combat and operational stress alan ogle, maj, usaf, bsc military psychology psy4990 university of...
TRANSCRIPT

Combat and Operational Stress
Alan Ogle, Maj, USAF, BSC
Military Psychology PSY4990
University of West Florida, Spring 09

Disclaimer: information in this briefing was compiled from multiple sources in the US military medical services. Many have been modified or shortened to fit the educational purpose, format and training time available. Views expressed are those of the author and do not reflect the official policy or position of the United States Air Force, Department of Defense, or the U.S. Government.

3
War
Bad news
There is a psychiatric cost to sending young men
and women to war
Really bad news
No one is immune
Good news
Vast majority survive
Really good news
Resiliency is the norm
The War (OIF/OEF)
Deployers: 1.64 million US Service Members
Casualties: 4,620 77 Air Force
Wounded: 32,409 473 Air Force
Data include dates: 7 Oct 01 – 21 Jun 08

Battlefield
Battlefield

7

OIF Combat ExperiencesU.S. Army 2003
Being attacked or ambushed - 89% Receiving incoming fire - 86% Being shot at - 93% Seeing dead bodies or remains - 95% Knowing someone seriously injured or killed - 86%
Three Signature Injuries of OIF/OEF
Extremity amputations 803 (Jul 08)
Traumatic Brain Injury 320,000 (Jan 08)
Post Traumatic Stress Disorder/ Depression 300, 000 (Jan 08)
OEF/OIF TBI and PTSDJan, 2008
Traumatic Brain Injury (TBI) 19.5% report experiencing a probable TBI during deployment Estimated 320,000 cases of TBI Total annual costs of the 2776 cases identified by mid-2007 is
$591-910M. Post Traumatic Stress Disorder (PTSD)
18.5% of veterans meet criteria for PTSD or Major Depressive Disorder (MDD)
14% of returning service members currently meet criteria for PTSD Estimated 300,000 cases of PTSD/MDD Estimated societal costs of PTSD/MDD for the 2 years after
returning from deployment is $4.0 – 6.2B 35% of OIF veterans access MH services after returning home

Occupational Morbidity (Jan, 2008)(six months following hospitalization)
45 - 50% Army AD members psychiatrically hospitalized left military service
11 – 12% Army AD members hospitalized for non-MH diagnoses left military service
Those separated for a MH condition had higher rates of disability than those separated for non-MH medical conditions

Vision: Healthy/Mission Ready Communities
Deployment Behavioral Health
13
Combat and Operational Stress Control
Combat stress includes all the physiological and emotional stresses encountered as a direct result of the dangers and mission demands of combat
Combat and operational stress control may be defined as programs developed and actions taken to prevent, identify, and manage adverse combat and operational stress reactions (COSR)
This program optimizes mission performance; conserves the fighting strength; and prevents or minimizes adverse effects of COSR
14
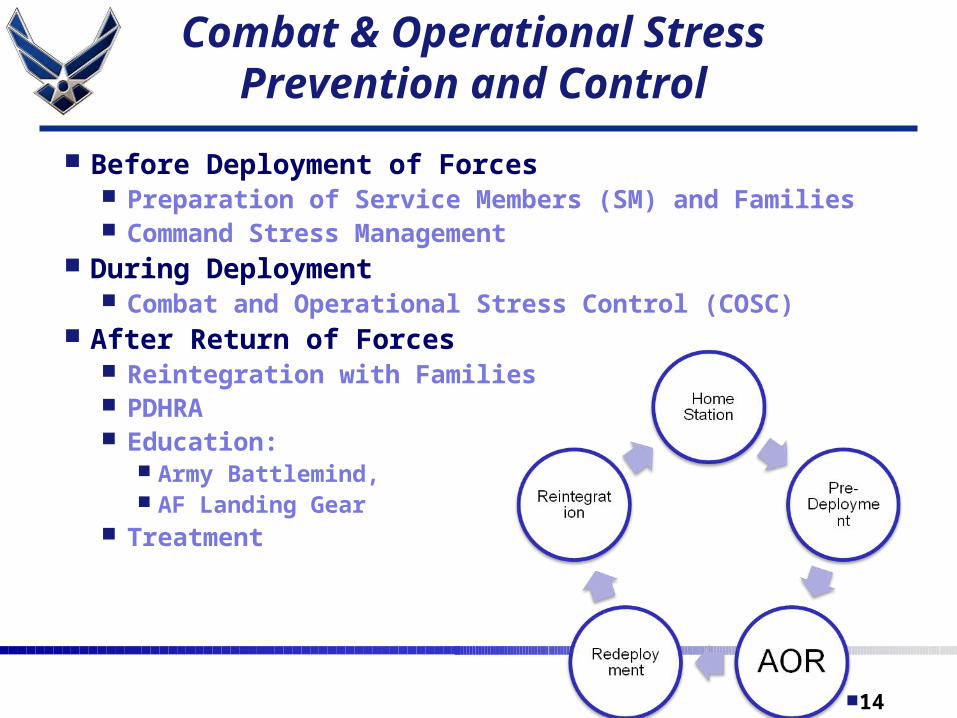
Before Deployment of Forces Preparation of Service Members (SM) and Families Command Stress Management
During Deployment Combat and Operational Stress Control (COSC)
After Return of Forces Reintegration with Families PDHRA Education:
Army Battlemind, AF Landing Gear
Treatment
Combat & Operational Stress Prevention and Control

15
Basics of Stress Management
Stress is normal part of life, healthy unless either excessive or individual has less developed stress management resources
Sources of potentially excessive stress: Multiple life stressors Deployment and Operational Stress High work stress coupled with poor unit cohesion Isolation from spouse/normal supports
Stress Management is balancing stress load and coping resources
16
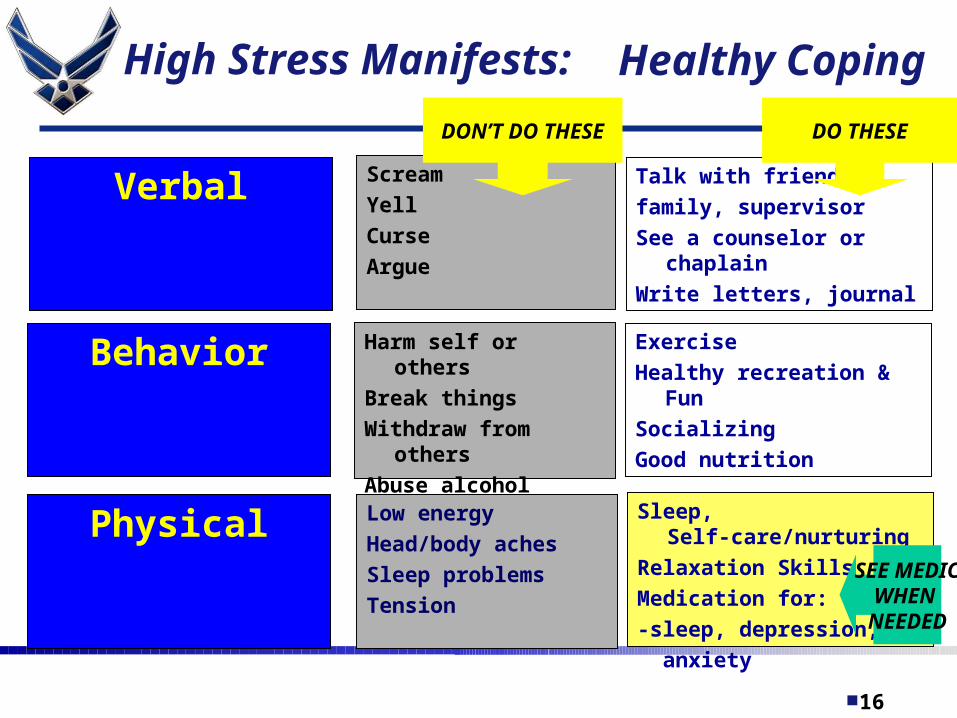
Healthy Coping
Verbal
Low energy
Head/body aches
Sleep problems
Tension
Behavior
Physical
Harm self or others
Break things
Withdraw from others
Abuse alcohol
Scream
Yell
Curse
Argue
Exercise
Healthy recreation & Fun
Socializing
Good nutrition
Talk with friends,
family, supervisor
See a counselor or chaplain
Write letters, journal
Sleep, Self-care/nurturing
Relaxation Skills
Medication for:
-sleep, depression,
anxiety
DON’T DO THESE DO THESE
SEE MEDICWHEN
NEEDED
High Stress Manifests:

17
Deployment Stress Control
Good leadership by officers / noncommissioned officers (NCOs)
Good equipment, supplies etc. Good unit cohesion, confidence, focus Pre-deployment training:
Realistic What to expect What is expected of them Healthy coping strategies Resources for help if needed

18
Care for Families
Service members need to know their families are taken care of Needs met—medical, financial, household etc. Ongoing communication-phone, mail, email, video
Healthy coping by families Unit support of families Family Readiness Groups (FRGs) Sample Training for Soldier and Spouse @
https://www.battlemind.army.mil/
19
Commanders
Officer and Enlisted leaders are the most important in unit stress management program
Attending to soldiers needs and concerns Good leadership Sample Leaders Training @
https://www.battlemind.army.mil/

Support During Deployment
Trauma Stress Response Teams/Unit Consultation
Mental health services in theater Combat Operational Stress Control Units (COSC) Air Force EMED CASF Theater Hospital
Post-Deployment Health Assessment

21
COSC Facilities
“Armor up,
Prevent when you can,
Treat when you must”

22
Combat and Operational Stress Control
Its goal is to return Soldiers fit for duty expeditiously
The purpose of COSC is to promote soldier and unit readiness by― Enhancing adaptive stress reactions Preventing maladaptive stress reactions Assisting soldiers with controlling COSRs Assisting soldiers with behavioral disorders

23
TRIAGE CATEGORIES FOR COSR CASES
The following are triage categories that may be used for COSR cases: Help-in-place Rest Hold Refer

24
TRIAGE CATEGORIES FOR COSR CASES
HELP-IN-PLACE (HIP) Help-in-place is used to identify those cases that do
not have severe COSR or BH disorders They are provided COSC consultation and education,
as appropriate, and remain on duty These interactions may occur in any setting Individual identifying information is not retained or
documented There is no implicit or explicit therapist-patient or
therapist-client relationship in HIP interactions
COSC Principles: BICEPS
Brevity--lasts 48 to 72 hours Immediacy--should be instituted as rapidly as possible Centrality--interventions should be in a central location,
separate from a medical facility Expectancy—Service members should be given a clear and
consistent message that they will return to duty with their unit
Proximity--management occurs near the front with close contact maintained between the member and his or her command
Simplicity--focus on the practical steps to restore function and health; and not on treatment and psychotherapy
26
Simplicity
Use brief and straightforward methods to restore physical well-being and self-confidence Reassure of normality Rest (respite from combat or break from the work) Replenish bodily needs (such as thermal comfort, water, food,
hygiene, and sleep) Restore confidence with purposeful activities and contact with his
unit Return to duty and reunite soldier with his unit

27
NONPATIENT STATUS
To prevent Soldiers with COSR from adopting the patient role, these guidelines should be followed: Keep the Soldier in uniform and hold him responsible for
maintaining Soldier standards Keep the Soldier separate from seriously ill or injured
patients Avoid giving him medications unless essential to manage
sleep Do not evacuate or hospitalize the Soldier unless
absolutely necessary Do not diagnose the soldier prematurely Transport the soldier via general-purpose vehicles, not
ambulances

28

29

30
Training Topics:Cont
Working with special populations
Special ops
Contractors
Door bangers
Convoy drivers
Flyers
Re-Deployment Support
Reintegration /Reunion education Landing Gear
Post-Deployment Health Reassessment Mental health services at home station
18 March class presentation: Post Deployment Mental Health Care

Resource Links
https://www.battlemind.army.mil/ PDHealth Predeployment information Air Force predeployment prep--family separations guide Army Behavioral Health predeployment information PDHealth Postdeployment information Postdeployment resources Military Spouse postdeployment information