coronally advanced flap alone or with connective tissue graft in the treatment of single gingival...
TRANSCRIPT

Coronally Advanced Flap Alone or WithConnective Tissue Graft in the Treatmentof Single Gingival Recession Defects:A Long-Term Randomized Clinical TrialDavor Kuis,* Ivana Sciran,* Vlatka Lajnert,† Damir Snjaric,‡ Jelena Prpic,*Sonja Pezelj-Ribaric,* and Andrija Bosnjak*
Background: Numerous surgical approaches for the treat-ment of single gingival recession (GR) defects are docu-mented in the literature. The aim of this 5-year, splitmouth–design, randomized clinical trial was to evaluate theeffectiveness of coronally advanced flap (CAF) alone versusCAF with connective tissue graft (CAF+CTG) in the treat-ment of single Miller Class I and II GR defects.
Methods: Thirty-seven patients with 114 bilateral, singleMiller Class I and II GR defects were treated with CAF onone side of the mouth and CAF+CTG on the other side. Clin-ical measurements (GR length [REC], keratinized tissuewidth [KT], complete root coverage [CRC], and percentageof root coverage [PRC]) were evaluated before surgery andafter 6, 12, 24, and 60 months.
Results: There was a significant reduction of REC and in-crease of KT after surgery in both groups. CAF+CTG showedsignificantly better results for all evaluated clinical parame-ters in all observed follow-up periods. Miller Class I defectsshowed better results in terms of REC, CRC, and PRC,whereas Miller Class II showed better results in KT, both in fa-vor of CAF+CTG. Miller Class I defects showed better resultsthan Miller Class II GR defects regardless of the surgical pro-cedure used.
Conclusions: Both surgical procedures were effective inthe treatment of single Miller Class I and II GR defects. TheCAF+CTG procedure provided better long-term outcomes(60 months postoperatively) than CAF alone. Long-term sta-bility of the gingival margin is less predictable for Miller ClassII GR defects compared to those of Class I. J Periodontol2013;84:1576-1585.
KEY WORDS
Clinical trials, randomized; connective tissue; gingivalrecession; surgery, plastic; surgical flaps.
Numerous surgical approaches forthe treatment of single MillerClass I and II gingival recession
(GR) defects are documented in the lit-erature.1,2 One of the most reliabletechniques that results in the best long-term clinical outcome is the coronallyadvanced flap (CAF) procedure.3-8 Thisprocedure may be used alone or incombination with connective tissue graft(CTG), barrier membrane, enamel ma-trix derivative, acellular dermal matrix,or platelet-rich plasma.5
Several systematic reviews have triedto evaluate the effectiveness of differentsurgical approaches on root coverage,including randomized clinical trials(RCTs) on treatment of single MillerClass I and II GR defects with a follow-upperiod of at least 6 months.1,5,8-13
The Consensus Report of the SixthEuropean Workshop on Periodontologyaffirmed that CAF as a stand-aloneprocedure was a safe and predictableapproach for root coverage in singleMiller Class I and II GR defects.14 CTGand enamel matrix derivative in combi-nation with CAF as a stand-alone pro-cedure provided better results than CAFalone. Complete root coverage (CRC),GR reduction, and keratinized tissue gainwere compared among different com-binations of treatments, and the mosteffective combination was CAF+CTG
* Department of Oral Medicine and Periodontology, School of Dentistry, Faculty ofMedicine, University of Rijeka, Rijeka, Croatia.
† Department of Prosthodontics, School of Dentistry, Faculty of Medicine, University ofRijeka.
‡ Private practice, Rijeka, Croatia.
doi: 10.1902/jop.2013.120451
Volume 84 • Number 11
1576
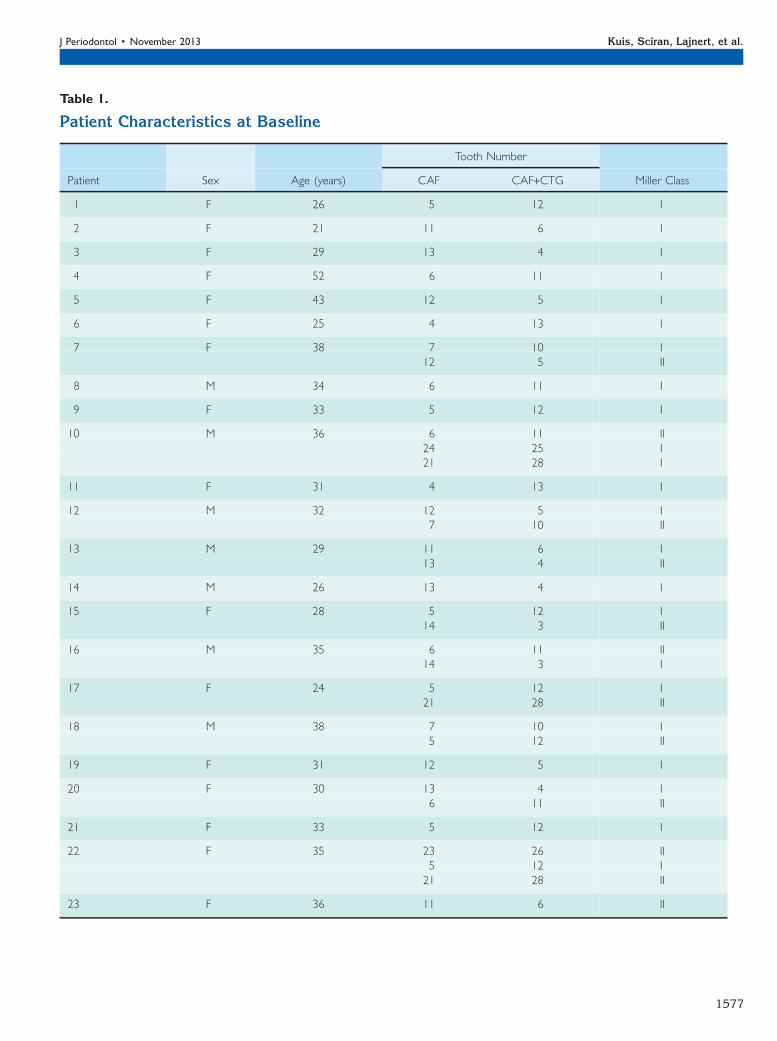
Table 1.
Patient Characteristics at Baseline
Tooth Number
Patient Sex Age (years) CAF CAF+CTG Miller Class
1 F 26 5 12 I
2 F 21 11 6 I
3 F 29 13 4 I
4 F 52 6 11 I
5 F 43 12 5 I
6 F 25 4 13 I
7 F 38 7 10 I12 5 II
8 M 34 6 11 I
9 F 33 5 12 I
10 M 36 6 11 II24 25 I21 28 I
11 F 31 4 13 I
12 M 32 12 5 I7 10 II
13 M 29 11 6 I13 4 II
14 M 26 13 4 I
15 F 28 5 12 I14 3 II
16 M 35 6 11 II14 3 I
17 F 24 5 12 I21 28 II
18 M 38 7 10 I5 12 II
19 F 31 12 5 I
20 F 30 13 4 I6 11 II
21 F 33 5 12 I
22 F 35 23 26 II5 12 I21 28 II
23 F 36 11 6 II
J Periodontol • November 2013 Kuis, Sciran, Lajnert, et al.
1577

(also known as bilaminar [subepithelial] techniquefor root coverage).5
According to the report,5 only two RCTs comparedCAF alone and in combination with CTG. The firstRCT from 2004 had a split-mouth design and includedonly 11 patients with bilateral single Miller Class I GRdefects (11 defects were treated with CAF and 11 withCAF+CTG); the follow-up period was 6 months.3 Thesecond RCT was a parallel-group, multicenter studythat included 85 patients with single Miller Class I andII GR defects (43 treated with CAF and 42 withCAF+CTG); the follow-up period was also 6 months.6
Both RCTs reported statistically significant differencesbetween groups in terms of keratinized tissue gain andCRC (both were greater in the CAF+CTG group).However, no statistically significant differences wereobserved in GR reduction. The consensus report5 alsoadvised that, to evaluate the stability of clinical out-comes of surgical procedures, long-term results withfollow-up periods of at least 5 years were needed.
The Cochrane systematic review from 2010,among other topics, underlined the importance of thefollow-up period.13 Only five of 24 RCTs that wereincluded in the review15-19 had a follow-up period of>12 months. Three of these RCTs17-19 reported thatthe amount of GR increased after 6 months. There-fore, long-term RCTs are necessary to adequatelyevaluate different root-coverage procedures.13
Interesting long-term results were presented ina study (although not an RCT) that analyzed multipleGR defects and also included Miller Class III defects,along with Miller Class I and II.20 The authors reportedan apical relapse of gingival margin in the CAF groupduring the 5-year follow-up. On the other hand,a coronal improvement of the gingival margin wasnoted in the CAF+CTG group.
Evidently, there is a lack of consistent long-termdata on single GR coverage and other clinical pa-rameters. The aim of this 5-year, split mouth–designRCT is to evaluate the effectiveness of CAF alone
Table 1. (continued)
Patient Characteristics at Baseline
Tooth Number
Patient Sex Age (years) CAF CAF+CTG Miller Class
24 M 26 13 4 II7 10 I
25 F 38 4 13 I
26 M 42 6 11 I14 3 II24 25 I22 27 I
27 F 45 5 12 II
28 F 47 12 5 I
29 F 20 6 11 II13 4 II
30 F 25 7 10 II13 4 II
31 F 25 4 13 II7 10 I
32 F 26 12 5 I
33 M 29 11 6 II
34 F 35 10 7 I
35 M 36 26 23 I20 29 I
36 F 33 6 11 II
37 M 30 3 14 II
CAF Versus CAF+CTG for Single Gingival Recession Defects Volume 84 • Number 11
1578

versus CAF+CTG in the treatment of single MillerClass I and II GR defects.
MATERIALS AND METHODS
PatientsThirty-seven patients (12 males and 25 females;aged 20 to 52 years, mean age: 31.14 years) areincluded in this study. The individuals were selectedfrom patients referred to the Dental Clinic, ClinicalHospital Center, Rijeka, Croatia, from March 2005 toOctober 2006. None of them ever smoked, all hadgood periodontal and overall health (ASA PhysicalClassification System, Class 1), and each had at leastone pair of bilateral single Miller Class I or II GRdefects. These bilaterally paired GR defects had tomeet the following criteria: (1) defects on the sametooth (left and right side of the jaw); (2) the same GRtype defect (Miller Class I or II); (3) an identifiablecemento-enamel junction (CEJ); and (4) no previousperiodontal surgery.
The majority of the patients (21) had only one pairof bilateral GR defects. Thirteen patients had twopairs, two patients had three pairs, and one patienthad four pairs of bilateral GR defects. Patients allcomplained about esthetics and/or hypersensitivity.GR depth of all 114 treated defects ranged from 1 to4 mm (2.65 – 0.73 mm).
Informed consent in written form (compiled in ac-cordance with the Helsinki Declaration) was obtainedfrom all the patients before the commencement of thestudy. Ethics Committees of the Clinical HospitalCenter, Rijeka, Croatia, and of the School of Medicine,University of Rijeka, Croatia, approved the consentform and experimental protocol at their respectivemeetings. Two different surgical procedures werecompared: CAF on one side of the mouth andCAF+CTG on the other side of the mouth of the samepatient. During the 5-year follow-up period, there wereno dropouts due to a careful follow-up routine andregular dental check-ups that were free of charge.
Clinical MeasurementsBefore the surgical procedures, bilateral single GRdefects were randomly assigned by coin toss to CAFor CAF+CTG. Clinical measurements were taken atbaseline and 6, 12, 24, and 60 months after thesurgical procedures by the same trained and cali-brated masked examiner (DK) using a periodontalprobe§ and a custom-made acrylic stent. The mea-surements included: 1) full-mouth plaque score(FMPS), the percentage of plaque-positive toothsurfaces, determined by the presence or absence ofplaque on four surfaces of each tooth; 2) full-mouthbleeding score (FMBS), the percentage of bleeding-positive tooth sites, calculated based on scores of0 (no bleeding) or 1 (bleeding) after probing for
probing depth (PD) on four sites per tooth; 3) PD, thedistance from gingival margin to the bottom of thegingival sulcus on mesio-, mid-, and disto-buccalsites of the treated tooth; 4) GR length (REC), thedistance from the CEJ to the gingival margin on themid-buccal site of the treated tooth; 5) keratinizedtissue width (KT), the distance from the mucogingivaljunction to the gingival margin on the mid-buccal siteof the treated tooth (no dye was used to identify themucogingival junction); and 6) clinical attachmentlevel (CAL), the distance from the CEJ to the bottomof the gingival sulcus on the mid-buccal site of thetreated tooth, calculated as PD + REC.
At 6, 12, 24, and 60 months post-surgery, REC andKT values were compared to those measured atbaseline for both surgical procedures. CRC was cal-culated as the percentage of teeth with complete rootcoverage, and percentage of root coverage (PRC) wascalculated according to the following formula:
PRC = RECbaseline �RECpostop
�RECbaseline
� ��100:
Initial TherapyAll patients received professional tooth cleaning andoral hygiene instructions 1 to 2 months before thesurgical procedures. To eliminate toothbrushinghabits that could be related to the etiology of the GRdefects, patients were instructed to use a soft manualtoothbrushi with small circular motion applyingminimal pressure.
Figure 1.Clinical photos of operated teeth at baseline and 5-year follow-up.A)GRdefect on tooth 6, baseline. B) 5 years after the CAF procedure ontooth 6. C) GR defect on tooth 11, baseline. D) 5 years after theCAF+CTG procedure on tooth 11.
§ PCP-UNC 15, Hu-Friedy, Rotterdam, The Netherlands.i CS 5490, Curaden, Kriens, Switzerland.
J Periodontol • November 2013 Kuis, Sciran, Lajnert, et al.
1579

Surgical ProceduresCAF procedure. After application of local anesthesia,an intrasulcular incision was made at the buccalaspect of the treated tooth and extended 3 mmhorizontally in the mesial and distal interdental gin-giva. Two oblique, divergent releasing incisions fol-lowed, extending beyond the mucogingival junction.A trapezoidal partial-thickness flap was raised be-yond the mucogingival junction to allow a passivecoronal displacement of the flap completely coveringthe CEJ. The adjacent papillae were de-epithelialized.A sling suture was placed to stabilize the flap in acoronal position, and interrupted sutures were placedon the releasing incisions using polypropylene5-0 sutures.¶
CAF+CTG procedure. The procedure was identicalto the CAF procedure with the addition of CTGharvested from the palate (premolar/molar area)using the trap-door approach. CTG was placed at theCEJ level and stabilized with mattress sutures. CTGwas completely covered by a previously raised flap inall cases.
All surgical procedures were performed by thesame operator (AB). After the surgical procedures,patients were requested to refrain from using thetoothbrush on treated sites for at least 2 weeks. A 1-minute rinse, 2 to 3 times a day for 2 weeks, with0.12% chlorhexidine digluconate# was prescribed.The sutures were removed from the palate wound(for CAF+CTG) after 7 days and from treated GRdefects after 14 days, when patients were allowed tocontinue with the oral hygiene routine as instructedearlier. The first control visit and professional cleaning(when needed) were performed 1 month after thesurgical procedure and subsequently in 6-monthintervals.
Statistical AnalysesStatistical analyses of data were performed usingsoftware programs.**,†† Power analysis indicatedthat with 26 GR defects in each group, the studywould have 80% power to detect a 0.5-mm differencein REC between the two groups. Descriptive statisticsare presented as means – SD for quantitative vari-ables (age, FMPS, FMBS, REC, KT, PRC) and per-centages for qualitative variables (CRC). To test thedifferences between the two groups (CAF andCAF+CTG), one-way analysis of variance (ANOVA)was used, and for post hoc analysis, the Tukey testwas used. To test the differences through time in eachgroup (CAF and CAF+CTG), repeated-measuresANOVA was used. For testing the differences among
Table
2.
REC
(mm)atBaselin
eand6,12,24,and60MonthsAftertheSurgicalProcedure
Miller
Class
IandII(n
=114)
Miller
Class
I(n
=68)
Miller
Class
II(n
=46)
Time(m
onths)
CAF(n
=57)
CAF+CTG
(n=57)
PCAF(n
=34)
CAF+CTG
(n=34)
PCAF(n
=23)
CAF+CTG
(n=23)
P
02.63–0.75
2.63–0.72
1.00
2.53–0.71
2.56–0.71
0.716
2.78–0.80
2.74–0.75
0.830
60.25–0.51
0.09–0.34
0.051
0.24–0.43
0.03–0.17
0.024*
0.26–0.63
0.17–0.49
0.507
12
0.28–0.49
0.09–0.34
0.021*
0.24–0.43
0.03–0.17
0.024*
0.35–0.57
0.17–0.49
0.161
24
0.35–0.52
0.12–0.38
0.005*
0.35–0.49
0.09–0.29
0.006*
0.35–0.57
0.17–0.49
0.161
60
0.46–0.60
0.19–0.44
0.001*
0.38–0.49
0.15–0.36
0.013*
0.57–0.73
0.26–0.54
0.047*
P†<0
.001*
<0.001*
<0.001*
<0.001*
<0.001*
<0.001*
Data
are
mea
n–SD.n=number
ofGRdefec
ts.
*Significa
ntdifference
(P<0
.05).
†REC
base
line(0
months)
versusthe5-yea
r(6
0months)
outcomewithin
trea
tmen
tgroups.
¶ Prolene 5-0, Ethicon, Somerville, MA.# Curasept ADS 212, Curaden.** Statistica 9.0, StatSoft, Tulsa, OK.†† MedCalc, Mariakerke, Belgium.
CAF Versus CAF+CTG for Single Gingival Recession Defects Volume 84 • Number 11
1580

‡3 matched sets of CRC frequencies, the Cochrane Qtest was used. All statistical values were consideredsignificant at the 0.05 level.
RESULTS
Patient characteristics at baseline are presented inTable 1. FMPS and FMBS at baseline were 17.90% –5.65% and 22.41% – 4.21%, respectively. These in-dices were significantly lower after 60 months(16.32% – 5.40% and 20.51% – 4.96%; P <0.05).Overall, REC was significantly reduced after 60months (2.63 – 0.73 versus 0.32 – 0.54 mm,P <0.001), as was CAL (3.79 – 0.77 versus 1.43 – 0.61mm, P <0.001). PD remained relatively unchanged(1.16 – 0.37 versus 1.11 – 0.31 mm, P = 0.241), asexpected.
Clinical photos of operated teeth at baseline andafter 5 years are presented in Figure 1. Baselinedefect-related characteristics (REC and KT) arepresented in the first row of Tables 2 and 3, re-spectively. There were no statistically significantdifferences between the two groups (CAF andCAF+CTG) in the amount of REC and KT at baseline.
After the surgical procedures, a statistically sig-nificant reduction of REC was observed comparedto baseline in both groups (Table 2). Statisticallybetter results were observed in the CAF+CTG groupafter 12 months, but this difference was not signifi-cant for 46 Miller Class II defects (23 treated withCAF and 23 treated with CAF+CTG).
The increase of KT after the surgical procedurewas observed in both groups (Table 3). A greaterincrease was observed in the CAF+CTG groupcompared to CAF alone in all observed follow-upperiods, but this difference was not significant for 68Miller Class I defects (34 treated with CAF and 34with CAF+CTG).
CRC ranged from 97.1% after 6 months for 34Miller Class I defects treated with CAF+CTG to 56.5%after 60 months for 23 Miller Class II defects treatedwith CAF (Table 4). Statistically higher percentageswere achieved and maintained in the CAF+CTGgroup, but surprisingly, not in 46 Miller Class II de-fects, where there was no significant difference inCRC between the two groups.
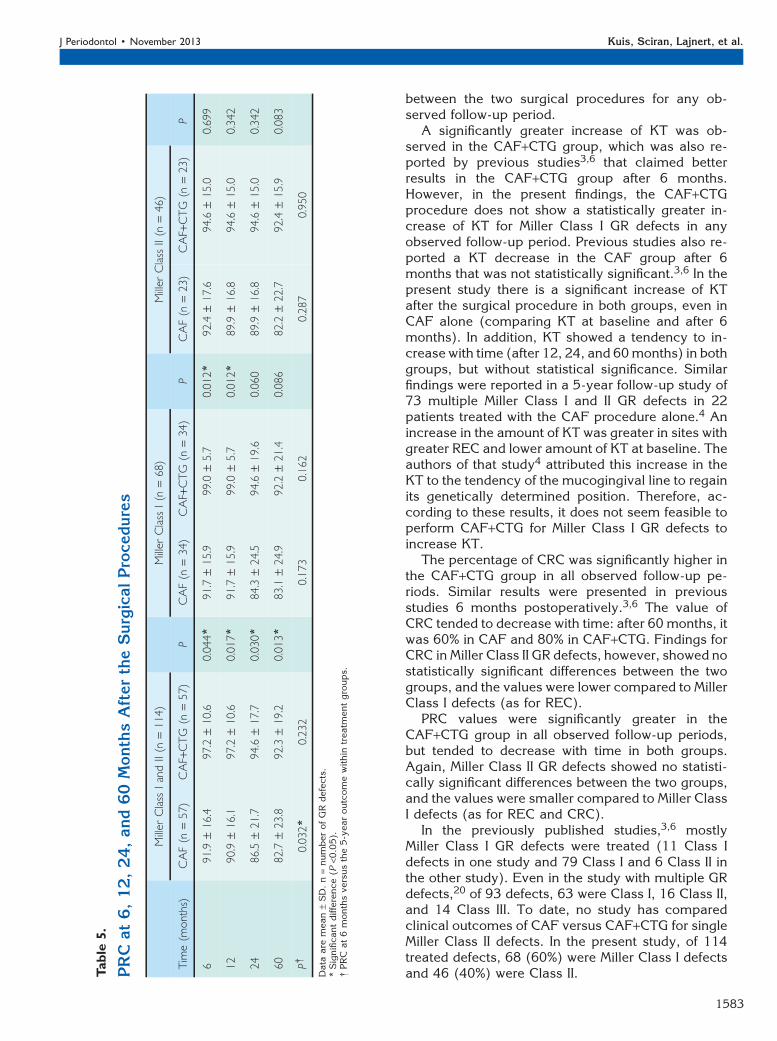
PRC varied from 99.0% after 6 months for MillerClass I defects treated with CAF+CTG to 82.2%after 60 months for 23 Miller Class II defectstreated with CAF (Table 5). A statistically signif-icant difference was demonstrated between thetwo groups in favor of CAF+CTG, but only whenall 114 defects (Miller Class I and II) were includedin the analysis. The difference was not significantfor Miller Class II defects in all observed follow-upperiods, and for Miller Class I defects after 12months.T
able
3.
KT(m
m)atBaselin
eand6,12,24,and60MonthsAftertheSurgicalProcedures
Miller
Class
IandII(n
=114)
Miller
Class
I(n
=68)
Miller
Class
II(n
=46)
Time(m
onths)
CAF(n
=57)
CAF+CTG
(n=57)
PCAF(n
=34)
CAF+CTG
(n=34)
PCAF(n
=23)
CAF+CTG
(n=23)
P
01.33–1.19
1.33–1.17
1.00
2.24–0.55
2.23–0.49
0.934
00
1.00
62.09–0.71
2.46–0.60
0.003*
2.44–0.61
2.62–0.60
0.166
1.57–0.51
2.21–0.52
<0.001*
12
2.21–0.75
2.58–0.60
0.004*
2.50–0.66
2.62–0.55
0.354
1.78–0.67
2.52–0.66
<0.001*
24
2.21–0.75
2.63–0.62
0.001*
2.50–0.66
2.65–0.60
0.247
1.78–0.67
2.61–0.66
<0.001*
60
2.25–0.76
2.70–0.60
<0.001*
2.53–0.66
2.71–0.58
0.166
1.83–0.72
2.70–0.63
<0.001*
P†<0
.001*
<0.001*
0.307
0.006*
<0.001*
<0.001*
Data
are
mea
n–SD.n=number
ofGRdefec
ts.
*Significa
ntdifference
(P<0
.05).
†KTbase
line(0
months)
versusthe5-yea
r(6
0months)
outcomewithin
trea
tmen
tgroups.
J Periodontol • November 2013 Kuis, Sciran, Lajnert, et al.
1581
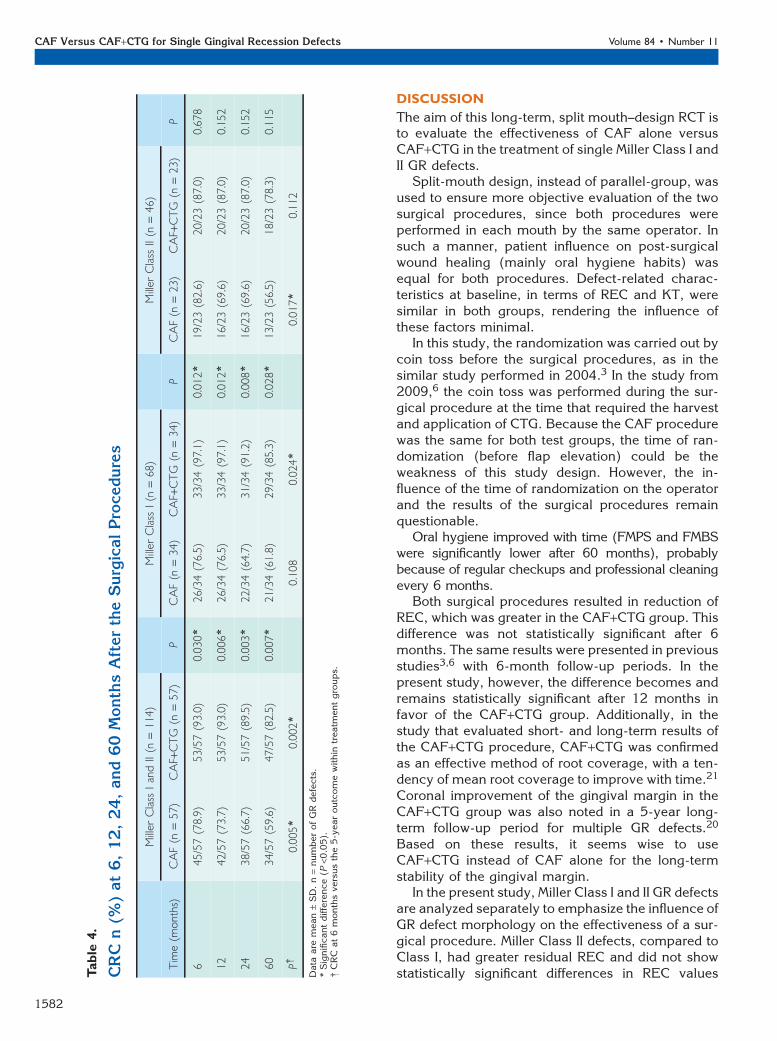
DISCUSSION
The aim of this long-term, split mouth–design RCT isto evaluate the effectiveness of CAF alone versusCAF+CTG in the treatment of single Miller Class I andII GR defects.
Split-mouth design, instead of parallel-group, wasused to ensure more objective evaluation of the twosurgical procedures, since both procedures wereperformed in each mouth by the same operator. Insuch a manner, patient influence on post-surgicalwound healing (mainly oral hygiene habits) wasequal for both procedures. Defect-related charac-teristics at baseline, in terms of REC and KT, weresimilar in both groups, rendering the influence ofthese factors minimal.
In this study, the randomization was carried out bycoin toss before the surgical procedures, as in thesimilar study performed in 2004.3 In the study from2009,6 the coin toss was performed during the sur-gical procedure at the time that required the harvestand application of CTG. Because the CAF procedurewas the same for both test groups, the time of ran-domization (before flap elevation) could be theweakness of this study design. However, the in-fluence of the time of randomization on the operatorand the results of the surgical procedures remainquestionable.
Oral hygiene improved with time (FMPS and FMBSwere significantly lower after 60 months), probablybecause of regular checkups and professional cleaningevery 6 months.
Both surgical procedures resulted in reduction ofREC, which was greater in the CAF+CTG group. Thisdifference was not statistically significant after 6months. The same results were presented in previousstudies3,6 with 6-month follow-up periods. In thepresent study, however, the difference becomes andremains statistically significant after 12 months infavor of the CAF+CTG group. Additionally, in thestudy that evaluated short- and long-term results ofthe CAF+CTG procedure, CAF+CTG was confirmedas an effective method of root coverage, with a ten-dency of mean root coverage to improve with time.21
Coronal improvement of the gingival margin in theCAF+CTG group was also noted in a 5-year long-term follow-up period for multiple GR defects.20
Based on these results, it seems wise to useCAF+CTG instead of CAF alone for the long-termstability of the gingival margin.
In the present study, Miller Class I and II GR defectsare analyzed separately to emphasize the influence ofGR defect morphology on the effectiveness of a sur-gical procedure. Miller Class II defects, compared toClass I, had greater residual REC and did not showstatistically significant differences in REC valuesT
able
4.
CRC
n(%
)at6,12,24,and60MonthsAftertheSurgicalProcedures
Miller
Class
IandII(n
=114)
Miller
Class
I(n
=68)
Miller
Class
II(n
=46)
Time(m
onths)
CAF(n
=57)
CAF+CTG
(n=57)
PCAF(n
=34)
CAF+CTG
(n=34)
PCAF(n
=23)
CAF+CTG
(n=23)
P
645/57(78.9)
53/57(93.0)
0.030*
26/34(76.5)
33/34(97.1)
0.012*
19/23(82.6)
20/23(87.0)
0.678
12
42/57(73.7)
53/57(93.0)
0.006*
26/34(76.5)
33/34(97.1)
0.012*
16/23(69.6)
20/23(87.0)
0.152
24
38/57(66.7)
51/57(89.5)
0.003*
22/34(64.7)
31/34(91.2)
0.008*
16/23(69.6)
20/23(87.0)
0.152
60
34/57(59.6)
47/57(82.5)
0.007*
21/34(61.8)
29/34(85.3)
0.028*
13/23(56.5)
18/23(78.3)
0.115
P†0.005*
0.002*
0.108
0.024*
0.017*
0.112
Data
are
mea
n–SD.n=number
ofGRdefec
ts.
*Significa
ntdifference
(P<0
.05).
†CRC
at6monthsve
rsusthe5-yea
routcomewithin
trea
tmen
tgroups.
CAF Versus CAF+CTG for Single Gingival Recession Defects Volume 84 • Number 11
1582
between the two surgical procedures for any ob-served follow-up period.
A significantly greater increase of KT was ob-served in the CAF+CTG group, which was also re-ported by previous studies3,6 that claimed betterresults in the CAF+CTG group after 6 months.However, in the present findings, the CAF+CTGprocedure does not show a statistically greater in-crease of KT for Miller Class I GR defects in anyobserved follow-up period. Previous studies also re-ported a KT decrease in the CAF group after 6months that was not statistically significant.3,6 In thepresent study there is a significant increase of KTafter the surgical procedure in both groups, even inCAF alone (comparing KT at baseline and after 6months). In addition, KT showed a tendency to in-crease with time (after 12, 24, and 60months) in bothgroups, but without statistical significance. Similarfindings were reported in a 5-year follow-up study of73 multiple Miller Class I and II GR defects in 22patients treated with the CAF procedure alone.4 Anincrease in the amount of KT was greater in sites withgreater REC and lower amount of KT at baseline. Theauthors of that study4 attributed this increase in theKT to the tendency of the mucogingival line to regainits genetically determined position. Therefore, ac-cording to these results, it does not seem feasible toperform CAF+CTG for Miller Class I GR defects toincrease KT.
The percentage of CRC was significantly higher inthe CAF+CTG group in all observed follow-up pe-riods. Similar results were presented in previousstudies 6 months postoperatively.3,6 The value ofCRC tended to decrease with time: after 60 months, itwas 60% in CAF and 80% in CAF+CTG. Findings forCRC in Miller Class II GR defects, however, showed nostatistically significant differences between the twogroups, and the values were lower compared to MillerClass I defects (as for REC).
PRC values were significantly greater in theCAF+CTG group in all observed follow-up periods,but tended to decrease with time in both groups.Again, Miller Class II GR defects showed no statisti-cally significant differences between the two groups,and the values were smaller compared to Miller ClassI defects (as for REC and CRC).
In the previously published studies,3,6 mostlyMiller Class I GR defects were treated (11 Class Idefects in one study and 79 Class I and 6 Class II inthe other study). Even in the study with multiple GRdefects,20 of 93 defects, 63 were Class I, 16 Class II,and 14 Class III. To date, no study has comparedclinical outcomes of CAF versus CAF+CTG for singleMiller Class II defects. In the present study, of 114treated defects, 68 (60%) were Miller Class I defectsand 46 (40%) were Class II.T
able
5.
PRC
at6,12,24,and60MonthsAftertheSurgicalProcedures
Miller
Class
IandII(n
=114)
Miller
Class
I(n
=68)
Miller
Class
II(n
=46)
Time(m
onths)
CAF(n
=57)
CAF+CTG
(n=57)
PCAF(n
=34)
CAF+CTG
(n=34)
PCAF(n
=23)
CAF+CTG
(n=23)
P
691.9
–16.4
97.2
–10.6
0.044*
91.7
–15.9
99.0
–5.7
0.012*
92.4
–17.6
94.6
–15.0
0.699
12
90.9
–16.1
97.2
–10.6
0.017*
91.7
–15.9
99.0
–5.7
0.012*
89.9
–16.8
94.6
–15.0
0.342
24
86.5
–21.7
94.6
–17.7
0.030*
84.3
–24.5
94.6
–19.6
0.060
89.9
–16.8
94.6
–15.0
0.342
60
82.7
–23.8
92.3
–19.2
0.013*
83.1
–24.9
92.2
–21.4
0.086
82.2
–22.7
92.4
–15.9
0.083
P†0.032*
0.232
0.173
0.162
0.287
0.950
Data
are
mea
n–SD.n=number
ofGRdefec
ts.
*Significa
ntdifference
(P<0
.05).
†PRC
at6monthsve
rsusthe5-yea
routcomewithin
trea
tmen
tgroups.
J Periodontol • November 2013 Kuis, Sciran, Lajnert, et al.
1583

Evaluation of the effectiveness of CAF andCAF+CTG for surgical treatment of Miller Class Iand Class II defects showed that in Miller Class IIdefects, the CAF+CTG procedure provides signifi-cantly better results only for KT values, but the samecould not be applied to REC, CRC, and PRC values inall observed follow-up periods. In contrast, in MillerClass I defects, the CAF+CTG procedure providedsignificantly better results for REC, CRC, and PRCvalues, but not for KT, in all observed follow-upperiods. It seems that baseline KT is a predictor forGR reduction in the CAF technique, where there is noincrease of flap thickness by means of CTG.22
Comparing the clinical outcomes between MillerClass I and Class II defects (regardless of the surgicalprocedure), Miller Class II defects showed poorerresults (greater REC and smaller KT, CRC, and PRC)in comparison to Miller Class I defects.
Back in 1985, Miller stated that 100% root cov-erage could be expected for both Class I and Class IIGR defects following the grafting procedure (theprocedure used at that time was free gingival graft).2
This could be why Miller Class I and II defects werenever separated in clinical trials; they are alwaysanalyzed together, even currently. In addition, datafrom reports on the treatment of Miller Class I and IIdefects show that it is not possible to achieve 100%root coverage regardless of the surgical procedureused (free gingival graft, CAF as a stand-aloneprocedure, or CAF in combination with other pro-cedures).23
Comparing this study’s clinical outcomes betweenMiller Class I and Class II defects, Miller Class II de-fects showed poorer results (greater REC and smallerKT, CRC, and PRC) in comparison to Miller Class Idefects. A similar conclusion was presented in thestudy that analyzed long-term results of CTG in theenvelope technique.24 The authors of that studystated that higher baseline Miller class results in lessfavorable prognoses for CRC and PRC. Consideringthe clinical outcomes of different surgical proceduresand separate analysis of Miller Class I and II defects,one may conclude that Miller Class II defects are lesspredictable than Class I in terms of gingival marginstability with time, regardless of the surgical pro-cedure used.
CONCLUSIONS
Both surgical procedures (CAF and CAF+CTG) areeffective in the treatment of single Miller Class I and IIGR defects, since both resulted in reduction of RECand increase of KT. CAF+CTG provided a better long-term clinical outcome than CAF alone; this is cor-roborated by all evaluated clinical parameters in allobserved follow-up periods. Single Miller Class I GRdefects showed better results in terms of REC, CRC,
and PRC, whereas Class II showed better results inKT, both in favor of CAF+CTG. Single Miller Class IGR defects showed better results than Class II forall evaluated clinical parameters in all observed fol-low-up periods. Long-term stability of the gingivalmargin is less predictable for single Miller Class IIGR defects than for Class I.
ACKNOWLEDGMENTS
The authors thank Assoc. Prof. Gordana Bruminifrom Department of Medical Informatics, Faculty ofMedicine, University of Rijeka, Croatia, for the statis-tical analysis and Drs. Sanja Mihalj�ci�c, Ivan Pulji�c,and Nejc Sok (all former students now in private den-tal practices) for help in the data collection. Thisstudy was prepared as a part of Ministry of Science,Education and Sports (Zagreb, Croatia) Grant No.062-06504450-0440. The authors report no conflictsof interest related to this study.
REFERENCES1. Oates TW, Robinson M, Gunsolley JC. Surgical thera-
pies for the treatment of gingival recession. A system-atic review. Ann Periodontol 2003;8:303-320.
2. Miller PD Jr. A classification of marginal tissue re-cession. Int J Periodontics Restorative Dent 1985;5:8-13.
3. da Silva RC, Joly JC, de Lima AF, Tatakis DN. Rootcoverage using the coronally positioned flap with orwithout a subepithelial connective tissue graft. J Peri-odontol 2004;75:413-419.
4. Zucchelli G, De Sanctis M. Long-term outcome follow-ing treatment of multiple Miller class I and II recessiondefects in esthetic areas of the mouth. J Periodontol2005;76:2286-2292.
5. Cairo F, Pagliaro U, Nieri M. Treatment of gingivalrecession with coronally advanced flap procedures: Asystematic review. J Clin Periodontol 2008; 35(Suppl.8)136-162.
6. Cortellini P, Tonetti M, Baldi C, et al. Does placement ofa connective tissue graft improve the outcomes ofcoronally advanced flap for coverage of single gingivalrecessions in upper anterior teeth? A multi-centre,randomized, double-blind, clinical trial. J Clin Peri-odontol 2009;36:68-79.
7. Pini-Prato GP, Rotundo R, Franceschi D, Cairo F,Cortellini P, Nieri M. Fourteen-year outcomes of coro-nally advanced flap for root coverage: Follow-up froma randomized trial. J Clin Periodontol 2011;38:715-720.
8. Cortellini P, Pini Prato G. Coronally advanced flap andcombination therapy for root coverage. Clinical strat-egies based on scientific evidence and clinical experi-ence. Periodontol 2000 2012;59:158-184.
9. Bouchard P, Malet J, Borghetti A. Decision-making inaesthetics: Root coverage revisited. Periodontol 20002001;27:97-120.
10. Roccuzzo M, Bunino M, Needleman I, Sanz M. Peri-odontal plastic surgery for treatment of localizedgingival recessions: A systematic review. J Clin Peri-odontol 2002;29 (Suppl. 3):178-194, discussion 195-196.
CAF Versus CAF+CTG for Single Gingival Recession Defects Volume 84 • Number 11
1584

11. Pagliaro U, Nieri M, Franceschi D, Clauser C, Pini-PratoG. Evidence-based mucogingival therapy. Part 1: Acritical review of the literature on root coverage pro-cedures. J Periodontol 2003;74:709-740.
12. Clauser C, Nieri M, Franceschi D, Pagliaro U, Pini-PratoG. Evidence-based mucogingival therapy. Part 2:Ordinary and individual patient data meta-analyses ofsurgical treatment of recession using complete rootcoverage as the outcome variable. J Periodontol 2003;74:741-756.
13. Chambrone L, Sukekava F, Araujo MG, Pustiglioni FE,Chambrone LA, Lima LA. Root-coverage proceduresfor the treatment of localized recession-type defects: ACochrane systematic review. J Periodontol 2010;81:452-478.
14. Palmer RM, Cortellini P; Group B of European Work-shop on Periodontology. Periodontal tissue engineeringand regeneration: Consensus Report of the SixthEuropean Workshop on Periodontology. J Clin Peri-odontol 2008; 35(Suppl. 8)83-86.
15. Paolantonio M, di Murro C, Cattabriga A, Cattabriga M.Subpedicle connective tissue graft versus free gingivalgraft in the coverage of exposed root surfaces. A 5-yearclinical study. J Clin Periodontol 1997;24:51-56.
16. Rosetti EP, Marcantonio RA, Rossa C Jr., Chaves ES,Goissis G, Marcantonio E Jr. Treatment of gingivalrecession: Comparative study between subepithelialconnective tissue graft and guided tissue regeneration.J Periodontol 2000;71:1441-1447.
17. Del Pizzo M, Zucchelli G, Modica F, Villa R, DebernardiC. Coronally advanced flap with or without enamelmatrix derivative for root coverage: A 2-year study.J Clin Periodontol 2005;32:1181-1187.
18. Spahr A, Haegewald S, Tsoulfidou F, et al. Coverage ofMiller class I and II recession defects using enamelmatrix proteins versus coronally advanced flap tech-
nique: A 2-year report. J Periodontol 2005;76:1871-1880.
19. de Queiroz Cortes A, Sallum AW, Casati MZ, Nociti FHJr., Sallum EA. A two-year prospective study ofcoronally positioned flap with or without acellulardermal matrix graft. J Clin Periodontol 2006;33:683-689.
20. Pini-Prato GP, Cairo F, Nieri M, Franceschi D, RotundoR, Cortellini P. Coronally advanced flap versus connec-tive tissue graft in the treatment of multiple gingivalrecessions: A split-mouth study with a 5-year follow-up. J Clin Periodontol 2010;37:644-650.
21. Harris RJ. Root coverage with connective tissue grafts:An evaluation of short- and long-term results. J Peri-odontol 2002;73:1054-1059.
22. Pini-Prato GP, Franceschi D, Rotundo R, Cairo F,Cortellini P, Nieri M. Long-term 8-year outcomes ofcoronally advanced flap for root coverage. J Periodon-tol 2012;83:590-594.
23. Pini-Prato GP. The Miller classification of gingival re-cession: Limits and drawbacks. J Clin Periodontol2011;38:243-245.
24. Rossberg M, Eickholz P, Raetzke P, Ratka-Kruger P.Long-term results of root coverage with connectivetissue in the envelope technique: A report of 20cases. Int J Periodontics Restorative Dent 2008;28:19-27.
Correspondence: Dr. Davor Kuis, Department of OralMedicine and Periodontology, School of Dentistry, Facultyof Medicine, University of Rijeka, Brace Branchetta 20,51000 Rijeka, Croatia. Fax: + 385-51-345630; e-mail:[email protected].
Submitted July 19, 2012; accepted for publicationNovember 21, 2012.
J Periodontol • November 2013 Kuis, Sciran, Lajnert, et al.
1585