complex regional pain syndrome (crps)complex regional pain syndrome (crps) justin hata, md uc irvine...
TRANSCRIPT
Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 1
Complex Regional PainSyndrome (CRPS)
Justin Hata, MDUC Irvine Healthcare
Assistant Clinical ProfessorDepartment of Anesthesiology & Perioperative CareDepartment of Physical Medicine & Rehabilitation
Chief, Pain Medicine DivisionDirector, UCI Center for Pain Management
Co-Director, UCI Comprehensive Spine Program
Disclosure Information
Western Occupational Health Conference2010
Justin Hata, MDAssistant Clinical Professor, UC Irvine Healthcare
“I have nothing to disclose.”“I will not discuss off-label use and/orinvestigational use in my presentation.”
Objectives
1. Define CRPS
2. Discuss work-up
3. Explore treatment options, includingmedications
4. Explore current concepts

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 2
Definition
International Association for the Study ofPain (IASP): A variety of painful conditions following injury
which appears regionally having a distalpredominance of abnormal findings,exceeding in both magnitude and duration theexpected clinical course of the inciting eventand often resulting in significant impairment ofmotor function, and showing variableprogression over time.
History1600’s: Ambrose Paredescribed persistent pain& contractures afterbloodletting procedure forKing Charles IX1700’s: Percivall Pottreports burning pain andatrophy in injured limbs1800’s: Claude Bernardmentioned a syndrome ofpain associated with thesympathetic nervoussystem
Silas Weir-Mitchell1864: “Causalgia” in Civil Warsoldiers with limb injuries “…the most terrible of all tortures
which a nerve wound mayinflict…Its favorite site is the foot orhand. . . Its intensity varies fromthe most trivial burning to a state oftorture...The part itself is not alonesubject to an intense burningsensation, but becomes exquisitelyhyperanesthetic, so that a touch ortap of the finger increases thepain."

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 3
Sudeck’s Atrophy
Early 1900’s: Paul HM Sudeck (Sudeck’sAtrophy, Sudeck’s Dystrophy)
Reflex Sympathetic Dystrophy(RSD)
1946: James Evans described “RSD”
Sympathetically Maintained Pain(SMP)
1986William J. RobertsIntroduced term “SMP”Based on observation that blockingsympathetic nervous system =improvement/regression of symptoms

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 4
SMP versus SIP
Pain relieved by blockade of the efferentsympathetic nervous system “RSD” previously used based on observation that
sympatholytic procedures relieved pain in manypatients
Not all patients with CRPS have SMP Not all SMP is CRPS
CRPS patient may have sympatheticallyindependent pain (SIP) introduced by Campbelland Meyer in 1992
Mechanism of SMP
Normal response to injury is activation ofsympathetic reflex arcSMP involves prolonged continuation ofthe sympathetic reflex arc Hyperdynamic state of vasoconstriction, tissue
ischemia, and pain Increased activity and _-adrenergic receptor
sensitivity of nociceptive neruons Nociceptors now activated by norepinephrine
release by sympathetic fibers
Central Pain SignalingNeurons
SympatheticNeurons
Peripheral Nociceptors
(α receptors)
PeripheralInjury _
Norepi Release _
Mechanism of SMP

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 5
1993 Special ConsensusWorkshop (IASP) in Orlando, FL“Complex Regional Pain Syndrome”Descriptive and general termNot meant to imply etiology/pathologySubtypes Type I: RSD (without “nerve damage”) Type II: Causalgia (with “nerve damage”) Sympathetically maintained pain (SMP) Sympathetically independent pain (SIP)
1993 IASP diagnostic criteria forCRPS
1. The presence of an initiating noxious event, ora cause of immobilization
2. Continuing pain, allodynia, or hyperalgesiadisproportionate to any known inciting event
3. Evidence at some time of edema, changes inskin blood flow, or abnormal sudomotor activityin the region of pain
4. Diagnosis is excluded by the existence of otherconditions that would otherwise account for thedegree of pain and dysfunction
2003 International ConsensusCRPS Workshop in Budapest
“Closed” (invitation only) workshop
35 attendees, 7 countries
Proposed modified clinical diagnosticcriteria for CRPS (IASP)

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 6
“Budapest” criteria
Current Terminology
CRPS Type I aka Reflex Sympathetic Dystrophy (RSD) Without major nerve damage
CRPS Type II aka Causalgia With major nerve damage
Sensory Disturbances
Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 7
Autonomic Disturbances
Sympathetic deficit Warmth Loss of vasoconstrictor reflexes
Sympathetic over-activity Sweating Coldness
Cold pattern commonly in CRPS patientswith the longest duration of pain Warm, dry limb of CRPS can evolve into a cool
moist limb as the condition progresses
Motor Disorders (MDs)
Loss of voluntary controlBradykinesiaDystoniaMyoclonusTremorMay occur early in the disease coursePrevalence of MDs increases as thedisease duration lengthens
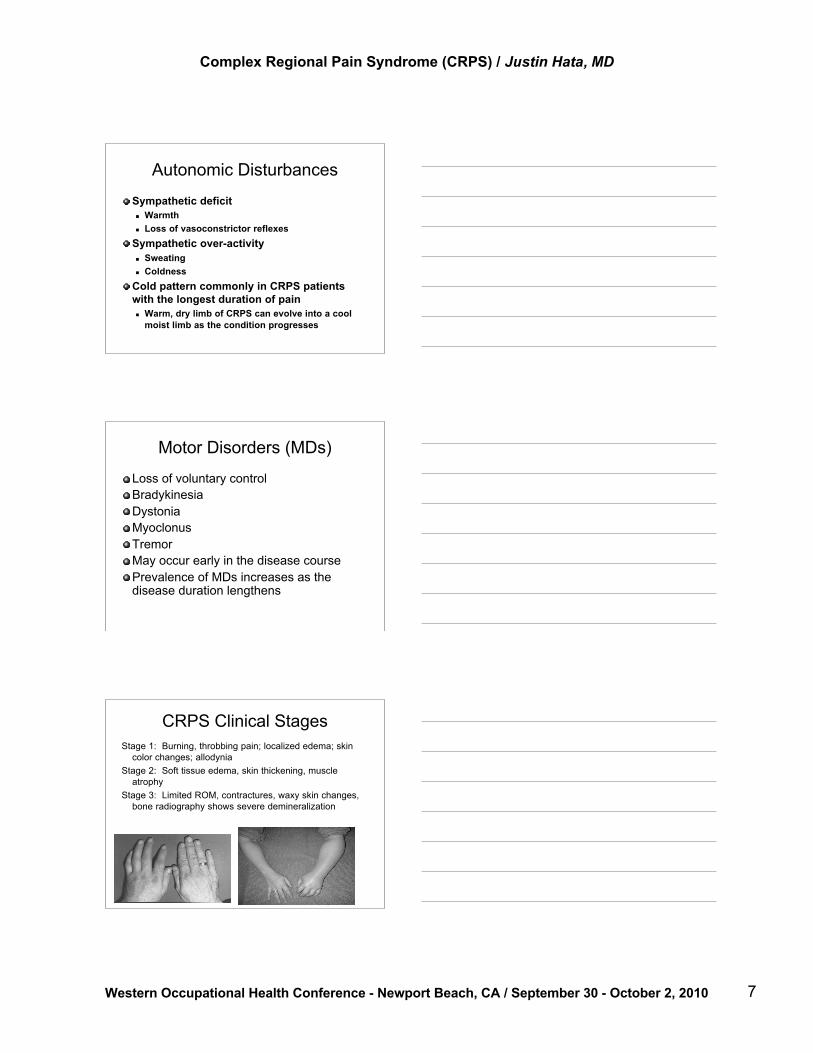
CRPS Clinical StagesStage 1: Burning, throbbing pain; localized edema; skin
color changes; allodyniaStage 2: Soft tissue edema, skin thickening, muscle
atrophyStage 3: Limited ROM, contractures, waxy skin changes,
bone radiography shows severe demineralization

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 8
Stages of CRPSAcute Dystrophic Atrophic
Pain Localized,severe,burning
Diffuse, throbbing Less severe, mayinvolve otherextremities
Extremity Warm Cold, cyanotic,edematous; musclewasting
Severe muscleatrophy, contractures
Skin Dry and red Sweaty Glossy and atrophic,waxy
X-ray Normal Osteoporosis Severe osteoporosis;ankylosis of joint
Duration 1-3 months 3-6 months Indefinite
Diagnostic TestsBone scintigraphy (stage 1 or 2)Plain radiographs (stage 2 or 3)fMRIQuantitative Sensory Testing (QST)Autonomic testing (QSART) Sweat output Skin temp
Diagnostic Injections for SMP Sympathetic Block Regional IV Blockade Phentolamine Infusion Test
Bone Scintigraphy
Bone scintigraphy –increased blood flow,pooling, and periarticularuptake (subacute stageup to 1 year)

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 9
X-Ray
X-ray – patchy demineralization(chronic stage)
fMRICRPS patients Marked differences of insular and Posterior Cingulate Cortex
(PCC) activation Activation of the anterior insula, PCC, and caudate Compared with controls, CRPS patients had stronger activation
of the PCC during painful stimulation of the symptomatic hand
Quantitative Sensory Testing
Quantitative Sensory Testing (QST) Non-invasive psychophysical method used to
assess severity of nerve damage Cold detection threshold Vibration detection threshold CRPS patients:
Increase in warm perception thresholdsDecrease of cold pain thresholds

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 10
Autonomic Testing
Infrared Thermography
Laser Doppler Flowmetry
Quantitative Sudomotor Axon ReflexTest (QSART)
Infrared Thermography
Non-invasive imaging technique measuringtemperature distribution in tissues
Laser Doppler Flowmetry
Non-invasive imaging technique to assessskin blood flow

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 11
Quantitative Sudomotor AxonReflex Test (QSART)
Autonomic function test of small nervefibers linked to sweat glandsMeasures Resting skin temperature Resting sweat output Stimulated sweat output
Treatment

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 12
Physical/Occupational Therapy
Both PT & OT have positive effectAcute Stage Immobilization Careful contralateral PT
Dystrophic Stage Passive PT with active isometric exercises Isotonic training Sensory desensitization program
2010 European EBM Guidelines forCRPS Type I
Multidisciplinary task forceLiterature review of treatment effects for CRPS IStudies published between 1980 – 2005Conclusions: For pain treatment: WHO analgesic ladder is advised For neuropathic pain: anticonvulsants and TCAs For inflammatory symptoms: free radical scavengers (DMSO or
N-acetylcysteine) To promote blood flow: vasadilatory medication and sympathetic
blockade show insufficient effect PT/OT advised to decrease functional limitations Vitamin C for primary prevention after wrist fx Further research needed!
Medications: 2010 European EBMGuidelines
No evidence or insufficient evidence forbeneficial effect Tylenol NSAIDs Opioids Local anesthetics Antidepressants Capsaicin Oral muscle relaxants Botulinum toxin Intrathecal baclofen administration

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 13
Medications: 2010 European EBMGuidelines
Limited evidence of beneficial effect Anticonvulsants: Limited evidence beneficial Ketamine: Limited evidence beneficial Free radical scavengers: Limited evidence
50% DMSO cream effective for warm CRPS IN-acetylcysteine for cold CRPS I
Corticosteroids: Limited evidence beneficial Bisphosphonates: Beneficial, unknown optimal dosing,
frequency, duration of treatment Calcium-channel blockers: Limited evidence
beneficial Calcitonin: Conflicting evidence
Sample Dosages
Gabapentin: 300 mg 3x/day, titrate up to800 mg 3x/dayDimethylsulphoxide (DMSO): 50% cream,apply 5x/day to the affected extremityN-acetylcysteine (NAC): 600 mgeffervescent tablets 3x/dayOral prednisone: 10 mg 3x/day untilclinical remission, max 12 weeksNifedipine: 20 mg 1x/day (acute phase)
Primary prevention medications(Pre-operative)
Primary prevention medications Vitamin C
500 mg/day x 50 days (7% vs 22% in casted wristfx)1000 mg/day x 45 days (2% vs 10% in wrist fxtreated with surgery
Guanethidine – Not indicated Calcitonin – Not indicated
Secondary prevention medications Regional anesthesia with lidocaine + clonidine
Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 14
InterventionsSympathetic blockade: Not useful for TxSympathectomy – Indications that may improvepain: surgical, chemical, or radiofrequencyIV Regional Block – No indication w/bretylium,guanethidine, local anesthetic, clonidine,ketoralac Possible improvement w/ketanserine or Infliximab*
Neuromodulation – Indication for painreduction and improved QOL: spinal cordstimulators (SCS)
Psychotherapy
Biofeedback
Stress Management
Relaxation Training
Family Therapy
Movement Disturbances Treatment
No RCT of PT, OT, or oral pharmacotherapy intreatment of MDs in CRPS.Splints or plaster casts are often ineffective May even worsen dystonic postures of CRPS
BZD and high doses of baclofen may bebeneficial in the treatment of dystonia andspasmsNo controlled studies for use of botulinum toxinin dystoniaIntrathecal baclofen: 1 study, small cohort,improved dystonia

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 15
Treatment Goals
Multidisciplinary approach Physical/Occupational therapy Medications Interventions Cognitive behavioral techniques Preventative measures
Early detection and treatment
Current ApplicationsIncreased risk of CRPS in modern day warfare Improvements in armor, military medicine result in
less deaths, but more severe injuries Military is focusing on prevention in combat zone
Regional techniques (epidural, CPNB) foranalgesia prior to surgery Decrease sensitization and prevention of prolonged
sympathetic activationObjectification of diagnostic criteria
Objectification of CRPS DiagnosticCriteria
R. Norman Harden (2010) “…scientifically problematic to add more data
elements that are also fully subjective (patientreport) or weakly objective (practitionerobservation)…”
“Hypothetically, objectifying and quantifyingas many criteria as possible will enhancediagnostic accuracy and research efficiency…”

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 16
Sensory FactorsQuantify pain by visual analog scale (VAS), if practical.Document qualities of pain using the McGill short-form.Quantify temperature allodynia by a standard Peltier-type device.Quantify mechanical allodynia using von Frey testing.Measure deep mechanical sensitivity by algometer, overmuscle and joint.Functional imaging provides the best data: a fullyobjective correlate with evoked pain (and hyperalgesia)Quantitative Sensory Testing
Vasomotor FactorsLaser Doppler: direct, fully objectivemeasure of vasomotor toneLimb temperature: indirect, yet objectivemeasure of cutaneous and subcutaneousblood flowMethods in order of objectivity andquantification: Infrared telethermography, thermistors,
thermometers, and temperature tape“Space suits”: manipulate and measurevasomotor tone experimentally
Sudomotor/Edema Factors
Can be objectively measured Quantitative sudomotor axon response testing
Indirectly measured (and patterned) using Bioimpedance (skin conductance testing) Skin potential fluctuations (sympathetic skin
response testing)Edema can be quantitated using volumetry

Complex Regional Pain Syndrome (CRPS) / Justin Hata, MD
Western Occupational Health Conference - Newport Beach, CA / September 30 - October 2, 2010 17
Motor FactorsSubjectively quantitate weakness by scoresFeatures of certain motor signs can be measured,such as bradykinesia and general activity (e.g.,accelerometer)Currently no reliable scores or metrics formyoclonus, athetosis, dystonia, or contractureSkin, nail, or hair trophic changes use subjectivemeasuresRange of motion: GoniometerBone density (Sudeck's atrophy) can be measuredSmall nerve density can be quantitated
Take Home Points
CRPS I (aka RSD) = NO nerve injuryCRPS II (aka causalgia) = nerve injuryNon-dermatomal pain out of proportion toinciting eventObjectification of autonomic, motor, trophic, orsensory changesSMP may or may not be presentMultidisciplinary treatment with medications, PT,interventions, psychotherapy
ReferencesProposed new diagnostic criteria for complex regional pain syndrome. Harden RN, Bruehl S,Stanton-Hicks M, Wilson PR. Pain Med. 2007 May-Jun;8(4):326-31.What does the mechanism of spinal cord stimulation tell us about complex regional painsyndrome? Prager JP. Pain Med. 2010 Aug;11(8):1278-83.Movement disorders in complex regional pain syndrome. van Hilten JJ. Pain Med. 2010Aug;11(8):1274-7.Vasomotor disturbances in complex regional pain syndrome--a review. Wasner G. Pain Med.2010 Aug;11(8):1267-73.Sensory disturbances in complex regional pain syndrome: clinical observations, autonomicinteractions, and possible mechanisms. Drummond PD. Pain Med. 2010 Aug;11(8):1257-66.Role of neuropeptide, cytokine, and growth factor signaling in complex regional pain syndrome.Kingery WS. Pain Med. 2010 Aug;11(8):1239-50.A hypothesis for the cause of complex regional pain syndrome-type I (reflex sympatheticdystrophy): pain due to deep-tissue microvascular pathology. Coderre TJ, Bennett GJ. Pain Med.2010 Aug;11(8):1224-38.Objectification of the diagnostic criteria for CRPS. Harden RN. Pain Med. 2010 Aug;11(8):1212-5.An update on the pathophysiology of complex regional pain syndrome. Bruehl S. Anesthesiology.2010 Sep;113(3):713-25.Evidence based guidelines for complex regional pain syndrome type 1. Perez RS, Zollinger PE,Dijkstra PU, Thomassen-Hilgersom IL, Zuurmond WW, Rosenbrand KC, Geertzen JH; CRPS Itask force. BMC Neurol. 2010 Mar 31;10:20.