coracoacromial ligament release for shoulder impingement syndrome using the universal subcutaneous...
TRANSCRIPT
Arthroscopy: The Journal of Arthroscopic and Related Surgery 8(1):2-9 Published by Raven Press, Ltd. Q 1992 Arthroscopy Association of North America
Coracoacromial Ligament Release for Shoulder Impingement Syndrome Using the Universal Subcutaneous
Endoscope System
Ichiro Okutsu, M.D., Setsuo Ninomiya, M.D., Yoshio Takatori, M.D., Ikki Hamanaka, M.D., and George J. Schonholtz, M.D., F.A.C.S.
Summary: We developed a new operative procedure of coracoacromial liga- ment release for shoulder impingement syndrome. The operative procedure was confirmed by cadaveric studies and applied to clinical cases in 40 shoul- ders of 37 patients who suffered from shoulder impingement without bony abnormalities. The subacromial space was observed under local anesthesia using the Universal Subcutaneous Endoscope (USE) system on an outpatient basis. A popping phenomenon was observed between the coracoacromial lig- ament and the greater tuberosity of the humerus, which was covered by the rotator cuff, and the coracoacromial ligament was resected with a rongeur under endoscopic visualization in all shoulders. Resection of the coracoacro- mial ligament relieved the impingement and clinical signs, as in open or ar- throscopic resection of the coracoacromial ligament. Resection of the coraco- acromial ligament using the USE system is a safe and less-stressful surgical invasion than open or standard arthroscopic resection of the coracoacromial ligament. Key Words: Endoscopic surgery-Shoulder impingement syn- drome-Subacromial space-Universal subcutaneous endoscope system- Portal.
Standard subacromial endoscopy or bursoscopy (l-3), is a promising approach to shoulder impinge- ment syndrome. This operative procedure entails less scar formation and allows earlier rehabilitation than open operative procedure. However, subacro- mial endoscopy should be performed under general or local anesthesia with traction of the affected limb needed for muscle relaxation and liquid irrigation. Standard endoscopic procedures can be as compli- cated for patients as open operative procedures.
We developed a new operative procedure for
From the Department of Orthopaedic Surgery, Japanese Red Cross Medical Center, Hiroo, Shibuya-ku (I.O., I.H.), and the Department of Orthopaedic Surgery, Faculty of Medicine, Uni- versity of Tokyo, Hongo, Bunkyo-ku (S.N., Y.T.), Tokyo, Ja- pan; and 8830 Cameron Street, Suite 333 (G.J.S.), Silver Spring, Maryland, U.S.A.
Address correspondence and reprint requests to Dr. I. Okutsu, Department of Orthopaedic Surgery, Japanese Red Cross Med- ical Center, 4-l-22, Hiroo, Shibuya-ku, Tokyo 150, Japan.
shoulder impingement syndrome under local anes- thesia without traction of the affected limb or liquid irrigation using the Universal Subcutaneous Endo- scope (USE) system (4,5), which can be performed on an outpatient basis.
The purpose of this paper is to describe the new endoscopic approach to the coracoacromial liga- ment release for shoulder impingement syndrome.
ANATOMIC CONSIDERATIONS
General information The rotator cuff and subacromial bursa exist in
the subacromial space, which is limited above by the coracoacromial arch (acromion, coracoacromial ligament, and coracoid process) and below by the humeral head. Compression of the rotator cuff and subacromial bursa between the coracoacromial arch and the greater tuberosity of the humerus may
2
USE SYSTEM AND SHOULDER IMPINGEMENT 3
cause shoulder pain or impingement syndrome (6 11). These symptoms can result from a decrease in the height (increased volume of the coracoacromial ligament, acromioclavicular osteophytes, acromial spurs, or a large coracoid process) and/or an in- crease in the volume (as in subacromial bursitis or rotator cuff tendonitis) of the subacromial space
(12). For an endoscopic approach to the subacromial
space, we should note the important structures of the shoulder, for example, the anterior and poste- rior humeral circumflex arteries and veins, the ce- phalic vein, the acromial artery, the axillary nerve, and the long head of the biceps tendon. Other im- portant structures such as the axillary vessels and brachial plexus are located medial to the coracoid process and far from the operative site (Fig. 1A and B). The anterior humeral circumflex artery arises from the axillary artery and is located 3 cm distal from the coracoid process. The artery winds around the anterior part of the surgical neck of the humerus and feeds the deltoid muscle. The posterior humeral circumflex artery also arises from the axillary ar- tery, traverses the quadrangular space, and is cov- ered by the deltoid muscle. The artery is located several centimeters distal from the acromion in the frontal plane. The anterior and posterior humeral circumflex veins run with the anterior and posterior humeral circumflex arteries, respectively. The ce- phalic vein runs up the anterolateral side of the up- per arm, passes through the deltopectoral triangle, and empties into the axillary vein. The acromial ar- tery arises from the thoracoacromial artery, runs close to the upper part of the coracoacromial liga- ment, and makes an arterial net (rete acromiale) at the acromion.
The axillary nerve arises from the posterior cord of the brachial plexus and traverses the quadrangu- lar space with the posterior humeral circumflex ar- tery, winds around the posterior part of the surgical neck of the humerus, and innervates the deltoid muscle.
The long head of the biceps tendon (the intracap- sular portion of the biceps tendon) arises from the superior posterior portion of the glenoid labrum, passes through the bicipital groove, and runs to the muscle belly of the biceps.
Cadaveric study Based on the above anatomy, we decided that the
site of our approach to the subacromial space and coracoacromial ligament would be 3 cm lateral and
5 cm distal to the coracoid process. We refer to this point as the anterior deltoid portal (Fig. 2). This portal is located between the clavicular (anterior fibers) and acromial part (central fibers) of the del- toid muscle. No important structures exist in this area or several centimeters lateral to and below the anterior portal, which is used for standard arthro- scopic surgery of a shoulder joint (2,3,13).
Before clinical applications, we applied our endo- scopic procedure to cadavers. Through blunt dis- section of the deltoid fascia and muscles, we ap- proached the subacromial space, reached the cora- coacromial ligament, and the ligament was resected with a rongeur without any problems (Fig. 1).
We conclude that the endoscope and surgical in- struments can be safely inserted from the anterior deltoid portal without injuring important structures adjacent to the operative site.
MATERIALS AND METHODS
From April 1988 to September 1990, 37 patients (40 shoulders) who suffered from shoulder impinge- ment syndrome, i.e., spontaneous shoulder joint pain, pain on motion, and some degree of restricted motion of the shoulder joint (6) were operated on at the Department of Orthopaedic Surgery of the Jap- anese Red Cross Medical Center. Seven patients (seven shoulders) were unavailable for follow-up study.
This study group consisted of 19 women (20 shoulders) and 11 men (13 shoulders). Nineteen right shoulders and 14 left shoulders were affected. Nineteen dominant shoulders were affected. The mean age of the patients was 49 years (range, 20-77 years). The duration of symptoms was l-84 months (mean, 13.3 months). The follow-up periods ranged from 12.7 to 41 months (mean, 29.7 months). Six shoulders presented a history of previous local trauma to the anterior part of the shoulder due to accidents during horseback riding, work, and traffic accidents. Other patients presented a history of overuse of the affected shoulders due to work or sports.
All patients complained of pain with forced for- ward elevation of the humerus against the acromion or with forward elevation, abduction, and rotation, internally or externally, as described by Hawkins and Kennedy (8). Positive impingement sign was noted in 23 affected shoulders. Healthy shoulders did not demonstrate a positive impingement sign. Tenderness was located at the coracoacromial liga-
Arthroscopy, Vol. 8. No. I, 1992

I. OKUTSU ET AL.
ment in all affected shoulders. The active and pas- sive range of motion of the affected shoulders were restricted to some degree. Nonsteroidal anti- inflammatory drugs were used daily; physiotherapy such as hot packs and/or active and passive mild range of motion exercises were not effective. How- ever, an injection of local anesthetic to the subacro- mial bursa as an impingement injection test (pain ablation test; 6) relieved the symptoms for up to 3 days in all patients. This kind of conservative treat-
FIG. 1. Anatomy. A: Cadaveric specimen. B: Schematic draw- ing. The sheath is inserted through the skin incision, which is located 3 cm lateral and 5 cm distal to the coracoid process, penetrates the deltoid muscle and enters the subacromial space. C: Cadaveric specimen. The external view of the coracoacromial ligament and the rotator cuff. The coracoacromial ligament is resected with the rongeur (arrow), which is inserted from the same skin incision and next to the endoscope system. AA, acromial artery; AC, acromion; AN, axillary nerve and artery; CAL, coracoacromial ligament; CP, coracoid process; DM, del- toid muscle; H, head of humerus; LB, long head of the biceps muscle; R, rotator cuff; S, sheath of the endoscope system.
ment continued for l-48 months before operation (mean, 7.3 months). Plain radiographs revealed no bony abnormalities as in hooked acromion, acro- mioclavicular osteophytes, or large coracoid pro- cess; however, calcification around the shoulder was demonstrated in one shoulder. We did not per- form ultrasound, arthrography, or magnetic reso- nance imaging.
The indications for operative treatment were the clinical signs (6-9), patient’s complaints, the effec-
Arthroscopy, Vol. 8, No. 1, 1992
USE SYSTEM AND SHOULDER 1MPINGEMENT
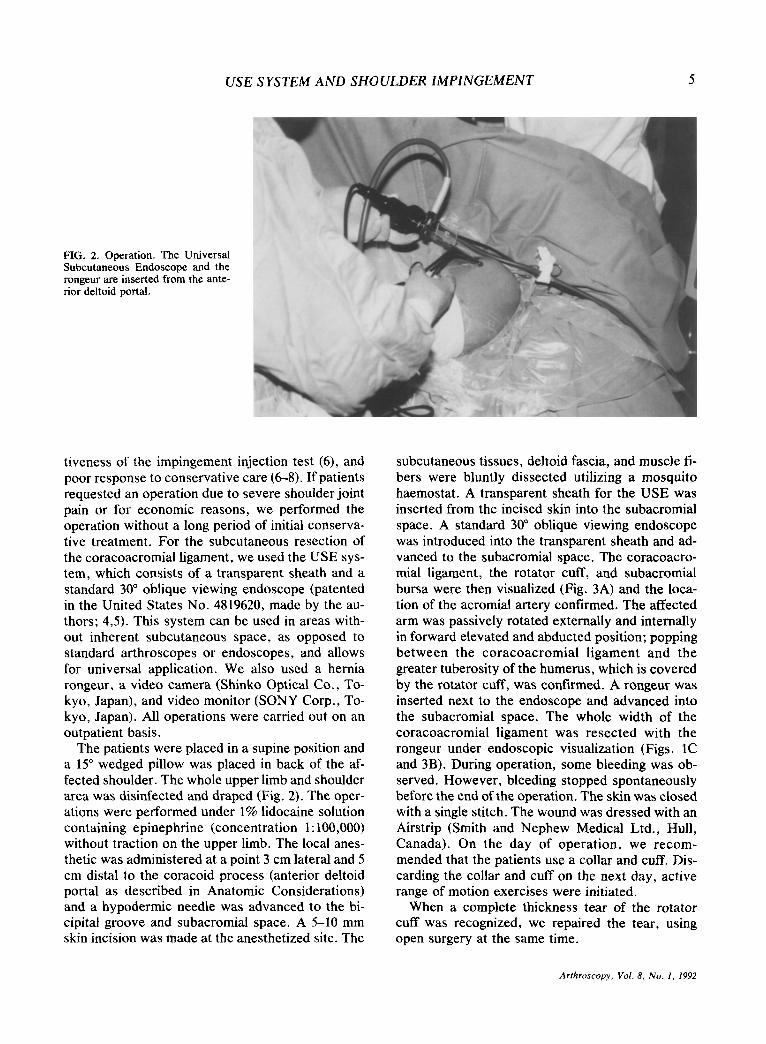
FIG . 2. Operation. The Universal Sub cutaneous Endoscope and the roq geur are inserted from the ante- rior deltoid portal.
tiveness of the impingement injection test (6), and poor response to conservative care (6-8). If patients requested an operation due to severe shoulder joint pain or for economic reasons, we performed the operation without a long period of initial conserva- tive treatment. For the subcutaneous resection of the coracoacromial ligament, we used the USE sys- tem, which consists of a transparent sheath and a standard 30” oblique viewing endoscope (patented in the United States No. 4819620, made by the au- thors; 4,5). This system can be used in areas with- out inherent subcutaneous space, as opposed to standard arthroscopes or endoscopes, and allows for universal application. We also used a hernia rongeur, a video camera (Shinko Optical Co., To- kyo, Japan), and video monitor (SONY Corp., To- kyo, Japan). All operations were carried out on an outpatient basis.
The patients were placed in a supine position and a 15” wedged pillow was placed in back of the af- fected shoulder. The whole upper limb and shoulder area was disinfected and draped (Fig. 2). The oper- ations were performed under 1% lidocaine solution containing epinephrine (concentration 1: 100,000) without traction on the upper limb. The local anes- thetic was administered at a point 3 cm lateral and 5 cm distal to the coracoid process (anterior deltoid portal as described in Anatomic Considerations) and a hypodermic needle was advanced to the bi- cipital groove and subacromial space. A 5-10 mm skin incision was made at the anesthetized site. The
subcutaneous tissues, deltoid fascia, and muscle fi- bers were bluntly dissected utilizing a mosquito haemostat. A transparent sheath for the USE was inserted from the incised skin into the subacromial space. A standard 30“ oblique viewing endoscope was introduced into the transparent sheath and ad- vanced to the subacromial space. The coracoacro- mial ligament, the rotator cuff, and subacromial bursa were then visualized (Fig. 3A) and the loca- tion of the acromial artery confirmed. The affected arm was passively rotated externally and internally in forward elevated and abducted position; popping between the coracoacromial ligament and the greater tuberosity of the humerus, which is covered by the rotator cuff, was confirmed. A rongeur was inserted next to the endoscope and advanced into the subacromial space. The whole width of the coracoacromial ligament was resected with the rongeur under endoscopic visualization (Figs. 1C and 3B). During operation, some bleeding was ob- served. However, bleeding stopped spontaneously before the end of the operation. The skin was closed with a single stitch. The wound was dressed with an Airstrip (Smith and Nephew Medical Ltd., Hull, Canada). On the day of operation, we recom- mended that the patients use a collar and cuff, Dis- carding the collar and cuff on the next day, active range of motion exercises were initiated.
When a complete thickness tear of the rotator cuff was recognized, we repaired the tear, using open surgery at the same time.
Arthroscopy. Vol. 8, No. I, 1992
6 I. OKUTSU ET AL.
3A,B
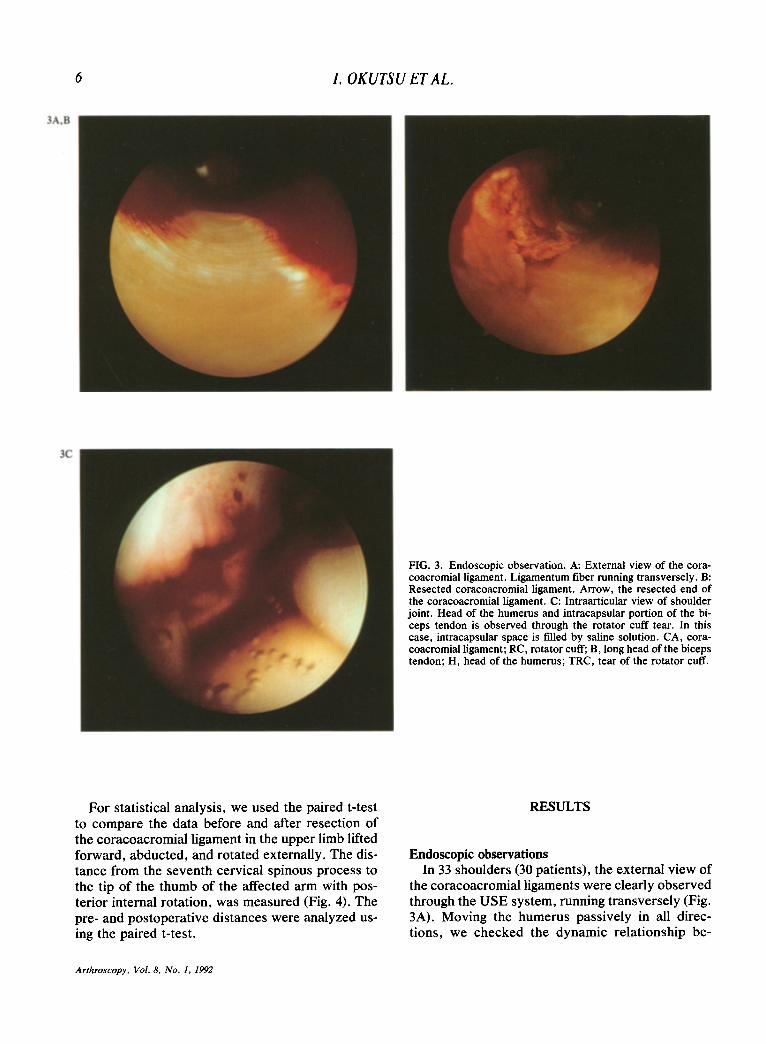
FIG. 3. Endoscopic observation. A: External view of the cora- coacromial ligament. Ligamentum fiber running transversely. B: Resected coracoacromial ligament. Arrow, the resected end of the coracoacromial ligament. C: Intraarticular view of shoulder joint. Head of the humerus and intracapsular portion of the bi- ceps tendon is observed through the rotator cuff tear. In this case, intracapsular space is tilled by saline solution. CA, cora- coacromial ligament; RC, rotator cuff, B, long head of the biceps tendon; H, head of the humerus; TRC, tear of the rotator cuff.
For statistical analysis, we used the paired t-test to compare the data before and after resection of the coracoacromial ligament in the upper limb lifted forward, abducted, and rotated externally. The dis- tance from the seventh cervical spinous process to the tip of the thumb of the affected arm with pos- terior internal rotation, was measured (Fig. 4). The pre- and postoperative distances were analyzed us- ing the paired t-test.
RESULTS
Endoscopic observations In 33 shoulders (30 patients), the external view of
the coracoacromial ligaments were clearly observed through the USE system, running transversely (Fig. 3A). Moving the humerus passively in all direc- tions, we checked the dynamic relationship be-
Arthroscopy, Vol. 8, No. 1, 1992
USE SYSTEM AND SHOULDER IMPINGEMENT 7
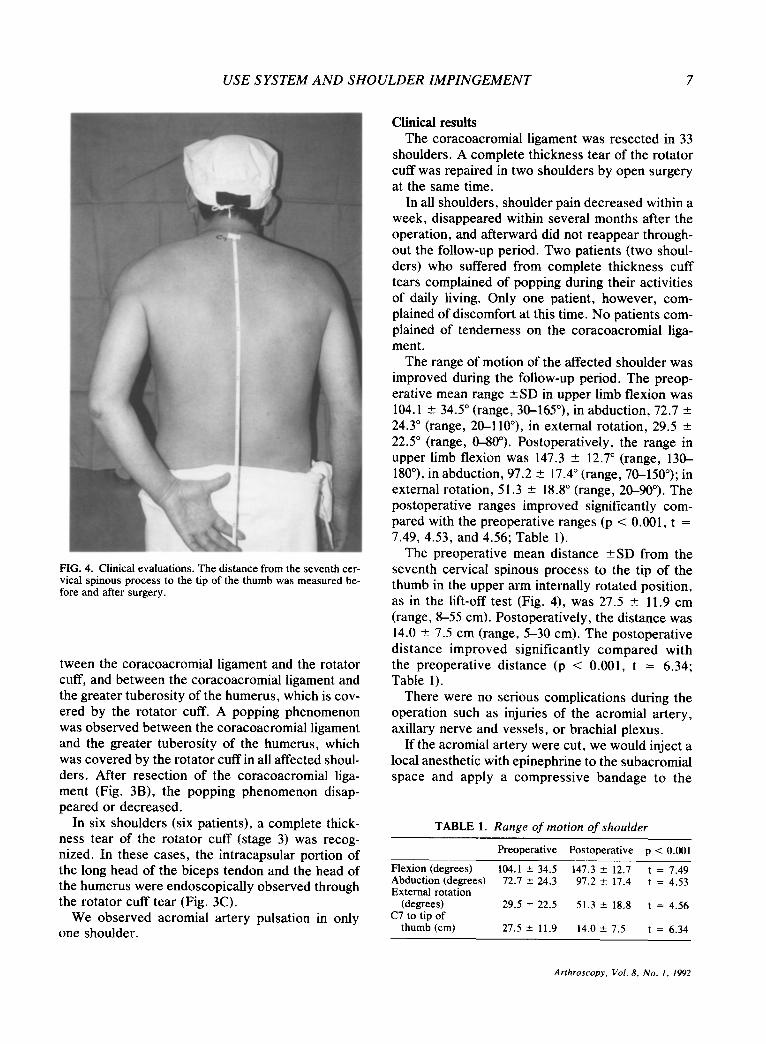
FIG. 4. Clinical evaluations. The distance from the seventh cer- vical spinous process to the tip of the thumb was measured be- fore and after surgery.
tween the coracoacromial ligament and the rotator cuff, and between the coracoacromial ligament and the greater tuberosity of the humerus, which is cov- ered by the rotator cuff. A popping phenomenon was observed between the coracoacromial ligament and the greater tuberosity of the humerus, which was covered by the rotator cuff in all affected shoul- ders. After resection of the coracoacromial liga- ment (Fig. 3B), the popping phenomenon disap- peared or decreased.
In six shoulders (six patients), a complete thick- ness tear of the rotator cuff (stage 3) was recog- nized. In these cases, the intracapsular portion of the long head of the biceps tendon and the head of the humerus were endoscopically observed through the rotator cuff tear (Fig. 3C).
We observed acromial artery pulsation in only one shoulder.
Clinical results The coracoacromial ligament was resected in 33
shoulders. A complete thickness tear of the rotator cuff was repaired in two shoulders by open surgery at the same time.
In all shoulders, shoulder pain decreased within a week, disappeared within several months after the operation, and afterward did not reappear through- out the follow-up period. Two patients (two shoul- ders) who suffered from complete thickness cuff tears complained of popping during their activities of daily living, Only one patient, however, com- plained of discomfort at this time. No patients com- plained of tenderness on the coracoacromial liga- ment.
The range of motion of the affected shoulder was improved during the follow-up period. The preop- erative mean range +SD in upper limb flexion was 104.1 2 34.5“ (range, 30-165”), in abduction, 72.7 2 24.3” (range, 20-llO”), in external rotation, 29.5 ? 22.5” (range, O-80”). Postoperatively, the range in upper limb flexion was 147.3 + 12.7” (range, 130- 180”), in abduction, 97.2 ? 17.4” (range, 7&150”); in external rotation, 51.3 + 18.8” (range, 20-90”). The postoperative ranges improved significantly com- pared with the preoperative ranges (p < 0.001, t = 7.49, 4.53, and 4.56; Table 1).
The preoperative mean distance +SD from the seventh cervical spinous process to the tip of the thumb in the upper arm internally rotated position, as in the lift-off test (Fig. 4), was 27.5 + 11.9 cm (range, 8-55 cm). Postoperatively, the distance was 14.0 2 7.5 cm (range, 5-30 cm). The postoperative distance improved significantly compared with the preoperative distance (p < 0.001, t = 6.34; Table 1).
There were no serious complications during the operation such as injuries of the acromial artery, axillary nerve and vessels, or brachial plexus.
If the acromial artery were cut, we would inject a local anesthetic with epinephrine to the subacromial space and apply a compressive bandage to the
TABLE 1. Range of motion of shoulder
Preoperative Postoperative p < 0.001
Flexion (degrees) 104.1 -c 34.5 147.3 t 12.7 t = 7.49 Abduction (degrees) 72.7 k 24.3 97.2 r 17.4 t = 4.53 External rotation
(degrees) 29.5 f 22.5 51.3 ” 18.8 t = 4.56 C7 to tip of
thumb (cm) 27.5 2 11.9 14.0 k 7.5 t = 6.34
Arthroscopy, Vol. 8. No. 1, 1992

8 I. OKUTSU ET AL.
shoulder. However, we did not experience this complication in this series.
Postoperatively, no patients suffered from subcu- taneous hematoma at the subacromial space. Imme- diate use of the upper limb did not cause any prob- lems .
DISCUSSION
Shoulder impingement syndrome was first de- scribed by Neer (7) in 1972 and afterward the syn- drome was classified into three stages (6): stage 1 (edema and hemorrhage), stage 2 (fibrosis and ten- donitis) and stage 3 (bone spurs and tendon rup- ture). The operations for stage 2, resection of the coracoacromial ligament, and stage 3, resection of the coracoacromial ligament and acromioplasty , can be successfully performed by open surgery un- der general anesthesia. Scars around the shoulder area, however, create anxiety for cosmetic reasons and early rehabilitation is restricted by surgical in- vasion. If the operation for shoulder impingement syndrome, however, could be safely performed un- der endoscopic visualization, a wide skin incision would not be necessary. In 1985, Ellman (1) devel- oped an endoscopic operative procedure for shoul- der impingement syndrome and overcame scarring and rehabilitation problems. It has also been shown that arthroscopic observation is effective for diag- nostic evaluation of shoulder problems. This proce- dure should be performed under general or local anesthesia with liquid irrigation and traction of the affected limb for muscle relaxation. Those proce- dures may cause subcutaneous hydrops formation and may discomfort patients. For this reason, ar- throscopic subacromial decompression may have as many demerits for patients as open operative pro- cedure (6-10).
Neer (6) reported that “arthroscopy has been less effective than arthrography in diagnosing cuff tears, . . . although it is considered by some to be helpful in the diagnosis of bursal-side, superficial, incom- plete tears.” We developed an operative procedure for shoulder impingement syndrome under local an- esthesia without the need for liquid irrigation or traction of the affected limb using the USE system (4,5). The surgical invasion involved in our endo- scopic procedure is the same as that involved in arthrography. However, our endoscopic procedure enables us to observe the dynamic relationship be- tween the coracoacromial ligament and the rotator
Arthroscopy, Vol. 8, No. 1. 1992
cuff, and between the coracoacromial ligament and the greater tuberosity of the humerus, which is cov- ered by the rotator cuff, conditions of the subacro- mial bursa (12) and complete thickness tears of the rotator cuff under endoscopic visualizations.
In clinical observations, range of motion of the shoulder joint was restricted in some cases due to pain and we noted a positive impingement sign in 23 affected shoulders. However, local anesthetic injec- tion to the subacromial space for an operation re- lieved the pain and improved the range of motion of the shoulder joint. We observed a popping between the coracoacromial ligament and the greater tuber- osity of the humerus in all 33 shoulders during en- doscopic observations.
If we can not observe a popping between the coracoacromial ligament and the greater tuberosity of the humerus, or find the cause of the shoulder problems related to the subacromial space and the rotator cuff, and/or clinical symptoms are not re- lieved after resection of the coracoacromial liga- ment, arthroscopic observation inside of the shoul- der, magnetic resonance imaging, and other exam- inations are necessary.
Some patients are able to compensate for rotator cuff function and some recover spontaneously in clinical course. We repaired cuff tears in two pa- tients. These patients were manual laborers and so open surgery was performed to ensure that the ro- tator cuff would be functional as soon as possible. In other cases who suffered from complete thick- ness tears, preoperative clinical signs disappeared and functional recovery was observed without any surgical interventions without resection of the coracoacromial ligament.
We conclude from clinical and endoscopic obser- vations, that the endoscope and surgical instru- ments can be safely inserted from the anterior del- toid portal without injuring important structures ad- jacent to the operative site and our surgical procedure is useful for diagnosis of stage 2 or stage 3 shoulder impingement syndrome. Resection of the coracoacromial ligament using the USE system may be useful for the treatment of stage 2 and stage 3 shoulder impingement syndrome.
REFERENCES
1. Ellman H. Arthroscopic subacromial decompression. A pre- liminary report. Orthop Tram 1985;9:43.

USE SYSTEM AND SHOULDER IMPINGEMENT 9
2. Mendoza FX, Nicholas JA, Rubinstein MP. The arthro- scopic treatment of subacromial impingement. Seminars Or- thop 1988;3:88-92.
3. Paulos LE, Hamer CD, Parker RD. Arthroscopic subacro- mial decompression for impingement syndrome of the shoul- der. Techniques Orthop 1988;3:33-9.
4. Okutsu I, Hamanaka I, Ninomiya S, Tamai K, Takatori Y, Abe I. Shoulder impingement syndrome in hemodialysis pa- tients. Arthroscopy 1989;14:59-62.
5. Okutsu I, Ninomiya S. Takatori Y, Ugawa Y. Endoscopic management of carpal tunnel syndrome. Arthroscopy 1989; 5:11-8.
6. Neer CS, Jr. Impingement lesions. Clin Orthop 1983;173: 70-7.
7. Neer CS, Jr. Anterior acromioplasty for the chronic im- pingement syndrome in the shoulder. J Bone Joint Surg [Am] 1972;54:41-SO.
8. Hawkins RJ, Kennedy JC. Impingement syndrome in ath- letes. Am J Sports Med 1980;8:151-8.
9. Ha’eri GB, Wiley AM. Shoulder impingement syndrome. C/in Orthop 1982;168:128-32.
10. Penny JN, Welsh RP. Shoulder impingement syndrome in athletes and their surgical management. Am J Sports Med 1981;9:11-5.
11. Uhthoff HK, Hammond DI, Sarkar K, Hooper GJ, Papoff WJ. The role of the coracoacromial ligament in the impinge- ment syndrome. Inter Orthop 1988;12:97-104.
12. Okutsu I, Ninomiya S, Takatori Y, Hamanaka I, Takemura T, Otsubo K, Otsubo 0. Endoscopic management of shoul- der pain in long-term haemodialysis patients. Nephrol Dial Transplanr 1991;6:117-9.
13. Schonholtz GJ. Arthroscopic surgery ofthe shoulder, elbow and ankle. Springfield: Charles C. Thomas Publisher, 1986:29-47.
Arthroscopy, Vol. 8, No. I, 1992