coding, documenting, billing & auditing psychological services: a 10 year of progress report...
TRANSCRIPT
Coding, Documenting, Billing & Auditing Psychological Services: a 10 year of progress report
Antonio E. PuenteDepartment of PsychologyUniversity of North Carolina at Wilmington 28403-3297Tel 910.962.3812, Fax 910.962.7010, e-mail [email protected]; web “clinicalneuropsychology.com”
North Carolina Psychological AssociationRaleigh, NC, March 3, 2000
Disclaimer
This workshop presents a list of recommendation for obtaining reimbursement for and documenting professional psychological services. These recommendations are based on the the author’s work with the AMA-CPT Panel (4th and 5th editions) as well as HCFA’s Medical Directors’ Workgroup and the Medicare Coverage Advisory Committee.
Disclaimer (continued)
These suggestions are being constantly revised and serve as general guidelines. Legal and third-party state and federal regulations may vary relative to these recommendations.
Acknowledgements
North Carolina Psychological AssociationAmerican Psychological Association
Practice Directorate Division of Clinical Neuropsychology
National Academy of NeuropsychologyUniversity of North Carolina at
Wilmington
Outline of PresentationHistory/Background of InvolvementDiagnosesProcedural CodingTime, Site of Service, ProviderReimbursementDocumentationAuditingRelated IssuesMedicareTestsFuture Trends

Purpose of My Involvement with Coding & MedicareShort Term
ReimbursementLong Term
Why the Focus on Medicare Bring Some Standardization to the Field Expand the Scope and Value of Clinical
Neuropsychology and Psychology Parity with Other Doctoral Level Health Providers
in Health Care Shape Psychology Towards a Biological Model
History/Background
North Carolina Psychological Association NCPA & NCPF President Blue-Cross Blue Shield
American Psychological Association Chair or Member of Approximately a Dozen
Committees/Boards, (e.g., CE, BCA) Division 40 Board- 1987 to present Two Terms on APA’s Council of Representatives-
Div. 40 (1994 to present) Policy and Planning Board
History/Background (continued)
American Medical Association CPT- 4 CPT- 5
APA’s Practice DirectorateBlue Cross/Blue Shield of North CarolinaHealth Care Financing Administration
Model Mental Health Policy Workgroup Medicare Coverage Advisory Committee
Medicare: Overview
Benefits Part A (Hospital) Part B (Supplementary) Part C (Medicare + Choice)
HCFA Vs. Local Carrier

Medicare: Local Medical Review Policy
Development of Local PolicyRestrictive
Reimbursement Model
DiagnosesProcedural CodeTimeSite of ServiceProviderFormula
Dx X Code X Time X Site X Provider

Procedural Coding
Defining CodingHistory of CodingCoding
Diagnoses
System (World Health Organization) DSM= 290-319 ICD = all other diagnoses
Referral Diagnosis Referral versus Final Diagnoses Rule-Out Diagnoses
Multiple Diagnoses Advisable for Medically Necessary First Diagnosis is Most Important

Defining CodingDescription of Professional Service
RenderedPurpose of Coding
Reimbursement Archival/Research Performance Assessment
Current Coding Systems SNOMED WHO / ICD AMA / CPT
History of CPT Coding
First Developed in 1966Currently Using the 4th EditionThe 5th Edition Will be Used in 2002A Total of 7,500 CodesAMA Developed and Owns the CPTUnder Contract with the HCFA
CPT & HCFA
Federal Register, August 17,2000 Health Insurance Reform: Standards for
Electronic Transactions The CPT is the standard code set for
reporting physician and other health care services

Developing Codes
Member/Society Generated IdeaAPA Practice Directorate Health Care Professionals Advisory
CommitteeIntegration with Specialty Groups within
American Medical Association/WorkgroupFormal Panel PresentationRelative Value of CodeTime Frame (3-6 years)

Overview of Coding
Total Possible Codes = 60+# Of Typically Reimbursed Codes = 5
interview, testing, & psychotherapy# Of Codes Sometimes Reimbursed = 35
family/group therapy biofeedback
# Of Codes Rarely Reimbursed = 20+ evaluation and management report evaluation and writing
Overview of Coding: An evolution of coding
PsychiatryNeurologyPhysical Medicine & Rehabilitation“Evaluation & Management”

Overview of Coding (cont.)
Psychiatry Interview (90801) Psychotherapy (90804 - 90857)
Types of Psychotherapy (regular vs interactive)# of “Patients” (individual vs group vs family)Locations of Intervention (in vs outpatient)Evaluation & Management vs RegularLength of Time (30, 60, 90)
BiofeedbackRegular vs Psychophysiological (90901 vs 90875)

Overview of Coding (cont.)
Central Nervous System Assessments/Test 96100 = Psychological Testing 96105 = Aphasia Testing 96110/1 = Developmental Testing 96115 = Neurobehavioral Status
Exam 96177 = Neuropsychological Testing
Overview of Coding (cont.)
Physical Medicine 97770 = Cognitive Skills Development Look for New/split Codes in the Near
Future

Overview of Coding (cont.)
Health & Behavior 909X1 assessment (15 minutes) 909X2 re-assessment 909X3 intervention- individual 909X4 intervention- group 909X5 intervention- family 909X6 intervention- family w/o pt. NOTE: codes have been valued and will be
available for use in 01.2002

Coding Modifiers
Acceptability Medicare = 95% Others = Approximately 80%
Modifiers 22 = Unusual or More Extensive Service 51 = Multiple Procedures 52 = Reduced Service 53 = Discontinued Service

New Category II Codes:Performance Measurement
Purpose Reduction of detailed chart review Provide performance measurement
Use Alphanumeric identifier with a letter in the
last field Evidenced-based measurement that
address conditions of high prevalence, risk or cost with established health outcomes

New Category III Codes:Emerging Technology Purpose
Collect data and assess efficacy of new procedures
Use Alphanumeric identifier
Example 0018T Repetitive Transcranial Magnetic Stimulation Delivery of high power, focal magnetic pulses for
direct stimulation of cortical neurons

Next Set of Codes
Splitting of the Neuropsychological (and possibly, later) the Testing Codes Rationale
5 Year Re-evaluationLack of Cognitive Component
ApproachIntegration with HCFAInvolvement of NAN, 40Group Survey Testing

Coding Overview
Coding Categories Psychiatry Neurology; CNS/Assessment Physical Medicine “Evaluation & Management”
Procedures Assessment Intervention
Overview of Coding (cont.)
Diagnosing If Problem is Psychiatric = DSM If Problem is Neurological = ICD
Matching Dx with CPT DSM = 90801, 96100, 90806 ICD = 96115, 96117, 97770

Reimbursement
HistoryProspective Payment SystemDefining RBRVSReimbursement Difficulties

Overview of the History of Reimbursement
Cost plus ReimbursementProspective Payment (PPS) &
Diagnostic Related Groups (DRGs)Customary. Prevailing, &
Reasonable(CPR)Resource Based Relative Value
System (RBRVS)Prospective Payment System
RBRVS: Purpose & History
Purpose: To Provide Equitable Payment for Medical Services
History Phase I: Initial 12 physician specialties Phase II: Psychiatry Phase III: Psychology
RBRVS: Overview
Major Components Physician Work Resource Value Unit Practice Expense Resource Value Unit Malpractice Component Resource Value
Unit Geographical Practice Cost Index
RBRVS: Conversion Factor
Dollar Value That Is Utilized to Convert the Resource Value Units and Geographic Practice Cost Indexes Into a Payment

RBRVS: Adoption
MedicareBlue Cross/Blue Shield = 87%Managed Care = 69%Medicaid = 55%Other = 44%

Prospective Payment System
Standard Scenario Included in inpatient bundled service
Alternative Scenario Bill under own provider number
Inpatient versus Patient

Reimbursement Difficulties
Physician Work ValuePhd/PsyD/EdD vs MDLocation Defined
Common Reasons for Lack of Reimbursement
Clerical ErrorsService Is Not CoveredNo Prior Authorization ObtainedExceeded Allocated Time LimitsInvalid or Incorrect Dx CodeCPT and Dx Do Not Match

Time
Defining Time Professional (not patient) Activity
AMA Definition Physicians also spend time during work,
before, or after the face-to-face time with the patient, performing such tasks as reviewing records and tests, arranging for services and communicating further with other professional and the patient through written reports and telephone contact
Testing Time Defined
Preparing to Test PatientReviewing of RecordsSelection of TestsScoring of TestsReviewing of ResultsInterpretation of ResultsPreparation and Report Writing

Testing Time Defined (continued)
Communicating Further With OthersFollow-up With Patient, Family,
and/or OthersArranging for Ancillary and/or Other
Services

Intervention Time Defined
All Time is Bundled in the Allocated Time 90806 = 45 minutes of total time 97770 = 15 minutes of total time

Time X Code
Interview & Assessment Hourly Increments
Intervention 15 30 45 90?
Quantifying Time
Rounding Round up or down to nearest increment
Time Does Not Include; Patient completing tests, forms, etc. Waiting time by patient Type of reports Non-professional time Literature searches, learning new
techniques, etc.

Site of Service
Inpatient Physical location Billing and business relations Origin of the patient Skilled and assisted nursing fascilities
Outpatient By definition, anything that is not
inpatient

Provider
Doctorate Medicare: PhD/PsyD/EdD = MD Non-Medicare: 0-50% less than MD
Non-Doctorate Social Security The special case of North Carolina

Medical NecessityDefinition
Reasonable and necessary for the diagnosis or treatment of an illness or injury or to improve the functioning of a malformed body member
Stand Alone Each activity must stand alone Point-to-point correspondence between
symptoms and proceduresLikely Types
Acute and emergency

Documentation
PurposeGeneral GuidelinesSpecific DocumentationTrendsSuggestions

Purpose of Documentation
Evaluate and Plan for TreatmentCommunication and Continuity of
CareClaims Review and PaymentResearch and Education
General Principles of Documentation
Complete and LegibleReason/Rationale for the EncounterAssessment, Impression, or
Diagnosi/esPlan for CareDate and Identity of Observer

Documentation History
Chief ComplaintHistory of Present Illness (HPI)Review of SystemsPast, Family, and/or Social History

Documentation of Chief Complaint
Concise Statement Describing the Symptom, Problem, Condition, Diagnosis, Physician Recommended Return, or other Factor that is the Reason for the Encounter.
Documentation of Present IllnessChronological Description of the
Development of the Patient’s Present Illness from the First Sign and/or Symptom or from the Previous Encounter to the Present. For Symptoms: Location, Quality, Severity,
Duration, Timing, Context, Modifying Factors Including Medications, Associated Signs, Symptoms, etc.
For Follow up: Changes in Condition Since Last Visit, Compliance with Treatment, etc.
Review of Systems
PsychiatricNeurologicalOther
Documentation of History
Past HistoryFamily HistorySocial History

Specific Documentation Suggestions: Psychiatric Interview
Name, Date, Observer, Dx/Impression
Mental Status Exam Language, Thought Processes, Insight,
Judgment, Reliability, Reasoning, Perceptions, Suicidality, Violence, Mood & Affect, Orientation, Memory, Attention, Intelligence
Specific Documentation Suggestions: Neurobehavioral Status ExamName, Date, Observer, Dx/ImpressionDefinition
Clinical assessment of thinking, reasoning and judgment
Variables Attention, Memory, Visuo-Spatial,
Language, Planning Acquired knowledge, attention, memory,
visual spatial abilities, language functioning, planning
Specific Documentation Suggestions: Testing
Name, Date, Observer, Dx/Impression
Names of TestsInterpretation of Tests ResultsDispositionTime

Defining PsychotherapyPurpose
Resolving problems or alleviating of emotional disturbances, or changing maladaptive patterns of behavior, or encouraging personal growth and development
Approaches Development of insight or affective
understanding, the use of behavior modifying techniques, the use of supportive interactions, the use of cognitive discussion of reality
the use of physical aids or non-verbal techs.
Specific Documentation Suggestion: Psychotherapy
Basic Elements Date Reason for Service Intervention Results Impression Disposition Identity Time
Specific Documentation Suggestion: Cog. Rehab.
Basic Elements Date Reason for Service Training activity Results Identity of Observer Time

Documentation Suggestions
Avoid Handwritten NotesDo Not Use Red InkDocument on Every Encounter, Every
Procedure, and Every PatientRe-Cap Status, Whenever Possible, At
Least Change From Session to SessionDocument Soon After Procedure
Trends
Issues of ConfidentialityOver-DiagnosingOver-DocumentingLimited Interventions & Diagnostic
Procedure

Auditing
Fraud & Abuse vs ErroneousSelf-Auditing SuggestionsRisk SituationsDevelopment of an Internal Auditing
System

Fraud vs Error
Fraud = Intentional, Pattern
Erroneous = Clerical, etc.
Self-Auditing Suggestions
Written PoliciesCompliance OfficerTraining & Education Lines of Communication Should ExistInternal Monitoring & AuditingEnforce Standards Alter as Necessary

Risk Areas for Fraud
Coding & BillingReasonable & Necessary ServicesDocumentationImproper Inducements
Fraudulent Claims Flags
UpcodingExcessive or Unnecessary Visits to ACFOutpatient Service 72 Hrs. Post-DischargeCPT Code Usage ShiftHigh Percentage of the Same CodesUse of Similar Time for Testing Across Pts.Medical Necessity (dx; interpretation)

Evaluating Effectiveness
Adequacy of Evidence Bias External Validity
Size of Effect From Not Effective to Breakthrough

Evaluating Effectiveness (continued)
Organized Approaches to Evaluation of Scientific Evidence American College of Physicians Agency for Health Care Policy and
Research BC/BS Technology Evaluation Center American College of Cardiology American College of Urology

Related IssuesGraduate Medical Education
allied health vs medical interns vs postdoctoral fellows

Related Issues
Incident to Definition
technical services that are an extension of the professional service(s)
inpatient as inpatient
Billingappropriate to provide technical services
anywherenot appropriate to bill technical services
inpatient

Tests
PurposeFundingSampleResults Summary
Tests: Purpose
Which Tests Are Being UsedHow Long Does Each Test TakeAddress More Carefully Pre, During,
and Post-Testing Time
Tests: Sample
Clinical APA
Neuropsychological NAN Total Possible Sample = 2700 Total Sampled = 1200 Total Used = 447

Tests: Time Spent Testing
Hours %0-4 215-9 1110-14 1615-20 19>20 33
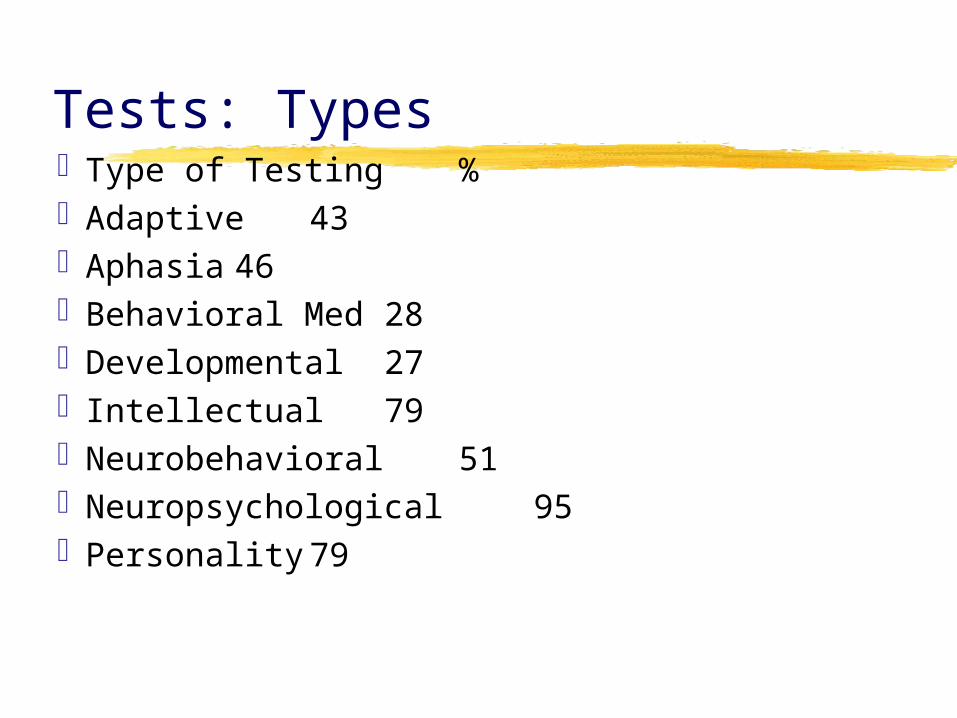
Tests: TypesType of Testing %Adaptive43Aphasia 46Behavioral Med 28Developmental 27Intellectual 79Neurobehavioral 51Neuropsychological 95Personality 79

Tests: Time X Test
Type Admin Score InterpretAdaptive 74 32 48Aphasia 61 24 39Beh Med 110 35 58Develop 113 36 59IQ 122 34 61Neurobeh 80 26 47Neuropsy 304 79 135
Future Trends
Surveys; Practice, Ongoing & New CodesHealth Care Finance AdministrationCommittee for the Advance of
Professional Practice Practice Directorate of the APAGeneral TrendsFuture of Clinical PsychologyResources
Surveys
Rationale for Surveys All Decisions are Empirical Reasonably Large Ns Adequate Data
Support Required If Asked, Participate Three Ongoing;
NAN/Division 40 Practice SurveyRe-evaluation of “Cognitive Rehabilitation”Splitting of Testing Codes

Health Care Financing AdministrationProblems
Definition of Physician (Social Security Practice Act of 1989)
Doctoral vs Non-Doctoral ProvidersDirections
Physician Work Value Practice Expense Matching of CPT with Reimbursement

Committee for the Advancement of Professional Practice
ObserversAttitude
Positive, Receptive New Full-time Staff Member for
Medicare Program (American College of Surgeons)
General TrendsFraud, Abuse, & Effects of RegulationsStandardizing & Expanding Into Non-
Traditional Areas“Boutique” Vs “Industrial” PsychologyPsychometrics as Clinical PsychologyAssessment & Rehabilitation
Psychology’s “Technical” PipelineEstablishment of “Grassroots Network”
Future of Professional Psychology
More (normative?) Data & A Few TheoriesMeasurement of the Cultural & SubjectiveLess Focus on Conserving the Medicare
Trust Fund & Stockholder Profits by Focusing on the Aged & Disabled
Appreciating that Brain is Inside a Person Which is Inside a System (Value?)
Conscilience

ResourcesWeb Sites
neuropsych; NANonline.org, Div40.org government; HCFA.gov, NIH.gov personal; clinicalneuropsychology.com
Publications APA Medicare Handbook (PP; 2000) NAN Bulletin (1994, 1997, 1998, 2000) Journal of Psychopathology & Behavioral
Assessment (1987) Professional Psychology (with Camara & Nathan,
2000)
Resources (continued)Initial Intake FormsPatient Service FormsCoding SheetBilling FormsMedicare/Cigna Information Including
Local Medical Review Revision PolicyBlue Cross/Blue Shield InformationCigna Behavioral Health Forms & ExampleWorkers Compensation Forms

Resources (continued)
CPT ProcessNew Health and Behavior
Assessment and Intervention CodesExisting CPT CodesPsychological Test Usage in
Professional Psychology (Camara, Nathan & Puente, 2000)