congenital aural atresia - utmb home - welcome · congenital aural atresia definition: “a birth...
TRANSCRIPT

Congenital Aural Atresia
Elizabeth J. Rosen, MD
Faculty Advisor: Arun K. Gadre, MD
The University of Texas Medical Branch
Department of Otolaryngology
Grand Rounds Presentation
January 8, 2003

Congenital Aural Atresia
Embryology
Classification
Evaluation
Surgical Repair
Results
Complications
Controversies
Congenital Aural Atresia
Definition: “a birth defect that is
characterized by hypoplasia of the external
auditory canal, often in association with
dysmorphic features of the auricle, middle
ear and, occasionally, the inner ear
structures” --Harold F. Schuknecht, 1989

Congenital Aural Atresia
Incidence: 1 in 10,000-20,000
Unilateral 3-5x more common than Bilateral
Males > Females
Right > Left
Inheritance—sporadic Autosomal recessive or dominant

Congenital Aural Atresia
Associations
– Hydrocephalus
– Posterior cranial
hypoplasia
– Hemifacial microsomia
– Cleft palate
– GU anomalies
Syndromes
– Treacher-Collins
– Goldenhar’s
– Crouzon’s
– Mobius’
– Klippel-Feil
– Fanconi’s
– DiGeorge
– Pierre Robin
– VATER
– CHARGE

Embryology
Auricle
– 4th week of gestation
– 1st and 2nd branchial arches
– Hillocks of His
1—tragus
2—helical crus
3—helix
4—antihelix
5—antitragus
6—lobule

Embryology
External Auditory
Canal
– 8th week of gestation
– 1st branchial groove
– Medial migration of a
solid core of epithelial
cells
– Recanalization during
6-7th months of
gestation

Embryology
Ossicles
– 4th week of gestation
– Meckel’s cartilage
Malleus head and neck
Incus body and short
process
– Reichert’s cartilage
Malleus handle
Incus long process
Stapes suprastructure
Embryology
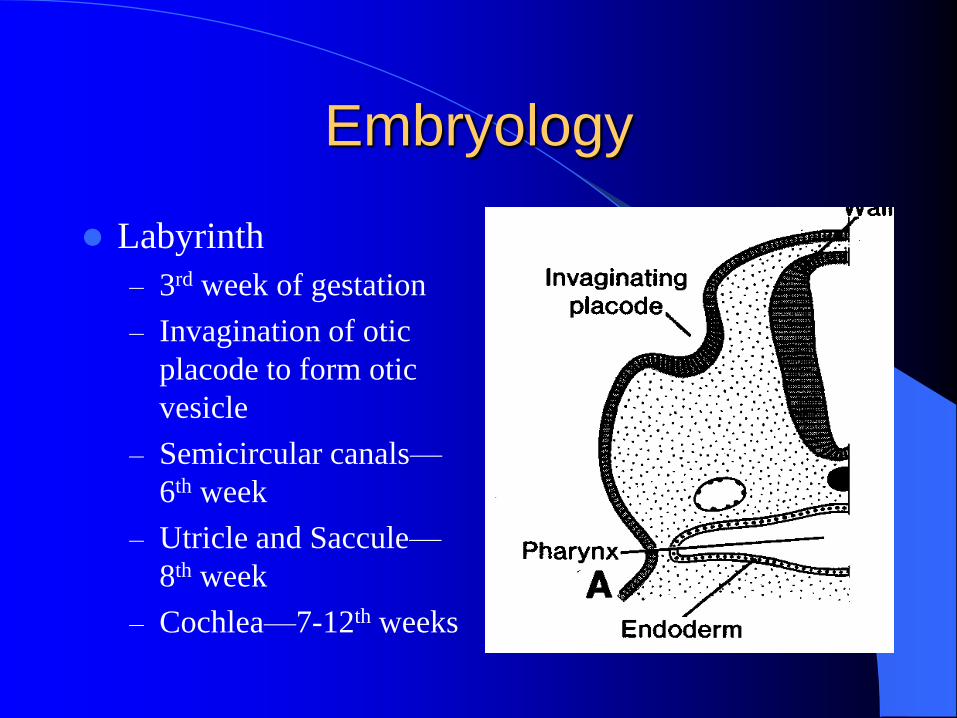
Labyrinth
– 3rd week of gestation
– Invagination of otic
placode to form otic
vesicle
– Semicircular canals—
6th week
– Utricle and Saccule—
8th week
– Cochlea—7-12th weeks
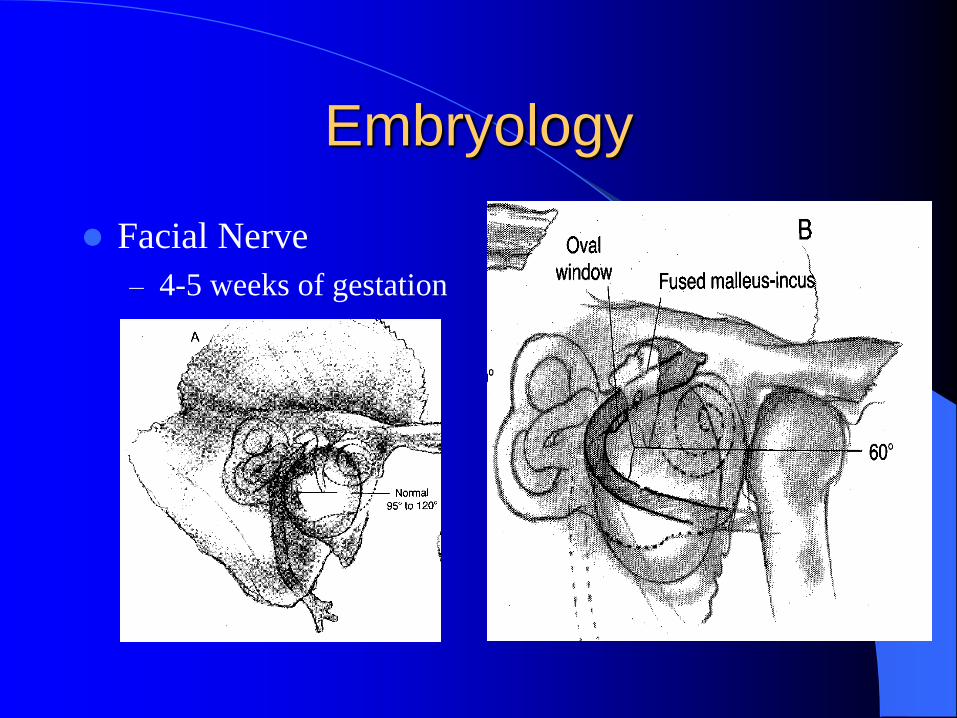
Embryology
Facial Nerve
– 4-5 weeks of gestation

Classification Altmann’s
– Grade I
Hypoplastic EAC, temporal bone, TM; normal or slightly hypoplastic middle ear cleft; normal or slightly deformed ossicles
– Grade II
Absent EAC; small middle ear cleft; osseous atresia plate; fixed and malformed ossicles
– Grade III
Absent EAC; markedly hypoplastic or absent middle ear cleft; absent or severely deformed ossicles
De la Cruz
– Minor
Normal mastoid
pneumatization
Normal oval window
Reasonable oval window-
facial nerve relationship
Normal inner ear
– Major
Poor pneumatization
Absent or abnormal oval
window
Abnormal horizontal facial
nerve
Anomalous inner ear
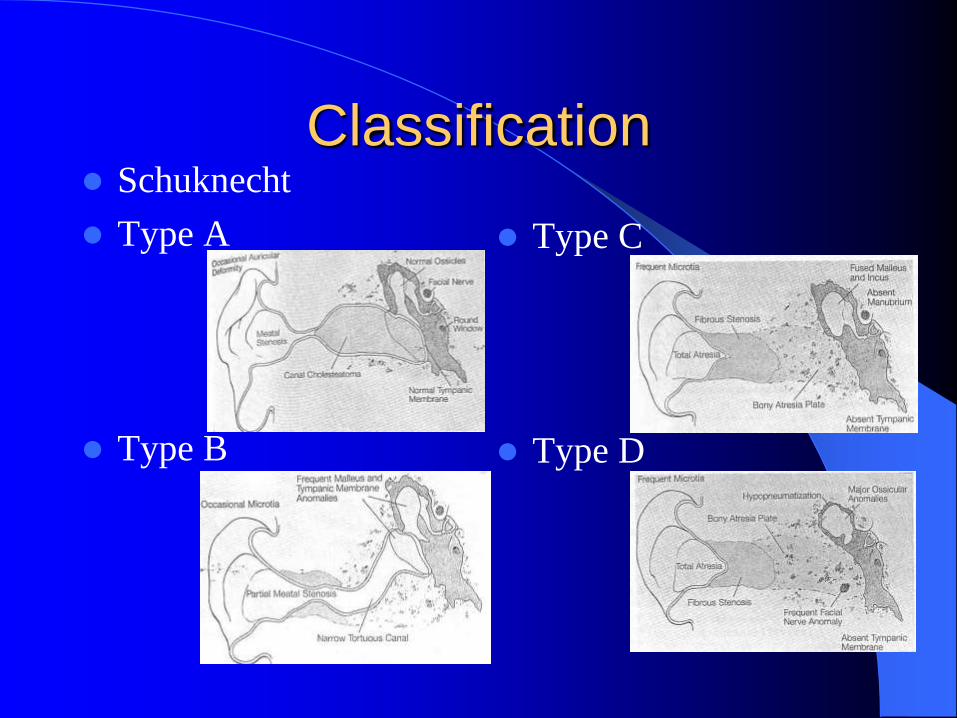
Classification Schuknecht
Type A
Type B
Type C
Type D

Classification
Jahrsdoerfer, 1992
– Based on HRCT
temporal bone findings
– Score correlates to
likelihood of
successful surgery

Evaluation
History
– Details of pregnancy
– Family history
Physical Examination
– Microtia
– Severity of EAC stenosis
– Craniofacial development

Evaluation
Audiologic Evaluation—ABR before
leaving the hospital
– Unilateral atresia
Auditory function of the “normal” ear
– Bilateral atresia
Establish presence of cochlear function
FIT WITH BONE CONDUCTION AID

Evaluation
High Resolution CT Temporal Bone
– Age 5-6 years
– Axial and Coronal
– Evaluate
Middle ear and mastoid pneumatization
Anatomy of ossicles
Inner ear morphology
Course of facial nerve
Surgical Repair
Candidacy
– ABSOLUTE REQUIREMENTS
1. Normal inner ear
2. Normal cochlear function
– HRCT Score
</= 5/10: poor
6/10: marginal
7/10: fair
8/10: good
9/10: very good
10/10: excellent

Surgical Repair
Timing
– Microtia repair should be performed prior to
undertaking atresia repair
– 5-6 years of age
– Controversy:
Between Stages 2 and 3 of microtia repair
2 months after completion of microtia repair

Surgical Repair
Transmastoid Approach
– Infrequently used
– Advantages:
More familiar approach
Identification of sinodural angle and lateral SCC as
landmarks
– Disadvantages:
Creation of mastoid cavity
– Larger defect to be skin grafted
– Prolonged healing
– Lifelong maintenance

Surgical Repair
Anterior Approach
– Popularized by Jahrsdoerfer, most frequently
utilized approach
– Advantage:
Avoidance of mastoid cavity
– Disadvantages:
Unfamiliar approach
Lack of landmarks

Surgical Repair
Video
– American Academy of Otolaryngology—Head
and Neck Surgery Foundation
Congenital Disorders—Volume #4
Harold F. Schuknecht, MD

Results
Difficult to interpret
– Different classification
of atresia
– Different criteria for
surgical candidacy
– Different definition of
“successful” outcome
– Different periods of
follow-up

Results
Stability of Hearing Levels
– Lambert, 1998
– Early postoperative period (<1yr)
60% 25dB or better
70% 30dB or better
– Prolonged follow-up (1-7.5yrs)
46% 25dB or better
50% 30dB or better

Complications EAC restenosis
– Highly variable: 8-50%
– Correlation to severity of atresia
TM lateralization
– 5-26% of cases
– Easier to prevent than to correct
Chronic infection
– Reconstructed EAC lacks normal keratin migration and cerumen production
– Create wide meatus, fix restenosis, frequent follow-up with canal debridement

Complications
Facial Nerve Injury
– 1.0-1.5%
– Vulnerability
Skin incision
Dissecting in the glenoid fossa
During canalplasty
Transposing the nerve
Dissecting preauricular soft tissue
– Prevention
Preoperative evaluation of HRCT
Intraoperative facial nerve monitoring

Complications
Sensorineural Hearing Loss
– Up to 15% of cases
– 4,000-8,000 Hz
– Acoustic trauma to the inner ear
Transmission of drill energy
Drill injury to ossicles
Manipulation of ossicular chain
– Avoidance—Meticulous technique

Controversies
Surgical Repair of Unilateral Atresia
– Historically
One hearing ear = normal speech and language development
No indication for surgery
– Recently
Unilateral hearing loss = auditory, linguistic and cognitive deficits
Improved preop evaluation, patient selection, surgical techniques, predictable results
Surgery indicated
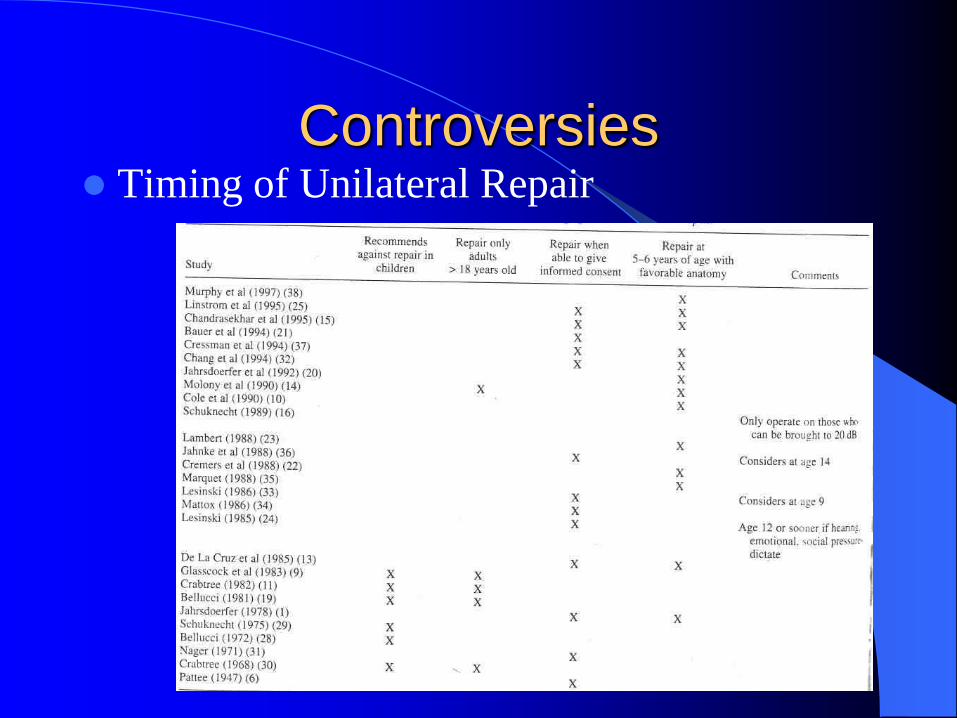
Controversies Timing of Unilateral Repair
Conclusion
Complex and Challenging Problem
Goals:
– Restore functional hearing
– Construct patent and infection-free EAC
Rewarding Surgery

Bibliography
•De la Cruz, A, Chandraseckhar, SS. Congenital Malformation of the Temporal Bone. In, Otologic
Surgery, D.E.Brackman, Ed. W.B. Saunders, Philadelphia; 1994.
•Kamerer, DB. Congenital and Acquired Atresia of the External Auditory Canal. In, Operative
Otolaryngology, Head and Neck Surgery, E.N.Meyers, Ed. W.B. Saunders, Philadelphia; 1997.
•Schuknecht, HF. Congenital Aural Atresia. Laryngoscope, 99; Sept 1989: 908-917.
•Lambert, PR. Congenital Aural Atresia. In, Head & Neck Surgery—Otolaryngology, 2nd Ed,
B.J.Bailey, Ed. Lippincott-Raven, Philadelphia; 1998.
•Bauer, GP, Wiet, RJ, Zappia, JJ. Congenital Aural Atresia. Laryngoscope, 104; Oct 1994: 1219-
1224.
•Jahrsdoerfer, RA, et al. Grading System for the Selection of Patients with Congenital Aural
Atresia. Am J Otology, 13 (1); Jan 1992: 6-12.
•Yeakley, JW, Jahrsdoerfer, RA. CT Evaluation of Congenital Aural Atresia: What the Radiologist
and Surgeon Need to Know. J Comput Assist Tomogr, 20 (5); Sept/Oct 1996: 724-731.
•Trigg, DJ, Applebaum, EL. Indications for the Surgical Repair of Unilateral Aural Atresia in
Children. Am J Otology, 19 (5); 1998: 679-686.
•Lambert, PR. Congenital Aural Atresia: Stability of Surgical Results. Laryngoscope, 108 (12);
Dec 1998: 1801-1805.
•Jahrsdoerfer, RA, Lambert, PR. Facial Nerve Injury in Congenital Aural Atresia Surgery. Am J
Otology, 19 (3); 1998: 283-287.
•Lambert, PR, De la Cruz, A, Choo, DI. Management of the Unilateral Atretic Ear. In,
Controversies in Otolaryngology, M.L.Pensak, Ed. Thieme, New York; 2001.