constipation pharmacotherapy constipation pharmacotherapy rastegarpanah clinical pharmacy department...
TRANSCRIPT


ConstipatioConstipation n
PharmacotherPharmacotherapyapy
RastegarpanahRastegarpanahClinical pharmacy DepartmentClinical pharmacy Department
Shariati GI Research CenterShariati GI Research CenterTehran university of medical sciencesTehran university of medical sciences
DEFINITION
A Disturbance In Bowel Function. A Disturbance In Bowel Function.
Stools Too Hard Or Too Small, Defecation Stools Too Hard Or Too Small, Defecation Too Difficult Or Infrequent.Too Difficult Or Infrequent.
““Normal” 3 Times / Day To 3 Times / WeekNormal” 3 Times / Day To 3 Times / Week
A Stool Frequency Of A Stool Frequency Of Less Than Three Per Less Than Three Per WeekWeek

EPIDEMIOLOGY
Prevalence Prevalence 12-19%12-19%
Prevalence Chronic Constipation Rises Prevalence Chronic Constipation Rises With Age, (With Age, (65 Years65 Years Of Age Or Older). Of Age Or Older).
In Old Age, 26% Of Men & In Old Age, 26% Of Men & 34%34% Of Women Of Women
Common In Pregnancy.Common In Pregnancy.
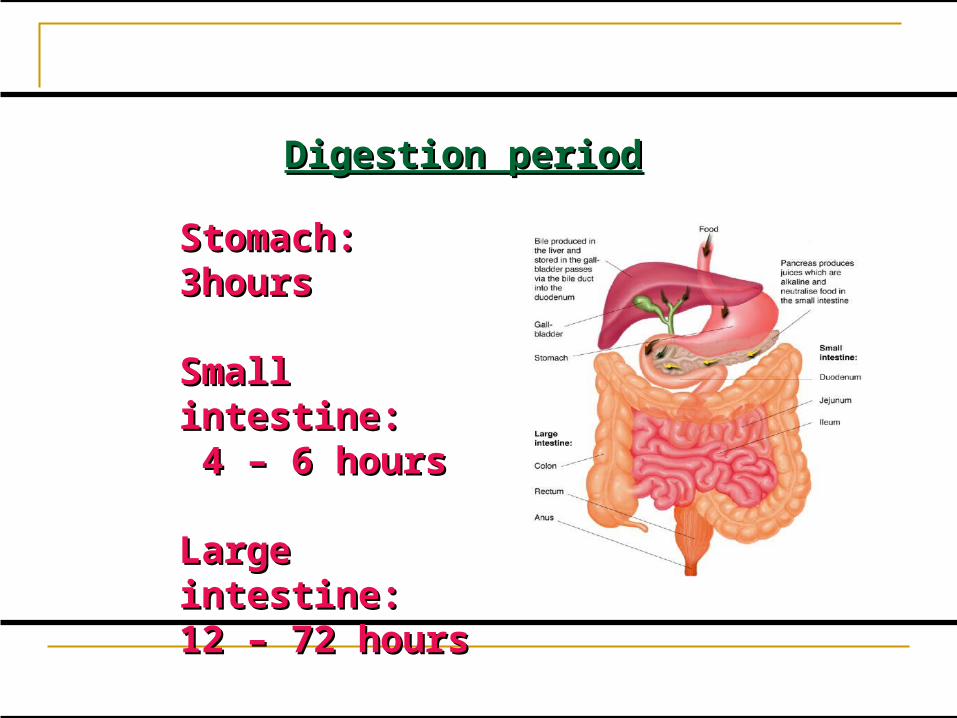
Digestion periodDigestion period
Stomach: Stomach: 3hours3hours
Small intestine:Small intestine: 4 – 6 hours4 – 6 hours
Large intestine: Large intestine: 12 – 72 hours12 – 72 hours
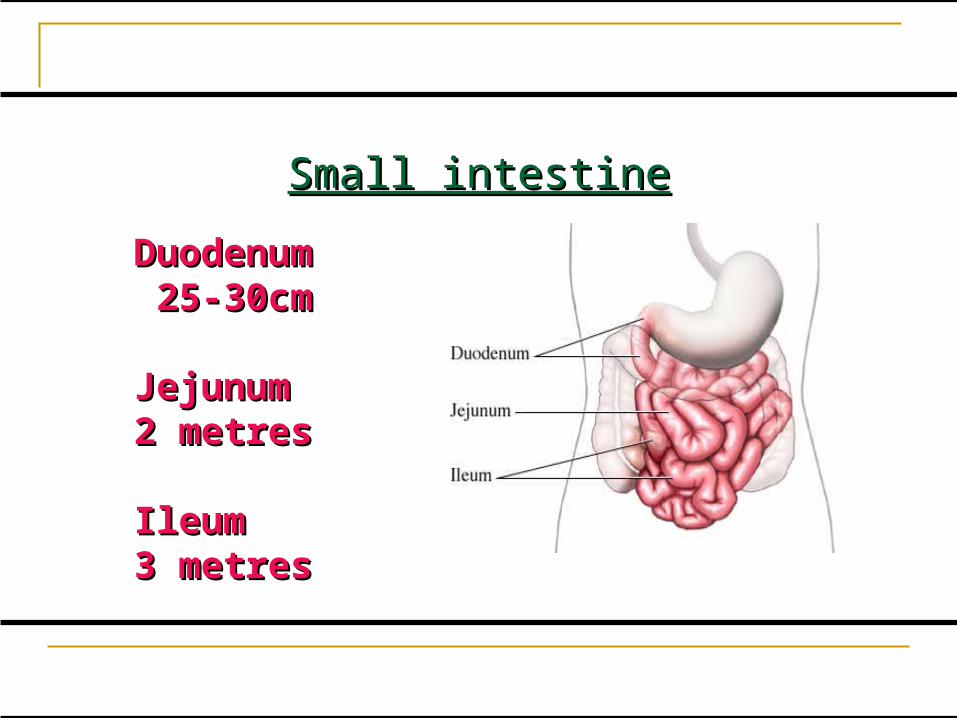
Small intestineSmall intestine
Duodenum Duodenum 25-30cm25-30cm
Jejunum Jejunum 2 metres2 metres
Ileum Ileum 3 metres3 metres
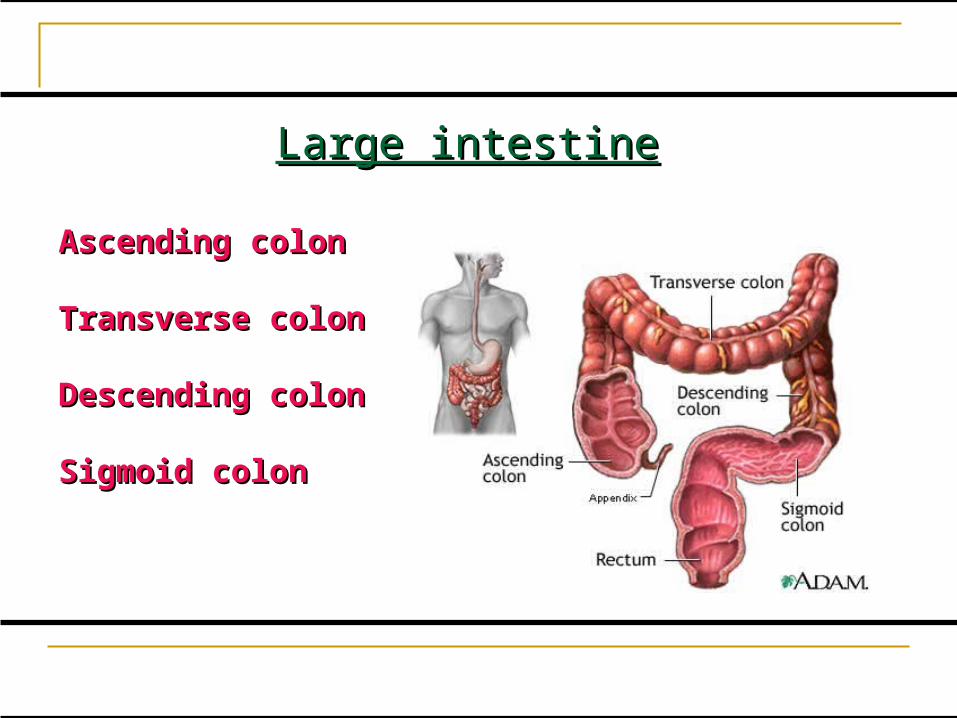
Large intestineLarge intestine
Ascending colonAscending colon
Transverse colonTransverse colon
Descending colonDescending colon
Sigmoid colonSigmoid colon
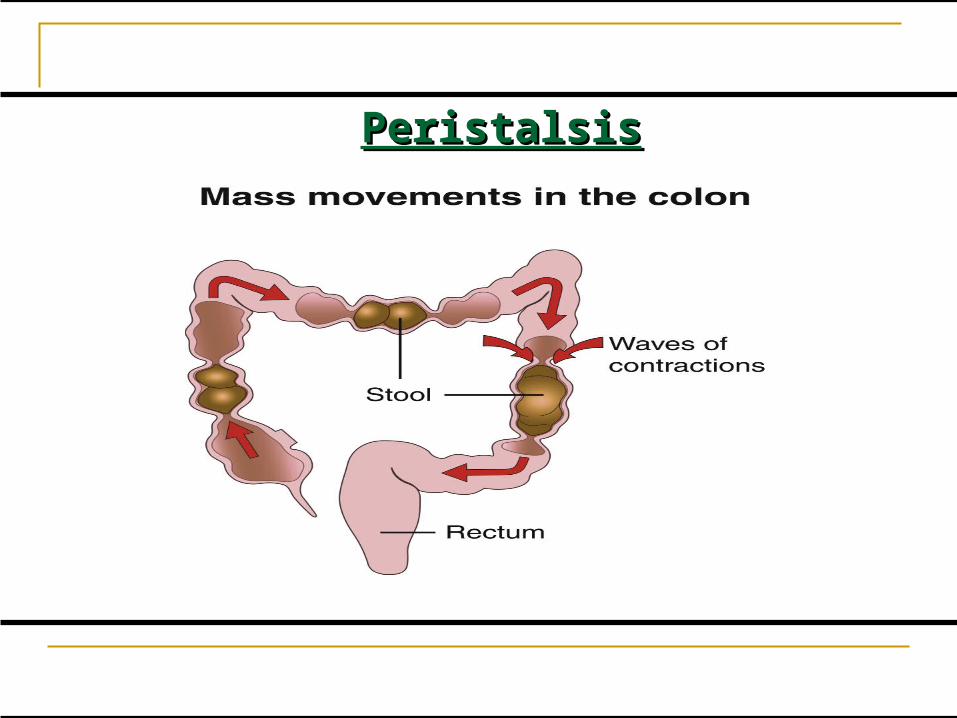
PeristalsisPeristalsis
ExcretionExcretion
1.1.Muscles work together to propel waste Muscles work together to propel waste matter (Peristalsis)matter (Peristalsis)
2.2.substances not absorbed by the body substances not absorbed by the body becomes faecesbecomes faeces
3.3.Faeces arrives in rectum to be expelled Faeces arrives in rectum to be expelled
What affects the bowel?What affects the bowel?
1.1. Poor dietPoor diet
2.2. Lack of fluidLack of fluid
3.3. Low MobilityLow Mobility
4.4. MedicationsMedications
5.5. SurgerySurgery
PATHOPHYSIOLOGY
ConstipationConstipation = disordered movement of = disordered movement of stool through colon or rectum stool through colon or rectum
Slowing of colonic transit idiopathic or: Slowing of colonic transit idiopathic or: Due to diseases Due to diseases Side effect of drugsSide effect of drugs
Etiology: Disease-Induced: 1. Irritable bowel syndrome2. Metabolic disorders (diabetes),3. Endocrine disorders (hypothyroidism),4. Neurogenic disorders (Diabetes
mellitus, Multiple sclerosis , Spinal cord injury).
Drug-Induced Psychogenic causes Life-style factors Old age Children

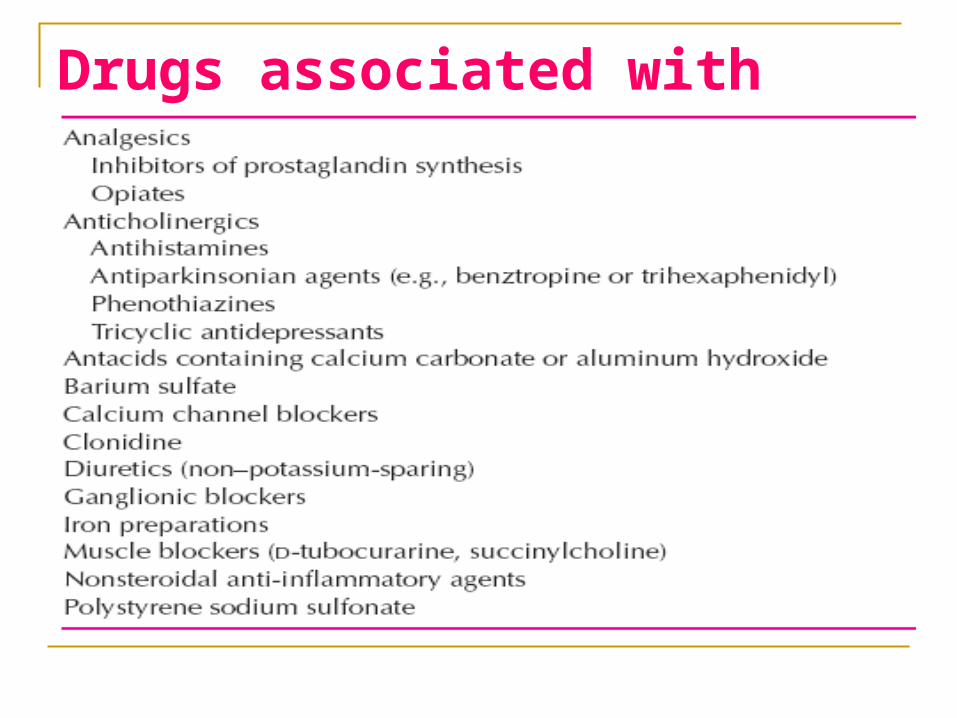
Drugs associated with constipation

Constipation in Constipation in ElderlyElderly Constipation Is Common: Constipation Is Common:
Improper Diets (Low In Fiber And Liquids)Improper Diets (Low In Fiber And Liquids) Diminished Abdominal Wall Muscular StrengthDiminished Abdominal Wall Muscular Strength Possibly Diminished Physical ActivityPossibly Diminished Physical Activity
Frequency Of Bowel Movements Is Not Decreased Frequency Of Bowel Movements Is Not Decreased With Aging. With Aging.
Diseases Such As Colon Cancer And Diverticulitis,Diseases Such As Colon Cancer And Diverticulitis, Drugs In Elderly:Drugs In Elderly:
Anticholinergics, Aspirin, Furosemide, Anticholinergics, Aspirin, Furosemide, Nitroglycerin, AmitriptylineNitroglycerin, Amitriptyline

Signs and Symptoms :Signs and Symptoms :1.1. Decrease in frequency of fecal Decrease in frequency of fecal
eliminationelimination
2.2. Difficult passage of dry hard stoolsDifficult passage of dry hard stools
3.3. Straining to have stoolStraining to have stool

Diagnostic Criteria Diagnosis Based On Presence Of Following Diagnosis Based On Presence Of Following For For
At Least Three Months (With Symptom Onset At Least Three Months (With Symptom Onset At Least Six Months Prior To Diagnosis). At Least Six Months Prior To Diagnosis).
Diagnostic CriteriaMust Have Must Have Two Or MoreTwo Or More Of Following: Of Following:
1.1. Hard StoolsHard Stools In 25% Of Defecations In 25% Of Defecations
2.2. Sensation Of Sensation Of Incomplete EvacuationIncomplete Evacuation For For At Least 25% Of Defecations At Least 25% Of Defecations
3.3. Sensation Of Sensation Of Anorectal Obstruction / Anorectal Obstruction / BlockageBlockage For At Least 25% Of For At Least 25% Of Defecations Defecations
4.4. Fewer Than Fewer Than Three DefecationsThree Defecations Per Week Per Week
CONSTIPATION
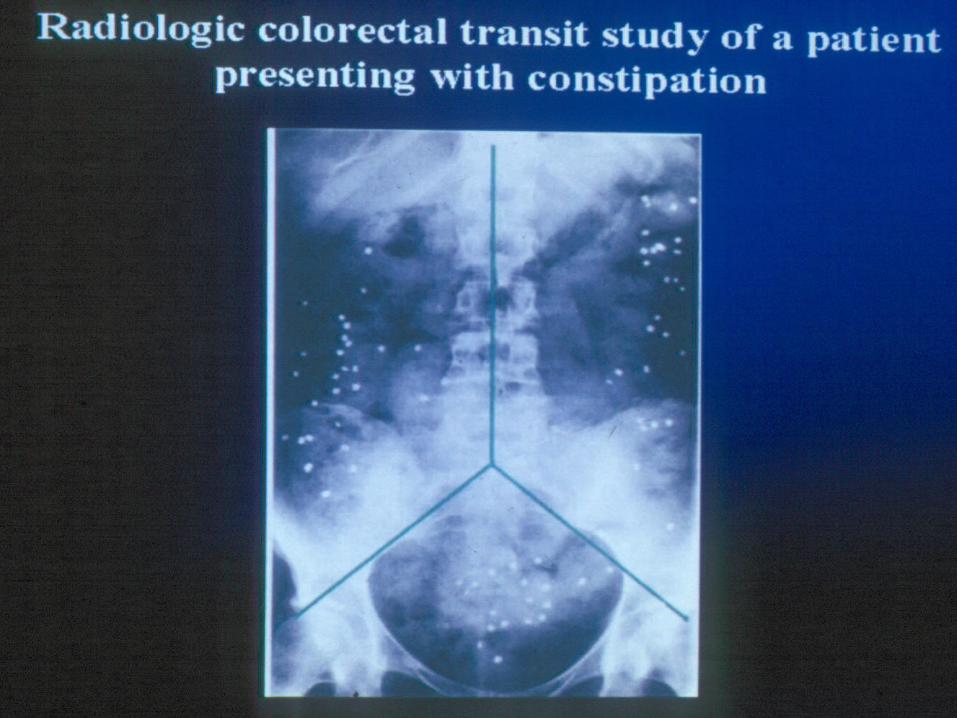
Diagnostic Studies: Colonic Transit Time (CTT):
radio-opaque markers & day 4 X-ray.
Ten markers daily for six days
No laxative and drugs

CTTCTT In Evaluating Patients With In Evaluating Patients With
Chronic Idiopathic Constipation.Chronic Idiopathic Constipation. It Is Available And Has No It Is Available And Has No
Complication.Complication. No Surgical Intervention Without No Surgical Intervention Without
Colonic Transit Study Is Colonic Transit Study Is Recommended .Recommended .
Patient Assessment
Obtain Lifestyle And Medical History Before Obtain Lifestyle And Medical History Before Making Any RecommendationsMaking Any Recommendations
Determine Reason For Use Of A LaxativeDetermine Reason For Use Of A Laxative
1. To Relieve Constipation1. To Relieve Constipation
2. To Evacuate The Bowel Prior To An 2. To Evacuate The Bowel Prior To An Upcoming Radiologic Or Endoscopic Upcoming Radiologic Or Endoscopic ExaminationExamination
Inquire About The Patient’s Current And Inquire About The Patient’s Current And Past Use Of Laxative ProductsPast Use Of Laxative Products

Treatment
If Underlying Disease Is Recognized, If Underlying Disease Is Recognized, Cause Should Be Correct It. Cause Should Be Correct It.
GI Cancer Removed Via Surgery. GI Cancer Removed Via Surgery. Endocrine And Metabolic Dz Corrected. Endocrine And Metabolic Dz Corrected. If Hypo-thyroidism, Thyroid-replacement If Hypo-thyroidism, Thyroid-replacement
Therapy .Therapy .
Refer to M.D. When……
Symptoms Have Persisted For Symptoms Have Persisted For More More Than 2 WeeksThan 2 Weeks
Recurred After Previous Dietary Or Recurred After Previous Dietary Or Lifestyle Changes Or Laxative UseLifestyle Changes Or Laxative Use
Patients With Patients With BloodBlood In The Stool In The Stool
ManagementManagement
1. Dietary Modification.
2. Increase In Daily Fiber.
3. Exercise (Even By Walking After Dinner)
4. Bowel Habits, Regular & Adequate Time To Respond To Urge To Defecate.
5. Increase Fluid Intake.
Non-drug Treatment
1.1. High Fiber Food: Wheat Grains, Oats, Or High Fiber Food: Wheat Grains, Oats, Or Fruits & VegetablesFruits & Vegetables
2.2. Adequate Fluid IntakeAdequate Fluid Intake
3.3. ExerciseExercise
4.4. Avoid Foods That Cause Constipation: Avoid Foods That Cause Constipation: (Cheeses & Sweets)(Cheeses & Sweets)
NON-PHARMACOLOGIC THERAPY
FiberFiber Increases Stool Bulk,Increases Stool Bulk, Retention Stool Water & Increases Rate Retention Stool Water & Increases Rate
TransitTransit Increase Frequency Of DefecationIncrease Frequency Of Defecation Fruits, vegetables, cereals have highest fiber Fruits, vegetables, cereals have highest fiber Bran, a by-product of milling of wheat, Bran, a by-product of milling of wheat, Trial of dietary high-fiber should be for at Trial of dietary high-fiber should be for at
least 1 month before effects on bowel least 1 month before effects on bowel function are determinedfunction are determined


Non Prescription MedicationsNon Prescription MedicationsOver The Counter (OTC)Over The Counter (OTC)
Types of laxatives:Types of laxatives:1.1. Bulk FormingBulk Forming
2.2. EmollientEmollient
3.3. LubricantLubricant
4.4. SalineSaline
5.5. Hyper-osmoticHyper-osmotic
6.6. StimulantStimulant
DRUG CLASSESDRUG CLASSES
Most Induce Bowel Evacuation By: Active Electrolyte Secretion Decreased Water And Electrolyte
Absorption Increased Intraluminal Osmolarity Increased Hydrostatic Pressure In The Gut
Three Classifications:Three Classifications:
1.1. Softening Of FecesSoftening Of Feces In 1 To 3 Days (Bulk- In 1 To 3 Days (Bulk-forming Laxatives, And Lactulose)forming Laxatives, And Lactulose)
2.2. Semifluid StoolSemifluid Stool In 6 To 12 Hours In 6 To 12 Hours (Bisacodyl);(Bisacodyl);
3.3. EvacuationEvacuation In 1 To 6 Hours (Magnesium In 1 To 6 Hours (Magnesium Hydroxide, Castor Oil, And Polyethylene Hydroxide, Castor Oil, And Polyethylene Glycol-electrolyte Solution).Glycol-electrolyte Solution).
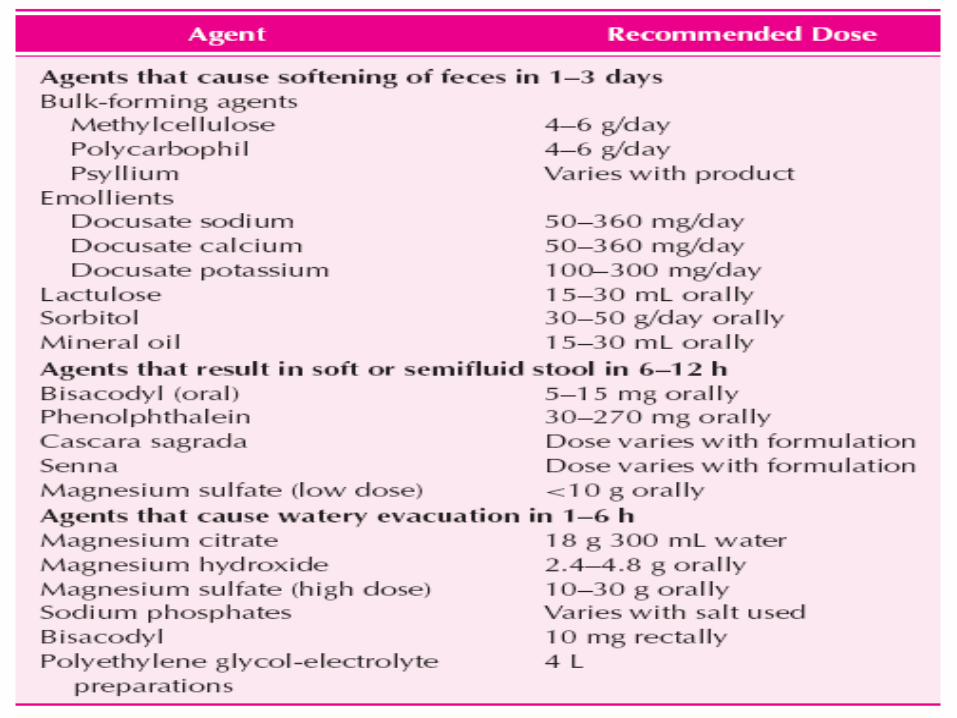
Dosage Recommendations for Laxatives and Cathartics
Bulk Forming LaxativesBulk Forming Laxatives
Derived From Agar, Or Psyllium SeedDerived From Agar, Or Psyllium Seed Synthetic, Methylcellulose & Carboxymethyl Synthetic, Methylcellulose & Carboxymethyl
Cellulose Sodium Cellulose Sodium Dissolve In Intestinal Fluid, Thus Creating Emollient Dissolve In Intestinal Fluid, Thus Creating Emollient
Gels That Increase Passage Of Intestinal ContentsGels That Increase Passage Of Intestinal Contents Stimulate Peristalsis Stimulate Peristalsis No Systemic AbsorptionNo Systemic Absorption

Bulk Forming LaxativesBulk Forming Laxatives
Onset of action is 12-24hrsOnset of action is 12-24hrs physiologic in promoting evacuation physiologic in promoting evacuation FIRST choice for constipationFIRST choice for constipation Examples are: Examples are:
Citrucel powder, Metamucil, Mitrolan Chewable Tablets
Bulk Forming LaxativesBulk Forming Laxatives
Caution In Younger Than 6 Yrs Of AgeCaution In Younger Than 6 Yrs Of Age Avoid In Intestinal Ulcerations, StenosisAvoid In Intestinal Ulcerations, Stenosis Interact With Anticoagulants, Digitalis Interact With Anticoagulants, Digitalis
Glycosides, And Salisylates Glycosides, And Salisylates Not Used For A Fast Clearing Effect Before A Not Used For A Fast Clearing Effect Before A
Diagnostic Procedure Diagnostic Procedure Used Daily And Continued In Most Patients, With Used Daily And Continued In Most Patients, With
Chronic Constipation. Chronic Constipation.
Emollient Laxatives
Anionic Surfactants, Softening Of Stool Systemically Absorbed (Solid) Onset Of Action (Oral) 24-72hrs As A Stool Softener, & To Prevent
Constipation And Maintain Regularity Example : Docusate SodiumDocusate Sodium Avoid In Pts Who Have Nausea, Vomiting, Or
Undetermined Abdominal Pain
Saline Laxatives
Non-absorbable Cations & Anions - Draw Water Into Intestine - Increase In Intra-luminal Pressure, Stimulates Intestinal Motility
Onset Of Action (Oral) 30min-3 Hrs,(Rectal) 2-5min
ONLY When Fast Clearance Of The Bowel Is Required Ex: Fleet Phospho-soda Avoid In Pts With CHF, Ileostomy, Renal Function
Impairment, Or Younger Than 6 Yrs Old
SALINE CATHARTICSSALINE CATHARTICS
Saline Cathartics Poorly Absorbed Ions Magnesium Sulfate Effects By Osmotic Action In Retaining Fluid In GI.
Magnesium Stimulates The Secretion Of Chole-cystokinin, A Hormone That Causes Stimulation Of Bowel Motility And Fluid Secretion.

M.O.MM.O.M
May Be Given Orally Or Rectally. Bowel Movement Within A Few Hours After
Oral Doses And In 1 Hour Or Less After Rectal
May Cause Fluid And Electrolyte Depletion. Magnesium Or Sodium Accumulation In
Patients With Renal Dysfunction
Hyper-Osmotic LaxativesHyper-Osmotic Laxatives
Combine An Osmotic & Local Effect Of Sodium Combine An Osmotic & Local Effect Of Sodium Stearate, Draws Water Into Rectum Stearate, Draws Water Into Rectum bowel bowel MovementMovement
Onset Of Action (Rectal) 30 MinOnset Of Action (Rectal) 30 Min Suppository FormSuppository Form Minimal Side EffectsMinimal Side Effects Example: Example: Glycerin Suppositories Glycerin Suppositories Avoid In Pts With Rectal IrritationAvoid In Pts With Rectal Irritation
GLYCERIN
Glycerin as a 1 & 3 g suppository and exerts Glycerin as a 1 & 3 g suppository and exerts its effect by osmotic action in the rectum. its effect by osmotic action in the rectum.
onset of action is less than 30 minutes.onset of action is less than 30 minutes. Glycerin is very safe infants, children. Glycerin is very safe infants, children. Its use is acceptable on for Its use is acceptable on for
constipation, in children.constipation, in children.
Lubricant LaxativesLubricant Laxatives
Prevent colonic absorption of fecal water, Prevent colonic absorption of fecal water, thus soften the stoolthus soften the stool
minimally absorbedminimally absorbed Onset of action (oral)6-8 hrs, (rectal) 5-15 minOnset of action (oral)6-8 hrs, (rectal) 5-15 min Avoid prolonged useAvoid prolonged use cause mal-absorption of fat-soluble vitaminscause mal-absorption of fat-soluble vitamins Example: Example: Mineral oil Mineral oil
LUBRICANTSLUBRICANTS
Mineral oil (Paraffin) only lubricant laxative
Mechanism from petroleum, coating stool and
allowing for easier passage inhibits colonic absorption of water,
increasing stool weight and decreasing stool transit time
Dose and ADR Mineral Oil
Orally Or Rectally In A Dose Of 15 To 45 MlOrally Or Rectally In A Dose Of 15 To 45 Ml Effect On Bowel After 2 Or 3 Days Of Use.Effect On Bowel After 2 Or 3 Days Of Use. In Debilitated Or Recumbent Patients, May In Debilitated Or Recumbent Patients, May
Aspirated, Lipoid-pneumoniaAspirated, Lipoid-pneumonia ADR: Decrease Absorption Of Fat-soluble ADR: Decrease Absorption Of Fat-soluble
Vitamins (Vitamins (A, D, E, And KA, D, E, And K) With Chronic Use ) With Chronic Use Even Orally, May Leak From The Anal Even Orally, May Leak From The Anal
Sphincter, Causing Soiling Of Clothing.Sphincter, Causing Soiling Of Clothing.

LACTULOSELACTULOSE
Lactulose - Disaccharide, used Orally Or Lactulose - Disaccharide, used Orally Or RectallyRectally
Metabolized By Colonic Bacteria To Low-Metabolized By Colonic Bacteria To Low-molecular-weight Acids, Result In molecular-weight Acids, Result In Osmotic Effect = Fluid Is Retained In The Osmotic Effect = Fluid Is Retained In The Colon.Colon.
The Fluid Retained In The Colon Lowers The Fluid Retained In The Colon Lowers The Ph And Increases Colonic PeristalsisThe Ph And Increases Colonic Peristalsis

LACTULOSELACTULOSE
Not First-line, Not More Effective Than Not First-line, Not More Effective Than Sorbitol Or Milk Of MagnesiaSorbitol Or Milk Of Magnesia
Alternative For Acute Constipation,Alternative For Acute Constipation, Useful In Elderly PatientsUseful In Elderly Patients Lactulose May Result Flatulence, Cramps, Lactulose May Result Flatulence, Cramps,
Diarrhea, And Electrolyte Abnormality.Diarrhea, And Electrolyte Abnormality.
Lactulose Dose Lactulose Dose Initial Dose 5 To 30 Ml Daily PO In A Initial Dose 5 To 30 Ml Daily PO In A
Single Dose Or In 2 Divided Doses; Single Dose Or In 2 Divided Doses; Doses Up To 45 Ml Daily Doses Up To 45 Ml Daily
Dose Is Adjusted To Patient's Needs Dose Is Adjusted To Patient's Needs Children Children
5 To 10 Years Initial Doses Of 10 Ml 5 To 10 Years Initial Doses Of 10 Ml Twice DailyTwice Daily
1 To 5 Years, 5 Ml Twice Daily 1 To 5 Years, 5 Ml Twice Daily Under 1 Year, 2.5 Ml Twice Daily. Under 1 Year, 2.5 Ml Twice Daily.
Sorbitol Sorbitol A Monosaccharide, Osmotic Action, A Monosaccharide, Osmotic Action, Primary Agent In Functional Primary Agent In Functional
Constipation Constipation As Effective As Lactulose, Less As Effective As Lactulose, Less
Expensive.Expensive. Sorbitol By Mouth Or Rectally As An Sorbitol By Mouth Or Rectally As An
Osmotic Laxative; Doses Of 20 To Osmotic Laxative; Doses Of 20 To 50 G. 50 G.
Stimulant LaxativesStimulant Laxatives 2 Classes: 2 Classes:
- Diphenylmethane (- Diphenylmethane (BisacodylBisacodyl))- Anthraquinone (- Anthraquinone (SennaSenna) )
Increases Propulsive Peristaltic Activity Increases Propulsive Peristaltic Activity By Local Irritation Of MucosaBy Local Irritation Of Mucosa
Onset Of Action:Onset Of Action:Senna (PO) 8-12 Hrs Senna (PO) 8-12 Hrs Bisacodyl: Oral/Rectal 15-60min, Bisacodyl: Oral/Rectal 15-60min,
Systemically AbsorbedSystemically Absorbed Major Use: For Evacuation Of Bowel Prior Major Use: For Evacuation Of Bowel Prior
To GI Surgery Or ExaminationTo GI Surgery Or Examination
BisacodylBisacodyl
Stimulating Mucosal Nerve Plexus Of Stimulating Mucosal Nerve Plexus Of ColonColon
Significant Inter-patient Variability Exists Significant Inter-patient Variability Exists With Dosing With Dosing
A Dose That Causes No Effect In One A Dose That Causes No Effect In One Patient May Result In Excessive Cramping Patient May Result In Excessive Cramping And Fluid Evacuation In Others.And Fluid Evacuation In Others.
Not Recommended For Regular Daily Use.Not Recommended For Regular Daily Use.
BisacodylBisacodyl
Acceptable Intermittently (Every Few Weeks) Acceptable Intermittently (Every Few Weeks) To Treat Constipation Or As A Bowel To Treat Constipation Or As A Bowel Preparation Preparation
Cause Abdominal Cramping Cause Abdominal Cramping Significant Fluid And Electrolyte Imbalances Significant Fluid And Electrolyte Imbalances
With Chronic Use.With Chronic Use. Should NotShould Not Use In Appendicitis Is A Use In Appendicitis Is A
Possibility (Perforation Of The Appendix May Possibility (Perforation Of The Appendix May Result) Or During Pregnancy Or LactationResult) Or During Pregnancy Or Lactation
ANTHRAQUINONEANTHRAQUINONE
Cascara, Sennosides, And Casanthrol. Gut Bacteria Metabolizes These Agents To
Their Active Compounds, Exact Mechanisms Of Action Not
Understood. Effects Are Limited To The Colon, Use Of These Agents Are Similar To Those
For The Diphenylmethane Derivatives. Intermittent Use Is Acceptable; Daily Use
Discouraged
Stimulant LaxativesStimulant Laxatives Sennakot, Sennakot S (With Sodium Docusate), Sennakot, Sennakot S (With Sodium Docusate),
Exlax, Dulcolax, Exlax, Dulcolax, Fijan Syrup (5.85 Mg Sennoside/5 Ml)Fijan Syrup (5.85 Mg Sennoside/5 Ml) Interact With H1 Blockers, Antacids If Interact With H1 Blockers, Antacids If
Administered Within 1 HrAdministered Within 1 Hr Avoid In PregnancyAvoid In Pregnancy Breast Feeding: Senna Laxative Reported Brown Breast Feeding: Senna Laxative Reported Brown
Discoloration Of Breast MilkDiscoloration Of Breast Milk Adverse Effects: Adverse Effects:
Severe Cramping, Electrolyte & Fluid Severe Cramping, Electrolyte & Fluid Deficiencies, Metabolic Acidosis/AlkalosisDeficiencies, Metabolic Acidosis/Alkalosis
CASTOR OILCASTOR OIL Castor Oil Metabolized In GI To Active Castor Oil Metabolized In GI To Active
Compound, Ricinoleic Acid, Compound, Ricinoleic Acid, Stimulates Secretory Processes, Decreases Stimulates Secretory Processes, Decreases
Glucose Absorption, And Promotes Intestinal Glucose Absorption, And Promotes Intestinal Motility, In Small Intestine. Motility, In Small Intestine.
Castor Oil Results In A Bowel Movement 1 To Castor Oil Results In A Bowel Movement 1 To 3 Hours. 3 Hours.
Because Strong Purgative Action, Should Because Strong Purgative Action, Should Not Used For Routine Treatment Of Not Used For Routine Treatment Of Constipation.Constipation.

Polyethylene GlycolPolyethylene Glycol
PEG Become Popular For Colon PEG Become Popular For Colon Cleansing Before Diagnostic Procedures Cleansing Before Diagnostic Procedures Or Colorectal Operations.Or Colorectal Operations.
Four Liters Of This Solution Is Four Liters Of This Solution Is Administered Over 3 HoursAdministered Over 3 Hours
Not Recommended For Routine Treatment Not Recommended For Routine Treatment Of Constipation And Should Be Avoided Of Constipation And Should Be Avoided In Patients With Intestinal Obstruction.In Patients With Intestinal Obstruction.
Acute Constipation infrequent use (less than every few
weeks) of laxative is acceptable. Relieved by use of a tap-water enema or a
glycerin suppository; if ineffective, use of oral sorbitol, low
doses of diphenylmethane or anthraquinone laxatives, or saline laxative (e.g., milk of magnesia)
If laxative is required for longer than 1 week, consult a physician

Bedridden or Geriatric patients For some bedridden or geriatric patients, or with
chronic constipation, bulk-forming laxatives first line of treatment,
Use of laxatives may be required frequently. Lowest effective dose and infrequently as
possible to maintain regular bowel function (more than three stools per week).
Milk of magnesia, and sorbitol or lactulose. Mineral oil should be avoided

Patient Counseling
Laxative use to treat constipation should be only on a temporary measure
If laxatives are not effective after 1 week, a physician should be consulted

Management 1-Management of chronic constipation
due to slow transit including:
patient education
behavior modification
dietary changes
drug therapy

2-Management of defecation involves:
biofeedback
sensory training
relaxation exercises
suppository programs
Patient education: reassurance explanation of normal bowel habits reduce use of laxatives and cathartics increase fluid and fiber intake use normal postprandial increases in colonic motility
by instructing patients to defecate after meals important in the morning when colonic motor activity
is highest

What Can You Do?
Become more physically active A 30 minute walk
every day may help keep you more regular
What Can You Do? Eat more fiber
More beans, whole grains and bran cereals, fresh fruits, vegetables
Limit foods with no fiber (cheese, meat, sweets, processed foods)

What Can You Do? Fiber supplements are best choice
Absorb water and make stool softer Safe to use everyday Be sure to drink at least 8 to 10
glasses of water everyday Add to diet slowly to prevent
problems with gas
What Can You Do?
Drink more water and other liquids (8 eight-ounce glasses a day) Liquid helps keep the
stool soft Avoid caffeine or
alcohol which can dehydrate you
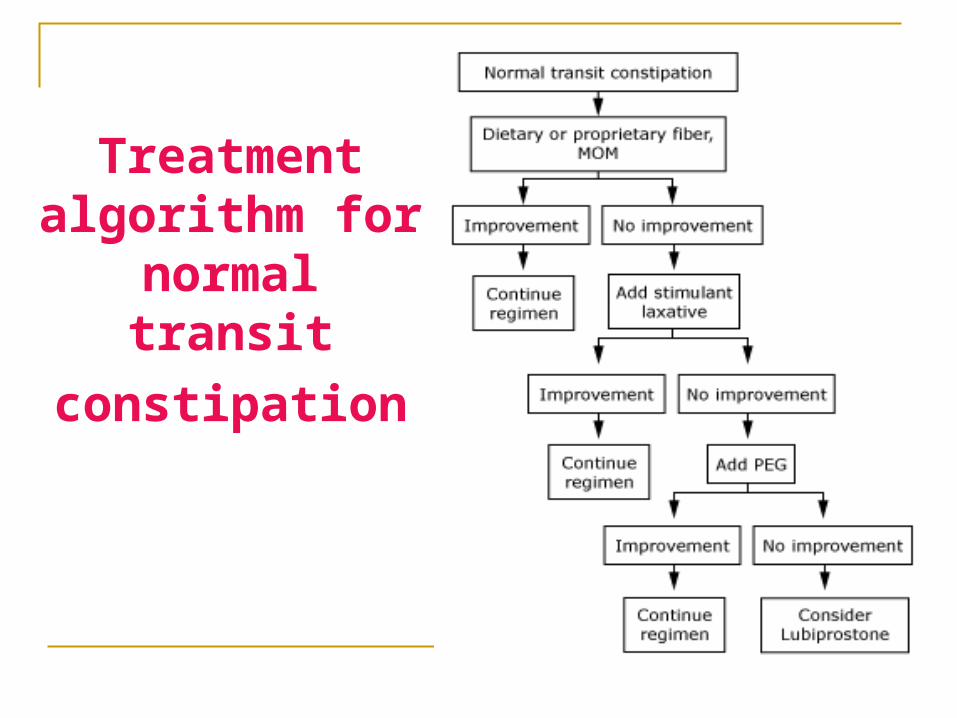
Treatment algorithm for
normal transit
constipation
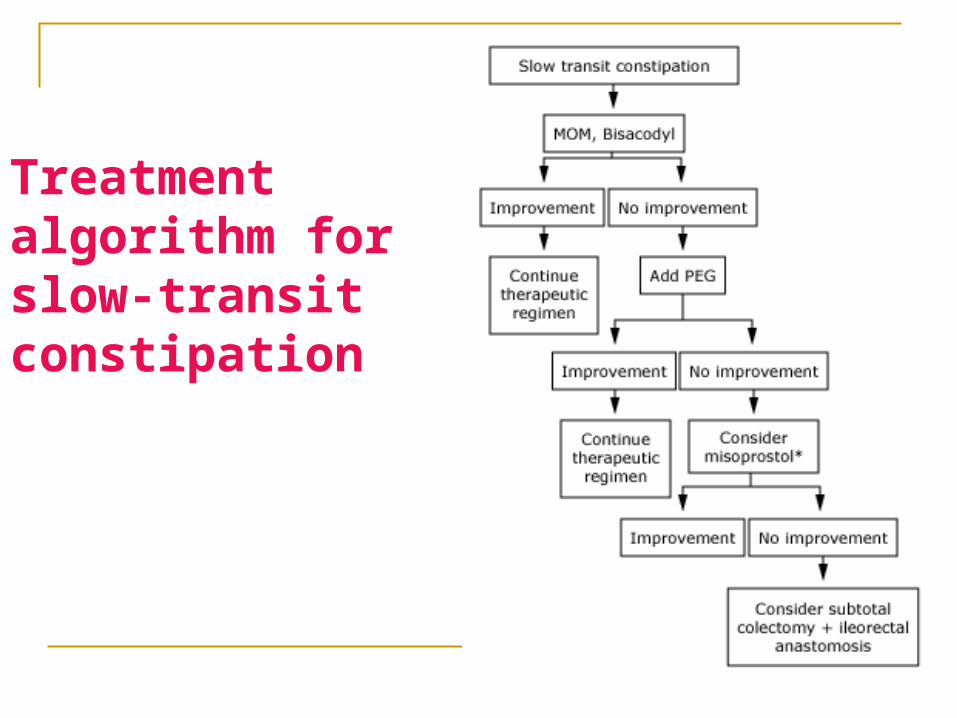
Treatment algorithm for slow-transit constipation

Thank you for your attention

Constipation in Infants & children Constipation common. Constipation common. neurologic, metabolic, or neurologic, metabolic, or
anatomic abnormalities. anatomic abnormalities. Management:Management: Dietary modification with high-Dietary modification with high-
fiber foodsfiber foods
Drugs for Constipation: Drugs for Constipation: Fluid & High fibers Fluid & High fibers Laxatives -osmotic: Laxatives -osmotic:
Polyethylene glycol (70 g powder)Polyethylene glycol (70 g powder) Lactulose (10g/15 ml syrup) Lactulose (10g/15 ml syrup) Sorbitol (5g powder)Sorbitol (5g powder) GlycerinGlycerin
Laxatives - stimulant: Laxatives - stimulant:
Bisacodyl (Dulcolax, Correctol) 5 mg tab;5,10 mg supp. Bisacodyl (Dulcolax, Correctol) 5 mg tab;5,10 mg supp. Castor oilCastor oilSennaSennaFigan syrup (5.85 mg sennoside B/5 ml) Figan syrup (5.85 mg sennoside B/5 ml)
Magnesium Hydroxide (Milk of magnesium Magnesium Hydroxide (Milk of magnesium MOM)MOM)240cc 8% Susp240cc 8% Susp
Thank you for your attention
Rastegarpanah