code blue do you know what to do? department of clinical education 2009
TRANSCRIPT
Code Blue
Do you know what to do?
Department of Clinical Education 2009

CODE BLUE
An IMPENDING or ACTUAL
CARDIAC/RESPIRATOR
Y ARREST

How To Call A Code Inside Stony Brook Hospital
•DIAL 321 from inhouse phone.
•Identify yourself (give name)
•Announce Code Blue for adults or Code Blue Pediatrics for a child
•Indicate EXACT FLOOR, TOWER & ROOM NUMBER OF PATIENT
•Example: Code Blue, T-16 North, room 240
•Wait for the operator to repeat and confirm location before hanging up.
•Do not hang up on the operator, let them hang up on you.

Response System For Cardiac/Respiratory Emergencies occurring outside of main hospital
East Campus: HSC & Basic Science Tower
Call University Police at 333 or by dialing 632-3333
University Police will contact EMS to respond
Off Site locations: Tech Park, Ambulatory Center
First person on the scene activate 911 to dispatch EMS ambulance

Adult Code Blue Team
Senior Medical Resident (team leader) Anesthesiologist or Anesthesiology
Resident Respiratory Therapist Unit Staff Nurse ICU Nurse will respond as assigned Primary RN stays with Patient!!!

ICU Nurse will respond as assigned:
18S ( SICU) responds to 13N, 14N, 18N, 19N, 19S
17S (MICU) responds to 17S ( dialysis ), 16S,16N,15N, 15S, 12S, 14S ( Endoscopy), 10N ( Adult Psychiatry), 12N (Antepartum)
ED responds to Level 1-4 (except burn and MRI) Maternity Center, 8N, 8S, 9N, 9S
CTICU responds to Burn, MRI CCU responds to Level 5 including CACU Nurse assigned to the patient will be present

Who arrives for a pediatric code? Some members will include: Pediatric Transport Resident If Ped. Transport Resident is
unavailable, the Senior Pediatric Urgent Care Resident
Pediatric Resident on Call for the ER will respond to codes in Pediatric Urgent Care
Unit Staff Nurse PICU Nurse Anesthesiologist Respiratory therapist

Additional Staff Responders All Codes Nurse Manager/Off Shift &/or designee Transporter Public Safety Officer for all codes in
non-patient areas Others involved:
Telephone operator, Unit Clerk, CNA, Distribution Services & Elevator transport

TEAMResponsibilitie
sIn A Code

NSC/ Secretarial support
Assure the Code Blue has been called Calls code: 321 in Hospital 911-out of hospital Prepares forms & Labels Makes phone calls/collects patient
records as directed
Post Code: calls distribution services to return cart

NURSING ASSISTANTS/PCT
Assist with moving Code cart to the patient room
Listen & Follow Directives from the RN
Clean patient area post code
Help transport patient to ICU unit if needed

HOSPITAL ATTENDANT
Is an employee from Distribution Services
Responds to the unit with a new code cart
Returns secured used cart to central sterile

Telephone Operator
Once code is received, initiates code blue page over address system and repeats 3 times
Alert Code Blue team members via pocket pagers
Alert MICU, OR and Anesthesia Alert the ED or nearest patient care
area if public address system or back up pocket pagers should fail

MEDICAL DOCTORS
Senior Medical Resident takes charge & clears the area
If certified, may intubate patient Administer emergency meds as
needed Notifies patients’ attending of arrest Communicates with family at the
earliest possible moment Decides on termination of the code

MD’s Continued
Code Successful—initiate arrangement for transfer to critical care unit
Code Unsuccessful—pronounces patient’s death & refers to autopsy
Completes progress note and reviews/signs Code Blue Resuscitation Record Authorizes all medication/interventions

Anesthesia Proceed to area of code blue
Serve as 2nd/3rd rescuer until team assembles
Inserts ETT when indicated and verifies position with CO2 Detector
Assists in attaching ETT to ventilator
Remains with patient until RT is able to maintain respiratory function of patient

Respiratory Therapist
Establishes and maintains airway Performs tracheal suctioning Assists/performs intubation if certified Provides adequate ventilatory support
via manual resuscitator &/or mechanical ventilator according to MD orders
Maintain & monitor ventilatory status Draw & analyzes ABG’s when indicated Assist in transfer of patient as indicated

Clinician/Charge Nurse/Nurse Manager/ADN
Ensure Code Cart/defibrillator present
Ensure Code Team has responded Assign responsibilities as needed
Code Cart/Medication Nurse Documentation
Assist as needed Removal of other patients & family
members, crowd control, pt. transfer

Registered Nurse/Code Cart RN
Apply multifunction electrode pads
Prepare cart for use/opens cart Puts intubation tray at patient’s
head Prepare & dispense emergency
meds Clearly announces name and
amount of meds handed off Prime IV tubing & make IV labels
Code Cart Nurse continued Charge defibrillator as per team leader
order Distribute supplies as needed from code
cart (bld. specimen tubes, ABG kits, etc.) At the end of the code, return all non-
disposable items (ie. O2 flow meter & suction) back to the used cart & LOCK
Ensure cart exchanged/new & checked for completeness. Sign check sheet
Nurse Recorder
Document code activities, assessments and time performed on the CPR Documentation Record
Can report on medications given including dose and time
Writes progress note on CPR Documentation Record
Complete code Blue Debriefing report and attach to copy of Documentation record
Place white copy of code blue sheet on patients’ chart along with all EKG strips or “complete disclosure” record
Send yellow copy to NM/ADN for review and forward to nursing office

Additional Nurse/designee
Get suction equipment set up and ready for use
Starts IVs/draws blood as needed Administers meds as directed by team
leader and calls out to Nurse Recorder Assist with compressions Assist team as directed

Code Team Positions
Coming soon—All staff members will be assigned Code positions daily
This will decrease confusion of roles and improve patient outcomes!
Training has begun on 16S
Pediatric Codes
Refer to Pediatric Unit for specific policy


How will you Repond?

A Person CollapsesPossible Cardiac Arrest
ASSESS responsiveness
ACTIVATE emergency response system
321
CALL A CODENOW !
I NEED HELP!!!!

NOTE THE TIME!
Military Time Only

CHECK for Airway, Breathing and Circulation

FOCUS: Basic CPR and Defibrillation A= airway: open the airway
B= Breathing: check breathing, provide positive-pressure ventilations
C= Circulation: check circulation, give chest compressions
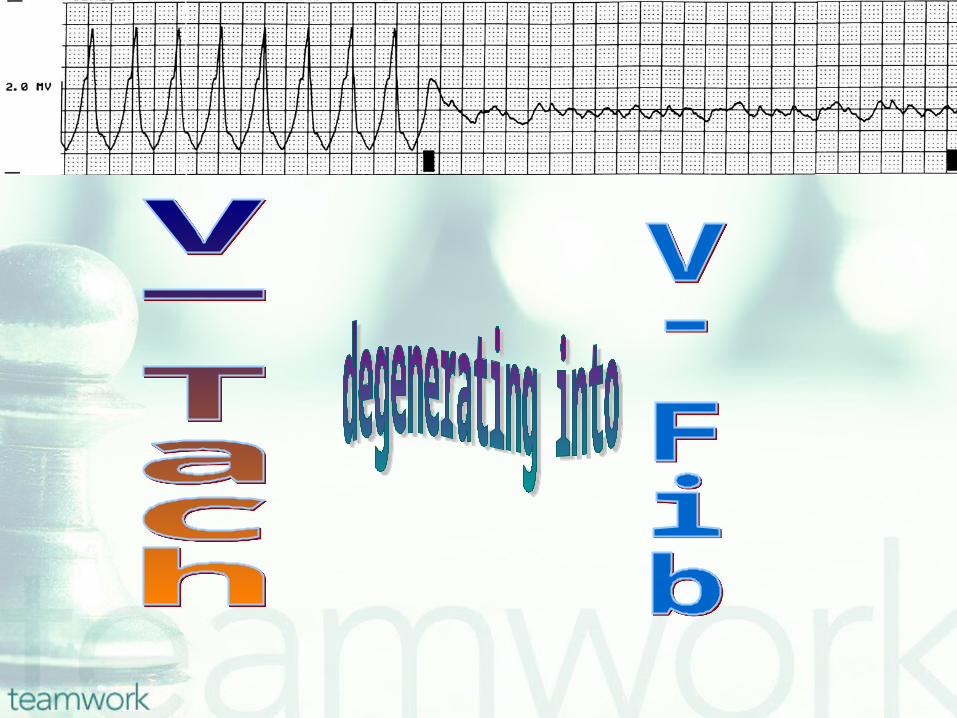
D= Defibrillation: assess for and shock/pulseless VT and V-Fib

Help is on the way
Senior Medical Residents
( team leaders)
Anesthesiologist/ Resident
Respiratory Therapist

ACLS A=Airway: place airway device as soon as possible B=Breathing: confirm proper placement by
PE B=Breathing: confirm proper placement by 2nd method
- End-tidal CO2 - Esophageal detector devices
B= Breathing: prevent airway device dislodgment:
Use ETT holder Use proven tape and tie B= Breathing: monitor oxygenation and
ventilation

ACLS C= Circulation: establish IV access
C= Circulation: identify rhythm
C=Circulation: give rhythm and condition
appropriate drugs.
D=Differential Diagnosis: search for and treat identified reversible causes.

The Code Cart has arrived!

Once The cart is here: Get Ambu bag/ ambu patient Attach ambu to 15L/02 Roll patient-place on backboard and
place pacer pads on Place chest leads-ZOLL Empty bottom drawer- equipment to
head of the patient Hook up suction Prepare drugs Document

DRAWER 1ACLS 1st Line Meds for 30-40 minute code
Adenosine
Amiodarone
Furosemide
Magnesium
Naloxone
•Procainamide
•Vasopressin
•Lidocaine
•Sodium Bicarbonate
•Atropine
•Epinephrine
•Dextrose

DRAWER 2
ABG kits NG tube (salem sump) 5 in 1 connector Zoll pads EKG paste/paper Gauze/ tape Pulse ox monitoring cables
DRAWER 3
Venipuncture Supplies
Phlebotomy Supplies

DRAWER 4
Emergency Cricothyrotomy Set
2 Trachs
CO2 Detector
Suction Catheters (red rubber)

DRAWER 5
IV solutions
IV tubings
Premixed Drips Dopamine Lidocaine
DRAWER 6
Laryngoscope Box Intubation Box Suction set up O2 Set up Central Lines
2 Triple Lumen Catheters Bipolar Pacing Wire

ZOLL-Stat-PadzNOTE: WHEN PLACING PATIENT ON THE
BACKBOARD PLACE stat-padz ON THE PATIENT!
Place pads in anterior/posterior position (sandwich left side of heart) if possibleStat-padz will Monitor, Defibrillate and
Pace as neededConnect to the Multifunction Cable

Paddles
Not recommended, but if used apply small chest electrodes to monitor rhythm White to the right; Smoke (black) over fire (red) on the left MFC must be attached to paddles Apply electrode gel to metal face Place one paddle at apex & one paddle at
the base of the heart

ZOLL Turn ZOLL on ( GRAY )
Gray area on ZOLL indicates monitor
**In an emergency situation, threatened by a lethal arrhythmia (V. Fib, pulseless V. Tach) a LIP/ACLS certified RN/PA may perform defibrillation

TO DEFIBRILLATE Think Red 1,2,3 & MD order Stat Padz or paddles
CHARGE ( default setting is 120 joules), use arrows up or down to change as per MD order
DISCHARGENumbers 1,2,3 match numbers on the ZOLL
“I’m clear, you’re clear, everybody clear??”


TO PACE OR CARDIOVERT Think green and MD order to
transcutaneous pace
When cardioverting remember the sync mode (soft key on bottom)
Joules will automatically default back to 120 ( ready to treat a lethal arrythmia)


Post Defibrillation
Document on CPR Record Continuous monitoring of the cardiac
rhythm is maintained. Document any changes (include EKG strips if possible)
Wash “paddle sites” carefully. Burns may result even with good technique
Change Statz Pads every 8 hours if left on/monitoring

LOCK THE CODE
CART
AFTER USE AND
BEFORE
RETURNING IT

HOW DO WE FILL OUT THE CODE BLUE SHEET?


CODE CARTLocked at all times
Check lock
Check Expiration Dates
Check Items on Cart
CPR board, IV pole, checklist & forms,
Portable oxygen, ZOLL, Pediatric Color
Medication Cards
Check once every 24 hours
Complete checklist

ZOLLClean Unit
Inspection
Supply availability
Power on sequence
Defibrillator
Pacemaker operation
Recorder function

Respiratory Arrest/ STAT Intubation Preparation Recommendations
1. Have Code Cart or STAT intubation tray readily available at patient’s bedside. Med/ Surg units will find the STAT Intubation kit in the bottom of the Code Cart.

2.Place patient on 100% non- rebreather face mask at
10L/minute or assist respirations with Ambu-bag as indicated (Note: Use with caution in patients with severe COPD with known CO2 retention).
3. If Code Blue has not been called
then- a. Call anesthesiologist on call
for emergencies (4-7481). b. STAT page Respiratory
Therapist c. STAT page Primary Team d. Consider calling RRT

4. Connect patient to all essential monitors, including but not limited to; BP cuff, EKG, pulse oximetry

5. Ensure Ambu-bag is at bedside.
6. Ensure suction system at bedside; canister, tubing and yankeur and check that system is properly functioning.
7.Assess patient’s IV access for patency. Insert new PIV if necessary. Consider Intra Osseous catheter for pediatric patients. Have available and primed at bedside; 1 liter bag of 0.9 Normal Saline ( or Lactated Ringer’s solution) to be infused upon MD/NP/PA order.

8. Anticipate pre-intubation sedation needs.

Are there any Questions??