computer patient interviewing & pilot medical assessment #icasm2015
TRANSCRIPT

Computer Patient Interviewing & Pilot Medical Assessment
Dr Richard Sills [email protected] #ICASM2015

Acklowledgements & Declarations
#ICASM2015
The AAME (UK) Has kindly contributed towards my attendance at the conference
I have a commercial relationship with Primetime Medical Software Inc (developers of the “Instant Medical History” CPI system)
Prof Ray Jones, Health Informatics, University of Plymouth
John Bachman MD, Professor of Primary Care, Mayo Clinic

Why particularly relevant
#ICASM2015
Recent tragic events
Need to improve Psychological Assessment
Need to be seen to be improving Psychological Assessment
Need to improve efficiency of Aeromedical Assessment and Documentation

From this conference
#ICASM2015
Significant under reporting of psychological symtpoms and sub-optimal documentation
Difficulty of persuading pilots to part with information
Need to ask specific questions

Anyone recognise this man?
#ICASM2015
A Canadian Physician, one of the fourfounding Professors of John HopkinsHospital, he is described as the"Father of Modern Medicine".

Sir William Osler (1849-1919)
#ICASM2015
“Talk to the Patient long enough & he will tell you what is wrong with him”

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
2007?

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
2004?

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
1996?

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
1989?

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
1988?

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
1979?
“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz
When was this published?
Before 1969?

“Toward Automating the Medical History”
#ICASM2015
“...to relieve the physician from routine, although important, time‑consuming activities, thereby extending his capabilities to provide medical care. If the time physicians spend in collecting, organizing, recording, and retrieving data could be reduced, at least in part, by information technology, more time would be available for actual delivery of medical care and at the same time the physician’s capabilities for collecting information from patients would be extended...”
by Mayne, Weksel, and Sholz (1968)

Important reviews
#ICASM2015
Jones RB, Knill-Jones RP. Electronic Patient Record Project: Direct Patient Input to the Record. Report for the Strategy Division of the Information Management Group of the NHS Management Executive: University of Glasgow, 1994. (Updated 1997).
Bachman JW. The patient-computer interview: A neglected tool that can aid the clinician. Mayo Clinic Proceedings 2003;78(1):67-78.
Slack WV. Cybermedicine for the patient. American Journal of Preventive Medicine 2007;32(5):S135-S136.

Highlights
#ICASM2015
Warner Slack paper 1960’s
Ray Jones paper 1990’s
Pringle, BMJ 1988
Prof Bachman literature review 2003
Slack WV. Cybermedicine for the patient.
Prof Bachman “evisits” 2010

Common conclusions
#ICASM2015
“A well designed computer system can be usedto interview patients about their medical history,signs and symptoms”
“Such systems are acceptable to the majorityof patients”
“Systems give patients more time to thinkabout questions”

From 1968
#ICASM2015
“A branching series of questions is developed toassist the medical history taking of the clinician. Standard, carefully worded questions are used tocollect a history, with systems having hundreds if not thousands of questions, but patients onlyanswering those relevant”

Professor Ray Jones
#ICASM2015
From the number of published research studies in which computers have been successfully used to interview patients, I think there is no need to spendtime discussing the following:
> A well designed computer system can be used to interview patients about their medical history, signs and symptoms.
> Such systems are acceptable to the majority of patients
@rjonesplymouth

Dr M Pringle
#ICASM2015
“Computers may be used acceptably to gather accurate information and to improve medicaldecisions without diminishing the role of thedoctor”
Using computers to take patient histories, M Pringle, Nottingham University Medical School,BMJ volume 297, Sept 1988

Professor John Bachman MD
#ICASM2015
“Computer Patient Interviewing is valid”
“Instant Medical History is the World leader”
Bachman JW. The patient-computer interview: A neglected tool that can aid the clinician. Mayo Clinic Proceedings 2003;78(1): 67-78.

Can a computer take a Psychiatric History?
#ICASM2015
“A program on an inexpensive microcomputer was designed to elicit personal histories from patients in a general psychiatric ward. Their answers were compared with the information recorded by the responsible psychiatric team. Where answers disagreed with the clinicians' records, the patient was interviewed to investigate the discrepancy”
“Most patients' computer histories revealed several items unknown to the clinicians and of importance in the management of the patient. Most patients (88%) found that the computer interrogation was as easy as a clinical interview”
“Computer assessment is proposed as a useful technique for the routine assessment of patients to augment the clinician's findings and to allow her to concentrate on the most relevant areas”
Carr AC. Ghosh A. Ancill RJ. Can a computer take a psychiatric history? Psychological Medicine. 13(1):151-8, 1983 Feb.

Comparison of computer-based & personal interviews
#ICASM2015
“A computer-based questionnaire can generate responses that are equivalent to the responses to a traditional personal interview. In some cases, a computer may be more successful in eliciting risk factors”
Hasley S A comparison of computer-based and personal interviews for the gynecologic history update. Obstetrics & Gynecology. 85(4):494-8, 1995 Apr.

Mayo Clinic eVisits 2010
#ICASM2015
“The e-visits made surgery visits unnecessary in 1012 cases (40%)”
“In the basic e-visit process, patients entered theirreported problem in free text (eg, “back pain”) and then answered questions one at a time. The questions branched such that the history was organised into a readable clinical format”
Pilot Study of Providing Online Care in a Primary Care Setting Steven C. Adamson, MD, and John W. Bachman, MD. Mayo Clinic Proceedings August 2010 vol. 85 no. 8704-710

History taking: How do we perform?
#ICASM2015
Physicians miss 54% of patients problems and 45% of their concerns
In 50% of visits patients and doctors do not agree on the presenting problem
50% of psychological problems are missed
Only 23 seconds before patient is interrupted(12 secs for medical residents)
Biggest complaint in patient “satisfaction” is poor physician communication skills.
(See Bachman Literature review for references)
History taking: how does the Computer Perform?
#ICASM2015

Strengths of Computerised interview
#ICASM2015
Structured, all questions are asked
Does not Interrupt
Good at obtaining sensitive information
Patients better prepared for a subsequent face toface consultation
Legible summaries and direct input to Electronic Record
Scales calculated well
Effective at improving care quality

Strengths of Computerised interview
#ICASM2015
All questions usually answered
Can be done anywhere, at Patient’s pace & with family help
Different languages
Better data- better research
Checklist
Does not require Clinician’s time
Acceptable to Patients in multiple studies

Patient can complete as little or as much as they feel able and thedepth of questioning can be tailoredto suit the clinical setting

Computers show no embarrassmentin asking important questions whereresponses deem that question is worth answering

Otolarngology History of Ear surgery for infectionAccidents and Injuries
History of Concussion. Bone fracture. Post head injury confusion and fatigue. Memory loss a few seconds before injury. Injury from ligaments. Head injury. Loss of consciousness Immediately at time of injury, a few seconds after injury, and for an undetermined time period. Torn ligament of the right foot. Rib sprains. Cervical sprain. Sprained middle back. Doesn't know Number of leg sprains. One leg torn ligament. Head laceration.
Family HistoryHistory of Heart disease (immediate family), Asthma (distant family).Sister
History of AsthmaSocial History
History of Thinking someone in family has a substance abuse problemActivities for Daily Living
History of Sports participation restricted for health reasonsSubstance Use
Tobacco UseHistory of Friend or family use tobacco
AlcoholHistory of Alcohol intake
Drug UsageHistory of Friends bring alcohol to School
Medication HistoryOngoing Medications
History of Prescription medication for more than 3 months. Medication stopped in the last month anddosage change. Prescribed medication very effective. Medications prescribed by another physician. Most of the time compliant with Prescription. Inhaler use.
Over-the-counter Medications History of Non-prescription medicationComplementary Medicines
History of Nutritional supplements in last month and for weight gainAdverse Drug Reactions

Otolarngology History of Ear surgery for infectionAccidents and Injuries
History of Concussion. Bone fracture. Post head injury confusion and fatigue. Memory loss a few seconds before injury. Injury from ligaments. Head injury. Loss of consciousness Immediately at time of injury, a few seconds after injury, and for an undetermined time period. Torn ligament of the right foot. Rib sprains. Cervical sprain. Sprained middle back. Doesn't know Number of leg sprains. One leg torn ligament. Head laceration.
Family HistoryHistory of Heart disease (immediate family), Asthma (distant family).Sister
History of AsthmaSocial History
History of Thinking someone in family has a substance abuse problemActivities for Daily Living
History of Sports participation restricted for health reasonsSubstance Use
Tobacco UseHistory of Friend or family use tobacco
AlcoholHistory of Alcohol intake
Drug UsageHistory of Friends bring alcohol to School
Medication HistoryOngoing Medications
History of Prescription medication for more than 3 months. Medication stopped in the last month anddosage change. Prescribed medication very effective. Medications prescribed by another physician. Most of the time compliant with Prescription. Inhaler use.
Over-the-counter Medications History of Non-prescription medicationComplementary Medicines
History of Nutritional supplements in last month and for weight gainAdverse Drug Reactions

Psychiatric Anxiety Disorders
He reported: Stress now.Risk Factors, Prevention and Patient issues
PreventionCounselling
He reported: Not wearing protective eye. Carried weapon 6 or more days last month.Nutrition
He reported Diet in last monthPatient Issues
He reported: Consulting another physicianSelf-assessment Scales
Title: Asthma Control TestDescription: 5-item scale to determine problems with asthma in the last month.Patient Score 20 – Asthma may be under control Scoring Key and Interpretation:0-19 : Asthma not well controlled20-25 : Asthma may be under controlReference: Nathan RA, Sorkness CA, Kosinski M, et al. Development of the Asthma Control Test a survey for assessing asthma control J Allergy Clin Immunol 2004,113 59-65
Title: Mental Health Inventory Screening Test (MHI-5)Description: Short 5-item version of the 18 item Mental Health Inventory for detecting affective disorders. No level of severity is revealed because of the brevity of the scale.Patient Score 9 – Passed mental health screenScoring Key and Interpretation:0-17 : Passed mental health screen18-30 : Failed mental health screenReference: Berwick, DM, Murphy, JM Goldman, PA, “Performance of a Five item Mentla Health Screening Test”, Med Care 1991, 29,2 169-176.
Title: Children of Alcoholics Screening Test (CAST)Description: 30-item inventory identifies children and adolescents who are living with at least one alcoholic parent. It measures children's feelings, attitudes, perceptions and experiences related to their parents' drinking behaviour. It reliably identified 100% ofthe children or both clinically diagnosed and self-reported alcoholics.Patient Score 11 – Severe family dysfunction due to alcoholismScoring Key and Interpretation:0-3 : Non-alcoholic family4-9 : Family problem with alcholism likely10-30: Severe family dysfunction due to alcoholismReference: Jones JW Chilren of Alcoholics Screening Test, (CAST) Chicago, III Camelot Unlimited 1983

Psychiatric Anxiety Disorders
He reported: Stress now.Risk Factors, Prevention and Patient issues
PreventionCounselling
He reported: Not wearing protective eye. Carried weapon 6 or more days last month.Nutrition
He reported Diet in last monthPatient Issues
He reported: Consulting another physicianSelf-assessment Scales
Title: Asthma Control TestDescription: 5-item scale to determine problems with asthma in the last month.Patient Score 20 – Asthma may be under control Scoring Key and Interpretation:0-19 : Asthma not well controlled20-25 : Asthma may be under controlReference: Nathan RA, Sorkness CA, Kosinski M, et al. Development of the Asthma Control Test a survey for assessing asthma control J Allergy Clin Immunol 2004,113 59-65
Title: Mental Health Inventory Screening Test (MHI-5)Description: Short 5-item version of the 18 item Mental Health Inventory for detecting affective disorders. No level of severity is revealed because of the brevity of the scale.Patient Score 9 – Passed mental health screenScoring Key and Interpretation:0-17 : Passed mental health screen18-30 : Failed mental health screenReference: Berwick, DM, Murphy, JM Goldman, PA, “Performance of a Five item Mentla Health Screening Test”, Med Care 1991, 29,2 169-176.
Title: Children of Alcoholics Screening Test (CAST)Description: 30-item inventory identifies children and adolescents who are living with at least one alcoholic parent. It measures children's feelings, attitudes, perceptions and experiences related to their parents' drinking behaviour. It reliably identified 100% ofthe children or both clinically diagnosed and self-reported alcoholics.Patient Score 11 – Severe family dysfunction due to alcoholismScoring Key and Interpretation:0-3 : Non-alcoholic family4-9 : Family problem with alcholism likely10-30: Severe family dysfunction due to alcoholismReference: Jones JW Chilren of Alcoholics Screening Test, (CAST) Chicago, III Camelot Unlimited 1983

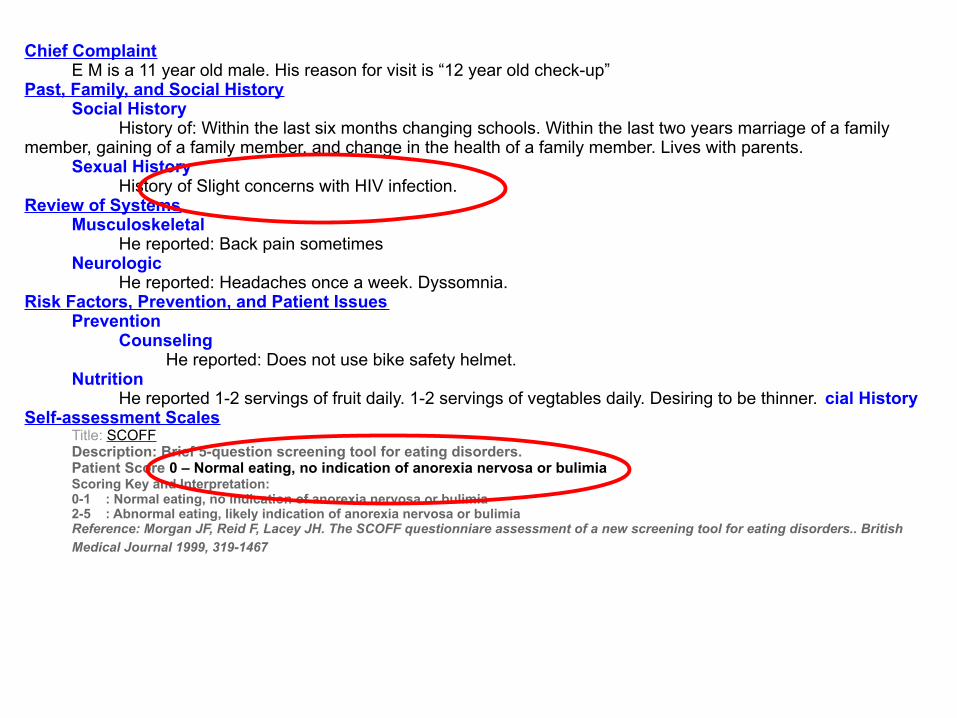
Chief Complaint E M is a 11 year old male. His reason for visit is “12 year old check-up”Past, Family, and Social History
Social HistoryHistory of: Within the last six months changing schools. Within the last two years marriage of a family
member, gaining of a family member, and change in the health of a family member. Lives with parents.Sexual History
History of Slight concerns with HIV infection.Review of Systems
MusculoskeletalHe reported: Back pain sometimes
NeurologicHe reported: Headaches once a week. Dyssomnia.
Risk Factors, Prevention, and Patient IssuesPrevention
CounselingHe reported: Does not use bike safety helmet.
NutritionHe reported 1-2 servings of fruit daily. 1-2 servings of vegtables daily. Desiring to be thinner. cial History
Self-assessment ScalesTitle: SCOFFDescription: Brief 5-question screening tool for eating disorders.Patient Score 0 – Normal eating, no indication of anorexia nervosa or bulimiaScoring Key and Interpretation:0-1 : Normal eating, no indication of anorexia nervosa or bulimia2-5 : Abnormal eating, likely indication of anorexia nervosa or bulimiaReference: Morgan JF, Reid F, Lacey JH. The SCOFF questionniare assessment of a new screening tool for eating disorders.. British Medical Journal 1999, 319-1467
Chief Complaint E M is a 11 year old male. His reason for visit is “12 year old check-up”Past, Family, and Social History
Social HistoryHistory of: Within the last six months changing schools. Within the last two years marriage of a family
member, gaining of a family member, and change in the health of a family member. Lives with parents.Sexual History
History of Slight concerns with HIV infection.Review of Systems
MusculoskeletalHe reported: Back pain sometimes
NeurologicHe reported: Headaches once a week. Dyssomnia.
Risk Factors, Prevention, and Patient IssuesPrevention
CounselingHe reported: Does not use bike safety helmet.
NutritionHe reported 1-2 servings of fruit daily. 1-2 servings of vegtables daily. Desiring to be thinner. cial History
Self-assessment ScalesTitle: SCOFFDescription: Brief 5-question screening tool for eating disorders.Patient Score 0 – Normal eating, no indication of anorexia nervosa or bulimiaScoring Key and Interpretation:0-1 : Normal eating, no indication of anorexia nervosa or bulimia2-5 : Abnormal eating, likely indication of anorexia nervosa or bulimiaReference: Morgan JF, Reid F, Lacey JH. The SCOFF questionniare assessment of a new screening tool for eating disorders.. British Medical Journal 1999, 319-1467

Chief Complaint A M is a 13 year old male. His reason for visit is “Pre-Participation Sports Exam”Past, Family, and Social History
Accidents and injuriesHistory of: Concussion. Injury torn ligaments. Head injury. Doesn't know number of leg torn ligaments. Doesn't know which bones were broken in lower leg. Head laceration.
Family HistoryMother
History of: AsthmaSocial History
History of: Physical assualt less than 2 monhts ago and by unknown personAllergy History
History of: No allergies to medicines, pollen, foods or stinging insectsPrior Available Tests
History of: Previous evaluation included an X-Ray of the shoulder. Treatment for musculoskeletal injury. Doesn't know number of leg X-Rays. Doesn't know number of arm X-Rays.
Review of SystemsEye
He reported: Vision changeNeurologic
He reported: Paresthesia post traumatic. Paralysis post traumatic. Headaches sometimes precipitated or aggravated by exertion.
Risk Factors, Prevention, and Patient IssuesPrevention
CounselingHe reported: Not weating protective eyewear
Time/Date10:16am August 6 2010

Chief Complaint A M is a 13 year old male. His reason for visit is “Pre-Participation Sports Exam”Past, Family, and Social History
Accidents and injuriesHistory of: Concussion. Injury torn ligaments. Head injury. Doesn't know number of leg torn ligaments. Doesn't know which bones were broken in lower leg. Head laceration.
Family HistoryMother
History of: AsthmaSocial History
History of: Physical assualt less than 2 monhts ago and by unknown personAllergy History
History of: No allergies to medicines, pollen, foods or stinging insectsPrior Available Tests
History of: Previous evaluation included an X-Ray of the shoulder. Treatment for musculoskeletal injury. Doesn't know number of leg X-Rays. Doesn't know number of arm X-Rays.
Review of SystemsEye
He reported: Vision changeNeurologic
He reported: Paresthesia post traumatic. Paralysis post traumatic. Headaches sometimes precipitated or aggravated by exertion.
Risk Factors, Prevention, and Patient IssuesPrevention
CounselingHe reported: Not weating protective eyewear
Time/Date10:16am August 6 2010

She denied pressure or pain in chest, heart murmur, intermittent chest pain, heavy squeezing tight chest pressure, edema, varicose veins, claudication.
GastrointestinalShe denied gastrointestinal symptoms, nausea, diarrhea, constipation, change in bowel habits, yellow rash.
GenitourinaryShe denied genitourinary symptoms, dysuria, vaginal discharge.
EndocrineShe denied gland trouble, diabetesm goutm or thyroid condition, change in thirst or appetite.
Hematological MuskuloskeletalShe denied excessive bleeding, swollen glands She denied rheumatic symptoms, swelling of
extremities.Neurologial
She reported frequent headaches, headaches more than twice a month, headache similar to previous headaches, onset of headaches under age of 24.She denied motor disturbances, dyssomnia, headaches usually periorbital at onset, periauricular headaches associated with opening jaw, headaches cause awakening from sleep, headaches more frequent certain days of the week, headaches occur in groups or clusters, aura preceeding headache, visual flashes or partial visual loss before the headache, alcohol or drugs precipitate a headache, chocolate consumption precipitates a headache, recently stopped taking any substance like a medication, drug, alcohol, caffeine or nicotine.Headaches areaccompanied by nuasea, vomitting, paresthesia or weakness associated with headache, eyes water or become red with headaches, headaches are accompanied by frequent urination, nasal congestion or discharge accompanying headaches.
PsychiatricShe reported history of suicidal idea or attempt, change in financial state within the last six months, change in responsibilities at work within the last six months, mild stressed feeling, enjoys interaction with opposite sex some of the time, normal thinking most of the time, normal activities most of the time, life full most of the time, irritable some of the time, iquickly becomes too tired to carry out activities, decisive most of the time, hopeful good part of the time, useful good part of the time, enjoy activities good part of the time. She denied personality changes in last six months, emotional complaints, recent stress, tobacco pipe, tobacco smokeless, tobacco use more than 10 years, personality change before headache.
Risk FactorsPhysical Conditioning
She reported less than 30 mins exercise per dayNutrition

She denied pressure or pain in chest, heart murmur, intermittent chest pain, heavy squeezing tight chest pressure, edema, varicose veins, claudication.
GastrointestinalShe denied gastrointestinal symptoms, nausea, diarrhea, constipation, change in bowel habits, yellow rash.
GenitourinaryShe denied genitourinary symptoms, dysuria, vaginal discharge.
EndocrineShe denied gland trouble, diabetesm goutm or thyroid condition, change in thirst or appetite.
Hematological MuskuloskeletalShe denied excessive bleeding, swollen glands She denied rheumatic symptoms, swelling of
extremities.Neurologial
She reported frequent headaches, headaches more than twice a month, headache similar to previous headaches, onset of headaches under age of 24.She denied motor disturbances, dyssomnia, headaches usually periorbital at onset, periauricular headaches associated with opening jaw, headaches cause awakening from sleep, headaches more frequent certain days of the week, headaches occur in groups or clusters, aura preceeding headache, visual flashes or partial visual loss before the headache, alcohol or drugs precipitate a headache, chocolate consumption precipitates a headache, recently stopped taking any substance like a medication, drug, alcohol, caffeine or nicotine.Headaches areaccompanied by nuasea, vomitting, paresthesia or weakness associated with headache, eyes water or become red with headaches, headaches are accompanied by frequent urination, nasal congestion or discharge accompanying headaches.
PsychiatricShe reported history of suicidal idea or attempt, change in financial state within the last six months, change in responsibilities at work within the last six months, mild stressed feeling, enjoys interaction with opposite sex some of the time, normal thinking most of the time, normal activities most of the time, life full most of the time, irritable some of the time, iquickly becomes too tired to carry out activities, decisive most of the time, hopeful good part of the time, useful good part of the time, enjoy activities good part of the time. She denied personality changes in last six months, emotional complaints, recent stress, tobacco pipe, tobacco smokeless, tobacco use more than 10 years, personality change before headache.
Risk FactorsPhysical Conditioning
She reported less than 30 mins exercise per dayNutrition

Patients collect info that Clinicians miss
#ICASM2015
40% of the time the questionnaire provided useful information that would not be typically elicited
Essential Questions aren't missed
Pilot’s Checklist

Relevance to Pilot Assessment
#ICASM2015
Psychological issues
Illicit Drugs
Alcohol
Documentation
Evidence strongly suggests that people will bemore honest with the CPI than face to face.

Completeness
#ICASM2015
CPI ensures that lines of investigation are not forgotten, leading to more complete data and fewer errors in diagnosis and better agreement between Patient and Doctor.
For example, a recent German hospital study found that computer histories reported an additional average of 3.5 problems per patient which were not recorded in corresponding physician histories. The authors recommended a combination of computer and physician histories as the best method.
Zakim D, Braun N, Fritz P, Alscher MD. Underutilization of information and knowledge in everyday medical practice: Evaluation of a computer-based solution. BMC Medical Informatics and Decision Making 2008;8:12.

Alcohol
#ICASM2015
Alcoholic Captain
“Wanted to be caught”
Wasn’t asked the right questions
CPI would have asked

Let Pilots do the work
#ICASM2015
The use of Computer Patient Interviewing allows pilotsto give a very full history whilst saving the AME time.
This will capture sensitive information at least as well as a face to face questions and probably more reliable.
Many more direct questions can be asked.
Standard Instruments can be administered and scoredas a routine (PHQ-9, GAD-7 etc)

Outcomes of using CPI
#ICASM2015
More complete questioning.
Better documentation which in turn will enhance the ability to compare responses over time.
Much better coded data.
Standard Instruments scored.
Improved assessment and particularly Psychological.
We will be seen to be improving our processes.

Change Management in Healthcare
#ICASM2015
“That the stethoscope will ever come into general use, notwithstanding its value, is extremely doubtful because its beneficial application requires much time and gives a good bit of trouble, both to the patient and the practitioner because it's hue and character are foreign and opposed to all our habits and associations”
The Times 1834

Thank you for your interest
#ICASM2015
Dr Richard Sills
+44 (0) 7940836337
slideshare.net/ICASM2015
(If you would like to add your slides to the collection please email them to me)

https://www.youtube.com/watch?v=uY32p_BqPw0

“Yes, yes, Mrs Jones... ...we'll talk about your chest pain in one minute. Right now I'm just trying to remember my password”

A machine cannot come betweenme and my Patient!
#ICASM2015
All of this is true
It need not happen

A case (thanks to Prof Bachman)
#ICASM2015
A patient who has hypertension comes to see you because in the last ten days she has noted that her blood pressure is elevated from its baseline.
Meds Lisinopril 20 mg daily
BP 152/93

Chief Complaint Time/Date Sonk is a 65 year old female. Her reason for visit is “Hypertension” 13:34pm. April 17, 2003History of Present Illness
SOnk reported: palpitations. Irregular, missed, or skipped heart beats.SOnk denied: angina pectoris. Pressure or pain in chest. Pale or white episodes sometimes.
Past, Family and Social HistoryPast Medical History
History of: last blood pressure high. Hypertension within five to ten years. Hypercholesterolemia. Hypertriglyceridemia.
Family HistoryHistory of family members with high blood pressure.
Social HistoryAlcohol
History of: alcohol use weeklyMedication History
Ongoing MedicationsHistory of: female hormoe medication. Conjugated estrogens. Non-prescription non-steroidal anti-inflammatory medication for pain.
Past Medications History of: estrogen replacement hormones. Estorgen and progesterone combination replacement
hormones. Estrogen progresterone combination therapy 11 to 15 years. Estrogen replacement therapy 11 to 15 years. Oral contraceptives.
Review of SystemsConstitutional Respiratory
SOnk denied: Overweight SOnk denied: dyspnea.Genitourinary Skin
SOnk denied: dyspnea. SOnk denied: acneMusculoskeletal Psychiatric
SOnk denied: legs painful. SOnk denied: recent stressNeurological Skin
SOnk denied: headaches. Tremulousness. SOnk reported: Paresis Risk Factors
Physical Conditioning Nutrition SOnk reported: <30 min per day exercise SOnk reported: Eating imported licorice

A case (thanks to Prof Bachman)
#ICASM2015
WHAT A DOC!!!!! 1) Her B/P is coming down: 138/80 and now 128/782) Her “numb feet” have responded well to the iron supplements. She is glad.3) She has stopped her licorice and excess salt intake4) She thanks you for sending her to the Patient Education class on Hypertension and YES you were right – she did learn something! This IS the truth and nothing but the truth....

What can we learn from this?
#ICASM2015
We can not judge quality of care by reviewinga chart!
Inputs are important
Computerised history provided more informationthat was critical to this case, and was valuableto the clinician

Embarrassing Topics
#ICASM2015
CPI allows patients to more easily disclose information about embarrassing topics eg. computer interviewing for pelvic floor symptoms in both primary care and hospital found ‘Despite the taboo nature of many of the items, the questionnaire was well received by women in both settings’
Radley SC, Jones GL, Tanguy EA, Stevens VG, Nelson C, Mathers NJ. Computer interviewing in urogynaecology: concept, development and psychometric testing of an electronic pelvic floor assessment questionnaire in primary and secondary care. BJOG 2006;113(2):231-238.