“comparitive study of early (24 hours) versus late (48
TRANSCRIPT

i
“COMPARITIVE STUDY OF EARLY (24 HOURS)
VERSUS LATE (48 HOURS) MISOPROSTOL
ADMINISTRATION AFTER MIFEPRISTONE FOR
TERMINATION OF EARLY PREGNANCY”
By
Dr. N. PRIYA, MBBS.
Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka, in partial
fulfillment of the requirements for the degree of
MASTER OF SURGERY
IN
OBSTETRICS AND GYNAECOLOGY
Under the guidance of
Prof.Dr. PRASHANT. S . JOSHI, MD , DNB.
ADICHUNCHANAGIRI INSTITUTE OF MEDICAL SCIENCES
B.G.NAGARA, NAGAMANGALA TALUK, MANDYA DISTRICT,
KARNATAKA
2016

ii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES
BANGALORE, KARNATAKA
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation titled "COMPARITIVE STUDY OF
EARLY (24 HOURS) VERSUS LATE (48 HOURS) MISOPROSTOL
ADMINISTRATION AFTER MIFEPRISTONE FOR TERMINATION OF
EARLY PREGNANCY"was carried out by me under the guidance of Dr.
PRASHANT. S. JOSHI, MD, DNB Professor, Department of Obstetrics and
Gynaecology, Adichunchanagiri Institute of Medical Sciences, B.G. Nagara, in
partial fulfillment of the requirement for the degree of M.S in Obstetrics and
Gynaecology.
This dissertation has not been submitted previously for the award of any
degree or diploma to any university by me.
Date: Signature of the candidate
Place: B.G.Nagara Dr. N. PRIYA

iii
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
BANGALORE, KARNATAKA
CERTIFICATE BY THE GUIDE
This is to certify that this dissertation entitled "COMPARITIVE STUDY OF
EARLY (24 HOURS) VERSUS LATE (48 HOURS) MISOPROSTOL
ADMINISTRATION AFTER MIFEPRISTONE FOR TERMINATION OF
EARLY PREGNANCY" is a bonafide research work done by Dr. N. PRIYA
,Postgraduate student, Department of Obstetrics and Gynaecology, Adichunchanagiri
Institute of Medical Sciences, B.G.Nagara, in partial fulfillment of the requirement for
degree of Master of Surgery in Obstetrics and Gynaecology.
Date: Signature of the Guide
Place: B.G.Nagara
Dr. PRASHANT.S.JOSHI MD., DNB.
Professor,
Department of Obstetrics and Gynaecology,
AIMS, B.G. Nagara - 571448

iv
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
BANGALORE, KARNATAKA
ENDORSEMENT BY
THE HEAD OF DEPARTMENT AND THE PRINCIPAL
This is to certify that the dissertation titled " COMPARITIVE STUDY OF
EARLY (24 HOURS) VERSUS LATE (48 HOURS) MISOPROSTOL
ADMINISTRATION AFTER MIFEPRISTONE FOR TERMINATION OF
EARLY PREGNANCY "is a bonafide research work done by Dr. N. PRIYA,
Postgraduate student, Department of Obstetrics and Gynaecology, under the guidance
of Dr. PRASHANT.S. JOSHI.,M.D,DNB. Professor, Department of Obstetrics and
Gynaecology,Adichunchanagiri Institute of Medical Sciences, B.G.Nagara, in partial
fulfillment of the requirement for degree of Master of Surgery in Obstetrics and
Gynaecology.
Signature of the Head of Department
Signature of the Principal
Dr. VIJAYALAKSHMI. S., MD, DGO
Professor & Head of Department,
Department of OBG,
AIMS, B.G. Nagara - 571448
Dr. M.G. Shivaramu
Principal
Adichunchanagiri Institute of Medical
Sciences,
B.G. Nagara – 571448
Date :
Place : B.G. Nagara

v
RAJIV GANDHI UNIVERSITY OF HEALTH SCIENCES,
BANGALORE, KARNATAKA
COPY RIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that Rajiv Gandhi University of Health Sciences, Karnataka,
shall have all rights to preserve, use and disseminate this dissertation in print or
electronic format for the academic/research purpose.
Date: Signature of the candidate
Place: B.G.Nagara Dr. N. PRIYA
© Rajiv Gandhi University of Health Sciences, Karnataka.

vi
ACKNOWLEDGEMENTS
At outset, I wish to thank GOD for his guidance and blessings in every step
of my life.
I am indebted to my guide Dr.PRASHANT.S.JOSHI , Professor, Department
of Obstetrics and Gynaecology, Adichunchanagiri Institute of Medical Sciences,
B.G.Nagara, for his expert guidance and inspiration during the preparation of this
dissertation. I am also grateful to him for his encouragement, for having faith in me
and providing me with a free hand to experiment and analyze.
I extend my deep sense of gratitude to Dr.S.VIJAYALAKSHMI ,Professor
and Head, Department of Obstetrics and Gynaecology, Adichunchanagiri Institute of
Medical Sciences, B.G.Nagara, for her valuable advice, guidance and constant
inspiration during the preparation of this dissertation.
I also extend my deep sense of gratitude to Dr.N.GOPAL, Professor,
Department of Obstetricsand Gynaecology, Adichunchanagiri Institute of Medical
Sciences, B.G.Nagara, for his advice and guidance during the preparation of this
dissertation.
I would like to thank Dr. M.G. SHIVARAMU,MD,The Principal,
Adichunchanagiri Institute of Medical Sciences, B.G.Nagara, for permitting me to
utilize the college and hospital facilities for the study.
I also sincerely thank my teachers Dr. Ravindra Pukale, Dr.Chiniwar,
Dr.Rameshbabu,Dr.ShilpaShivanna,Dr.Mahendra,Dr.Bharathi,

vii
Dr.SavithaRathod, Dr. Subbappa, Dr.Indiradevi and Dr.Ramya for their
constant encouragement and guidance.
I am very much thankful to my mother Premalatha, my father Nallaiyan,
my Husband Prasanna , Dr.Chellathai, Dr.Subbaraju, Dr.Sathyabama,
Dr.Arunraj, Dr.Nanthini, Dr.Gowtham, Dr.Preetha & Dr.Vasantharagavan
without whom this dissertation would not have been successful.
I thank my colleagues, my juniors & my friends for their support.
Last, but not the least my heartfelt thanks to all my patients for their
Cooperation in every possible ways.
Date: Signature of the candidate
Place: B.G.Nagara Dr. N. PRIYA

viii
LIST OF ABBREVIATIONS USED
mcg : Microgram
mg : Milligram
Hrs : Hours
Vs : Versus
No : number
WHO : World Health Organisation
FDA : Food and Drug Administration
Kg/m2
: Kilogram/meter 2
ng/ml : Nanogram/milliliter
Wks : Weeks
CNS : Central nervous system
PG : Prostaglandin
COX : Cyclo-oxygenase
Mins : minutes
HCG : Human Chorionic Gonadotrophin
Yrs : Years

ix
ABSTRACT
Background
Medical method of abortion – a combination of Mifepristone followed by
prostaglandin analogue such as Misoprostol has been used up to 9 completed weeks
since last menstrual period. Misoprostol is the prostaglandin of choice for most
settings since it is cheap and does not require refrigeration.
The availability of safe and effective medical methods for inducing abortion
remains limited at present. However, rapid development and ongoing research may
lead to their wider introduction in the near future.
Objectives
The aim of the present study is to compare the efficacy of Mifepristone
followed after 24 hours by Misoprostol with the standard protocol (Mifepristone
followed by Misoprostol after 48 hours).
Materials and methods
This prospective case control study was conducted in 120 patients up to 63
days period of gestation who was diagnosed with early pregnancy failure & suitable
for medical abortion from a period of November 2013-October 2015.
Subjects in study arm was given 200 mg oral Mifepristone followed by 800
mcg vaginal Misoprostol after 24 hours, whereas those in control arm was
given 200 mg oral Mifepristone followed by 800 mcg of vaginal Misoprostol
after 48 hours.
Women who did not have bleeding in the first 8 hrs following 800 mcg
Misoprostol were given subsequent 200 mcg of vaginal Misoprostol. Doses

x
were repeated at 4th hourly interval to a maximum Misoprostol dose of
1200mcg.
Sequential allocation was done in the ratio of 1:1.
Statistical analysis
It was done by using Student t test & chi-square test. Descriptive and
inferential statistical analysis has been carried out in the present study.
Summary of results
Out of 135 patients screened 15 patients were excluded as per exclusion
criteria and 120 patients were taken for study. Mean induction to abortion interval in
study group was in the range of 5-6 hrs versus 6-7 hrs in control group with P value of
0.772 .The success rate in study group versus control group is 78.3 % versus 81.6%
with P value of 0.29 .11/58 patients required curettage in study group compared to
6/55 in control group.Side effect profile between 24 vs 48 hour regimen was
statistically insignificant.
Conclusion
Vaginal Misoprostol can be safely administered 24 hours following
Mifepristone compared to 48 hours regimen with equal efficacy.
Keywords
Medical abortion, Mifepristone, Misoprostol, Early pregnancy failure.

xi
TABLE OF CONTENTS
Sl No. TITLE PAGE NO
1. INTRODUCTION 1
2. AIMS AND OBJECTIVES 4
3. REVIEW OF LITERATURE 5
4. MATERIALS AND METHODS 41
5. RESULTS 45
6. DISCUSSION 62
7. CONCLUSION 75
8. SUMMARY 76
9. RECOMMENDATIONS 78
10. BIBLIOGRAPHY 79
11. ANNEXURE
PROFORMA
KEY TO MASTER CHART
MASTER CHART
89
92
93

xii
LIST OF TABLES
Table
no Contents Page:no
1. Possible risk factors for Early pregnancy failure 6
2. Effect of Mifepristone on various phases of menstrual
cycle
16
3. Milestones in the discovery of Prostaglandins 19
4. Absorption kinetics of Misoprostol 29
5. Metabolism and excretion of Misoprostol 30
6. Distribution profile of Misoprostol 30
7. Age distribution of patients 46
8. Obstetric index 48
9. Gestational age 50
10. Misoprostol application-abortion interval 52
11. Number of doses of Misoprostol 54
12. Success rate 56
13. Curettage (Failure ) rate 58
14. Side effect profile 59
15. Comparison of Mean age distribution 63
16. Comparison of Parity distribution 64
17. Comparison of Gestational age 65
18. Studies supporting shorter induction abortion interval in
24-Hour group
66
19. Studies reporting longer induction abortion interval in 24-
Hour group compared to 48 hour group.
67
20. Comparison of Success rate 68
21. Comparison of vital parameters of our study with other
related studies.
70

xiii
LIST OF GRAPHS
Graph
no Contents Page no
1. Age distribution of patients 47
2. Obstetric index 49
3. Gestational age 51
4. Misoprostol application-abortion interval 53
5. Doses of Misoprostol 55
6. Success rate 57
7. Side effect profile 59
8. Percentage distribution of side effects 60

xiv
LIST OF FIGURES
Figure
No Contents Page.no
1. Subchorionic hemorrhage 10
2. USG image showing Early pregnancy failure 11
3. Factors influencing Success rate of each management
modality 12
4. Mifepristone approval worldwide -2014 13
5. Mechanism of action of RU486 14
6. Additional properties of Mifepristone 15
7. Eicosanoids synthesis pathway 22
8. Prostaglandin chemical structure & synthesis 23
9. Arachidonic acid pathway 24
10. Prostaglandin and Thromboxane synthesis pathway 25
11. Chemical structure of Misoprostol 26
12. Geographic distribution of Misoprostol approval 27
13. Mean plasma concentrations of Misoprostol acid over time
with oral and vaginal administration. 29
14. Uterine activity in Montevideo Units induced by Misoprostol
given at different routes of administration. 31
15. Three-dimensional ultrasound showing measurement of the
gestational sac volume in an 8 week missed abortion 39
16. Study Summary 61

INTRODUCTION

1
INTRODUCTION
Medical abortion is a safe, effective and non invasive alternative for early
pregnancy termination. It holds great promise to access to safe abortion practices in
developing countries like India. Drug control general of India approved 600 mg of
Mifepristone coupled with 400 mcg of Misoprostol for early pregnancy termination
up to 49 days period of gestation[1-4].
25-50% of pregnancies encounter spontaneous pregnancy loss which usually
occurs up to 13 weeks of gestation.This spontaneous first trimester pregnancy loss can
be described by various non standardized terminologies such as early pregnancy
failure, blighted ovum, anembryonic gestation and missed abortion which are
confusing but still commonly used terms. The total rate of pregnancy loss after
implantation, including clinically recognized spontaneous abortions is 31 percent.[5]
Sonographic diagnostic criteria for early pregnancy failure[6]
Crown-rump length (CRL) of ≥7 mm and no heartbeat on a transvaginal scan,
Mean sac diameter (MSD) of ≥β5 mm and no embryo on a transvaginal scan,
Absence of embryo with heartbeat ≥β weeks after a scan that showed a
gestational sac without a yolk sac,
Absence of embryo with heartbeat ≥11 days after a scan that showed a
gestational sac with a yolk sac.
Non invasive management modalities for early pregnancy termination.
The success rate of expectant management which is clearly an option for
embryonic death or anembryonic gestation is influenced by various factors such as

2
unpredictable expulsion, uncertainty, anxiety resulting from pregnancy loss, often
makes expectant management less appealing to patients[7, 8]
Characteristics of Medical management [9]
Medical management with Misoprostol for early pregnancy failure appears to
offer more prompt evacuation and has become an increasingly popular alternative
with the following features,
Avoids invasive procedure and anesthesia.
Requires two or more visits.
Takes days to weeks to complete the process.
Available during early pregnancy with high success rate (approx-95%).
Moderate amount of bleeding which rarely becomes heavy.
Requires follow-up to ensure completion of abortion.
Requires patient participation throughout a multiple-step process.
WHO recommendation for medical methods of abortion[10]
“The WHO multinational trial with respect to side effects and acceptability of
medical methods have found that 85% of participants had successful outcome for the
procedure. Significantly higher acceptability was found among parous women
(compared to nulliparous women).
In 2003, World Health Organization (WHO) recommended that oral/vaginal
Misoprostol should be administered 36–48 hours after oral Mifepristone.However
based on the studies conducted by Singh et al and Schaff et al, it has been proved

3
that the interval of 48 hours can be safely reduced to even 8 hours without
compromising safety and efficacy [11]
.
In our study interval of 24 hours has been chosen based on the
pharmacokinetics of Mifepristone, which exerts its response in the uterus by blocking
the action of progesterone . It has also been reported that 40% of patients started to
bleed prior to Misoprostol administration, indicating that the abortion process has
already started[12].
Thus when the process of abortion starts even before administration of
Misoprostol, the rationale behind waiting for 48 hours has to be questioned and this
concept forms the baseline of our study.

OBJECTIVES

4
AIMS AND OBJECTIVES OF STUDY
The aim of the present study is to compare the efficacy of Mifepristone
followed by Misoprostol after 24 hours with the standard protocol
(Mifepristone followed by Misoprostol after 48 hours).
To evaluate whether 24 hour interval regimen will be an alternative to
standard 48 hour regimen without compromising its safety.

REVIEW OF LITERATURE

5
REVIEW OF LITERATURE
Early pregnancy loss.
Methods of termination.
Medical management.
Pharmacology of Mifepristone.
Historical review and Biochemistry of Prostaglandins.
Pharmacology of Misoprostol.
Mifepristone – Misoprostol interval regimen.
Review Studies.
EARLY PREGNANCY LOSS [13-20]
.
Introduction
Etiology
Types
Pathology
Diagnosis
Management
Introduction
Pregnancy is a significant event in woman’s life. Emotional attachment to the
Pregnancy and developing baby begins early in first trimester. Experiencing a first
trimester loss is a difficult and vulnerable time for most of the women. When it
occurs, the grief can be as profound as for any perinatal or other major loss [13, 14]
.

6
Spontaneous abortion (a pregnancy that ends spontaneously before the fetus has
reached a viable gestational age) is among the most common complications of
pregnancy.
Approximately 12–15% of recognized pregnancies and 17–22% of all pregnancies
ends in spontaneous abortion [13, 14]
.
Etiology
There is no clear cut etiology for first trimester pregnancy loss, instead we
have multiple risk factors which increases the likelihood of pregnancy loss.[15]
Table 1 : Possible risk factors for early pregnancy failure [16,17]
Maternal age >35 years.
Body mass index < 20 kg/m2, irrespective of age.
Increased serum cortisol levels.
Increased stress in life.
Low serum progesterone levels (< 12 ng/ml) prior to 7 wks of gestation.
Non-steroidal anti-inflammatory drug (NSAID) use.
Poor glycemic control.
Obesity.
Thyroid dysfunction.
Acute infections (Listeria, toxoplasmosis, parvovirus B19, rubella, herpes).
Hypercoagulable states.
Smoking.

7
TYPES OF EARLY PREGNANCY LOSS [13]
Spontaneous abortion
A pregnancy that ends spontaneously before the fetus has reached a period
of viability. The World Health Organization defines it as expulsion or extraction of
an embryo or fetus weighing 500 g (typically corresponds to a gestational age of 20
weeks) [13]
.
Threatened abortion
Bleeding through the cervical os with suprapubic pain during the first half of
pregnancy warrants threatened abortion in a patient. On examination, the uterine size
corresponds to gestational age, cervix is long and closed and fetal cardiac activity will
be detectable if the gestation is sufficiently advanced [13]
.
Inevitable abortion
Inevitable abortion is the pending abortion where the patient presents with
increased bleeding, intensely painful uterine cramps and dilated cervix. The products
of conception can often be felt or visualized through the internal cervical os[13]
.
Incomplete abortion
Incomplete abortion is the abortion with significant retained products of
conception which commonly occurs after 12 weeks of gestation. On examination, the
cervical os is open, products may be observed in the vagina/ cervix, and uterus is
smaller than expected for gestational age with painful cramps. There can be variable
amount of bleeding and it can be severe enough to cause hypovolemic shock [13]
.

8
Complete abortion
Complete abortion usually occurs before 12 weeks of gestation where the
entire contents of uterus are expelled. More than one-third of all cases are complete
abortions.On examination uterus will be small, well contracted with a closed cervix;
slight vaginal bleeding and mild cramping can be present [13]
.
Missed abortion
Refers to in utero death of the embryo or fetus prior to the 20th
week of
gestation, with prolonged retention of pregnancy for about 4 to 8 weeks. Vaginal
bleeding may occur and cervix is usually closed [13]
.
Septic abortion
Septic abortion accompanies fever, chills, malaise, abdominal pain, vaginal
bleeding, and frequently purulent discharge. Physical examination reveals
tachycardia, tachypnea, lower abdominal tenderness, and a tender uterus with dilated
cervix.Commonest organism causing infections are Staphylococcus aureus, Gram-
negative bacilli, or some Gram-positive cocci. Mixed infections (anaerobic organisms
and fungi) has also been encountered. Spreading of infection can lead to salphingitis,
generalized peritonitis, and septicemia [13]
.

9
PATHOLOGY OF EARLY PREGNANCY FAILURE [16, 17]
Maternal blood does not circulate within the placenta until about 9 weeks of
gestation. Prior to this time, trophoblastic cells serve to“plug” maternal spiral arteries,
preventing flow to these arteries and into the intervillous space until the villi mature
and begin to grow into the myometrium.
Minimal exposure to the high levels of oxygen in maternal blood during the
first trimester of human pregnancy is critical as the fetus and the placental villi are
exquisitely sensitive to oxidative stress. If exposed prematurely, pregnancy loss may
result. Thus histopathologic studies of fetal and placental tissue after pregnancy loss
shows premature intervillous blood flow.
Although Doppler flow may not be sensitive enough for assessing pregnancy
outcome, it has shown promise in predicting success of expectant management in
incomplete pregnancy loss. Presence of blood flow in the intervillous space using
Colour Doppler during evaluation of a threatened abortion increases the chance for
subsequent complete pregnancy loss with expectant management by fourfold.

10
Detection of First Trimester Loss
Presence of cardiac activity after 5 weeks and length of embryo of 2 mm declines the
risk of spontaneous loss to 3-6% [18]
.
Abnormal Sonographic findings suggestive of pregnancy loss prior to detection
of a heartbeat [18-20].
Gestational sac smaller than expected for dates.
An abnormal appearing yolk sac that is large, irregular, free floating, or calcified
should be followed by repeat ultrasonographic evaluation.
Although reproducibility is poor, placental abnormalities such as increased
echogenicity, increased thickness of trophoblast, or subchorionic hemorrhage
have been hypothesized as potential markers for subsequent pregnancy loss [18-20]
.
Figure 1 : Subchorionic hemorrhage [13]

11
Presence of subchorionic hemorrhage in first trimester with vaginal bleeding
raises the concern and anxiety of patients. But the timing of the bleeding has the most
important prognostic implications.
< 6 weeks - No increase in adverse pregnancy outcome [18-20].
>7weeks -10% chance of early pregnancy loss or later
pregnancy complications[18-20].
Figure 3 : Pregnancy outcome in Subchorionic hemorrhage in relation to
Gestational age.
Figure 2 : USG image showing Early pregnancy failure
Management of first trimester pregnancy loss [13]
There are three forms of management [13]
Expectant Management
Medical management
Surgical management.

12
The success rate of above three lines of management is influenced by
Figure 3 : Factors influencing Success rate of each management modality
MEDICAL MANAGEMENT
Mifepristone (RU 486)[21-26]
History : Roussel Uclaf (RU) was the French pharmaceutical company which first
developed RU486 in the early 1980s. The 486 designation is the shortened version of
compound name “γ8486” [21, 22].
Type of
pregnancy loss
Gestational
age
Hemodynamic
status of the
patient
Presence of
infection
Patients
preference

13
Figure 4 : Mifepristone approval worldwide - 2014
Mechanism of action[21-23]
Mifepristone (RU-486), a derivative of norethindrone, binds to progesterone
receptors with an affinity greater than progesterone but does not activate the receptor,
thereby acting as an antiprogestin.
Progesterone induces hyperpolarization of the cell membrane, which makes
the myocytes less sensitive to electrical stimulation thereby inhibits contractility of
uterus. It also causes inhibition of gap junction formation, which counteracts
coordinated uterine contractions. This actions of progesterone was antagonized by
Mifepristone which causes
Necrotisation of the decidua,
Softening of the cervix,
Increases both uterine contractility and prostaglandin sensitivity.

14
Figure 5 : Mechanism of action of RU486
Human studies have suggested that uterine contractility does not increase until
24–36 hours after Mifepristone administration. At this point, the myometrium is five
times more sensitive to the stimulatory effects of exogenous prostaglandins [23, 24]
.
Additional properties
Mifepristone also posseses anti-glucocorticoid action and weak anti-
androgenic activity.It is devoid of estrogenic properties [23, 24].

15
Figure 8: Additional properties of Mifepristone

16
Table 2: Effect of Mifepristone on various phases of Menstrual cycle[23-26]
In normally menstruating women, the effect of Mifepristone depends on the
timing of administration.
Phase of menstrual cycle
Effect of Mifepristone
First half of luteal phase
Independent of luteolysis menstrual induction occurs
During mid- luteal phase
Produces bleeding within a few days
During late luteal phase
Bleeding will be noticed within 1 to 3 days, reduces the
length of luteal phase of the present cycle and lengthening
of the subsequent follicular phase.
Day1, 2, 3 of the menstrual
cycle
No effect on cycle length
Late follicular phase
Prevents LH surge thereby prolongs the follicular phase
and new surge will be delayed by next 15 days.

17
Pharmacokinetics[24, 25, 26]
Absolute bioavailability of Mifepristone following intake of 200 mg was 69%.
It follows a non-linear pharmacokinetics and its volume of distribution and clearance
are inversely proportional to concentration of α1-acid glycoprotein (AAG).Volume of
distribution is also time as well as dose-dependent .Peak levels will be attained in the
serum 1-3 hours following its intake.
Mifepristone is about 98% plasma protein bound with high affinity to α1-acid
glycoprotein. It crosses the placenta with the maternal/fetal ratio of 9.1 and 17.1
respectively.
Mifepristone is metabolized in liver by means of successive demethylations
and by hydroxylation. 10% of the drug will be eliminated in the urine and 90% in the
faeces.
Tolerability[24, 25, 26 ]
Being a well tolerated drug Mifepristone causes uterine bleeding which
generally lasts for maximum 12 days.The sort of bleeding will be similar to that of
menstrual bleeding .It rarely requires curettage and blood transfusion and usually can
be controlled with hemostatic drugs.

18
80% of patients develops pain following 4th hourly administration of prostaglandin
and it can be well managed with non-narcotic analgesia. Whereas 20% of the patient
still requires parenteral narcotic analgesia.
Adverse Effects[26]
Most common adverse effects which patients encounter are
Abdominal pain
Fever
Nausea
Vomiting
Anorexia
Drug interactions with Mifepristone[25, 26]
Specific drug or food interactions have not been proved.
Based on the drug metabolism by CytochromeP-34A, Ketoconazole,
Erythromycin inhibits its metabolism as well as increases serum concentration.
Anticonvulsants such as Phenytoin, Phenobarbitone, Carbamazepine,
Rifampicin, Dexamethasone lowers the serum concentration of Mifepristone.
19
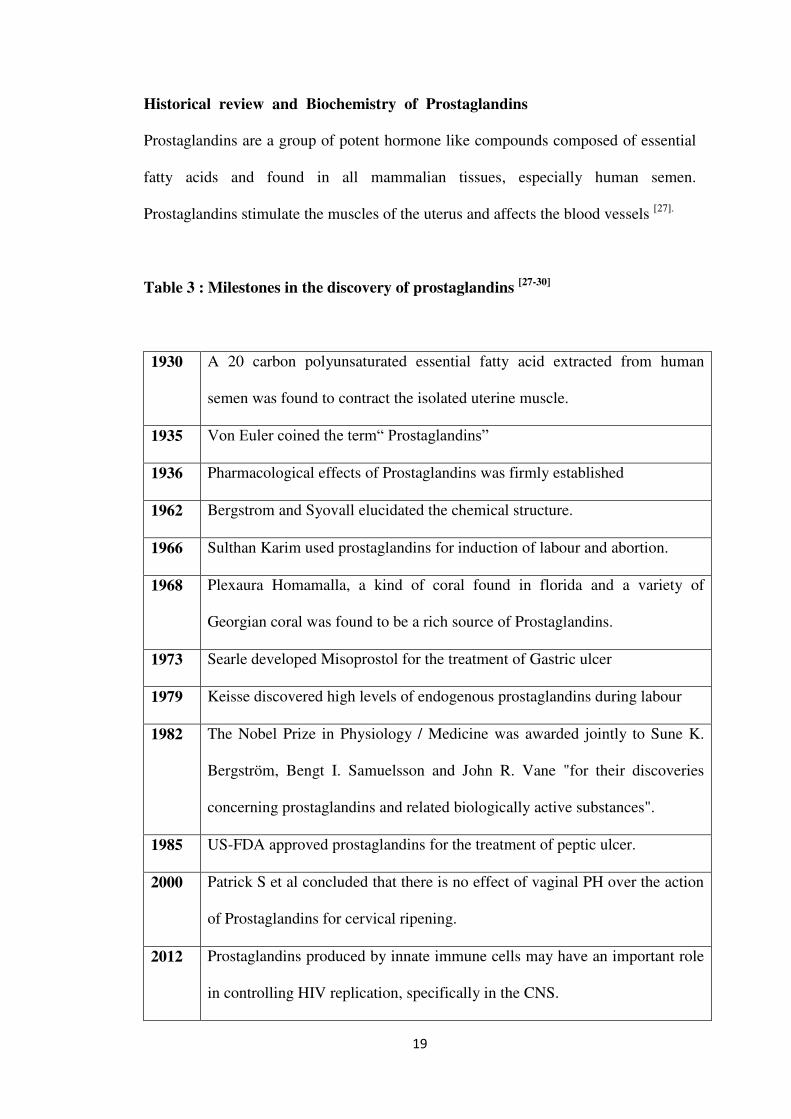
Historical review and Biochemistry of Prostaglandins
Prostaglandins are a group of potent hormone like compounds composed of essential
fatty acids and found in all mammalian tissues, especially human semen.
Prostaglandins stimulate the muscles of the uterus and affects the blood vessels [27].
Table 3 : Milestones in the discovery of prostaglandins [27-30]
1930 A 20 carbon polyunsaturated essential fatty acid extracted from human
semen was found to contract the isolated uterine muscle.
1935 Von Euler coined the term“ Prostaglandins”
1936 Pharmacological effects of Prostaglandins was firmly established
1962 Bergstrom and Syovall elucidated the chemical structure.
1966 Sulthan Karim used prostaglandins for induction of labour and abortion.
1968 Plexaura Homamalla, a kind of coral found in florida and a variety of
Georgian coral was found to be a rich source of Prostaglandins.
1973 Searle developed Misoprostol for the treatment of Gastric ulcer
1979 Keisse discovered high levels of endogenous prostaglandins during labour
1982 The Nobel Prize in Physiology / Medicine was awarded jointly to Sune K.
Bergström, Bengt I. Samuelsson and John R. Vane "for their discoveries
concerning prostaglandins and related biologically active substances".
1985 US-FDA approved prostaglandins for the treatment of peptic ulcer.
2000 Patrick S et al concluded that there is no effect of vaginal PH over the action
of Prostaglandins for cervical ripening.
2012 Prostaglandins produced by innate immune cells may have an important role
in controlling HIV replication, specifically in the CNS.

20
Biochemistry of prostaglandins [31-34]
“Prostaglandins are composed of a Cyclopentanone nucleus with two side chains.
Primary prostaglandins contain a 15 hydroxyl group with a 13, 14 trans double bond.
Categories of prostaglandins
Currently three classes of prostaglandins are recognized and these are
categorized on the basis of
Number of double bonds present within the prostaglandin molecule
Fatty acid from which they are derived.
Prostaglandins of 1 series have single double bond and are derived from
dihomo linolenic acid, those of 2 series have two double bonds and are derived from
arachidonic acid, and those of the 3 series have three double bonds and are derived
from eicosapentaenoic acid.
Categorisation of the thromboxanes and leukotrienes are also done depending
on the number of double bonds in the molecule. Each type of prostaglandin is
allocated a group letter (e.g., A, B, C, D, E, F, G, H), depending on the functional
substitutions in the cyclopentanone nucleus.
For example, in prostaglandin F (PGF), F indicates Prostaglandin has two
hydroxyl groups in the cyclopentanone ring (F series) ,2 indicates presence of
two double bonds ,α indicates hydroxyl grouping at carbon 9 is in the α
configuration.

21
Prostaglandin Synthetase Pathway [31-34]
The incorporation of molecular oxygen into arachidonic acid and fatty acids
results in the formation of unstable intermediate molecules. This action is mediated by
Prostaglandin synthetase (cyclooxygenase moiety) and this intermediate molecules
are referred as prostaglandin endoperoxides ( PGG and PGH).
Two separate genes encodes two PGH synthases : one is a constitutive enzyme
found virtually in all tissues, termed as PGH synthase 1 or Cyclo-oxygenase 1.The
second enzyme called PGH synthase 2 or COX 2 Which is inducible and is markedly
upregulated during cellular differentiation by cytokines or hormones.

22
Figure 7 : Eicosanoid synthesis pathway

23
Figure 8 : Prostaglandin Chemical Structure and Synthesis

24
Figure 9 : Arachidonic Acid Pathway

25
Figure 10 : Prostaglandin and Thromboxane Synthesis Pathway

26
PHARMACOLOGY OF MISOPROSTOL
History [35]
PGE1 analogue Misoprostol (15-deoxy-16-hydroxy-16-methyl PGE1),
developed in 1973 by Searle for the treatment and prevention of gastric ulcer. First
marketing authorization was given in 1985 and now more than 80 countries approved
its use, mostly under the brand name of Cytotec.
Figure 11 : Chemical structure of Misoprostol

27
Figure 12 : Geographic distribution on the approval of Misoprostol.
Available in market as 200 mcg, 100 mcg, 50 mcg and even 25 mcg [35]
Licensed indication for Misoprostol includes[35]
Gastric ulcer
Vaginal suppository for induction of labour

28
Misoprostol wears the crown among prostaglandin analogues in the market
due to the following advantages over other prostaglandins:
The licensed doses used for abortion has limited effect on the bronchi or
blood vessels.
Remains stable at room temperature, thus can be stored for many years.
Available for oral, vaginal, sublingual or rectal administration.
Cost-effective [35]
.
Mechanism of action / Uses [35, 36]
Enhances the gastric mucosal defence mechanism and helps in the healing as
well as prevention of gastric ulcer, especially NSAID induced gastric ulcer
and thus exerts its cytoprotective action.
Used for treatment of missed and incomplete miscarriages.
Helps in induction of abortion and cervical preparation before uterine
instrumentation as it encourages collagen disintegration and dissolution.
Used in late pregnancy for induction of labour and prophylaxis for the
treatment of postpartum hemorrhage through its uterotonic action.

29
Pharmacokinetics [35-37]
Table 4: Absorption kinetics of Misoprostol.
Absorption[35-37]
Rapid as well as complete absorption following oral intake.
The rate of absorption is reduced by food, whereas the extent of absorption is
food independent.
Associated antacid use reduces the total bioavailability.
Vaginal administration causes regular uterine contractions in contrast to oral
route where the chances of tonic contractions are more.
Peak plasma levels are obtained in 12 minutes whereas terminal half life is 20-
40 mins
Figure 13 : Mean plasma concentrations of Misoprostol acid over time with oral
and vaginal administration.

30
Table 5: Metabolism and Excretion of Misoprostol.
Metabolism and Excretion [35-37]
Misoprostol is converted in to its pharmacologically active metabolite,
Misoprostol free acid by liver de-esterification enzymes.
It is free of drug interactions and it does not induce the hepatic Cytochrome P-
450 enzyme system.
Further oxidation of Misoprostol occurs in liver.
Mainly excreted in urine.
Misoprostol free acid is known to get excreted in breast milk.
Table 6: Distribution profile of Misoprostol
Onset and duration of action for various routes of administration [37-40]
Route of administration Onset of action Duration of action
Oral 8 ms approx 2 hrs
Sublingual 11 ms 3 hrs
Vaginal 20 ms 4 hrs
Rectal 100ms 4 hrs

31
Figure 14 : Uterine activity in Montevideo Units induced by Misoprostol given
at different routes of administration.
Pharmacokinetics in breast milk [38-40]
Following oral administration Misoprostol free acid is found in breast milk
within 30 minutes.
Peak concentration in breast milk will be attained in 1 hour, whereas this peak
concentration level is found to be less than maternal plasma level.

32
Misoprostol free acid level found in breast milk will be undetectable 4-5 hrs
following feeding.
Side effects[40-43]
Abdominal pain, fever, shivering, nausea, vomiting and diarrhea are the common
adverse effects which are dose-dependent and self limiting.Very high doses of
Misoprostol along with Trifluoperazine has been reported to cause rhabdomyolysis,
hyperthermia, hypoxemia.
Teratogenicity[43-45]
Congenital facial palsy (Moebius syndrome) has been reported in the fetus of women
who took high dose Misoprostol in first trimester.Transverse limb defects,
arthrogryposis, hydrocephalus have been documented in some studies as rare
teratogenic effects.
Contraindications for medical management with Misoprostol[45-47]
HB < 10 gm/dl,
Previous cesarean section,
Previous Myomectomy,
Uterine perforation,
Cardiac anomaly,
Bleeding disorders,
Anti‐coagulation therapy,
Steroid treatment,
Renal disease.

33
Mifepristone - Misoprostol interval regimen.
The regimen approved by United states Food and Drug administration for
medical abortion up to 49 days is 600 mg of oral Mifepristone followed by 400 mcg
of vaginal Misoprostol 48 hours later with a success rate of 92%.This 36-48 hours is
recommended based on the fact that Mifepristone increases the sensitivity of
myometrium to prostaglandins which starts within 24 hours and it increases till 36-48
hrs. Compared with this regimen alternative evidence based regimens such as 200 mg
of oral Mifepristone followed by 800 mcg of vaginal Misoprostol 24 hours later
shows a success rate of 95-99% up to 63 days of gestation.24 hour regimen has
proved to be more effective regimen which needs lesser time for expulsion with fewer
side effects, low costs and more convenient [46, 47]
.
A Multicentre, randomized, control trial ( i.e) Comparison of Misoprostol 6
to 8 hours versus 24 hours after Mifepristone for abortion by Crenin et al reported the
overall success rate was 96% ( CI 94–97) in the 6-8 hrs interval group, compared to
98% (CI 97–99) in the 24 hrs interval group with(p= 0.005).Regarding side effects,
women in the short interval group experienced significantly lesser side effects than
those in the standard interval group. Assessment of pain and amount of bleeding were
similar in both the groups. About 90% of women in each group considered the
regimen they had received to be acceptable.Thus crenin concluded that 6-8 hrs
interval between Mifepristone and Misoprostol was equally efficacious alternative to
24 hour regimen with significantly less side effects and more acceptability[48].

34
A Recent prospective randomized control study done by Chaudhri P et al in
2014 in which he compared 24 hours versus 48 hours interval between Mifepristone
and Misoprostol for termination of pregnancy in 98 healthy women reported the
success rate of 95% in 24 hour group and 93.6% in 48 hour group with the p value of
0.38.The mean induction to abortion interval was (8.6±4.1hours in 24 hr group versus
8.7±γ.9hours; P=0.γ7 in 48 hr group). He reported longer induction to abortion
interval in nulliparous women in both the groups.He concluded that 24 hour interval
between Mifepristone and Misoprostol is equally efficacious to standard FDA
approved 48 hrs regimen for termination of pregnancy [49]
.
An open randomized trial done by Maarit mentula et al in 2011 which
included 227 women undergoing medical termination where oral Mifepristone (200
mg) was followed by vaginal Misoprostol (400 mcg) after one day versus two
days.He reported a longer induction to abortion interval of 8.5 hours (in 24 hours
group)versus 7.2 hours(in 48 hour group) with P value of 0.038.He reported 1 hr
longer induction abortion interval in 24 hour group.The rate of surgical evacuation
was higher in the 2-day group i.e., 37% in 48 hour group versus 25% in one day group
with 95% confidence interval.Finally Maarit Mentula et el concluded as “Both one-
and two-day dosing intervals seem to be suitable for medical termination of
pregnancy.However, evaluated on the basis of surgical evacuation, the one-day
interval could be supported as an option” [50].
A study conducted by Crenin et al in 2007 which includes 1128 women with
gestational age up to 63 days were given Mifepristone and vaginal Misoprostol
together versus 24 hour later showed that complete abortion rate did not differ greatly

35
among the two treatment groups (group1–Mifepristone and vaginal administration of
Misoprostol done together had complete abortion rate of 95.1%, CI 93-96.8%; group
2 (24 hrs later), 96.9% success rate with CI 95.1-98.2% and P value of.003) [51]
.
Chen Ay et al in their study included 1080 women up to 63 days period of
gestation. Women were given 200 mg oral Mifepristone followed by 800 mcg vaginal
Misoprostol administered on one or two dosing schedules. 6-8 hours was assigned as
group 1 whereas 24 hours was assigned as group 2.Participants recorded daily
bleeding in a diary over a period of 5 weeks. He concluded that total duration of
bleeding ranged from 1 to 54 days (median 7 days), and spotting ranged from 1 to 80
days(median 56 days) in both groups. Neither duration of bleeding nor duration of
spotting were related to the interval between Mifepristone and Misoprostol. Increased
gestational age was correlated with longer duration of bleeding (p=.007) and spotting
(p<.0001), and nulliparity was associated with longer bleeding time (p=0.003) [52]
.
A prospective randomized trial evaluated by Schaff et al who studied the
outcomes of 2, 255 pregnant women with gestation age up to 56 days of gestation
undergoing medical abortion using the following regimen: 200 mg oral Mifepristone
followed by 800 mcg vaginal Misoprostol self administered, 24 hours, 48 hours and
72 hours later. A second dose of Misoprostol was administered if the abortion was
not complete following 8 days after Mifepristone.He concluded that “complete
abortion rates were 98% (CI: 97-99%) for Misoprostol after 1 day, 98% (CI: 97-
99%) for those using Misprostol after 2 days, and 96% (CI: 95-97%) among those
using Misoprostol after 3 days. Abdominal cramps and nausea were the most

36
common side effects reported across all groups and over 90% of women found the
procedure to be acceptable” [53].
A study done by Ashok et al regarding the effect of Mifepristone on cervical
ripening, dilatation and softening has found that the priming effect of Mifepristone
after 48 hours is significantly more pronounced than after 24 h [54].
Heikinheimo et al in their study showed that women who received
Mifepristone 24 hour before the procedure had a significantly lower baseline cervical
dilatation (7.5 mm vs. 8.3 mm; p value of.05) and required greater mechanical force
to dilate the cervix than women who received Mifepristone 48 hour before the
procedure. Similarly, the mean interval from induction to expulsion was significantly
shorter when prostaglandins was initiated 48 h (6:20 h) after Mifepristone compared
to 24 hour (7:25 h).This is in contrast to the findings of other studies documented
prior[55]
.
Review studies on Medical methods of abortion.
The review study conducted by Weeks et al which reviews many randomized
control trial suggests that vaginal Misoprostol when compared with placebo speeds
up the miscarriage process (complete or incomplete), it also reduces the need for
curettage. No significant side effects have been documented in this study. Lower
doses of Misoprostol have found to be inferior in efficacy to single dose of 800 mcg
Misoprostol which proves more effective [56]
.

37
Elrafey et al in his partially randomized study compared surgical and medical
evacuation and found that 20% of women expressed a strong preference for medical
management. The main reasons given for their choice were ‘avoidance of anaesthesia’
and the feeling of being ‘more in control’ [57].
Hinshaw et al documented higher success rate of up to 96% associated with
high-dose vaginal Misoprostol for incomplete miscarriage [58]
.
Two randomized control trial done by Tang, Ngoc NT suggested that the oral,
sublingual and vaginal routes of Misoprostol are equally effective. In one study done
by Tang et al, missed miscarriages managed with either oral or sublingual
Misoprostol showed success rates of 87.5% (95%CI 74–95%) in both groups. This
randomized controlled trial by Ngoc et al where women, managed with either oral or
vaginal Misoprostol, also showed no significant difference in successful outcome
(oral 89% versus vaginal 92.9%)[59, 60]
.
The randomised trial done by Demetroulis and Trinderet al showed no
statistical difference in efficacy between surgical and medical evacuation for
incomplete miscarriage and for early fetal demise at gestations less than 71 days or
sac diameter less than 24mm. Patient acceptability for both methods was equal.
There was a reduction in clinical pelvic infection after medical evacuation (7.1 versus
13.2%, P < 0.001).With increasing gestation and sac size, acceptability of medical
methods fell to 85% [61, 62]
.

38
Studies done by Nelison, Wieringaet al concentrating on variety of doses,
regimens and routes of administration have found that lower doses and oral
administration are less effective, and greater side effects have been associated with
sublingual administration. Thus the ongoing studies are still inconclusive regarding
the optimal doses and routes of administration[63, 64].
Marwan Odeh et al reported that success rate of medical treatment for missed
abortion is highly varying, ranging from 13% to 94%.He also reported that this
variance is due to the fact that success rate in medical management is largely
influenced by many factors such as lack of standard parameters to predict the
success, difference in the regimens used, and due to different definitions for
successful outcome [65, 66]
.
He also concluded that there is no correlation between gestational sac volume
and the success rate of medical treatment for early pregnancy failure, while the factors
such as previous term pregnancy, higher number of previous pregnancies and a higher
blood hCG level adversely affect the success rate of medical treatment for early
pregnancy failure.The study also suggests this factors should be explained to the
patient during pre treatment counseling only [65, 66]
.

39
Figure 15 : Three-dimensional ultrasound image showing measurement of the
gestational sac volume in an 8 week missed abortion [66]
The American College of Obstetricians and Gynecologists recommends
800μg vaginal or 600μg sublingual Misoprostol for missed abortions; sublingual
administration can be repeated every 3 hours for two additional doses. The reported
success rate for vaginal administration of Misoprostol is up to 97%. More prolonged
waiting periods or repeated dosing leads to higher success rates [67, 68].

40
Study done by Ashok et al to evaluate the efficacy of 200 mg Mifepristone
followed 36-48 hours later by 800 mcg vaginal Misoprostol for termination of
pregnancies up to 63 days period of gestation. The complete abortion rate was
97.5%. Two percent aborted following Mifepristone administration alone. The
median induction abortion interval observed was 4.15 hours [69]
.

MATERIAL AND METHODS

41
METHODOLOGY
SOURCE OF DATA
We conducted a Prospective case-control study in the Department of
Obstetrics and Gynaecology, Adichunchanagiri institute of medical sciences,
B.G.Nagara from the period November 2013 to October 2015.We included all
pregnant women with gestational age of less than 9 weeks diagnosed with intrauterine
pregnancy failure as confirmed by ultrasonogram and undergoing medical abortion
and who are willing for follow up. Sample size was 120 ( among 135 patients
screened, 120 fulfilled the inclusion criteria- 60 in study group and 60 in control
group).Study group includes women who were given Vaginal Misoprostol 24 hours
following Mifepristone whereas 48 hour interval between Mifepristone and
Misoprostol stands as control group.
Exclusion criteria
1. Women in whom ectopic gestation is suspected (even clinically).
2. Women who are not willing for follow up protocols.
3. Breast feeding mothers.
4. Women with haemoglobin of lessthan 10 gm/dl.
5. Women with previous cervical surgery - scarred cervix.
6. Women with previous scar in the uterus.
7. Women with asthma/glaucoma/adrenal insufficiency/poorly controlled
seizures/cardiovascular disease/coagulopathy.
8. Women on systemic corticosteroid therapy/anticoagulant therapy.
9. Pregnancy with IUCD in situ.

42
PROCEDURE:
Informed written consent of the patient was taken after explaining the
complete procedure in patients own understandable language.
PREPARATION OF THE PATIENT
Complete history was taken and thorough general and systemic examination
was carried out.
Speculum and vaginal examination was done in all the patients.
Patients were counselled about the method they were allocated and side effects
of the drug.
Sequential allocation was done in the ratio of 1:1.
Subjects in study arm was given 200 mg oral Mifepristone followed by 800
mcg vaginal Misoprostol after 24 hours, where as those in control arm was
given 200 mg oral Mifepristone followed by 800 mcg of vaginal Misoprostol
after 48 hours.
Women who did not have bleeding in the first 8 hours following 800 mcg
Misoprostol were given subsequent 200 mcg of vaginal Misoprostol.Doses
were repeated at 4th
hourly interval to a maximum Misoprostol dose of
1200mcg.
All subjects were informed about the signs and symptoms of expulsion and
need for follow-up.
All women was given a 24 hour contact telephone number for any post
treatment advice.

43
They were asked to come for follow-up after 14 days when transvaginal
ultrasound (TVS) was performed to confirm whether expulsion process was
complete.
If retained products of conception was documented on check scan, depending
on the amount of retained products of conception and amount of bleeding,
Curettage was performed and products sent for histopathological
examination.

44
STATISTICAL ANALYSIS
Statistical Methods: Descriptive and inferential statistical analysis has been
carried out in the present study. Results on continuous measurements are
presented on Mean SD (Min-Max) and results on categorical measurements
are presented in number (%). Significance is assessed at 5 % level of
significance.
Chi-square test/ Fishers exact test has been used to find the significance of
study parameters on categorical scale between two groups.
Student t test (two tailed, independent) has been used to find the significance
of study parameters on continuous scale between two groups (Inter group
analysis).
The P value was calculated and if P value of less than or equal to 0.05 was
considered as statistically significant.

RESULTS

45
RESULTS
In this Prospective case-control study conducted in the Department of
Obstetrics and Gynaecology, Adichunchanagiri institute of medical sciences, from
the period of November 2013 to October 2015, 135 pregnant women with gestational
age of less than 9 weeks diagnosed with intrauterine pregnancy failure as confirmed
by ultrasonogram and undergoing medical abortion were screened and 15 patients
were excluded as per exclusion criteria .
Totaly 120 patients who fulfilled the inclusion criteria was taken (60 in study
group and 60 in control group).Study group includes women who were given 800
mcg of Vaginal Misoprostol 24 hours following Mifepristone whereas 48 hour
interval between Mifepristone and Misoprostol stands as control group.
Analysis of results were done with respect to the following factors,
Age distribution
Parity status
Socioeconomic status
Misoprostol Application – Abortion interval
Need for subsequent doses of Misoprostol
Complete abortion rate
Curettage (Failure) rate
Side effects profile
Patient’s preference

46
Age distribution
Majority of patients who underwent medical abortion (both in study as well as
control group) were in the age group of 20-30 years contributing 80.8%, which was
followed by patients in age group 31-40 years, constituting 12.5%.
Mean value for age in control group is 24.89 ±3.74 and in study group it is
25.35 ± 3.84 years.
10 % of women were in the elderly age group of 31-40 yrs in control group
whereas 15 % of women were in the age group of 31-40 yrs in the study group.
5 % of women in control group and 8 % of women in study group belongs to
teenage group.
Table 7: Age distribution of patients studied
Age in yrs
Study Group
(n=60)
Control
Group
(n=60)
Total
(n=120)
<20 5(8.3%) 3(5%) 8(6.6%)
20-30 46(76.7%) 51(85%) 97(80.8%)
31-40 9(15%) 6(10%) 15(12.5%)
Mean ± SD 25.35±3.84 24.89±3.74 25.1±3.73
Samples of age are matched with P = 0.507,Chi Square test

47
Graph 1: Age distribution of patients studied
Socioeconomic status (According to Modified B.G. Prasad classification – reviewed
on May 2014). 57% of patients in study group and 47% of patients in control group
who underwent medical abortion belongs to lower middle class, who cannot afford for
multiple clinic visits, and surgical procedures.
Majority of women in lower middle class preferred 24 hours
regimen , as the process of abortion will be completed in short span of time so that
0
10
20
30
40
50
60
70
80
90
20-30 31-40
control group
study group

48
their daily work and earnings wont get affected . Whereas women in middle class and
upper middle class did not had any specific preference to 24 hour regimen whose life
is not totally dependent on their daily wages.
Obstetric index
73.3% of women who underwent 48 hour interval regimen and 66.6% of women
who underwent 24 hour interval regimen were Multiparous with the P value of 0.425
which is not significant. 26 % of the patients who underwent 48 hour interval regimen
and 33.3% of the patients who underwent 24hour interval regimen were Primigravida.
Table 8: Obstetric Index
Obstetric Index
Study Group
(n=60)
Control
Group
(n=60)
Total
(n=120)
Multigravida 40(66.6%) 44(73.3%) 84(70%)
Primigravida 20(33.3%) 16(26%) 36(30%)
P=0.425, Not significant, Chi-Square test

49
Graph 2: Obstetric Index
0
10
20
30
40
50
60
70
80
Multigravida Primigravida
Control group
Study group

50
Period of gestation
The main indication for which medical abortion was done in our study is
early pregnancy failure (Blighted ovum) and missed abortion. Majority of patients
were in the gestational age between 8-9 weeks with 46.6 %.P value documented is
0.934 which is not significant.
Table 9: Gestational age (weeks)
Gestational age
(weeks)
Study Group
(n=60)
Control
Group
(n=60)
Total
(n=120)
< 7 17(28.4%) 18(30%) 35(29.1%)
7 to < 8 14(23.3%) 15(25%) 29(24.1%)
8-9 29(48.3%) 27(45%) 56(46.6%)
P=0.934, Not significant, Chi-Square test

51
Graph 3 : Gestational age (weeks)
0
10
20
30
40
50
60
< 7 wks 7 to < 8 wks 8-9 wks
Controlgroup
Study group

52
Misoprostol application to Abortion interval
71.6 % of patients in control group and 68.3 % of patients in study group
expelled the abortus in less than 8 hours following the vaginal administration of 800
mcg of Misoprostol. Whereas 16.6 % of patients in control group and 21.7 % in study
group expelled in 8-12hrs. 11.8 % of women in 48 hour group and 10 %in 24 hour
group required time interval of 13-24 hours for their expulsion with P value of 0.772
which is not significant.
Table 10: Misoprostol application to abortion interval (hours)
P value of 0.772 , Not significant, Chi-square test
Misoprostol application to
abortion interval (hrs)
Study Group
(n=60)
Control
Group
(n=60)
Total
(n=120)
<8hrs 41(68.3%) 43(71.6%) 84(70%)
8-12 hrs 13(21.7%) 10(16.6%) 23(19.2%)
13-24 hrs 6(10%) 7(11.8%) 13(10.8%)

53
Graph 4: Misoprostol application to abortion interval (hours)
0
10
20
30
40
50
60
70
80
< 8 hrs 8-12 hrs 13-24 hrs
Control group
Study group

54
Doses of Misoprostol
61% of women in control group and 70 % of women in study group required a
single dose of 800 mcg of Misoprostol for their expulsion. Whereas 20 % of patients
in control group and 23.3% in study group required an additional dose of 200 mcg of
Misoprostol. 18.3 % of patients in control group and 6.6 % in study group required 3
doses of Misoprostol (including the first dose of 800 mcg) and they expelled in 13-24
hrs.
Table 11: Number of doses of Misoprostol
No of doses of Misoprostol Study Group
(n=60)
Control
Group
(n=60)
Total
(n=120)
1(800 mcg) 42(70%) 37(61.6%) 79(65.8.%)
2(800+200 mcg) 14(23.3%) 12(20%) 26(21.6%)
3(800+200+200 mcg) 4(6.6%) 11(18.3%) 15(12.5%)
P=0.154, Not significant, Chi-Square test

55
Graph 5 : Number of doses of Misoprostol
0
10
20
30
40
50
60
70
80
1 dose 2 doses 3 doses
Control group
Study group

56
Success rate
Out of 120 patients who underwent medical abortion, 7 patients did not turn
up for check scan, thus their expulsion status was not known. Out of 113 patients
who underwent check scan 81% of women in control group and 78 % of women in
study group had complete expulsion.
18 % of patients required curettage in study group, whereas 10 % of patients
required curettage in control group. The P value obtained is 0.29 which is not
significant.
Table 12: Success rate
USG
Study Group
(n=60)
Control
Group
(n=60)
Total
(n=120)
Complete Expulsion 47(78.3%) 49(81.6%) 96(80%)
Incomplete Expulsion 11(18.3%) 6(10%) 17(14.1%)
Lost follow up 2(3.3%) 5(8.3%) 7(5.8%)
P=0.2904, Not significant, Fishers exact test.
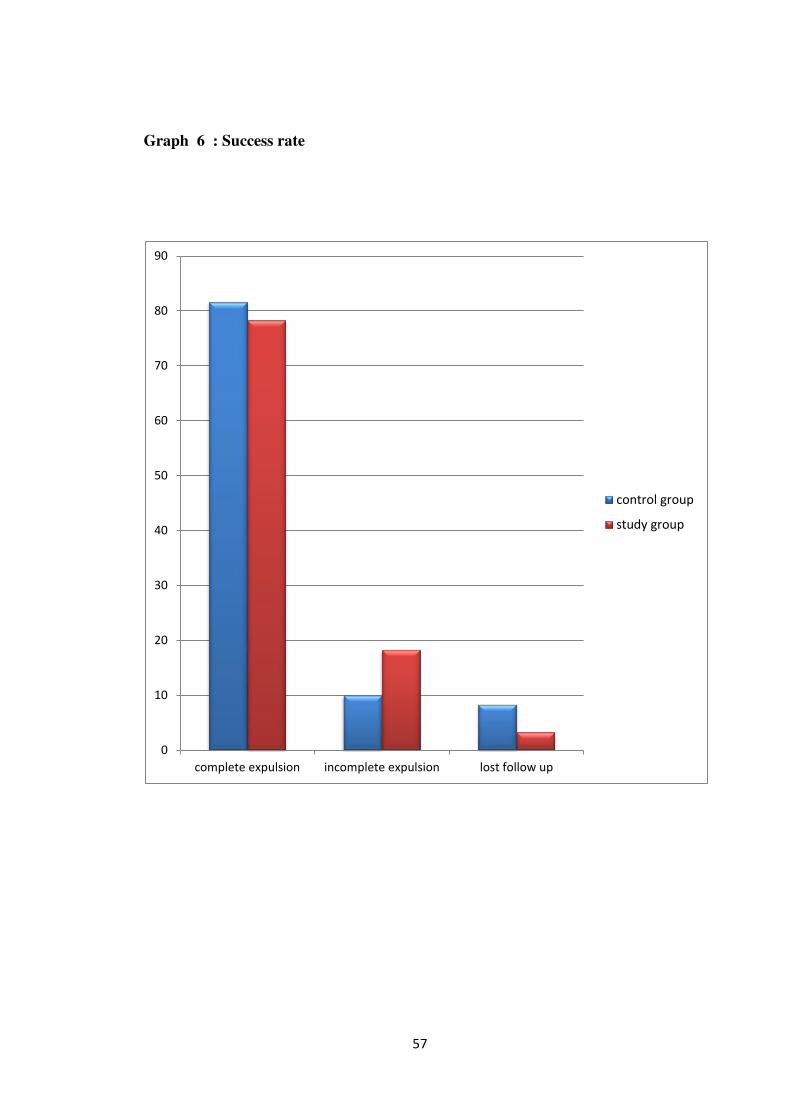
57
Graph 6 : Success rate
0
10
20
30
40
50
60
70
80
90
complete expulsion incomplete expulsion lost follow up
control group
study group

58
Table 13: Surgical evacuation
Curettage
Study Group
(n=58)(60-2)
Control
Group
(n=55)(60-5)
Total
No 47(81%) 49(89%) 96(84.9%)
Yes 11(18.9%) 6(10.9%) 17(15%)
P=0.2959, not significant, Fishers exact test.
Side effect profile
Regarding side effect profile 21.6 %, 1.6%, 1.6 %, 11.6%, 5 % of women in study
group had diarrhea, fever with chills, vomiting, fever and chills. Most common side
effect which patients encountered in study group was diarrhoea.
In control group 6.6 %, 3.3 %, 11.6 %, 3.3 %, 8.3 % of women in had
diarrhea, fever with chills, vomiting, fever alone and chills alone respectively. Most
common side effect in control group was vomiting. Very few of the patients with side
effects in both the groups required symptomatic treatment. Others had spontaneous
relief of symptom followed by completion of procedure.
There was no statistically significant difference in the percentage of side effect
profile between the study and control groups.

59
Table 14: Side effect profile
Side effects Control Group
(n=60)
Study Group
(n=60)
Total
(n=120)
Number of patients with side
effects 20(33.3%) 25(41.6%) 45(37.5%)
Diarrhea 4(6.6%) 13(21.6%) 17(14.1%)
Fever with Chills 2(3.3%) 1(1.6%) 3(2.5%)
Fever 2(3.3%) 7(11.6%) 9(7.5%)
Vomiting 7(11.6%) 1(1.6%) 8(6.6%)
Chills alone 5(8.3%) 3(5%) 8(6.6%)
P=0.234, Not significant, Chi-Square test
Graph 7: Side effect profile
0
10
20
30
40
50
60
70
Nil Yes
control group
study group

60
Graph 8: Percentage distribution of Side effects
0
5
10
15
20
25
DiarrheaFever with
chillsFever
VomitingChills alone
control group
study group

61
Figure 16 : Study Summary
Sample size-120
Study group
60
Mean induction abortion
interval-5-6 hrs
Success rate --78.3%
Curettage rate--18.3%
Control group
60
Mean induction abortion
interval----6-7 hrs
Success rate--81.6%
Curettage rate-10-%

DISCUSSION

62
DISCUSSION
Medical abortion has been a revolution in obstetrics practice, for the ease and
safety it provides to the clinician and the patient, as well as its role in preventing
deaths due to unsafe abortions in developing countries like India [70]
.
The challenge of medical abortion, therefore, is to find the best balance
between Mifepristone and Misoprostol (i.e) to find the optimal dose, route of
administration, interval between the two drugs, and knowledge on side effect profile
so that highest level of efficacy and good tolerance will be maintained[71, 72, 73]
.
Though several studies focusing on shorter interval between Mifepristone and
Misoprostol are available in the literature, stratification of 24 hour versus 48 hour
regimen and efficacy in both the groups in early pregnancy has not been researched in
detail.
Studies done by Shi Ye et al and Swahn et al showed that Mifepristone dosage
between 100 mg and 800 mg attains a constant level in serum, and the serum levels
are less variable, based on this fact 200 mg of Mifepristone was chosen for this
study[74, 75]
.
Rationale behind vaginal administration of Misoprostol in this study is due to
its higher success rate of 95% compared with 87% success rate with oral Misoprostol,
as well as due to its slow rise and sustained action for a long period[70]
.

63
Half of the women who received Misoprostol after 48 hours started having
bleeding as early as 3 hours and they continued to bleed until they expel, thus
reducing the time interval results in lesser time needed for expulsion, lesser duration
of exposure to undesirable side effects[70, 76]
.
Mean age distribution
Mean age of patients who underwent medical abortion in our study was
25.1±3.73 in the range of (20-30 yrs) which was comparable with the study conducted
by Verma et al in which mean age distribution in study group is 28.14 yrs and 27.92
yrs in control group in the range of 21-30 yrs. Mean age distribution of present study
is also comparable to the study conducted by Sonal k et al (26.44 yrs), Von Hertzen et
al (26.4 yrs)and Guest et al (25.7 yrs).Minority of patients who underwent medical
abortion for the indication of early pregnancy failure belongs to teenage group, but
none of them had any complications which reinforces the fact that medical abortion
saves the patient from the complications of unsafe abortions in developing
countries[70, 77-79]
.
Table 15: Comparison of Mean age distribution
Study
Maternal mean age in
years in 24 hour group
Maternal mean age in years
in 48 hour group
Present study 25.35±3.84 24.89±3.74
Von hertzen et al78
26.4± 5.7 26.1± 5.4
Verma et al70
24.6± 5.1 25.4± 5.7
Schaff et al80
28(27.4-28.3) 28(27.5-28.4)
Mentula et al81
23(20-27) 23(20-29)

64
Parity distribution
70% of women who approached for medical abortion were Multiparous.
Among 84 multiparous women who underwent medical abortion in both study and
control group, 12 patients underwent curettage whereas 72 patient expelled
successfully with drugs. Among the total number of women who underwent curettage
in our study 70.5 % of them were multiparous and 29.4 % were nulliparous which is
controversial to the fact that failure rate of medical abortion in nulliparous women
will be more compared to multiparous.
The parity distribution in the present study is comparable to the study
conducted by Verma et al, Von Hertzen et al, Guest et al and Schaff et al where
majority of the women who approached for medical abortion were
multiparous,[70,78,79,80]
Table 16: Comparison of Parity distribution
Study Study group
(24 hour group)
Control group
(48 hour group)
Present study 66.6% 73.3%
Von hertzen et al78
68% 75.6%
Schaff et al80
63.5% 70.3%

65
Gestational age in weeks
Cut off for the gestational age taken in our study is 63 days where the success
rate of medical abortion is found to be high (80%). 45% of women in control group
and 48.3 % of women in study group belongs to 8-9 wks of gestation which is
comparable to Von Hertzen et al where also majority of women in both study and
control group belongs to 7-9 wks POG.
Chaudri et al proposed the rate of successful abortions with the 24 hour and
48 hour dosing intervals (95.8% and 93.6%, respectively; P=0.γ8), at 7-9 weeks
period of gestation[70, 78, 79, 82]
.
Table 17: Comparison of gestational age.
Study Gestational age in
weeks
Present study 8-9 weeks
Verma et al70
7-9 weeks
Von Hertzen et al78
7-9 weeks
Guestet al79
6-8 weeks
Chaudri et al82
7-9 weeks

66
Induction – Abortion interval
Mean induction to abortion interval in study group was in the range of 5-6 hrs
versus 6-7 hrs in control group with P value of 0.772 .There was no statistically
significant difference between the two which implies the women can be given a
choice of 24hrs regimen which helps her to complete the abortion process within
short span of time. This shorter induction abortion interval in study group is
comparable to the interval reported by Verma et al (4 hrs), Von Herzen et al (4-5
hrs)[70, 78]
.
Whereas it is contrast to longer induction to abortion interval in 24 hour group
than in 48 hour group as reported by Heikinheimo et al, Mentula et al, Hou et al. The
shortest induction abortion interval with the highest complete abortion rate in our
study can also be attributable to 800 mcg of Misoprostol for induction dose as study
done by Ashok et al, Carbonell et al, Chai et al summarizes that high dose of
Misoprostol for induction increases abortion rate with shorter induction abortion
interval [55, 81-85]
.
Table 18: Studies supporting shorter induction abortion interval in 24-Hour
group.
Present study 5-6 hrs
Verma et al70
4 hrs
Von Herzen et al78
4-5 hrs
Schaff et al 80
4-5 hrs

67
Table 19: Studies reporting longer induction abortion interval in 24-Hour group
compared to 48 hr group.
Study 24 hour Group 48 hour group
Hou et al82
7 hrs 6.7 hrs
Heikinheimo et al55
7.4 hrs 6.3 hrs
Mentula et al81
8.5 hrs 7.2 hrs
Complete abortion rate / Success rate
Complete abortion rate with 24 hours was 78.3% compared to 81.6% in 48
hours regimen with P value of 0.29 in our study.The difference in abortion rate
between the two groups is statistically negligible and helps us to prove that 24 hrs
regimen is equally efficacious in achieving complete abortion rate compared to the
standard 48 hour regimen.
This statistically insignificant difference in complete abortion rate between 24
and 48 hour group proved in this study is comparable with the study done by Verma
et al, Von hertzen et al, Schaff et al[70, 78, 80]
.

68
Table 20: Comparison of Success rate
Study 24 hour regimen 48 hour regimen
Present study 78.3% 81.6%
Verma et al70
94% 95%
Von Hertzenet al78
94% 92.5%
Schaff et al80
98% 98%
Mentula et al81
95% 94%
Side effect profile
Majority of women in both the study and control group had diarrhea and
vomiting as their major side effect, next to abdominal cramps, attributable to
Misoprostol which was managed with non-narcotic analgesia. None of the patients
had any life threatening complications.
Thus the safety profile of 24 hour regimen reported in our study is supported
by other studies conducted by Verma et al, Von hertzen et al, Guest et al, Hou et al
and Mentula et al[70, 78, 81, 82].

69
Based on the above three factors 24 hour regimen which achieves complete
abortion rate with shorter induction abortion interval without compromising its safety
profile can be safely prescribed for the women who approaches for medical abortion
as an alternative to 48 hour group.

70
Table 21: Summarizing vital factors of our study with other studies on shorter interval regimen.
Serial no: Our study
Efficacy of Misoprostol
administration 24 hours
after Mifepristonefor
termination of early
pregnancy.
Verma et al [70]
Two mifepristone doses and
two intervals of misoprostol
administration for termination
of early pregnancy: a
randomized factorial
controlled equivalence trial.
Von Hertzen
et al[78]
Randomised control
trial comparing the
efficacy of same-day
administration of
mifepristone and
misoprostol for
termination of
pregnancy with the
standard 36 to 48 hour
protocol
Guest J et al[79]
Vaginal Misoprostol
Administered 1, 2, or
3 Days After
Mifepristone for Early
Medical Abortion-A
Randomized Trial
Schaff et al[80]
1.Type of study Prospective Case-control
study
Prospective case-control
study
Randomised
control trial
Randomised control trial Prospective
Randomized
Trial
2.Year
of Study
2013-2015 2011 2009 2007
2000
3.Sample size
120
200
2181
450
2295

71
4.Mean Age
20-30yrs
In 48 hrs gp –
24.89±3.74
In 24 hrs gp
-25.35±3.84
P-0.507
21-30 yrs in both the
groups
26.4 yrs (5.7) in 24 hrs group.
26.1 yrs(5.4)in 48 hrs group
25.7 yrs (6.5) in same
day
24.4 (6.4)yrs in 48 hrs
group
28(27.4-28.3)yrs
in 24 hrs group
28(27.5-28.4) yrs
in 48 hrs group
5.Parity
Index
73.3% of women who
underwent 48 hour interval
regimen and 66.6% of
women who underwent 24
hour interval regimen were
Multiparous .
96% and 99% of women
in study and control
group are multiparous
Majority of women in this
study were nulliparous.
91% of the patients in
study group(same day)
and 88 % of the patients
in control group did not
had any previous
miscarriages
P value of nulliparous
women-0.52.
P value of multi who
did not had any
previous abortions -
0.23
Multiparous women
outweighed the
number of nulliparous
women.

72
6.Average
period of
gestation
Range –
8-9
Wks
Range -
4‑9 weeks
Range of
7-9 wks
Range of
6-8wks
Range of 6-7 wks
(45.2-46.3 days)
7.Mean
Induction
abortion
interval
5-6 hrs in
24 hrs group
6-7 hrs in 48 hrs
group
P value-0.772
4 hrs in 24 hrs group.
4-5 hrs in 48 hrs group.
P value-0.25
Both intervals were equivalent
within a 5% margin.
Range of 4-7 hrs
4-6 hrs in both the
groups
4-5 hrs in both the
groups. There were no
differences among
groups.
P value =0.05
8.
Success rate
(or)
complete
abortion rate
78.3% in 24 hrs group and
81.6% in 48 hrs group
P value of 0.29
94% in 24 hrs group
95% in 48 hrs group
P value -0.7
94% in 24 hrs group.
92.5 % in 48 hrs group
79 % in same day
regimen.
92 % in 48 hours group.
98% in 24 hr group
and
98%
at 2 days,

73
9.Side effect
Profile
No Statistically Significant
difference in both the
groups.
P value of
0.234
P value of vomiting is
0.06.
P value of diarrhea is 0.6.
Majority of patients who
had side effects belongs
to 48 hr regimen
P value of vomiting is 0.6380
P value of diarrhoea is
0.0805.
Majority of patients had
nausea as a common side
effect next to abdominal pain
and they belong to 48 hr
regimen.
With P value of 0.6203.
Relative risk of 1.21 for
nausea, 1.17 for
vomiting and 1.36 for
diarrhea.
Majority of patients in
both the groups had
nausea, vomiting and
diarrhea as their side
effect and they belong to
same day regimen.
13 unexpected
or serious adverse
events occurred:
6 in those
using Misoprostol
after 1 day; 4
in those using
it after 2 days;
and 3 in those
using it
after 3 days
10.
Patient s
Preference
70% of women strongly
agreed.
30% were neutral
Statistically not
Analysed
Not commented Women in the same day
regimen preferred
shorter time interval
which is more
acceptable than the 36 to
48 hour protocol.
Patients clearly
preferred the shortest
waiting time possible.
86% in 24 hr group
strongly agreed for
shorter interval regimen
compared to 79% in the
day 2 group

74
11.
Conclusion
Vaginal Misoprostol can be
safely administered 24
hours following
Mifepristone with
promising efficacy.
Efficacy of 24 h interval
was similar to that of 48
h interval for medical
abortion of pregnancy
less than 9 weeks without
compromising the safety
Both the 24 and 48 hour
regimens are equally
efficacious to achieve
complete abortion in early
pregnancy.
Oral Mifepristone 200
mg followed by vaginal
Misoprostol 800
micrograms after 6-
8hours is not as
effective at achieving a
complete abortion
compared with the 36 to
48 hour protocol.
Vaginal Misoprostol,
800 µg, can be used
from 1 to 3 days after
Mifepristone 200 mg,
for early medical
abortion, and need not
be administered strictly
48 hours after
Mifepristone.

SUMMARY AND
CONCLUSION

75
CONCLUSION
Vaginal Misoprostol can be safely administered 24 hours following
Mifepristone instead of waiting for 48 hours.
Efficacy in achieving complete abortion rate is almost equal to 48 hours
regimen and most acceptable from patients side also.
Reduces multiple outpatient visits, without increasing the rate of surgical
evacuation.
Thus 24 hours regimen serves as an alternative to 48 hour regimen with equal
efficacy and acceptable side effect profile thereby helping women to complete their
abortion process in short span of time, with highest patient satisfaction and cost
effectiveness by preventing multiple clinic visits.

76
SUMMARY
The present study is a Prospective Case control study “Comparative study of
early (24 hours) versus late (48 hours) Misoprostol administration after Mifepristone
for termination of early pregnancy” was conducted at Adichunchanagiri Institute of
medical sciences from November 2013- October 2015.
All pregnant women of less than 9 weeks of gestation with early pregnancy
failure such as blighted ovum, Missed abortion which was confirmed
sonographically were included in this study (provided they fulfill our inclusion
criteria).
Subjects in study arm was given 200 mg oral Mifepristone followed by 800 mcg
vaginal Misoprostol after 24 hours, where as those in control arm was given 200
mg oral Mifepristone followed by 800 mcg of vaginal Misoprostol after 48 hours.
120 cases were studied.
Mean value for age in control group is 24.89 ±3.74 and in study group it is 25.35
± 3.84 years.
57% of patients in study group and 47% of patients in control group who
underwent medical abortion belongs to lower middle class.
73.3% of women who underwent 48 hour interval regimen and 66.6% of women
who underwent 24 hour interval regimen were Multiparous with the P value of
0.425 which is not significant.
Majority of patients were in the gestational age between 8-9 weeks contributing
46.6 %.
Mean Misoprostol application to abortion interval in study group was in the range
of 5-6 hrs versus 6-7 hrs in control group with P value of 0.772.

77
The Success rate in study group versus control group is 78.3 % versus 81.6 %
with P value of 0.29.
11/58 patients required curettage in study group compared to 6/55 in control
group.
Side effect profile between 24 hour vs 48 hour regimen was statistically
insignificant.
70% of women strongly agreed, 30% were neutral for 24 hr regimen.
Thus vaginal Misoprostol can be safely administered 24 hours following
Mifepristone compared to 48 hours regimen with equal efficacy.

78
RECOMMENDATIONS
1. Medical methods can be safely prescribed for women who undergoes abortion as
it reduces the complications of surgical evacuation of uterus in untrained hands of
rural India.
2. Since most of the women encountered in this study belongs to lower middle class,
who rely on daily wages for their life, instead of prolonging the abortion process
for 48 hours, it can be safely reduced to 24 hours, thus saving their precious time.

BIBLIOGRAPHY

79
BIBLIOGRAPHY
1. Organization WHO. Safe abortion: technical and policy guidance for health
systems. Geneva: WHO 2003;19(4):45-52
2. Chhabra R. Abortion in India: an overview. Demography India. 1996;25:83-92.
3. Malhotra A, Nyblade L, Parasuraman S, MacQuarrie K, Kashyap N. Realizing
reproductive choice and rights: abortion and contraception in India. International
centre for research on women (ICRW) 2003;7-25.
4. Elul B, Barge S, Verma S, Kumar N, Bracken H, Sadhvani H. Unwanted
pregnancy and induced abortion: data from men and women in Rajasthan, India:
Citeseer 2004;8:24-40.
5. Wilcox AJ, Weinberg CR, O'Connor JF, Baird DD, Schlatterer JP, Canfield RE, et
al. Incidence of early loss of pregnancy. N Engl J Med 1988;319(4):189-94.
6. Campion EW, Doubilet PM, Benson CB, Bourne T, Blaivas M. Diagnostic criteria
for nonviable pregnancy early in the first trimester. N Engl J Med
2013;369(15):1443-51.
7. Ballagh SA, Harris HA, Demasio K. Is curettage needed for uncomplicated
incomplete spontaneous abortion?. Am J Obstet Gynecol 1998;179(5):1279-82.
8. Luise C, Jermy K, May C, Costello G, Collins WP, Bourne TH. Outcome of
expectant management of spontaneous first trimester miscarriage: observational
study. BMJ 2002;324(7342):873-5.
9. Van Abortusartsen NG. Guideline for counselling women considering termination
of pregnancy 2011;25-8.
10. Grossman D. Medical methods for first trimester abortion: RHL commentary. The
WHO Reproductive Health Library Geneva: World Health Organization
2004;46(12)163-9.

80
11. Singh KC, Ummat S, Rajaram S, Goel N. First trimester abortion with
mifepristone and three doses of sublingual misoprostol: a pilot study.Aust N Z J
Obstet Gynaecol 2005;45(6):495-8.
12. Schaff EA, Fielding SL, Westhoff C. Randomized trial of oral versus vaginal
misoprostol 2 days after mifepristone 200 mg for abortion up to 63 days of
pregnancy. J.Contraception 2002;66(4):247-50.
13. Sheiner EK. Bleeding during pregnancy: a comprehensive guide: Springer Science
and Business Media 2011;10-25.
14. Brier N. Grief following miscarriage: a comprehensive review of the literature.J
Womens Health (Larchmt) 2008;17:451–64.
15. Zinaman MJ, Clegg ED, Brown CC, O’Connor J, Selevan SG.Estimates of human
fertility and pregnancy loss. Fertil Steril 1996;65:503–9.
16. Ellish NJ, Saboda K, O’Connor J, Nasca PC, Stanek EJ, Boyle C. A prospective
study of early pregnancy loss. Hum Reprod 1996;11:406–12.
17. Allison JL, Sherwood RS, Schust DJ. Management of first trimester pregnancy
loss can be safely moved into the office. Rev Obstet Gynecol 2011;4(1):5.
18. Jauniaux E, Johns J, Burton G. The role of ultrasound imaging in diagnosing and
investigating early pregnancy failure. Ultrasound Obstet Gynecol 2005;25(6):613-
24.
19. Rowling SE, Coleman BG, Langer JE, Arger PH, Nisenbaum HL, Horii SC. First-
trimester US parameters of failed pregnancy. Radiology.1997;203(1):211-
7.Available at http://dx.doi.org/10.1148/radiology.203.1.9122395.
20. Juliano M, Dabulis S, Heffner A. Characteristics of women with fetal loss in
symptomatic first trimester pregnancies with documented fetal cardiac activity.
Ann Emerg Med 2008;52(2):143-7.

81
21. Benhamou B, Garcia T. A single amino acid that determines the sensitivity of
progesterone receptors to RU486.Science 1992;255(5041):206-9.
22. Baulieu EE. RU 486 (mifepristone). A short overview of its mechanisms of action
and clinical uses at the end of 1996.Ann N Y Acad Sci 1997;828:47–58.
23. Moguilewsky M, Philibert D. Biochemical profile of RU 486.In: Balieu EE, Segal
SJ, editors. The antiprogestin steroid RU 486 and human fertility control. New
York7 Plenum Press;1985:87– 97.
24. Lahteenmaki P, Heikinheimo O, Croxatto H, Spitz I, Shoupe D, Birgerson L, et al.
Pharmacokinetics and metabolism of RU 486.J Steroid Biochem 1987;27:859–
63.
25. Gravanis A, Schaison G, George M, De Brux J, Satyaswaroop P, Baulieu E, et al.
Endometrial and pituitary responses to the steroidal antiprogestin RU 486 in
postmenopausal women. J Clin Endocrinol Metab 1985;60:156– 63.
26. Brogden RN, Goa KL, Faulds D. Mifepristone. Drugs. 1993;45(3):384-409.
27. WilliamCB, Pery HV. Lipid derived autocoids.Chapter 26, Goodman and
Gilman’s, 9th
edition, Hardman G Joe and Limbard E.Zee, 1996;601- 616.
28. Song J. Use of misoprostol in obstetrics and gynecology. Obstetrical and
gynecological survey. 2000;55(8):503-10.
29. Speroff Leon, Marc A Fritz. Prostaglandins.In:ClinicalGynaecologic
endocrinology and infertility.7th
edn, Williams and Wilkins.2005;291-317.
30. Bertin J, Barat C, Méthot S, Tremblay MJ. Interactions between prostaglandins,
leukotrienes and HIV-1: Possible implications for the central nervous system.
Retrovirology2012;9(1):4.
31. Hall A, Behrman H. The prostaglandins: basic chemistry and action.Reproductive
endocrinology, infertility, genetics 1985;5-8.

82
32. Funk CD. Prostaglandins and leukotrienes: advances in eicosanoid biology.
Science 2001;294(5548):1871-5.
33. Novy MJ, Liggins GC. Role of prostaglandins, prostacyclin, and thromboxanes in
the physiologic control of the uterus and in parturition.Semin Perinatol 1980;
4(1):45-66.
34. Fiala C, Danielsson KG. Review of medical abortion using mifepristone in
combination with a prostaglandin analogue.J.Contraception2006;74(1):66-86.
35. Foy R, Penney G, Grimshaw J, Ramsay C, Walker A, MacLennan G, et al. A
randomised controlled trial of a tailored multifaceted strategy to promote
implementation of a clinical guideline on induced abortion care. BJOG
2004;111(7):726-33.
36. Wood AJ, Goldberg AB, Greenberg MB, Darney PD. Misoprostol and
pregnancy.N Engl J Med 2001;344(1):38-47.
37. Weeks AD, Fiala C, Safar P. Misoprostol and the debate over off‐label drug use.
BJOG 2005;112(3):269-72.
38. ACOG Committee Opinion. Number 283, May 2003.New US Food and Drug
Administration labeling on Cytotec (misoprostol) use and pregnancy.Obstet
Gynecol 2003;101:1049-50.
39. Foote EF, Lee DR, Karim A, Keane WF, Halstenson CE. Disposition of
misoprostol and its active metabolite in patients with normal and impaired renal
function.J Clin Pharmacol 1995;35(4):384-9.
40. Zieman M, Fong SK, Benowitz NL, Banskter D, Darney PD. Absorption kinetics
of misoprostol with oral or vaginal administration. Obstet Gynecol 1997;90(1):88-
92.

83
41. Khan RU, El-Refaey H, Sharma S, Sooranna D, Stafford M. Oral, rectal, and
vaginal pharmacokinetics of misoprostol. Obstet Gynecol 2004;103(5):866-70.
42. Schaff EA, DiCenzo R, Fielding SL. Comparison of misoprostol plasma
concentrations following buccal and sublingual administration.J.Contraception
2005;71(1):22-5.
43. Tang O, Gemzell-Danielsson K, Ho P. Misoprostol: pharmacokinetic profiles,
effects on the uterus and side-effects. Int J Gynaecol Obstet 2007;99:S160-7.
44. Pang M, Lee T, Chung T. Incomplete miscarriage: a randomized controlled trial
comparing oral with vaginal misoprostol for medical evacuation. Hum
Reprod2001;16(11):2283-7.
45. Creinin MD, Huang X, Westhoff C, Barnhart K, Gilles JM, Zhang J. Factors
related to successful misoprostol treatment for early pregnancy failure. Obstet
Gynecol. 2006;107(4):901.
46. Obstetricians ACo, Gynecologists. Medical management of first-trimester
abortion. ACOG practice bulletin no. 143.Obstet Gynecol. 2014;123:676-92.
47. Fjerstad M, Trussell J, Sivin I, Lichtenberg ES, Cullins V. Rates of serious
infection after changes in regimens for medical abortion.N Engl J Med
2009;361(2):145-51.
48. Creinin MD, Fox MC, Teal S, Chen A, Schaff EA, Meyn LA, et al. A randomized
comparison of misoprostol 6 to 8 hours versus 24 hours after mifepristone for
abortion.Obstet Gynecol 2004;103(5):851-9.
49. Chaudhuri P, Mandal A, Das C, Mazumdar A. Dosing interval of 24hours versus
48hours between mifepristone and misoprostol administration for mid-trimester
termination of pregnancy. Int J Gynecol Obstet. 2014;124(2):134-8.

84
50. Mentula M, Suhonen S, Heikinheimo O. One-and two-day dosing intervals
between mifepristone and misoprostol in second trimester medical termination of
pregnancy-a randomized trial. Hum Reprod 2011;26(10):2690-7.
51. Creinin MD, Schreiber CA, Bednarek P, Lintu H, Wagner M-S, Meyn LA, et al.
Mifepristone and misoprostol administered simultaneously versus 24 hours apart
for abortion: a randomized controlled trial. Obstet Gynecol 2007;109(4):885-94.
52. Chen AY, Mottl-Santiago J, Vragovic O, Wasserman S, Borgatta L. Bleeding
after medication-induced termination of pregnancy with two dosing schedules of
mifepristone and misoprostol. J. Contraception 2006;73(4):415-9.
53. Schaff EA, Fielding SL, Westhoff C, Ellertson C, Eisinger SH, Stadalius LS, et al.
Vaginal misoprostol administered 1, 2, or 3 days after mifepristone for early
medical abortion: a randomized trial. JAMA 2000;284(15):1948-53.
54. Ashok PW, Flett GM, Templeton A. Mifepristone versus vaginally administered
misoprostol for cervical priming before first-trimester termination of pregnancy: a
randomized, controlled study. Am J Obstet Gynecol 2000;183(4):998-1002.
55. Heikinheimo O, Suhonen S, Haukkamaa M. One-and 2-day mifepristone–
misoprostol intervals are both effective in medical termination of second-trimester
pregnancy. Reprod Biomed Online 2004;8(2):236-9.
56. Weeks A. Medical treatment for early fetal death (less than 24 weeks): RHL
commentary. The WHO Reproductive Health Library Geneva: World Health
Organization 2007;342:110-8.
57. El-Refaey H, Rajasekar D, Abdalla M, Calder L, Templeton A. Induction of
abortion with mifepristone (RU 486) and oral or vaginal misoprostol. N Engl J
Med 1995;332(15):983-7.

85
58. Hinshaw HKS. Medical management of miscarriage. In :Grudzinkas TG, O’Brien
PMS, editors. Problems in early pregnancy: advances in diagnosis and
management. London: RCOG press, 1997; 284‐95.
59. Tang OS, Ong CY, Tse KY, Ng EH, Lee SW, Ho PC. A randomized trial to
compare the use of sublingual misoprostol with or without an additional 1 week
course for the management of first trimester silent miscarriage.Hum Reprod
2006;21(1):189-92.
60. Ngoc NTN, Blum J, Westheimer E, Quan TTV, Winikoff B. Medical treatment of
missed abortion using misoprostol.Int J Gynecol Obstet 2004;87(2):138-42.
61. Trinder J, Brocklehurst P, Porter R, Read M, Vyas S, Smith L. Management of
miscarriage: expectant, medical, or surgical?- Results of randomised controlled
trial (miscarriage treatment (MIST) trial). BMJ 2006;332(7552):1235-40.
62. Demetroulis C, Saridogan E, Kunde D, Naftalin AA. A prospective randomized
control trial comparing medical and surgical treatment for early pregnancy failure.
Hum Reprod 2001;16:365–9.
63. Neilson JP, Hickey M, Vazquez J. Medical treatment for early fetal death (less
than 24 weeks). Cochrane Database Syst Rev. 2006;3:CD002253.
64. Wieringa-de Waard M, Hartman EE, Ankum WM, Reitsma JB, Bindels PJ,
Bonsel GJ. Expectant management versus surgical evacuation in first trimester
miscarriage: health-related quality of life in randomized and non-randomized
patients. Hum Reprod 2002;17(6):1638-42.
65. Odeh M, Tendler R, Kais M, Maximovsky O, Ophir E, Bornstein J. Early
pregnancy failure: factors affecting successful medical treatment.Isr Med
Assoc J 2010;12(6):325-8.

86
66. Marwan Odeh M, Rene Tendler M, Mohamad Kais M, Olga Maximovsky M, Ella
Ophir M, Jacob Bornstein M.Early Pregnancy Failure: Factors affecting
successful medical treatment. Isr Med Assoc J 2010;12(6):325-8.
67. Obstetricians ACo, Gynecologists. ACOG Committee Opinion No. 427:
Misoprostol for post abortion care. Obstet Gynecol 2009;113(2 Pt 1):465-8.
68. Jha M, Chitrakar N, Shakya B, Jha R. Efficacy of Misoprostol as a Post Abortion
Care. Nepal J Obstet Gynaecol 2014;8(2):71-4.
69. Ashok P, Penney G, Flett G, Templeton A. An effective regimen for early medical
abortion: a report of 2000 consecutive cases. Hum Reprod 1998;13(10):2962-5.
70. Verma ML, Singh U, Singh N, Shankhwar P, Srivastava D. Efficacy of
misoprostol administration 24 hours after mifepristone for termination of early
pregnancy. Indian J Med Sci 2011;65(12):511.
71. Bhutta S, Aziz S, Korejo R. Surgical complications following unsafe abortion. J
Pak Med Assoc 2003;53(7):286-9.
72. Nojomi M, Akbarian A, Ashory-Moghadam S. Burden of abortion: induced and
spontaneous. Arch Iran Med 2006;9(1):39-45.
73. Shah I, Ahman E. Unsafe abortion: global and regional incidence, trends,
consequences, and challenges.J Obstet Gynaecol Can 2009 ;31(12):1149-58.
74. Shi Y-e, Ye Z-h, He C-h, Zhang G-q, Xu J-q, Van Look P, et al. Pharmacokinetic
study of RU 486 and its metabolites after oral administration of single doses to
pregnant and non-pregnant women.J. Contraception 1993 ;48(2):133-49.
75. Swahn M, Wang G, Aedo A, Cekan S, Bygdeman M. Plasma levels of
antiprogestin RU 486 following oral administration to non-pregnant and early
pregnant women.J. Contraception 1986;34(5):469-81.

87
76. Spitz IM, Bardin CW, Benton L, Robbins A. Early pregnancy termination with
mifepristone and misoprostol in the United States.N Engl J Med
1998;338(18):1241-7.
77. Sonal K, Meenal P, Hemant D. A prospective trial using mifepristone and vaginal
misoprostol in termination of pregnancies up to 63 days of gestation. J Obstet
Gynaecol India 2013;63(6):370-72.
78. Von Hertzen H, Piaggio G, Wojdyla D, Marions L, My Huong N, Tang O, et al.
Two mifepristone doses and two intervals of misoprostol administration for
termination of early pregnancy: a randomised factorial controlled equivalence
trial.BJOG 2009;116(3):381-9.
79. Guest J, Chien P, Thomson M, Kosseim M. Randomised controlled trial
comparing the efficacy of same‐day administration of mifepristone and
misoprostol for termination of pregnancy with the standard 36 to 48 hour protocol.
BJOG 2007;114(2):207-15.
80. Schaff EA, Fielding SL, Westhoff C, Ellertson C, Eisinger SH, Stadalius LS, et al.
Vaginal misoprostol administered 1, 2, or 3 days after mifepristone for early
medical abortion: a randomized trial. JAMA 2000;284(15):1948-53.
81. Mentula M, Suhonen S, Heikinheimo O. One-and two-day dosing intervals
between mifepristone and misoprostol in second trimester medical termination of
pregnancy-a randomized trial. Hum Reprod 2011;26(10):2690-7.
82. Hou S, Zhang L, Chen Q, Fang A, Cheng L. One- and two-day mifepristone-
misoprostol intervals for second trimester terminationof pregnancy between 13
and 16 weeks of gestation. Int J Gynaecol Obstet 2010;111:126–30.

88
83. Ashok PW, Templeton A, WagaarachchiPT, Flett GM.Midtrimester medical
termination of pregnancy: a review of 1002 consecutive cases. Contraception
2004;69:51–58.
84. Carbonell JL, Torres MA, Reyes R, Ortega L, Garcıa-Gallego F, Sanchez
C.Second-trimester pregnancy termination with 600mcg vs.400 mcg vaginal
misoprostol and systematic curettage post expulsion: a randomized trial.
Contraception 2008;77:50–55.
85. Chai J, Tang OS, Hong QQ, Chen QF, Cheng LN, Ng E, et al. A randomized trial
to compare two dosing intervals of misoprostol following mifepristone
administration in second trimester medical abortion. Hum Reprod 2009;24:320–4.

ANNEXURES

89
ANNEXURE
PROFORMA
COMPARITIVE STUDY OF EARLY (24 HOURS) VERSUS LATE (48
HOURS) MISOPROSTOL ADMINISTRATION AFTER MIFEPRISTONE
FOR TERMINATION OF EARLY PREGNANCY.
By : Dr.N.Priya
Guide : Dr. Prashant S Joshi
Name : Education :
Age : Occupation :
MR NO : Per capita income :
Address :
Socioeconomic status :
Married life :
Consanguinity :
Obstetric score :
H/O previous deliveries :
Period of pregnancy :
Whether any medical disease associated with pregnancy :
Menstrual History :
Previous menstrual cycles -
Last menstrual period -
Past Medical History :
Drug History :
Family History :
Personal History :

90
General Physical Examination
Built :
Nourishment :
Pallor :
Height :
Weight :
Pulse rate :
Blood pressure :
Respiratory rate :
Per abdomen examination :
Per speculum examination :
Per vaginal examination :
Investigations
Ultrasonogram findings :
Coagulation profile :
Hb and HCT before induction with misoprostol :
Hb and HCT 48 hrs after expulsion :
Date of application of Misoprostol :
Time of first vaginal application of misoprostol :
Intial dosage :
Number of doses applied :
Date of expulsion :
Time of expulsion :
91
Induction expulsion interval :
USG after expulsion : Complete / incomplete
Whether underwent curettage later :
Side effects if any :
Follow up after 1month :

92
KEY TO MASTER CHART
Sl. no : Serial number
MR no : Medical Records number
Obs code : Obstetric code
GA : Gestational age
Hrs : Hours
W : Weeks
D : Days
M : Multigravida
P : Primigravida
MAAI : Misoprostol application to expulsion interval
USG : Ultrasonogram
C : Complete
I : Incomplete

93
MASTER CHART
Sl.
No. Name
Ag
e (Y
ears
)
M R
No
Obs
Code
GA
(wks)
Misoprostol
application
to
expulsion
interval
No
of
doses
Cu
rett
age
Ult
raso
und
Sid
e ef
fect
s
Inte
rval
Reg
imen
1 Manjula 20 839788 P 7W2D 13 3 No C vomiting 48 hrs
2 Lakshmi 24 843107 P 6W3D 7 1 No C Diarrhoea 48 hrs
3 Jayamma 25 844122 M 7W 10 2 Yes I - 48 hrs
4 Chaithra 19 846100 P 8W4D 9 1 No C Fever with
chills 48 hrs
5 Kusuma 22 870102 P 7W4D 10 2 No Lost
follow
up
48 hrs
6 prashanthi 24 872144 M 7W 6 ½ 1 No C - 48 hrs
7 Manmatha 20 874153 P 8W1D 14 3 No C - 48 hrs
8 Thimmamma 21 875180 P 8W4D 6 1 No C Chills 48 hrs
9 Susheela 28 14-
7001 M 7W5D 6 1 No C Vomiting 48 hrs
10 Shantha 27 14-
7129 M 8W4D 10 2 Yes I Febrile 48 hrs
11 Jaisheela 26 14-
6482 M 6W3D 5 1 No C - 48 hrs
12 Radhamani 25 14-
7210 M 8W4D 12 2 No C - 48 hrs
13 Latha 19 14-
7742 P 8W2D 6 ½ 1 No C - 48 hrs
14 Shashikala 25 14-
7814 M 6W5D 11 2 Yes I - 48 hrs
15 Sunitha 22 14-
7911 P 7W 5 1 No C Diarrhoea 48 hrs
16 Mahalakshmi 23 14-
8011 P 8W5D 7 1 No C - 48 hrs
17 Fardeen 24 14-
8044 M 8W6D 5 1 No C Chills 48 hrs
18 Manjula 21 14-
8120 P 8W 12 2 No
Lost
follow
up
48 hrs
19 Deepika 25 892421 M 7W6D 7 ½ 1 No C - 48 hrs
20 Roopashree 20 893011 M 8W2D 10 ½ 2 No C Fever 48 hrs
21 Savitha 24 893124 M 7W2D 13 ½ 3 No C Fever with
chills 48 hrs
22 Padma 25 893241 M 8W3D 6 1 No C Diarrhoea 48 hrs
23 Nethravathi 22 894431 M 7W1D 5 1 No C - 48 hrs

94
Sl.
No. Name
Ag
e (Y
ears
)
M R
No
Obs
Code
GA
(wks)
Misoprostol
application
to
expulsion
interval
No
of
doses
Cu
rett
age
Ult
raso
und
Sid
e ef
fect
s
Inte
rval
Reg
imen
24 Mangala 23 14-
9021 M 8W 14 3 No C
Vomiting and
diarrhoea 48 hrs
25 Shabana
Begum 31
14-
9122 M 8W2D 7 1 No
Lost
follow
up
48 hrs
26 Susheela 26 14-
9442 M 7W 7 1 Yes I Chills 48 hrs
27 Pramila 25 14-
9524 M 8W1D 10 1/2 2 No C - 48 hrs
28 Mamatha Shree 32 14-
9538 M 8W2D 6 1 No C - 48 hrs
29 Anitha 27 14-
9630 M 8W3D 10 1/2 2 Yes I Vomiting 48 hrs
30 Nandini 23 894466 P 6W3D 5 1/2 1 No C - 48 hrs
31 Rekha 22 892012 P 6W5D 14 3 Yes I - 48 hrs
32 Harshiya
Sulthana 25 895018 M 7W6D 5 1/2 1 No C Diarrhoea 48 hrs
33 Chaithra 34 897216 M 6W 4 1/2 1 No C Vomiting 48 hrs
34 Sameena 30 899212 M 8W 5 1/2 1 No C - 48 hrs
35 Sunanda 26 901012 M 8W2D 6 1/2 1 No C - 48 hrs
36 Rashmi 21 902210 M 6W5D 13 1/2 3 No C Vomiting 48 hrs
37 Kumari 25 910764 M 8W6D 13 3 No C - 48 hrs
38 Usha Rani 23 911768 M 6W6D 6 1/2 1 No C - 48 hrs
39 Nagarathna 25 912770 M 8W1D 5 1 NO C - 48 hrs
40 Divyashree 28 930712 M 8W3D 5 1/2 1 Lost
follow
up
48 hrs
41 Lakshmi 34 942515 M 6W5D 6 1 No C - 48 hrs
42 Savitha 26 943680 M 6W5D 5 1/2 1 No C - 48 hrs
43 Ashwini 29 945806 M 8W 5 1/2 1 No C Vomiting 48 hrs
44 Shivamma 24 950504 M 8W 14 3 No C - 48 hrs
45 Nagamma 21 15-
3018 P 7W2D 5 1
Lost
follow
up
48 hrs
46 Fathima 27 15-
3426 M 7W 6 1 No C - 48 hrs
47 Reshma 22 15-
4012 P 7W2D 6 1/2 1 No C - 48 hrs

95
Sl.
No. Name
Ag
e (Y
ears
)
M R
No
Obs
Code
GA
(wks)
Misoprostol
application
to
expulsion
interval
No
of
doses
Cu
rett
age
Ult
raso
und
Sid
e ef
fect
s
Inte
rval
Reg
imen
48 Asha 24 15-
4624 M 8W1D 5 ½ 1 No C Chills 48 hrs
49 Padma 28 15-
4721 M 7W4D 6 ½ 1 No C - 48 hrs
50 Ramya 23 15-
4822 M 7W1D 6 1 No C Chills 48 hrs
51 Farzana 20 15-
5011 M 6W 7 1 No C _ 48 hrs
52 Suchitra 24 22270 M 8W2D 6 1 No C _ 48 hrs
53 Kavitha 28 22248 P 7W4D 10 2 No C _ 48 hrs
54 Rathna 32 22264 P 8W 14 3 No C _ 48 hrs
55 Regima 19 15-
5110 M 6W 6 1 No C - 48 hrs
56 Nanthini 23 951231 M 7w 1D 9 2 No C - 48 hrs
57 Sangeetha 27 961228 M 8W 10 2 No C - 48 hrs
58 Girija 28 966223 M 8W4D 12 1/2 3 No C - 48 hrs
59 Prema 32 15-
5212 M 8W 13 1/2 3 No C - 48 hrs
60 Bhavana 24 15-
4214 M 6W2D 7 1 No C - 48hrs
61 Pallavi 25 11401 P 7W2D 7 1 No C Diarrhoea 24 hrs
62 Sowmya 26 11338 M 8W 5 1 No C _ 24 hrs
63 Kusuma 24 13458 P 8W2D 13 2 No C Diarrhoea 24 hrs
64 Padma 25 821865 M 8W3D 6 1 No C _ 24 hrs
65 Shilpa 21 839788 P 7W 7 1 No C _ 24 hrs
66 Uma 24 20834 M 8W2D 7 1 No C _ 24 hrs
67 Shwetha 28 856161 M 6W2D 8 1 Yes I _ 24 hrs
68 Vishala 19 106693 P 6W4D 12 2 No C _ 24 hrs
69 Ashwini 23 107089 P 8W5D 7 ½ 1 Yes I _ 24 hrs
70 Shantha 24 24904 M 6W1D 10 2 No C Chills 24 hrs
71 Vaishnavi 22 104687 M 8WID 5 1 No C _ 24 hrs
72 Sowjanya 23 109423 P 6W2D 6 1 No C _ 24 hrs
73 Shwetha 26 110186 M 7W4D 10 2 Yes I _ 24 hrs
74 Prathima 26 110198 M 8W 8 1 No C Fever 24 hrs
75 Ashwini 25 25707 P 8W2D 7 1 Yes I _ 24 hrs

96
Sl.
No. Name
Ag
e (Y
ears
)
M R
No
Obs
Code
GA
(wks)
Misoprostol
application
to
expulsion
interval
No
of
doses
Cu
rett
age
Ult
raso
und
Sid
e ef
fect
s
Inte
rval
Reg
imen
76 Mahalakshmi 23 20204 P 6W6D 12 2 No C Diarrhoea 24 hrs
77 Varalakshmi 25 113363 M 6W 9 2 Yes I Diarrhoea 24 hrs
78 Chandrakala 19 13458 P 7W5D 13 3 No C Fever 24 hrs
79 Pushpa 31 878168 M 8W3D 7 1 Yes I _ 24 hrs
80 Tasneem 28 883107 M 8W5D 6 1 No C Vomiting 24 hrs
81 Chaithra 33 880769 M 7W4D 14 3 No C Fever+chills 24 hrs
82 Ayesha Begum 26 885366 M 8W 5 1 No C Diarrhoea 24 hrs
83 Nagarathna 25 897137 M 6W4D 7 1 No C _ 24 hrs
84 Geetha 22 897187 P 8W1D 13 2 No C Chills 24 hrs
85 Naziya 20 899983 P 8W1D 5 1 Yes I Chills 24 hrs
86 Asneem 32 719306 M 7W2D 10 2 No C _ 24 hrs
87 Chaithra 27 743818 M 8W 5 1 No C _ 24 hrs
88 Radhamani 24 745585 P 6W1D 6 1 No C Fever 24 hrs
89 Preetha rani 22 746743 P 8W6D 7 1/2 1 No C _ 24 hrs
90 Chandrakala 25 757983 M 7W 9 2 No C Diarrhoea 24 hrs
91 Pooja 27 771457 M 8W3D 6 1 No C Fever 24 hrs
92 lakshmama 25 775371 P 8W 10 1/2 2 No C Nil 24 hrs
93 Chaitra 26 795963 M 7W 1d 5 1/2 1 Yes I _ 24 hrs
94 Pushpa 20 799802 P 8W6D 6 1/2 1 No C Fever 24 hrs
95 Afreen taj 30 806504 M 6W6D 6 1 No C Diarrhoea 24 hrs
96 Ramya 29 810512 M 7W2D 7 1/2 1 No C _ 24 hrs
97 Varalakshmi 27 824122 M 9W 11 2 No C Diarrhoea 24 hrs
98 Mangalamma 26 841210 M 8W 7 1 No C _ 24 hrs
99 Mamatha 24 848566 P 7W4D 6 1/2 1 No C Fever 24 hrs
100 Yashaswini 23 850611 P 8W2D 5 1 NO C Diarrhoea 24 hrs
101 Harshitha 22 854100 P 6W2D 7 1 Yes I - 24 hrs
102 Chethana 33 854108 M 8W 7 1/2 1 No Not
done Lost follow up 24 hrs
103 Vanitha 30 855124 M 8W5D 7 1/2 1 No C _ 24 hrs
104 Jaheena 32 860108 M 8W6D 6 1 No C Diarrhoea 24 hrs

97
Sl.
No. Name
Ag
e (Y
ears
)
M R
No
Obs
Code
GA
(wks)
Misoprostol
application
to
expulsion
interval
No
of
doses
Cu
rett
age
Ult
raso
und
Sid
e ef
fect
s
Inte
rval
Reg
imen
105 Chaithra 29 864124 P 7W 6 1 No C - 24 hrs
106 Bhagyamma 24 869100 M 8W2D 7 1 No C Diarrhoea 24 hrs
107 Kusuma 23 871112 M 6W 6 1/2 1 No Not
done Lost follow up 24 hrs
108 Nagamani 22 880110 M 8W 5 1/2 1 No C - 24 hrs
109 Vaishnavi 24 881412 M 7W3D 7 1/2 1 No C - 24 hrs
110 Ranjani 19 892212 M 8W 11 2 No C _ 24 hrs
111 Sashikala 32 912442 P 6W6D 14 3 No C _ 24 hrs
112 vani 19 934521 M 7W 7 1 No C - 24 hrs
113 Pramila 24 15-
3221 M 6W5D 6 1 No C - 24 hrs
114 Fathima 26 15-
5290 M 8W 10 2 No C - 24 hrs
115 Reshmi 31 15-
3211 M 8W4D 11 2 No C - 24 hrs
116 Padma 34 922311 M 8W 13 3 No C - 24 hrs
117 Sushma 19 923886 M 8W2D 6 1 No C - 24 hrs
118 Divya 22 15-
4313 M 8W4D 5 1 No I - 24 hrs
119 Reshma 32 15-
3772 M 8w2d 5 1/2 1 No I - 24hrs
120 Swathi 22 110211 M 8W 7 1 No C Fever +
vomiting 24 hrs