) • Apparently, I caught the palsy very early in evolution and
more concerned with the retina (act quickly to avoid vitreous hemorrhage)….so, not really burned.
Medial Longitudinal Fasciculus
Remember this Convergence intact
Internuclear Ophthalmoplegia (INO) many time misdiagnosed as a “partial” IIIn. palsy.
* INO

2/20/2014
9
Don’t label an INO (internuclear ophthalmoplegia) as a “partial” third nerve. Usually MS patient. If vascular, the patient is usually seen as an inpatient with a non-isolated INO.
Cannot adduct eye with a version
Can with convergence
Case in Point
• 68 yo male c/o diplopia, constant
• Cannot adduct OS, thinking L INO, however, he cannot adduct during convergence (not an INO)
• Otherwise feeling well, isolated problem
• Does have OS ptosis but dermatochalasis, levator function was full and = to OD
• MRI, MRA, neurology consult
• Neurologist says L IIIn. Palsy (ah……no)
• MRA occlusion of blood flow to medial rectus
• Resolved completely within 2 months
• Never seen or heard of such a cause = “Miscellaneous”
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
The Sixth Nerve
• Sixth nerve starts in the Pons • Travels forward then vertical to enter Dorello’s canal • Then forward past internal carotid artery in cavernous sinus • Entering superior orbital fissue • On to lateral rectus
Don’t forget GCA and Elev ICP with pap
Brainstem Syndrome • V, VII, and VII, VIII may be involved bec of proximity • Ipsilateral conjugate horizontal gaze palsy (remember 6 sends fibers to contralateral medial rectus • Numerous other neurologic problems since in brainstem…….therefore not isolated you will get further eval.
VIII
VII
VI V
Elevated ICP • Downward stem displacement • VI stretched palsies, bilat • 30% Pseudotumor have SNP • More…
Petrous Apex Syndrome • SNP • Ipsil decr hearing • Ipsil facial pain • Ipsil facial paralysis • Following otitis media
Cavernous Sinus Syndrome • Involvement of III, IV, and V • Horners • Optic n. compression • Pituitary gland involvment • …..not isolated… further eval
Orbital Syndrome • Proptosis • ON atrophy, edema • Trigeminal ophthalmic
involvement • Tumor, trauma, orbit
inflamm, cellulitis
STEP 2 – R/O SIXTH NERVE (lateral rectus) PALSY
• The most straight forward evalution
• Only problem is could be thrown off by patient fixating with the paretic eye…the fellow good eye is turned in
• Reduced abduction of the affected eye

2/20/2014
10
Yoked – Herings Law of Equal Innervation
• LR OD and MR OS “yoked” both muscles receive the same innervation to move the eyes together
• Same for convergence
• Same for torsional movements
Constantine Hering – Hering’s Law of Equal innervation “Father” of homeopathy Founded Philadelphia College of Homeopathy Born: January 1, 1800
It takes a lot of effort
to move this paretic
eye from the adducted
position to the central one
The OD lateral rectus
and the OS medial rectus
are “yoked” muscles. The
normal medial rectus reacts
to a high level of effort
It takes less effort to
Abduct the normal
OD eye, less “yoked”
power to the OD –
Therefore will not turn
in as much and smaller
angle of diplopia
R. Six Nerve Palsy
Sixth Nerve Palsy (SNP) SIX NERVE PALSIES
• Q: The patient here has an isolated SNP, now, which eye has the palsy?
• A: It could be either one
• It depends on which eye the patient chooses to fixate with and many times they will fixate with the PARETIC eye - ?why
I chose to fixate with my paretic eye for
a very good reason!!
If I fixate with my left eye I see double like this:
When I fixate with my right eye I see double like this:
The eye with the SNP
So, I will fixate with my right paretic eye.
More effort to abduct eye with lateral rectus palsy
Means equal amount of innervation to the medial rectus and it (being normal) goes way in
• 78yo male with his two daughters
• c/o diplopia constant
• Fixating with OD
• OS eso
• Daughters say “he has a problem with his left eye”
• Has obvious R SNP
• I explain how problem is not the left but the right eye ……in detail
• They say, “OK, how are you gonna fix dad’s left eye”

2/20/2014
11
Management of Isolated SNP
• Age under 50: greater probability of neoplasm, therefore – MRI brain with and without contrast, MRA, LP, neuro consult
• Over age 50 (?50, is that old?): most likely ischemic mononeuropathy, if not resolved in 3 months then do comprehensive evaluation
– CBC, ESR, CRP(looking for GCA), GTT, ANA
Duanes Syndrome • Prenatal lesion, nuclear cells that
give rise to abducens nerve are absent
• Type I (85% of cases)(of three) is isolated abduction deficit, unilateral or bilateral, with or without an esotropia
• May be confused with a SNP • A portion of III innervates the
lateral rectus muscle • This causes co-contracture of MR
and LR and the characteristic retraction
• Symptoms, usually no diplopia
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
Fourth Nerve Palsy • The most difficult of the three nerve palsies
depending on how you think about it
• Typically learn mnemonic schemes which are totally unecessary and just not the way to go since you have to remember the mnemonic scheme, so you need a mnemonic to recall the mnemonic……..and so on…..
• The diagnostic approach I developed has worked great for me for decades
No need to memorize schemes
Parks 3 step

2/20/2014
12
Nuclear –fascicular syndrome • Hemorrhage, infarction, demylenation, trauma
Subarachnoid space syndrome • The classic trauma cause • Causes bilateral FNP
Cavernous sinus syndrome • Associated III, V, VI, Horners
Orbital syndrome • Associated III, VI, proptosis, • Chemosis, conj injecion • Trauma, inflammation, tumor
STEP 2 – R/O FOURTH NERVE (superior oblique) PALSY
• For me, this was the most difficult to do
• I decided didn’t want to us mnemonic schemes (they would be forgotten)
• I didn’t want to spend much time doing cover testing
• Then was reading a book on dipolpia and saw that the IVn. was referred to as the “reading nerve”
FNP diagnostic approach
• The fourth nerve has also been called the “reading nerve” since eye in adducted and infraducted position while reading
• Diplopia increased with adduction of the involved eye, the eye with the FNP (reading position)
• Diplopia increased with infraduction of the involved eye (reading position)
So, • If you move into the field of paralysis the
diplopia will increase
• Adduction…….increase the reading nerve
• Depression…..increase the reading nerve
• Intortion (head tilt to same side shoulder)….increase
• OK ---- I didn’t want to do cover testing and prism measurement like orthoptists do, (I didn’t have all day) so I moved to……
THE MADDOX ROD
Ernest Edmund Maddox 1863 – 1933 OMD
Ernest E. Maddox, M.D. British OMD
This is the reflection you see, and the patient sees a solid red streak in same orientation

2/20/2014
13
(What you see)
(What they see)
OD sees H red streak
OS sees transilluminator light
NORMAL
(What you see)
(What they see)
So we have a left hyper (right hypo)
(I’m not including the tilt caused by the FNP if the OD was involved)
What you see
What they see
That becomes greater with adduction of hyper eye
What you see
What they see
That becomes less with abduction of hyper eye
What you see
What they see
More hyper with downgaze
What you see
What they see
Less hyper with head tilt to R shoulder
OS must extort

2/20/2014
14
What you see
What they see
More hyper head tilt to L shoulder
OS tries to intort, Unopposed SR pulls eye up
= LEFT FOURTH NERVE PALSY
• Most older patients cannot do this, stiff neck
• Must have assistant move
head with hands
HEAD TILT
FACE TURN
• All of my patients, when asked to tilt the head, instead do a face turn
• You must watch for this
About the Head Tilt
• Head tilt to R shoulder – OD tries to intort (sup obliq) and OS tries to extort (inf obliq) – Secondary action: Sup obliq tries to depress, Inf obliq
and Sup rectus counter elevates (antagonists)
– With FNP the eye elevates and elevates more with head tilt to same side of palsy
– Some patients figure out that if they tilt head to opposite side of palsy, their diplopia resolves
• Head tilt to L shoulder – OD tries to extort (inf obliq) and OS tries to intort (sup obliq)
Management of isolated FNP
• “Young person” – imaging, MRI brain and brainstem, CBC
• “Older person” if diabetic and hypertensive may choose to follow with no further testing
• From trauma - follow
Fourth is an intorter, if compromised the eye will extort and the patient will see the opposite - intortion, which can be quantified subjectively like this
Red white
R hyper with subjective intorsion
A cyclotorsion of more than 10 implies bilateral FNP
WHY NOT JUST DO THIS TEST INSTEAD OF MADDOX OD (as previously done)? • Is you patient that reliable? • You could

2/20/2014
15
Isolated FNP
• Congenital – usually discovered late (50’s and 60’s…what? 50’s are late?.....), head tilt
• Acquired and isolated – MRI for patients <45yo with no hx of head trauma
– MRI for patients 45-55 with no vasculopathic risk factors or hx of trauma
– BP, fasting blood sugar, glycosylated hemoglobin
– If GCA suspected: ESR, CRP, CBC
– If no resolution after 3 months: Neuro consult, MRI with and without contrast, MRA, LP
An 18-year-old with head tilt
complained of intermittent diplopia
for several months Muscle balance
measured 8Δ of right hypertropia in
primary position and 16Δ in left gaze
(adduction)..
CONGENITAL FOURTH NERVE PALSY with decompensation
Snapshots at ages 12 and 2 demonstrate habitual head tilt consistent with right superior oblique palsy
Age 12 Age 2
Age 18
Before surgery After surgery
• You may see decompensated fourth nerve palsies
• Their vertical fusional reserves will be higher than normal – like 4,5, 8, 10 etc.
instead of 1,2 or 3 • Just use a vertical prism bar, neutralize the hyper, then
go up and down to evaluated the reserves
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
A Decompensated Vertical Phoria
• Fairly common with aging
• Fusional reserves decline with aging
• Typically in 90s phorias decomp and need prism
• The larger the phoria and earlier the decomp
• Decomp with sickness and certain drugs
• The separation between streak and light stay same regardless of gaze up, down, left or right
• Its COMITANT
What you see
What they see
OK, right hyper

2/20/2014
16
What you see
What they see
What you see
What they see
What you see
What they see
What you see
What they see
PRISM!
• I measure phoria • Trial and error loose
prisms over glasses using phoria measurement as starting point
• Tell patient it will take 3 tries to get it right • Give about 75% of
maximal prism • Usually get it right first
time, if not second time • After about 3-4 years
usually need more prism
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……

2/20/2014
17
Be on Guard for These
• Myasthenia gravis
• Thyroid eye disease (Graves)
• Internuclear ophthalmoplegia
• Non-isolated CN palsies
• Giant cell arteritis
• Cranial nerve palsies III, IV, VI, isolated or non-isolated • Decomp heterophorias
• Myasthenia gravis • Thyroid eye disease • Internuclear ophthalmoplegia • Non-isolated CN palsies • Giant cell arteritis
Myasthenia Gravis
• Keep your mind open to this, if suspect start asking more questions
• Mechanism: skeletal muscle acetycholine receptors blocked by antibodies
• Usually females in 20s and 30s • Ptosis, diplopia (worse with prolonged effort or as day
progresses) • Difficulty in swallowing/breathing medical emergency • May involve pharyngeal muscles change in voice taking on a
more nasal quality
Antibodies
MG continued
• Can mimic any CN palsy III, IV, VI • Lid droop accentuated by having pt maintaing upgaze for 2
min • Manually elevating more ptotic lid will cause other more
normal lid to become more ptotic (= “enhanced ptosis”) • From downgaze to primary position lids will overshoot then
come to rest in their customary position = Cogans sign • Upgaze paresis, unilateral or bilateral especially when
ptosis is present • Pseudo INO (internuclear ophthalmoplegia) • Blood test for MG antibodies available, not always accurate • Tensilon (block breakdown of acetylcholine, increases the
neurotransmitter at neuromuscular junction, dramatically reverses ptosis or diplopia)
Common Things, other than TNP, FNP, SNP, decompensation of heterophoria
• Myasthenia Gravis
– May mimic specific cranial nerve palsies
– Pupil never involved
– Variable presentation, diplopia for short durations, then longer durations, apparent SNP there one day and not the next
– Definitely does not act like a vascular or compressive CN palsy
• 40 something female
• Presented with what I thought was a mild L SNP. No ptosis. Just out of the blue.
• Followed in one week – resolved (not acting like a vascular or compressive)
• Later re-appeared Tensilon test in office, (+) for MG, her diplopia resolved with injection and she felt as if she “came back to life”
Case in Point Thyroid Eye Disease (TED)
• Elevation and abduction abnormalities most common defect
• Muscle fibers eventually start to degenerate fibrosis
• Muscle fibrosis increase in chronic inflammatory cells restrictive myopathy and diplopia

2/20/2014
18
#1
Inferior
Rectus
#2
Medial
Rectus
#3
Superior
Rectus
#4
Lateral
Rectus
Involvement of EOMS in TED
*
*
(restriction with elevation)
(restriction with abduction)
and last but no least
Giant Cell Arteritis • Mechanism: necrotizing vasculitis of
medium and large extracranial arteries, T cells invade the wall of the artery, macrophages enter and cause lumen to close ischemia
• Diplopia in 10-15% of presentations • Literature mainly reports pupil sparing TNP • Just ask about:
Transient visual loss Scalp tenderness Jaw claudication (pain with chewing,
ischemia masseter muscle) Loss of apetitie, weight loss, night sweats PMR – pain and stiffness in proximal muscle
groups worse in AM and after activity
• If suspect: ESR, CRP, CBC, see primary care physician
Simple easy approach Make sure binocular
diplopia
Rule out a Cranial Nerve Palsy
III, VI, and IV (use Maddox Rod for IV)
If a CN palsy – determine isolated
vs. nonisolated
If not CN palsy – evaluate for comitance
(use Maddox Rod)
If comitant than most likely a
decomensated heterophoria
Evaluate oral medications (esp.
new ones)
Rx prism
Use of the Maddox rod is KEY in evaluation of the Fourth Nerve and…… In diagnosis of decompensated heterophorias
Be on guard: • Any non-isolated CN palsy or pupil involvement • Myasthenia Gravis • Thyroid Eye Disease (muscle restriction) • Internuclear Ophthalmoplegia • Giant Cell Arteritis (ischemia of EOM), other signs • …..and more……
we are done
All right…………………diplopia!!
fini

2/20/2014
1
Definition of “secondary glaucoma” controversial
AOA definition =This type of glaucoma occurs as a result of an injury or other eye disease. It may be caused by a variety of medical conditions, medications, physical injuries, and eye abnormalities.
Glaucomas that are associated with separate and distinct and identifiable pathological processes
Some definions do not include pigmentary or pseudoexfoliative glaucoma but most do
Some have big warning signs and you have to follow carefully
Pigmentary Dispersion Syndrome
Pseudoexfoliative Syndrome
Retinal ischemia
Inflammation leading to pupil seclusion or PAS
Your using steroids and need to remember to monitor IOP
If you miss them some how, it can be devastating
If your treating, you typically must be more aggressive
So…….that’s why
Pigmentary Glaucoma
Pseudoexfoliative Glaucoma
Neovascular Glaucoma
Uveitic Glaucoma
Steroid Induced Glaucoma
How many kinds of glaucoma are there?
Becker-Shaffer’s Diagnosis and Therapy of the Glaucomas
Stemper, Lieberman, Drake
Mosby/Elsevier 8th ed. 2009
A. Angle closure glaucoma A. Primary angle closure
B. Plateau iris
C. Phacomorphic block
B. Secondary angle closures A. Neovascular glaucoma
B. Iridocorneal endothelial syndromes
C. Ciliary block glaucoma
D. Iris cysts E. Intraocular tumors
C. Open angle glaucoma
A. Primary open angle glaucoma D. Secondary open-angle glaucoma
A. Pigmentary glaucoma
B. Pseudoexfoliative glaucoma C. Steroid glaucoma
D. Lens induced glaucoma (3)
E. Glaucoma after cataract surgery (6) A. UGH syndrome
F. Glaucoma associated with intraocular hemorrhage (3)
G. Glaucoma after vitrectomy (2)
H. Glaucoma with uveitis (9)
I. Glaucoma with intraocular tumors (6)
J. Amyloidosis
K. Increased episcleral venous pressure (3)
L. Developmental glaucoma (anomalies of the anterior segment at birth)
A. Primary congenital glaucoma (present at birth) (4)
B. Secondary glaucomas (10)
This text: 76 different
types in total
R.P. Sharp, O.D.
Assistant Professor
University of the Incarnate Word
Rosenberg School of Optometry
Pigmentary Glaucoma
Pseudoexfoliative Glaucoma
Neovascular Glaucoma
Uveitic Glaucoma
Steroid Induced Glaucoma

2/20/2014
2
These patients have a variation of anatomy that causes this problem and others PDS PG – greater fluctuations and peaks in IOP than POAG Retinal detachments They tend to be greater steroid responders Youger age
Common symptom is 20-40yo c/o blurred vision after exercise 1% to 2.5% of glucomas seen Predominantly young adults Strong association with myopia Mainly in Caucasians, rare in African Americans and Asians Typical patient is Caucasian in 20s or 30s Inheritance: sporadic
PDS and pigmentary glaucoma (PG) are two stages of the same disease process
The triad: Mid-peripheral radial iris
transillumination defects (“transillumination” and “retroillumination” describing same process)
Krukenberg Spindle Dense pigmentation of the trabecular
meshwork
Krukenberg’s Spindle (or K-spindle) – pigment deposited on corneal endothelium in vertical orientation (follows thermal flow pattern of pigment flowing from the posterior chamber) Extracellular pigment and.. Intracellular pigment phagocytized by
the endo
PDS has 10% risk of conversion to PG at 5 years and 15% in 15 years
Young myopic males with initial IOP of >21 are at increased risk of conversion
Anyone with PDS you must be vigilant
Baseline data Visual Field
Optic nerve and NFL imaging
Photos of retroillumination defects
Monitor for changes, at least annual or q6mo
Patient education
Have very deep anterior chambers, both central and peripheral
A concave curvature of the peripheral iris Can see during SLE and gonioscopy
Iris is larger
Mild iridodonesis (the iris can be seen jiggling anteriorly-posteriorly during small eye movements when observing with slit lamp)
The concave iris periphery
Gonioscopic appearance of The concave iris
Mechanical theory – the concave shape of the iris (as one views from the slit lamp) allows the iris to rub against the anterior lens zonules releasing pigment from the posterior iris epithelium
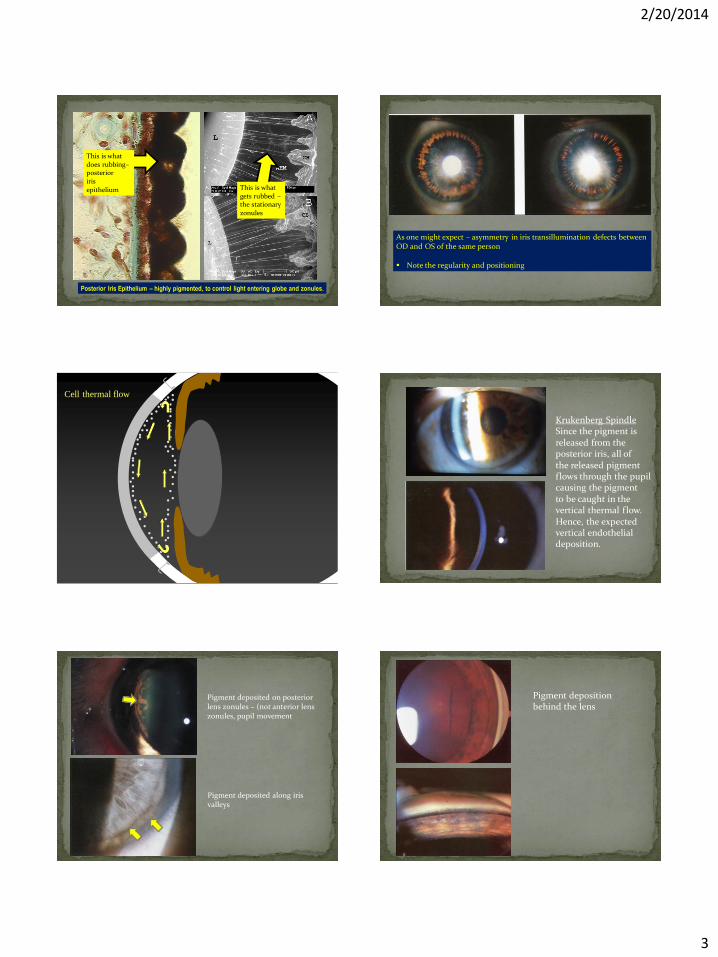
The posterior iris epithelium is highly pigmented
This released pigment then gets caught in the aqueous thermal flow – eventually depositing on the corneal endothelium (K-spindle) and in the trabecular meshwork (TM)
Outflow is compromised and IOP elevates
2/20/2014
3
Posterior Iris Epithelium – highly pigmented, to control light entering globe and zonules.
This is what does rubbing– posterior iris epithelium This is what
gets rubbed – the stationary zonules
As one might expect – asymmetry in iris transillumination defects between OD and OS of the same person Note the regularity and positioning
Cell thermal flow
Krukenberg Spindle Since the pigment is released from the posterior iris, all of the released pigment flows through the pupil causing the pigment to be caught in the vertical thermal flow. Hence, the expected vertical endothelial deposition.
Pigment deposited along iris valleys
Pigment deposited on posterior lens zonules – (not anterior lens zonules, pupil movement
Pigment deposition behind the lens

2/20/2014
4
The released pigment goes everywhere: angle, anterior iris surface, on the zonules, on the lens
A patient with pigmentary G can engage in sports activity, like basketball (jumping up and down), and experience a large release of pigment
Severe elevation of IOP
Corneal edema (endo pump cannot keep up with aqueous forcing it’s way in)
Halos (from corneal edema)
This can be blocked by use of topical Pilocarpine (pulls iris tight and reduces concave shape)
Regular pupillary block (as opposed to reverse block) This is mechanism for angle closure glaucoma (a.k.a. narrow
angle glaucoma) The pupil sphincter applies pressure against the lens making
it difficult for the aqueous to f low through Pressure builds up in the posterior chamber and pushes the
iris forward (iris bombe) causing TM block and a rapid and severe rise in IOP (up to and beyond 80mm Hg)
Pigmentary Glaucoma and Reverse Pupillary Block If you performed a laser peripheral iridotomy on a pigmentary
glaucoma concave iris, the iris straightens, and the pressure drops
This has led to the concept of reverse pupillary block
Normal aqueous flow
Pupillary block of aqueous flow
Iris bombe starts
Narrow Angle Glaucoma Mechanism
This is fascinating……
The act of blinking compresses the anterior chamber
Blinking pushes the iris and aqueous humor posteriorly pushing the iris against the lens zonules
The rubbing releases pigment which circulates creating the problems
During ultrasound biomicroscopy with normal lid position the iris is concave
B) Lid pressure bows iris backwards causing iris to contact zonules releasing pigment
A) Iris configuration when the lid is not in contact with the globe
The pupil then “burps” pigment into the anterior Chamber – this repeats itself over and over – pigment accumulates in the TM, up goes IOP

2/20/2014
5
With lid in normal position the iris is concave
Apply lid speculum which removes lid pressure from the globe
The iris gradually becomes LESS CONCAVE
Pressure builds in the posterior chamber pushing the iris forward
Remove the lid speculum and blinking is restored the original concave configuration is reestablished
Lens zonules are attached fairly close to the center of the lens Plenty of zonules for the iris to rub against
Blinking
Pupil dilation – try measuring IOP after dilation while in your office
Sports (especially jumping, “heading” the ball in soccer, boxing, jogging, every patient is different)
Head strikes in boxing or MMA fighting
PIGMENTARY DISPERSION SYNDROME (the anatomical tendency to release pigment is there to some degree – 0-100)
0 25 50 75 100 The continuum of disease presentation
PIGMENTARY GLAUCOMA
High tendency to go glaucoma
Low tendency to go glaucoma
This appears to be the case… Pigment dispersion can lessen with time
(This makes sense, once it’s rubbed away and replacement of pigment is reduced with the aging process)
The K-spindle becomes less prominent TM pigmentation becomes less prominent Increased aqueous outflow, so the IOP drops down to
normal levels May explain some nonprogressive cases of normal-tension
glaucoma i.e., ONH cupping, VF loss, normal IOP May have had pigmentary glaucoma and elevated IOP in the
past
With miosis, the iris is lifted away from the zonules
The transillumination defects fill in and can even disappear

2/20/2014
6
Take photos of iris transillumination defects
Measure IOP 1 hour after maximal dilation
Frequent gonioscopy
Pilocarpine is not well tolerated by younger patients
Medical therapy: CAI’s , B-Adrenergic antagonists, prostaglandin analogs
Be careful with miotics, could exacerbate a tendency for retinal detachments
A peripheral iridotomy should be considered to resolve the “reverse” pupillary block, use argon laser not YAG
Argon Laser Trabeculoplasty (ALT) is option, need lower power setting due to higher energy absorption by pigment. Selective Laser Trabeculoplasty (SLT) can be done as well.
Many patients eventually require a trabeculectomy
Reversing iris concavity Low concentration pilocarpine – ½% or 1% trial Can use Pilo ½% drop OU before immediately before sports
activity This pulls the iris away from the zonules MAKE SURE YOU DO DFE with attention to the periphery –
why? PG patients have higher incidence of lattice and retinal
detachments
Prevention of pigment release
Therefore – lowering the IOP
Prostaglandin analog works well (TravatanZ, Xalatan,etc.) with Pilo
Peripheral iridotomy Patient selection is key Those patients that have IOP spike after pupil dilation Patients under age 40 who have symptoms with exercise Use Argon laser, not the YAG laser – less pigment release
ALT and SLT good options Must keep power levels down to minimize pigment
release Works better in younger patients
Trabeculectomy The last stand, as needed
Before peripheral iridotomy
After peripheral iridotomy
Pigmentary glaucoma may diminish with age
E.g., treatment started at 30 may end and not be needed at age 60 or 70

2/20/2014
7
R.P. Sharp, O.D.
Rosenberg School of Optometry
University of the Incarnate Word
Pigmentary Glaucoma
Pseudoexfoliative Glaucoma
Neovascular Glaucoma
Uveitic Glaucoma
Steroid Induced Glaucoma
Pseudoexfoliative Syndrome = PXS
Pseudoexfoliative Glaucoma = PXG
Pseudoexfoliative material, filaments = PXF
The “pseudo” is in reference to true exfoliation of the lens capsule that occurs with exposure to infrared radiation (glass blowers)
This is the problem, tangled balls of fine filaments……..?origin
Glaucoma – Science and Practice Morrison, Pollack Thieme
aa
C O N T R O V E R S Y Source of PXF material
Abnormal production of basement membranes vs
Elastic fiber degeneration
A basement membrane is a mixture of material secreted by epithelial cells throughout the entire body
Laminin, fibronectin, elastin, heparan sulfate and chondroitin sulfate
PXF is a disordered extracellular matrix synthesis
But where is it coming from??????
PXF is found in posterior iris epithelium with a disorganized and duplicated basement membrane with degeneration and disruption AND PXS PXG IS ASSOCIATED WITH IRIS TRANSILLUMINATION DEFECTS AS WELL AS EXCESSIVE PIGMENT IN THE ANGLE

2/20/2014
8
Normal elastic tissue consists of a central core of amorphous, insoluable protein – elastin
Surrounded by microfibrils
Guess what’s present in PXF?
Elastin
Tropoelaastin
Fibrillin
PXF material SHARES LIGHT MICROSCOPIC STAINING CHARACTERISTICS WITH LENS ZONULAR FIBERS
Similar in amino acid composition and structure to microfibrils of elastin
With PXS and PXG there is atrophy of the posterior iris epithelium and IRIS TRANSILLUMINATION DEFECTS in some cases (not in all)
With PXS and PXG there is an association of lens zonular fibers weakness which can lead to LENS DISLOCATION during/after cataract surgery or without cataract surgery
Single nucleotide polymorphyisms in the lysyl oxidase-like LOXL1 gene are associated with PXG in many patient populations
The LOXL1 gene is an enzymatic protein important in extracellular matrix metabolism and turnover.
Changes in the extracellular matrix of PXF tissues have been hypothesized to be the mechanism responsible for the development of PXG
• Zonular fibers at peripheral and equatorial region of lens
• Granular balls of PXF
Glaucoma – Science and Practice Morrison, Pollack Thieme
Accumulation of material on lens
Broken zonular fibers
Pseudoexfoliative material
SCANNING EM
Glaucoma – Science and Practice Morrison, Pollack Thieme
Schlemms canal (sc) Arrows show tangle of randomly arranged fine filaments and
thicker fibrils Glaucoma – Science and Practice Morrison, Pollack Thieme
Schlemms Canal
(added resistance to movment
of aqueous into Schlemms Canal)

2/20/2014
9
There is PXF throughout the eye and body
PXF in conjunctiva, optic nerve sheath, EOMs, eyelids
PXF in lung, heart, liver, skin and gallbladder
Streeten, B.W., et.al. Pseudoexfoliative fibrillopathy in visceral organs of a patient with pseudoexfoliation Syndrome. Arch Ophthalmol 1992;110(12):1757-62
Note use of term “fibril”
PXF associated with vascular disease (cardiac, cerebral, vessel, etc.), sensorineural hearing loss, elevated homocysteine levels
Associations are WEAK and CONTROVERSIAL
PXS appears unilateral in about 50% of cases at the time of diagnosis
Probably a bilateral process with asymmetric presentation
Autopsy studies show fellow “normal” eye did have PXF distribution present
So….it’s probably there but not clinically apparent
In the Early Manifest Glaucoma Trial, 55% of patients with PXS developed PXG after a mean observation rate of 8.7 years
Therefore: must carefully watch your PXS patients
Consider diurnal IOP evaluation Come to office for two half days with a novel to read One AM, measure IOP qh One PM, measure IOP qh
Establish a baseline with ONH/NFL imaging Establish a baseline with VF At least annual exams And of course….patient education
“Target” with clear intermediate zone
Pupil must be dilated to see this
Material connects central disk with intermediate zone
Glaucoma – Science and Practice Morrison, Pollack Thieme
PXF at pupil margin
Prior to dilation
Look again after dilation
Or might be able to see on lens (phakia) before dilation

2/20/2014
10
Repeated pupil movement “peels” material
After cataract extraction, material on anterior hyaloid face of vitreous
Glaucoma – Science and Practice Morrison, Pollack Thieme
PXF material causes degenerative changes in the iris
Iris retroillumination defects*** (ddx PG and many other things that cause iris trans defects)
Increased vascular permeability and impairment of the blood aqueous barrier function
Pupils are difficult to dilate for this reason
Iris ghost vessel
PXF surrounds the obliterated lumen
Note: pigment is liberated from the iris (not rubbed off like pigment
dispersion) and is deposited in the trabecular meshwork
This is postmortem
This PXF presence (or origin disease) can weaken the zonules
Lens dislocation (without surgery)
Implant dislocation during or after catarat surgery
May need to remind cataract surgeon that patient is PXE, PXS, PXG
• Mother with pseudoexfoliative glaucoma needed cataract surgery • Toni discussed PXG with cataract surgeon
• Surgeon was chosen for experience with PXG patients
• Lens dislocated
• Vitreous prolapsed
• Retinal detachment
• Multiple complications
• A nightmare
Iatrogenic zonular dehiscence causing vitreous prolapse into the anterior chamber
Complete or partial lens prolapse into the vitreous cavity
Posterior capsular tears created during cataract surgery
Poorer dilation so smaller capsulorhexis making sugery less easily visualized
Increased postoperative cell and f lare, so need to keep on steroids longer This is due to a propensity for PXF iris vessels to leak serum
PXF/PXG patients should have their cataracts removed earlier – less stress on zonules when you are phacoemulsifying a “softer” nucleus as opposed to a more hardened nucleus
Mature cataract dislocation with PXS
Glaucoma – Science and Practice Morrison, Pollack Thieme
Dislocated lens with PXE on zonules
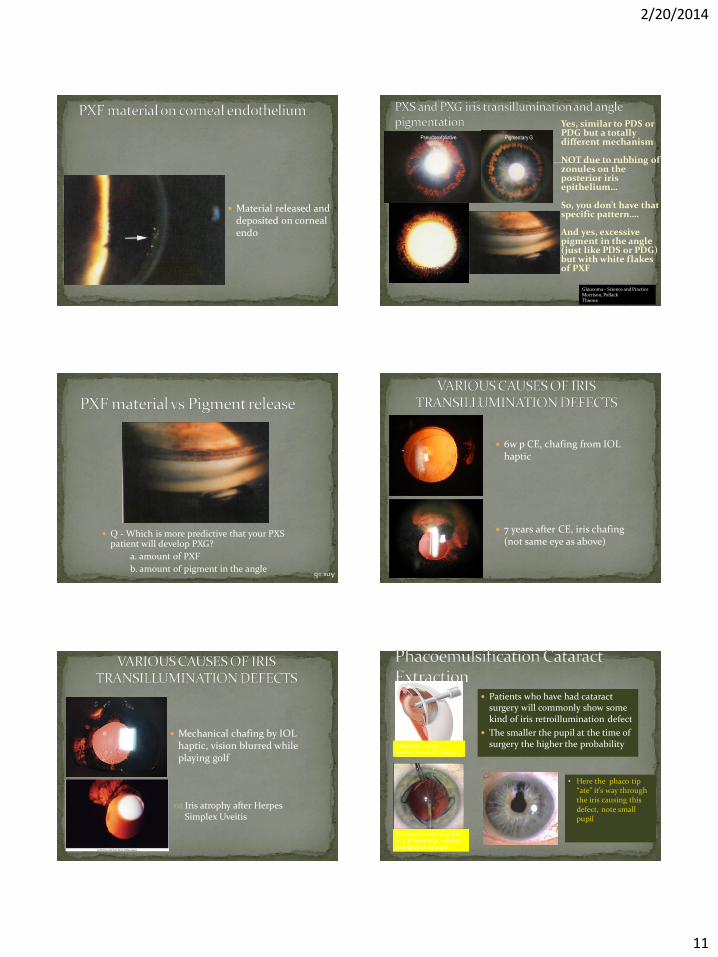
2/20/2014
11
Material released and deposited on corneal endo
Yes, similar to PDS or PDG but a totally different mechanism NOT due to rubbing of zonules on the posterior iris epithelium… So, you don’t have that specific pattern…. And yes, excessive pigment in the angle (just like PDS or PDG) but with white flakes of PXF
Glaucoma – Science and Practice Morrison, Pollack Thieme
Pigmentary G Pseudoexfoliative
Q - Which is more predictive that your PXS patient will develop PXG?
a. amount of PXF
b. amount of pigment in the angle Ans =b
6w p CE, chafing from IOL haptic
7 years after CE, iris chafing (not same eye as above)
Mechanical chafing by IOL haptic, vision blurred while playing golf
Iris atrophy after Herpes Simplex Uveitis
Patients who have had cataract surgery will commonly show some kind of iris retroillumination defect
The smaller the pupil at the time of surgery the higher the probability Ultrasonic energy
used to “emulsify” cataract
You want the iris out of the way of this energy – devices to help open the pupil
• Here the phaco tip “ate” it’s way through the iris causing this defect, note small pupil

2/20/2014
12
Small white round KPs
OD OS
(the same person)
Ernest Fuchs Austrian Ophthalmologist
Keratic Precipitates
AA
Figure 14.60 Fuchs uveitis syndrome. (a) and (b) Keratic precipitates; (c) stromal iris atrophy rendering the sphincter
pupillae prominent and small pupillary nodules; (d) stromal nodules and mature cataract; (e) posterior pigment layer atrophy seen on retroillumination; (f) angle vessels (Courtesy of C Pavesio - figs b and d)
Iris transillumination defects here
PXF decreases aqueous outflow
Pigment release also decreases aqueous outflow
PXF – on surface of lens or IOL
Up to 20% of pseudoexfoliative cases are missed if examined with undilated pupils (1)
Pupils may not dilate well with PXS/PSG
May see phacodonesis (abnormal lens movement or “jiggling” with small eye movements)
May see iridodonesis
(1) Forsius H. Pseudoexfolation sydrome in various ethnic populations. Acta Ophthalmologica 1988; 66(suppl 184):71-85.
If you do NOT routinely dilate pupils: You’re going to miss
fundus pathology You’re going to miss
PXS/PXG You will not be able to
appropriately manage anything that has to do with cataracts
1) More difficult to control than COAG
2) Higher IOP than COAG
3) Poorer response to ocular medications
4) May cause weakened lens zonules – a risk associated with inevitable cataract surgery (zonular rupture during cataract surgery, a little higher risk factor)
So, your going to have to fight this guy as aggressive as he tries to get you
PXG Monster

2/20/2014
13
Medial therapy similar to COAG Meds:
B-adrenergic agonists A-adrenergic agonists Miotics CAIs Prostaglandin analogs – Xalatan, Travatan, Lumigan
Sequence: Monotherapy Adjunctive therapy Maximal medical therapy Surgical intrvention
Good response to SLT or ALT
Good response with Trabeculectomy (same as COAG)
Some statistics (Thorburn W. The outcome of visual function in
capsular glaucoma. Acta Ophthalmologica 1988;66(suppl 184):141-147)
The old term for PXG is “capsular glaucoma”
Before patients died, 61% had undergone either ALT or Trab
25% became blind in at least one eye
8% blind in both eyes
15% with bilateral PXG became blind
(Published in 2010)
Pigmentary Glaucoma
Pseudoexfoliative Glaucoma
Neovascular Glaucoma
Uveitic Glaucoma
Steroid Induced Glaucoma
Neovascular Glaucoma
A nightmare
A nightmare
Retinal ischemic tissue releases vasoproliferative substance (otherwise known as VEGF, vascular endothelial growth factor) which migrates past/around/through the vitreous to the anterior segment
Pre-existing vessels sprout new vessels which easily tear, hemorrhage, leak, and leak fibrin molecules with myofibroblasts
If enough fibrin molecules are leaked, a fibrin membrane can form which can contract (thanks to the myofibroblasts)
If the membrane is attached along a surface, that surface will be pulled together
Neovascular Glaucoma

2/20/2014
14
Movement of vasoproliferative substance
(1) Hemi BRVO,
vigilant, gonio first visit, check iris
(2) CRVO, some CWS, more vigilant – gonio every visit, r/o NVI
(3) CRVO, ischemic, very vigilant – gonio every visit, r/o NVI
(4) Very ischemic CRVO, extremely vigilant – same as above but more effort in looking
Vein Obstructions When does one need to be vigilant for
neovascular glaucoma?
(1) (2)
(3) (4)
Gonio every visit
Careful search NVI every visit
Treatment by Retinal specialist (they will be looking too)
Proliferative Diab Ret
CRAO’s can be obstructed from 1% to 100% so ischemia can vary
Look for NVI and do gonio
Frequency depends on amount of ischemic signs
Central Retinal Artery Obstructions
Must take some
time to carefull search
Start at rim and go out
Try red fee filter too
Neovascularization of Iris (NVI)
New blood vessel
leaks fibrin
The fibrin
accumulates…
..and accumulates…

2/20/2014
15
..and accumulates…
..then contracts…
A B
A B
The myofibroblasts cause contraction of the fibrous membrane
Retina
Choroid
& RPE
Fibrovascular Membrane –
attached to retina
Fibrovascular Membrane –
attached to retina
The fibrovascular (neovascular)
membrane contracts pulling the
retina with it
and there you have a
TRACTIONAL RETINAL
DETACHMENT (TRD)
As opposed to a:
Rhegmatogenous RD
Serous RD
Tractional retinal detachment
The membrane pulls the retina away from the RPE and forms another plane of tissue
Fibrovascular membrane
Progressive PAS formation in neovascular glaucoma
The neovascular membrane contracts and pulls the flaccid iris up against the
angle forming PAS
The iris is actually pulled
inside out, the posterior iris
epithelium is pulled out on
the anterior iris surface = ectropion
uvea

2/20/2014
16
NVG is a “pulling” mechanism, where
the iris is pulled up to the angle by
fibrovascular membrane contraction
NAG is a “pushing” mechanism
where the pupillary block causes
pressure to build behind the floppy
iris and it is pushed forward
Myofibroblasts in the
fibrovascular membrane
contract pulling the iris
up to the angle forming
peripheral anterior
synechiae (PAS)
Most likely etiologies: (1) ischemic central retinal vein obstruction and (2) proliferative diabetic retinopathy (again, ischemia)
NV starts at pupil margin, this is a 10 on a 1-10 scale
NV forms in the angle causing PAS
Ectropion uvea
Using the Volk G4 with
flange (better control)
I go mm by mm, slowly, 360
degrees
Rule out NV
No diversions
…concentrate…..
How I evaluate angle for NV
Initially we’re utilizing a retinal specialist the day of
diagnosis (a true emergency)
Intravitreal anti-VEGF injection (about 6 weeks for full
effect)
PRP (pan retinal photocoagulation)
Topical glaucoma medication
Atropine and topical steroid if photophobic
A glaucoma surgeon for the rest
Trabeculectomy or aqueous shunt
NVG - treatment
Must be looking for NVG when you think you have an acute
Narrow Angle Glaucoma attack in your chair
Many times the cornea is edematous and you may have difficulty
seeing iris details
Be suspicious when:
Patient is diabetic and fellow eye has signs of retinal ischemia
(NFL infarcts, moderate changes, etc….)
The fellow eye chamber is deep (it should be similar to eye with
NAG attack)
Comments NVG

2/20/2014
17
The key to managing NVG is to
watch any patient with retinal
ischema carefully looking for
NV of iris and NV in the angle
Early detection, early treatment
and avoidance of glaucoma
E.g., with an ischemic CRVO
you might see the patient every
week
The Key to NVG
Uveitic Glaucoma
Pigmentary Glaucoma
Pseudoexfoliative Glaucoma
Neovascular Glaucoma
Uveitic Glaucoma
Steroid Induced Glaucoma
Uveitis-induced ocular hypertension
• There is no optic nerve damage or field loss
• But, there is elevated IOP
• So, not uveitic glucoma
Uveitic Glaucoma or Inflammatory
Glaucoma
• There is evidence of optic nerve damage or field
loss, etc.
Terminology
About 25% of uveitis patients will develop increase in IOP at some time during course of inflammatory disease
More common with granulomatous as opposed to nongranulomatous
Main problem is obstruction of outflow
Can produce a glaucoma that is severe and not treatable with medical therapies
Statistics
The longer you treat a uveitis the greater the chances you will have a complication that elevates IOP, so, tighten up the follow up as time progresses
Look for the following problems
Sometimes the patient will for whatever reason stop steroid or mydriatic use and help create problems
….or…they won’t show up for f/u appointments…then finally show up with complications
The trouble is…..uveitis can produce a glaucoma that is not only severe but resistant to all medical therapies
In general:
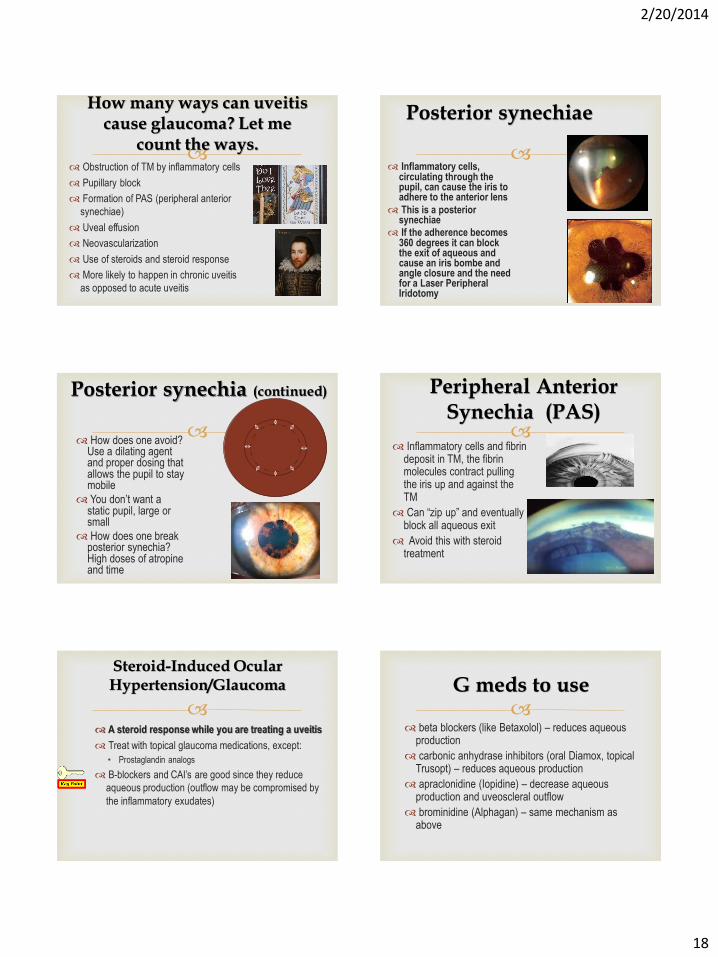
2/20/2014
18
Obstruction of TM by inflammatory cells
Pupillary block
Formation of PAS (peripheral anterior
synechiae)
Uveal effusion
Neovascularization
Use of steroids and steroid response
More likely to happen in chronic uveitis
as opposed to acute uveitis
How many ways can uveitis cause glaucoma? Let me
count the ways.
Inflammatory cells, circulating through the pupil, can cause the iris to adhere to the anterior lens
This is a posterior synechiae
If the adherence becomes 360 degrees it can block the exit of aqueous and cause an iris bombe and angle closure and the need for a Laser Peripheral Iridotomy
Posterior synechiae
How does one avoid?
Use a dilating agent and proper dosing that allows the pupil to stay mobile
You don’t want a static pupil, large or small
How does one break posterior synechia? High doses of atropine and time
Posterior synechia (continued)
Inflammatory cells and fibrin
deposit in TM, the fibrin molecules contract pulling the iris up and against the TM
Can “zip up” and eventually block all aqueous exit
Avoid this with steroid treatment
Peripheral Anterior Synechia (PAS)
A steroid response while you are treating a uveitis
Treat with topical glaucoma medications, except:
• Prostaglandin analogs
B-blockers and CAI’s are good since they reduce
aqueous production (outflow may be compromised by
the inflammatory exudates)
Steroid-Induced Ocular Hypertension/Glaucoma
beta blockers (like Betaxolol) – reduces aqueous production
carbonic anhydrase inhibitors (oral Diamox, topical Trusopt) – reduces aqueous production
apraclonidine (Iopidine) – decrease aqueous production and uveoscleral outflow
brominidine (Alphagan) – same mechanism as above
G meds to use

2/20/2014
19
Prostaglandin analogs (like Xalatan) – increases
uveoscleral outflow, reported to produce inflammation
and cystoid macular edema
Miotics – may contribute to posterior synechiae, cause
ciliaty body muscle spasm, enhance blood-aqueous
barrier
G meds to NOT use
Basically trying to break the
adhesion between the iris
and the TM
Making a direct opening into
the canal of schlemm
Goniosynechialysis or Trabeculodialysis
Direct outlet of aqueous
from anterior chamber to
subconjunctival space
Express Shunt
Cryogenic “old school” produces ischemic necrosis of CB and ciliary epithelium
Ciliary Body Ablation
Contact diode laser – destruction of ciliary epithelium
aa
Endoscopic Cyclophotocoagulation
Endoscopic view during procedure
Diode laser
Rick Sharp, O.D.
Associate Professor – Rosenberg School of Optometry
Adjunct Assistant Professor – University of Houston College of Optometry

2/20/2014
20
Pigmentary Glaucoma
Pseudoexfoliative Glaucoma
Neovascular Glaucoma
Uveitic Glaucoma
Steroid Induced Glaucoma
Steroid Responders – people who have an increase in IOP when using steroids
Steroid Glaucoma – G caused by steroid use
Steroid Induced Ocular Hypertension
Terminology
Steroids cause changes in the TM Cellular – function and morphology Biochemical – extracellular matrix production increase Molecular – cytoskeleton , gene cell expression AND THESE CHANGES RESEMBLE THOSE OF POAG!!
Outflow is reduced This typically takes weeks sometimes days depending on
the individual IOP elevates Glaucoma Children age 5-6y old are more likely to be a steroid
responder thought to be due to a difference in the TM anatomy at this age (functional immaturity). By age 8 functional maturity is reached
Mechanism Mechanism
EFFECT OF STEROID ON TM CELLCYTOSKELETON
Normal TM cell actin microfilament bundles forming linear arrays of stress fibers
Steroid induced reorganization of microfilaments into these stellate figures call cross linked actin networks
Steroids suppress phagocytic processes of the trabecular endothelium causing accumulation of debris in the meshwork
….which decreases aqueous outflow
Mechanism
-Armaly MF. Statistical attributes of the steroid hypertensive response in the clinically normal eye. Invest Ophthalmol 1965;4:187-197
-Becker B. Intraocular pressure response to topical corticosteroids. Invest Ophthalmol 1965;4: 198-205
Steroid Responders
Two studies independent from each other in 1960s
Dexamethasone and betamethasone (not prednisolone)
.1% drops tid or qid x 4-6 weeks
Results: 4-6% termed “high responders”, IOP >31 (or greater than
15 above the subjects baseline IOP)
33% termed “moderate responders”, IOP 20-31 (or 5-15 above baseline)
Remainder (let’s say 100-(33+5)=62%) 62% were termed “nonresponders”
So lets round off at 60 non/40 low with 5% high responders
2/20/2014
21
Ahh…..no
Elevated IOP can persist in some cases Pre-existing glaucoma, just now off steroids?
The steroid “converts” the eye to POAG
Using topical steroids with POAG patients produces a moderate or high response in nearly all subjects (Armaly MF. Effect of corticosteroid on intraocular lpressure and fluid dynamics, II: the effect of dexamethasone in the glaucomatous eye. Arch Ophthalmol 1963;70:492-499….and….Becker B, Hahn KA. Topical corticosteroids and heredity in primary open-angle glauocoma. Am J Ophthalmol 1964;57:543-551)
This is important!!! Your glaucoma patients getting cataract surgery or trabeculectomy surgery will be on steroids afterwards – expect the IOP to elevate You might mistakenly conclude the trabeculectomy has
failed, it may be fine with IOP elevation due to steroid use
No big deal – just stop the steroids, right?
Now isn’t THIS special!
Families of patients with POAG tend to be
responders
There seems to be a link between the glaucoma gene GLC1A, TIGR and steroid induction into the TM
High steroid responders are more likely to develop POAG
Diabetics and high myopes have higher rates of steroid responsiveness
Responders and POAG
IOP elevation directly related to dose
Topical - eyedrops
Periocular administration – subconjunctival injection, retrobulbar injection
Systemic – oral or injected
Inhaled
Transdermal
Intranasal
In other words….all routes of steroid treatment
What steroids are we considering?
General practitioner or PA may prescribe a topical
steroid or antibiotic-steroid combination – not too often these days
Then refills are given and given and given and the patient continues to take the meds
I have met several patients with severe VF loss who have sued their PCPs over this
General Practitioners and refills
Initally the patient has undiagnosed glaucoma and
elevated IOP
Uveitis starts and the CB produces less aqueous and the IOP goes down. You then measure IOP.
You start prednisolone acetate (Pred Forte) and after two weeks the IOP goes up and up as the CB recovers and makes more aqueous
You conclude the patient is a steroid responder
You eventually take them off the steroid
The IOP does NOT go down (your back to the unknown and undiagnosed glaucoma situation from the beginning)
The Uveitis-Steroid Pitfall
Your patient is being treated with a long term steroid
(oral or transdermal), IOP goes up, optic neuropathy goes so far
Then the steroid is stopped and the IOP goes down
You then see the patient with glaucomatous changes and VF loss with normal IOP and conclude patient has NTG
The Normal Tension Glaucoma Pitfall
Isn’t THAT special!
2/20/2014
22
You have a uveitis that is not therapeutically responding
to topical steroid (you’re in the Uveitis-Steroid Pitfall) and your patients IOP is at a normal level
You do sub-tenons steroid injection without knowing if your patient is a steroid responder
The patient just happens to be a high responder
The IOP goes up to 75mmHG
You can’t get the steroid out (cannot aspirate out)
You start topical and oral meds to lower the IOP
May even need a trabeculectomy
This is a known risk anytime you do a sub-tenons
Risk of NOT sub-tenon vs. doing the sub-tenons
Sub-tenons depo nightmare
Isn’t THAT special!
From most likely (and most effective) to least likely (and less effective):
Durezol (difluprednate ophthalmic emulsion) – fabulous, no BAK, ?effect on IOP, be careful
Dexamethasone
Prednisolone (Pred Forte)
Flurometholone (FML), Rimexolone (Vexol), Loteprednol (Lotemax)
Topical steroids less likely to cause a response
fini
Boulder Colorado
CE Outline for CE in the Southwest –Dallas, TX (March 22-23, 2014)
Jennifer Deakins, OD and Jenny Terrell, OD
Community-Based Eye Care: Optometry’s Role in Public Health
I. Community Eye Clinic
a. Brief history of the clinic
b. Patients served
c. Educational component
II. Patient Access
a. Professional services
b. Medications
i. Insured
ii. Uninsured
1. Individual manufacturers
a. Most companies have their own patient assistance program
(PAP)
2. “Clearinghouse” websites for assistance
a. www.needymeds.org (non-profit resource info about PAP)
b. www.rxhope.com (supported by PhRMA and companies)
c. Follow-up visits
i. Transportation issues
ii. Updated contact information
III. Barriers to Healthcare
a. Health literacy level
b. Patient’s budgeting priorities
c. Co-morbidities
d. Citizenship/residential status
IV. Referrals for surgical/tertiary care
a. Local medical society may provide assistance
b. Building relationships with retina, cornea, etc
c. Specific challenges to emergency care
V. Adding Philanthropic Care to Your Practice

a. Patients to sign waiver
b. Community based organizations
c. How to find the resources in your community
VI. Community Resources
a. Local churches
b. United Way -211
c. FQHC’s
d. County hospitals
e. Challenges in coordinating care with non-profit orgs

CE in the Southwest March 23, 2014 Speaker: Jenny Terrell, OD Course Title: Professional Responsibility (1 hr)
I. Prescriptions, ophthalmic and drug a. Optical Board Rule 361.359
1. Ophthalmic lens prescription must include: a. Signature of the optometrist or therapeutic optometrist (not
printed or stamped) b. The information and parameters the optometrist or therapeutic
optometrist considers relevant and necessary. ii. The prescription may not contain a restriction that limits the parameters to a
private label not available to the optical industry as a whole. b. Drug Board Rule §280.10(d)
i. A therapeutic optometrist may prescribe oral medications only in the following classifications of oral pharmaceuticals: (1) one 10-day supply of oral antibiotics; (2) one 72-hour supply of oral antihistamines; (3) one seven-day supply of oral nonsteroidal anti-inflammatories; (4) one three-day supply of any analgesic identified in Schedules III, IV, and V of 21 U.S.C. Section 812; and (5) any other oral pharmaceutical recommended by the Optometric Health Care Advisory Committee and approved by the board and the Texas State Board of Medical Examiners. (d) A therapeutic optometrist may independently administer oral carbonic anhydrase inhibitors for emergency purposes only and shall immediately refer the patient to an ophthalmologist. (e) A therapeutic optometrist may inject appropriate medication for a patient who has an anaphylactic reaction to counteract the anaphylaxis. The therapeutic optometrist shall immediately refer the patient to a physician.
c. Doctor identification on prescriptions II. Definition of Standard of Care
a. Why is it important? b. Standard of Care Defined:
i. standard of care n. the watchfulness, attention, caution and prudence that a
reasonable person in the circumstances would exercise. If a person's actions do
not meet this standard of care, then his/her acts fail to meet the duty of care
which all people (supposedly) have toward others. Failure to meet the standard
is negligence, and any damages resulting therefrom may be claimed in a lawsuit
by the injured party. The problem is that the "standard" is often a subjective
issue upon which reasonable people can differ. (See: negligence, duty of care)
ii. Medical: Standard of care: 1. A diagnostic and treatment process that a clinician
should follow for a certain type of patient, illness, or clinical circumstance. In

legal terms, the level at which the average, prudent provider in a given
community would practice. It is how similarly qualified practitioners would have
managed the patient's care under the same or similar circumstances. The
medical malpractice plaintiff must establish the appropriate standard of care
and demonstrate that the standard of care has been breached.
III. Reclassification of hydrocodone a. Schedule II
i. “Substances in this schedule have a high potential for abuse which may lead to severe psychological or physical dependence.”
b. Schedule III i. “Substances in this schedule have a potential for abuse less than substances in
Schedules I or II and abuse may lead to moderate or low physical dependence or high psychological dependence.”
c. Currently, hydrocodone alone is classified as Schedule II but drugs containing less than 15mg of hydrocodone per dosage unit or in combination with acetaminophen are classified as schedule III controlled substances
d. APhA joint letter on Nov 11, 2013: i. “While we appreciate the efforts of the FDA to address the serious issue of
prescription drug abuse, we believe rescheduling hydrocodone is not the solution,”
e. New requirements for pharmacies that will increase burden such as “the provision of additional secure storage, recordkeeping, and inventory management.”
f. Reclassification may present problems in allowing patients in need access to the drugs g. No more phone orders h. Patients need more frequent visits to prescribers to obtain prescriptions since schedule
II drugs may not be refilled. This will cause more emergency room visits and ultimately drive the cost of health care higher
i. ASHP: (American Society of Health-System Pharmacists): Nov 5, 2013 i. “Based on an assessment using the criteria the [DEA] considers when
determining whether to control or reschedule a drug, ASHP believes that hydrocodone combination products are similar to other controlled substances found in Schedule II and should therefore be assigned to Schedule II,”
j. What does it mean for optometry? i. Reclassification would mean that OD’s could no longer prescribe any drug with
hydrocodone for pain management. 1. Vicodin 2. Lortab
IV. Medicaid Fraud and Abuse audits a. CMS definitions
i. Fraud – making false statements or representations of material facts to obtain some benefit or payment for which no entitlement would otherwise exist.
ii. Abuse – practices that, either directly or indirectly, result in unnecessary costs to the Medicare Program.
1. Misusing codes on a claim 2. Charging excessively for services or supplies, and 3. Billing for services that were not medically necessary.
b. Fraud

i. How does the ACA address fraud and abuse? 1. Uses a web-portal to identify providers that have been terminated. 2. Increases provider screening and enrollment requirements. 3. Requires states to suspend Medicaid payments in cases where there are
credible allegations of fraud or abuse 4. Gives states the power to temporarily suspend activity among new
providers to prevent waste, fraud and abuse 5. Requires state Medicaid programs to establish Recovery Audit
Contractor (RAC) programs to identify and recover overpayments and underpayments.
6. Mandates the use of the Nation Correct Coding Initiative (NCCI) 7. Encourages data system enhancements to identify fraud and abuse.
Federal funds are made available to help states implement such systems 8. Requires that physicians document a face-to-face encounter (telehealth
permitted) with a Medicaid beneficiary before ordering home health services, medical supplies or equipment.
c. States cracking down i. Primarily other health care professions
1. Be careful to bill properly 2. Be careful of anti-kickback violations
a. The Anti-kickback statute prohibits, giving, receiving or soliciting any items of value, either directly or indirectly for the purposes of inducing or rewarding items or services that are reimbursable by the federal government.
b. Violators are subject to monetary penalties, imprisonment or both
ii. Safe harbor regulations 1. According to the Office of the Inspector General, safe harbor
regulations: a. “describe various payment and business practices that,
although they potentially implicate the Federal anti-kickback statute, are not treated as offenses under the statute.”
b. Examples include lease of space, lease of equipment, warrantees, discounts and many more
c. Each example has a number of stipulations that must be met d. A complete list of Safe Harbor Regulations may be found at :
http://oig.hhs.gov/compliance/safe-harbor-regulations/ V. Peer Assistance Program
a. Professional Recovery Network i. Established in 1981 by the Texas Pharmacy Association
ii. Optometry was added September 1, 2010 iii. Helps professionals, students and professional staff in the fields of pharmacy,
optometry, dentistry and veterinary medicine overcome potential impairment due to substance abuse issues or mental illness.
iv. The reporting and treatment are confidential v. The goal is to provide public safety while preventing disciplinary action against a
professional license. vi. The above criteria apply if the individual complies with their treatment program.
b. Referrals i. Self
ii. 3rd party iii. Investigator iv. Board Order
c. Contact information: i. PRN Hotline: 1-800-727-5152
ii. PRN Address: 6207 Bee Caves Road, Suite 120, Austin, TX 78746 iii. Website: http://www.txprn.com/