combination vaccine within sanofi pasteur brief history ... sp combo.pdf · combination vaccine...
TRANSCRIPT
Combination Vaccine within Sanofi Pasteur
Brief History and focus on Pentaxim experience
Calmet J. September 2011

The trio that made it possible Veyrier-du-Lac, 1978
Charles Mérieux
Hans Cohen Jonas Salk
The Sanofi Pasteur combination approach is enrooted in Polio, through Injectable Polio
The problem in 1975
1. Safety of OPV in question
2. Efficacy in routine immunization with 3 OPV sub-optimal in the tropics
The challenge for IPV
1. Industrialize IPV production
2. Standardize antigenicity (test in vitro)
3. Demonstrate immunogenicity and efficacy both in developed and developing countries
4. License new product in all countries

Clinical Studies were conducted in West Africa
1 – Studies of immunogenicity of IPV of different
potency, adsorbed and non-adsorbed
Poliovirus Vaccines Type 2 Type 3 Type 1
320 32 64
8 16
4 2
80
20
5 0,5 1
Adsorbed
&
Non-adsorbed
Control : TT
2 – Studies of immunogenicity of 40-4-16 followed by 40-
8-32 D-Ag units for type 1, 2 and 3 respectively
3 – Studies of immunogenicity, effectiveness and
efficacy in Kolda, Sénégal
Dr. AL. Van Wezel and Dr. A. Kaboré
in Burkina Faso on an AMP mission for
FAIR
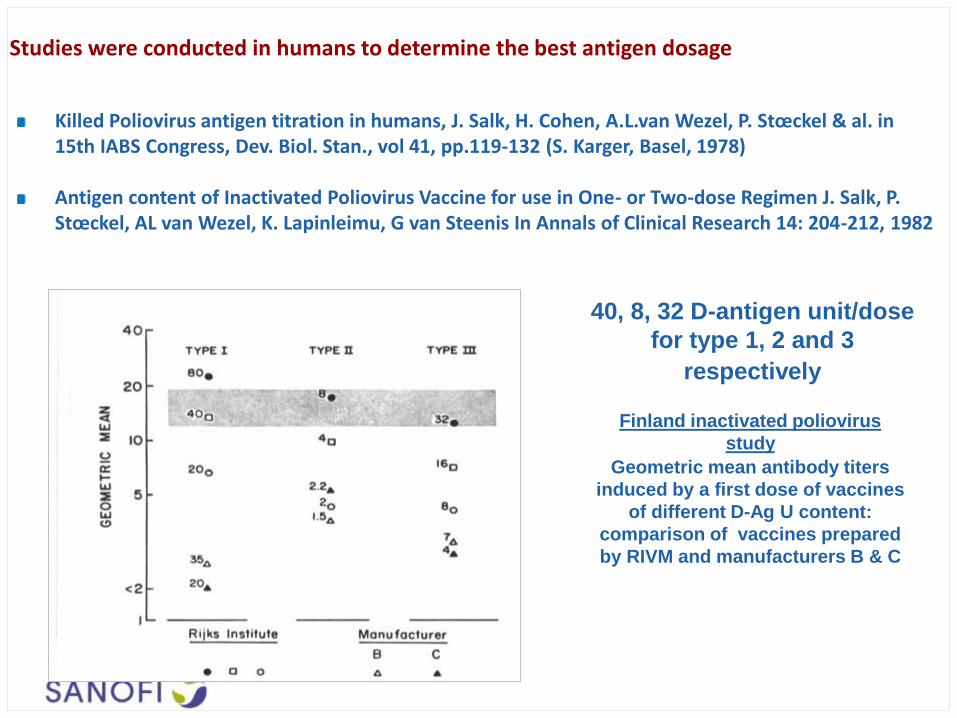
Studies were conducted in humans to determine the best antigen dosage
Killed Poliovirus antigen titration in humans, J. Salk, H. Cohen, A.L.van Wezel, P. Stœckel & al. in 15th IABS Congress, Dev. Biol. Stan., vol 41, pp.119-132 (S. Karger, Basel, 1978) Antigen content of Inactivated Poliovirus Vaccine for use in One- or Two-dose Regimen J. Salk, P. Stœckel, AL van Wezel, K. Lapinleimu, G van Steenis In Annals of Clinical Research 14: 204-212, 1982
40, 8, 32 D-antigen unit/dose
for type 1, 2 and 3
respectively
Finland inactivated poliovirus
study
Geometric mean antibody titers
induced by a first dose of vaccines
of different D-Ag U content:
comparison of vaccines prepared
by RIVM and manufacturers B & C

Clinical efficacy of a new, enhanced-potency, inactivated poliovirus vaccine was demonstrated during an outbreak of paralytic poliomyelitis in Senegal in 1986-87
Enhanced-potency vaccine (eIPV): 40, 8, 32 D-antigen unit/dose for type 1, 2 and 3 respectively The outbreak provided an opportunity to conduct a vaccine efficacy study of e-IPV in the Kolda region where it had been used since 1980. 89 cases, confirmed to have Poliomyelitis, were enrolled in a case control study, 5 matched controls being obtained for each case
Estimates of efficacy of e-IPV* in Kolda (Sénégal)
1 dose vs 0 doses
2 doses vs 0 doses
36% (0% - 67%)
89% (62% - 97%)
The Lancet, April 23, 1988
*AMP began a pilot vaccine delivery program in the Kolda region of Senegal in 1980. AMP used the quadruple DTwP-
eIPV vaccine prepared by Institut Mérieux. The formulation for Polio type 1,2 and 3 was respectively 40-4-16 D-antigen
units per dose in 1980 & 1981, and 40-8-32 thereafter. The vaccine was delivered by mobile team using jet injectors.

56 countries have already introduced IPV in their routine pediatric public vaccination schedule
Countries that have introduced IPV as of January 2011
Sources: WHO data + sanofi pasteur internal analysis
Countries that plan to introduce IPV

[1] Adapted from Orenstein WA. In: Brown et al. Dev Biol Stand. Basel 1997
Advantages of acP Vaccines Led to Increased Use and Increased Compliance
The base of combination vaccines (DTP) is affected by a technological shift: From whole cell to Acellular Pertussis

Since nearly 30 years, sanofi pasteur has developed a wide range of IPV-containing vaccines
Vaccine Product name 1st license Volume distributed since 1st
licensure Countries were registered
IPV Imovax Polio France, 1982 Over 272 M doses Over 90 countries
DTacP-IPV
Tetraxim Sweden, 1998 Over 15M doses Over 80 countries
Quadracel* Canada, 1997 Over 6,5M doses Australia, Canada, Mexico,
New Zealand
DTacP-IPV//Hib Pentaxim Sweden, 1997 Over 100M doses Over 100 countries
Pentacel* Canada, 1997 Over 55M doses North America
DTacP-IPV-Hib Pediacel Canada, 2000 Over 30M doses Over 45 countries
TdacP-IPV Adacel Polio Germany, 2001 Over 18M doses 25 countries
Td-IPV Revaxis Germany, 1999 Over 65M doses 54 countries
*mrc5-IPV containing vaccines
Sanofi pasteur marketed IPV containing vaccines as of May 2011

• 1st licensed in Sweden in 1997
• Licensed in >100 countries
• >110 Million doses distributed to date
* Licensed under the trade name PENTAVAC® in the European Union
PENTAXIM® Experience
Countries where PENTAXIM®* is licensed

PENTAXIM® : Increasing use in National Immunization Programs
• Pentaxim® is used Private markets of 80 countries around the world.
• Past / current National Immunization Program (NIP) / Public market use includes: • Austria, Belgium, France, Germany Iceland, Italy, Ireland, Spain, Portugal, Nordic countries
• Estonia, Latvia, Lithuania, Romania, Slovenia, Ukraine
• Dutch Antilles, French Polynesia, French Guiana, Guadeloupe, Martinique, Mayotte, New Caledonia
• Recent Pentaxim® Public Markets introductions has enabled the switch from wcP/OPV to acP/IPV: • Mexico
• Turkey
• Malaysia
• South Africa
• Planned expanded use of Pentaxim® in NIP in various regions of the world

• PENTAXIM®: administered in primary series during the first year of life has been
investigated under numerous schedules: • 2-3-4 months in 5 studies in France, Turkey and China
• 2-4-6 months in 4 studies in France, Sweden, Chile and Thailand
• 3-4-5 months in the study in China
• 3-5 months in the study in Sweden
• EPI schedule (6-10-14 weeks) in India, the Philippines and S. Africa
• In addition, PENTAXIM®
• Assessed in comparison to administration of separate vaccines in 3 studies
• Co-administration of Pentaxim with Hep B vaccines was assessed in 6 studies
• Booster administered in the second year of life investigated in most studies
PENTAXIM® has been Extensively Studied in Numerous Immunogenicity and Safety Trials around the Globe
() Langue et al. ESPID, 1997 () Mallet et al. ESPID, 1997 () Reinert. ESPID, 1997 () Kanra et al. Vaccine, 2000 () Li et al. 13th APCP, 2009 () Carlsson et al.
PIDJ, 1998 () Lagos et al. PIDJ, 1998 () Thisyakorn et al. SA J TMPH, 2010 () Dutta et al. 3rd APCP, 2009
() Madhi et al. 13th ICID, 2008 () Capeding et al. Bull WHO, 2008;86(6) () SP. Study A181 IVBI/A3R08396 ()
Immunogenicity of PENTAXIM®
Primary vaccination
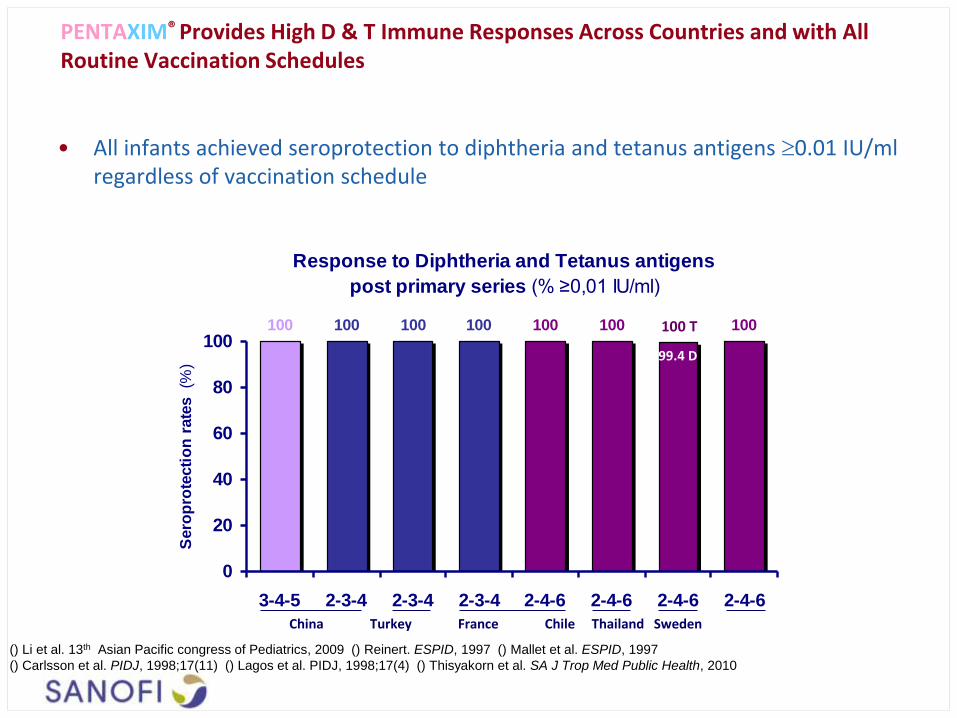
• All infants achieved seroprotection to diphtheria and tetanus antigens 0.01 IU/ml regardless of vaccination schedule
PENTAXIM® Provides High D & T Immune Responses Across Countries and with All Routine Vaccination Schedules
Response to Diphtheria and Tetanus antigens
post primary series (% ≥0,01 IU/ml)
100 100 100 100 100 99,4 100100
0
20
40
60
80
100
3-4-5 2-3-4 2-3-4 2-3-4 2-4-6 2-4-6 2-4-6 2-4-6
Sero
pro
tecti
on
rate
s (
%)
China Turkey France Chile Thailand Sweden
99.4 D
100 T
() Li et al. 13th Asian Pacific congress of Pediatrics, 2009 () Reinert. ESPID, 1997 () Mallet et al. ESPID, 1997
() Carlsson et al. PIDJ, 1998;17(11) () Lagos et al. PIDJ, 1998;17(4) () Thisyakorn et al. SA J Trop Med Public Health, 2010

• Seroconversion rates to PT & FHA antigens are similarly high (90.8% and 92.5% respectively) under all primary vaccination schedules
PENTAXIM® Provides High Immune Responses to PT and FHA across Countries and with All Routine Vaccination Schedules
Response to FHA antigen post primary series
(% ≥4-fold rise)
95.9 93.693.093.992.510095.999.6
0
20
40
60
80
100
3-4-5 2-3-4 2-3-4 2-3-4 2-4-6 2-4-6 2-4-6 2-4-6
Response to PT antigen post primary series
(% ≥4-fold rise)
100 98.9
100 90.8 92.4 94.1 91.393.9
0
20
40
60
80
100
3-4-5 2-3-4 2-3-4 2-3-4 2-4-6 2-4-6 2-4-6 2-4-6
Sero
co
nversio
n r
ate
s (
%)
Response to pertussis antigens post primary series
PT FHA (% 4-fold rise) (% 4-fold rise)
China Turkey France Chile Thailand Sweden China Turkey France Chile Thailand Sweden
() Li et al. 13th Asian Pacific congress of Pediatrics, 2009 () Reinert. ESPID, 1997 () Mallet et al. ESPID, 1997
() Carlsson et al. PIDJ, 1998;17(11) () Lagos et al. PIDJ, 1998;17(4) () Thisyakorn et al. SA J Trop Med Public Health, 2010

Response to Poliovirus antigens (PV1, PV2 and PV3)
post primary series (% 1/dil ≥8)
100100100100100100
0
20
40
60
80
100
3-4-5 2-3-4 2-3-4 2-3-4 2-4-6 2-4-6 2-4-6 2-4-6
Sero
pro
tecti
on
rate
s (
%)
• Seroprotection rates to all poliovirus antigens post primary vaccination are similarly high (>99%) under all vaccination schedules
China Turkey France Chile Thailand Sweden
Range 99.6-100
Range 99.3-100
PENTAXIM® Provides High Immune Responses to All Polio-viruses across Countries with All Routine Vaccination Schedules
() Li et al. 13th Asian Pacific congress of Pediatrics, 2009 () Reinert. ESPID, 1997 () Mallet et al. ESPID, 1997
() Carlsson et al. PIDJ, 1998;17(11) () Lagos et al. PIDJ, 1998;17(4) () Thisyakorn et al. SA J Trop Med Public Health, 2010
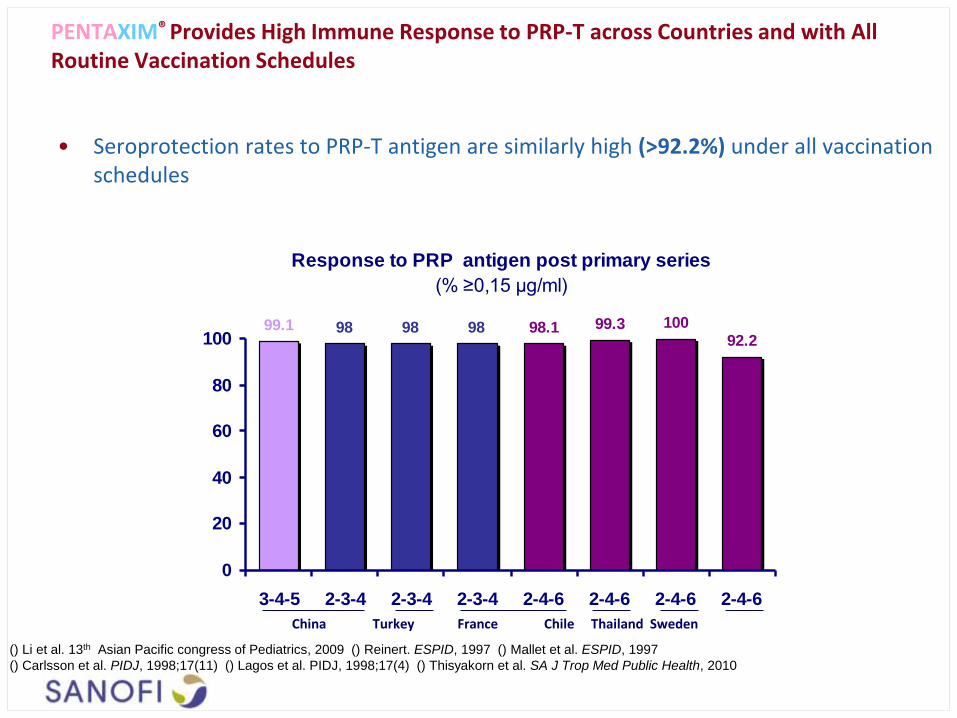
Response to PRP antigen post primary series
(% ≥0,15 µg/ml)
99.1 98 98 98 98.1 99.3 10092.2
0
20
40
60
80
100
3-4-5 2-3-4 2-3-4 2-3-4 2-4-6 2-4-6 2-4-6 2-4-6
• Seroprotection rates to PRP-T antigen are similarly high (>92.2%) under all vaccination schedules
PENTAXIM® Provides High Immune Response to PRP-T across Countries and with All Routine Vaccination Schedules
China Turkey France Chile Thailand Sweden
() Li et al. 13th Asian Pacific congress of Pediatrics, 2009 () Reinert. ESPID, 1997 () Mallet et al. ESPID, 1997
() Carlsson et al. PIDJ, 1998;17(11) () Lagos et al. PIDJ, 1998;17(4) () Thisyakorn et al. SA J Trop Med Public Health, 2010

Safety of PENTAXIM®
Sanofi Pasteur. Data in File
9.8
26.9
8.3
30.9
1.2
15.8
22.9
53.3
13.9 17.2
29.5
1.0
TETRAXIM™
DTwcP-IPV
% o
f s
ym
pto
ms
redness induration pain fever fever irritability abnormal vomiting drowsiness
[38-38.9°C] ≥39°C crying
0
10
20
30
40
50
60
70
80
11.6
4.7
21.3
34.4
9.7
23.5
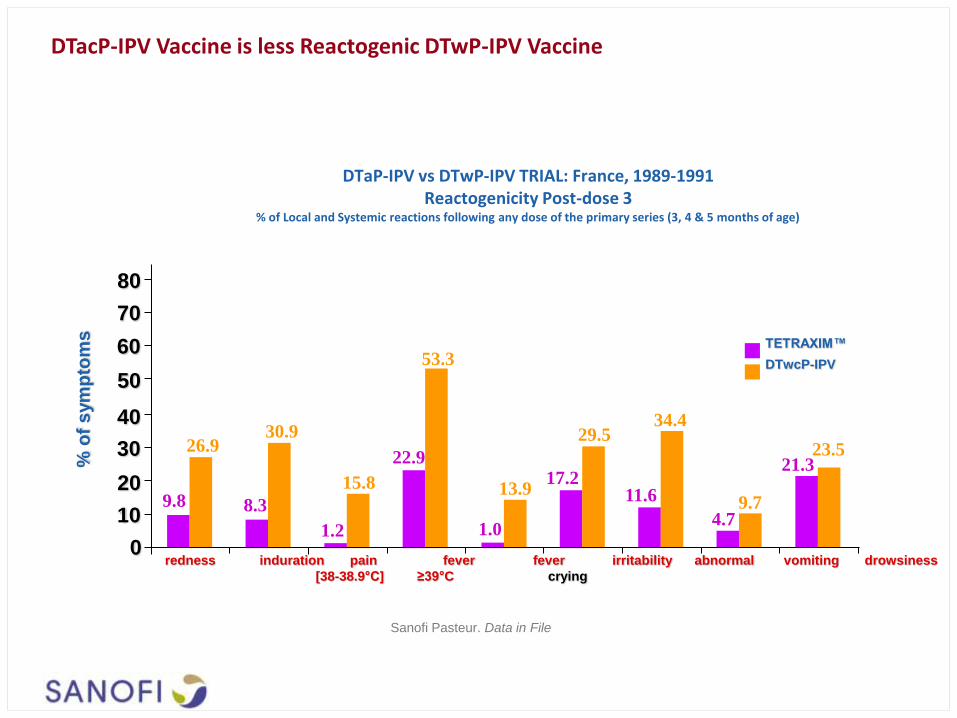
DTaP-IPV vs DTwP-IPV TRIAL: France, 1989-1991 Reactogenicity Post-dose 3
% of Local and Systemic reactions following any dose of the primary series (3, 4 & 5 months of age)
DTacP-IPV Vaccine is less Reactogenic DTwP-IPV Vaccine

• The safety of Pentaxim vs Tetraxim + Hib was assessed in 2195 French infants primed at 2-3-4 and boosted at 16-24 months of age (Reinert; Clin rep) • Incidences of local reactions were similarly low in both vaccine groups
Local reactions following any dose of primary vaccination
(at 2-3-4 months) and booster (at 16-24 months)
(France 1995, 2195 infants)
0.6
11.114.4
1.1
9.512.4
3.4
23.120.4
2.9
21.418.2
0
20
40
60
80
100
Induration Redness other
Inc
ide
nc
e (
%)
() Reinert et al. ESPID, 1997; Ab. 75
Pentaxim® (n=3248 primary doses)
(n= 589 booster doses)
DTaP-IPV (n=3202 primary doses)
(n= 555 booster doses)
PENTAXIM®: As Well Tolerated As Separate Injections of DTaP-IPV and Hib
Primary Booster Primary Booster Primary Booster
Induration Redness Other

• Incidences of systemic reactions were similar in both vaccine groups
• Most fever episodes were below 39°C (fever 39°C <1.0% in both groups after primary series)
Incidence of fever increased after the booster (22.1 and 23.8% respectively)
• No HHE, seizure, nor SAE related to vaccination were detected reported after primary or booster vaccination in either group
PENTAXIM®: As Well Tolerated As Separate Injections of DTaP-IPV and Hib
() Reinert et al. ESPID, 1997; Ab. 75
Systemic reactions following any dose of primary vaccination
at 2-3-4 months of age
(France 1995, 2195 infants)
7.1
0.2
15.19.79.3 7.2
0.1
19.6
9.99.5
0
20
40
60
80
100
Fever ³38°C Drowsiness Irritability Inconsolable crying Other
Incid
en
ce (
%)
Pentaxim® (3254 doses)
DTaP-IPV (3211 doses)

Data from the 10-year Report
(1 Oct 1997 – 31 Dec 2007)
Swedish National Surveillance System
Swedish Institute for Infectious Disease
Control
Long-term impact of PENTAXIM® in the
reduction and control of pertussis in Sweden
(1997-2007)

• 1979 – withdrawal of wcP vaccine in Sweden due to safety concerns [1]
• 1996 – introduction of acP vaccines, switching from DT to DTacP at 3-5-12m; 3-dose coverage
reached 98-99% within a year. [1]
Without pertussis vaccination (1979-96), pertussis remained highly endemic in Sweden until introduction of acP vaccines
Cases of pertussis per year in Sweden [adapted from (1)]
[1] Gustafsson L, Carlsson RM. TEN YEAR REPORT – Pertussis surveillance in Sweden progress report October 1, 1997 – December 31, 2007.

Age-specific incidence of pertussis before and after introduction
of DTacP in 1996 (national cohort) [adapted from (1)]
Introduction of acellular pertussis vaccines reduced the incidence of pertussis in Sweden
• Birth cohorts after introduction of acP had a much lower age-specific incidence of pertussis than had the corresponding age-groups before introduction of acP
• The modest increase in pertussis incidence approximately 5 years after the acP doses were administered could suggest waning of protection.
[1] Gustafsson L, Carlsson RM. TEN YEAR REPORT – Pertussis surveillance in Sweden progress report October 1, 1997 – December 31, 2007.

Conclusions
• Acellular/IPV combination vaccines are well documented in terms of • Safety
• Effectiveness
• Programmatic suitability
• With more than 30 years of experience, Sanofi Pasteur can: • Provide a wide range of different combination vaccines, adapted to various scheme,
including for booster dose.
• Provide a documented effectiveness of its Pentavalent vaccine when used in national programs
• Considering the changes both in terms of epidemiology (disappearance of polio, shift in age of pertussis) and technology (switch to acellular pertussis), all parameters are in line with a safe introduction of a combination vaccine in most region of the globe as long as the region is non polio endemic and the program can be sustainably funded by the public sector.