congenital diaphragmatic hernia evidence based … · • full term baby born by nsvd • born to a...
TRANSCRIPT

Congenital Diaphragmatic HerniaEvidence Based Management
Saima Aftab MDPSA Chief Neonatology
Director Fetal Care Center NCHDirector National Victor Center
Affiliate Faculty Brigham and Women’s Hospital
& Harvard School of Medicine.

Case 1
• Called to a STAT c section for FHR decelerations. • The mother is a 21 yr old G2P1, she has had poor prenatal care (two visits
at a health center) has a h/o substance abuse. • Her blood type is A pos, her stat HIV and Hep B are neg, her other
prenatal labs are pending GBS is unknown. • The baby is 38 weeks per LMP (roughly) and fundal height/US is consistent
with a term baby.• Baby delivers is limp, apneic and has a HR of 60.

Case 1
• Warm dry stim, suction. No response so PPV started followed by MRSOPA HR not detectable…. (yikes!!!)
• Baby intubated with a 3.5, CPR (coordinated with ventilation) started….• Low HR Epi given via low UVC followed by cycles of (PPV/CPR)• NO HR detected after 15 min of resuscitation• H’s and T’s??? • Two boluses given for hypovolemia• (Does the baby have a Tension Pneumothorax? Or Tamponade)• Should we needle the chest????• Wait X ray is here should we shoot a film first?????

Case 1

Case 1
• Large bore replogle was placed and put to suction• HR improved to 70s• CPR stopped ongoing ventilation• Surgery called and baby emergently transferred to the NICU• Placed on ECMO on arrival
Dx of Large Left Congenital Diaphragmatic Hernia

Case 2
• Full term baby born by NSVD• Born to a 21 yr old G1P0 Blood Type O pos, Hep B neg, HIV neg, RPR NR,
GC/CT neg, GBS neg• Mild tachypnea after birth but transitioned well and went to the term
nursery• Noted to have an apneic spell on DOL 3• Admitted to the NICU for a workup• D stick and BMP/CBC unremarkable• EKG unremarkable

Case 2

Babies don’t always read textbooks

Goals and Objectives
• Epidemiology and Pathophysiology of CDH• Prenatal Diagnosis• Delivery Room Care• Post-natal ICU care• Surgical Repair• CDH Outcomes• CDH Management in the era of Fetal Care.
Epidemiology of CDH
• It affects 1 in 3000 live births• More common in males • May be associated with a genetic syndrome in
10-15% of the time • Miami Dade County has about 9 CDH• Broward has 11• Palm Beach County has 10

Pathophysiology of CDH
Post-Lateral region 70% (Bochdalek)>Anterior 25% (Morgagni) >Central 2-5% (Hiatal

Pathophysiology of CDH• Herniation of abdominal contents into the thoracic cavity• Lung Hypoplasia• Decreased airway generations • Thickened alveolar septae• Lack of complexity of the acinus• Increased arterial wall thickness
*Changes are seen in both lungs (regardless of which side the CDHis on)

Pathophysiology
• All these changes lead to underdeveloped lungs (Oxygenation and Ventilation issues)
• Increased risk of barotrauma and air leaks• Pulmonary Hypertension• Myocardial Dysfunction and Rt Heart Failure• Hypotension and poor perfusion

Prenatal Diagnosis of CDH
• US screening identifies about 70% of CDH• Findings may include herniated bowel or liver
seen in the chest or midline shift• Doppler of the umbilical vein and hepatic vessels
or gallbladder are useful landmarks• Differential diagnosis includes diaphragmatic
eventration• Lung Head ratio and Percent Predicted Values

Prenatal Diagnosis of CDH
• MRIs are a useful diagnostic tool to confirm dx
• To distinguish between eventrationand CDH
• To do lung volumetric assessment• Can quantify the amount of liver
herniation*Use for antenatal lung vascularization not validated yet

Antenatal Management of CDH
• Referral to a Tertiary Care Hospital (ideally with a Fetal Care Program)
• Consideration of In-Utero Therapies• Multidisciplinary consultations with Surgery,
Cardiology, Genetics• Risk stratification to allow for delivery planning• Tour the NICU/PICU• Engage Palliative Care where appropriate• Planning for delivery (who, what, when, why)

In Utero Therapy
In utero repair may be offered for isolated defects but not offered if there is liver herniation
FETO Rapair

Delivery Room Care
• Warm, dry, suction, and provide oxygen as indicated per the NRP algorithm.• No resuscitation with positive pressure by mask (if possible). • Evaluate breathing pattern and pre-ductal oxygen saturations.
• Intubate if any respiratory distress or respiratory failure. A cuffed endotracheal tube is preferred.
• If normal respiratory status, appropriate oxygen saturations in room air, and normal Apgars, consider transporting to NICU in room air.
• Place 10Fr double lumen sump to evacuate the stomach. (e.g. Replogle).1,2
• Access: UAC, UVC (double lumen preferred)• Essential evaluation: Blood gases, Chest xray

Post natal Management• For infants requiring intubation and ventilation (Level B-C; Class 2) -
• Surfactant has not been shown to be of any benefit in term infants with CDH; consider use in premature infants (< 35 weeks). If surfactant indicated, give Curosurf.
• If the infant develops a metabolic acidosis, allow time to improve. Consider normal saline bolus ONLY for signs of intravascular volume depletion.
• Sodium bicarbonate is not recommended to treat metabolic acidosis.• Avoid neuromuscular blockade. • Provide appropriate sedation to minimize stress that can exacerbate PPHN.
Consensus guidelines support the use of narcotics for sedation.• Cardiology should be consulted early and echocardiograms to evaluate function
and guide use of inotropes or pressors

Care in the NICU
• Fluids: D10W at 60 mL/kg/day• Evaluation:• Chest xray – AP and lateral (can be done after line
placement if stable.)• Echocardiogram• Cranial Ultrasound (Stat if needed for ECLS)• Labs: ABG, iCa, lactate, CBC with differential• AM Labs (after 12 hours of age): Metabolic panel,
Mg, phos, BNP, iCa, lactate, gases as needed• Access: UAC, UVC (double lumen preferred) or
PICC line (double lumen preferred)

Ventilator ManagementConventional Ventilation
Gentle ventilation is defined as:• Over the first 4 hours: Allow permissive hypercapnia; goal PaCO2 is less than 65.• Goal in hour 1-2: pre-ductal saturation > 70%• Goal in hour 3-4: pre-ductal saturation > 80%• Goal after hour 4: pre-ductal saturation > 85%• Allow the infant to be tachypneic with shallow breathing.
• In DR: Use rate of 60, PIP (peak inspiratory pressure) 16, PEEP 5, inspiratory time 0.3 seconds.
• Adjust PIP to obtain a gentle chest rise. Increase PIP in 2 cm H2O increments TO max 25 cm H2O

Ventilator Management
Failure of conventional ventilation: Failure = PCO2 > 70 x2, pre-ductal saturations < 80% on FiO2 = 1.Consider use of high frequency ventilation in infant with concern for severe
pulmonary hypoplasia.• High Frequency Jet ventilation (HFJV) - Preferred for refractory PCO2 > 75.
Best for air leak syndromes. • Monitor xrays with goal of diaphragm at 10 ribs maximum
• High Frequency Oscillatory Ventilation (HFOV) – Best for chest wall edema or anasarca or another choice for refractory PCO2 > 75.
• Monitor xrays with goal of diaphragm at 10 ribs maximum

ECMO Criteria
• Failure to maintain pH > 7.24 and pre-ductal O2saturation > 80% for > 60 minutes
• Refractory hypotension despite inotrope/vasopressor support
• Inadequate oxygen delivery with persistent metabolic acidosis (base deficit > 10) or rising serum lactate
• Prolonged use of 100% oxygen that cannot be weaned (> 4 hours)
• Unstable saturations with routine cares (diapering, repositioning, etc)
• No contraindications (cyanotic heart disease, weight < 1600 g, EGA < 33 weeks, IVH > grade 2)
•

Sedation for CDH Patients
• Avoid neuromuscular blockade when possible• Use NICU comfort protocol for analgesia – morphine prn and then
morphine drip• Add Dexmedetomidine drip for sedation• If necessary use Lorazepam prn• Follow NPASS scores and avoid over-sedation

Hypotension Management of CDH
Age Mean BPGoal (~ 25-75%ile)
Systolic BP5-95%ile
< 24 h 45-56 55-77
24-48 h 45-58 57-83
> 48 h 48-60 58-87
Blood pressure Cardiac functionNormal Abnormal (all doses in
mcg/kg/min)Normal Continue monitoring Milrinone (preferred) - 0.25
-1Dobutamine - 5-15 Epinephrine - 0.05 -1
Low Norepinephrine - 0.05-0.5 mcg/kg/minVasopressin - 10-50 milliunits/kg/hour
Dopamine* - 5-20 Epinephrine* 0.05 -1
Avoid excessive volume resuscitation unless cardiac under filling seen on echocardiogram. Maximum of two 10 mL/kg boluses.Hydrocortisone, 1st line of treatment: 1 mg/kg/dose, every 6-8 hours depending on when BP falls. Wean as tolerated to off.

Management of Pulmonary Hypertension
• Inhaled nitric oxide (iNO) (Level C; Class 2A))• Early iNO has no effect on the combined end point of death and ECLS.
• iNO use should be limited to neonates with suprasystemic PVR with right-to-left shunting across the ductus arteriosus and the foramen ovale, after optimal lung inflation and establishing that the LV is functioning well.
• Caution: iNO in neonates with impaired left ventricular (LV) systolic and diastolic function can worsen pulmonary venous hypertension and cause pulmonary edema.
• Consider using milrinone , if there is LV dysfunction, associated high left atrial pressures and left-to-right shunting at the level of the foramen ovale,

Timing of CDH Repair
• No uniform criteria for pre operative stabilization.• No consensus or evidence for better outcomes for repair on ECMO
Long Term Prognosis of CDH
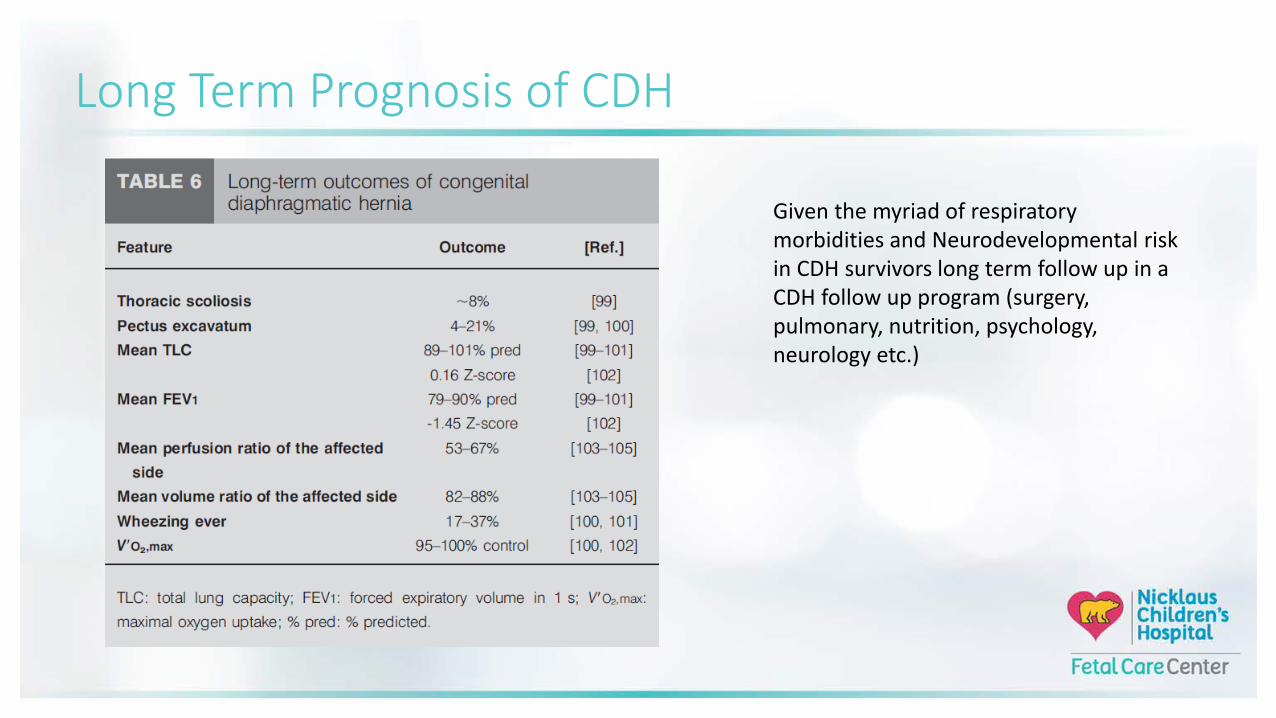
Given the myriad of respiratory morbidities and Neurodevelopmental risk in CDH survivors long term follow up in a CDH follow up program (surgery, pulmonary, nutrition, psychology, neurology etc.)

Fetal Care Program at NCH- Who we are
Devoted to the care of fetal patients with medical needs requiring intervention at birth
• Our mission: to provide compassionate and comprehensive care for babies with a high risk medical condition as they begin their life journey
• Our vision: is to be the region’s leader in providing the most advanced and supportive care for healthy mothers delivering high risk babies

Fetal Care Center
• Fetal care center to diagnose, evaluate, and provide specialized treatments spanning the full range of fetal anomalies.
• Special Delivery Unit (SDU) for healthy mothers with no pre-existing conditions or health problems
• Provides concierge navigated, coordinated, multi-disciplinary approach to the care of the high risk fetus

Fetal Care Team Medical Director Clinical Director
Fetal Care Navigator (24/7 availability)
• Multidisciplinary Approach• Cardiology • Cardiovascular Surgery• Plastics• Neurology• General Surgery• Nephrology• Genetics• Endocrinology• Orthopedics

Questions?