colchester hospital university foundation trust -...
TRANSCRIPT

Colchester HospitalUniversityFoundation Trust
March 2018
An integrated approach tooptimising patient carethrough performanceimprovements across Quality,Performance and Finance

Colchester Hospital University Foundation Trust 2
ContentsEvery Patient Every Day Programme1 3
Colchester’s approach to sustainableimprovement2 7
Principles for sustainable improvement3 8
Clinical Quality & Governance4 9
Operational Performance5 11
Financial Balance6 13
Future focus against the supporting principles7 15
Reflections from the Trust8 16
Key Contacts9 17
Section
Appendix
STAARR Behaviours of LeadershipA 18

Colchester Hospital University Foundation Trust 3
Ever
yPa
tien
tEv
ery
Day
Pro
gram
me In December 2015, the Care Quality Commission (CQC) rated Colchester
Hospital University NHS Foundation Trust (CHUFT) as “inadequate” andidentified a number of significant failings. A follow-up visit in April 2016showed insufficient improvement had been made, leading to arecommendation by the CQC to the Secretary of State for Health thatCHUFT should be placed into administration.
Ipswich Hospitals NHS Trust (IHT) was subsequently asked by NHSImprovement (NHSI) to consider entering into a partnership with CHUFTto help resolve the issues facing the Trust and as an alternative toadministration. In May 2016 the Boards of both CHUFT and IHTcommitted to entering into a long-term partnership, built on a foundationof collaborative working established between the two Trusts over recentyears. The Chair and Chief Executive of IHT, with the support of NHSI,were also appointed into these roles at CHUFT; additionally, the IHTBoard approved the secondment and subsequent appointment of itsMedical Director into the role of Managing Director at CHUFT.
In July 2016, with the agreement of NHSI, the Trust embarked upon aprogramme of clinical, operational and financial turnaround with theoverarching objective of improving the safety and quality of services topatients.
EY was commissioned as the Trust’s delivery partner in August 2016 andworked alongside CHUFT to establish and deliver the Every Patient EveryDay (EPED) Programme. The purpose of the programme was to improvethe quality of patient care and experience across the organisation byaddressing the clinical, performance, operational and financial issues thatwere evident.
The programme was initially set up with a 12 month timeframe; whilst itwas recognised that transformation and embedding a new culture wouldrequire a longer timescale, it was important to set clear goals andimprovement trajectories for the programme in the short to mediumterm.
Colchester Hospital University Foundation Trust 4
The programme was centred on three key modules of work:1. Quality & Governance – establishing a fit for purpose governance
framework and responding to the CQC concerns2. Operational Improvement & CIP delivery – establishing operational grip
and achieving the Trust’s control total3. Cross-cutting improvements (performance and efficiency) - delivering
against agreed 18 week trajectories and performance metrics
Robust programme governance supported the overall objective ofensuring that the Trust transforms into a sustainable and stableorganisation with a relentless focus on providing the highest quality ofcare to patients and the local population. The programme has beendelivered and monitored via a Programme Management Office (PMO),which has provided the governance to deliver at the scale and pacerequired, and to support the transition of capability and knowledge to theTrust.
Given the need to drive improvements at pace over the first 12 months ofthis programme, the Trust and NHSI recognised the need for theadditional capacity and experience that EY were able to bring to EPED.CHUFT staff and the EY team worked jointly to drive the required change.
Through the efforts employed and improvements made as part of theprogramme, the Care Quality Commission returned to the organisation inJuly 2017 and observed marked improvement across all areas of theTrust.
As a result the Trust received an overall score of ‘Requires Improvement’,and 3 of 5 rating areas scoring ‘Good’: Effective, Caring and Well-led andhas been removed from quality special measures.

Colchester Hospital University Foundation Trust 5
The Colchester Hospital University NHS FoundationTrust has been in special measures longer than anyother hospital. To date approaches to resolving issuesraised by external bodies have been siloed, where aslower rate of embedded change was furtherexacerbated by a number of interims and vacancies.Interventions had concentrated on responding to theissues raised by the CQC and others rather than afundamental review of care provided to patients.
At this pivotal stage of improvement at the Trust, itwas extremely important to have the right mix ofindividual skills and processes; Colchester sufferedfrom the absence of both at the beginning of theprogramme. Change can be successful in the shortterm with one or the other, but a combination of thetwo is required for sustainable improvement.
The benefit of having EY supporting ourtransformation work at the Trust was the skills,experience and resilience they brought with them.Together we’ve developed some strong processeswhich are the foundation of improvementsustainability. This could not have been done withoutthe integrated approach forming the heart of theEvery Patient Every Day (EPED) programme of changeacross clinical quality, operational performance andfinancial balance.
The standard response of Colchester to externalregulatory reports has been to develop action plans,undertake the actions and assume that improvementwill have been delivered. For example, we previouslydeveloped an action plan to address concerns aroundEnd of Life Care, which focused on delivery of training.However, through a clear performance managementframework with Key Performance Indicators withinEPED, we actually found that, although the action planwas delivered, the improvements in the area have notsurfaced.
Foreword
.
Nick Hulme
Chief ExecutiveOfficerColchesterHospitalUniversity NHSFoundation Trust,Ipswich HospitalNHS Trust
Colchester Hospital University Foundation Trust 6
The Every Patient Every Day programme has successfully refocused theTrust’s direction from building changes in response to external regulators,to proactively driving sustainable change around the patient’s journey toensure continued high quality care.
Working with external providers to deliver the programme of change hasprovided us with a stronghold of support and knowledge throughout thisjourney. The knowledge that EY have brought with them has beeninvaluable, along with the discipline and rigour to maintain programmemomentum. I’d recommend that when undertaking a change of this size, itis paramount to get the skills transfer right; we’ve struggled with this aswe’ve not had the individuals in place –it is important to considerorganisational development at the beginning of the programme.
Finally, the primary takeaway from this programme has been the need toimplement integrated change across the three areas: clinical quality,operational performance and financial improvements. This premise formsthe foundation of sustainable improvements across the Trust and drives aquicker pace of change than when conducted in isolation.
Nick Hulme
Chief Executive OfficerColchester Hospital University NHS Foundation Trust,Ipswich Hospital NHS Trust
Colchester’s approach to sustainable improvement
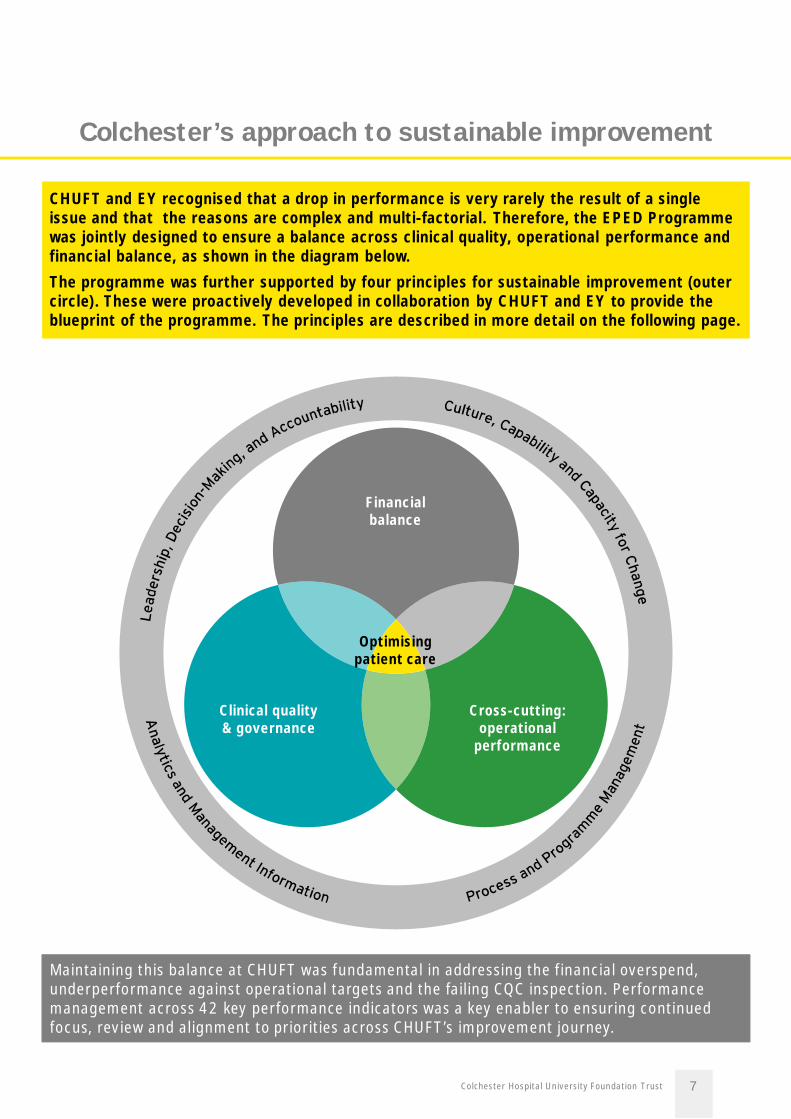
CHUFT and EY recognised that a drop in performance is very rarely the result of a singleissue and that the reasons are complex and multi-factorial. Therefore, the EPED Programmewas jointly designed to ensure a balance across clinical quality, operational performance andfinancial balance, as shown in the diagram below.The programme was further supported by four principles for sustainable improvement (outercircle). These were proactively developed in collaboration by CHUFT and EY to provide theblueprint of the programme. The principles are described in more detail on the following page.
Maintaining this balance at CHUFT was fundamental in addressing the financial overspend,underperformance against operational targets and the failing CQC inspection. Performancemanagement across 42 key performance indicators was a key enabler to ensuring continuedfocus, review and alignment to priorities across CHUFT’s improvement journey.
Financialbalance
Cross-cutting:operational
performance
Clinical quality& governance
Optimisingpatient care
Colchester Hospital University Foundation Trust 7
Colchester Hospital University Foundation Trust 8
Principles for sustainable improvement
► Trust leaders and regulators need to be united in creating acompelling vision and momentum to drive wholesale change;for example, the threat of administration triggered theestablishment of EPED
► A clear and evidence-based approach to decision-making isneeded to build momentum for change
► Everyone from Ward to Board needs to be held accountable fordelivering change in a way that is robust, respectful and timely
► An organisational development strategy needs to ensure thatsenior and operational leaders (clinical and non-clinical) areadequately prepared to shape and lead the work to ensure thesustainability of the transformation
► Changing organisational culture takes time, but identifyingchange champions and tackling poor behaviour/practice is vital
► Workforce levels should be assessed for sustainability up frontto put in place early mitigation. In the medium term, a clearrecruitment strategy, and talent and performance managementplans are required to build capacity and capability
► However, building capability and capacity is not a short-termprocess, so interim capacity and clear handover planning needsto be built in from the start
► Data-driven decisions and accountability rely on insightfulanalytics, which need to be rapidly put in place
► Progress needs to be tracked continually through a set ofrelevant, consistent and automatically-generated metrics
► Actions should drive change in metrics, and decisions – byworkstream SROs, divisional leadership teams, and executives –should be informed by these metrics
The following four principles were used to drive the success of CHUFT’s Every Patient EveryDay improvement journey. Reflections about how these were applied and evidenced inpractice are included in the workstream reviews on pages 9-14.
► Clear and rigorous programme management is at the heart ofchange management and prioritisation. This needs to be robustand challenging for executives and regulators, and shouldreflect on lessons from previous phases
► Clear and consistent leadership communications are vital tomotivate and ensure clarity for all staff

Clinical Quality & Governance
What worked well at Colchester Learnings for next time► Senior executives as SROs. The Trust recognised
that its executives needed to act as SROs duringthe early months of the programme, committingsignificant time, in order to drive the changeneeded. This enabled quick decision-making andrapid implementation of priorities, setting the tonefor Operational Managers to subsequently take onleadership of the programme
► Being able to work directly with interdependentworkstreams, e.g. Deteriorating Patient andEmergency Department (ED) Performance,ensured that the work to improve sepsis wasembedded in the wider improvement plans in ED
► Clinical leadership embedded in the clinicalimprovement and design work
► A rapid review of the audit methodology forDeteriorating Patients led to a revised andimproved approach, yielding a greater sample sizeand a more accurate picture of compliance. Thisresulted in a more robust improvement plan formanagement of deteriorating patients
► KPIs need careful consideration – programmemetrics need to ensure they are driving the rightchange. A number of governance KPIs did notprovide effective insight, being too high-level andreliant on aggregated source data. Patientoutcome KPIs need to be complemented by KPIsto reflect structural and process changeimprovement
► The scale and pace of the programme needs to beconsistently communicated
► Clinical engagement needs to be consistent andaligned to strategic requirements, programmemilestones and KPIs
► Earlier involvement of divisional leadership – thiswas impacted by workforce gaps and ultimatelyslowed down delivery
► Earlier involvement of the Patient Voice couldhave strengthened the effectiveness andengagement of the changes being implemented bythe programme
Critical Success Factors
Critical analysis of performance information andintelligenceThe accuracy of information in relation to care delivery is vital.Equally important is the ability and desire to critically challenge andanalyse data. The predisposition to have a natural curiosity towarddata acts not only to provide clarity on the basis for making decisions,but also to strengthen the ability to consistently monitor and assureprogress.
Revised Ward to Board governance systemsHospitals are complex so ensuring the connectivity of all thecomponent parts of Ward to Board Governance is imperative. It iscrucial that governance processes work as close to the patient aspossible. This should be through well-engaged clinical and operationalteams, within a well-defined governance framework. All staff needsupport to understand their role in governance and the organisationalframework in which their contribution operates.
Focused clinical improvement design and deliveryA key principle driving clinical re-design is the recognition thatunderperformance against national best practice in clinical carerequires improvement. The change process needs to be owned byclinical leaders who are motivated to transform care at the requiredscale and pace. The clinical vision has to be supported by well-designed operational plans, accountable leadership and outcome-focused KPIs.
Principles
1
3
4
21
21
Colchester Hospital University Foundation Trust 9
Achievements
Qualitative impact Quantitative impact
Det
erio
rati
ngPa
tien
tsG
over
nanc
eE
ndof
Life
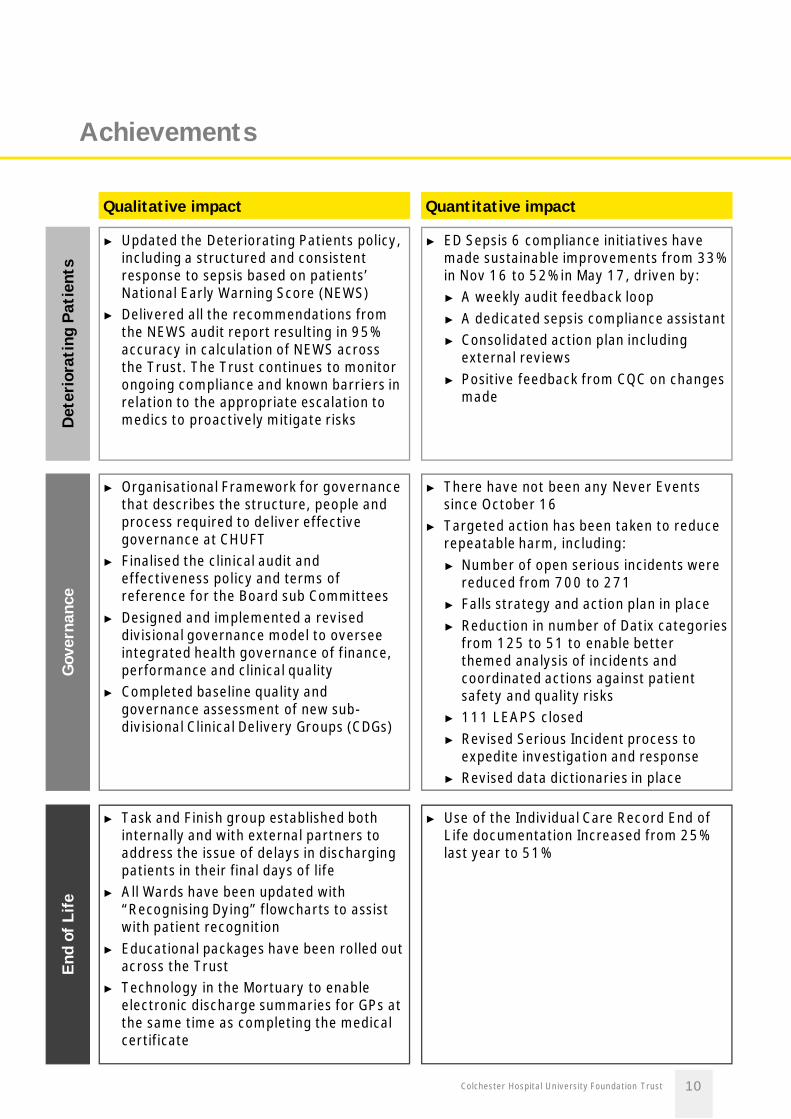
► Updated the Deteriorating Patients policy,including a structured and consistentresponse to sepsis based on patients’National Early Warning Score (NEWS)
► Delivered all the recommendations fromthe NEWS audit report resulting in 95%accuracy in calculation of NEWS acrossthe Trust. The Trust continues to monitorongoing compliance and known barriers inrelation to the appropriate escalation tomedics to proactively mitigate risks
► ED Sepsis 6 compliance initiatives havemade sustainable improvements from 33%in Nov 16 to 52% in May 17, driven by:► A weekly audit feedback loop► A dedicated sepsis compliance assistant► Consolidated action plan including
external reviews► Positive feedback from CQC on changes
made
► Organisational Framework for governancethat describes the structure, people andprocess required to deliver effectivegovernance at CHUFT
► Finalised the clinical audit andeffectiveness policy and terms ofreference for the Board sub Committees
► Designed and implemented a reviseddivisional governance model to overseeintegrated health governance of finance,performance and clinical quality
► Completed baseline quality andgovernance assessment of new sub-divisional Clinical Delivery Groups (CDGs)
► There have not been any Never Eventssince October 16
► Targeted action has been taken to reducerepeatable harm, including:► Number of open serious incidents were
reduced from 700 to 271► Falls strategy and action plan in place► Reduction in number of Datix categories
from 125 to 51 to enable betterthemed analysis of incidents andcoordinated actions against patientsafety and quality risks
► 111 LEAPS closed► Revised Serious Incident process to
expedite investigation and response► Revised data dictionaries in place
► Task and Finish group established bothinternally and with external partners toaddress the issue of delays in dischargingpatients in their final days of life
► All Wards have been updated with“Recognising Dying” flowcharts to assistwith patient recognition
► Educational packages have been rolled outacross the Trust
► Technology in the Mortuary to enableelectronic discharge summaries for GPs atthe same time as completing the medicalcertificate
► Use of the Individual Care Record End ofLife documentation Increased from 25%last year to 51%
Colchester Hospital University Foundation Trust 10
Operational Performance
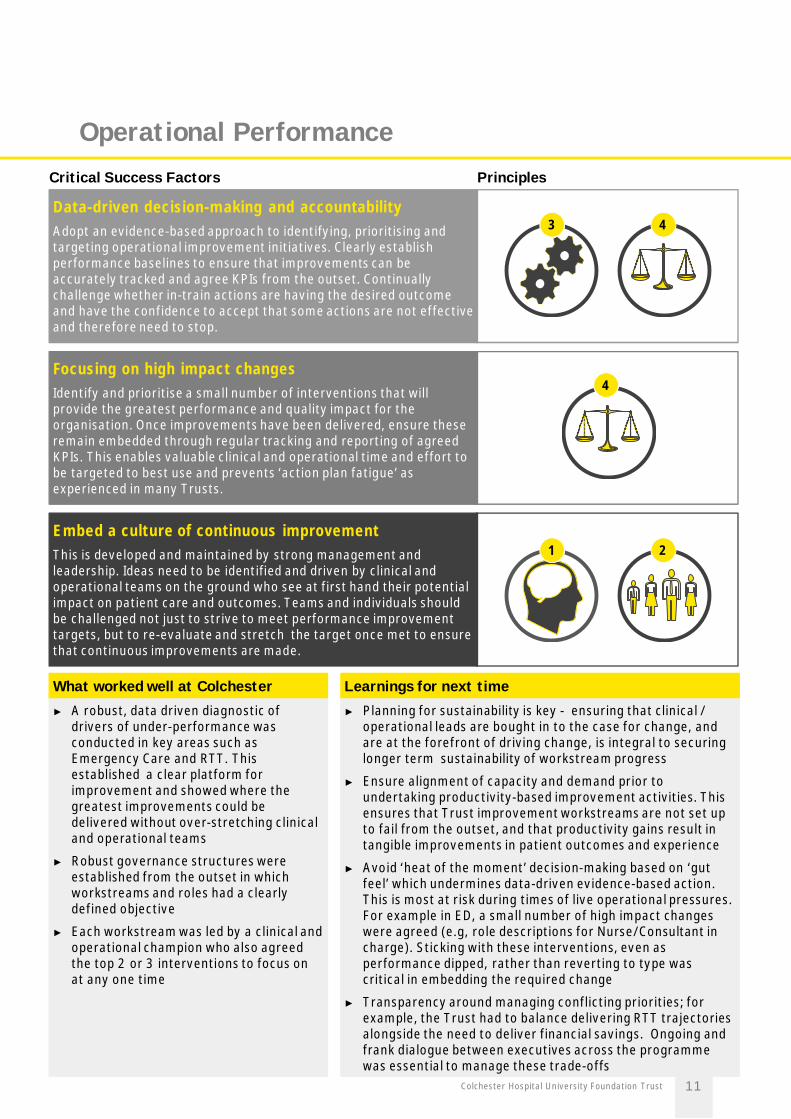
What worked well at Colchester Learnings for next time► A robust, data driven diagnostic of
drivers of under-performance wasconducted in key areas such asEmergency Care and RTT. Thisestablished a clear platform forimprovement and showed where thegreatest improvements could bedelivered without over-stretching clinicaland operational teams
► Robust governance structures wereestablished from the outset in whichworkstreams and roles had a clearlydefined objective
► Each workstream was led by a clinical andoperational champion who also agreedthe top 2 or 3 interventions to focus onat any one time
► Planning for sustainability is key - ensuring that clinical /operational leads are bought in to the case for change, andare at the forefront of driving change, is integral to securinglonger term sustainability of workstream progress
► Ensure alignment of capacity and demand prior toundertaking productivity-based improvement activities. Thisensures that Trust improvement workstreams are not set upto fail from the outset, and that productivity gains result intangible improvements in patient outcomes and experience
► Avoid ‘heat of the moment’ decision-making based on ‘gutfeel’ which undermines data-driven evidence-based action.This is most at risk during times of live operational pressures.For example in ED, a small number of high impact changeswere agreed (e.g, role descriptions for Nurse/Consultant incharge). Sticking with these interventions, even asperformance dipped, rather than reverting to type wascritical in embedding the required change
► Transparency around managing conflicting priorities; forexample, the Trust had to balance delivering RTT trajectoriesalongside the need to deliver financial savings. Ongoing andfrank dialogue between executives across the programmewas essential to manage these trade-offs
Critical Success Factors
Data-driven decision-making and accountabilityAdopt an evidence-based approach to identifying, prioritising andtargeting operational improvement initiatives. Clearly establishperformance baselines to ensure that improvements can beaccurately tracked and agree KPIs from the outset. Continuallychallenge whether in-train actions are having the desired outcomeand have the confidence to accept that some actions are not effectiveand therefore need to stop.
Focusing on high impact changesIdentify and prioritise a small number of interventions that willprovide the greatest performance and quality impact for theorganisation. Once improvements have been delivered, ensure theseremain embedded through regular tracking and reporting of agreedKPIs. This enables valuable clinical and operational time and effort tobe targeted to best use and prevents ‘action plan fatigue’ asexperienced in many Trusts.
Embed a culture of continuous improvementThis is developed and maintained by strong management andleadership. Ideas need to be identified and driven by clinical andoperational teams on the ground who see at first hand their potentialimpact on patient care and outcomes. Teams and individuals shouldbe challenged not just to strive to meet performance improvementtargets, but to re-evaluate and stretch the target once met to ensurethat continuous improvements are made.
Principles
43
4
21
Colchester Hospital University Foundation Trust 11
Achievements
Qualitative impact Quantitative impact
Pla
nned
Car
e&
Out
pati
ents
Urg
ent
&E
mer
genc
yC
are,
Pati
ent
Flow
Wor
kfor
ce
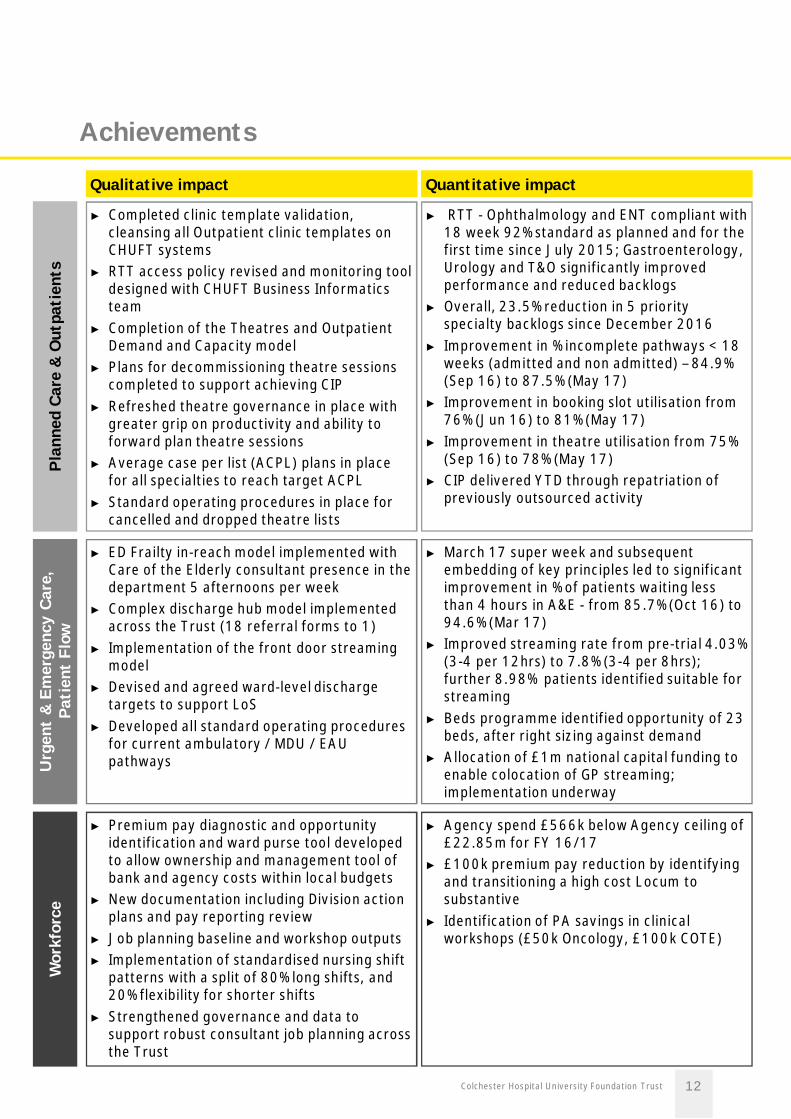
► Completed clinic template validation,cleansing all Outpatient clinic templates onCHUFT systems
► RTT access policy revised and monitoring tooldesigned with CHUFT Business Informaticsteam
► Completion of the Theatres and OutpatientDemand and Capacity model
► Plans for decommissioning theatre sessionscompleted to support achieving CIP
► Refreshed theatre governance in place withgreater grip on productivity and ability toforward plan theatre sessions
► Average case per list (ACPL) plans in placefor all specialties to reach target ACPL
► Standard operating procedures in place forcancelled and dropped theatre lists
► RTT - Ophthalmology and ENT compliant with18 week 92% standard as planned and for thefirst time since July 2015; Gastroenterology,Urology and T&O significantly improvedperformance and reduced backlogs
► Overall, 23.5% reduction in 5 priorityspecialty backlogs since December 2016
► Improvement in % incomplete pathways < 18weeks (admitted and non admitted) – 84.9%(Sep 16) to 87.5% (May 17)
► Improvement in booking slot utilisation from76% (Jun 16) to 81% (May 17)
► Improvement in theatre utilisation from 75%(Sep 16) to 78% (May 17)
► CIP delivered YTD through repatriation ofpreviously outsourced activity
► ED Frailty in-reach model implemented withCare of the Elderly consultant presence in thedepartment 5 afternoons per week
► Complex discharge hub model implementedacross the Trust (18 referral forms to 1)
► Implementation of the front door streamingmodel
► Devised and agreed ward-level dischargetargets to support LoS
► Developed all standard operating proceduresfor current ambulatory / MDU / EAUpathways
► March 17 super week and subsequentembedding of key principles led to significantimprovement in % of patients waiting lessthan 4 hours in A&E - from 85.7% (Oct 16) to94.6% (Mar 17)
► Improved streaming rate from pre-trial 4.03%(3-4 per 12hrs) to 7.8% (3-4 per 8hrs);further 8.98% patients identified suitable forstreaming
► Beds programme identified opportunity of 23beds, after right sizing against demand
► Allocation of £1m national capital funding toenable colocation of GP streaming;implementation underway
► Premium pay diagnostic and opportunityidentification and ward purse tool developedto allow ownership and management tool ofbank and agency costs within local budgets
► New documentation including Division actionplans and pay reporting review
► Job planning baseline and workshop outputs► Implementation of standardised nursing shift
patterns with a split of 80% long shifts, and20% flexibility for shorter shifts
► Strengthened governance and data tosupport robust consultant job planning acrossthe Trust
► Agency spend £566k below Agency ceiling of£22.85m for FY 16/17
► £100k premium pay reduction by identifyingand transitioning a high cost Locum tosubstantive
► Identification of PA savings in clinicalworkshops (£50k Oncology, £100k COTE)
Colchester Hospital University Foundation Trust 12
Financial Balance
What worked well at Colchester Learnings for next time► A combination of cross-cutting and Divisional
workstreams helped deliver efficiencies andeconomies of scale with Executive leadership
► Instilling financial rigour and discipline from line-by-line challenge on budgets through to applicationof controls
► Starting CIP identification early for April deliverysupported a forecast outturn over 60% greaterthan the previous financial years achievement.This process should be continuous throughout theyear
► Creating simple, relevant dashboards with useful,actionable information helped teams focus andprioritise efforts e.g. premium pay reductions
► Consider sustainability of the transformationalwork early to ensure there is an equipped resourceto drive and enable CIP identification and deliverypost any external support; aligning PMO /transformation capacity early
► Capacity needs to be created to enableoperational teams to deliver on the financialagenda despite any ongoing operationalpressures; again, aligning PMO andtransformation capacity early to provideconsistent support
► Executive teams need to have the time to agreethe high risk schemes they are willing to pursue atthe outset (in the context of the overall risk profileof the organisation) to avoid scheme ‘drop-out’part way through the year, for example, bedreconfiguration
Critical Success Factors
Engage widely and set expectations on deliveryDelivering financial balance is not optional and needs to be a priorityfor all managers and clinical leaders. Clear and consistent messagingfrom the Executive team is essential. The expectation of what needsbe delivered must be set out clearly with roles and responsibilitiesarticulated and clear lines of accountability. This needs to beembedded into business as usual with a training and developmentprogramme that ensures people have the capacity and capability todo this.
Utilise top-down and bottom-up approaches foridentification of opportunity areasA combination of top-down and bottom-up identification of newopportunities will maximise the ability to deliver on objectives. Theinstinct and knowledge of operational and clinical Trust staff is crucialfor generating locally owned schemes. Combining the need forfinancial savings with a clinical and operational improvement lens at aspecialty level helps secure the buy-in to drive service change.
Question accepted ‘norms’ and leave no stone unturnedOpportunities for improvement can be difficult to identify, especiallywhen an organisation has cost improvement fatigue. Exploringoperational challenges that lead to financial pressures andunderstanding any deficit drivers at specialty level will highlightopportunities. Curiosity and challenging the status quo will generatenew ideas, and new models or approaches to delivering care shouldbe explored. Every idea should be scoped through to an evidencedconclusion.
Principles
21
1
3
4
2
Colchester Hospital University Foundation Trust 13
Achievements
Qualitative impact Quantitative impact
Cos
tIm
prov
emen
tP
rogr
amm
e
► A baseline of the CIP programme andgovernance framework enabled strengthsto be recognised and areas forimprovement to be addressed
► A suite of controls was established quicklyto reduce the run rate expenditure acrosspay and non-pay in parallel to CIPdevelopment and delivery
► Increased Trust focus, understanding andengagement on CIP
► Developed updated approach for key CIPgovernance processes including QualityImpact Assessments (QIAs) to ensurerobust and streamlined process
► Increased ownership and accountabilityfor delivery of CIP
► Provided immediate bandwidth in thedivisions to properly structure and deliverCIP schemes
► CIP and run rate controls have collectivelysupported the achievement of achallenging 2016/17 control total
► A CIP target double the size of 2016/17has been set for 2017/18 totalling £17mwith £14.1m identified and Divisionsmeeting their control totals at a bottomline month on month. Specifically:► £12.4m schemes (73%) identified
(£8.8m Green, £2.2m Amber and£1.4m Red)
► Additional pipeline of hopper schemesof £1.7m
► Run rate at month 2 only marginally offplan
Colchester Hospital University Foundation Trust 14
Colchester Hospital University Foundation Trust 15
Future focus against the supporting principles
► Embed STAARR behaviours of leadership: Sustainability, Timeliness,Attendance, Accountability, Rigour and Resilience (see Appendix A) will beused to drive the right behaviours across the organisation and ensure continualchallenge to the improvement programme
► Agree and implement an organisational development strategy that will:► Ensure that development is pragmatic and applied to the organisation’s
current context and needs, rather than development in abstract► Develop of a targeted engagement strategy for the Trust’s staff and patients
to inspire motivation and enact changes drive high quality patient care,building on the ‘Every Patient Every Day’ brand
► Set out and articulate for the organisation (and NHSI) how theTransformation Programme will encompass important elements oforganisational and cultural development, as an integrated, rather than aseparate exercise
► Support the three Clinical Divisional Directors and their teams to succeed intheir roles and accelerate delivery through the divisions (the Trust hasrecently gone through a major divisional restructuring)
► Self-service analytics will be used to encourage inquisitive thinking and supportimprovement
► Statistical Process Control will be used to ensure assurance is only gained whena significant improvement is achieved
► Continue to drive rigorous programme management through the newImprovement Team, ensuring alignment to the Trust’s corporate objectives
► Leadership and robust challenge to workstreams to ensure ongoing progressand control in anticipating risks and issues, and continued rigour and disciplinein programme reporting
The EPED Programme was designed to ensure a holistic approach to improvement across quality,performance and finance. CHUFT and EY recognise that the improvement journey is work in progress.Broadly, the next phases of the journey are:
• Clinical Quality & Governance: Continue to ensure that the Board critically challenge theirgovernance credentials and are able to make well-informed decisions based on high qualityinformation, and that the Divisional Governance continues to evolve with progress evaluated
• Operational Performance: Continue to build on improvement interventions to date by ensuring thatthese are embedded as part of the day to day running of the hospital, moving away from theperception that initiatives are ‘on top’ of the day job and embedding these improvements into thecore business
• Financial Balance: Develop a medium-term plan which will involve more innovative andtransformational thinking to deliver savings required, including the long term partnership with IHT

Colchester Hospital University Foundation Trust 16
Ref
lect
ions
from
the
Trus
t
The following worked well:• Introduction of structure in to the improvement process• A good rhythm to the PMO work, reporting etc.• Good engagement by the departments / divisions• Confidence built with external stakeholders• Clear progress in some areas
Going forward, we need to:• Keep up the rhythm and clear reporting• Ensure focus on delivery• Track the outcomes and change tack if things are not working• Ensure all the supporting resources (transformation, OD, quality improvement, BI, IT software
development, recruitment, training etc.) are aligned to the areas of priority
Dr Shane GordonDirector of Integration
“
”
EY have brought with them the bandwidth, discipline, rigour, analytics, knowledge and PMO tohelp drive an integrated programme of change across the Trust to delivery high quality patientcare. The key has been working with EY individuals that have clinical experience which has beenvital to implementing improvements; they’ve been able to understand what and why there arebarriers to change and how to overcome them, and Trust individuals identify with them as a result.
Dr Barbara BuckleyManaging Director
”
“During this programme of change, the benefit has been in embracing a structured approach andthe support, experience and perspective that independent parties can bring. The capacity andbandwith EY brought allowed us to drive and kick start the programme.
Dawn ScrafieldDirector of Finance ”“
I found the most useful aspect of EY involvement (in addition to bringing some structure andrigour to programme management) was their ability to share best practice from other NHSproviders to support our improvement plan. I found this very helpful with the Theatreproductivity work and I am sure the surgical division had their eyes opened to what worked well inother organisations around reducing DNAs, improved practice with the consent process, makingbest use of theatre availability, detailed analysis of what caused inefficiency etc. We simplywouldn’t have had the bandwidth, skill and expertise to analyse and make use of data to thisextent, hopefully we won’t lose momentum with this type of approach now they are no longer hereto support us.
Chris HowlettDirector of Estates and Facilities ”
“
The programme must be calibrated so that all 3 areas are equal – prioritising one over the other isdetrimental to the overall success of the Trust.
Dawn ScrafieldDirector of Finance”“
It is vital that all 3 components (clinical quality and governance, operational performance andfinancial improvements) are integrated and implemented together. Although it’s been hard work,it has led to quicker, equal improvements across all elements, taking the wider staff with theprogramme on the improvement journey.This approach is integral to the running of the Trust, such that during the course of theprogramme, the appetite for change to drive patient care has become Business-as-usual.Bringing knowledge across each of the three key areas and sharing the learning has been vital e.g.Cross-cutting and CIP have worked closely together to drive a coordinated approach to delivery.
Dr Barbara BuckleyManaging Director
”“

Transformation requires collaboration for sustainability. The improvements at Colchesterwere only achieved through a combination of experience and expertise of NHSI, theColchester Hospital University Team and EY.
Key Contacts
Colchester Hospital Team EY Team
Dr Susan Thomas
PartnerDirect Tel: + 44 20 7951 3753Mobile: + 44 7787 792 566Email: [email protected]
Emma Maclellan-Smith
Engagement DirectorDirect Tel: + 44 113 298 2514Mobile: + 44 7826 513 678Email: [email protected]
Nick Hulme
CEODirect Tel: + 44 1206 742840Mobile: + 44 7789 205205Email: [email protected]
Dr Barbara Buckley
Managing DirectorDirect Tel: + 44 1206 742 785Mobile: + 44 7930 876 732Email: [email protected]
Dawn Scrafield
Director of FinanceDirect Tel: + 44 1206 746 059Mobile: + 44 7887 890 531Email: [email protected]
Richard Lewis
Health Advisory Lead & QA PartnerDirect Tel: + 44 20 7951 0534Mobile: + 44 7970 652278Email: [email protected]
Colchester Hospital University Foundation Trust 17
Colchester Hospital University Foundation Trust 18
Appendix A: STAAR Behaviours of Leadership
What Executive SRO behaviours should we exhibit to ensure sustainable and innovationsolutions at scale and pace?
S – Sustainability Leaders’ actions should consider sustainability in decision-making –an assessment should be made of any short-term or interim measuresput in place, how these will be addressed in the longer term andencourage review of dependencies for a holistic programme view. Weshould be mindful of the over-reliance on ‘work arounds’.
T – Timeliness: Leaders should consistently ensure there are timescales by whichimprovement should be measured. – this should be aligned to theaccountability for delivery, how this will be measured and the forum bywhich the action will be updated. For anticipated delays, this should becommunicated in advance with alternative timings proposed.
A – Attendance Leaders should ensure attendance and prioritise decision-makingforums across the organisation – the delegation of responsibility forattendance at core meetings needs to be agreed and adhered to – anylikely non-attendance by senior leaders should be delegated with theexpectation that delegates are briefed to represent the nominated leadappropriately, ensuring consistency of message and progress.
A – Accountability Leadership behaviours should make clear the accountability requiredat every level for their areas of responsibility – accountability foractions should be well articulated and transparent at all Leadershipand Operational levels across the Trust.
R – Rigour Leadership should rigorously and constructively test, analysedecisions, actions, and performance agreed KPIs – all leaders shouldtake responsibility to constructively challenge that verbal and writtenreports are representative and have been tested. This should bedelivered via a positive challenge that is integral to innovation andproblem solving.
R – Resilience Leadership should promote and ensure both system and peopleresilience – all leaders should ensure that systems, people andprocesses can withstand the pressure that come to bear in the contextin which they work, e.g., the processes by which clinical standards aremet need to be resilient enough to withstand busy periods. Personaland professional support should be routinely factored for individuals aspart of management supervision and development. This enables rolemodelling, prioritisation and strategic thinking to permeate theorganisation.

Notes
Colchester Hospital University Foundation Trust 19

Colchester Hospital University Foundation Trust 20
Colchester Hospital University Foundation Trust 21

Colchester Hospital University Foundation Trust 22

EY | Assurance | Tax | Transactions | Advisory
About EYEY is a global leader in assurance, tax, transaction and advisoryservices. The insights and quality services we deliver help build trustand confidence in the capital markets and in economies the worldover. We develop outstanding leaders who team to deliver on ourpromises to all of our stakeholders. In so doing, we play a critical rolein building a better working world for our people, for our clients andfor our communities.
EY refers to the global organization, and may refer to one or more, ofthe member firms of Ernst & Young Global Limited, each of which is aseparate legal entity. Ernst & Young Global Limited, a UK companylimited by guarantee, does not provide services to clients. For moreinformation about our organization, please visit ey.com.
Ernst & Young LLPThe UK firm Ernst & Young LLP is a limited liability partnership registered in England andWales with registered number OC300001 and is a member firm of Ernst & Young GlobalLimited.
Ernst & Young LLP, 1 More London Place, London, SE1 2AF.
© 2017 Ernst & Young LLP. Published in the UK.All Rights Reserved.
ED None
EYG no. 00652-184GBL
EY-000034402-01 (UK) 06/17. Creative Services Group London.
In line with EY’s commitment to minimise its impact on the environment, thisdocument has been printed on paper with a high recycled content.
Information in this publication is intended to provide only a general outline of the subjectscovered. It should neither be regarded as comprehensive nor sufficient for making decisions,nor should it be used in place of professional advice. Ernst & Young LLP accepts noresponsibility for any loss arising from any action taken or not taken by anyone using thismaterial.
ey.com/uk