congenital unilateral infiltrating facial lipomatosiscongenital unilateral infiltrating facial...
TRANSCRIPT
West Indian Med J 2017; 66 (1): 189
189
DOI: 10.7727/wimj.2014.250
Congenital Unilateral Infiltrating Facial Lipomatosis
The Editor,
Sir,
Slavin et al in 1983 described Congenital diffuse infiltratinglipomatosis of the face (CDIL-F), which is an unfamiliar clin-ical entity characterized by collections of nonencapsulated,mature adipocytes that infiltrate locally, leading to craniofa-cial deformities with a tendency for recurrence after surgery(1). Affected children do not have abnormal psychomotor de-velopment but the facial asymmetry causes cosmetic concerns.We present the radiological findings in our case.
A one-year-old female presented with progressively in-creasing swelling over the right face since birth with the earlyeruption of deciduous teeth. The swelling on the right side ofthe face was soft, non-tender, ill-defined and diffuse causingunilateral facial hypertrophy (Fig. 1).
Congenital diffuse infiltrating lipomatosis of the face ischaracterized by nonencapsulated proliferation of mature adi-pose tissue causing diffuse infiltration of muscle and adjacentsoft-tissue. There are presence of fibrous tissue, nerve bun-dles and vessels with a thickened wall without lipoblasts andsigns of malignancy. Skeletal findings in CDIL-F are sclero-sis and the hyperplasia of the skull, cervical vertebrae, hemi-mandibular hyperplasia (of the ramus and/or condyle),accelerated dentoskeletal growth and zygomatic hyperplasia(2).
Differential diagnoses of CDIL-F are lymphatic or vas-cular malformations, lipomas (intermuscular/intramuscular,angiolipomas/fibrolipomas, liposarcoma and lipoblastomato-sis) and congenital overgrowth syndromes causing progressivehemifacial hyperplasia.
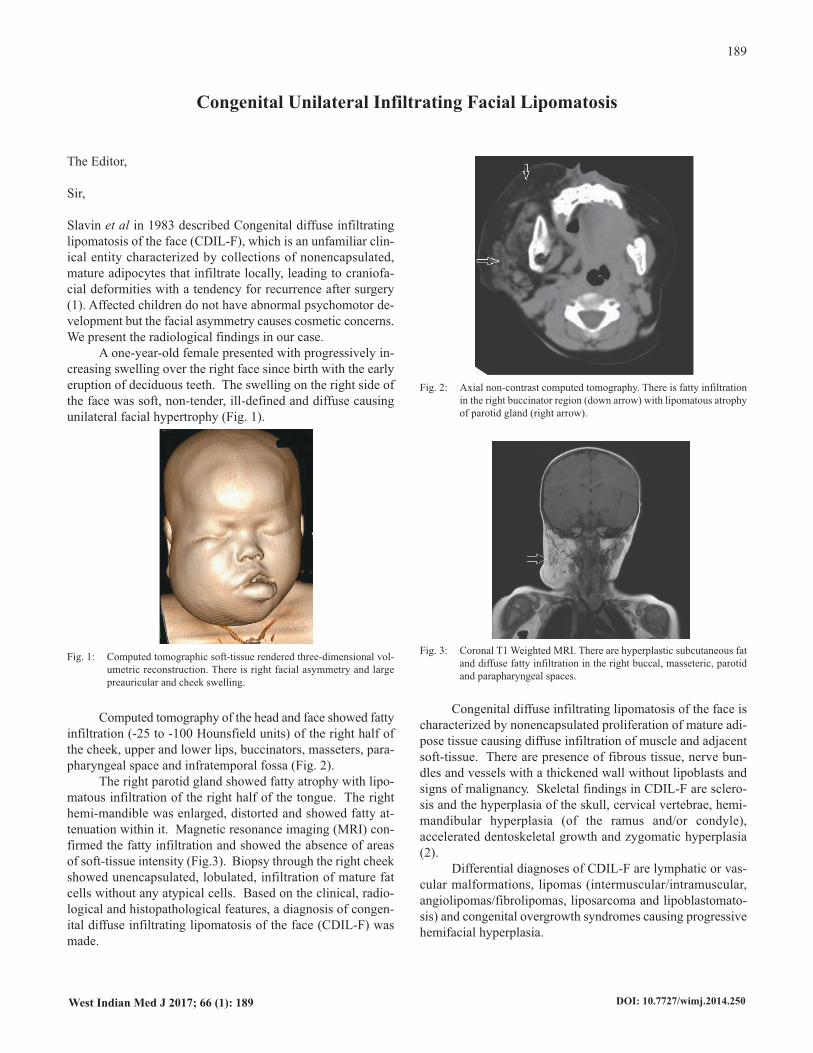
Computed tomography of the head and face showed fattyinfiltration (-25 to -100 Hounsfield units) of the right half ofthe cheek, upper and lower lips, buccinators, masseters, para-pharyngeal space and infratemporal fossa (Fig. 2).
The right parotid gland showed fatty atrophy with lipo-matous infiltration of the right half of the tongue. The righthemi-mandible was enlarged, distorted and showed fatty at-tenuation within it. Magnetic resonance imaging (MRI) con-firmed the fatty infiltration and showed the absence of areasof soft-tissue intensity (Fig.3). Biopsy through the right cheekshowed unencapsulated, lobulated, infiltration of mature fatcells without any atypical cells. Based on the clinical, radio-logical and histopathological features, a diagnosis of congen-ital diffuse infiltrating lipomatosis of the face (CDIL-F) wasmade.
Fig. 1: Computed tomographic soft-tissue rendered three-dimensional vol-umetric reconstruction. There is right facial asymmetry and largepreauricular and cheek swelling.
Fig. 2: Axial non-contrast computed tomography. There is fatty infiltrationin the right buccinator region (down arrow) with lipomatous atrophyof parotid gland (right arrow).
Fig. 3: Coronal T1 Weighted MRI. There are hyperplastic subcutaneous fatand diffuse fatty infiltration in the right buccal, masseteric, parotidand parapharyngeal spaces.

190
The role of sonography, computed tomography (CT) andmagnetic resonance imaging (MRI) is very contributory inmaking the diagnosis. Ultrasound helps in identifying the dif-fuse, fatty, infiltrative and non-vascular nature of the lesion butits true anatomical extent can be depicted by cross-sectionalimaging only. Computed tomography scan shows a diffuse,non-uniform fatty infiltration with Hounsfield Unit being inthe negative range of fat along with a unilateral hyperplasia ofcraniofacial bones as seen in the present case. The predomi-nantly fatty nature of the condition is confirmed on MRI. Inchildren, the lesion exhibiting high signal intensity (isointenseto fat) on T1 and T2-weighted images and hypointensity onfat-suppressed sequences along with strong clinical correlationeliminate the need for biopsy.
This entity is managed primarily by wide local excision(3).
Keywords: Congenital, face, lipomatosis
SV KashikarFrom: Department of Radiology, Jawaharlal Nehru Medical College, Sawangi Meghe, Wardha, India.
Correspondence: Dr SV Kashikar, Behind Magnanwadi, Ramnagar, Wardha, Maharashtra 442001, India. Email: [email protected]
REFERENCES1. Slavin SA, Baker DC, McCarthy JG, Muffarij A. Congenital infiltrating
lipomatosis of the face: clinicopathologic evaluation and treatment. Plast Reconstr Surg1983; 72: 158–64.
2. Bouletreau P, Breton P, Freidel M. Congenital infiltrating lipomatosis ofthe face: case report. J Oral Maxillofac Surg 2000; 58: 807–10.
3. Padwa BL, Mulliken JB. Facial infiltrating lipomatosis. Plast Reconstr Surg 2001; 108: 1544–4.
Letters