correlates of insight in first episode psychosis
TRANSCRIPT

www.elsevier.com/locate/schres
Schizophrenia Research 70 (2004) 187–194
Correlates of insight in first episode psychosis
Matcheri S. Keshavana,*, Jonathan Rabinowitzb, Goedele DeSmedtc,Phillip D. Harveyd, Nina Schoolere
aDepartment of Psychiatry, Western Psychiatric Institute and Clinic, Pittsburgh, PA, USAbSchool of Social Work, Bar-Ilan University, Ramat Gan, Israel
c International Clinical Research and Development, Janssen Research Foundation, Beerse, BelgiumdDepartment of Psychiatry, Mt. Sinai School of Medicine, New York, NY, USA
ePsychiatry Research, Long Island Jewish Medical Center, New Hyde Park, NY, USA
Received 15 August 2003; received in revised form 7 November 2003; accepted 12 November 2003
Available online 25 January 2004
Abstract
Impaired insight is common in schizophrenia and may be related to poor treatment adherence. Few studies have examined
the clinical and neurocognitive correlates of insight in early schizophrenia. Early course schizophrenia, schizoaffective, and
schizophreniform disorder patients (n = 535) were studied. The Positive and Negative Symptom Scale (PANSS) was used to
assess psychopathology, and a broad range of neuropsychological functions was assessed. Using hierarchical stepwise multiple
regression analyses, we examined the association of clinical, neurocognitive, and premorbid measures with the level of insight.
Impaired insight was associated with overall symptomatology, including positive, negative, and general psychopathology and
with deficits in cognitive functioning. In descending order of robustness, the significant variables were PANSS general
psychopathology ( p< 0.0001), Rey Auditory Verbal Learning Test ( p< 0.0004), Clinical Global Impression ( p < 0.005),
PANSS positive ( p < 0.007), and premorbid adjustment—general subscale ( p = 0.02). Among the PANSS general
psychopathology items, unusual thought content was most robustly associated with impaired insight ( p < 0.00000). Insight
impairment is very common in early schizophrenia, and appears to be associated with a broad range of psychopathology and
deficits in multiple cognitive domains. These observations suggest that deficits in insight may be related to a generalized
dysfunction of neural networks involved in memory, learning, and executive functions.
D 2003 Elsevier B.V. All rights reserved.
Keywords: Insight; First episode; Psychosis
1. Introduction researchers in psychotic disorders (Amador and David,
Over the past several years, there has been a great
deal of interest in the topic of insight among clinical
0920-9964/$ - see front matter D 2003 Elsevier B.V. All rights reserved.
doi:10.1016/j.schres.2003.11.007
* Corresponding author. UPMC Health System-Western Psychi-
atric Institute and Clinic, Room 984, 3811 O’Hara Street, Pittsburgh,
PA 15213, USA. Tel.: +1-412-624-2794; fax: +1-412-624-1459.
E-mail address: [email protected] (M.S. Keshavan).
1998). Insight into psychotic illness is multidimension-
al, and involves several aspects of clinical psychopa-
thology and cognition. Several studies have examined
clinical correlates of insight among chronic schizo-
phrenic patients, but the findings have been generally
inconsistent particularly in reference to correlations
with symptom severity (Buckley et al., 2001). Poor
insight has been associated with female gender (Peralta

M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194188
and Cuesta, 1998), poorer functioning (Dickerson et
al., 1997), premorbid impairment (Debowska et al.,
1998), prolonged illness duration (Drake et al., 2000),
and low levels (Carroll et al., 1999; Moore et al., 1999)
or high levels (Collins et al., 1997) of depression.
Impaired insight has been found to be correlated with
positive symptoms (Amador et al., 1994; Baier et al.,
2000; Kim et al., 1997), negative and disorganized but
not positive symptoms (Cuesta et al., 1998), negative as
well as positive symptoms (Debowska et al., 1998;
Kemp and Lambert, 1995), or with neither positive nor
negative symptoms (Schwartz and Petersen, 1999).
This variability in research findings may be at least
partially explained on the basis of small sample sizes,
different phases of the illness being studied, heteroge-
neous samples, inappropriate statistical methods, and
nonrandom sampling (Schwartz, 2000).
Although for years poor insight in schizophrenia
has been explained on the basis of various psycho-
logical phenomena, such as denial and willful prefer-
ence for psychosis, recent studies suggest that insight
deficits may reflect neurocognitive impairments per-
haps due to prefrontal and parietal lobe dysfunctions.
It has been proposed that schizophrenia-related im-
pairment in insight might be similar to anosognosia
seen in neurological illnesses (Amador and David,
1998). Some studies show a relationship between
impaired insight and neurocognition (Mohamed et
al., 1999), but others do not (Carroll et al., 1999;
McCabe et al., 2002). Such inconsistencies again
might be related to variable methodology, particularly
small sample sizes and varying populations and
phases of illness studied (Smith et al., 2000).
Attitudes towards treatment and insight into the
illness may vary during the course of the illness; it is
therefore important to examine course-specific patterns
and correlates of insight in schizophrenia. Only a few
studies to our knowledge have examined first episode
psychotic patients (Drake and Lewis, 2003; Mintz et
al., 2003). Studies of this population allow us to
examine the association between insight, symptom-
atology, and neurocognition without the potential con-
founds of illness chronicity. We examined the
relationships between insight, clinical measures (posi-
tive, negative symptoms, general psychopathology,
and Clinical Global Impression), premorbid adjust-
ment, age of onset, illness duration, and cognitive
performance on a variety of tasks tapping into attention,
memory, and executive functions—known to be im-
paired in schizophrenia (Elvevag and Goldberg, 2000).
2. Methods
The data for this study were collected as part
of a multicenter trial sponsored by the Janssen
Research Foundation titled ‘‘Double-blind evaluation
of risperidone vs. haloperidol on the long-term
morbidity of early psychotic patients’’ (RIS-INT
35) conducted in 11 countries. Since the languages
differed across the sites, a systematic procedure
(Harvey et al., 2003) was used to ensure that the
translations of all of the tests were valid. Briefly, a
local expert was identified in each country where
English was not the language of assessment. This
expert assisted in the translation of the instructions
and test stimuli, with these translations then con-
firmed by backtranslation.
The data set at baseline included 535 subjects (155
females and 380 males; age 16–45 years) with a
DSM-IV diagnosis of schizophrenia (n = 264), schiz-
ophreniform (n = 231), or schizoaffective disorder
(n = 40). To be eligible, the patient had to have the
diagnosis of schizophrenia, schizophreniform, or
schizoaffective disorder for less than a year, and must
have received 12 weeks or less of lifetime exposure to
antipsychotic medication. Patients with a diagnosis of
axis I psychiatric disorder other than the above, those
with a current substance use disorder, those with
significant medical illness, pregnant women, and
those with mental retardation were excluded. Three-
quarters of the sample were white (n = 400), 12%
(n = 64) were black, 3% (n = 17) were Hispanic, 2%
(n = 11) were Oriental, and 8% (n = 43) were from
assorted other groups. Fourteen percent (n = 76) of the
sample had no high school education, 26.6% (n = 141)
had some high school education, 21.5% (n = 114)
completed high school, 29.9% (n = 159) completed
some post high school education, and 7.7% (n = 41)
completed college. All subjects provided written in-
formed consent after full description of the study. The
Institutional Review Boards of each of the participat-
ing sites approved the study.
Psychopathology was quantified using the Positive
and Negative Symptom Scale (PANSS) (Kay et al.,
1987). The PANSS provides total, positive symptoms,

M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194 189
negative symptoms, and general psychopathology
scale scores. The Lack of Insight and Judgment item
of the PANSS general psychopathology subscale
provides quantified (1–7 from absent to extreme)
information on insight at baseline prior to institution
of treatment. Overall severity of illness was rated
using the Clinical Global Impression (CGI) scale.
Premorbid adjustment was assessed using the Premor-
bid Adjustment Scale (PAS) (Cannon-Spoor et al.,
1982). PAS determines premorbid functioning during
four periods: childhood, early adolescence, late ado-
lescence, and adulthood.
Cognitive assessments were also conducted at
baseline, prior to initiation of study treatment, and
included abstraction and concept flexibility (Wiscon-
sin Card Sorting Test, WCST; categories, total errors),
verbal fluency, memory (Wechsler Memory Scale—
Revised visual reproduction immediate and delayed;
Rey Auditory Verbal Learning Test, RVLT; learning
trials 1–5), and attention/psychomotor speed (the
Computerized Continuous Performance Test, CPT d’
total, and the Wechsler Adult Intelligence Scale—
Revised (WAIS-R) Digit Symbol, raw score). To
further examine the relationship between cognitive
function and level of insight, we also obtained a
Table 1
Comparison of means (S.E.) of cognitive measures by level of insight
Level of insight
(high to low)
CPT d’
total
RVLT
learning
trials 1–5
WMS-R VR
delayed recall
total score
WMS-R VR
immediate recal
total score
1 0.85 (0.09) 46.33 (1.45) 30.53 (0.95) 33.23 (0.90)
n= 58 60 60 60
2 0.87 (0.09) 44.41 (1.45) 28.25 (1.11) 32.22 (0.80)
n= 56 64 63 64
3 0.80 (0.06) 43.09 (1.16) 26.53 (0.84) 31.05 (0.64)
n= 105 106 107 107
4 0.81 (0.06) 41.74 (1.01) 25.38 (0.89) 31.25 (0.62)
n= 145 158 154 157
5 0.65 (0.07) 39.31 (1.67) 25.43 (1.24) 29.61 (1.07)
n= 59 68 65 67
6 Mean 0.64 (0.10) 36.61 (1.83) 21.92 (1.55) 28.30 (1.07)
n= 44 49 50 50
Combined
significance
0.1910 0.0002 0.0014 0.0093
Linear 0.0210 0.0000 0.0000 0.0003
Quadratic 0.372 0.567 0.960 0.834
Overall significance on the multivariate test: F= 1.67, df = 45, 2145, p= 0
CPT=Continuous Performance Test; RVLT=Rey Verbal Learning Tes
Revised, Visual Reproduction; WCST=Wisconsin Card Sorting Test.
composite cognitive measure by adding the z-scores
of the cognitive measures.
Patients were divided into aggregate groups on the
basis of their level of insight and comparisons were
made between the resulting groups on demographic
(education, sex, age, and age of first symptoms),
premorbid, clinical (PANSS, CGI, and diagnosis),
and cognitive measures using General Linear Model
(GLM) MANOVA testing for linear and nonlinear
effects. A separate model was used for each domain
because there was a high correlation between variables
(e.g., the various cognitive measures). The significant
variables in each domain were entered into a stepwise
multiple regression to identify the variables, which
independently explained more of the variance. A final
stepwise regression model that included the variables
found to be significant in each domain was run.
3. Results
Almost 12% of the patients (n = 62) had no im-
pairment in insight, 12.4% (n = 66) had ‘‘minimal’’
impairment, 20.9% (n= 111) had ‘‘mild impairment,’’
31.4% (n = 167) had ‘‘moderate impairment,’’ 13.7%
l
VF category
fluency—
total score
VF letter
fluency—
total score
WAIS-R DS
raw score
WCST
categories
WCST
total errors
37.83 (1.49) 29.38 (1.49) 46.88 (1.67) 4.82 (0.21) 35.33 (2.64)
60 60 59 60 60
40.61 (1.65) 31.83 (1.59) 46.16 (1.74) 4.59 (0.24) 36.34 (3.03)
64 63 63 58 58
36.66 (1.08) 30.15 (1.12) 42.85 (1.31) 4.09 (0.21) 42.33 (2.42)
108 108 108 102 102
36.97 (0.89) 30.19 (0.94) 42.92 (1.2) 3.99 (0.18) 43.53 (2.06)
157 157 157 150 150
34.87 (1.39) 28.00 (1.40) 42.40 (1.70) 3.56 (0.29) 48.33 (3.37)
68 68 68 63 63
32.35 (1.39) 25.28 (1.49) 39.69 (1.74) 2.86 (0.34) 57.13 (3.82)
49 50 49 44 46
0.0023 0.0309 0.1425 0.0000 0.0000
0.0006 0.0131 0.0107 0.0000 0.0000
0.126 0.014 0.865 0.272 0.105
.0035.
t; VF =Verbal Fluency; WMS-RVR—Wechsler Memory Scale—

Fig. 1. The relation between the composite cognitive measure and insight showing a strong linear trend.
M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194190
(n = 73) had ‘‘moderate–severe impairment,’’ 9.4%
(n= 50) had ‘‘severe’’ impairment, and three patients
had ‘‘extreme’’ impairment in insight. For the purpo-
ses of the analysis, the last two groups were combined
(50 + 3). There was a significant linear difference in
cognitive functioning, symptomatology, and premor-
bid functioning by level of insight in a MANOVA
model presented in Table 1. shows the analysis of the
cognitive variables. There were significant linear
differences on seven of the nine cognitive measures;
specifically, there were differences on the cognitive
assessments of abstraction and concept flexibility
(Wisconsin Card Sorting Test, WCST; categories,
total errors), verbal fluency, memory (Wechsler Mem-
ory Scale—Revised visual reproduction immediate
and delayed; and the Rey Auditory Verbal Learning
Test, RVLT; learning trials 1–5) but not on the two
measures of attention/psychomotor speed [Computer-
ized Continuous Performance Test, CPT d’ total, and
Table 2
Comparison of means (S.E.) of symptom measures by level of insight
Level of insight Sample Positive and Negative Symp
(high to low) sizeGeneral psychopathology
1 62 31.66 (1.24)
2 66 36.79 (1.26)
3 111 37.96 (0.80)
4 167 42.76 (0.67)
5 73 45.47 (1.15)
6 53 49.43 (1.15)
Combined significance 0.0000
Linear 0.0000
Quadratic 0.9688
Multivariate test: F = 8.03, df = 20, 2100, p= 0.0000.
CGI =Clinical Global Impression scale.
the Wechsler Adult Intelligence Scale—Revised
(WAIS-R) Digit Symbol, raw score]. The relationship
between the composite cognitive measure and insight
(Fig. 1) showed a strong linear trend (combined
significance, df = 5, 523, F = 5.11, p< 0.0001; linear
term, df = 1, F = 24.45, p < 0.0001; deviation from
linearity, df= 4, F = 0.39, p = 0.82), suggesting that
less insight is associated with lower cognitive func-
tioning. Stepwise linear regression of the significant
cognitive variables found that when used together, the
significant measures were the Rey Auditory Verbal
Learning Test (learning trials 1–5) (standardized
coefficient = 0.18, t = 3.74, p = 0.0002) and WCST
(categories, total errors) (standardized coef-
ficient =� 0.156, t = 3.17, p= 0.002).
There was a significant linear association between
insight and the three PANSS subscales (positive,
negative, and general psychopathology) and the
CGI in a MANOVA presented in Table 2. Including
tom Scale CGI
Negative Positive
16.84 (0.86) 16.02 (0.73) 3.87 (0.13)
20.18 (0.81) 16.83 (0.67) 4.05 (0.13)
20.16 (0.54) 19.41 (0.46) 4.24 (0.08)
22.37 (0.56) 21.40 (0.46) 4.59 (0.06)
23.62 (0.87) 22.45 (0.70) 4.88 (0.09)
25.94 (0.87) 25.02 (0.70) 5.25 (0.09)
0.0000 0.0000 0.0000
0.0000 0.0000 0.0000
0.9899 0.6574 0.1705
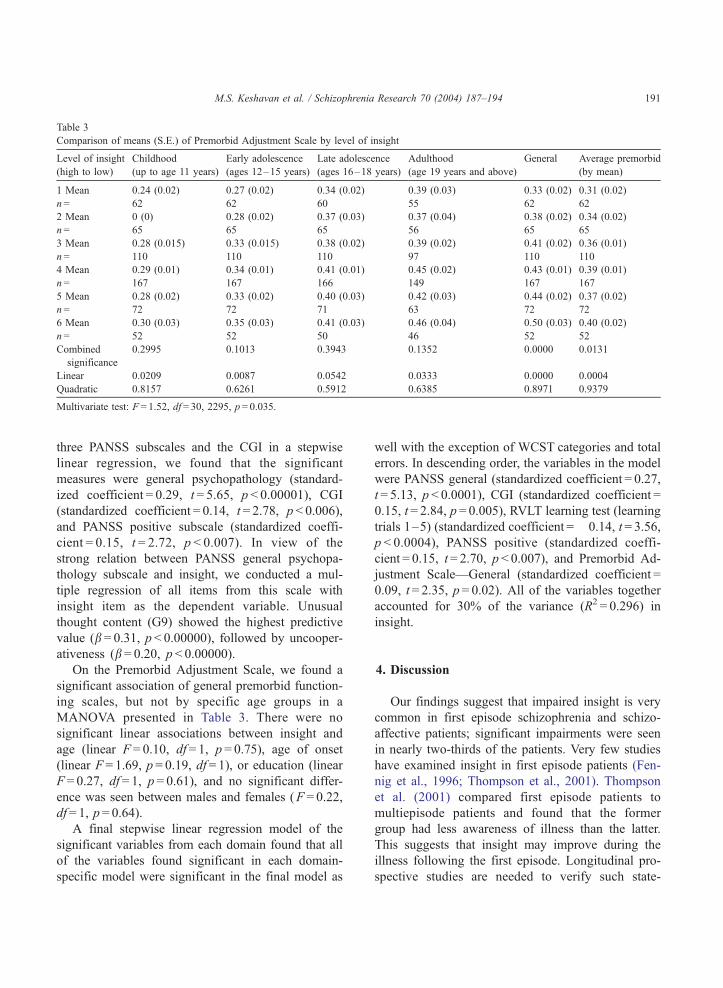
Table 3
Comparison of means (S.E.) of Premorbid Adjustment Scale by level of insight
Level of insight
(high to low)
Childhood
(up to age 11 years)
Early adolescence
(ages 12–15 years)
Late adolescence
(ages 16–18 years)
Adulthood
(age 19 years and above)
General Average premorbid
(by mean)
1 Mean 0.24 (0.02) 0.27 (0.02) 0.34 (0.02) 0.39 (0.03) 0.33 (0.02) 0.31 (0.02)
n= 62 62 60 55 62 62
2 Mean 0 (0) 0.28 (0.02) 0.37 (0.03) 0.37 (0.04) 0.38 (0.02) 0.34 (0.02)
n= 65 65 65 56 65 65
3 Mean 0.28 (0.015) 0.33 (0.015) 0.38 (0.02) 0.39 (0.02) 0.41 (0.02) 0.36 (0.01)
n= 110 110 110 97 110 110
4 Mean 0.29 (0.01) 0.34 (0.01) 0.41 (0.01) 0.45 (0.02) 0.43 (0.01) 0.39 (0.01)
n= 167 167 166 149 167 167
5 Mean 0.28 (0.02) 0.33 (0.02) 0.40 (0.03) 0.42 (0.03) 0.44 (0.02) 0.37 (0.02)
n= 72 72 71 63 72 72
6 Mean 0.30 (0.03) 0.35 (0.03) 0.41 (0.03) 0.46 (0.04) 0.50 (0.03) 0.40 (0.02)
n= 52 52 50 46 52 52
Combined
significance
0.2995 0.1013 0.3943 0.1352 0.0000 0.0131
Linear 0.0209 0.0087 0.0542 0.0333 0.0000 0.0004
Quadratic 0.8157 0.6261 0.5912 0.6385 0.8971 0.9379
Multivariate test: F = 1.52, df = 30, 2295, p= 0.035.
M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194 191
three PANSS subscales and the CGI in a stepwise
linear regression, we found that the significant
measures were general psychopathology (standard-
ized coefficient = 0.29, t = 5.65, p < 0.00001), CGI
(standardized coefficient = 0.14, t = 2.78, p < 0.006),
and PANSS positive subscale (standardized coeffi-
cient = 0.15, t = 2.72, p < 0.007). In view of the
strong relation between PANSS general psychopa-
thology subscale and insight, we conducted a mul-
tiple regression of all items from this scale with
insight item as the dependent variable. Unusual
thought content (G9) showed the highest predictive
value (b = 0.31, p < 0.00000), followed by uncooper-
ativeness (b = 0.20, p < 0.00000).
On the Premorbid Adjustment Scale, we found a
significant association of general premorbid function-
ing scales, but not by specific age groups in a
MANOVA presented in Table 3. There were no
significant linear associations between insight and
age (linear F = 0.10, df = 1, p = 0.75), age of onset
(linear F = 1.69, p = 0.19, df = 1), or education (linear
F = 0.27, df = 1, p = 0.61), and no significant differ-
ence was seen between males and females (F = 0.22,
df = 1, p = 0.64).
A final stepwise linear regression model of the
significant variables from each domain found that all
of the variables found significant in each domain-
specific model were significant in the final model as
well with the exception of WCST categories and total
errors. In descending order, the variables in the model
were PANSS general (standardized coefficient = 0.27,
t= 5.13, p < 0.0001), CGI (standardized coefficient =
0.15, t = 2.84, p = 0.005), RVLT learning test (learning
trials 1–5) (standardized coefficient =� 0.14, t= 3.56,
p < 0.0004), PANSS positive (standardized coeffi-
cient = 0.15, t= 2.70, p < 0.007), and Premorbid Ad-
justment Scale—General (standardized coefficient =
0.09, t = 2.35, p = 0.02). All of the variables together
accounted for 30% of the variance (R2 = 0.296) in
insight.
4. Discussion
Our findings suggest that impaired insight is very
common in first episode schizophrenia and schizo-
affective patients; significant impairments were seen
in nearly two-thirds of the patients. Very few studies
have examined insight in first episode patients (Fen-
nig et al., 1996; Thompson et al., 2001). Thompson
et al. (2001) compared first episode patients to
multiepisode patients and found that the former
group had less awareness of illness than the latter.
This suggests that insight may improve during the
illness following the first episode. Longitudinal pro-
spective studies are needed to verify such state-

M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194192
related change, and the factors that may underlie the
acquisition of insight.
While several studies have examined the relation-
ship between insight and cognitive performance, the
literature has been somewhat inconsistent. Some have
failed to find a relationship between poor insight and
global cognitive functioning (Cuesta and Peralta,
1994; Dickerson et al., 1997; Kemp and David,
1996; Smith et al., 2000). However, these studies
are difficult to interpret because of low statistical
power (Cuesta and Peralta, 1994), the use of only
global cognitive performance (Kemp and David,
1996), or an exclusive focus to examine prefrontally
mediated cognitive functions (Lysaker and Bell, 1994;
Young et al., 1993; Young et al., 1998). Additionally,
most previous studies examining the relation between
insight and neurocognition have examined chronic or
multiepisode patients. However, Drake and Lewis
(2003) found an association between perseverative
errors on WCST and poor insight, even in a relatively
small sample of early course (within 5 years of onset)
psychotic patients. In our study, we examined the
relationship between insight and a broad range of
cognitive functions in a large homogeneous group of
early course patients. While cognitive performance
measures reflecting prefrontal functions (such as
WCST and CPT) were significantly correlated with
impaired insight, cognitive measures that may reflect
the functioning of other brain regions such as the
temporal lobe (RVLT learning test) were more strong-
ly correlated with insight. This suggests that impaired
insight in schizophrenia may be mediated by a broad
range of cognitive dysfunctions caused by a distrib-
uted neuronal network disorder involving the associ-
ation cortex structures (Andreasen et al., 1999;
McCarley et al., 1999; Pearlson et al., 1996). While
a recent study has suggested that poor insight is
associated with specific frontal regions (Flashman et
al., 2001) as well as overall reductions in brain
volume (Flashman et al., 2000), other brain regions
have to be examined as well.
Our data showed robust relationships between
insight impairment and all three domains of PANSS
psychopathology (positive, negative, and general).
This contrasts with previous studies as discussed
earlier, which have tended to find relationships one
or other (Amador et al., 1994; Cuesta et al., 1998;
Debowska et al., 1998; Kemp and Lambert, 1995;
Kim et al., 1997). Studies finding no relationships
between psychopathology and insight tend to have
comprised of relatively small sample sizes (Flashman
et al., 2001; Laroi et al., 2000; McEvoy et al., 1996),
suggesting the possibility that negative findings may
be related to low statistical power to detect subtle
effects. Additionally, first episode patients who have
high levels of both insight impairments as well as
symptomatology may offer sufficient variance and are
better suited to find the predicted relationships be-
tween psychopathology and insight. Interestingly,
among the PANSS general psychopathology items,
unusual thought content (G9) was most highly asso-
ciated with insight. This is not surprising since the G9
item has been found to be closely related to the
positive and disorganized symptom factor in schizo-
phrenia (Brazo et al., 1996). Unusual thought pro-
cesses may lead to impairments in insight either by a
pattern of denial or misattribution of the symptom
experiences; it remains to be determined whether this
path to insight is related to, or independent of,
symptom unawareness that may be mediated by
cognitive impairments (Lysaker et al., 2003).
Thus, cognitive impairment specifically on meas-
ures of abstraction and concept flexibility, verbal
fluency, as well as symptomatology and poor pre-
morbid functioning are associated with poor insight
early in the course of schizophrenia. Insight in
schizophrenia is important because of its implica-
tions for treatment adherence. Nonadherence occurs
in over 80% among schizophrenia patients (Corrigan
et al., 1990) and is particularly prominent in first
episode patients (Novak-Grubic and Tavcar, 1999).
Early psychoeducation (Pekkala and Merinder,
2001) and psychotherapeutic interventions such as
motivational interviewing (Bustillo et al., 2001;
Kemp et al., 1998) can improve treatment adherence
in schizophrenia. However, not all studies confirm
the efficacy of psychosocial treatments in improving
treatment adherence in schizophrenia (O’Donnell et
al., 2003); clearly, impaired insight as well as
cognitive deficits are among the well-known predic-
tors of poor treatment adherence. Knowledge of the
prevalence and correlates of impaired insight at
illness onset can guide the clinical approach and
also provide the framework for later reassessment of
the degree of treatment-related change. Poor insight
in patients with unusual thought content and delu-

M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194 193
sions may potentially improve with cognitive behav-
ioral techniques (Turkington et al., 2002); on the
other hand, patients with illness unawareness related
to impaired cognitive function might have improve-
ments in insight with cognitive remediation treat-
ments (Bell et al., 2001; Hogarty and Flesher, 1999).
However, one cannot be too optimistic about the
effectiveness of such treatments, since many factors,
including structural and functional brain alterations,
are likely to be involved in the pathogenesis of
insight deficits. Pharmacological interventions that
may address cognitive impairments are also worth
considering in our efforts to improve insight. The
possibility that novel antipsychotics may have dif-
ferential therapeutic effects on insight is also worth
examining in large-scale clinical trials.
The strengths of this study include the large sample
size and the choice of early course schizophrenia
patients. Limitations include the cross-sectional nature
of this data analyses and the use of data from a single
item on PANSS to ascertain the level of insight,
making it difficult to tease apart the correlates of the
different dimensions of insight. However, our findings
are meaningful for clinicians in practice who need to
make brief global assessments of insight and judg-
ment. Further, the fact that there were a number of
differential correlations with level of insight argues
against the interpretation that this single item is not
reliable enough to identify variation in insight levels.
Future studies need to separately examine the corre-
lates of the specific components of impaired insight
(i.e., unawareness and misattribution) (McEvoy et al.,
1996; McGorry and McConville, 2000) in schizophre-
nia. Also needed are longitudinal evaluations of state-
related changes in insight and their relation to im-
paired cognition.
Acknowledgements
This work was supported by the Janssen Research
Foundation (RIS-INT 35). The authors would like to
thank Michael Davidson, Robin Emsley, and Patrick
McGorry for their advice as well as all the principal
investigators of the RIS-INT 35 Study, Janssen
Research Foundation, International Clinical Research
and Development (Beerse, Belgium) for their contri-
bution to the data collected.
References
Amador, X., David, A., 1998. Insight and Psychosis Oxford
Univ. Press, New York, NY.
Amador, X.F., Flaum, M., Andreasen, N.C., Strauss, D.H., Yale,
S.A., Clark, S.C., et al., 1994. Awareness of illness in schizo-
phrenia and schizoaffective and mood disorders. Arch. Gen.
Psychiatry 51, 826–836.
Andreasen, N.C., Nopoulos, P., O’Leary, D.S., Miller, D.D., Was-
sink, T., Flaum, M., 1999. Defining the phenotype of schizo-
phrenia: cognitive dysmetria and its neural mechanisms. Biol.
Psychiatry 46, 908–920 (see comments).
Baier, M., DeShay, E., Owens, K., Robinson, M., Lasar, K., Peter-
son, K., et al., 2000. The relationship between insight and clin-
ical factors for persons with schizophrenia. Arch. Psychiatr.
Nurs. 14, 259–265.
Bell, M., Bryson, G., Greig, T., Corcoran, C., Wexler, B.E., 2001.
Neurocognitive enhancement therapy with work therapy: effects
on neuropsychological test performance. Arch. Gen. Psychiatry
58, 763–768.
Brazo, P., Ribeyre, J.M., Petit, M., Dollfus, S., 1996. Identification
by typological analysis of distinct groups of schizophrenic
patients. Applicability of a disorganized schizophrenia subtype.
Encephale 22, 165–174.
Buckley, P.F., Hasan, S., Friedman, L., Cerny, C., 2001. Insight and
schizophrenia. Comp. Psychiatry 42, 39–41.
Bustillo, J.R., Lauriello, J., Horan, W.P., Keith, S.J., 2001. The
psychosocial treatment of schizophrenia: an update. Am. J. Psy-
chiatry 158, 163–175.
Cannon-Spoor, E., Potkin, S.G., Wyatt, R.J., 1982. Measurement of
premorbid adjustment in chronic schizophrenia. Schizophr. Bull.
8, 470–484.
Carroll, A., Fattah, S., Clyde, Z., Coffey, I., Owens, D.G., John-
stone, E.C., 1999. Correlates of insight and insight change in
schizophrenia. Schizophr. Res. 35, 247–253.
Collins, A.A., Remington, G.J., Coulter, K., Birkett, K., 1997. In-
sight, neurocognitive function and symptom clusters in chronic
schizophrenia. Schizophr. Res. 27, 37–44.
Corrigan, P.W., Liberman, R.P., Engel, J.D., 1990. From noncom-
pliance to collaboration in the treatment of schizophrenia. Hosp.
Community Psychiatry 41, 1203–1211.
Cuesta, M.J., Peralta, V., 1994. Lack of insight in schizophrenia.
Schizophr. Bull. 20, 359–366.
Cuesta, M.J., Peralta, V., Zarzuela, A., 1998. Psychopathological
dimensions and lack of insight in schizophrenia. Psychol. Rep.
83, 895–898.
Debowska, G., Grzywa, A., Kucharska-Pietura, K., 1998. Insight in
paranoid schizophrenia—its relationship to psychopathology
and premorbid adjustment. Comp. Psychiatry 39, 255–260.
Dickerson, F.B., Boronow, J.J., Ringel, N., Parente, F., 1997. Lack
of insight among outpatients with schizophrenia. Psychiatr.
Serv. 48, 195–199.
Drake, R.J., Lewis, S.W., 2003. Insight and neurocognition in
schizophrenia. Schizophr. Res. 62, 165–173.
Drake, R.J., Haley, C.J., Akhtar, S., Lewis, S.W., 2000. Causes and
consequences of duration of untreated psychosis in schizophre-
nia. Br. J. Psychiatry 177, 511–515.
M.S. Keshavan et al. / Schizophrenia Research 70 (2004) 187–194194
Elvevag, B., Goldberg, T.E., 2000. Cognitive impairment in
schizophrenia is the core of the disorder. Crit. Rev. Neurobiol.
14, 1–21.
Fennig, S., Everett, E., Bromet, E.J., Jandorf, L., Fennig, S.R.,
Tanenberg-Karant, M., et al., 1996. Insight in first-admission
psychotic patients. Schizophr. Res. 22, 257–263.
Flashman, L.A., McAllister, T.W., Andreasen, N.C., Saykin, A.J.,
2000. Smaller brain size associated with unawareness of ill-
ness in patients with schizophrenia. Am. J. Psychiatry 157,
1167–1169.
Flashman, L.A., McAllister, T.W., Johnson, S.C., Rick, J.H.,
Green, R.L., Saykin, A.J., 2001. Specific frontal lobe subre-
gions correlated with unawareness of illness in schizophrenia:
a preliminary study. J. Neuropsychiatry Clin. Neurosci. 13,
255–257.
Harvey, P.D., Artiola i Fortuny, L., Vester-Blockland, E., De Smedt,
G., 2003. Cross-national cognitive assessment in schizophrenia
clinical trials: a feasibility study. Schizophr. Res. 59, 243–251.
Hogarty, G.E., Flesher, S., 1999. Practice principles of cognitive
enhancement therapy for schizophrenia. Schizophr. Bull. 25,
693–708.
Kay, S.R., Fiszbein, A., Opler, L.A., 1987. The positive and nega-
tive syndrome scale (PANSS) for schizophrenia. Schizophr.
Bull. 13, 261–276.
Kemp, R., David, A., 1996. Psychological predictors of insight
and compliance in psychotic patients. Br. J. Psychiatry 169,
444–450.
Kemp, R.A., Lambert, T.J., 1995. Insight in schizophrenia and its
relationship to psychopathology. Schizophr. Res. 18, 21–28.
Kemp, R., Kirov, G., Everitt, B., Hayward, P., David, A., 1998.
Randomised controlled trial of compliance therapy. 18-Month
follow-up. Br. J. Psychiatry 172, 413–419.
Kim, Y., Sakamoto, K., Kamo, T., Sakamura, Y., Miyaoka, H.,
1997. Insight and clinical correlates in schizophrenia. Comp.
Psychiatry 38, 117–123.
Laroi, F., Fannemel, M., Ronneberg, U., Flekkoy, K., Opjords-
moen, S., Dullerud, R.et al., , 2000. Unawareness of illness
in chronic schizophrenia and its relationship to structural brain
measures and neuropsychological tests. Psychiatry Res. 100,
49–58.
Lysaker, P., Bell, M., 1994. Insight and cognitive impairment in
schizophrenia. Performance on repeated administrations of the
Wisconsin Card Sorting Test. J. Nerv. Ment. Dis. 182, 656–660.
Lysaker, P.H., Lancaster, R.S., Davis, L.W., Clements, C.A., 2003.
Patterns of neurocognitive deficits and unawareness of illness in
schizophrenia. J. Nerv. Ment. Dis. 191, 38–44.
McCabe, R., Quayle, E., Beirne, A.D., Anne Duane, M.M., 2002.
Insight, global neuropsychological functioning, and symptom-
atology in chronic schizophrenia. J. Nerv. Ment. Dis. 190,
519–525.
McCarley, R.W., Wible, C.G., Frumin, M., Hirayasu, Y., Levitt, J.J.,
Fischer, I.A., et al., 1999. MRI anatomy of schizophrenia. Biol.
Psychiatry 45, 1099–1119.
McEvoy, J.P., Hartman, M., Gottlieb, D., Godwin, S., Apperson,
L.J., Wilson, W., 1996. Common sense, insight, and neuro-
psychological test performance in schizophrenia patients.
Schizophr. Bull. 22, 635–641.
McGorry, P.D., McConville, S.B., 2000. Insight in psychosis. Harv.
Ment. Health Lett. 17, 3–5.
Mintz, A.R., Dobson, K.S., Romney, D.M., 2003. Insight in schizo-
phrenia: a meta-analysis. Schizophr. Res. 61, 75–88.
Mohamed, S., Fleming, S., Penn, D.L., Spaulding, W., 1999. In-
sight in schizophrenia: its relationship to measures of executive
functions. J. Nerv. Ment. Dis. 187, 525–531.
Moore, O., Cassidy, E., Carr, A., O’Callaghan, E., 1999. Unaware-
ness of illness and its relationship with depression and self-
deception in schizophrenia. Eur. Psychiatry 14, 264–269.
Novak-Grubic, V., Tavcar, R., 1999. Treatment compliance in first-
episode schizophrenia. Psychiatr. Serv. 50, 970–971 (letter;
comment).
O’Donnell, C., Donohoe, G., Sharkey, L., Owens, N., Migone, M.,
Harries, R., et al., 2003. Compliance therapy: a randomised
controlled trial in schizophrenia. BMJ 327, 834.
Pearlson, G.D., Petty, R.G., Ross, C.A., Tien, A.Y., 1996. Schizo-
phrenia: a disease of heteromodal association cortex? Neuro-
psychopharmacology 14, 1–17.
Pekkala, E., Merinder, L., 2001. Psychoeducation for Schizophre-
nia. In The Cochrane Library, Oxford.
Peralta, V., Cuesta, M.J., 1998. Factor structure and clinical validity
of competing models of positive symptoms in schizophrenia.
Biol. Psychiatry 44, 107–114.
Schwartz, R.C., 2000. Insight and suicidality in schizophrenia: a
replication study. J. Nerv. Ment. Dis. 188, 235–237.
Schwartz, R.C., Petersen, S., 1999. The relationship between in-
sight and suicidality among patients with schizophrenia. J. Nerv.
Ment. Dis. 187, 376–378.
Smith, T.E., Hull, J.W., Israel, L.M., Willson, D.F., 2000. Insight,
symptoms, and neurocognition in schizophrenia and schizoaf-
fective disorder. Schizophr. Bull. 26, 193–200.
Thompson, K.N., McGorry, P.D., Harrigan, S.M., 2001. Reduced
awareness of illness in first-episode psychosis. Comp. Psychia-
try 42, 498–503.
Turkington, D., Kingdon, D., Turner, T., 2002. Effectiveness of a
brief cognitive–behavioural therapy intervention in the treat-
ment of schizophrenia. Br. J. Psychiatry 180, 523–527.
Young, D.A., Davila, R., Scher, H., 1993. Unawareness of illness
and neuropsychological performance in chronic schizophrenia.
Schizophr. Res. 10, 117–124.
Young, D.A., Zakzanis, K.K., Bailey, C., Davila, R., Griese, J.,
Sartory, G., et al., 1998. Further parameters of insight and neu-
ropsychological deficit in schizophrenia and other chronic men-
tal disease. J. Nerv. Ment. Dis. 186, 44–50.