corehem: developing comparative effectiveness outcomes for ... · or factor ix (hemophilia b) in...
TRANSCRIPT

j
coreHEM: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia Final Report
May 21, 2018 | Version 1.0

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
i
TABLE OF CONTENTS Executive Summary ............................................................................................................... ii
Methods .................................................................................................................................................... ii Results ....................................................................................................................................................... ii Impact ....................................................................................................................................................... ii
Funding ................................................................................................................................ iii coreHEM Writing and Editing Team ...................................................................................... iii Acknowledgements .............................................................................................................. iii Introduction .......................................................................................................................... 1
Background ............................................................................................................................................... 1 Rationale ................................................................................................................................................... 1
Methods ............................................................................................................................... 2 Participant Recruitment ............................................................................................................................ 3 Developing an Outcome List for Voting .................................................................................................... 3
Grouping Outcomes into Domains ........................................................................................................ 4 Delphi ........................................................................................................................................................ 4
Delphi Voting......................................................................................................................................... 5 Delphi Analysis ...................................................................................................................................... 6 Round 1A Sub-survey ............................................................................................................................ 6
In-person Consensus Meeting .................................................................................................................. 6 Measurements and Instruments ........................................................................................................... 7
Results .................................................................................................................................. 8 Final Core Outcome Set ............................................................................................................................ 8 Measurements and Instruments ............................................................................................................ 10
Discussion ........................................................................................................................... 13
References .......................................................................................................................... 17
Appendix One – The coreHEM Participants .......................................................................... 19
Appendix Two - Literature Search Abstraction Plan .............................................................. 21
Appendix Three - Targeted Literature Search References ..................................................... 22 Cochrane Reviews ................................................................................................................................... 22 Journal Articles ........................................................................................................................................ 22 clinicaltrials.gov References .................................................................................................................... 27 Gene Therapy Literature ......................................................................................................................... 40
Appendix Four – Participant and Patient Interviews ............................................................. 41
Appendix Five – Interview Questions ................................................................................... 43
Appendix Six- Intial Outcome List for Voting Mapped to COMET Taxonomy ......................... 44
Appendix Seven – Delphi Voting Reference Document ......................................................... 47
Appendix Eight – Delphi Round One Results ......................................................................... 56
Appendix Nine – Delphi Round Two Results ....................................................................... 107
Appendix Ten - Example Personalized Feedback ................................................................ 149
Appendix Eleven – Worksheet used at in-person meeting .................................................. 150
Appendix Twelve- Delphi Timeline and Participation Rates ................................................ 153
Appendix Thirteen – Delphi Round Three Results ............................................................... 154
Appendix Fourteen – Core Outcome Set Definitions ........................................................... 155
Appendix Fifteen – Recognition of the core outcome set .................................................... 156

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
ii
EXECUTIVE SUMMARY METHODS coreHEM was initiated by the National Hemophilia Foundation in partnership with the Center for Medical Technology Policy and McMaster University. The aim of the project was to determine a core set of outcomes to evaluate efficacy, safety, comparative effectiveness, and value for hemophilia gene therapy. coreHEM utilized a multi-stakeholder collaborative process that included patients and patient advocates, clinicians, hemophilia researchers, US and international payers and HTA groups, representatives from government organizations, and life science companies with hemophilia gene therapy in development. A core technical group and a steering committee were appointed. coreHEM used a modified Delphi consensus process that was adapted from the COMET Initiative approach. A literature review and key informant interviews were used to create an initial list of outcomes, organized based on the COMET Initiative naming schematic for domains. A rating scale from 1 (not important to include in the core set) to 9 (critical to include) was used. Participants could suggest new outcomes to include or recover after deletion. Outcomes were eliminated if <70% of voters rated the outcome 7-9. But, if the patient stakeholder group average score was 7 or higher, the outcome was re-proposed for voting in subsequent rounds (a mechanism implemented to ensure that the “patient important” outcomes were not overturned by other stakeholder groups early in the process without the opportunity for additional discussion.) Project principal investigators were not part of the voting panel for the Delphi.
RESULTS coreHEM was conducted between May and November 2017, and the data analysis completed on December 20th, 2017. The project included three online survey rounds and one in-person meeting. The initial list of candidate outcomes included 48 outcomes, from which six core outcomes were identified as crucial for evaluating the effectiveness of gene therapy: frequency of bleeds, factor activity level, duration of expression, chronic pain, mental health status, utilization of the healthcare system (direct costs). During the process, the group agreed to separately list core outcomes and relevant adverse events, as the latter would be required for regulatory purposes. The adverse events that were voted as important by the group were liver toxicity, short-term immune response to FVIII/FIX, immune response to gene therapy (cytotoxic), and thrombosis in the short-term adverse events domain, development of other disorders, vector integration into the host genome, and duration of vector neutralizing response in the long-term adverse events domain, and cause of death in the mortality domain. During a breakout session at the in-person meeting, participants outlined parameters for the types of measurements/instruments that would ideally be used to measure the core set.
IMPACT coreHEM recruited an international multi-stakeholder panel with participants from over 40 organizations from nine countries. The project had sponsorship and participation by seven companies in the hemophilia gene therapy space. coreHEM achieved consensus on a core outcome set in less than 1 year, and initiated work on outlining parameters for the types of measurements and instruments that should be used to measure and report the core set. Participating organizations took part in the coreHEM project with the goal of identifying a core set of outcomes for use in future clinical studies of gene therapy in hemophilia. Collectively, they believe this

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
iii
recommended core outcome set, developed with multi-stakeholder input, will be useful in future assessments of gene therapies for hemophilia. They encourage product developers and other researchers to consider this recommended core outcomes set when developing study protocols for future clinical trials, registries and other studies.
FUNDING coreHEM was funded by a grant from the National Hemophilia Foundation and with participation fees from the following life science industry companies and academic gene therapy groups: Bayer AG, BioMarin Pharmaceutical Inc, Pfizer Inc, Shire Plc, Spark Therapeutics, St. Jude Children’s Research Hospital, and uniQure B.V. Alnylam Pharmaceuticals, Novo Nordisk, and Roche Genentech participated in the in-person meeting as observers, and contributed a meeting attendance fee. Observers did not vote in the Delphi. Project participants did not receive an honorarium for participating in the Delphi or attendance at the meeting. The Steering Committee served as voting panelists and additionally provided project guidance and oversight without compensation. Grants, participation and attendance fees supported all project-related expenses, including salaries for CMTP project staff, in-person consensus meeting expenses and travel costs.
coreHEM WRITING AND EDITING TEAM Principal Investigators Alfonso Iorio, MD, PhD, FRCPC (McMaster University); Mark W. Skinner, JD (National Hemophilia Foundation and Institute for Policy Advancement, Ltd.); Sean Tunis, MD, MSc (Center for Medical Technology Policy). CMTP (Center for Medical Technology Policy) Jennifer Al Naber, MS, MSPH; Elizabeth Clearfield, MHS; Janelle King; Donna Messner, PhD; Julie Simmons, CMP.
ACKNOWLEDGEMENTS Appendix 1 lists the coreHEM Steering Committee, Delphi voters, in-person consensus meeting observers, and key informants who provided interviews.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
1
INTRODUCTION BACKGROUND Hemophilia is a genetic bleeding disorder caused by a deficiency of coagulation factor VIII (hemophilia A) or factor IX (hemophilia B) in the blood clotting pathway. Hemophilia A occurs in 1 in 10,000 live births and hemophilia B occurs in about 1 in 50,000; it is considered a rare disease with an estimated 20,000 and 400,000 people living with the disease in the US and worldwide, respectively.1,2 Persons living with hemophilia experience various degrees of bleeding, depending on residual coagulation factor levels. Bleeding occurs most commonly in joints, soft tissue, and muscles, causing short-term symptoms (acute bleeding, acute pain) and long-term-complications (chronic pain, hemophilia arthropathy, or disability). Acute and chronic complications may dramatically reduce health-related quality of life (HRQoL) of persons living with hemophilia (PWH). Hemophilia is managed either by maintaining a routine of prophylactic infusions of the missing clotting factor (Factor VIII, FVIII or Factor IX, FIX), or treatment with on-demand infusions at the time of a bleed. The goal of disease management is to control the frequency and severity of bleeds and prevent joint damage and other complications associated with bleeding episodes. Recent gene therapy trials in hemophilia have reported promising results, demonstrating that gene therapy could yield a long-term functional “cure” by changing or replacing the missing and abnormal genes.3-7 A “cure” may come in the form of a permanent correction of the underlying genetic defect or through prevention of all complications of living with hemophilia;8 a functional cure eliminates the day-to-day burden, though the underlying genetic disease remains. This would allow the body to produce the previously-missing clotting factor without the need for, or with a much-reduced need for, factor replacement therapy. Gene therapy would be life-changing for patients, relieving them of many of the daily burdens and limitations they currently endure. Phase 3 trials of gene therapy are beginning. This new treatment technology has the potential to change the landscape of hemophilia management. Therefore, we are at an opportune time to establish the standards for collecting and reporting on relevant, well-specified outcomes that are important to patients. Outcomes associated with a functional “cure” may be different than the outcomes used to assess the current standard of care.
RATIONALE A core outcome set is a minimum set of outcomes that should be measured and reported in all clinical trials for a specific condition.9 Currently, there are no guidelines on which outcomes should be included in the hemophilia gene therapy trials, and each trial may choose to include certain outcomes based on factors such as time, availability of clinical and laboratory resources, interest to the investigators, funding, or whether a specific outcome will highlight a benefit of a specific product. Heterogeneity in the outcomes measured and reported across clinical trials on the same disease or of the same intervention make it difficult to compare the studies with each other and can lead to uncertainty about which treatment is best for patients. Even worse, in the field of rare diseases an inability to pool results across studies may prevent attainment of the critical evidence body mass needed to support adoption of a new treatment modality. Hemophilia clinical trials that collect the same outcome may report the results differently. For example, one study may report a mean level of circulating FVIII/FIX and another study may instead report the percentage of participants who have reached a certain (and sometimes arbitrary) threshold of FVIII/FIX. In systematic reviews, data from certain studies may not be included in meta-analyses if the outcome definition, timing of outcome collection, or measurement instrument was not consistent with other trials, or if the outcome was not collected on or reported at all.10,11 The lack of relevant or comparable outcomes in clinical research studies for a given condition undermines efforts across the healthcare sector to make evidence-based health policy decisions and improvements to

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
2
health care delivery. The use of core outcome sets, agreed-upon minimum sets of outcomes that should be measured and reported in all clinical studies for related evaluations of a specific condition, can offer a potential solution. The development of a core outcome set can help to address some of the problems associated with heterogeneity of outcome collection and reporting.12,13
Core outcome sets are developed with robust input of relevant stakeholders who agree on a minimum set of outcomes through a structured consensus process. Defining and uniformly implementing a core set of outcomes for inclusion across trials and gene therapy products would enhance the predictability and consistency of the assessment and appraisal of these treatments by payers and Health Technology Assessment (HTA) organizations when making coverage and reimbursement decisions.a From the payer perspective, core outcomes have the additional advantage of facilitating comparison of results from different trials and potentially reducing the risk of selective outcome reporting. Patient involvement and support by patient organizations should ensure that the outcomes are meaningful to, and their measurement acceptable by, patients enrolled in trials, and adoption of the technology in clinical practice foreseeable. Overall, multi-stakeholder input on core outcomes sets helps to assure alignment across the basic evidence needs of regulatory authorities, payers, and patients, and can therefore smooth the regulatory review and market access process for companies using these core outcomes.
METHODS The goal of coreHEM was to develop a core outcome set for use in hemophilia gene therapy clinical trials. The project used a modified Delphi consensus process that included three online surveys and one in-person meeting. The objective of the project was to develop a set that, when used, will help evaluate efficacy, safety, comparative effectiveness and value of gene therapy for hemophilia. The methods recommended by the Core Outcomes Measures in Effectiveness Trials (COMET) Initiative were consulted and adapted for rapid turn-around given the plans for near-term initiation of several pivotal trials. The study was registered in COMET’s database of core outcome set projects. Standard definitions, adapted from COMET, were used throughout the project (Table 1). Although we used a modified Delphi on an accelerated timeline, each of the 11 quality standards recommended by COMET as part of the Core Outcome Set-STAndards for Development (COS-STAD) recommendations were fulfilled.14 The coreHEM protocol underwent ethical review by Chesapeake IRB (Reference Pro00023013) and determined to be exempt from IRB oversight.
a An example of an HTA assessment on hemophilia performed by the Swedish Agency for Health Technology Assessment and
Assessment of Social Services is available here15: http://www.sbu.se/en/publications/sbu-assesses/treatment-of-hemophilia-a-and-b-and-von-willebrand-disease/

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
3
Table 1. coreHEM Definitions
Definition Example
Core outcome set
An agreed set of outcomes which should be measured and reported, as a minimum, in all trials of a specific clinical area or of a specific condition.9
WHO/ILAR core set for rheumatoid arthritis clinical trials16
Domain A broad category, an element of a person’s overall health and life in relation to their treatment.
Physical Functioning
Outcome Contained within each domain, “what” we want to measure.
Joint Impairment
Measurements or Instruments
“How” something is measured; measurement/instrument is a tool to measure an outcome. The tool can be a single question, a questionnaire with a composite score, a score obtained through physical examination, laboratory measurement, or observation of an image
X-Ray Pettersson score, range of motion, Hemophilia Joint Health Score (HJHS)
PARTICIPANT RECRUITMENT The consensus project involved stakeholders from all aspects of the product lifecycle, including patients, clinicians, life science industry representatives, academic researchers, regulators, and post-regulatory decision-makers such as payers and HTA groups (full participant list in Appendix 1). Participant recruitment began in April 2017 and continued through early September 2017 when all stakeholder groups were sufficiently represented and at which time the Delphi began. Participants were invited to an introductory webinar that provided more detail on the methods and goals of the project. The coreHEM team worked to ensure a balance between the stakeholder groups, based on pre-defined categories, including approximately equal numbers of patients or patient advocates; clinicians; US and international payers and HTA groups; research funders; and regulators. Two representatives from each participating life science company with a gene therapy product for hemophilia in phase 1 or later clinical trials were invited, with the total number of participants from the life sciences industry not exceeding the total number of non-industry participants. One academic gene therapy group also participated and was allowed two representatives. The stakeholder groups included some individuals who were not specifically trained in hemophilia and blood disorders but who otherwise had extensive knowledge of outcomes research, methods research, or systematic review experience, and provided insight on selecting well-specified outcomes that can measure value in a new treatment such as gene therapy. Forty-nine individuals representing the various stakeholder groups participated in the Delphi. A steering committee of six participants was selected, and included one patient, one clinician, one US payer, one international payer, and two representatives from the life science industry (one each from a company working on a gene therapy product for hemophilia A and hemophilia B).
DEVELOPING AN OUTCOME LIST FOR VOTING A non-structured literature review was used to generate a starting list of potential outcomes for the core outcome set. From the literature review, a list of outcomes already in use in hemophilia trials was compiled. We abstracted outcomes from Cochrane review on hemophilia, records on interventions for

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
4
hemophilia on clinicaltrials.gov, and from reports in the journal Haemophilia. The search terms and data abstraction rules are described in Appendix 2. The references that were reviewed and from which outcomes were abstracted are listed in Appendix 3. Because our core set was focused on gene therapy, a number of studies describing gene therapy in other fields were references. They are listed separately in Appendix 3. Interviews with participants were conducted to complement the literature search. To ensure that our initial list was not missing any relevant outcomes, we asked questions that reflected each interviewee’s personal knowledge about and experience with hemophilia. This also served as an opportunity to suggest novel outcomes that have not been used before but were potentially relevant for gene therapy trials. Individual interviews were held with coreHEM participants in-person at the International Society on Thrombosis and Hemostasis XXVIth Congress (July 2017) to understand various stakeholder perspectives and priorities regarding the most important outcomes to measure. Interviewees were invited to suggest novel outcomes for the hemophilia gene therapy space that may not yet be in the literature. Patient/patient advocate interviews which included a balance of US / international perspectives were held by teleconference or during the National Hemophilia Foundation’s Annual Meeting (August 2017). A list of participants and patients interviewed is available in Appendix 4. The structured list of questions used for the interviews is available in Appendix 5. Grouping Outcomes into Domains The coreHEM project team and Steering Committee developed and reviewed the comprehensive list of outcomes generated from the literature review and interviews grouped across 10 domains. Domain names and groupings were based on the outcome naming taxonomy proposed by COMET,17 with some modifications recommended by the coreHEM Steering Committee to better reflect the hemophilia landscape. The initial list of coreHEM outcomes and domains for voting mapped to the COMET domains is provided in Appendix 6.
DELPHI A modified Delphi process was used to arrive at consensus on a core outcome set, with a special focus on patient-important and patient-reported outcomes.18-21 The coreHEM Delphi process included a total of three surveys (Round 1-Round 3, with an extra round of deliberations at the in-person meeting [Advisory Vote for Round 3]) plus one sub-survey to confirm results (Round 1A) (Figure 1b). SurveyMonkey® software was used for the online voting. The survey was pilot-tested by non-participants with an interest in the project; suggestions from pilot testers were reviewed and incorporated.
b Adapted from Iorio A, Skinner MW, Clearfield E, et al.; for the coreHEM panel. Core outcome set for gene therapy in
haemophilia: Results of the coreHEM multistakeholder project. Haemophilia. 2018;00:1–6. https://doi.org/10.1111/hae.13504

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
5
Figure 1. Overview of the coreHEM Process and outcome selection. Delphi Voting Voters rated each outcome on a scale from 1 (not important to include in a core set) to 9 (critical to include) indicating the importance of including each outcome in clinical trials of gene therapy for hemophilia; three categories of importance were assigned (Table 2). Participants could review outcome definitions via circulated reference documents and through links in the online survey (Appendix 7). The response period lasted approximately 10 days for each Delphi round; participants received email reminders to complete the survey. Participants could suggest new outcomes to include or recover after deletion. Project Principal Investigators were not part of the voting panel for the Delphi.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
6
Delphi Analysis The outcome list was condensed and prioritized using the definitions of consensus shown in Table 3. Using the rating scale from 1-9, outcomes were eliminated if <70% of voters rated the outcome 7-9. But, if the patient stakeholder group average score was 7 or higher, the outcome was re-proposed for voting in subsequent rounds (a mechanism implemented to ensure that the “patient important” outcomes were not overwhelmed by other stakeholder groups early in the process without the opportunity for additional discussion. For the final voting round (Round 3), the “patient-important” retention category was dropped and outcomes needed to reach high consensus to be included in the core set.
Upon completion of voting for each round, mean ratings by stakeholder group were graphed for each outcome, along with a histogram showing the number of people who selected each rating and a scatterplot showing the scope of the votes for that outcome on the 1-9 scale, broken down into seven stakeholder categories (Appendix 8 for Delphi Round 1 Results, Appendix 9 for Delphi Round 2 Results). Voters received personalized feedback on a summary table that contained the overall mean rating for each outcome and the mean rating by stakeholder group, color-coded to show whether their selection was higher or lower than the mean rating for their stakeholder group (Appendix 10). Round 1A Sub-survey In order for participants to see the effect of the consensus criteria on the outcome list and to confirm agreement with the group decisions, a sub-survey (Round 1A) was developed. Participants could confirm, by voting agree or disagree, their agreement with the results. New outcome suggestions from the free-text comments were also assessed in Round 1A. Results from Round 1A informed the development of Round 2.
IN-PERSON CONSENSUS MEETING The in-person consensus meeting was held on November 14-15, 2017 in Baltimore, Maryland. The meeting was attended by 41 voters (84% of voters), and 8 observers. An evening reception on November 14th included three level-setting presentations on hemophilia, gene therapy, and core outcome sets. The agenda for the full day meeting on the 15th included a multi-stakeholder panel and plenary sessions. Attendees were assigned to breakout sessions ensuring a balanced stakeholder mix for each subgroup; during the breakout sessions, participants discussed one or more of the outcomes retained in the process until then, each one bringing the specific perspective of their stakeholder group.
Table 2. Levels of Importance (on a scale of 1-9)
1-3 The outcome is not important to include in the core outcome set
4-6 The outcome is important but not critical to include in the core outcome set
7-9 The outcome is critical to include in the core outcome set
Table 3. coreHEM Consensus Definitions
Consensus to Select (high consensus) An outcome in which ≥70% of all voters rated the outcome with a score of 7, 8, or 9 (“critical importance”)
Consensus to Select (patient-important) An outcome in which <70% of all voters rated the outcome 7, 8 or 9, but the stakeholders in the Patient group gave the outcome an average rating of ≥7
Consensus to Eliminate An outcome in which <70% of voters rated the outcome 7, 8, or 9, AND the Patient group average rating was <7

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
7
An Advisory Vote for Round 3 was held in real time and included three questions about combining remaining outcomes. Measurements and Instruments A final session of the in-person meeting was dedicated to explore how to measure outcomes that would-be part of the core set. Each breakout group was assigned to discuss certain outcomes already included or which were candidates for inclusion in the core set. Discussion questions were based on the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) guidelines.22 COSMIN has developed methodological standards for the studies measurement properties, with the goal of improving the selection of measurements/instruments. Table facilitators directed the conversation to define parameters of an ideal instrument or measurement and build upon the collective knowledge of the group to identify measurements/instruments already being used in hemophilia or that they were aware of from other therapeutic fields that may apply to the novel outcomes in the coreHEM set. The full worksheet is provided in Appendix 11. A summary of parameters that were to be considered was developed from the COSMIN and COMET Initiative guideline (Table 4). The breakout session ended with a report-back to the large group; additionally, each breakout group discussion was recorded and transcribed, and a narrative summary was provided to coreHEM participants following the conclusion of the Delphi and completion of data analysis.
Table 4. Parameters to consider for measurements and instruments
Parameter Items to Consider
Definition • What does the item measure?
• Does it only measure one thing, or do several results/ideas fit into the outcome?
How to measure? • What type of measurement/instrument is ideal to measure this outcome? (survey a patient fills out, clinical assessment a doctor performs, a laboratory test, etc.)
Feasibility • How long should/does it take to measure this outcome?
• How long is too long?
• What is/should be the patient/clinician burden associated with this measure?
Generic vs disease-specific • Should this outcome be measured using a generic instrument/measurement, or a hemophilia-specific instrument/measure?
Timing and recall • When should the outcome be measured?
• How often the outcome should be measured?
• How often should the outcome be reported?
• If using an instrument for a patient-reported outcome, how far back should the patient have to remember to answer the questions?
Current landscape • Are there instruments/measurements currently being used that could capture this outcome?
• If so, would it be adequate/appropriate to use with gene therapy?
• Do the existing instruments capture the difference between gene therapy and current standard of care (are they sensitive enough)?
Related measurements • Do other therapeutic areas also measure this outcome?
• Which instruments do they use?

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
8
RESULTS The targeted literature search was performed in July and August 2017. Overall, we abstracted outcomes from 52 journal articles, 195 records on clinicaltrials.gov and nine Cochrane reviews. Individual interviews were held with 12 coreHEM participants (24% of the group) to gain perspective on how trial endpoints and related outcomes may change with gene therapy technology. Seven patients were interviewed; these interviews included a particular focus on living with hemophilia, outcomes that are important in day-to-day life, and outcomes that a patient could foresee affected by a treatment that potentially represents a functional cure. The outcome list that was developed for voting included 48 outcomes that had been identified from the literature review and/or interviews with coreHEM participants. Forty-nine Delphi voters agreed to be part of coreHEM (Table 5). Participation rates were >90% for each Delphi round (Appendix 12). After Round 2, three outcomes with high consensus were included in the core set without further discussion or vote at the meeting (frequency of bleeds, factor activity level, and duration of expression). Seven outcomes, although not high consensus by the primary definition, met criteria as “patient-important” and were also included for discussion at the meeting: target joints, mental health (anxiety/depression/coping/worry), feeling of physical health/general health perception, transformational psychological or emotional impact of experiencing a cure (or that of having made an irreversible treatment decision whatever the outcome), risk aversion (including confidence to participate in physical activity/sports/play), burden of treatment regimen on patient/family, and chronic pain (frequency/intensity/duration/character). This ensured that patient-important outcomes would not be dismissed without careful consideration of the group. In addition, participants could request that an outcome previously eliminated be added back in for discussion at the in-person meeting by providing, in writing, a request and explanation for why the outcome required further discussion and another vote. One outcome was re-introduced into the discussion in this way (utilization of the healthcare system [direct costs]). In the final voting round, three more outcomes were selected to be part of the core set (chronic pain, utilization of the healthcare system [direct costs], and mental health status, an outcome that represents a combination of the mental health [anxiety/depression/coping/worry] outcome and the transformational psychological or emotional impact of experiencing a cure [or that have having made an irreversible treatment decision] outcome, which was suggested and voted on at the consensus meeting). The results of the final Delphi voting round are available in Appendix 13.
Table 5. coreHEM Stakeholder Group Summary
Stakeholder Group Number of Voters % of Total Voters
Patients/Patient Advocates 5 10.2
Clinicians 5 10.2
Researchers 5 10.2
Regulators 4 8.1
Public Research Funding Agencies 3 6.1
HTA Organizations 6 12.2
Payers 9 18.4
Life Science 12 24.5
FINAL CORE OUTCOME SET The coreHEM Delphi produced three categories of results (Figure 2):
1) The recommended core outcome set, including frequency of bleeds, factor activity level, duration of expression, chronic pain, utilization of the healthcare system (direct costs), and

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
9
mental health condition. Three of these achieved high consensus in Round 2 (frequency of bleeds, factor activity level, and duration of expression), while the other three (chronic pain, mental health status, and utilization of the healthcare system [direct costs]) achieved high consensus in the final voting round. The six outcomes are intended to be measured and reported in each clinical trial for hemophilia gene therapy.
2) Adverse events that were rated as critically important by the group and/or by patients. Following voting Round 2, a decision was made to omit adverse events from the outcome list presented for further voting, since adverse events are typically collected to meet regulatory requirements and for post-market surveillance. These were not included as part of the core outcome set, however, their importance to panelists warranted highlighting for consideration in trial planning and longitudinal data collection. The adverse event outcomes were categorized as three domains: short-term adverse events, long-term adverse events, and mortality.
3) Additional outcomes that did not reach the threshold for inclusion in the core set, but which were rated as highly important by the majority of the group but did not reach the inclusion threshold of 70% (i.e. 50-69% of participants voted the outcome as “critical to include” on the Delphi rating scale). These were: duration/frequency/type of physical activity/sport/play (65% of panel calling this a “critically important” outcome) and feeling of physical health/general health perception (52% of voters calling it critical). As these two are the only outcomes rated >50% from the Physical Functioning and Perceived Health Status domains (respectively), they are proposed as a complement to the core set and may be desirable to be considered for measurement in clinical trials when and where feasible. (As noted above, product developers using core outcomes may also use additional outcome measures relevant to the specific study purposes and design.)
Definitions for the core outcomes, additional outcomes and adverse events are provided in Appendix 14.
Figure 2. Three groups of outcomes selected by coreHEM Delphi voting.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
10
MEASUREMENTS AND INSTRUMENTS For the measurement and instrument breakout group discussions at the in-person meeting, one group was assigned all three of the clinical/physiological outcomes (frequency of bleeds, factor activity level, and duration of expression), and one group discussed chronic pain. Two groups each were assigned to discuss the two topics of mental health and utilization of healthcare system (direct costs). The summaries of these discussions are presented in Tables 4-7.
Table 4. Parameters to measure clinical outcomes for gene therapy in hemophilia
Clinical Outcome
Parameter Frequency of bleeds Factor activity level Duration of expression
Definition The group did not reach consensus.
--
How to measure? Patient reported; group debated whether ultrasound should be required to confirm a bleed
Validated factor activity assay; two are available: chromogenic and one-stage
Feasibility Measurements are subjective, but easy to record. Imaging, if required to confirm, is not invasive, but it does add the burden of the patient going to clinic.
*Feasibility was not discussed
Measuring factor activity level to determine if expression is durable is likely to become part of long-term follow-up within the comprehensive care setting for people who receive gene therapy. If it transitions to be measured at an annual clinic visit, feasibility is high.
Generic vs disease-specific Measuring bleeds is hemophilia-specific
Factor activity level is hemophilia-specific
Duration of expression is hemophilia-specific, in particular for those who receive gene therapy
Timing and recall A bleed should be reported as it happens, but the bleed rate will be calculated and reported annually. It would be useful to obtain more information about the cause of the bleed (e.g. was it a traumatic injury). A short questionnaire could be filled out each time a bleed occurs.
During trial, measured frequently. After trial, ideally measured every 6 months. In the long term, if gene therapy allows a patient to be treated as having a mild hemophilia phenotype, this may only be measured once per year.
Pivotal trials will have mandated observation of 5 to 15 years during which factor activity level, and consequently duration of expression will be measured. Like factor activity level, it will be measured frequently during the trials and will likely transition to be measured once per year. Factor level might be validated as a surrogate for it in the long term.
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
11
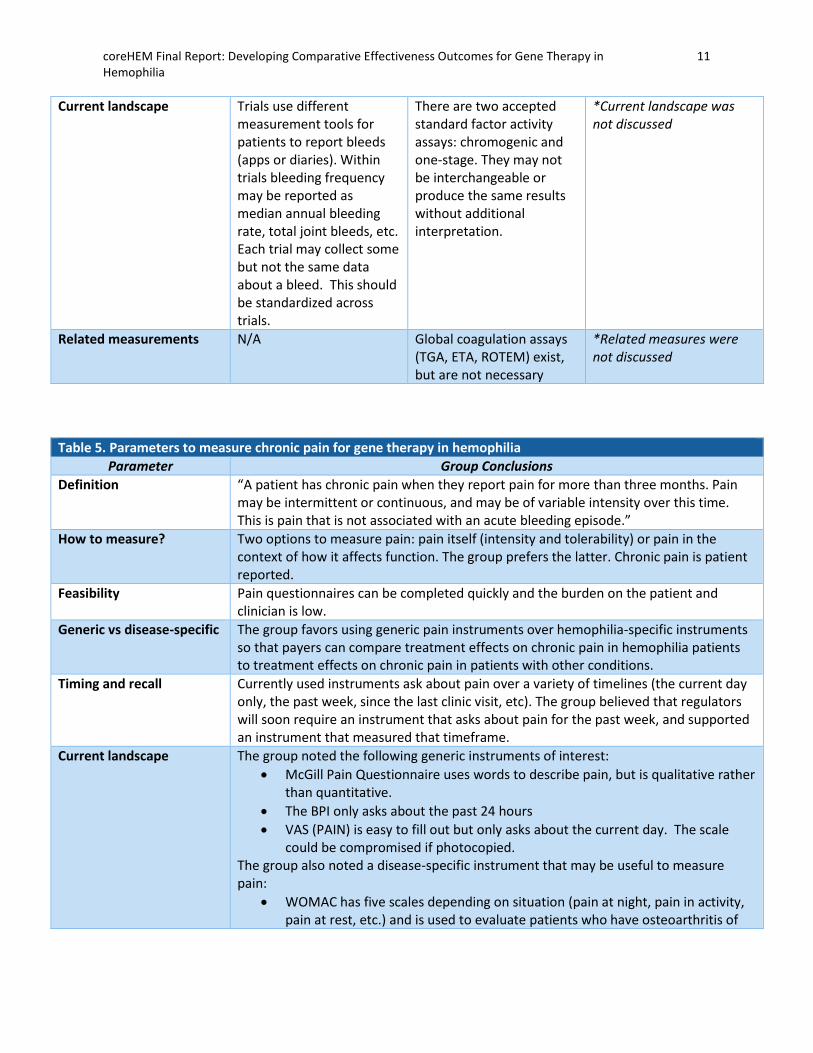
Current landscape Trials use different measurement tools for patients to report bleeds (apps or diaries). Within trials bleeding frequency may be reported as median annual bleeding rate, total joint bleeds, etc. Each trial may collect some but not the same data about a bleed. This should be standardized across trials.
There are two accepted standard factor activity assays: chromogenic and one-stage. They may not be interchangeable or produce the same results without additional interpretation.
*Current landscape was not discussed
Related measurements N/A Global coagulation assays (TGA, ETA, ROTEM) exist, but are not necessary
*Related measures were not discussed
Table 5. Parameters to measure chronic pain for gene therapy in hemophilia
Parameter Group Conclusions
Definition “A patient has chronic pain when they report pain for more than three months. Pain may be intermittent or continuous, and may be of variable intensity over this time. This is pain that is not associated with an acute bleeding episode.”
How to measure? Two options to measure pain: pain itself (intensity and tolerability) or pain in the context of how it affects function. The group prefers the latter. Chronic pain is patient reported.
Feasibility Pain questionnaires can be completed quickly and the burden on the patient and clinician is low.
Generic vs disease-specific The group favors using generic pain instruments over hemophilia-specific instruments so that payers can compare treatment effects on chronic pain in hemophilia patients to treatment effects on chronic pain in patients with other conditions.
Timing and recall Currently used instruments ask about pain over a variety of timelines (the current day only, the past week, since the last clinic visit, etc). The group believed that regulators will soon require an instrument that asks about pain for the past week, and supported an instrument that measured that timeframe.
Current landscape The group noted the following generic instruments of interest:
• McGill Pain Questionnaire uses words to describe pain, but is qualitative rather than quantitative.
• The BPI only asks about the past 24 hours
• VAS (PAIN) is easy to fill out but only asks about the current day. The scale could be compromised if photocopied.
The group also noted a disease-specific instrument that may be useful to measure pain:
• WOMAC has five scales depending on situation (pain at night, pain in activity, pain at rest, etc.) and is used to evaluate patients who have osteoarthritis of

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
12
the knee and hip, including pain, stiffness, and physical functioning of the joints23
*There are other instruments currently available which include pain domains, but were not put forward by the group. This cell notes only the instruments discussed by the breakout group at the in-person meeting.
Related measurements The group considered whether pain medication use could be a good proxy for chronic pain, but reporting may be inaccurate and the two do not always correlate. Pain instruments (other than WOMAC) specific to other therapeutic areas were not mentioned.
Table 6. Parameters to measure mental health for gene therapy in hemophilia
Parameter Group Conclusions
Definition “The impact of the intervention on the emotional well-being of the recipient, including mental health.”
How to measure? An instrument with a summary score that asks about the reasons for mental health status (rather than just the presence or absence of depression/anxiety) would be ideal.
Feasibility A concise questionnaire taking 10-15 minutes, would be feasible.
Generic vs disease-specific Anxiety and depression are general, but things like coping (with a disease, or with effects of a cure) are disease-specific. A generic and a disease-specific instrument used simultaneously can help show the effect of gene therapy; a positive change in the disease-specific instrument without a similar change in a generic instrument could indicate improvement due to the therapy.
Timing and recall The amount of time before a change in mental health status associated with gene therapy may be linked to a patient’s expectations about treatment and how quickly they should expect a change. The instrument should be administered at study enrollment and every 3-6 months during a trial.
Current landscape For depression and anxiety, the group noted the Hospital Anxiety Depression Scale (HADS), HAM-A, GAD-7, the BDI and the clinically Useful Anxiety Outcome Scale (CUXOS). Quality of life questionnaires such as the EQ-5D have domains with questions about mental health status. The patient advocacy organization PatientsLikeMe has a quality of life instrument that could be tailored to hemophilia. The group was not aware of currently-existing instruments to measure the transformational aspect of being cured.
Related measurements To capture the transformational changes to mental health, the group suggested the following fields that may have instruments that could be related: surgery, cancer survival, non-emergency bypass surgery, post-partum depression, and organ transplant literature. Ultimately, qualitative data may be required to capture how a cure affects mental health status.
Table 7. Parameters to measure utilization of the healthcare system (direct costs) for gene therapy in hemophilia
Parameter Group Conclusions
Definition “Use of the healthcare systems physical products and services (adverse events requiring hospitalization, non-study-mandated clinic visits, factor use) whose costs are borne directly by standard payers.”

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
13
How to measure? Annual report of the costs incurred within the healthcare system for a patient calculated either by 1) summing the actual cost each year, or 2) observing the number of units of something that is used and then applying a standard price to each unit.
Feasibility These events and related resource utilization are typically already captured on a CRF by clinical research staff
Generic vs disease-specific Factor usage is a large cost that is hemophilia-specific. However, as this is a data point rather than an instrument, a discussion generic vs. disease-specific is not relevant.
Timing and recall Since this would be collected from a CRF, data collection would coincide with clinic visits. Reporting forms or apps should be standardized, so that events that are part of the direct cost burden are captured similarly across all trials.
Current landscape The information needed for direct costs is already measured; events in which a patient utilizes the healthcare system are all collected and reported on a case report form.
Related measurements N/A
DISCUSSION coreHEM is unique among core outcome set initiatives in that the voting group included a significant number of HTA and payer representatives (the combined number of HTA representatives and payers was equal to the combined number of patients/patient advocates, clinicians and researchers). Making up 12.2% and 18.4% of the voting panel, respectively, the number of these types of stakeholders is greater than in any core outcome set initiative that we are aware of. Initiating a conversation with HTA groups and payers before pivotal trials begin allows the life science companies to take multiple points of view into account in the protocol development stage. Because these therapies will be costly, it is important that the trial not only show safety and effectiveness for regulatory approval, but benefits for the patient experience that can compete to show the value of the product when decisions must be made about which product to recommend and reimburse. A core outcome set, if used as recommended, can ensure that outcomes from various trials are comparable. HTA and other decision-makers who are part of the conversation can advocate for outcomes that may make assessment more straightforward. Having representatives from HTA and payer groups as part of the voting group and in-person discussion also allows these stakeholders to meet with those who will use the product and hear real stories about why certain outcomes are important to these patients and clinicians. Participating organizations took part in the coreHEM project with the goal of identifying a core set of outcomes for use in future clinical studies of gene therapy in hemophilia. Collectively, they believe this recommended core outcome set, developed with multi-stakeholder input, will be useful in future assessments of gene therapies for hemophilia. They encourage product developers and other researchers to consider this recommended core outcomes set when developing study protocols for future clinical trials, registries and other studies. Several of the participating payer and HTA organizations have approved specific language recognizing the core outcome set (Appendix 15). The original Delphi method developed by RAND was designed to allow the participating experts to influence one another through the provisions of feedback, comments, and analyses from round to round.24 However, this feedback was anonymized (or semi-anonymized by the use of code names) and communications between the experts was mediated through the research group. This was done to prevent undue influence of particularly senior or distinguished participants, and also conversely to encourage the opinions and insights of more junior experts to be considered seriously.25 In addition to the aspect of anonymity, the Delphi method is considered a “structured communication” in which there

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
14
is feedback of individual contributions of information and knowledge, assessment of the group judgement or view, and opportunity for individuals to revise views.26 A later, “modified” version of the Delphi was developed by RAND which included an in-person meeting to eliminate this mediation and allow for direct interaction of the experts.27 These researchers concluded that effective meeting facilitation would be able to manage these interpersonal issues. This is the approach that we have also used. This approach is particularly warranted since the coreHEM group is multi-stakeholder in composition (multiple types of expertise are in the room, not a single group of people in the same field). Hence, while voting decisions are made individually, the in-person meeting provides opportunities for co-learning to inform the vote. A potential limitation of this study was that we included only five patients/patient advocates in the voting group. However, this represents 10% of all voters, and was equal to the number of clinicians and researchers who took part in the project. Some core outcome set initiatives are now including a large number of patients in their Delphi; participation is offered to any patient presenting with the condition at specific medical centers involved with the core outcome set project. Due to the timing of the pivotal hemophilia gene therapy trials, coreHEM required a rapid turn-around in which large-scale invites of that nature were not possible. Instead, patients were selected and invited to be part of the project because they are well-versed and/or previously involved in other hemophilia trials, studies, or had roles in patient organizations and were aware of the changing hemophilia treatment field. The targeted literature review to develop the initial list of outcomes was supplemented by interviews with patients in order to ensure that outcomes of particular importance to patients that may or may not have been used previously in hemophilia trials were on our list for voting. We also included one of our patient/patient advocate representatives as part of our Steering Committee, who advised on team decisions from a patient perspective. Finally, our built-in rules to keep the patient-important outcomes in the list for discussion prior to the final Delphi round was included in our analysis rules so that the patient voice would not be overwhelmed by other stakeholder groups. Because of these measures, we feel confident that the patient perspective remained strong throughout the process and that other stakeholder groups intentionally sought out the patient point of view. It is possible that there was a bias among the patients and patient advocates who agreed to participate in coreHEM; patients particularly invested in the future of gene therapy may have been more likely to agree to participate in the project or be interviewed during the background research stage. While our built-in rules ensured that the patient opinion was given weight among the opinions of other stakeholder groups, we cannot be sure that the opinion of the patients was coming from a broad-based representation. It is possible that with a different group of patients/patient advocates, the results would differ. However, we feel that by maintaining a balanced multi-stakeholder group we have developed a set of six outcomes that can show the effectiveness and value of gene therapy, while remaining acceptable, in general, to the patients who must endure the trials and the disease. The six outcomes in the set are versatile and well-rounded. Two are outcomes measured within a clinical setting (factor activity level and duration of expression). Three are patient reported outcomes: frequency of bleeds (which is within the physiological / clinical domain), chronic pain, and mental health (reflecting a physical and emotional manifestation of hemophilia). The remaining outcome is an economic outcome utilizing data captured within a health system and reflecting the potential importance of cost impacts of these treatments. The list also reflects a set that can capture the novelty of gene therapy while providing a basis of comparison to existing therapies. For example:

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
15
• Frequency of bleeds is a “legacy” outcome that has been used in past hemophilia trials. Including it in the core set enables some degree of comparisons of efficacy and effectiveness with existing treatments.
• Factor activity level was used as an early measure in hemophilia treatment but had fallen out of favor as prophylactic treatment became standard. As gene therapy shows promise to achieve near-normal factor activity levels, measurement of factor level may reemerge as a relevant outcome for regulatory approval.28
• Duration of expression replaces pharmacokinetic measurements of previous treatments, and can represent the long-term value of an investment in gene therapy.
• Chronic pain and mental health outcomes will capture the impact of gene therapy as a functional cure, and changes in these outcomes should reflect the transformational nature of gene therapy.
• Measurement of direct costs of healthcare resource allows for a value-based approach (where value equals costs relative to outcomes) and may reflect the expected changes to a gene therapy patients’ medical needs, if factor use and hospitalizations are greatly reduced, considering the expected high prices of gene therapy.
Multi-stakeholder agreement on a core set of outcomes is an important achievement that can help to ground comparisons between gene therapies and traditional ones, and among the gene therapies themselves. However, the optimal value of the core set will only be achieved if agreement is also reached on common standards and instruments for measurement and reporting of each outcome.29
Guidance on how to measure and report the outcomes in the core set is therefore a necessary component. As noted, participants discussed measurement instruments during the afternoon session of the in-person meeting. However, this discussion only sketched overall priorities the group might specify for a general framework. Specific instruments or approaches for measurement were not selected. Nevertheless, with the input from these discussions and analysis of the nature of the recommended outcomes, the project team can envision a pathway for selecting the appropriate measurement/instrument for each outcome in the coreHEM set, and planning for this work is underway. Some of the outcomes in the core set have straightforward measurements that could be implemented presently or shortly following some further limited discussion to standardize definitions.
• Frequency of bleeds is a patient-reported outcome recorded and followed clinically. Consistent rules of how and when a trial participant should report a bleed requiring factor use can help equalize data collection, and therefore reporting, of this outcome. It does not require an instrument but will require agreement on definition. It is typically reported annually. A standardized method to measure and report bleeds could be developed after agreement on details such as whether confirmatory imaging is needed, how bleeds should be reported, and associated questions about the bleed (e.g., mechanism for patient-reporting).
• For factor level and duration of expression, scientific debate over which assay is preferred may be necessary. However, regulators may soon harmonize requirements which will likely become the standard. Duration of expression is an extension of factor activity level, and is measured over time, but may require post-approval studies to fully capture gene therapy’s effect on this outcome.
• For utilization of the healthcare system (direct costs), the breakout group that discussed this outcome at the in-person meeting proposed three events which account for the majority of
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
16
direct costs associated with hemophilia: adverse events requiring hospitalization, non-study-mandated clinic visits, and factor use. These events are already collected and reported during trials, and the costs could be summed annually.
Chronic pain and mental health require instruments, and possibly qualitative data collection. To capture the transformational aspect of a functional cure and the related effects on pain and mental health, instruments that have been previously used to measure these outcomes may not be sufficient; alternative instruments may need to be identified or developed. For chronic pain, the coreHEM participants supported a general rather than hemophilia-specific instrument, to allow for payers and other post-regulatory decision makers to make comparisons to treatments in other therapeutic areas. For mental health, until an appropriate instrument is identified to capture the transformation of a cure, we suggest using a general and a hemophilia-specific instrument in tandem to help delineate changes in mental health that are due to treatment from those unrelated to hemophilia or disease. Upcoming instruments on “life interference” may fulfill the need for a way to measure the transformational changes of a cure. Further research on the benefits or drawbacks of the various instruments already available (in hemophilia or other therapeutic fields) for these outcomes is required. Follow-on work will be needed to answer the questions outlined above and develop a consensus particularly on measurement of chronic pain and mental health. The effort should be informed by guidance published jointly by the Core Outcome Measures in Effectiveness Trials (COMET) initiative and the COnsensus-based Standards for the selection of health Measurement Instruments (COSMIN) initiative on selecting outcome measurement instruments.22 That said, based on the discussion above, a more streamlined and rapid process of selecting instruments is conceivable while still serving the needs of patients and all relevant stakeholders.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
17
REFERENCES
1. Sharma A, Easow Mathew M, Sriganesh V, Reiss UM. Gene therapy for haemophilia. Cochrane Database of Systematic Reviews 2016, Issue 12. Art. No.: CD010822. DOI: 10.1002/14651858.CD010822.pub3.
2. “Types of Bleeding Disorders”. National Hemophilia Foundation. https://www.hemophilia.org/Bleeding-Disorders/Types-of-Bleeding-Disorders/Hemophilia-A.
3. Nathwani AC, Tuddenham EG, Rangarajan S, Rosales C, McIntosh J, Linch DC, et al. Adenovirus-associated virus vector-mediated gene transfer in hemophilia B. New England Journal of Medicine. 2011; 365 (25): 2357-65.
4. Nathwani AC, Reiss UM, Tuddenham EG, Rosales C, Chowdary P, McIntosh J, et al. Long-term safety and efficacy of factor IX gene therapy in hemophilia B. New England Journal of Medicine 2014; 371(21):1994-2004.
5. Miesbach W, Tangelder M, Klamroth R, Schutgens R, Coppens M, Kampmann P, et al. Updated results from a dose escalating study in adult patients with haemophilia B treated with AMT-060 (AAV5-hFIX) gene therapy. Haemophilia 2016; 22(Suppl 4): 151-2.
6. George LA, Sullivan SK, Giermasz A, Rasko JE, Samelson-Jones BJ, Ducore J, et al. Hemophilia B Gene Therapy with a High-Specific-Activity Factor IX Variant. N Engl J Med. 2017;377(23):2215-2227.
7. Rangarajan S, Walsh L, Lester W, Perry D, Madan B, Laffan M, et al. AAV5–Factor VIII Gene Transfer in Severe Hemophilia A. N Engl J Med. N Engl J Med. 2017(26);377:2519-2530.
8. Skinner MW, Lillicrap DP, McMillan J, Castro Ozelo M, Pierce GF. What is a cure and how do we get there? Haemophilia. 2004; 10(s4):115-118.
9. Williamson PR, Altman DG, Blazeby JM, Clarke M, Devane D, Gargon E, Tugwell P. Developing core outcome sets for clinical trials: issues to consider. Trials. 2012; 13 (1):132.
10. Ioannidis JP, Horbar JD, Ovelman CM, Brosseau Y, Thorlund K, Buus-Frank ME, et al. Completeness of main outcome across randomized trials in entire discipline: survey of chronic lung disease outcomes in preterm infants. BMJ. 2015; 350: h72.
11. Saldanha IJ, Li Tianjing, Yang C, Owczarzak J, Williamson PR, Dickersin K. Clinical trials and systematic reviews addressing similar interventions for the same condition do not consider similar outcomes to be important: a case study in HIV/AIDS. Journal of Clinical Epidemiology. 2017; 84: 85-94.
12. Kirkham JJ, Gargon E, Clarke M, Willilamson PR. Can a core outcome set improve the quality of systematic reviews? – a survey of the Co-ordinating Editors of Cochrane review groups. Trials. 2013; 14 (21).
13. Tunis SR, Clarke M, Gorst SL, Gargon E, Blazeby JM, Altman DG, Williamson PR. Improving the relevance and consistency of outcomes in comparative effectiveness research. J Comp Eff Res. 2016;5(2):193-205.
14. Kirkham JJ, Davis K, Altman DG, Blazeby JM, Clarke M, Tunis S, et al. Core Outcome Set-STAndards for Development: The COS-STAD recommendations. PLoS Med. 2017;14(11): e1002447
15. SBU. Treatment of Hemophilia A and B and von Willebrand disease. Stockholm: Swedish Council
on Health Technology Assessment (SBU); 2012. SBU report no 208E.
16. Boers M, Tugwell P, Felson DT, van Riel P, Kirwan JR, Edmonds JP, et al. World Health Organization and International League of Associations for Rheumatology core endpoints for

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
18
symptom modifying antirheumatic drugs in rheumatoid arthritis clinical trials. J Rheumatol. 1994; suppl 41) 21: 86-9.
17. Dodd S, Clarke M, Becker L, Mavergames C, Fish R, Williamson PR. A taxonomy has been developed for outcomes in medical research to improve knowledge discovery. J Clin Epidemiol. 2017; pii: S0895-4356(17)30589-9.
18. Elwyn G, O’Connor A, Stacey D, Volk R, Edwards A, Coulter A, et al. Developing a quality criteria framework for patient decision aids: online international Delphi consensus process. BMJ 2006; 333(7565): 417.
19. Hsu CC, Sandford BA. The Delphi technique: making sense of consensus. Pract Assessment, Res Eval. 2007; 12: 1-8.
20. Sinha IP, Smyth RL, Williamson PR. Using the Delphi technique to determine which outcomes to measure in clinical trials: recommendations for the future based on a systematic review of existing studies. PLoS Med. 2011; 8(1): e1000393.
21. Custer RL, Scarcella JA, Stewart BR. The modified Delphi technique: a rotational modification. Journal of Vocational and Technical Education. 1999; 15(2): 1-10.
22. Prinsen CA, Vohra S, Rose MR, Boers M, Tugwell P, Clarke M, Williamson PR, Terwee CB. How to select outcome measurement instruments for outcomes included in a “Core Outcome Set”–a practical guideline. Trials. 2016 Dec;17(1):449.
23. Bellamy, N. The WOMAC knee and hip osteoarthritis indices: development, validation, globalization and influence on the development of the AUSCAN hand OA indices. Clinical and Experimental Rheumatology. 2005; 23(5):S148.
24. Dalkey NC. Delphi. RAND Corporation. Santa Monica CA; 1967. 25. Yousuf MI. Using experts’ opinions through Delphi technique. Practical assessment, research &
evaluation. 2007 May; 12(4):1-8. 26. Linstone HA, Turoff M, editors. The Delphi method. Reading, MA: Addison-Wesley; 1975 Dec. 27. Fitch K, Bernstein SJ, Aguilar MD, Burnand B, LaCalle JR, Lazaro P, et al. The RAND/UCLA
appropriateness method user’s manual. RAND Corporation. Santa Monica CA; 2001. 28. Pierce GF, Ragni MV, van den Berg HM, et al. Establishing the appropriate primary endpoint in
haemophilia gene therapy pivotal studies. Haemophilia. 2017;23(5):643-644. 29. Saldanha IJ, Dickersin K, Wang X, Li T. Outcomes in Cochrane systematic reviews addressing four
common eye conditions: an evaluation of completeness and comparability. PLOS one. 2014; 9 (10): e1094000.
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
19
APPENDIX 1 – The coreHEM Participants
APPENDIX ONE – THE coreHEM PARTICIPANTS Principal Investigators. Alfonso Iorio, MD, PhD, FRCPC (McMaster University); Mark W. Skinner, JD (National Hemophilia Foundation and Institute for Policy Advancement, Ltd.); Sean Tunis, MD, MSc (Center for Medical Technology Policy). coreHEM Internal Working Group. Jennifer Al Naber, MS, MSPH (Center for Medical Technology Policy); Elizabeth Clearfield, MHS (Center for Medical Technology Policy); Donna Messner, PhD (Center for Medical Technology Policy). Steering Committee. Ronald Akehurst, BSc (Econ), DSC, Hon MFPHM (BresMed Health, University of Sheffield, Committee Member National Institute for Health and Care Evidence (NICE)); Mohit Jain, PhD, MBA (BioMarin); Edmund Pezalla, MD, MPH, PhD (enlightenment bioconsult, LLC); Glenn F. Pierce, MD, PhD (Third Rock Ventures); Leonard Valentino, MD, FAAP (Spark Therapeutics); Michelle Witkop, DNP, FNP-BC (National Hemophilia Foundation). Voting Panel. Andreas Altemark, GMACS (Bayer); Suzanne Belinson, MPH, PhD (Blue Cross and Blue Shield Association); Jason Booth, MPH (Shire); Philipp Dahm, MD, MHSc, FACS (University of Minnesota and Minneapolis VA Health Care System); Gerard Dolan, MB, ChB, FRCP (Edin), FRCP, FRCPath (NHS England, St Thomas’ Hospital, London, UK); Karen Facey, PhD (University of Edinburgh); Samantha Gouw, MD, PhD (Academic Medical Center Amsterdam and Leiden University Medical Center); Daniel Hart, BSc, MBChB, FRCP, FRCPath, PhD (The Royal London Hospital Haemophilia Centre, Barts and the London School of Medicine and Dentistry, QMUL, UK); Anneliese Hilger, PhD (Paul-Ehrlich-Institute); Craig Hooper, PhD (National Center on Birth Defects and Developmental Disabilities (NCBDDD), Centers for Disease Control (CDC)); Keith Hoots, MD (National Heart, Lung, and Blood Institute (NHLBI), National Institutes of Health (NIH)); James Jorgenson, RPh, MS, FASHP (Visante, Inc. & Visante Limited); Daniel Keene, MD, MA, FRCPC (Health Canada); Joanne Kim, MSc, PhD (Canadian Agency for Drugs and Technologies in Health (CADTH)); Snejana Krassova, MD, MMBS (Bayer); Gregory LeCleir (Bayer); David Lillicrap, MD, FRCPC (Queen’s University); Maria Lopes, MD, MS (Magellan Health); Peter Marks, MD, PhD (US Food and Drug Administration (FDA)); Paul Monahan, MD (Shire); Gyasi Moscou-Jackson, PhD, MHS, RN (Patient-Centered Outcomes Research Institute (PCORI)); Jennifer Murray, PharmD, BCGP (Myers and Stauffer, LC); Michelle Mujoomdar, PhD (EUnetHTA); Ellis Neufeld, MD, PhD (St. Jude Children’s Research Hospital); Jamie O’Hara, MSc (HC Economics, Ltd and Haemophilia Society); Brian O’Mahony, FACSLM, FIBMS (Irish Haemophilia Society, Ltd and European Haemophilia Consortium); Marie Österberg, PhD (Swedish Agency for Health Technology Assessment and Assessment of Social Services (SBU)); Charles Petrie, PhD (Pfizer); Vanita Pindolia, PharmD, BCPS (Henry Ford Health System); Steven Pipe, MD (University of Michigan); Andreas Pleil, PhD (Pfizer); Philip Reilly, MD, JD (Third Rock Ventures); Ulrike Reiss, MD (St. Jude Children’s Research Hospital); Michelle Rice (National Hemophilia Foundation (NHF); Sol Ruiz, PhD (Spanish Medicines Agency (AEMPS)); Lew Sandy, MD (UnitedHealth Group); Eileen Sawyer, PhD (uniQure); Michael Sharp, RPh (SharpRx Pharmaceutical Consultation Services); Amy Sood, PharmD (Canadian Agency for Drugs and Technologies in Health (CADTH)); Clive Spiegler, PhD (Spark Therapeutics); Peter Tugwell, MD, MSc (Center for Global Health); Alain Weill (World Federation of Hemophilia (WFH)); Sophie Werkö, MSc, PhD (Swedish Agency for Health Technology Assessment and Assessment of Social Service (SBU)); Wing Yen Wong, MD (BioMarin); Steven Zelenkofske, DO (uniQure). Observers. Donna Coffin, MSc (World Federation of Hemophilia (WFH); Katherine High, MD (Spark Therapeutics); John Ko, PharmD, MS (Alnylam Pharmaceuticals); Gallia Levy, MD, PhD (Genentech);

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
20
APPENDIX 1 – The coreHEM Participants
David Rind, MD (Institute for Clinical and Economic Review (ICER)); Ian Saldanha, MBBS, PhD (Johns Hopkins Bloomberg School of Public Health); Beverly Shea, PhD (Ottawa Hospital Research Institute and University of Ottawa); Karin Wahlander, MD, PhD (Novo Nordisk). Pilot Testers. Donna Coffin, MSc (World Federation of Hemophilia (WFH)); Samantha Craigie, MSc (McMaster University); Declan Noone (Irish Haemophilia Society); Ian Saldanha, MBBS, PhD (Johns Hopkins Bloomberg School of Public Health), Victoria Zuk (McMaster University). Interviews. Randall Curtis, MBA (Factor VIII Computing); Samantha Gouw, MD, PhD (Academic Medical Center Amsterdam and Leiden University Medical Center); Daniel Hart, BSc, MBChB, FRCP, FRCPath, PhD (The Royal London Hospital Haemophilia Centre, Barts and the London School of Medicine and Dentistry, QMUL, UK); Mohit Jain, PhD, MBA (BioMarin); James Jorgenson, RPh, MS, FASHP (Visante, Inc. & Visante Limited); Snejana Krassova, MD, MMBS (Bayer); Declan Noone, MEng (Irish Haemophilia Society); Jamie O’Hara, MSc (HC Economics, Ltd and Haemophilia Society); David Page (Canadian Hemophilia Society); Edmund Pezalla, MD, MPH, PhD (enlightenment bioconsult, LLC); Glenn F. Pierce, MD, PhD (Third Rock Ventures); Eileen Sawyer, PhD (uniQure); Clive Spiegler, PhD (Spark Therapeutics); Michelle Witkop, DNP, FNP-BC (National Hemophilia Foundation). Technical Support. Janelle King (Center for Medical Technology Policy); Julie Simmons, CMP (Center for Medical Technology Policy).

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
21
APPENDIX 2 – Literature Search Abstraction Plan
APPENDIX TWO - LITERATURE SEARCH ABSTRACTION PLAN
Targeted Literature Search Abstraction Plan
Source Timeframe for Search Search Term Outcomes Reviewed
Cochrane Reviews All available hemophilia Primary and secondary outcomes reported in the Methods section
Haemophilia journal articles
Previous 5 years of archives
N/A – all titles reviewed
1. Outcomes reported in the Methods section
2. Outcomes reported in the Results section (if required)
Clinicaltrials.gov Records first posted
in the previous 5 years
hemophilia
From the trial record:
• Current Primary Outcome Measures
• Current Secondary Outcome Measures
• Current Other Outcome Measures

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
22
APPENDIX 3 – Targeted Literature Search References
APPENDIX THREE - TARGETED LITERATURE SEARCH REFERENCES
COCHRANE REVIEWS Athale AH, Marcucci M, Iorio A. Immune tolerance induction for treating inhibitors in people with congenital haemophilia A or B. Cochrane Database of Systematic Reviews 2014, Issue 4. Art. No.: CD010561. DOI: 10.1002/14651858.CD010561.pub2. Cassis F, Emiliani F, Pasi J, Palareti L, Iorio A. Psychological interventions for people with hemophilia (Protocol). Cochrane Database of Systematic Reviews 2012, Issue 11. Art. No.: CD010215. DOI: 10.1002/14651858.CD010215. Iorio A, Marchesini E, Marcucci M, Stobart K, Chan AKC. Clotting factor concentrates given to prevent bleeding and bleeding-related complications in people with hemophilia A or B. Cochrane Database of Systematic Reviews 2011, Issue 9. Art. No.: CD003429. DOI: 10.1002/14651858.CD003429.pub4. Iorio A, Remmington T, Jahnke N, Dwan K, Hall N. Desmopressin acetate (DDAVP) for preventing and treating bleeding in people with mild or moderate haemophilia A (Protocol). Cochrane Database of Systematic Reviews 2015, Issue 12. Art. No.: CD011985. DOI: 10.1002/14651858.CD011985. Jiang L, Liu Y, Zhang L, Santoro C, Rodriguez A. Rituximab for treating inhibitors in people with inherited severe hemophilia. Cochrane Database of Systematic Reviews 2017, Issue 7. Art. No.: CD010810. DOI: 10.1002/14651858.CD010810.pub3. Matino D, Makris M, Dwan K, D'Amico R, Iorio A. Recombinant factor VIIa concentrate versus plasma-derived concentrates for treating acute bleeding episodes in people with haemophilia and inhibitors. Cochrane Database of Systematic Reviews 2015, Issue 12. Art. No.: CD004449. DOI: 10.1002/14651858.CD004449.pub4. Sharma A, Easow Mathew M, Sriganesh V, Reiss UM. Gene therapy for haemophilia. Cochrane Database of Systematic Reviews 2016, Issue 12. Art. No.: CD010822. DOI: 10.1002/14651858.CD010822.pub3. Zeng Y, Zhou R, Duan X, Long D, Yang S. Interventions for treating acute bleeding episodes in people with acquired hemophilia A. Cochrane Database of Systematic Reviews 2014, Issue 8. Art. No.: CD010761. DOI: 10.1002/14651858.CD010761.pub2. Zeng Y, Zhou R, Duan X, Long D. Rituximab for eradicating inhibitors in people with acquired haemophilia A. Cochrane Database of Systematic Reviews 2016, Issue 7. Art. No.: CD011907. DOI: 10.1002/14651858.CD011907.pub2.
JOURNAL ARTICLES Abshire TC, Brackmann HH, Scharrerr I, Hoots K, Gazengel C, Powell JS, Gorina E, Kellermann E, Vosburg E. Sucrose formulated recombinant human antihemophilic factor VIII is safe and efficacious for treatment of hemophilia A in home therapy – Internation Kogenate-FS Study Group. Thromb Haemost. 2000 June:83(6):811-6. Baumann K, Akins S, Funk S, Hernandez G, Kempton C, Wang M, Buckner T, Cooper D. Functional Impairment, Pain, and Pain Management in Us Adult People with Hemophilia (pwh): Initial Lessons from the Pain, Functional Impairment, and Quality of Life (p-fiq) Study. Haemophilia. 2015 Nov 1;21(6):e543.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
23
APPENDIX 3 – Targeted Literature Search References
Biondo F, Santoro C, Baldacci E, Leporace A, Foà R, Mazzucconi M. Different prophylaxis regimens in young severe hemophilia A patients: efficacy, Fviii consumption, and therapy compliance. Haemophilia. 2012 Mar 1;18:20. Carvalhosa AM, Henrard S, Lambert C, Hermans C. Physical and mental quality of life in adult patients with haemophilia in Belgium: the impact of financial issues. Haemophilia. 2014 Jul 1;20(4):479-85. Chowdary P, Kearney S, Regnault A, Hoxer CS, Yee DL. Improvement in health‐related quality of life in patients with haemophilia B treated with nonacog beta pegol, a new extended half‐life recombinant FIX product. Haemophilia. 2016 Jul 1;22(4). DeKoven M, Karkare S, Lee WC, Kelley LA, Cooper DL, Pham H, Powers J, Wisniewski T. Impact of haemophilia with inhibitors on caregiver burden in the United States. Haemophilia. 2014 Nov 1;20(6):822-30. Forsyth AL, Gregory M, Nugent D, Garrido C, Pilgaard T, Cooper DL, Iorio A. Haemophilia Experiences, Results and Opportunities (HERO) Study: survey methodology and population demographics. Haemophilia. 2014 Jan 1;20(1):44-51. George L, Sullivan S, Luk A, Anguela X, Teitel J, High K. Preliminary results of a phase 1/2 trial of SPK-9001, a hyperactive FIX variant delivered by a novel capsid, demonstrate consistent factor IX activity levels at the lowest dose cohort. Haemophilia. 2016 Jul 1;22(Suppl 4):151-2. Guh S, Grosse SD, McAlister S, Kessler CM, Soucie JM. Healthcare expenditures for males with haemophilia and employer‐sponsored insurance in the United States, 2008. Haemophilia. 2012 Mar 1;18(2):268-75. Guh S, Grosse SD, McAlister S, Kessler CM, Soucie JM. Health care expenditures for Medicaid‐covered males with haemophilia in the United States, 2008. Haemophilia. 2012 Mar 1;18(2):276-83. Hermans C, Klamroth R, Richards M, Moerloose P, Garrido RP. Outcome measures in European patients with haemophilia. Haemophilia. 2017 Mar 1;23(2):222-9. Hua B, Lee A, Fan L, Li K, Zhang Y, Poon MC, Zhao Y. Low‐dose factor VIII infusion in Chinese adult haemophilia A patients: pharmacokinetics evidence that daily infusion results in higher trough level than with every‐other‐day infusion with similar factor VIII consumption. Haemophilia. 2017 May 1;23(3):417-21. Jiménez‐Yuste V, Oldenburg J, Rangarajan S, Peiró‐Jordán R, Santagostino E. Long‐term outcome of haemophilia A patients after successful immune tolerance induction therapy using a single plasma‐derived FVIII/VWF product: the long‐term ITI study. Haemophilia. 2016 Nov 1;22(6):859-65.
Kachooei AR, Badiei Z, Zandinezhad ME, Ebrahimzadeh MH, Mazloumi SM, Omidi‐Kashani F, Moradi A, Mahdavian‐Naghashzargar R, Razi S. Influencing factors on the functional level of haemophilic patients assessed by FISH. Haemophilia. 2014 Mar 1;20(2):185-9.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
24
APPENDIX 3 – Targeted Literature Search References
Konkle BA, Stasyshyn O, Chowdary P, Bevan DH, Mant T, Shima M, Engl W, Dyck-Jones J, Fuerlinger M, Patrone L, Ewenstein B. Pegylated, full-length, recombinant factor VIII for prophylactic and on-demand treatment of severe hemophilia A. Blood. 2015 Aug 27;126(9):1078-85. Klamroth R, Miesbach W, Staritz P. Prospective evaluation of treatment regimens, efficacy and safety of a recombinant factor VIII concentrate in haemophilia A: the German EffeKt study. Haemophilia. 2016 Sep 1;22(5):684-91. Lalezari S, Coppola A, Lin J, Enriquez MM, Tseneklidou‐Stoeter D, Powell J, Ingerslev J. Patient characteristics that influence efficacy of prophylaxis with rFVIII‐FS three times per week: a subgroup analysis of the LIPLONG study. Haemophilia. 2014 May 1;20(3):354-61. Lissitchkov T, Hampton K, Depka M, Hay C, Rangarajan S, Tuddenham E, Holstein K, Huth‐Kühne A, Pabinger I, Knaub S, Bichler J. Novel, human cell line‐derived recombinant factor VIII (human‐cl rhFVIII; Nuwiq®) in adults with severe haemophilia A: efficacy and safety. Haemophilia. 2016 Mar 1;22(2):225-31. Martinowitz U, Lissitchkov T, Lubetsky A, Jotov G, Barazani‐Brutman T, Voigt C, Jacobs I, Wuerfel T, Santagostino E. Results of a phase I/II open‐label, safety and efficacy trial of coagulation factor IX (recombinant), albumin fusion protein in haemophilia B patients. Haemophilia. 2015 Nov 1;21(6):784-90. Mahlangu J, Powell JS, Ragni MV, Chowdary P, Josephson NC, Pabinger I, Hanabusa H, Gupta N, Kulkarni R, Fogarty P, Perry D. Phase 3 study of recombinant factor VIII Fc fusion protein in severe hemophilia A. Blood. 2014 Jan 16;123(3):317-25. Mahlangu J, Paz P, Hardtke M, Aswad F, Schroeder J. TRUST trial: BAY 86‐6150 use in haemophilia with inhibitors and assessment for immunogenicity. Haemophilia. 2016 Nov 1;22(6):873-9. Manco-Johnson MJ, Abshire TC, Shapiro AD, Riske B, Hacker MR, Kilcoyne R, Ingram JD, Manco-Johnson ML, Funk S, Jacobson L, Valentino LA. Prophylaxis versus episodic treatment to prevent joint disease in boys with severe hemophilia. New England Journal of Medicine. 2007 Aug 9;357(6):535-44. Marco A, Aznar J, Querol F, PÉrezalenda S, Jaca M, Vila C, GarcÍa-dasÍ M, Cid A, Haya S. Secondary prophylaxis in adult severe haemophilic patients: a prospective study in a single center. Haemophilia. 2012 Mar 1;18:22. Mehramiri A, Parand S, Haghpanah S, Karimi M. Attitudes of haemophilic patients towards their health and socio‐economic problems in Iran. Haemophilia. 2012 Jan 1;18(1):122-8. Miesbach W, Klamroth R, Schutgens R. Updated results from a dose escalating study in adult patients with haemophilia B treated with AMT-060 (AAV5-hFIX) gene therapy. WHF 2016, Late-Breaking Abstract. Haemophilia. 2016;22:151-2. Nathwani AC, Reiss UM, Tuddenham EG, Rosales C, Chowdary P, McIntosh J, Della Peruta M, Lheriteau E, Patel N, Raj D, Riddell A. Long-term safety and efficacy of factor IX gene therapy in hemophilia B. N Engl J Med. 2014 Nov 20;2014(371):1994-2004.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
25
APPENDIX 3 – Targeted Literature Search References
Nathwani AC, Tuddenham EG, Rangarajan S, Rosales C, McIntosh J, Linch DC, Chowdary P, Riddell A, Pie AJ, Harrington C, O'beirne J. Adenovirus-associated virus vector–mediated gene transfer in hemophilia B. New England Journal of Medicine. 2011 Dec 22;365(25):2357-65. Negrier C, Young G, Abdul Karim F, Collins PW, Hanabusa H, Colberg T, Goldman B, Walsh CE. Recombinant long‐acting glycoPEGylated factor IX (nonacog beta pegol) in haemophilia B: assessment of target joints in multinational phase 3 clinical trials. Haemophilia. 2016 Jul 1;22(4):507-13. Niu X, Poon JL, Riske B, Zhou ZY, Ullman M, Lou M, Baker J, Koerper M, Curtis R, Nichol MB. Physical activity and health outcomes in persons with haemophilia B. Haemophilia. 2014 Nov 1;20(6):814-21. Nolan B, Mahlangu J, Perry D, Young G, Liesner R, Konkle B, Rangarajan S, Brown S, Hanabusa H, Pasi KJ, Pabinger I. Long‐term safety and efficacy of recombinant factor VIII Fc fusion protein (rFVIIIFc) in subjects with haemophilia A. Haemophilia. 2016 Jan 1;22(1):72-80. Nugent D, Kalnins W, Querol F, Gregory M, Pilgaard T, Cooper DL, Iorio A. Haemophilia Experiences, Results and Opportunities (HERO) study: treatment‐related characteristics of the population. Haemophilia. 2015 Jan 1;21(1). Ozelo M, Chowdary P, Regnault A, Busk AK. Impact of severe haemophilia A on patients' health status: results from the guardian™ 1 clinical trial of turoctocog alfa (NovoEight®). Haemophilia. 2015 Jul 1;21(4):451-7. Pai M, Key NS, Skinner M, Curtis R, Feinstein M, Kessler C, Lane SJ, Makris M, Riker E, Santesso N, Soucie JM, Yeung CHT, Iorio A, Schünemann HJ. NHF-McMaster Guideline on Care Models for Haemophilia Management. Haemophilia. 2016;22: 6–16. doi: 10.1111/hae.13008 Pasi J, Wong W, Rangarajan S, Wilde J, Perry D, Madan B. Interim results of an open-label, phase 1/2 study of BMN 270, an AAV5-FVIII gene transfer in severe hemophilia A. Haemophilia. 2016 Jul 27;22(suppl 4):151-2. Poonnoose P, Carneiro JD, Cruickshank AL, El Ekiaby M, Perez Bianco RP, Ozelo MC, De Bosch N, Baghaipour M, Tien SL, Chuansumrit A, D'amico EA. Episodic replacement of clotting factor concentrates does not prevent bleeding or musculoskeletal damage–the MUSFIH study. Haemophilia. 2017 Jul 1;23(4):538-46. Powell JS, Pasi KJ, Ragni MV, Ozelo MC, Valentino LA, Mahlangu JN, Josephson NC, Perry D, Manco-Johnson MJ, Apte S, Baker RI. Phase 3 study of recombinant factor IX Fc fusion protein in hemophilia B. New England Journal of Medicine. 2013 Dec 12;369(24):2313-23. Riva S, Gringeri A, Fusco F, Mantovani L. Direct costs of children with haemophilia A undergoing prophylaxis or episodic treatment: results from the Esprit study. Haemophilia. 2012 Mar 1;18:18. Riva S, Gringeri A, Mantovani L, Mannucci PM, Von Mackensen S. Hr-qol in children with hemophilia A: results from the Esprit study. Haemophilia. 2012 Mar 1;18:29.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
26
APPENDIX 3 – Targeted Literature Search References
Saxena K, Lalezari S, Oldenburg J, Tseneklidou‐Stoeter D, Beckmann H, Yoon M, Maas Enriquez M. Efficacy and safety of BAY 81‐8973, a full‐length recombinant factor VIII: results from the LEOPOLD I trial. Haemophilia. 2016 Sep 1;22(5):706-12. Santagostino E, Lentz SR, Busk AK, Regnault A, Iorio A. Assessment of the impact of treatment on quality of life of patients with haemophilia A at different ages: insights from two clinical trials on turoctocog alfa. Haemophilia. 2014 Jul 1;20(4):527-34. Santagostino E, Martinowitz U, Lissitchkov T, Pan-Petesch B, Hanabusa H, Oldenburg J, Boggio L, Negrier C, Pabinger I, von Depka Prondzinski M, Altisent C. Long-acting recombinant coagulation factor IX albumin fusion protein (rIX-FP) in hemophilia B: results of a phase 3 trial. Blood. 2016 Apr 7;127(14):1761-9. Shapiro AD, Mahlangu JN, Perry D, Pasi J, Quon DV, Chowdary P, Tsao E, Li S, Innes A, Pierce GF, Allen GA. Treatment of bleeding episodes with recombinant factor VIII Fc fusion protein in A‐LONG study subjects with severe haemophilia A. Haemophilia. 2017 May 1;23(3):392-9. Shinkoda Y, Shirahata A, Fukutake K, Takamatsu J, Shima M, Hanabusa H, Mugishima H, Takedani H, Kawasugi K, Taki M, Matsushita T. A phase III clinical trial of a mixture agent of plasma‐derived factor VIIa and factor X (MC710) in haemophilia patients with inhibitors. Haemophilia. 2017 Jan 1;23(1):59-66. Serban M, Skotnicki AB, Colovic M, Jinca C, Klukowska A, Laguna P, Wolf DM. Clinical efficacy, safety and pharmacokinetic properties of the plasma‐derived factor IX concentrate Haemonine® in previously treated patients with severe haemophilia B. Haemophilia. 2012 Mar 1;18(2):175-81. Song CK, Quon DV, Dolan G, Recht M, Guzman-Becerra N, Epstein JD, Wong WY. Access to prophylaxis benefits hemophilia A subjects in both low and high Iu/capita countries: adult subset analysis of a multicenter, open-label, randomized, phase 4 clinical study of rahf-pfm. Haemophilia. 2012 Mar 1;18:19-20. Tiede A, Oldenburg J, Lissitchkov T, Knaub S, Bichler J, Manco‐Johnson MJ. Prophylaxis vs. on‐demand treatment with Nuwiq®(Human‐cl rhFVIII) in adults with severe haemophilia A. Haemophilia. 2016 May 1;22(3):374-80. Tuddenham EG. Gene therapy trial in severe haemophilia B-interim results. Haemophilia. 2012 Mar 1;18:10. Valentino LA, Rusen L, Elezovic I, Smith LM, Korth‐Bradley JM, Rendo P. Multicentre, randomized, open‐label study of on‐demand treatment with two prophylaxis regimens of recombinant coagulation factor IX in haemophilia B subjects. Haemophilia. 2014 May 1;20(3):398-406. Verma SP, Dutta TK, Mahadevan S, Nalini P, Basu D, Biswal N, Ramesh A, Charles D, Vinod KV, Harichandra Kumar KT. A randomized study of very low‐dose factor VIII prophylaxis in severe haemophilia–A success story from a resource limited country. Haemophilia. 2016 May 1;22(3):342-8. Windyga J, Lin VW, Epstein JD, Ito D, Xiong Y, Abbuehl BE, Ramirez JH. Improvement in health‐related quality of life with recombinant factor IX prophylaxis in severe or moderately severe haemophilia B patients: results from the BAX326 Pivotal Study. Haemophilia. 2014 May 1;20(3):362-8.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
27
APPENDIX 3 – Targeted Literature Search References
Wu R, Sun J, Xiao J, Liu Y, Xue F, Wang H, Tang L, Zhao Y, Li K, Yang R, Hu Y. A prospective study of health‐related quality of life of boys with severe haemophilia A in China: comparing on‐demand to prophylaxis treatment. Haemophilia. 2017 May 1;23(3):430-6. Wyrwich KW, Krishnan S, Auguste P, Poon JL, Maltzahn R, Yu R, Pierce GF, Mei B, Mahlangu J, Mackensen S. Changes in health‐related quality of life with treatment of longer‐acting clotting factors: results in the A‐LONG and B‐LONG clinical studies. Haemophilia. 2016 Nov 1;22(6):866-72.
CLINICALTRIALS.GOV REFERENCES NCT00037557. Study Evaluating rFIX; BeneFIX in Severe Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT000375 NCT00038935. Study Evaluating BDDRFVIII and ReFacto AF in Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00038935 NCT00108758. Efficacy of NovoSeven® in Bleeding Prophylaxis in Hemophilia. https://clinicaltrials.gov/ct2/show/NCT00108758 NCT00108797. Trial of NovoSeven® in Haemophilia - Joint Bleeds. https://clinicaltrials.gov/ct2/show/NCT00108797 NCT00141843. Study to Establish Bioequivalence of ReFacto AF (BDDrFVIII) With Advate (FLrFVIII) in Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00141843 NCT00162019. Pharmacokinetics, Efficacy and Safety Study of IMMUNATE SD (Human Plasma-Derived Coagulation Factor VIII Concentrate) in HemophiliaA Patients. https://clinicaltrials.gov/ct2/show/NCT00162019 NCT001686309. The FEIBA NovoSeven Comparative Study. https://clinicaltrials.gov/ct2/show/NCT001686309 NCT00207597. Joint Outcome Study. https://clinicaltrials.gov/ct2/show/NCT00207597. NCT00221195. Efficacy Study of Activated Prothrombin Complex for Prevention of Bleeds in Hemophilia A With Inhibitors (ProFEIBA). https://clinicaltrials.gov/ct2/show/NCT00221195. NCT00243386. Prophylaxis Study of Recombinant Factor VIII Manufactured Protein-Free (rAHF-PFM) in Patients With Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00243386 NCT00245245. Study of Recombinant Porcine Factor VIII (FVIII) in Hemophilia and Inhibitors to FVIII. https://clinicaltrials.gov/ct2/show/NCT00245245 NCT00245297. Study of the Efficacy of Human Recombinant Factor VIII (Kogenate FS) Reconstituted in Pegylated Liposomes. https://clinicaltrials.gov/ct2/show/NCT00245297

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
28
APPENDIX 3 – Targeted Literature Search References
NCT00284193. Combination Therapy of Low Doses of rFVIIa and FEIBA for Severe Hemophilia A Patients With an Inhibitor to Factor VIII. https://clinicaltrials.gov/ct2/show/NCT00284193. NCT00289536. Dose-Response Study of Recombinant Factor VIII Manufactured Protein-Free (rAHF-PFM) in Patients With Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00289536 NCT00323856. Safety Study of Alphanate in Previously Treated Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00323856 NCT00324493. Musculoskeletal Function in Hemophilia. https://clinicaltrials.gov/ct2/show/NCT00324493 NCT00331006. Rituximab to Treat Severe Hemophilia A (RICH). https://clinicaltrials.gov/ct2/show/NCT00331006 NCT00515710. LTFU for Gene Transfer Subjects With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT00515710 NCT00543439. Study Evaluating Prophylaxis Treatment & Characterizing Efficacy, Safety, & PK Of B-Domain Deleted Recombinant FVIII. https://clinicaltrials.gov/ct2/show/NCT00543439 NCT00571584. High Dose of Activated Recombinant Human Factor VII for Treatment of Mild/Moderate Joint Bleeds in Haemophilia Patients With Inhibitors. https://clinicaltrials.gov/ct2/show/NCT00571584 NCT00581126. Study Evaluating BENEFIX in Previously Treated Patients With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT00581126 NCT00586521. BAY14-2222 Prophylaxis and Joint Function Improvement (Adults). https://clinicaltrials.gov/ct2/show/NCT00586521 NCT00623480. Trial to Evaluate the Effect of Secondary Prophylaxis With rFVIII Therapy in Severe Hemophilia A Adult and/or Adolescent Subjects Compared to That of Episodic Treatment (SPINART). https://clinicaltrials.gov/ct2/show/NCT00623480 NCT00623727. BAY79-4980 Compared to rFVIII-FS in Previously Treated Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00623727 NCT00716716. Phase I/IIa Study of FIXFc in Hemophilia B Patients. https://clinicaltrials.gov/ct2/show/NCT00716716 NCT00749476. Study Evaluating BeneFIX in Patients With Haemophilia B, Previously Treated With Plasma Derived Factor IX. https://clinicaltrials.gov/ct2/show/NCT00749476 NCT00765726. Study Evaluating The Safety Of Xyntha In Usual Care Settings. https://clinicaltrials.gov/ct2/show/NCT00765726 NCT00768287. Study of Recombinant Factor IX Product, IB1001, in Subjects With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT00768287

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
29
APPENDIX 3 – Targeted Literature Search References
NCT00782470. Evaluation of the Reasons and Consequences of Bleeding in Late Teens and Early Adulthood Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00782470 NCT00837356. Comparison of the Action of Drugs in the Body and Safety of N8 and Advate® in Haemophilia A Subjects. https://clinicaltrials.gov/ct2/show/NCT00837356 NCT00840086. Safety and Efficacy of Turoctocog Alfa in Haemophilia A Subjects (guardian™1). https://clinicaltrials.gov/ct2/show/NCT00840086 NCT00851721. Efficacy and Safety Study of Prophylactic Versus On-Demand Treatment With Feiba NF in Subjects With Hemophilia A or B and a High Titer Inhibitor. https://clinicaltrials.gov/ct2/show/NCT00851721 NCT00868530. Study Evaluating On-Demand Treatment Of Xyntha In Chinese Subjects. https://clinicaltrials.gov/ct2/show/NCT00868530 NCT00874926. EFFEKT - Efficacy and Safety of Long-term Treatment With KOGENATE Bayer/FS. https://clinicaltrials.gov/ct2/show/NCT00874926 NCT00879541. Study of a pd vWF/FVIII, Biostate®, in Subjects With Haemophilia A. https://clinicaltrials.gov/ct2/show/NCT00879541 NCT008866606. Study Evaluating On-Demand Treatment With BeneFIX In Chinese Subjects. https://clinicaltrials.gov/ct2/show/NCT008866606 NCT00914459. Study Evaluating Safety And Efficacy Of Moroctocog Alfa (AF-CC) In Previously Treated Hemophilia A Patients. https://clinicaltrials.gov/ct2/show/NCT00914459 NCT00922792. Safety and Mode of Action of a Single Dose and Multiple Doses of Long Acting Activated Recombinant Human Factor VII in Patients With Haemophilia A and B. https://clinicaltrials.gov/ct2/show/NCT00922792 NCT00927667. Joint Status in Subjects With Severe Hemophilia A in Relation to Different Treatment Regimens. https://clinicaltrials.gov/ct2/show/NCT00927667 NCT009471937. Study of Ataluren (PTC124®) in Hemophilia A and B. https://clinicaltrials.gov/ct2/show/NCT009471937 NCT00950170. Study of Safety And Efficacy Of ReFacto AF In Previously Untreated Hemophilia A Patients In The Usual Care Setting. https://clinicaltrials.gov/ct2/show/NCT00950170 NCT00951405. Safety and Efficacy of 3 Different Doses of Long Acting Factor VII in Haemophilia A or B Patients With Inhibitors. https://clinicaltrials.gov/ct2/show/NCT00951405 NCT00956345. Safety of 40K Pegylated Recombinant Factor IX in Non-Bleeding Patients With Haemophilia B. https://clinicaltrials.gov/ct2/show/NCT00956345
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
30
APPENDIX 3 – Targeted Literature Search References
NCT00969319. Effekt-2 - Efficacy and Safety of Long-term Treatment With KOGENATE® FS in Latin America. https://clinicaltrials.gov/ct2/show/NCT00969319 NCT00979238. Dose-escalation study of a self complementary adeno-associated viral vector for gene transfer in hemophilia B. https://clinicaltrials.gov/ct2/show/NCT00979238 NCT00984126. Safety and Efficacy of Turoctocog Alfa (N8) in Prevention and On-demand Treatment of Bleeding Episodes in Subjects With Haemophilia A: An Extension to Trials NN7008-3543, NN7008-3545, NN7008-3600, NN7008-3893 and NN7008-4015. https://clinicaltrials.gov/ct2/show/NCT00984126 NCT00989196. Clinical Study to Investigate the Pharmacokinetics, Efficacy, Safety and Immunogenicity of a Recombinant FVIII in Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT00989196 NCT00995046. Individually Tailored Prophylaxis in Patients With Severe Hemophilia A (OPTIPHASE). https://clinicaltrials.gov/ct2/show/NCT00995046 NCT01027364. Study of recombinant factor IX Fc fusion protien (rFIXFc) in participants with hemophilia B. https://clinicaltrials.gov/ct2/show/NCT01027364 NCT01027377. Study of Recombinant Factor VIII Fc Fusion Protein (rFVIIIFc) in Subjects With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01027377 NCT01029340. Trial to Evaluate the Efficacy and Safety of a New Full Length Recombinant Human FVIII for Hemophilia A (Leopold I). https://clinicaltrials.gov/ct2/show/NCT01029340 NCT01051544. Study of First TIME Immunotolerance Induction in Severe Hemophilia A Patients With Inhibitor at High Risk of Failure: Comparison With FVIII Concentrates With or Without Von Willebrand Factor - RES.I.S.T. Naive (RESIST NAIVE). https://clinicaltrials.gov/ct2/show/NCT01051544 NCT01053715. Quality of Life Study of Helixate NexGen. https://clinicaltrials.gov/ct2/show/NCT01053715 NCT01085344. Canadian Hemophilia Prophylaxis Study (CHPS). https://clinicaltrials.gov/ct2/show/NCT01085344 NCT01125813. Efficacy and Safety Study of Human-cl rhFVIII in PTPs With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01125813 NCT01128881. IMMUNINE Pre-Treatment Study. https://clinicaltrials.gov/ct2/show/NCT01128881 NCT01159587. Prophylaxis Versus On-demand Therapy Through Economic Report (POTTER). https://clinicaltrials.gov/ct2/show/NCT01159587 NCT01174446. Pivotal Study (Pharmacokinetics, Efficacy, Safety) of BAX 326 (rFIX) in Hemophilia B Patients. https://clinicaltrials.gov/ct2/show/NCT01174446.
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
31
APPENDIX 3 – Targeted Literature Search References
NCT01178294. Study of Modified Recombinant Factor VIII (OBI-1) in Subjects With Acquired Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01178294 NCT01181128. Study to Evaluate the Safety, Pharmacokinetics and Efficacy of Recombinant Factor VIII Fc Fusion Protein (rFVIIIFc) in Previously Treated Subjects With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01181128 NCT01191372. First-in-Human and Proof-of-Mechanism Study of ARC19499 Administered to Hemophilia Patients. https://clinicaltrials.gov/ct2/show/NCT01191372 NCT01228669. Safety of NNC 0172-0000-2021 in Healthy Male Subjects and Subjects With Haemophilia A or B (Explorer 1). https://clinicaltrials.gov/ct2/show/NCT01228669 NCT01233258. A Trial to Compare Prophylaxis Therapy to On-demand Therapy With a New Full Length Recombinant FVIII in Patients With Severe Hemophilia A (Leopold II). https://clinicaltrials.gov/ct2/show/NCT01233258 NCT01233440. Safety and Pharmacokinetic Study of a Recombinant Coagulation Factor IX Albumin Fusion Protein in Subjects With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT01233440 NCT01238367. A Single Dose Trial of Recombinant Factor VIII (N8) in Japanese Subjects With Haemophilia A: An Extension to Trial NN7008-3543. https://clinicaltrials.gov/ct2/show/NCT01238367 NCT01286779. BAX 326 (rFIX) Continuation Study. https://clinicaltrials.gov/ct2/show/NCT01286779 NCT01322620. Survey Evaluating the Psychosocial Effects of Living With Haemophilia (HERO). https://clinicaltrials.gov/ct2/show/NCT01322620 NCT01333111. Safety and Efficacy of NNC-0156-0000-0009 in Haemophilia B Patients (paradigm™ 2). https://clinicaltrials.gov/ct2/show/NCT01333111 NCT01335061. Study To Compare On-Demand Treatment To A Prophylaxis Regimen Of BeneFIX In Subjects With Moderately Severe to Severe HemophiliaB. https://clinicaltrials.gov/ct2/show/NCT01335061 NCT01341912. Study to Investigate the Long-term Efficacy and Safety of Human-cl rhFVIII in Previously Treated Patients (PTPs). https://clinicaltrials.gov/ct2/show/NCT01341912 NCT01361126. A Safety and Efficacy Study of a Recombinant Factor IX in Patients With Severe Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT01361126 NCT01392547. Efficacy and Safety of NNC 0078-0000-0007 in Patients With Congenital Haemophilia and Inhibitors (adept™2). https://clinicaltrials.gov/ct2/show/NCT01392547 NCT01395810. Safety and Efficacy of NNC-0156-0000-0009 After Long-Term Exposure in Patients With Haemophilia B: An Extension to Trials NN7999-3747 and NN7999-3773 (paradigm™ 4). https://clinicaltrials.gov/ct2/show/NCT01395810

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
32
APPENDIX 3 – Targeted Literature Search References
NCT01405742. Hemophilia Adult Prophylaxis Study: Factor VIII in Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01405742 NCT01425723. Long-Term Safety and Efficacy of rFIXFc in the Prevention and Treatment of Bleeding Episodes in Previously Treated Participants With Hemophilia B (B-YOND). https://clinicaltrials.gov/ct2/show/NCT01425723 NCT01434511. Study of Modified Recombinant Factor VIII (OBI-1) in Subjects With Congenital Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01434511 NCT01454739. Long-Term Safety and Efficacy of rFVIIIFc in the Prevention and Treatment of Bleeding Episodes in Previously Treated Participants With Hemophilia A (ASPIRE). https://clinicaltrials.gov/ct2/show/NCT01454739 NCT01480180. Evaluation of Safety and Efficacy, Including Pharmacokinetics, of NNC 0129-0000-1003 When Administered for Treatment and Prophylaxis of Bleeding in Subjects With Haemophilia A (pathfinder™2). https://clinicaltrials.gov/ct2/show/NCT01480180 NCT01486927. An Open-label Safety, Efficacy and Pharmacokinetic Study of a Recombinant FVIII Compared to Recombinant Human Antihemophilic FVIII in Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01486927 NCT01496274. A Safety and Efficacy Study of a Recombinant Fusion Protein Linking Coagulation Factor IX With Albumin (rIX-FP) in Patients With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT01496274 NCT01510418. Socialization of Adult Men With Congenital Hemophilia A or B (PWBCD). https://clinicaltrials.gov/ct2/show/NCT01510418 NCT01568580. Efficacy and Safety of Recombinant Factor VIII (GreenGene) in Patients With Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01568580 NCT01580293. A Trial Investigating Safety and Efficacy of Treatment With BAY94-9027 in Severe Hemophilia A (PROTECT-VIII). https://clinicaltrials.gov/ct2/show/NCT01580293 NCT01599819. BAX 855 dose-escalation safety study. https://clinicaltrials.gov/ct2/show/NCT015998919 NCT01619046. Safety, Efficacy and Pharmacokinetics of GreenGene™ F to Previously Treated Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01619046 NCT01620801. Hemophilia B gene therapy with AAV8 Vector. https://clinicaltrials.gov/ct2/show/NCT01620801 NCT01623960. Quality of Life in Adult Patients with Severe Hemophilia in Turkey (TurkHaemQoL). https://clinicaltrials.gov/ct2/show/NCT01623960 NCT01625390. A Phase 2/ 3 Trial to Evaluate the Efficacy and Safety of BAY86-6150. https://clinicaltrials.gov/ct2/show/NCT01625390

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
33
APPENDIX 3 – Targeted Literature Search References
NCT01687608. Open-label single ascending dose of adeno-associated virus serotype 8 factor IX gene therapy in adults with hemophilia B. https://clinicaltrials.gov/ct2/show/NCT01687608 NCT01712438. Human-cl-rhFVIII in Previously Untreated Patients. https://clinicaltrials.gov/ct2/show/NCT01712438 NCT01736475. Study investigating a PEGylated recombinant factor VIII (BAX 855) for hemophilia A (PROLONG-ATE Study). https://clinicaltrials.gov/ct2/show/NCT01736475 NCT01757405. Recombinant Factor VIIa BI (rFVIIa BI) Treatment of Acute Bleeding Episodes Per an On-demand Regimen. https://clinicaltrials.gov/ct2/show/NCT01757405 NCT01800435. A Comparison Study of Bypassing Agent Therapy With and Without Tranexamic Acid in Haemophilia A Patients With Inhibitor (BPATXAS). https://clinicaltrials.gov/ct2/show/NCT01800435 NCT01817868. Comparison of Efficacy, Safety and Costs of Recombinant FVIII Products Between On-demand and Secondary Prophylaxis Groups in Haemophilia A Patients. https://clinicaltrials.gov/ct2/show/NCT01817868 NCT01863758. Assess the Safety and Efficacy of Individually Tailored Prophylaxis With Human-cl rhFVIII in Patients With Severe Haemophilia A. https://clinicaltrials.gov/ct2/show/NCT01863758 NCT01921855. Study of FVIIa Variant BAY86-6150 (B0189) in Subjects With Moderate or Severe Hemophilia Types A or B With or Without Inhibitors (MATCHBOX). https://clinicaltrials.gov/ct2/show/NCT01921855 NCT01945593. Phase 3b Continuation Study of the Safety and Efficacy of Prophylactic BAX 855 in PTPs With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT01945593 NCT01959919. Evaluation Of Acceptability And Satisfaction Of Hemophilia Patients Treated With FusENGO. https://clinicaltrials.gov/ct2/show/NCT01959919 NCT01988532. Impact of Pain on Functional Impairment and Quality of Life in Adults With Hemophilia. https://clinicaltrials.gov/ct2/show/NCT01988532 NCT01992549. Study to Investigate Immunogenicity, Efficacy and Safety of Treatment With Human-cl rhFVIII. https://clinicaltrials.gov/ct2/show/NCT01992549. NCT02020369. Phase III Study of Coagulation FVIIa (Recombinant) in Congenital Hemophilia A or B Patients With Inhibitors. https://clinicaltrials.gov/ct2/show/NCT02020369. NCT02027778. Safety and Efficacy Extension Study of GreenGene™ F in Previously Treated Patients Diagnosed With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02027778. NCT02035384. Safety and Efficacy of Turoctocog Alfa During Long-Term Treatment of Severe and Moderately Severe Haemophilia A (guardian™ 5). https://clinicaltrials.gov/ct2/show/NCT02035384.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
34
APPENDIX 3 – Targeted Literature Search References
NCT02035605. Safety and Efficacy of Turoctocog Alfa During Long-Term Treatment of Severe and Moderately Severe Haemophilia A (guardian™ 5). https://clinicaltrials.gov/ct2/show/NCT02035384. NCT02048111. Study of Recombinant Factor IX Product, IB1001, in Previously Treated Subjects With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02048111. NCT02053792. A Safety and Efficacy Extension Study of a Recombinant Fusion Protein Linking Coagulation Factor IX With Albumin (rIX-FP) in Patients With Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02053792. NCT02060305. Intra-articular Bevacizumab for Recurrent Hemarthroses at Target Joints With Chronic Hemophilic Synovitis. https://clinicaltrials.gov/ct2/show/NCT02060305. NCT02093741. ADVATE 2 mL Post-Authorization Safety Surveillance (PASS). https://clinicaltrials.gov/ct2/show/NCT02093741. NCT02137850. Safety and Efficacy of Turoctocog Alfa Pegol (N8-GP) in Previously Untreated Patients With Haemophilia A (pathfinder™6). https://clinicaltrials.gov/ct2/show/NCT02137850. NCT02141074. Safety and Efficacy of Nonacog Beta Pegol (N9-GP) in Previously Untreated Patients With Haemophilia B (paradigm™6). https://clinicaltrials.gov/ct2/show/NCT02141074. NCT02170402. China ADVATE PTP Study. https://clinicaltrials.gov/ct2/show/NCT02170402. NCT02172950. An Open-label Safety and Efficacy Study of Recombinant FVIII in Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02172950. NCT02190149. Study of Prophylaxis, ACtivity and Effectiveness (SPACE) in Hemophilia Patients Currently Treated With ADVATE or RIXUBIS (SPACE). https://clinicaltrials.gov/ct2/show/NCT02190149. NCT02191436. Adherence to Treatment in Hemophilia (ADHERENCE). https://clinicaltrials.gov/ct2/show/NCT02191436. NCT02196207. Hemophilia Inhibitor Prevention (INHIBIT) Trial (INHIBIT). https://clinicaltrials.gov/ct2/show/NCT02196207. NCT02198430. Multidisciplinary Evaluation of Patients With Hemophilia (HOLISTIC). https://clinicaltrials.gov/ct2/show/NCT02198430. NCT02207218. To Investigate Safety and Efficacy of NovoEight® (rFVIII) During Long-term Treatment of Haemophilia A in Japan. https://clinicaltrials.gov/ct2/show/NCT02207218. NCT02231944. An Open Study to Investigate the Safety and Efficacy of Replenine®-VF in Severe Haemophilia B Patients. https://clinicaltrials.gov/ct2/show/NCT02231944.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
35
APPENDIX 3 – Targeted Literature Search References
NCT02234319. Study to Determine the Safety and Efficacy of rFIXFc in Untreated Males With Severe Hemophilia B (PUPs B-LONG). https://clinicaltrials.gov/ct2/show/NCT02234319. NCT02234323. An Open Label Study to Determine the Safety and Efficacy of Replacement Factor VIII Protein (Known as rFVIIIFc) in Untreated Males With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT0223423. NCT02241694. To Quantify the Range of Main Psychosocial Factors Affecting Patients and Caregivers in Their Daily Lives (HERO). https://clinicaltrials.gov/ct2/show/NCT02241694. NCT02246868. An Open Study to Investigate the Safety and Efficacy of Optivate in Severe Haemophilia A Patients. https://clinicaltrials.gov/ct2/show/NCT02246868. NCT02256917. Assess the Efficacy and Safety of Personalized Prophylaxis Human-cl rhFVIII in Patients With Severe Haemophilia A. https://clinicaltrials.gov/ct2/show/NCT02256917. NCT02280265. Efficacy and Safety of ADVATE Standard Prophylaxis to Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02280265. NCT02282410. Evaluate Efficacy and Safety of ADVATE in the Standard Prophylaxis Treatment of Severe or Moderately Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02282410. NCT02314325. Subclinical Joint Bleeding in Irish Adults With Severe Haemophilia A on Personalised Prophylaxis Regimens (PERSONAL). https://clinicaltrials.gov/ct2/show/NCT02314325. NCT02336178. Safety and Efficacy of Benefix in Patients With Hemophilia B in Usual Care Settings in China. https://clinicaltrials.gov/ct2/show/NCT02336178. NCT02392156. Fc factOrs and Real-World hemophiliA Patient-ReporteD Outcomes (FORWARD). https://clinicaltrials.gov/ct2/show/NCT02392156. NCT02396342. Trial of AAV5-hFIX in severe or moderately severe hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02396342. NCT02396862. Patient Functioning and Well-being, Economic, and Clinical Impact of Hemophilia A and Its Treatment (ECHO). https://clinicaltrials.gov/ct2/show/NCT02396862. NCT02418793. A Study of a Long-Acting r-Factor 7a (Factor VIIa) in Adult Men With Hemophilia A or B. https://clinicaltrials.gov/ct2/show/NCT02418793. NCT02439710. Patient Reported Outcomes Burdens and Experiences - Phase 2 (PROBE). https://clinicaltrials.gov/ct2/show/NCT02439710. NCT02448680. A Phase III Study on the Safety, Pharmacokinetics and Efficacy of Coagulation Factor VIIa (PERSEPT2). https://clinicaltrials.gov/ct2/show/NCT02448680. NCT02479087. Safety/Efficacy Study to Assess Whether FVIII/VWF Concentrate Can Induce Immune Tolerance in Haemophilia A Patients (ITI). https://clinicaltrials.gov/ct2/show/NCT02479087.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
36
APPENDIX 3 – Targeted Literature Search References
NCT02484092. A gene therapy study for hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02484092. NCT02484638. Study of Recombinant Factor VIIa Fusion Protein (rVIIa-FP, CSL689) for On-demand Treatment of Bleeding Episodes in Patients With Hemophilia A or B With Inhibitors. https://clinicaltrials.gov/ct2/show/NCT02484638. NCT02490787. Trial Investigating Safety, Pharmacokinetics and Pharmacodynamics of Concizumab Administered Subcutaneously to Haemophilia A Subjects. https://clinicaltrials.gov/ct2/show/NCT02490787. NCT02492984. PF-05208756, Moroctocog Alfa (AF-CC), Xyntha For Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT0242984. NCT02502409. Natural History Study of Factor IX Treatment and Complications (B-Natural). https://clinicaltrials.gov/ct2/show/NCT02502409. NCT02546622. ATHN 2: Factor Switching Study. https://clinicaltrials.gov/ct2/show/NCT02546622. NCT02554526. Basic Study of Combination Therapy Based on APCC-induced FVllI Activation in Hemophilia A Patients With Inhibitors. https://clinicaltrials.gov/ct2/show/NCT02554526. NCT02554773. An Open-label Extension Study of an Investigational Drug, ALN-AT3SC, in Patients With Moderate or Severe Hemophilia A or B. https://clinicaltrials.gov/ct2/show/NCT02554773. NCT02568202. Bridging Hemophilia B Experiences, Results and Opportunities Into Solutions (B-HERO-S). https://clinicaltrials.gov/ct2/show/NCT02568202. NCT02569359. Efficacy and Safety of Shea Nut Oil in Hemophilic Arthropathy. https://clinicaltrials.gov/ct2/show/NCT02569359. NCT02571569. A Single Escalating Dose and Multiple Dose Study of BAY 1093884 in Subjects With Severe Hemophilia Types A or B, With or Without Inhibitors. https://clinicaltrials.gov/ct2/show/NCT02571569. NCT02576795. Gene therapy study in severe haemophilia A patients. https://clinicaltrials.gov/ct2/show/NCT02576795. NCT02581969. Extension at 10 Years of the: "Observational Study Evaluating Efficacy and Costs of Secondary Prophylaxis vs On-demand Therapy With Kogenate Bayer in Patients With Severe Haemophilia A." (POTTER 10). https://clinicaltrials.gov/ct2/show/NCT02581969. NCT02582060. Individualizing Hemophilia Prophylaxis Using Thromboelastography. https://clinicaltrials.gov/ct2/show/NCT02582060. NCT02585960. BAX 855 PK-Guided Dosing. https://clinicaltrials.gov/ct2/show/NCT02585960. NCT02601170. Platelet-Rich Plasma Intra-Articular Injection in Treating Hemophilic Arthropathy. https://clinicaltrials.gov/ct2/show/NCT02601170.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
37
APPENDIX 3 – Targeted Literature Search References
NCT02615691. BAX 855 Previously Untreated Patient (PUP). https://clinicaltrials.gov/ct2/show/NCT02615691. NCT02618915. Safety and dose finding study of DTX101 (AAVrh10FIX) in adults with moderate/severe to severe hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02618915. NCT02622321. A Study to Evaluate the Efficacy, Safety, and Pharmacokinetics of Prophylactic Emicizumab Versus no Prophylaxis in Hemophilia A Participants With Inhibitors (HAVEN 1). https://clinicaltrials.gov/ct2/show/NCT02622321. NCT02622646. Personalized Prophylactic Treatment With Advate® in Severe or Moderate Haemophilia A Patients. https://clinicaltrials.gov/ct2/show/NCT02622646. NCT02634424. PK Driven Prophylaxis for Hemophilia A (OBTC). https://clinicaltrials.gov/ct2/show/NCT02634424. NCT02674997. GAS-Hem Feasibility Study. https://clinicaltrials.gov/ct2/show/NCT02674997. NCT02695160. Ascending dose study of genome editing by zinc finger nuclearse therapeutic SB-FIX in subjects with severe hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02695160. NCT02697370. Efficacy and Cost Effectiveness of Pharmacokinetic Dosing in Haemophilia A. https://clinicaltrials.gov/ct2/show/NCT02697370. NCT02716194. BAX 826 Dose-Escalation Safety Study. https://clinicaltrials.gov/ct2/show/NCT02716194. NCT02718677. Efficacy & Safety of REFACTO AF in Prophylaxis Treatment. https://clinicaltrials.gov/ct2/show/NCT02718677. NCT02796222. Factor Product Utilization and Health Outcomes in Patients With Hemophilia. https://clinicaltrials.gov/ct2/show/NCT02796222. NCT02825706. Educational Physiotherapy in Haemophilia. https://clinicaltrials.gov/ct2/show/NCT02825706. NCT02847637. A Clinical Trial to Evaluate Prophylactic Emicizumab Versus no Prophylaxis in Hemophilia A Participants Without Inhibitors (HAVEN 3). https://clinicaltrials.gov/ct2/show/NCT02847637. NCT02866526. Determinants and Consequences of the Transition to Adulthood Among Adolescents With Haemophilia (TRANSHEMO). https://clinicaltrials.gov/ct2/show/NCT02866526. NCT02870114. National Survey of People with Haemophilia in Portugal. https://clinicaltrials.gov/ct2/show/NCT02870114. NCT02870452. Effectiveness of Psychological Interventions in Haemophilia (PSY_HaEMOPEQ). https://clinicaltrials.gov/ct2/show/NCT02870452.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
38
APPENDIX 3 – Targeted Literature Search References
NCT02908243. Outcomes of Prophylaxis and On-demand Treatment for Severe Hemophiliacs and Collection of Baseline Data in Hemophiliacs in Taiwan. https://clinicaltrials.gov/ct2/show/NCT02908243. NCT0290398. A Multi-centre, Comparative, Double Blind, Randomised Cross-over Trial Investigating Single Dose Pharmacokinetics and Safety of Turoctocog Alfa Pegol From the Pivotal Process and Turoctocog Alfa Pegol From the Commercial Process in Patients With Severe Haemophilia A (pathfinder™7). https://clinicaltrials.gov/ct2/show/NCT02920398. NCT02921945. Efficacy and Safety Study of SCT800 for On-demand Treatment With in Patients With Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02921945. NCT02930317. Evaluate Efficacy and Safety of Recombinant Factor VIII (rFVIII) Treatment of Severe or Moderately Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02930317. NCT02938585. Efficacy and Safety of Turoctocog Alfa for Prophylaxis and Treatment of Bleeding Episodes in Previously Treated Chinese Patients With Haemophilia A (guardian TM 7). https://clinicaltrials.gov/ct2/show/NCT02938585. NCT02941783. Drug Use Investigation of Kovaltry in Hemophilia A Patients. https://clinicaltrials.gov/ct2/show/NCT02941783. NCT02954575. Clinical Study to Investigate the PK, Efficacy, and Safety of Wilate in Patients With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT02954575. NCT02971969. Long-Term Safety, Tolerability, and Efficacy of DTX101 (AAVrh10FIX) in Adults With Moderate/Severe to Severe Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT02971969. NCT02974855. PF-06741086 Multiple Dose Study in Severe Hemophilia. https://clinicaltrials.gov/ct2/show/NCT02974855. NCT02976753. Prospective, Non-interventional Study to Evaluate the Effectiveness of Elocta Compared to Conventional Factor Products. https://clinicaltrials.gov/ct2/show/NCT02976753. NCT03001830. Gene Therapy for Haemophilia A. (GO-8). https://clinicaltrials.gov/ct2/show/NCT03001830. NCT03003533. A Gene Transfer Study for Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT03003533. NCT03020160. A Study to Evaluate the Efficacy, Safety, Pharmacokinetics, and Pharmacodynamics of Emicizumab Given Every 4 Weeks in Participants With Hemophilia A (HAVEN 4). https://clinicaltrials.gov/ct2/show/NCT03020160. NCT03061201. Dose-Ranging Study of Recombinant AAV2/6 Human Factor 8 Gene Therapy SB-525 in Subjects With Severe Hemophilia A. https://clinicaltrials.gov/ct2/show/NCT03061201. NCT03091751. Efficacy and Safety of AlphaNine Versus BeneFIX in Patients With Severe Hereditary Haemophilia B. https://clinicaltrials.gov/ct2/show/NCT03091751.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
39
APPENDIX 3 – Targeted Literature Search References
NCT03093480. A Study to Evaluate Efficacy of rFVIIIFc for Immune Tolerance Induction (ITI) in Severe Hemophilia A Participants With Inhibitors Undergoing the First ITI Treatment (verITI-8 Study). https://clinicaltrials.gov/ct2/show/NCT03093480. NCT03103542. Study of rFVIIIFc for ITI in Haemophilia A Patients With Inhibitors Who Have Failed Previous ITI Therapies (ReITIrate). https://clinicaltrials.gov/ct2/show/NCT03103542. NCT03154437. An Expanded Access Program of Emicizumab in Participants With Hemophilia A With Inhibitors. https://clinicaltrials.gov/ct2/show/NCT03154437. NCT03157154. Bleeding Risk Evaluation in Haemophilia Patients Under Antiplatelet Therapies (ERHEA). https://clinicaltrials.gov/ct2/show/NCT03157154. NCT03179748. Study Investigating Novoeight®/NovoEight® (Turoctocog Alfa) in Mexican Haemophilia A Patients. https://clinicaltrials.gov/ct2/show/NCT03179748. NCT03186677. Dose-escalation Study to Investigate the Safety, PK, and PD of ISU304/CB2679d in Hemophilia B Patients. https://clinicaltrials.gov/ct2/show/NCT03186677. NCT03191799. A Study to Evaluate the Safety and Tolerability of Prophylactic Emicizumab in Hemophilia A Patients With Inhibitors (STASEY). https://clinicaltrials.gov/ct2/show/NCT03191799. NCT03196284. A Trial Evaluating the Efficacy and Safety of Prophylactic Administration of Concizumab in Haemophilia A and B Patients With Inhibitors (explorer™4). https://clinicaltrials.gov/ct2/show/NCT03196284. NCT03196297. A Trial Evaluating Efficacy and Safety of Prophylactic Administration of Concizumab in Patients With Severe Haemophilia A Without Inhibitors (explorer™5). https://clinicaltrials.gov/ct2/show/NCT03196297. NCT03205163. A Safety, Tolerability, and Pharmacokinetics Study of a Single Intravenous Injection of Recombinant Coagulation Factor VIII Fc - Von Willebrand Factor - XTEN Fusion Protein (rFVIIIFc-VWF-XTEN) (BIVV001) in Previously Treated Adults With Severe Hemophilia A (EXTEN-A). https://clinicaltrials.gov/ct2/show/NCT03205163. NCT03217032. Gene Modified autoHST for Type A or B Hemophilia. https://clinicaltrials.gov/ct2/show/NCT03217032. NCT03287999. Inter Individual Variability in Initiation Pathway Activation and Regulation and Phenotypic Heterogeneity in Patients With Haemophilia A and B (InPath). https://clinicaltrials.gov/ct2/show/NCT03287999. NCT03344003. Immune Tolerance Induction in Haemophilia A Patients Using Wilate (PREVAIL). https://clinicaltrials.gov/ct2/show/NCT03344003. NCT0364182. Study Comparing On-Demand Treatment With Two Prophylaxis Regimens Of BeneFIX In Patients With Severe Hemophilia B. https://clinicaltrials.gov/ct2/show/NCT0364182.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
40
APPENDIX 3 – Targeted Literature Search References
GENE THERAPY LITERATURE Hirawat S, Welch EM, Elfring GL, Northcutt VJ, Paushkin S, Hwang S, Leonard EM, Almstead NG, Ju W, Peltz SW, Miller LL. Safety, tolerability, and pharmacokinetics of PTC124, a nonaminoglycoside nonsense mutation suppressor, following single‐and multiple‐dose administration to healthy male and female adult volunteers. The Journal of Clinical Pharmacology. 2007 Apr 1;47(4):430-44. Kerem E, Konstan MW, De Boeck K, Accurso FJ, Sermet-Gaudelus I, Wilschanski M, Elborn JS, Melotti P, Bronsveld I, Fajac I, Malfroot A. Ataluren for the treatment of nonsense-mutation cystic fibrosis: a randomised, double-blind, placebo-controlled phase 3 trial. The Lancet Respiratory Medicine. 2014 Jul 1;2(7):539-47. NCT00803205. Study of Ataluren (PTC124) in Cystic Fibrosis https://clinicaltrials.gov/ct2/show/NCT00803205. NCT00847379. Phase 2b Extension Study of Ataluren (PTC124) in Duchenne/Becker Muscular Dystrophy (DMD/BMD). https://clinicaltrials.gov/ct2/show/NCT00847379. Welch EM, Barton ER, Zhuo J, Tomizawa Y, Friesen WJ, Trifillis P, Paushkin S, Patel M, Trotta CR, Hwang S, Wilde RG. PTC124 targets genetic disorders caused by nonsense mutations. Nature. 2007 May;447(7140):87.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
41
APPENDIX 4 – Participant and Patient Interviews
APPENDIX FOUR – PARTICIPANT AND PATIENT INTERVIEWS
Interviewee Date of Interview
Location of Interview
Randall Curtis, MBA Member Board of Directors Hemophilia Council of California Co-Investigator Patient Reported Outcomes, Burdens, and Experiences (PROBE) Study
August 24, 2017 NHF’s 69th Annual Meeting Chicago, USA
Samantha Gouw, MD, PhD Pediatric Hematologist Academic Medical Center Amsterdam Clinical Epidemiologist Leiden University Medical Center
July 12, 2017 ISTH XXVI Congress Berlin, Germany
Daniel Hart, MD, PhD Senior Lecturer/Honorary Consultant Haematologist Barts and the London School of Medicine and Dentistry
July 10, 2017 ISTH XXVI Congress Berlin, Germany
Mohit Jain, PhD, MBA Executive Director, Market Access EUMEA BioMarin
July 11, 2017 ISTH XXVI Congress Berlin, Germany
James Jorgenson, RPh, MS, FASHP Chief Executive Officer & Chairman of the Board Visante, Inc. & Visante Limited
August 25, 2017 NHF’s 69th Annual Meeting, Chicago, USA
Snejana Krassova, MD, MMBS VP, Head of Medical Affairs Therapeutic Area Hematology Bayer
July 11, 2017 ISTH XXVI Congress, Berlin, Germany
Declan Noone, MEng, MSc Project Coordinator, PARTNERS Programme European Haemophilia Consortium Health Economist HCD Economics
August 24, 2017 NHF’s 69th Annual Meeting, Chicago, USA
Jamie O’Hara, MSc Trustee Haemophilia Society Director HCD Economics Ltd
August 25, 2017 NHF’s 69th Annual Meeting, Chicago, USA
Brian O’Mahony, FACSLM, FIBMS Chief Executive Irish Haemophilia Society, Ltd President European Haemophilia Consortium
August 2, 2017 Phone interview
David Page August 29, 2017 Phone interview

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
42
APPENDIX 4 – Participant and Patient Interviews
National Executive Director Canadian Hemophilia Society
Edmund Pezalla, MD, MPH, PhD Subject Matter Expert Formerly with Aetna Consultant and CEO Enlightenment bioconsult, LLC
August 25, 2017 NHF’s 69th Annual Meeting, Chicago, USA
Glenn Pierce, MD, PhD Entrepreneur in Residence Third Rock Ventures
July 10, 2017 ISTH XXVI Congress, Berlin, Germany
Eileen Sawyer, PhD Director, Global Medical Affairs uniQure
August 25, 2017 NHF’s 69th Annual Meeting, Chicago, USA
Clive Spiegler, PhD Head of Portfolio & New Product Planning Spark Therapeutics
July 10, 2017 ISTH XXVI Congress, Berlin, Germany
Michelle Witkop, DNP, FNP-BC Head of Research National Hemophilia Foundation (NHF)
August 25, 2017 NHF’s 69th Annual Meeting, Chicago, USA

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
43
APPENDIX 5 – Interview Questions
APPENDIX FIVE – INTERVIEW QUESTIONS
• For patients: Are there any health indicators (outcomes) related to your hemophilia that you regularly keep track of for yourself that your doctor does not ask about?
• Thinking of your ideal core outcome set for gene therapy in hemophilia, what type of balance would you want to have between hemophilia-specific outcomes (such as circulating factor VIII or IX levels) and gene-therapy specific outcomes (such as immune system reactions)?
• What is the most important outcome to you when you hear about a trial of a new treatment for hemophilia? (What results do you look at first in a study report/what do you ask the doctor about first when he/she recommends a new treatment?)
• Do you think the thresholds of “treatment success” will be different for gene therapy compared with conventional treatment? (right now, the goal is trough levels of 1% - would you want higher?)
o Related: Will “treatment success” be defined by a different measure in gene therapy than it has been before?
• How do you think outcomes that will be measured in gene therapy studies will differ from outcomes measured in other intervention trials?
• Will some outcomes that are measured today be no longer relevant in gene therapy trials?
• In what ways do you imagine that gene therapy might improve patient quality of life and function compared to current therapies?
• Why are some outcomes used more than others? What prevents certain outcomes from being more widely used? What needs to be done to promote greater use of a set of core outcomes across hemophilia trials?

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
44
APPENDIX 6 – Initial Outcome List Mapped to COMET Taxonomy
APPENDIX SIX- INTIAL OUTCOME LIST FOR VOTING MAPPED TO COMET TAXONOMY
coreHEM Domains COMET Categories (mapped list)
ADVERSE EVENTS
Short Term --
Infusion site reactions Adverse events/effects
Liver toxicity Adverse events/effects
Immune response to FVIII/FIX (inhibitor development) Adverse events/effects OR Immune system outcomes
Immune response to gene therapy Adverse events/effects OR Immune system outcomes
Germline transmission (vector shedding) Adverse events/effects
Long Term --
Vector integration into host genome Adverse events/effects
Development of unusual disorders (auto-immune diseases/cancers/etc.) Adverse events/effects
Immune response to FVIII/FIX (inhibitor development) Adverse events/effects OR Immune system outcomes
MORTALITY
Cause of death Mortality/survival
Age of death Mortality/survival
PHYSIOLOGIAL/CLINICAL
Frequency of bleeds Physiological/clinical – Blood and lymphatic system outcomes
Severity of bleeds Physiological/clinical – Blood and lymphatic system outcomes
Factor activity level Physiological/clinical – Blood and lymphatic system outcomes
Duration of factor expression Physiological/clinical – Blood and lymphatic system outcomes
PHYSIOLOGICAL/CLINICAL: PAIN/DISCOMFORT
Acute pain (including frequency/intensity/duration/character) Physiological/clinical - Musculoskeletal and connective tissue outcomes
Interference of acute pain on daily life/activities of daily living (e.g. walking, lifting a full glass of water, sexual activity, etc)
Functioning – Physical functioning
Chronic pain (including frequency/intensity/duration/character) Physiological/clinical - Musculoskeletal and connective tissue outcomes

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
45
APPENDIX 6 – Initial Outcome List Mapped to COMET Taxonomy
Interference of chronic pain on daily life/activities of daily living (e.g. walking, lifting a full glass of water, sexual activity, etc)
Functioning – Physical functioning
EMOTIONAL FUNCTIONING: WELL-BEING
Mental health (including anxiety/depression/coping/worry) Functioning – Emotional functioning/wellbeing
Vitality/tiredness/fatigue Functioning – Emotional functioning/wellbeing
Contentment/happiness/elation/exhilaration (mood) Functioning – Emotional functioning/wellbeing
SOCIAL FUNCTIONING
Identify as a person with hemophilia (including disclosure) Perceived health status OR Functioning – Social functioning
Sense of belonging to a community Functioning – Social functioning
Feeling of inequality compared to peers Functioning – Social functioning AND Functioning – Physical functioning AND Perceived health status
Sexual intimacy Functioning – Social functioning
PHYSICAL FUNCITIONING
Duration, frequency, intensity of physical activity/sports/play Functioning – Physical functioning
Sexual activity Functioning – Physical functioning
Mobility (including use of mobility aids) Functioning – Physical functioning
Target joints Physiological/clinical - Musculoskeletal and connective tissue outcomes
Joint function Physiological/clinical - Musculoskeletal and connective tissue outcomes
ROLE FUNCTIONING
Independence Functioning – Physical functioning AND Global quality of life
Education (School) --
Education attainment/achievement (absenteeism, grades) Functioning – Role functioning
Education choice (where to go to school, decisions regarding field of study) Personal circumstance
Employment (Work) --
Career choice (location, type of work, taking a job because it supplies insurance) Personal circumstance
Work absenteeism Functioning – Role functioning
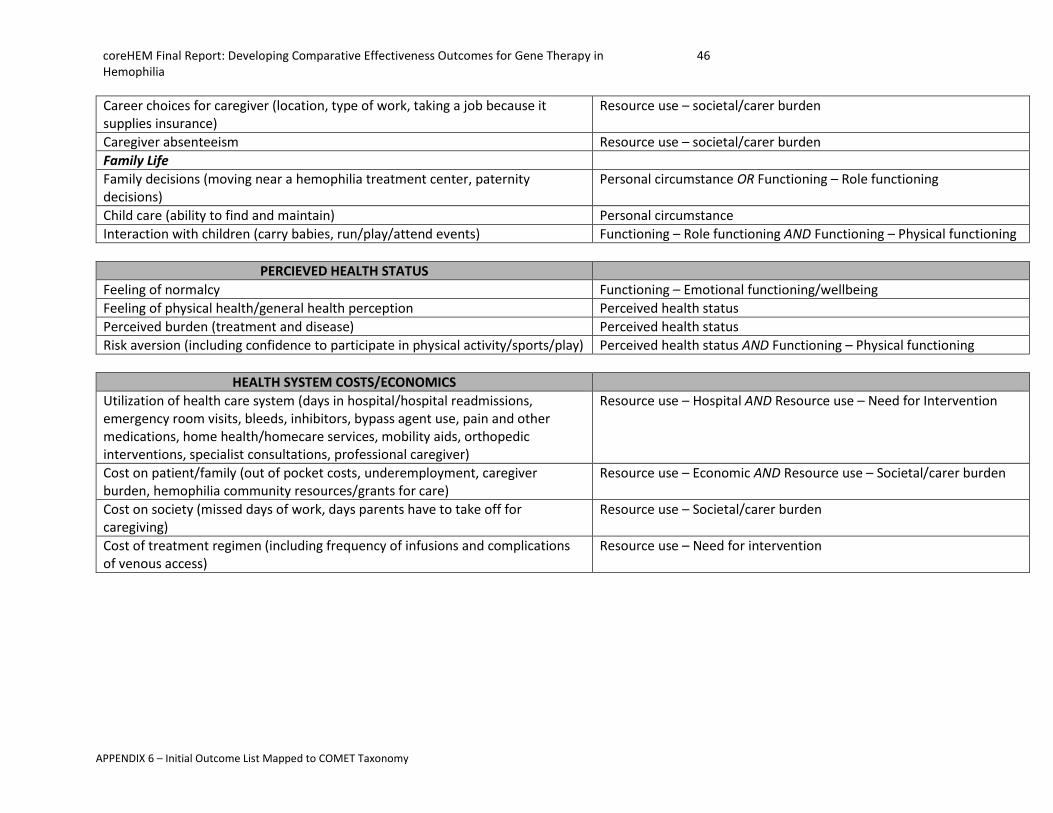
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
46
APPENDIX 6 – Initial Outcome List Mapped to COMET Taxonomy
Career choices for caregiver (location, type of work, taking a job because it supplies insurance)
Resource use – societal/carer burden
Caregiver absenteeism Resource use – societal/carer burden
Family Life
Family decisions (moving near a hemophilia treatment center, paternity decisions)
Personal circumstance OR Functioning – Role functioning
Child care (ability to find and maintain) Personal circumstance
Interaction with children (carry babies, run/play/attend events) Functioning – Role functioning AND Functioning – Physical functioning
PERCIEVED HEALTH STATUS
Feeling of normalcy Functioning – Emotional functioning/wellbeing
Feeling of physical health/general health perception Perceived health status
Perceived burden (treatment and disease) Perceived health status
Risk aversion (including confidence to participate in physical activity/sports/play) Perceived health status AND Functioning – Physical functioning
HEALTH SYSTEM COSTS/ECONOMICS
Utilization of health care system (days in hospital/hospital readmissions, emergency room visits, bleeds, inhibitors, bypass agent use, pain and other medications, home health/homecare services, mobility aids, orthopedic interventions, specialist consultations, professional caregiver)
Resource use – Hospital AND Resource use – Need for Intervention
Cost on patient/family (out of pocket costs, underemployment, caregiver burden, hemophilia community resources/grants for care)
Resource use – Economic AND Resource use – Societal/carer burden
Cost on society (missed days of work, days parents have to take off for caregiving)
Resource use – Societal/carer burden
Cost of treatment regimen (including frequency of infusions and complications of venous access)
Resource use – Need for intervention

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
47
APPENDIX 7 – Delphi Voting Reference Document
APPENDIX SEVEN – DELPHI VOTING REFERENCE DOCUMENT
DELPHI ROUND 1 REFERENCE DOCUMENT
BACKGROUND
PROJECT GOAL Determine a set of clearly defined, “core set” of outcomes to measure, demonstrate and differentiate the effectiveness and value of gene therapy in hemophilia.
DEFINITIONS These following definitions are adapted from the Core Outcome Measures in Effectiveness Trials (COMET) Initiative. The COMET Initiative brings together researchers interested in the development and application of core outcome sets.3
• Core outcome set – An agreed standardized collection of outcomes which should be measured and reported, as a minimum, in all trial for a specific clinical area or of a specific condition4
• Domain - A domain is a broad category, an element of a person’s overall health and life in relation to their treatment (for example, mobility/physical functioning)
• Outcomes - Each domain contains one or more outcomes, which are the “what” we want to measure. Within the mobility/physical functioning domain, an example of an outcome might be joint impairment.
• Measurements or Instruments - Each outcome can be measured using measurements or instruments – the “how” something is measured. A measurement/instrument is a tool to measure an outcome. The tool can be a single question, a questionnaire with a composite score, a score obtained through physical examination, laboratory measurement, or observation of an image.5 In our example, there are several measurements or instruments to assess joint impairment e.g. X-Ray Petterssen score, change in range of motion, Hemophilia Joint Health Score (HJHS).
PURPOSE We are conducting the survey now because gene therapy represents a pivotal moment in therapeutics for hemophilia. For the first time, patients may have an opportunity not merely to manage their condition, but to cure it.
3 http://www.comet-initiative.org/about/overview 4 Williamson , PR. "Developing core outcome sets for clinical trials: issues to consider." Trials 2012, 13:132. 5 http://www.comet-initiative.org/glossary/cos/
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
48
APPENDIX 7 – Delphi Voting Reference Document
Historically, the clinical standards, measures, and concepts used in hemophilia clinical trials have been designed to assess disease management. These standards, measures, and concepts must now be updated to reflect a new generation of potentially curative therapies and the dramatic benefits they offer to patients over existing treatments. The Delphi exercise is therefore designed to survey experts and stakeholders in the hemophilia community on a CORE SET of outcomes that should be measured in gene therapy clinical trials for interventions in hemophilia. Note that specifying a core set does not prevent study designers from adding measures, as appropriate; it “sets a floor, not a ceiling,” for outcomes. We will address the adequacy of measures/instruments for outcomes judged most important in a later stage of this exercise.
INSTRUCTIONS FOR VOTING In the survey, we will ask you to rate the importance of DOMAINS and OUTCOMES as core outcomes in gene therapy clinical trials for hemophilia. On each page, you will see a scale that ranges from 1 to 9. For this survey, a higher number is equal to higher importance to be included in a core outcome set. The number you select should be based on how important you think each outcome is to be included in the core set:
• Numbers 1-3 should be selected if you feel that the outcome we are asking you about an
outcome that is not important to be included in the core set
• Numbers 4-6 indicate that the outcomes are important but not critical to include in a core set
• Numbers 7-9 indicate that the outcomes are critical to include in a core set
Your assessment of importance:
• should be based on what you believe will be the most valuable information for decision-makers:
regulatory approval, care decisions by patients and providers, coverage and reimbursement
decisions
• should consider new risks and benefits not previously seen in older generations of treatments
• should not consider whether adequate and well validated measures currently exist
This reference document provides further detail about the outcomes included in the coreHEM Delphi Round 1 survey. As you work through the survey, you may refer to this document for descriptions of the outcomes that are listed.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
49
APPENDIX 7 – Delphi Voting Reference Document
OVERVIEW OF THE DOCUMENT The order of the outcomes here parallels the order of the outcomes presented in the online survey. You may refer to this document and use the information provided to assist in your rating of importance for each outcome.
ROUND 1 GUIDANCE For the first round of the Delphi voting, we will only be asking about domains and outcomes. After the panel has voted on the outcomes, or “what” to measure, we will then ask about the measures/instruments, or “how” we will measure, in a later round. Think about the outcomes you think should be included in our core outcome set. We want to know if the outcomes are important regardless of whether there are already “good” measures or instruments to report on the outcome.
HOW THIS DOCUMENT IN STRUCTURED For each outcome we will ask you about, we provide a brief description of what it is/what it measures. Structure
DOMAIN NAME: The domain category
Outcome name: A brief description of the outcome. Sample
DOMAIN: PHYSICAL FUNCTIONING
Joint function: how well one can move, flex and bend (their range of motion), or any impairment, weakening or damage, including functional loss and pain to the points of the body where bones meet (for example, shoulders, knees and elbows)

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
50
APPENDIX 7 – Delphi Voting Reference Document
DOMAIN: ADVERSE EVENTS Adverse event outcomes are safety outcomes, or measures of how safe a certain treatment is. Adverse events are undesired health problems or experiences associated with the use of a medical product, in this scenario, gene therapy. Adverse events may occur quickly after treatment or may take many years to develop. We have divided the adverse events into those which happen within one year after gene therapy and those which happen beyond one year after gene therapy.
SHORT TERM (UP TO 12 MONTHS) Infusion reactions: response to infusion of gene therapy product, including pain, swelling, or itching at
the injection site Liver toxicity: gene therapy products are targeted to enter liver cells; liver toxicity, measured by
elevated liver enzymes, may occur Immune response to FVIII/FIX (Inhibitor development): when the gene for the missing clotting factor
(FVIII or FIX) is inserted into the cell, it is possible that the body may not recognize FVIII or the FIX that the cells are now producing and will initiate an immune response against it; if the body develops antibodies against the FVIII/FIX, it is called an inhibitor (patients with inhibitors may require special and expensive treatments for bleeds that can bypass the immune response against the needed clotting factor)
Immune response to gene therapy: when gene therapy is administered, the patient’s body may mount
an immune response against elements of the product injected (antibodies against the viral vector, gene therapy vector capsid-specific T cells, etc.)
Germline transmission (vector shedding): the virus/vector spread within the body and excretion outside
of the body (in blood, saliva, urine, stool, semen, nasal secretions, feces) could be a potential public health concern if there is human to human transmission
LONG TERM (BEYOND 12 MONTHS) Vector integration into host genome: the DNA of the virus becomes integrated into the human cells,
potentially altering the expression of the genes or causing other genes to become inactivated Development of other disorders: development of serious medical problems associated with gene
therapy such as auto-immune diseases or cancer Immune response to FVIII/FIX (Inhibitor development): when the gene for the missing clotting factor
(FVIII or FIX) is inserted into the cell, it is possible that the body may not recognize FVIII or the FIX that the cells are now producing and will initiate an immune response against it; if the body develops antibodies against the FVIII/FIX, it is called an inhibitor

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
51
APPENDIX 7 – Delphi Voting Reference Document
DOMAIN: MORTALITY (SURVIVAL) Cause of death: official determination of the reason for a patient’s death Age of death: the age at which a person dies
DOMAIN: PHYSIOLOGICAL/CLINICAL
Frequency of bleeds: how often a person with hemophilia experiences a bleed (an example measure is
the annualized bleed rate, ABR) Severity of bleeds: the seriousness/intensity of a bleed (joint bleeds, muscle bleeds, intracranial hemorrhage, whether a bleed requires treatment with FVIII/FIX and how much) Factor activity level and duration of expression: the amount of clotting factor in the blood, measured as
a percentage, and how long after gene therapy that level lasts (normal clotting factor activity is described as 100 percent, though anywhere in the range of 50 to 150 percent is considered normal; for people with hemophilia A, the activity level of Factor VIII (FVIII) would be measured, and for people with hemophilia B, the activity level of Factor IX (FIX) would be measured)
DOMAIN: PAIN/DISCOMFORT
Acute pain: the presence of sharp but limited pain related with tissue damage including the frequency,
intensity, duration and character of the pain Interference of acute pain on daily life/activities of daily living: the influence of acute pain on a
person’s ability to go throughout their day for example, walking, lifting a full glass of water, sexual activity, etc.
Chronic pain: the presence of persistent pain that can last for a long time including the frequency,
intensity, duration and character of the pain Interference of chronic pain on daily life/activities of daily living: the influence of chronic pain on a
person’s ability to go throughout their day for example, walking, lifting a full glass of water, sexual activity, etc.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
52
APPENDIX 7 – Delphi Voting Reference Document
DOMAIN: EMOTIONAL FUNCTIONING: WELL-BEING Emotional functioning assesses how gene therapy for hemophilia and having hemophilia impacts a person’s emotions and well-being. These outcomes measure a person’s satisfaction in life and how they feel about themselves and their disease.
Mental health (including anxiety/depression/coping/worry): a person’s psychological condition;
whether a person feels anxiety or depression about having and living with hemophilia, how they cope with the disease and the psychological elements of having a lifelong illness, how much they worry about their condition
Vitality/tiredness/fatigue: how full of life a person feels, and enthusiasm for living; may be associated
with level of tiredness and fatigue Contentment/happiness/elation/exhilaration (mood): a person’s mood and attitudes toward their
decision to receive gene therapy treatment
DOMAIN: SOCIAL FUNCTIONING Social functioning assesses how gene therapy for hemophilia and having hemophilia impacts a person’s social health, such as their ability to have a social life, and companions, if desired, and their behavior and participation in social situations.
Identifying as a person with hemophilia (disclosure): the experience of revealing hemophilia status to
others Sense of belonging in a community: the feeling of being part of the hemophilia community, and having
shared experiences with others who have hemophilia Feeling of inequality compared to peers: envy or sadness about inability to do certain activities (for
example, participate in an extreme sport) due to having hemophilia Sexual intimacy: relating to romantic relationships, the confidence and level of comfort to get close to a
person and pursue romantic/sexual relationships
DOMAIN: PHYSICAL FUNCTIONING Physical functioning outcomes measure how well a person with hemophilia can perform the physical requirements throughout daily life.
Duration, frequency, intensity and type of physical activity/sports/play: characterization of the
physical activity that a person can comfortably do, how long and how often they can do it and how much effort it requires (physical activity may include exercise, or general activities that have a physical element such as gardening, dancing, cleaning)
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
53
APPENDIX 7 – Delphi Voting Reference Document
Sexual activity: a person’s ability to engage in the physical aspect of sex Mobility: a person’s ability to move, including the use of mobility aids such as a wheelchair, a walker,
canes and crutches Target joints: joints that bleed often; this could be a measure of the presence of, the number of, or
changes in target joints Joint function: how well one can move, flex and bend (their range of motion), or any impairment,
weakening or damage, including functional loss and pain to the points of the body where bones meet (for example, shoulders, knees and elbows)
DOMAIN: ROLE FUNCTIONING Role functioning describes the impact of hemophilia on a person’s ability to fulfil the roles of their life, in their education and career, and to perform roles as a family member and a member of society.
Independence: including a person’s ability to go about their daily life and perform the activities of self-
care without or with minimal assistance, a person’s confidence in being able to have financial and job security, and to know how to treat their hemophilia
EDUCATION (SCHOOL) Education attainment/achievement: the ability to receive an education, including absenteeism from
school, grades and academic achievement Education choice: decisions about school including where to attend college/university (need to be close
to a hemophilia treatment center?), regarding field of study (choosing to major in a field that has sedentary/non-physical jobs), etc.
EMPLOYMENT (WORK) Career choice: for a person with hemophilia, decisions made about employment including choosing a
career due to physical restrictions, or within a career field, and type of desk job over physical work, the location of the chosen career and taking a job because it provides health insurance (rather than starting a private business, for example)
Work absenteeism: missed days/time from work associated with aspects of having and/or treating
hemophilia Career choice for caregiver: employment decisions made by a caregiver such as taking a job for health
insurance benefits for the family, choosing not working in order to be a primary caretaker for a person with hemophilia, choosing a job in a certain location or with flexible hours
Caregiver absenteeism: missed days/time from work of a parent or caregiver to take care of a person
with hemophilia

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
54
APPENDIX 7 – Delphi Voting Reference Document
FAMILY LIFE Family decisions: choices made to accommodate a person with hemophilia that affect family life, such
as moving to a certain area to be near a hemophilia treatment center and paternity decisions Child care: ability to find and maintain care for a child with hemophilia Interact with children: the ability for a parent with hemophilia to engage in interactions with children
that involve movement and physical activity, such as carrying a baby, getting down to the floor to play with toys, or run and play outside
DOMAIN: PERCEIVED HEALTH STATUS This domain includes outcomes that are associated with a person’s view on their disease and their opinions about their health status.
Feeling of normalcy: the feeling of being able to live a life that is perceived as “normal,” based on a
person’s individual description of normal Feeling of physical health/general health perception: how a person with hemophilia feels about their
overall state of health Perceived burden (treatment and disease): the feeling of the amount of work and effort a person with
hemophilia must put into maintaining their treatment regimen and live with the disease Risk aversion: decisions made by a person with hemophilia to pursue or avoid certain activities based on
current health and expected requirements/results of participating in that activity (including confidence to participate in physical activity/sports/play)
DOMAIN: RESOURCE USE Resource use refers to the costs associated with treatment and with living as a person with hemophilia. This can mean economic costs, the use of resources at a hospital or associated with medical treatment, and the burden on the patient, the patient’s family and on society. Utilization of health care system: measures of uses and related costs incurred from the need of
healthcare and treatment associated with hemophilia, including days in hospital, hospital readmissions, emergency room visits, bleeds, inhibitors, bypass agent use, pain and other medications, home health/homecare services, mobility aids, orthopedic interventions, specialist consultations, and professional caregivers
Cost on patient/family: out of pocket costs to the patient and the family that are not covered by health
insurance or not included in healthcare costs such as paying for specialists beyond the allowed number of visits, paying for products that are needed due to complications of hemophilia (such as custom orthotics), underemployment (taking a lower-paying job because of flexible schedules or

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
55
APPENDIX 7 – Delphi Voting Reference Document
type of insurance provided), caregiver burden, and access to hemophilia community resources/grants for care
Cost on society: the burden of costs to the community around the person with hemophilia, such as
missed days of work/days parents have to take off for caregiving, productivity levels associated with missing work, costs of premiums of others in insurance pools
Cost of treatment regimen: costs of products needed to maintain health, including frequency of
infusions and complications of venous access

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
56
APPENDIX 8 Delphi Round 1 Results
APPENDIX EIGHT – DELPHI ROUND ONE RESULTS
coreHEM DELPHI ROUND 1 RESULTS OCTOBER 9, 2017

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
57
APPENDIX 8 Delphi Round 1 Results
coreHEM Delphi Round 1 Results Scored 1-3 (%) Scored 4-6 (%) Scored 7-9 (%) Patient Average Decision
DOMAIN: Short Term Adverse Events (<12 months) Infusion site reaction 35 45 18 4.4 Eliminate Liver toxicity 0 6 92 8.6 Retain Immune response to FVIII/FIX (inhibitor development) 0 8 90 9.0 Retain Immune response to gene therapy 2 10 86 8.2 Retain Germline transmission (vector shedding) 14 20 57 8.0 Retain (patient-important)
DOMAIN: Long Term Adverse Events (beyond 12 months) Vector integration into host genome 4 18 71 8.0 Retain Development of other disorders (auto-immune diseases/cancers/etc.)
4 8 86 8.2 Retain
Immune response to FVIII/FIX (inhibitor development) 0 12 86 9.0 Retain
DOMAIN: Mortality Cause of death 8 6 84 7.4 Retain Age of death 10 22 63 5.4 Eliminate
DOMAIN: Physiological/Clinical Frequency of bleeds 0 8 92 7.6 Retain Severity of bleeds 4 18 78 5.8 Retain Factor activity level 2 14 84 8.8 Retain Duration of expression 4 10 84 8.8 Retain
DOMAIN: Pain/Discomfort Acute pain (including frequency/intensity/duration/character) 8 41 49 7.0 Retain (patient-important) Interference of acute pain on daily life/activities of daily living 4 29 65 6.6 Eliminate Chronic pain (including frequency/intensity/duration/character) 6 33 59 7.6 Retain (patient-important) Interference of chronic pain on daily life/activities of daily living 2 22 74 7.2 Retain (patient-important)
DOMAIN: Emotional Functioning Mental health (e.g. anxiety/depression/coping/worry) 6 37 55 7.4 Retain (patient-important) Vitality/tiredness/fatigue 10 43 45 6.4 Eliminate Mood (e.g. contentment/happiness/elation/exhilaration) 14 49 35 6.4 Eliminate
DOMAIN: Social Functioning Identifying as a person with hemophilia (disclosure) 29 51 14 4.0 Eliminate

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
58
APPENDIX 8 Delphi Round 1 Results
Sense of belonging to a community 37 49 8 4.2 Eliminate Feeling of inequality compared to peers 22 45 27 4.2 Eliminate Romantic relationships 27 37 35 4.2 Eliminate
DOMAIN: Physical Functioning Duration, frequency, intensity and type of physical activity/sports/play
4 31 63 6.4 Eliminate
Sexual activity 16 37 45 5.6 Eliminate Mobility (including use of mobility aids) 2 18 78 8.0 Retain Target joints 4 31 61 8.0 Retain (patient-important) Joint function 4 20 74 7.8 Retain
DOMAIN: Role Functioning Independence 6 12 80 6.6 Retain Education attainment/achievement 20 33 43 5.2 Eliminate Education choice 33 41 22 5.0 Eliminate Career choice for patient (location/type of work/insurance) 20 35 41 5.2 Eliminate Patient work absenteeism 6 22 69 7.4 Retain (patient-important) Caregiver career choice (location, type of work, taking a job because it supplies insurance)
29 41 29 5.2 Eliminate
Caregiver work absenteeism 14 31 53 7.0 Retain (patient-important) Family decisions (moving near a hemophilia treatment center, paternity decisions)
29 47 22 5.0 Eliminate
Childcare (ability to find and maintain) 31 47 20 4.6 Eliminate Interaction with children (carry babies, run/play) 20 39 39 5.8 Eliminate
DOMAIN: Perceived Health Status Feeling of normalcy 8 37 53 7.0 Retain (patient-important) Feeling of physical health/general health perception 6 27 65 6.8 Eliminate Perceived burden (treatment and disease) 6 37 55 6.6 Eliminate Risk aversion (including confidence to participate in physical activity/sports/play)
12 33 53 6.2 Eliminate
DOMAIN: Resource Use Utilization of health care system 0 29 71 8.0 Retain Cost to patient/family 4 29 67 8.0 Retain (patient-important) Burden of treatment regimen on patient/family 2 18 80 8.4 Retain Societal costs 6 31 63 7.0 Retain (patient-important)

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
59
APPENDIX 8 Delphi Round 1 Results
SHORT TERM ADVERSE EVENTS - Infusion site reactions
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Infusion Site Reaction
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Infusion Site Reaction
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Infusion Site Reaction
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
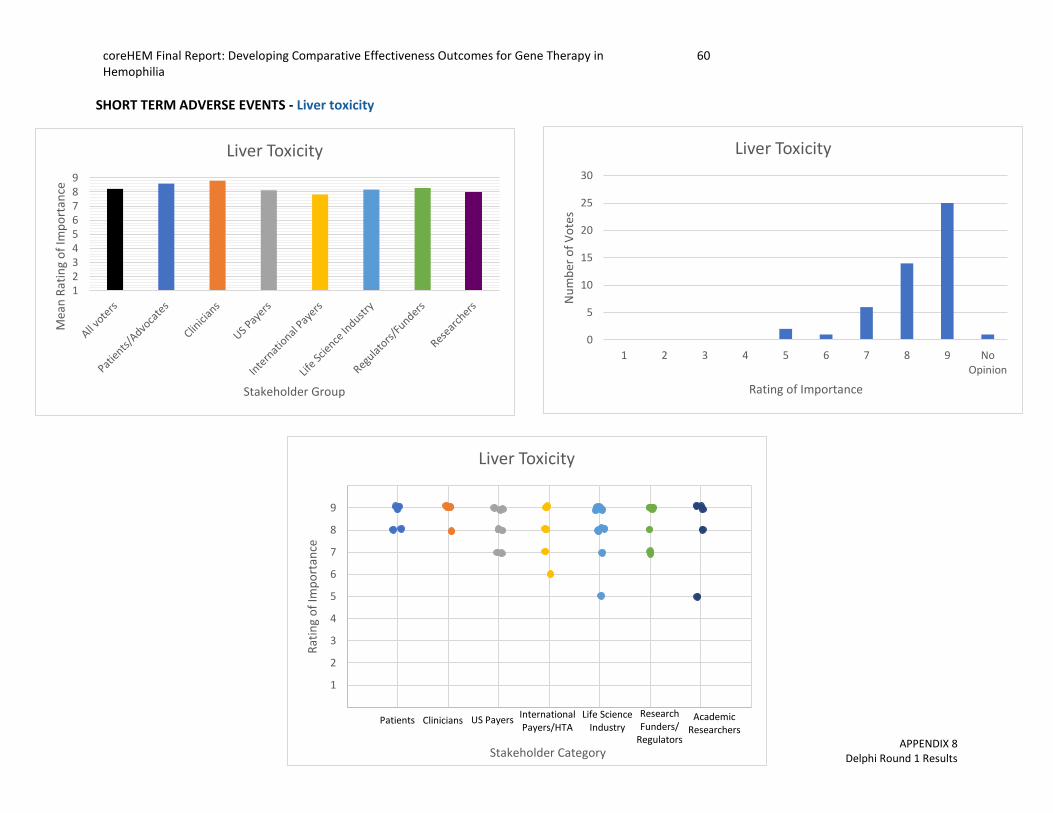
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
60
APPENDIX 8 Delphi Round 1 Results
SHORT TERM ADVERSE EVENTS - Liver toxicity
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Liver Toxicity
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Liver Toxicity
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Liver Toxicity
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
61
APPENDIX 8 Delphi Round 1 Results
SHORT TERM ADVERSE EVENTS - Immune response to FVIII/FIX (Inhibitor development)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Immune Response to FVIII/FIX(Inhibitor development)
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Immune Response to FVIII/FIX(Inhibitor development)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Immune Response to FVIII/FIX(Inhibitor development)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
62
APPENDIX 8 Delphi Round 1 Results
SHORT TERM ADVERSE EVENTS - Immune response to gene therapy
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Immune Response to Gene Therapy
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Immune Response to Gene Therapy
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Immune Response to Gene Therapy
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
63
APPENDIX 8 Delphi Round 1 Results
SHORT TERM ADVERSE EVENTS - Germline transmission/vector shedding
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Germline Transmission/Vector Shedding
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Germline transmission/Vector Shedding
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Germline Transmission/Vector Shedding
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
64
APPENDIX 8 Delphi Round 1 Results
LONG TERM ADVERSE EVENTS - Vector integration into host genome
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Vector Integration Into Host Genome
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Vector Integration into Host Genome
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Vector Integration into Host Genome
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
65
APPENDIX 8 Delphi Round 1 Results
LONG TERM ADVERSE EVENTS - Development of other disorders
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Development of Other Disorders (auto-immune diseases/cancers/etc.)
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Development of Other Disorders (auto-immune diseases/cancers/etc.)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Development of Other Disorders
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
66
APPENDIX 8 Delphi Round 1 Results
LONG TERM ADVERSE EVENTS - Immune response to FVIII/FIX (Inhibitor development)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Immune Response to FVIII/FIX(Inhibitor development)
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Immune Response to FVIII/FIX(Inhibitor development)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Immune Response to FVIII/FIX(Inhibitor development)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
67
APPENDIX 8 Delphi Round 1 Results
MORTALITY - Cause of death
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Cause of Death
0
5
10
15
20
25
30
35
40
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Cause of Death
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Cause of Death
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
68
APPENDIX 8 Delphi Round 1 Results
MORTALITY - Age of death
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Age of Death
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Age of Death
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Age of Death
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
69
APPENDIX 8 Delphi Round 1 Results
PHYSIOLOGICAL/CLNICAL - Frequency of bleeds
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Frequency of Bleeds
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Frequency of Bleeds
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Frequency of Bleeds
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
70
APPENDIX 8 Delphi Round 1 Results
PHYSIOLOGICAL/CLNICAL - Severity of bleeds
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Severity of Bleeds
0
5
10
15
20
25
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Severity of Bleeds
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Severity of Bleeds
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
71
APPENDIX 8 Delphi Round 1 Results
PHYSIOLOGICAL/CLNICAL - Factor activity level
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Factor Activity Level
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Factor Activity Level
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Factor Activity Level
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
72
APPENDIX 8 Delphi Round 1 Results
PHYSIOLOGICAL/CLNICAL – Duration of factor expression
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Duration of Factor Expression
0
5
10
15
20
25
30
35
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Duration of Factor Expression
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Duration of Factor Expression
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
73
APPENDIX 8 Delphi Round 1 Results
PAIN/DISCOMFORT - Acute pain
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Acute Pain (frequency/intensity/duration/character)
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Acute Pain (frequency/intensity/duration/character)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Acute Pain (frequency/intensity/duration/character)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
74
APPENDIX 8 Delphi Round 1 Results
PAIN/DISCOMFORT - Interference of acute pain on daily life/activities of daily living
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Interference of acute pain on daily life
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Interference of acute pain on daily life
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Interference of acute pain on daily life
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
75
APPENDIX 8 Delphi Round 1 Results
PAIN/DISCOMFORT - Chronic pain
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Chronic Pain (frequency/intensity/duration/character)
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Chronic Pain (frequency/intensity/duration/character)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Chronic Pain (frequency/intensity/duration/character)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
76
APPENDIX 8 Delphi Round 1 Results
PAIN/DISCOMFORT - Interference of chronic pain on daily life/activities of daily living
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Interference of Chronic Pain on Daily Life
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Interference of Chronic Pain on Daily Life
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Interference of Chronic Pain on Daily Life
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
77
APPENDIX 8 Delphi Round 1 Results
EMOTIONAL FUNCTIONING - Mental health (including anxiety/depression/coping/worry)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Mental Health (anxiety/depression/coping/worry)
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Mental Health(anxiety/depresion/coping/worry)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Mental Health (anxiety/depression/coping/worry)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
78
APPENDIX 8 Delphi Round 1 Results
EMOTIONAL FUNCTIONING - Vitality/tiredness/fatigue
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Vitality/tiredness/fatigue
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Vitality/tiredness/fatigue
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Vitality/tiredness/fatigue
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
79
APPENDIX 8 Delphi Round 1 Results
EMOTIONAL FUNCTIONING - Contentment/happiness/elation/exhilaration (mood)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Mood(contentment/happiness/elation/exhilaration)
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Mood(contentment/happiness/elation/ehxilaration)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Mood(contentment/happiness/elation/ehxilaration)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
80
APPENDIX 8 Delphi Round 1 Results
SOCIAL FUNCTIONING - Identifying as a person with hemophilia (disclosure)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Identifying as a person with hemophilia (disclosure)
02468
101214161820
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Identifying as a person with hemophilia (disclosure)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Identifying as a person with hemophilia (disclosure)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
81
APPENDIX 8 Delphi Round 1 Results
SOCIAL FUNCTIONING - Sense of belonging in a community
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Sense of belonging to a community
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Sense of belonging to a community
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Sense of belonging to a community
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
82
APPENDIX 8 Delphi Round 1 Results
SOCIAL FUNCTIONING - Feeling of inequality compared to peers
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Feeling of inequality compared to peers
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Feeling of inequality compared to peers
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Feeling of inequality compared to peers
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
83
APPENDIX 8 Delphi Round 1 Results
SOCIAL FUNCTIONING - Romantic relationships
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Romantic Relationships
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Romantic Relationships
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Romantic Relationships
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
84
APPENDIX 8 Delphi Round 1 Results
PHYSICAL FUNCTIONING -Duration, frequency, intensity, and type of physical activity/sports/play
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Duration, frequency, intensity and type of physical activity/sports/play
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Duration, frequency, intensity and type of physical activity/sports/play
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Duration, frequency, intensity and type of physical activity/sports/play
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
85
APPENDIX 8 Delphi Round 1 Results
PHYSICAL FUNCTIONING -Sexual activity
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Sexual Activity
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Sexual Activity
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Sexual Activity
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
86
APPENDIX 8 Delphi Round 1 Results
PHYSICAL FUNCTIONING -Mobility
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Mobility
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Mobility
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Mobility
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
87
APPENDIX 8 Delphi Round 1 Results
PHYSICAL FUNCTIONING -Target joints
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Target Joints
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Target Joints
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Target Joints
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
88
APPENDIX 8 Delphi Round 1 Results
PHYSICAL FUNCTIONING -Joint function
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Joint Function
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Joint Function
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Joint Function
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
89
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Independence
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Independence
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Independence
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Independence
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
90
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Education attainment/achievement
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Educational Attainment/Achievement
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Educational Attainment/Achievement
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Educational Attainment/Achievement
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
91
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Education choice
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Education Choice
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Education Choice
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Education Choice
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
92
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Career choice
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Career Choice for Patient
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Career Choice for Patient
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Career Choice for Patient
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
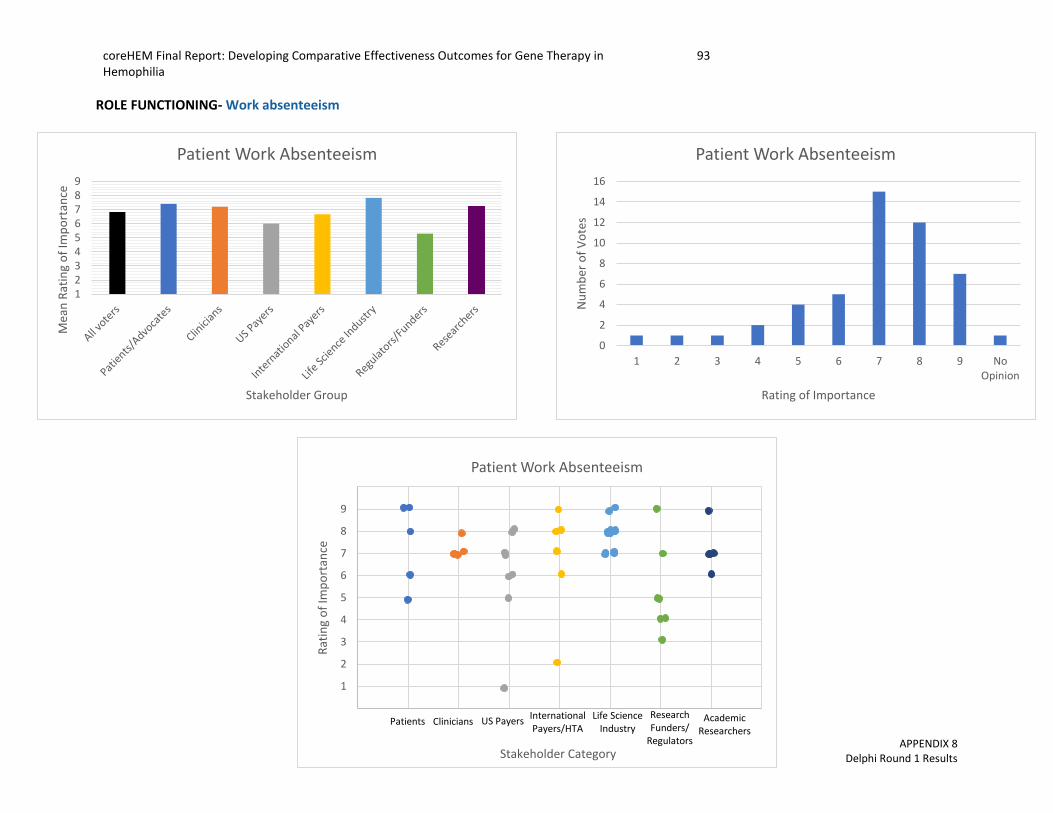
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
93
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Work absenteeism
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Patient Work Absenteeism
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Patient Work Absenteeism
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Patient Work Absenteeism
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
94
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Career choice for caregiver
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Caregiver Career Choice
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Caregiver Career Choice
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Caregiver Career Choice
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
95
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Caregiver absenteeism
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Caregiver Work Absenteeism
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Caregiver Work Absenteeism
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Caregiver Work Absenteeism
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
96
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Family decisions
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Family Decisions
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Family Decisions
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Family Decisions
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
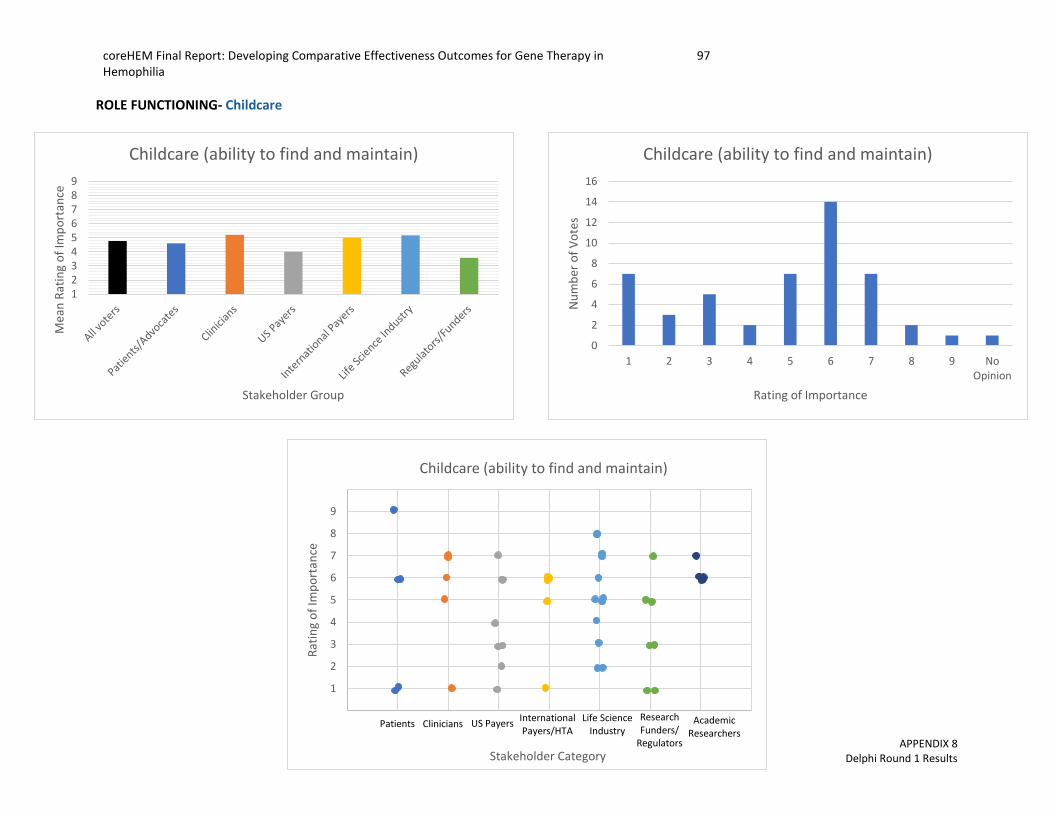
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
97
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Childcare
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Childcare (ability to find and maintain)
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Childcare (ability to find and maintain)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Childcare (ability to find and maintain)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
98
APPENDIX 8 Delphi Round 1 Results
ROLE FUNCTIONING- Interaction with children
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Interaction with Children
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Interaction with Children
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Interaction with Children
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
99
APPENDIX 8 Delphi Round 1 Results
PERCEIVED HEALTH STATUS - Feeling of normalcy
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Feeling of Normalcy
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Feeling of Normalcy
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Feeling of Normalcy
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
100
APPENDIX 8 Delphi Round 1 Results
PERCEIVED HEALTH STATUS - Feeling of physical health/general health perception
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Feeling of Physical Health/General Health Perception
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Feeling of Physical Health/General Health Percpetion
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Feeling of Physical Health/General Health Perception
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
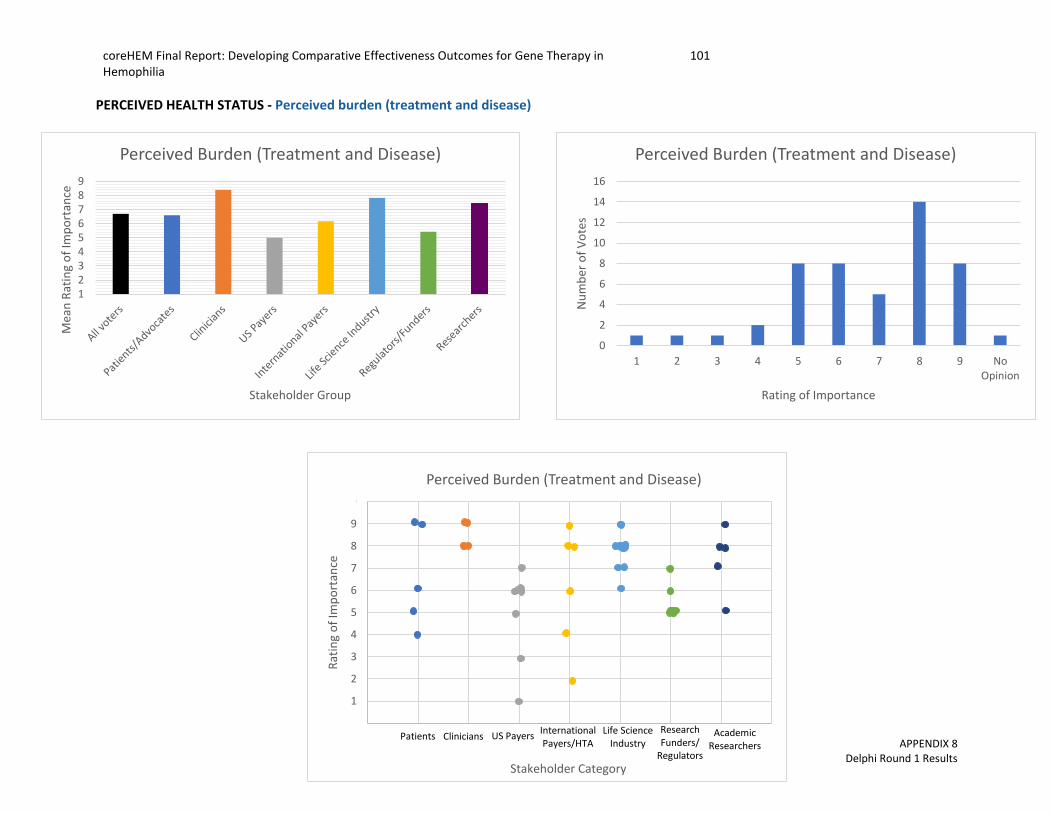
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
101
APPENDIX 8 Delphi Round 1 Results
PERCEIVED HEALTH STATUS - Perceived burden (treatment and disease)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Perceived Burden (Treatment and Disease)
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Perceived Burden (Treatment and Disease)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Perceived Burden (Treatment and Disease)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
102
APPENDIX 8 Delphi Round 1 Results
PERCEIVED HEALTH STATUS - Risk aversion
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Risk Aversion
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Risk Aversion
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Risk Aversion
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
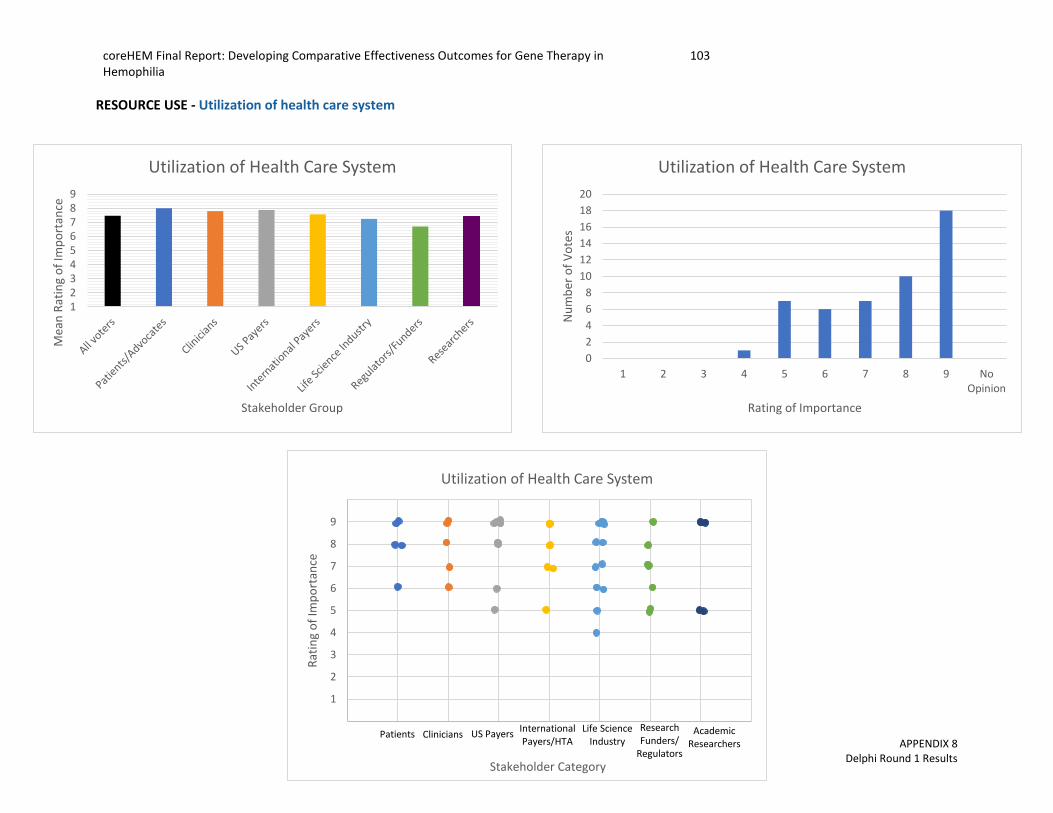
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
103
APPENDIX 8 Delphi Round 1 Results
RESOURCE USE - Utilization of health care system
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Utilization of Health Care System
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Utilization of Health Care System
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Utilization of Health Care System
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
104
APPENDIX 8 Delphi Round 1 Results
RESOURCE USE - Cost on patient/family
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Cost to Patient/Family
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Cost to Patient/Family
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Cost to Patient/Family
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
105
APPENDIX 8 Delphi Round 1 Results
RESOURCE USE – Societal Costs
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Societal Costs
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Societal Costs
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Societal Costs
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
106
APPENDIX 8 Delphi Round 1 Results
RESOURCE USE - Cost of treatment regimen
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Burden of Treatment Regimen on Patient/Family
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9 NoOpinion
Nu
mb
er o
f V
ote
s
Rating of Importance
Burden of Treatment Regimen on Patient/Family
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Burden of Treatment Regimen Patient/Family
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
107
APPENDIX 9 Delphi Round 2 Results
APPENDIX NINE – DELPHI ROUND TWO RESULTS
coreHEM DELPHI ROUND 2 RESULTS
NOVEMBER 8, 2017
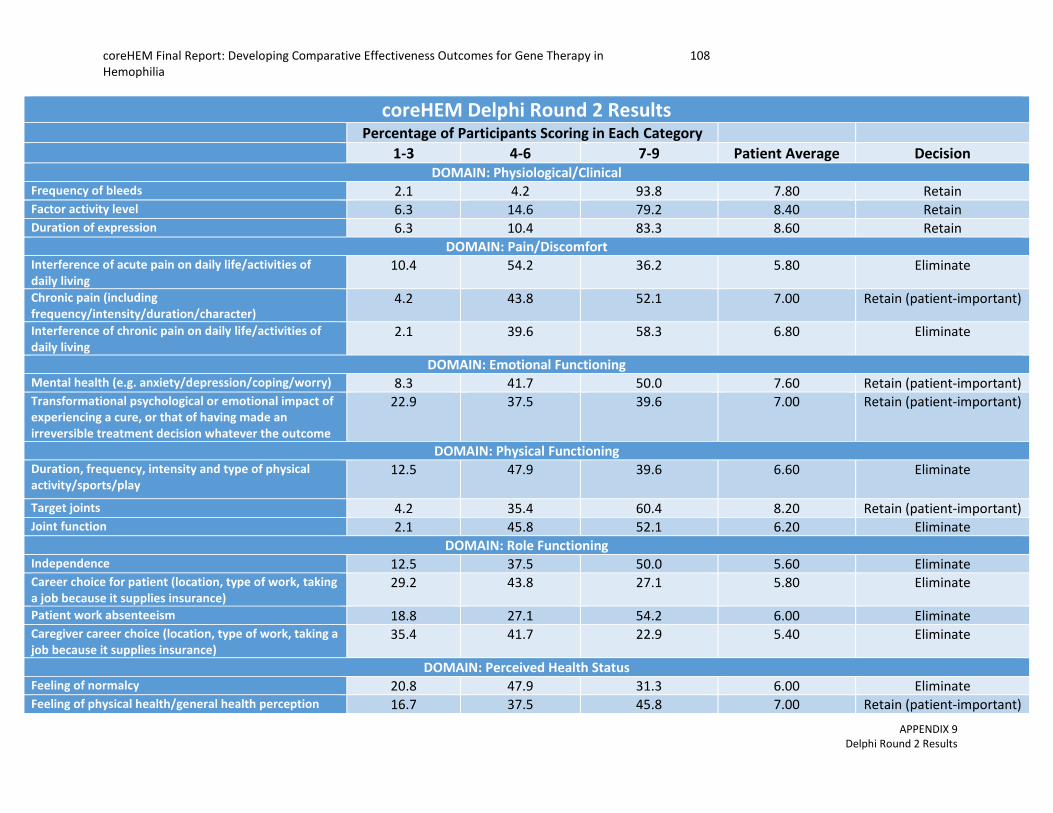
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
108
APPENDIX 9 Delphi Round 2 Results
coreHEM Delphi Round 2 Results Percentage of Participants Scoring in Each Category 1-3 4-6 7-9 Patient Average Decision
DOMAIN: Physiological/Clinical Frequency of bleeds 2.1 4.2 93.8 7.80 Retain Factor activity level 6.3 14.6 79.2 8.40 Retain Duration of expression 6.3 10.4 83.3 8.60 Retain
DOMAIN: Pain/Discomfort Interference of acute pain on daily life/activities of daily living
10.4 54.2 36.2 5.80 Eliminate
Chronic pain (including frequency/intensity/duration/character)
4.2 43.8 52.1 7.00 Retain (patient-important)
Interference of chronic pain on daily life/activities of daily living
2.1 39.6 58.3 6.80 Eliminate
DOMAIN: Emotional Functioning Mental health (e.g. anxiety/depression/coping/worry) 8.3 41.7 50.0 7.60 Retain (patient-important) Transformational psychological or emotional impact of experiencing a cure, or that of having made an irreversible treatment decision whatever the outcome
22.9 37.5 39.6 7.00 Retain (patient-important)
DOMAIN: Physical Functioning Duration, frequency, intensity and type of physical activity/sports/play
12.5 47.9 39.6 6.60 Eliminate
Target joints 4.2 35.4 60.4 8.20 Retain (patient-important) Joint function 2.1 45.8 52.1 6.20 Eliminate
DOMAIN: Role Functioning Independence 12.5 37.5 50.0 5.60 Eliminate Career choice for patient (location, type of work, taking a job because it supplies insurance)
29.2 43.8 27.1 5.80 Eliminate
Patient work absenteeism 18.8 27.1 54.2 6.00 Eliminate Caregiver career choice (location, type of work, taking a job because it supplies insurance)
35.4 41.7 22.9 5.40 Eliminate
DOMAIN: Perceived Health Status Feeling of normalcy 20.8 47.9 31.3 6.00 Eliminate Feeling of physical health/general health perception 16.7 37.5 45.8 7.00 Retain (patient-important)

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
109
APPENDIX 9 Delphi Round 2 Results
Perceived burden (treatment and disease) 16.7 41.7 41.7 6.60 Eliminate Risk aversion (including confidence to participate in physical activity/sports/play)
20.8 41.7 37.5 7.40 Retain (patient-important)
DOMAIN: Resource Use Utilization of health care system 8.3 31.3 60.4 6.60 Eliminate
Burden of treatment regimen on patient/family 8.3 37.5 54.2 7.00 Retain (patient-important)
DOMAIN: Short Term Adverse Events (<12 months) Liver toxicity 2.1 16.7 81.3 8.20 Retain Germline transmission 16.7 33.3 50.0 6.20 Eliminate Vector shedding 18.8 47.9 33.3 6.00 Eliminate Immune response to FVIII/FIX (inhibitor development) 2.1 25.0 72.9 8.40 Retain Immune response to gene therapy 0.0 20.8 79.2 8.00 Retain Anaphylactic response to treatment 10.4 25.0 64.6 5.40 Eliminate Thrombosis (blood clots) 2.1 27.1 70.8 6.80 Retain Heart function (cardiac enzymes, ECG, Echo) 14.6 50.0 35.4 5.60 Eliminate
DOMAIN: Long Term Adverse Events (beyond 12 months) Vector integration into host genome 8.3 39.6 52.1 7.40 Retain (patient-important) Development of other disorders (auto-immune diseases/cancers/etc.)
2.1 25.0 72.9 7.80 Retain
Immune response to FVIII/FIX (inhibitor development) 8.3 25.0 66.7 5.80 Eliminate Birth defects/childhood malignancy of offspring 22.9 22.9 54.2 5.80 Eliminate Duration of vector-neutralizing immune response which affects ability to re-administer vector
6.3 35.4 58.3 7.80 Retain (patient-important)
DOMAIN: Mortality Cause of death 10.4 18.8 70.8 7.40 Retain Age of death 22.9 39.6 37.5 5.60 Eliminate Survival time from gene therapy treatment to death 10.4 31.3 58.3 6.20 Eliminate

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
110
APPENDIX 9 Delphi Round 2 Results
ADVERSE EVENTS AND MORTALITY OUTCOMES
RETAINED ELIMINATED Liver toxicity Germline transmission Short-term immune response to FVIII/FIX (inhibitor) Vector shedding Immune response to gene therapy Anaphylactic response to treatment Thrombosis (blood clots) Heart function (cardiac enzymes, ECG, Echo) Vector integration into host genome Long-term immune response to FVIII/FIX (inhibitor) Development of other disorders (auto-immune disease/cancers) Birth defect/childhood malignancy of offspring Duration of vector-neutralizing response Age of death Cause of death Survival time from gene therapy treatment to death

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
111
APPENDIX 9 Delphi Round 2 Results
RETAINED SHORT-TERM ADVERSE EVENTS - Liver toxicity
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Liver Toxicity
0
5
10
15
20
25
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Liver Toxicity
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Liver Toxicity
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
112
APPENDIX 9 Delphi Round 2 Results
RETAINED SHORT-TERM ADVERSE EVENTS - Immune response to FVIII/FIX (Inhibitor development)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Short-term Immune Response to FVIII/FIX(Inhibitor development)
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Short-term Immune Response to FVIII/FIX(Inhibitor development)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Short-term Immune Response to FVIII/FIX(Inhibitor development)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
113
APPENDIX 9 Delphi Round 2 Results
RETAINED SHORT-TERM ADVERSE EVENTS - Immune response to gene therapy
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Immune Response to Gene Therapy
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Immune Response to Gene Therapy
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Immune Response to Gene Therapy
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
114
APPENDIX 9 Delphi Round 2 Results
RETAINED SHORT-TERM ADVERSE EVENTS – Thrombosis (blood clots)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Thrombosis (blood clots)
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Thrombosis (blood clots)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Thrombosis (blood clots)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
115
APPENDIX 9 Delphi Round 2 Results
RETAINED LONG-TERM ADVERSE EVENTS - Vector integration into host genome
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Vector Integration into Host Genome
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Vector Integration into Host Genome
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Vector Integration into Host Genome
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
116
APPENDIX 9 Delphi Round 2 Results
RETAINED LONG-TERM ADVERSE EVENTS - Development of other disorders (auto-immune disease/cancers)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Development of Other Disorders (auto-immune disease/cancers)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Development of Other Disorders (auto-immune disease/cancers)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Development of Other Disorders (cancers, auto-immune disease, etc.)
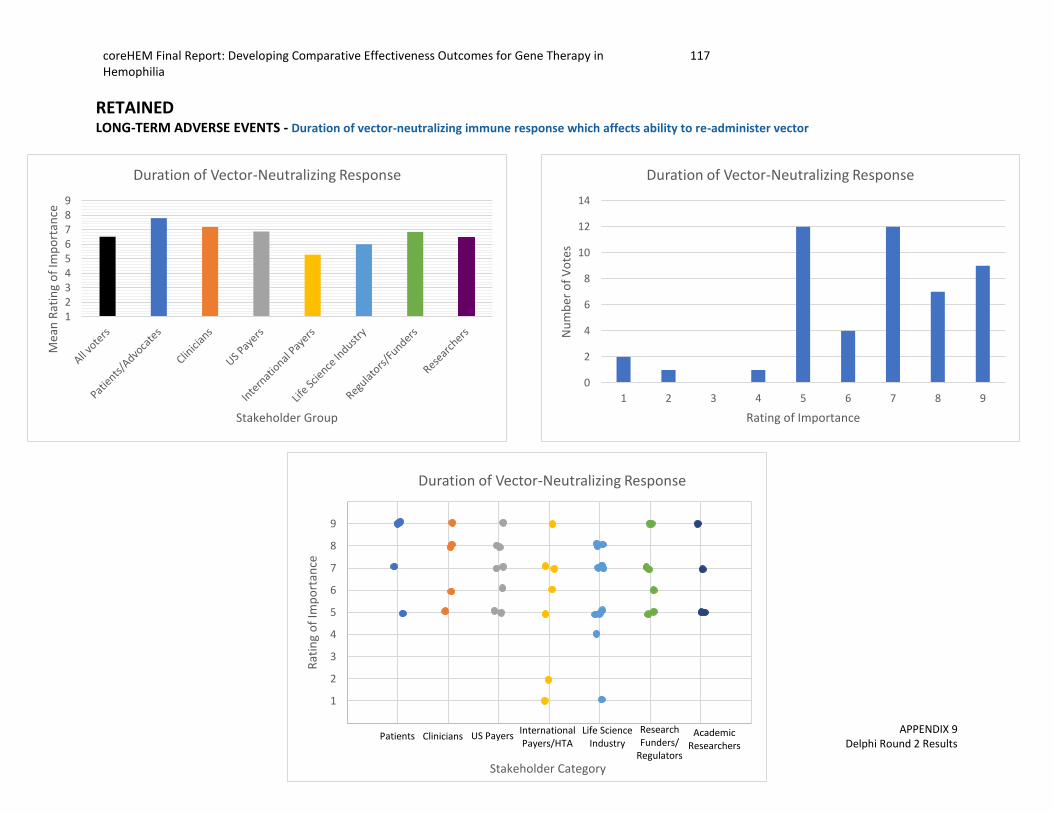
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
117
APPENDIX 9 Delphi Round 2 Results
RETAINED LONG-TERM ADVERSE EVENTS - Duration of vector-neutralizing immune response which affects ability to re-administer vector
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Duration of Vector-Neutralizing Response
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Duration of Vector-Neutralizing Response
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Duration of Vector-Neutralizing Response
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
118
APPENDIX 9 Delphi Round 2 Results
RETAINED MORTALITY - Cause of death
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Cause of Death
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Cause of Death
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Cause of Death
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
119
APPENDIX 9 Delphi Round 2 Results
ELIMINATED SHORT-TERM ADVERSE EVENTS – Germline Transmission
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Germline Transmission
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Germline Transmission
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Germline Transmission
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
120
APPENDIX 9 Delphi Round 2 Results
ELIMINATED SHORT-TERM ADVERSE EVENTS – Vector Shedding
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Vector Shedding
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Vector Shedding
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Vector Shedding
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
121
APPENDIX 9 Delphi Round 2 Results
ELIMINATED SHORT-TERM ADVERSE EVENTS – Anaphylactic response to treatment
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Anaphylactic Response
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Anaphylactic Response
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Anaphylactic Response
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
122
APPENDIX 9 Delphi Round 2 Results
ELIMINATED SHORT-TERM ADVERSE EVENTS – Heart function (cardiac enzymes, ECG, Echo)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Heart Function
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Heart Function
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Heart Function
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
123
APPENDIX 9 Delphi Round 2 Results
ELIMINATED LONG-TERM ADVERSE EVENTS – Long-term immune response to FVIII/FIX (Inhibitor development)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Long-Term Immune Response to FVIII/FIX(Inhibitor development)
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Long-Term Immune Response to FVIII/FIX(Inhibitor development)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Long-Term Immune Response to FVIII/FIX(Inhibitor development)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
124
APPENDIX 9 Delphi Round 2 Results
ELIMINATED LONG-TERM ADVERSE EVENTS – Birth defects/childhood malignancy of offspring
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Birth Defects/Childhood Malignancy of Offspring
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Birth Defects/Childhood Malignancy of Offspring
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Birth Defects/Childhood Malignancy of Offspring
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
125
APPENDIX 9 Delphi Round 2 Results
ELIMINATED MORTALITY – Age of death
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Age of Death
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Age of Death
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Age of Death
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
126
APPENDIX 9 Delphi Round 2 Results
ELIMINATED MORTALITY – Survival time from gene therapy to death
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Survival time from gene therapy treatment to death
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Survival time from gene therapy treatment to death
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Survival time from gene therapy treatment to death
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
127
APPENDIX 9 Delphi Round 2 Results
OTHER OUTCOMES
RETAINED ELIMINATED Frequency of bleeds Interference of acute pain on daily life/activities of daily living
Factor activity level Interference of chronic pain on daily life/activities of daily living Duration of expression Duration, frequency, intensity, type of physical activity/sports/play Chronic pain (frequency/intensity/duration/character) Joint function Mental health (e.g. anxiety/depression/coping/worry) Independence Transformational psychological or emotional impact of a cure Career choice for patient Feeling of physical health/general health perception Patient work absenteeism Risk aversion Caregiver career choice Burden of treatment regimen on patient/family Feeling of normalcy
Perceived burden (of treatment and disease) Utilization of health care system

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
128
APPENDIX 9 Delphi Round 2 Results
RETAINED PHYSIOLOGICAL/CLNICAL - Frequency of bleeds
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Frequency of Bleeds
0
5
10
15
20
25
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Frequency of Bleeds
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Frequency of Bleeds
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
129
APPENDIX 9 Delphi Round 2 Results
RETAINED PHYSIOLOGICAL/CLNICAL - Factor activity level
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Factor Activity Level
0
2
4
6
8
10
12
14
16
18
20
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Factor Activity Level
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Factor Activity Level
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
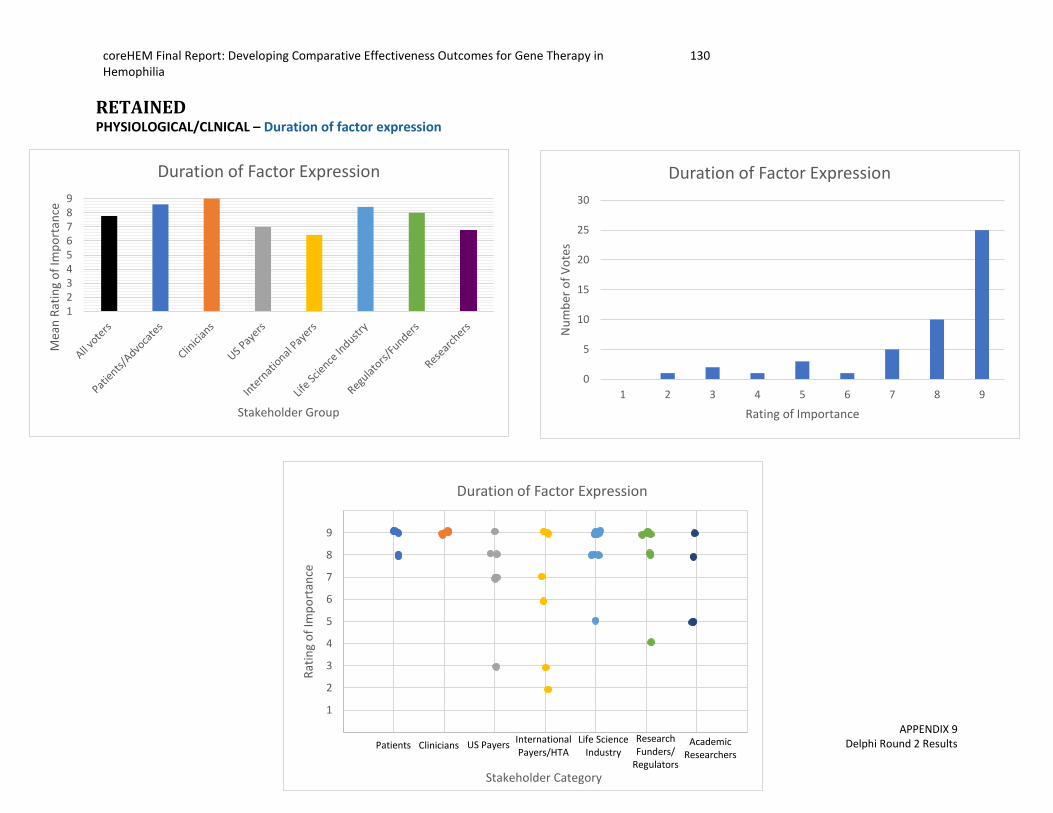
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
130
APPENDIX 9 Delphi Round 2 Results
RETAINED PHYSIOLOGICAL/CLNICAL – Duration of factor expression
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Duration of Factor Expression
0
5
10
15
20
25
30
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Duration of Factor Expression
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Duration of Factor Expression
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
131
APPENDIX 9 Delphi Round 2 Results
RETAINED PAIN/DISCOMFORT - Chronic pain (frequency/intensity/duration/character)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Chronic pain (frequency/intensity/duration/character)
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Chronic pain (frequency/intensity/duration/character)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Chronic pain (frequency/intensity/duration/character)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
132
APPENDIX 9 Delphi Round 2 Results
RETAINED EMOTIONAL FUNCTIONING - Mental health (including anxiety/depression/coping/worry)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Mental Health (anxiety/depression/coping/worry)
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Mental Health (anxiety/depresion/coping/worry)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Mental Health (anxiety/depression/coping/worry)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
133
APPENDIX 9 Delphi Round 2 Results
RETAINED EMOTIONAL FUNCTIONING - Transformational psychological or emotional impact of experiencing a cure, or that of having made an irreversible
treatment decision whatever the outcome
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Transformational psychological or emotional impact of experiencing a cure
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Transformational psychological or emotional impact of experiencing a cure
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Transformational psychological or emotional impact of experiencing a cure
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
134
APPENDIX 9 Delphi Round 2 Results
RETAINED PHYSICAL FUNCTIONING -Target joints
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Target Joints
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Target Joints
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Target Joints
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
135
APPENDIX 9 Delphi Round 2 Results
RETAINED PERCEIVED HEALTH STATUS - Feeling of physical health/general health perception
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Feeling of physical health/general health perception
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Feeling of physical health/general health perception
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Feeling of physical health/general health perception
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
136
APPENDIX 9 Delphi Round 2 Results
RETAINED PERCEIVED HEALTH STATUS - Risk aversion (including confidence to participate in physical activity/sports/play)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Risk Aversion
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Risk Aversion
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Risk Aversion
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
137
APPENDIX 9 Delphi Round 2 Results
RETAINED RESOURCE USE – Burden of treatment regimen on patient/family
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Burden of Treatment on Patient/Family
0
2
4
6
8
10
12
14
16
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Burden of Treatment on Patient/Family
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Burden of Treatment on Patient/Family
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
138
APPENDIX 9 Delphi Round 2 Results
ELIMINATED PAIN/DISCOMFORT – Interference of acute pain on daily life/activities of daily living
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Interference of Acute Pain on Daily Life/Activities of Daily Living
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Interference of Acute Pain on Daily Life/Activities of Daily Living
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Interference of Acute Pain on Daily Life/Activities of Daily Living
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
139
APPENDIX 9 Delphi Round 2 Results
ELIMINATED PAIN/DISCOMFORT – Interference of chronic pain on daily life/activities of daily living
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Interference of Chronic Pain on Daily Life/Activities of Daily Living
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Interference of Chronic Pain on Daily Life/Activities of Daily Living
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Interference of Chronic Pain on Daily Life/Activities of Daily Living
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
140
APPENDIX 9 Delphi Round 2 Results
ELIMINATED PHYSICAL FUNCTIONING – Duration, frequency, intensity, type of physical activity/sports/play
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Duration, frequency, intensity and type of physical activity/sports/play
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Duration, frequency, intensity and type of physical activity/sports/play
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Duration, frequency, intensity and type of physical activity/sports/play
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
141
APPENDIX 9 Delphi Round 2 Results
ELIMINATED PHYSICAL FUNCTIONING – Joint Function
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Joint Function
0
2
4
6
8
10
12
14
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Joint Function
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Joint Function
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
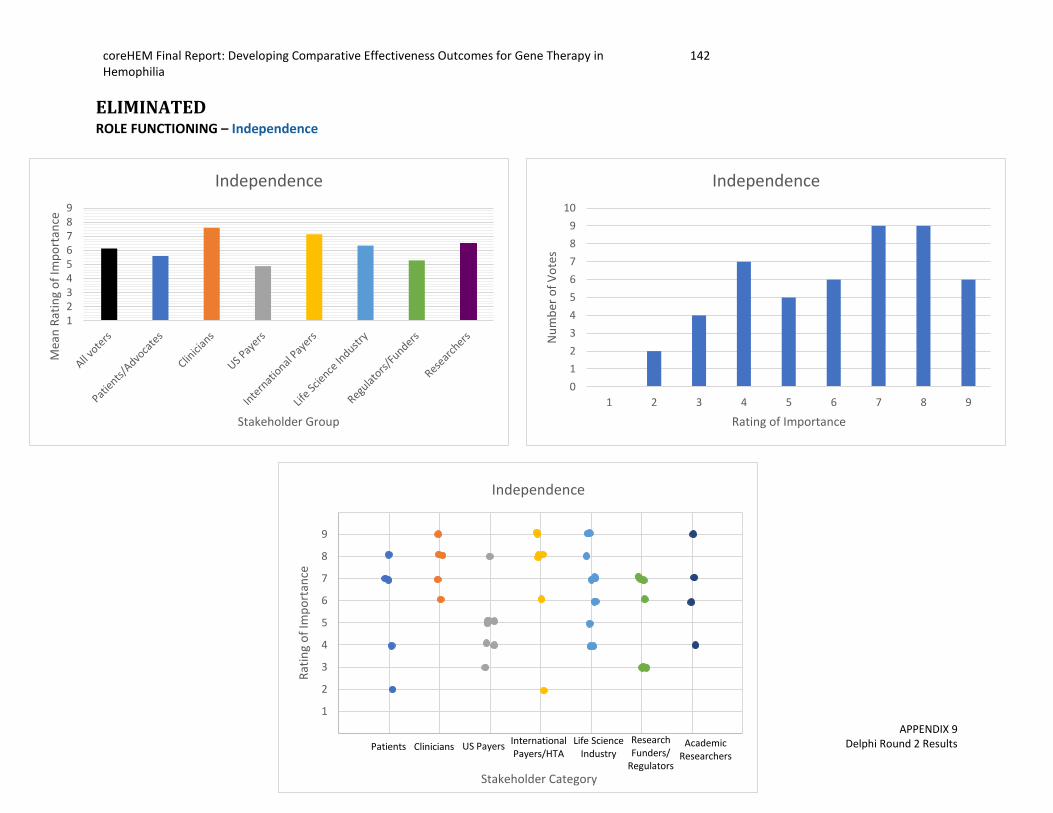
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
142
APPENDIX 9 Delphi Round 2 Results
ELIMINATED ROLE FUNCTIONING – Independence
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Independence
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Independence
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Independence
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
143
APPENDIX 9 Delphi Round 2 Results
ELIMINATED ROLE FUNCTIONING – Career choice for patient (location, type of work, taking a job because it supplies insurance)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Career Choice for Patient
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Career Choice for Patient
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Career Choice for Patient
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
144
APPENDIX 9 Delphi Round 2 Results
ELIMINATED ROLE FUNCTIONING – Patient work absenteeism
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Patient Work Absenteeism
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Patient Work Absenteeism
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Patient Work Absenteeism
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
145
APPENDIX 9 Delphi Round 2 Results
ELIMINATED ROLE FUNCTIONING – Caregiver career choice (location, type of work, taking a job because it supplies insurance)
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Caregiver Career Choice
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Caregiver Career Choice
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Caregiver Career Choice
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
146
APPENDIX 9 Delphi Round 2 Results
ELIMINATED PERCEIVED HEALTH STATUS – Feeling of normalcy
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Feeling of Normalcy
0
1
2
3
4
5
6
7
8
9
10
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Feeling of Normalcy
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Feeling of Normalcy
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
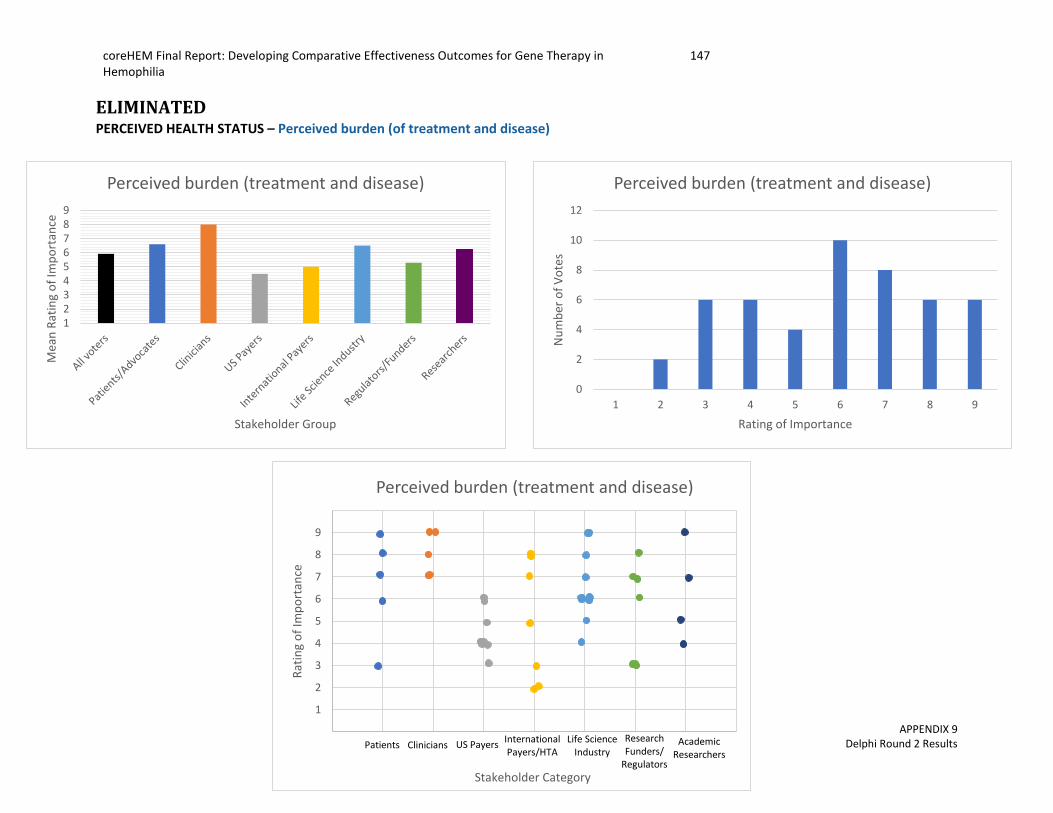
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
147
APPENDIX 9 Delphi Round 2 Results
ELIMINATED PERCEIVED HEALTH STATUS – Perceived burden (of treatment and disease)
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Perceived burden (treatment and disease)
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Perceived burden (treatment and disease)
0
2
4
6
8
10
12
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Perceived burden (treatment and disease)

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
148
APPENDIX 9 Delphi Round 2 Results
ELIMINATED RESOURCE USE–Utilization of healthcare system
123456789
Mea
n R
atin
g o
f Im
po
rtan
ce
Stakeholder Group
Utilization of healthcare system
0
2
4
6
8
10
12
14
16
18
1 2 3 4 5 6 7 8 9
Nu
mb
er o
f V
ote
s
Rating of Importance
Utilization of healthcare system
0
1
2
3
4
5
6
7
8
9
10
Rat
ing
of
Imp
ort
ance
Stakeholder Category
Utilization of healthcare system
Patients Clinicians US PayersInternationalPayers/HTA
Life Science Industry
ResearchFunders/
Regulators
Academic Researchers
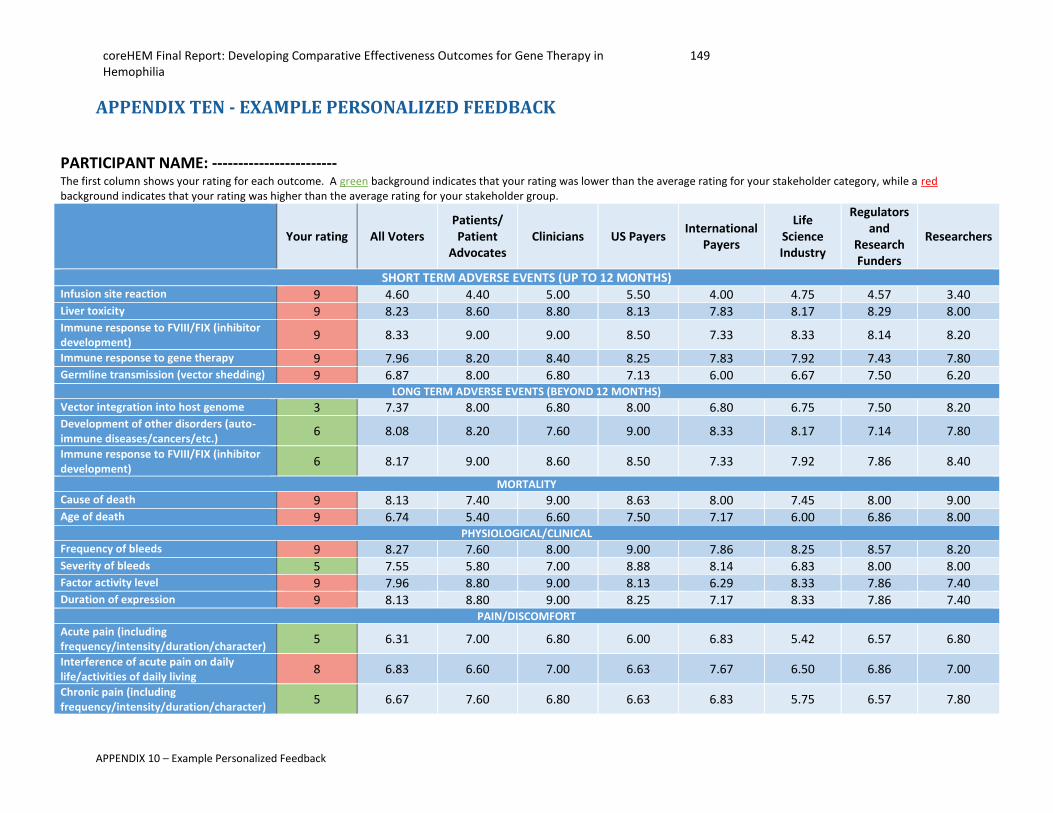
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
149
APPENDIX 10 – Example Personalized Feedback
APPENDIX TEN - EXAMPLE PERSONALIZED FEEDBACK
PARTICIPANT NAME: ------------------------ The first column shows your rating for each outcome. A green background indicates that your rating was lower than the average rating for your stakeholder category, while a red background indicates that your rating was higher than the average rating for your stakeholder group.
Your rating All Voters Patients/ Patient
Advocates Clinicians US Payers
International Payers
Life Science Industry
Regulators and
Research Funders
Researchers
SHORT TERM ADVERSE EVENTS (UP TO 12 MONTHS) Infusion site reaction 9 4.60 4.40 5.00 5.50 4.00 4.75 4.57 3.40 Liver toxicity 9 8.23 8.60 8.80 8.13 7.83 8.17 8.29 8.00 Immune response to FVIII/FIX (inhibitor development)
9 8.33 9.00 9.00 8.50 7.33 8.33 8.14 8.20
Immune response to gene therapy 9 7.96 8.20 8.40 8.25 7.83 7.92 7.43 7.80 Germline transmission (vector shedding) 9 6.87 8.00 6.80 7.13 6.00 6.67 7.50 6.20
LONG TERM ADVERSE EVENTS (BEYOND 12 MONTHS)
Vector integration into host genome 3 7.37 8.00 6.80 8.00 6.80 6.75 7.50 8.20 Development of other disorders (auto-immune diseases/cancers/etc.)
6 8.08 8.20 7.60 9.00 8.33 8.17 7.14 7.80
Immune response to FVIII/FIX (inhibitor development)
6 8.17 9.00 8.60 8.50 7.33 7.92 7.86 8.40
MORTALITY
Cause of death 9 8.13 7.40 9.00 8.63 8.00 7.45 8.00 9.00 Age of death 9 6.74 5.40 6.60 7.50 7.17 6.00 6.86 8.00
PHYSIOLOGICAL/CLINICAL
Frequency of bleeds 9 8.27 7.60 8.00 9.00 7.86 8.25 8.57 8.20 Severity of bleeds 5 7.55 5.80 7.00 8.88 8.14 6.83 8.00 8.00 Factor activity level 9 7.96 8.80 9.00 8.13 6.29 8.33 7.86 7.40 Duration of expression 9 8.13 8.80 9.00 8.25 7.17 8.33 7.86 7.40
PAIN/DISCOMFORT
Acute pain (including frequency/intensity/duration/character)
5 6.31 7.00 6.80 6.00 6.83 5.42 6.57 6.80
Interference of acute pain on daily life/activities of daily living
8 6.83 6.60 7.00 6.63 7.67 6.50 6.86 7.00
Chronic pain (including frequency/intensity/duration/character)
5 6.67 7.60 6.80 6.63 6.83 5.75 6.57 7.80

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
150
APPENDIX 11 – Measurement/instrument worksheet from Consensus Meeting
APPENDIX ELEVEN – WORKSHEET USED AT IN-PERSON MEETING FOR DISCUSSION ON MEASUREMENTS/INSTRUMENTS
Table number: ____________________
Outcome discussed: ____________________ With your group, discuss the following parameters related to your outcome:
1. What is your group’s definition of the outcome (e.g. what is this outcome trying to measure, and does it measure only one thing, or are there several results/ideas that fit into this outcome)?
2. What type of measurement/instrument would be ideal to measure this outcome (for example, a survey a patient fills out, a clinical assessment a doctor performs, a laboratory test, etc., or a combination of some of these)?
3. Feasibility: a. How long should/does it take to measure this outcome? How long is too long? b. What is/should be the patient/clinician burden associated with this measure?
4. Should this outcome be measured using a generic instrument/measure, or a hemophilia-specific instrument/measure? Why?
5. What are some of the measurement metrics that your group have discussed (such as when should the outcome be measured, how often it should be measured, how it should be reported?)

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
151
APPENDIX 11 – Measurement/instrument worksheet from Consensus Meeting
Instruments/Measurements Currently Being Used 1. Are there any instruments/measurements currently being used that could capture this outcome?
a. If instruments exist, are they adequate/appropriate for use with gene therapy? If
applicable, consider whether existing instruments capture the difference between gene therapy and current standard of care (are they sensitive enough?).
b. If instruments DO NOT exist, what would a novel measure be? How would it fit the ideal instrument described in #2 above?
2. What are the pros and cons of the instruments/measurements listed above?
3. Do any of the instruments/measurements above capture the outcome in the way the group has been discussing? How? If not, could things about the instrument/measurement be altered to match what has been discussed above?
Instruments/Measurements in Other Therapeutic Fields
1. What other therapeutic areas may also measure this outcome?

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
152
APPENDIX 11 – Measurement/instrument worksheet from Consensus Meeting
2. Name any specific instruments/measurements in other therapeutic areas that you are aware of that may capture the same idea/outcome we are trying to assess with this measure?

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
153
APPENDIX 12 – Delphi Timeline and Participation Rates
APPENDIX TWELVE- DELPHI TIMELINE AND PARTICIPATION RATES
coreHEM Delphi Timeline and Participation Rates
Date Sent Cut-off
Date for Response
Type of Voting on Outcomes
Additional Tasks Free text
comments
# Voters Completed
(Participation Rate)
# Outcomes to Rate
Notes
Round 1 September
8th September
22nd Rate importance on scale from 1-9
Rank domains ✓ 49 100%) 48 -11 new outcomes were proposed by participants
Round 1A (Sub-Survey)
October 11th
October 18th
Agree/Disagree with outcomes for “Retention” and “Elimination”
Vote to include or not include new outcomes
✓ 36 (73%) 59
-Re-vote on 48 from Round 1 plus 11 new outcomes
Round 2 October
24th November
5th Rate importance on scale from 1-9
List top 5 outcomes and top 5 adverse events
48 (98%) 37
-3 outcomes reached high consensus and were directly included in the core set
-Adverse events separated and 8 adverse events with high consensus were moved to the coreHEM list of important adverse events
Advisory Vote for Round 3 (at meeting)
November 15th
November 19th
Rate importance on scale from 1-9
Vote to combine selected outcome based on deliberations at meeting
42 (86%) 9
-3 questions about combining outcomes; one combination was accepted
Round 3 November
20th December
2nd
Rate importance on scale 1-9; confirm or change vote from Advisory Vote at the in-person meeting
--
48 (98%) 8
-3 additional outcomes included in the core set
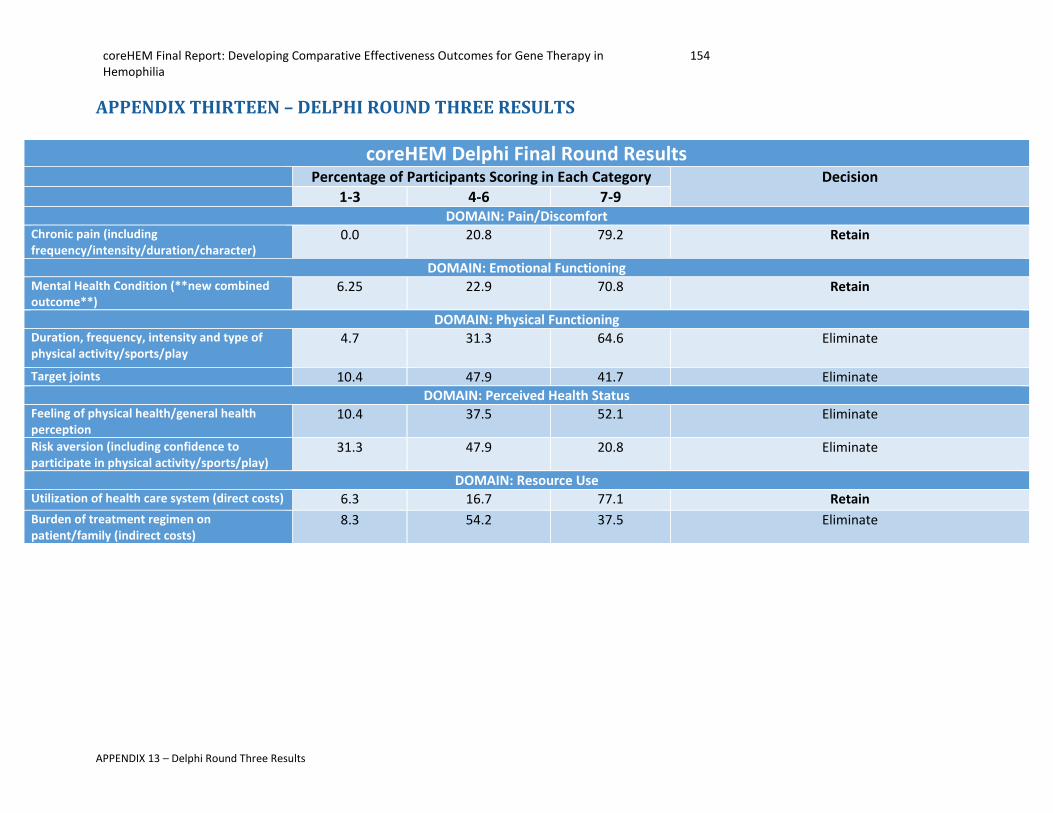
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
154
APPENDIX 13 – Delphi Round Three Results
APPENDIX THIRTEEN – DELPHI ROUND THREE RESULTS
coreHEM Delphi Final Round Results Percentage of Participants Scoring in Each Category Decision 1-3 4-6 7-9
DOMAIN: Pain/Discomfort Chronic pain (including frequency/intensity/duration/character)
0.0 20.8 79.2 Retain
DOMAIN: Emotional Functioning Mental Health Condition (**new combined outcome**)
6.25 22.9 70.8 Retain
DOMAIN: Physical Functioning Duration, frequency, intensity and type of physical activity/sports/play
4.7 31.3 64.6 Eliminate
Target joints 10.4 47.9 41.7 Eliminate
DOMAIN: Perceived Health Status Feeling of physical health/general health perception
10.4 37.5 52.1 Eliminate
Risk aversion (including confidence to participate in physical activity/sports/play)
31.3 47.9 20.8 Eliminate
DOMAIN: Resource Use Utilization of health care system (direct costs) 6.3 16.7 77.1 Retain
Burden of treatment regimen on patient/family (indirect costs)
8.3 54.2 37.5 Eliminate
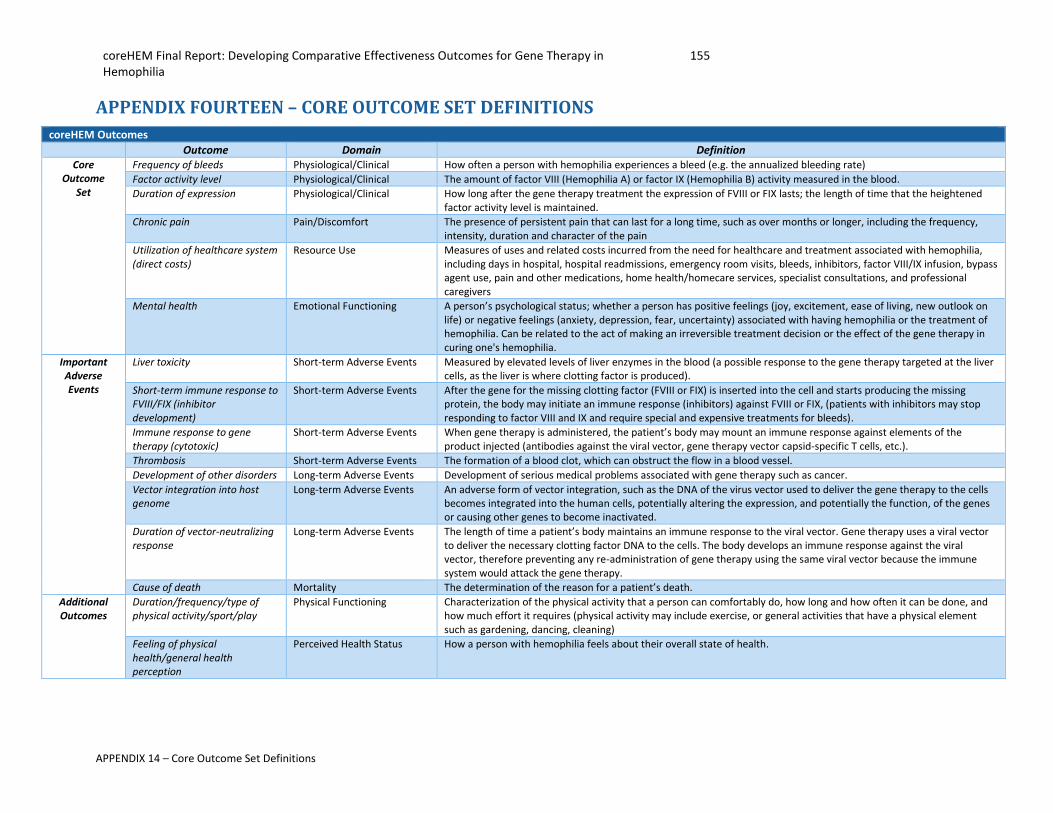
coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
155
APPENDIX 14 – Core Outcome Set Definitions
APPENDIX FOURTEEN – CORE OUTCOME SET DEFINITIONS
coreHEM Outcomes
Outcome Domain Definition Core
Outcome Set
Frequency of bleeds Physiological/Clinical How often a person with hemophilia experiences a bleed (e.g. the annualized bleeding rate)
Factor activity level Physiological/Clinical The amount of factor VIII (Hemophilia A) or factor IX (Hemophilia B) activity measured in the blood.
Duration of expression Physiological/Clinical How long after the gene therapy treatment the expression of FVIII or FIX lasts; the length of time that the heightened factor activity level is maintained.
Chronic pain Pain/Discomfort The presence of persistent pain that can last for a long time, such as over months or longer, including the frequency, intensity, duration and character of the pain
Utilization of healthcare system (direct costs)
Resource Use Measures of uses and related costs incurred from the need for healthcare and treatment associated with hemophilia, including days in hospital, hospital readmissions, emergency room visits, bleeds, inhibitors, factor VIII/IX infusion, bypass agent use, pain and other medications, home health/homecare services, specialist consultations, and professional caregivers
Mental health Emotional Functioning A person’s psychological status; whether a person has positive feelings (joy, excitement, ease of living, new outlook on life) or negative feelings (anxiety, depression, fear, uncertainty) associated with having hemophilia or the treatment of hemophilia. Can be related to the act of making an irreversible treatment decision or the effect of the gene therapy in curing one's hemophilia.
Important Adverse Events
Liver toxicity Short-term Adverse Events Measured by elevated levels of liver enzymes in the blood (a possible response to the gene therapy targeted at the liver cells, as the liver is where clotting factor is produced).
Short-term immune response to FVIII/FIX (inhibitor development)
Short-term Adverse Events After the gene for the missing clotting factor (FVIII or FIX) is inserted into the cell and starts producing the missing protein, the body may initiate an immune response (inhibitors) against FVIII or FIX, (patients with inhibitors may stop responding to factor VIII and IX and require special and expensive treatments for bleeds).
Immune response to gene therapy (cytotoxic)
Short-term Adverse Events When gene therapy is administered, the patient’s body may mount an immune response against elements of the product injected (antibodies against the viral vector, gene therapy vector capsid-specific T cells, etc.).
Thrombosis Short-term Adverse Events The formation of a blood clot, which can obstruct the flow in a blood vessel.
Development of other disorders Long-term Adverse Events Development of serious medical problems associated with gene therapy such as cancer.
Vector integration into host genome
Long-term Adverse Events An adverse form of vector integration, such as the DNA of the virus vector used to deliver the gene therapy to the cells becomes integrated into the human cells, potentially altering the expression, and potentially the function, of the genes or causing other genes to become inactivated.
Duration of vector-neutralizing response
Long-term Adverse Events The length of time a patient’s body maintains an immune response to the viral vector. Gene therapy uses a viral vector to deliver the necessary clotting factor DNA to the cells. The body develops an immune response against the viral vector, therefore preventing any re-administration of gene therapy using the same viral vector because the immune system would attack the gene therapy.
Cause of death Mortality The determination of the reason for a patient’s death.
Additional Outcomes
Duration/frequency/type of physical activity/sport/play
Physical Functioning Characterization of the physical activity that a person can comfortably do, how long and how often it can be done, and how much effort it requires (physical activity may include exercise, or general activities that have a physical element such as gardening, dancing, cleaning)
Feeling of physical health/general health perception
Perceived Health Status How a person with hemophilia feels about their overall state of health.

coreHEM Final Report: Developing Comparative Effectiveness Outcomes for Gene Therapy in Hemophilia
156
APPENDIX 15 – Recognition of the Core Outcome Set
APPENDIX FIFTEEN – RECOGNITION OF THE CORE OUTCOME SET The Institute for Clinical and Economic Review (ICER), the Swedish Agency for Health Technology Assessment and Assessment of Social Service (SBU), the Canadian Agency for Drugs and Technologies in Health (CADTH), Blue Cross Blue Shield Association (BCBSA), and SharpRx Pharmaceutical Consultation Services have recognized the coreHEM core outcome set as follows:
• Our organization participated in the coreHEM project, with the goal of identifying a core set of outcomes for use in future clinical studies of gene therapy in hemophilia.
• We will consider this recommended core outcomes set, along with other relevant outcomes, in future assessments of gene therapies for hemophilia.
• The choice of outcomes in clinical studies is one of many factors that are considered in assessments done by our organization.
The Institute for Clinical and Economic Review (ICER), the Swedish Agency for Health Technology Assessment and Assessment of Social Service (SBU), Blue Cross Blue Shield Association (BCBSA), and SharpRx Pharmaceutical Consultation Services additionally agree:
• We would encourage product developers and other researchers to consider this recommended core outcomes set when developing study protocols for future clinical trials, registries and other studies.