competitive voucher schemes for better health for vulnerable populations and poor central american...
TRANSCRIPT

Competitive Voucher Schemes for Better Health
for Vulnerable Populations and Poor
Central American Health Institute ICAS
Anna Gorter MD PhD
Zoyla Segura MD MSc
Peter Sandiford MD PhD
Clinic at the Private Sector Advisory Services of the World Bank, Washington DC, US, November 6, 2002.

ICAS
• Instituto CentroAmericano de la Salud• NGO, founded in 1992• improve the health of the peoples of Central
America• especially the poorest and vulnerable• action-research• using innovative approaches • pioneer in use of competitive voucher schemes

ICAS Voucher schemes
• Nicaragua, second poorest country LA• Market failure to serve certain poor and
vulnerable population groups:– Sex workers, drug addicts and gay men– Adolescents, especially poor “high-risk”– Older, poor, rural women at risk for cervical cancer
• Search for alternative approaches• 1995 voucher trial sex workers successful• Voucher programs set up, learning by doing

Why including private sector
Public Sector has serious limitations:• Low efficiency• Failure of providing care to needy, poor and/or
marginalized populations:– Unresponsive to patients’ expectations– Low subjective / technical quality– Limited range / choice of services– Insufficient tax revenue to fund health services for all
Including the private sector may improve overall performance of health service provision

Why competitive voucher schemes?
• Difficult to transparently contract private sector
• Vouchers can restrict consumption to that which is ‘socially desirable’ and target certain groups
• Are a demand subsidy and therefore introduce fewer market distortions than supply subsidies
• Do not directly effect entry or exit into market for health services
Can be a good way to get public subsidies to high priority populations for the provision of clearly defined packages of cost-effective services

Objectives of vouchers
• increased equity in access to health• greater choice • improved quality of services• increased service use by vulnerable groups • more effective and efficient targeting• use of existing infra-structure• greater use of private sector providers• technical and allocative efficiency gains• results

Some advantages
• offer potential for donors to target the poor• strengthening and expanding private sector• open the public sector up to direct competition• open way for broader public private partnerships• greater innovation in delivery of services• greater decentralization of decision making• flexible to changing demands• practical transitional measure to develop pro
poor financial policies

Under what country circumstances?
• Where traditional health service provision has failed to reach certain groups or quality
• Where service providers exist in public and private sector (NGO and for- profit)
• Where competition is culturally /legally “accepted”• Where private service provision is cheaper and
more effective or if more expensive at least more cost effective

For what kind of health conditions/services?
• public health concerns • poverty reduction• to improve quality services • to improve screening activities• targeting marginalized and/or difficult-to-reach
populations

Why vouchers for sex workers to combat AIDS?
• AIDS is the most devastating pandemic in history
• STIs enhance transmission of HIV, so treating them reduces AIDS incidence
• STIs (including HIV) are sustained by ‘core groups’ such as sex workers
• interventions targeting core groups offer the most cost-effective way to prevent AIDS

however
• Sex workers are difficult to reach• Government programs can be successful but
in poor countries these are usually forced and stigmatizing
• Patients use either private clinics insufficiently or public clinics where their STIs goes unrecognized
• Need to target and deliver client-friendly health services of high technical quality which cure STIs and promote safer behavior

Design Features
• who will be the voucher agency• the criteria for service package• the specifications for service providers • the value of the voucher (full or part subsidized)• value paid to providers (varied or fixed)• recipient strategies (universal or targeted)• how often are vouchers distributed• information system • monitoring and evaluation
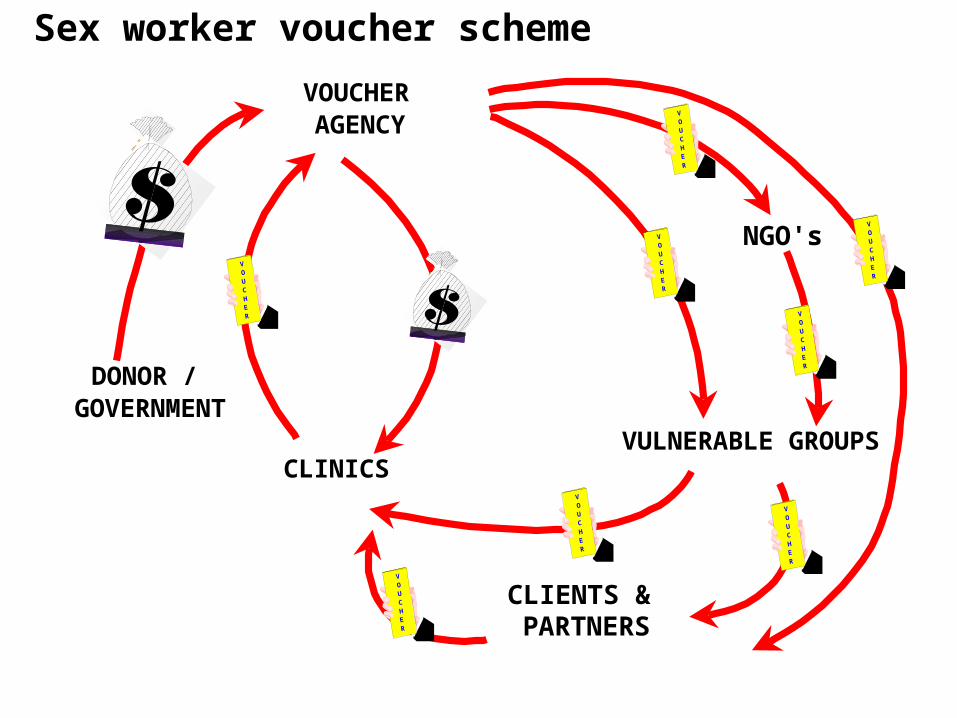
VULNERABLE GROUPSCLINICS
VOUCHER AGENCY
DONOR / GOVERNMENT
NGO's
VOUCHER
VOUCHER
VOUCHER
VOUCHER
VOUCHER
CLIENTS & PARTNERS
VOUCHER
VOUCHER
VOUCHER
Sex worker voucher scheme

Methods used
ICAS is the voucher agency and responsible for: • Mapping of prostitution sites• Feedback from vulnerable groups • Defining “best practice” service package• Defining specifications for service providers• Competitive tender/contracting clinics• Training clinic staff • Distribution of vouchers • Management of information system• Monitoring of quality of medical attention• Evaluation

Buying of the Services
• Study of size / composition of market and prices • Clinics are invited individually and compete for
8-12 contracts on price, quality and location • Clinics are paid individually negotiated price• Contracts reviewed each round, new clinics
invited to join, worst performer usually dropped• One laboratory is contracted (second for quality
control)• Condoms, medical supplies and training are
centrally procured by competitive tender

Monitoring Performance Clinics
• through street interviews with 10% of female voucher redeemers
• through medical record review• redemption rates of each clinic • follow-up consultation rates in each clinic• incidentally through mystery patients
(e.g. new services such as HIV testing)

Type of Providers Contracted
Total Actually
Public 3 0
Private 7 2
NGO 11 5
Total 21 7
Over 7 years 21 different providers have been contracted, operating 27 clinics. 14 providers were dropped. At the moment 7 providers with 11 clinics contracted

Some Results
• In 7 years > 18,000 vouchers distributed• > 7,000 consultations provided• > 2,700 STIs detected and treated
• each round 40%-50% sex workers used voucher • about 25% of male vouchers were redeemed• prevalence HIV sex workers increased just
slowly, from 0.8% in ’91 to 2% in ’99 and much less than in surrounding countries

STIs decreased in sex workers who used voucher >once
0%
10%
20%
30%
40%
STIs Go Syph Trich
Prevalence
First visitLast visit

Voucher schemes evolvedover time
• Process of action research: learning by doing• First seen as a way of inviting sex workers to
use health services • Introduction of contracts and competition
between clinics necessary to improve quality • Indicators to monitor performance • We involved sex workers to tailor services • Cost effective analysis to reduce costs• Success sex worker scheme lead to the
development of other schemes
Further development
• Through pilot, knowledge obtained of:– Epidemiological profile of STIs rates– Redemption rates different vulnerable groups – Costs of the services provided
• Available funds further determine number of vouchers to be distributed
• Targeting strategy, vouchers distributed through:– NGOs working with these vulnerable groups (for free)– ICAS field workers– Through clinics for partners/clients of voucher users

Development Voucher• To prevent counterfeiting vouchers are:– Numbered– Stamped with ICAS seal– Laminated
• Have expiration date• No measure taken
against trafficking• Clinics have to return voucher with
blood test and other samples– Prevents exchange vouchers for cash

What about black markets and voucher transferability?
• No strong measures to prevent voucher transfer • Transfer occurs with sex-worker vouchers (15%)• Compared to direct recipients these patients have
slightly lower STI rates, but much higher as general population
• In case of the vouchers distributed by sex workers to their clients, unknown how much transferred
• however > 50% of male users have one or more STIs, so transfer is to men with very high STI rates

Adverse selection
• In the case of the AIDS programs this is the objective, treat as much STIs as possible and attract the most needy patients
• Providers are remunerated for predefined service packages and extra costs are born by the voucher scheme

Why Competition Essential?
• Huge difference between competitive voucher schemes and vouchers which can only be redeemed at one provider or one type of provider (e.g. public providers)
• Without competition no choice of provider for the consumer, no shift of power, no incentive of lowering costs, improving quality and treating marginalized populations

Prices paid for consultation
• Baseline study estimated cost of outpatient consultation in public facility at US$ 7.65
• Program paid initially US$ 6.70 for each consultation and follow-up consultation
• Increased slightly at first, but average price paid now is US$ 5.10

Costs over time
• Costs service package (tests, drugs, condoms etc) excluding costs consultation reduced from about 50 US$ to 15 US$, while number of services offered increased
• Sex worker scheme in Managua is actually maintained with 60.000 US$ per year (was almost triple in first year, included research activities)
• Per capita cost of program < US$0.05 and < 1% of health expenditure

Increase quality
• Before: use of ineffective treatment protocols • Introduction “best practice” protocols
increased technical quality dramatically• Before program human quality of: – medical doctors was acceptable – gate keepers was very low
• Training staff improved quality considerably, but also treating sex workers reduced prejudice
• No need for embarrassing questions, since voucher declares that bearer is sex worker

Service Utilization
• Uptake of services by sex workers has increased, although SW were already using health services regularly, but without declaring their profession (STIs went unrecognized)
• Earlier uptake was ineffective, since technical quality was low
• Over time voucher redemption increased from less than 40% to almost 55%

Increased equity
• Because vouchers target poor sex workers• Because vouchers remove cost and quality
barriers to service uptake by sex workers• Because there is an additional self-selection by
those sex workers with the greatest needs• It are the poorest and most needy who make
much more use of their voucher

Lessons learned about competitive voucher schemes
• Useful in solving certain public health concerns• Can lead to considerable health gains• Setting up is complex and takes time to develop• High start-up costs, costs go down over time• Once set up, easy to run and to scale up• Although demand side approach, evokes response
from supply side and mobilizes private sector