coronary artery disease imaging - home - dialogues in ... · coronary artery disease imaging fausto...
TRANSCRIPT

245
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
EditorialCoronary artery disease imaging - R. Ferrari, K. Fox 247
Lead Article Coronary artery disease imaging - F. J. Pinto, I. Z. Cabrita, N. Cortez Dias 249
Expert Answers to Three Key Questions Coronary artery disease imaging: what is the role of magnetic resonance imaging? A. G. Dastidar, C. Bucciarelli-Ducci 267
Coronary artery disease imaging: what is the role of coronary computed tomography angiography? - U. Sechtem 277
What is the role of intracoronary imaging? - F. Prati, L. Gatto, V. Ramazzotti 287
Summaries of Ten Seminal Papers - I. Z. Cabrita, F. P. Figueiras, F. J. Pinto 293
Bibliography of One Hundred Key Papers 305
Multimodality cardiovascular molecular imaging, part II M. Nahrendorf and others
Appropriateness criteria for cardiovascular imaging use inclinical practice: a position statement of the ESC/EACVI taskforce – M. Garbi and others
Outcomes of anatomical versus functional testing for coronaryartery disease – P. S. Douglas and others
Cardiovascular imaging practice in Europe: a report from theEuropean Association of Cardiovascular Imaging – P. Lancellotti
and others
Echocardiographic chamber quantification in the era of multimodality imaging: beware of unintended consequencesH. Feigenbaum
Low-dose CT coronary angiography with a novel IntraCyclemotion-correction algorithm in patients with high heart rate orheart rate variability – D. Andreini and others
Prognostic value of coronary artery calcium scoring in additionto single-photon emission computed tomographic myocardialperfusion imaging in symptomatic patients – E. M. Engbers and
others
Workstation-based calculation of CTA-based FFR for interme-diate stenosis – M. Kruk and others
Echocardiographic and fluoroscopic fusion imaging for proce-dural guidance: an overview and early clinical experience –J. J. Thaden and others
Diagnostic performance of the 3D bull’s eye display of SPECTand coronary CTA fusion – T. Nakahara and others
Coronary Artery Disease Imaging
246
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Anand I, MD Prof MedicineLa Jolla, CA, USA
Avkiran M, PhD Cardiovascular Research The Rayne InstituteSt Thomas’ HospitalLondon, UK
Bassand JP, MDDept of CardiologyUniversity Hospital Jean MinjozBesançon, France
Bertrand ME, MDHôpital CardiologiqueLille, France
Böhm M, MDSaarland University HospitalHomburg/Saar, Germany
Bolli R, MDDivision of CardiologyUniversity of LouisvilleLouisville, KY, USA
Borer JS, MDHoward Gilman Institute for Heart Valve DiseaseSchiavone Institute for Cardio-vascular Translational ResearchState University of New YorkDownstate Medical Center, New York, NY, USA
Coats A, MDFaculty of MedicineUniversity of SydneySydney, Australia
Cowie M, MD, PhDDept of Clinical CardiologyNational Heart & Lung InstituteLondon, UK
Danchin N, MDDept of CardiologyHôpital Européen Georges PompidouParis, France
Dargie HJ, MDCardiac ResearchWestern InfirmaryGlasgow, UK
Erol C, MDAnkara UniversityFaculty of MedicineAnkara, Turkey
Fox KA, MDDept of Cardiological ResearchUniversity of EdinburghEdinburgh, UK
Fuster V, MD, PhDCardiovascular InstituteMount Sinai Medical CenterNew York, NY, USA
Consulting Editors
Editors in ChiefFerrari R, MD, PhDChair of Cardiology University Hospital of Ferrara, Cona (Ferrara),Italy
Fox K, MD, FRCPNational Heart and Lung InstituteInstitute of Cardiovascular Medicine and ScienceRoyal Brompton Hospital, London, UK
Hasenfuss G, MDDept of CardiologyGeorg-August UniversitätGöttingen, Germany
Heusch G, MD, PhDWest German Heart and Vascular Centre EssenInstitute for Pathophysiology University of Essen MedicalSchoolEssen, Germany
Hori M, MD, PhDDept of Internal Medicine and TherapeuticsOsaka University Graduate School of MedicineOsaka, Japan
Hu D, MDHeart Institute Intervention Center People Hospital of PekingUniversity Beijing, China
Komajda M, MDDept of CadiologyCHU Pitié-SalpêtrièreParis, France
Libby P, MDCardiovascular MedicineBrigham & Women’s HospitalBoston, MA, USA
Lonn E, MDHamilton Health Sciences General SiteHamilton, Ontario, Canada
Lüscher T, MDDepartment of CardiologyUniversity Heart Center University Hospital Zürich, Switzerland
Lopez-Sendon JL, MDCCU Dept of CardiologyHospital University Gregorio MaranonMadrid, Spain
Maggioni AP, MDANMC Research CenterFirenze, Italy
Marber MS, MD, PhDCardiovascular Research The Rayne Institute St Thomas’ HospitalLondon, UK
Oktay E, MDDept Cardiology Dokuz Eylul University Faculty of Medicine İzmir, Turkey
Oto A, MDMedical Office, Hacettepe University School of MedicineAnkara, Turkey
Patrono C, MDDept of PharmacologyUniversity La SapienzaRome, Italy
Pepine CJ, MDDept of MedicineUniversity of FloridaGainesville, FL, USA
Pfeffer MA, MD, PhDDept MedicineBrigham and Women’s HospitalBoston, MA, USA
Pinto F, MDCardiology DepartmentFaculdade de MedicinaUniversidade de LisboaLisbon, Portugal
Rapezzi C, MDInstitute of CardiologyUniversity of BolognaBologna, Italy
Rosen MR, MDDept of Pharmacology & PediatricsColumbia University College of Physicians & SurgeonsNew York, NY, USA
Ryden L, MD, PhDDept of CardiologyKarolinska University Hospital SolnaStockholm, Sweden
Schneider MD, MDBaylor College of MedicineHouston, TX, USA
Seabra-Gomes RJ, MDInstituto do CoracaoHospital Santa CruzCarnaxide, Portugal
Shah A, MDCardiovascular DivisionJames Black CentreBritish Heart Foundation Centreof ExcellenceKing’s College London London, UK
Simoons ML, MDThoraxcenterErasmus University Medical CenterRotterdam, The Netherlands
Sipido K, MD, PhDDept Cardiovascular SciencesKatholieke Universiteit LeuvenLeuven, Belgium
Steg PG, MDDept of CardiologyHôpital Bichat–Claude BernardParis, France
Swedberg K, MD, PhDDept of MedicineSahlgrenska University Hospital OstraGöteborg, Sweden
Tardif JC, MDMontreal Heart InstituteMontreal, Quebec, Canada
Tavazzi L, MDDivision of CardiologyPoliclinico San Matteo IRCCSPavia, Italy
Tendera M, MD3rd Division of CardiologySilesian School of MedicineKatowice, Poland
Vanhoutte PM, MDDept of PharmacologyUniversity of Hong Kong Faculty of MedicineHong Kong, China
Widimsky P, MD, PhDVinohrady CardiocenterCharles University HospitalPrague, Czech Republic
Wijns WC, MDCardiovascular Center AalstOLV Hospital, Aalst, Belgium
Zamorano JL, MDUniversity Francisco deVitoria/Hospital Ramón y CajalMadrid, Spain

Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
247
hings have changed so much since I obtained my medical degree—fortunately
mostly for the better—that I sometimes feel as if I should return to university to
resit the same degree. I am sure that this is the case for all fields of medicine
and not just for cardiology. In only a few years, the technological innovations and
the close, fruitful relationship between industry and academia have created a revolution
in cardiology. Cardiologists no longer require only a stethoscope to listen to the heart.
Today, we can see the heart and its coronary arteries, and we can witness the heart’s
movements and functions with a precision that was unthinkable a few years ago.
The first ECG waves were recorded by Willem Einthoven in 1903, thus developing the
first electrocardiogram. This development led to “cardiology” becoming a medical
specialty, and those doctors who knew how to use an electrocardiogram were called
“cardiovascular specialists.” In 1953, a physician named Inge Gudmar Edler and an
engineer named Carl Hellmuth Hertz borrowed a shipyard sonar machine to conduct
the first human echocardiogram, which led to echocardiography becoming a widely
accepted method for cardiovascular research in the 1960s. And today, after many
advancements, we have three-dimensional imaging possibilities.
But we can do so much more. We can enter a small submarine and navigate inside
the coronary arteries, discovering all of the abnormalities along the route. Nowadays,
thanks to intracoronary imaging, it is also possible to discover the composition of the
coronary plaque, assess the kind of stent that would be more suitable for the particular
lesion identified, and determine whether the stent is inserted correctly. Francesco
Prati, Laura Gatto, and Vito Ramazzotti describe the specific advantages and limitations
of the most important imaging techniques used today—optical coherence tomography,
intravascular ultrasound, and near-infrared spectroscopy.
If you do not fancy entering a submarine and prefer a more real picture, then you have
two additional imaging tools—computer magnetic resonance and coronary computed
tomography angiography. Amardeep G. Dastidar and Chiara Bucciarelli-Ducci demon-
T
•••
Roberto Ferrari, MD, PhD
Kim Fox, MD, FRCP
Editorial
CORONARY ARTERY DISEASE IMAGING
Copyright © 2016, AICH - Servier Research Group. All rights reserved www.dialogues-cvm.org
strate that, due to its high spatial resolution, computer magnetic resonance plays an
amazing role in the diagnosis of patients, and it plays an even more important role in
risk stratification. Computer magnetic resonance allows us to determine, with a high
degree of precision, the extent of the scar and ischemic tissue. When computer magnetic
resonance is combined with late gadolinium enhancement to scrutinize myocyte via-
bility and first-pass perfusion with a vasodilator, you obtain all of the information you
need to make a suitable diagnosis and determine the appropriate treatment choice.
Udo Sechtem reviews all of the improvements that have made coronary computed
tomography angiography safer by reducing the radiation exposure and, at the same
time, more accurate by improving the spatial resolution to provide extremely clear
pictures of the coronary arteries. These achievements are contributing to the ever-in-
creasing role of coronary computed tomography angiography in preventive medicine,
stable coronary artery disease, and coronary artery bypass vasodilation.
As always, you need an overview of the pros and cons, especially when dealing with
technology; these are detailed for coronary artery disease imaging in the excellent
lead article by Fausto Pinto, Inês Z. Cabrita, and Nuno Cortez Dias. From a clinical
perspective, the authors delineate the roles played by ultrasound, echocardiography,
single-photon emission computed tomography, positron emission tomography, and
molecular imaging.
The enormous availability of imaging techniques available for cardiologists is such that
we now need a new profession – an “imaging doctor.” An imaging doctor would be
someone who can decide which is the best imaging tool to answer a given question.
This diagnosis will reduce the number of unnecessary examinations, and this will con-
sequently save money. Fausto Pinto and others also address the question concerning
whether or not the economic impact of these emerging technologies is sustainable.
Cardiology will soon be confronted with the issue of the cost:benefit ratio of each
technique. There is no doubt that imaging will take a central role in the correct diagno-
sis and treatment of patients, but only if used in a manner that is timely, appropriate,
and tailored for each patient. These advancements in technology will save lives, and
life does not have a price.
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Editorial - Ferrari, Fox
248
•••

249
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imagingFausto J. Pinto, MD, PhD1; Inês Z. Cabrita, PhD2; Nuno Cortez Dias, MD1
1University Hospital Santa Maria - Department of Cardiology - Lisbon Academic Medical Centre - CCUL - Lisbon - PORTUGAL2AIDFM-CETERA - Academic Consulting Research Organization - CCUL - Lisbon - PORTUGAL
Cardiovascular disease represents the leadingcause of death worldwide with ischemic heartdisease being the number one cardiovasculardisease in most countries. An increasing amount
of evidence has emerged on the added value of cur-rently available imaging methodologies for the diag-nosis of and monitoring of the disease processes.1,2
Additionally, they may play a significant role in theearly detection of disease and prevention. These dif-ferent imaging methods include: (i) ultrasound/echo-cardiography and their various modalities; (ii) nuclearimaging (eg, single-photon emission computed to-mography [SPECT], positron emission tomography[PET], cardiac computed tomography [CT], magneticresonance imaging [MRI], cardiac magnetic resonance[CMR]); (iii) hybrid imaging; (iv) molecular imaging;and (v) invasive imaging (eg, conventional angiography,intravascular ultrasound [IVUS], and optical coher-ence tomography [OCT]). Over the last few years, enor-mous and exciting developments have not only occurredfrom a technical, but also from a medical viewpoint,3-9
and these developments have been significant for themanagement of coronary artery disease (CAD).
Copyright © 2016, AICH - Servier Research Group. All rights reserved www.dialogues-cvm.org
Keywords: cardiovascular imaging; cardiovascular magnetic resonance;coronary artery disease; CT angiography; echocardiography; nuclear imagingAddress for correspondence:Fausto J. Pinto, MD, PhD, University Hospital Santa Maria, Department ofCardiology, Lisbon Academic Medical Centre, CCUL, Lisbon, Portugal(e-mail: [email protected])
Dialogues Cardiovasc Med. 2016;21:249-263
Cardiovascular disease represents the leading causeof death worldwide. Different imaging methods areavailable to aide in both the diagnosis of coronaryartery disease and monitoring of the disease process-es, including ultrasound/echocardiography, nuclear imaging, hybrid imaging, molecular imaging, andinvasive imaging. Over the last few years, develop-ments have been made not only from a technical, butalso from a medical viewpoint, and these develop-ments have been significant for the management ofcoronary artery disease. This review will briefly discussthe main cardiac imaging techniques for the assess-ment of coronary artery disease by focusing on threemain areas: (i) coronary artery anatomy, lumen size,and atherosclerotic plaques; (ii) myocardial perfusion;and (iii) myocardial viability. The advancements inimaging technology have expanded the use of imag-ing for coronary artery disease, and it is now consid-ered an important tool for the prevention and diagnosisof coronary artery disease and the monitoring of thedifferent therapeutic strategies. Cardiovascular im-aging has been included in the current internationalguidelines, demonstrating its appropriateness for themanagement of patients with suspected or knowncoronary artery disease.
SELECTED ABBREVIATIONS AND ACRONYMS
CAC coronary artery calcium
CAD coronary artery disease
CMR cardiac magnetic resonance
CT computed tomography
DE-CMR delayed contrast enhancement CMR
DSE dobutamine stress echocardiogram
IVUS intravascular ultrasound
MPI myocardial perfusion imaging
MRI magnetic resonance imaging
MSCT multislice computed tomography
OCT optical coherence tomography
PET positron emission tomography
SPECT single-photon emission computed tomography
Whether the economic impact of these emerging tech-nologies is sustainable is a question the cardiologycommunity will have to answer in the near future whenconsidering the cost-benefit ratio of the selected diag-nostic tool.10,11 The main cardiac imaging modalitiesfor the assessment of CAD will be briefly discussed inthis review with a focus on the three main areas whereimaging plays a central role: (i) assessment of thecoronary artery anatomy, lumen size, and atheroscle-rotic plaques; (ii) assessment of myocardial perfusion;and (iii) assessment of myocardial viability.
CORONARY ANATOMY ASSESSMENT
In patients with an excellent acoustic window, it maybe possible to visualize the origin and proximal coro-nary arteries with two-dimensional echocardiography(2DE), which is especially significant for cases involvinggiant coronary aneurysms or for children to screen forthe coronary involvement of Kawasaki disease.12 How-ever, transthoracic echocardiography is insufficient to
delineate the anatomical course or lumen size of coro-nary arteries, and it does not visualize atheroscleroticplaques. Catheter coronary angiography is the goldstandard imaging modality to assess coronary arteryanatomy. Catheter coronary angiography provides ex-cellent visualization of the coronary artery lumen, andit has a spatial resolution of 0.25 mm and a temporalresolution of 6 ms. It is a technique that requires expos-ing the patient to ionizing radiation (3 mSv on aver-age), and it is an invasive procedure that has very rare,but potentially serious complications. However, it al-lows for the diagnosis and, if necessary, treatment ofthe disease in the same session. It does not assess thecoronary vascular wall properties, but this assessmentis usually done by complementing catheter coronaryangiography with intracoronary ultrasound imaging.
Noninvasive coronary artery imaging is very challeng-ing, and the following factors must be consideredwhen assessing the coronary anatomy: (i) high spatialresolution is needed to assess small and tortuous ves-
250
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
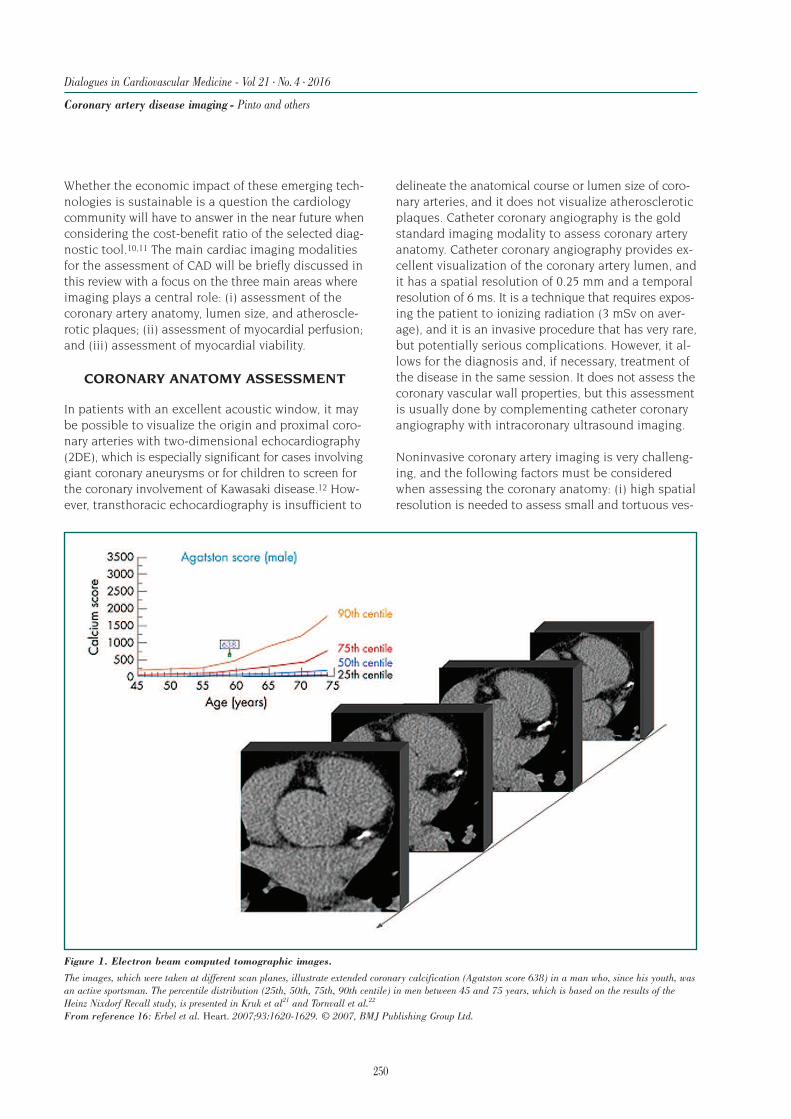
Figure 1. Electron beam computed tomographic images.
The images, which were taken at different scan planes, illustrate extended coronary calcification (Agatston score 638) in a man who, since his youth, wasan active sportsman. The percentile distribution (25th, 50th, 75th, 90th centile) in men between 45 and 75 years, which is based on the results of theHeinz Nixdorf Recall study, is presented in Kruk et al21 and Tornvall et al.22
From reference 16: Erbel et al. Heart. 2007;93:1620-1629. © 2007, BMJ Publishing Group Ltd.
sels; (ii) high temporal resolution is required becausethe coronary arteries undergo substantial motionthroughout the cardiac cycle with superimposed res-piratory movements; and (iii) high tissue detail andblood-tissue contrast is necessary to delineate the lu-men size throughout the coronary system, to identifycalcified and noncalcified coronary plaques, and todistinguish epicardial coronary arteries from surround-ing epicardial fat and the parallel running veins.
Computed tomography coronary angiography
CT coronary angiography can obtain a quantitativemeasure of coronary calcium, and it provides infor-mation related to coronary tree anatomy, includinganatomical course, lumen size, and artery wall status.Furthermore, it has the potential to detect both calci-fied and noncalcified atherosclerotic plaques.
The detection of coronary artery calcium (CAC) by elec-tron-beam CT or multidetector CT has gained somerelevance due to the documented association betweenCAC scores and the risk of cardiovascular events.13,14
An increase in CAC scores over time (CAC progression)improves the prediction of coronary heart diseaseevents. In a 2012 study, Okwuosa et al15 determinedwhether novel markers that do not involve ionizingradiation could predict CAC progression in a popula-tion of 2620 individuals who were at a low risk forcoronary heart disease events (Framingham risk score<10%) and who had a follow-up CAC measurement.The authors concluded that in individuals at a lowpredicted risk according to the Framingham risk score,traditional risk factors predicted CAC progression inthe short term with good discrimination and calibra-tion. In addition, prediction improved minimallywhen various novel markers were added to the model(Figure 1).16-22
In an extensive document, Waugh et al20 assessed theclinical and cost-effectiveness of CT screening for asymp-tomatic CAD. In addition, Waugh et al wanted to es-tablish whether CAC scores predict coronary eventsand add anything to the risk factor scores and whethermeasuring CAC changes the patient’s treatment. How-ever, no randomized control trials (RCTs) have assessedthe value of CT screening in reducing cardiac events.Seven studies were identified that assessed the asso-ciation between CAC scores on CT and cardiac out-comes in asymptomatic people (n=30 599 people). As the CAC score increased, so did the risk of cardiacevents. The correlation between CAC and cardiac risk
was consistent across the studies. There was evidencethat CAC scores varied among people with the sameFramingham risk factor scores and that within the sameFramingham bands, individuals with higher CAC scoreshad significantly higher cardiac event rates. This find-ing applied mainly when the CAC scores exceeded 300.Information is still needed regarding: (i) the distribu-tion of risk factor scores and CAC scores in asympto-
251
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
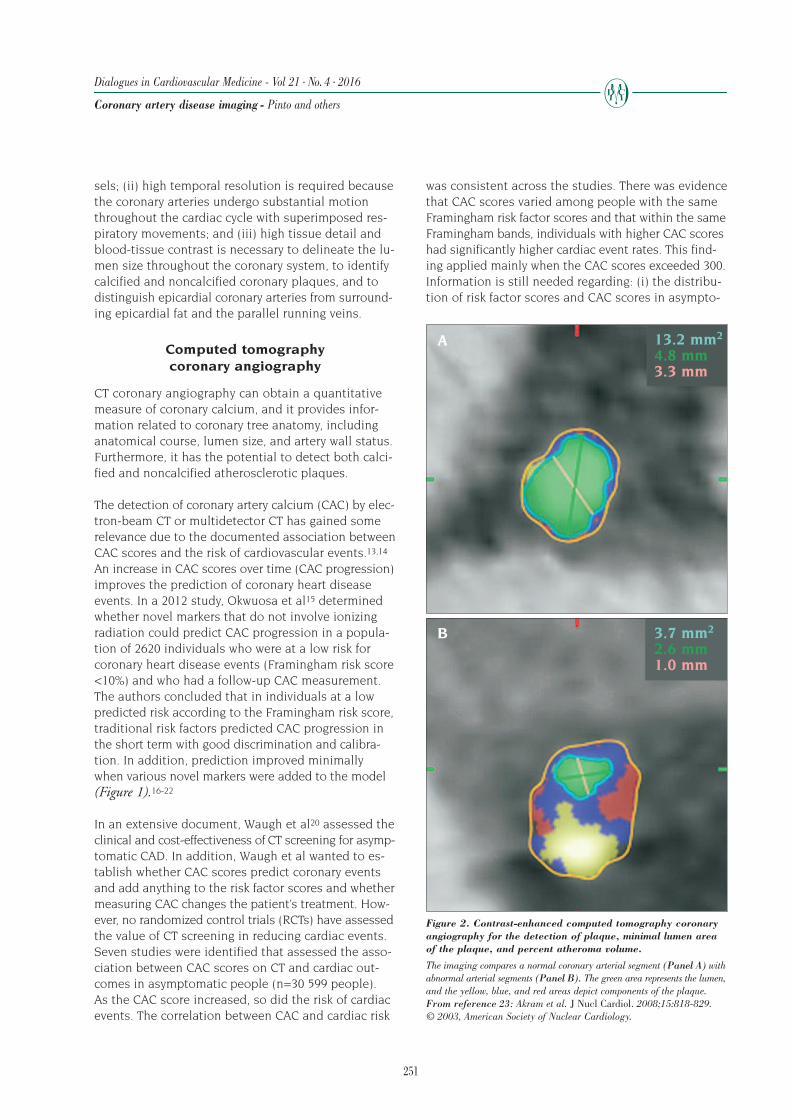
Figure 2. Contrast-enhanced computed tomography coronaryangiography for the detection of plaque, minimal lumen areaof the plaque, and percent atheroma volume.
The imaging compares a normal coronary arterial segment (Panel A) withabnormal arterial segments (Panel B). The green area represents the lumen,and the yellow, blue, and red areas depict components of the plaque. From reference 23: Akram et al. J Nucl Cardiol. 2008;15:818-829. © 2003, American Society of Nuclear Cardiology.
A
B
13.2 mm2
4.8 mm3.3 mm
3.7 mm2
2.6 mm1.0 mm

252
matic people; (ii) the level of concordance betweenrisk factor scores and CAC scores; (iii) the risk of car-diac events per annum according to CAC score andrisk factor scores; (iv) information on the acceptabilityof CT screening after information about the radiationdose; and (v) an RCT to study the addition of CT screen-ing to current risk factor–based practice.20
Multislice computed tomography (MSCT) and dual-scanMSCT have improved the spatial and temporal reso-lution of acquired images, making it possible to usecardiac CT for noninvasive coronary angiography. Infact, cardiac CT is the best noninvasive modality forvisualizing the coronary anatomy. ECG gating shouldbe utilized when coronary artery visualization is re-quired to improve coronary delineation and imagequality. Recent studies23 demonstrated that MSCT isable to visualize both the vessel lumen and wall todetect and characterize the atherosclerotic plaque(Figure 2, page 251).
Cardiac CT easily identifies calcified plaques, but italso has a moderate accuracy to detect noncalcified(lipid-rich) and mixed plaques. In patients with chestpain, the extent of noncalcified atherosclerosis as as-sessed by MSCT was correlated with mortality. Prospec-tive clinical studies are required to clarify the prognosticvalue of cardiac CT in this context. Plaque characteri-zation promises to help in the detection of vulnerableplaques. However, it is not currently possible or rec-ommended to use cardiac CT in routine clinical prac-tice. Single- and multicenter studies demonstratedthat CT coronary angiography has a high negative pre-dictive value (ruling out significant disease), but alow positive predictive value (plaque calcification fre-quently precludes accurate visualization of the lumenleading to overestimation of luminal stenosis). Thus,from a clinical perspective, the most important advan-tage of MSCT is the possibility of ruling out significantCAD convincingly.
Current clinical applications of CT coronary angiography • Noninvasive exclusion of CAD in patients at an in-termediate risk who have undergone one or more in-conclusive stress tests, including patients with atypicalangina pectoris and ambiguous results of previousstress tests.• Evaluation of the origin and course of anomalouscoronary arteries to provide a better characterizationthan CMR, but special efforts to reduce the radiationexposure should be undertaken since these patientsare often young.
• Assessment of the patency of coronary grafts anddetection of stenosis within the bypass or at the con-nection with the primitive coronary tree (Figure 3).9
CT coronary angiography is not recommended in high-risk patients, such as individuals with typical anginaor positive stress tests, in whom the prognosis is morerelated to functional parameters, such as ischemiaand left ventricular dysfunction than to anatomicalplaque measurement. CT coronary angiography is notappropriate as a screening examination in asympto-matic individuals or patients at low risk because of itsassociated radiation exposure, contrast administration,and risk of false positives. New developments in thefield will open the way for new potential uses of thistechnique.21,24
Magnetic resonance coronary angiography
Advances in the CMR technique, including the use ofparallel image acquisition, fat suppression (T2 prepa-ration), ECG-gating algorithms, and diaphragmaticmonitoring with navigator echoes, improved the spa-tial and temporal resolution, making it possible to vi-sualize the coronary arteries.10,22,25,26 The anatomicalevaluation of the entire coronary tree and lumen sizeare still tough to visualize, partially because the spa-tial resolution of CMR is still lower than cardiac CT(0.8 to 1.1 mm vs 0.4 to 0.5 mm).
CMR coronary angiography is not ready for the reliabledetermination of the location and extent of CAD inroutine clinical practice. However, CMR coronary an-giography has proven clinically valuable to assess theproximal portions of the coronary system and coronarygrafts. The technique can evaluate the origin and courseof the proximal coronary artery and detect anomalouscoronary artery origins and coronary fistulas.
It can also be used for the detection and follow-up of coronary aneurysms caused by Kawasaki disease.Lastly, CMR coronary angiography can assess the pa-tency of coronary artery bypass grafts, although diffi-culty remains for the visualization of the connectionwith the native coronary circulation where stenosesare often located.
Further technological advances, with acquisitions bywhole-heart sequences, higher field magnets, highermultiple receiver channel coils, and new intravascularparamagnetic agents, promise to improve the qualityof coronary CMR images.27-30
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others

253
ASSESSMENT OF MYOCARDIAL PERFUSION AND ISCHEMIA
Currently, there are many noninvasive techniques toassess myocardial perfusion and ischemia, includingstress echocardiography, SPECT-myocardial perfusionimaging (MPI), PET, CMR, and cardiac CT. All of thesetechniques use either exercise or pharmacologic stressto produce heterogeneity of blood flow between myo-cardial regions supplied by normal arteries and thoseregions perfused by stenotic vessels to induce ischemia.
Pharmacological stress can be generated by infusion ofvasodilators (dipyridamole or adenosine) or inotropicagents (dobutamine stress). Despite acting by differ-ent mechanisms, all methods administered with theappropriate doses have similar ischemic potency.Dobutamine increases contractility and myocardial oxy-gen demand, resulting in ischemia in regions suppliedby stenotic arteries. Dipyridamole inhibits adenosineuptake, which induces adenosine accumulation. Thestimulation of adenosine receptors induces potentvasodilatation, which is less pronounced in those areas supplied by stenotic coronary arteries. Thus, flowis diverted away (coronary steal) and the blood flowmisdistribution produces ischemia.
Stress echocardiography
Standard stress echocardiography detects stress-in-duced myocardial ischemia efficiently, but it is unableto assess myocardial perfusion directly,7,31-33 whichreduces its sensitivity since regional wall motion ab-
normalities do not becomeapparent until the diseasebecomes moderate to severe.The major advantages ofstress echocardiography in-clude higher specificity, wideravailability, bedside exami-nations, lower costs, its radi-ation-free nature, and highertemporal/spatial resolution.
Myocardial contrast echo-cardiography is a techniquethat uses microbubbles toassess myocardial perfusion.Microbubbles remain withinthe intravascular space; thus,steady-state myocardial con-trast intensity reflects thecapillary blood volume.
Delivering a high-energy ultrasound destroys micro-bubbles within the myocardial capillaries. The subse-quent rate of contrast replenishment reflects myocar-dial blood flow in the tissues. Combining myocardialcontrast echocardiography with pharmacologicalstress provides an incremental value for the assess-ment of CAD.
Stress echocardiography has several limitations thatjustify the permanent search for alternatives, includ-ing the high dependence on operator skills, high inter-and intraobserver variability, and the reliance on theacoustic window quality. The SPECT-MPI imagingstress test is the most widely used to assess myocar-dial perfusion, but the use of CMR and PET continuesto increase.
Single-photon emission computed tomography
SPECT-MPI performed at rest and during stress is arobust, well-validated, and widely available techniqueto assess regional myocardial perfusion.32,34 SPECT isbased on the detection of the heterogeneous uptakeof radiotracers during stress, which is caused by theinability to increase myocardial perfusion within theterritory of stenotic arteries (Figure 4, page 254).9
The major advantages of SPECT in comparison withstress echocardiography include: (i) higher feasibilityand lower operator dependency; (ii) higher sensitivity(≈86%), especially for a single-vessel disease involvingthe left circumflex; (iii) higher accuracy in the presence
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
A C DB
Figure 3. Noninvasive assessment of coronary bypass grafts.
Panels A and B. 3D rendering and multiplanar reconstruction of a coronary artery bypass graft of the rightcoronary artery after stent implantation in the proximal part. Panels C and D. Stenosis of a proximal coro-nary artery bypass graft to the right coronary artery in another patient. A left mammarian bypass to the leftanterior is crossing the coronary artery bypass graft. From reference 9: Cortez Dias N, Almeida A, Pinto F. Multimodality imaging: When echo is not enough. In Gillam LD, Otto CM, eds. Advanced Approaches in Echocardiography. 1st ed. Philadelphia, PA: Saunders,an imprint of Elsevier Inc; 2011:199-246.

254
of extensive resting wall motion abnormalities; and(iv) it is the most cost-effective technique for patientswith an intermediate risk of coronary events.
SPECT is unable to provide absolute quantification ofblood flow. In fact, only relative differences in perfu-sion are assessed from one region of the myocardiumto the region with the highest myocardial counts, whichfrequently results in an underestimation of the extentof CAD in patients with 3-vessel and/or left main CAD,particularly if balanced ischemia occurs during stress.The three available perfusion tracers (thallium-201,
99mTc-labeled sestamibi, and tetrofosmin) provide sim-ilar accuracy in the identification of CAD. AlthoughSPECT is very sensitive for detecting CAD (the absenceof reversible perfusion defects has a negative predic-tive value of 95%), it is only moderately specific (≈74%).The specificity of SPECT-MPI is diminished when arti-facts caused by soft-tissue attenuation are interpretedas perfusion defects. Dedicated hardware and soft-ware enable image reconstruction for different typesof attenuation, reducing artifacts originating from thediaphragm, breast tissue, or adipose tissue in obesepatients. In addition to assessing myocardial perfusion,
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
Figure 4. Exercise and rest Tc-99m tetrofosmin SPECT images in a patient with 3-vessel CAD and severe LV systolic dysfunction.
Panel A. On images obtained after stress, uptake is absent at the apex and it is severely reduced at the inferior and anterior walls (arrows). Panel B. At rest,there is significant improvement in the mid-apical parts of the anterior and inferior walls (asterisk). However, there is no change at the apex. Panel C. ECG gat-ing of the resting tomograms showing the endocardial border at end systole and end diastole. There is akinesia of the apical parts of the anterior and inferiorwalls. As the latter two regions are ischemic, viable, and akinetic, they fulfill the criteria for myocardial hibernation and are likely to recover function afterrevascularization. In contrast, there is akinesia of the apex, which, when combined with the lack of viability and ischemia, suggests myo-cardial infarction.Abbreviations: CAD, coronary artery disease; LV, left ventricular; SPECT, single-photon emission computed tomography.From reference 9: Cortez Dias N, Almeida A, Pinto F. Multimodality imaging: When echo is not enough. In Gillam LD, Otto CM, eds. AdvancedApproaches in Echocardiography. 1st ed. Philadelphia, PA: Saunders, an imprint of Elsevier Inc; 2011:199-246.
A. Stress
B. Rest
C. Function
Vertical axis Horizontal axis Short axis

255
ECG-gated SPECT evaluates the regional and globalLV contractility and wall thickening. ECG-gated SPECTis only possible with the use of 99mTc-labeled tracers.
The use of ECG gating with the simultaneous evalua-tion of perfusion and myocardial function improvesthe differentiation of scars from attenuation artifactsand provides important prognostic information. Theextent and severity of inducible perfusion defects havea diagnostic value, which can be used to identify pa-tients who are likely to benefit from revascularizationprocedures and to provide prognostic stratification(correlates with the risk of coronary events and sud-den death). The absence of perfusion defects almostexcludes the existence of flow-limiting coronary steno-sis, and it is associated with a low risk (<1%) of futurecoronary events. The prognostic accuracy of gatedSPECT derives from the simultaneous assessment ofthe most important prognostic factors, which includesthe following: (i) extension of necrotic myocardial tis-sue; (ii) extension and severity of inducible ischemia,which is the best predictor of nonfatal myocardial in-
farction; and (iii) left ventricular volume and systolicfunction—the post-stress ejection fraction is the bestpredictor of cardiac death.
Positron emission tomography
PET is the gold-standard assessment of myocardialperfusion because it is the only technique that allowsfor the absolute quantification of coronary blood flowat rest and coronary reserve during hyperemia.35,36
Quantification of myocardial blood flow improves theassessment accuracy in patients with multivessel dis-ease and balanced myocardial ischemia in whom theabsence of a normal reference segment may produce afalse negative with SPECT-MPI (Figure 5).35,37
The most commonly used tracers for assessing myocar-dial perfusion with PET are 13N-ammonia, rubidium-82(82Rb), and 15O-labelled water. These tracers have ahigh-energy emission, meaning that they are particu-larly indicated for obese subjects, and they have a shorthalf-life, which guarantees that the tissues are only
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
Figure 5. Exercise (Ex) and rest (R) Tc-99m sestamibi and exercise F-18-FDG images in a patient with 3-vessel CAD.
The perfusion images show no focal defects since balanced ischemia was present. However, the F-18-FDG images show intense and abnormally increasedglobal uptake in all three vascular territories. Abbreviations: CAD, coronary artery disease; FDG, fluorine-18-2-deoxygluclose.From reference 37: He et al. Circulation. 2003;108:1208-1213. © 2003, Wolters Kluwer Health, Inc.
Short axis
Vertical long axis
EX
R
FDG
EX
R
FDG
Horizontal long axis
256
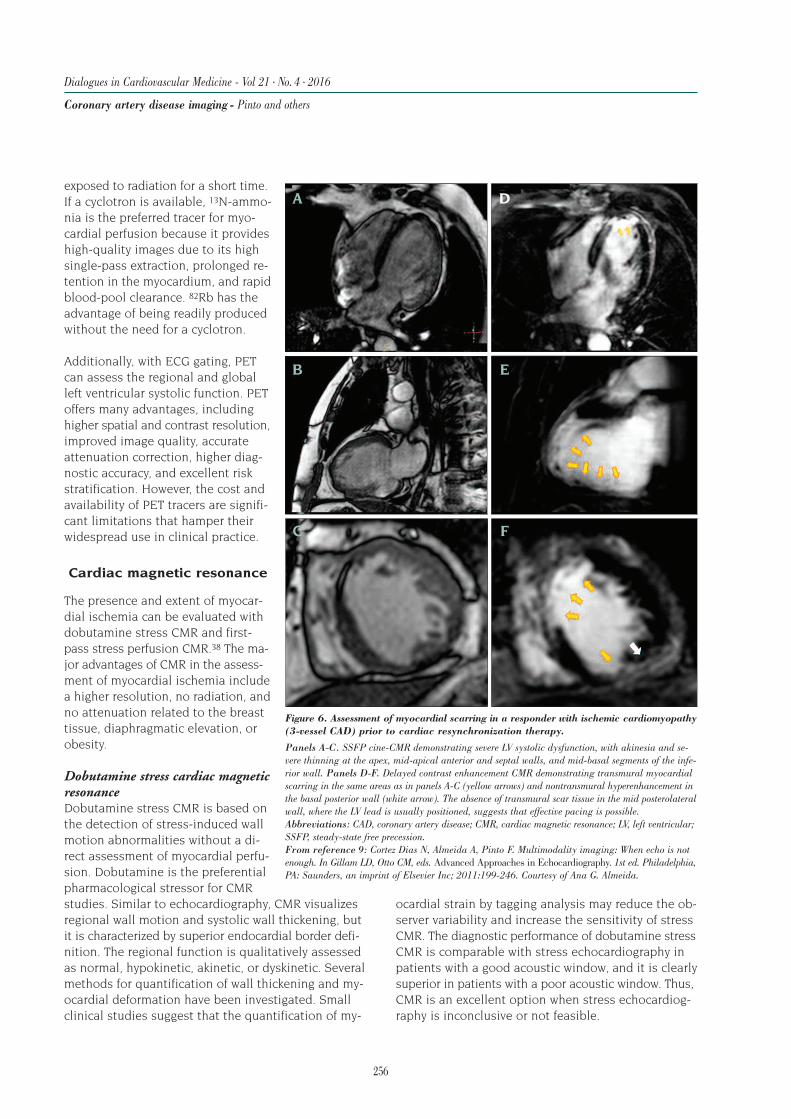
exposed to radiation for a short time.If a cyclotron is available, 13N-ammo-nia is the preferred tracer for myo-cardial perfusion because it provideshigh-quality images due to its highsingle-pass extraction, prolonged re-tention in the myocardium, and rapidblood-pool clearance. 82Rb has theadvantage of being readily producedwithout the need for a cyclotron.
Additionally, with ECG gating, PETcan assess the regional and globalleft ventricular systolic function. PEToffers many advantages, includinghigher spatial and contrast resolution,improved image quality, accurate attenuation correction, higher diag-nostic accuracy, and excellent riskstratification. However, the cost andavailability of PET tracers are signifi-cant limitations that hamper theirwidespread use in clinical practice.
Cardiac magnetic resonance
The presence and extent of myocar-dial ischemia can be evaluated withdobutamine stress CMR and first-pass stress perfusion CMR.38 The ma-jor advantages of CMR in the assess-ment of myocardial ischemia includea higher resolution, no radiation, andno attenuation related to the breasttissue, diaphragmatic elevation, orobesity.
Dobutamine stress cardiac magneticresonance Dobutamine stress CMR is based onthe detection of stress-induced wallmotion abnormalities without a di-rect assessment of myocardial perfu-sion. Dobutamine is the preferentialpharmacological stressor for CMRstudies. Similar to echocardiography, CMR visualizesregional wall motion and systolic wall thickening, butit is characterized by superior endocardial border defi-nition. The regional function is qualitatively assessedas normal, hypokinetic, akinetic, or dyskinetic. Severalmethods for quantification of wall thickening and my-ocardial deformation have been investigated. Smallclinical studies suggest that the quantification of my-
ocardial strain by tagging analysis may reduce the ob-server variability and increase the sensitivity of stressCMR. The diagnostic performance of dobutamine stressCMR is comparable with stress echocardiography inpatients with a good acoustic window, and it is clearlysuperior in patients with a poor acoustic window. Thus,CMR is an excellent option when stress echocardiog-raphy is inconclusive or not feasible.
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
Figure 6. Assessment of myocardial scarring in a responder with ischemic cardiomyopathy(3-vessel CAD) prior to cardiac resynchronization therapy.
Panels A-C. SSFP cine-CMR demonstrating severe LV systolic dysfunction, with akinesia and se-vere thinning at the apex, mid-apical anterior and septal walls, and mid-basal segments of the infe-rior wall. Panels D-F. Delayed contrast enhancement CMR demonstrating transmural myocardialscarring in the same areas as in panels A-C (yellow arrows) and nontransmural hyperenhancement inthe basal posterior wall (white arrow). The absence of transmural scar tissue in the mid posterolateralwall, where the LV lead is usually positioned, suggests that effective pacing is possible. Abbreviations: CAD, coronary artery disease; CMR, cardiac magnetic resonance; LV, left ventricular;SSFP, steady-state free precession. From reference 9: Cortez Dias N, Almeida A, Pinto F. Multimodality imaging: When echo is notenough. In Gillam LD, Otto CM, eds. Advanced Approaches in Echocardiography. 1st ed. Philadelphia,PA: Saunders, an imprint of Elsevier Inc; 2011:199-246. Courtesy of Ana G. Almeida.
A D
B E
C F

257
Stress perfusion cardiac magnetic resonance Myocardial perfusion is analyzed at rest and during in-fusion of adenosine by measuring the changes in thefirst-pass signal in the myocardium after a fast intra-venous injection of paramagnetic contrast. The myo-cardial concentration of the contrast agent at rest andduring stress directly reflects blood flow. Thus, as forPET, regional myocardial perfusion and perfusion re-serve can be measured. Myocardial areas supplied bycoronary vessels with high-grade stenosis receive lesscontrast than adjacent normally perfused regions, andit will appear relatively hypointense.
The excellent spatial resolution of CMR detects perfu-sion defects limited to the subendocardium, which isimpossible for all other imaging modalities, and itevaluates the ischemia transmurality. In routine clinicalpractice, myocardial perfusion is either qualitativelyscored or semiquantitatively analyzed (using the up-slope method). Recent advances made it possible toquantify myocardial perfusion using a deconvolutionmethodology, which promises to improve the diag-nostic accuracy and identify collateral perfusion–dependent myocardium. Further advances in perfusionanalysis software should make the process less time-consuming and more clinically applicable.
In stress perfusion CMR, regional wall motion andthickening at rest and during stress are also compared,which provides critical information regarding the func-tional significance of perfusion defects. Late gadolini-um enhancement images are also acquired, yieldingadditional information about infarction/scar and thedifferentiation of peri-infarct ischemia (Figure 6).10
First-pass perfusion cardiac computed tomography
Myocardial perfusion assessment with MSCT may bedone dynamically or as a first-pass perfusion.39 Three-dimensional MSCT data sets may be analyzed withprecise volumetric quantification of myocardial perfu-sion. Cardiac CT may provide a comprehensive assess-ment with anatomical evaluation of the coronary treeusing CT coronary angiography, assessment of myocar-dial perfusion with first-pass perfusion cardiac CT,and detection of delayed hyperenhancement (to eval-uate infarction and necrosis). The total radiation doserequired to acquire the complete data set is compara-ble with the exposure in a standard SPECT study. De-spite recent advances, the prognostic value and diag-nostic accuracy of cardiac CT for assessing myocardialperfusion remain unclear.
Hybrid imaging: SPECT-CT and PET-CT
Hybrid nuclear CT scanners and software fusion of datasets obtained from stand-alone scanners allow imagefusion of CT coronary angiography and nuclear imag-ing.40-43 The major advantage of hybrid imaging is theintegration of information regarding coronary calciumand coronary anatomy obtained by CT, with functionalinformation on cardiac perfusion and/or metabolismobtained with SPECT or PET (Figure 7).40 The poten-tial of such a comprehensive and noninvasive evalua-tion seems high, especially since the visualization ofcoronary stenosis complemented by the simultaneousassessment of its hemodynamic significance can theo-retically improve specificity without compromising sen-
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
Figure 7. Image fusion of a low-dose gated adenosine stressSPECT-MPI with 13 MBq99mTc-tetrofosmin and CTCAusing prospective ECG-triggering.
Panel A. Fused SPECT-CT demonstrat-ed a perfusion defect at stress in the an-terior myocardium (black arrows) thatcorresponds to the total occlusion (whitearrow) in the proximal LAD. Panel B.Occlusion of the LAD was confirmed byinvasive coronary angiography. Abbreviations: CT, computedtomography; CTCA, computed tomogra-phy coronary angiography; LAD, leftanterior descending coronary artery;MPI, myocardial perfusion imaging;SPECT, single-photon emission computedtomography. From reference 40: Herzog et al. EurHeart J. 2009;30:644. © 2009, OxfordUniversity Press.
A B

sitivity. With multimodality imaging, maximum diag-nostic and prognostic information can be potentiallyobtained, including information on subclinical coronaryatherosclerosis, which would not be detected with nu-clear imaging alone. These new multimodality imagingsystems carry enormous potential for rapid and efficientdiagnosis, but their clinical impact and cost-effective-ness still needs to be evaluated in large clinical trials.
ASSESSMENT OF MYOCARDIAL VIABILITY
Systolic left ventricular dysfunction due to CAD is thecomplex result of necrosis and scarring, but also offunctional and morphological adaptive abnormalitiesof the viable myocardium.44-53 Although the viablemyocardium encompasses normally contracting andhypocontractile tissue; the term usually refers to thedownregulation of contractile function in the survivingmyocardium as a response to a periodic or sustainedreduction in coronary blood flow. The main goal ofassessing myocardial viability is to detect dysfunction-al myocardium that can potentially improve contrac-tile function if a normal blood supply is restored withcoronary revascularization (either surgical or percuta-neous). In patients with extensive areas of viable my-ocardium, revascularization may improve symptoms,ventricular function, and survival (5-fold lower annualmortality rate when compared with medical treatmentalone). For patients with a nonviable myocardium,revascularization seems to have no survival benefitover medical therapy.
Several noninvasive imaging modalities evaluate myo-cardial viability, including dobutamine stress echocar-diogram (DSE), myocardial contrast echocardiography,SPECT, PET, CMR, and hybrid imaging modalities.These imaging modalities have various advantages andlimitations when assessing distinct characteristics ofthe viable, but dysfunctional, myocardium. Large-scaleprospective head-to-head comparisons are needed todetermine their accuracy in detecting viable myocardi-um and predicting a patient’s response to therapy.Since the use of a single viability test may not be op-timal, the value of sequential multimodality imagingshould be considered. The assessment of myocardialviability should start with a resting echocardiographicstudy, evaluating the acoustic window, endocardialborders, and wall thickening in all segments, the sever-ity of wall motion abnormalities, and left ventricularejection fraction. Resting echocardiograms providevaluable information to help choose the most appro-priate viability test for an individual patient.
Patients with adequate acoustic windows and withoutsevere left ventricular dysfunction at rest are particu-larly suitable for DSE. Patients with severe left ventric-ular dysfunction are a subgroup in which DSE is lessaccurate; therefore, SPECT, PET, CMR, and delayed con-trast enhancement CMR (DE-CMR) are better in thispatient group. SPECT, PET, CMR, and DE-CMR alsoprovide a better assessment of patients with pooracoustic windows (Figure 7). The choice of diagnosticimaging modality relies heavily on the expertise of themedical center. Recent advances in fusion imaging inwhich the PET perfusion and 18F-fluorodeoxyglucose(FDG) uptake patterns are superimposed on CMR images shows the extent of myocardial scar simulta-neously with the extent of both hibernating and non-hibernating viable myocardium. The clinical value ofmultimodality imaging needs to be determined in fu-ture clinical research studies.
Single-photon emission computed tomography
Among the radionuclide imaging techniques availableto assess myocardial viability, the most commonlyused is SPECT with either thallium-201 or 99mTc-labeledsestamibi (Figure 4). Thallium is a perfusion agentand a tracer of myocardial viability because its redis-tribution is mainly due to active uptake by intact car-diomyocytes. Technetium tracers do not redistribute,and they cannot provide an independent distinctionbetween perfusion and viability. The main advantageof using technetium tracers is their ability to performECG gating to assess ventricular function. SeveralSPECT protocols to evaluate myocardial viability areused under stress and/or rest, including imaging from8 to 72 hours after stress injection, reinjection of thetracer at rest on the same day as the stress injection,or a resting injection on a separate day. Sublingualnitrates improve resting perfusion and thus the detec-tion of viability when 99mTc-labelled tracers are used.SPECT is more sensitive, but less specific than DSEfor predicting functional improvement after revascu-larization. It is speculated that the small amounts ofviable tissue additionally recognized by SPECT maybe unable to contribute to the recovery of left ventric-ular function. The threshold of maximal myocardialuptake currently used to identify viability is ≥50%, al-though the best threshold would probably be higher.
Positron emission tomography
PET evaluates myocardial viability by qualitative andquantitative assessment of myocardial function, per-
258
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others

fusion, and metabolism. The viable tissue is metabol-ically active, whereas dysfunctional myocardial cellsobtain energy by using glucose instead of fatty acidmetabolism (Figure 5). The detection of myocardialhibernation with PET is based on the combination ofone tracer that assesses perfusion (usually 13N-am-monia or 82Ru) with the glucose analog FDG, whichevaluates metabolism. Normal tissue has a normalfunction, perfusion, and metabolism; stunned myocar-dium has a diminished function, but a normal or analmost normal perfusion and variable glucose metab-olism; hibernating myocardium has diminished func-tion and perfusion, but a preserved or increased glu-cose metabolism (metabolism-perfusion mismatch);and scar tissue has reduced function, perfusion, andmetabolism (metabolism-perfusion match).
Several nonrandomized retrospective studies showedthat FDG-PET predicts the recovery of regional func-tion after revascularization with high sensitivity (71%to 100%), but a relatively low specificity (33% to 91%).The major disadvantages of PET for assessing myo-cardial viability are its limited availability, high cost,and significant exposure to radiation without any rel-evant additional benefit (when compared with radia-tion-free alternatives).
Cardiac magnetic resonance
The two most important CMR techniques to assessmyocardial viability are DE-CMR and dobutamine CMR.Both are excellent options when stress echocardiog-raphy is inconclusive or not feasible, particularly inpatients with poor acoustic windows. DE-CMR is thetechnique most commonly used, and it will probablybecome the routine procedure for CMR assessment of myocardial viability.
Delayed contrast enhancement cardiac magnetic resonance DE-CMR is a newly established technique to detectacute or chronic infarct areas, which appear as brightregions in inversion recovery images that are acquired5 to 20 min after the intravenous injection of para-magnetic contrast. Assessment of viability is based onanatomical myocardial tissue characterization, and itdoes not require pharmacological tests. Viable myo-cardium (normal, stunned, or hibernating) has a normaldistribution volume of the contrast medium and doesnot have hyperenhancement. Acutely infarcted myo-cardium shows hyperenhanced areas due to the passivediffusion of contrast into the intracellular space ofnecrotic cells. Chronic infarcts (fibrotic tissue) appear
as hyperenhanced areas due to the increased intersti-tial space between collagen fibers and delayed washoutdue to reduced capillary density.
Due to its superior spatial resolution, DE-CMR is effec-tive in identifying the presence, location, and transmur-al extent of the nonviable myocardium. It can detectsmall regions of subendocardial infarct with highersensitivity than all other imaging modalities. The ex-tent of contrast enhancement on a segmental basis isuseful to predict contractile recovery after revascular-ization. Wall motion improvement can be expected indysfunctional segments if the hyperenhancing portiondoes not exceed 50% of the wall thickness. An improve-ment in left ventricular ejection fraction after revascu-larization correlates with the amount of poorly func-tioning, but not hyperenhanced myocardium. Unlikestress tests (either DSE or dobutamine CMR), whichhave a lower accuracy if severe rest dysfunction ispresent, DE-CMR seems to perform better in thesepatients.
Historical studies suggest that DE-CMR has a highersensitivity (≈90%), but a lower specificity (≈50%) thanDSE, which is mainly due to the variable functionalrecovery in myocardial segments with a 25% to 75%hyperenhancement. In patients who have multiple seg-ments with intermediate transmurality (25% to 75%),complementary use of DE-CMR and dobutamine CMRmay be the optimal CMR strategy for predicting func-tional recovery after revascularization, but no compar-ative studies have been performed yet.
Dobutamine stress cardiac magnetic resonance Dobutamine CMR assesses contractile reserve duringlow-dose dobutamine stress testing. The improvementin contractile function with low-dose dobutamine isindicative of myocardial viability. Similar to echocar-diography, CMR visualizes regional wall motion andsystolic wall thickening, but it is characterized by su-perior endocardial border definition. The diagnosticperformance of dobutamine CMR to predict regionalrecovery after revascularization is comparable with DSEin patients with good acoustic windows, but it is su-perior in all other patients.
Cardiac computed tomography
Similar to DE-CMR, the assessment of myocardial vi-ability using cardiac CT is based on the detection ofmyocardial retention of contrast within areas of non-viable tissue. On delayed enhanced cardiac CT, myo-cardial infarction shows increased attenuation values
259
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others
due to a combination of delayed wash-in and washoutkinetics and an increased distribution volume withinthe expanded interstitial compartment. Although pre-liminary studies proved the reliability of delayed en-hanced cardiac CT to detect and characterize scars, itcurrently cannot be recommended as a tool for rou-tine assessment of myocardial viability. The most im-portant limitations of delayed enhanced cardiac CTthat preclude its clinical application include the radi-ation exposure and the absence of trials proving itsusefulness for predicting the recovery of contractilefunction after revascularization.
Hybrid fusion imaging: SPECT-CMR and PET-CMR
Fusion imaging merges two disparate image datasetsinto one functional image, enhancing the ability ofdetermining functional consequences of anatomicalpathology. Recent software advances have provided thecapability to merge CMR and nuclear imaging (SPECT-PET) datasets. This multimodality assessment prom-ises to improve the detection and characterization ofboth viable and nonviable myocardium.
The anatomical characterization of nonviable tissueby DE-CMR and the functional evaluation of viablemyocardium by nuclear imaging modalities are obvi-ously complementary. Regions of chronic myocardialinfarction typically exhibit wall thinning. However,chronically hypoperfused myocardium may also bethinned and yet contain substantial amounts of viablemyocardium.
• SPECT or PET are often unable to detect viable myocardium within thinned segments due to partialvolume effect and because the amount of FDG seenmay not appear high enough to display the mismatchpattern.• Complimentary assessment with DE-CMR makesthe absence of substantial scarring within that segmentevident and thus suggests that the myocardium is viable.• DE-CMR cannot distinguish hibernating myocardiumfrom normally perfused myocardium in regions ofnontransmural hyperenhancement (the area contigu-ous with subendocardial hyperenhancement merelyshows an absence of scarring).• Complimentary assessment of perfusion can be ben-eficial since contractile recovery will likely occur if theregion is perfused by an artery with severe stenosis sothat a portion of dyssynergy could be attributed toresting hypoperfusion.
The clinical impact of this new imaging technique ontreatment strategy and patient outcomes still needsto be determined.
CONCLUSION
Cardiovascular imaging has improved over the lastfew years, mostly due to the important technologicaldevelopments that expanded the potential clinicalapplications. For CAD, the use of imaging has expand-ed significantly, and it is now considered an impor-tant tool for the prevention and diagnosis of CAD andthe monitoring of the various therapeutic strategies.Its inclusion in the current international guidelines isproof that the appropriate use of cardiovascular im-aging is currently necessary for the management ofpatients with suspected or known CAD. Future devel-opments are around the corner, including molecularimaging, fusion imaging, etc. These developments willmake it possible to be even more precise in the under-standing of the pathophysiology of CAD, establishingan earlier diagnosis (detection of subclinical disease),and monitoring the individual patient.40,41,54
REFERENCES
1. Pinto FJ.
Coronary artery disease: variation in ischaemic heart disease betweenEU countries.
Nat Rev Cardiol. 2013;10:555-556.
2. Lancellotti P, Płońska-Gościniak E, Garbi M, et al.
Cardiovascular imaging practice in Europe: a report from theEuropean Association of Cardiovascular Imaging.
Eur Heart J Cardiovasc Imaging. 2015;16:697-702.
3. Hackam DG, Shojania KG, Spence JD, et al.
Influence of noninvasive cardiovascular imaging in primary pre-vention: systematic review and meta-analysis of randomized trials.
Arch Intern Med. 2011;171:977-982.
4. Greenland P, Smith SC Jr, Grundy SM.
Improving coronary heart disease risk assessment in asymptomaticpeople: role of traditional risk factors and noninvasive cardiovas-cular tests.
Circulation. 2001;104:1863-1867.
5. Shaw LJ, Berman DS, Blumenthal RS, et al.
Clinical imaging for prevention: directed strategies for improveddetection of presymptomatic patients with undetected atherosclero-sis—Part I: clinical imaging for prevention.
J Nucl Cardiol. 2008;15:e6-e19.
260
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others

261
6. Wang TJ.
Assessing the role of circulating, genetic, and imaging biomarkersin cardiovascular risk prediction.
Circulation. 2011;123:551-565.
7. Nihoyannopoulos P, Pinto FJ.
Ischemic heart disease. In Badano L, Fox K, Sicari R, Zamorano JL, eds.
The EAE Textbook of Echocardiography. Oxford, UK: OxfordUniversity Press; 2011.
8. Garbi M, Habib G, Plein S, et al.
Appropriateness criteria for cardiovascular imaging use in clinicalpractice: a position statement of the ESC/EACVI taskforce.
Eur Heart J Cardiovasc Imaging. 2014;15:477-482.
9. Cortez Dias N, Almeida A, Pinto F.
Multimodality imaging: when echo is not enough. In Gillam LD,Otto CM, eds.
Advanced Approaches in Echocardiography. 1st ed. Philadel-phia, PA: Saunders, an imprint of Elsevier Inc; 2011:199-246.
10. Leal J, Luengo-Fernández R, Gray A, Petersen S,Rayner M.
Economic burden of cardiovascular diseases in the enlargedEuropean Union.
Eur Heart J. 2006;27:1610-1619.
11. Gershlick AH, de Belder M, Chambers J, et al.
Role of non-invasive imaging in the management of coronary arterydisease: an assessment of likely change over the next 10 years.
Heart. 2007;93:423-431.
12. Francisco AR, Menezes MN, Guimarães T, Pinto FJ,Almeida AG.
Giant coronary aneurysm in a patient with non-ST myocardial infarction.
Eur Heart J Cardiovasc Imaging. 2016;17:778.
13. Chen J, Krumholz HM.
How useful is computed tomography for screening for coronary artery disease? Screening for coronary artery disease with electron-beam computed tomography is not useful.
Circulation. 2006;113:125-146.
14. Pletcher MJ, Tice JA, Pignone M, Browner WS.
Using the coronary artery calcium score to predict coronary heartdisease events: a systematic review and meta-analysis.
Arch Intern Med. 2004;164:1285-1292.
15. Okwuosa TM, Greenland P, Burke GL, et al.
Prediction of coronary artery calcium progression in individualswith low Framingham Risk Score: the Multi-Ethnic Study ofAtherosclerosis.
JACC Cardiovasc Imaging. 2012;5:144-153.
16. Erbel R, Möhlenkamp S, Kerkhoff G, Budde T,Schmermund A.
Non-invasive screening for coronary artery disease: calcium scoring.
Heart. 2007;93:1620-1629.
17. Erbel R, Möhlenkamp S, Moebus S, et al; HeinzNixdorf Recall Study.
Coronary risk stratification, discrimination, and reclassificationimprovement based on quantification of subclinical coronary atherosclerosis: the Heinz Nixdorf Recall study.
J Am Coll Cardiol. 2010;56:1397-1406.
18. Owens DS, Budoff MJ, Katz R, et al.
Aortic valve calcium independently predicts coronary and cardio-vascular events in a primary prevention population.
JACC Cardiovasc Imaging. 2012;5:619-625.
19. Abdulla J, Asferg C, Kofoed KF.
Prognostic value of absence or presence of coronary artery diseasedetermined by 64-slice computed tomography coronary angiographya systematic review and meta-analysis.
Int J Cardiovasc Imaging. 2011;27:413-420.
20. Waugh N, Black C, Walker S, McIntyre L, Cummins E,Hillis G.
The effectiveness and cost-effectiveness of computed tomographyscreening for coronary artery disease: systematic review.
Health Technol Assess. 2006;10:iii-iv, ix-x, 1-41.
21. Kruk M, Wardziak L, Demkow M, et al.
Workstation-based calculation of CTA-based FFR for intermediatestenosis.
JACC Cardiovasc Imaging. 2016;9:690-699.
22. Tornvall P, Gerbaud E, Behaghel A, et al.
Myocarditis or “true” infarction by cardiac magnetic resonance inpatients with a clinical diagnosis of myocardial infarction withoutobstructive coronary disease: a meta-analysis of individual patientdata.
Atherosclerosis. 2015;241:87-91.
23. Akram K, Rinehart S, Voros S.
Coronary arterial atherosclerotic plaque imaging by contrast-en-hanced computed tomography: fantasy or reality?
J Nucl Cardiol. 2008;15:818-829.
24. Andreini D, Pontone G, Mushtaq S, et al.
Low-dose CT coronary angiography with a novel IntraCycle motion-correction algorithm in patients with high heart rate or heart ratevariability.
Eur Heart J Cardiovasc Imaging. 2015;16:1093-1100.
25. Collste O, Sörensson P, Frick M, et al.
Myocardial infarction with normal coronary arteries is commonand associated with normal findings on cardiovascular magneticresonance imaging: results from the Stockholm MyocardialInfarction with Normal Coronaries study.
J Intern Med. 2013;273:189-196.
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others

262
26. Stark MM, Schwartz RS, Satran D, et al.
“No culprit” ST-elevation myocardial infarction: role of cardiacmagnetic resonance imaging.
Crit Pathw Cardiol. 2014;13:135-140.
27. Abdel-Aty H, Simonetti O, Friedrich MG.
T2-weighted cardiovascular magnetic resonance imaging.
J Magn Reson Imaging. 2007;26:452-459.
28. Kellman P, Aletras AH, Mancini C, McVeigh ER, Arai AE.
T2-prepared SSFP improves diagnostic confidence in edema imag-ing in acute myocardial infarction compared to turbo spin echo.
Magn Reson Med. 2007;57:891-897.
29. Piechnik SK, Ferreira VM, Dall’Armellina E, et al.
Shortened modified Look-Locker Inversion recovery (ShMOLLI) forclinical myocardial T1-mapping at 1.5 and 3 T within a 9 heart-beat breathhold.
J Cardiovasc Magn Reson. 2010;12:69.
30. Park CH, Choi EY, Kwon HM, et al.
Quantitative T2 mapping for detecting myocardial edema afterreperfusion of myocardial infarction: validation and comparisonwith T2-weighted images.
Int J Cardiovasc Imaging. 2013;29(suppl 1):65-72.
31. Sicari R, Nihoyannopoulos P, Evangelista A, et al;European Association of Echocardiography.
Stress echocardiography expert consensus statement.
Eur Heart J. 2009;30:278-289.
32. Wolk MJ, Bailey SR, Doherty JU, et al; ACCFAppropriate Use Criteria Task Force.
ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013multimodality appropriate use criteria for the detection and riskassessment of stable ischemic heart disease.
J Am Coll Cardiol. 2014;63:380-406.
33. Picano E.
Stress Echocardiography.
6th ed. Switzerland: Springer; 2015.
34. Underwood SR, de Bondt P, Flotats A, et al.
The current and future status of nuclear cardiology: a consensusreport.
Eur Heart J Cardiovasc Imaging. 2014;15:949-955.
35. Jain D, He ZX.
Direct imaging of myocardial ischemia: a potential new paradigmin nuclear cardiovascular imaging.
J Nucl Cardiol. 2008;15:617-630.
36. Nahrendorf M, Sosnovik DE, French BA, et al.
Multimodality cardiovascular molecular imaging, part II.
Circ Cardiovasc Imaging. 2009;2:56-70.
37. He ZX, Shi RF, Wu YJ, et al.
Direct imaging of exercise-induced myocardial ischemia with fluo-rine-18-labeled deoxyglucose and Tc-99m-sestamibi in coronaryartery disease.
Circulation. 2003;108:1208-1213.
38. Hussain ST, Chiribiri A, Morton G, et al.
Perfusion cardiovascular magnetic resonance and fractional flowreserve in patients with angiographic multi-vessel coronary arterydisease.
J Cardiovasc Magn Reson. 2016;18:44.
39. Pontone G, Grancini L, Andreini D, Pepi M,Bartorelli AL.
Myocardial perfusion imaging using dual-energy computed tomography: a clinical case.
Eur Heart J Cardiovasc Imaging. 2013;14:835.
40. Herzog BA, Husmann L, Landmesser U, Kaufmann PA.
Low-dose computed tomography coronary angiography and my-ocardial perfusion imaging: cardiac hybrid imaging below 3mSv.
Eur Heart J. 2009;30:644.
41. Engbers EM, Timmer JR, Ottervanger JP, Mouden M,Knollema S, Jager PL.
Prognostic value of coronary artery calcium scoring in addition tosingle-photon emission computed tomographic myocardial perfu-sion imaging in symptomatic patients.
Circ Cardiovasc Imaging. 2016;9:e003966.
42. Pazhenkottil AP, Nkoulou RN, Ghadri JR, et al.
Prognostic value of cardiac hybrid imaging integrating single-photon emission computed tomography with coronary computed tomography angiography.
Eur Heart J. 2011;32:1465-1471.
43. Pazhenkottil AP, Nkoulou RN, Ghadri JR, et al.
Impact of cardiac hybrid single-photon emission computed tomog-raphy/computed tomography imaging on choice of treatment strategy in coronary artery disease.
Eur Heart J. 2011;32:2824-2829.
44. Bonow RO, Maurer G, Lee KL, et al; STICH TrialInvestigators.
Myocardial viability and survival in ischemic left ventricular dysfunction.
N Engl J Med. 2011;364:1617-1625.
45. Rizzello V, Poldermans D, Bax JJ.
Assessment of myocardial viability in chronic ischemic heart disease:current status.
Q J Nucl Med Mol Imaging. 2005;49:81-96.
46. Beanlands RS, Hendry PJ, Masters RG, deKemp RA,Woodend K, Ruddy TD.
Delay in revascularization is associated with increased mortalityrate in patients with severe left ventricular dysfunction and viable
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others

263
myocardium on fluorine 18-fluorodeoxyglucose positron emissiontomography imaging.
Circulation. 1998;98(suppl 19):II51-II56.
47. Senior R, Lahiri A.
Dobutamine echocardiography predicts functional outcome afterrevascularisation in patients with dysfunctional myocardium irre-spective of the perfusion pattern on resting thallium-201 imaging.
Heart. 1999;82:668-673.
48. Bax JJ, Visser FC, Poldermans D, et al.
Time course of functional recovery of stunned and hibernating seg-ments after surgical revascularization.
Circulation. 2001;104(suppl 1):I314-I318.
49. Bax JJ, Schinkel AF, Boersma E, et al.
Early versus delayed revascularization in patients with ischemiccardiomyopathy and substantial viability: impact on outcome.
Circulation. 2003;108(suppl 1):II39-II42.
50. Wei K, Jayaweera AR, Firoozan S, Linka A, SkybaDM, Kaul S.
Basis for detection of stenosis using venous administration of mi-crobubbles during myocardial contrast echocardiography: bolus orcontinuous infusion?
J Am Coll Cardiol. 1998;32:252-260.
51. Janardhanan R, Moon JC, Pennell DJ, Senior R.
Myocardial contrast echocardiography accurately reflects transmu-rality of myocardial necrosis and predicts contractile reserve afteracute myocardial infarction.
Am Heart J. 2005;149:355-362.
52. Pinto FJ.
Myocardial viability: the search for a perfect method is not over yet.
Eur Heart J. 2000;21:1039-1040.
53. Perrone-Filardi P, Pinto FJ.
Looking for myocardial viability after a STICH trial: not enoughto close the door.
J Nucl Med. 2012;53:349-352.
54. Thaden JJ, Sanon S, Geske JB, et al.
Echocardiographic and fluoroscopic fusion imaging for proceduralguidance: an overview and early clinical experience.
J Am Soc Echocardiogr. 2016;29:503-512.
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Coronary artery disease imaging - Pinto and others


265
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
What is the role of intracoronary imaging?F. Prati, L. Gatto, V. Ramazzotti
Coronary artery disease imaging: what is the role of coronary computed tomography angiography?
U. Sechtem
Expert Answers to Three Key Questions
Coronary artery disease imaging: what is the role of magnetic resonance imaging?A. G. Dastidar, C. Bucciarelli-Ducci
1
2
3
Coronary Artery Disease Imaging

schemic heart disease (IHD) isa global burden, and it remainsthe leading cause of death inthe UK and worldwide. Accurate
assessment of the presence and ex-tent of IHD is a crucial step in themanagement of this condition. Non-invasive imaging plays a vital rolein the diagnosis and risk stratifica-tion of patients with IHD. Over thelast decade, cardiac magnetic reso-nance imaging (CMR) has emergedas a very promising noninvasiveimaging modality in the assessmentof IHD due to its multiparametricnature, high spatial resolution, highreproducibility, and superior tissuecharacterization properties, all ofwhich are reflected in a large bodyof evidence in the literature. CMR
provides not only comprehensiveinformation on the presence andextent of myocardial scarring andischemia, but also an accurate as-sessment of left and right ventricularfunction, which guides the detec-tion and differential diagnosis, assists in clinical decision-makingprocess, and improves risk stratifi-cation. Among the multiparametrictechniques available in CMR, lategadolinium enhancement (LGE)(viability imaging) and first-passperfusion during vasodilator stress(ischemia imaging) are the corner-stones of CMR in the assessment ofIHD. The present article describesthe current knowledge and evidenceon CMR in the assessment of chron-ic IHD.
I
267Copyright © 2016, AICH - Servier Research Group. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Ischemic heart disease (IHD) is aglobal burden, and it remains theleading cause of death worldwide.Accurate assessment of the presenceand extent of IHD is a crucial stepin the management of this condi-tion. Noninvasive imaging plays avital role in the diagnosis and riskstratification of patients. Over thelast decade, cardiac magnetic resonance (CMR) imaging hasemerged as a very promising non-invasive imaging modality in theassessment of IHD due to its multi-parametric nature, high spatialresolution, high reproducibility, andsuperior tissue characterizationproperties, all of which are reflectedin a large body of evidence in theliterature. CMR provides compre-hensive information in the assess-ment of IHD, which guides the detection and differential diagnosis,assists in the clinical decision-mak-ing process, and improves riskstratification.
Keywords: cardiovascular magnetic reso-nance; ischemic heart diseaseAddress for correspondence:Dr Chiara Bucciarelli-Ducci, NIHR BristolCardiovascular Biomedical Research Unit,CMR Unit, Bristol Heart Institute, UpperMaudlin Street, Bristol, BS2 8HW, UK(e-mail: [email protected])Dialogues Cardiovasc Med. 2016;21:267-276
Coronary artery disease imaging: what is the roleof magnetic resonance imaging?Amardeep G. Dastidar, MBBS, MRCP; Chiara Bucciarelli-Ducci, MD, PhD, FESC, FRCP
Bristol Heart Institute - NIHR Bristol Cardiovascular Biomedical Research Unit - Bristol - UK
SELECTED ABBREVIATIONS AND ACRONYMS
CABG coronary artery bypass grafting
CE-MARC Clinical Evaluation of MAgnetic resonance imaging in Coronary heart disease
CMR cardiac magnetic resonance
EDWT end-diastolic wall thickness
FAME Fractional flow reserve versus Angiography for Multivessel Evaluation
FFR fractional flow reserve
IHD ischemic heart disease
LGE late gadolinium enhancement
MR-INFORM MR perfusion ImagiNg and Fractional flOw Reserve to guideManagement of patients with stable coronary artery disease [study]
PET positron emission tomography
RWMA regional wall motion abnormality
SPECT single-photon emission computed tomography

VIABILITY ASSESSMENT
Rationale
In the context of ischemic cardiomy-opathy, dysfunctional myocardiumcan recover systolic function fol-lowing surgical revascularization.1
The patients with the most severeleft ventricular (LV) systolic dys-function carry the highest operativerisk,2 but they potentially benefitthe most from coronary artery by-pass grafting (CABG) in terms oflong-term survival.3 However, notevery patient who has ischemic car-diomyopathy with severe LV dys-function regains meaningful systolicfunction following revascularization.Thus, in the context of coronary artery disease, dysfunctional myo-cardium can be the expression ofeither nonviable (necrotic) myo-cardium or viable, but “hibernating,”myocardium, which is in a down-regulated functional state due tochronic ischemia, but the myocardi-um maintains the possibility of regaining function if the coronaryblood flow is restored.
Establishing the presence and ex-tent of myocardial viability in thedysfunctional ischemic myocardiumis clinically important to guide sur-gical revascularization. This conceptis supported by pooled data from3088 patients included in a meta-analysis of 24 studies. This meta-analysis demonstrated a significantsurvival benefit from revasculariz-ing ischemic cardiomyopathy pa-tients with a viable dysfunctionalmyocardium vs medical manage-ment, but no significant differencewas observed between the two treat-ments in patients with a nonviablemyocardium.4 Furthermore, the roleof imaging in assessing myocardialviability to guide the managementof patients with chronic ischemicsystolic LV dysfunction is recognizedin the 2014 ESC/EACTS guidelines
on myocardial revascularization.5 Inparticular, the interaction betweenhibernating myocardium and earlyrevascularization was comparedwith medical therapy, which showedimproved survival with revascular-ization, especially when the extentof viability exceeded 10% of themyocardium.6
Several CMR parameters can beused to assess myocardial viability,including LGE, end-diastolic wallthickness (EDWT), and regional wallmotion abnormality (RWMA) andcontractile reserve.
Late gadolinium enhancement There are multiple imaging modal-ities available to assess viability,such as dobutamine stress echo-cardiography, single-photon emis-sion computed tomography (SPECT),and positron emission tomography(PET).4 However, the ESC/EACTSguidelines on myocardial revascu-larization5 recognize the high diag-nostic accuracy for assessing thetransmurality of myocardial scar byCMR combined with its ability toassess contractile reserve. CMRprovides the highest spatial reso-lution compared with other estab-lished techniques, which enablesCMR to detect as little as an esti-mated 1 g of infarcted myocardiumcompared with the approximate10-g lower limit of SPECT.7 In addi-tion, the reproducibility of the CMRassessment of a chronic infarct isexcellent.8 However, the guidelinesalso concede that the overall dif-ferences in performance betweenmodalities are small, and that lo-cal experience and availability arelikely the major determinants ofwhich technique should be used.5
LGE imaging forms an integral partof the viability assessment by CMR.The principles underpinning CMRviability imaging are different fromthose with stress echocardiography
or nuclear imaging. Briefly, viabilityimaging by CMR is based on the in-travenous administration of a gado-linium-based contrast agent that is metabolically inert, but promptlydiffuses from the intravascular poolinto the extracellular tissue com-partment to reduce the myocardialT1 relaxation times (and to a lesserdegree, the T2 relaxation times).Therefore, the contrast agent accu-mulates in areas of increased extra-cellular space, which is normallycaused by a pathological (ischemicor nonischemic) process. This re-sults in an increased signal returnfrom the tissue containing contrastaccumulation. In fact, in normalmyocardium, the contrast promptlywashes out of the tissue, whereasin nonischemic and ischemic heartdisease (indeed in both acute andchronic myocardial infarction), thecontrast will accumulate with a muchlonger contrast washout.
The optimal time for infarct imag-ing is between 10 to 20 minutes after administering the contrastagent. The accumulation process islikely due to an expanded volumeof distribution in both acute andchronic infarction, but via differentmechanisms. In acute myocardialinfarction, the accumulation resultsfrom increased intracellular uptakedue to disrupted cell membranes inacute infarction; whereas, in chronicmyocardial infarction, it is due toincreased extracellular trappingwithin the increased extracellularspace between the collagen fibersof the chronically scarred myocardi-um.9 An inversion-recovery sequenceis invariably used to exaggerate the difference in signal return fromnormal and infarcted tissue follow-ing the administration of a contrastagent. This inversion signal effective-ly nulls any T1 signal from normalmyocardium, which appears black(hypointense) on the subsequentimage, whereas the infarcted tissue
268
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

still containing contrast will appearapproximately 10-fold brighter (hy-perintense) compared with standardT1-weighted sequences.10
The first step in the LGE assess-ment is simply to determine thepresence or absence of any LGE,which has prognostic implications.Kwong et al11 demonstrated thatthe presence of any degree of LGEin chronic myocardial infarctionpatients led to a 6-fold increase inthe risk of major adverse cardiacevents. The number of segmentsdemonstrating LGE is also impor-tant. In a multicenter, internal studyof 1560 patients, a multivariateanalysis demonstrated than thenumber of segments with LGE wasan independent predictor of mor-tality over a 2.4-year follow-up pe-riod.12 The presence of LGE may bea better prognostic marker in pa-tients with chronic coronary arterydisease than the traditional meas-urement of ejection fraction.12,13 Ina recent study, myocardial scar byLGE was associated with markedlypoorer outcomes in patients with
diabetes mellitus, while the presenceof inducible myocardial ischemiawas found to be predictive both inpatients with and without diabetesmellitus. Both markers surpassedthe predictive value of convention-al atherogenic risk factors both inpatients with and without diabetesmellitus.14
Owing to its spatial resolution,CMR can move beyond the binaryassessment of whether LGE ispresent or absent and quantify thepercentage of the LV wall that is affected by LGE.7 Several methodsexist to quantify transmurality, in-cluding semiautomated objectivetechniques.15 However, subjectivevisual assessment is the most com-monly employed technique in clin-ical settings.16
The importance of LGE transmural-ity in assessing viability in chroniccoronary artery disease was high-lighted in the landmark paper byKim et al,17 which demonstratedthat the lack of LGE prior to treat-ment in patients with ischemic LV
dysfunction undergoing revascular-ization by either CABG or angioplas-ty corresponded to a 78% chanceof segmental functional recoveryon CMR at 3 months postinterven-tion. In comparison, when 51% to75% of the myocardium demon-strated LGE before the intervention,only 10% of the segments function-ally recovered, falling to 2% with atransmural LGE >75% (Figure 1).However, when 1% to 50% of LGEwas present, the likelihood of func-tional recovery was indeterminate(≈50%). Further quantification isrequired to guide the decision re-garding viability in such intermedi-ate myocardial segments. Selvana-yagam et al18 produced similarresults in patients undergoing sur-gical revascularization with a longerCMR follow-up interval of 6 months.Moreover, in patients with ischemicLV dysfunction who are treated med-ically, the presence of dysfunction-al, but viable, myocardium delin-eated by CMR was an independentpredictor of mortality, suggestingthat such patients would benefitinstead from revascularization.19
269
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci
Figure 1. Late gadolinium enhancement transmurality in assessing viability in chronic coronary artery disease.
Panel A. Subendocardial enhancement (white arrow) due to myocardial infarction in the left circumflex artery territory with preserved myocardial viability.Panel B. Transmural enhancement (white arrow) due to myocardial infarction in the left anterior descending territory with nonviable myocardium andthrombus (black arrow).
A
B

The STICH trial (Surgical Treatmentfor IschemiC Heart failure) recentlyquestioned the role of viability,showing that the assessment of my-ocardial viability in patients withcoronary artery disease and LV dys-function did not identify patientswith a differential survival benefitfrom CABG vs medical therapyalone.20 However, there were manypitfalls around the viability imagingin the study (eg, viability imagingwas not randomized, but offered atthe physician’s discretion; multipleviability modalities and no CMR;change in the definition of viability).Further studies are underway toclarify the role of viability imagingin patients with LV dysfunction.
End-diastolic wall thickness The degree of myocardial thinningis related to previous infarct trans-murality.21 An EDWT <6 mm has alow probability of functional recov-ery after revascularization.22,23
However, the clinical utility of thisparameter is limited by the factthat a thinned myocardium can alsorepresent extreme hibernation, withthe potential for an increase in wallthickening and functional recoveryafter revascularization.24
RWMA and contractile reserve RWMA may be systematically iden-tified only when the degree of trans-mural infarct is >50%.25 In isolation,these parameters will underesti-mate infarct size and they will nothelp distinguish the patients withno infarct from those with a trans-mural infarct between 1% and 50%.The poor performance of RWMA inassessing infarct size may be theresult of through-plane myocardialmotion during systole, falsely cre-ating the impression of myocardialshortening on the short axis cines.25
Furthermore, normally contractingmyocardium adjacent to an infarctcan “pull” the infarcted tissue dur-ing systole, simulating contractile
function.25 However, RWMA assess-ment has a role in determining theviability in patients with intermedi-ate LGE of 1% to 50% transmuralitywhen combined with a stressoragent. Kaandorp et al26 demonstrat-ed contractile reserve, as confirmedby the return of regional contractil-ity in response to low-dose dobut-amine stress, in 61% of segmentswith indeterminate LGE in 48 is-chemic cardiomyopathy patients,which implied viability in these seg-ments. Objective quantification ofmyocardial strain in response to low-dose dobutamine can be achievedwith myocardial tagging,27 whichrequires tag lines to be imposedon the cine images at the time ofimage acquisition, or by using anovel postprocessing feature track-ing software that can be applied tostandard cine images.2
Romero et al29 demonstrated theimportance of integrating CMR pa-rameters for viability assessmentin the meta-analysis of 24 studiesthat included 698 patients. Thisanalysis showed that LGE providedthe highest sensitivity (95%) andnegative predictive value (90%),whereas low-dose dobutamine of-fered the best specificity (91%) andpositive predictive valve (93%).
ISCHEMIA ASSESSMENT
Rationale
According to the FAME study (Frac-tional flow reserve versus Angiog-raphy for Multivessel Evaluation),30
revascularization of patients withsymptomatic, but stable, coronaryartery disease should be guided bythe presence of significant myocar-dial ischemia as quantified by frac-tional flow reserve (FFR) at angiog-raphy to achieve prognostic benefitin terms of reduced mortality, ratesof nonfatal infarction, and repeatrevascularization. Furthermore, a
meta-analysis of 11 636 patientswith suspected coronary artery dis-ease with a mean follow-up of 32months demonstrated that confirm-ing the absence of ischemia confersprognostic benefit with very lowannual event rates for cardiovascu-lar death (0.3%) and myocardial in-farction (0.4%).31 When consideringCMR in IHD, the importance of as-sessing ischemia in addition to vi-ability is unclear at the present,32
and a prospective outcome studyto address this question is stillawaited. The ongoing MR-INFORMstudy (MR perfusion ImagiNg andFractional flOw Reserve to guideManagement of patients with stablecoronary artery disease) is assess-ing whether a CMR stress perfusionstrategy is noninferior to FFR instable coronary artery disease.33
The ongoing ISCHEMIA trial (Inter-national Study of ComparativeHealth Effectiveness with Medicaland Invasive Approaches) willdemonstrate whether patients withmoderate to severe ischemia onstress imaging (SPECT, CMR, stressecho) will benefit from coronaryangiography and revascularization.34
Ischemia assessment by CMR canbe performed by either stress per-fusion imaging or stress functionalimaging, although perfusion mayalso be included with the latter.
Stress first-pass myocardial perfu-sion for inducible perfusion defectsFirst-pass myocardial perfusionCMR was first described by Atkinsonet al using inversion-recovery gra-dient-echo imaging after injectinga bolus of a T1-shortening contrastagent to observe contrast agenttransit through the cardiac chambersand myocardium.35 Subsequently,the technique has undergone sev-eral developments, including im-proved spatial resolution, speed ofacquisition, myocardial coverage,and improved signal-to-noise ratio,thereby increasing the overall accu-
270
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

racy of the technique. Myocardialperfusion imaging is usually carriedout at peak stress with intravenousvasodilator stress (most commonlywith adenosine) and at rest. At peakstress, the images can demonstrateareas of hypoperfusion, which is asurrogate for myocardial ischemia.Due to its high spatial resolution(up to 2 to 3 mm), CMR myocardialperfusion imaging is superior toother imaging modalities in reliablyidentifying subendocardial ischemia.Recent developments have reduced
the spatial resolution to ≈1 mm.36
Moreover, higher performing scan-ners with high magnetic fields (3T)can improve the signal-to-noise ra-tio, thus improving the diagnosticyield of the technique by identify-ing even smaller perfusion defectsand increasing the ability to ruleout artifacts.37
In perfusion CMR, the stressor isoften a vasodilator agent, most com-monly adenosine, which results incoronary artery dilatation. Coronaryarteries with significant stenosiswill dilate less than unobstructedvessels, effectively resulting in a“steal” phenomenon with relative
hypoperfusion of the myocardiumsubtended by the stenosed coronaryartery (Figure 2). Consequently, va-sodilator stress CMR is an inappro-priate modality to assess ischemicburden associated with myocardialbridging of coronary arteries or amalignant coronary course wherethe coronary obstruction is dynamicand worsens with increased cardiacworkload. Therefore, chronotropicand inotropic stressors are recom-mended instead (exercise or dobu-tamine). Ischemia is demonstrated
as a myocardial perfusion defecton first-pass imaging with an intra-venous gadolinium-chelate contrastagent. First-pass imaging is usuallyperformed at both peak stress and atrest (20 min after stress). Inducibleperfusion defects appear as a hypo-intense area (dark area, ie, no per-fusion or delayed-contrast perfu-sion due to coronary stenosis), butunfortunately, artifacts could mim-ic inducible perfusion defects andtend to appear in conjunction withcontrast arrival in the LV cavity.
Therefore, the acquisition of bothsets of images (at stress and at rest)is useful to distinguish a true per-
fusion defect from artifact. Hypo-intensity that is only present in thestress images is suggestive of aninducible perfusion defect, whereashypoperfusion present in both stressand rest images is suggestive of anartifact.
Dipyridamole and regadenoson arealternative vasodilator stress agents.Dipyridamole inhibits the cellularuptake and metabolism of adeno-sine, which causes an increase inthe interstitial adenosine concen-tration. Regadenoson is an adeno-sine receptor agonist. These agentsgive rise to a super physiologic in-crease in vascular flow as opposedto the approximate 2-fold increasein vascular flow seen with dobuta-mine or exercise. In contrast toadenosine or dipyridamole stressprotocols involving continuous infusion for 3 to 5 minutes, the re-gadenoson stress protocol uses asingle-bolus injection to obviate theneed for a second intravenous line.The contraindications for adeno-sine or adenosine agonists includehigh-degree atrioventricular block,obstructive airway disease, and con-comitant administration of dipyri-damole or carbamazepine. Thesecontraindications are infrequent, butof important general knowledge forany clinician referring patients forstress CMR. Caffeinated food anddrink should be avoided before thetest as it reduces the efficacy of thestressor.
In clinical practice, the perfusionimages are reported qualitatively,and they are based on the assess-ment of the presence and extent ofmyocardial hypoperfusion (trans-murality and number of segments)and the correspondence with thecoronary artery territories. Quanti-tative assessment of myocardialperfusion is predominantly confinedto the research domain. Semiquan-titative assessment of first-pass
271
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci
Figure 2. Basal, mid, and apical short-axis (left to right) stress (Panel A) and rest(Panel B) perfusion images with inducible myocardial perfusion defect (white arrows).
A
B

perfusion by measuring changes inmyocardial signal intensity overtime provides information on rela-tive perfusion; in addition, there isalso research on the quantificationof absolute myocardial blood flowwith CMR.38
There are several challenges forstress perfusion imaging. A com-monly encountered imaging artifactis the dark-rim artifact, which ap-pears at the interface of the bloodpool and the subendocardium, whichmay mimic a perfusion defect. Thephysics behind its etiology is in-completely understood, but it canbe distinguished from pathologybecause it appears as soon as thecontrast arrives in the LV cavity, itrapidly fades away (but may reoc-cur during the second pass of con-trast), and it is usually darker thana true perfusion defect. This artifactmay compound the challenges pre-sented by assessing severe triple-vessel coronary artery disease bystress perfusion CMR. The lack of a region of normal perfusion to actas a reference standard makes as-sessment difficult in this condition.
However, in these cases, endo-epi-cardial perfusion gradients mayserve as a marker of ischemia.39
Equally, the assessment of microvas-cular obstruction (ie, cardiac syn-drome X) can be challenging in thecontext of a dark-rim artifact, par-ticularly because subendocardialperfusion defects crossing anticipat-ed coronary artery territory bound-aries are recognized imaging fea-tures on stress perfusion CMR inthese patients.40
Vasodilator stress CMR correlateswell with FFR, which is the currentin-vivo gold standard assessment ofhemodynamically significant coro-nary stenosis.41 Other modalitiesexist to assess ischemia, but in arecent meta-analysis of 166 articles
assessing SPECT, PET, and CMR forthe detection of angiographic coro-nary artery disease,42 The CMR diag-nostic accuracy was similar to PET(pooled sensitivity, 89%; 95% confi-dence interval [CI], 88% to 91% and pooled specificity, 76%; 95% CI,73% to 78%), and CMR achieved thehighest diagnostic performance, butwithout exposure to ionizing radia-tion. Stress CMR also performs favorably in cost-effective analysesassessing diagnostic pathways forthe work-up of suspected coronaryartery disease.
MR-IMPACT (Magnetic ResonanceImaging for Myocardial PerfusionAssessment in Coronary artery disease Trial), the first multicenter,multivendor, randomized trial, sug-gested perfusion CMR as a valuablealternative to SPECT.44 The subse-quent MR-IMPACT II trial showedthat perfusion CMR was superiorto SPECT, while its specificity wasinferior to SPECT.45 The large, pros-pective CE-MARC study (ClinicalEvaluation of MAgnetic resonanceimaging in Coronary heart disease)established CMR’s high diagnosticaccuracy in IHD and its superiorityover SPECT.46 In both sexes, CMRhas a greater sensitivity than SPECTwith no intersex differences.47 StressCMR also performs favorably incost-effective analyses assessingdiagnostic pathways for the workupof suspected coronary artery dis-ease.43 The recently published 5-yearfollow-up study of CE-MARC indi-cates that compared with SPECT,CMR is a stronger predictor of riskfor major adverse cardiovascularevents (MACEs), which is independ-ent of cardiovascular risk factors,angiography result, or initial patienttreatment.48 This further supportsthe role of CMR as a slightly supe-rior alternative to SPECT for the diagnosis and management of pa-tients with suspected coronaryheart disease.
In a small group of patients show-ing CMR evidence of a significantmyocardial-inducible perfusion de-fect and viability, chronic total oc-clusion recanalization was shownto reduce ischemic burden, whichfavors reverse remodeling and ame-liorates quality of life.49
Stress functional imaging for inducible RWMA Ischemia assessment via function-al stress imaging is performed bycomparing the ventricular functionat rest with peak stress. Regionalventricular function can be assessedvisually50 or by measuring wall motion, thickening, and strain.51
Although there is some initial ex-perience showing that physical exer-cise can be performed in the CMRscanner with a compatible supineergometer,52 stress CMR functionalimaging is commonly achieved withdobutamine.
As a b-agonist, dobutamine stimu-lates myocardial b-receptors, re-sulting in increased myocardialcontractility, heart rate, and strokevolume. The principle of dobuta-mine stress CMR is that the agentis administered at increasing doseswith interval imaging until the tar-get heart rate (which may requirethe administration of atropine) isachieved or angina symptoms areexperienced. Abnormal blood pres-sure response and development ofsevere arrhythmia should promptcessation of the test. When thecoronary vasculature is normal, my-ocardial contractility will progres-sively increase with an increasingdobutamine dose. In the presenceof a flow-limiting coronary steno-sis, the myocardium will becomeincreasingly ischemic with an in-creasing dobutamine dose, and theresultant systolic dysfunction willbe manifest as a new RWMA that isrelative to the baseline images atlower doses. The regain of function
272
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

in areas of RWMA at baseline is ev-idence of contractile reserve in hi-bernating myocardium.
The role of stress CMR in ischemiaassessment has been recognized inthe International guidelines on theassessment of coronary artery dis-ease. The 2013 European Societyof Cardiology (ESC) guidelines onthe management of stable coronaryartery disease list stress perfusionCMR as one of the recommendedmodalities to noninvasively assesspatients with a pretest probabilityof coronary artery disease between15% and 85% (class I recommenda-tion).53 The National Institute forHealth and Care Excellence (NICE)recommends noninvasive ischemiaimaging, including stress CMR, inpatients in whom stable angina isnot excluded by clinical assess-ment with an estimated 30% to 60%likelihood of coronary artery dis-ease and in patients with an esti-mated 61% to 90% likelihood ofcoronary artery disease after theresting ECG, providing that revas-cularization is not being consideredor if invasive angiography is notclinically appropriate or tolerated bythe patient.54 Stress CMR receiveda class IIa recommendation in sev-eral clinical settings in the 2012ACCF/AHA chest pain guidelines,giving a class I recommendationfor exercise ECG, nuclear perfusion,and stress echocardiography.55
Stress CMR received a class IIa rec-ommendation in several clinicalsettings in the 2012 ACC/AHA chestpain guidelines.55
The most common method for quan-tifying the presence of ischemia indobutamine stress CMR is visualanalysis of the worsening RWMAusing the American Heart Associa-tion 16 (or 17) segment model.Using this approach, a sensitivityof 83% to 96% and a specificity of80% to 100% can be achieved.56
Quantifying RWMA by myocardialtagging in this context increasesdiagnostic accuracy.57 Furthermore,employing an objective strain analy-sis technique may enable detectionof ischemic myocardium below con-ventional levels of peak stress,58 po-tentially reducing the requirementfor higher-dose protocols.
Finally, the role of combining stressperfusion and stress functional im-aging for ischemia has been inves-tigated. In a study on 455 patients,this approach showed an increasedsensitivity, but a reduced specifici-ty, with no overall change in accu-racy.59 However, this approach mightbe particularly beneficial in patientswith concentric hypertrophy andremodeling because RWMA can bemore difficult in this patients sub-set.60
ASSESSMENT OF CHRONICCOMPLICATIONS FROMMYOCARDIAL INFARCTION
CMR also has a role in assessingchronic complications following amyocardial infarction. CMR is su-perior to echocardiography for theidentification of ventricular thrombi,which appear as dark-filling defectson early gadolinium enhancementor LGE imaging, typically on theendocardial surface of infarcts(Figure 1).61,62 CMR is also able todetect other chronic complicationsof a myocardial infarction, includingventricular aneurysm, pseudoa-neurysms, and mitral regurgitation.Furthermore, the high spatial reso-lution of CMR can assess the in-volvement of the right ventricle ina myocardial infarction when com-pared with echocardiography.63
FUTURE PERSPECTIVE
Quantitative myocardial perfusionreserve assessment by CMR is apromising new dimension.64 In an
animal model, CMR-derived quan-titative blood flow estimates havebeen correlated with true myocardialblood flow.65 Perfusion CMR is, intheory, more related to coronary flowreserve (CFR) than FFR, although it has been validated against bothCFR and FFR.66,67 Recently, exercisestress CMR has been investigatedin healthy volunteers, showing thatpeak exercise wall motion as as-sessed by cine CMR is feasible, andit can be performed as rapidly asstress echocardiography.68
The evidence on assessing IHD withan advanced T1 relaxometry tech-nique seems promising. A recentstudy has shown that T1 mappingat rest and during adenosine stresscan differentiate between normal,infarcted, ischemic, and remote my-ocardium with distinctive T1 pro-files. The results of ischemia detec-tion by noncontrast stress/rest T1mapping were also encouraging. 69
CONCLUSION
CMR is a well-established, compre-hensive, and increasingly used non-invasive imaging modality for theassessment of patients with IHD.CMR can assess cardiac anatomy,function, myocardial perfusion, andtissue characterization, without ex-posure to ionizing radiation, and itcan be done in less than 1 hour. Itsuse in IHD is supported by robustand rapidly expanding evidence.
The challenge is to delineate howCMR can improve patient manage-ment and improve clinical out-comes in a cost-effective manner.
Acknowledgments. This work was supported by
the Bristol NIHR Cardiovascular Biomedical
Research Unit at the Bristol Heart Institute. The
views expressed are those of the authors and not
necessarily those of the UK National Health
Service, National Institute for Health Research,
or Department of Health.
273
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

REFERENCES
1. Rees G, Bristow JD, Kremkau EL,et al.
Influence of aortocoronary bypass surgeryon left ventricular performance.
N Engl J Med. 1971;284:1116-1120.
2. Alderman EL, Fisher LD, Litwin P,et al.
Results of coronary artery surgery in patientswith poor left ventricular function (CASS).
Circulation. 1983;68:785-795.
3. Muhlbaier LH, Pryor DB, Rankin JS,et al.
Observational comparison of event-free survival with medical and surgical therapyin patients with coronary artery disease. 20 years of follow-up.
Circulation. 1992;86(suppl 5):II198-II204.
4. Allman KC, Shaw LJ, HachamovitchR, Udelson JE.
Myocardial viability testing and impact ofrevascularization on prognosis in patientswith coronary artery disease and left ven-tricular dysfunction: a meta-analysis.
J Am Coll Cardiol. 2002;39:1151-1158.
5.Windecker S, Kolh P, Alfonso F, et al.
2014 ESC/EACTS Guidelines on myocardialrevascularization.
Eur Heart J. 2014;35:2541-2619.
6. Ling LF, Marwick TH, Flores DR, et al.
Identification of therapeutic benefit fromrevascularization in patients with left ventric-ular systolic dysfunction: inducible ischemiaversus hibernating myocardium.
Circ Cardiovasc Imaging. 2013;6:363-372.
7. Wagner A, Mahrholdt H, Holly TA,et al.
Contrast-enhanced MRI and routine singlephoton emission computed tomography(SPECT) perfusion imaging for detection of subendocardial myocardial infarcts: animaging study.
Lancet. 2003;361:374-379.
8. Mahrholdt H, Wagner A, Holly TA,et al.
Reproducibility of chronic infarct size meas-urement by contrast-enhanced magneticresonance imaging.
Circulation. 2002;106:2322-2327.
9. Kim RJ, Choi KM, Judd RM.
Assessment of myocardial viability by contrastenhancement. In: Higgins CB, Roos AD, eds.
Cardiovascular MRI and MRA. Philadel-phia, PA, USA: Lippincott; 2003:209-237.
10. Simonetti OP, Kim RJ, Fieno DS,et al.
An improved MR imaging technique for thevisualization of myocardial infarction.
Radiology. 2001;218:215-223.
11. Kwong RY, Chan AK, Brown KA, et al.
Impact of unrecognized myocardial scar detected by cardiac magnetic resonance im-aging on event-free survival in patients pre-senting with signs or symptoms of coronaryartery disease.
Circulation. 2006;113:2733-2743.
12. Klem I, Shah DJ, White RD, et al.
Prognostic value of routine cardiac magneticresonance assessment of left ventricularejection fraction and myocardial damage:an international, multicenter study.
Circ Cardiovasc Imaging. 2011;4:610-619.
13. Catalano O, Moro G, Perotti M, et al.
Late gadolinium enhancement by cardiovas-cular magnetic resonance is complementaryto left ventricle ejection fraction in predictingprognosis of patients with stable coronaryartery disease.
J Cardiovasc Magn Reson. 2012;14:29.
14. Giusca S, Kelle S, Nagel E, et al.
Differences in the prognostic relevance ofmyocardial ischaemia and scar by cardiacmagnetic resonance in patients with andwithout diabetes mellitus.
Eur Heart J Cardiovasc Imaging. 2016;17:812-820.
15. Amado LC, Gerber BL, Gupta SN,et al.
Accurate and objective infarct sizing by con-trast-enhanced magnetic resonance imagingin a canine myocardial infarction model.
J Am Coll Cardiol. 2004;44:2383-2389.
16. Hsu LY, Natanzon A, Kellman P,Hirsch GA, Aletras AH, Arai AE.
Quantitative myocardial infarction on delayedenhancement MRI. Part I: animal validationof an automated feature analysis and com-bined thresholding infarct sizing algorithm.
J Magn Reson Imaging. 2006;23:298-308.
17. Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversiblemyocardial dysfunction.
N Engl J Med. 2000;343:1445-1453.
18. Selvanayagam JB, Kardos A,Francis JM, et al. Value of delayed-enhancement cardiovascularmagnetic resonance imaging in predictingmyocardial viability after surgical revascu-larization.
Circulation. 2004;110:1535-1541.
19. Gerber BL, Rousseau MF, Ahn SA,et al. Prognostic value of myocardial viability bydelayed-enhanced magnetic resonance inpatients with coronary artery disease andlow ejection fraction: impact of revascular-ization therapy.
J Am Coll Cardiol. 2012;59:825-835.
20. Bonow RO, Maurer G, Lee KL, etal; STICH Trial Investigators. Myocardial viability and survival in ischemicleft ventricular dysfunction.
N Engl J Med. 2011;364:1617-1625.
21. Baer FM, Smolarz K, JungehülsingM, et al. Chronic myocardial infarction: assessment ofmorphology, function, and perfusion by gra-dient echo magnetic resonance imaging and99mTc-methoxyisobutyl-isonitrile SPECT.
Am Heart J. 1992;123:636-645.
22. Schinkel AF, Bax JJ, Poldermans D,Elhendy A, Ferrari R, Rahimtoola SH. Hibernating myocardium: diagnosis andpatient outcomes.
Curr Probl Cardiol. 2007;32:375-410.
23. Kaandorp TA, Lamb HJ, van derWall EE, de Roos A, Bax JJ. Cardiovascular MR to access myocardialviability in chronic ischaemic LV dysfunction.
Heart. 2005;91:1359-1365.
24. John AS, Dreyfus GD, Pennell DJ. Images in cardiovascular medicine. Reversiblewall thinning in hibernation predicted bycardiovascular magnetic resonance.
Circulation. 2005;111:e24-e25.
25. Mahrholdt H, Wagner A, Parker M,et al. Relationship of contractile function totransmural extent of infarction in patientswith chronic coronary artery disease.
J Am Coll Cardiol. 2003;42:505-512.
274
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

26. Kaandorp TA, Bax JJ, Schuijf JD,et al.
Head-to-head comparison between contrast-enhanced magnetic resonance imaging anddobutamine magnetic resonance imagingin men with ischemic cardiomyopathy.
Am J Cardiol. 2004;93:1461-1464.
27. Bree D, Wollmuth JR, Cupps BP,et al.
Low-dose dobutamine tissue-tagged magneticresonance imaging with 3-dimensional strainanalysis allows assessment of myocardial via-bility in patients with ischemic cardiomyopathy.
Circulation. 2006;114(suppl 1):I33-I36.
28. Schuster A, Paul M, Bettencourt N,et al.
Cardiovascular magnetic resonance myocar-dial feature tracking for quantitative viabil-ity assessment in ischemic cardiomyopathy.
Int J Cardiol. 2013;166:413-420.
29. Romero J, Xue X, Gonzalez W,Garcia MJ.
CMR imaging assessing viability in patientswith chronic ventricular dysfunction due tocoronary artery disease: a meta-analysis ofprospective trials.
JACC Cardiovasc Imaging. 2012;5:494-508.
30. Tonino PA, De Bruyne B, PijlsNH, et al; FAME Study Investigators.
Fractional flow reserve versus angiography forguiding percutaneous coronary intervention.
N Engl J Med. 2009;360:213-224.
31. Lipinski MJ, McVey CM, BergerJS, Kramer CM, Salerno M.
Prognostic value of stress cardiac magneticresonance imaging in patients with knownor suspected coronary artery disease: a sys-tematic review and meta-analysis.
J Am Coll Cardiol. 2013;62:826-838.
32. Schuster A, Nagel E.
Letter by Schuster and Nagel regarding article,“Predicting benefit from revascularization inpatients with ischemic heart failure: imag-ing of myocardial ischemia and viability.”
Circulation. 2011;124:e296.
33. Hussain ST, Paul M, Plein S, et al.
Design and rationale of the MR-INFORMstudy: stress perfusion cardiovascular mag-netic resonance imaging to guide the man-agement of patients with stable coronaryartery disease.
J Cardiovasc Magn Reson. 2012;14:65.
34. Shaw LJ, Berman DS, PicardMH, et al; NIH/NHLBI-Sponsored ISCHEMIA Trial Investigators.
Comparative definitions for moderate-severeischemia in stress nuclear, echocardiography,and magnetic resonance imaging.
JACC Cardiovasc Imaging. 2014;7:593-604.
35. Atkinson DJ, Burstein D,Edelman RR.
First-pass cardiac perfusion: evaluationwith ultrafast MR imaging.
Radiology. 1990;174(3 pt 1):757-762.
36. Plein S, Ryf S, Schwitter J,Radjenovic A, Boesiger P, Kozerke S.
Dynamic contrast-enhanced myocardialperfusion MRI accelerated with k-t sense.
Magn Reson Med. 2007;58:777-785.
37. Cheng AS, Pegg TJ, KaramitsosTD, et al.
Cardiovascular magnetic resonance perfu-sion imaging at 3-tesla for the detection ofcoronary artery disease: a comparison with1.5-tesla.
J Am Coll Cardiol. 2007;49:2440-2449.
38. Patel AR, Antkowiak PF,Nandalur KR, et al.
Assessment of advanced coronary arterydisease: advantages of quantitative cardiacmagnetic resonance perfusion analysis.
J Am Coll Cardiol. 2010;56:561-569.
39. Motwani M, Kidambi A,Greenwood JP, Plein S.
Advances in cardiovascular magnetic reso-nance in ischaemic heart disease and non-ischaemic cardiomyopathies.
Heart. 2014;100:1722-1733.
40. Panting JR, Gatehouse PD, YangGZ, et al.
Abnormal subendocardial perfusion in car-diac syndrome X detected by cardiovascularmagnetic resonance imaging.
N Engl J Med. 2002;346:1948-1953.
41. Lockie T, Ishida M, Perera D, et al.
High-resolution magnetic resonance my-ocardial perfusion imaging at 3.0-Tesla todetect hemodynamically significant coro-nary stenoses as determined by fractionalflow reserve.
J Am Coll Cardiol. 2011;57:70-75.
42. Jaarsma C, Leiner T, Bekkers SC,et al.
Diagnostic performance of noninvasive my-ocardial perfusion imaging using single-photon emission computed tomography,cardiac magnetic resonance, and positronemission tomography imaging for the detec-tion of obstructive coronary artery disease:a meta-analysis.
J Am Coll Cardiol. 2012;59:1719-1728.
43. Walker S, Girardin F, McKenna C,et al.
Cost-effectiveness of cardiovascular magneticresonance in the diagnosis of coronary heartdisease: an economic evaluation using datafrom the CE-MARC study.
Heart. 2013;99:873-881.
44. Schwitter J, Wacker CM, van Rossum AC, et al.
MR-IMPACT: comparison of perfusion-cardiac magnetic resonance with single-photon emission computed tomography forthe detection of coronary artery disease in amulticentre, multivendor, randomized trial.
Eur Heart J. 2008;29:480-489.
45. Schwitter J, Wacker CM, Wilke N,et al; MR-IMPACT Investigators.
MR-IMPACT II: Magnetic ResonanceImaging for Myocardial PerfusionAssessment in Coronary artery diseaseTrial: perfusion-cardiac magnetic resonancevs. single-photon emission computed tomog-raphy for the detection of coronary arterydisease: a comparative multicentre, multi-vendor trial.
Eur Heart J. 2013;34:775-781.
46. Greenwood JP, Maredia N,Younger JF, et al.
Cardiovascular magnetic resonance andsingle-photon emission computed tomographyfor diagnosis of coronary heart disease(CE-MARC): a prospective trial.
Lancet. 2012;379:453-460.
47. Greenwood JP, Motwani M,Maredia N, et al.
Comparison of cardiovascular magneticresonance and single-photon emission com-puted tomography in women with suspectedcoronary artery disease from the ClinicalEvaluation of Magnetic Resonance Imagingin Coronary Heart Disease (CE-MARC) Trial.
Circulation. 2014;129:1129-1138.
275
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

48. Greenwood JP, Herzog BA,Brown JM, et al.
Prognostic value of cardiovascular magneticresonance and single-photon emission com-puted tomography in suspected coronaryheart disease: long-term follow-up of aprospective, diagnostic accuracy cohort study.
Ann Intern Med. 2016 May 10. Epubahead of print.
49. Bucciarelli-Ducci C, Auger D, Di Mario C, et al.
CMR guidance for recanalization of coronarychronic total occlusion.
JACC Cardiovasc Imaging. 2016;9:547-556.
50. Hoffmann R, von Bardeleben S,Kasprzak JD, et al.
Analysis of regional left ventricular func-tion by cineventriculography, cardiac mag-netic resonance imaging, and unenhancedand contrast-enhanced echocardiography:a multicenter comparison of methods.
J Am Coll Cardiol. 2006;47:121-128.
51. Rutz AK, Ryf S, Plein S, BoesigerP, Kozerke S.
Accelerated whole-heart 3D CSPAMM formyocardial motion quantification.
Magn Reson Med. 2008;59:755-763.
52. Pieles GE, Szantho G, RodriguesJCL, et al.
Adaptations of aortic and pulmonary arteryflow parameters measured by phase-contrastmagnetic resonance angiography duringsupine aerobic exercise.
Eur J Appl Physiol. 2014;114:1013-1023.
53. Montalescot G, Sechtem U,Achenbach S, et al.
2013 ESC guidelines on the managementof stable coronary artery disease.
Eur Heart J. 2013;34:2949-3003.
54. NICE clinical guideline 95.
Chest pain of recent onset: assessment anddiagnosis of recent onset chest pain or dis-comfort of suspected cardiac origin.
www.nice.org.uk/guidance/CG95. PublishedMarch 2010. Accessed August 02, 2016.
55. Fihn SD, Gardin JM, Abrams J, et al.
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis andmanagement of patients with stable ischemicheart disease.
J Am Coll Cardiol. 2012;60:e44-e164.
56. Strach K, Meyer C, Schild H,Sommer T.
Cardiac stress MR imaging with dobutamine.
Eur Radiol. 2006;16:2728-2738.
57. Kuijpers D, Ho KY, van DijkmanPR, Vliegenthart R, Oudkerk M.
Dobutamine cardiovascular magnetic reso-nance for the detection of myocardial ischemiawith the use of myocardial taggin
Circulation. 2003;107:1592-1597.
58. Korosoglou G, Lehrke S,Wochele A, et al.
Strain-encoded CMR for the detection of inducible ischemia during intermediate stress.
JACC Cardiovasc Imaging. 2010;3:361-371.
59. Gebker R, Jahnke C, Manka R,et al.
Additional value of myocardial perfusionimaging during dobutamine stress magnet-ic resonance for the assessment of coronaryartery disease.
Circ Cardiovasc Imaging. 2008;1:122-130.
60. Gebker R, Mirelis JG, Jahnke C,et al.
Influence of left ventricular hypertrophyand geometry on diagnostic accuracy ofwall motion and perfusion magnetic reso-nance during dobutamine stress.
Circ Cardiovasc Imaging. 2010;3:507-514.
61. Mollet NR, Dymarkowski S,Volders W, et al.
Visualization of ventricular thrombi withcontrast-enhanced magnetic resonance imag-ing in patients with ischemic heart disease.
Circulation. 2002;106:2873-2876.
62. Weinsaft JW, Kim HW, Shah DJ,et al.
Detection of left ventricular thrombus bydelayed-enhancement cardiovascular mag-netic resonance prevalence and markers inpatients with systolic dysfunction.
J Am Coll Cardiol. 2008;52:148-157.
63. Kumar A, Abdel-Aty H,Kriedemann I, et al.
Contrast-enhanced cardiovascular magneticresonance imaging of right ventricular infarction.
J Am Coll Cardiol. 2006;48:1969-1976.
64. Patel AR, Antkowiak PF,Nandalur KR, et al.
Assessment of advanced coronary arterydisease: advantages of quantitative cardiacmagnetic resonance perfusion analysis.
J Am Coll Cardiol. 2010;56:561-569.
65. Schuster A, Zarinabad N, IshidaM, et al.
Quantitative assessment of magnetic reso-nance derived myocardial perfusion measure-ments using advanced techniques: micros-phere validation in an explanted pig heartsystem.
J Cardiovasc Magn Reson. 2014;16:82.
66. Kurita T, Sakuma H, Onishi K, et al.
Regional myocardial perfusion reserve deter-mined using myocardial perfusion magneticresonance imaging showed a direct correla-tion with coronary flow velocity reserve byDoppler flow wire.
Eur Heart J. 2009;30:444-452.
67. Costa MA, Shoemaker S,Futamatsu H, et al.
Quantitative magnetic resonance perfusionimaging detects anatomic and physiologiccoronary artery disease as measured by coro-nary angiography and fractional flow reserve.
J Am Coll Cardiol. 2007;50:514-522.
68. Thavendiranathan P, DickersonJA, Scandling D, et al.
Comparison of treadmill exercise stress cardiac MRI to stress echocardiography inhealthy volunteers for adequacy of left ventricular endocardial wall visualization: a pilot study.
J Magn Reson Imaging. 2014;39:1146-1152.
69. Liu A, Wijesurendra RS, FrancisJM, et al.
Adenosine stress and rest T1 mapping candifferentiate between ischemic, infarcted,remote, and normal myocardium withoutthe need for gadolinium contrast agents.
JACC Cardiovasc Imaging. 2016;9:27-36.
276
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
IHD and cardiac magnetic resonance imaging - Dastidar and Bucciarelli-Ducci

277
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
oronary computed tomog-raphy angiography (CCTA)has opened a new road tothe understanding of coro-
nary artery disease (CAD). Sincethe early beginnings of CCTA, theuse of electron-beam computed to-mography (CT) to depict coronaryarteries has significantly progressedand has achieved superb spatialresolution with ever-declining radia-tion requirements. This article willreview the use of CCTA in preven-tive medicine, in patients with sta-ble CAD, and in patients with acutecoronary syndromes.
TECHNIQUE
Coronary artery imaging requireshigh temporal and spatial resolu-tion to capture the fast moving smallstructures accurately. State-of-the-
art CT machines achieve temporalresolutions down to 66 ms with spa-tial resolutions ranging from 0.5 to0.625 mm.1 By employing a combi-nation of high-pitch spiral acquisi-tions at a low kV and raw data-basediterative reconstruction, CCTA cannow be performed at a radiationdose as low as 0.06 mSv with suffi-cient image quality in selected patients.2 The dose of radiation increases and the image qualitydecreases with an increasing heartrate. Thus, it is recommended togive b-blockers to patients with aresting heart rate >65 bpm.3 Onlythe patients with adequate breathholding capabilities, without severeobesity, with a favorable calciumscore (eg, Agatston score <400)and distribution, in sinus rhythm,and with a heart rate ≤65 bpmshould be considered for CCTA.4
If a calcium score is not obtainedand calcifications are only seen onthe completed coronary CT angio-gram, it may be prudent to refrainfrom stenosis quantification in areasof extensive calcifications. Even insegments without severe calcifica-tions, CCTA tends to underestimatethe coronary lumen and hence thecoronary stenosis severity. Whencompared with the cross-sectionalareas of the lumen measured byintravascular ultrasound, CT valuestend to be smaller with higher inter-observer variability.5 CCTA requiresthe application of contrast media,which limits its use in patients withchronic kidney disease.
Copyright © 2016, AICH - Servier Research Group. All rights reserved www.dialogues-cvm.org
C
Coronary artery disease imaging: what is the role ofcoronary computed tomography angiography?Udo Sechtem, MD
Abteilung für Kardiologie - Robert-Bosch-Krankenhaus - Stuttgart - GERMANY
Keywords: coronary artery calcium; coro-nary artery disease; coronary computed tomography angiography Address for correspondence:Prof Dr Udo Sechtem, Abteilung fürKardiologie, Robert-Bosch-Krankenhaus,Auerbachstr. 110 D-70136 Stuttgart,Germany (e-mail: [email protected])Dialogues Cardiovasc Med. 2016;21:277-286
Techniques, such as coronary com-puted tomography angiography(CCTA), have been instrumentalfor the advancements in our un-derstanding of coronary arterydisease. The advent of CCTA willsignificantly change the treatmentapproach for three types of pa-tients. For asymptomatic, buthigh-risk patients, CCTA canidentify the presence, extent, andcontent of plaque formation quick-ly and precisely to determine thebest option for medical therapy.For patients with stable coronaryartery disease, CCTA can reliablyexclude epicardial stenosis to min-imize the number of patients whowill need to undergo invasivecoronary angiography. Finally,for patients with low-risk acutecoronary syndromes, the combina-tion of high-sensitivity troponinsand CCTA will safely reduce thenumber of subsequent outpatientprocedures, which will lessen theburden on often-underfinancedhealth care systems.
SELECTED ABBREVIATIONSAND ACRONYMS
CAC coronary artery calcium
CAD coronary artery disease
CCTA coronary computed tomo-graphy angiography
FFR fractional flow reserve
MESA Multi-Ethnic Study of Atherosclerosis
SPECT single-photon emission computed tomography
TAG transluminal attenuation gradient

PREVENTIVE MEDICINE
In asymptomatic subjects with ath-erosclerotic risk factors, screeningfor coronary artery calcium (CAC) isa powerful tool to determine prog-nosis with a predictive power be-yond that of customary risk scores,such as the Framingham score orthe ESC SCORE (European Societyof Cardiology Systematic COronaryRisk Evaluation). Usually, theamount of coronary calcification isexpressed using the Agatston score,which weighs both the density andthe extent of the calcifications. Tech-nically, CAC scoring is performedwithout using contrast media, andthe radiation burden is <1 mSv.Prognostic studies confirm the su-perior predictive benefit of CAC. Forinstance, Silverman et al6 reportedthe CAC scores for 6698 individualsfrom the MESA study (Multi-EthnicStudy of Atherosclerosis), and theresults confirm that the prevalenceof intense calcifications (CAC >300)increased with an increasing num-ber of conventional risk factors.Nevertheless, one-third of the pa-tients with ≥3 risk factors had a CACscore of 0. Among patients with zerorisk factors, 5% had a CAC score>300. Interestingly, patients withzero risk factors and a CAC score>300 had an event rate 3.5-timeshigher than individuals with ≥3 riskfactors and a CAC score of 0 (10.9/1000 vs 3.1/1000 person-years).Consequently, the 2016 Europeanguidelines on cardiovascular dis-ease prevention in clinical practice7
consider the CT CAC score to be arisk modifier with reclassificationpotential vs conventional risk scores.
CCTA has also been proposed as a means of having a more preciseprediction of coronary events inprimary prevention. Compared withthe CAC scoring, CCTA adds infor-mation about noncalcified andmixed plaques. The former may be
prognostically important in youngpatients in whom plaque may notyet have had the time to becomepartially calcified. However, in alarge series of patients followed-upfor 22 months, Cho et al showedthat asymptomatic patients with a CAC score of 0 with noncalcifiedplaque did not have an additionalrisk for exclusive noncalcified plaquecompared with asymptomatic pa-tients without noncalcified plaque.8
In another study by Cho et al, 7590asymptomatic patients were fol-lowed-up for a median of 24 months.Patients with obstructive 2- or 3-vessel disease or left main coronaryartery disease experienced higherrates of death and myocardial in-farction (P<0.05). Both CAC scoresand CCTA significantly improvedthe performance of standard riskfactor prediction models, but theincremental discriminatory valueassociated with their inclusion wasmore pronounced for both thecomposite outcome (all-cause mor-tality and myocardial infarction)and CAC scoring. The net reclassifi-cation improvement resulting fromthe addition of CCTA to a modelbased on standard risk factors andCAC scoring was negligible.9 A re-cent subanalysis of the data indi-cated that there was an incremen-tal value of CCTA (the number ofvessels with ≥50% stenosis was usedto grade the extent and severity ofCAD) in individuals with a CACscore >100, but not for those witha score ≤100.10
Another recent study by Dedic et alpointed in the same direction. Theyfound an additional prognostic ben-efit provided by CCTA in asympto-matic high-risk patients (diabetesmellitus, familial hypercholesterol-emia, peripheral artery disease, orsevere hypertension) beyond theinformation given by age, sex, andCAC scoring.11 Thus, it is not yet
clear whether CCTA is useful inasymptomatic individuals, althoughthere is evidence indicating that itmay be helpful beyond CAC scor-ing in high-risk individuals.
STABLE CAD
Diagnostic performance of CCTA
CCTA is increasingly employed inpatients with symptoms compatiblewith stable CAD to diagnose or ex-clude obstructive and nonobstruc-tive plaque formation in the coro-nary arteries. CCTA has opened anew window to the heart, providing,for the first time, the opportunity toview the walls of the coronary ar-teries directly without introducingcatheters. Over the past severalyears, a wealth of information basedon CCTA has accumulated, whichhas changed our view on what maybe important in the managementof patients with CAD. At a timewhen symptomatic patients whoare undergoing tests to detect myo-cardial ischemia only have an ap-proximate detection rate of 5%,12 itmay be prudent to use CCTA alter-natively to exclude the presence ofsignificant coronary artery stenosesquickly and reliably. Such a strategymay be able to guide patient man-agement in a more efficient andless costly way, especially wheninitiating secondary preventionmedications, such as statins andacetylsalicylic acid.
Like all other tests, the performanceof CCTA depends on the patientpopulation studied, the equipment,the type of patient preparation used,and other variables. Data are sur-prisingly coherent concerning thehigh sensitivity of the technique,but specificity falls steeply with in-creasing amounts of calcium,13 in-creasing pretest probability for thepresence of obstructive coronary
278
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
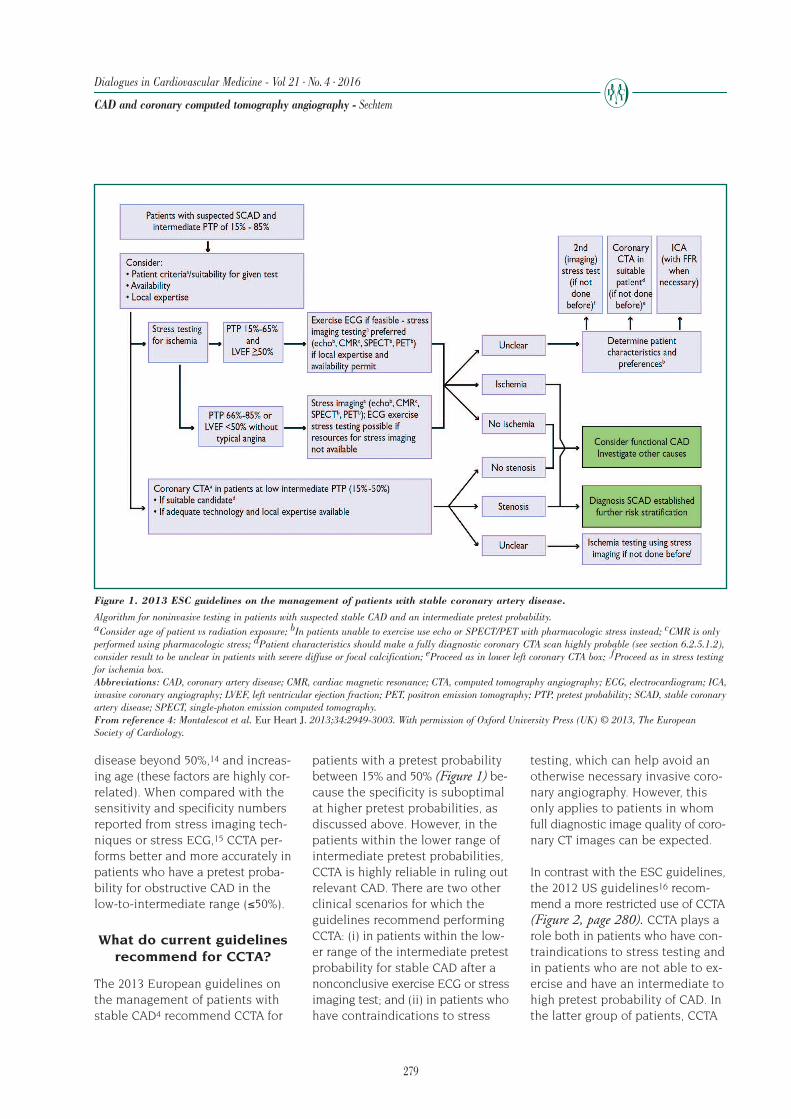
279
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
disease beyond 50%,14 and increas-ing age (these factors are highly cor-related). When compared with thesensitivity and specificity numbersreported from stress imaging tech-niques or stress ECG,15 CCTA per-forms better and more accurately inpatients who have a pretest proba-bility for obstructive CAD in thelow-to-intermediate range (≤50%).
What do current guidelinesrecommend for CCTA?
The 2013 European guidelines onthe management of patients withstable CAD4 recommend CCTA for
patients with a pretest probabilitybetween 15% and 50% (Figure 1) be-cause the specificity is suboptimalat higher pretest probabilities, asdiscussed above. However, in thepatients within the lower range ofintermediate pretest probabilities,CCTA is highly reliable in ruling outrelevant CAD. There are two otherclinical scenarios for which theguidelines recommend performingCCTA: (i) in patients within the low-er range of the intermediate pretestprobability for stable CAD after anonconclusive exercise ECG or stressimaging test; and (ii) in patients whohave contraindications to stress
testing, which can help avoid anotherwise necessary invasive coro-nary angiography. However, thisonly applies to patients in whomfull diagnostic image quality of coro-nary CT images can be expected.
In contrast with the ESC guidelines,the 2012 US guidelines16 recom-mend a more restricted use of CCTA(Figure 2, page 280). CCTA plays arole both in patients who have con-traindications to stress testing andin patients who are not able to ex-ercise and have an intermediate tohigh pretest probability of CAD. Inthe latter group of patients, CCTA
Figure 1. 2013 ESC guidelines on the management of patients with stable coronary artery disease.
Algorithm for noninvasive testing in patients with suspected stable CAD and an intermediate pretest probability. aConsider age of patient vs radiation exposure; bIn patients unable to exercise use echo or SPECT/PET with pharmacologic stress instead; cCMR is onlyperformed using pharmacologic stress; dPatient characteristics should make a fully diagnostic coronary CTA scan highly probable (see section 6.2.5.1.2),consider result to be unclear in patients with severe diffuse or focal calcification; eProceed as in lower left coronary CTA box; fProceed as in stress testingfor ischemia box.Abbreviations: CAD, coronary artery disease; CMR, cardiac magnetic resonance; CTA, computed tomography angiography; ECG, electrocardiogram; ICA,invasive coronary angiography; LVEF, left ventricular ejection fraction; PET, positron emission tomography; PTP, pretest probability; SCAD, stable coronaryartery disease; SPECT, single-photon emission computed tomography.From reference 4: Montalescot et al. Eur Heart J. 2013;34:2949-3003. With permission of Oxford University Press (UK) © 2013, The EuropeanSociety of Cardiology.

is competing with pharmacologicalstress testing using scintigraphy,echocardiography, or cardiac mag-netic resonance imaging. The focuson patients within the range of high-er pretest probabilities is surpris-ing because intermediate pretestprobability is defined in the USguidelines as 20% to 70%, whereashigh pretest probability is defined as71% to 95%. This definition meansthat in the opinion of the US guide-lines, CCTA should be used in agroup of patients in whom the like-lihood of severe calcification israther high, and suboptimal imag-ing results are expected.
The 2010 NICE guidelines were thefirst to give a broader role to CCTA(Figure 3).17 In patients with an es-timated pretest probability between10% and 29%, the algorithm beginswith CT calcium scoring. If the cal-cium score is zero, the guidelinesrecommend looking for other causes
of chest pain, especially functionalCAD, such as epicardial coronaryvasospasm or microvascular coro-nary disease. If the calcium score is>400, invasive coronary angiogra-phy is recommended for diagnosticpurposes. CCTA is recommendedfor patients with a score between 1
280
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
Initiate guidelinedirected medical
therapy
Resting ECGinterpretable?
Contraindications to stress testing?
Patient able to exercise?
Previous coronary revascularization?
Low likelihood IHD
Intermediate likelihood IHD
Intermediate to high likelihood IHD
Intermediate to high
likelihood IHD
Low likelihood
IHDNo
No
No
No
Yes
Yes
Yes
Yes
OR
OR
Standardexercise
ECG
PharmCMR orCCTA
Pharmstressecho
Pharmstress MPI
or echo
MPIor echo w/
exercise
Standardexercise
ECG
MPI orecho w/ exercise
or pharm CMR
CCTA
Figure 2. The 2012ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guidelines for thediagnosis and management ofpatients with stable ischemicheart disease.
Diagnostic pathway as outlinedin the US guidelines. CCTA playsa minor role in these guidelines,yet it is recommended in patientswho have a high pretest likelihoodfor the presence of significant epi-cardial coronary artery stenosis. Abbreviations: CCTA, coronaryCT angiography; CMR, cardiacmagnetic resonance; ECG, electro-cardiogram; IHD, ischemic heartdisease; MPI, myocardial perfusionimaging.From reference 16: Fihn et al. J Am Coll Cardiol. 2012;60:e44-e164. © 2012, American Collegeof Cardiology Foundation and theAmerican Heart Association, Inc.
Estimated likelihood ofCAD 10% to 29%
Treat as stable angina
Investigateother
causes ofchest pain**
SignificantCAD
CT calciumscoring
Followpathway for61% to 90%
CAD
Appropriate functionnalimaging test. If reversible
myocardial ischemia is found, treat as stable
angina. If not, investigate other
causes of chest pain**
** Consider investigating other causesof angina, such as hypertrophic cardiomyopathy or syndrome X in people with typical angina-like chestpain if investigation excludes flow-limiting disease in the epicardialcoronary arteries
64-slice (or above)CT coronaryangiography
CAC score=1-400
CAC score >400
YES
Uncertain
NO
CAC score=0 Figure 3. The stable chest pain pathwayfrom the 2010 NICE guidelines on the
management of patients withrecent-onset chest pain.
This is the suggested mode of testing in patientswith a 10% to 29% pretest probability for the
presence of a stenosing CAD when stable anginacannot be diagnosed or excluded by clinical
assessment alone. Abbreviations: CAD, coronary artery disease;
CT, computed tomography.From reference 17: NICE clinical guideline 95.Chest pain of recent onset: assessment and diagnosisof recent onset chest pain or discomfort of suspectedcardiac origin. www.nice.org.uk/guidance/CG95.
© 2010, National Institute for Health andClinical Excellence.

281
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
and 400. If significant coronary ar-tery stenosis is observed (>400),then the diagnosis of “stable angina”should be made and patients shouldbe treated accordingly. Patientswho have no stenosis should beevaluated further for the presenceof functional CAD or other causes ofchest pain. Patients with inconclu-sive results after CCTA (ie, whethera stenosis is present and not) arerecommended to undergo appropri-ate functional testing.
This brief overview shows that thethree main current guidelines differsubstantially in their recommenda-tions for when CCTA makes senseas a diagnostic tool. However, therecommendations of the 2012 USguidelines were somewhat revised inthe 2014 focused update,18 wherethe guidelines now give a similarrecommendation as the ESC guide-lines, namely to use CCTA for pa-tients in whom the diagnosis ofstable CAD is still inconclusive afternoninvasive stress testing. In suchpatients, the US guidelines nowrecommend CCTA as an alternativeto invasive coronary angiography.For indications and contraindica-tions to CCTA, the 2014 updaterefers to the 2010 expert consensusdocument19 and the 2010 appropri-ate use criteria for cardiac CT.20
However, the somewhat surprisingrecommendation to use CCTA inpatients with a high pretest likeli-hood of CAD was not revised.
The 2016 NICE guidelines on theassessment and diagnosis of recent-onset chest pain are publicly beingdiscussed, and they should be avail-able in November. These new guide-lines propose abandoning pretestprobabilities for selecting appro-priate patient management, andthey recommend going straight toCCTA in patients in whom stableangina cannot be diagnosed or ex-cluded by clinical assessment alone
(https://www.nice.org.uk/guidance/indevelopment/gid-cgwave0827).Moreover, CCTA is recommended asthe initial test in patients in whomclinical assessment indicates typi-cal or atypical angina or chest pain.Functional ischemia testing is rele-gated to a role of an additionaltest if the coronary CT angiogramis nondiagnostic or shows stenosisof uncertain functional significance.
If such an approach appears in thefinal version of the guidelines, itwould be a significant change incurrent thinking. The potential dan-ger is that many patients will havesevere calcifications that will resultin a nondiagnostic CCTA, which willthen lead to additional functionalimaging tests. It remains to be seenwhether such an approach will be-come a fast and cost-effective path-way to diagnose stable CAD andwhether the approach will help ap-propriately risk stratify patients.
Functional assessment of stenosis severity using
CT techniques
An often-used argument againstthe broader application of CCTA isthe inability of the anatomic imagesto provide information about my-ocardial ischemia associated withspecific lesions. Several approachesto solving this problem are currentlybeing pursued. One approach is touse the anatomic information fromthe CT images to improve the iden-tification of coronary artery lesionsthat cause ischemia. In a recentstudy, Park et al looked at plaquefeatures associated with invasivefractional flow reserve (FFR)–definedmyocardial ischemia in 252 patientswho had a CCTA assessment.21
Ischemia was present in 151 of 407coronary lesions (37%). Aggregateplaque volume was associated witha 50% increased risk of ischemiaper 5% additional aggregate plaque
volume. Ischemic lesions had a 3-to 5-times higher prevalence thannonischemic lesions when therewere low attenuation and spottycalcification within the plaque andpositive remodeling. Thus, when indoubt, plaque characteristics shouldbe considered in the diagnosticprocess to identify ischemia-causinglesions, but this tool is currentlynot precise enough, and it is toocomplex to be clinically useful.
Another way of using the informa-tion from standard CCTA datasetsis by applying computational fluiddynamics for the derivation of non-invasive FFR. A recent publicationsummarized the three main stud-ies22 that compared the FFR-CTmethod with invasive FFR.23-25 Themain benefit of FFR-CT seems tobe to increase the unusually poorspecificity of CCTA (25% to 42%) to somewhat better values (54% to79%). Calculation of FFR-CT is cur-rently expensive and takes time,the number of patients studied issmall, and the positive predictivevalue of FFR-CT (65%) is not highenough to preclude the need forconfirmation by invasive FFR.
There have also been attempts touse the attenuation of contrastdistal to a stenosis to characterizestenosis severity. In some studies,the transluminal attenuation gradi-ent (TAG), which is computed as thelinear regression coefficient betweenthe luminal contrast attenuation in Hounsfield units and the lengthfrom the ostium of the coronary ves-sel, was a useful adjunct to stenosisassessment based on anatomy.26,27
Although there is no commonly ac-cepted cut-off value associated withthe functional relevance of a coro-nary lesion, TAG is consistentlylower distal to a high-grade stenosis,which may help interpret the CTangiogram correctly, especially ifcoronary calcification is present.28

282
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
However, when comparing TAG withinvasive FFR for determining thesignificance of a coronary stenosis,Stuijfzand et al did not find an in-cremental diagnostic benefit of TAGvs 256-slice CCTA alone.29 Thisnegative result is not unexpectedbecause there are several technicaland flow-related factors beyondstenosis severity that influence dis-tal contrast attenuation.30
Finally, CT myocardial perfusionimaging under pharmacologicalstress has been developed to deter-mine the hemodynamic significanceof a stenosis.30 Static acquisitionsuse a single dataset obtained dur-ing first-pass enhancement tomeasure attenuation levels in is-chemic and nonischemic areas. Incontrast, dynamic CT perfusion im-aging acquires a sequential datasetduring the passage of contrast me-dia, making it possible to construct
a time-signal intensity curve fromwhich myocardial blood flow canbe calculated. The disadvantage ofthe dynamics strategy is the approx-imate 10 mSv increase in radiationexposure. However, acquisition ofstatic myocardial perfusion imagesalso requires an additional CT scan,which results in an additional radi-ation exposure of approximately2.5 mSv.30 Many studies have shown
a good agreement between CT myo-cardial perfusion imaging and sin-gle-photon emission computed to-mography (SPECT), invasive coronaryangiography, and perfusion cardiacmagnetic resonance. These studiesare nicely summarized in a recent2015 review by Goncalves et al.30
Most of these studies showed thatthe addition of stress CT myocardialperfusion imaging increases theaccuracy of CCTA for detecting re-
versible myocardial ischemia. Again,it is mainly related to the specificityof CCTA, which is increased by alsoconsidering CT myocardial perfusionimaging (Figure 4).31 In a recentstudy where stress CT myocardialperfusion imaging was comparedwith FFR, Ko et al showed that thespecificity and the positive predic-tive value increased from 84% to98% and from 82% to 97%, respec-tively, when CCTA was included.31
The main issue with using CT myo-cardial perfusion imaging clinicallyis the radiation issue because car-diac magnetic resonance and echo-cardiography provide similar infor-mation without radiation exposure.Thus, myocardial perfusion imag-ing using CT currently remains aresearch tool, but this may changewith further improvements in CTtechnology. In summary, all of thecurrently investigated approachesfor using cardiac CT to diagnosemyocardial ischemia are not yetclinically established.
Prognosis
Furthermore, CCTA also has a proventrack record of providing stable andreliable prognostic information, especially in stable symptomaticpatients who have no atherosclero-sis.32 Revascularization of patientsidentified by CCTA to harbor signif-icant obstructive CAD may improveprognosis, just as it worsens prog-nosis in those shown by CCTA tohave only a mild disease.33 Patientswith diffuse severe coronary athero-sclerosis without epicardial stenosismay indicate myocardial ischemiaboth by FFR34 or perfusion imag-ing,35 and these patients also havea significantly worse prognosis.36
In fact, diffuse severe coronary ath-erosclerosis is associated with high-er rates of all-cause death, cardiacdeath, and myocardial infarctionthan a more focal atherosclerosisor the complete absence of plaque.
Figure 4. Computed tomography perfusion imaging and invasive angiography in a 55-year-old female with chest pain.
Computed tomography myocardial perfusion imaging demonstrated, on axial and sagittal cuts, re-versible nontransmural ischemia in the mid- to distal-anterior, anteroseptal, and anterolateral walls(red arrows). On invasive angiography, there was severe stenosis in the mid-left anterior descendingartery, with a fractional flow reserve of 0.33 recorded in the distal vessel. There was no angiographiccorrelate for the lateral ischemia. Abbreviations: CTP, computed tomography myocardial perfusion imaging; FFR, fractional flow reserve.From reference 31: Ko et al. Eur Heart J. 2012;33:67-77. © 2012, Oxford University Press.

283
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
The unfavorable outcomes in thesepatients are similar to that of pa-tients with multivessel obstructivedisease.37 This observation mayappear initially paradoxical, but itmay be explained by the known riskfor acute complications associatedwith nonobstructive plaque38 andthe risk of associated microvasculardisease and microvascular ischemia,which frequently accompanies epi-cardial plaque formation.
In a recent trial, 10 000 symptomaticstable patients were randomized toeither a strategy of initial anatomictesting using CCTA or an approachusing functional testing. The resultsshowed similar outcomes for bothstrategies,39 and the rates of hardcoronary events were low in botharms. More patients in the CT groupunderwent invasive catheterization(12.2% vs 8.1%), but the CT strategyled to fewer catheterizations show-
ing no obstructive CAD than func-tional testing (3.4% vs 4.3%). Morepatients in the CT group underwentrevascularization (6.2% vs 3.2%), butthis did not lead to differences inthe outcomes; however, the studywas underpowered to detect suchdifferences.
ACUTE CORONARY SYNDROME
CCTA is also a promising tool to beused in patients with acute coronarysyndromes. These patients oftenhave low-risk features, such as ab-sent or stable troponin at low levelsand a normal ECG or an ECG with-out significant changes during thetime in the emergency department.It is in this group of patients thatquick and reliable ruling out of coro-nary stenosis and plaque formationis desirable. Several randomizedstudies40-42 reported very low event
rates secondary to a normal CCTAduring follow-up after patients weredischarged from the emergency de-partment. Based on the data, it isclear that patients fulfilling the cri-teria listed above can be safely senthome. One can argue that many ofthese patients probably had no acutecoronary syndrome, but just acutechest pain and were at a very lowrisk of developing a myocardial in-jury. Therefore, the availability ofCCTA in the emergency room mightlead to unnecessary and unjusti-fied testing and application of ra-diation. However, current demandby patients and lawyers for diag-nostic certainty may render suchclinical management unavoidable.
More recently, a multicenter studyfrom the Netherlands randomizedpatients with acute chest pain orsymptoms suggestive of ACS to ei-ther CCTA or standard care accord-
Figure 5. Direct discharge rate from emergency departments and length of hospitalization with CCTA vs SOC.
Panel A. Direct discharge rates from the emergency department in three randomized clinical trials of CCTA vs SOC. While there was a significantly higherdirect discharge rate in two previous trials—ACRIN-PA and ROMICAT—from the US, the addition of high-sensitivity troponins to SOC reduced the dif-ference in discharge rates to a nonsignificant level in the BEACON trial. Note that the direct discharge rate in the SOC group was higher in the BEACONtrial than in the CCTA arms of the other two trials. Panel B. Length of hospitalization stay was significantly higher in the SOC arms of the two US trials,whereas it was equal to the CCTA arm in the BEACON trial. Note that the length of stay in both arms of the BEACON trial was shorter than that of theCCTA arms in the two US trials. Again, this was probably due to the higher level of diagnostic confidence due to the use of high-sensitivity troponins.Abbreviations: ACRIN-PA, American College of Radiology Imaging Network-Pennsylvania; BEACON, Better Evaluation of Acute Chest Pain with Com-puted Tomography Angiography; CCTA, coronary CT angiography; ROMICAT, Rule Out Myocardial Infarction/ischemia using Computer Assisted Tomog-raphy; SOC, standard of care.From reference 43: Dedic et al. J Am Coll Cardiol. 2016;67:16-26. © 2016, American College of Cardiology Foundation.

284
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
ing to current guidelines, and eachgroup had 243 patients.43 This studyincluded patients in whom serumtroponin levels were up to 3 timesthe upper limit of the 99th per-centile. Exclusion criteria includedsymptoms that clearly had a non-cardiac origin, history of CAD, aclinical need for urgent invasivecoronary angiography, clinical in-stability, impaired renal function,severe arrhythmias, and a body massindex >40 kg/m². The primary out-come (ie, the number of patientsrequiring revascularization within30 days) was similar (9% with CT vs7% with standard care) in the twogroups. Similar results were alsoreported for the frequency of unde-tected ACS (0.5% with CT vs 1% withstandard care). The number of pa-tients who could be discharged im-mediately from the emergency de-partment was similar between thetwo groups, which was also true forthe median length of stay. The num-ber of outpatient tests was lower in the CT group (4% vs 11%; P<0.01)and the direct medical costs after30 days were lower in the CT group(€337 vs €511; P<0.01).
The Netherland study differs some-what from the other randomizedtrials as the early performance ofCCTA did not shorten the length ofstay or reduce the number of hos-pital admissions (Figure 5, page283).43 This result may have beendue to the use of high sensitivitytroponins that had not been avail-able in the previous studies. Thepositive role of high-sensitivity tro-ponins is also reflected in the largenumber of patients who could bedirectly discharged from the emer-gency department in the study.
Their number was 2- to 4-timeshigher than reported in previousrandomized trials (Figure 5).41-43However, another important differ-ence between this study and the
previous US trials was the differenthealth care system in theNetherlands, which gives differentincentives to patient care. The re-sults of this study may be transfer-able to other European emergencysystems, and it may help make theemergency room workup of pa-tients suspected to have acutecoronary syndromes cheaper with-out compromising safety.
CONCLUSIONS
The advent of CCTA will significant-ly alter our approach to asympto-matic high-risk patients, patientswith stable coronary artery disease,and patients with low-risk acutecoronary syndromes. In the firstgroup of patients, we will be ableto quickly and precisely identifythe presence, extent, and contentof plaque formation to help us allocate medical therapy better tothose who will profit the most. Thesecond group will have the benefitof a reliable exclusion of epicardialstenosis without having to undergoinvasive coronary angiography,which is still used in too many ofthese patients. Finally, in the thirdgroup of patients, the combinationof high-sensitivity troponins andCCTA will safely reduce the numberof subsequent outpatient proceduresand save considerable amounts ofmoney for our often-underfinancedhealth care systems.
REFERENCES
1. Flohr TG, De Cecco CN, SchmidtB, Wang R, Schoepf UJ, Meinel FG.
Computed tomographic assessment of coro-nary artery disease: state-of-the-art imagingtechniques.
Radiol Clin North Am. 2015;53:271-285.
2. Schuhbaeck A, Achenbach S,Layritz C, et al.
Image quality of ultra-low radiation expo-sure coronary CT angiography with an ef-fective dose <0.1 mSv using high-pitch spiralacquisition and raw data-based iterativereconstruction.
Eur Radiol. 2013;23:597-606.
3. Abbara S, Arbab-Zadeh A, CallisterTQ, et al.
SCCT guidelines for performance of coronarycomputed tomographic angiography.
J Cardiovasc Comput Tomogr.2009;3:190-204.
4. Montalescot G, Sechtem U,Achenbach S, et al.
2013 ESC guidelines on the management ofstable coronary artery disease.
Eur Heart J. 2013;34:2949-3003.
5. Kim C, Hong SJ, Shin DH, et al.
Limitations of coronary computed tomograph-ic angiography for delineating the lumenand vessel contours of coronary arteries inpatients with stable angina.
Eur Heart J Cardiovasc Imaging.2015;16:1358-1365.
6. Silverman MG, Blaha MJ, KrumholzHM, et al.
Impact of coronary artery calcium on coro-nary heart disease events in individuals atthe extremes of traditional risk factor burden:the Multi-Ethnic Study of Atherosclerosis.
Eur Heart J. 2014;35:2232-2241.
7. Piepoli MF, Hoes AW, Agewall S,et al.
2016 European Guidelines on cardiovasculardisease prevention in clinical practice.
Eur Heart J. 2016;23:NP1-NP96.
8. Cho I, Suh JW, Chang HJ, et al.
Prevalence and prognostic implication of non-calcified plaque in asymptomatic populationwith coronary artery calcium score of zero.
Korean Circ J. 2013;43:154-160.
9. Cho I, Chang HJ, Sung JM, et al.
Coronary computed tomographic angiographyand risk of all-cause mortality and nonfatalmyocardial infarction in subjects withoutchest pain syndrome from the CONFIRMRegistry (coronary CT angiography evalua-tion for clinical outcomes: an internationalmulticenter registry).
Circulation. 2012;126:304-313.

285
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
10. Cho I, Chang HJ, Ó Hartaigh B, et al.
Incremental prognostic utility of coronaryCT angiography for asymptomatic patientsbased upon extent and severity of coronaryartery calcium: results from the COronaryCT Angiography EvaluatioN For ClinicalOutcomes InteRnational Multicenter (CONFIRM) study.
Eur Heart J. 2015;36:501-508.
11. Dedic A, Ten Kate GJ, Roos CJ,et al.
Prognostic value of coronary computed to-mography imaging in patients at high riskwithout symptoms of coronary artery disease.
Am J Cardiol. 2016;117:768-774.
12. Rozanski A, Gransar H, Hayes SW,et al.
Temporal trends in the frequency of induciblemyocardial ischemia during cardiac stresstesting: 1991 to 2009.
J Am Coll Cardiol. 2013;61:1054-1065.
13. Gueret P, Deux JF, Bonello L, et al.
Diagnostic performance of computed tomog-raphy coronary angiography (from theProspective National Multicenter MultivendorEVASCAN Study).
Am J Cardiol. 2013;111:471-478.
14. Meijboom WB, van Mieghem CA,Mollet NR, et al.
64-slice computed tomography coronaryangiography in patients with high, interme-diate, or low pretest probability of significantcoronary artery disease.
J Am Coll Cardiol. 2007;50:1469-1475.
15. Nielsen LH, Ortner N, NorgaardBL, Achenbach S, Leipsic J, Abdulla J.
The diagnostic accuracy and outcomes aftercoronary computed tomography angiographyvs. conventional functional testing in patientswith stable angina pectoris: a systematic review and meta-analysis.
Eur Heart J Cardiovasc Imaging.2014;15:961-971.
16. Fihn SD, Gardin JM, Abrams J, et al.
2012 ACCF/AHA/ACP/AATS/PCNA/SCAI/STS guideline for the diagnosis and man-agement of patients with stable ischemicheart disease.
J Am Coll Cardiol. 2012;60:e44-e164.
17. NICE clinical guideline 95.
Chest pain of recent onset: assessment anddiagnosis of recent onset chest pain or dis-comfort of suspected cardiac origin.
www.nice.org.uk/guidance/CG95. PublishedMarch 2010. Accessed July 19, 2016.
18. Fihn SD, Blankenship JC,Alexander KP, et al.
2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients withstable ischemic heart disease.
J Am Coll Cardiol. 2014;64:1929-1949.
19. Mark DB, Berman DS, Budoff MJ,et al.
ACCF/ACR/AHA/NASCI/SAIP/SCAI/SCCT2010 expert consensus document on coronarycomputed tomographic angiography.
J Am Coll Cardiol. 2010;55:2663-2699.
20. Taylor AJ, Cerqueira M, HodgsonJM, et al.
ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteriafor cardiac computed tomography.
Circulation. 2010;122:e525-e555.
21. Park HB, Heo R, ó Hartaigh B, et al.
Atherosclerotic plaque characteristics by CTangiography identify coronary lesions thatcause ischemia: a direct comparison tofractional flow reserve.
JACC Cardiovasc Imaging. 2015;8:1-10.
22. Hecht HS.
The game changer?
J Am Coll Cardiol. 2014;63:1156-1158.
23. Koo BK, Erglis A, Doh JH, et al.
Diagnosis of ischemia-causing coronarystenoses by noninvasive fractional flow re-serve computed from coronary computed tomographic angiograms. Results from theprospective multicenter DISCOVER-FLOW(Diagnosis of Ischemia-Causing StenosesObtained Via Noninvasive Fractional FlowReserve) study.
J Am Coll Cardiol. 2011;58:1989-1997.
24.Min JK, Leipsic J, Pencina MJ, et al.
Diagnostic accuracy of fractional flow reservefrom anatomic CT angiography.
JAMA. 2012;308:1237-1245.
25. Norgaard BL, Leipsic J, Gaur S,et al; NXT Trial Study Group.
Diagnostic performance of noninvasivefractional flow reserve derived from coronarycomputed tomography angiography in sus-pected coronary artery disease: the NXT trial(Analysis of Coronary Blood Flow UsingCT Angiography: Next Steps).
J Am Coll Cardiol. 2014;63:1145-1155.
26. Wong DT, Ko BS, Cameron JD, et al.
Transluminal attenuation gradient in coro-nary computed tomography angiography isa novel noninvasive approach to the identi-fication of functionally significant coronaryartery stenosis: a comparison with fractionalflow reserve.
J Am Coll Cardiol. 2013;61:1271-1279.
27. Zheng M, Wei M, Wen D, et al.
Transluminal attenuation gradient in coro-nary computed tomography angiographyfor determining stenosis severity of calcifiedcoronary artery: a primary study with dual-source CT.
Eur Radiol. 2015;25:1219-1228.
28. Choi JH, Min JK, Labounty TM, et al.
Intracoronary transluminal attenuationgradient in coronary CT angiography fordetermining coronary artery stenosis.
JACC Cardiovasc Imaging. 2011;4:1149-1157.
29. Stuijfzand WJ, Danad I,Raijmakers PG, et al.
Additional value of transluminal attenuationgradient in CT angiography to predict he-modynamic significance of coronary arterystenosis.
JACC Cardiovasc Imaging. 2014;7:374-386.
30. Goncalves Pde A, Rodriguez-Granillo GA, Spitzer E, et al.
Functional evaluation of coronary diseaseby CT angiography.
JACC Cardiovasc Imaging. 2015;8:1322-1335.
31. Ko BS, Cameron JD, Meredith IT,et al.
Computed tomography stress myocardialperfusion imaging in patients consideredfor revascularization: a comparison withfractional flow reserve.
Eur Heart J. 2012;33:67-77.

32. Min JK, Dunning A, Lin FY, et al;CONFIRM Investigators.
Age- and sex-related differences in all-causemortality risk based on coronary computedtomography angiography findings resultsfrom the International Multicenter CON-FIRM (Coronary CT Angiography Evalua-tion for Clinical Outcomes: An InternationalMulticenter Registry) of 23,854 patientswithout known coronary artery disease.
J Am Coll Cardiol. 2011;58:849-860.
33. Min JK, Berman DS, Dunning A,et al.
All-cause mortality benefit of coronary revas-cularization vs. medical therapy in patientswithout known coronary artery disease un-dergoing coronary computed tomographicangiography: results from CONFIRM(COronary CT Angiography EvaluatioNFor Clinical Outcomes: An InteRnationalMulticenter Registry).
Eur Heart J. 2012;33:3088-3097.
34. Park SJ, Kang SJ, Ahn JM, et al.
Visual-functional mismatch between coronaryangiography and fractional flow reserve.
JACC Cardiovasc Interv. 2012;5:1029-1036.
35. Lanza GA, Buffon A, Sestito A, et al.
Relation between stress-induced myocardialperfusion defects on cardiovascular magneticresonance and coronary microvascular dys-function in patients with cardiac syndrome X.
J Am Coll Cardiol. 2008;51:466-472.
36. Taqueti VR, Hachamovitch R,Murthy VL, et al.
Global coronary flow reserve is associatedwith adverse cardiovascular events independ-ently of luminal angiographic severity andmodifies the effect of early revascularization.
Circulation. 2015;131:19-27.
37. Bittencourt MS, Hulten E,Ghoshhajra B, et al.
Prognostic value of nonobstructive and ob-structive coronary artery disease detected bycoronary computed tomography angiographyto identify cardiovascular events.
Circ Cardiovasc Imaging. 2014;7:282-291.
38. Arbab-Zadeh A, Nakano M,Virmani R, Fuster V.
Acute coronary events.
Circulation. 2012;125:1147-1156.
39. Douglas PS, Hoffmann U, PatelMR, et al; PROMISE Investigators.
Outcomes of anatomical versus functionaltesting for coronary artery disease.
N Engl J Med. 2015;372:1291-1300.
40. Goldstein JA, Chinnaiyan KM,Abidov A, et al; CT-STATInvestigators.
The CT-STAT (Coronary Computed Tomo-graphic Angiography for Systematic Triageof Acute Chest Pain Patients to Treatment)trial.
J Am Coll Cardiol. 2011;58:1414-1422.
41. Litt HI, Gatsonis C, Snyder B, et al.
CT angiography for safe discharge of pa-tients with possible acute coronary syndromes.
N Engl J Med. 2012;366:1393-1403.
42. Hoffmann U, Truong QA,Schoenfeld DA, et al; ROMICAT-IIInvestigators.
Coronary CT angiography versus standardevaluation in acute chest pain.
N Engl J Med. 2012;367:299-308.
43. Dedic A, Lubbers MM, Schaap J,et al.
Coronary CT angiography for suspectedACS in the era of high-sensitivity troponins:randomized multicenter study.
J Am Coll Cardiol. 2016;67:16-26.
286
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
CAD and coronary computed tomography angiography - Sechtem
287
IMAGING MODALITIES FORASSESSING CORONARYATHEROSCLEROSIS
ngiography is a road map-ping technique that canaddress lumen narrowingdue to coronary atheroscle-
rosis. Since its introduction over50 years ago, angiography is still thegold standard for assessing athero-sclerotic impairment of coronaryarteries and for providing guidanceduring percutaneous coronary inter-ventions (PCI). However, angiogra-phy only depicts the luminal nar-rowing caused by coronary plaques;therefore, it is unable to study ath-erosclerotic lesions with accuracy.
Apart from extensive calcifications,which can be revealed with angiog-raphy, lipid and fibrous componentscannot be identified. In some cas-es, complicated plaques can alsobe identified. In fact, intracoronarythrombi typically cause angiograph-ic haziness, whereas plaque ulcera-tion can be visualized when theplaque crater is connected to thelumen. Angiography is certainly aninappropriate technique to studyplaque vulnerability. However, evenwith its inherent limitation of sim-ply offering a luminal view, angiog-raphy can be utilized to quantifyatherosclerosis extension. For thisspecific task, a dedicated scoringsystem has been developed.1,2
What is the role of intracoronary imaging?Francesco Prati, MD1,2,3; Laura Gatto, MD1,2; Vito Ramazzotti, MD2
1CLI-Foundation, Rome, ITALY2Cardiology Department, San Giovanni Hospital, ITALY3Ettore Sansavini, Health Science Foundation, Cotignola, ITALY
A
Copyright © 2016, AICH - Servier Research Group. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Keywords: atherosclerosis; coronary angiog-raphy; intravascular ultrasound; near-infrared spectroscopy; optical coherence tomography; vulnerable plaque Address for correspondence:Francesco Prati, MD, Cardiology Unit, SanGiovanni Hospital, Via dell’Amba Aradam,8-00184 Rome, Italy(e-mail: [email protected])
Dialogues Cardiovasc Med. 2016;21:287-292
Intravascular imaging modalitiesare used by interventional cardiol-ogists to assess atheroscleroticplaque features and stent deploy-ment results, overcoming somelimits of coronary angiography.Optical coherence tomography, intravascular ultrasound, andnear-infrared spectroscopy are themost commonly used intravasculartechniques. Each technique has spe-cific advantages and limitationsthat make each one appropriate forspecific purposes. In the last years,offline analysis software has beendeveloped to diagnose plaque tissuecomponents, such as macrophages,better and improve coronary stentassessment, even in a three-dimen-sional view (carpet view). Althoughoptical coherence tomography andintravascular ultrasound have beenprincipally used for research pur-poses, recent evidence supports aclinical role for intracoronary im-aging techniques in guiding per-cutaneous coronary interventions,mainly for complex procedures.
SELECTED ABBREVIATIONS AND ACRONYMS
ACS acute coronary syndrome
ADAPT-DES Assessment of Dual AntiPlatelet Therapy with Drug-Eluting Stents [trial]
CLI-OPCI Centro per la Lotta contro l’Infarto-Optimisation of Percutaneous Coronary Intervention [study]
IB-IVUS integrated backscatter intravascular ultrasound
IVUS intravascular ultrasound
MACE major adverse cardiac event
NIRS near-infrared spectroscopy
OCT optical coherence tomography
PCI percutaneous coronary intervention
PROSPECT Providing Regional Observations to Study Predictors of Events in the Coronary Tree [trial]
TCFA thin-cap fibroatheroma
VH-IVUS virtual histology intravascular ultrasound
VIVA VH-IVUS in Vulnerable Atherosclerosis [study]
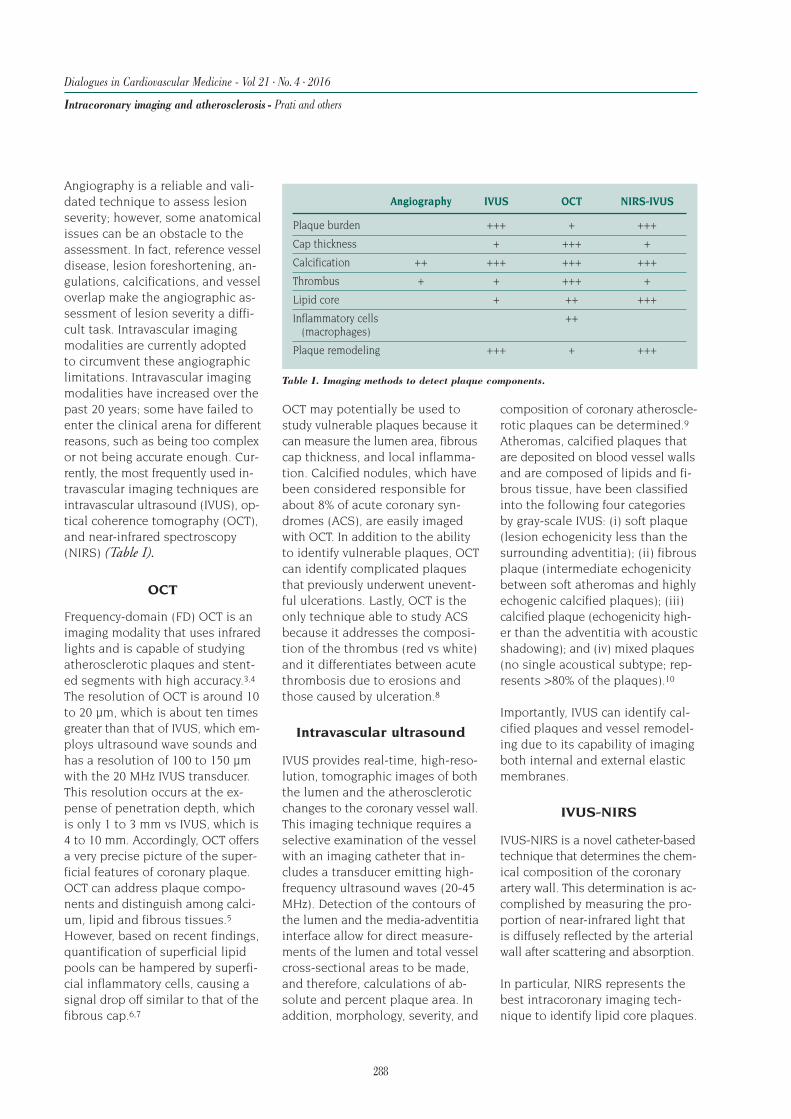
288
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Intracoronary imaging and atherosclerosis - Prati and others
Angiography is a reliable and vali-dated technique to assess lesionseverity; however, some anatomicalissues can be an obstacle to theassessment. In fact, reference vesseldisease, lesion foreshortening, an-gulations, calcifications, and vesseloverlap make the angiographic as-sessment of lesion severity a diffi-cult task. Intravascular imagingmodalities are currently adoptedto circumvent these angiographiclimitations. Intravascular imagingmodalities have increased over thepast 20 years; some have failed toenter the clinical arena for differentreasons, such as being too complexor not being accurate enough. Cur-rently, the most frequently used in-travascular imaging techniques areintravascular ultrasound (IVUS), op-tical coherence tomography (OCT),and near-infrared spectroscopy(NIRS) (Table I).
OCT
Frequency-domain (FD) OCT is animaging modality that uses infraredlights and is capable of studyingatherosclerotic plaques and stent-ed segments with high accuracy.3,4
The resolution of OCT is around 10to 20 µm, which is about ten timesgreater than that of IVUS, which em-ploys ultrasound wave sounds andhas a resolution of 100 to 150 µmwith the 20 MHz IVUS transducer.This resolution occurs at the ex-pense of penetration depth, whichis only 1 to 3 mm vs IVUS, which is4 to 10 mm. Accordingly, OCT offersa very precise picture of the super-ficial features of coronary plaque.OCT can address plaque compo-nents and distinguish among calci-um, lipid and fibrous tissues.5
However, based on recent findings,quantification of superficial lipidpools can be hampered by superfi-cial inflammatory cells, causing asignal drop off similar to that of thefibrous cap.6,7
OCT may potentially be used tostudy vulnerable plaques because itcan measure the lumen area, fibrouscap thickness, and local inflamma-tion. Calcified nodules, which havebeen considered responsible forabout 8% of acute coronary syn-dromes (ACS), are easily imagedwith OCT. In addition to the abilityto identify vulnerable plaques, OCTcan identify complicated plaquesthat previously underwent unevent-ful ulcerations. Lastly, OCT is theonly technique able to study ACSbecause it addresses the composi-tion of the thrombus (red vs white)and it differentiates between acutethrombosis due to erosions andthose caused by ulceration.8
Intravascular ultrasound
IVUS provides real-time, high-reso-lution, tomographic images of boththe lumen and the atheroscleroticchanges to the coronary vessel wall.This imaging technique requires aselective examination of the vesselwith an imaging catheter that in-cludes a transducer emitting high-frequency ultrasound waves (20-45MHz). Detection of the contours ofthe lumen and the media-adventitiainterface allow for direct measure-ments of the lumen and total vesselcross-sectional areas to be made,and therefore, calculations of ab-solute and percent plaque area. Inaddition, morphology, severity, and
composition of coronary atheroscle-rotic plaques can be determined.9
Atheromas, calcified plaques thatare deposited on blood vessel wallsand are composed of lipids and fi-brous tissue, have been classifiedinto the following four categoriesby gray-scale IVUS: (i) soft plaque(lesion echogenicity less than thesurrounding adventitia); (ii) fibrousplaque (intermediate echogenicitybetween soft atheromas and highlyechogenic calcified plaques); (iii)calcified plaque (echogenicity high-er than the adventitia with acousticshadowing); and (iv) mixed plaques(no single acoustical subtype; rep-resents >80% of the plaques).10
Importantly, IVUS can identify cal-cified plaques and vessel remodel-ing due to its capability of imagingboth internal and external elasticmembranes.
IVUS-NIRS
IVUS-NIRS is a novel catheter-basedtechnique that determines the chem-ical composition of the coronaryartery wall. This determination is ac-complished by measuring the pro-portion of near-infrared light thatis diffusely reflected by the arterialwall after scattering and absorption.
In particular, NIRS represents thebest intracoronary imaging tech-nique to identify lipid core plaques.
Angiography IVUS OCT NIRS-IVUS
Plaque burden +++ + +++
Cap thickness + +++ +
Calcification ++ +++ +++ +++
Thrombus + + +++ +
Lipid core + ++ +++
Inflammatory cells ++(macrophages)
Plaque remodeling +++ + +++
Table I. Imaging methods to detect plaque components.

A lipid core plaque is defined as afibroatheroma containing a necroticcore that is at least 200 µm thick,with a circumferential span of atleast 60 degrees on cross-section.NIRS cannot distinguish between asuperficial and a deep lipid coreplaque; for this reason, it needs tobe combined with an additionaltechnique, such as IVUS, to locatethe lipid pool across the vessel layers.11
Postprocessing of OCT and IVUS images
A postprocessing analysis of bothOCT and IVUS images can be car-ried out using dedicated software.Grayscale IVUS is not capable ofdistinguishing plaque types; as aresult, both virtual histology (VH)IVUS and integrated backscatter(IB) IVUS have been used to elabo-rate the backscattered IVUS signalfurther to enhance differentiationof the major plaque components.VH-IVUS uses an autoregressionmodel to generate multiple spectralparameters of the backscatteredultrasound signal to produce a tis-sue map of the plaque components:fibrous (dark green), fibro-fatty (yel-low-green), necrotic core (red), anddense calcium (white).
The PROSPECT trial (Providing Re-gional Observations to Study Pre-dictors of Events in the CoronaryTree) was the first prospective nat-ural history study of vulnerableplaque.12 PROSPECT linked VH-IVUS–derived thin-cap fibroathero-ma (TCFA), defined as a necroticcore–rich plaque (>10%) withoutevident overlying fibrous tissue andwith a percent plaque volume of40%, with clinical events.
The IB-IVUS technique uses math-ematical manipulation of the ultra-sound backscatter signal to improvethe ability of IVUS to detect vulner-
able plaques. IB values for the vari-ous plaque components can then becalculated to construct color-codedIB-IVUS maps that can be catego-rized into one of five groups: throm-bus, intimal hyperplasia/lipid core,fibrous, mixed, and calcified tissues.
OCT images can be postprocessedusing new software called “CarpetView,” which unfolds the vessel, re-constructs it as an open structure,and displays it as a three-dimen-sional reconstruction. The softwarecan improve the offline serial com-parisons of both coronary plaqueand stented segments, enabling thematching of the imaged cross-sec-tion at different time points.13
Dedicated software capable of quan-tifying macrophages using OCT images has also been developed.Macrophages are inflammatory cellsthat play a central role in plaquedestabilization by releasing prote-olytic enzymes and other proinflam-matory mediators that in turn, canlead to fibrous cap rupture and sub-sequent plaque thrombosis. TheTearney Lab (Boston, MA, USA) developed software that measuresOCT signal variance (ie, named nor-malized standard deviation), a pa-rameter that tends to increase in thepresence of a significant macrophagecontent.14 However, a normalizedstandard deviation may overestimatemacrophage presence due to arti-facts. Thus, other tissue property in-dexes have been proposed to charac-terize macrophage presence further.
The average size of macrophages isusually 20 to 50 µm, although theymay eventually generate larger cellscalled foam cells, which can be iden-tified using granulometry. A two-step algorithm can identify a sig-nificant macrophage presence withhigh accuracy; the normalized stan-dard deviation should be appliedfirst, followed by granulometry.7
Improving the reproducibility ofOCT measurements of metrics ofplaque vulnerability is a major taskto augment the ability of OCT todetect vulnerable lesions and iden-tify the progression-regression ofplaque components in response tospecific treatments. The convention-al manual analysis is obtained byselecting the cross-section with thethinnest part of the fibrous cap. Thisapproach is subject to interobserv-er variability and does not capturethe three-dimensional morphologyof the fibrous cap. For this reason,a computer-aided method that pro-vides a volumetric analysis of thefibrous cap and the relevant thick-ness at every point in the fibrouscap boundary has been validated.15
CLINICAL RELEVANCE OFIMAGING FINDINGS
OCT can identify fresh coronarythrombi that may be missed by an-giography. In a substantial numberof patients with ACS, typically non–ST-segment elevation myocardialinfarction (NSTEMI), angiographydoes not show significant lesionsor clear signs of acute thrombosis.A coronary thrombus, which is theultimate event of ACS, can be welldepicted by OCT because of its optimal resolution. Therefore, OCThas a vital role in diagnosing culpritlesions of ACS when there is uncer-tainty with the angiography assess-ment. Furthermore, OCT can depictthe pathophysiology of ACS by dif-ferentiating between plaque erosionand ulceration. The latter aspectwas related to a worse outcome,which serves as a marker of a moreaggressive clinical condition.16
In a serial study carried out on patients with ST-segment elevationmyocardial infarction (STEMI),Souteyrand et al showed that themorphology of a ruptured plaqueremains almost unchanged over
289
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Intracoronary imaging and atherosclerosis - Prati and others

290
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Intracoronary imaging and atherosclerosis - Prati and others
time, while a thrombosis due toerosion has a smooth plaque surfaceduring follow-up.17 It is reasonableto defer any coronary interventionwhen there is plaque ulcerationdetected at IVUS or OCT unless asignificant luminal narrowing or afresh thrombus is present. In fact,ulcerations tend to remain stablewithout causing cardiac events.18 Inthe presence of superficial macro-phage clusters, lipid pools may notbe easily detected. Macrophagescan scatter the OCT signal in thesame manner as lipid pools, leadingto an overestimation of lipid poolextension.
The recent combination of NIRSwith gray-scale IVUS in a single im-aging catheter allows simultaneousassessment of plaque compositionin terms of both chemical (NIRS)and morphologic (IVUS) character-istics. Specifically, NIRS can be usedto quantify plaque lipid content.Yonetsu et al compared NIRS-IVUSwith OCT for the detection of lipidsin nontarget lesions in a cohort ofACS and stable angina patients. Theyshowed a poor overall agreementbetween NIRS and OCT for the de-tection of lipids. In particular, inthe presence of superficial calcifica-tion, the OCT analysis of nontargetlesions leads to a misinterpreta-tion of the lipid content.19 In addi-tion, histopathological studies haveshown that an accumulation offoamy macrophages on the luminalsurface of the vessel wall, which isidentified by OCT with a typical ap-pearance of a thin bright line withtrailing shadows, may mimic lipidmaterials, thereby affecting the accurate tissue analysis of deeperstructures.
PLAQUE VULNERABILITY
Muller et al described “vulnerableplaques” as nonculprit lesions thatpotentially lead to cardiac events.20
Such lesions are characterized by alarge lipid pool, a thin fibrous cap,a relatively small lumen area, andmacrophage-dense inflammation onor beneath the surface.6 A recenthistopathological study carried outby Narula et al, quantified the fea-tures related to plaque vulnerabilitybetter. Lesions causing suddendeath were compared with othervulnerable plaques that did notcause events. Such lesions had afibrous cap thickness <84 µm, alarge lipid pool, a minimal lumenarea <4.0 mm2, and the presenceof local inflammation.21
PROSPECT evaluated the naturalhistory of atherosclerosis by study-ing 697 ACS patients treated withPCI on the culprit lesion plus opti-mal medical therapy. All patientshad three-vessel imaging with gray-scale and VH-IVUS. The studyshowed that both culprit and non-culprit lesions were equally respon-sible for major adverse cardiacevents (MACE) over 3 years. Mostnonculprit lesions causing follow-up events had a mild angiographicnarrowing at baseline. A multivari-ate analysis carried out with IVUSdata identified three independentpredictors of MACE: plaque burden≥70%, minimal lumen area ≤4.0 mm2,and TCFA at VH-IVUS, identified asa lipid-rich atheroma with only athin fibrous layer of intimal tissuecovering the necrotic core.12
Likewise, in the VIVA study (VH-IVUSin Vulnerable Atherosclerosis), three-vessel VH-IVUS was performed in170 patients with stable angina orACS before and after PCI. During 1.7years of follow-up, 19 lesions (13nonculprit and 6 culprit lesions)resulted in MACE (death, myocardialinfarction, unplanned revascular-ization). Nonculprit lesion factorsresponsible for total MACE includedplaque burden >70% and minimallumen area <4 mm2, while VH-IVUS
TCFA and plaque burden >70% wereassociated with nonstenotic MACE.22
This evidence suggests that VH-IVUS can identify vulnerable plaqueswith a greater risk of MACE duringfollow-up.
The Italian multicenter CLIMA Reg-istry has been conceived to relatethe OCT morphology of atheroscle-rotic lesions located in the left an-terior descending artery with clinicaloutcomes at follow-up. During fol-low-up, MACE was defined as thepresence of cardiac death or anteriorACS (including STEMI or NSTEMI).In the patient group with MACE atfollow-up (mean 2.7 years), vulner-able plaques occurred more often(11.4% vs 0.3%; P<0.00001) withthe following features of vulnera-bility: lumen area <4.0 mm2, thinfibrous cap (<70 µm), circumferen-tial extension of the lipid pool of atleast 2 quadrants, and local inflam-mation (unpublished data).
OCT-GUIDED PCI
In 2012, our group published theCLI-OPCI study (Centro per la Lottacontro l’Infarto-Optimisation ofPercutaneous Coronary Interven-tion), which analyzed the clinicalimpact of OCT findings on improv-ing the outcomes of patients under-going PCI. This multicenter study23
addressed the role of OCT guidance,and by using a propensity scoreadjustment, the study compared theclinical outcome of 335 patients receiving OCT-guided interventionwith patients in the control group.OCT guidance improved the 1-yearcomposite event of cardiac deathor nonfatal myocardial infarctionafter PCI in a real-world population.The study also addressed the issueof how to treat OCT findings thatare indicative of suboptimal stentdeployment. In 34.7% of the stentedsegments, according to the OCT results, a further intervention with

291
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Intracoronary imaging and atherosclerosis - Prati and others
either balloon dilation (22.3%) or ad-ditional stenting (12.4%) was needed.The study concluded that specificquantitative OCT thresholds are re-quired to improve the clinical out-comes of patients undergoing PCI.
OCT studies in patients with ACShave shown that in-stent tissue pro-trusion due to the presence of aresidual thrombus is common. Re-cent data revealed that a residualintrastent thrombus is related to aperiprocedural myocardial infarc-tion if left untreated.24 Preliminarydata showed that additional OCT-driven in-stent balloon dilatationcould significantly reduce the in-stent thrombus area percentagewithout worsening the microcircu-latory indexes. As another crucialapplication, OCT can clarify themechanisms of restenosis andthrombosis early or late after theindex procedure, guiding repeatrevascularization, thus minimizingthe risk of additional adverse events.
Assessment of stent underexpan-sion by OCT can be obtained bycomparing the minimal stent areawith the reference lumen area. Ad-ditionally, a threshold of an absoluteminimum lumen cross-sectionalarea within the stent could be ap-plied; previously, the target mini-mum stent area advocated to pre-vent failure was an area of at least5.0 to 5.5 mm2.
In the 2015 CLI-THRO study, ourgroup addressed the incidence ofsuboptimal OCT results in 21 con-secutive patients exhibiting suba-cute thrombosis. The patients werematched 1:2 with a control groupof 42 patients from the Rome HeartResearch core lab database. OCTshowed that the minimum lumenarea and the minimum stent areameasurements were significantlysmaller in the stent thrombosisgroup; in addition, there was a high-
er frequency of stent underexpan-sion, edge dissection, and refer-ence lumen narrowing.25
IVUS-GUIDED PCI
Randomized studies conducted inthe 1990s evaluated the usefulnessof an IVUS-guided approach of bare-metal stent expansion to reducerestenosis. Most of these studieswere underpowered and restrictedto noncomplex lesions.10 After theintroduction of drug-eluting stents,the benefits of IVUS was ques-tioned given the improved out-comes with drug-eluting stents vsbare-metal stents.
A recent substudy of the ADAPT-DEStrial (Assessment of Dual AntiPla-telet Therapy with Drug-ElutingStents) compared IVUS and angiog-raphy-guided PCIs in terms of 1-yearoutcomes26 in 8583 consecutivepatients. IVUS was utilized in 39%of the patients, while angiographyalone was utilized in the remaining61%. Interestingly, in the IVUS-guid-ed arm, interventional cardiologistschanged the PCI strategy in 74% ofpatients, mainly employing a largerstent or balloon. The overall 1-yearrate of adjudicated MACE, definedas cardiac death, definite/probablestent thrombosis, or myocardial in-farction, was significantly lower inthe IVUS-guided group comparedwith the angiography-guided group(3.1% vs 4.7%; HR, 0.67; 95% CI, 0.53-0.84; P=0.0006). However, the dif-ference was mainly due to a reducedincidence of definite/probable stentthrombosis together with a lowerrate of spontaneous and target ves-sel–related myocardial infarction.The benefits of IVUS were especiallyevident in patients with ACS andcomplex lesions, although signifi-cant reductions in MACE occurredin all patient subgroups, includingthose with stable angina and single-vessel disease.26
CONCLUSION
Intravascular imaging techniqueshave been broadly used for researchpurposes to study coronary athero-sclerosis and to understand thepathophysiology of acute coronaryevents better. IVUS guidance of PCIshas an established role, and thereis preliminary evidence for a clinicalimpact of OCT.
REFERENCES
1. Gensini GG.
A more meaningful scoring system for determining the severity of coronary heartdisease.
Am J Cardiol. 1983;51:606.
2. Sianos G, Morel MA, Kappetein AP,et al.
The SYNTAX Score: an angiographic toolgrading the complexity of coronary arterydisease.
EuroIntervention. 2005;1:219-227.
3. Prati F, Regar E, Mintz GS, et al.
Expert review document on methodology,terminology, and clinical applications ofoptical coherence tomography: physicalprinciples, methodology of image acquisition,and clinical application for assessment ofcoronary arteries and atherosclerosis.
Eur Heart J. 2010;31:401-415.
4. Prati F, Guagliumi G, Mintz GS, et al.
Expert review document part 2: methodology,terminology and clinical applications of optical coherence tomography for the assessment of interventional procedures.
Eur Heart J. 2012;33:2513-2520.
5. Jang IK, Tearney GJ, MacNeill B,et al.
In vivo characterization of coronary athero-sclerotic plaque by use of optical coherencetomography.
Circulation. 2005;111:1551-1555.

292
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Intracoronary imaging and atherosclerosis - Prati and others
6. Virmani R, Kolodgie FD, BurkeAP, Farb A, Schwartz SM.
Lessons from sudden coronary death: acomprehensive morphological classificationscheme for atherosclerotic lesions.
Arterioscler Thromb Vasc Biol.2000;20:1262-1275.
7. Di Vito L, Agozzino M, Marco V, et al.
Identification and quantification of macro-phage presence in coronary atheroscleroticplaques by optical coherence tomography.
Eur Heart J Cardiovasc Imaging. 2015;16:807-813.
8. Tearney GJ, Regar E, Akasaka T,et al; International Working Groupfor Intravascular Optical CoherenceTomography.
Consensus standards for acquisition, meas-urement, and reporting of intravascular op-tical coherence tomography studies.
J Am Coll Cardiol. 2012;59:1058-1072.
9. Nissen SE, Yock P.
Intravascular ultrasound: novel patho-physiological insights and current clinicalapplications.
Circulation. 2001;103:604-616.
10. Mintz GS, Nissen SE, AndersonWD, et al.
American College of Cardiology clinicalexpert consensus document on standards foracquisition, measurement and reporting ofintravascular ultrasound studies (IVUS).
J Am Coll Cardiol. 2001;37:1478-1492.
11. Gardner CM, Tan H, Hull EL, et al.
Detection of lipid core coronary plaques inautopsy specimens with a novel catheter-based near-infrared spectroscopy system.
JACC Cardiovasc Imaging. 2008;1:638-648.
12. Stone GW, Maehara A, LanskyAJ, et al; PROSPECT Investigators.
A prospective natural-history study of coro-nary atherosclerosis.
N Engl J Med. 2011;364:226-235.
13. Gabriele A, Marco V, Gatto L, et al.
Reproducibility of the Carpet View system:a novel technical solution for display andoff line analysis of OCT images.
Int J Cardiovasc Imaging. 2014;30:1225-1233.
14. Tearney GJ, Yabushita H, HouserSL, et al.
Quantification of macrophage content inatherosclerotic plaques by optical coherencetomography.
Circulation. 2003;107:113-119.
15. Wang Z, Chamie D, Bezerra HG,et al.
Volumetric quantification of fibrous capsusing intravascular optical coherence tomography.
Biomed Opt Express. 2012;3:1413-1426.
16. Niccoli G, Montone RA, Di Vito L,et al.
Plaque rupture and intact fibrous cap as-sessed by optical coherence tomographyportend different outcomes in patients withacute coronary syndrome.
Eur Heart J. 2015;36:1377-1384.
17. Souteyrand G, Arbustini E,Motreff P, et al.
Serial optical coherence tomography imagingof ACS-causing culprit plaques.
EuroIntervention. 2015;11:319-324.
18. Di Vito L, Prati F, Arbustini E,Crea F, Maseri A.
A “stable” coronary plaque rupture docu-mented by repeated OCT studies.
JACC Cardiovasc Imaging. 2013;6:835-836.
19. Yonetsu T, Suh W, Abtahian F, et al.
Comparison of near-infrared spectroscopyand optical coherence tomography for detection of lipid.
Catheter Cardiovasc Interv. 2014;84:710-717.
20. Muller JE, Abela GS, Nesto RW,Tofler GH.
Triggers, acute risk factors and vulnerableplaques: the lexicon of a new frontier.
J Am Coll Cardiol. 1994;23:809-813.
21. Narula J, Nakano M, Virmani R,et al.
Histopathologic characteristics of athero-sclerotic coronary disease and implicationsof the findings for the invasive and nonin-vasive detection of vulnerable plaques.
J Am Coll Cardiol. 2013;61:1041-1051.
22. Calvert PA, Obaid DR, O’SullivanM, et al.
Association between IVUS findings and ad-verse outcomes in patients with coronaryartery disease: the VIVA (VH-IVUS inVulnerable Atherosclerosis) Study.
JACC Cardiovasc Imaging. 2011;4:894-901.
23. Prati F, Di Vito L, Biondi-ZoccaiG, et al.
Angiography alone versus angiography plusoptical coherence tomography to guide de-cision-making during percutaneous coronaryintervention: the Centro per la Lotta control’Infarto-Optimisation of Percutaneous Coro-nary Intervention (CLI-OPCI) study.
EuroIntervention. 2012;8:823-829.
24. Porto I, Di Vito L, Burzotta F, et al.
Predictors of periprocedural (type IVa) my-ocardial infarction, as assessed by frequency-domain optical coherence tomography.
Circ Cardiovasc Interv. 2012;5:89-96.
25. Prati F, Kodama T, Romagnoli E,et al.
Suboptimal stent deployment is associatedwith subacute stent thrombosis: optical coher-ence tomography insights from a multicentermatched study. From the CLI Foundationinvestigators: the CLI-THRO study.
Am Heart J. 2015;169:249-256.
26. Witzenbichler B, Maehara A,Weisz G, et al.
Relationship between intravascular ultra-sound guidance and clinical outcomes afterdrug-eluting stents: the assessment of dualantiplatelet therapy with drug-eluting stents(ADAPT-DES) study.
Circulation. 2014;129:463-470.

Appropriateness criteria for cardiovascular imaging use in clinical practice: a position statement of the ESC/EACVI taskforce
M. Garbi and others.Eur Heart J Cardiovasc Imaging. 2014
293Copyright © 2016, AICH - Servier Research Group. All rights reserved
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
1 6
2 7
Workstation-based calculation of CTA-based FFR for intermediate stenosis
M. Kruk and others. JACC Cardiovasc Imaging. 2016
8
Summaries of Ten Seminal PapersInês Z. Cabrita, PhD1; Francisca P. Figueiras, PhD1; Fausto J. Pinto, MD, PhD2
1CETERA - Academic Consulting Research Organization - Association for Research and Development of the Faculty of Medicine (AIDFM) - Lisbon - PORTUGAL
2University Hospital Santa Maria - Department of Cardiology - Lisbon Academic Medical Centre CCUL - Lisbon - PORTUGAL (e-mail: [email protected])
Dialogues Cardiovasc Med. 2016;21:293-303
4Cardiovascular imaging practice in Europe: a report from the European Association of
Cardiovascular Imaging P. Lancellotti and others. Eur Heart J. 2015
9Echocardiographic and fluoroscopic fusion
imaging for procedural guidance: an overview andearly clinical experience
J. J. Thaden and others. J Am Soc Echocardiogr. 2016
Diagnostic performance of the 3D bull’s eye display of SPECT and coronary CTA fusion
T. Nakahara and others.JACC Cardiovasc Imaging. 2016
10
Prognostic value of coronary artery calcium scoringin addition to single-photon emission computed
tomographic myocardial perfusion…E. M. Engbers and others.
Circ Cardiovasc Imaging. 2016
5
Outcomes of anatomical versus functional testingfor coronary artery disease
P. S. Douglas and others. N Engl J Med. 2015
3
Selection of seminal papers by Fausto J. Pinto, MD, PhDUniversity Hospital Santa Maria - Department of Cardiology - Lisbon Academic Medical Centre - CCUL - Lisbon - Portugal
www.dialogues-cvm.org
Echocardiographic chamber quantification in the era of multimodality imaging: beware
of unintended consequences H. Feigenbaum. J Am Soc Echocardiogr. 2015
Coronary Artery Disease Imaging
Multimodality cardiovascular molecular imaging, part II M. Nahrendorf and others.
Circ Cardiovasc Imaging. 2009
Low-dose CT coronary angiography with a novelIntraCycle motion-correction algorithm…
D. Andreini and others.Eur Heart J Cardiovasc Imaging. 2015
Highlights of the years by Sherri Smith, PhDPublications office

294
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
olecular imaging has the potential to impact cardiovascular medicine in severalways, including risk assessment, earlydisease detection, development of person-alized and targeted therapeutic regimens,
and monitoring of therapeutic efficacy and outcome. Inaddition to these direct implications, molecular imagingwill affect clinical care indirectly by facilitating a more rapiddevelopment of novel pharmaceutics and improving thebasic understanding of cardiovascular pathophysiology.
Nahrendorf et al summarized the available targeted imag-ing probes and the specific future applications of molecularimaging for the identification and evaluation of criticalpathophysiological processes of the cardiovascular system.Novel imaging strategies for the evaluation of inflammation,thrombosis, apoptosis, necrosis, vascular remodeling, andangiogenesis were also included in the review. Nahrendorfet al also examined the role of targeted imaging for somecardiovascular diseases, such as atherosclerosis, ischemicinjury, postinfarction remodeling, and heart failure, andthe emerging fields of regenerative, genetic, and cell-based therapies.
Particular emphasis is placed on multimodal imaging, asthese hybrid techniques promise to advance the field bycombining approaches with complementary strengths andoffsetting limitations. The routine application of molecularimaging in the management of patients with cardiovasculardisease is likely very close to being achieved. Molecularimaging should develop further with appropriate educa-tion of the cardiovascular community and the increasedavailability of various hybrid-imaging systems (ie, single-photon emission computed tomography [SPECT]/computedtomography [CT], positron emission tomography [PET]-CT,PET-magnetic resonance imaging [MRI]) that will facilitatequantification of molecular imaging agents. A number ofchallenges, however, stand in the way of realizing thesepromises. Current imaging systems have not been opti-mized for cardiac applications due to the inadequate cor-rection for cardiac and respiratory motion and a lack ofquantitative software for targeted agents. The full realiza-
tion of the promise of cardiovascular molecular imagingwill thus require an ongoing and concerted collaborationbetween industry and both the basic science and imagingcommunities.
“Smart” amplification strategies, comparative head-to-headanalysis of markers, improved reporter performance, andimproved hardware will enable the detection of minusculeor trace amounts of novel targets. These noninvasive andtargeted approaches will need to be tested for their prog-nostic value, cost effectiveness, and potential long-termtoxicity to translate these technological advances into improved patient care.
M
Multimodality cardiovascular molecular imaging, part II
M. Nahrendorf, D. E. Sosnovik, B. A. French, F. K. Swirski, F. Bengel, M. M. Sadeghi, J. R. Lindner, J. C. Wu, D. L. Kraitchman, Z. A. Fayad, et al
Circ Cardiovasc Imaging. 2009;2:56-70
The longest-lasting total solar eclipse of the 21st century occurs; the search for exoplanets begins with the launch of the Kepler space
observatory; and army ant specialist Carl Rettenmeyer dies at age 78
2009

295
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
nterest from the scientific community is growing re-garding the appropriate use of cardiovascular imag-ing techniques for diagnosis and decision makingin Europe. A dedicated taskforce has been appointedby the European Society of Cardiology (ESC) and
the European Association of Cardiovascular Imaging (EACVI)to develop appropriateness criteria for cardiovascular im-aging use in clinical practice in Europe. Cardiovascularimaging is characterized by continuously evolving technol-ogy developments in all modalities. Therefore, assistancewith the decision-making process regarding both the choiceof imaging modality in a certain clinical scenario and thefuture development of availability at local, national, andEuropean levels becomes crucial.
The appropriateness criteria involve the evidence, guide-line-based criteria, and best practice–based criteria forthe appropriate use of cardiovascular imaging modalitiesin clinical practice, which are meant to assist in the deci-sion-making process. These appropriateness criteria will bedeveloped to ensure the best use of diagnostic cardiovas-cular imaging resources for a given individual, the rationaluse of cardiovascular imaging resources for all individualsin need of diagnosis, the most efficient use of availablefunds for society, and the judicious implementation ofevolving technology and evidence in clinical practice.
The determination of appropriateness criteria, updated atregular 3-year intervals, will start with the appointment ofa panel of reviewers consisting of experts in each cardio-vascular imaging modality and a voting panel. The panelwill make a selection of clinical scenarios; review the evi-dence, guidelines, position papers, etc; define indications;and assign an appropriateness score. For more informationon the development process, please see Figure 1 fromthe paper by Garbi et al.
The appropriateness criteria, statement papers, education-al material, supporting clinical implementation, and allrelated documents will be made available online and dis-tributed actively to different entities (eg, European Com-mission, the European National Societies, Working Groups,
and Associations). Additionally, web-based tools and ap-plications will be developed to assist with the clinical de-cision-making process and the selection of an appropriateimaging test for a particular indication.
The appropriateness criteria will be patient-centered, fa-cilitating the best use of cardiovascular imaging resourcesfor an individual who needs a test, while encouraging thebest use of material resources for the entire society, struc-tured development of resources, efficient financial expen-diture, and homogenization of care across Europe.
I
Appropriateness criteria for cardiovascular imaging use in clinicalpractice: a position statement of the ESC/EACVI taskforce
M. Garbi, G. Habib, S. Plein, D. Neglia, A. Kitsiou, E. Donal, F. Pinto, J. Bax, S. Achenbach, B. A. Popescu, et al
Eur Heart J Cardiovasc Imaging. 2014;15:477-482
Eyesight has been restored in six patients using a new gene therapy technique;
the tsetse fly genome sequencing project is complete after a 10-year multimillion dollar effort;
and the length of a day for an exoplanet is measured for the first time
2014

atients who have symptoms suggestive of coro-nary artery disease are often evaluated with theuse of diagnostic testing, although limited dataare available from randomized trials to guidecare. The coronary computed tomography an-
giography (CCTA) technique is one possible tool that mayreduce unnecessary invasive testing and improve patientoutcomes. However, the impact of data from noninvasive vsinvasive testing on the management of the disease andclinical outcomes is unknown. The PROMISE trial (PROspec-tive Multicenter Imaging Study for Evaluation of chestpain) was designed to compare health-related outcomesbetween CCTA and functional testing in patients presentingwith symptoms of coronary artery disease that requiredfurther evaluation.
Douglas et al randomly assigned 10 003 symptomatic pa-tients to a strategy of initial anatomical testing with theuse of either CCTA or functional testing (exercise electro-cardiography, nuclear stress testing, or stress echocardiogra-phy). The composite primary end point was death, myo-cardial infarction, hospitalization for unstable angina, ormajor procedural complications. Secondary end points in-cluded radiation exposure and invasive cardiac catheteriza-tion that did not show obstructive coronary artery disease.
The mean age of the patients was 60.8±8.3 years, 52.7%were women, and 87.7% had chest pain or dyspnea on exertion. The mean pretest likelihood of obstructive coro-nary artery disease was 53.3%±21.4%. Over a median fol-low-up period of 25 months, a primary end point eventoccurred in 164 of 4996 patients in the CCTA group (3.3%)and in 151 of 5007 (3.0%) in the functional testing group(adjusted hazard ratio, 1.04; 95% confidence interval, 0.83to 1.29; P=0.75). CCTA was associated with fewer catheter-izations showing no obstructive coronary artery diseasethan functional testing (3.4% vs 4.3%; P=0.02), althoughmore patients in the CCTA group underwent catheterizationwithin 90 days after randomization (12.2% vs 8.1%). Themedian cumulative radiation exposure per patient was low-er in the CCTA group than in the functional testing group(10.0 mSv vs 11.3 mSv), but 32.6% of the patients in the
functional testing group had no exposure, so the overallexposure was higher in the CCTA group (mean, 12.0 mSvvs 10.1 mSv; P<0.001).
In conclusion, in symptomatic patients with suspectedcoronary artery disease who required noninvasive testing,an initial strategy of CCTA was not associated with betterclinical outcomes than functional testing over a medianfollow-up of 2 years.
296
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
Outcomes of anatomical versus functional testing for coronary artery disease
P. S. Douglas, U. Hoffmann, M. R. Patel, D. B. Mark, H. R. Al-Khalidi, B. Cavanaugh, J. Cole, R. J. Dolor, C. B. Fordyce, M. Huang, et al; PROMISE Investigators
N Engl J Med. 2015;372:1291-1300
P
Biodegradable nanoparticles are used to kill brain cancer cells in animals;
two lost cities in the Honduras jungle are discovered; and an almost completely intact skeleton of a terror bird is found in Argentina
2015

297
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
pidemiology changes in cardiovascular diseaseand an aging population are expected to resultin an increased need for cardiovascular imaging(CVI). However, reliable statistics on the use ofCVI in Europe are lacking. The European Associ-
ation of Cardiovascular Imaging (EACI) and the EuropeanSociety of Cardiology (ESC) Taskforce on CVI establishedthe status of CVI use across Europe. In 2013, a survey with relevant information regarding CVI was sent to every national imaging/echocardiography society and workinggroup. The survey was designed to assess existing education,training, certification and national accreditation programs,health care organizations, and reimbursement systems.
The percentage of countries with a national certificationin CVI for cardiologists was different between imagingmodalities. Transthoracic and transesophageal echocar-diography were commonly certified techniques, and aboutone-third of the countries had a certification program forthe other imaging modalities. The majority of national societies recommended the Imaging Taskforce of the EACI(EACVI) certification, but one-fifth of the societies hadtheir national certification system. Irrespective of the CVImodality, a national accreditation for centers/laboratorieswas not required for practice in most countries.
Overall, there were diverse country-specific regulations forperforming CVI and a widespread lack of national certifi-cation/accreditation. However, the majority of countriesrecommended the EACVI certification and one-fifth of thecountries applied it as a national certification. Cardiologistscommonly performed echocardiography, but not computedtomography (CT), cardiovascular magnetic resonance im-aging (CMR), or nuclear imaging. However, in most coun-tries, medical imaging performance requires a specialistlicense (eg, cardiologist, radiologist, and a nuclear imagingspecialist). Unexpectedly, a predefined period of trainingin CVI during specialization was absent in one-third of thecountries. In addition, only a few countries offered officialnational certification guidelines to perform CVI examina-tions. Interestingly, the adherence to ESC/EACVI guidelinesin CVI was reported in a high number of European countries.
Finally, the access to CVI examinations in the publichealth care system was marked by a long waiting periodin some countries.
The current mapping of the practice of CVI techniquesacross Europe represents the first comprehensive projectof the ESC/EACVI Taskforce on CVI. The report symbolizesa preliminary step for further data collection and network-ing with national imaging societies and working groups.In the future, direct comparisons among the different ESCcountries should help standardize health care resourcesby promoting knowledge of their status and by bringingthis information to the attention of all public authorities.It is the hope that such data collection will contribute toimproved quality of care through a better use of resources(avoid unnecessary procedures and expenses) and a con-sequent reduction in the waiting time, thus increasing theavailability of CVI.
E
Cardiovascular imaging practice in Europe: a report from theEuropean Association of Cardiovascular Imaging
P. Lancellotti, E. Płońska-Gościniak, M. Garbi, C. Bucciarelli-Ducci, B. Cosyns, N. Cardim, M. Galderisi, T. Edvardsen, D. Neglia, S. Plein, et al
Eur Heart J. 2015;16:697-702
The Japanese L0 Series maglev becomes the first train to operate at a speed of 600 km/hour;
NASA’s MESSENGER spacecraft concludes its 4-year orbital mission over Mercury; and the opah is confirmed as the first
warm-blooded fish
2015

298
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
he primary purpose of the recently publishedupgrade to the guideline document for echo-cardiographic chamber quantification is to setstandard measurements, labels, and orienta-tions to improve the communication and
standardization among all echocardiography laboratoriesboth in the United States and in Europe. Another aim ofupgrading the document was to integrate echocardiographicchamber quantification with other cardiovascular imagingmodality categories, with a notorious effort to recognizeechocardiography as part of the noninvasive cardiovascularimaging modalities. In this paper, Feigenbaum clearly emphasizes that as with all changes or ‘‘advances,’’ thereare likely to be unexpected or unintended consequences,which has been the case for this modality.
An early effort to improve the communication and coher-ence between echocardiography and nuclear cardiologywas to change echocardiography’s standard 16-segmentwall motion scoring system by adding a 17th segment atthe apex. Echocardiography representatives agreed to makethe change so that the scoring would be compatible withthe nuclear apical perfusion and multiple-gated acquisi-tion scan for apical motion. However, it was later decidedthat due to recording specifications in echocardiographywhen using the 17-segment model to assess wall motionor regional strain, the 17th segment (the apical cap) shouldnot be included.
Another effort was made to obtain standard echocardio-graphic segmentation labels and orientation so that theywould be similar to those used in nuclear perfusion. Un-fortunately, this was not possible; for example, it was notpossible to standardize the labels for the right ventricleand the papillary muscle. Importantly, the back wall of theleft ventricle, which had been labeled ‘‘posterior,’’ is nowbeing labeled ‘‘inferior lateral’’ to make it compatible withnuclear cardiology. This change has caused some compre-hensible controversy. Besides the desire to set standardmeasurements, labels, and orientation, there are likely tobe significant differences between echocardiography andcardiac computed tomography and magnetic resonance.
Care must be taken with the concept of integrated and‘‘consensus’’ multimodality imaging applications in theclinical setting.T
Echocardiographic chamber quantification in the era of multimodality imaging: beware of unintended consequences
H. Feigenbaum
J Am Soc Echocardiogr. 2015;28:847-850
Lokiarchaeota, a transitional form between Archaea and Eurkaryotes, is discovered;
the US Fish and Wildlife Service declares that the eastern cougar is extinct; and
the first artificial ribosome is created
2015

299
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
hile coronary computed tomography an-giography (CCTA) has achieved good diag-nostic performance, motion artifacts dueto a high heart rate or high heart ratevariability significantly affect the image
quality of CCTA. As a result, a motion-correction algo-rithm has been developed. In this study by Andreini et al,the impact of this algorithm when used in conjunctionwith low-dose prospective ECG-triggering CCTA on motionartifacts, image quality, and coronary assessability wasevaluated. Only one previous study assessed the diagnosticperformance of the motion-correction algorithm in con-junction with retrospective ECG-triggering CCTA in a smallpatient population referred for transcatheter aortic valveimplantation. A secondary aim of the study was to evalu-ate the diagnostic accuracy of CCTA performed with themotion-correction algorithm and standard reconstructionin comparison with invasive coronary angiography—thegold-standard imaging technique.
Of the 410 consecutive patients undergoing CCTA for sus-pected coronary artery disease who were considered forinclusion in this study, 120 patients with a prescanningheart rate >70 bpm or a heart rate variability >10 bpmduring scanning irrespective of prescanning heart rate orboth were selected. Mean prescanning heart rate and heartrate variability were 70±7 bpm and 10.9±4 bpm, respec-tively. Overall, the mean effective dose of radiation was3.4±1.3 mSv, while a lower dose (2.4±0.9 mSv) was meas-ured for padding of 80 ms. In a segment-based analysis,coronary assessability was significantly higher (P<0.0001)with motion correction (97%) when compared with stan-dard reconstruction (81%) due to a significant reduction(P<0.0001) in severe artifacts (54 vs 356 cases, respectively).An artifact subanalysis showed a significantly lower number of motion artifacts and artifacts related to chestmovement with motion correction (16 and 4 cases) thanwith standard reconstruction (286 and 24 cases; P<0.0001and P<0.05, respectively).
In conclusion, this study showed that in a subset of patientswith high prescanning heart rate, increased heart rate
variability, and high mean maximum heart rate duringscanning, CCTA with motion-correction reconstructionachieved good image quality, very high coronary assess-ability, and a lower radiation exposure.W
Low-dose CT coronary angiography with a novel IntraCyclemotion-correction algorithm in patients with high heart rate orheart rate variability
D. Andreini, G. Pontone, S. Mushtaq, E. Bertella, E. Conte, C. Segurini, A. Baggiano, A. L. Bartorelli, A. Annoni, A. Formenti, et al
Eur Heart J Cardiovasc Imaging. 2015;16:1093-1100
The genes responsible for the 200-year lifespan of the bowhead whale are mapped;
astronomers identify a method to determine a star’s age from how fast it spins; and
an exoplanet with a gigantic ring system that is 200times larger than that around Saturn is discovered
2015

ingle-photon emission computed tomography(SPECT) myocardial perfusion imaging is well es-tablished for the prognostic evaluation of patientswith suspected coronary artery disease. However,this functional imaging modality is not able to de-
tect nonflow-limiting coronary artery disease. The increasedinterest in using coronary artery calcium (CAC) to identifysubclinical atherosclerosis has demonstrated a close correlation with atherosclerotic plaque burden. With the advent of combined SPECT and computed tomographycameras, it is possible to acquire both SPECT images andCAC scores in a single session.
Engbers et al investigated the prognostic value of CAC scor-ing as an adjunct to SPECT in a population who are at a low-to intermediate-risk for stable coronary artery disease. Atotal of 4897 symptomatic patients with no history of coro-nary artery disease who were referred for SPECT and CACscoring were included. Major adverse cardiac events weredefined as late revascularization (>90 days after scanning),nonfatal myocardial infarction, and all-cause mortality.
The frequency of abnormal SPECT increased with higherCAC scores, from 12% in patients with CAC scores of 0%to 19%, 32%, 37%, and 50% among those with CAC scores1 to 99, 100 to 399, 400 to 999, and ≥1000, respectively(P<0.001). During a median follow-up of 940 days (25th to75th percentile, 581-1377), 278 major adverse cardiacevents were observed, and the overall incidence of majoradverse cardiac events was 2.3% per year. A stepwise in-crease in major adverse cardiac events was present withincreasing CAC scores, both in patients with a normal SPECTresult (annual event rate CAC score 0, 0.6%; CAC score≥1000, 5.5%) and an abnormal SPECT result (annual eventrate CAC score 0, 0.4%; CAC score ≥1000, 7.6%). After mul-tivariate analysis, both SPECT results and CAC scoreswere independent predictors of major adverse cardiacevents (CAC score ≥1000: hazard ratio, 7.7; P<0.001 andlarge perfusion defect on SPECT: hazard ratio, 3.7; P<0.001).
CAC score and SPECT are independent predictors of majoradverse cardiac events in patients suspected of coronary
artery disease. Our findings strongly support acquiring aCAC score in addition to SPECT in symptomatic patientsto define the risk of events during follow-up better.S
Prognostic value of coronary artery calcium scoring in addition to single-photon emission computed tomographic myocardialperfusion imaging in symptomatic patients
E. M. Engbers, J. R. Timmer, J. P. Ottervanger, M. Mouden, S. Knollema, P. L. Jager
Circ Cardiovasc Imaging. 2016;9:e004876
300
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
Strimvelis, the first gene therapy for children, receives regulatory approval by the European
Commission; scientists perform the first spectroscopy of the atmospheres of Earth-sized exoplanets using the Hubble telescope; and
Solar Impulse 2 becomes the first solar-powered aircraft to circumnavigate the Earth
2016

301
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
oronary computed tomography angiography(CCTA) is a common diagnostic test indicatedin patients with an intermediate probabilityof coronary artery disease. However, it oftenends up in a diagnosis of intermediate coro-
nary stenosis that leads to further functional testing. CCTA–based fractional flow reserve (CCTA-FFR) is an emergingmethod for the noninvasive functional diagnosis of coro-nary artery disease. This imaging technique is the resultof the fusion of both an anatomical test and a computa-tionally simulated surrogate of FFR, providing a “one-stopshop” diagnostic tool. Both method developers and clini-cians pursue a better understanding of the technique andaim to compare the clinical value across different CCTA-FFR results.
Kruk et al conducted a study to evaluate the proportion of patients with intermediate coronary stenosis diagnosedon CCTA, who may be saved from any further testing dueto the use of CCTA-FFR. The study involved determiningthe upper and lower CCTA-FFR thresholds that predictnonischemic and ischemic stenosis, respectively, (basedon an invasive FFR cutpoint ≤0.80) with ≥90% accuracy,and subsequently determining the proportion of patientswho fall between these thresholds.
A total of 90 patients were included in this prospective,single-center, cohort study, and 96 lesions were analyzed.The patients who underwent routine CCTA due to an in-termediate probability of having a significant coronary artery stenosis and who had a CCTA diagnosis of at leastone intermediate coronary stenosis (50% to 90% by visualestimation) in an artery ≥2 mm in diameter were sched-uled to undergo invasive FFR within 6 months of the CCTAexamination.
The study demonstrated that an invasive FFR ≤0.8 wasobserved in 41 of 96 lesions (42.7%). According to a Bland-Altman analysis, CCTA-FFR underestimated FFR by 0.01and the 95% limit of agreement was ±0.19. The CCTA-FFRthresholds for which the positive and negative predictivevalues were each ≥90% (corresponding to an FFR ≤0.80)
were >0.87 or <0.74, respectively, and they involved 49 lesions (51%) and 45 of the 90 patients. The authors con-cluded that this hybrid diagnostic approach (the prototypeCCTA-FFR based on CCTA) may discriminate between is-chemic vs nonischemic stenoses in around 50% of patientswith an intermediate coronary stenosis, potentially savingthem from further functional testing. Further studies areneeded for the validation of the methodology in an inde-pendent multicenter cohort.
Workstation-based calculation of CTA-based FFR for intermediate stenosis
M. Kruk, Ł. Wardziak, M. Demkow, W. Pleban, J. Pręgowski, Z. Dzielińska, M. Witulski, A. Witkowski, W. Rużyłło, C. Kępka
JACC Cardiovasc Imaging. 2016;9:690-699
C
Yoshinori Ohsumi is awarded the 2016 Nobel Prize in Physiology or Medicine;the world’s first baby is born using the
controversial new “three parent” technique; andasprosin, a fasting-induced glucogenic
protein hormone, is discovered
2016

302
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
uring the last few years, there has been anexponential growth in the novel percutaneousstructural heart interventions developed totreat valvular and structural heart conditionsthrough a transcatheter approach. Investiga-
tional device-based therapies, such as transcatheter aorticvalve replacement, transcatheter mitral valve repair, leftatrial appendage occlusion, and percutaneous paravalvularleak closure, have necessitated increased sophisticatedimaging guidance that is not supported solely by fluoroscopy.
There has been increased interest in the multimodalityimaging that has fueled the development of fusion imag-ing to facilitate procedural guidance. Echocardiographicand fluoroscopic fusion imaging combines the precisecatheter and device visualization of fluoroscopy with thesoft tissue anatomy and color flow Doppler informationafforded by echocardiography in a single image. This typeof fusion imaging allows for precise catheter manipulationsunder fluoroscopic guidance while visualizing critical tis-sue anatomy provided by echocardiography. Thaden et alelegantly review this emerging technology’s strengths,limitations, and potential clinical applications.
Image registration is the first step of fusion imaging, andit involves reorientation of one image (echocardiographyimage) to match the orientation of a second image (fluo-roscopy). These fusion images are compatible with 2Dechocardiographic imaging with or without color Doppler,simultaneous multiplane echocardiographic imaging, and3D echocardiographic imaging.
Three-dimensional volume data sets can also be displayedas the complete volume of data, which can be cropped inthe plane of the fluoroscopic image to display soft tissueanatomy relevant to the procedure or as a partial-thick-ness slice that can be moved from near to far and in thedirection of the fluoroscopic beam. Procedure-specificconsiderations have been made concerning transseptalpuncture, left atrial appendage occlusion, paravalvularleak closure, and transcatheter mitral valve repair.
In conclusion, echocardiographic guidance for tran-scatheter mitral valve repair is essential for proceduralsuccess and remains challenging in current clinical prac-tice. As with many new devices and technologies, a learn-ing curve is involved. In some cases, performing the imag-ing study while also manipulating the fusion imagingsystem can be a challenge. Furthermore, it would be in-teresting to know whether this technology and its accura-cy will be important to improve the outcomes of patientsundergoing structural procedures.
Echocardiographic and fluoroscopic fusion imaging for procedural guidance: an overview and early clinical experience
J. J. Thaden, S. Sanon, J. B. Geske, M. F. Eleid, N. Nijhof, J. F. Malouf, C. S. Rihal, C. J. Bruce
J Am Soc Echocardiogr. 2016;29:503-512
D
Oxygen is detected in the Martian atmosphere;a successful monkey head transplant
is conducted; and a pregnant Tyrannosaurus rexis discovered
2016

Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Summaries of Ten Seminal Papers - Cabrita and others
yocardial perfusion single-photon emis-sion computed tomography (SPECT) andcoronary computed tomography angio-graphy are distinct diagnostic imagingmodalities that provide functional and
anatomical information, respectively. SPECT/coronarycomputed tomography angiography hybrid imaging mightbe one of the forms that routine myocardial perfusion imaging will take because image fusion significantly im-proves detection of hemodynamically significant coronarylesions.
Nakahara et al developed a display method to present thefusion data of myocardial perfusion SPECT and coronarycomputed tomography angiography into a single imagethat they call the fusion-based bull’s eye. A 3D display ismostly used when reviewing SPECT/coronary computedtomography angiography fusion images, although multi-directional interpretation is required to sweep the entireheart. Fusion-based bull’s eye images are generated from3D fusion data by determining a cardiac axis, adding a cylindrical object around the aortic root, obtaining apanoramic image from circumferential data of the 3D images, and converting it into a polar coordinate displayimage. The diagnostic performances between SPECT, conventional 3D fusion, and the fusion-based bull’s eye asregards the presence of hemodynamically relevant coro-nary vessels were compared in 39 patients with abnormalSPECT findings.
Of an evaluated 105 coronary segments in 35 patients with-out coronary artery bypass grafting, SPECT showed 17segments (16%) equivocal to determine hemodynamicallyrelevant coronary vessels. The fusion-based bull’s eye cor-rected the diagnoses of 5 segments, where SPECT provideda false-negative in 2 segments and a false-positive in 3 segments, with only 2 equivocal segments (P=0.0017).
The fusion-based bull’s eye also revealed 4 culprit lesionsin all 4 patients with coronary artery bypass grafting. Therewas no discordance between the fusion-based bull’s eyeand conventional 3D fusion.
The fusion-based bull’s eye had the same capacity as con-ventional 3D fusion to solve equivocal SPECT findings orcorrect the diagnosis in 24 of 109 (22%) coronary segmentsfor culprit lesion detection. Although the fusion-basedbull’s eye generation is currently a time-consuming process,the process is simple and understandable. In addition,the fusion-based bull’s eye can be applied to patients withcoronary artery bypass grafting. In the circumstance thatboth SPECT and coronary computed tomography angiog-raphy are available, the fusion-based bull’s eye will becomeone of the selected choices for reviewing the anatomic andfunctional information at the same time.
Diagnostic performance of the 3D bull’s eye display of SPECTand coronary CTA fusion
T. Nakahara, Y. Iwabuchi, K. Murakami
JACC Cardiovasc Imaging. 2016;9:703-711
M
303
DNA is sequenced in outer space for the first time;the second largest meteorite ever found is exhumed near Gancedo, Argentina; and
Jemma Redmond, Irish biochemist and a pioneer of 3D bioprinting, dies at age 38
2016


305Copyright © 2016, AICH - Servier Research Group. All rights reserved www.dialogues-cvm.org
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Abbara S, Arbab-Zadeh A, Callister TQ, et al. SCCT guidelines for performance of coronary computed tomographicangiography.
J Cardiovasc Comput Tomogr. 2009;3:190-204.
Alderman EL, Fisher LD, Litwin P, et al. Results of coronary artery surgery in patients with poor left ventric-ular function (CASS).
Circulation. 1983;68:785-795.
Allman KC, Shaw LJ, Hachamovitch R, Udelson JE. Myocardial viability testing and impact of revascularization on prognosis in patients with coronary artery disease and left ventric-ular dysfunction: a meta-analysis.
J Am Coll Cardiol. 2002;39:1151-1158.
Amado LC, Gerber BL, Gupta SN, et al. Accurate and objective infarct sizing by contrast-enhanced magneticresonance imaging in a canine myocardial infarction model.
J Am Coll Cardiol. 2004;44:2383-2389.
Arbab-Zadeh A, Nakano M, Virmani R, Fuster V. Acute coronary events.
Circulation. 2012;125:1147-1156.
Baer FM, Smolarz K, Jungehülsing M, et al. Chronic myocardial infarction: assessment of morphology, function, and perfusion by gradient echo magnetic resonance imaging and 99mTc-methoxyisobutyl-isonitrile SPECT.
Am Heart J. 1992;123:636-645.
Bittencourt MS, Hulten E, Ghoshhajra B, et al. Prognostic value of nonobstructive and obstructive coronary artery disease detected by coronary computed tomography angiography to identify cardiovascular events.
Circ Cardiovasc Imaging. 2014;7:282-291.
Bonow RO, Maurer G, Lee KL, et al; Myocardial viability and survival in ischemic left ventricular STICH Trial Investigators. dysfunction.
N Engl J Med. 2011;364:1617-1625.
Bucciarelli-Ducci C, Auger D, Di Mario C, et al. CMR guidance for recanalization of coronary chronic total occlusion.
JACC Cardiovasc Imaging. 2016;9:547-556.
Calvert PA, Obaid DR, O’Sullivan M, et al. Association between IVUS findings and adverse outcomes in patients with coronary artery disease: the VIVA (VH-IVUS in Vulnerable Atherosclerosis) Study.
JACC Cardiovasc Imaging. 2011;4:894-901.
Catalano O, Moro G, Perotti M, et al. Late gadolinium enhancement by cardiovascular magnetic resonanceis complementary to left ventricle ejection fraction in predicting prognosis of patients with stable coronary artery disease.
J Cardiovasc Magn Reson. 2012;14:29.
Bibliography of One Hundred Key Papersselected by Fausto J. Pinto, MD, PhD
University Hospital Santa Maria - Department of Cardiology - Lisbon Academic Medical Centre - CCUL - Lisbon - PORTUGAL(e-mail: [email protected])
Coronary Artery Disease Imaging

Cho I, Chang HJ, Ó Hartaigh B, et al. Incremental prognostic utility of coronary CT angiography for asymptomatic patients based upon extent and severity of coronary artery calcium: results from the COronary CT Angiography EvaluatioN For Clinical Outcomes InteRnational Multicenter (CONFIRM) study.
Eur Heart J. 2015;36:501-508.
Cho I, Suh JW, Chang HJ, et al. Prevalence and prognostic implication of non-calcified plaque in asymptomatic population with coronary artery calcium score of zero.
Korean Circ J. 2013;43:154-160.
Costa MA, Shoemaker S, Futamatsu H, et al. Quantitative magnetic resonance perfusion imaging detects anatomicand physiologic coronary artery disease as measured by coronary angiography and fractional flow reserve.
J Am Coll Cardiol. 2007;50:514-522.
Dedic A, Lubbers MM, Schaap J, et al. Coronary CT angiography for suspected ACS in the era of high-sensitivity troponins: randomized multicenter study.
J Am Coll Cardiol. 2016;67:16-26.
Di Vito L, Agozzino M, Marco V, et al. Identification and quantification of macrophage presence in coronaryatherosclerotic plaques by optical coherence tomography.
Eur Heart J Cardiovasc Imaging. 2015;16:807-813.
Douglas PS, Hoffmann U, Patel MR, et al; Outcomes of anatomical versus functional testing for coronary PROMISE Investigators. artery disease.
N Engl J Med. 2015;372:1291-1300.
Engbers EM, Timmer JR, Ottervanger JP, Mouden M, Prognostic value of coronary artery calcium scoring in addition to Knollema S, Jager PL. single-photon emission computed tomographic myocardial perfusion
imaging in symptomatic patients.
Circ Cardiovasc Imaging. 2016;9:e003966.
Erbel R, Möhlenkamp S, Kerkhoff G, Budde T, Non-invasive screening for coronary artery disease: calcium scoring.Schmermund A. Heart. 2007;93:1620-1629.
Fihn SD, Blankenship JC, Alexander KP, et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stableischemic heart disease.
J Am Coll Cardiol. 2014;64:1929-1949.
Flohr TG, De Cecco CN, Schmidt B, Wang R, Computed tomographic assessment of coronary artery disease: Schoepf UJ, Meinel FG. state-of-the-art imaging techniques.
Radiol Clin North Am. 2015;53:271-285.
Garbi M, Habib G, Plein S, et al. Appropriateness criteria for cardiovascular imaging use in clinical practice: a position statement of the ESC/EACVI taskforce.
Eur Heart J Cardiovasc Imaging. 2014;15:477-482.
Gebker R, Jahnke C, Manka R, et al. Additional value of myocardial perfusion imaging during dobutaminestress magnetic resonance for the assessment of coronary artery disease.
Circ Cardiovasc Imaging. 2008;1:122-130.
Gerber BL, Rousseau MF, Ahn SA, et al. Prognostic value of myocardial viability by delayed-enhanced magnetic resonance in patients with coronary artery disease and low ejection fraction: impact of revascularization therapy.
J Am Coll Cardiol. 2012;59:825-835.
306
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers

Goldstein JA, Chinnaiyan KM, Abidov A, et al; The CT-STAT (Coronary Computed Tomographic Angiography for CT-STAT Investigators. Systematic Triage of Acute Chest Pain Patients to Treatment) trial.
J Am Coll Cardiol. 2011;58:1414-1422.
Goncalves Pde A, Rodriguez-Granillo GA, Spitzer E, et al. Functional evaluation of coronary disease by CT angiography.
JACC Cardiovasc Imaging. 2015;8:1322-1335.
Greenland P, Smith SC Jr, Grundy SM. Improving coronary heart disease risk assessment in asymptomatic people: role of traditional risk factors and noninvasive cardiovas-cular tests.
Circulation. 2001;104:1863-1867.
Greenwood JP, Maredia N, Younger JF, et al. Cardiovascular magnetic resonance and single-photon emission computed tomography for diagnosis of coronary heart disease (CE-MARC): a prospective trial.
Lancet. 2012;379:453-460.
Greenwood JP, Motwani M, Maredia N, et al. Comparison of cardiovascular magnetic resonance and single-photonemission computed tomography in women with suspected coronary artery disease from the Clinical Evaluation of Magnetic Resonance Imaging in Coronary Heart Disease (CE-MARC) Trial.
Circulation. 2014;129:1129-1138.
Gueret P, Deux JF, Bonello L, et al. Diagnostic performance of computed tomography coronary angio-graphy (from the Prospective National Multicenter Multivendor EVASCAN Study).
Am J Cardiol. 2013;111:471-478.
Hackam DG, Shojania KG, Spence JD, et al. Influence of noninvasive cardiovascular imaging in primary prevention: systematic review and meta-analysis of randomized trials.
Arch Intern Med. 2011;171:977-982.
Hoffmann R, von Bardeleben S, Kasprzak JD, et al. Analysis of regional left ventricular function by cineventriculography, cardiac magnetic resonance imaging, and unenhanced and contrast-enhanced echocardiography: a multicenter comparison of methods.
J Am Coll Cardiol. 2006;47:121-128.
Hoffmann U, Truong QA, Schoenfeld DA, et al; Coronary CT angiography versus standard evaluation in acute ROMICAT-II Investigators. chest pain.
N Engl J Med. 2012;367:299-308.
Hussain ST, Chiribiri A, Morton G, et al. Perfusion cardiovascular magnetic resonance and fractional flow reserve in patients with angiographic multi-vessel coronary artery disease.
J Cardiovasc Magn Reson. 2016;18:44.
Hussain ST, Paul M, Plein S, et al. Design and rationale of the MR-INFORM study: stress perfusion cardiovascular magnetic resonance imaging to guide the manage-ment of patients with stable coronary artery disease.
J Cardiovasc Magn Reson. 2012;14:65.
Jain D, He ZX. Direct imaging of myocardial ischemia: a potential new paradigm in nuclear cardiovascular imaging.
J Nucl Cardiol. 2008;15:617-630.
Janardhanan R, Moon JC, Pennell DJ, Senior R. Myocardial contrast echocardiography accurately reflects transmu-rality of myocardial necrosis and predicts contractile reserve after acute myocardial infarction.
Am Heart J. 2005;149:355-362.
307
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers

Jang IK, Tearney GJ, MacNeill B, et al. In vivo characterization of coronary atherosclerotic plaque by use of optical coherence tomography.
Circulation. 2005;111:1551-1555.
John AS, Dreyfus GD, Pennell DJ. Images in cardiovascular medicine. Reversible wall thinning in hibernation predicted by cardiovascular magnetic resonance.
Circulation. 2005;111:e24-e25.
Kaandorp TA, Lamb HJ, van der Wall EE, de Roos A, Cardiovascular MR to access myocardial viability in chronic Bax JJ. ischaemic LV dysfunction.
Heart. 2005;91:1359-1365.
Kim C, Hong SJ, Shin DH, et al. Limitations of coronary computed tomographic angiography for delineating the lumen and vessel contours of coronary arteries in patients with stable angina.
Eur Heart J Cardiovasc Imaging. 2015;16:1358-1365.
Kim RJ, Wu E, Rafael A, et al. The use of contrast-enhanced magnetic resonance imaging to identify reversible myocardial dysfunction.
N Engl J Med. 2000;343:1445-1453.
Klem I, Shah DJ, White RD, et al. Prognostic value of routine cardiac magnetic resonance assessment of left ventricular ejection fraction and myocardial damage: an international, multicenter study.
Circ Cardiovasc Imaging. 2011;4:610-619.
Ko BS, Cameron JD, Meredith IT, et al. Computed tomography stress myocardial perfusion imaging in patients considered for revascularization: a comparison withfractional flow reserve.
Eur Heart J. 2012;33:67-77.
Korosoglou G, Lehrke S, Wochele A, et al. Strain-encoded CMR for the detection of inducible ischemia duringintermediate stress.
JACC Cardiovasc Imaging. 2010;3:361-371.
Kuijpers D, Ho KY, van Dijkman PR, Vliegenthart R, Dobutamine cardiovascular magnetic resonance for the detection Oudkerk M. of myocardial ischemia with the use of myocardial tagging.
Circulation. 2003;107:1592-1597.
Kwong RY, Chan AK, Brown KA, et al. Impact of unrecognized myocardial scar detected by cardiac magnetic resonance imaging on event-free survival in patients presenting with signs or symptoms of coronary artery disease.
Circulation. 2006;113:2733-2743.
Lanza GA, Buffon A, Sestito A, et al. Relation between stress-induced myocardial perfusion defects on cardiovascular magnetic resonance and coronary microvascular dysfunction in patients with cardiac syndrome X.
J Am Coll Cardiol. 2008;51:466-472.
Lipinski MJ, McVey CM, Berger JS, Kramer CM, Prognostic value of stress cardiac magnetic resonance imaging in Salerno M. patients with known or suspected coronary artery disease: a systematic
review and meta-analysis.
J Am Coll Cardiol. 2013;62:826-838.
Litt HI, Gatsonis C, Snyder B, et al. CT angiography for safe discharge of patients with possible acute coronary syndromes.
N Engl J Med. 2012;366:1393-1403.
308
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers

Mahrholdt H, Wagner A, Parker M, et al. Relationship of contractile function to transmural extent of infarctionin patients with chronic coronary artery disease.
J Am Coll Cardiol. 2003;42:505-512.
Meijboom WB, van Mieghem CA, Mollet NR, et al. 64-slice computed tomography coronary angiography in patients withhigh, intermediate, or low pretest probability of significant coronary artery disease.
J Am Coll Cardiol. 2007;50:1469-1475.
Min JK, Berman DS, Dunning A, et al. All-cause mortality benefit of coronary revascularization vs. medicaltherapy in patients without known coronary artery disease under-going coronary computed tomographic angiography: results from CONFIRM (COronary CT Angiography EvaluatioN For Clinical Outcomes: An InteRnational Multicenter Registry).
Eur Heart J. 2012;33:3088-3097.
Min JK, Leipsic J, Pencina MJ, et al. Diagnostic accuracy of fractional flow reserve from anatomic CT angiography.
JAMA. 2012;308:1237-1245.
Mintz GS, Nissen SE, Anderson WD, et al. American College of Cardiology clinical expert consensus document on standards for acquisition, measurement and reporting of intravas-cular ultrasound studies (IVUS).
J Am Coll Cardiol. 2001;37:1478-1492.
Mollet NR, Dymarkowski S, Volders W, et al. Visualization of ventricular thrombi with contrast-enhanced magneticresonance imaging in patients with ischemic heart disease.
Circulation. 2002;106:2873-2876.
Montalescot G, Sechtem U, Achenbach S, et al. 2013 ESC guidelines on the management of stable coronary artery disease.
Eur Heart J. 2013;34:2949-3003.
Motwani M, Kidambi A, Greenwood JP, Plein S. Advances in cardiovascular magnetic resonance in ischaemic heart disease and non-ischaemic cardiomyopathies.
Heart. 2014;100:1722-1733.
Nahrendorf M, Sosnovik DE, French BA, et al. Multimodality cardiovascular molecular imaging, part II.
Circ Cardiovasc Imaging. 2009;2:56-70.
Narula J, Nakano M, Virmani R, et al. Histopathologic characteristics of atherosclerotic coronary disease and implications of the findings for the invasive and noninvasive detection of vulnerable plaques.
J Am Coll Cardiol. 2013;61:1041-1051.
NICE clinical guideline 95. Chest pain of recent onset: assessment and diagnosis of recent onset chest pain or discomfort of suspected cardiac origin.
www.nice.org.uk/guidance/CG95. Published March 2010. Accessed July 19, 2016.
Nielsen LH, Ortner N, Norgaard BL, Achenbach S, The diagnostic accuracy and outcomes after coronary computed Leipsic J, Abdulla J. tomography angiography vs. conventional functional testing in patients
with stable angina pectoris: a systematic review and meta-analysis.
Eur Heart J Cardiovasc Imaging. 2014;15:961-971.
Nissen SE, Yock P. Intravascular ultrasound: novel pathophysiological insights and current clinical applications.
Circulation. 2001;103:604-616.
309
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers

Norgaard BL, Leipsic J, Gaur S, et al; NXT Trial Diagnostic performance of noninvasive fractional flow reserve derivedStudy Group. from coronary computed tomography angiography in suspected
coronary artery disease: the NXT trial (Analysis of Coronary Blood Flow Using CT Angiography: Next Steps).
J Am Coll Cardiol. 2014;63:1145-1155.
Okwuosa TM, Greenland P, Burke GL, et al. Prediction of coronary artery calcium progression in individuals with low Framingham Risk Score: the Multi-Ethnic Study of Atherosclerosis.
JACC Cardiovasc Imaging. 2012;5:144-153.
Owens DS, Budoff MJ, Katz R, et al. Aortic valve calcium independently predicts coronary and cardio-vascular events in a primary prevention population.
JACC Cardiovasc Imaging. 2012;5:619-625.
Panting JR, Gatehouse PD, Yang GZ, et al. Abnormal subendocardial perfusion in cardiac syndrome X detected by cardiovascular magnetic resonance imaging.
N Engl J Med. 2002;346:1948-1953.
Park SJ, Kang SJ, Ahn JM, et al. Visual-functional mismatch between coronary angiography and fractional flow reserve.
JACC Cardiovasc Interv. 2012;5:1029-1036.
Patel AR, Antkowiak PF, Nandalur KR, et al. Assessment of advanced coronary artery disease: advantages of quantitative cardiac magnetic resonance perfusion analysis.
J Am Coll Cardiol. 2010;56:561-569.
Pazhenkottil AP, Nkoulou RN, Ghadri JR, et al. Prognostic value of cardiac hybrid imaging integrating single-photonemission computed tomography with coronary computed tomography angiography.
Eur Heart J. 2011;32:1465-1471.
Plein S, Ryf S, Schwitter J, Radjenovic A, Boesiger P, Dynamic contrast-enhanced myocardial perfusion MRI accelerated Kozerke S. with k-t sense.
Magn Reson Med. 2007;58:777-785.
Pletcher MJ, Tice JA, Pignone M, Browner WS. Using the coronary artery calcium score to predict coronary heart disease events: a systematic review and meta-analysis.
Arch Intern Med. 2004;164:1285-1292.
Porto I, Di Vito L, Burzotta F, et al. Predictors of periprocedural (type IVa) myocardial infarction, as assessed by frequency-domain optical coherence tomography.
Circ Cardiovasc Interv. 2012;5:89-96.
Prati F, Di Vito L, Biondi-Zoccai G, et al. Angiography alone versus angiography plus optical coherence tomography to guide decision-making during percutaneous coronaryintervention: the Centro per la Lotta contro l’Infarto-Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) study.
EuroIntervention. 2012;8:823-829.
Prati F, Kodama T, Romagnoli E, et al; Suboptimal stent deployment is associated with subacute stent CLI Foundation Investigators. thrombosis: optical coherence tomography insights from a multi-
center matched study: the CLI-THRO study.
Am Heart J. 2015;169:249-256.
Rees G, Bristow JD, Kremkau EL, et al. Influence of aortocoronary bypass surgery on left ventricular performance.
N Engl J Med. 1971;284:1116-1120.
310
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers

Romero J, Xue X, Gonzalez W, Garcia MJ. CMR imaging assessing viability in patients with chronic ventriculardysfunction due to coronary artery disease: a meta-analysis of prospective trials.
JACC Cardiovasc Imaging. 2012;5:494-508.
Rozanski A, Gransar H, Hayes SW, et al. Temporal trends in the frequency of inducible myocardial ischemia during cardiac stress testing: 1991 to 2009.
J Am Coll Cardiol. 2013;61:1054-1065.
Schinkel AF, Bax JJ, Poldermans D, Elhendy A, Hibernating myocardium: diagnosis and patient outcomes. Ferrari R, Rahimtoola SH. Curr Probl Cardiol. 2007;32:375-410.
Schwitter J, Wacker CM, Wilke N, et al; MR-IMPACT II: Magnetic Resonance Imaging for Myocardial MR-IMPACT Investigators. Perfusion Assessment in Coronary artery disease Trial: perfusion-
cardiac magnetic resonance vs. single-photon emission computed tomography for the detection of coronary artery disease: a compara-tive multicentre, multivendor trial.
Eur Heart J. 2013;34:775-781.
Shaw LJ, Berman DS, Picard MH, et al; Comparative definitions for moderate-severe ischemia in stress nuclear,NIH/NHLBI-Sponsored ISCHEMIA Trial Investigators. echocardiography, and magnetic resonance imaging.
JACC Cardiovasc Imaging. 2014;7:593-604.
Sianos G, Morel MA, Kappetein AP, et al. The SYNTAX Score: an angiographic tool grading the complexity of coronary artery disease.
EuroIntervention. 2005;1:219-227.
Silverman MG, Blaha MJ, Krumholz HM, et al. Impact of coronary artery calcium on coronary heart disease events in individuals at the extremes of traditional risk factor burden: the Multi-Ethnic Study of Atherosclerosis.
Eur Heart J. 2014;35:2232-2241.
Souteyrand G, Arbustini E, Motreff P, et al. Serial optical coherence tomography imaging of ACS-causing culprit plaques.
EuroIntervention. 2015;11:319-324.
Stone GW, Maehara A, Lansky AJ, et al; A prospective natural-history study of coronary atherosclerosis.PROSPECT Investigators. N Engl J Med. 2011;364:226-235.
Taqueti VR, Hachamovitch R, Murthy VL, et al. Global coronary flow reserve is associated with adverse cardiovas-cular events independently of luminal angiographic severity and modifies the effect of early revascularization.
Circulation. 2015;131:19-27.
Taylor AJ, Cerqueira M, Hodgson JM, et al. ACCF/SCCT/ACR/AHA/ASE/ASNC/NASCI/SCAI/SCMR 2010 appropriate use criteria for cardiac computed tomography.
Circulation. 2010;122:e525-e555.
Tearney GJ, Regar E, Akasaka T, et al; International Working Consensus standards for acquisition, measurement, and reporting Group for Intravascular Optical Coherence Tomography. of intravascular optical coherence tomography studies.
J Am Coll Cardiol. 2012;59:1058-1072.
Tonino PA, De Bruyne B, Pijls NH, et al; Fractional flow reserve versus angiography for guiding percutaneous FAME Study Investigators. coronary intervention.
N Engl J Med. 2009;360:213-224.
311
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers
Tornvall P, Gerbaud E, Behaghel A, et al. Myocarditis or “true” infarction by cardiac magnetic resonance in patients with a clinical diagnosis of myocardial infarction without obstructive coronary disease: a meta-analysis of individual patient data.
Atherosclerosis. 2015;241:87-91.
Underwood SR, de Bondt P, Flotats A, et al. The current and future status of nuclear cardiology: a consensus report.
Eur Heart J Cardiovasc Imaging. 2014;15:949-955.
Wagner A, Mahrholdt H, Holly TA, et al. Contrast-enhanced MRI and routine single photon emission computedtomography (SPECT) perfusion imaging for detection of subendo-cardial myocardial infarcts: an imaging study.
Lancet. 2003;361:374-379.
Wang TJ. Assessing the role of circulating, genetic, and imaging biomarkers in cardiovascular risk prediction.
Circulation. 2011;123:551-565.
Wei K, Jayaweera AR, Firoozan S, Linka A, Skyba DM, Basis for detection of stenosis using venous administration of Kaul S. microbubbles during myocardial contrast echocardiography: bolus
or continuous infusion?
J Am Coll Cardiol. 1998;32:252-260.
Weinsaft JW, Kim HW, Shah DJ, et al. Detection of left ventricular thrombus by delayed-enhancement cardio-vascular magnetic resonance prevalence and markers in patients with systolic dysfunction.
J Am Coll Cardiol. 2008;52:148-157.
Windecker S, Kolh P, Alfonso F, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization.
Eur Heart J. 2014;35:2541-2619.
Wolk MJ, Bailey SR, Doherty JU, et al; ACCF/AHA/ASE/ASNC/HFSA/HRS/SCAI/SCCT/SCMR/STS 2013 ACCF Appropriate Use Criteria Task Force. multimodality appropriate use criteria for the detection and risk
assessment of stable ischemic heart disease.
J Am Coll Cardiol. 2014;63:380-406.
Yonetsu T, Suh W, Abtahian F, et al. Comparison of near-infrared spectroscopy and optical coherence tomography for detection of lipid.
Catheter Cardiovasc Interv. 2014;84:710-717.
Zheng M, Wei M, Wen D, et al. Transluminal attenuation gradient in coronary computed tomog-raphy angiography for determining stenosis severity of calcified coronary artery: a primary study with dual-source CT.
Eur Radiol. 2015;25:1219-1228.
312
Dialogues in Cardiovascular Medicine - Vol 21 . No. 4 . 2016
Bibliography of One Hundred Key Papers