conference review the ketogenic diet: from molecular ... research 68 (2006) 145–180 conference...
TRANSCRIPT

Epilepsy Research 68 (2006) 145–180
Conference review
The ketogenic diet: From molecular mechanismsto clinical effects�
John Freemana, Pierangelo Veggiottib, Giovanni Lanzib,Anna Tagliabuec, Emilio Peruccab,d,∗
a The John M. Freeman Pediatric Epilepsy Center, Johns Hopkins Medical Institutions, Baltimore, MD, USAb Institute of Neurology, IRCCS C. Mondino Foundation, Pavia, Italy
c Department of Health Sciences, Human Nutrition and Dietetics, University of Pavia, Pavia, Italyd Clinical Pharmacology Unit, Department of Internal Medicine and Therapeutics,
University of Pavia, Piazza Botta 10, 27100 Pavia, Italy
Received 18 October 2005Available online 5 December 2005
Abstract
nd generalen andternational
nt effects,ies on thecacy
related tonsiderableential roleludingdomizedh needed
Recent years have witnessed an increased interest from pediatric neurologists, neuropediatricians, epileptologists aneurologists in the use of the ketogenic diet (KD) for the management of refractory epilepsies, particularly in childradolescents. This article summarizes current knowledge on various issues related to its use, as discussed at a recent inworkshop. Aspects discussed in some detail include (i) the putative mechanisms responsible for the diet’s anticonvulsabased on results of biochemical and neurophysiological studies in experimental models; (ii) consensus and controversmodalities of initiation of the diet, and different protocols of implementation; (iii) indications and contraindications; (iv) effidata, also in relation to seizure type, syndromic form and patients age; (v) adverse effects; (vi) methodological aspectsassessment of the diet’s clinical effects, and perspectives for future research. Overall, the data reviewed indicate that coadvances have been made in understanding the modes of action of the diet, its efficacy and tolerability profiles and its potin different types of epilepsy. Although clinical studies performed to date have important methodological limitations, incsuboptimally characterized patients’ populations and an uncontrolled design, a number of innovative, prospective ranstudy protocols have been recently proposed and are being implemented. The results of these will hopefully provide muchigh-quality information to better define the role of the diet in the treatment algorithms in different epilepsy syndromes.
Keywords: Ketogenic diet; Epilepsy; Mechanisms of action; Efficacy; Safety; Review
� Summary of a Workshop held at the Institute of Neurology IRCCS C. Mondino Foundation, Pavia, Italy, 24 September 2005.∗ Corresponding author. Tel.: +39 0382 986360; fax: +39 0382 22741.
E-mail address: [email protected] (E. Perucca).
0920-1211/$ – see front matterdoi:10.1016/j.eplepsyres.2005.10.003

146 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
1. Introduction
Recent years have witnessed an increased interestfrom pediatric neurologists, neuropediatricians, epilep-tologists and general neurologists in the use of theketogenic diet (KD) for the management of refractoryepilepsies. In parallel with this interest, a number ofstudies have been completed addressing a wide rangeof issues related to this diet, from its mechanisms ofaction in animal models to its efficacy and tolerabilityprofiles in different populations of patients. In recog-nition of this, the Institute of Neurology IRCCS C.Mondino Foundation in Pavia, Italy, took the initiativeof organizing, on 24 September 2005, an internationalworkshop whose purposes were to (i) discuss the ratio-nale for the use of the KD, and bridge basic sciencedata with evidence from clinical experience; (ii) reviewcritically and update current acquisitions on the use ofthe diet in the epilepsies; (iii) highlight controversiesconcerning indications and modes of application; (iv)identify areas and methodology for future research.
The workshop, which was attended by many lead-ing experts from both sides of the Atlantic, provided aforum for constructive interaction between many disci-plines which contribute to our knowledge in this area.The purpose of this manuscript is to summarize infor-m wella iatedd
2p
J
TH
uresa versa ed.T enm ase”a tom1 es,s al’ss esa nd
consider the affected individual to have divine, shamin-istic abilities (Fadiman, 1997). This can result in animportant example of cross-cultural misunderstand-ing. Seizures have also been ascribed to: “humors”,“toxins”, and infections (Lennox, 1960). Treatmentshave been empirical and have ranged from magic,to the ingestion of, or abstinence from certain foodsand even of certain animal and human parts. Irritationand counter-irritation, trephination, prayer, and fastinghave been prescribed. The removal of various organsand even death because of demonic possession has beenused as treatment.
Bromide, the first useful antiepileptic drug (AED),was used in the 1850s for “hystero-epilepsy” and laterused successfully in other forms of seizures. Phenobar-bital introduced in 1917 and phenytoin in 1937 werebut the first of what has become a plethora of newAEDs. Lack of understanding of the cause of seizuresand epilepsy has, over time, seemed to be the motherof therapeutic intervention and invention. While wehave learned much about the physiology of neuronalexcitation and inhibition, even today we understandlittle about what causes most seizures or what triggerstheir occurrence. Our treatments, therefore, continueto remain largely empirical. The KD is only one of themore recent, empirically derived, effective therapies.
medH edf m-i inga 20d .,2 ivet d tob nt”f dieth o-h thiss s ontt fectso t the1 toina Med-i KD.
arly1 cen-t ve or
ation that was presented at this workshop, ass the main points that emerged from the associscussions.
. Dietary treatments for epilepsy: a historicalerspective
.M. Freeman
he John M. Freeman Pediatric Epilepsy Center, Johnsopkins Medical Institutions, Baltimore, MD, USAIndividual seizures, as well as the repeated seiz
ssociated with epilepsy are frightening to obsernd may affect the quality of life of those affecthroughout the millennia their etiology has beysterious. Epilepsy, termed “The Sacred Disend “The Falling Sickness”, has been ascribedany causes, including demonic possession (Tempkin,976). Even among the modern day Hmong tribeizures are ascribed to problems with the individuoul (Fadiman, 1997). The Hmong consider seizurs indication of possession of “a healing spirit” a
In the early 1920s, an osteopathic physician naugh Conklin “discovered” that epilepsy, “result
rom intoxication of the brain from substances cong from the intestine”, and devised a “cure” by fastnd having the patient imbibe only water for up toays thus putting the intestine at rest (Freeman et al002). At a time when there were few other effect
reatments for seizures, the diet was documentee effective. This was termed “The Water Treatme
or epilepsy. It was found that a calorie-restrictedigh in fats, with sufficient protein and limited carbydrates could mimic the biochemical changes oftarvation and could preserve its beneficial effecthe seizures (Freeman et al., 2002). In modified formhis has been became today’s KD. The beneficial eff this dietary treatment were confirmed throughou930s, and but then largely forgotten as first phenynd then other anticonvulsants became available.
cation was far easier to prescribe and take than theInterest in the KD was re-awakened during the e
990s and since then multiple studies from manyres have concluded that the diet can be as effecti

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 147
even more effective in the management of children withdifficult-to-control seizures than other currently avail-able anticonvulsant medications (Freeman et al., 1998;Freeman and Vining, 1998). At Johns Hopkins, 150consecutive children with multiple seizure types andhaving at least two seizures per day were started on theKD and followed up (Hemingway et al., 2001a; Madyet al., 2003). Slightly more than half of the children whohad averaged >400 seizures per month at diet onset con-tinued the diet for 1 year, and 27% of those children,had had a >90% decrease in their seizures. Three to6 years later a similar percentage of this same grouphad continued, now off the diet, with few seizures, andmany had decreased or eliminated their medications.There are no studies of AEDs documenting similarlygood outcomes over comparable time periods.
The KD has been reported to be effective across awide variety of ages, seizure types and severities (Madyet al., 2003; Kossoff et al., 2002a) as well as differentetiologies (Kossoff et al., 2002a, 2005). It can be usedin liquid form (Kossoff et al., 2004a,b), for bottle ortube feeding, and perhaps even in a modified form asthe Atkins diet (Kossoff et al., 2003). The diet has fewsignificant side effects and when properly superviseddoes not cause weight gain or substantial growth abnor-malities (Vining et al., 2002) and has minimal effectso
isu rumlI sid-e dR s ofa at-m
3p
J
DU
or-m ast-i ents
are met by lipolysis and�-oxidation of fatty acids ratherthan by the breakdown of carbohydrates. Thus, the KDmaintains an anabolic nutritional state in a metabolicsituation of fasting. Any diet providing nutritional fatfor the generation of ketones that serve as an alternativefuel to body tissues may be called “ketogenic”. Ketonesmay produce an anticonvulsant effect, presumably dueto changes in (a) cerebral energy metabolism; (b) cellproperties decreasing excitability; (c) neurotransmitterfunction; (d) circulating factors acting as neuromodula-tors, and (e) brain extracellular milieu (Schwartzkroin,1999).
For the treatment of intractable childhood epilepsytwo types of KDs have thus far been developed. Thediets differ in their composition of free fatty acids.The traditional long-chain triglyceride (LCT) diet ismost commonly used (Swink et al., 1997; Lefevre andAronson, 2000). A second type, the medium-chaintriglyceride (MCT) diet is more ketogenic but lessused as it often causes gastrointestinal side effects. Anongoing clinical trial at Great Ormond Street Hospi-tal (London, UK) is currently comparing both waysof giving the diet. Finally, several infant formulas arenow available in the USA and in Europe (Nordli etal., 2001; Klepper et al., 2002). Despite the world-wide use of the diet (Kossoff et al., 2005) (Fig. 1) anda cha-n vel-o ons,t l asa tingp ctantt nes.A tresf ared na-t os-p y/P -s ducea op-k tas orldw ndw ardC n-t
n serum lipid profiles (Kwiterovich et al., 2003).How the diet exerts its anticonvulsant effects
nknown, but is thought possibly to relate to seevels of beta-hydroxy butyrate (Gilbert et al., 2000).ts mechanisms of action are the subject of conrable research, and of a recent book (Stafstrom anho, 2004). Perhaps understanding the mechanismction of the KD will lead to new approaches to treent of the epilepsies.
. The ketogenic diet: definitions and standardrotocols
. Klepper
epartment of Pediatrics and Pediatric Neurology,niversity of Essen, Essen, Germany
The KD is a high-fat, low carbohydrate, nocaloric diet that mimicks the metabolic state of f
ng. During a prolonged fast, body energy requirem
n increasing understanding of the underlying meisms, no international protocols have yet been deped. Age, groups, indications and contraindicati
he initiation, ratio, and duration of the diet, as welnticonvulsant co-medications are left to the treahysicians. Medical associations have been relu
o promote the diet and the development of guidelis a result, both in the USA and in Europe cen
ollow individual protocols and the data obtainedifficult to evaluate. A substantial number of inter
ional clinical studies follow the Johns Hopkins Hital protocol (http://www.neuro.jhmi.edu/Epilepseds/ketodiet.htm) (Swink et al., 1997). In Germanpeaking countries, a consensus on how to intrond maintain the diet that closely follows the Hins protocol was introduced in 2003 (Klepper el., 2004) (http://www.neuropaediatrie.com). Free KDoftware and a list of pediatric centres on the wide web providing a KD program in the USA aorldwide is available on the website of the Packhildren’s Hospital Stanford University Medical Ce
er (http://www.stanford.edu/group/ketodiet/).
148 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
Fig. 1. Countries providing the ketogenic diet (highlighted in grey) as identified in a recent survey. Updated fromKossoff et al. (2005). Reproducedwith permission from the author and from the publisher.
Indications for the KD are intractable child-hood epilepsy, glucose transporter type 1 (GLUT1)deficiency syndrome, and pyruvate dehydrogenasecomplex deficiency. Before initiating a KD contraindi-cations such as�-oxidation defects, liver or metabolicdisease interfering with glucose or ketone homeostasisneed to be excluded. A full history as well as a clinicaland nutritional assessment is necessary. Finally, thecompliance of patient and caretakers is essential. In theJohns Hopkins Hospital protocol and in the Germanconsensus protocol patients are admitted to the hospitaland ketosis is initiated by fasting. Reasons for hospital-isation are the difficulties of fasting in children and thepotential hazards of prolonged fasting as an outpatient.Others have described benefits of the non-fasting KDcompared with the initial fasting KD but prospective,randomized trials are not yet available to settle thiscontroversial issue (Kim et al., 2004a; Wirrell et al.,2002). During fasting, basic laboratory parameters, inparticular blood glucose and ketones in blood and urineneed to be monitored closely, preferably at the bedside.Once ketosis is established the diet will be introducedstarting with one-third of calories per meal. Calories areincreased to two thirds of calories per meal after every24 h and patients are discharged when the total amount
of calories per meal is well tolerated. During admissionpatients, parents, and caretakers are educated aboutsuitable food items, the calculation, and the preparationof ketogenic meals by the dietician. Multivitamins,minerals, and trace elements are supplemented.Follow-up demands regular outpatient admissions andeasy access to the treating pediatrician and dietician.Side effects of the diet such as kidney stones and bloodlipids need to be monitored (Kwiterovich et al., 2003;Ballaban-Gil et al., 1998). The time course of theintroduction of a KD and essential investigations asoutlined in the German consensus protocol is shown inFig. 2.
Despite the resurgence of the diet several controver-sial issues about this treatment remain. KD protocolsdiffer in the necessity of the initial fast as outlinedabove, the duration of the diet, fluid restriction, theuse of MCT versus LCT fatty acids, and the needfor carnitine supplements. Other issues such as thepotential long-term adverse effects or the potentialinteractions of the diet with AEDs remain largely unan-swered. Future progress in KD protocols will requirean international expert panel to clarify definitions anddevelop standard protocols. Recommendations shouldbe authorized by an international medical society to

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 149
Fig. 2. Algorithm of the introduction of the ketogenic diet as agreed by the consensus in German speaking countries (Klepper et al., 2004).
ensure quality control and to provide an interactive plat-form for physicians using the KD.
4. Implementation and monitoring: nutritionalaspects
A. Tagliabue
Human Nutrition and Dietetics, Department of AppliedHealth Sciences, University of Pavia, Pavia, Italy
4.1. Introduction
To obtain a level of ketosis adequate for seizurecontrol, low amounts of carbohydrates and highamounts of fat are administered in a rigidly con-trolled ratio. The use of such an unbalanced diet inchildren requires particular attention in implementa-tion and monitoring. The main nutritional problemsthat require careful monitoring arise from marginalor overt nutritional deficits (energy, proteins, mineralsand vitamins) or from excess nutrients (lipids, satu-rated fat and cholesterol) which are peculiar to thisdiet.
4.2. Fasting versus non-fasting at initiation
Ketosis is usually induced with a short period offasting (Freeman et al., 1996), followed by a gradualintroduction of the high-fat diet. From a biochemicaland physiological point of view, however, a period offast is notnecessary to induce and maintain a con-dition of metabolic ketosis. The key issue is whetherfasting can beuseful when initiating the diet in childrenwith epilepsy. Advantages of fasting include a shortertime to onset of ketosis, improved screening condi-tions for identifying underlying metabolic disorders,and the need for a hospital admission period whichallows to teach the family about the preparation ofmeals and the monitoring of ketosis (Katyal et al., 2000;Kossoff et al., 2005). On the other hand, disadvantagesof fasting include psychological stress, the risk of hypo-glycemia or dehydration, and the cost or inconveniencyof hospitalisation and repeated blood tests. In a world-wide survey, fasting was found to be preferred in mostcountries, though it was shortened or eliminated bymost physicians in Canada, UK, India, Sweden, TheNetherlands and Korea (Kossoff and McGrogan, 2005).Unfortunately, only few groups that use the non-fasting

150 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
protocol have reported on their experience (Wirrell etal., 2002; Vaisleib et al., 2004; Kim et al., 2004a) andonly one centre has compared the two protocols intheir patients (Kim et al., 2004a). In the latter study,no significant difference was found in time to strongurinary ketosis between the two groups. As for earlyside-effects, moderate dehydration was less frequent innon-fasted subjects, but the incidence of hypoglycemiawas not different between groups.Wirrell et al. (2002)reported that time to ketosis and diet efficacy in eightinpatients managed without fasting were similar tothose described with fasting protocols. Groups usingthe non-fasting protocol have also compared inpatientversus outpatient initiation of the diet, and found no sig-nificant differences in seizure control between the twoapproaches (Vaisleib et al., 2004). More informationfrom well-designed prospective studies, however, areneeded to assess optimal non-fasting protocols and out-patient initiation of the diet. In any case, when the dietis initiated without hospitalisation, adequate facilitiesmust be available to instruct families on meal prepara-tion and monitoring techniques.
4.3. Providing adequate energy supply
It is extremely important to provide adequate energyi asf thec r 7-d , orb ces( ge(e uals asalm ingt eds.G foodr atek ightl satef
4a
ro-t ins
which can be included in the diet, but it is generallypossible to give 1 g protein per kg of body weight. Thisis slightly less than the RDA for infants (1.5 g/kg/day)and for children aged 1–3 years (1.1 g/kg/day), but it isadequate for older children. Proteins must be of highquality (i.e. rich in essential amino acids), which is usu-ally the case because foods which are rich in animalproteins usually are also rich in fat.
A marginal intake of proteins, calories or other nutri-ents can affect growth. Two prospective (Vining et al.,2002; Liu et al., 2003) and several retrospective studies(Couch et al., 1999; Williams et al., 2002) have shown adecrease in growth percentiles andz scores in childrenon the KD. These children were subjected to caloricrestriction at initiation of the diet with adjustments dur-ing the course of the treatment to match individualneeds, and therefore no weight or height impairmentwas expected. In the latest study, a retrospective chartreview byPeterson et al. (2005), children were giventheir usual caloric intake since the beginning of treat-ment. A decrease in height-for-agez scores was foundat 6 and 12 months, which was significant only in sub-jects with high urinary ketosis (80–160 mg/dl). As apoint of interest, subjects who stayed on the diet for12 months tended to consume fewer kilocalories. At 6months the weight change was predicted by kilocalo-r h isn wthi ac-t thm teinl thata ea-s sessc ucedb y ber ncea icalt lin-i
4
ain-t itor-i henp cor-r ured
ntake to avoid protein (muscle mass) utilizationuel. To this purpose, energy requirements ofhild need to be determined by means of 3- oay food diaries to estimate usual caloric intakey referral to the recommended dietary allowanRDA) for healthy children of the same age ranFood and Nutrition Board, 2002). However, groupstimates can give inaccurate results in individubjects. In our protocol, we measure individual betabolic rate by indirect calorimetry before start
he diet and every 3 months, to adjust caloric neastrointestinal disturbances, poor appetite,
efusal, or intermittent fasting to restore adequetosis may determine a low energy intake and weoss. We use a liquid formulated snack to compenor poor caloric intake when needed.
.4. Ensuring appropriate intake of proteins andmino acids
The maintenance of a constant ratio of fat to peins + carbohydrates limits the amount of prote
ies intake, but at 12 months it was not. Researceeded to identify factors that permit normal gro
n some children but not in others. In clinical price, all children on the KD should have their growonitored by growth charts, and energy and pro
evels should be adjusted to assist growth at a ratellows seizure control to be maintained. Because murement of body weight alone does not permit to ashanges in body protein content (muscle mass) indy the diet, other estimates of body composition maequired (arm anthropometry, bioelectrical impedanalysis or dual X-ray absorptiometry). Biochem
ests (plasma proteins) may aid in identifying subccal protein deficiency.
.5. Monitoring intake of carbohydrates
A low intake of carbohydrates is essential to main ketosis. Measuring urine ketones allows monng of adherence to the low carbohydrate intake. Wossible, blood ketones, which have been shown toelate better with seizure control, should be meas

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 151
Table 1Nutritional monitoring protocol
Nutritional risk Clinical effect Monitoring method
Energy deficits Weight loss; growth impairment Anthropometry (weight, height, skinfold thickness);resting metabolic rate measurements
Protein deficits Muscle mass loss, bone metabolismimpairment
Arm muscle circumference; plasma proteins (albumin,pre-albumin, transferrin)
Lipid excess (saturated) Atherosclerosis Plasma lipids profileCalcium deficits Osteopenia and osteoporosis Dual X-ray energy absorptiometry, bone metabolism
markersSelenium and potassium deficits Cardiac complications Whole blood or serum levelsWater-soluble vitamins deficits Dermatitis, anemia, neurological symptoms,
etc.Plasma and urine levels, blood count
(Gilbert et al., 2000). The low content of starchy foodand vegetables makes the KD extremely poor in fiber,which can cause constipation.
4.6. Optimizing intake of lipids
In a recent study of 141 children, the classic dietwas found to cause a significant increase in athero-genic apoB-containing lipoproteins and a decrease inthe anti-atherogenic HDL cholesterol after 6 months;significant but less marked changes persisted in thosechildren who were followed up for 12 and 24 months(Kwiterovich et al., 2003). To reduce cardiovascularrisk, the ratio of poly-unsaturated + mono-unsaturatedfatty acids to saturated fatty acids needs to be increasedin ketogenic meals, and blood lipid profile should bechecked regularly.
4.7. Minerals and vitamins
Due to the limited food choice, the classic KD is alsodeficient in minerals and vitamins, and needs to be sup-plemented with sugar-free products. Inadequate cal-cium intake and limited sun exposure can impair bonemineralization in children already at risk of osteopeniaand osteoporosis due to long-term AED therapy (Shet,2 in-e
4
il-d itionas re-s ded.
Careful monitoring of nutritional status during treat-ment is necessary to prevent malnutrition. The risk ofmalnutrition is particularly high in children with poornutrition at baseline (Bertoli et al., 2002). Main nutri-tional risks and monitoring methods are summarizedin Table 1.
5. Maximizing acceptability and compliance
S. Bertoli
International Center for the Assessment of NutritionalStatus (ICANS), University of Milan, Milan, Italy
The composition of the KD is expressed by a ratioof fat to protein and carbohydrates weights equal to 4(fat):1 (protein + carbohydrates); proteins are providedin order to meet but not to exceed the recommendedamount of 1 g/kg of body weight, whereas total caloricintake is based on age-adjusted standards. This impliesthat 90% of dietary calories are derived from fat andno more than 2–3% are derived from carbohydrates.To maintain a stable ketosis, strict adherence to thedietary plan is required, and even small deviations infood preparation or the intake of small amounts of foodoutside the dietary plan may reduce blood ketones,causing a substantial reduction in the diet’s efficacy( 98
ctso andu tinga effi-c tings ck-i oneh n 1
004). Therefore, routine examinations of bone mral density and/or bone enzymes are required.
.8. Conclusions
Implementation and monitoring of the KD in chren needs a dedicated team to assess basal nutrtatus in order to improve caloric and nutrient pcription. Adequate supplementation is always nee
l
Casey et al., 1999; Carroll and Koenigsberger, 19).The potential short- and long-term side effe
f the diet, together with the diet’s harshnessnpalatability are the most important factors affecdversely compliance and, consequently, clinicalacy. Although large multicentre studies investigapecifically long-term compliance on the diet are lang, a review of the literature indicates that less thanalf of the patients remain on the diet for more tha

152 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
year (Hemingway et al., 2001a; Freeman et al., 1998;Lightstone et al., 2001). Discontinuations are due tomedical and non-medical reasons.
Our experience in a total of 32 children placed onthe KD between September 1994 and August 2005showed that 24 discontinued the diet after 1–33 months(18 within the first 12 months). Of these, 18 (75%)discontinued for medical reasons, specifically due tolack or loss of efficacy (16 patients) or adverse compli-cations (3 patients, including 2 with severe metabolicacidosis and one with repeated probably diet-unrelatedchest infections). Six children discontinued the diet fornon-medical reasons; these included caregivers’ issuesand patients’ unwillingness to continue on the diet. Infact, the diet’s acceptance and compliance are stronglydependent on the collaboration of both the child and theparents. The preparation of meals can be burdensomefor parents, who must pay great attention in choosing,weighing and cooking every dietary component. Onthe other hand, the direct involvement of parents in the
management of their child’s epilepsy often makes thediet more acceptable than expected. The poor palatabil-ity of some ketogenic meals is not a common cause ofinadequate compliance, and it is almost never a causefor discontinuation. By contrast, ingestion of additional“forbidden foods” is one of the most common causes ofan insufficient level of ketosis, and may be due to inter-ference from a “sympathetic” relative or friend or theresult of the child’s own industry. The latter possibilityis more frequent in older children and in children withmild cognitive impairment. To maximize acceptability,at our institution the nutritional and neurological teamshave established a collaborative, highly interactive pro-tocol (Table 2).
The recent introduction of nutritionally completepowdered formulas has provided an additional tool toimprove compliance when suitable food is unavailableor cannot be conveniently administered, for exampleduring illness. Regular monitoring of ketone bodieswith urinary sticks or with capillary measurements
Table 2Protocol for maximizing compliance with the ketogenic diet
Operator
Before starting the diet
the diensider
tient’s
impai
of a se
I, cooke of thesistanc
At 2 wee
Nm rela ietician
ements
M
D ation
Enrolment motivated patients/familyDetailed description to family and patients of both the role of
epilepsy (history, efficacy, side effects, etc.), palatability coadherence to meal preparation instructions
Dietary history. Seven-day diary with careful evaluation of paorder personalize at best the dietary plan
Clinical evaluation to identify possible chewing or swallowingdietary strategies
Compilation of a questionnaire concerning the acceptabilityfoods (lecithin, butter, high fat cream, olives, etc.)
nduction period (hospital)Training of parents to instruct them on how to choose, weighContinuous dietician’s presence and assistance during intakContinuous neurologist’s and nutritionist’s monitoring and as
hospital admissionfter discharge from the hospitalDaily phone contacts with dietician and nutritionist in the firs
eurological and nutritional evaluation every 3 months24 h/day availability of nutritionist and dietician for any probleDietary adjustments according to changing nutritional requir
appetite, and to meet any other potential requirementonitoring of ketones every day with urinary sticks
elivery of a short manual containing the most important inform
of the diet. The manual is directed to all people involved in the m(including school teachers, educators, physiatrists, grandparentsNeurologistt in the treatment ofations, and need for strict
Neurologist, nutritionist
food habits and tastes in Dietician
rment requiring special Nutritionist
lected list of ketogenic Parents
and serve ketogenic meals Dieticianfirst ketogenic meals Dietician
e during the period of Neurologist, nutritionist
ks Nutritionist
Nutritionistted to diet management Neurologist, nutritionist, d, to changing taste and Nutritionist, dietician
Parents
required for maintenance Nutritionist, dietician
anagement of the patient, etc.)
J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 153
with user-friendly instruments that determine simul-taneously blood ketones and blood glucose, and thecompilation of daily diary of seizures, are essential tothe physician not only to assess compliance but also toevaluate the relationship between ketosis and seizurecontrol.
A synergic collaboration between the patient’s fam-ily and the epilepsy team is essential for a successfuluse of the diet. In contrast with using AEDs, managingepilepsy with the diet requires very active caregivers’involvement, and families are prone to balance theirefforts to the extent of perceived results. If there is goodefficacy, acceptance and compliance are greatly facil-itated. In the long-term management of responders,we observed a reduced efficacy in 25% of patients andthis was almost invariably associated with a reducedacceptance of the diet and with reduced plasmaketones. A reasonable hypothesis is that the reductionof compliance was the cause, and the decreasedplasma ketones and loss of the diet’s efficacy werethe consequence. However, some kind of metabolicadaptation leading to reduced ketosis despite sub-stantial compliance with the diet cannot be excluded.Reduced compliance is frequently a late consequenceof the family’s frustration when it becomes difficult orimpossible to attain stable ketosis or effective seizuresc
6i
Ja
a
Do
6
ofe un-d thed il toa ;F int bout
its effects on brain function, but few studies addressedmechanisms of the diet’s action. Indeed, it was not untilthe mid-1990s that a resurgence in interest led to sus-tained research efforts into this non-medicinal therapy.
That dietary factors can influence brain functionshould not be surprising, and the concept of treatinga chronic disorder such as epilepsy with nutritionalapproaches holds an intrinsic appeal. During the historyof the diet’s use, clinicians have attempted to modify itsclassic formulation to improve tolerability, and in thehopes of enhancing efficacy. Recent variations on thistheme include the Atkins diet (Kossoff et al., 2003), thelow glycemic-index diet (Pfeifer and Thiele, 2004), anddiets supplemented or enriched in polysaturated fattyacids (PUFAs) (Schlanger et al., 2002; Fuehrlein et al.,2004). This interest has brought together investigatorsfrom diverse fields to focus on how systemic metabolicchanges induced by a high-fat, low-carbohydrate diet –which results in prominent ketosis – can dampen neu-ronal excitability and/or hypersynchrony, the presumedend product(s) of the diet’s action.
There have been numerous mechanistic hypothe-ses to explain the anticonvulsant activity of the KD.These include (1) changes in brain pH (e.g., acido-sis which would favour neuronal inhibition throughproton-sensitive ion channels) (Al-Mudallal et al.,1 nce(a .,2 ta( rt bykD -i withw ucho e ofk evi-d moree
6a
thep oneb ace-t diet
ontrol.
. How does the ketogenic diet work? A looknto the mechanisms of action
.M. Rhoa, P.G. Sullivanb
Barrow Neurological Institute, St. Joseph’s Hospitalnd Medical Center, Phoenix, AZ, USA;
bSpinal Cord and Brain Injury Research Center,epartment of Anatomy and Neurobiology, Universityf Kentucky, Lexington, KY, USA
.1. Introduction
One of the perplexing mysteries in the fieldpilepsy is the question of how the KD works. This famental question is all the more compelling sinceiet may yield considerable success when AEDs fadequately control seizure activity (Vining et al., 1998reeman et al., 1998). Ever since its introduction
he early 1920s, investigators have been curious a
996); (2) changes in electrolyte and water balaMillichap and Jones, 1964); (3) direct inhibitoryctions of fatty acids (i.e., PUFAs) (Cunnane et al002); (4) neurotransmitter alterations (Erecinska el., 1996; Szot et al., 2001; Yudkoff et al., 2001a,b); and5) changes in energy metabolism, reflected in paetone body production and metabolism (Appleton andeVivo, 1974; Pan et al., 1999). Because of the strik
ng ketosis associated with the diet, and the easehich beta-hydroxybutyrate can be measured, mf the attention in this field has focused on the roletone bodies as mediators. However, little directence in this regard has emerged to date (for axtensive review, seeStafstrom and Rho, 2004).
.2. Anticonvulsant effects of ketone bodies andctions on inhibitory neurotransmission
When fats are metabolized preferentially asrimary energy source, the liver produces ketodies (beta-hydroxybutyrate, acetoacetate and
one). The prominent ketosis accompanying the

154 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
led Keith (1933) to consider whether ketone bodieswere in fact anticonvulsant compounds. Seizuresacutely induced by thujone (the active constituent ofwormwood oil) in rabbits were blocked by pretreat-ment with acetoacetate (Keith, 1933), an observationthat was recently confirmed in an audiogenic seizuresusceptible mouse model (Rho et al., 2002). Therehave also been several historical reports of acetonepossessing anticonvulsant effects (Helmholz andKeith, 1930; Keith, 1931; Jenney and Pfeiffer, 1958;Yamashita, 1976; Vodickova et al., 1995). The mostextensive characterization of acetone’s anticonvulsantproperties was conducted byLikhodii et al. (2003),who demonstrated dose-dependent suppression ofseizures by acetone administered intraperitoneally infour separate animal models of seizures and epilepsy:(1) the maximal electroshock (MES) test, which mod-els human tonic–clonic seizures; (2) the subcutaneouspentylenetetrazole (PTZ) test, which models humantypical absence seizures; (3) the amygdala kindlingtest, which models human complex partial seizureswith secondary generalization; and (4) the AY-9944test, which models chronic atypical absence seizures.Despite what appears to be broad-spectrum activityexhibited by acetone, the precise anticonvulsant mech-anism(s), however, remain(s) unclear. Interestingly,e dietw vels( M)a scopy( noc ct oft ithe arei eart( calt onso nota Ps)a onsa ouse alc ntsea
ionsa ised
at the centre of molecular bioenergetics—responsiblefor cellular homeostasis but also the critical determi-nant of cell survival or death. As fatty acids comprisethe bulk of the KD composition, and undergo beta-oxidation in mitochondria, it is presumed that thisimportant metabolic shift alters the balance of impor-tant substrates and neurotransmitters, and at the sametime, affects respiratory chain function with concomi-tant effects on mitochondrial respiration and controlof oxidative stress, among other actions. Additionally,ketone bodies may be juxtaposed not simply as passivebystanders. Ketone bodies are generated by liver mito-chondria as alternative substrates for fuel consumption(when the availability of glucose is low during fast-ing states), especially by the brain. However, recentevidence suggests that ketone bodies may also servea teleological function in preserving brain function asneuroprotective agents (Kashiwaya et al., 2000; Tieu etal., 2003; Reger et al., 2004; Veech et al., 2001; Veech,2004).
Yudkoff and colleagues have proposed that in theketotic state, there are major shifts in brain aminoacid handling, the most significant of which is thereduction of aspartate relative to glutamate, reflectinga shift in the equilibrium of the aspartate aminotrans-ferase reaction (Yudkoff et al., 2001a, 2004a,b). Thisa uro-t rateo bep oxy-l it-t thes ta 5A bee -i tentp hens ck-e one( dyd ildk iso-f ndG uc-t ta ionm rela-
pileptic patients who responded favourably to theere found to have elevations in brain acetone le
with estimated concentrations upwards of 1 ms measured by magnetic resonance spectroSeymour et al., 1999). Curiously, there has beenlear demonstration of a direct anticonvulsant effehe principal ketone body, beta-hydroxybutyrate (wither stereoisomer). While these in vivo studies
ntriguing, at a cellular level, ketones do not appo acutely influence synaptic transmission.Thio et al.2000)utilized standard cellular electrophysiologiechniques and found that millimolar concentratif beta-hydroxybutyrate and acetoacetate didffect: (1) excitatory post-synaptic potentials (EPSnd population spikes in CA1 pyramidal neurfter Schaffer collateral stimulation; (2) spontanepileptiform activity in the hippocampal–entorhinortex slice seizure model; and (3) whole-cell currevoked by glutamate, kainate, and�-aminobutyriccid (GABA) in hippocampal neurons.
Further mechanistic considerations focus on actt the level of the mitochondrion, the organelle po
daptation in the metabolism of the excitatory neransmitter glutamic acid (i.e., a decrease in thef glutamate transamination to aspartate) wouldredicted to increase the rate of glutamate decarb
ation to GABA, the major inhibitory neurotransmer, since more glutamate would be available forynthesis of both GABA and glutamine (Erecinska el., 1996; Yudkoff et al., 1996, 1997, 2001a,b, 200).n increase in brain GABA levels would thenxpected to dampen seizure activity (Fig. 3). Interest
ngly, in a variety of seizure models, the most consisrotection afforded by the KD was observed weizures were evoked by the GABA receptor blors picrotoxin, bicuculline and gamma-butyrolactBough et al., 2003). Further, a recent animal stuemonstrated that caloric restriction, resulting in metosis, enhanced expression in the brain of bothorms of glutamic acid decarboxylase (GAD65 aAD67, the biosynthetic enzymes for GABA prod
ion), suggesting an increase in GABA levels (Cheng el., 2004). However, while increased GAD expressight suggest enhanced GABA synthesis, the

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 155
Fig. 3. Diagram illustrating the metabolic inter-relationships between brain metabolism of glutamate, ketone bodies and glucose. In ketosis,3-OH-butyrate (beta-hydroxybutyrate) and acetoacetate contribute heavily to brain energy needs. A variable fraction of pyruvate (1) is ordinarilyconverted to acetyl-CoA via pyruvate dehydrogenase. In contrast, all ketone bodies generate acetyl-CoA which enters the tricarboxylic acid (TCA)cycle via the citrate synthetase pathway (2). This involves the consumption of oxaloacetate, which is necessary for the transamination of glutamateto aspartate. Oxaloacetate is then less available as a reactant of the aspartate aminotransferase pathway which couples the glutamate–aspartateinterchange via transamination to the metabolism of glucose through the TCA cycle. Less glutamate is converted to aspartate and thus, moreglutamate is available for synthesis of GABA (3) through glutamic acid decarboxylase (GAD). Adapted fromYudkoff et al. (2004c)withpermission.
tionship between GAD expression and GABA levelsis not entirely clear, and depends on numerous vari-ables (Rimvall and Martin, 1992, 1994; Rimvall etal., 1993); increased GAD expression might actuallyreflect decreased GABA production. GAD expressionis more accurately interpreted in the context of mRNAexpression, GAD protein levels, GABA levels andturnover.
Clinically, few measures of excitatory or inhibitoryneurotransmission have been reported in patientstreated with the KD, or who became ketotic throughother means.Dahlin et al. (2005)recently reportedchanges in several amino acids in the cerebrospinalfluid of patients on a KD, the most notable observa-tion being that GABA levels were higher in respondersthan in nonresponders. Moreover, in very good respon-ders (i.e., >90% seizure reduction), GABA levels weresignificantly higher at baseline as well as during thediet. On the other hand, CSF aspartate levels remainedunchanged. The collective evidence from laboratoryand clinical observations strongly suggests that theKD may enhance brain GABAergic inhibition, but not
via the more established mechanism of post-synapticGABAA receptor modulation shared by several anti-convulsant medications.
6.3. The role of PUFAs and modulation ofmitochondrial uncoupling proteins (UCPs)
Ketone bodies are not the only substrates thatincrease during treatment with the KD. The diet ismostly comprised of fats, constituting≥90% of thetotal calories by weight, and poly-unsaturated fattyacids (PUFAs) may represent a key fat constituent.Certain PUFAs are known to inhibit fast, voltage-dependent sodium channels (Xiao et al., 1995, 1998)and L-type calcium channels (Xiao et al., 1997).Such actions would be expected to dampen membraneexcitability. More relevant, however, are reports thatPUFAs may help reduce seizure activity (Yehuda etal., 1994; Voskuyl et al., 1998; Schlanger et al., 2002;Fuehrlein et al., 2004) and are elevated in patientstreated with the diet (Fraser et al., 2003). Similar tothe effects seen in cardiovascular disease models, it is

156 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
Fig. 4. Uncoupling action of an uncoupling protein (UCP). The electron transport chain builds up a proton gradient across the inner mitochondrialmembrane (IMM) which provides the proton-motive force for ATP production (conversion of ADP to ATP through ATP synthase [ComplexV]). The uncoupling proteins provide an alternative pathway for proton re-entry into the mitochondrial matrix, thereby generating heat insteadof ATP. Two major hypotheses for how this occurs have been proposed: (1) the UCP transports protons directly; or (2) electroneutral, protonatedfatty acids diffuse across the inner mitochondrial membrane and the proton is released in the matrix. The fatty acid anion is transported back tothe intermembrane space by the UCP, and the cycle repeats. Adapted fromMattiasson and Sullivan (in press), with permission.
hypothesized that PUFAs possess anticonvulsant activ-ity through modulation of voltage-gated ion channels(Vreugdenhil et al., 1996; Xiao and Li, 1999).
Fatty acids are also known to induce the activity ofUCPs (seeFig. 4), several of which have been identifiedin the mammalian brain (Horvath et al., 2003; Mattsonand Liu, 2003; Sullivan et al., 2003, 2004a; Krauss etal., 2005; Mattiasson and Sullivan, in press). Activationof mitochondrial UCPs results in a reduction of theproton gradient across the inner mitochondrial mem-brane, which dissipates heat and reduces ATP synthe-sis, calcium influx into the mitochondrial matrix, andreactive oxygen species (ROS) production (Horvath etal., 2003). Mitochondrial ROS production is intimatelylinked to the mitochondrial membrane potential (�Ψ ),and a high�Ψ promotes ROS production throughincreased electron shunting. UCPs dissipate�Ψ byincreasing proton conductance, resulting in decreasedROS formation. Even a modest reduction of�Ψ cansignificantly reduce ROS production (Votyakova andReynolds, 2001). The relevance of these observationsto the KD’s actions was recently illustrated bySullivan
et al. (2004b), who demonstrated that the diet increasedmitochondrial UCP activity and decreased ROS forma-tion in mouse hippocampus.
Reduction of calcium influx and ROS productionare actions that are highly relevant to neuroprotec-tion. However, how do such changes relate to ananticonvulsant effect? It is now well known that thedramatic metabolic and bioenergetic changes in thebrain that accompany seizure activity can contributeto neuronal injury, in part through oxidative mecha-nisms (Liang et al., 2000; Frantseva et al., 2000; Uedaet al., 2002; Cock, 2002; Cock et al., 2002). Lessappreciated is the notion that oxidative stress itselfcan provoke seizure activity. Increased mitochondrialfree radical load, occurring through a variety of mech-anisms, has been shown to produce seizure activity(Willmore et al., 1978; Patel, 2004) or enhance sus-ceptibility to seizure provocation (Liang and Patel,2004; Patel, 2004). Electrophysiological studies havealso confirmed the seizure-provoking effects of oxida-tive stress. Exogenous H2O2 administration can mimicacute oxidative stress in vitro, and several studies have

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 157
shown that H2O2 exposure can induce neuronal hyper-excitability. In acute thalamo-cortical and hippocampalslices from rodents, H2O2 caused epileptiform activityboth during infusion as well as after washout (Frantsevaet al., 1998; Avshalumov and Rice, 2002).
Thus, there are emerging data that seizures may beprecipitated by oxidative stress, and that a reductionin free radical formation may prevent seizure activity.While none of the clinically available anticonvulsantmedications are believed to act principally throughantioxidant mechanisms, the KD has been shownto reduce ROS formation (Sullivan et al., 2004b),through induction of several brain-specific mitochon-drial UCPs. Additionally, in a preliminary study,Kimet al. (2004b)demonstrated that the ketone bodies beta-hydroxybutyrate and acetoacetate (in millimolar con-centrations) prevented H2O2-induced hyperexcitabil-ity in acute neocortical brain slices and dissociatedneurons, and that ketones were capable of signifi-cantly reducing ROS formation in isolated mitochon-dria. These observations suggest that the diet mayprotect against seizure activity (and may also be neuro-protective) through antioxidant mechanisms activatedby fatty acids and ketones.
6.4. Actions mediated by the ATP-sensitive (K )a
on-d es ine neu-r P-s lyc aticb them d byh er-p .
s asw ip-p orsalvi ich,i edt tion(e sn est
that ketone bodies block repetitive firing of SNPR neu-rons through activation of KATP channels (G. Yellen,personal communication). It remains unclear, however,whether the biochemical changes induced by the dietactually favour or negate activation of KATP channels(Vamecq et al., 2005). Certainly, prior observationshave suggested that the diet increases the level of bioen-ergetic substrates in the brain (De Vivo et al., 1978;Pan et al., 1999). Additionally, it is known that acuteseizure activity is accompanied by increases in glucosemetabolism (Chugani et al., 1994). These findings maysuggest an inhibition, not activation, of KATP channels.
In addition to the plasmalemmal KATP channel,there exists a mitochondrial form, localized to theinner mitochondrial membrane, that is likely to be dis-tinct in terms of molecular composition, pharmacologicregulation, and biological function(s) (Busija et al.,2004). While the specific role(s) of mitochondrial KATP(mitoKATP) channels has (have) yet to be elucidated,published data suggest that activation of these channelsmay reduce ROS formation (Ferranti et al., 2003), andby extension, potentially reduce neuronal excitability.While there remains some controversy regarding theeffects of mitochondrial KATP channels on ROS pro-duction (Krenz et al., 2002; Xu et al., 2004), publishedreports may reflect tissue-specific and/or methodolog-i rtedta tmP
etst ta theK s-s per-f ranee lsm eenm ilitys smo-l ensi-t orsh theo Kc thatt (V
ATP
nd the two pore domain (K2P) potassium channels
When one considers the pivotal role that mitochria play in energy production, and asks how changnergy metabolism might translate to alterations inonal membrane excitability, the involvement of ATensitive potassium (KATP) channels must be strongonsidered. KATP channels, first described in pancreeta cells, regulate insulin release by modulatingembrane potential. These channels are inhibiteigh ATP/ADP ratios, and activated (resulting in hypolarization) when intracellular ATP levels are low
KATP channels have been identified in neuronell as glia in different brain areas, including hocampus, hypothalamus, substantia nigra and dagus nerve. The highest expression of KATP channelss in the substantia nigra pars reticulata (SNPR) whn addition to other well-known functions, is believo be a subcortical modulator of seizure propagaIadarola and Gale, 1982; Depaulis et al., 1994). Whilexperimental data linking the KD to KATP channels iot yet forthcoming, preliminary observations sugg
cal differences. Interestingly, ROS has been repoo activate mitochondrial KATP channels (Avshalumovnd Rice, 2003; Lebuffe et al., 2003), an action thaay contribute to ischemic preconditioning (Gross andeart, 2003).In considering the multitude of molecular targ
hat are likely to be affected by the KD,Vamecq el. (2005)have hypothesized that an alternative toATP channel is the K2P (i.e., two pore domain) potaium channel. K2P channels represent a diverse suamily of channels that can regulate baseline membxcitability (Franks and Honore, 2004). These channeay represent a more likely physiological link betwetabolic activity and plasma membrane excitab
ince they can be modulated by changes in pH, oality, temperature, mechanical pressure, and are sively activated by certain PUFAs—all of these factave been explored to one extent or another. Onther hand, while the link between PUFAs and2Phannels is tantalizing, there is no evidence to datehe KD induces stable changes in pH or osmolalityDeivo et al., 1978; Al-Mudallal et al., 1996).

158 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
6.5. Conclusions
Within the last decade, several putative moleculartargets and novel insights have emerged. Not surpris-ingly, given all of the metabolic, physiological andhormonal changes induced by the KD, there is a mul-tiplicity of relevant mediators involved and it is likelythat no single mechanism, however well substantiated,will explain all of the diet’s clinical effects. The com-plex mechanisms that are involved in seizure genesisand epileptogenicity, as well as the diverse treatmentapproaches taken clinically, strongly suggest that suc-cessful approaches, including the KD are likely basedon fundamental mechanisms that are multiple, paralleland possibly synergistic.
7. Clinical evidence of efficacy: an overviewfrom major trials
E. Kossoff
The John M. Freeman Pediatric Epilepsy Center, JohnsHopkins Medical Institutions, Baltimore, MD, USA
7.1. Introduction
Despite 20 AEDs on the market, many of which haveb e ofp dlyr nglyuf ska gerdW ane ticep ardr ized,c
lueS d toaa rei nsH1 e( d,t ateda hat
“it is unlikely that this degree of benefit can result froma placebo response and/or spontaneous remission”.In all studies combined, 16% were seizure-free, 32%greater than 90% improved, and 56% with a 50% orhigher response.
Three years later, with more data available, theCochrane Library performed their own review of the lit-erature from 1966 to 2003 (Levy and Cooper, 2003). Inthis review, utilizing more stringent criteria, they wereless convinced about the diet’s efficacy. Their statedobjective was to find randomized, controlled studies toprove the diet’s efficacy. None were found. They con-cluded “there is no reliable evidence from randomizedcontrolled trials to support the use of KDs for peoplewith epilepsy”. However, the reviewers still classifiedthe diet as a “possible option” because “a small num-ber of observational studies lend some support for abeneficial effect.”
With this confusing data, how does the diet fit into aphysician’s treatment algorithm? In 2001,Epilepsy andBehavior published “The Expert Consensus Guide-lines”, in which 100 adult and pediatric epileptologistsreviewed clinical case scenarios and provided theirtreatment options in order of preference (Karceski,2001). Among this group, the diet did not fare well.For idiopathic generalized epilepsy, the diet ranked in1 oft , buto er-a ), thed
7
re-s ti-p noxG syn-d neo eter-m in1 ryt gly,1 0%i dietb toinat nly
een introduced in the past decade, the incidencharmacological intractability has not been markeeduced. Partly as a result of this, the KD is increasised in every continent (Kossoff et al., 2005). Many
amilies of children with intractable epilepsy now about the KD at clinic visits, and the diet is no loniscouraged by physician (Hemingway et al., 2001b).hat is, however, the evidence for its efficacy? In
ra in medicine of increasing guidelines and pracarameters, many neurologists want straightforwecommendations based on evidence from randomontrolled trials.
In 2000, an article written for the Blue Cross Bhield insurance company in the U.S. attemptenalyze all studies available at the time (Lefevrend Aronson, 2000). In this article, 11 studies we
dentified; 9 of which were retrospective from Johopkins. Only two were prospective (Vining et al.,998; Freeman et al., 1998), one was multicentrVining et al., 1998). Although none were controllehe authors of this review felt that the diet demonstr“significant reduction in seizure frequency” and t
5th position in a list of possible therapies; 74%he physicians considered it an appropriate choicenly as third-line therapy. Even in symptomatic genlized epilepsies (e.g., Lennox Gastaut syndromeiet ranked no higher than 9th to 11th place.
.2. Evidence from retrospective studies
Information on studies with over 20 patients is pented inTable 1. All studies generally describe mulle and varied seizure types, most commonly Lenastaut syndrome and other generalized epilepsyromes typically with difficult-to-control seizures. Of the earliest retrospective studies was by Dr. Pan from the Mayo Clinic in Rochester, Minnesota925 (Peterman, 1925). He reported on a “new dieta
reatment” in 17 children aged 1–15 years. Amazin0 (60%) were seizure-free, and 4 (23%) were >9
mproved. Relatively few papers followed and theecame less popular with the introduction of phenynd other AEDs.Hopkins and Lynch (1970)reported
he treatment of 34 patients with a 3:1 ratio KD. O
J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 159
three (8.8%) were seizure-free, but 71% had either“much” or “moderate” improvement.
In 1986, the modern era of KD studies began withSill’s report (Sills et al., 1986) of 50 patients treatedwith an MCT diet. Of these, 44% had a >50% improve-ment in seizures, and 8 (16%) were seizure-free. Inter-estingly, 86% of the children with absence epilepsyand 50% of those with myoclonic–astatic epilepsy hada >50% improvement.
Kinsman et al. (1992)reviewed 58 children fromJohns Hopkins Hospital; 67% had a >50% improve-ment, with 29% having a “near complete” response.Almost two thirds were able to reduce medications andmore than one-third were reportedly more alert andinteractive. Due to the interest elicited by this publi-cation, many other studies at Johns Hopkins Hospital,including four important prospective studies in the pastdecade, were subsequently completed (see below).
Two studies in infants have been recently published.One reported that 54% of 32 infants had a >50%response (19% seizure-free); in this population, thediet was remarkably well tolerated and ketosis wasattained easily (Nordli et al., 2001). A retrospectivereview of 23 children specifically with intractableinfantile spasms found that 6 (46%) of the 13 remain-ing on the diet at 12 months had a >90% spasmr ara erl
pi-t rtedo facedmt r ana oler-a cals
thel uingt .,1 01;C .,2
7
ta of
three diets including the classic, MCT, and a modifi-cation, 81% showed a >50% response (Table 1). Theclassic diet had the highest efficacy and was the besttolerated. In 1998, two prospective studies from JohnsHopkins were published. The first (Vining et al., 1998)was a multicentre (seven hospitals) study of 51 chil-dren aged 1–8 years with intractable epilepsy, who hada mean of 230 seizures per month and had failed anaverage of seven AEDs. At 6 months, 53% had a >50%response, 6 (12%) were seizure-free and 73% remainedon the diet. The second prospective study from JohnsHopkins was a single-centre study of 150 consecutivechildren aged 1–16 years with more than two seizuresper week that had failed at least two AEDs and werefollowed-up for 1 year (Freeman et al., 1998). At base-line, children had a mean of 410 seizures per month anda history of exposure to 6.2 AEDs. In this group, 71%were able to remain on the diet, and 51% had a >50%improvement, 32% with a >90% reduction at 6 months.In general, those who discontinued the diet before 1year did so due to inefficacy rather than restrictiveness.No specific seizure type preferentially improved, butage older than 8 years at diet initiation was slightlyless likely to show an improvement. In comparing out-come on the diet to many new add-on medications,the authors considered the diet as potentially moree
ate( edi 0%ra 20c ni-ta ada tra-d ithn nes.I osisa ortedf nda der-w
tud-iO un-t ofp
eduction (Kossoff et al., 2002a). Age less than 1 yend trials of two or fewer AEDs correlated with high
ikelihood of improvement.A retrospective study from Johns Hopkins Hos
al and the University of Texas at Houston repon 45 adolescents aged 12–19 years who hadany years of epilepsy (Mady et al., 2003). Despite
he concerns that the diet might be too restrictive fodolescent population, seizure improvement and tbility were remarkably similar to those in more typichool-age children.
The KD’s use worldwide has blossomed sinceate 1990s, with many retrospective studies contino report high response rates (Table 1) (Hassan et al999; Vaisleib et al., 2004; Kankirawatana et al., 20oppola et al., 2002; Franc¸ois et al., 2003; Kim et al004a; Klepper et al., 2004).
.3. Prospective uncontrolled studies
In the first modern prospective study,Schwartz el. (1989)reported that, of 63 patients given one
ffective.A small study on a modified low-carbohydr
Atkins) diet in six children and adults publishn 2003 reported that four patients had a >5esponse, correlating with level of ketosis (Kossoff etl., 2003). A follow-up prospective study assessedhildren with intractable epilepsy for 6 months, iially with 10 g of carbohydrate per day (Kossoff etl., in press). Nearly two thirds of the patients hsignificant seizure reduction, a similar to the
itional KD. The diet was very well tolerated wo significant weight loss nor cases of kidney sto
nterestingly, the presence of large urinary ketppeared to be less important than commonly rep
or the KD. Further studies in both children adults with this novel ketogenic therapy are unay.A summary of outcome data in prospective s
es including at least 20 patients is given inTable 3.verall, results show some disparity between co
ries, with 6-month efficacy rates ranging from 27%atients with a 50% seizure reduction in Italy (Coppola

160 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
Table 3A summary of retrospective and prospective efficacy studies of the ketogenic diet including over 20 patients and published since 1970 (notincluding abstract presentations)
Reference No. of patients Age range (years) >90% improvement rateat 6 months
>50% improvement rateat 6 months
Hopkins and Lynch (1970) 34 1–13 71Sills et al. (1986) 50 2–15 24 44Schwartz et al. (1989)a 59 <5–54 41 81Kinsman et al. (1992) 58 0.2–7 29 67Vining et al. (1998)a 51 1–9 29 53Freeman et al. (1998)a 150 1–16 32 51Hassan et al. (1999) 52 2–9 67Kankirawatana et al. (2001)a 35 0.2–13 75Nordli et al. (2001) 32 0.5–1.5 55Kossoff et al. (2002a) 23 0.5–2 39 72Coppola et al. (2002)a 56 1–23 27Francois et al. (2003) 29 0.3–12.5 41Mady et al. (2003) 45 12–19 29 50Kim et al. (2004a) 124 2–7 53 (3 months) 76 (3 months)Klepper et al. (2004) 111 0.1–18 17 31Vaisleib et al. (2004) 54 2–14 65
a Prospective studies.
et al., 2002) to 75% of patients with a >90% reductionin Thailand (Kankirawatana et al., 2001).
7.4. Prospective randomized studies
Four randomized studies are being completed in theUSA and UK. In a study from Johns Hopkins, 20 chil-dren with intractable Lennox Gastaut syndrome wereadmitted, fasted, slowly advanced onto the KD over3 days and randomized to either receive an additionaldaily solution containing saccharin or glucose. After 1week, they were crossed to the opposite arm before dis-charged to home. The study, currently being analyzed,was the first to prove that the KD could be studied in adouble-blinded, randomized, placebo-controlled man-ner. Dr. Helen Cross at Great Ormond Street Hospital inLondon is completing a prospective randomized studycomparing the classical KD with an MCT oil diet, witha control period of 4–16 weeks incorporated for eachindividual patient. Dr. Christina Bergqvist at the Chil-dren’s Hospital of Philadelphia is currently analyzinga third randomized study of the value of a fasting com-pared to a gradual initiation of the diet. A fourth studyby our group is examining the Atkins diet in children,randomized to either 10 or 20 g of carbohydrate perday, with a crossover period after 3 months for eachp
7.5. Conclusions
The efficacy of the KD was initially assessed mostlyin small, single-centre, retrospective studies. In recentyears, reports of the diet’s efficacy worldwide have con-tinued to show that approximately half of patients willhave half their seizures, and about one-third in totalwill have one-tenth their baseline number of seizures.Prospective studies have confirmed these data, and fourrandomized studies are in the process of completion.Although clearly a need exists for further prospectivestudies, the quality of evidence for the diet’s efficacy isimproving over time.
8. Seizures type and epilepsy syndrome aspredictors of response
P. Veggiotti, R. Epifanio, F. Longaretti, G. Lanzi
Department of Child Neurology and Psychiatry, Insti-tute of Neurology, IRCCS C. Mondino Foundation,University of Pavia, Pavia, Italy
8.1. Introduction
Few studies have investigated clinical outcome afters es.
atient. tarting the KD in well-defined epileptic syndrom
J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 161
Moreover, there are no randomized trials comparing thediet with placebo or with AEDs, and most of the largescale studies conducted to date only reported resultsafter short term treatment. For these reasons, definingthe comparative efficacy of the KD in relation to spe-cific syndromes or seizure types is no easy task. Inthis report, this aspect will be addressed by reviewingbriefly data from the literature and by presenting ourpersonal experience.
8.2. Literature data
With respect to response to the diet in relation toseizures type, several studies have reported particu-larly favourable outcomes in children with myoclonicseizures (Wheless and Sankar, 2003); these data, how-ever, refer to observations in large series of patientswith drug resistant epilepsies, and there are no pub-lished studies that document the comparative efficacyof the diet in different types of myoclonic epilepsies.A study byMaydell et al. (2001)did not find any sig-nificant difference in the diet’s efficacy when patientswith partial seizures were compared with those withgeneralized seizures.
Studies relating response to specific epilepsy syn-dromes are even fewer. Efficacy of the KD in LennoxG ;M i-t eses as fter5 he1 nics
.( insti dif-f Ds.H lo-ge ntsw ibil-i ralb e ofc tor ofa
t vere
myoclonic epilepsy of infancy (Dravet syndrome). Inthis report, 20 patients meeting the diagnostic criteriafor the syndrome were enrolled; 10 of the 13 childrenwho remained on the diet for a duration of follow-upof 1–4 years had a significant reduction of seizures.These results are of particular interest because of thehomogeneity of the cohort and the long-term follow-up.
8.3. Our experience
We took part in an Italian multicentre studythat assessed 56 children, adolescents and youngadults with refractory epilepsy; and we also reportedseparately our personal experience in a total of 36patients (including 16 who had taken part in themulticentre study) (Coppola et al., 2002; Bertoli etal., 2005). In these studies, which included patientswith partial and generalized symptomatic epilep-sies, myoclonic–astatic epilepsy, Lennox Gastautsyndrome and others epileptic encephalopaties, wedid not identify a statistically significant relationshipbetween outcomes on the diet and either seizure typeor epilepsy syndrome. Subsequent evaluation of ourexperience, however, have led us to hypothesize agood response of the diet can be especially observed inp they tients( ffusem at 9m asei ta mayr sisf verem tiont somer re ise turet diesiC et nsc eirc thats ainst psyc ents
astaut syndrome has been reported (Wheless, 2004ckay et al., 2005), but diagnostic electro-clinical cr
eria do not appear to have been always fulfilled in thtudies.Freeman and Vining (1999)have describedignificant reduction in seizure frequency (>50%) adays of the introduction of the diet in all of t
7 Lennox Gastaut patients with atonic or myocloeizures included in their study.
Recently,Nordli et al. (2001)and Kossoff et al2002a)reported a beneficial effect of the diet aganfantile spasms in patients with West syndrome oferent etiologies unresponsive to conventional AEowever, efficacy rates in relation to specific etioies, or specific EEG patterns, were not specified.Thant al. (2005)also reported favourable results in patieith infantile spasms, and did not exclude the poss
ty of a good outcome even in patients with structurain abnormalities. In the latter report, the presencomplex partial seizures was regarded as a predicn unfavourable response to the KD.
A recent study byCaraballo et al. (2005)reported onhe effectiveness of the KD in the treatment of se
atients with diffuse migrational disorders. Duringears between 1994 and 2004 we treated seven pamean age 8.2 years, range 2.8–16.1) showing diigrational disorders; four of them experienced,onths since the introduction of the diet, a decre
n seizure frequency between 50% and 90%.Than el. (2005)have also suggested that these patientsespond particularly well to the diet. A biological baor putatively better responses in patients with seigrational disorders may be found in the observa
hat the cerebral structure of these patients bearsesemblance to the foetal brain’s structure. Thevidence that, as in suckling rats, the more immahe cerebral cortex is, the more it uses ketone bonstead of glucose as an energetic substrate (Crino andhou, 2000; Morris, 2005); accordingly, it is possibl
hat patients with diffuse cortical malformatioould utilize more efficiently ketone bodies in therebral metabolism. While it is acknowledgedurgical intervention, whenever possible, remhe treatment of choice in drug refractory epileaused by focal cortical dysplasia, some pati

162 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
may benefit from the diet, at least before surgery isapplied.
It has been suggested that patients with Laforabody disease may also respond favourably to the diet(Minassian, 2001). Given the pathophysiology of thisdisorder, it is reasonable to hypothesize that the diet,by promoting the brain utilization of ketones insteadof glucose, might reduce glycogen synthesis and pos-sibly decrease polyglucosan accumulation and slowdown the progression of the disease. In a pilot study(Cardinali et al, submitted for publication) we assessedthe effects of the diet in five patients with Laforabody disease (average age at our first observation:13.2± 3.2 years), in order to determine the feasibilityof its long-term term use in adolescents with this condi-tion, and its potential impact on clinical outcome. Thediet was well tolerated in all five patients for a periodof 28.4± 8.8 months, but the illness showed a progres-sive deterioration, with worsening of the myoclonus,appearance of new seizure types, and increased fre-quency of generalized tonic–clonic seizures. Moreover,four of the five patients showed a significant declinein cognitive functions, with special reference to mem-ory, long lasting attention and performance abilities.These findings seem to argue against a protective roleof the diet on the progression of the disorder, but fur-t sionsc rtedo dis-e ronald bser-v ases ouldb develo sible( ofe llyd asep
8
andl oft ec-t s ofp aren racti-
cal implications for the selection of the best candidatesfor treatment.
9. Is there a role for the ketogenic diet beyondchildhood?
E. Kossoff
John M. Freeman Pediatric Epilepsy Center, JohnsHopkins Medical Institutions, Baltimore, MD, USA
In one of the earliest publications (Peterman, 1924)reporting significant benefits from ketosis, patientstreated with the diet ranged from 3.5 to 35 years,although no information was provided as to the influ-ence of age on outcome. In subsequent years, the dietwas increasingly used for adults; the largest seriesreported to date, published in 1930 (Barborka, 1930)included 100 patients aged 16–51 years. Only 27 wereaged 30 or above, and 38 were under age 20 andcould be more appropriately classified as adolescents.Ketosis typically occurred, but interestingly severalpatients had improved seizure control without persis-tent ketosis. Overall, 56% had a >50% response and12% were seizure-free, outcomes remarkably similarto those reported for children in the next 80 years. Inter-estingly, the authors commented that “there seems tob rdedt unga yt -t eralp e 56w ecentsy allyf ringt l.( e oft
D in1 izuref Jef-fw ted4 , 6( 7%)h s ofc eve
her studies are necessary before definite concluan be drawn. Moreover, our patients were stan the diet years after the clinical onset of thease, when Lafora bodies accumulation and neuegeneration had already become established. Oations in a knockout mouse model of the diseuggest that whatever treatment is applied, it she started as early as possible, because alreadyped pathological changes do not appear to reverGanesh et al., 2002). This raises the possibilityxploring the potential value of the KD in geneticaiagnosed, pre-symptomatic siblings of Lafora diseatients.
.4. Conclusions
There is inadequate information on how short-ong-term outcome on the KD relates to the typehe epileptic disorder and/or ictal semiology. Prospive studies with large and homogeneous cohortatients with well-defined electro-clinical featureseeded to address this issue, which has obvious p
-
e no question but that the patient who can be affohe best opportunity for treatment is the child or yodult. . . whereas older patients. . . are the least likel
o be benefited” (Barborka, 1930). Although not sysematically monitored, cholesterol increased in sevatients; amenorrhea occurred in 12 (21%) of thomen treated, an occurrence also seen in a rtudy of adolescents (Mady et al., 2003). For nearly 70ears, thereafter, the KD was used only sporadicor adults in some centres. In a 1989 study compahe MCT oil diet to the classical KD,Schwartz et a1989)described 4 adults out of 63 patients. Nonhe 4 adults had any significant improvement.
In 1999, a retrospective assessment of the K1 adults (9 women, age 19–45 years, baseline se
requency 2–30 per month) was reported from theerson centre in Philadelphia (Sirven et al., 1999). Allere treated with a typical calorie and fluid restric:1 ratio diet after a 24–72 h fast. At 8 months55%) had a >50% seizure reduction and 3 (2ad a >90% improvement, similar to most studiehildren. Only two patients were unable to achi

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 163
and maintain ketosis; all patients reported constipa-tion and all women described menstrual irregularities.Cholesterol increased over 6 months from a baseline of208 to 291 mg/dl and triglycerides were only slightlyincreased from 190 to 203 mg/dl. A follow-up studyfrom the same group with 15 additional patients (total26) was presented at the 2003 meeting of the Ameri-can Epilepsy Society in poster form (Nei et al., 2003).Similarly to the previous study, 54% had a >50%response, and the authors were able to differentiateoutcome based on seizure type. They indicated that the12 patients with symptomatic generalized epilepsy hadthe best outcome, with 73% having a >50% response,compared with only 27% of the 11 adults with partialepilepsy. Improvement, when it occurred, tended to bein the initial 2 weeks of the diet. Diet duration wasrelatively short, only 7 months on average. Only 11%continued the KD for 2 years, and all of these patientshad symptomatic generalized epilepsy. Weight loss wasalso described, with a mean decrease of 6.7 kg. Furtherinformation about these two studies are detailed in atextbook chapter on adults and the KD (Sperling andNei, 2004).
In 2001, a retrospective study of 45 highly moti-vated adolescents with intractable epilepsy (age 12–19years) was reported (Mady et al., 2003). Six monthsa iet,w and8 ilart1 es ilart2 tob thed ndm ostc
fiedA orc reeo age( da tely,w thed t, a4 cess.T or 3
months but had no measurable seizure reduction. Theolder patient was unable to create ketones because hewas given carbohydrates in his chronic care facility, anddiscontinued the diet after 8 months. Encouraged by theabove results, we have started a study of adults aged 18and over using a modified Atkins diet; carbohydratesare limited to initially 15 g per day and medicationsare left unchanged for the first month. Daily multivi-tamin and calcium supplementation is provided, andfrequent serum and urine laboratory monitoring is per-formed. In approximately 10 patients to date, resultsare mixed and continue to be correlated with level ofketosis.
In conclusion, studies of the use of the KD for ado-lescents and adults are still in their “infancy” despiteover 80 years of clinical use for children. Efficacyappears to be similar to published studies of children.Further prospective studies, including perhaps a lessrestrictive modified Atkins diet, are warranted. Sideeffects such as weight loss, dysmenorrhea, constipa-tion, and dyslipidemia will need monitoring in anyfuture studies.
10. Discussion summary—implementationprocedures and efficacy data
E
IaP
Q cine,t vesm olledt didn izuret ernsb
A ctives KDm ma-r m-i vend osev on-i bep im-
fter diet initiation, 28/45 (62%) remained on the dith 6/28 (21%) having 50–90% seizure reduction/28 (29%) having >90%. These results were sim
o those observed in younger children (Vining et al.,998; Freeman et al., 1998). Patients with multipleizure types (generalized epilepsy) did best, simo the adult study from the Jefferson centre (Nei et al.,003). The restrictions of the diet did not appeare a major problem, with only 22% discontinuingiet primarily for this reason. Weight loss (60%) aenstrual dysfunction (45% of females) were the m
ommon side effects.A small case series of the benefits of a modi
tkins diet (providing more protein and no fluidalorie restriction) was reported in 2003, with thut of six patients being older than 18 years ofKossoff et al., 2003). An 18-year-old female ha
90% improvement in seizures almost immediaith large urinary ketosis, and was maintained oniet for 20 months without side effects. In contras2-year-old man and 52-year-old man had less suche younger man maintained moderate ketosis f
. Perucca
nstitute of Neurology, IRCCS C. Mondino Foundation,nd Clinical Pharmacology Unit, University of Pavia,avia, Italy
. By current standards of evidence-based medihe quality of the studies conducted with the KD leauch to be desired. We have no adequately contr
rials that demonstrate efficacy, and most reportsot characterize adequately patients in terms of se
ype and epilepsy syndrome. How can these conce addressed?
. Everyone acknowledged that we need prospetudies of better quality. While the nature of theakes blinding difficult, recent developments sum
ized in Dr. Kossoff’s presentation show that randozed studies are now being initiated, and that eouble-blind protocols (e.g., by administering glucersus saccharin in addition to the diet, with the mtoring of ketosis by an external investigator) canractically and ethically feasible, at least over l

164 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
ited assessment periods. While limitations of currentevidence are acknowledged, Dr. Freeman and otherpresenters remarked that the time course and mag-nitude of improvement is hardly compatible with aplacebo response or with the natural history of theseizure disorder. It is hard to question the diet’s effi-cacy when children with a long standing history offrequent daily seizures improve dramatically duringthe fasting period and remain persistently improvedfor months and years thereafter. Outcome data in termsof sustained seizure freedom observed with the KDappear to be greater than those reported for “histor-ical controls” included in AED trials. Nevertheless,it is a fact that overall the quality of the efficacydata is not satisfactory, and that it is important infuture studies to use prospective controlled designs,and to include patients with better defined epilepsysyndromes.
Q. There seems to be controversy about what imple-mentation procedure is best. We have been presentedwith different initiation protocols, controversial data onthe need for hospital admission, even different types ofdiets.
A. We do not have adequate data to answer these issues.Again, randomized comparative studies are needed tod ndo uchk r thel pe-c pitala nta-g g off bet-t itiona , fore edm thep tkinsd dieti TheA ept-a d itm icald uret d asa atp
Q. Dr. Tagliabue described a rather comprehensive setof investigations to monitor the effects of the diet.Should these be all part of our routine monitoring pro-cedures?
A. Dr. Tagliabue clarified that some of the investiga-tions, for example some anthropometric and metabolicmeasurements, are conducted in her centre as part of aresearch protocol, and should not be regarded as nec-essary in a routine setting. Some tests, such as bonemass determinations and abdominal ultrasound, mayonly be required on a case-by-case basis, for examplewhen nutritional status and liver enzymes justify con-cerns with bone mineralization loss, or when the findingof blood in urine raises suspicions about possible renalstones. It appeared from the discussion that laboratorymonitoring at some European centres tends to be moreintensive than in North America. In any case, there wasagreement that the need for testing for nutritional defi-ciencies can be minimized by providing patients withappropriate supplementation of vitamins and minerals.
Q. How can we best monitor ketosis, by determinationsin blood or by simply checking urine ketones?
A. Dr. Kossoff commented that one study did suggestan improved outcome with monitoring blood ketones( att oodt withs hatd opti-m
Q wsa esa
A arelya loodl nts,e ther esti-g ftent mil-i
Q thed oesn forew
etermine the value of fasting, fluid restriction, ather initiation procedures, to determine how metosis is needed for seizure control, and whetheevel of ketosis should to be adjusted in relation to sific patients’ characteristics. On the issue of hosdmission, most participants considered it advaeous to ensure adequate involvement and trainin
amily members. Hospital admission also ensureser adjustment of dietary needs, and prompt recognnd treatment of potential early adverse effectsxample in children with a previously unrecognizetabolic defect. There was some discussion onros and cons of alternative diets, such as the Aiet. The prevailing view was that the classical
s the best documented in terms of efficacy data.tkins diet has some attractiveness in terms of accbility, particularly in adolescents and adults, anight be offered when compliance with the classiet is anticipated to be problematic. However, fail
o respond to the Atkins diet should not be regarden indication that the classical diet will not work in thatient.
Gilbert et al., 2000). Overall, however, he felt thhere is still insufficient evidence to conclude that blesting ensures an improved outcome comparedimply monitoring urinary ketones. He also felt tevices for monitoring blood ketones are less thanal at the current state of technology.
. What do we do when blood biochemistry shobnormalities, particularly high levels of triglyceridnd cholesterol?
. There was consensus that dyslipidemias are rcause for discontinuing the diet. Changes in b
ipids can usually be managed by dietary adjustme.g. by altering the caloric intake and/or modifyingatio of unsaturated to saturated fat. On further invation, some cases of problematic dyslipidemias o
urn out to reflect co-morbid conditions, such as faal hypertriglyceridemia.
. If a child does well on the KD, how long shouldiet be continued? On the other hand, if the diet dot appear to work, how long should we go on bee give it up?

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 165
A. There was agreement that duration of treatmentshould be determined on a case-by-case basis. InGLUT1 deficiency syndrome and in pyruvate dehy-drogenase (E1) deficiency syndrome, the diet usuallyneeds to be continued for several years. In epilep-sies that responded well to the KD, discontinuationof the diet may be considered after about 2 years. Innon-responders, a trial of about 3 months will usu-ally be sufficient to conclude that diet is not going tohelp.
11. Adverse effects and contraindications
J. Campistol
Department of Neuropediatrics, Hospital Sant Joan deDeu, Barcelona University, Barcelona, Spain
11.1. Introduction
Before starting the KD, clinicians need to be awareof the type of epilepsy, the characteristics of thepatients, the type of potential adverse effects, and thediet’s medical contraindications (Kossoff, 2004; Kanget al., 2005).
1
nots enti a;C ri ntalr
TE
G
DSCHPB ,
lic
Table 5Long-term or late-onset adverse effects of the ketogenic diet
Growth retardationHepatic failureConstipationExacerbation of gastro-esophageal refluxMineral deficienciesVitamin deficienciesUrolithiasisOsteopeniaCardiomyopathyProlonged QT intervalOptic neuropathyBasal ganglia injuryAnemiaBiochemical disturbances (hypocarnitinemia, dyslipidemias,
elevated very long chain fatty acids)
Most of the early onset adverse effects of the diet(Table 4) are transient and can be carefully managedwith conservative strategies. These include gastroin-testinal disturbances such as nausea, loss of appetite,refusal to drink, and vomiting, usually associated withgastritis and fat intolerance. Another disturbance isconstipation that can be caused by a decrease in inges-tion of food and fibers; laxatives or enemas can suc-cessfully control it.
Dehydration is one of the most common com-plications that occur early after initiation of thediet (Wheless, 2001; Kang et al., 2004). It can beprevented by avoiding a fasting period and/or byencouraging oral or intravenous intake of fluidswithout dextrose (Wheless, 2001). Potentially seriouscomplications include sepsis, cardiomyopathy, lipoidaspiration pneumonia, hepatitis and acute pancreatitis.Sometimes these complications may be related toconcomitant use of some AEDs, especially valproicacid (VPA). Fatal fulminating sepsis in sporadic caseshas been attributed to pre-existing metabolic disease(Kang et al., 2004). Overall, serious complications maylead to discontinuation of the diet in 6–12% of patients.
The list of early onset biochemical disturbancescomprises hypoglycemia, hypertriglyceridemia (whichmay lead to pancreatitis), hypercholesterolemia, tran-s ases( ne-m bolica g eta ane
1.2. Adverse effects
Most side effects of the diet are mild and doignificantly affect the acceptability of the treatmn the majority of patients (Hemingway et al., 2001oppola et al., 2002). In general, tolerability is poore
n young patients with refractory epilepsy and meetardation than in other populations.
able 4arly onset adverse effects of the ketogenic diet
astrointestinal effects (nausea, vomiting, loss of appetite,constipation)
ehydrationepsisardiomyopathyepatitisancreatitisiochemical disturbances (hypoglycemia, hypertriglyceridemiahyperuricemia, hypertransaminemia, hypercholesterolemia,hypoproteinemia, hypomagnesemia, hyponatremia, metaboacidosis)
ient hyperuricemia, increased liver transaminespecially in patients receiving VPA), hypoproteiia, hypomagnesemia, hyponatremia and metacidosis (Galvan et al., 2001; Wheless, 2001; Kanl., 2004; Coppola et al., 2002; Vining, 1999; Freemt al., 2000).

166 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
Long-term or late-onset adverse effects (Table 5)include growth retardation (mainly related to proteindeficiency), hepatic failure, vitamin and mineral defi-ciencies, immune disturbances (impaired neutrophilefunction, related to imbalanced diet and protein restric-tion) and cardiomiopathy, which may also be seen inthe early phases of treatment (Vining, 1999; Coppolaet al., 2002; Wheless, 2001; Galvan et al., 2001; Furthet al., 2000; Vining et al., 2002). Another late-onsetcomplication is nephrolithiasis, which may result fromchronic acidosis, dehydration, and fat malabsorption,and may be more common in patients receiving car-bonic anhydrase inhibitors such as topiramate (TPM)and/or zonisamide (ZNS). Osteopenia may be causedby nutritional deficiencies, reduced sunlight exposure,immobilisation and underlying AEDs.
Late-onset biochemical disturbances include sec-ondary hypocarnitinemia, iron deficiency anemia, vita-min and mineral deficiencies, increased uric acidproduction, low serum bicarbonate levels, persistenthyponatremia, sustained metabolic acidosis, and dys-lipidemias (Vining, 1999; Kossoff, 2004; Furth et al.,2000).
Physicians should be aware of the above compli-cations, so that they can be carefully monitored andsuccessfully prevented and treated as appropriate. Ther ullyw hichm ilityo en-t za-t asedh ge
1
rali andk driald ne
ofm dur-i ne mw itined ns-
ferase I and II and carnitine translocase) or secondary.Fatty acid defects are absolute contraindications tothe diet, and this is especially true for medium chainacyl-CoA dehydrogenase deficiency (MCAD). Otherdefects in fat metabolism that can exacerbate ketotichypoglycemia are long-chain acyl-CoA dehydrogenasedeficiency (LCHAD), short chain acyl-CoA dehydro-genase deficiency (SCHAD) and mitochondrial andketone metabolism defects (Wheless, 2001; Kang et al.,2005). The KD should never be used in children withpyruvate carboxylase deficiency, in whom its adminis-tration may have fatal consequences.
The diagnosis of inborn errors of metabolism isoften difficult. Patients can present with refractoryepilepsy and non-specific symptoms that can beattributed to seizures or drugs. In some of these cases,the epilepsy may be secondary to inborn errors ofmetabolism, a possibility which should be consideredalways and particularly in children with associateddevelopmental delay of unknown aetiology, hypoto-nia, exercise intolerance, cyclic vomiting, fatigability,hepatomegaly, cardiomyopathy, pigmentary retinitis,hypoacusia, metabolic acidosis, hypoglycemia orunexpected ketonuria. In other cases of intractableepilepsy, the MRI findings, funduscopy, and nerveconduction velocity may give useful clues to diagno-s cingt cale rinea ty ofa nedb eta
rorso redm c-t s ani oss-i brale ya i-t yru-v inased duet tich
ichm revi-
isk of side effects, in any case, should be carefeighed against the potential benefits of the diet, way include better seizure control and the possibf reducing AEDs, which may result in improved att
ion and vigilance, improved behaviour, normaliion of the circadian wake–sleep cycle, and decreyperkinesia and impulsivity (Nordli et al., 2001; Kant al., 2005; Coppola et al., 2002).
1.3. Contraindications
Medical contraindications of the KD include sevenborn errors of metabolism such as defects in fatetone metabolism, porphyria and some mitochonisorders (Wheless, 2001; Franc¸ois et al., 2003; Galvat al., 2001).
If a child has an unrecognized inborn erroretabolism, serious complications may occur
ng the initial fasting period (Wheless, 2001; Galvat al., 2001). Relevant inborn errors of metabolishere the diet can be hazardous include carneficiencies, either primary (carnitine palmitoyltra
is. In such cases, and especially before introduhe KD, it is essential to conduct a careful clinivaluation and a biochemical screening (plasma, und, in some cases, CSF) to exclude the possibilin inborn error of metabolism which can be worsey the diet (Galvan et al., 2001; Moreno-Villaresl., 2001; Kossoff, 2004).
On the other hand, in some other inborn erf metabolism or mitochondriopathies where alteitochondrial function leads to glycolysis dysfun
ion, the KD may be beneficial because it providemportant alternative energy source capable of crng the blood–brain barrier and maintaining cerenergy metabolism (Cuellar and Molinero, 2003; Levnd Cooper, 2003; Kang et al., 2004). These cond
ions include glucose transport defects, some pate dehydrogenase deficiencies, phosphofructokeficiency and some mithocondrial cytopathies
o Complex I deficiency presenting with hypoketoypoglycemia.
Some patients have immunologic defects whay worsen with the diet, and in these cases p
J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 167
ous screening for immunologic disorders is required(Kang et al., 2005; Freeman et al., 2000; Franc¸ois etal., 2003; Wheless, 2001).
Particular caution should be exercised when usingthe diet in patients treated with VPA, TPM, ZNSand acetazolamide, even though use of these drugs isnot considered a formal contraindication to the diet(Galvan et al., 2001; Coppola et al., 2002; Kang et al.,2005).
Finally, the diet is not a viable option whenever ade-quate compliance with implementation and monitoringprocedures is not expected.
12. Potential interactions between theketogenic diet and drugs
G. Coppolaa, M. Fiorilloa, E. Ammendolaa, R. DellaCorteb, G. Capanob, A. Pascottob
aClinic of Child Neuropsychiatry, Second University ofNaples, Italy;
bClinic of Paediatrics, Federico II University,Naples, Italy
12.1. Introduction
eiveA therm t ori ofi o bec
1
Dsh s ofi drena thatp oftenb hsV icm ucet iet.T erredu een( ual
patient. Special concerns, however, exist when the KDis combined with AEDs which may produce adverseeffects similar to those associated with the diet.Important examples of such effects include metabolicacidosis, acute pancreatitis, hepatitis, urolithiasis, andcardiomiopathy.
Both the diet and carbonic anhydrase inhibitingAEDs such as topiramate, zonisamide and aceta-zolamide may cause metabolic acidosis, and thereis a higher risk of acidosis when the diet is co-administered with these agents.Takeoka et al. (2002)found a <20% decrease in bicarbonate levels in 9out of 14 TPM-treated children, which was mostlyseen at the time of diet induction. It was suggestedthat bicarbonate levels be monitored carefully whenthe diet is co-administered with TPM and that bicar-bonate supplements be given if the patient becomessymptomatic.
Acute pancreatitis is a rare but often fatal com-plication (Stewart et al., 2001); it can be caused byhypertriglyceridemia (Toskes, 1990), and may be pre-cipitated by valproic acid (Chapman et al., 2001). Ifpancreatitis occurs after initiating the diet, discontinu-ation of the diet and adequate supportive treatment arerequired for a successful recovery.Kang et al. (2004)reported one patient who developed pancreatitis earlyi atedw iet,a ord-i .( attya inp oica ti-c theu theK adA on-t
thedb h ast rtedb rera thec d theK om-
Patients started on the KD often continue to recED treatment, and there is also a possibility of oedications being administered for concomitan
ntercurrent conditions. Therefore, the possibilitynteractions between the diet and drugs needs tonsidered.
2.2. Interactions between the diet and AEDs
Potential interactions between the diet and AEave been little investigated. There are report
ncreased sedation in phenobarbital-treated chilfter starting the diet, and it has been statedhenobarbital dosage may need to be reduced,y about 30%, particularly in children with higerum phenobarbital levels at baseline (Kossoff andining, 2004). No particular underlying antiepileptedication has been found to increase or red
he probability of a favourable response to the dherefore, as far as efficacy is concerned, the prefnderlying AED should be the one which has bor is expected to be) most effective in the individ
n the course of the KD; the patient had been treith valproic acid for 2 years before starting the dnd recovered only after abandoning the diet. Acc
ng to De Vivo et al. (1998)and Ballaban-Gil et al1998), hepatitis can be caused by impairment of fcid oxidation or carnitine deficiency, especiallyatients in whom the diet is combined with valprcid. Kang et al. (2004), however, found no statisally significant association between hepatitis andse of valproic acid in their patients managed withD. All 10 patients with hepatitis from their series hST and ALT values of less than 200 mg/dl and c
inued on the diet.Urolithiasis is another possible complication of
iet (Furth et al., 2000; Kielb et al., 2000), and maye facilitated by carbonic anhydrase inhibitors, suc
opiramate and zonisamide. The four patients repoy Kang et al. (2004)with calcium oxalate stones weeceiving topiramate in addition to the diet.Kossoff etl. (2002b), however, were unable to confirm thatombined use of carbonic anhydrase inhibitors anD increases the risk of kidney stones. They rec

168 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
mended that all patients treated with this combinationbe given increased hydration and that urine alkalin-ization be considered for children with previous renalabnormalities, a family history of urolithiasis, hema-turia, or elevated urine calcium-to-creatinine ratios. Ifrenal stones are found, they suggested discontinuationof the carbonic anhydrase inhibitor.
Cardiomyopathy is a potentially fatal complicationof the diet, which may manifest as bradycardia, dimin-ished QRS voltage and prolonged QT intervals (Best etal., 2000). It has been reported to correlate with sele-nium deficiency (Bergqvist et al., 2003), low serumbicarbonate, elevated serum beta-hydroxybutyrate andcarnitine deficiency (De Vivo et al., 1998; Kang et al.,2004), though some authors did not find evidence ofhypocarnitinemia on the diet (Freeman et al., 2000;Coppola et al., in press). As valproic acid may alsoreduce carnitine levels, there may be a potential foran interaction leading to an increased risk for thisside effect. Most authors, however, agree that carnitinesupplementation should be reserved only to hypocar-nitinemic patients manifesting clinical symptoms suchas generalized weakness, excessive fatigue, decreasedmuscle force or mild cardiomegaly (De Vivo et al.,1998).
To reduce the risk of adverse interactions with thed oadd od-i nda ully;h ben-z ssaryt wsi-neea tiona ietw oft ese5 er-i up,1 dur-i 0%s con-c t ito latet
12.3. The ketogenic diet and general anesthesia
The KD is not incompatible with induction of gen-eral anesthesia. The first experiences with general anes-thesia in patients on the diet dates back toHinton etal. (1982), who described changes in metabolic vari-ables, consisting of mild metabolic acidosis and slightdecreases in pH, in three patients undergoing simpleinhalation anesthesia for minor surgery. More recently,Valencia et al. (2002)reported their experiences in ninechildren aged 1–6 years who underwent general anes-thesia for surgical procedures, some requiring morethan one procedure. At the time of anesthesia, thesechildren were receiving the diet for a mean period of21 months (range 2–60 months) and continued on ituntil the “nothing by mouth” preparation period, whichlasted 12 h. The diet was restarted post-operatively oncase-by-case criteria; initially, children were adminis-tered carbohydrate-free fluids and were then placed onthe diet. In 9 out of 24 procedures, general anesthesialasted≥3 h, and in one patient >11.5 h. Blood glu-cose remained unchanged even during prolonged pro-cedures; this may relate to the experimental observationthat the ketotic state produced by the diet may offer pro-tection from insulin-induced hypoglycemia (Johnsonand Weiner, 1978). There was, however, a trend form longp othp werea tiente ; int e ina itrico ium;i fully.P pli-c my-o o,1c KDt re xi-d eda o ad the1 l.( renf KD.
iet, physicians may consider reducing the AED luring use of the diet. Some authors advice not to m
fy AED therapy for many months until efficacy adverse effects of the diet have been evaluated fowever, early reduction of some AEDs, such asodiazepines and phenobarbitone, may be neceo minimize side effects, such as excessive droess and generalized hypotonia (Vining, 1997). Oth-rs, however, advocate early AED reduction (Freemant al., 1998). Recently,Kossoff et al. (2004)evalu-ted the impact of early versus late AED reducfter initiation of the diet. Six months after the das initiated, AED reduction was possible in 53
he 81 (65%) children included in the study. Of th3 children, 30 (57%) underwent early AED tap
ng in less than a month. In the early taper gro7% experienced a transient seizure increase
ng AED reduction, but all these children had >5eizure decrease after 3 months. The authorsluded that early reduction of AEDs is safe, buffers no specific advantage in comparison to
apering.
etabolic acidosis to develop during the course ofrocedures, where a mild reduction occurred in bH and bicarbonates. In a few cases, patientsdministered bicarbonates intravenously. No paxperienced peri- or post-operative complicationshe five children on TPM, there was an increascidosis. Most commonly used anesthetics were nxide, hysoflurane, sevoflurane, and thiopental sod
n three cases, propofol was administered uneventropofol, however, may by itself cause severe comations such as metabolic acidosis, lipemia, rabdolisis, and myocardial failure (Hanna and Ramund998; Wolf et al., 2001; Baumeister et al., 2004). In onease, propofol was fatal in a 10-year-old boy on thereated for refractory status epilepticus (Baumeistet al., 2004). Propofol may derange fatty acid oation by impairing the entry of long-chain esterificylcarnitine into the mitochondria, thus leading teficiency of the mitochondrial respiratory chain at1-complex level. For this reason,Baumeister et a2004)state that propofol should not be used in childor long lasting anesthesia, especially those on the

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 169
12.4. Interactions with carbohydrate-containingmedications
Some medications contain carbohydrates in theirformulation, potentially altering the ratio of fats to car-bohydrates and proteins in the diet regimen. If this isoverlooked, ketosis can be inhibited with potential lossof seizure control. Care providers and parents should bealerted about the carbohydrates in some medications,including not only glucose content, but also the con-tent of reduced carbohydrates such as glycerin. Listsof carbohydrate content of the most frequently usedmedications have been published (Lebel et al., 2001;McGhee and Katyal, 2001).
13. Clinical trials of ketogenic products:methodological aspects
R. Butler
SHS International, Research and Development Depart-ment, Liverpool, UK
13.1. Introduction
The increasing use of the KD has led to greaterd canb hesep y ande althp is toe el ofe e int ncew eds bee
Fors tion,f ularf nalr highM entr ostmT rod-u tarya tion.
Simply, specialised nutritional products can make thediet easier to achieve for both prescribers and carers,more palatable for the patient and ultimately providemore choice for all.
KetoCal was developed in response to requests fromclinicians and dietitians looking for a nutritionallycomplete tube feed suitable for administration of theKD. The product is presented as a powdered formuladesigned to mimic the classical diet in a ratio of 4:1 andprovides a convenient alternative to mixing a modularketogenic liquid feed. As the product is nutritionallycomplete, the time demand for calculation of the dietis also minimized. When the product was developedin 2001, there was already an emerging consensus onthe efficacy of the KD in refractory epilepsy (Lefevreand Aronson, 2000); therefore, the initial goal for thetrial program was simple—to show that the productwas capable of mimicking the KD in terms of attainingand maintaining ketosis andnot to show that the dietitself is efficacious in attaining seizure control. Datafrom two pilot case series were collected to test productacceptability and efficacy in achieving ketosis beforeinitiating a multicentre trial. Some of the difficultiesin obtaining quality data in KD trials became apparentearly in the trial program, while others became clearonly during the development of the multicentre trial.
1
les-c il-l -t oft orye witht um-b of aK es,t s ofa hilet ool,t itablep reda imest es,t nowa elyt ess,
emand for specialist nutritional products thate administered safely and easily to patients. Troducts must be adequately assessed for safetfficacy, thereby ensuring the confidence of herofessionals and consumers alike. The challengensure that the data collected provides a high levvidence, which can pose an interesting challengrials involving a dietary product. Recent experieith the KetoCal clinical trial program has highlightome of the methodological problems that mayncountered in this area.
The KD may be achieved from regular foods.ome, however, using regular foods is not an opor example those who are tube fed. For others, regoods alone may not provide the specific nutritioequirements or variety needed, for example aCT content or full vitamin, mineral and trace elem
equirements. Further, the KD is inadequate in micronutrients if not supplemented (Liu et al., 2003).here is a real need for specialised nutritional pcts. Whilst such products can help to achieve diedequacy, they also serve another important func
3.2. Patient numbers and patient access
In Europe, the population of children and adoents with active epilepsy is approximately 0.9 mion (Forsgren et al., 2005), and those with refracory epilepsy are estimated to be less than 30%his number. Further, not all children with refractpilepsy are considered appropriate for treatment
he diet, either for social and/or medical reasons. Ners diminish further when the target populationD study is fully defined. For the initial case seri
he aim was to recruit children aged 1–16 yearge with refractory epilepsy who were tube fed. W
hese criteria alone limited the available patient phe greatest concern was ensuring access to the suatients. Although historically the KD has been offes a treatment option at limited centres, and somet
o limited patient numbers within individual centrhe increasing demand, funding and resourcesvailable has allowed the diet to be offered routino a greater number of patients. To maximize acc

170 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
recruitment took place at multiple centres across mul-tiple countries.
13.3. Inclusion and exclusion criteria
While achieving adequate recruitment is a prob-lem common to many clinical trials, other challengesare more specific to trials of nutritional products. Forexample, as in the case of KetoCal, products are oftendesigned for a specific age range, thereby limitingpatient numbers. In addition, the quantity of productconsumed can be critical. It was of great importance inthe case series to ensure that sufficient product be con-sumed daily to allow outcome measures to be attributedto the product rather than other oral intake. For exam-ple, although KetoCal can be used as a milk-shake stylemeal replacement/emergency regime, patients usingthis mode of intake could not be guaranteed to consumesufficient product daily. Moreover, it is not ethical toencourage those who can eat regular meals to consumethe majority of their energy requirements from a liquidsupplement. Thus, the target population became chil-dren who were tube fed, to ensure a minimum of 80% ofprescribed energy requirements were derived from theproduct. To document this, participants /careers com-pleted daily intake records.
1
lti-c datac ac-t umo ingc eyc anyu e
data on growth and seizure frequency are recorded, tobe used as a comparison to data collected during theintervention phase.
Dr. Helen Cross at Great Ormond Street (GOS) Hos-pital in London has developed an interesting alternativemethodological approach, which allows incorporationof a randomized control group (Fig. 6). At the screeningvisit, patients are randomized to the MCT or classicaldiet, and then they are further randomized to commencethe diet after either a 4-week, or a 16-week period. This12-week difference allows one group to continue stan-dard treatment while the other receives the ketogenic,thereby effectively incorporating a parallel-group con-trol. Such a study design begins to address the criticismconcerning the lack of published data on the efficacyof the diet using a control group (Lefevre and Aronson,2000; Thiele, 2003; Levy and Cooper, 2003).
13.5. Data collection methods
When numerous sites are involved in a clinical trial,it is essential that data collection be consistent betweenthe centres. During the design of the protocol for theKetoCal multicentre trial, the methods for the assess-ment of mental development, cognitive changes andquality of life generated much debate. In fact, assess-m ntlybo ncyw dedt thusa
1
calc for
m of th
3.4. Study design
The study design adopted for the KetoCal muentre trial incorporates a prospective baseline foromparison. In this study, tube fed children with refrory epilepsy are to be given KetoCal for a minimf 6 months. The baseline is established by followhildren for a 2-month period during which time thontinue to receive their standard feed alongsidenderlying AEDs (Fig. 5). During the run-in, baselin
Fig. 5. Schematic diagra
ent methods of these parameters vary significaetween countries (Levy and Cooper, 2003). The obvi-us difficulty arising here is the lack of consistehen it comes to data collation. It is recommen
hat all studies in this area use validated scales,llowing for comparative data analysis.
3.6. Conclusions
All clinical studies pose unique methodologihallenges, and those involving nutritional products
e KetoCal multicentre trial.
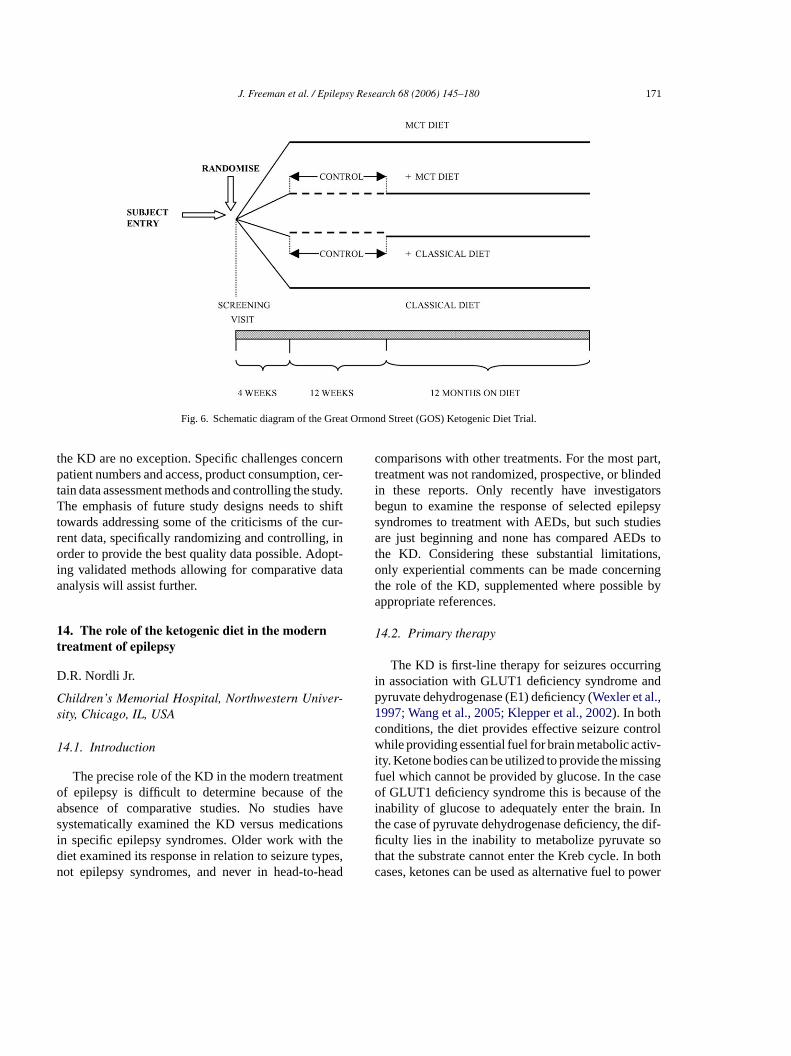
J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 171
Fig. 6. Schematic diagram of the Great Ormond Street (GOS) Ketogenic Diet Trial.
the KD are no exception. Specific challenges concernpatient numbers and access, product consumption, cer-tain data assessment methods and controlling the study.The emphasis of future study designs needs to shifttowards addressing some of the criticisms of the cur-rent data, specifically randomizing and controlling, inorder to provide the best quality data possible. Adopt-ing validated methods allowing for comparative dataanalysis will assist further.
14. The role of the ketogenic diet in the moderntreatment of epilepsy
D.R. Nordli Jr.
Children’s Memorial Hospital, Northwestern Univer-sity, Chicago, IL, USA
14.1. Introduction
The precise role of the KD in the modern treatmentof epilepsy is difficult to determine because of theabsence of comparative studies. No studies havesystematically examined the KD versus medicationsin specific epilepsy syndromes. Older work with thediet examined its response in relation to seizure types,n head
comparisons with other treatments. For the most part,treatment was not randomized, prospective, or blindedin these reports. Only recently have investigatorsbegun to examine the response of selected epilepsysyndromes to treatment with AEDs, but such studiesare just beginning and none has compared AEDs tothe KD. Considering these substantial limitations,only experiential comments can be made concerningthe role of the KD, supplemented where possible byappropriate references.
14.2. Primary therapy
The KD is first-line therapy for seizures occurringin association with GLUT1 deficiency syndrome andpyruvate dehydrogenase (E1) deficiency (Wexler et al.,1997; Wang et al., 2005; Klepper et al., 2002). In bothconditions, the diet provides effective seizure controlwhile providing essential fuel for brain metabolic activ-ity. Ketone bodies can be utilized to provide the missingfuel which cannot be provided by glucose. In the caseof GLUT1 deficiency syndrome this is because of theinability of glucose to adequately enter the brain. Inthe case of pyruvate dehydrogenase deficiency, the dif-ficulty lies in the inability to metabolize pyruvate sothat the substrate cannot enter the Kreb cycle. In bothc ower
ot epilepsy syndromes, and never in head-to- ases, ketones can be used as alternative fuel to p
172 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
brain energy needs. In this manner, the diet is not onlyan anticonvulsant treatment, but it also treats the othernon-epileptic manifestations of these diseases. In addi-tion, Wexler et al. (1997)reported increased longevityand improved mental development in patients withE1 deficiency who had earlier initiation of the diet orgreater carbohydrate restriction. It has also been shownthat the diet is effective in the treatment of GLUT1deficiency syndrome, although even early treatmentmay not eliminate neurological disabilities (Wang etal., 2005; Klepper et al., 2002).
14.3. Secondary treatment
The KD may be considered as an alternate treatment,usually after the failure of valproic acid, for generalizedepilepsies, particularly those with myoclonic seizuresincluding early myoclonic epilepsy, early infantileepileptic encephalopathy, and myoclonic-absenceepilepsy. Given the effectiveness of the diet in thetreatment of myoclonic epilepsies, it could be consid-ered as first line treatment for patients with those verysevere epileptogenic encephalopathies that are notori-ously difficult to control with medications, includingthe Lennox Gastaut syndrome. Recently, Fejermanand colleagues (Fejerman et al., 2005) reported ont verem e).T psy( on).S edi-c e ort cyo thisp ase.I d atJ d beu noty
ests fi smsd itho
1
uret roup
uses it very rarely in patients with symptomaticlocalization-related epilepsies. A recent publicationshowed that patients with complex partial seizuresas the predominant seizure type fared less well thanpatients with other forms of seizure types (Than et al.,2005).
14.5. Contraindications
As important as understanding when the diet maybe used to good advantage is knowledge of when toavoid the diet. The KD is absolutely contraindicated inchildren with pyruvate carboxylase deficiency, whereadministration of the diet may be lethal. We havenever used the diet in patients with fatty acid oxidationdisorders or organic acidurias like 3-hydroxy-methylglutaryl Co-A lyase deficiency. Although we used toavoid the diet in certain respiratory chain abnormali-ties, recently a group from South Korea showed thatthe diet can be used successfully in some patientswith respiratory chain abnormalities (Chul Kang et al.,2005).
15. Unsolved questions and priorities for futureresearch
N
Nv
thee t oft tivec
lastr ablei stiona ents tarta
e toi m-p ed ed y int zurea uldj
he effectiveness of the KD in the treatment of seyoclonic epilepsy of infancy (Dravet syndromhe diet is also useful in myoclonic–astatic epilepersonal observations, in preparation for publicatiince most parents prefer the convenience of a mation, it is unusual to try the KD before at least onwo AEDs have failed, but given the lack of efficaf drugs and some of the advantages of the KDolicy should be re-examined in each individual c
ndeed, a retrospective review of patients treateohns Hopkins showed that the diet can indeesed as first line treatment in epilepsies that areet intractable (Rubenstein et al., 2005).
The KD can also be beneficial in infants with Wyndrome (Kossoff et al., 2002a). In our series onfants treated with the diet, those with infantile spaid slightly better than those infants presenting wther types of seizures (Nordli et al., 2001).
4.4. Tertiary treatment
The diet can be used for a wide variety of seizypes and epilepsy syndromes. However, our g
. Bahi-Buisson
ecker Enfants Malades Hospital, Inserm U663, Uni-ersity Rene Descartes Paris V, Paris, France
Even though many advances in understandingffects of the KD have been made recently, mos
he clinical data remain to be confirmed by prospecontrolled trials.
The diet is traditionally considered a therapy ofesort, but recent data suggest that it could be valun new-onset epilepsy. These data raise the quebout the appropriate place of the diet in the treatmchedule: which patients, when to start, how to snd for how long to maintain the diet.
One of the challenges in future research will bdentify predictive factors of good, immediate, colete, and sustainedresponse. Today, few predictivata are available (Than et al., 2005). It seems that thiet could be more effective when introduced earl
he course of epilepsy, and in patients with high seictivity. But should it be maintained for years or wo
ust a few weeks offer optimal benefit?

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 173
In our experience, the diet seems to work partic-ularly well in epilepsies that have experienced recentworsening. However, this needs to be confirmed andexplained. The optimal duration of the diet is alsoa major issue. There is growing evidence that themetabolic tolerability may become a problem after 2–3years on the diet. This contrasts with the fact that evenwhen there has been an apparent major benefit, there israrely relapse when stopping the diet. This would sup-port the notion that at times the diet is maintained fortoo long. May be there is a sizeable number of patientswho do not really benefit from the diet for more than afew weeks, and in whom the diet could be given withmajor benefit only for a few weeks. All this needs to beinvestigated prospectively and requires a multicentrecollaboration.
The optimalmethods of initiating the diet need tobe clarified since outpatient protocols without fluidrestriction are claimed to give the same results as theinpatient protocols (Vaisleib et al., 2004).
In the field of biochemical research, the mecha-nisms of action of the diet still remain to be iden-tified. The relationship between ketosis and seizurecontrol remains unclear. Indeed, in spite of the factthat ketosis is believed to be necessary for clinicalefficacy, the correlation between the anticonvulsanta notc ayc od-i SFo2
1i
E
IaP
Q ol’sp s area iallyc
A ree-m erse
events observed during treatment with the diet, a cause-effect relationship has not been established. Clearly,neither the diet, nor any other therapy is free of sideeffects. The physician and the patient or family mustweigh the risks, side effects, and consequences of thediet against the risks, consequences and side effects ofthe alternative therapies. The diet is certainly not allnatural or holistic, but neither are medications. Whatare the risks of the diet and what are the consequencesof those risks? Those were summarized by Dr. Freemanas follows:
• The diet works equally well in most forms ofepilepsy in most patients, and has few complications.
• Most side effects are indeed mild, do not affectacceptability and rarely lead to diet discontinuation.It is well tolerated by younger and retarded patients.However, there is evidence for its usefulness in ado-lescents and adults as well.
• Dehydration due to decreased intake during the ini-tiation of the diet occurs, but is easily managed, andmay not be considered a side effect. Fasting has itsown specific benefits, and it is still recommendedroutinely at John’s Hopkins.
• Sepsis is not a side effect of the diet. Cardiomy-opathy has been reported but its relation to the diet
d aheionas
ably
• u-risk
indi-thenotith
• ndsthe
• eenentticon-h inthat
ction of the diet and the level of ketosis islearly established. Potentially useful insights mome from measurement of the levels of ketone bes, their metabolites, neurotransmitters in the Cf patients during chronic ketosis (Yudkoff et al.,004a,b).
6. Discussion summary—risks to benefit ratio,ndications and conclusions
. Perucca
nstitute of Neurology, IRCCS C. Mondino Foundation,nd Clinical Pharmacology Unit, University of Pavia,avia, Italy
. The list of adverse events given in Dr. Campistresentation is quite long, but some of these eventnecdotal. Which adverse effects should we especoncerned with?
. This issue was extensively addressed by Dr. Fan. He remarked that, for some anecdotal adv
is unclear. One patient at John’s Hopkins hacardiomyopathy prior to the diet, did well on tdiet, but was taken off the diet when the conditrecurred and died 9 months later, off the diet. Wthe cardiomyopathy related to the diet? Probnot.Lipoid aspiration occurs when aspirating individals are fed lipids. Gastroesophageal reflux and aof aspiration may be regarded as relative contracations to the KD. Hepatitis and pancreatitis, onother hand, occur in patients on AEDs and areprevented by the KD; pancreatitis may occur whypertriglyceridemia.The incidence of “serious complications” depeon the definition of “serious” but is very rare ondiet.Biochemical “disturbances” have indeed breported. Asymptomatic hypoglycemia is frequduring diet initiation. A persistent asymptomablood sugar of less than 80 mg/dl is a common csequence of a diet low in carbohydrate and higfat, but is it a side effect? Some centres believe

174 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
keeping glucose in the “low” range is therapeutic inand of itself.
• Growth retardation is mild in younger children onthe KD for prolonged period of time and catches upafter the diet is stopped.
• Slightly elevated lipids are also common, but theirlong-term consequences are unclear, and their lev-els after diet discontinuation have not been studied.Marked elevations are uncommon and may be man-aged with diet adjustments without having to stopthe diet.
• Nephrolithiasis is common (6%) and needs tobe closely followed and managed. However,nephrolithiasis is virtually never a reason for removea child from the diet.
In summary, there are consequences to every actionand inaction that we, as physicians, undertake. Thereare consequences to every AED we choose, but alsoconsequences to not choosing a medication. Thereare clearly consequences to the KD, most of thembeneficial—a decrease in seizures, a decrease in medi-cations, an increasing clarity to intellect, as medicationsare decreased. There are also side effects to the diet,most of them mild. It is important when counseling par-e thei vid-i esec witho ntali is-e andw cesd g tos
Q ntialr roica
A s isn ver,t ts area d Dr.K ntso tan-t Ds.A eenr diet
together with valproic acid, these disorders also occurin patients taking valproic acid alone (or the diet alone),and the evidence pointing to valproic acid as a potentialrisk factor is only circumstantial. Dr. Campistol, how-ever, mentioned that in his practice he preferred, as ameasure of caution and whenever possible, to avoidstarting the diet in children on high dosages of val-proic acid. As for other potential side effects, Dr. Nordliremarked that, in his experience, use of the KD togetherwith carbonic anhydrase inhibitors such as topiramateand zonisamide increases the risks for nephrolithiasisand, possibly, metabolic acidosis. Dr. Kossoff, how-ever, disagreed.
Q. It is clear that some of the benefits of the KD resultfrom a reduction in AED load. How long should wewait before tapering down medications, and how manypatients can have their AEDs discontinued completely?
A. Dr. Kossoff reported that the practice at JohnsHopkins is usually to reduce barbiturates and benzo-diazepines shortly after starting the diet. In general,however, medications begin to be reduced after a childhas been on the diet for about 3 months. However, thereare no adequate studies to guide the optimal policywith respect to reduction of AED therapy. In his centre,about one third of children stabilized on the KD havec tak-i
Q dataf ac-u elyt ce.
A hil-d izede hosew thatp a-t thath erem e),m noxG ande alsop renw nces wasg ow-
nts prior to beginning the diet to be specific as toncidences of side effects, especially when rare. Prong a list of all of the bad things that occur rarely to thhildren who are already handicapped by seizures,r without the additional handicaps of motor or me
mpairment, some with underlying and unknown dases, without putting the side effects into contextithout noting their frequency or their consequenoes a disservice to the population we are tryinerve.
. How much should we be concerned about poteisks of starting the diet in patients who are on valpcid, zonisamide and topiramate?
. There was consensus that use of these AEDot an absolute contraindication to the diet. Howe
here was no agreement on whether these patient special risk for adverse effects. Dr. Freeman anossoff felt that the safety record of the KD in patien valproic acid, zonisamide and topiramate is subs
ially similar to that seen in patients on other AElthough pancreatic and/or hepatic toxicity has b
eported occasionally in children treated with the
ompleted successful tapering, and are no longerng any AED.
. While we understand that we have no goodrom formal studies, it would be useful to hear the flty’s opinion about what types of epilepsies are lik
o show the best response based on their experien
. Dr Nordli commented that, in his experience, cren with cryptogenic and symptomatic generalpilepsies tend to respond more favourably than tith focal epilepsies, though he acknowledgedreliminary reports in children with diffuse migr
ion disorders are promising. Epilepsy syndromese felt may respond well to the diet include sevyoclonic epilepsy of infancy (Dravet syndromyoclonic–astatic epilepsy, West syndrome, Lenastaut syndrome, early myoclonic epilepsy,arly infantile epilepsy encephalopathy. There areromising reports in Rett’s syndrome, and in childith autism. On the other hand, intractable abseeizures generally do not do well on the diet. Thereeneral consensus on Dr. Nordli’s comments. H

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 175
ever, it was equally agreed that we lack good predictorsof outcome on the KD, and that prospective studiesin homogeneous cohorts with specific epilepsy syn-dromes are needed. Everyone expressed the wish thatthe workshop, together with the present report, couldact as catalyst towards establishing networks of inter-ested physicians and developing collaborative proto-cols to address the many gaps in knowledge that stillremain.
Acknowledgements
We wish to thank the Institute of Neurology IRCCSC. Mondino Foundation, the University of Pavia, andNutricia S.p.A. (Milan, Italy) for educational grantsin support of the organization of the workshop, andCollegio Ghislieri, Pavia, for hosting the event.
References
Al-Mudallal, A.S., LaManna, J.C., Lust, W.D., Harik, S.I., 1996.Diet-induced ketosis does not cause cerebral acidosis. Epilepsia37, 258–261.
Appleton, D.B., DeVivo, D.C., 1974. An animal model of the keto-genic diet. Epilepsia 15, 211–227.
A iont hip-
A iveentSci.
B S.,psia
B keto-.
B ber-usions 35,
B .A.,hy: a
B al-oneent.
B tri-psy:nol.
Best, T.H., Franz, D.N., Gilbert, D.L., Nelson, D.P., Epstein, M.R.,2000. Cardiac complications in pediatric patients on the keto-genic diet. Neurology 54, 2328–2330.
Bough, K.J., Gudi, K., Han, F.T., Rathod, A.H., Eagles, D.A., 2003.An anticonvulsant profile of the ketogenic diet in the rat. EpilepsyRes. 50, 313–325.
Busija, D.W., Lacza, Z., Rajapakse, N., Shimizu, K., Kis, B., Bari,F., Domoki, F., Horiguchi, T., 2004. Targeting mitochondrialATP-sensitive potassium channels—a novel approach to neuro-protection. Brain Res. Rev. 46, 282–294.
Caraballo, R., Cersosimo, R., Sakr, D., Cresta, A., Escobal, N., Fejer-man, N., 2005. Ketogenic diet in patients with Dravet syndrome.Epilepsia 46, 1539–1544.
Cardinali, S., Canafoglia, L., Bertoli, S., Franceschetti, S., Lanzi, G.,Tagliabue, A., Veggiotti, P. A pilot study of a ketogenic diet inpatients with Lafora body disease. Epilepsy Res., submitted forpublication.
Carroll, J., Koenigsberger, D., 1998. The ketogenic diet: a practicalguide for caregivers. J. Am. Diet. Assoc. 98, 316–321.
Casey, J.C., McGrogan, J., Pillas, D., Pyzik, P., Freeman, J., Vining,E.P., 1999. The implementation and maintenance of the ketogenicdiet in children. J. Neurosci. Nurs. 31, 294–302.
Chapman, S.A., Wacksman, G.P., Patterson, B.D., 2001. Pancreatitisassociated with valproic acid: a review of the literature. Pharma-cotherapy 21, 1549–1560.
Cheng, C.M., Hicks, K., Wang, J., Eagles, D.A., Bondy, C.A., 2004.Caloric restriction augments brain glutamic acid decarboxylase-65 and -67 expression. J. Neurosci. Res. 77, 270–276.
Chugani, H.T., Rintahaka, P.J., Shewmon, D.A., 1994. Ictal patternsof cerebral glucose utilization in children with epilepsy. Epilepsia5, 813–822.
C 5.ood279.
C ss inBrain
C J.B.,von,
atedpsy
C , S.,e,hil-y: an
C ato,chil-new
.C ordli,
utri-Am.
C Curr.
vshalumov, M.V., Rice, M.E., 2002. NMDA receptor activatmediates hydrogen peroxide-induced pathophysiology in rapocampal slices. J. Neurophysiol. 87, 2896–2903.
vshalumov, M.V., Rice, M.E., 2003. Activation of ATP-sensitK+ (K(ATP)) channels by H2O2 underlies glutamate-dependinhibition of striatal dopamine release. Proc. Natl. Acad.U.S.A. 100, 11729–11734.
allaban-Gil, K., Callahan, C., O’Dell, C., Pappo, M., Moshe,Shinnar, S., 1998. Complications of the ketogenic diet. Epile39, 744–748.
arborka, C.J., 1930. Epilepsy in adults: results of treatment bygenic diet in one hundred cases. Arch. Neurol. 6, 904–914
aumeister, F.A., Oberhoffer, R., Liebhaber, G.M., Kunkel, J., Ehardt, J., Holthausen, H., Peters, J., 2004. Fatal propofol infsyndrome in association with ketogenic diet. Neuropediatric250–252.
ergqvist, A.G., Chee, C.M., Lutchka, L., Rychik, J., Stallings, V2003. Selenium deficiency associated with cardiomyopatcomplication of the ketogenic diet. Epilepsia 44, 618–620.
ertoli, S., Striuli, L., Testolin, G., Cardinali, S., Veggiotti, P., Svatori, G.C., Tagliabue, A., 2002. Nutritional status and bmineral mass in children treated with ketogenic diet. RecProg. Med. 93, 671–675.
ertoli, S., Cardinali, S., Veggiotti, P., Tagliabue, A., 2005. Nutional and pharmacological management of childhood epileketogenic diets and common AEDs. Curr. Med. Chem. ImmuEndocrinol. Metab. Agents 5, 113–123.
hul Kang, H., Joo Kim, Y., Wook Kim, D., Dong Kim, H., 200Efficacy and safety of the ketogenic diet for intractable childhepilepsy: Korean multicentric experience. Epilepsia 46, 272–
ock, H.R., 2002. The role of mitochondria and oxidative streneuronal damage after brief and prolonged seizures. Prog.Res. 135, 187–196.
ock, H.R., Tong, X., Hargreaves, I.P., Heales, S.J.R., Clark,Patsalos, P.N., Thom, M., Groves, M., Schapira, A.H.V., ShorS.D., Walker, M.C., 2002. Mitochondrial dysfunction associwith neuronal death following status epilepticus in rat. EpileRes. 48, 157–168.
oppola, G., Veggiotti, P., Cusmai, R., Bertoli, S., CardinaliDionisi-Vici, C., Elia, M., Lispi, M.L., Sarnelli, C., TagliabuA., Toraldo, C., Pascotto, A., 2002. The ketogenic diet in cdren, adolescents and young adults with refractory epilepsItalian multicentric experience. Epilepsy Res. 48, 221–227.
oppola, G., Epifanio, G., Auricchio, G., Federico, R.R., ResicG., Pascotto, A., in press. Plasma free carnitine in epilepsydren, adolescents and young adults treated with old andantiepileptic drugs with or without ketogenic diet. Brain Dev
ouch, S.C., Schwarzman, F., Carroll, J., Koenigsberger, D., ND.R., Deckelbaum, R.J., DeFelice, A.R., 1999. Growth and ntional outcomes of children treated with the ketogenic diet. J.Diet. Assoc. 99, 1573–1575.
rino, P.B., Chou, K., 2000. Epilepsy and cortical dysplasias.Treat. Options Neurol. 2, 543–552.
176 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
Cuellar, R., Molinero, M., 2003. The treatment of children with dif-ficult to control epilepsy. Rev. Neurol. 37, 371–375.
Cunnane, S.C., Musa, K., Ryan, M.A., Whiting, S., Fraser, D.D.,2002. Potential role of polyunsaturates in seizure protectionachieved with the ketogenic diet. Prostaglandins Leukotr. Essent.Fatty Acids 67, 131–135.
Dahlin, M., Elfving, A., Ungerstedt, U., Amark, P., 2005. The keto-genic diet influences the levels of excitatory and inhibitory aminacids in the CSF of children with refractory epilepsy. EpilepsyRes. 64, 115–125.
De Vivo, D.C., Leckie, M.P., Ferrendelli, J.S., McDougal Jr., D.B.,1978. Chronic ketosis and cerebral metabolism. Ann. Neurol. 3,331–337.
De Vivo, D.C., Bohan, T.P., Coulter, D.L., Dreifuss, F.E., Greenwood,R.S., Nordli Jr., D.R., Shields, W.D., Stafstrom, C.E., Tein, I.,1998.l-Carnitine supplementation in childhood epilepsy: currentperspectives. Epilepsia 39, 1216–1225.
Depaulis, A., Vergnes, M., Marescaux, C., 1994. Endogenous controlof epilepsy: the nigral inhibitory system. Prog. Neurobiol. 42,33–52.
Erecinska, M., Nelson, D., Daikhin, Y., Yudkoff, M., 1996. Regu-lation of GABA level in rat brain synaptosomes: fluxes throughenzymes of the GABA shunt and effects of glutamate, calcium,and ketone bodies. J. Neurochem. 67, 2325–2334.
Fadiman, A., 1997. The Spirit Catches You and You Fall Down.Farrar, Strauss, Giroux, New York, p. 21.
Fejerman, N., Caraballo, R., Cersosimo, R., 2005. Ketogenic dietin patients with Dravet syndrome and myoclonic epilepsies ininfancy and early childhood. Adv. Neurol. 95, 299–305.
Ferranti, R., da Silva, M.M., Kowaltowski, A.J., 2003. MitochondrialATP-sensitive K+ channel opening decreases reactive oxygen
F aryFats,nal
F emi-urol.
F nicren.
F theirarma-
F angesuitry326.
F nca,.,
ode-97,
F sa-fatty
enic
Freeman, J.M., Vining, E.P., 1998. Ketogenic diet: a time-tested,effective, and safe method for treatment of intractable childhoodepilepsy. Epilepsia 39, 450–451.
Freeman, J., Vining, E., 1999. Seizures decrease rapidly after fasting:preliminary studies of the ketogenic diet. Arch. Pediatr. Adolesc.Med. 153, 946–949.
Freeman, J.M., Kelly, M.T., Freeman, J.B., 1996. The Epilepsy DietTreatment (An Introduction to The Ketogenic Diet), 2nd ed.Demos Vermande, New York, NY.
Freeman, J.M., Vining, E.P.G., Pillas, D.J., Pyzik, P.L., Casey, J.C.,Kelly, M.T., LCSW, 1998. The efficacy of the ketogenic diet-1998: a prospective evaluation of intervention in 150 children.Pediatrics 102, 1358–1363.
Freeman, J.M., Kelly, M.T., Freeman, J.B., 2000. The KetogenicDiet, 3rd ed. Demos Medical Publishers, New York.
Freeman, J.M., Kelly, M.T., Freeman, J.B., 2002. The KetogenicDiet: A Treatment for Epilepsy, 3rd ed. Demos Medical Publish-ers, New York.
Fuehrlein, B.S., Rutenberg, M.S., Silver, J.N., Warren, M.W., Theri-aque, D.W., Duncan, G.E., Stacpoole, P.W., Brantly, M.L., 2004.Differential metabolic effects of saturated versus polyunsatu-rated fats in ketogenic diets. J. Clin. Endocrinol. Metab. 89,1641–1645.
Furth, S.L., Casey, J.C., Pyzik, P.L., Neu, A.M., Docimo, S.G., Vin-ing, E.P., Freeman, J.M., Fivush, B.A., 2000. Risk factors forurolithiasis in children on the ketogenic diet. Pediatr. Nephrol.15, 125–128.
Galvan, M., Arellano, M., Sans, A., Sanmarti, F.X., Gomez, L., Ver-net, A., Campistol, J., 2001. Dieta cetogena: una alternativa validaen epilepsias refractarias? Rev. Neurol. 33, 1–5 (in Spanish).
Ganesh, S., Delgado-Escueta, A.V., Sakamoto, T., Avila, M.R.,, T.,, T.,wa,
for-lonusMol.
G diet:yrate
G l pre-285,
H poxiarol-
H agne,nt of52.
H the09.
H . Thepec-
H gingtered
species generation. FEBS Lett. 536, 51–55.ood and Nutrition Board, Institute of Medicine, 2002. Diet
References Intakes for Energy, Carbohydrate, Fiber,Fatty Acids, Cholesterol, Proteins and Amino Acids. NatioAcademy Press, Washington, DC.
orsgren, L., Beghi, E., Oun, A., Sillanpaa, M., 2005. The epidology of epilepsy in Europe—a systematic review. Eur. J. Ne12, 245–253.
rancois, L.L., Manel, V., Rousselle, C., David, M., 2003. Ketogeregime as anti-epileptic treatment: its use in 29 epileptic childArch. Pediatr. 10, 300–306 (in French).
ranks, N.P., Honore, E., 2004. The TREK K2P channels androle in general anaesthesia and neuroprotection. Trends Phcol. Sci. 25, 601–608.
rantseva, M.V., Perez Velazquez, J.L., Carlen, P.L., 1998. Chin membrane and synaptic properties of thalamocortical circcaused by hydrogen peroxide. J. Neurophysiol. 80, 1317–1
rantseva, M.V., Perez Velazquez, J.L., Tsoraklidis, G., MendoA.J., Adamchik, Y., Mills, L.R., Carlen, P.L., Burnham, M.W2000. Oxidative stress is involved in seizure-induced neurgeneration in the kindling model of epilepsy. Neuroscience431–435.
raser, D.D., Whiting, S., Andrew, R.D., Macdonald, E.A., MuVeloso, K., Cunnane, S.C., 2003. Elevated polyunsaturatedacids in blood serum obtained from children on the ketogdiet. Neurology 60, 1026–1029.
Machado-Salas, J., Hoshii, Y., Akagi, T., Gomi, H., SuzukiAmano, K., Agarwala, K.L., Hasegawa, Y., Bai, D.S., IshiharaHashikawa, T., Itohara, S., Cornford, E.M., Niki, H., YamakaK., 2002. Targeted disruption of the Epm2a gene causesmation of Lafora bodies, neurodegeneration, ataxia, myocepilepsy and impaired behavioral response in mice. Hum.Genet. 11, 1251–1262.
ilbert, D.L., Pyzic, P.L., Freeman, J.M., 2000. The ketogenicseizure control correlates better with serum beta-hydroxibutthan with urine ketones. J. Child Neurol. 15, 787–790.
ross, G.J., Peart, J.N., 2003. KATP channels and myocardiaconditioning: an update. Am. J. Physiol. Heart Circ. Physiol.H921–H930.
anna, J.P., Ramundo, M.L., 1998. Rhabdomyolysis and hyassociated with prolonged propofol infusion in children. Neuogy 50, 301–303.
assan, A.M., Keene, D.L., Whiting, S.E., Jacob, P.J., ChampJ.R., Humphreys, P., 1999. Ketogenic diet in the treatmerefractory epilepsy in childhood. Pediatr. Neurol. 21, 548–5
elmholz, H.F., Keith, H.M., 1930. Eight years’ experience withketogenic diet in the treatment of epilepsy. JAMA 95, 707–7
emingway, C., Freeman, J.M., Pillas, D.J., Pyzik, P.L., 2001aketogenic diet: a 3–6 years follow-up of 150 children prostively enrolled. Pediatrics 108, 898–905.
emingway, C., Pyzik, P.L., Freeman, J.M., 2001b. Chanphysician attitudes toward the ketogenic diet: a parent-cen

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 177
approach to physician education about a medication alternative.Epilepsy Behav. 2, 574–578.
Hinton, W., Schwartz, R.H., Loach, A.B., 1982. Diet induced ketosisin epilepsy and anaesthesia. Metabolic changes in three patientson a ketogenic diet. Anaesthesia 37, 39–42.
Hopkins, I.J., Lynch, B.C., 1970. Use of ketogenic diet in epilepsyin childhood. Aust. Paediatr. J. 6, 25–29.
Horvath, T.L., Diano, S., Barnstable, C., 2003. Mitochondrial uncou-pling protein 2 in the central nervous system: neuromodulator andneuroprotector. Biochem. Pharmacol. 65, 1917–1921.
Iadarola, M.J., Gale, K., 1982. Substantia nigra: site of anticon-vulsant activity mediated by gamma-aminobutyric acid. Science218, 1237–1240.
Jenney, E.H., Pfeiffer, C.C., 1958. The convulsant effect ofhydrazides and the antidotal effect of anticonvulsants andmetabolites. J. Pharmacol. Exp. Ther. 122, 110–123.
Johnson, W.A., Weiner, M.W., 1978. Protective effects of ketogenicdiets on signs of hypoglicemia. Diabetes 27, 1087–1091.
Kang, H.C., da Chung, E., Kim, D.W., Kim, H.D., 2004. Early-and late-onset complications of the ketogenic diet for intractableepilepsy. Epilepsia 45, 1116–1123.
Kang, H.C., Kim, Y.J., Kim, D.W., Kim, H.D., 2005. Efficacy andsafety of the ketogenic diet for intractable childhood epilepsy:Korean multicentric experience. Epilepsia 46, 272–279.
Kankirawatana, P., Jirapinyo, P., Kankirawatana, S., Wongarn, R.,Thamanasiri, N., 2001. Ketogenic diet: an alternative treatmentfor refractory epilepsy in children. J. Med. Assoc. Thai. 84,1027–1032.
Karceski, S. (Ed.), 2001. The expert consensus guideline series: treat-ment of epilepsy. Epilepsy Behav. 2, A1–A50.
Kashiwaya, Y., Takeshima, T., Mori, N., Nakashima, K., Clarke, K.,in
cad.
K ne,xpe-39,
K tally
K con-
K ithi-66.
K ofting
K .M.,acute
K an,zure
K , S.,02.rit.
Klepper, J., Leiendecker, B., Riemann, E., Baumeister, F.A., 2003.The ketogenic diet in German-speaking countries: update. Klin.Padiatr. 216, 277–285 (in German).
Kossoff, E.H., 2004. More fat and fewer seizures: dietary therapiesfor epilepsy. Lancet Neurol. 3, 415–420.
Kossoff, E.H., McGrogan, J.R., 2005. Worldwide use of the keto-genic diet. Epilepsia 46, 280–289.
Kossoff, E.H., Vining, E.P.G., 2004. The ketogenic diet. In: Shorvon,S.D., Perucca, E., Fish, D.R., Dodson, E.W. (Eds.), The Treat-ment of Epilepsy. Blackwell Science, Oxford, pp. 262–268.
Kossoff, E.H., Pyzik, P.L., McGrogan, J.R., Vining, E.P., Freeman,J.M., 2002a. Efficacy of the ketogenic diet for infantile spasms.Pediatrics 109, 780–783.
Kossoff, E.H., Pyzik, P.L., Furth, S.L., Hladky, H.D., Freeman,J.M., Vining, E.P., 2002b. Kidney stones, carbonic anhydraseinhibitors, and the ketogenic diet. Epilepsia 43, 1168–1171.
Kossoff, E.H., Krauss, G.L., McGrogan, J.R., Freeman, J.M., 2003.Efficacy of the Atkins diet as therapy for intractable epilepsy.Neurology 61, 1789–1791.
Kossoff, E.H., McGrogan, J.R., Freeman, J.M., 2004a. Benefits ofan all-liquid ketogenic diet. Epilepsia 45, 1163.
Kossoff, E.H., Pyzik, P.L., McGrogan, J.R., Rubenstein, J.E., 2004b.The impact of early versus late anticonvulsant reduction afterketogenic diet initiation. Epilepsy Behav. 5, 499–502.
Kossoff, E.H., Thiele, E.A., Pfeifer, H.H., McGrogan, J.R., Freeman,J.M., 2005. Tuberous sclerosis complex and the ketogenic diet.Epilepsia 46, 1684–1686.
Kossoff, E.H., McGrogan, J.R., Bluml, R.M., Pillas, D.J., Ruben-stein, J.E., Vining, E.P., in press. A modified Atkins diet is effec-tive for the treatment of intractable pediatric epilepsy. Epilepsia.
Krauss, S., Zhgn, C.-Y., Lowell, B.B., 2005. The mitochondrial. 6,
K .D.,TP-dicals
365–
K ree-smaen.
L Thes forSci.
L e, H.,con-. J.
L nt ofacy.
L and
L rane
Veech, R.L., 2000.d-Beta-hydroxybutyrate protects neuronsmodels of Alzheimer’s and Parkinson’s disease. Proc. Natl. ASci. U.S.A. 97, 5440–5444.
atyal, N.G., Koehler, A.N., McGhee, B., Foley, C.M., CrumriP.K., 2000. The ketogenic diet in refractory epilepsy: the erience of Children’s Hospital of Pittsburgh. Clin. Pediatr.153–159.
eith, H.M., 1931. The effect of various factors on experimenproduced convulsions. Am. J. Dis. Child 41, 532–543.
eith, H.M., 1933. Factors influencing experimentally producedvulsions. Arch. Neurol. Psych. 29, 148–154.
ielb, S., Koo, H.P., Bloom, D.A., Faerber, G.J., 2000. Nephrolasis associated with the ketogenic diet. J. Urol. 164, 464–4
im, D.W., Kang, H.C., Park, J.C., Kim, H.D., 2004a. Benefitsthe nonfasting ketogenic diet compared with the initial fasketogenic diet. Pediatrics 114, 1627–1630.
im, D.Y., van Brederode, H., Sullivan, P.G., Spain, W.J., Rho, J2004b. Ketone bodies protect neocortical neurons againstoxidative stress. Epilepsia 45 (Suppl. 7), 199.
insman, S.L., Vining, E.P., Quaskey, S.A., Mellits, D., FreemJ.M., 1992. Efficacy of the ketogenic diet for intractable seidisorders: review of 58 cases. Epilepsia 33, 1132–1136.
lepper, J., Leiendecker, B., Bredahl, R., AthanassopoulosHeinen, F., Gertsen, E., Florcken, A., Metz, A., Voit, T., 20Introduction of a ketogenic diet in young infants. J. InheMetab. Dis. 25, 449–460.
uncoupling-protein homologues. Nat. Rev. Mol. Cell. Biol248–261.
renz, M., Oldenburg, O., Wimpee, H., Cohen, M.V., Garlid, KCritz, S.D., Downey, J.M., Benoit, J.N., 2002. Opening of Asensitive potassium channels causes generation of free rain vascular smooth muscle cells. Basic Res. Cardiol. 97,373.
witerovich Jr., P.O., Vining, E.P., Pyzik, P., Skolasky Jr., R., Fman, J.M., 2003. Effect of a high-fat ketogenic diet on plalevels of lipids, lipoproteins, and apolipoproteins in childrJAMA 290, 912–920.
ebel, D., Morin, C., Laberge, M., Achim, N., Carmant, L., 2001.carbohydrate and caloric content of concomitant medicationchildren with epilepsy on the ketogenic diet. Can. J. Neurol.28, 322–340.
ebuffe, G., Schumacker, P.T., Shao, Z.H., Anderson, T., IwasVanden Hoek, T.L., 2003. ROS and NO trigger early preditioning: relationship to mitochondrial KATP channel. AmPhysiol. Heart Circ. Physiol. 284, H299–H308.
efevre, F., Aronson, A., 2000. Ketogenic diet for the treatmerefractory epilepsy in children: a systematic review of efficPediatrics 105, E46.
ennox, W.G., 1960. Epilepsy and Related Disorders. LittleBrown, Boston.
evy, R., Cooper, P., 2003. Ketogenic diet for epilepsy. CochDatabase Syst. Rev., 3, CD001903.

178 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
Liang, L.P., Ho, Y.S., Patel, M., 2000. Mitochondrial superoxide pro-duction in kainate-induced hippocampal damage. Neuroscience10, 563–570.
Liang, L.P., Patel, M., 2004. Mitochondrial oxidative stress andincreased seizure susceptibility in Sod2(−/+) mice. Free Radic.Biol. Med. 36, 542–554.
Lightstone, L., Shinnar, S., Callahan, C.M., O’Dell, C., Moshe, S.L.,Ballaban-Gil, K.R., 2001. Reasons for failure of the ketogenicdiet. Neurosci. Nurs. 33, 292–295.
Likhodii, S.S., Serbanescu, I., Cortez, M.A., Murphy, P., Snead III,O.C., Burnham, W.M., 2003. Anticonvulsant properties of ace-tone, a brain ketone elevated by the ketogenic diet. Ann. Neurol.54, 219–226.
Liu, Y.M., Williams, S., Basualdo-Hammond, C., Stephens, D., Cur-tis, R., 2003. A prospective study: growth and nutritional statusof children treated with the ketogenic diet. J. Am. Diet. Assoc.103, 707–712.
Mady, M.A., Kossoff, E.H., Mc Gregor, A.L., Wheless, J.W., Pyzik,P.L., Freeman, J.M., 2003. The ketogenic diet: adolescents cando it, too. Epilepsia 44, 847–851.
Mattiasson, G., Sullivan, P.G., in press The emerging roles of UCP2 inhealth, disease and therapeutics. Antioxidants Redox Signaling.
Mattson, M.P., Liu, D., 2003. Mitochondrial potassium channels anduncoupling proteins in synaptic plasticity and neuronal cell death.Biochem. Biophys. Res. Commun. 304, 539–549.
Maydell, B.V., Wyllie, E., Akhtar, N., Kotagal, P., Powasky, K., Cook,K., Weinstock, A., Rothner, A.D., 2001. Efficacy of ketogenicdiet in focal versus generalized seizures. Pediatr. Neurol. 25,208–212.
McGhee, B., Katyal, N., 2001. Avoid unnecessary drug-related car-bohydrates for patients consuming the ketogenic diet. J. Am.
M S.,Pae-
M minoncediet.
M tho-
M ato,
Rev.
M erit.
N enicl. 9),
N .Y.,01.108,
P tosisa 40,
Patel, M., 1951-1962. Mitochondrial dysfunction and oxidativestress: cause and consequence of epileptic seizures. Free Radic.Biol. Med. 37.
Peterman, M.G., 1924. The ketogenic diet in the treatment ofepilepsy: a preliminary report. Am. J. Dis. Child 28, 28–33.
Peterman, M.G., 1979. Ketogenic diet in epilepsy. JAMA 84.Peterson, S.J., Tangney, C.C., Pimentel-Zablah, E.M., Hjelmgren,
B., Booth, G., Berry-Kravis, E., 2005. Changes in growth andseizure reduction in children on the ketogenic diet as a treat-ment for intractable epilepsy. J. Am. Diet. Assoc. 105, 718–725.
Pfeifer, H.H., Thiele, E.A., 2004. Low glycemic index diet as analternative to the ketogenic diet in the treatment of intractableepilepsy in childhood. Epilepsia 45 (Suppl. 7), 184.
Reger, M.A., Henderson, S.T., Hale, C., Cholerton, B., Baker, L.D.,Watson, G.S., Hyde, K., Chapman, D., Craft, S., 2004. Effects ofbeta-hydroxybutyrate on cognition in memory-impaired adults.Neurobiol. Aging 25, 311–314.
Rho, J.M., Anderson, G.D., Donevan, S.D., White, H.S., 2002.Acetoacetate, acetone, and dibenzylamine (a contaminant inl-(+)-beta-hydroxybutyrate) exhibit direct anticonvulsant actionsin vivo. Epilepsia 43, 358–361.
Rimvall, K., Martin, D.L., 1992. Increased intracellular g-aminobutyric acid selectively lowers the level of the largerof two glutamate decarboxylase proteins in cultured GABAer-gic neurons from rat cerebral cortex. J. Neurochem. 58, 158–166.
Rimvall, K., Sheikh, S.N., Martin, D.L., 1993. Effects of increasedgamma-aminobutyric acid levels on GAD67 protein and mRNAlevels in rat cerebral cortex. J. Neurochem. 60, 714–720.
Rimvall, K., Martin, D.L., 1994. The level of GAD67 protein isma-
R gan,genic
S ithepsy
S 989.ical
S eptic
S .D.,ents),
S leptic
S A.,and
S , D.,for40,
Diet. Assoc. 101, 87–101.ckay, M., Bicknell-Royle, Nation, J., Humphey, M., Harvey,
2005. The ketogenic diet in refractory childood epilepsy. J.diatr. Child Health 41, 353–357.
illichap, J.G., Jones, J.D., 1964. Acid–base, electrolyte, and aacid metabolism in children with petit mal. Etiologic significaand modifications by anticonvulsant drugs and the ketogenicEpilepsia 90, 239–255.
inassian, B.A., 2001. Lafora’s disease: towards a clinical, palogic, and molecular synthesis. Pediatr. Neurol. 25, 21–29.
oreno-Villares, Oliveros-Leal, L., Simon-Heras, R., Mateos-BeF., 2001. La vuelta a la dieta cetogena: que papel desempena enel tratamiento de las convulsiones infantiles refractarias?Neurol. 32, 1115–1119.
orris, A.A., 2005. Cerebral ketone body metabolism. J. InhMetab. Dis. 28, 109–121.
ei, M., Sperling, M.R., Liporace, J.D., Sirven, J.I., 2003. Ketogdiet in adults: response by epilepsy type. Epilepsia 44 (Supp282.
ordli Jr., D.R., Kuroda, M.M., Carroll, J., Koenigsberger, DHirsch, L.J., Bruner, H.J., Seidel, W.T., De Vivo, D.C., 20Experience with the ketogenic diet in infants. Pediatrics129–133.
an, J.W., Bebin, E.M., Chu, W.J., Hetherington, H.P., 1999. Keand epilepsy: 31P spectroscopic imaging at 4.1 T. Epilepsi703–707.
highly sensitive to small increases in intraneuronal gamaminobutyric acid levels. J. Neurochem. 62, 1375–1381.
ubenstein, J.E., Kossoff, E.H., Pyzik, P.L., Vining, E.P., McGroJ.R., Freeman, J.M., 2005. Experience in the use of the ketodiet as early therapy. J. Child Neurol. 20, 31–34.
chlanger, S., Shinitzky, M., Yam, D., 2002. Diet enriched womega-3 fatty acids alleviates convulsion symptoms in epilpatients. Epilepsia 43, 103–104.
chwartz, R.H., Eaton, J., Bower, B.D., Aynsley-Green, A., 1Ketogenic diets in the treatment of epilepsy: short-term clineffects. Dev. Med. Child Neurol. 31, 145–151.
chwartzkroin, P.A., 1999. Mechanisms underlying the anti-epilefficacy of the ketogenic diet. Epilepsy Res. 37, 171–180.
eymour, K.J., Bluml, S., Sutherling, J., Sutherling, W., Ross, B1999. Identification of cerebral acetone by 1H-MRS in patiwith epilepsy controlled by ketogenic diet. MAGMA 8 (133–42.
het, R.D., 2004. Metabolic concerns associated with antiepimedications. Neurology 63 (Suppl. 4), S24–S29.
ills, M.A., Forsythe, W.I., Haidukewych, D., MacDonald,Robinson, M., 1986. The medium chain triglyceride dietintractable epilepsy. Arch. Dis. Child 61, 1168–1172.
irven, J., Whedon, B., Caplan, D., Liporace, J., GlosserO’Dwyer, J., Sperling, M., 1999. The ketogenic dietintractable epilepsy in adults: preliminary results. Epilepsia1721–1726.

J. Freeman et al. / Epilepsy Research 68 (2006) 145–180 179
Sperling, M.R., Nei, M., 2004. The ketogenic diet in adults. In:Stafstrom, C., Rho, J. (Eds.), Epilepsy and the Ketogenic Diet.Humana Press, Totowa, NJ.
Stafstrom, C.E., Rho, J.M., 2004. Epilepsy and the Ketogenic Diet.Humana Press, Totowa, NJ.
Stewart, W.A., Gordon, K., Camfield, P., 2001. Acute pancreatitiscausing death in a child on the ketogenic diet. J. Child Neurol.16, 682.
Sullivan, P.G., Dube, C., Dorenbos, K.D., Steward, O., Baram, T.Z.,2003. Mitochondrial uncoupling protein-2 protects the immaturebrain from excitotoxic neuronal death. Ann. Neurol. 53, 711–717.
Sullivan, P.G., Spring, J.E., Hal, E.D., Scheff, S.W., 2004a.Mitochondrial uncoupling as a therapeutic target follow-ing neuronal injury. J. Bioenerg. Biomembr. 36, 353–356.
Sullivan, P.G., Rippy, N., Dorenbos, K., Concepcion, R., Agarwal,A., Rho, J.M., 2004b. The ketogenic diet increases mitochondrialuncoupling protein levels and activity in mouse hippocampus.Ann. Neurol. 55, 576–580.
Swink, T.D., Vining, E.P., Freeman, J.M., Freeman, J.M., 1997. Theketogenic diet. Adv. Pediatr. 44, 297–329.
Szot, P., Weinshenker, D., Rho, J.M., Storey, T.W., Schwartzkroin,P.A., 2001. Norepinephrine is required for the anticonvulsanteffect of the ketogenic diet. Brain Res. Dev. Brain Res. 129,211–214.
Takeoka, M., Riviello Jr., J.J., Pfeifer, H., Thiele, E.A., 2002. Con-comitant treatment with topiramate and ketogenic diet in pedi-atric epilepsy. Epilepsia 43, 1072–1075.
Tempkin, O., 1976. The Falling Sickness, 2nd ed. Johns HopkinsUniversity Press.
T gan,om-
sia 46,
T ents:
T notns-
T S.D.,ed-rial. Clin.
T Clin.
V andpsia
U it-ationxp.
V iet:atr.
Vamecq, J., Vallee, L., Lesage, F., Gressens, P., Stables, J.P., 2005.Antiepileptic popular ketogenic diet: emerging twists in anancient story. Prog. Neurobiol. 75, 1–28.
Veech, R.L., Chance, B., Kashiwaya, Y., Lardy, H.A., Cahill Jr., G.F.,2001. Ketone bodies, potential therapeutic uses. IUBMB Life 51,241–247.
Veech, R.L., 2004. The therapeutic implications of ketone bodies:the effects of ketone bodies in pathological conditions: ketosis,ketogenic diet, redox states, insulin resistance, and mitochon-drial metabolism. Prostaglandins Leukotr. Essent. Fatty Acids70, 309–319.
Vining, E.P.G., Freeman, J.M., Ballaban-Gil, K., Camfield, C.S.,Camfield, P.R., Holmes, G.L., Shinnar, S., Shuman, R., Tre-vathan, E., Wheless, J.W., 1998. A multicenter study of theefficacy of the ketogenic diet. Arch. Neurol. 55, 1433–1437.
Vining, E.P.G., 1997. Ketogenic diet. In: Engel Jr., T.A., Pedley(Eds.), Epilepsy: A Comprehensive Textbook. Lippincott-Raven,Philadelphia, pp. 1339–1344.
Vining, E.P.G., 1999. Clinical efficacy of the ketogenic diet. EpilepsyRes. 37, 181–190.
Vining, E.P.G., Pyzik, P., McGrogan, J., Hladky, H., Anand, A.,Kriegler, S., Freeman, J.M., 2002. Growth of children on theketogenic diet. Dev. Med. Child Neurol. 44, 796–802.
Vodickova, L., Frantik, Vodickova, A., 1995. Neutrotropic effects andblood levels of solvents at combined exposures: binary mixturesof toluene,o-xylene and acetone in rats and mice. Cent. Eur. J.Public Health 3, 57–64.
Voskuyl, R.A., Vreugdenhil, M., Kang, J.X., Leaf, A., 1998. Anti-convulsant effect of polyunsaturated fatty acids in rats, using thecortical stimulation model. Eur. J. Pharmacol. 341, 145–152.
Votyakova, T.V., Reynolds, I.J., 2001. DeltaPsi(m)-dependent andbrain
V af,ulatecad.
W Sun,cal,8.
W ahl,.S.,
eatedons.
W erapy
W strofic
W clonicures.
W 002.diet407.
W 78.jec-
han, K.D., Kossoff, E.H., Rubenstein, J.E., Pyzik, P.L., McGroJ.R., Vining, E.P., 2005. Can you predict an immediate, cplete, and sustained response to the ketogenic diet? Epilep580–582.
hiele, E., 2003. Assessing the efficacy of antiepileptic treatmthe ketogenic diet. Epilepsia 44 (Suppl. 7), 26–29.
hio, L.L., Wong, M., Yamada, K.A., 2000. Ketone bodies dodirectly alter excitatory or inhibitory hippocampal synaptic tramission. Neurology 54, 325–331.
ieu, K., Perier, C., Caspersen, C., Teismann, P., Wu, D.C., Yan,Naini, A., Vila, M., Jackson-Lewis, V., Ramasamy, R., Przborski, S., 2003.d-Beta-hydroxybutyrate rescues mitochondrespiration and mitigates features of Parkinson disease. JInvest. 112, 892–901.
oskes, P.P., 1990. Hyperlipidemic pancreatitis. Gastroenterol.N. Am. 19, 783–791.
alencia, I., Pfeifer, H., Thiele, E.A., 2002. General anesthesiathe ketogenic diet: clinical experience in nine patients. Epile43, 525–529.
eda, Y., Yokoyama, H., Nakajima, A., Tokumaru, J., Doi, T., Msuyama, Y., 2002. Glutamate excess and free radical formduring and following kainic acid-induced status epilepticus. EBrain Res. 147, 219–226.
aisleib, I.I., Buchhalter, J.R., Zupanc, M.L., 2004. Ketogenic doutpatient initiation, without fluid or caloric restriction. PediNeurol. 31, 198–202.
-independent production of reactive oxygen species by ratmitochondria. J. Neurochem. 79, 266–277.
reugdenhil, M., Bruehl, C., Voskuyl, R.A., Kang, J.X., LeA., Wadman, W.J., 1996. Polyunsaturated fatty acids modsodium and calcium currents in CA1 neurons. Proc. Natl. ASci. U.S.A. 93, 12559–12563.
ang, D., Pascual, J.M., Yang, H., Engelstad, K., Jhung, S.,R.P., De Vivo, D.C., 2005. Glut-1 deficiency syndrome: clinigenetic, and therapeutic aspects. Ann. Neurol. 57, 111–11
exler, I.D., Hemalatha, S.G., McConnell, J., Buist, N.R., DH.H., Berry, S.A., Cederbaum, S.D., Patel, M.S., Kerr, D1997. Outcome of pyruvate dehydrogenase deficiency trwith ketogenic diets. Studies in patients with identical mutatiNeurology 49, 1655–1661.
heless, J., 2001. The ketogenic diet: an effective medical thwith side effects. J. Child Neurol. 16, 633–635.
heless, J., 2004. Nonpharmacological treatment of the cataepilepsy of childhood. Epilepsia 45 (Suppl. 5), 17–22.
heless, J., Sankar, R., 2003. Treatment strategies for myoseizures and epilepsy syndromes with myoclonic seizEpilepsia 44 (Suppl. 11), 27–37.
illiams, S., Basualdo-Hammond, C., Curtis, R., Schuller, R., 2Growth retardation in children with epilepsy on the ketogenic(A retrospective chart review). J. Am. Diet. Assoc. 102, 405–
illmore, L.J., Sypert, G.W., Munson, J.V., Hurd, R.W., 19Chronic focal epileptiform discharges induced by in

180 J. Freeman et al. / Epilepsy Research 68 (2006) 145–180
tion of iron into rat and cat cortex. Science. 200, 1501–1503.
Wirrell, E.C., Darwish, H.Z., Williams-Dyjur, C., Blackman, M.,Lange, V., 2002. Is a fast necessary when initiating the ketogenicdiet? J. Child Neurol. 17, 179–182.
Wolf, A., Weir, P., Segar, P., Stone, J., Shield, J., 2001. Impairedfatty acid oxidation in propofol infusion syndrome. Lancet 357,606–607.
Xiao, Y.F., Li, X., 1999. Polyunsaturated fatty acids modify mousehippocampal neuronal excitability during excitotoxic or convul-sant stimuli. Brain Res. 846, 112–121.
Xiao, Y.F., Kang, J.X., Morgan, J.P., Leaf, A., 1995. Blockingeffects of polyunsaturated fatty acids on Na+ channels of neona-tal rat ventricular myocytes. Proc. Natl. Acad. Sci. U.S.A. 92,11000–11004.
Xiao, Y.F., Gomez, A.M., Morgan, J.P., Lederer, W.J., Leaf, A., 1997.Suppression of voltage-gated L-type Ca2+ currents by polyun-saturated fatty acids in adult and neonatal rat cardiac myocytes.Proc. Natl. Acad. Sci. U.S.A. 94, 4182–4187.
Xiao, Y.F., Wright, S.N., Wang, G.K., Morgan, J.P., Leaf, A., 1998.Fatty acids suppress voltage-gated Na+ currents in HEK293t cellstransfected with the alpha-subunit of the human cardiac Na+
channel. Proc. Natl. Acad. Sci. U.S.A. 95, 2680–2685.Xu, Z., Ji, X., Boysen, P.G., 2004. Exogenous nitric oxide generates
ROS and induces cardioprotection: involvement of PKG, mito-chondrial KATP channels, and ERK. Am. J. Physiol. Heart Circ.Physiol. 286 (4), H1433–H1440.
Yamashita, J., 1976. Convulsive seizure induced by intracerebralinjection of semicarbazide (an anti-vitamin B6) in the mouse.J. Nutr. Sci. Vitaminol. (Tokyo) 22, 1–6.
Yehuda, S., Carasso, R.L., Mostofsky, D.I., 1994. Essential fatty acidpreparation (SR-3) raises the seizure threshold in rats. Eur. J.Pharmacol. 254, 193–198.
Yudkoff, M., Daikhin, Y., Nelson, D., Nissim, I., Erecinska, M.,1996. Neuronal metabolism of branched-chain amin acids. Fluxthrough the aminotransferase pathway in synaptosomes. J. Neu-rochem. 66, 2136–2145.
Yudkoff, M., Daikhin, Y., Nissim, I., Grunstein, R., Nissim, I., 1997.Effects of ketone bodies on astrocyte amino acid metabolism. J.Neurochem. 69, 682–692.
Yudkoff, M., Daikhin, Y., Nissim, I., Lazarow, A., Nissim, I., 2001a.Brain amino acid metabolism and ketosis. J. Neurosci. Res. 66,272–281.
Yudkoff, M., Daikhin, Y., Nissim, I., Lazarow, A., Nissim, I., 2001b.Ketogenic diet, amino acid metabolism, and seizure control. J.Neurosci. Res. 66, 931–940.
Yudkoff, M., Daikhin, Y., Nissim, I., Lazarow, A., Nissim, I., 2004a.Ketogenic diet, brain glutamate metabolism and seizure control.Prostaglandins Leukotr. Essent. Fatty Acids 70, 277–285.
Yudkoff, M., Daikhin, Y., Nissim, I., Nissin, I., 2004b. The ketogenicdiet, interactions with brain amino acid handling. In: Staftrom,C.E., Rho, J.M. (Eds.), Epilepsy and the Ketogenic Diet. HumanaPress, Totowa, NJ, pp. 181–191.
Yudkoff, M., Daikhin, Y., Nissim, I., Lazarow, A., Nissim, I., 2004c.Ketogenic diet, amino acid metabolism and seizure control.Prostaglandin Leukotr. Essent. Fatty Acids 70, 277–285.
Yudkoff, M., Daikhin, Y., Nissim, I., Horyn, O., Lazarow, A.,Luhovyy, B., Wehrli, S., Nissim, I., 2005. Response of brainamino acid metabolism to ketosis. Neurochem. Int. 47, 119–128.