costing enaps using onehealth tool - unicef · pdf filecosting enaps using onehealth tool ......
TRANSCRIPT

Costing ENAPs Using
OneHealth Tool
Training Module
Developed by
Dr. Neil Thalagala (MBBS, MSc, MD),
Ministry of Health, Sri Lanka
South to South Collaboration for Health

1
Contents Background ..................................................................................................................... 4
Objectives of the training ................................................................................................. 5
The training approach ..................................................................................................... 5
About “ENAP_Sample” projection ................................................................................... 6
SESSION ONE ............................................................................................................... 6
OneHealth Tool and Costing Concepts ........................................................................... 6
1.1 One Health Tool & Costing Concepts .................................................................. 7
1.2 Installing the software .......................................................................................... 7
1.3 Setting up a new projection ................................................................................... 7
SESSION TWO ............................................................................................................. 12
Basic Configuration of OneHealth ................................................................................. 12
Projections .................................................................................................................... 12
2.1 Create program area/subgroup/intervention hierarchy ...................................... 13
2.1.1 Edit/Create programme areas ....................................................................... 15
1.2.1 Edit /create subgroups ............................................................................... 18
1.3 Customise interventions: ................................................................................. 20
2.2.1 Select default interventions ......................................................................... 20
2.2.2 Create custom interventions ......................................................................... 21
2.2.3 Assign interventions ...................................................................................... 24
2.2.4 Indicate delivery channel availability ............................................................. 26
2.4 Edit staff types ..................................................................................................... 27
2.5 Edit Facility types ................................................................................................. 32
2.6 Edit drugs & Supplies .......................................................................................... 33
2.7 Indicate MOH budget ........................................................................................... 33
2.8 Edit Currency and Inflation .................................................................................. 34
SESSION THREE ......................................................................................................... 35
Customizing OneHealth Modules .................................................................................. 35
3.1 Customization of Health Services module: Intervention costing .......................... 38
3.1.1 Specify Target Populations ............................................................................... 41

2
3.1.2 Specify population in needs .............................................................................. 43
3.1.3 Specify Intervention coverage ........................................................................... 44
3.1.4 Current stock .................................................................................................... 45
3.1.5 Treatment input ................................................................................................. 46
3.1.6 Specify delivery channels ................................................................................ 50
3.1.7 Intervention overview ...................................................................................... 51
3.2 Customization of Health Systems Module: Human Resources ............................ 52
3.2.1 Baseline data ................................................................................................... 52
A. Staff baseline .................................................................................................... 53
B. HR calculation options ....................................................................................... 54
C. Staff salaries & benefits .................................................................................... 54
D. Staff time utilization .......................................................................................... 56
E. Attrition and retention incentives ........................................................................ 56
F. Pre service training .......................................................................................... 56
G. Recruitment baseline ........................................................................................ 57
H. In-service training .............................................................................................. 58
3.2.2 Target setting .................................................................................................... 58
3.3 Customization of Health Systems Module: Infrastructure .................................... 61
3.3.1 Baseline data .................................................................................................... 61
A. Facilities ............................................................................................................ 62
B. Medical equipment ............................................................................................ 62
C. Facility furniture ................................................................................................ 63
D. Vehicles ............................................................................................................ 63
E. ICT equipment .................................................................................................. 65
3.3.2 Target setting ................................................................................................... 67
3.4 Customization of Health Systems Module: Logistics ........................................... 71
3.5 Customization of Health Systems Module: Health information system & Health
financing & Governance ............................................................................................ 72
3.6 Customization of Health Services module: Programme costing ......................... 72
Customization of: Programme management /Administration in other modules ............. 73
Impact module overview ................................................................................................ 74

3
Reviewing results of OneHealth .................................................................................... 75
Financial space overview .............................................................................................. 76
Budget mapping overview ............................................................................................. 76
Scenarios ...................................................................................................................... 76

4
Background It is observed that in Sri Lanka, Maldives, Nepal, and Bhutan, despite many advances in
child health programs, too many newborns continue to die in and around birth. In
response to this gap in health response, four countries are in the process of developing
Every Newborn Action Plans (ENAPs).
It is important that intervention scale up targets proposed during these plans should
have commensurate health system developments, so that increasing service demands
would have adequate skilled providers, infrastructure and material supplies.
The success of these developments depends on the availability of adequate financing
resources. Though, these financial requirements can be met in limited settings, in others
priorities and scale up targets have to be revised to account for financial constraints.
It is preferable that those who are involved in planning should have a sound awareness
and skills in health programme costing so that they prepare realistic and effective
ENAPs in the contexts of financial constraints. Accurate cost estimates of various
planned actions, especially if carried out simultaneously with planning, can help making
of feasible and realistic targets. On the other hand, costing requires plans to be focused
and prescriptive enough so that final outputs are clearly enumerated. Therefore,
conducting planning and costing together will have synergistic effects.
Considering above issues, UNICEF ROSA is organizing a capacity building workshop
on OneHealth Tool (OHT) based strategic planning and costing to enhance the planning
and costing capacity of experts, who are involved in EANP planning in above countries.
OneHealth Tool (OHT) is expected to encourage holistic planning and costing
approaches that simultaneously consider intervention scale ups, quality improvements
and health system developments. It is expected that after the training, local
counterparts, who will be making ENAP plans will have better knowledge and skills on
the process.

5
Objectives of the training The objective of this training is to:
1. To understand the costing approaches and analytical frameworks used in OHT
2. To impart knowledge and skills among participants on use of OHT in costing
health program and systems
3. To develop an initial versions of country specific ENAP cost projections that will
be further refined after returning to respective countries.
About this manual
This manual provides step by step guides related to this training course. It presents the
session details, and other detailed instructions that trainees should follow during next 4
days. Several other companion documents/files that will be used during the training are
included in the pen drive given to you.
The training approach We intend to use an imaginary ENAP for the purpose of learning. A completed cost
projection (“ENAP_Sample”) based on this ENAP is included in the pen drive given to
you.
We, the facilitators will help you to understand OHT functions and guide you on how to
make this kind of a projection in step wise manner. Over next 4 days you will be
producing a parallel projection named “ENAP_Practice” after learning the OHT.
In addition we will use sample projections to demonstrate some of the additional
functions of OHT. You can practice on these projections as well.
Each session will be accompanied by plenary presentations on thematic aspects and
demonstrations of relevant OHT functions. During the session you will be developing
the “ENAP_Practice” projection. While doing so. you can contemplate on how you can
customize the OHT to suit your country’s ENAP.
On the last day of training, you will develop an initial framework of the cost projection
based on your countries ENAP.

6
About “ENAP_Sample”
projection The sample ENAP of the country X proposes to scale up the following direct and
indirect newborn care interventions along with commensurate system improvements.
The interventions focused by the plan include:
Newborn Health Program
Antenatal care
1. Basic ANC (Iron, Folic acid,
Calcium supplementation,
Nutritional supplements,
investigations examinations,
Tetanus toxoid (pregnant
women), Syphilis detection and
treatment (pregnant women),
Vitamin B for mothers
Intra-natal care (Facility)
1. Management of Normal Labor
2. Management of obstructed
labor/LSCS
3. Antenatal corticosteroids for
preterm labor
4. Antibiotics for PRoM
Intra-natal care (Home)
1. Home deliveries and neonatal
resuscitation
Essential newborn care
1. Neonatal resuscitation
(institutional)
2. Provision of thermal care at birth
3. Early initiation of breast feeding
4. Hygienic code and skin care
5. Vitamin K
Care of sick newborns
1. Newborn sepsis management
2. Treatment of local infections
(Newborn)
3. Care of LBW/Pre mature
4. Feeding counselling and support
for low-birth-weight infants
Annual birth cohort of the country X is around 875,472 births. Nearly 4,186,013 under
five children are found in the country. Country X has a population of 53.3 Million.

2
Antenatal care is predominantly provided by midwives (70%) while 30% of mothers visit
medical officers serving at primary care hospitals named as station hospitals.
Seventy five percent of deliveries are reported as home deliveries of which 15% are not
having trained assistance. Other are attended by Midwives (80%) or Lady Health
Visitors (20%).
Twenty five percent of deliveries occur in hospitals. Of them (of this 25%) 10 % occur at
67 District Hospitals (CEMONC) and others are occurring at 660 Station hospitals
(BEMONC facilities) (60%) and 330 Township hospitals (CEMONC) (30%).
The ENAP plan indicates the following present and target coverage levels for the
interventions.
Intervention Hierarchy
Baseline coverage from impact module (2016)
Target coverage used to assess impact and intervention costs (2020)
Every newborn Program
Antenatal care
1. Tetanus toxoid (pregnant women) 50 80
2. Syphilis detection and treatment (pregnant women) 36.7 50
3. Basic ANC 60 80
4. Vitamin B for mothers 40 80
Intra-natal care (Facility)
1. Labor and delivery management 20 50
2. Active management of the 3rd stage of labour 5 50
3. Management of obstructed labor 5 15
4. Induction of labor (beyond 41 weeks) 80 100
5. Management of eclampsia (Magnesium sulphate) 40 100
6. Antenatal corticosteroids for preterm labor 40 100
7. Antibiotics for pPRoM 40 100
Intra-natal care (Home)
1. Home deliveries and neonatal
resuscitation
64 50
Essential newborn care
1. Neonatal resuscitation (institutional) 80 100
2. Breastfeeding counselling and support 50 95
3. Kangaroo mother care 30 95
4. Chlorhexidine 30 50
5. Vitamin K 10 70

3
Intervention Hierarchy
Baseline coverage from impact module (2016)
Target coverage used to assess impact and intervention costs (2020)
Care of sick newborn
1. Treatment of local infections (Newborn) 55 80
1. Feeding counselling and support for low-birth-weight infants 30 50
2. Newborn sepsis - Full supportive care 28 50
Maternal and child care is supplied by Midwives, Lady Health Visitors, Health Assistants
attached to 1320 Rural Health Centers (RHC) in the country. Antenatal clinics are held
at RHC premises. Around 60% of mothers are reported to attend antenatal care clinics.
The Director General of Health Services of the country X, 67, Regional Directors are
responsible for Governance and administration of the health system. Other health
personnel related to ENAP are given in the table below. In addition 2650 administrative
personnel are attached to various curative care institutions.
Needs assessment study conducted prior to EANP production highlighted that there are
no neonatologists in the country and pediatricians are covering for their activities it is
proposed in ENAP that 50 neonatologists will be appointed over next 5 year period.
Baseline HR * and infrastructure status in the country X
Institu
tio
ns
Med
ical
Offic
ers
Obs/G
yn
specia
lists
Ped
iatr
icia
ns
Neon
ato
log
ists
Nurs
es
Mid
wiv
es
Lady H
ealth
Vis
itors
Anesth
etists
Station Hospital (Primary) 660 2640 5280 1320
Township hospital 330 3960 250 50 3960 1320 330
District General Hospital 67 2010 100 80 0 2680 670 67
RHC 1320 6600 2640
(* the number staff reflect the numbers entering 2016)
The ENAP of the country X targets for the following infrastructure establishments.

4
1. Construction of a new newborn care rooms for each 100 township hospitals
situated in the hard to reach areas ( Average cost 22, 000,000)
2. Establishing a new midwife training school (800 m2)
3. Building 20 station hospitals and 40 RHC
4. 40 station hospitals need equipment replacement (average cost per facility
1,800,000 MMK)
5.
The cost of constructing one square meter will be 550,000 MMK. Average annual utility
cost of institutions are as follows:
Facility Amount(MMK)
Rural Health Centre 30,000.00
Station Hospitals 90,000.00
Township Hospitals 150,000.00
District General Hospitals 450,000.00
Regional directors office 200,000.00
Director Generals Office 300,000.00
Midwife training school 300,000.00
.
6. It is also planned to provide 100 ambulances; 20 in each year to selected
hospitals (cost of an ambulance is around 80,000,000 MMK / Fuel cost – 1000
MMK per liter, annual maintenance cost 5% of construction/ Driver annual salary
350,000 MMK)
7. One computer each will be provided to 100 TSP hospitals to maintain a newborn
health related data base.
8. ENAP also proposes to supply the selected list of medical equipment to RHCs
and Station Hospitals
ENAP proposes to increase the number of midwives by increasing the training of
midwives by taking necessary measures to increase the midwife training capacity. It is
proposed to increase the training enrollments by 50 trainees in each year until 2020,
where the 350 midwifery students will be enrolled.
To do that government is planning to set up a new training facility having 10 tutors
(annual salary 800000 MMK) and 10 admin staff (annual salary 400,000 MMK) and 20
supporting staff (Salary) 300,000 MMK. Remember to add these staff from the second
year where the new training facility will be started. Construction of the 800 square meter
building and supply of equipment, have to be completed within the first year. Therefore,
the new training center staff have to be working from the second year.

5
The ENAP proposes the following program management activities
1. Development of newborn information system
2. EMONC training for Station Hospital medical officers, PHMs and LHVs.
Organized as a cascade training.
3. Development of communication strategy and implementation
4. Piloting of neonatal mortality and morbidity system in 100 selected hospitals
5. Regular supervision of ENAP implementation by Bi Annual progress review,
quarterly district meetings
6. Evaluate the effectiveness of use of mother support group to promote breast
feeding and kangaroo mother care
7. Development and implementation of national guidelines on Essential Newborn
care.
There is a centrally operated M & E system that report the annual expenditure account
worth of 50,000,000 MMK and a national drug supply store (total running budget of
100,000,000 MMK).
Other details required for projection will be provided at relevant sections.

6
SESSION ONE
OneHealth Tool and Costing Concepts

7
1.1 One Health Tool & Costing Concepts
This topic will be covered as a plenary presentation.
1.2 Installing the software
A copy of OneHealth software is included in the pen drive given to you. Install the
software to your computer following the demonstration made by the facilitator. You can
download the latest version of OneHealth at:: http://www.futuresinstitute.org/ or the
latest beta version at: http://spectrumbeta.futuresinstitute.org/
Now let’s try to set up our first projection. First follow the demonstration and
proceed to set up a new projection & name it as “ENAP_Practice” and complete
the set up as instructed below.
1.3 Setting up a new projection
Create a new folder in your computer and name it as “ENAP_Practice”.
Now open OneHealth tool. Select the option of creating a new projection.

8
Give the projection the name: “ENAP_Practice”.
Set the Year Boundaries for your project within OneHealth as: a) First year: 2016
(this is the base year), b) (C) Last year: 2020
NOTE:
Entering these data means that you will produce costs for the 5 years of scale up (2016
- 2020).
Next, activate modules for use in your projection
OneHealth: Select all of the boxes
Click on the file tab “Impact Modules”. These are the modules that calculate the
demographic and mortality impact of your intervention scale up. However your cursor
over each of the names such as “Demographic Projection (DemProj)”. Read the
descriptions of each impact module.
Select all except for LiST Costing, HIV Incidence (Goals) and the Resource Needs
Model
Then select a country (Myanmar) from which to retrieve demographic and other default
data:

9
Click OK and then Next at bottom of the screen.
Say OK for the following message if it comes.

10
Click next and choose:
Programme area for Programme or Delivery Channel mode
Click Next
Choose target setting for Human resources based on target setting or policy decisions.
Click next costing templates for Logistics costing templates or Logistics
optimizer
for the questions asked in next 3 dialogues.
You should now see the Configuration editor of the OneHealth Tool as shown below.
This editor is also available from the main menu: OneHealth Configuration icon that is
circled above.
Now close the dialogue.
Observe the icons by clicking OneHealth Tool & Home tabs.
Click about, Options, and exit

11
OneHealth data is saved to your hard-drive only clicking save or save as. Clicking OK
in any editor only saves the data to virtual memory.
Now save the projection and reopen it.
You can open more than one projection at a time. However, the projection specifications
have to be the same. You have to close the open projection before if you want to open
another projection with different specifications.

12
SESSION TWO
Basic Configuration of OneHealth
Projections

13
2.1 Create program area/subgroup/intervention hierarchy
During OneHealth configuration you can stipulate the main characteristics of the health
system to be costed in OHT. i.e. What kinds of programs sub programs, what kinds of
interventions are included in programs, who are the service providers, what types of
institutions are involved etc.
Hence, OHT configuration allows us to input most basic health system blocks related
information needed for projection, they include:
1. Programme area: subgroup hierarchy,
2. Types of interventions that are implemented under this hierarchy.
3. Various categories of human resource types/staff who implement those,
4. Infrastructure/Facility types used in the programme.
5. It also allows us to customize drug and supplies of the programme,
6. Adjustments for currency changes and inflation
7. Select a feature that allows us to calculate the cost as an increment to the
total health budget.
NOTE: Items 3 to 5 can also be accessed in health systems module as well.
Open/ focus the ENAP_Practice projection. Click on the menu item, Health
Services, revealing the icon banner shown below.
Click on OneHealth configuration.

14
You can see editing icons for programme areas, subgroups and interventions. Select
default interventions, manage custom interventions, Organize interventions and Delivery
Channel Availability.
OneHealth comes with default programme areas, sub groups and interventions.
However, they may not represent the health programmes structure of the health system
you are trying to cost. So you have to edit these items to suit the health system,
programs to be cost.
You can:
1. Use default programme areas as it is or edit them to suit your programme. You
can also add new ones as well

15
2.1.1 Edit/Create programme areas
Click on Edit programme areas.
You can see the following default interventions in the data editor:
Maternal/new-born and reproductive health
Child health
Immunization
Malaria
TB
HIV/AIDS
Nutrition
WASH
Non-communicable disease
You can rearrange and add programs in this editor so that you can ensure that your
new projection resemble the health system you are going to cost.
The following steps will walk you through process by which you can create program
areas suggested on the ENAP_ Sample projection
What is the program, subgroup and intervention hierarchy you would select for
the country X ENAP plan? .Make a sketch of it in a piece of paper.
Now look at the diagram shown below. Is your sketch different

16
There is no hard & fast rule for this. You can create the hierarchy the way you want.
Keep in mind how you would like result to be displayed
Think of another way of organizing these interventions to packages
Now let us try to create the above program /subgroup/intervention hierarchy in
Add a new program area: Every New-born Program
Sub groups
Program areas

17
Click OK.
Now you can either chose to Delete other Default programme areas or
leave them as it is. If you delete a program area, the tool will ask you to
reassign the interventions belongs to the deleted programme area to an
existing program areas. It is practically better to wait till intervention
assigning is completed to delete un necessary program areas.
Note that even if you do not want them some programme areas (TB/HIV,
NCD) cannot be deleted. TB program area can be deleted but cannot be
edited. You can leave them as it is. They will not be cost as long as one of
the parameters of intervention cost is left sero or by assigning
interventions belong to them to delivery channel that will not be costed.
By now you have added the new program area: Every New-born Program areas to suit
your projection.
Now proceed to edit sub groups.

18
1.2.1 Edit /create subgroups
Click on the edit sub groups icon.
The dialogue box shows a menu of different programme areas under which subgroups
to be created or edited.
Click ok. Then you see a new editor in which you can add subgroups of
your choice. You can create /edit/ delete sub groups. Now create all the
sub groups you want under programme area: Every New Born Program:
what are they?
……………………………………….
……………………………………….
……………………………………….
……………………………………….
……………………………………….

19
Once you create all subgroups under a programme area, click OK.
Now you have completed configuring OneHealth to include the program area –
subgroup framework required to assign interventions. See the diagram again

20
Next step is the configuration of interventions under the Programme areas: Subgroup
hierarchy you just created.
1.3 Customise interventions:
OneHealth comes with various default interventions. You can select them as they are
(with or without editing their contents such as treatments, providers etc.) if they are
appropriate for your purpose.
Even though you can create the whole intervention list out of scratch. However, it is
advantageous to use the existing ones as much as possible as they are linked to impact
module programmes and their impacts will be used in the final outcomes. Customizing
and linking new interventions to impact modules may be a complex task though not
impossible.
The interventions that are not found in the default list have to be created.
2.2.1 Select default interventions
In ENAP_SAMPLE projection we are going to use both default and custom
interventions.
Go back to page 6. It presents the set of interventions identified in the ENAP of the
country X.
Now let us going find out, which of the above interventions are found in default lists of
interventions.
Now click on select default interventions
Observe how the list is organized

21
Open an excel file and make a list of default interventions that may be related to
the sample ENAP_projection introduced above
Observe the excel file comparison of default and required interventions
As you can see we may have to adapt/ modify some of the default interventions or
we may have to use more than one default interventions to denote some of the
planned interventions (e.g. Management of normal delivery)
Now try to select the default interventions you intend to use for this practice
projection. First deselect all interventions and then go on selecting the ones you
have chosen
Facilitator will demonstrate this step
2.2.2 Create custom interventions
Once selection of default interventions is over, you have to create your own
interventions
Find out what are the interventions that are required to be created as they are not
already available in OHT
……………………………………….
……………………………………….
……………………………………….

22
Click on manage custom interventions dialogue
Click on create interventions
Add a name of an intervention to be created under relevant programme area
and sub group

23
Click OK

24
Go on adding all custom interventions selected for the model programme.
Save your projection.
NOTE:
You can observe the completed projection, ENAP_Sample by opening it along with
ENAP_Practice. It will be used for demonstration purpose while we progress.
Go to the ENAP folder in your pen drive and open the ENAP_Sample projection.
Remember you can open it as it also has the same specifications as ENAP_Practice
projection.
You can see both projections are open. The one active appears in bold. There is also a
set active icon in the main ribbon.
2.2.3 Assign interventions
Next task is to make sure that these interventions are placed according to the program
area: subgroup hierarchy of the ENAP. You can change the assignment of interventions
through assign interventions icon.
Focus ENAP_Practice projection, Click on Assign interventions. You see a list of
interventions by programme areas: subgroups. Some of the interventions are still
not appropriately allocated. They are housed in the original default areas. You
have to move them to the appropriate place in the hierarchy.

25
Browse down to observe the Every Newborn Program section in the list. Observe
how Program areas and subgroups are organize
You can see only the newly created interventions are in this section
Now you have to move the selected default interventions to appropriate
subgroups
You can do this by selecting interventions to move and clicking move intervention
button.
Note that when defining we put newly created interventions in their respective
program area: subgroup hierarchy. Hence, you do not have to move them.
Now complete moving the interventions.
Well done. Now you have completed assigning interventions. Browse through the
assign intervention dialogue and see whether everything is alright. There should not be
interventions appearing in other programme areas.

26
2.2.4 Indicate delivery channel availability
One health allows to disaggregation of cost by delivery channels (Community,
Outreach, Clinic and Hospital). In order to do that you should indicate to the tool what
proportions of a particular interventions deliveries directed through each channel.
Click on Delivery channel availability button
Observe the how this function is organized.
Now contemplate on; through which delivery channel/s the selected interventions
are delivered in the field.
Organize the delivery channel availability of “ENAP_Practice” file. You can get
directions by reviewing “ENAP Sample” file.
Close the dialogues and save the projection.

27
2.4 Edit staff types
Again click on the “OneHealth Configuration”.
Four more areas to be configured, before moving to other detailed inputs related to
modules.

28
Click on “Module specific” tab. Unclick “Use only default staff types” and “Use
only default facility types”
Click on “Edit staff types”. Select default staff types except one and press
delete.

29
Now check which of the following types of human resources required for the
model Every New-born care programme is already available in the default
staff list.
i. Obstetricians
ii. Anesthetists
iii. Pediatricians
iv. Neonatologists
v. Medical Officers
vi. Nurses
vii. Midwives
viii. Lady Health visitors
ix. Health Assistants
x. Regional directors
xi. Director General of Health Services
xii. Administrative personnel
xiii. Tutors
xiv. Admin assistants
xv. Supporting staff
Prepare a list of those who are absent in an Excel sheet column
The copy & paste them to the staff types editor by right clicking

30
Now click next and associate custom staff types with default staff types and
designate appropriate staff division. You have 2 options.
You can either add new staff types directly to treatment list or associate them
with the most resembling default staff type or may use other if no existing
default category is appropriate. (Only service provider types can be directly
added)
Then you have to indicate whether the custom type is service provider or
management /support staff.

31

32
2.5 Edit Facility types
Now click the edit facility types and add a customized list of facility types
relevant to model Every New-born Program.
Read the section describing ENAP sample projection (Page 3) and identify
what are the infrastructure facilities of projection. Think about administrative
facilities as well.
……………………………………..
……………………………………
……………………………………..
………………………………………
………………………………………..
Type this list in Excel and paste it in to “edit facility type” editor.
Now proceed to “Next” and match “default facility type”, “’Default delivery
channel” and “ Support facility” fields.

33
Now you have completed configuring basic information about interventions, staff types
and facility types. Three more actions have to be conducted to complete the basic
configuration of the projection
2.6 Edit drugs & Supplies
OneHealth configuration icon can be used to customize the drug list. However, it will be
easier if it can be done when adding “treatment inputs” to respective interventions.
2.7 Indicate MOH budget
Now look at the “Budget” icon. Leave it intact as we do not use this feature. Click the
hyperlink to see what it is used for.

34
2.8 Edit Currency and Inflation
Now click on currency and inflation on tab and adjust currency values and
inflation rates.
This ends the basic configuration of OneHealth Tool. Now we have to proceed to
customize the other inputs necessary for various cost and impact projections.
Save the projection once again.

35
SESSION THREE
Customizing OneHealth Modules

36
Reading exercise :
One characteristic feature of OneHealth is that the inputs pertaining to different modules
are entered in different places. You have to have a clear understanding of this feature in
order to understand the analytical logic of this software.
In OneHealth, costs pertaining to different health system blocks are calculated
separately in different modules. All these modules need specific inputs to base their
calculations. They are entered at different menus or portals of OneHealth.
Cost of providing drugs and supplies for interventions and cost of background activities
required for health programming such as providing specific human resources (e.g
special consultants/project staff), cost for training, supervision, monitoring and
evaluation are calculated in Health Services Module.
Human resource costs, infrastructure costs, logistic costs, Health information system
costs and governance costs are determined through the Health Systems Module.
In addition each of these health system sub modules has options to enter the costs
required for sustaining the particular health system block or its function. They are
identified differently in different modules. For example Programme costing of Health
Services module and Administration of Governance module and Programme
management of other modules serve more or less same purpose: i.e. that they imply
the cost vested on running cost or cost needed for sustaining the particular health
system block or function.
Impact module provides population numbers in which the costing is based. In addition
impact modules provides various output or results of their own.
The following list shows the organization and names of different input portals (menus) of
OneHealth tool. You have to carefully customize these basic data before reading cost
projections.

37
Basic data input portals (menus) of OneHealth.
1. Health services module:
a. Programme /Channel
analysis
i. Intervention costing
ii. Programme costing
2. Health systems module-
a. Infrastructure
i. Baseline data
ii. Target setting
iii. Programme
management
b. Human resources
i. Baseline data
ii. Target setting
iii. Programme
management
c. Logistics module
i. Baseline data
ii. Target setting
iii. Programme
management
d. Health information system
i. Baseline data
ii. Target setting
iii. Programme
management
e. Health financing
i. Direct costs
ii. Programme
management
f. Governance
i. Baseline data
ii. Administration
g. Financial space
i. Baseline data
3. Budget mapping
a. Global fund summary
b. Edit budget categories
c. Map budget categories
d. Edit funding sources
e. Map funding sources
4. Impact modules
a. DemProj
i. Projection
parameters
ii. Demographic data
b. AIM
i. Programme
statistics
ii. Eligibility for
treatment
iii. Advance Options
iv. Incidence
v. Sex/age pattern
c. TB
i. Epidemiology
ii. Policy goals
d. List
i. Configuration
ii. Health, Mortality,
economic status
iii. Coverage
iv. Effectiveness
e. FamPlan
i. Configuration
ii. Family planning
goal
iii. Distribution of
fertility related risks
Browse through the different modules and be familiar with the above menus.

38
3.1 Customization of Health Services module: Intervention costing
Costs pertaining drugs and supplies and the cost incurred on sustaining a particular
programme (payments of programme specific staff, in service training, supervision costs
etc...) Are calculated from the Health Services Module.
In this section we are studying how basic data required to calculate drugs and supplies
cost are entered through the Intervention costing dialogue boxes of the Health services
module ( Programme or Chanel analysis).
Let’s now try to customize OneHealth Intervention costing menus to suit model Every
Newborn care programme.
Go to health services tab and click on Programme or channel analysis.
Click on the first ribbon icon. You can see Programme areas
Remember the inputs of this section are programme specific and you have to repeat
inputs for each programme separately.

39
Select the Everynewborn program and then click on intervention costing.
Observe the various inputs.
You can see several submenus. Inputs under these menus provides data required for
calculating the cost pertaining to drugs & supplies used for the interventions of different
programme areas.

40
Target population (TP) means the population group for whom the intervention is
relevant. It can also be defined as population across which the population in need for
intervention is defined. For example, the population in need for comprehensive
emergency obstetric care would be defined relative to the respective TP: The number of
women who are pregnant
Population in need (PIN) is the percent of TP who should be receiving the intervention,
per year.
Intervention Coverage (IC) is the percent of PIN who are provided with intervention or
coverage of intervention
Delivery channel (DC) is the percent of clients for a particular intervention, who receive
the intervention through a specific delivery channel.
As described earlier in the introductory presentation, Health Services module calculates
the costs incurred drugs & supplies used to deliver interventions.
Above four parameters are used to assess the number of cases for whom an
intervention is delivered
The basic equation for calculating the number of the cases treated at delivery
channel/facility type j at time t is as follows:
Num_Casesi,j,t = IC i,t * PIN i,t * DC j,t * TP i,t
In more simple terms:

41
(Num_Cases = IC% * PIN % * DC %t * TP # )
For example
Intervention TP PIN IC DC Number of cases
BCG vaccine 350,000 (Births)
100% 95% 100 % (all hospital)
350000 *1* 0.95*1 (332,500)
ORS
1,750,000 (1-59 months)
350% (Avg episodes year=3.5)
60% 100% ( all filed)
1,750,000*3.5*0.6*1 (3,675,000)
IV severe diarrhea
1,750,000 (1-59 months)
350%*1% (1% of diarrhea cases will be severs
100% 100% 1,750,000*3.5*1*1 61,250.00
NOTE:
Remember when you multiply a % it should be converted to a proportion first.
3.1.1 Specify Target Populations
Save & Close all open projections.
Now open a new projection with default interventions. Give a name for the
projection (Observe), save in a new folder on your desktop. Select the
country. Choose your country and comply with the requests of the tool and
finish the projection and close the configuration dialogue. Go to Health
service module and then in to intervention costing module.

42
And click on target population and browse through various target populations in
different program areas.
Open Help icon. And read the contents. Close target population icon and click on
population in need. Check the default values.
Close the new projection. Tell “no” to save.
Open ENAP_Practice projections again

43
Now customize target populations for all your interventions. Remember TP
means the population group for whom the intervention is relevant.
Note that there is an option for direct entry of population that disregards projected
population numbers.
Remember to look repeatedly in all programme areas.
3.1.2 Specify population in needs
Now, try to customize PIN related to all interventions. Remember PIN is the
percent of TP who should be receiving the intervention per year.
Pay special attention to defining PIN in child birth management, and whenever not all
target population does not require intervention.
Pay attention to the equation described above. Read Intervention Assumptions
document in the pen drive
You can examine “ENAP_Sample” to overview the PINS used there.
Special considerations in enumerating PIN will be discussed by your facilitator at
this point

44
3.1.3 Specify Intervention coverage
Intervention coverages are required for both estimating mortality impact and
intervention-related costs. Coverage should be adjusted rationally over projection
period. Different types of interpolations are available (e.g., Linear, S-Shaped, and Front
Loaded, exponential).
The calculated frontier coverage from Bottleneck Analysis is noted for your reference.
When you have completed your coverage scale-up plan, these values should be sent to
impact modules by clicking “Transfer coverages to impact modules”.
Only by clicking this button will ensure your changes to interventions scale up will be
reflected in impact module coverages. Coverages for interventions without calculated
impact (marked in red) are saved automatically in the Intervention Coverages editor.
Click on Intervention overages.

45
Click the help button and read. Close it click show all years of scale up.
Try to add current coverage. Then decide on end line coverage and practice
interpolation, duplication functions.
Right click and observe functions available.
Transfer your changes to impact modules.
Complete the coverage for “ENAP_Practice ” projection and observe
ENAP_Sample and compare.
3.1.4 Current stock
This feature is not well developed and will not be used. Click on it and read the
description.

46
3.1.5 Treatment input
As you have already learned OneHealth uses the inputs from TP, PIN, and IC to
estimate the number of annual subjects who needs different interventions. Inputs put in
from the Treatment input menu will be used to calculate the average drug & supply cost
per a case.
Drugs & supply cost for a particular intervention is determined by multiplying this figure
by the number of cases calculated by formula shown above (Num_Cases = IC% *
PIN % * DC %t * TP # ).
Focus on ENAP_Practice and open Intervention costing: treatment inputs:

47
You can see some figures are filled for default interventions you have selected earlier.
Observe the display heading” Average drug and supply cost for case.
Now double click on one of the filled cells in labour and delivery management
row.
Observe the detailed treatment inputs. Try to understand how the total average
cost for labour and delivery management at clinic level is computed. Different
rows show various drugs and supply items required for a particular intervention.
The last column shows the cost for an average case.
All the row total of the different drug/supply items of particular interventions is summed
to calculate the average drug & supply cost per a case. Observe the editor carefully.

48
Now close the box and open the box relevant to Antibiotics for PROM.

49
Note that row totals are weighted for percent receiving the item. For example, at a
glance one may think, if units for case is 42 and Unit cost is 14.92, then cost per case
should be 42 x 2.07 =626.64. However, it is shown as 501.46. That is because only 80
% of cases are getting Amoxicillin.
Remember, the number of cases equals to 5 % (PIN) of all pregnant mothers(TP).
However, only 80% of this number of mother will need antibiotics. Therefore 626.64 is
multiplied by 80% to get the 501.46.
Now click on medical personnel and outpatient /inpatient tabs. Observe, how the
figures are entered.
Now let us try to customize treatment inputs editors to suit Sample Every
Newborn Program.
Please note that before completing this section you should be aware of the standard
treatment/management protocols (Drugs, other supplies, Investigations, Dosage
schedules) and the unit costs of all materials used. This should be found out from the
health system information.
In order to save time you can observe the sample treatment protocols used in the
ENAP_sample file.
Make sure both files (ENAP_Sample and ENAP_ Practice) are opened.
Copy the treatment inputs of both projections in to a new excel sheet in parallel
manner so that you can compare them easily.
Study each protocol in your group. See whether they are different form each
other and also from what you already know.
Remember that you have to use standard protocols approved by your MOH
when you do the actual projection of your countries ENAP. The protocols used
here are OHT defaults and some adaptations based on country experience.
Now complete treatment inputs including staff time and visits and inpatient days.
Observe the additional functions in the treatment input editor. You will have
demonstration of the use of these features.
Try to practice them for yourselves.

50
3.1.6 Specify delivery channels
OneHealth needs to be informed through which channel the delivery of an intervention
takes place. The tool has several default channels.
Those channels indicated with an asterisk will not be cost. So if we want to ensure
some intervention not be cost. One way is to set its delivery channel to one of them.
Focus ENAP_Practice projection. Go to intervention costing: delivery channels
menu.

51
Ensure all your ENAP model interventions are channelled through your intended
channel ( Community/Outreach/clinic/Hospital). Note that percentages should be
added to 100. And you have to repeat the process for both baseline and end
year.
3.1.7 Intervention overview
Intervention overview allows you to check all your intervention costing inputs through a
single screen. So that you are ensured all inputs are in line with your plans.
Focus ENAP_Practice projection and observe the screen.
This brings to the end of intervention costing inputs. Now we have to customize
programme costing inputs.

52
3.2 Customization of Health Systems Module: Human Resources
Human resources module cost human resource costs. Several baseline data items have
to be provided here.
3.2.1 Baseline data
Focus on ENAP_Practice projection. Go to Health System module. Click,
Infrastructure and then Baseline data.
Click configuration of staff types. As you can see from the figure below. Still all
default program staff types are also remaining. You can delate them to make
reduce the clutter of the editor as well as outputs.

53
A. Staff baseline
Click on staff baseline. Observe how staff types are appearing in each tabs;
Facility, Admin district, Admin Regional, Admin National

54
Now add the staff baseline numbers based on model Every Newborn program.
They are enumerated in the section “About ENAP_Sample Projection” (Page 5).
You can observe “ENAP_Sample” file also.
Add the baseline staff numbers accordingly. BE MINDFUL ABOUT LEVELS OF
THEIR WORK (Facility, Admin Regional …etc..)
B. HR calculation options
Click on Human resource calculation options
As you can see there are 2 main options for calculating HR requirement. For the
initial learning we use the first method. However, facilitator will describe and
demonstrate how to compute HR results based on policy options.
C. Staff salaries & benefits
Now focus on salaries and benefits editor. As you can see 4 parameters have to
be added in this section. In reality you have to get these data from the accounts
departments.
NOTE:
This editor can be used with Annual Salary alone also. As you know different
people in the same staff category may have different annual salaries. So the
practical way is to get the median salary (50th percentile) of the staff category and
use it for calculation. Depending on the age distribution of the staff you may shift
the annual salary to another percentile as well.

55
Not that numbers of some of the staff categories are circled. Their annual salaries are
adjusted to reflect their contribution to Newborn Care related activities. You can do it by
multiplying their annual salary by respective proportional contributions. See table below
for details
Health service providers Proportional Contribution to ENC in time Annual Salary Adjusted salary
Anesthetists 0.1 1,500,000.0 150,000.00
Lady Health visitors 1.0 400,000.0 400,000.00
Medical Officers 0.3 750,000.0 225,000.00
Midwives 1.0 450,000.0 450,000.00
Neonatologists 1.0 1,500,000.0 1,500,000.00
Nurses 0.15 475,000.0 71,250.00
Ob\Gyns 0.8 1,500,000.0 1,200,000.00
Pediatricians 0.3 1,500,000.0 450,000.00
Health management and support personnel
Administrative personnel 0.1 400,000.0 40,000.00

56
Director General of Health Services 0.1 2,000,000.0 200,000.00
Regional directors 0.1 1,750,000.0 175,000.00
Complete adding salary details to “ENAP_Practice” projection
D. Staff time utilization
Close the dialogue and click on staff time utilization. Observe headings. How would you
calculate % of time spent on activities other than training and service provision?
Check the ENAP_Sample projection and complete the staff tie utilization table in
ENAP_Practice projection.
E. Attrition and retention incentives
Open these two dialogues and observe. Meaning of them will be discussed. Check in
ENAP_Sample, to see how retirement incentive is being managed for midwives to retain
them for extra time (5 years) as a strategy to reduce staff draining.
F. Pre service training
Through this menu we can add the basic data required to cost the pre service training
costs of the human resources of the programme.
Add the following parameters for pre service training of PHMs.

57
Now open the recruitment baseline
G. Recruitment baseline
Observe the column headings
Add the following parameters and interpret the auto generated numbers

58
H. In-service training
In-service training here means non programme specific training. E.g efficiency bar
courses, English courses etc.. You can create training types and add cost and numbers
by staff type.
Open the dialogue and check.
Now we have completed baseline data customization.
3.2.2 Target setting
In this section we can adjust the target for increase of staff over years.
Focus on ENAP_Practice projection and observe how data are organized.
In configuration menu check what type of target setting methods are used. Read
help to get more details.

59
Next 3 menus can be used to set up scale up plans for increasing the number of
workers.
Fill the data using the following description.
Ensure all the staff except Obstetricians, pediatricians, and midwives in the system are
remaining in the system by recruiting to cover retirements and other types of attritions.
The ENAP plan to increase the number of Obstetricians and pediatricians to 400 and
200 respectively by 2020. The increase will be linearly interpolated.
Read about the method of scaling up in the OHT help
ENAP proposes to increase the number of midwives by increasing the training of
midwives by taking necessary measures to increase the midwife training capacity. It is
proposed to increase the training enrollments by 50 trainees in each year until 2020,
where the 350 midwifery students will be enrolled.

60
To do that government is planning to set up a new training facility having 10 tutors
(annual salary 800000 MMK) and 10 admin staff (annual salary 400,000 MMK) and 20
supporting staff (Salary) 300,000 MMK. Remember to add these staff from the second
year where the new training facility will be started. Construction of the 800 square meter
building and supply of equipment, have to be completed within the first year. Therefore,
the new training center staff have to be working from the second year.
The following table will describe how to estimate the target number of midwives in each
year after adjusting for retirements and new recruitments.
Year 2015 2016 2017 2018 2019 2020
Remaining at the end of year 9910
Number entering to 2016 9910 9807 9755 9753 9799
Number retiring during 2016 (2.5%) 248 245 244 244 245
-248 -245 -244 -244 -245
Average number of retiring during the year 124 123 122 122 122
-124 -123 -122 -122 -122
Number recruited 145 193 242 290 338
Avg. Number paid during the year 9931 9878 9875 9921 10015
Number entering the following year 9807 9755 9753 9799 9892
Review it to understand the logic of calculations. These will be explained by the
facilitator.
Complete the staff target setting in the ENAP_Practice file.
Compare your values with those of ENAP_Sample and find out reasons for
differences
Remember to repeat this process in all levels (Facility, Admin district etc..)
Now set up scale up target for Midwife training. To increase the enrolment by 50
trainees in each of the subsequent years. Remember to add target graduation
while adjusting for failure rate
Add the new recruitment targets for training center staff. See description above.
Remember to enter all calculation parameters of HR types.
Keep a note to add the cost of establishing new training center to the
infrastructure costs.

61
3.3 Customization of Health Systems Module: Infrastructure
3.3.1 Baseline data
Focus ENAP_Practice file go to Health Systems: Infrastructure: Baseline data
You can see 7 sub menus from configuration of facility types to ICT equipment. You
have already configured facility types while you did basic configuration.
Delete unnecessary default facilities from the facility configuration editor
Go to facilities.

62
A. Facilities
Observe headings. Go through all tabs.
Read the section “About ENAP Sample” section and prepare a list of
infrastructure additions proposed in the ENAP.
Browse through “ENAP_Sample file and try to understand the values are entered
in the context of respective infrastructure additions.
This section will be described by the facilitator.
Pay special attention on how to adjust for partial contributions of shared
resources.
Now customize the ENAP _Practice projection accordingly.
Now we have completed customizing facility details according to the ENAP
infrastructure proposals.
B. Medical equipment
The data required for calculating the medical equipment used in facilities are entered
here. Either you can select them from the default lists provided or load your custom
lists.
Medical equipment are added with constructions. In addition 1/nth ( n= work life) of
medical equipment are bought each year.

63
Open ENAP sample projections. Go to Infrastructure: baseline: medical
equipment.
Observe entries. See how entries related RHC and Station Hospitals are entered
here. Customized csv files with special list of items meant for RHCs and station
hospitals are entered to the ENAP Sample file. No medical equipment is
specified for other centres.
Observe the CSV files by opening them. They are provided in the pen drive
Load these files to ENAP practice file and complete other entries related to
medical equipment
C. Facility furniture
Customization of this section is exactly similar to the previous section
Observe the ENAP_Sample projection. Default values in the OHT is loaded in to
Station hospital and RHCs.
Do the same in the ENAP_Practice file.
Check the infrastructure summary section in the results.
D. Vehicles
Go to vehicles menu and add aa ambulance
Click next and add the following.
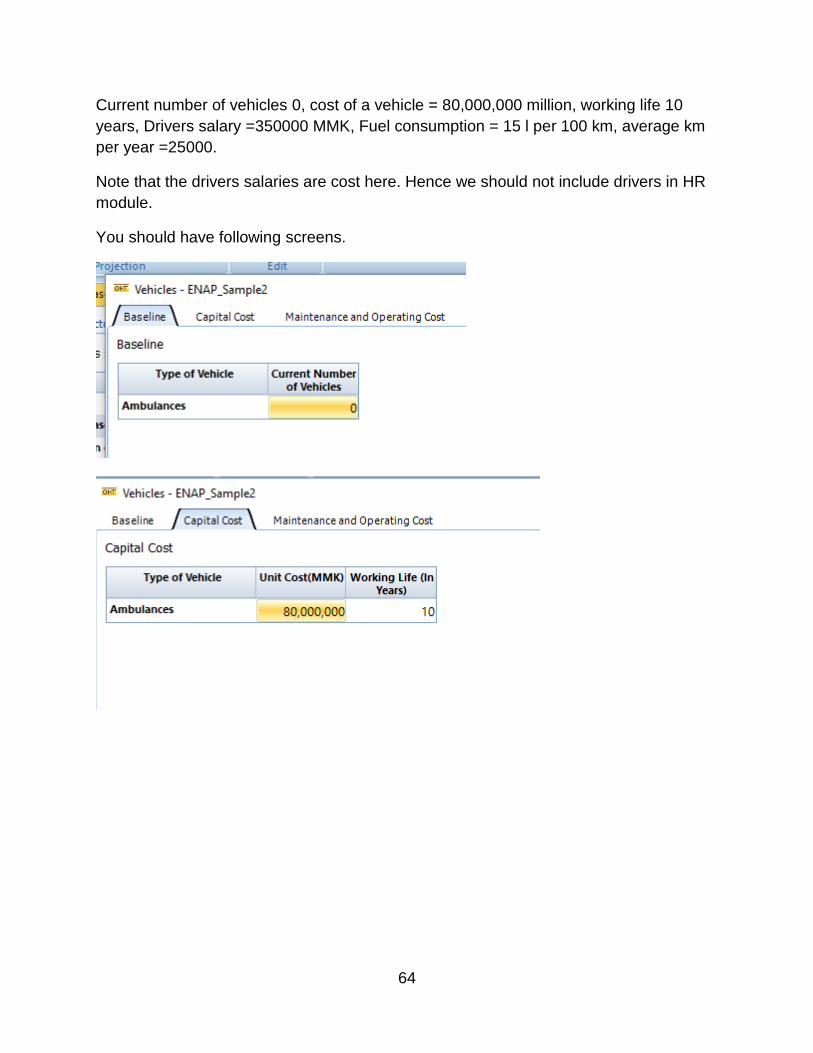
64
Current number of vehicles 0, cost of a vehicle = 80,000,000 million, working life 10
years, Drivers salary =350000 MMK, Fuel consumption = 15 l per 100 km, average km
per year =25000.
Note that the drivers salaries are cost here. Hence we should not include drivers in HR
module.
You should have following screens.

65
E. ICT equipment
Adding baseline data for ICT equipment are similar to vehicles.
Add the following data in ENAP_Practice projection.
Currently 0computers are available
Cost =1,500,000 MMK, working life 3 years
Operating cost 3%, repair cost 2%
You should have the following screens:

66

67
This ends baseline data customization of infrastructure module.
3.3.2 Target setting
Go to Infrastructure: target setting: configuration menu. And adjust the
configuration as follows:
You have to set targets for the following

68
Now open the target based on existing plans where you can put targets to build
new infrastructure.
Depending on how you set configurations the dialogues available will differ. Based on
the configurations you made: the following dialogue box will appear.

69
You can enter the number of facilities targeted to be operational in each year and get
the tool to calculate the number of facilities that should start construction in each year. It
will be based on the entries you mad in the upper box and the duration specified for
construction in baseline data: facilities.

70
Next is to add the rehabilitation targets. You can specify the number of facilities needing
small, medium and large scale rehabilitations and number of facilities that needs
equipment replacement and the respective costs have been already added in baseline
data.
Focus ENAP sample projection and add the following data for medium scale
rehabilitation and equipment replacement.
Try to understand the following
1. The new constructions ( 20 Station hospitals, 40 RHCS, and Midwife
training centre is entered as new constructions and they are associated
with medical equipment furniture lists
2. Newborn care rooms in 100 Station hospitals are entered as large scale
rehabilitations
3. Equipment replacement in 40 station hospitals are entered as equipment
replacement
Carefully observe how baseline values and targets together provides the
calculation logic over years.

71
This section has some known conflicts that require reorganization of results.
They will be explained by the facilitator.
After understanding the section complete the ENAP _Practice file.
3.4 Customization of Health Systems Module: Logistics
Logistic module can calculate expenses incurred in distribution of commodities, cost
pertaining to safety stocks, wastages etc.. and maintaining logistic system. Is has 4
types of baseline data to be adjusted as indicated in the following screen shot. .
You can add, edit warehouse list, and operating costs. The details on vehicles used for
logistic purposes also added here. Baseline data on warehouse workers also added
here. This section is quite simple.
Go to ENAP Sample Practice_ projection and see how these menus are
customized.
Your facilitator will explain how this section works.
Try to complete the ENAP_Practice section with the supervisor
The drugs supplies icons found in the baseline and target settings sections of logistics
module can be used to add additional supplies that are not related to interventions.

72
Amount of drugs purchased for making allowances for safety stocks and wastages can
also be adjusted here.
For example if the programme provides UNIFORMs to Midwives and LHVs, the data
related to cost of purchasing of Uniform cloths can be added here. In addition, the
materials given for each health worker (e.g ambu bag for midwives), or institutions can
be added here.
3.5 Customization of Health Systems Module: Health information system &
Health financing & Governance
These 3 modules are relatively simple and still in the process of development. We are
not going to customize them for ENAP model. These actions mostly concerns over all
health system of the country not only ENAP. If you want to add any costs associated
with Information system or governance expenses they can be added through the
Programme costing/management editors of other module.
However use of these sections will be explained to you by the facilitator
3.6 Customization of Health Services module: Programme costing
Programme costing inputs concerns the specific inputs related to organization and
functioning of a programme. These are different form drugs and other commodities,
infrastructure and general human resources. The default cost items are in built to the
OneHealth. You can select the options require for your programme and add any other
item.
1. Programme-Specific Human Resources
2. Training
3. Supervision
4. Monitoring and Evaluation
5. Infrastructure and Equipment
6. Transport
7. Communication, Media & Outreach
8. Advocacy
9. General Programme Management
10. Other

73
OneHealth distinguishes 2 types of human resources. Programme specific human
resources and Health system staff. In Sri Lankan context, if you hire a consultant who is
not currently not an employee of the Ministry of health can be an example of a
programme specific staff. The inputs related to programme specific staff goes in
programme costing menu where as those related to general staff such as Medical
officers , Midwives go as Human resource inputs.
Focus on MCH_Practice file and observe the program cost editor of the health
services module.
Review the program activity list of ENAP given in the section “ About
ENAP_Sample Projection.
Your facilitator will explain how you should customize this section to cost these
program activities.
Afterwards, do it by your slef in the ENAP_Practice file.
Customization of: Programme
management
/Administration in other
modules An editor somewhat similar both in structure and purpose is available from health
systems modules.
i. Infrastructure: Programme management
ii. Human resources: Programme management
iii. Logistics module: Programme management
iv. Health information system: Programme management
v. Health financing : Programme management
vi. Governance :Administration
We are not going to use these editors in MCHFP model costing.
However their uses are explained to you by a facilitator.

74
Impact module overview
OHT is associated with very sophisticated impact assessment tools.
These sections will be described using examples and you can also observe the features
by perusing the ENAP sample file.

75
Reviewing results of
OneHealth Now we have completed customizing most important baseline data in various
modules and set targets at relevant points. It is very easy to review results. Just
go to result sections in your ENAP Practice File and check results. And also
check in summary and standard outputs.

76
Financial space overview
Budget mapping overview
Scenarios
These 3 sections are quite complex and May not even be used in ENAP costing.
However the to make the training complete, these sections will be demonstrated to you
by the facilitator using different projections. Later you will be able to practice them
yourself.
END