cognitive decline and the role of hearing aids - starkeypro · cognitiv 2 more specifically,...
TRANSCRIPT

1C o g n i t i v e D e c l i n e a n d t h e R o l e o f H e a r i n g A i d s
Brief History of Cognitive and Auditory Research
Research scholars began investigating the interaction between hearing and cognition more than three decades ago (Duquesnoy, 1983; Bronkhors & Plomp, 1988). In fact, ground-breaking research that studied cognition and hearing was conducted in the 1950s by Broadbent, Cherry and others in Cambridge (Broadbent, 1958). Following World War II, scientists embarked on studying the connection between cognitive and auditory processing; however, it was not until the 1990s that the study of cognition and hearing started to gain momentum and the number of publications linking hearing and cognition started to remarkably grow (Arlinger et al., 2009).
Because listening and understanding speech is a complex task that involves a wide variety of sensory and cognitive processes, researchers have always sought to understand how the brain builds meaningful descriptors of the auditory world. Further, the critical implications and impact of cognition-audition interactions on the diagnosis and treatment of hearing loss have lead researchers to combine their efforts in studying auditory and cognitive functions. As reported by Arlinger and colleagues, 2009, there are numerous factors that have contributed toward the convergence of auditory and cognitive research—some of them are listed in Table 1.
Connection Between Hearing Loss and Cognitive Decline
A large and growing body of literature exists on the connection between hearing loss and cognitive decline. Hearing loss has been associated with greater declines in cognitive function in older adults than in their counterparts without hearing loss (Lin et al., 2013; Lin et al., 2004; Lindenberger & Baltes, 1994; Ulhmann et al., 1989; Tay et al., 2006; Baltes & Lindenberger, 1997). For example, audiometric hearing thresholds have been linked to cognitive performance on test-specific tasks involving memory and executive and global functions in older adults (Lin et al. 2011a, b).
Cognitive Decline and the Role of Hearing Aids
Dania Rishiq, Ph.D.
CONTRIBUTING FACTOR REFERENCE
The need to understand the listener’s performance in real-world environments
Bregman, 1990; McAdams & Bigand, 1993; Neuhoff, 2004
The need to understand how aging and impairments change performance
Schneider & Pichora-Fuller, 2000; Wahlin, MacDonald, de Frias, Nilsson & Dixon, 2006)
How to design new communication technologies using advanced signal processing
Edwards, 2007
How to design educational and rehabilitation programs that improve performance
Kraus, McGee, Carrell, King, Tremblay & Nicol, 1995; Tremblay, 2007
The emergence of new research tools, such as eye-movement tracking devices and advanced physiological methods
Durlach & Mavor, 1995; Allopenna et al., 1998; Belin et al., 1999; 2000
The proposal of new models for cognition-audition interaction
Holt & Lotto, 2008; Stenfelt & Ronnberg, 2009
Factors contributing toward the convergence of auditory and cognitive research
Table 1
2C o g n i t i v e D e c l i n e a n d t h e R o l e o f H e a r i n g A i d s
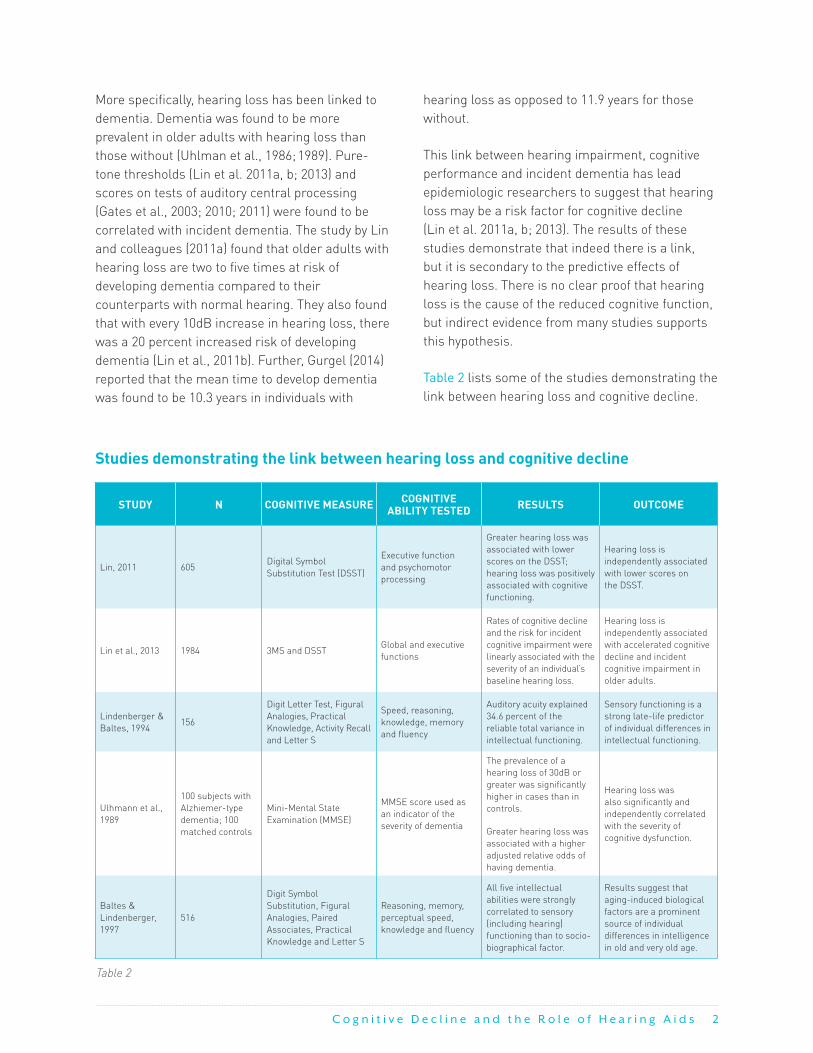
More specifically, hearing loss has been linked to dementia. Dementia was found to be more prevalent in older adults with hearing loss than those without (Uhlman et al., 1986; 1989). Pure-tone thresholds (Lin et al. 2011a, b; 2013) and scores on tests of auditory central processing (Gates et al., 2003; 2010; 2011) were found to be correlated with incident dementia. The study by Lin and colleagues (2011a) found that older adults with hearing loss are two to five times at risk of developing dementia compared to their counterparts with normal hearing. They also found that with every 10dB increase in hearing loss, there was a 20 percent increased risk of developing dementia (Lin et al., 2011b). Further, Gurgel (2014) reported that the mean time to develop dementia was found to be 10.3 years in individuals with
hearing loss as opposed to 11.9 years for those without.
This link between hearing impairment, cognitive performance and incident dementia has lead epidemiologic researchers to suggest that hearing loss may be a risk factor for cognitive decline (Lin et al. 2011a, b; 2013). The results of these studies demonstrate that indeed there is a link, but it is secondary to the predictive effects of hearing loss. There is no clear proof that hearing loss is the cause of the reduced cognitive function, but indirect evidence from many studies supports this hypothesis.
Table 2 lists some of the studies demonstrating the link between hearing loss and cognitive decline.
STUDY N COGNITIVE MEASURE COGNITIVE ABILITY TESTED RESULTS OUTCOME
Lin, 2011 605Digital Symbol Substitution Test (DSST)
Executive function and psychomotor processing
Greater hearing loss was associated with lower scores on the DSST; hearing loss was positively associated with cognitive functioning.
Hearing loss is independently associated with lower scores on the DSST.
Lin et al., 2013 1984 3MS and DSSTGlobal and executive functions
Rates of cognitive decline and the risk for incident cognitive impairment were linearly associated with the severity of an individual’s baseline hearing loss.
Hearing loss is independently associated with accelerated cognitive decline and incident cognitive impairment in older adults.
Lindenberger & Baltes, 1994
156
Digit Letter Test, Figural Analogies, Practical Knowledge, Activity Recall and Letter S
Speed, reasoning, knowledge, memory and fluency
Auditory acuity explained 34.6 percent of the reliable total variance in intellectual functioning.
Sensory functioning is a strong late-life predictor of individual differences in intellectual functioning.
Ulhmann et al., 1989
100 subjects with Alzhiemer-type dementia; 100 matched controls
Mini-Mental State Examination (MMSE)
MMSE score used as an indicator of the severity of dementia
The prevalence of a hearing loss of 30dB or greater was significantly higher in cases than in controls.
Greater hearing loss was associated with a higher adjusted relative odds of having dementia.
Hearing loss was also significantly and independently correlated with the severity of cognitive dysfunction.
Baltes & Lindenberger, 1997
516
Digit Symbol Substitution, Figural Analogies, Paired Associates, Practical Knowledge and Letter S
Reasoning, memory, perceptual speed, knowledge and fluency
All five intellectual abilities were strongly correlated to sensory (including hearing) functioning than to socio-biographical factor.
Results suggest that aging-induced biological factors are a prominent source of individual differences in intelligence in old and very old age.
Table 2
Studies demonstrating the link between hearing loss and cognitive decline

3C o g n i t i v e D e c l i n e a n d t h e R o l e o f H e a r i n g A i d s
Explanatory Hypotheses
Two main explanatory hypotheses have been proposed to explain the mechanisms underlying the association between hearing loss and cognitive decline. The first hypothesis suggests that hearing loss and cognitive decline share a common neuropathologic origin, such as age-related neurodegenerative changes caused by microvascular diseases and inflammation (Lindenberger, & Baltes, 1994; Baltes & Lindenberger, 1994). In other words, this model proposes that hearing loss and cognitive impairment in older adults may share the same underlying pathology.
The second hypothesis, known as the “cascade” hypothesis, argues for a causal relationship between hearing loss and cognitive decline, and suggests that hearing loss exists in conjunction with or interacts with other risk factors to accelerate cognitive loss (Lin et al., 2013).
According to this hypothesis, hearing loss may impact cognition in three main ways:
1. Long-term auditory deprivation may result in reduced cognitive function (Birren, 1964; Wahl & Heyl, 2003).
2. One possibility is that the link between hearing loss and cognitive decline is mediated by lifestyle factors. Hearing loss may result in reduced participation in social leisure activities and in withdrawal from social interactions. In fact, hearing loss is independently associated with social isolation and depression (Gates & Mills, 2005). There is also a connection between social isolation and depression and cognitive decline (Plassman et al., 2007, Steffens et al., 2006). The cascade hypothesis suggests that social isolation can lead to depression and other psychological consequences that may affect cognitive function.
3. Hearing loss may result in increased compensatory cognitive effort exerted to fill in the gaps caused by missing speech
information, which may result in a shortage of cognitive resources dedicated for encoding speech into memory in an already reduced working memory in older adults (Schneider et al., 2010; Tun et al., 2012; Pichora-Fuller & Singh, 2006).
A third hypothesis suggests that the reduced cognitive function seen in older adults can be confounded by hearing loss. Individuals with hearing loss are at a disadvantage if cognitive tests are to be administered using auditory stimuli (Gussekloo et al. 2005). This hypothesis seems unlikely because the link between hearing loss and cognitive decline remains unaltered whether cognitive tests are administered through the auditory or visual modality (Tay et al., 2006). In order to account for hearing loss when
Figure 2. Cascade and common cause hypotheses. Duplicate figure from Dawes, P (2014). Can Hearing Aids Prevent Cognitive Decline and Dementia? Audacity, 4: 20–22.
Cascade Model
Common Cause Model
Age-related changes in
the nervous system
Hearing loss
Cognitive decline
Hearing loss
Cognitive decline
Sensory deprivation
Social isolation
and lack of stimulation

4C o g n i t i v e D e c l i n e a n d t h e R o l e o f H e a r i n g A i d s
administering cognitive tests, an effort should be made to ensure that the auditory signal is presented at an adequate level. In addition, visual stimuli can be used as an alternative to auditory stimuli when testing cognitive performance in patients with hearing loss.
Hearing Aids and Cognition (Review of Studies)
A small number of studies have examined the effects of hearing aid use on cognitive performance in older listeners. The findings of these studies were inconclusive. The inconclusive results may be attributed to differences in methodology. For example, some of the cognitive tests used in these
studies employed auditory stimuli; therefore, improvements in cognitive function may be due to improved audibility with hearing aids. Also, there was a lack of information on whether amplification was well fitted and whether the hearing loss had been appropriately compensated for.
Up to date, there is a lack of strong evidence on the long-term protective effects of hearing aid use against cognitive decline (Kalluri & Humes, 2012). Further research is needed as to whether hearing aid use could prevent, reduce, arrest or reverse cognitive decline in older adults.
Table 3 lists some of the studies that looked into the effects of hearing aid use on cognitive function in older adults.
STUDY COGNITIVE MEASURE
HEARING AID USE
SHOWED IMPROVEMENT IN COGNITIVE FUNCTION?
MODE OF ADMINISTRATION COMMENTS
Mulrow et al., 1990
Short Portable Mental Status Questionnaire (SPMSQ)
4 months Yes Verbally
The SPMSQ is commonly used as a simple screening tool that is not designed to detect changes in cognitive function.
Acar et al., 2011 MMSE 3 months Yes Verbally Cognitive test was administered verbally
Lin, 2011 DSST
At least once a day over the preceding year
Yes. HA use was positively associated with cognitive function
DSST is a nonverbal test.
Results must be interpreted with caution because of the small number (n = 13) of participants using hearing aids.
Choi et al. 2011Visual Verbal Learning Test (VVLT)
6 months Yes, significant changes in the total score
VisualDue to the small sample size, the findings of this study should be interpreted with some caution (n = 18)
Tesch-Römer, 1997
Executive function and memory
6 months No Verbal and nonverbalSince the subjects were not randomly assigned, six months of HA use is too short to cause any significant change.
Van Hooren et al., 2005
Processing speed, reasoning, memory, knowledge and verbal fluency (broad range of cognitive tests)
12 monthsNo improvement was observed.
Verbal and nonverbal
Older adults did not pursue intervention for eight to 12 years after the first notice of a hearing impairment
Wong et al. 2014 MMSE6.9 (4.3) years
No. Out of the eight domains measured on the MMSE, auditory factors (i.e. duration of hearing aid use, aided noise composite SRTs, and aided sound-field thresholds) predicted the scores on five MMSE domains that required understanding of the verbal instructions
Auditory and visual
Monaural hearing aid fittings
Table 3

5C o g n i t i v e D e c l i n e a n d t h e R o l e o f H e a r i n g A i d s
Implications on Clinical Practice
It is crucial for clinicians to learn whether earlier or better hearing healthcare could arrest, reverse or slow down the progression of cognitive decline in older adults (Pichora-Fuller, 2010). Further, older adults with hearing loss tend to wait a long time before they wear hearing aids. Therefore, it is important for hearing healthcare professionals to know whether or not to make evidence-based recommendations to try hearing aids early on.
In order to address these clinical questions and many more, a carefully planned longitudinal study is still required to examine the casual relationship between the long-term use of appropriately fitted hearing aids and the progression of cognitive function.
References
Acar, B., Yurekli, M., Babademez, M., Karabulut, H., & Karase, R. (2011). Effects of hearing aids on cognitive functions and depressive signs in elderly people. Archives of Gerontology and Geriatrics, vol. 52, no. 3, pp. 250–252.
Allopenna, P. D., Magnuson, J. S., & Tanenhaus, M. K. (1998). Tracking the time course of spoken word recognition using eye movements: Evidence for continuous mapping models. Journal of Memory and Language, 38, 419–439.
Arlinger S., Lunner T., Bjorn L., & Pichora-Fuller K. (2009). Scandinavian Journal of Psychology, 50, 371–384.
Baltes, P. B. & Lindenberger, U. (1997). Emergence of a powerful connection between sensory and cognitive functions across the adult life span: “A new window to the study of cognitive aging?” Psychology and Aging, 12, 12–21.
Belin, P., Zatorre, R. J., Hoge, R., Evans, A. C., & Pike, B. (1999). Event-related fMRI of the auditory cortex. NeuroImage, 10, 417– 429.
Belin, P., Zatorre, R. J., Lafaille, P., Ahad, P., & Pike, B. (2000). Voice-selective areas in human auditory cortex. Nature, 403, 309– 312.
Birren, J. (1964). The Psychology of Aging. Englewood Cliffs, NJ: Prentice-Hall
Bregman, A. (1990). Auditory scene analysis: “The perceptual organization of sound.” Cambridge, Mass: MIT Press.
Broadbent, D. E. (1958). Perception and communication. Amsterdam: Elsevier Science
Bronkhorst, A. W. & Plomp, R. (1988). Binaural speech intelligibility in noise for hearing-impaired listeners. J Acoust Soc Am, 86, pp. 1374–1383.
Choi, A., Shim, H., Lee, S., Yoon, S., & Joo, E. (2011). Is cognitive function in adults with hearing impairment improved by the use of hearing aids? Clinical and Experimental Otorhinolaryngology, vol. 4, no. 2, pp. 72–76.
Durlach, N. I. & Mavor, A. S. (1995). Virtual reality: scientific and technological challenges, National Research Council (US). Committee on Virtual Reality Research and Development. Washington, DC: National Academies Press.
Duquesnoy, A. J. (1983). The intelligibility of sentences in quiet and in noise in aged listeners. J Acoust Soc Am, 74, pp. 1136–1144.
Edwards, B. (2007). The future of hearing aid technology. Trends in Amplification, 11, 31–46.
Gates, G. A., Anderson, M. L., McCurry, S. M., Feeney, M. P., & Larson, E. B. (2011). Central auditory dysfunction is a harbinger of Alzheimer’s dementia. Archives of Otolaryngology — Head and Neck Surgery, 137, 390-395. doi: 10.1001/archoto.2011.28
Gates, G. A., Gibbons, L. E., McCurry, S. M., Crane, P. K., Feeney, M. P., & Larson, E. B. (2010). Executive dysfunction and presbycusis in older persons with and without memory loss and dementia. Cognitive and Behavioral Neurology, 23, 218-223. doi: 10.1097/WNN.0b013e3181d748d7
Gates, G. A. & Mills, J. H. (2005). Presbycusis. Lancet. 366(9491): 1111–1120.
Gussekloo, J., de Craen, A. J. M., Oduber, C., van Boxtel, M. P. J., & Westendorp, R. G. J. (2005). Sensory impairment and cognitive functioning in oldest-old subjects: the leiden 85+ study. American Journal of Geriatric Psychiatry, vol. 13, no. 9, pp. 781–786.
Gurgel, R. K., Ward, P. D., Schwartz, S., Norton, M. C., Foster, N. L., & Tshanz, J. T. (2014). Relationship of hearing loss and dementia: a prospective, population-based study. Otology and Neurotology, 35, 755-781. doi: 10.1097/MAO.0000000000000313
Holt, L. L. & Lotto, A. J. (2008). Speech perception within an auditory cognitive science framework. Current Directions in Psychological Science, 17, 42–46.
Kalluri, S. & Humes, L. E. (2012). Hearing technology and cognition. American Journal of Audiology, vol. 21, no. 2, pp. 338–343.
Kraus, N., McGee, T., Carrell, T. D., King, C., Tremblay, K., & Nicol, T. (1995). Central auditory system plasticity associated with speech discrimination training. Journal of Cognitive Neuroscience, 7, pp. 25–32.
Lin, F. R., Yaffe, K., Xia, J., Xue, Q. L., Harris, T. B., Purchase-Helzner, E., & Simonsick, E. M. (2013). Hearing loss and cognitive decline in older adults. JAMA Internal Medicine, 173, pp. 293–299. doi:10.1001/jamainternmed.2013.1868
Lin, M. Y., Guttierrez, P. R., Stone, K. L., Yaffe, K., Ensrud, K. E., Fink, H. A., . Study of Osteoporotic Fractures Research Group. (2004). Vision impairment and combined vision and hearing impairment predict cognitive and functional decline in older women. Journal of the American Geriatric Society, 52, pp. 1996–2002.
Lin, F. R., Yaffe, K., Xia, J., et. al. (2013). “Hearing loss and cognitive decline in older adults,” JAMA Internal Medicine, vol. 173, no. 4, pp. 293–299.
Lin, F. R. (2011). “Hearing loss and cognition among older adults in the United States,” Journals of Gerontology A: Biological Sciences and Medical Sciences, vol. 66, no. 10, pp. 1131–1136.
Lin, F. R., Ferrucci, L., Metter, E. J., An, Y., Zonderman, A. B., & Resnick, S. M. (2011). “Hearing loss and cognition in the Baltimore longitudinal study of aging.” Neuropsychology, vol. 25, no. 6, pp. 763–770.

© 2016 Starkey Hearing Technologies. All Rights Reserved. 3/16 WTPR2728-00-EE-SG
Starkey.com
@StarkeyHearing
facebook.com/starkeyhearing
Lindenberger, U. & Baltes, P. B. (1994). Sensory functioning and intelligence in old age: A strong connection. Psychology and Aging, 9, pp. 339–355.
McAdams, S. & Bigand, E. (1993). Thinking in Sound: The cognitive psychology of human audition. Oxford, UK: Oxford University Press.
Mulrow, C. D., Aguilar, C., Endicott, J. E., et al. (1990). “Quality-of-life changes and hearing impairment: a randomized trial,” Annals of Internal Medicine, vol. 113, no. 3, pp. 188–194.
Neuhoff, J. G. (2004). Ecological psychoacoustics. New York: Academic Press.
Pichora-Fuller, M. K. & Singh, G. (2006). “Effects of age on auditory and cognitive processing: implications for hearing aid fitting and audiologic rehabilitation.” Trends in Amplification, vol. 10, no. 1, pp. 29–59.
Pichora-Fuller, M. K. (2010). Using the brain when the ears are challenged helps healthy older listeners compensate and preserve communication function (pp. 53-65). In L. Hickson (Ed.). Hearing care for adults. Phonak: Stäfa, Switzerland.
Plassman, B.L., Langa, K.M., Fisher, G.G. Heeringa, S.G., Weir, D.R., Ofstedal, M.B., Wallace, R.B. (2007). Prevalence of dementia in the United States: The aging, demographics, and memory study. Neuro epidemiology, 29, 125-132. http://dx.doi.org/10.1159/000109998
Schneider, B. & Pichora-Fuller, M. K. (2000). Implications of sensory deficits for cognitive aging. In F. I. M. Craik & T. Salthouse (Eds.). The handbook of aging and cognition, 2nd edn (pp. 155– 219). Mahwah, NJ: Lawrence Erlbaum.
Schneider, B. A., Pichora-Fuller, K., & Daneman, M. (2010). “Effects of senescent changes in audition and cognition on spoken language,” in The Aging Auditory System, Gordon-Salant, S., R. Frisina, D., Popper, A. N., & Fay, R. R., Eds., vol. 34 of Springer Handbook of Auditory Research, pp. 167–210, Springer, New York, NY.
Steffens, T., Lesinski-Schiedat, A., Strutz, J., Aschendorff, A., Klenzner, T., Rühl, S., . . . Lenarz, T. (2008) The benefits of sequential bilateral cochlear implantation for hearing-impaired children. Acta Otolaryngol 128(2):164–176.
Stenfelt, S. & Rönnberg, J. (2009). Cognitive hearing science: from hearing to listening. Scandinavian Journal of Psychology, 50, 385-393.
Tay, T., Wang, J. J., Kifley, A., Lindley, R., Newall, P., & Mitchell, P. (2006). “Sensory and cognitive association in older persons: Findings from an older Australian population,” Gerontology, vol. 52, no. 6, pp. 386–394.
Tesch-Römer, C. (1997). Psychological effects of hearing aid use in older adults. Journal of Gerontology.
Tremblay, K. (2007). Training-related changes in the brain: Evidence from human auditory-evoked potentials. Seminars in Hearing, 28, pp. 120–132.
Tun, P. A., Williams, V. A., Small, B. J., & Hafter, E. R. (2012). “The effects of aging on auditory processing and cognition,” American Journal of Audiology, vol. 21, no. 2, pp. 344–350.
Uhlmann, R. F., Larson, E. B., Rees, T. S., Koepsell, T. D., & Duckert, L. G. (1989a). Relationship of hearing impairment to dementia and cognitive dysfunction in older adults. Journal of the American Medical Association, 261, pp. 1916–1919.
Uhlmann, R. F., Teri, L., Rees, T. S., Mozlowski, K. J., & Larson, E. B. (1989b). Impact of mild to moderate hearing loss on mental status testing. Journal of the American Geriatric Society, 37, pp. 223–228.
Uhlmann, R. F., Larson, E. B., & Koepsell, T. D. (1986). Hearing impairment and cognitive decline in senile dementia of the Alzheimer’s type. Journal of the American Geriatrics Society, 34, pp. 207-210.
Van Hooren, S. A., Anteunis, L. J., Valentijn, S. A., Bosma, H., Ponds, R. W., Jolles, J. & van Boxtel, M. P. (2005). Does cognitive function in older adults with hearing impairment improve by hearing aid use? International Journal of Audiology, 44, pp. 265–271.
Wahl, H. W. & Heyl, V. (2003). Connections between vision, hearing, and cognitive function in old age. Generations, 27, pp. 39–45.
Wahlin, A., MacDonald, S. W. S., de Frias, C. M., Nilsson, L. G., & Dixon, R. A. (2006). How health and biological age influences chronological age and sex differences in cognitive aging: Moderating, mediating, or both? Psychology and Aging, 21, pp. 318–332.
Wong, L. L., Yu, J. K., Chan, S. S., & Tong, M. C. (2014). Screening of cognitive function and hearing impairment in older adults: a preliminary study. Biomed Res In. http://dx.doi.org/10.1155/2014/867852