comparative evaluation of defecography phase to non ... lifelong...
TRANSCRIPT
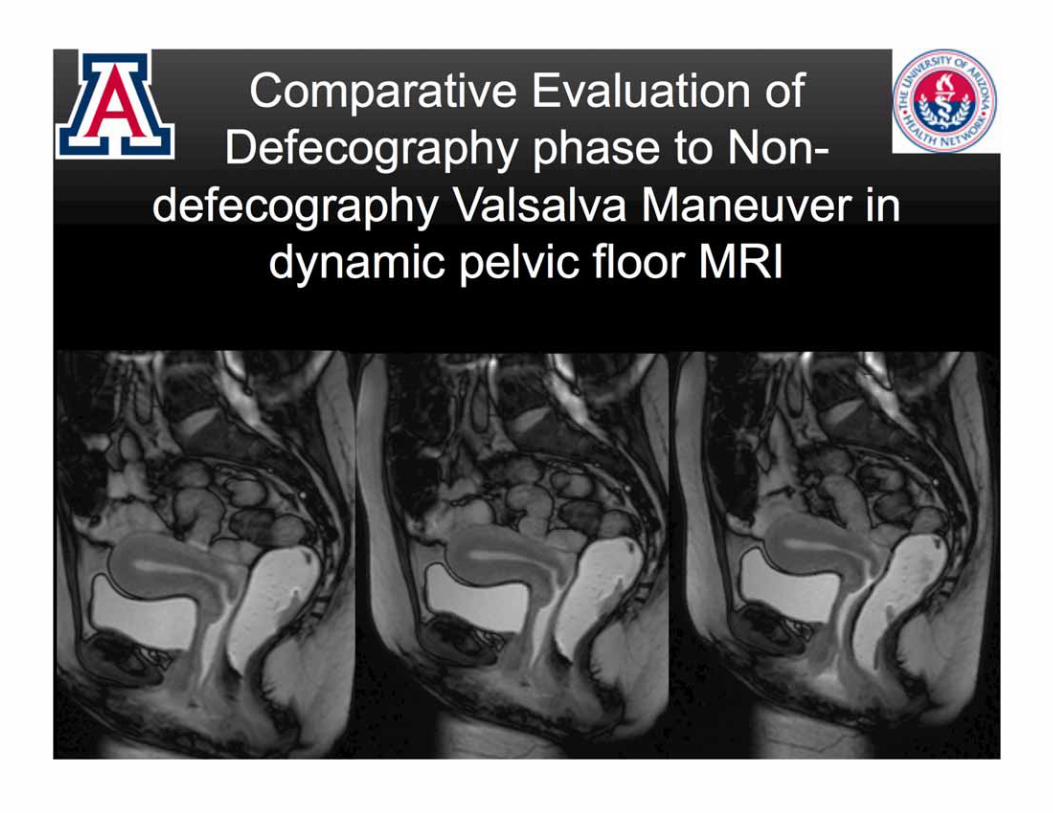
Comparative Evaluation of Defecography phase to Non-
defecography Valsalva Maneuver in dynamic pelvic floor MRI
No Financial disclosures
Authors: Hina Arif1, Bobby Kalb1,Arash Meshksar1, Iva Petkovska1, Ferenc Pommersheim1, James Costello1, Joel Funk2 ,
Christian Twiss 2, Diego Martin1
Departments of Medical imaging 1 and Urology 2
University of Arizona, Tuscon, AZ.

• Hidden women's health epidemic
• 50% middle aged & older are affected
• Large health care cost: 30% reoperations
• Unmet clinical need:
• Paucity in understanding complex pelvic floor
dynamics
• Limited pre operative evaluation: • High recurrence rates • Repeat surgery
PELVIC FLOOR DYSFUNCTION

To evaluate the utility of Defecography phase (DP) in
dynamic pelvic floor MRI, in comparison to non-
defecography Valsalva maneuver (VM).
PURPOSE

METHOD AND MATERIALS
All female patients who presented to pelvic floor clinic between Oct 2011- August 2015
Urinary: Sensation of incomplete emptying, urgency, incontinence,
nocturia, frequency
Fecal: incontinence, urgency, constipation
Vaginal prolapse or Dyspareunia
Findings of pelvic floor prolapse were demonstrated by Baden Walker system
PHYSICAL EXAMINATION
CLINICAL COMPLAINTS
INCLUSION CRITERIA
Study IRB-approved, HIPPA compliant
a) did not have a pelvic MRI performed, b) were of male gender, c) were unable to tolerate the gel administration or d) did not demonstrate expulsion of rectal
gel during defecography maneuvers.
EXCLUSION CRITERIA

MRI TECHNIQUE
MR Image acquisition:
• Fast imaging with steady-state free precession technique (True FISP)
• Mid sagittal acquisition was performed at rest, and during VM & DF
• 350-mm2 field of view, 256 × 208 matrix, partial Fourier acquisition of 7/8, 8-mm
section thickness, flip angle of 40°, acceleration factor of two Rest VM DF
Patient Preparation
• Insertion of ultrasound gel into rectum & vagina
• Instructions to strain (exert pressure against closed sphincter) and defecate
(expulsion of gel) during different phase of acquisition

• Image review :
• Image analysis was done in blinded
fashion by two radiologists with 13 & 5
years of experience in abdominal & pelvic
MRI
• HMO system was employed for quantification
of pelvic floor descent
• Pubo-coccygeal line (PCL)
• M-line
• H-line
• Presence of organ prolapse
• Quantification of degree of organ prolapse
MR IMAGE ANALYSIS
Fielding J R Radiographics 2002;22:295-304

MR IMAGE ANALYSIS
Vertical distance of the
neck of urinary bladder
below the PCL
Cystocoele Ano-rectal junction prolapse Utero-vaginal Prolapse
• M-line >2cm
• Rectum below the H-line
Descent from its position
on static images
RESULTS Statistics:
• Change in measurements of the PCL, H-line and M-line was calculated
between straining and defecation sequences.
• An unpaired t-test was used to compare the changes in measurements
between straining and defecation sequences for the PCL, H-line and M-
line, the degree of anorectal and vaginal prolapse, and the number of
patients with cystocele and rectocele.
• A p-value of < 0.05 was considered statistically significance.
Patient Demographics:
• The final study cohort consisted of 237 patients that met study
inclusion criteria (mean age 63 years, range 35-82 years).

RESULTS
Anorectal Prolapse
Cystourethrocele Vaginal vault prolapse
100%
71% 71%
86%
14%
43%
Defecography phase Valsalva maneuver

0
1
2
3
4
5
6
Cystocele Vaginal
prolapse Anorectal prolapse
Defecography phase Valsalva manoeuvre
Org
an
prol
apse
in
cm
Rectal descent = z = 2.80, p < 0.01 Cystocele descent = z = 5.70, p < 0.01 Vaginal vault descent = z = 4.14, p < 0.01
P <0.01
RESULTS

PCL H-line M-line
Resting phase
10.2 6.2 3.2
Valsalva manoeuvre
10.5 7.8 5.5
Defecography phase
7.8 13.4 7.6
RESULTS

• Imaging of pelvic floor is complex; quantification and
assessment of pelvic floor prolapse remains challenging to the
radiologist and surgeons
• Defecography phase in dynamic pelvic floor MR unmasks a
greater degree of instability involving either of the
compartments of pelvic floor
• Better detection, and quantification of severity of cystocele,
vaginal prolapse and ano-rectal junction prolapse can be done
on DF in comparison to VM
DISCUSSION

CYSTOCELE GLOBAL PELVIC FLOOR PROLAPSE
Valsalva Maneuver Defecography Phase

ANO RECTAL PROLAPSE & RECTOCELE
Valsalva Maneuver Defecography Phase

Valsalva Maneuver Defecography Phase
UTERO-VAGINAL PROLAPSE

• Pelvic floor structures may show mild instability or even
appear normal on the straining phase, with marked
prolapse subsequently revealed on DP imaging
CONCLUSION
• Imaging in the Era of Comparative Effectiveness demands
evaluation pelvic floor dysfunction on the defecography
phase on dynamic pelvic floor MR examinations, which
currently and commonly based on assessment of pelvic
floor structures on only straining/Non-defecography
Valsalva Maneuver
• Goh V, Halligan S, Kaplan G, et al. Dynamic MR imaging of the pelvic floor in asymptomatic subjects AJR Am J Roentgenol 2000; 174:661–66.
• Hecht EM, Lee VS, Tanpitukpongse TP, et al. MRI of pelvic floor dysfunction: dynamic true fast imaging with steady-state precession versus HASTE. AJR Am J Roentgenol 2008; 191:352–358.
• Lockhart ME, Fielding JR, Richter HE, et al. Reproducibility of dynamic MR imaging pelvic measurements: a multi-institutional study. Radiology 2008; 249:534-40.
• Maglinte DD, Bartram CI, Hale DA, et al. Functional imaging of the pelvic floor. Radiology 2011; 258:23-39.
• Mondot L, Novellas S, Senni M, et al. Pelvic prolapse: static and dynamic MRI. Abdom imaging 2007; 32:775-83.
• Pannu HK, Kaufman HS, Cundiff GW, et al. Dynamic MR imaging of pelvic organ prolapse: spectrum of abnormalities. Radiographics 2000; 20:1567-82.
• Pannu HK, Scatarige JC, et al. Comparison of supine magnetic resonance imaging with and without rectal contrast to fluoroscopic cystocolpoproctography for the diagnosis of pelvic organ prolapse. J Comput Assist Tomogr 2009; 33:125–130.
• Roos JE, Weishaupt D, Wildermuth S, et al. Experience of 4 years with open MR defecography: pictorial review of anorectal anatomy and disease. Radiographics. 2002; 22:817-32.
• Woodfield CA, Krishnamoorthy S, Hampton BS, et al. Imaging pelvic floor disorders: Trend toward comprehensive MRI. AJR Am J Roentgenol 2010; 194:1640-9.
• Boyadzhyan L, Raman SS, Raz S. Role of static and dynamic MR imaging in surgical pelvic floor dysfunction. Radiographics 2008; 28:949-67.
• Fielding JR. Practical MR imaging of female pelvic floor weakness. Radiographics 2002; 22:295-304.
• Law YM, Fielding JR. MRI of pelvic floor dysfunction: Review. AJR Am J Roentgenol 2008; 191:S45-53.
• Reiner CS, Weishaupt D. Dynamic pelvic floor imaging: MRI techniques and imaging parameters. Abdom Imaging 2012 Epub.
• Bertschinger KM, Hetzer FH, Roos JE, et al. Dynamic MR imaging of the pelvic floor performed with patient sitting in an open-magnet unit versus with patient supine in a closed-magnet unit. Radiology 2002; 223:501–08.
• Colaiacomo MC, Masselli G, Polettini E, et al. Dynamic MR imaging of the pelvic floor: a pictorial review. RadioGraphics 2009
• El Sayed RF, El Mashed S, Farag A, et al. Pelvic floor dysfunction: Assessment with combined analysis of static and dynamic MR imaging findings. Radiology 2008; 248:518
• Flusberg M, Sahni VA, Erturk SM, et al. Dynamic MR defecography: assessment of the usefulness of the defecation phase. AJR Am J Roentgenol 2011; 196:W394–W399.
REFERENCES