colloque ri 2014 : intervention de gina ogilvie, md, (university of british columbia)
TRANSCRIPT
HPV vaccine policies: How innovative
partnerships led to policy relevant HPV
vaccine research
Recherche interventionnelle contre le
cancer
November 2014
Gina Ogilvie MD MSc FCFP DrPHMedical Director, Clinical Prevention Services
BC Centre for Disease Control
Professor, University of British Columbia
Conflict of Interest and Disclosure
• None
Objectives
• Review how an innovative funding
mechanism and partnerships led to policy
relevant HPV vaccine research
• Examine policy impacts of the findings of
the 2 v 3 dose HPV vaccine studies
• Review ongoing strategies for evaluation of
reduced doses of the HPV vaccine
The Canadian HPV Vaccine Research Priorities Workshop,
2005National Priorities workshop in 2005
•To establish research priorities for HPV vaccine
•Multidisciplinary team of clinicians and policy makers
Deeks S et al. CCDR 2006;32S1:66

Participants
• Invitational workshop with 55 invitees
• 2 international invitees (UK and US)
• Equal representation from Vaccinology, STI and
Cancer (OB/Gyne)
• Balanced representation from clinical,
epidemiological and psycho-social experts
• Vaccine industry observers
• Academics, public health, decision-makers
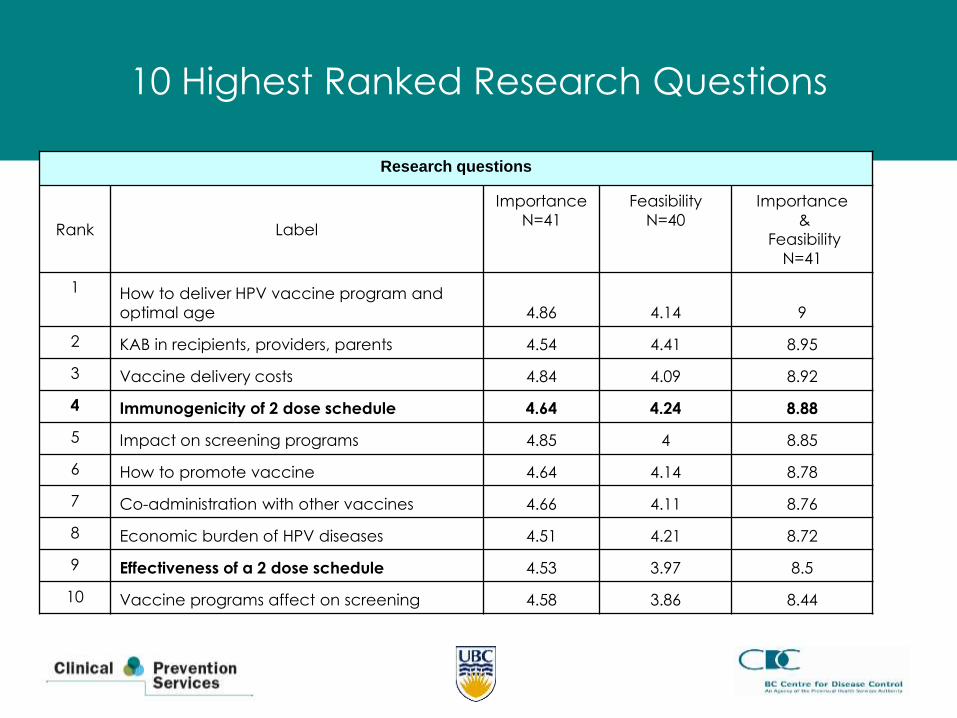
10 Highest Ranked Research Questions
Research questions
Rank Label
Importance
N=41
Feasibility
N=40
Importance
&
Feasibility
N=41
1 How to deliver HPV vaccine program and
optimal age 4.86 4.14 9
2 KAB in recipients, providers, parents 4.54 4.41 8.95
3 Vaccine delivery costs 4.84 4.09 8.92
4 Immunogenicity of 2 dose schedule 4.64 4.24 8.88
5 Impact on screening programs 4.85 4 8.85
6 How to promote vaccine 4.64 4.14 8.78
7 Co-administration with other vaccines 4.66 4.11 8.76
8 Economic burden of HPV diseases 4.51 4.21 8.72
9 Effectiveness of a 2 dose schedule 4.53 3.97 8.5
10 Vaccine programs affect on screening 4.58 3.86 8.44
Priorities Workshop, 2005
• Research priorities mostly on program delivery issues and
shorter vaccine schedules
• Challenge: little financial support and expertise in this
area of research
• Infrastructures needed: common goals, interdisciplinary
groups, access to databases and modeling
• Challenge: relatively low feasibility
Moving priorities forward
• Selected priorities from workshop identified by
public health leaders and Ministries of Health
• Committed to 3% use of vaccine budget (one-time)
for evaluation
• Several provinces collaborated to fund clinical trial
on reduced dose trials
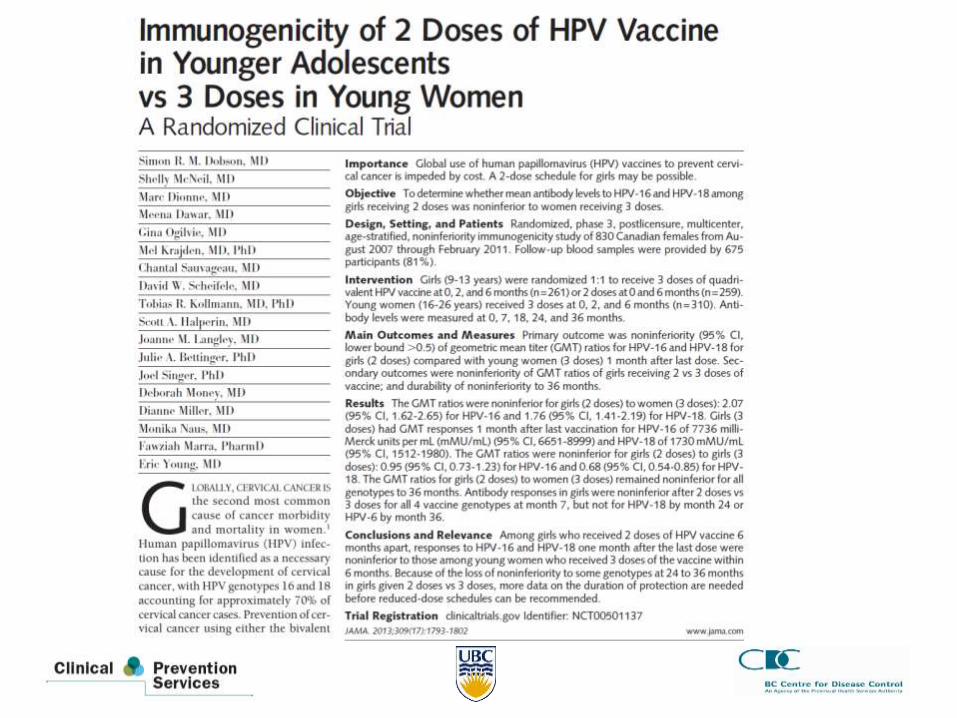
Clinical trial, Q-HPV vaccine: BC GOV01
• To evaluate the antibody response to the licensed
3-dose schedule as compared with the 2-dose
schedules, overall across age groups
• To evaluate the antibody response to 2 doses in
subjects 9–14 years* as compared to 3 doses in
subjects aged 15–25 years†
– Non-inferiority was demonstrated if the upper
limit (UL) of the 95% CI for the GMT ratio (3-
dose/2-dose) was <2
• To evaluate the safety and reactogenicity of the
vaccine in all study groups
9
*Target population for HPV vaccination, †Age group in which efficacy was demonstrated
10
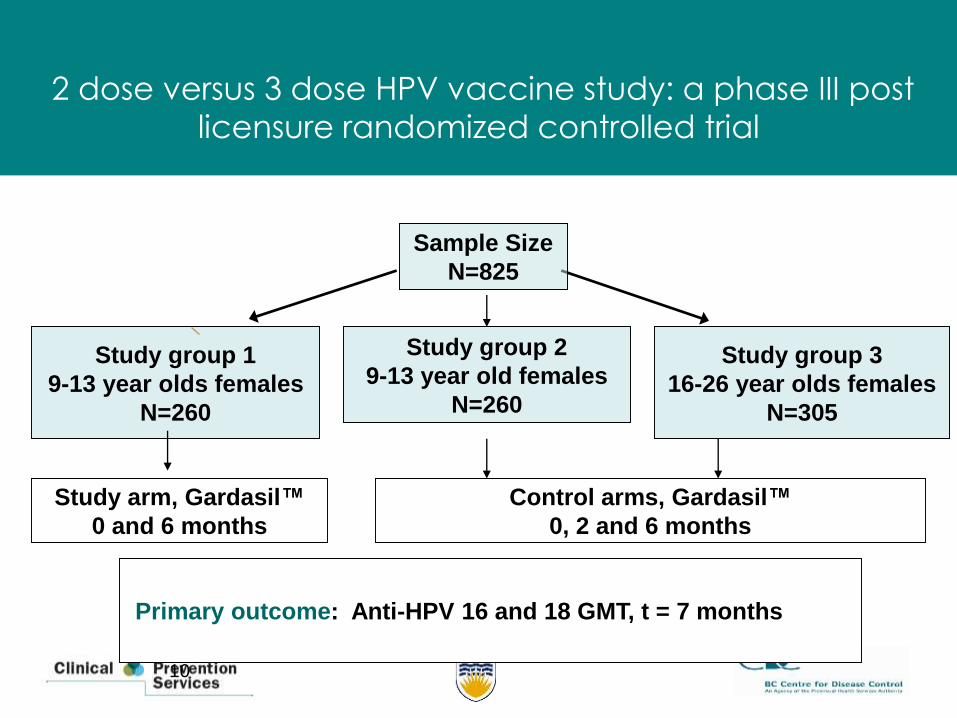
2 dose versus 3 dose HPV vaccine study: a phase III post
licensure randomized controlled trial
Sample Size
N=825
Study arm, Gardasil™
0 and 6 months
Control arms, Gardasil™
0, 2 and 6 months
Study group 1
9-13 year olds females
N=260
Study group 3
16-26 year olds females
N=305
Primary outcome: Anti-HPV 16 and 18 GMT, t = 7 months
Study group 2
9-13 year old females
N=260
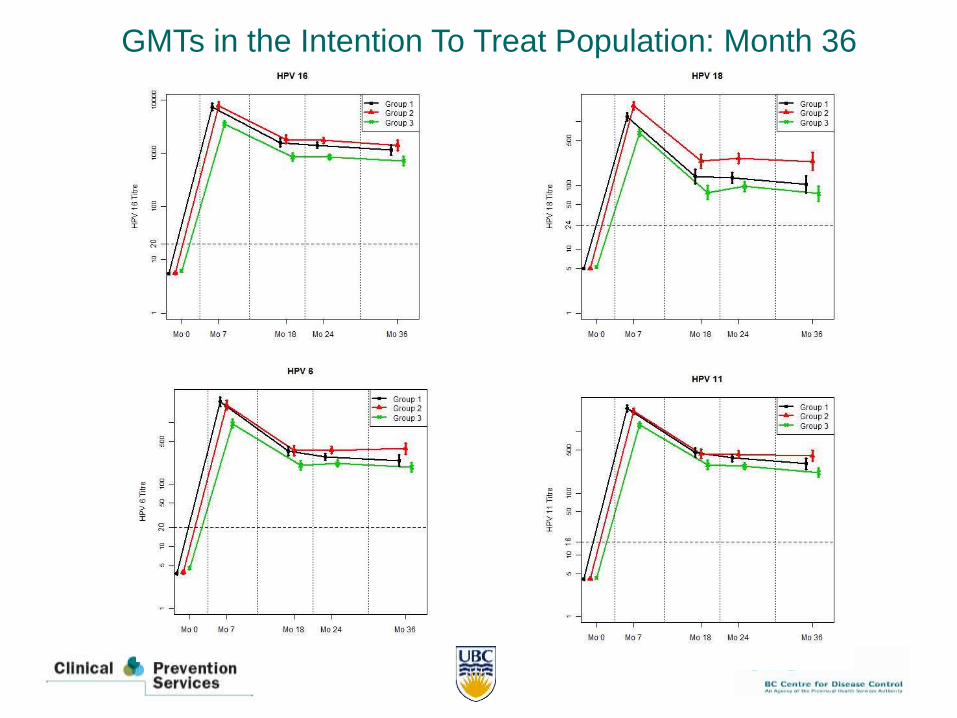
GMTs in the Intention To Treat Population: Month 36
Summary of findings: BCGOV01
• 2-dose antibody titers in pediatric population non-inferior to 3-dose titers in young adults at Month 36
• Use of broad spectrum of assays shows strong, ongoing antibody response in 2-dose recipients
• Antibody decay curves of 2 dose girls at Month 36 parallel those of 3-dose efficacy population
• Plateau level mirrors that of 3 dose young women
• Vaccine efficacy of 3-dose in 16-26 at 100%, and have found non-inferior titers in 2-dose – implying that 2 dose vaccine schedule will be at least as efficacious as 3 dose
• Despite high vaccine efficacy, only covers 70% of subtypes, indicating that girls will require ongoing cervical cancer screening
Knowledge Translation
• Extensive presentations at academic conferences
• Organized expert workshops at leading academic
and policy conferences (IPV; ISSTDR; CIC)
• Publication in academic journals
• Reach out to leading policy committees (NACI)
• Dataset from BCGov01 given to Merck
• Merck prepared a Clinical Study Report
– Audited BCGov01
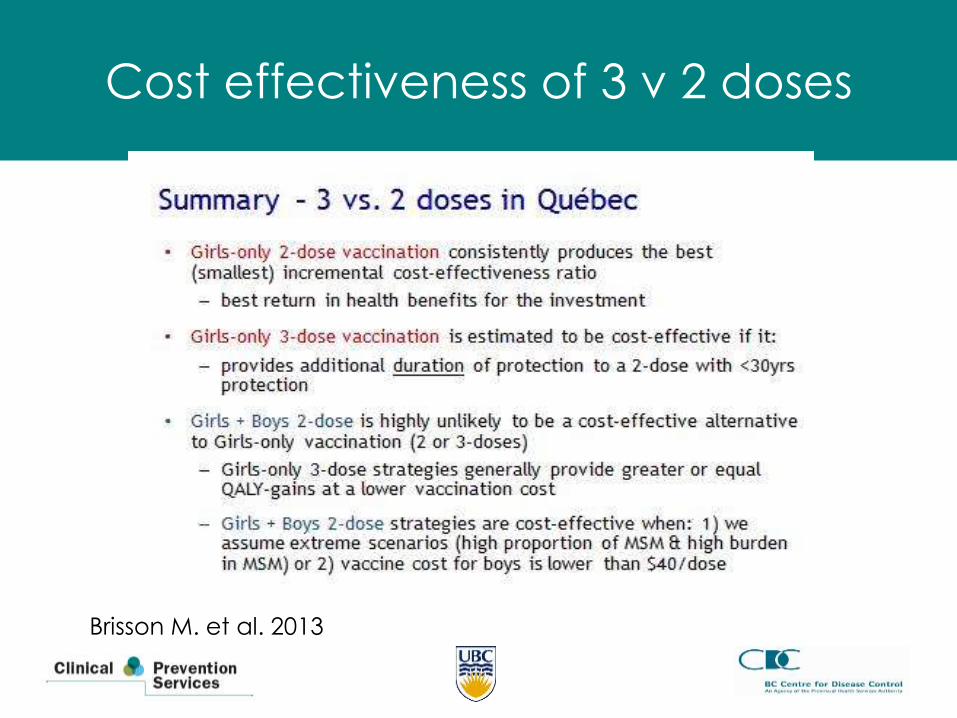
Cost effectiveness of 3 v 2 doses
Brisson M. et al. 2013
Knowledge translation: Policy agencies
• European Medicines Agency qHPV: April
2014
(bHPV: 2 dose indication, Nov 2013)
• WHO: evidence review by SAGE (March
2014)
• Recommendations by the WHO based on
the SAGE review (May 2014)
Gardasil approved for two dose schedule for girls 9-14 in April 2014
Supported by data from Dobson S. et al. (2013)
Cervarix approved for two dose schedule for girls 9-14 in December
2013
Supported by data from Puthankakit T. et al (2013) and
Romanowski B et al. (2013)
‘ The World Health Organisation's expert advisory group said that two shots of vaccine against human papillomavirus (HPV), rather than the three
doses currently recommended, will offer sufficient protection to girls so long
as they have it before they reach the age of 15.’ Guardian, April 2014
Approvals of Two Dose
HPV Vaccine Series
• European Union (EU):– bHPV: (0,6 months) in females ages 9-14 years
– qHPV: (0,6 months) in males and females ages 9-13 years
• Asia:– bHPV: Bangladesh, Pakistan– qHPV: the Philippines
• Africa:– bHPV: Ghana, Nigeria
– qHPV: South Africa
• the Americas:– bHPV: El Salvador, Guyana, Haiti, Panama, Suriname
– qHPV: Brazil, Colombia, the Dominican Republic
– bHPV and qHPV: Chile, Guatemala, Honduras

Implemented alternate dosing of HPV
vaccine
Jurisdictions reporting using a two dose
schedule are:
– Quebec, Switzerland, South Africa, UK,
France, The Netherlands, Chile, Spain,
Austria, Mexico, Colombia, Canada
What led to success?
• Shared agreement of priorities
• Non-industry funding, but partnered with industry
• Methods that embraced a pragmatic randomized
trial design
• Anticipatory design – what will the future hold?
• Extensive sharing of: trial methods; preliminary
results; ongoing results
• Collaboration between expert laboratory partners,
clinicians, public health
Key Challenges
• Funding
• Selecting rationale endpoints
• Different parameters for licensing vs
dose/schedule change
• Jurisdictions with variety of expectations for
changing policy
Lessons learned from the HPV vaccine non-
inferiority trial
• Article reviewers, journal editors and policy
decision makers are very uneasy about:
– The duration of immune response in girls
– ………… for both 2 and 3 dose recipients
– The comparison being with 3 doses in young women in
spite of these being the proven efficacy group
– The basis of the criterion for non-inferiority
– It is the comparison of the efficacy of 2
doses in girls with 3 doses in girls that
matters long-term
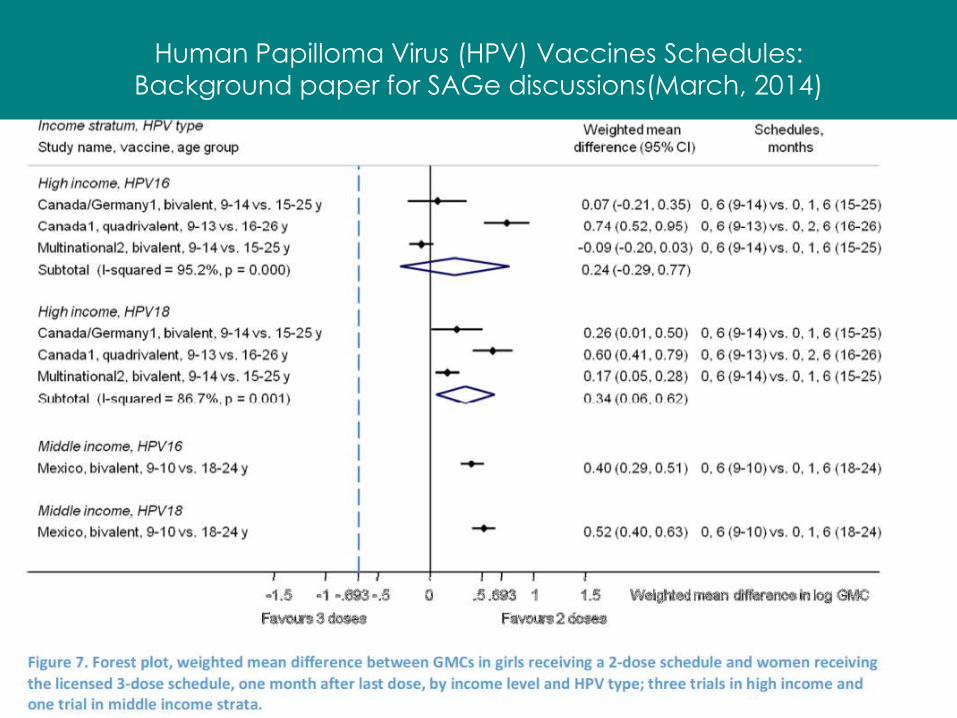
Human Papilloma Virus (HPV) Vaccines Schedules: Background paper for SAGe discussions(March, 2014)

Policy makers: what is said and done
• Based on BCGov01 Month 24 findings (2 doses are non-inferior to 3), CD Policy recommended use of 2 + 1 dose program in province of British Columbia
• Commitment to ongoing monitoring of program to decide on impact of alternate program
• Alternate dosing program started in September 2010
• Plans to monitor both antibody titers and efficacy for informing next steps
25
IARC Working Group Report, Meeting
Sept 2013
• Virological endpoints could
accelerate vaccine evaluation and
licensure
– reproducible
– clearer when there might be co-infection
IARC Working Group Report, 2014
• Vaccine shown to be effective in one
population:– Immuno-bridging is sufficient to extend to other
populations
– Recommend non-inferiority as appropriate
endpoint “independent of the number of
vaccine doses”
– Recommends post-licensure monitoring of
disease reduction
• QUEST plans to examine the long term efficacy of the reduced dose schedule of Q-HPV
• National study to comprehensively evaluate the durability of protection and efficacy of a 2-dose Q-HPV vaccination program compared to a 3-dose program by building on the existing infrastructure of the extended dose Q-HPV provincial vaccine programs in Quebec and British Columbia and the trial infrastructure and partnerships of BC GOV01
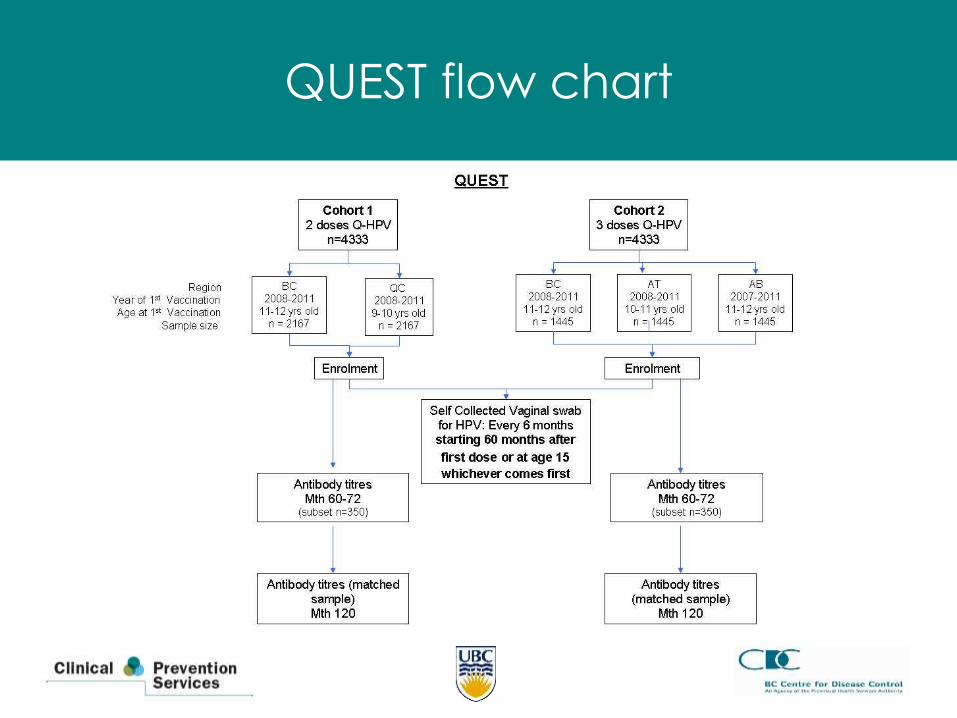
QUEST flow chart
Primary Objective:
• To evaluate if a 2 dose regimen of Q-HPV is non-inferior to a 3 dose schedule in the prevention of type specific persistent HPV16, 18, 6 or 11 infection in young women at 19 years of age
Secondary Objectives:
• To evaluate if a 2 dose regimen of Q-HPV is non-inferior to a 3 dose schedule in the prevention of type specific persistent HPV16, 18, 6 or 11 infection at month 60 and 120 post dose one or at age 15 in girls vaccinated at the age of 9 – 12 years
• To compare the mean antibody levels and seropositivity (for HPV types 16, 18, 6, or 11) in girls who have received 2 doses of Q-HPV to levels in girls who have received 3 doses at Months 60 and 120 post vaccination
31
Objectives
Secondary Objectives (continued): • To evaluate cumulative type specific persistence of HPV 16, 18, 6
or 11 at months 60, 84, 96 108 and 120 post dose 1 in girls vaccinated at the age of 9 – 12 years
• To evaluate if a 2 dose regimen of Q-HPV is non-inferior to a 3 dose schedule in the prevention of self-reported condyloma infection in young women
• To evaluate if a 2 dose regimen of Q-HPV is non-inferior to a 3 dose schedule in the prevention of type specific persistent HPV16, 18, 6 or 11 infection in young women at 15 years of age.
• To evaluate if a 2 dose regimen of Q-HPV is non-inferior to a 3 dose schedule in the prevention of type specific persistent HPV 31, 33, 35, 45, 52 and 59 infection in young women to 19 years of age
•
32
Objectives
Considerations
1. From modest beginnings, the results of
BCGov01 had far reaching consequences
2. Licensed indications matter
3. Vaccine uptake rates matter even more
4. Can Policy Decision Making Bodies come
to agreements with Regulators?
“We need to have a conversation”
• Thank you