congenital “giant” naevus: a preliminary report of a new surgical approach
TRANSCRIPT
British .Ioumol of Plastic Surgery (1987), 40,410-419 @ 1987 The Trusteesof British Association of Plastic Surgeons
Congenital “giant” naevus: a preliminary report of a new surgical approach
A. L. H. MOSS
Summary-A new approach to the treatment of congenital “giant” naevi is described, using a curette in the first few weeks of life. This attempts to minimise the disadvantages of established methods of treatment. The technique is relatively atraumatic as there appears to be a natural cleavage plane within the dermis removing the pigmentation. Ten patients have been treated with this procedure with a follow-up of 3 months to 5 years; 3 patients have produced poor and unsatisfactory curettings, which has resulted in return of pigmentation. One case developed hype~rophic scarring following a wound infection and delayed healing. The other 6 cases have encouraging appearances although the hairs in some lesions remain. It is too early to say if malignant potential has been removed but perhaps it has been reduced by decreasing the total number of melanocytes and naevus cells.
The management of congenital naevi remains controversial as there is no universal agreement as to their malignant potential (Kopf et al., 1979; Rhodes and Melski, 1982; Arons and Hurwitz, 1983). The cosmetic deformity of these large naevi alone is an indication for considering treatment (Trozak et al., 1975; Arons and Hurwitz, 1983) but the established methods do not guarantee an acceptable appearance. A new surgical technique is described which attempts to minimise the disadvantages of established methods of treating the “giant” naevus. It is based on the observation that there appears to be in these naevi, in the newborn, a natural cleavage plane between the upper dermis, containing the majority of naevus cells and melanocytes, and the deeper dermis (Johnson, 1977).
Operative technique
It is essential that the technique is used before 6 months of age but preferably as early as is feasible. It becomes progressively more difficult to perform as the two dermal elements become more adherent with increasing age.
Under general anaesthesia, the area to be treated should be held firmly. With a sharp curette, the naevus is scraped from its centre in the direction of the lines of maximum relaxation (Fig. 1A and B).
Based on a paper presented to the British Association of Plastic* Surgeons Summer Meeting in Liverpool, July 1986.
The stripping should be relatively atraumatic and avascular although it becomes more difficult right at the periphery of the lesion (Fig. IC, D). This junctional rim usually requires shaving with a scalpel or dermabrasion. Up to 25% body surface area has been treated without requiring blood transfusion as there is minimal bleeding. The raw areas are dressed routinely, as for a split skin graft donor site, and left undisturbed for 7 to 10 days.
MateriaIs and methods
Ten babies have been treated with the described technique, the first in July 1981 and the last in May 1986. There was an equal sex distribution. The age at the start of treatment ranged from 2 weeks to 4 months; 6 months was the oldest age at curettage as it became progressively more difficult to find the natural cleavage plane; 7 babies underwent only one session of curettage (the others required 2, 4 and 5 procedures, respectively, all in the early part of the series). Six patients had naevi that could be described as the “garment” variety, while the remainder had smaller lesions (3.65 cm2 average size).
R@SUltS
In seven babies, there were satisfactory curettings (Fig. 1B) which resulted in no return of pigment with acceptable appearance in 6 patients (Figs 2,3,
410

CONGENITAL ‘GIANT’ NAEVUS: A PRELIMINARY REPORT OF A NEW SURGICAL APPROACH 411
Fig. 1
Figure l--(A) The sharp curette separating a~a~mat~~a~~y the upper dermis with the naevus cells from the non-~l~~di~~ deeper dermis. (B) The typical curettings that may be elevated from an avascufar plane. {C) The fesion after curettage. Nate in the top right of the photograph t&e traumatic attempts to curette the junctional and normal skin. (D) Typicat minimal blood loss from the operative case.
4). One case developed a beta ~~ernol~i~ strepto- coccal infection in the treated area resulting in a full thickness loss, with subsequent split skin grafting. This baby of North African extract developed hypertrophic scarring, the only case to do so in the series (Figs 5A and B).
In three cases, the curettings were poor and u~satisfa~to~ [Figs GA, 3 and 6). These patients developed sufficient repi~e~tation to require excision and grafting. 1t is interesting to note that
these three patients had the smaller variety of congenital naevus and may reflect a different type. The histology of these and other patients with congenital naevi will require further study, as it may be possible to predict which lesions may be amenable to this treatment.
At present, two patients have abnormal hair growth but this is not a problem. The last baby to be treated has an unclassi~able tumo~r in associa- tion with the “bathing trunk” naevus.

412 BRITISH JOURNAL OF PLASTIC SURGERY
Fig. 2
Figure 2-(A) Case 1. “Bathing trunk” naevus at 2 weeks of age, just prior to curettage, in one session and not requiring blood transfusion. (B) One-year follow-up.
Discussion
There is disagreement about the definition and incidence of “giant” congenital naevi (Arons and Hurwitz, 1983), and the incidence of malignant transformation still remains uncertain. Figures range from 1.8 to 42% (Pers, 1963; Greeley et al., 1965; Dellon et al., 1976; Kopf et al., 1979; Rhodes and Melski; 1982; Arons and Hurwitz, 1983). The lower figure is more realistic and is supported by our own experience (Moss and Briggs, 1986). However, it has also been strongly advocated that not only these “giant” lesions should be removed because of their malignant potential, but in fact all congenital naevi should be excised for the same reason (Solomon, 1980; Rhodes et al., 1982). When premalignancy is the indication for excision of the “giant” variety of congenital naevus, it should be performed early as the neoplastic changes appear
to occur before the age of 6 years (Trozak et al., 1975; Rhodes and Melski, 1982; Arons and Hur- witz, 1983).
The appearance and resulting psychological consequences are important indications alone for surgical treatment (Trozak et al., 1975; Arons and Hurwitz, 1983). Pers (1963) showed that 53.9% of patients with congenital “giant” naevi had signifi- cant psychological or emotional disturbances as a result of their lesion.
The surgical methods available for treating these congenital “giant” naevi have recently been re- viewed (Arons and Hurwitz, 1983), but the tech- niques have many disadvantages. Dermabrasion is inaccurate in that, if performed too superficially, it can result in the return of the naevus while if too deeply, hypertrophic scarring or changes in pigmen- tation may occur. (These changes are seen in the naevus of the left buttock that was dermabraded in
CONGENITAL ‘GIANT’ NAEVUS: A PRELIMINARY REPORT OF A NEW SURGICAL APPROACH 413
Fig. 3
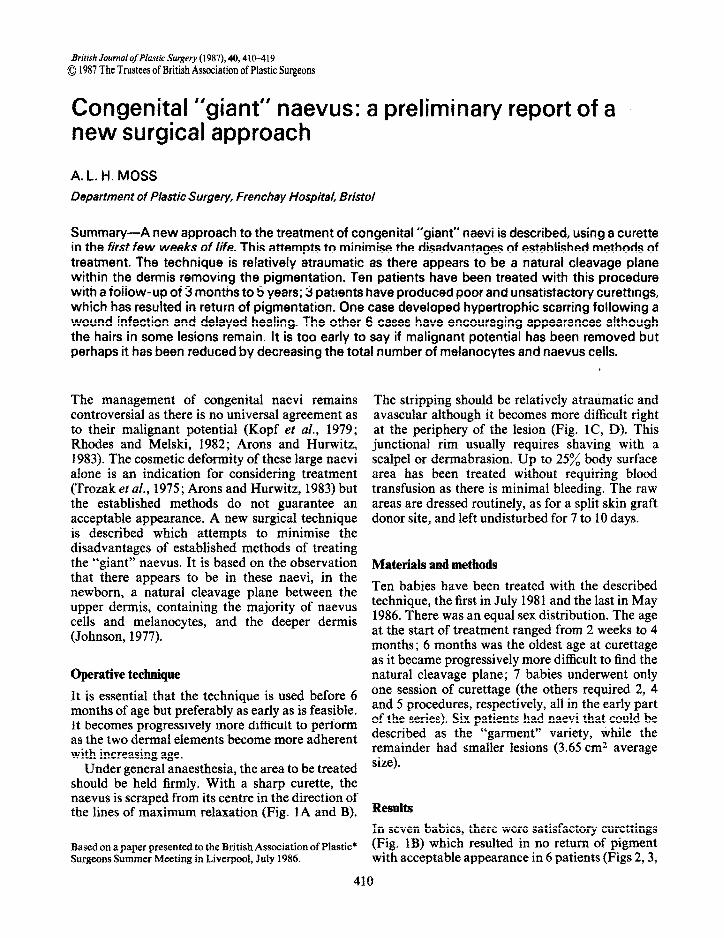
Figure 3-(A) Case 2. “Cloak” naevus at 3 months of age, anterior view. This baby, the second in the series, required 5 sessions to curette (between 3-6 months of age), with blood being given on the first two occasions only. The periphery of the naevus required dermabrasion. (B) Posterior view at 3 months of age. (C) Anterior view at 4 years of age. Note the slight return of pigment at the edge of the original naevus. (D) Posterior view at 4 years of age. This shows the hair growth in the curetted naevus. There is return of pigment and hair as well as hypertrophic scarring in the naevus of the left buttock which was dermabraded. The other naevi may make donor sites for split skin grafting limited.
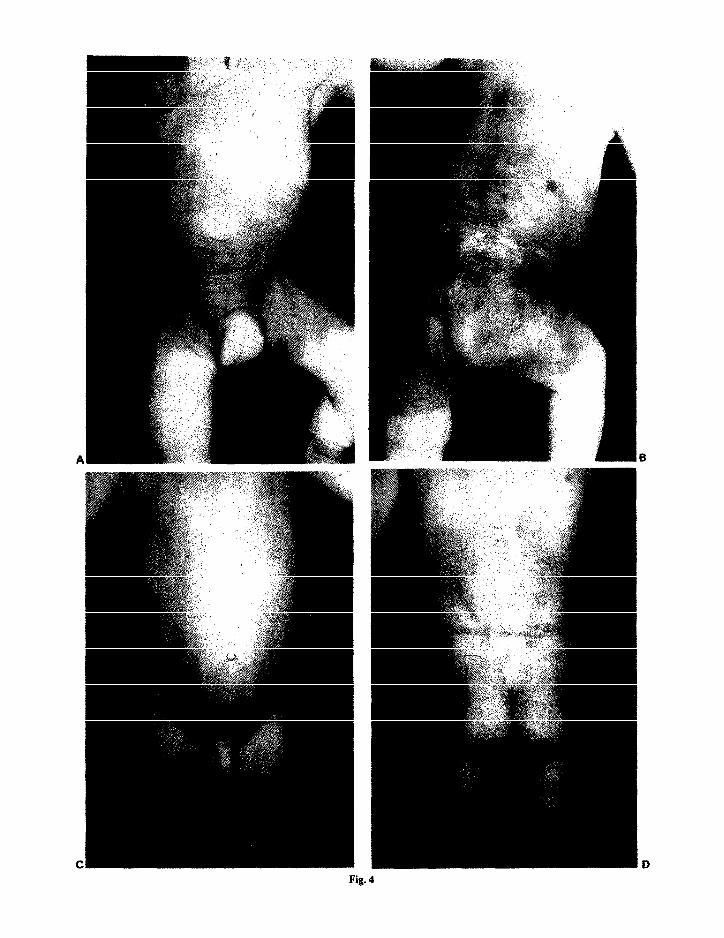
Fig. 4
CONGENITAL ‘GIANT’ NAEVUS: A PRELIMINARY REPORT OF A NEW SURGICAL APPROACH 415
Fig. 5
Figure 5-(A) Case 4. Congenital naevus involving the circumfer- ence of the thigh in this 5-week baby of North African origin. This lesion was curetted in one session. He developed a beta haemolytic streptococcal infection resulting in a full thickness loss. This required split skin grafting. (B) The appearance at 22 months after grafting showing the area of hypertrophic scarring as a result of delayed healing.
Fig. 4
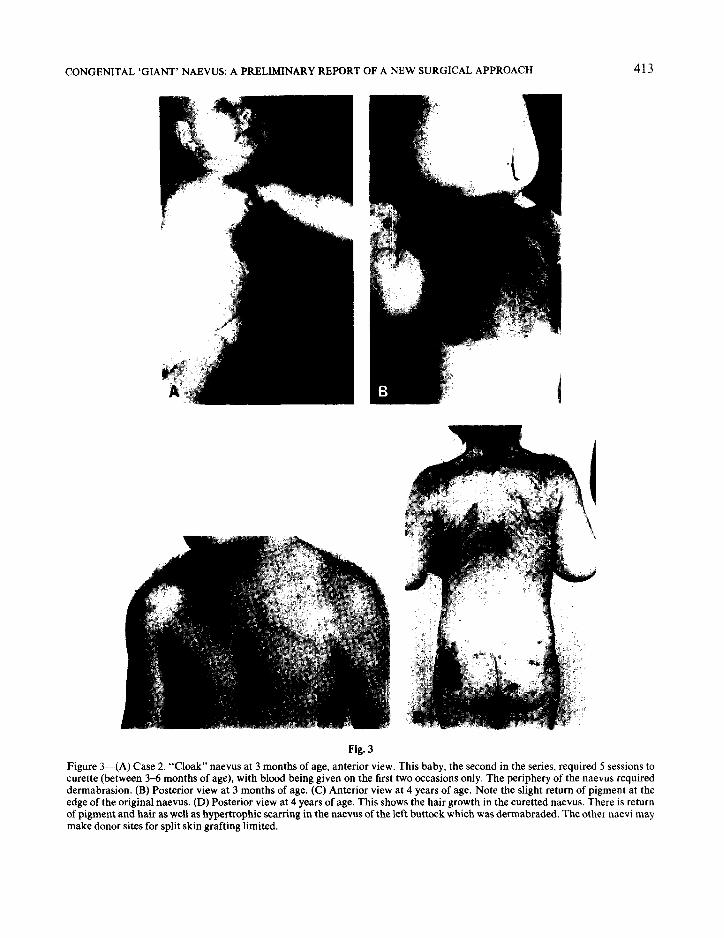
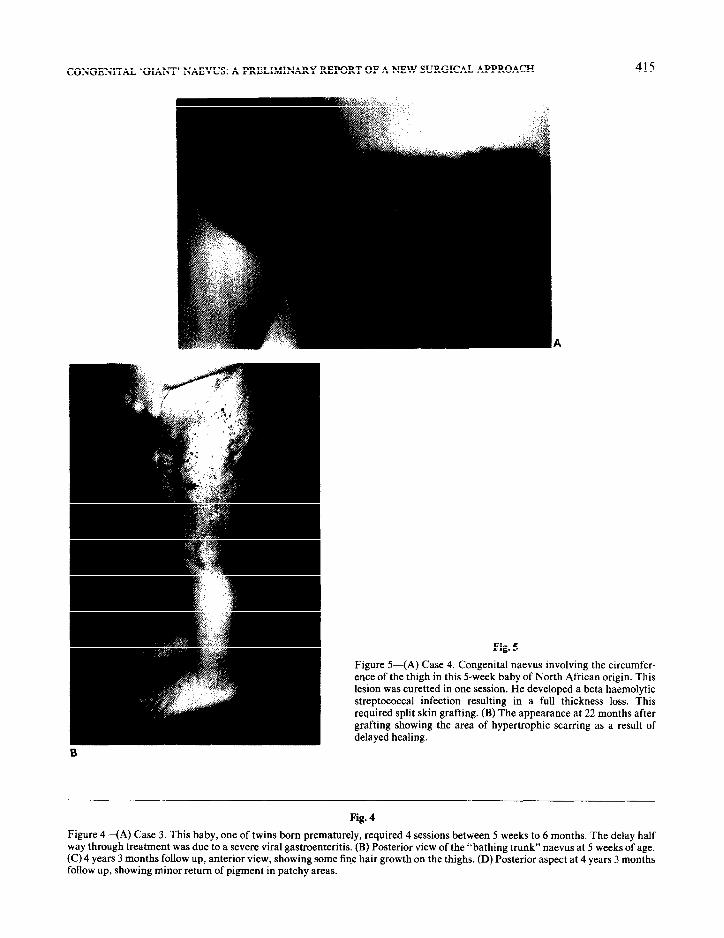
Figure 4-(A) Case 3. This baby, one of twins born prematurely, required 4 sessions between 5 weeks to 6 months. The delay half way through treatment was due to a severe viral gastroenteritis. (B) Posterior view of the “bathing trunk” naevus at 5 weeks of age. (C) 4 years 3 months follow up, anterior view, showing some fine hair growth on the thighs. (D) Posterior aspect at 4 years 3 months follow up, showing minor return of pigment in patchy areas.

416 BRITISH JOURNAL OF PLASTIC SURGERY
Figure 6--(A) Case 5. A congenital naevus in a baby curetted at 3 months of age. (E) The return of pigmen~tion at 17”months review.
The poor and unsatisfactory curettings. (0
Case 2, Fig. 3D.) Excision, even tangential shaving, however careful, can be a major surgical insult requiring blood transfusions and several general anaesthetics. Some authors advocate that, as naevus cells can be found in the subcutaneous tissues including the deep fascia, these should be removed in toto (Deffon et al,, 1976; Rhodes et ai., 1981; Arons and Nurwitz, 1983) but this can result in a mutilating contour deformity. The application of split skin grafting can leave an ~ac~eptable appearance, particularly in junctional areas or if delayed healing has occurred. Repigmentation in
both split and full thickness skin grafts can occur. Donor sites may also be a limiting factor, as they may be covered with pigmented lesions (Greeley et aI., 1965).
Serial excision of the naevus or the grafted area may not be appropriate in some instances due to its size or anatomical site. Similarly, the use of tissue expansion has a limited place in the treatment of these “giant” naevi. Also, it must be noted that the excision of the congenital “giant” naevus has not prevented the occurrence of neoplasia (Shaw, 1962; Rhodes et al., 1981).

CONGENITAL ‘GIANT’ NAJZVUS: A PREL~M~N~Y RBPORT OF A NBW SURGICAL APPROACH
Fig. 7
Figure 7--<A) ~js~~~i~ section of skin #~ta~n~n~ a congenital naevus. Note the heavily ~~~rn~nted naevus cells in the upper dermis. The fewer dermis contains scattered naevus cells between cohagen 6bres. (H&E, x 13.5). (fr) H~sto~ogi~~ section of the curetted material showing it to consist of epidermis, with underlying papillary and upper reticular dermis. The tatter contains numerous naevus cells, some of which are heavily pigmented. Note the sharp edge along the deep aspect of the specimen. @i&E, x 68). (C) Histological section of skin to show the junction of a congenital naevus that has not been treated {Left) with that of an area &at has been curetted (Right). Note that the treated area has no pigmented naevns ceils in the upper dermis but there is a slight increase in fibrosis in this layer (H&E, x 68).
Mark 9f 62. (1973) have maintained that there are ~isto~ogi~a~ di~~~n~es between congenitd and acquired aaevi. They showed &at naevus c&s are found, more commonly in the congenital variety, deep into the dermis and adnexal structures, and may even be seen in fat and muscle. In the reticular dermis and subcutis, naevus cells in congenital naevi are usually disposed as single ceils between the colfagen bundles and fat cells, not as groups in the manner of ordinary intrade~~ naevus cells, The deep naevns cells often show neuroid appear- ance. Naevus cells in ~~~~enital naevi may also be found in the hair f&ides, in erector pifi muscles,
within the nerve sheath and in the intim~ of blood vessels (~~~o~e~, t983). Walton et al. (f975), on the other hand, have shown that, in the? ffe~~~~, the naevus cells are mainly limited to the upper dermis (Fig. 7A). The probable reason for the difference in the histological findings is the age of the patient when the biopsies were performed. In the paper by Mark et ai. (1973), only 37% of the patient presented between birth and 9 years of age. One may theF&xe speeufate that the naeviig cells migrate deeper into the dermis as the ksion matures, as observed in acquired fesions, where the progression is from junctional ta compound to
418 BRITISH JOURNAL OF PLASTIC SURGERY
dermal naevus. Therefore, if one could remove the upper dermis with the majority of the pigmented naevus cells and melanocytes, the likelihood of developing cutaneous malignant melanoma should be radically reduced. Other neural malignancies may still develop as these naevi are derivated from neural ectodermal tissue. Neuroblastoma, neuri- lemmoma, undifferentiated neural tumours and malignant blue naevus have been recorded in association with congenital “giant” naevi (Solomon et al., 1980).
Johnson (1977) was the first to observe the phenomenon of a natural cleavage plane between the upper dermis with most of the pigmented naevus cells and the lower dermis. He reported the case of a baby with a congenital naevus of the scalp being delivered with forceps. Part of the naevus was accidentally removed with the instrument and the resulting raw area was allowed to heal sponta- neously. There was no return of pigment in this region. On this evidence, he treated the rest of the naevus with de~abrasion. With a 17-year follow- up, there was no return of pigment except in the superficially abraded eyebrow. In the two cases reported by Miller and Becker (1979), both derma- brasion and tangential shaving were used, starting at four weeks of age, with a follow-up of 12 and 19 months respectively. The only return of pigment was noted in areas that were treated late when biopsies showed a progressive descent of the naevus cells into the deeper dermis.
The t~hnique described above has the advantage of being more accurate and less traumatic than dermabrasion or tangential shaving. This results in minimal blood loss, allowing larger areas to be treated in one session, Therefore fewer anaesthetics without the need for blood transfusions make the treatment of these lesions a logistical possibility.
This atraumatic separation between the two parts of the dermis demonstrated by the above technique (Fig. 7B and C) appears to be limited by the age of the patient (and naevus) since it becomes progressively more difficult to perform as the baby approaches 6 months of age. It is noted that the normal skin as well as the junctional area cannot be curetted in this atraumatic fashion (Fig. 1C). It is still unexplained why this cleavage plane should exist in the immature naevus and will be further studied. Similarly, the histology of all these patients is being reviewed to see if there is an obvious difference between those naevi which are easily curettable and those with poor curettings resulting in return of pigmen~tion. As the numbers of
patients with these lesions are small, more infor- mation should be obtained from biopsy material, even if surgery is not performed.
The appearance in the majority of patients treated is encouraging although the review period in some is short. The residual hair remains but is a minor problem. The follow-up is still too short to see whether neoplastic changes will occur but as most of the naevus cells are removed from the junctional area, the potential for developing a cutan~us malignant melanoma should be reduced theoretica~y to the same risk as in the general population.
Conclusions
Curettage of congenital “giant” naevi in the first few weeks of life is recommended as an atraumatic technique for removing the upper dermis with most of the pigmented naevus cells. There is less intra- and postoperative morbidity than with accepted surgical methods and there is ~tentially a more pleasing cosmetic appearance. Early removal of the naevus has the theoretical advantage of reducing the chance of cutaneous malignant melanoma to that of the general population.
Acknowledgements
I would like to thank Dr Frank Van Genechten who initiated the technique, the Medical Photographic Department, Frenchay Hospital, for the photographs, Dr Nassif fbrahim, Consultant His~pathoiogjst, Frenchay Hospital, for reviewing the manu- script, histology and photomicrographs and the Consultant Plastic Surgeons, Frenchay Hospital, for allowing me to include their patients in the series.
References
Amus, M. S. and Hnrwitz, S. (1983). Congential nevocellular nevus: A review of the treatment controversy and a report of 46 cases. Piustic ami Reconstructive Surgery, 72,355.
De&n, A. L., Ed&m, R. L. and Chmtien, P. B. (1976). Defining the m~ignant potential of the giant pigmented nevus. P&x& and Reco~t~t~ Surgery, 57,611.
Greeley, P. W., Middleton, A. G. and Co&n, J. W. (1965). Incidence of malignancy in pigmented nevi. Plastic and Reconstrucfive Surgery, 36,26.
Johnson, H. A. (1977). Permanent removal of pigmentation from giant hairy naevi by dermabrasion in early life. British Journal of Pbstic Surgery, 30,321.
Kopf, A. W., Bart, R. S. and Hennesse y, P. (1979). Congenital nevocytic nevi and malignant melanomas. Journui of rhe American Academy of Dermatdogy, 1,123.
McGovern, V. J. (1983). Melanoma: Histological diagnosis and prognosis. (Biopsy Interpretation Series). New York: Raven Press.

CONGENITAL ‘GIANT’ NAEVUS: A PRELIMINARY REPORT OF A NEW SURGICAL APPROACH 419
Mark, G. J., Milnn, M. C., Liteplo, M. G., Reed, R. J. and Clark, W. H. (1973). Congenital melanocytic nevi of the small and garment type. Human Pathology, 4,395.
Miier, C. J. and Becker, D. W. (1979). Removing pigmentation by dermabrading naevi in infancy. British Journal of Plastic Surgery, 32, 124.
Moss, A. L. H. and Briggs, J. C. (1986). Cutaneous malignant melanoma in the young. British Journal of Plastic Surgery, 39, 537.
Pers, M. (1963). Naevus pigmentosus giganticus: Indikationer for operative behandling. Ugeskriftfor Lager, 125,613.
Rhodes, A. R. and Mel&i, J. W. (1982). Small congenital nevocellular nevi and the risk of cutaneous melanoma. Journal of Paediatrics, 100,219.
Rhodes, A. R., Wood, W. C., Bolter, A. J. and Milnn, M. C. (198 1). Nonepidermal origin of malignant melanoma associ- ated with a giant congenital nevocellular nevus. Plastic and Reconstructive Surgery, 67,782.
Rhodes, A. R., Sober, A. J., Day, C. L., Melski, J. W., Harris& T. J., Mikrn, M. C. and Fitzpatrick, T. B. (1982). The malignant potential of small congenital nevocellular nevi. Journal of the American Academy of Dermatology, 6,230.
Shaw, M. H. (1962) Malignant melanoma arising from a giant hairy naevus. British Journalof Plastic Surgery, 15,426.
Solomon, L. M. (1980). The management of congenital melano- cytic nevi. Archivesof Dermatology, 116, 1017.
Solomon, L., Eng, A. M., Bene, M. and Loeffel, E. D. (1980). Giant congenital neuroid melanocytic nevus. Archives af Dermatology, 116,318.
Trozak, D. J., Rowland, W. D. and Hu, F. (1975). Metastatic malignant melanoma in prepubertal children. Paediatrics, 55, 191.
Walton, R. G., Jacobs, A. H. and Cox, A. J. (1976). Pigmented lesions in newborn infants. British Journal of Dermatology, 95, 389.
The Author
A. L. H. Moss, FRAYS, Senior Registrar, Department of Plastic and Reconstructive Surgery, Frenchay Hospital, Bristol BS16 1LE.
Requests for reprints to the author.