common paediatric ent problems - dubaiallergy.com · common paediatric ent problems bsme school...
TRANSCRIPT

Common Paediatric ENT
problems
BSME School Nursing Course
June 2 2016
Dr David Cremonesini
Aims
Management of:
Sore throats
Sleep apnoea
Earache
Neck lumps
Case 1
Fareed is 10yr old boy with lumps in his
neck
He had fever/sore throat 2 weeks ago now
ok
Mother worried about the lumps
He’s a bit tired
No weightloss/bruising/night sweats
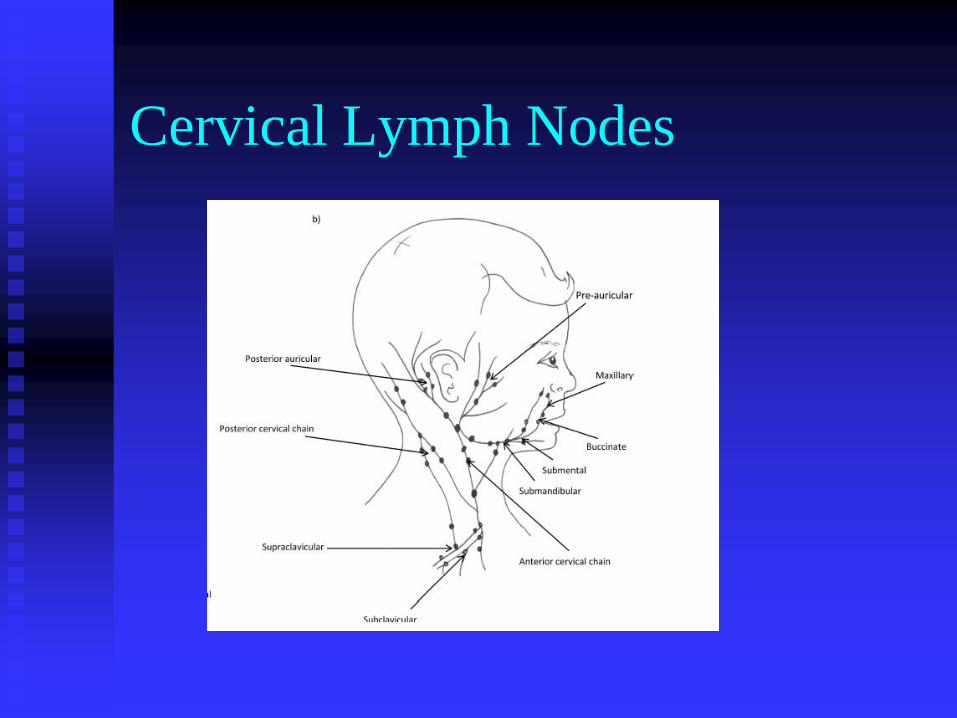
Cervical Lymph Nodes
Common problem in children
Thin necks so easily felt
Get lots of upper respirtaory infections
Studies show around 50% of healthy children
will have palpable lymph nodes at some point
Vast majority a benign response to self-
limiting infection but parents worry about
malignancy
Cervical Lymphadenopathy
-causes Infectious
viral
bacterial typical and atypical
Infected eczema
Oncology
leukaemia / lymphoma
Secondary
Kawasaki
Connective tissue disorders
Is it a node?
Cervical lymphadenopathy -
history Age
Onset and persistence of symptoms
Recent health
URTI / LRTI
Bruising
Weight loss, fever etc
PMH – immunodeficiency, CT disorders
Immunisation status

Cervical Lymphadenopathy -
Exam Growth and nutritional status
Skin – rashes, bruising / purpura, eczema
Is it a node?
Other nodes – axilla/ groin
ENT – esp tonsils
Chest
Abdomen – spleen
Actual lump:
Size, location, consistency, mobility, pain
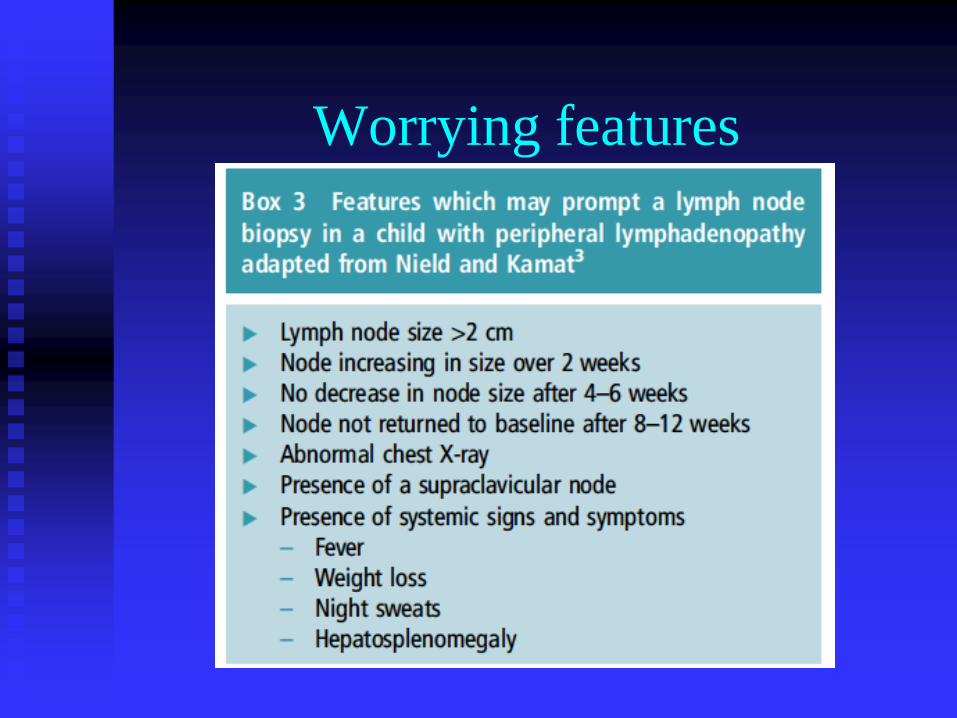
Worrying features
Case 2
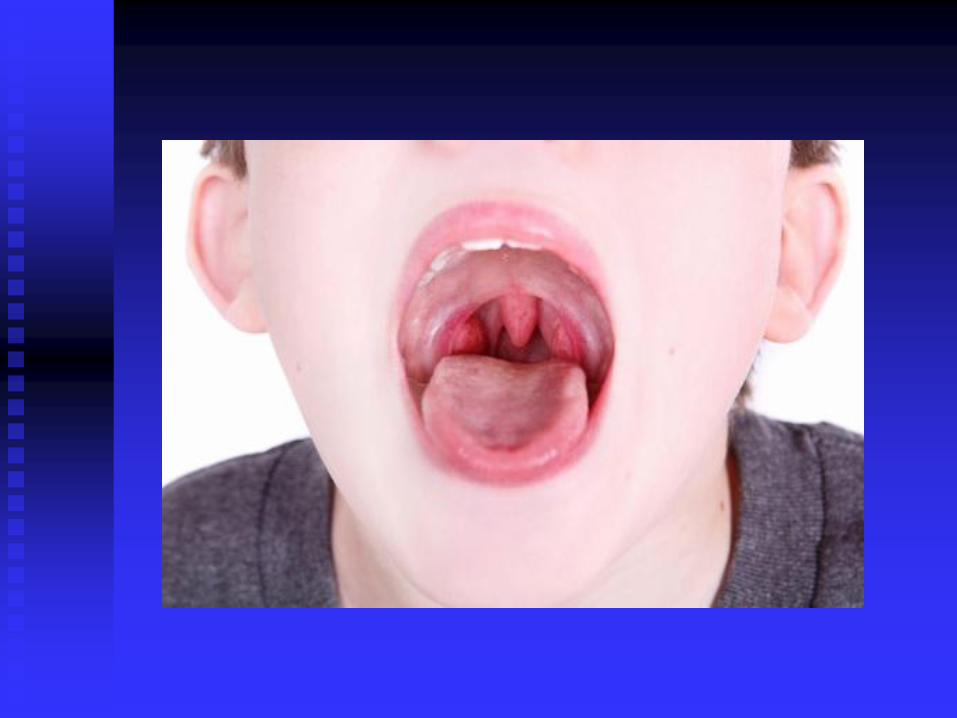
Leo is 5year old boy with sore throat
2 days, no fever
Throat looks red, what do you advise?
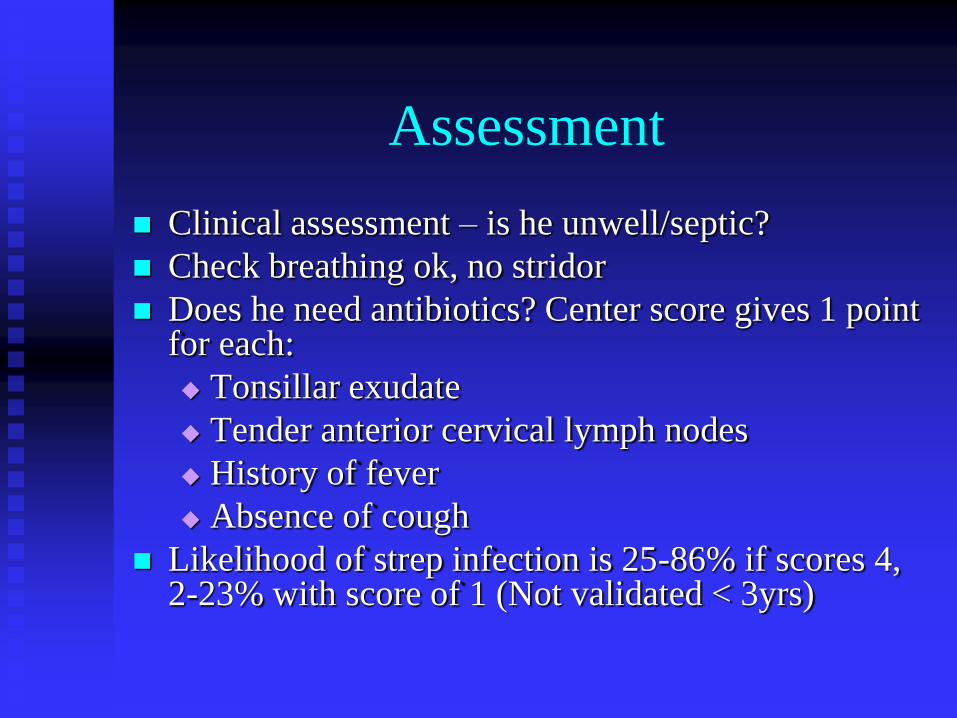
Assessment
Clinical assessment – is he unwell/septic?
Check breathing ok, no stridor
Does he need antibiotics? Center score gives 1 point for each:
Tonsillar exudate
Tender anterior cervical lymph nodes
History of fever
Absence of cough
Likelihood of strep infection is 25-86% if scores 4, 2-23% with score of 1 (Not validated < 3yrs)
Management
No antibiotics for symptomatic relief
Pain relief, paracetamol first line
Little evidence for lozenges, gargles and
sprays
Eat cool, soft food, drink plenty of fluids
Avoid smoking/smoky environments
Antibiotics
Should not be given routinely
In cases that warrant them first line is
Penicillin V / Amoxicillin for 10 days
2nd line is azithromycin for 5 days
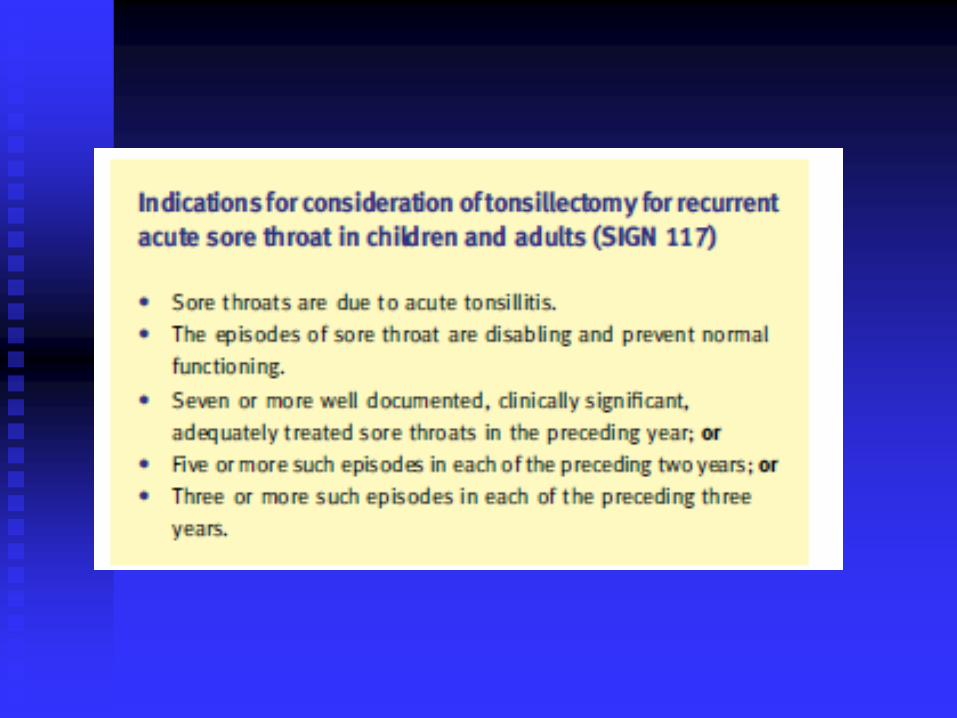
Recurrent sore throats
When should we take the tonsils out?
Benefit of tonsillectomy increases with the
severity and frequency of sore throats.
If not sure, watch and wait for 6 months
with parents reporting number and severity
of attacks
Antibiotic prophylaxis not recommended
Contraindications to
tonsillectomy
Caution if known bleeding disorder
Postpone surgery if episode of tonsilitis
within 2 weeks of date of surgery
Adenoidectomy contraindicated in presence
of cleft palate repair
Main risk is post-op bleeding, 2-5% chance
needing to go back to theatre
Case 2
Johnny is 3 years old
Mouth breathing all the time
At nursery is sleepy, not hungry in the
morning
Mother says he snores at night and is
worried his behavior is changing
What do you advise?
Sleep apnoea
Causes Airway –
Within - Obstruction
adenoids / tonsils
Structure airway
Trachomalacia, Pierre Robin
Muscle weakness Vocal cord paralysis
Without airway
Compression – vascular ring, fat
GI – reflux
Central – odines curse, seizure, arrythmia
Sleep apnoea
Presentation
Snoring / apnoea
Mouth breathing when awake
Day time tiredness
Poor school performance
Headache
Enuresis
Pulmonary hypertension / cor pulmonale
Sleep apnoea
Exam
Dysmorphic – facial abnormalities
Signs muscle disease
ENT – palate, tonsils
Nasal obstruction
Chest – deformity / distress

Sleep apnoea
Investigation
Oximetry
ENT opinion
plesmography
Early morning gas
ECG / echocardiography
Why is it a problem
Prevalence estimated 2-3% in children <10yrs
Recurrent obstruction leads to repeated desaturation each of which may cause arousal = sleep fragmentation
Sleep important esp growth hormone secretion and consolidation of memory
Associated with negative effect on cognition and behaviour with clear improvement post op
Can persist to adult life
Treatment
Adenotonsillectomy first line, though v
young children may only need adenoids
Small number problem may persist, then
consider CPAP/medicines
KEY MESSAGE is detection and
intervention
Case 3
Jessica has earache
Crying and in pain
No fever
You have a look in the ear…...
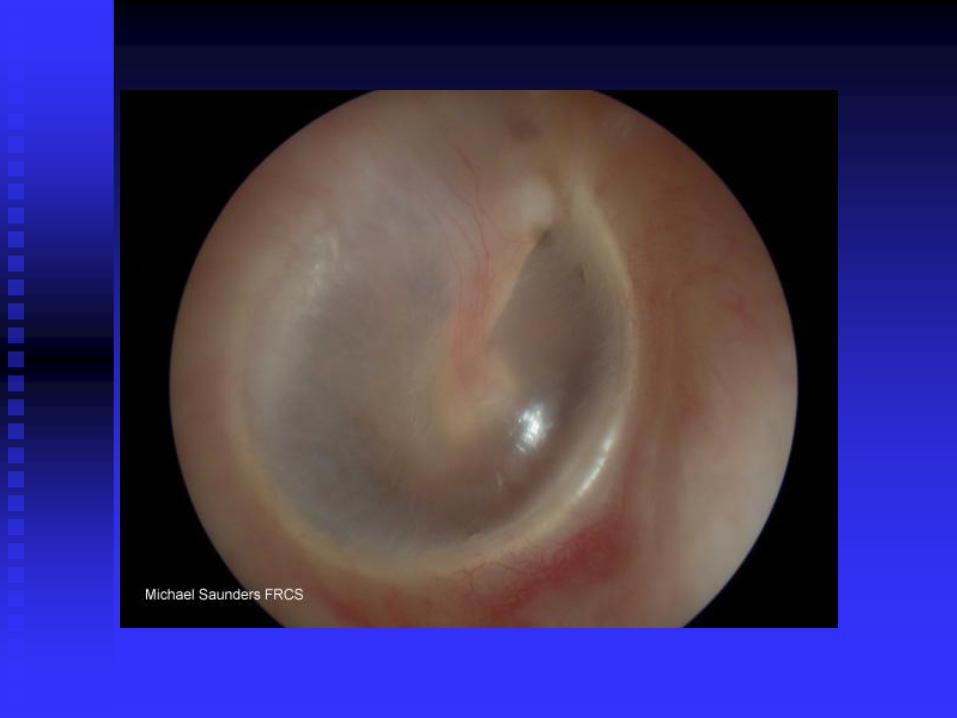
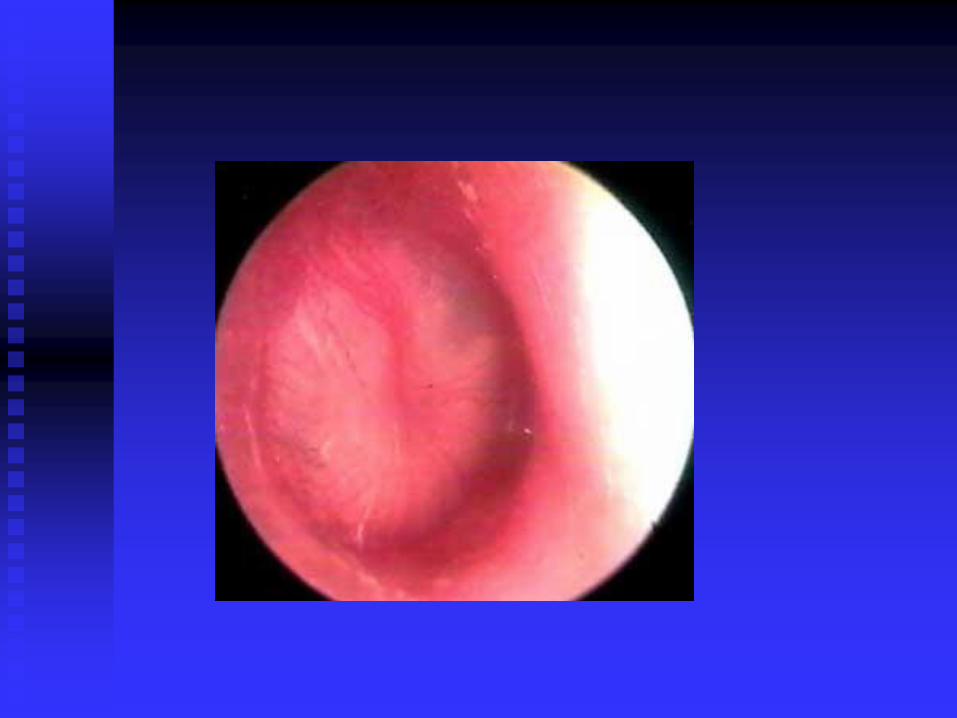
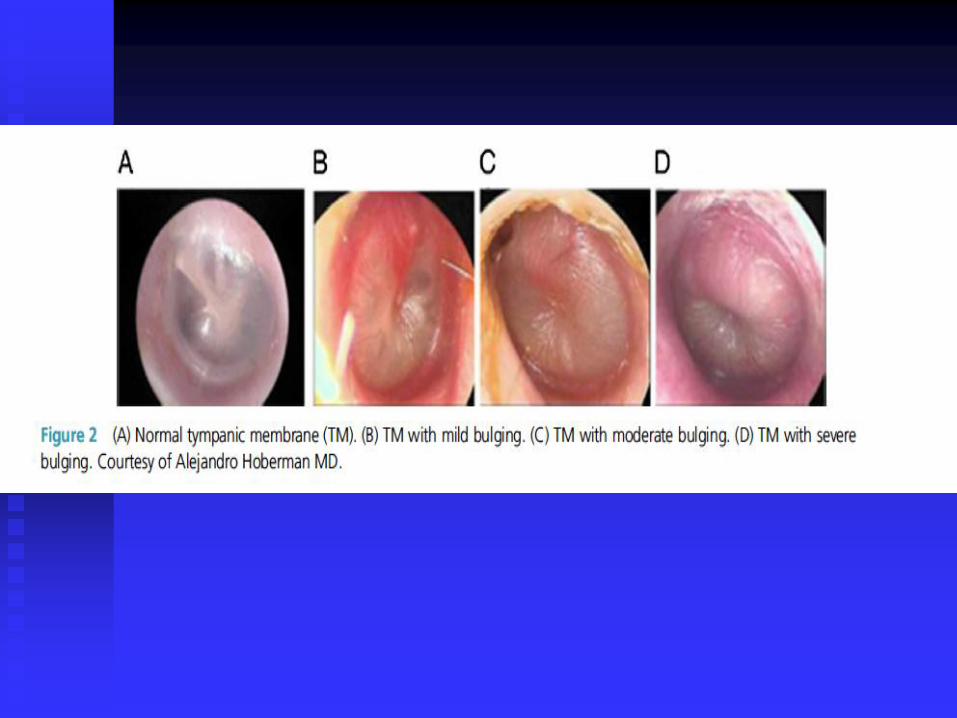
Diagnosing Acute Otitis Media
Look at position of the tympanic membrane
Moderate to severe bulging of TM or new
onset earache not due to otitis externa
May hve it if present with mild bulging,
<48hrs of pain and/or intense redness of TM
Severe AOM – AOM with moderate to
severe pain or fever > 39ºC
Acute Otitis Media
1.5 episodes of AOME/year in average child
Daycare, passive smoke, or wood burning heat – X 3-7 Age variable attack rate, most <2yo, big drop at 5yo
Males > females, 1.8:1
Otitis prone children average 3 episodes/6 months
Seasonal (less in summer)
Association with conjunctivitis or sinusitis
Viral prodromes frequently noted
Immunodeficiency predisposes: Ig deficiency, HIV
Genetic predisposition: Down syndrome, cleft palate, family history
Otitis Media
Inflammatory reaction to foreign antigens in the middle ear that cannot adequately drain via the eustachian tube.
Three major divisions
Acute otitis media with effusion (AOME)
Otitis media with effusion (OME)
Chronic draining otitis media (CDOM)
AOME or OME may be intermittent, persistent, or recurrent
Why does it happen
Altered ear “toilet”: secretions and refluxing
bacteria inadequately cleared
Stagnation of middle ear contents
Bacteria multiply in middle ear
Inflammatory/immune response (as much as 1
cc/hr)
Treatment
Simple analgesia – ibuprofen and/or paracetamol
Antibiotics wont help pain in first 24 hours
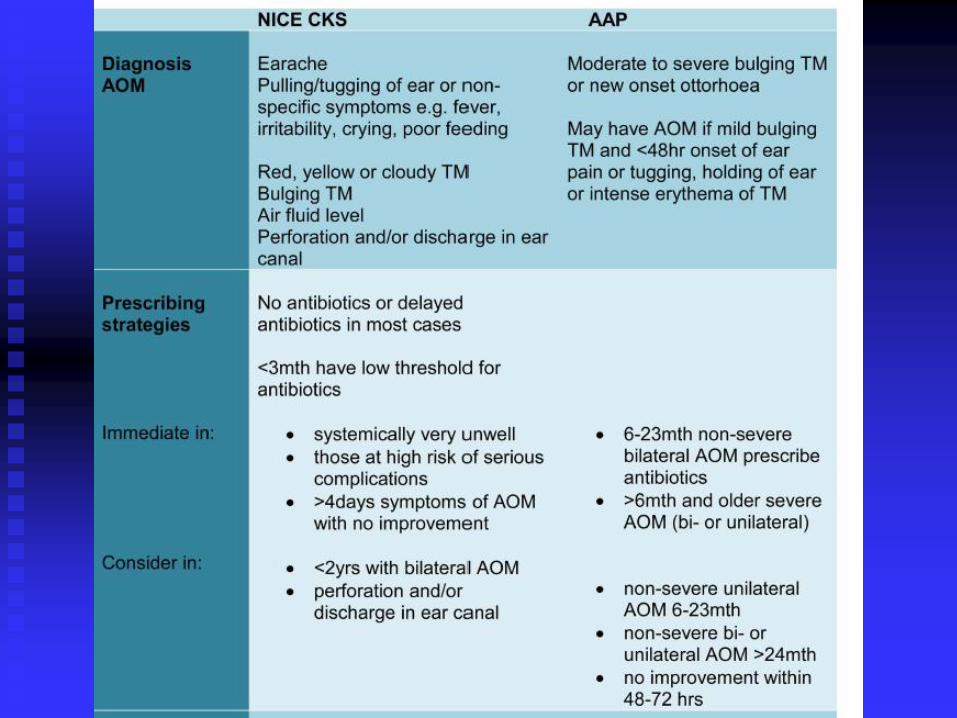
Antibiotics prescribed if:
Severe AOM in children > 6mths
Non-severe bilateral AOM 6-23mths
First choice is amoxicillin
Abx or observation for those with non-severe unilateral AOM (6-23mths) or non-severe uni or bi in > 2years. Give Abx if worsens after 2-3 days
Give for 5 days and longer if symptoms don’t improve
Key points
Routine Abx not warranted in non-severe
Ensure imms and adequate pain relief
Offer to observe/review in 2-3 days, maybe
seek advice if gets worse
Glue ear
Otitis Media with Effusion (OME)
commonest caus of childhood hearing loss
85% of children will experience episode of
OME during childhood, 50% resolve
spontaneously by 3 mths
Increase risk if not breastfed ot attend
daycare
Important to advise against smoking

Presentation
Hearing loss not main feature
Poor speech
Inattentiveness in class
Behavioural concerns
Reduced social interaction
Poor balance in younger children
OME - exam
Growth
Development
ENT
LRTI
Tympanometry
Hearing tests

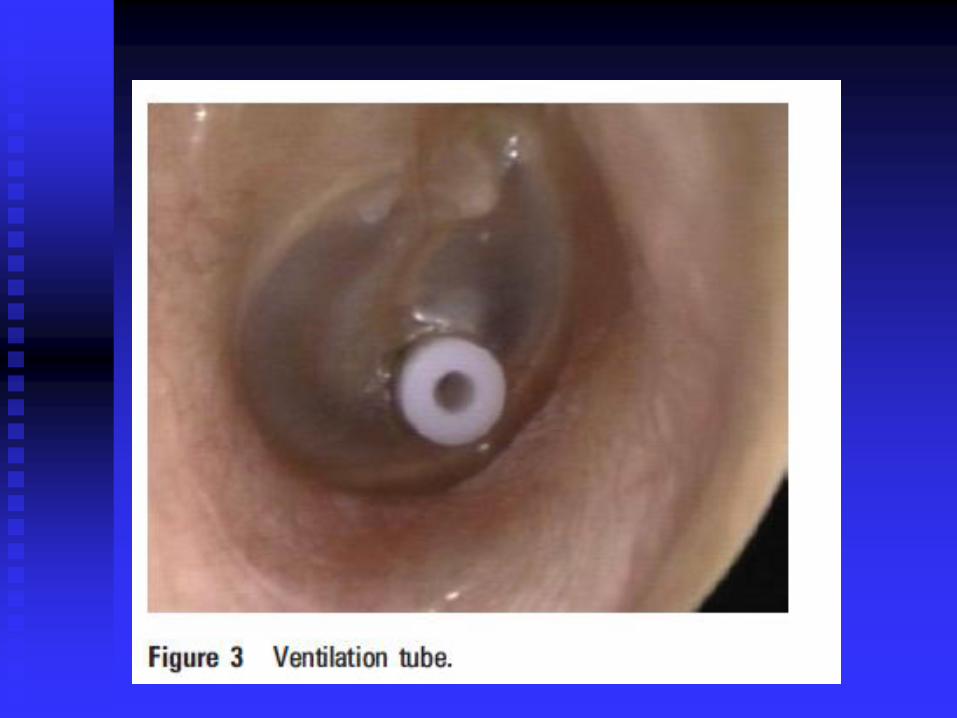
Management
Once confirmed, active monitoring over 3 months recommended
Usual first line is grommets
Medications rarely effective – little evidence for
Surgeyr if doesn’t resolve or gets worse during watching periodwith adverse affect on speech/education performance
Difficulty is knowing when to intervene or when ok to watch and wait, as after 12 mths likely to resolve
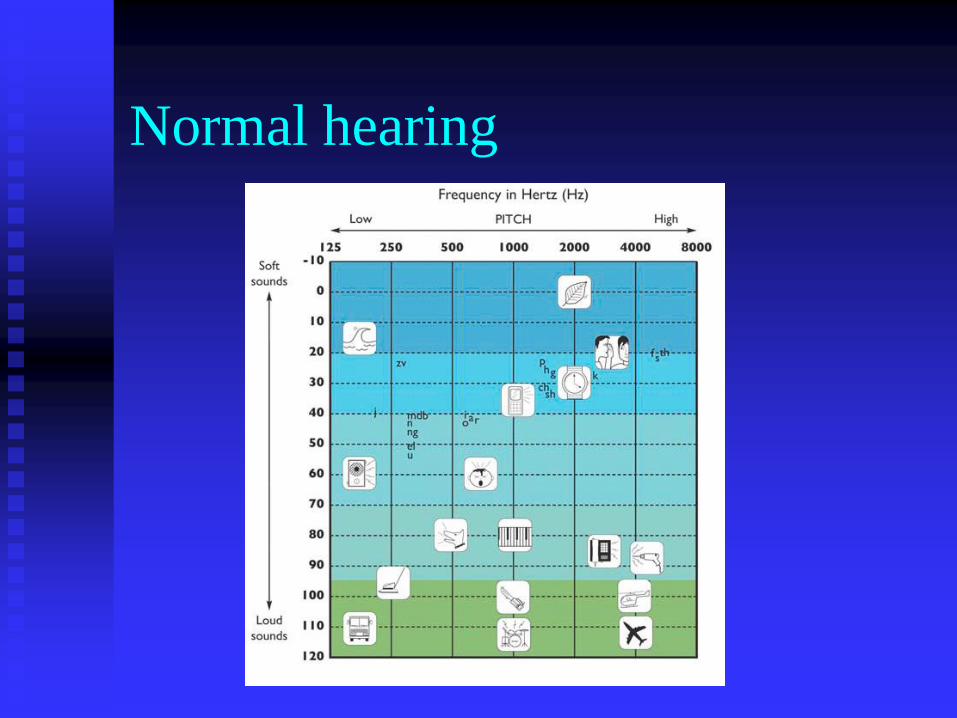
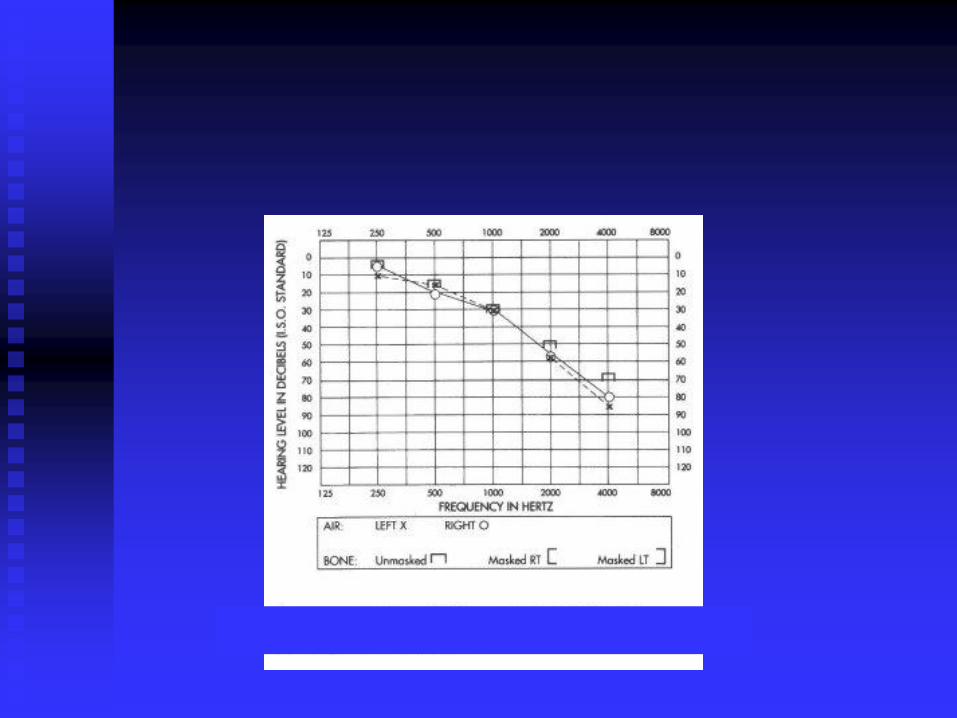
Normal hearing
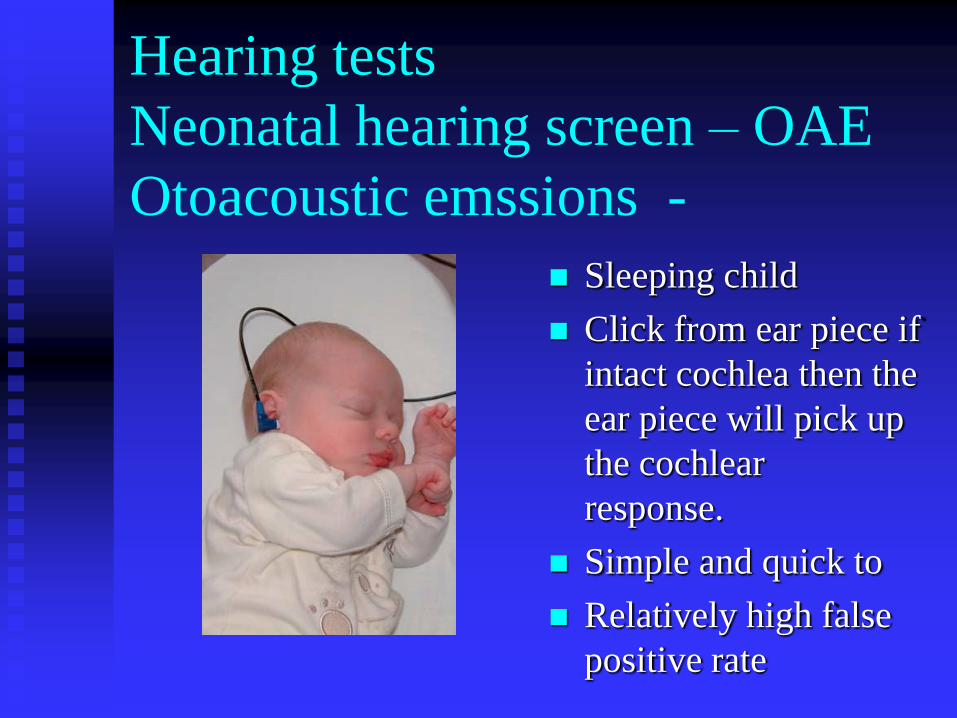
Hearing tests
Neonatal hearing screen – OAE
Otoacoustic emssions -
Sleeping child
Click from ear piece if
intact cochlea then the
ear piece will pick up
the cochlear
response.
Simple and quick to
Relatively high false
positive rate
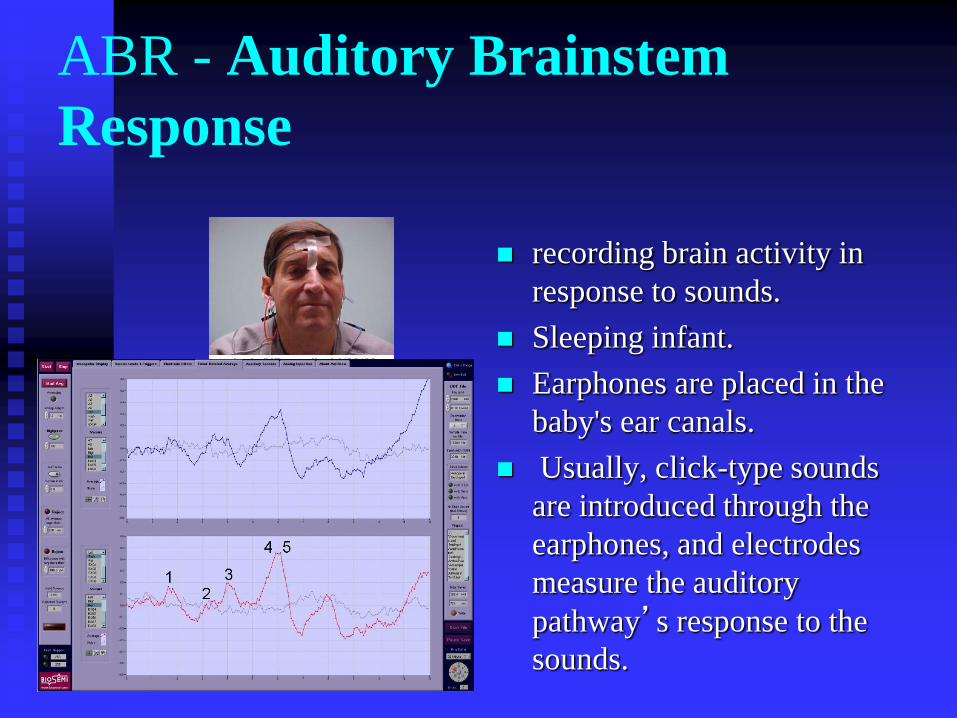
ABR - Auditory Brainstem
Response
recording brain activity in
response to sounds.
Sleeping infant.
Earphones are placed in the
baby's ear canals.
Usually, click-type sounds
are introduced through the
earphones, and electrodes
measure the auditory
pathway’s response to the
sounds.
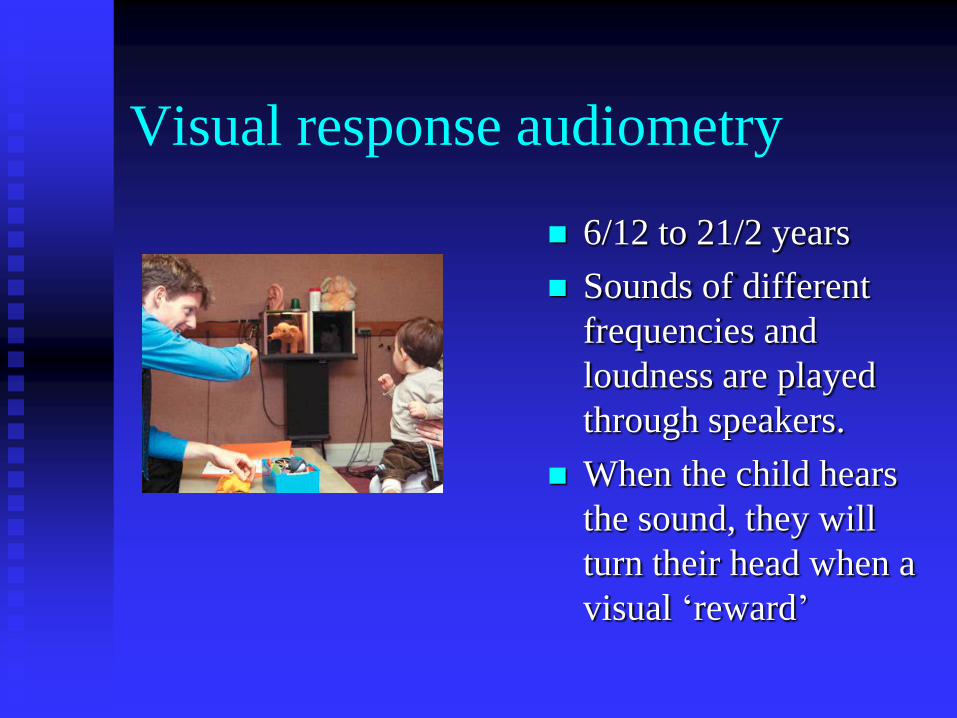
Visual response audiometry
6/12 to 21/2 years
Sounds of different
frequencies and
loudness are played
through speakers.
When the child hears
the sound, they will
turn their head when a
visual ‘reward’
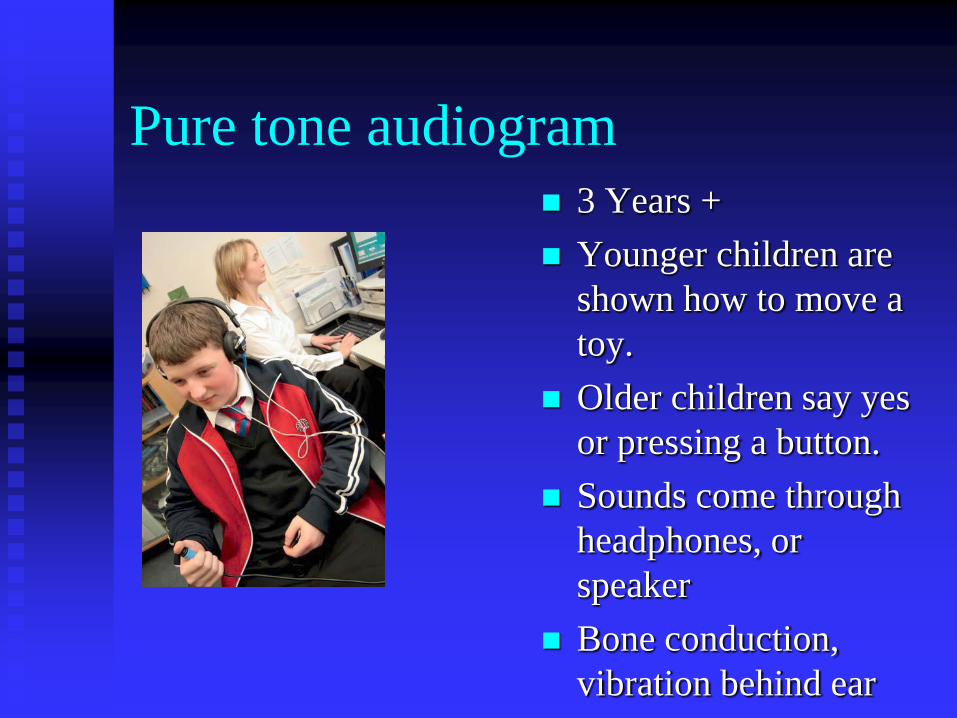
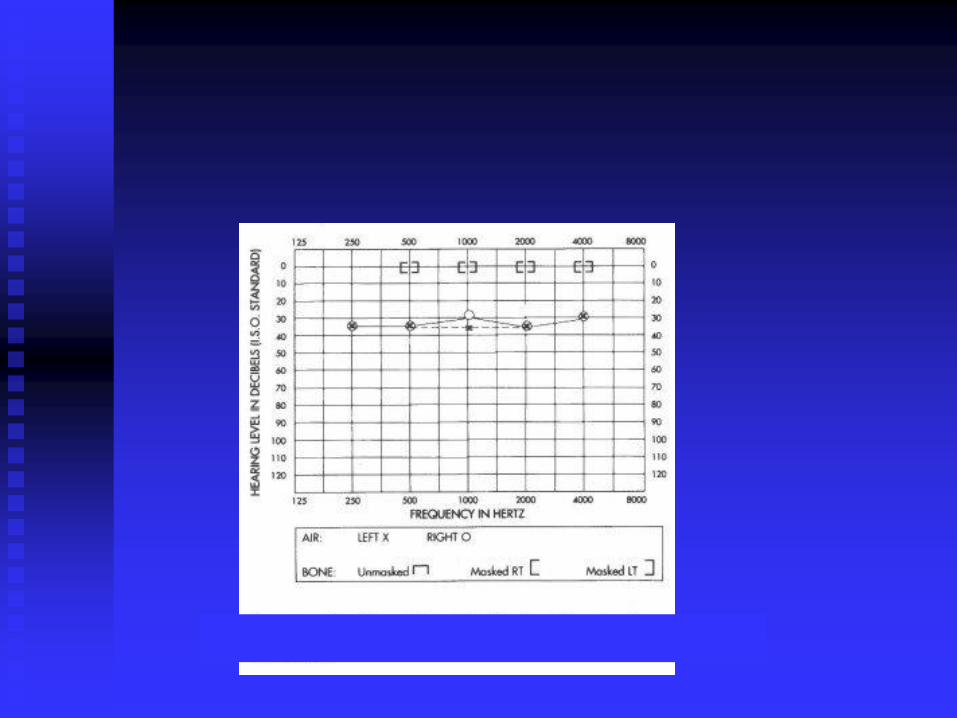
Pure tone audiogram
3 Years +
Younger children are
shown how to move a
toy.
Older children say yes
or pressing a button.
Sounds come through
headphones, or
speaker
Bone conduction,
vibration behind ear
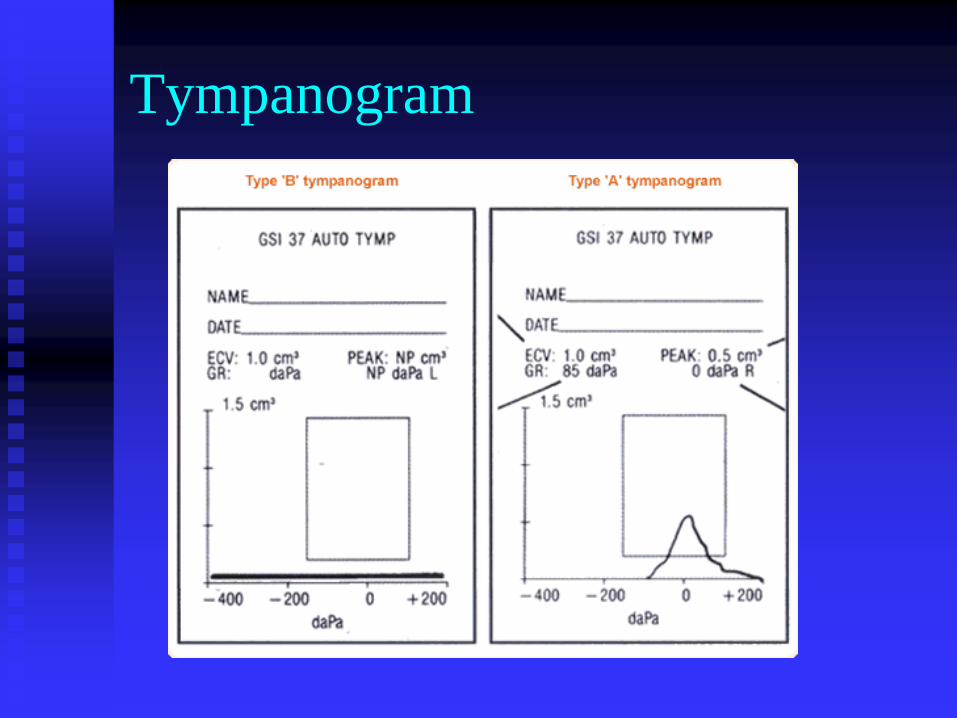
Tympanogram
OME Treatment
Wait 3 months
Risks and benefits
Advise on educational / behavioural strategies
Auto inflation – if will and can use
Avoid decongestants, antihistamines,
antibiotics, steriods, homeopathy, dietary
modification, acupuncture
Useful advice - preschool
Maximize hearing
‘Together time’ with parent
Reading picture books together
Visual cause and effect toys
Use of gestures
Encourage Peer group play
Encourage Imaginative play
Advice – school aged child
Classroom organization
Sitting at the front of the class
Better ear towards the teacher
Reduce ambient noise e.g. carpets, blinds, double glazed windows, material on walls, e.g. pin boards. Soft furnishings absorb noise.
Cue Using child’s name
OME treatment
If >25dB hearing loss for > 3/12 the grommets
50% of children who require one set of tubes will need second set within 1 year, and 15% will require a 3rd set
Some evidence that prolonged or repeated tube placement leads to excessive scarring of TM and permanent damage to TM
No evidence of long-term improvement in hearing due to tube placement
If refused / inappropriate then use hearing aids


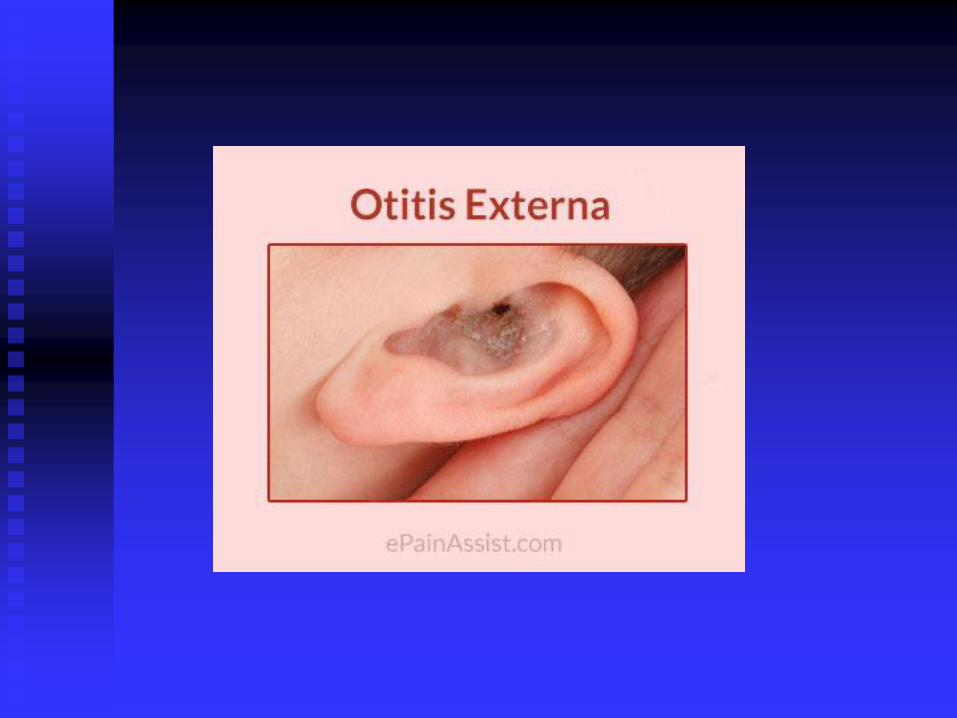
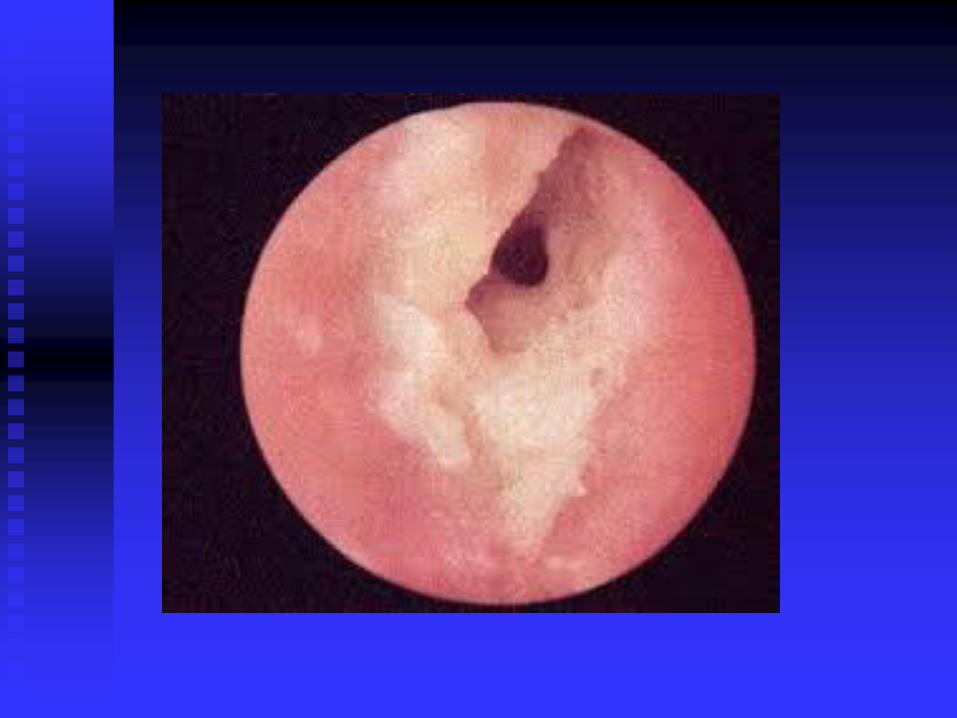
Otitis Externa
Inflammation of skin of ear canal
Swimming common association
External canal maybe:
Red/narrow/swollen
Pain on moving pinna/tragal tenderness
Discharge maybe from burst TM, then pain
better
Treatment
Topical antibiotic/steroid drops eg
Gentisone HC
Give for 2 weeks and review
If very swollen need ENT sooner
Redness spreading beyond ear needs urgent
review
Managing at home
Regular analgesia
Lie head on pillow, problem ear facing up,
give drops, massage the tragus and keep
still for 5-10mins
Keep ear dry
Continue for 1 week after symptom
resolution