come ventilare il paziente ipossiemico acuto andrea vianello fisiopatologia e terapia intensiva...
TRANSCRIPT

Come ventilare il paziente ipossiemico
acutoAndrea Vianello
Fisiopatologia e Terapia Intensiva RespiratoriaOspedale – Università di Padova
Non-Invasive Ventilation has demonstrated good efficacy in reducing risk of intubation and mortality; however, some potential etiologies of acute respiratory failure are associated with a high risk of NIV failure, which may lead to great hospital mortality.
Walkey AJ. Annals ATS 2013; 10:10-7

Talking about NIV failure:1. Epidemiology & Aetiology
2. Remedies to avoid failure
3. Transition to IMV: dancing in
the dark

Rate of NIV failure is extremely different according to study design,
severity of illness and level of monitoring

Overall NIV failure: 16.3%
Sixty-two RCTs including a total of 5870 patients

• Evaluation of all 449 patients receiving NPPV for a 1-yr period for acute or acute on chronic RF– CPE (n=97) – AECOPD (n=87)– non-COPD acute hypercapnic
RF (n=35) – postextubation RF (n=95)– acute hypoxemic RF (n=144)
• Intubation rate was 18%, 24%, 38%, 40%, and 60%, respectively
• Hospital mortality for patients with acute hypoxemic RF who failed NPPV was 64%
Schettino G. Crit Care Med 2008; 36:441-7
NIV – Real Life

Schettino G, Crit Care Med 2008; 36:441-7

Epidemiology
•Rationale: evidence supporting use of NIV varies widely for different causes of ARF.
•Population: 11,659,668 cases of ARF from the Nationwide Inpatient Sample during years 2000 to 2009;
•Objectives: To compare utilization trends and outcomes associated with NIV in patients with and without COPD.

Acute respiratory failure-associated diagnosis
Changing etiologies of ARF among patients receiving NIV

• 20% of patients without a COPD diagnosis who received NIV IMV;• 13.4% of patients with COPD who received NIV IMV;• Patients experiencing NIV failure before transition to IMV had greater hospital mortality than those initially on IMV

• Rationale: The patterns and outcomes of NIV use in patients hospitalized for AECOPD nationwide are unknown.
• Population: 7,511,267 admissions for acute AE occurred from 1998 to 2008;
• Objectives: To determine the prevalence and trends of NIV in AECOPD.

Use of NIPPV or IMV as first-line respiratory support in patients hospitalized with AECOPD

The percentage of patients transitioned from NIV to IMV ≈ 5% and did not increase from 1998 to 2008

Reasons for low rate of IMV use after NPPV, compared to
clinical trial:
• End of life decision to not accept IMV
• Patients died before IMV could be
started
• Good selection of appropriate patients

• High mortality rate (≈30%) ;↑ over time
• OR for death:1.63, compared to those initially on IMV
• ↑hospital stay

Reasons for high mortality rate in patients transitioned to IMV
• Increased use of NIPPV in patients difficult to ventilate?
• Continuation of NIPPV despite a lack of early improvement?

Aetiology of NIV failureA. Failure to adequately
ventilate/oxygenateA. Delayed NIV treatment
B. Inappropriate ventilatory technique
C. Patient’s clinical condition
B. Dependence on non-invasive
support
Lack of improvement of acute illness
C. Complications

NIV failure is predicted by:- Advanced age- High acuity illness on admission (i.e.
SAPS-II >34)- Acute respiratory distress syndrome- Community-acquired pneumonia with or
without sepsis- Multi-organ system failure
NIV trial in hypoxemic RF is justified if patients are carefully selected according to available guidelines, known risk factors and predictors for NIV failure.

NIV failure is predicted by:- Advanced age- High acuity illness on admission (i.e.
SAPS-II >34)- Acute respiratory distress syndrome- Community-acquired pneumonia with or
without sepsis- Multi-organ system failure


Retrospective analysis 59 episodes of ARF in 47
COPD patients• NIV success: 46• NIV failure: 13
Predictors for NIV failure:• Higher PaCO2 at admission• Worse functional condition• Reduced treatment
compliance
• Pneumonia
NIV in acute COPD: correlates for success
Ambrosino N, Thorax 1995;50:755-7
NIV failure
Other Pneumonia
%
0
20
40
60
n=8
p=0.019n=5

Summary of published studies for idiopathic pulmonary fibrosis
patients in the ICU

Retrospective analysis 60 episodes of ARF in ALS
patients managed by IMV via ETI• Initially on IMV: 31• Transitioned from NIV to
IMV: 29
• Dependence on NIV: 7 Predictors for survival:
• Age at admissionPercent survival of patients after
tracheostomy, stratified by age group
≥ 60 yrs
< 60 yrs
Patients with ALS

NIV complicationsComplication Inciden
ce (%)
MajorAspiration pneumonia <5
Haemodinamyc collapse Infrequent
Barotrauma Rare
MinorNoise 50-10
CO2 rebreathing 50-100
Discomfort 30-50
Claustrophobia 5-20
Nasal skin lesions 2-50

Pneumotorax associated with long-term non-invasive positive pressure ventilation in Duchenne muscular dystrophyVianello A , Arcaro, G, Gallan F, Ori C, Bevilacqua M
Neuromusc Dis 2004;14:353-55

NIV complicationsComplication Inciden
ce (%)
MajorAspiration pneumonia <5
Haemodynamic collapse Infrequent
Barotrauma Rare
MinorNoise 50-100
CO2 rebreathing 50-100
Leak/Discomfort 30-50
Claustrophobia 5-20
Nasal skin lesions 2-50

NIV reasons for failure
ACPE COPD Non COPD
ALI/ARDS
Hypoxemia + + +++
Hypercapnia + ++ +
Leak/Mask intol
+ + ++ ++
Secretion + + +
Mentation + + + +
Agitation + ++
Progression + +++
Failure Rate 18% 24% 37% 60%Schettino G, Crit Care Med 2008; 36:441-7

Remedies to avoid NIV failure
1.Select patients carefully2.Assess risk for failure; diagnosis,
etc3.Select comfortable mask4.Optimize vent settings5.Facilitate secretion removal6.Treat agitation7.Monitor closely in proper
location8.Assess response after 1 to 2 hrs

Remedies to avoid NIV failure
1.Select patients carefully2.Assess risk for failure;
diagnosis, etc3.Select comfortable mask4.Optimize vent settings5.Facilitate secretion removal

• Respiratory arrest• Inability to tolerate the device,
because of claustrophobia, agitation or uncooperativeness
• Inability to protect the airway, due to swallowing impairment
• Excessive secretions not sufficiently managed by clearance techniques
• Recent upper airway surgery
NIV should not be used in:
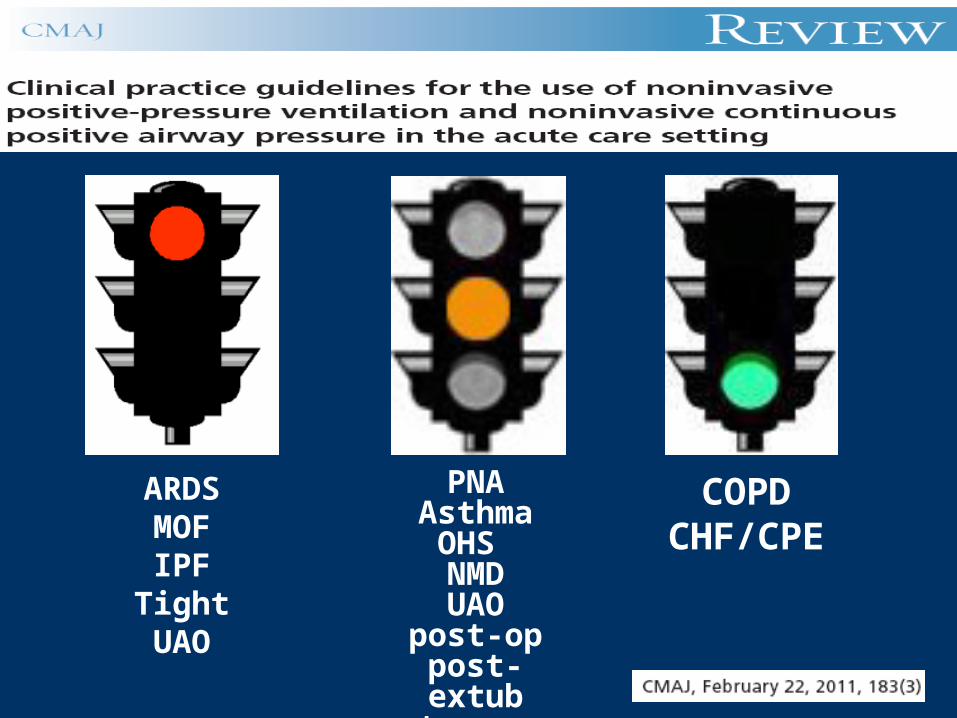
COPDCHF/CPE
PNAAsthma
OHS NMDUAO
post-oppost-extub
trauma
ARDSMOFIPF
Tight UAO
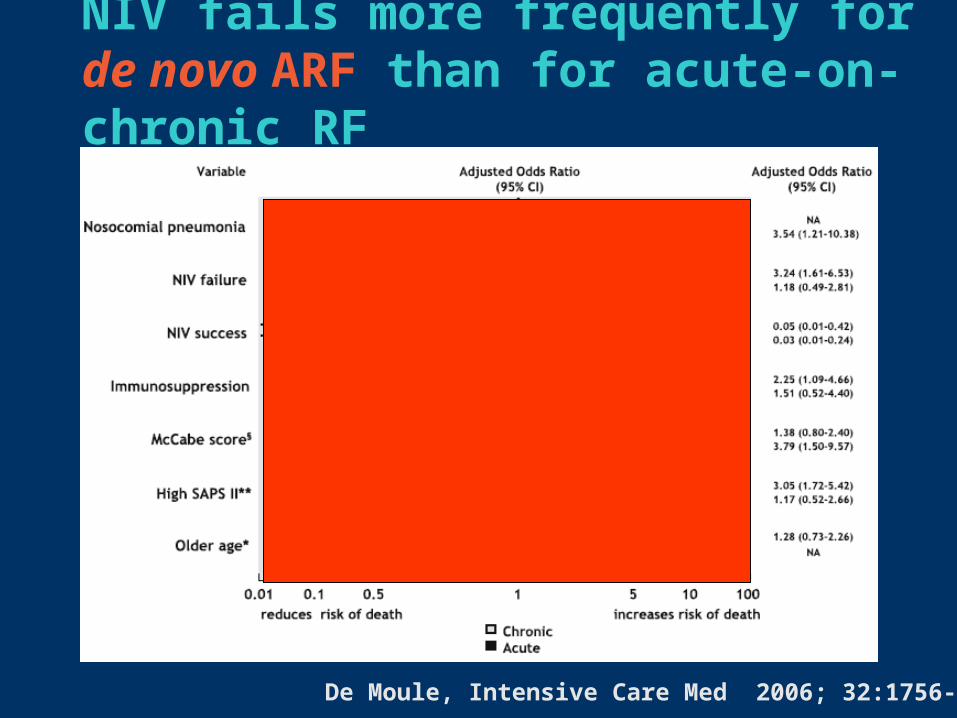
NIV fails more frequently for de novo ARF than for acute-on-chronic RF
De Moule, Intensive Care Med 2006; 32:1756-65
Remedies to avoid NIV failure
1.Select patients carefully2.Assess risk for failure;
diagnosis, etc3.Select comfortable mask4.Optimize vent settings5.Facilitate secretion removal
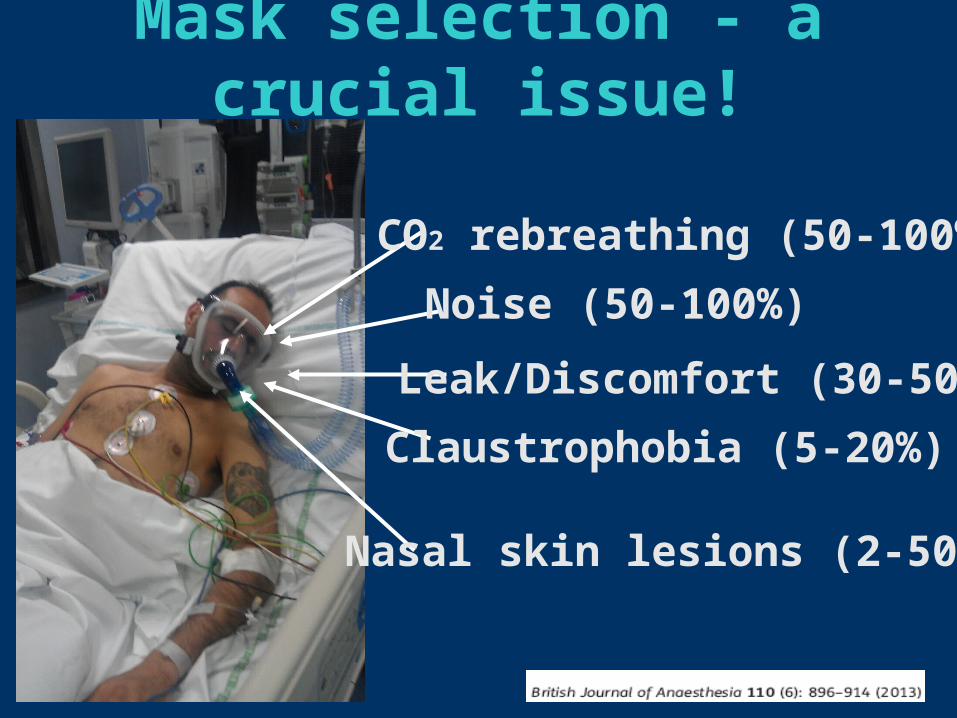
Mask selection - a crucial issue!
Noise (50-100%)
CO2 rebreathing (50-100%)
Leak/Discomfort (30-50%)
Claustrophobia (5-20%)
Nasal skin lesions (2-50%)

Choose correct interface and size!
Although there is no difference in ETI or mortality, RCT have reported that nasal mask is less tolerated than oronasal mask
Girault, Crit Care Med 2009;37:124-31Cuvelier, Intensive Care Med 2009;35:519-26
• The use of an oronasal mask is suggested rather than a nasal mask in patients who have ARF.• No recommendation about the use of an oronasal mask versus full face mask.

Remedies to avoid NIV failure
1.Select patients carefully2.Assess risk for failure;
diagnosis, etc3.Select comfortable mask4.Optimize vent settings5.Facilitate secretion removal

ICU Ventilator
VentilatorsFactors influencing preferred ventilator:
Personal experienceLocationAvailable monitoring
Leak compensationTrigger sensitivityHandlingFlexibilityAlarms
Portable Ventilator

The golden rule does not apply to ventilator setting, however:
• Pressure preset modes reduce the risk of failure and are recommended for COPD decompensated patients. French Guidelines for NIV treatment, 2008
• The “lung-protective” strategy may reduce the risk of barotrauma in patients with exacerbated ILD.
Fernandez-Perez ER, Chest 2008; 133:1113-9

Remedies to avoid NIV failure
1.Select patients carefully2.Assess risk for failure;
diagnosis, etc3.Select comfortable mask4.Optimize vent settings5.Facilitate secretion removal

Enhancement of secretion clearance
• Adequate hydration/humidification• Manually assisted cough• Cough assist• Antibiotics• Expectorants, mucolytics not of
known value

Am J Phys Med Rehabil 2005;84:83-8

Transition to IMV: when is in the interest of a patient?
• Hospital mortality: 64% (Schettino, 2008)
• Mortality rate: 30%; prolonged hospitalization (Chandra, 2011)
• Great hospital mortality (Walkey, 2013)

Transition to IMV(personal experience, 2011-2013)
Number of subjects 62
Age (mean ± SD) , yrs 65.4±19.3
Gender (males, females)
26, 36
Ineffective NIV, n (%) Severe hypercapnia Severe hypoxemia
52 (83.8)25 (42.4)21 (35.6)
Dependence on NIV, n (%)
8 (13.3)
NIV complication, n (%)
2 (3.4)
Tracheotomy, n (%) 16 (28.8)
Outcome , n (%) Died during hosp Discharged from hosp
41 (66.1)21 (33.9)

Kaplan-Meier function of overall survival
Median survival:46 days
(95% CI, 43 to 162)
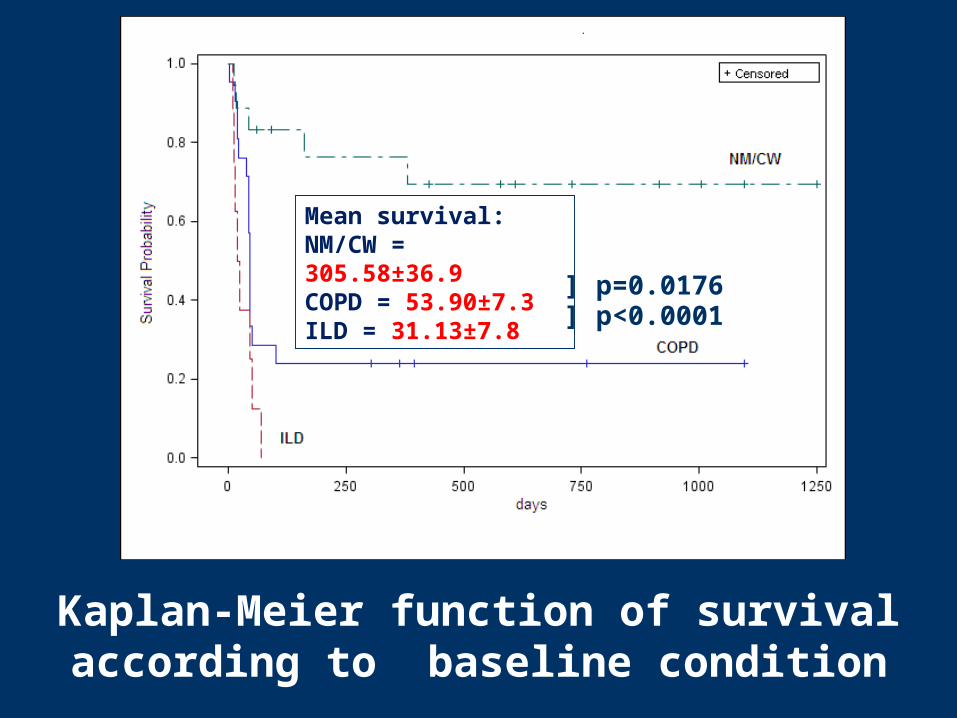
Kaplan-Meier function of survival according to baseline condition
Mean survival:NM/CW = 305.58±36.9COPD = 53.90±7.3 ILD = 31.13±7.8
] p=0.0176] p<0.0001

Kaplan-Meier function of survival for dichotomus age (50 and >50)
Median survival:50 = 380.0 d (95%CI, 15.0 to n.c.)>50 = 45.0 d (95%CI,24.0 to 54.0)
] p=0.0071

Remarks
• Mortality rate among patients transitioned to IMV is very high;
• The outcome of patients with ILD is extremely poor.
Should IPF/COPD patients be excluded from IMV after failing a NIV trial?

Conclusions• The boundaries for the use of NIV
continue to expand, however:
• Transitioning from NIV to IMV may not be in the interest of some categories of patients.
• The routine use of NIV in all patients with severe ARF is not yet supported• Caution should be used with NIV among patients at high risk of failure