copd in icu
TRANSCRIPT

COPD in ICU
Dr Laura-Jane Smith
ST5 Respiratory Medicine

COPD refresher
Caring for patients with COPD in ICU
Patient selection for ICU?

SMOKING IS COOL
True False

WHAT DO WE DIE FROM?


COPD REFRESHER

1. COPD is caused solely by cigarette smoking
2. COPD is characterised by reversible flow limitation
3. Marijuana inhalation causes airflow limitation
True False
True False
True False

Inhaled noxious
particles
(eg cigarette smoke,
solid fuel fire smoke)
Inflammation,
white cell
recruitment
Bronchial wall
thickening
and fibrosis
Mucous gland
hyperplasia
Alveolar
destruction
(neutrophil
proteases)
CHRONIC
BRONCHITIS
SMALL AIRWAYS
NARROWING AND
OBSTRUCTION
EMPHYSEMA, BULLAE
LOSS OF ELASTIC RECOIL
DYNAMIC AIRWAYS
COLLAPSE

Images from Eureka: Respiratory Medicine 2015. Smith, Quint, Brown

• Loss of alveolar volume
• Impaired ventilation (poor respmechanics)
• Obstruction and air trapping
Baseline impaired oxygenation
• Hypoxaemia due to infection/inflammation
• Worsening airflow limitation
• V/Q mismatch
Poor tolerance of small
pulmonary insult
• Increased minute volume (but Vt limited)
• Increased RR (dec exp time and worse air trapping)
• Dynamic hyperinflation
Maladaptive patient response
• Respiratory efficiency declines
• Work of breathing unsustainable
• Patient tires
Respiratory failure
Path
op
hys
iolo
gy o
f ac
ute
res
pir
ato
ry f
ailu
re in
CO
PD
Chest wall mechanics
Nutritional deficiencies
Pulmonary hypertension
Chronic CO2 retention
Diaphraghmatic weakness
Obesity
Rocco, Monica, et al. "Respiratory failure in COPD." Trends in Anaesthesiaand Critical Care 3.3 (2013): 105-108.

Standard treatment
• Oxygen
• Bronchodilators
• Corticosteroids
• Antibiotics
• Prophylactic LMWH
• NIV?

CARING FOR PATIENTS WITH COPD IN ICU

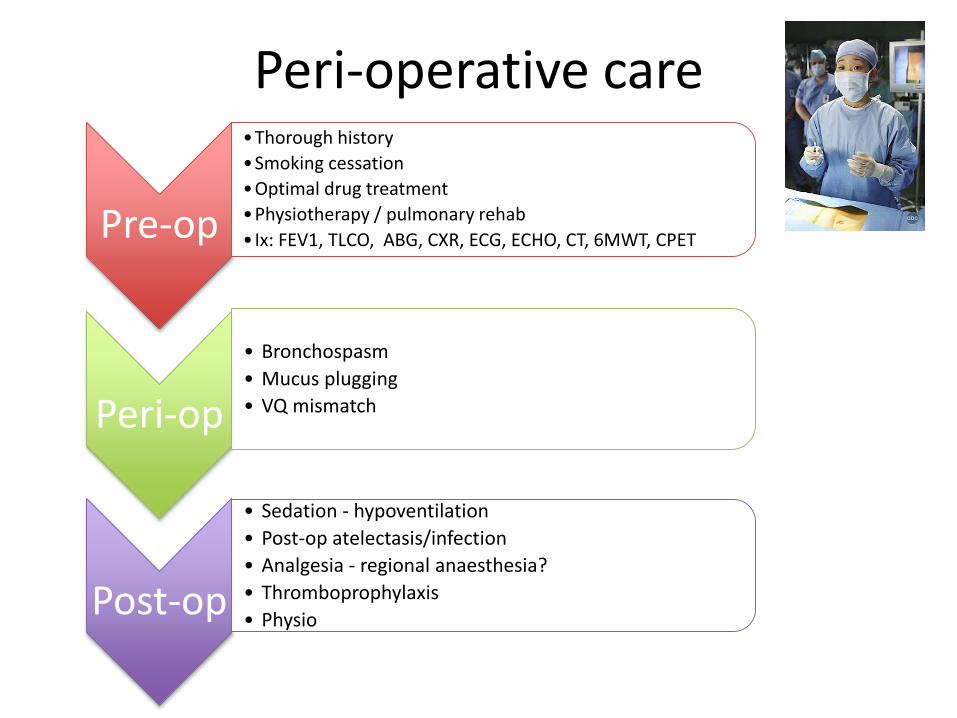
Pre-op
•Thorough history
•Smoking cessation
•Optimal drug treatment
•Physiotherapy / pulmonary rehab
• Ix: FEV1, TLCO, ABG, CXR, ECG, ECHO, CT, 6MWT, CPET
Peri-op
• Bronchospasm
• Mucus plugging
• VQ mismatch
Post-op
• Sedation - hypoventilation
• Post-op atelectasis/infection
• Analgesia - regional anaesthesia?
• Thromboprophylaxis
• Physio
Peri-operative care

Meet Ethel…
• 85 years old• Current smoker 10/day• Infective exacerbation of COPD - worsened despite early
initiation of rescue pack• No previous ICU admission. Required NIV following THR,
and 2 years ago following flu. Last exac treated in community 4/12 ago. Returned to baseline function
• Co-morbidities: MI with PCI age 65, mild LVSD, hypothyroidism, THR age 80
• Lives in sheltered accommodation, walks to corner shop twice a week, family do main shopping, has cleaner as breathless on hoovering, dresses self. Daughter helps bathe weekly, otherwise daily strip wash (independent).

Treatment
• Oxygen
• Bronchodilators
• Corticosteroids
• Antibiotics
• Prophylactic LMWH
On admission:pH 7.28PaO2 11.7PaCO2 7.9HCO3 27.9FiO2 35%
T: 35.5P: 110bpm BP: 100/55RR: 30
Hb 14.7g/dLPlt 152x10^9/LWCC 17.2x10^9/LNa 143 mmol/LK 4.0 mmol/LUr 6.0 mmol/LCreat 110 umol/LBili 12 umol/LAlb 38 g/L
At 2am: pH 7.07PaO2 9.2PaCO2 11.29HCO3 24.4FiO2 24%
1. Early initiation of NIV leads to better outcomes
1. Ipratropium nebulisersincrease viscosity of secretions
2. NIV is contraindicated if pH < 7.1
True False
True False
True False

Non-invasive ventilation
Avoids complications of invasive ventilation including airway trauma, sedation, VAP
Can be offered outside ICU
Early initiation, better outcomes1
Younger, cooperative, moderate hypercarbia (6 -12) and moderate acidosis (7.1 – 7.3), better outcomes2
1. Celikel T, Sungur M, Ceyhan B, et al. Comparison of noninvasive positive pressure ventilation with standard medical therapy in hypercapnic acute respiratory failure. Chest. 1998;114:1636–42
2. Evans T, Albert R, Angus D, et al. Noninvasive Positive Pressure Ventilation in acute respiratory failure. Am J Respir Crit Care Med. 2001;163:283–91

Predicting NIV failure
pH <7.25
RR >30APACHE II > 29
GCS <11
Confalonieri M, Garuti G, Cattaruzza MS, et al. A chart of failure risk for noninvasive ventilation in patients with COPD exacerbation. Eur Respir J. 2005;25:348–55
70% risk of intubation
pH < 7.25 90% risk of intubation
At
adm
issi
on
A
t 2
ho
urs

TO INTUBATE OR NOT TO INTUBATE
Intubate Don’t

HOW SHOULD WE SELECT PATIENTS?
The million dollar question

Who survives ICU?
Who leaves hospital?
How much does it cost?
What QoLdo survivors
have?
Who wants to come to
ICU?

CAOS
Wildman, Martin J., et al. "Implications of prognostic pessimism in patients with chronic obstructive pulmonary disease (COPD) or asthma admitted to intensive care in the UK within the COPD and asthma outcome study (CAOS): multicentre observational cohort study." BMJ 335.7630 (2007): 1132.
Who survives
ICU?
Doctors are pessimistic – or are they?
Survival:• to discharge from
ICU/HDU 80% • to discharge from
hospital 70%• at 180 days 62%
Who leaves hospital?

SUPPORTWho
survives ICU?
Who leaves hospital?
Connors Jr, Alfred F., et al. "Outcomes following acute exacerbation of severe chronic obstructive lung disease. The SUPPORT investigators (Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments)." American journal of respiratory and critical care medicine 154.4 (1996): 959-967.
Survival:
• to hospital discharge 89%
• at 60 days 80%
• at 180 days 66%
• at 1 year 57%
• at 2 years 51%
Cost:
• $7000 ($4100 - £16000)
LOS:
• 9 days (5 – 15 days)
Readmissions:
• 446 patients were readmitted 754 times in next 6/12

SUPPORTWho
survives ICU?
Who leaves hospital?
Connors Jr, Alfred F., et al. "Outcomes following acute exacerbation of severe chronic obstructive lung disease. The SUPPORT investigators (Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments)." American journal of respiratory and critical care medicine 154.4 (1996): 959-967.
Survival time independently related to:
• Severity of illness
• BMI
• Age
• Prior functional status
• PaO2/FiO2
• CCF
• Serum albumin
• Cor pulmonale
“Patients and caregivers should be aware of the likelihood of
poor outcomes following hospitalization for exacerbation
of COPD associated with hypercarbia.”

Who survives
ICU?
Who leaves hospital?
Ai-Ping, Chua, Kang-Hoe Lee, and Tow-Keang Lim. "In-hospital and 5-year mortality of patients treated in the ICU for acute exacerbation of COPD: a retrospective study." CHEST Journal 128.2 (2005): 518-524.
Survival:
• to hospital discharge 75%
• at 6 months 61%
• at 1 year 57%
• At 3 years 39%
• At 5 years 24%
Hospital mortality correlated with:
• Age
• Hx of MV
• Long term steroid use
• Albumin level
• APACHE II score
• Duration of hospitalisation
No factors predictive of mortality at 5 years were identified.
IFYMOPITITCUFAEOCOPD

POOP-COPD-IMV
Nevins, Michael L., and Scott K. Epstein. "Predictors of outcome for patients with COPD requiring invasive mechanical ventilation." CHEST Journal 119.6 (2001): 1840-1849.
Survival:
• to hospital discharge 72% – 88% if no comorbid illness
Who survives
ICU?
Who leaves hospital?
Hospital mortality correlated with:
Univariate analysis
• >72hr IMV (37% vs 16% p<0.01)
• Prev IMV (33% vs 11% p=0.0001)
• Failed extubation attempt (36% vs 7% p = 0.0001)
Multiple logistical regression
• high APS >6hr after IMV
• malignancy
• Comorbidity
• IMV >72hrDisposition of patients at time of discharge from hospitalCCF = chronic care facility
TO INTUBATE OR NOT TO INTUBATE
Intubate Don’t
APACHE II = 32 = 76% mortality

HRQL in ICU survivorsWhat QoL
do survivors have?
Berkius, Johan, et al. "A prospective longitudinal multicentre study of health related quality of life in ICU survivors with COPD." Crit Care 17.5 (2013): R211.

CAOSWhat QoL
do survivors have?
Wildman, Martin James, et al. "Survival and quality of life for patients with COPD or asthma admitted to intensive care in a UK multicentre cohort: the COPD and Asthma Outcome Study (CAOS)." Thorax 64.2 (2009): 128-132.

© 2003 by the Society of Critical Care Medicine and Lippincott Williams & Wilkins. Published by Lippincott Williams & Wilkins, Inc.
2
Medical futility: Predicting outcome of intensive care unit patients by nurses and doctors-A prospective comparative study*.Frick, Sonia; Uehlinger, Dominik; ZuercherZenklusen, Regula
Critical Care Medicine. 31(2):456-461, February 2003.DOI: 10.1097/01.CCM.0000049945.69373.7C
Figure 1 . Answers of survivors 6 months after intensive care unit discharge for whom treatment had been considered futile or questionable in regard to survival by nurses or doctors. indep., independent;dep., dependent.
What QoLdo survivors
have?
Frick S, Uehlinger DE, Zuercher Zenklusen RM. Medical futility: predicting outcome of intensive care unit patients by nurses and doctors—a prospective comparative study. Crit Care Med 2003;31:456-61.

I WANT ADDITIONAL QUANTITY OF LIFE AT ALL COSTS
True False

Who wants to come to
ICU?
Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med 2002;346:1061-6.

Who wants to come to
ICU?
Fried TR, Bradley EH, Towle VR, Allore H. Understanding the treatment preferences of seriously ill patients. N Engl J Med 2002;346:1061-6.
“The provision of care at the end of life should honor
patients' preferences. If these preferences are to be
honored, they must first be understood.“

COPD vs lung cancer
Claessens, Michael T., et al. "Dying with lung cancer or chronic obstructive pulmonary disease: insights from SUPPORT. Study to Understand Prognoses and Preferences for Outcomes and Risks of Treatments." Journal of the American Geriatrics Society 48.5 Suppl (2000): S146-53.
Who wants to come to
ICU?
Who wants to come to
ICU?

I HAVE WRITTEN AN ADVANCE DIRECTIVE
True False

YouGov poll 2014

http://compassionindying.org.uk/

Conclusions
• Smoking is not cool• Patient selection is key to ensuring good
outcomes for patients with COPD admitted to ICU, and using resources appropriately
• We have inadequate data/tools to predict prognosis in COPD. Previous functional status, BMI, and comorbidities are probably best
• ICU and specialities need to work together to improve process of decision making
• We are missing opportunities for advance care planning. We must involve patients earlier/more meaningfully

@drlaurajane