coreicd - rhythm basics - wikispacesmedicineg.wikispaces.com/file/view/ecg and ryythm...
TRANSCRIPT


Rhythm Disorders
Dr. Maged M. El Samady
MBBCh, MSc, MRCPCH, FRCP(UK)

Overview
• The Conduction System
• Rhythm Disorders:
Bradyarrhythmia
Tachyarrhythmia

THE CONDUCTION SYSTEM
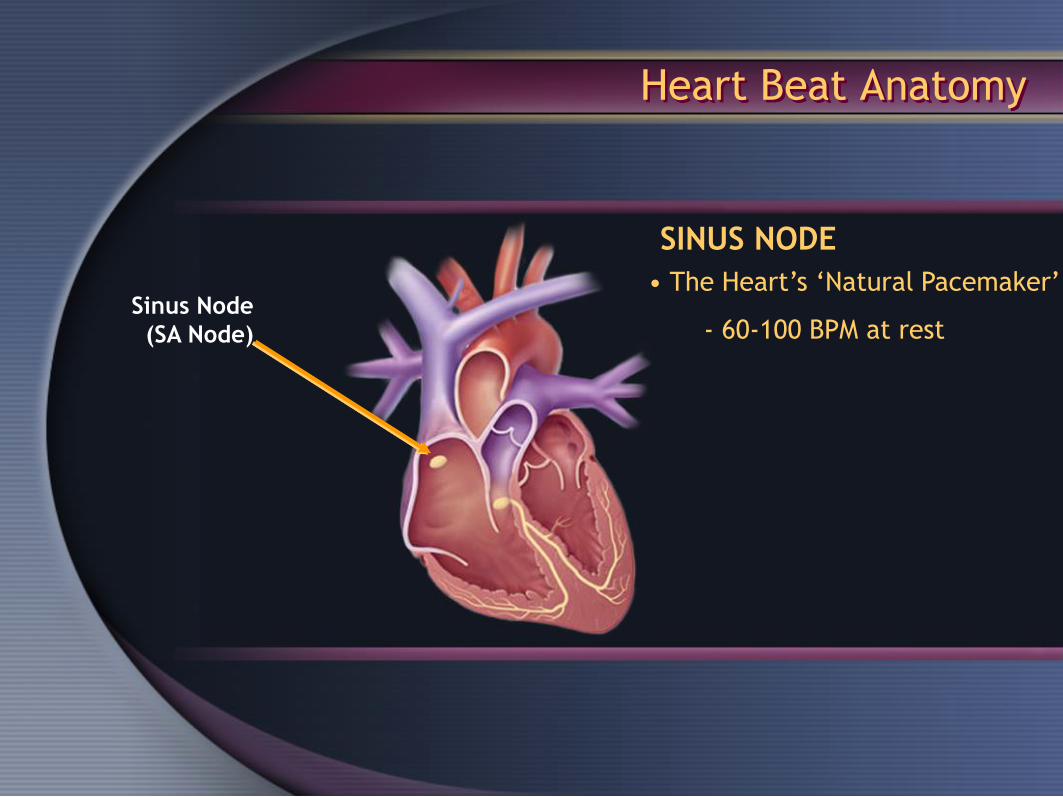
Heart Beat Anatomy
Sinus Node
(SA Node)
• The Heart’s ‘Natural Pacemaker’
- 60-100 BPM at rest
SINUS NODE

Heart Beat Anatomy
AV NODE
Sinus Node
(SA Node)
Atrioventricular
Node (AV Node)
• Receives impulse from
SA Node
• Delivers impulse to the His-
Purkinje System
• 40-60 BPM if SA Node fails to
deliver an impulse

Heart Beat Anatomy
BUNDLE OF HIS
Sinus Node
(SA Node)
Atrioventricular
Node (AV Node)
Bundle of His
• Begins conduction to
the Ventricles
• AV Junctional Tissue:
40-60 BPM

Heart Beat Anatomy
Atrioventricular
Node (AV Node)
Sinus Node
(SA Node)
Bundle of His
Bundle Branches
Purkinje Fibers
• Bundle Branches
• Purkinje Fibers
• Moves the impulse through
the ventricles for contraction
• Provides ‘Escape Rhythm’:
20-40 BPM
THE PURKINJE NETWORK

Normal Sinus Rhythm
Click heart to
view animation
*Animation

Impulse Formation In SA Node

Atrial Depolarization

Delay At AV Node
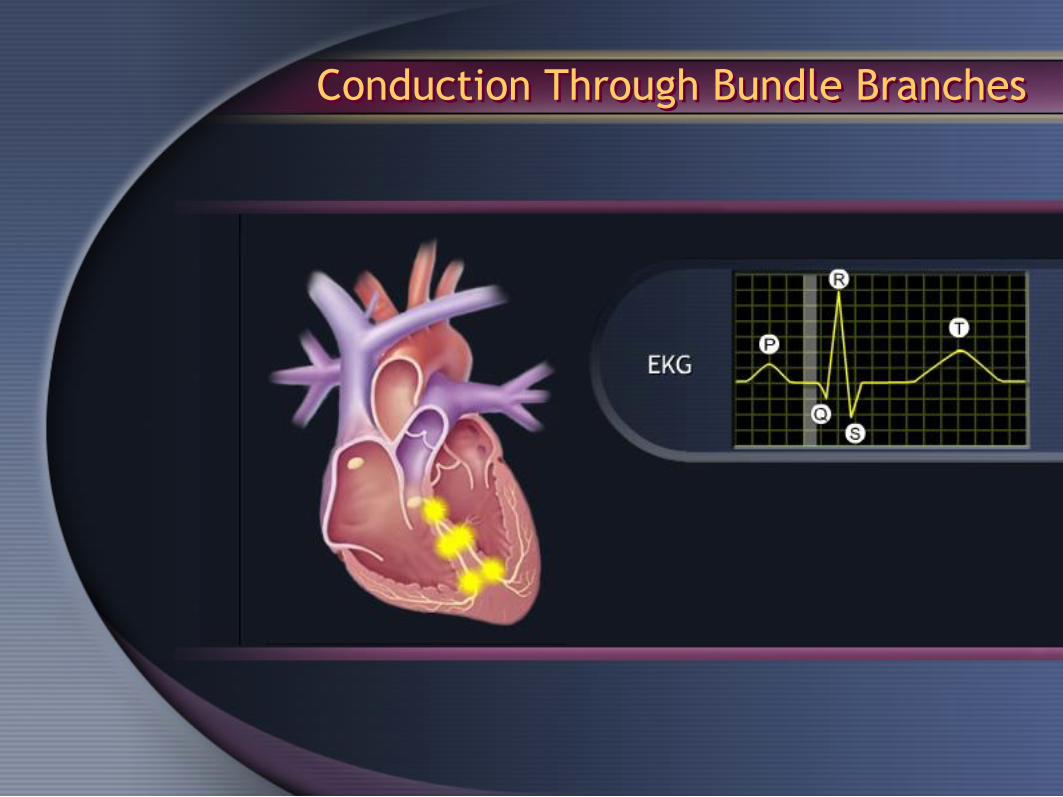
Conduction Through Bundle Branches

Conduction Through Purkinje Fibers

Ventricular Depolarization

Plateau Phase of Repolarization

Final Rapid (Phase 3) Repolarization

Normal ECG Activation
Automaticity
Cardiac Cells have
AUTOMATICITY!

Automaticity
• Spontaneously depolarize
• Generally present in:
Cardiac Cells
• Upper (SA Node)
- 60-100 BPM
• Middle (AV Junction)
- 40-60 BPM
• Lower (Purkinje Network)
- 20–40 BPM

Automaticity
Once a pacemaker cell initiates an impulse,
its neighboring cells follow suit – like dominos!


STANDARD SURFACE 12
LEADS ECG

ECG LIMB LEADS
3 BIPOLAR LEADS:
I, II and III
3 UNIPOLAR LEADS:
aVR, aVL and aVF

LIMB LEADS I, II & III

LIMB LEADS aVR, aVL & aVF
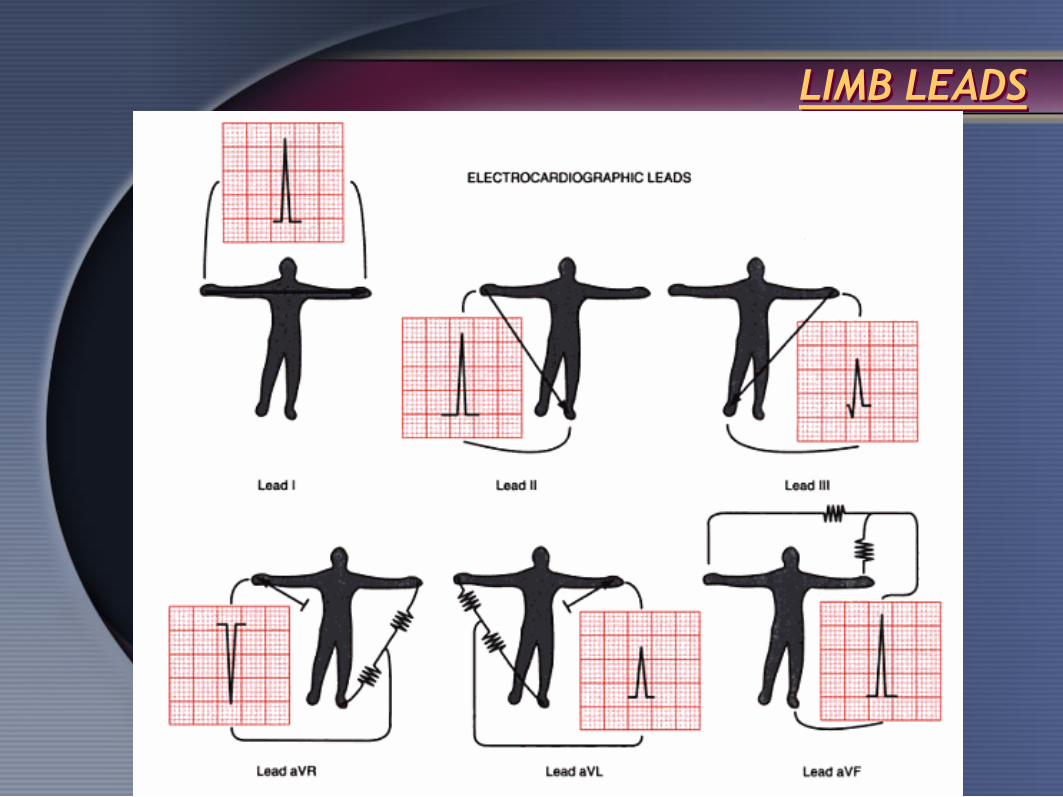
LIMB LEADS

LIMB LEADS
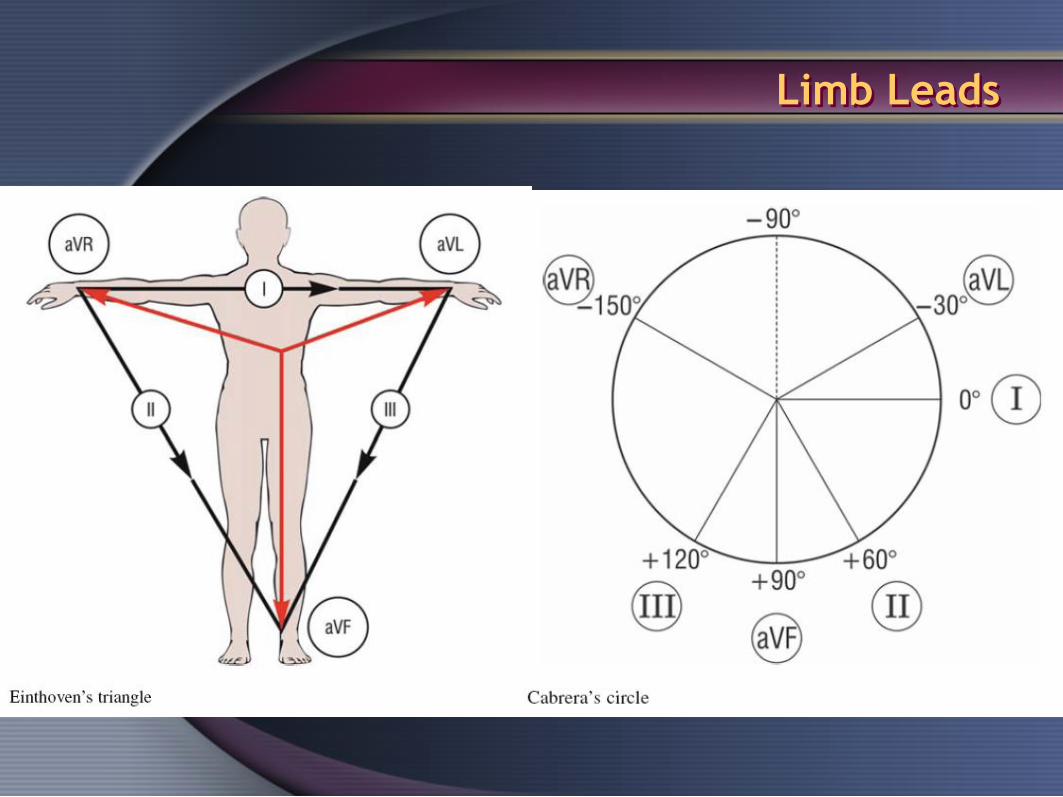
Limb Leads


CHEST LEADS
V1: Rt. 4th space
V2: Lt. 4th space
V3: In-between
V2&V4
V4: At apex
V5: Ant. Axillary line
V6: Mid. Axillary line
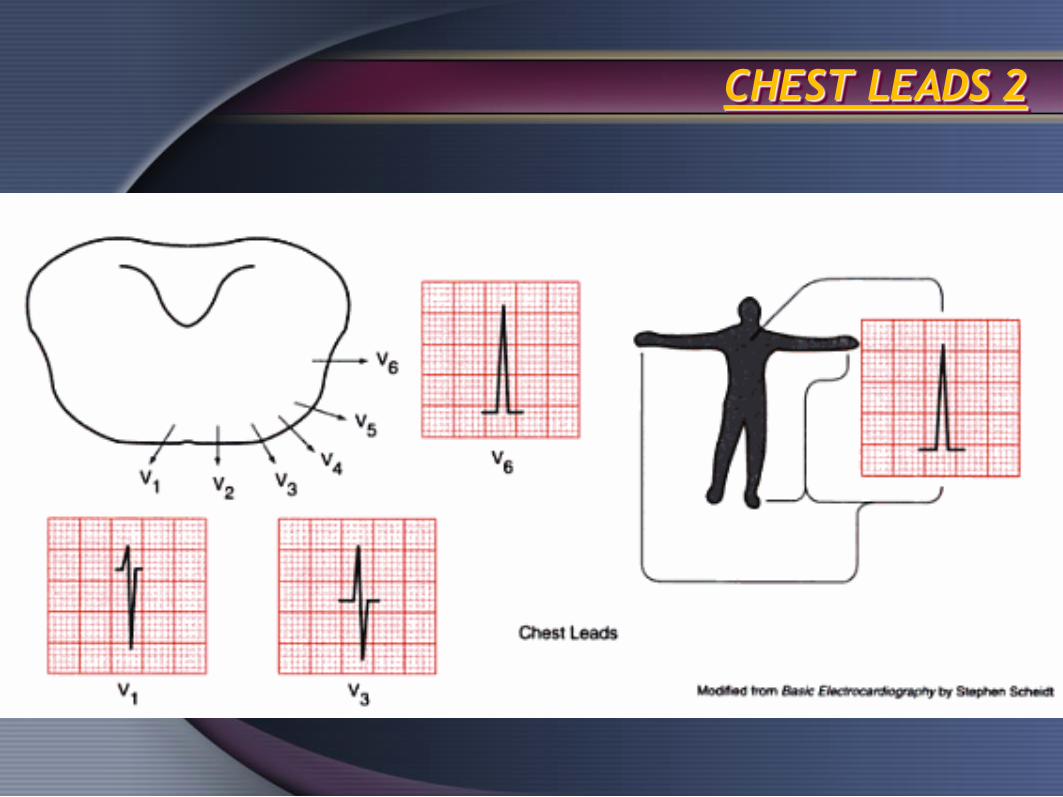
CHEST LEADS 2


ECG WAVES& INTERVALS

Reading ECGs
Normal Ranges in Milliseconds:
• PR Interval 120 – 200 ms
• QRS Complex 60 – 100 ms
• QT Interval 360 – 440 ms
Intervals and Timing

Developmental Changes in the ECG
• Gradual decrease in heart rate
• Gradual lengthening of the PR interval
• Gradual lengthening of the QRS
interval
• Shift from right to left ventricular
dominance

Rate and Intervals Based on Age
Adapted from: Benson, D.W. (1989 (

Reading ECG Squares
• Each square = 40 ms
• Each interval = 200 ms
Intervals and Timing

ECG INTERPRETATION
RATE
RHYTHM
AXIS
CHAMBERS HYPERTROPHY
S-T & T WAVE CHANGES

Question?
How do we measure heart rate?
BPM(Beats Per Minute)

Calculate Rate
• Option 1
– Count the # of R waves in a 6 second
rhythm strip, then multiply by 10.
– Reminder: all rhythm strips in the Modules
are 6 seconds in length.
Interpretation? 9 x 10 = 90 bpm
3 sec 3 sec

Calculate Rate
• Option 2
– Find a R wave that lands on a bold line.
– Count the # of large boxes to the next R
wave. If the second R wave is 1 large box
away the rate is 300, 2 boxes - 150, 3
boxes - 100, 4 boxes - 75, etc.
R wave
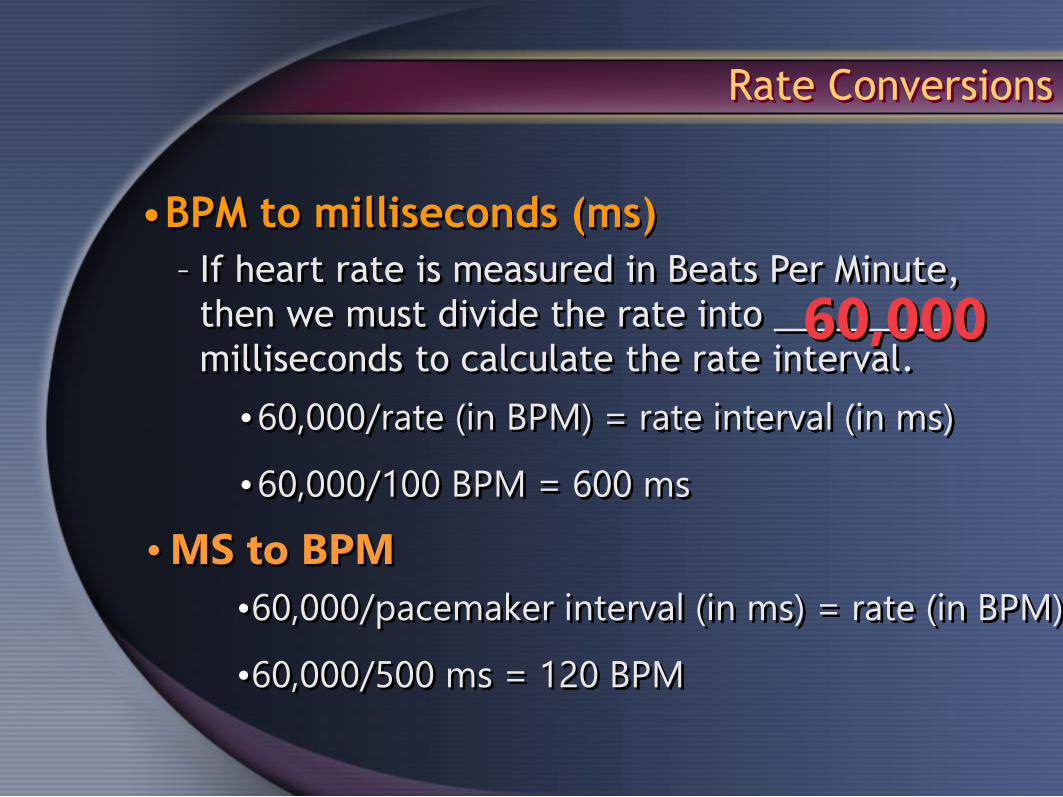
•BPM to milliseconds (ms)
– If heart rate is measured in Beats Per Minute,
then we must divide the rate into _________
milliseconds to calculate the rate interval.
•60,000/rate (in BPM) = rate interval (in ms)
•60,000/100 BPM = 600 ms
60,000
•60,000/pacemaker interval (in ms) = rate (in BPM)
•60,000/500 ms = 120 BPM
•MS to BPM
Rate Conversions

Rate Conversions
How fast is this rhythm?
Milliseconds = ? 830 BPM = ? 72
60,000 / 830 = 72

Rate Conversions
How fast is this rhythm?
Milliseconds = ? 400 BPM = ? 150
60,000 / 400 = 150

Normal ECG for 1 day old infant
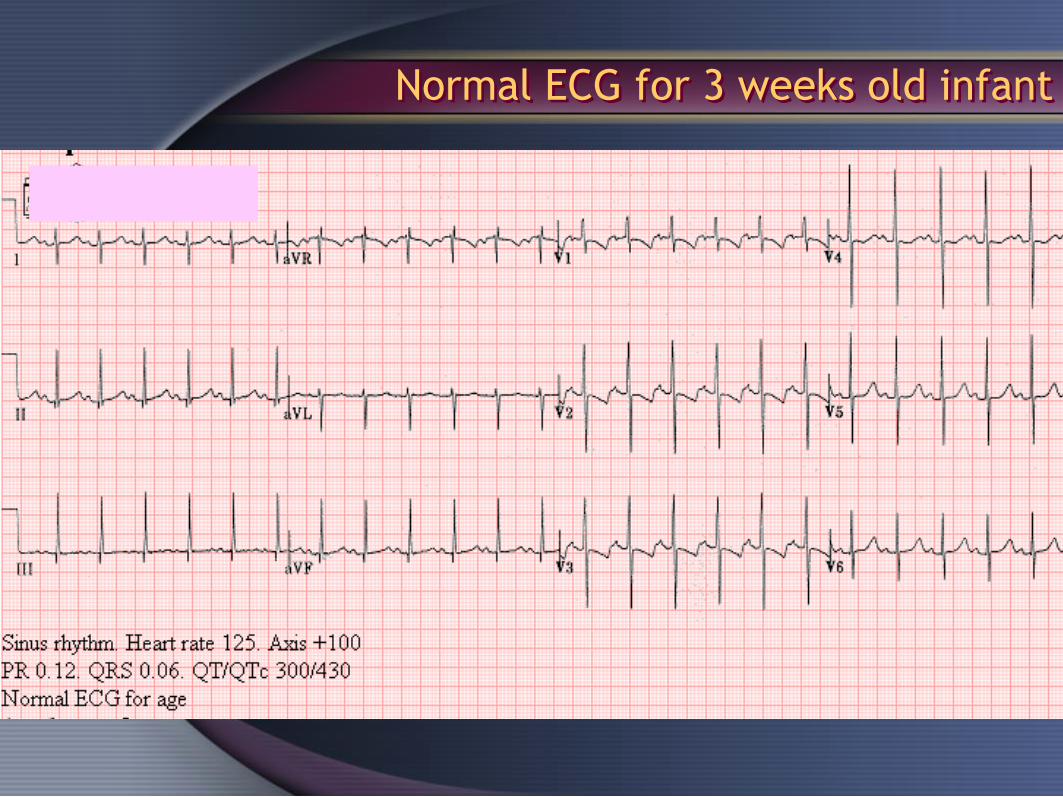
Normal ECG for 3 weeks old infant

Normal ECG for 3 months old infant

Normal ECG for 2 years old child

Normal ECG for 6 years old child

Normal ECG for 15 years old male
RHYTHM DISORDERS

Abnormally Slow = Bradycardia
• Failure due to disease
Excessively Rapid = Tachycardia
• Due to sympathetic nervous system
Mechanisms of Rhythm Disorders
Abnormal Automaticity

Slowed or Blocked Conduction
• Impulse generated normally
• Impulse slowed or blocked as it makes its way
through the conduction system
Mechanisms of Rhythm Disorders
*Animation
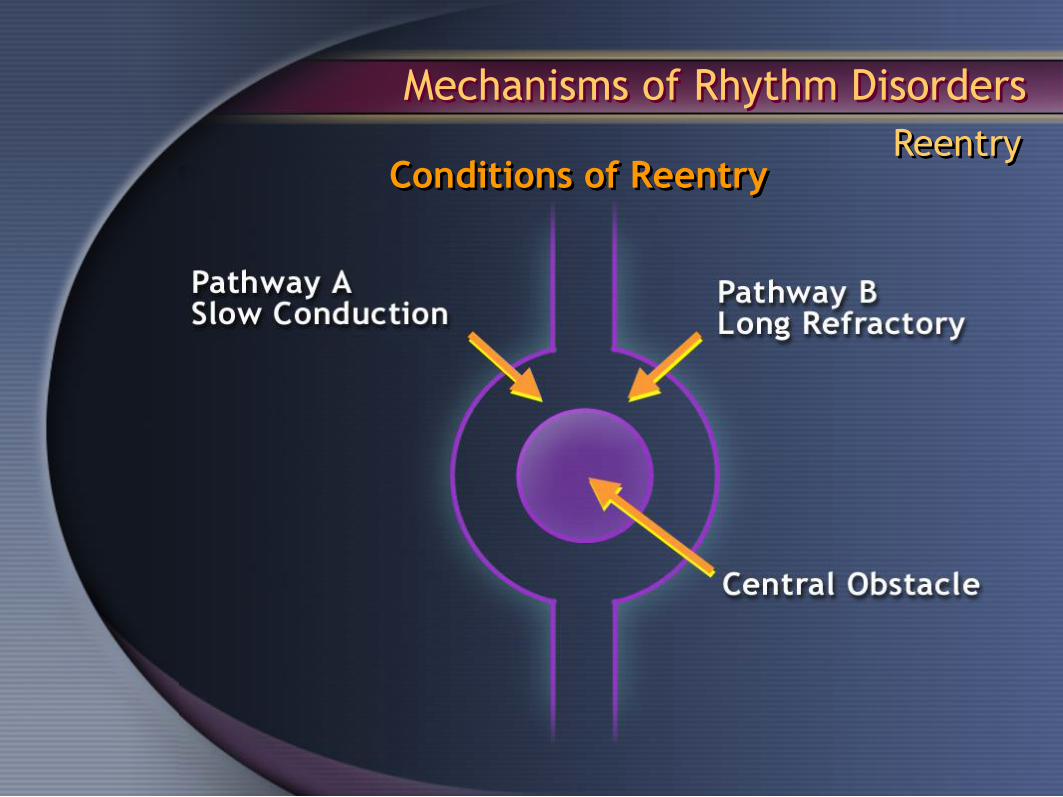
Mechanisms of Rhythm Disorders
ReentryConditions of Reentry

Mechanisms of Rhythm Disorders
Reentry
Substrate + Trigger = Reentry

Mechanisms of Rhythm Disorders
Reentry
RHYTHM DISORDERS
Bradyarrhythmias
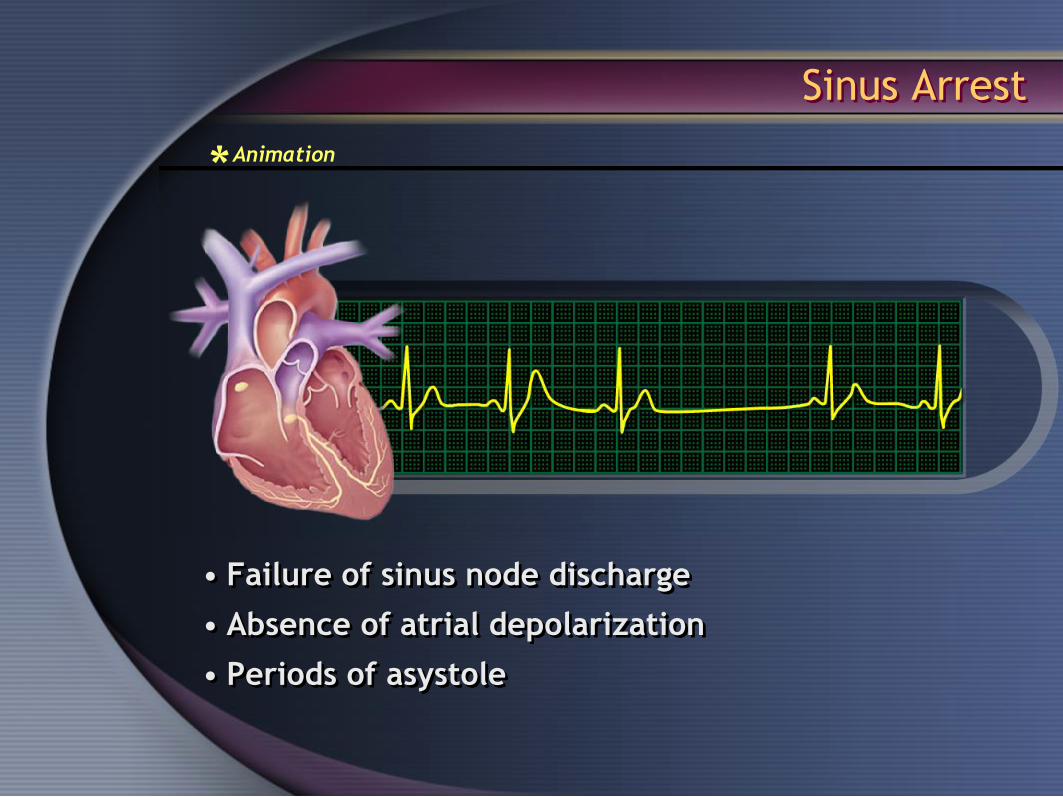
• Failure of sinus node discharge
• Absence of atrial depolarization
• Periods of asystole
Sinus Arrest
*Animation
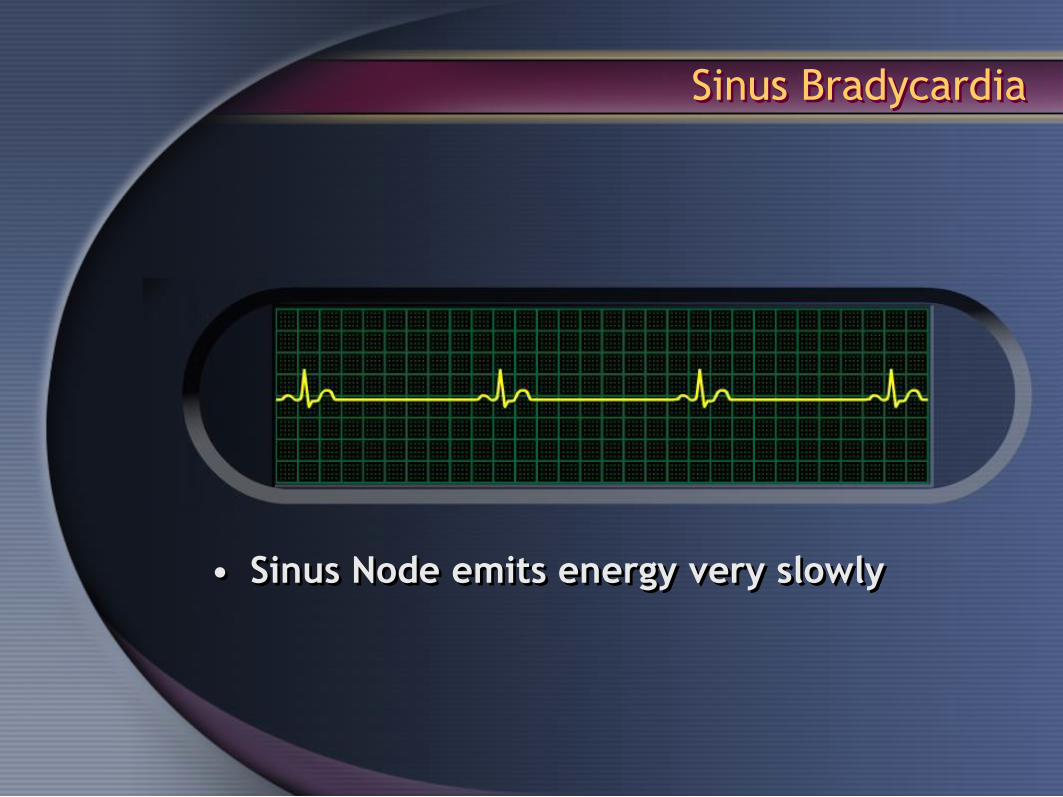
• Sinus Node emits energy very slowly
Sinus Bradycardia

• Intermittent episodes of slow and
fast rates from the SA node or atria
• Brady <60 BPM
• Tachy >100 BPM
Brady/Tachy Syndrome

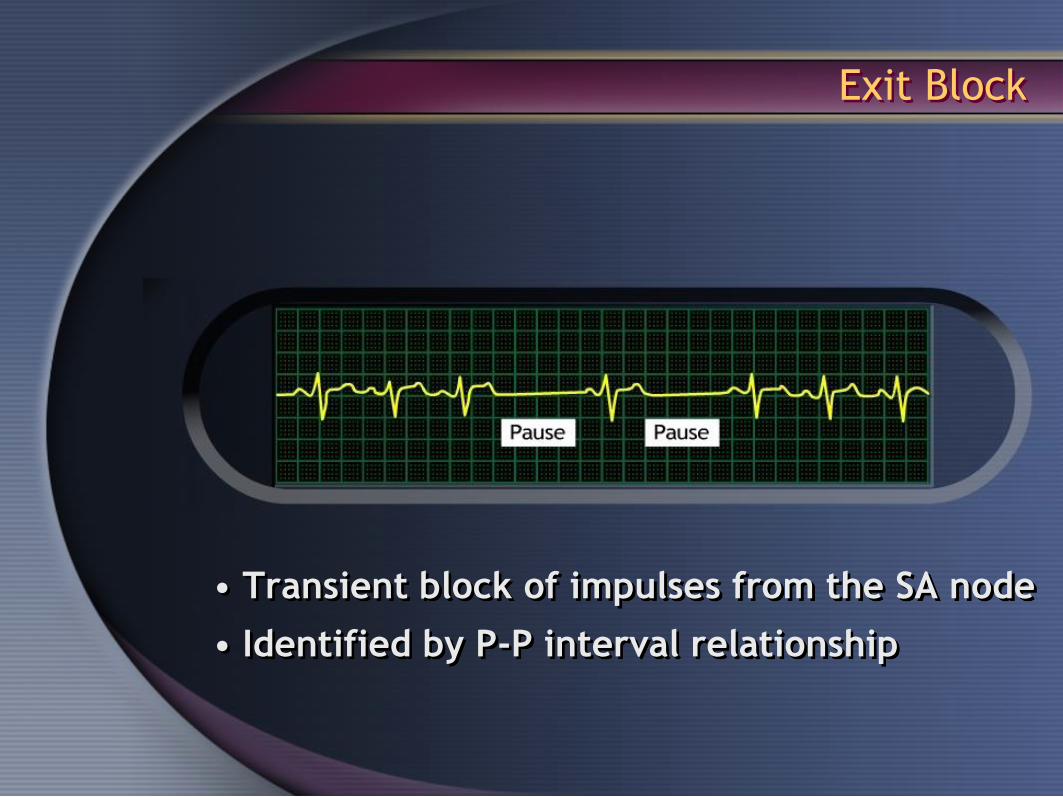
• Transient block of impulses from the SA node
• Identified by P-P interval relationship
Exit Block

First-Degree AV Block
• PR interval > 200 ms
• Delayed conduction through the AV Node
- Example shows PR Interval = 320 ms

• Progressive prolongation of the PR interval until
there is failure to conduct and a ventricular beat
is dropped
Known as Wenckebach Block
Second-Degree AV Block - Mobitz I
*Animation

• Regularly dropped ventricular beats
– Ex: 2:1 block (2 P-waves to 1 QRS complex)
– Atrial rate = 75 BPM
– Ventricular rate = 42 BPM
Second-Degree AV Block – Mobitz II

• No impulse conduction from the atria to the ventricles
– Ventricular rate = 37 BPM
– Atrial rate = 130 BPM
– PR interval = variable
Third-Degree AV Block
*Animation
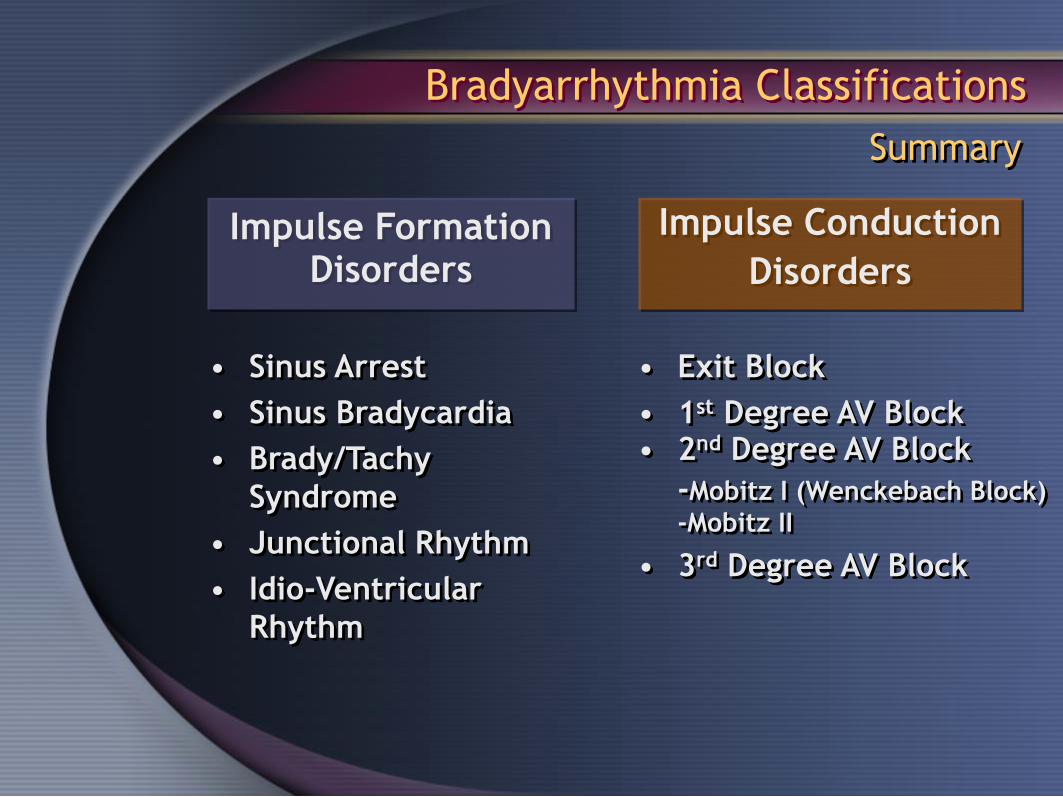
Summary
• Sinus Arrest
• Sinus Bradycardia
• Brady/Tachy
Syndrome
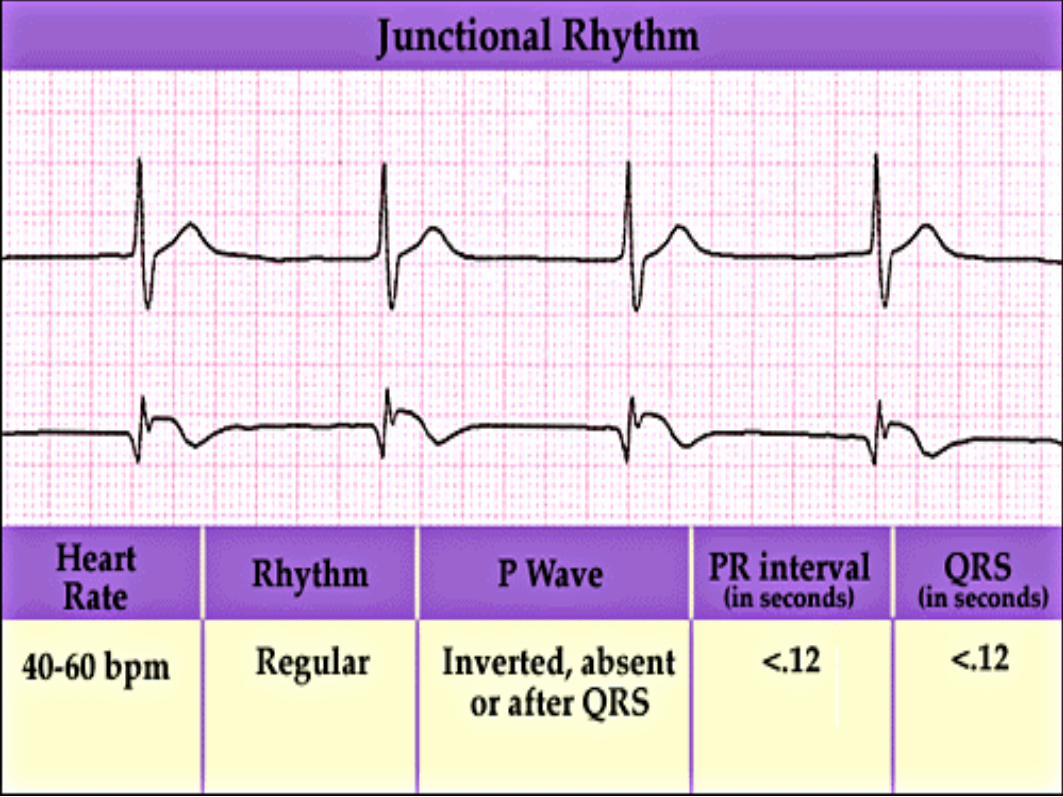
• Junctional Rhythm
• Idio-Ventricular
Rhythm
• Exit Block
• 1st Degree AV Block• 2nd Degree AV Block
-Mobitz I (Wenckebach Block)
-Mobitz II
• 3rd Degree AV Block
Impulse FormationDisorders
Impulse Conduction
Disorders
Bradyarrhythmia Classifications

RHYTHM DISORDERS
Tachyarrhythmias

•Paroxysmal
– Ectopic focus, sudden onset, abrupt cessation
•Sustained
– Duration of > 30 seconds
– Requires intervention to terminate
•Non-Sustained
– At least 6 beats or < 30 seconds
– Spontaneously terminates
•Recurrent
– Occurs periodically
– Periods of no tachycardia are longer than periods
of tachycardia
Terms Describing Tachycardias

• Incessant– Long periods of tachy, short periods of NSR
•Monomorphic– Single focus
– Complexes are similar with equal intervals
•Polymorphic– Multiple foci
– Complexes appear different with varied intervals
•SVT (Supraventricular Tachycardia)– Originating from above the ventricles
Terms Describing Tachycardias

Tachyarrhythmia Classifications
Classification Based on Disorder
Impulse FormationDisorders
TachycardiasImpulse Conduction
Disorders

Sinus Tachycardia
• Origin: Sinus Node
• Rate: 100-180 BPM
• Mechanism: Abnormal (Hyper) Automaticity

Atrial Tachycardia
• Origin: Atrium - Ectopic Focus
• Rate: >100 BPM
• Mechanism: Abnormal Automaticity
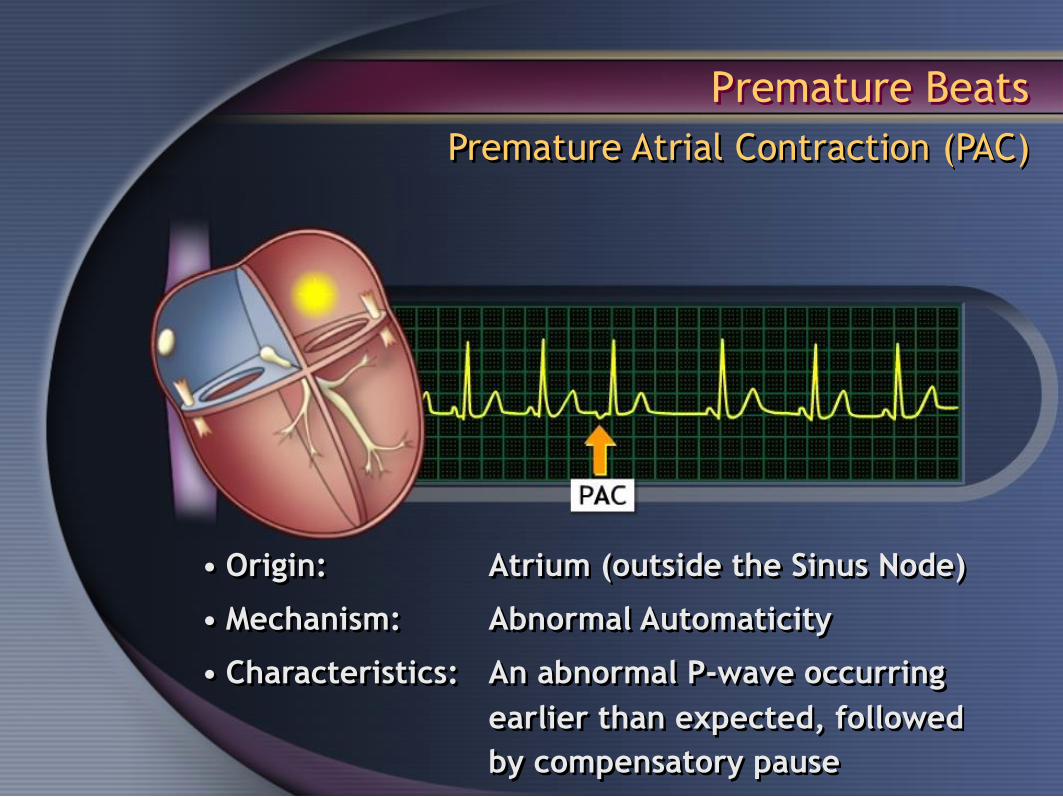
Premature Beats
Premature Atrial Contraction (PAC)
• Origin: Atrium (outside the Sinus Node)
• Mechanism: Abnormal Automaticity
• Characteristics: An abnormal P-wave occurring
earlier than expected, followed
by compensatory pause

Premature Junctional Contraction
• Origin: AV Node Junction
• Mechanism: Abnormal Automaticity
• Characteristics: A normally conducted complex with
an absent p-wave, followed by a
compensatory pause
Premature Beats

Premature Ventricular Contractions (PVCs)
• Origin: Ventricles
• Mechanism: Abnormal Automaticity
• Characteristics: A broad complex occurring earlier
than expected, followed by a
compensatory pause
Premature Beats

PVC Patterns
•Bigeminy
- Every other beat
•Trigeminy
- Every third beat
•Quadrigeminy
- Every fourth beat
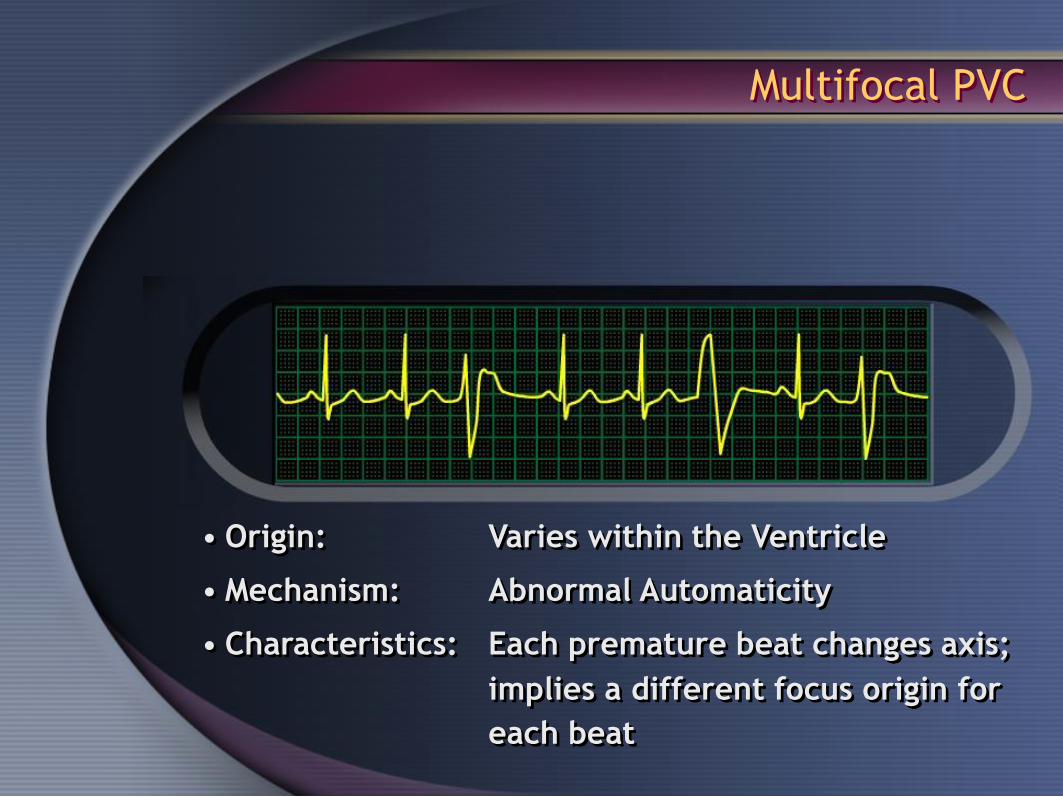
• Origin: Varies within the Ventricle
• Mechanism: Abnormal Automaticity
• Characteristics: Each premature beat changes axis;
implies a different focus origin for
each beat
Multifocal PVC

Accelerated Idio-Junctional Rhythm
• Origin: AV Node or Junctional Tissue
• Mechanism: Abnormal Automaticity
• Characteristics: Occurs when cells depolarize at a
rate faster than the Sinus Node

Accelerated Idioventricular Rhythm
• Origin: Ventricle
• Mechanism: Abnormal Automaticity
• Rate: Ventricular rate >sinus rate, but <VT
• Characteristic: Dominates and takes over the rhythm

Sinus Rhythm being taken over by an Idioventricular Rhythm
Accelerated Idioventricular Rhythm

Atrial Flutter
• Origin: Right & Left Atrium
• Mechanism: Reentry
• Characteristics: Rapid, regular p-waves
*Animation

Atrial Fibrillation (AF)
• Origin: Right and/or left atrium
• Mechanism: Multiple wavelets of reentry
• Rate 400 BPM
• Characteristics: Random, chaotic rhythm;
atria quiver; associated with
irregular ventricular rhythm
*Animation

Atrial Fibrillation (AF)

Multifocal Firing
Other AF Mechanisms
• Mechanism: Abnormal Automaticity (multi-sites)
• Characteristics: Many depolarization waves;
activation occurs asynchronously;
not in rhythm with sinus node

• Mechanism: Abnormal Automaticity (single-
focus, usually in the Posterior
Left Atrium)
• Characteristics: Rapid discharge; single ectopic site
Other AF Mechanisms
Single Focus Firing

Atrial Flutter vs. Atrial Fibrillation
Atrial Flutter
Summary of Disease Characteristics
Underlying
Mechanism
Pattern
Atrial Rate
Ventricular Rate
Rhythm
Atrial Fibrillation
• Multiple wavelet reentry
• Multiple/single focus
firing
• Wavy baseline
• 400 BPM
• Varies w/conduction
• Grossly Irregular
• Reentry via macro
reentrant circuit
• Saw tooth baseline
• 250 to 400 BPM
• Varies w/conduction
• Usually regular

•Extra pathway + AV Node = reentry
•2 Types– Orthodromic
• A to V through node, then enters accessory pathway to loop
• Produces narrow complex SVT
– Antidromic
• A to V through accessory pathway, then enters node to loop
• Produces wide-complex SVT
•An SVT caused by the existence of an extra
pathway from the atria to the ventricles
AVRT

Orthodromic
• Mechanism: Reentry
• Rate: 180 - 260 BPM, sometimes faster
• Characteristics: Extra electrical pathway to ventricles
Wolf-Parkinson-White (WPW)
Syndrome is most common
AVRT
*Animation

Antidromic
• Mechanism: Reentry
• Rate: 180 - 260 BPM, sometimes faster
• Characteristics: Extra electrical pathway to ventricles;
produces wide complex tachycardia
AVRT
*Animation

• Accessory Pathway = Bundle of Kent
• Orthodromic - 90% - AV node – antegrade conduction;
- Extra pathway – retrograde conduction
• Antidromic – 10% - Extra pathway – antegrade conduction
- AV node – retrograde conduction
Wolff-Parkinson-White

• Origin: Outside the AV Node
• Mechanism: Reentry
• Rate: 180-260 BPM – can be faster
• Characteristics: Short PR Interval (< 120 ms),wide
QRS (> 110 ms), obvious delta wave
Wolff-Parkinson-White

• Origin: AV Node
• Mechanism: Reentry
• Rate: 150 - 230 BPM, faster in teenagers
• Characteristics: Normal QRS with absent P-waves;
most common SVT in adults
AVNRT

AVRT vs. AVNRT

AVRT
• 180 – 260 BPM
• Narrow QRS if orthodromic
• Wide QRS if antidromic
• Delta wave + in SR
• PR < 120 ms
• 1:1 Conduction
AVNRT• 150 – 230 BPM
• Narrow QRS
• Short RP interval
• No delta waves
• Initiating PR long
• P-waves buried in QRS
• Conduction 1:1, or 2:1when distal block present
AVRT vs. AVNRT

• Origin: Ventricles (Single Focus)
• Mechanism: Reentry Initiated by abnormal
Automaticity or Triggered activity
• Characteristics: Rapid, wide, and regular QRS
EKG Characteristics
Monomorphic VT
*Animation

• Origin: Ventricles (Wandering Single Focus)
• Mechanism: Reentry with movement in the circuit
Initiated by Abnormal Automaticity or
Triggered activity
• Characteristics: Wide and irregular QRS Complex that
changes in axis
Polymorphic VT
*Animation
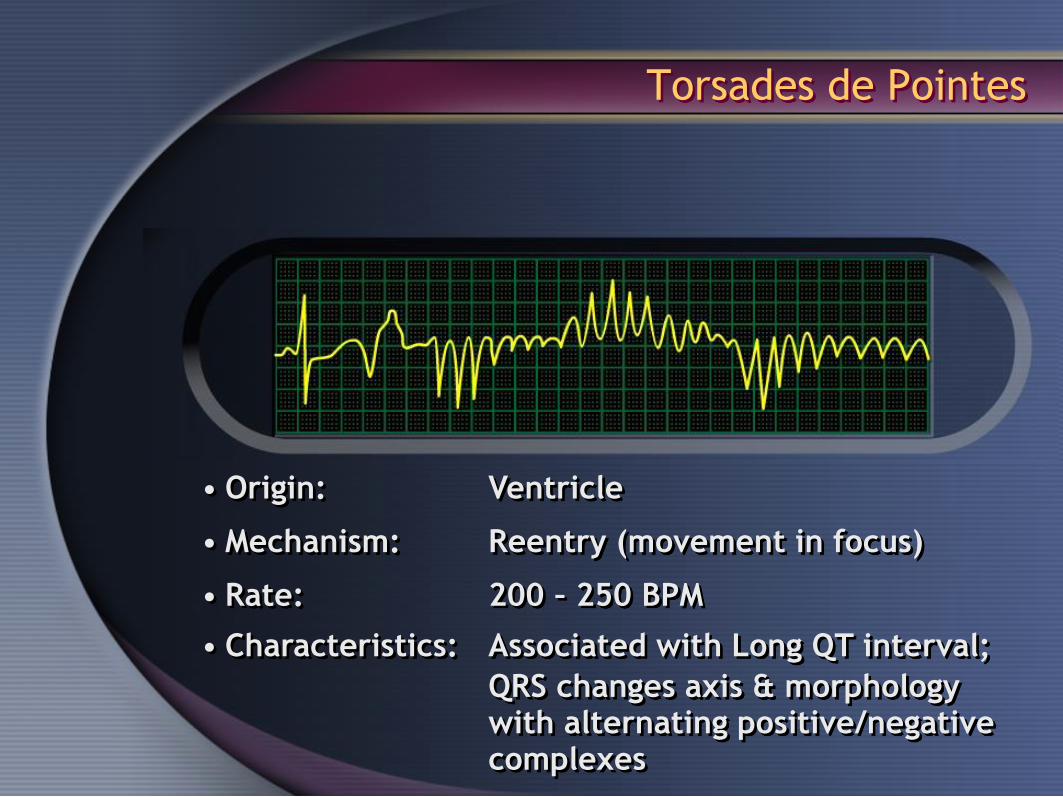
• Origin: Ventricle
• Mechanism: Reentry (movement in focus)
• Rate: 200 – 250 BPM
• Characteristics: Associated with Long QT interval;
QRS changes axis & morphology with alternating positive/negative complexes
Torsades de Pointes

• Origin: Ventricle
• Mechanism: Multiple Wavelets of reentry
• Characteristics: Irregular with no discrete QRS
Ventricular Fibrillation (VF)
*Animation
Tachyarrhythmia Classifications
Summary
Impulse FormationDisorders
Impulse Conduction
Disorders
• Atrial Flutter
• Atrial Fibrillation
• AVRT
•AVNRT
• Ventricular Tachycardia
• Ventricular Fibrillation
• Sinus Tachycardia• Atrial Tachycardia
• Premature Contractions
• Accelerated Idio-
Junctional Rhythm
• Accelerated
Idioventricular
Rhythm (AIVR)

Based on origin
• Sinus Tachycardia
• Atrial Tachycardia
• Accelerated Idio-Junctional Rhythm
• Atrial Flutter
• Atrial Fibrillation
• AVRT
• AVNRT
Tachyarrhythmia Classifications
• Accelerated Idioventricular
Rhythm (AIVR)
• Ventricular Fibrillation (VF)
• Ventricular Tachycardia (VT)

RHYTHM DISORDERS
Common Causes

Causes of Rhythm Disorders
Congenital
• Present at birth due to genetics,
environment
Heart Disease
• Myocardial Infarction, Cardiomyopathy,
High Blood Pressure
Chemically Induced
• Diet Pills, Cold Medicine, Illegal Drugs,
Caffeine, Tobacco, Alcohol
Causes of Rhythm Disorders
Secondary to other conditions
• Hyper-Thyroid
• Neurocardiogenic Syncope
- Hypersensitive Carotid Sinus Syndrome (CSS)
- Vasovagal Syncope (VS)

Thank You