cochrane database of systematic reviews (reviews) || transcutaneous electrical nerve stimulation...
TRANSCRIPT

Transcutaneous electrical nerve stimulation (TENS) for
chronic low-back pain (Review)
Milne S, Welch V, Brosseau L, Saginur M, Shea B, Tugwell P, Wells G
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2005, Issue 2
http://www.thecochranelibrary.com
1Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

T A B L E O F C O N T E N T S
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2SYNOPSIS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2CRITERIA FOR CONSIDERING STUDIES FOR THIS REVIEW . . . . . . . . . . . . . . . . . .
3SEARCH STRATEGY FOR IDENTIFICATION OF STUDIES . . . . . . . . . . . . . . . . . . . .
3METHODS OF THE REVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4DESCRIPTION OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4METHODOLOGICAL QUALITY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
4DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6NOTES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6POTENTIAL CONFLICT OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . .
6ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
6REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
10Characteristics of included studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
13Characteristics of excluded studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14Table 01. Clinical Relevance . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14GRAPHS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
14Comparison 01. TENS vs Placebo, end of treatment (2 days) . . . . . . . . . . . . . . . . . . .
14Comparison 02. TENS vs Placebo, end of treatment (approx 1 month) . . . . . . . . . . . . . . . .
15Comparison 03. TENS vs Placebo, Follow up (3 months) . . . . . . . . . . . . . . . . . . . . .
15Comparison 04. TENS vs Placebo, Follow up (6 months) . . . . . . . . . . . . . . . . . . . . .
15Comparison 05. TENS- High Quality vs. Low Quality, End of Treatment (1 month) . . . . . . . . . . .
15INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15COVER SHEET . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
16GRAPHS AND OTHER TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
16Comparison 05. 01 Pain, continuous, patient-assessed . . . . . . . . . . . . . . . . . . . . . .
17Comparison 05. 01 Pain, continuous, patient-assessed . . . . . . . . . . . . . . . . . . . . . .
17Comparison 05. 02 Pain Improvement, VAS (0-100) . . . . . . . . . . . . . . . . . . . . . .
18Comparison 05. 03 Pain frequency (1 - 5, 1 = never, 5 = all the time) . . . . . . . . . . . . . . . . .
18Comparison 05. 04 Stiffness (VAS) . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19Comparison 05. 05 Flexion ROM . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
19Comparison 05. 06 Extension (degrees) . . . . . . . . . . . . . . . . . . . . . . . . . . .
20Comparison 05. 07 Function (Change from baseline) . . . . . . . . . . . . . . . . . . . . . .
20Comparison 05. 08 Self-Rated Activity Level . . . . . . . . . . . . . . . . . . . . . . . . .
21Comparison 05. 09 Use of services . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
21Comparison 05. 10 Patient Satisfaction . . . . . . . . . . . . . . . . . . . . . . . . . . .
22Comparison 05. 11 McGill Work . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
22Comparison 05. 12 Lasegue’s SLR (degrees) . . . . . . . . . . . . . . . . . . . . . . . . .
23Comparison 05. 13 SLR (degrees) . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
23Comparison 05. 01 Pain, continuous, patient-assessed . . . . . . . . . . . . . . . . . . . . . .
24Comparison 05. 01 Pain, continuous, patient-assessed . . . . . . . . . . . . . . . . . . . . . .
24Comparison 05. 01 Pain, continuous, patient assessed . . . . . . . . . . . . . . . . . . . . . .
25Comparison 05. 02 Disability . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iTranscutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Transcutaneous electrical nerve stimulation (TENS) forchronic low-back pain (Review)
Milne S, Welch V, Brosseau L, Saginur M, Shea B, Tugwell P, Wells G
This record should be cited as:
Milne S, Welch V, Brosseau L, Saginur M, Shea B, Tugwell P, Wells G. Transcutaneous electrical nerve stimulation (TENS) for chronic
low-back pain. The Cochrane Database of Systematic Reviews , Issue . Art. No.: CD003008. DOI: 10.1002/14651858.CD003008.
This version first published online: 23 October 2000 in Issue , .
Date of most recent substantive amendment: 03 August 2000
A B S T R A C T
Background
Low back pain (LBP) affects a large proportion of the population. Transcutaneous electrical nerve stimulation (TENS) was introduced
more than 30 years ago as an alternative therapy to pharmacological treatments for chronic pain. However, despite its widespread use,
the effectiveness of TENS is still controversial.
Objectives
The aim of this systematic review was to determine the efficacy of TENS in the treatment of chronic LBP.
Search strategy
We searched MEDLINE, EMBASE, PEDro and the Cochrane Controlled Trials Register up to June 1, 2000.
Selection criteria
Only randomized controlled clinical trials of TENS for the treatment of patients with a clinical diagnosis of chronic LBP were included.
Abstracts were excluded unless further data could be obtained from the authors.
Data collection and analysis
Two authors independently selected trials and extracted data using predetermined forms. Heterogeneity was tested with Cochran’s Q
test. A fixed effects model was used throughout for continuous variables, except where heterogeneity existed, in which case, a random
effects model was used. Results are presented as weighted mean differences (WMD) with 95% confidence intervals (95% CI), where the
difference between the treated and control groups was weighted by the inverse of the variance. Standardized mean differences (SMD)
were calculated by dividing the difference between the treated and control by the baseline variance. SMD were used when different
scales were used to measure the same concept. Dichotomous outcomes were analyzed with odds ratios.
Main results
Five trials were included, with 170 subjects randomized to the placebo group receiving sham-TENS and 251 subjects receiving active
TENS (153 for conventional mode, 98 for acupuncture-like TENS). The schedule of treatments varied greatly between studies ranging
from one treatment/day for two consecutive days, to three treatments/day for four weeks. There were no statistically significant
differences between the active TENS group when compared to the placebo TENS group for any outcome measures. Subgroup analysis
performed on TENS application and methodological quality did not demonstrate a significant statistical difference. Remaining pre-
planned subgroup analysis was not conducted due to the small number of included trials and the variety of outcome measures reported.
Authors’ conclusions
The results of the meta-analysis present no evidence to support the use of TENS in the treatment of chronic low back pain. Clinicians
and researchers should consistently report the characteristics of the TENS device and the application techniques used. New trials on
TENS should make use of standardized outcome measures. This meta-analysis lacked data on how TENS effectiveness is affected by
four important factors: type of applications, site of application, treatment duration of TENS, optimal frequencies and intensities.
1Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

S Y N O P S I S
There is no evidence from trials to show the effects of transcutaneous electrical nerve stimulation (TENS) for chronic low back pain.
Low back pain (LBP) affects a large number of people and can severely limit work and recreation. Transcutaneous electrical nerve
stimulation (TENS) is a therapeutic non-invasive therapy that stimulates nerves electrically via electrodes placed onto the skin. The
review of trials found no evidence to show the effectiveness of TENS when used alone for chronic low back pain. More research is
needed.
B A C K G R O U N D
Low back pain (LBP) is the largest cause of workmen’s compensa-
tion in the USA and Canada. Sixty to 90% of the adult population
is at risk of developing LBP at some point in their lifetime (An-
dersson, 97, Coste, 89, Deyo, 87a, Skovron, 92). Of those who
develop acute LBP, 30% develop chronic LBP (Bowman, 91). LBP
has a significant impact on functional ability, restricting occupa-
tional activities with marked socio-economic repercussions (Van
Tulder, 99,Deyo, 87b).
The actual treatment for LBP is comprised of a number of dif-
ferent interventions such as drug therapy, surgery, physiotherapy,
and alternative therapies. The treatment goals are to relieve pain,
reduce muscle spasm, improve range of motion and strength and
ultimately improve functional status. The effectiveness and sever-
ity of adverse side effects of these treatments and physical ther-
apeutic modalities for LBP varies (Delitto, 93,Ottenbacher, 95,
Schlapbach, 91, Stratford, 93).
Transcutaneous electrical nerve stimulation (TENS) is a therapeu-
tic non-invasive modality mainly used for pain relief by electrically
stimulating peripheral nerves via skin surface electrodes (APTA,
93, Barr, 99). TENS was added more than 30 years ago to ex-
isting physical agents used in medicine and physiotherapy in the
treatment of LBP. The development and application of TENS was
based on the underlying Gate Theory conceptualised by Melzack
and Wall (Melzack and Wall, 82).
According to this theory, the TENS mechanism generates neuro-
regulatory peripheral and central effects (Coderre, 93,Han,
91,Janko, 80,Willer, 88) which modulate pain transmission
(Levin, 93,Fields,Melzack and Wall, 82). It was proposed that
by applying low intensity stimulation, the nervous system could
modify the perception of pain by counter-stimulating the large
diameter fibres (Melzack, 65).
Higher intensity of TENS are more likely effective to facilitate
these neuro-regulation and modulation (Langley, 84, Melzack,
75). However, several types of TENS applications, differing in in-
tensity and electrical characteristics, are used in clinical practice:
1) high frequency (40-150 Hz, 50-100usec pulse width, mod-
erate intensity); 2) low frequency (1-4 Hz, 100-400 usec pulse
width, high intensity); 3) burst frequency (1-4Hz with high inter-
nal frequency, 100-250 usec pulse width, high intensity) and 4)
hyperstimulation (1-4Hz, 10-500 msec pulse width, high inten-
sity) (Jette, 97).
A meta-analysis on the effect of TENS on various clinical con-
ditions showed that TENS has no effect on musculoskeletal pain
syndromes (Reeve, 96). However, this meta-analysis did not ex-
amine LBP alone. A more recent meta-analysis (Van Tulder, 99)
has led to the same conclusion. These authors (Van Tulder, 99)
did not restrict their inclusion criteria to placebo-controlled RCTs.
Furthermore, the Philadelphia Panel (2001a; 2001b) recommends
there is poor evidence to include or exclude TENS alone as an in-
tervention for chronic LBP. This EBCPG is in concordance with
the BMJ (BMJ, 99) recommendations. In contrast, the Québec
Task Force (Quebec Task Force) recommended TENS as a reha-
bilitation modality for symptomatic pain relief, but this recom-
mendation included other forms of electroanalgesia. Insufficient
information regarding adverse effects was reported by BMJ (BMJ,
99).
The aim of this systematic review was to determine the effec-
tiveness of TENS in the treatment of chronic LBP. A secondary
objective was to determine the most effective method of admin-
istering TENS for chronic LBP, including the optimal: 1) fre-
quency/intensity; 2) application techniques; 3) duration of treat-
ment; and 4) site of application.
O B J E C T I V E S
To determine the effectiveness of transcutaneous electrical nerve
stimulation (TENS) in the treatment of chronic low back pain.
C R I T E R I A F O R C O N S I D E R I N G
S T U D I E S F O R T H I S R E V I E W
Types of studies
Only randomized controlled trials (RCTs) with greater than 5
patients with LBP, per group, were eligible. This sample size limit
was applied based on clinical experience.
Types of participants
Only trials with outpatients aged 18 years and over with a diagnosis
of chronic (greater than 12 weeks) low back pain were included.
2Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Only patients with low back pain of musculoskeletal origin were
selected. Radicular signs were not excluded. Subacute low back
pain was excluded, defined as a population with pain duration
between 4 and 12 weeks.
Types of intervention
All modes of TENS, including acupuncture-like, were included
in this review. Sham TENS was considered an acceptable placebo
group. Articles were excluded if either the active or placebo
treatment groups received TENS treatment percutaneously with
acupuncture needles. Acupuncture, even as a sham, may have ef-
fects on pain, stiffness, and physical disability (Takeda and Wes-
sel,94).
Types of outcome measures
The outcome measures included for analysis were the ones that are
most likely to be used in physical therapy for LBP and published
in paper by the International Back Group (Deyo, 98): 1) Pain;
2) Functional (for example, measured by the Roland Disability
Scale); 3) Well being (Ex. patient global assessment); 4) Disability;
5) Disability -special (Ex. loss of work, sick days); 6) Satisfaction
with care.
S E A R C H S T R A T E G Y F O R
I D E N T I F I C A T I O N O F S T U D I E S
See: search strategy
We searched MEDLINE up to June 2000, EMBASE to June
2000, the Cochrane Controlled Trials Register (CCTR), Issue
2, 2000 and The Physiotherapy Evidence Database (PEDro)
up to June 2000. Details of the search strategy are given in
the appendix. The electronic search was complemented by
the following hand searches: 1) Bibliographic references; 2)
Current Contents up to week 21, 2000 (to identify articles
not yet indexed in Medline); 3) Abstracts published in special
issues of specialized journals or in Conference Proceedings were
also included; 4) Co-ordinating offices of the trials registries of
the Cochrane Field of Physical and Related Therapies and the
Cochrane Musculoskeletal Group were contacted.
Reference lists were hand-searched for further identification of
published work, presentations at scientific meetings and personal
communications. Content experts were contacted for additional
studies and unpublished data. If data could not be obtained,
abstracts were not used.
The sensitive search strategy for RCTs described by Haynes et
al (Haynes, 94) was used and combined with the following text
words and Mesh terms to identify TENS and low back pain:
TENS:
exp electric stimulation therapy/
((electric$ adj nerve) or therapy).tw.
electrostimulation.tw.
electroanalgesia.tw.
(tens or altens).tw.
electroacupuncture.tw.
(high volt or pulsed or current).tw.
(electromagnetic or electrotherap$).tw.
Back pain:
exp back/
exp back injuries/
exp back pain/
back.hw,tw.
(spine or spinal).tw.
sacrococcygeal.tw.
lumbar.tw.
sciatica/ or sciatic$.tw.
lumbosacral.tw.
cauda equina.hw,tw.
backache.tw.
M E T H O D S O F T H E R E V I E W
Two authors (L.B.,S.M.) independently selected the trials to be
included in the review and all articles selected by at least one of
the authors were retrieved for closer examination. These authors
were not blinded to the journal or authors. There was no cut-off
based on methodological quality or source of financial support.
From each included trial, we collected information regarding
the trial design, patient characteristics, dosages and treatment
duration, and baseline and end of study outcomes. Follow-up
data were included where possible. Data concerning details of
the study population, intervention and outcomes were extracted
independently by two authors (M.S., S.M., L.B.). Differences in
data extraction were resolved by referring back to the original
article and establishing consensus. A third author was consulted to
help resolve differences. Additional information was sought from
the authors of the primary studies, when incompletely reported in
the publications.
Data on the outcomes from each trial were pooled to arrive at an
overall estimate of the effectiveness of TENS. Where possible, the
analyses were based on intention-to-treat data from the individual
trials. In cases where trials reported outcomes as graphs, the mean
scores and standard deviations were estimated from these graphs.
Subgroup and sensitivity analyses were attempted to determine the
effects of the method of TENS administration, methodological
quality and treatment duration on outcomes.
For continuous data, results are presented as weighted mean
differences (WMD). However, where different scales were used
to measure the same outcome or concept, standardized mean
differences (SMD) were used. For dichotomous data, an odds ratio
(OR) was calculated (Petitti 94). The OR cannot be interpreted
as a relative risk because prevalence of the outcome studied is high
3Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

(Henneken, 87). A test for heterogeneity was calculated using a
Chi square test. Fixed effects models were used throughout, unless
statistical heterogeneity was significant, in which case, a random
effects model was used. Publication bias was not assessed due to
the small number of included studies.
D E S C R I P T I O N O F S T U D I E S
The literature search identified 61 articles. The specialized reg-
ister of the Cochrane Field of Physical and Related Therapies,
the Cochrane Musculoskeletal Group and handsearches of refer-
ence lists provided no additional references. Contact with experts
yielded one trial (Jarzem, 97). Of these, 21 were potentially rele-
vant trials, and five met the inclusion criteria. Ten trials were ex-
cluded due to lack of control group or randomisation or placebo
comparison. Five were excluded because the number of patients
with chronic low back pain was too small (< 10) or the patients
did not meet the inclusion criteria (Lehmann, 83, Lundeberg,
84b, Jeans, 79,Schuster, 80,Thorsteinsson, 78). Two trials were
excluded for an inappropriate treatment group (Hackett, 88, Mac-
donald, 95). One RCT published in abstract form only was in-
cluded (Jarzem, 97). Data from this trial were obtained from the
authors with the assistance of the Cochrane Back Group Editorial
Board.
Of the five RCTs of TENS for chronic low back pain, four reported
pain or pain relief as an outcome. Physical measures such as lumbar
flexion / extension or SLR were reported by 2 trials and disability
on the Roland scale was reported by two trials.
The mean age ranged from 36 to 52 years and the mean time from
onset of low back pain varied from 4 to 12 years. The schedule of
treatments varied greatly between studies ranging from one treat-
ment/day for two consecutive days, to three treatments/day for
four weeks. All trials included patients with chronic low back pain
of musculoskeletal origin, however, not all the trials described the
subgroups of specific diagnosis (Ex. neurologic signs, disc involve-
ment, radiculopathy).
M E T H O D O L O G I C A L Q U A L I T Y
The quality of the studies was assessed by two independent au-
thors (L.B., S.M.) using a validated five point scale (Jadad, 96),
which includes the appropriateness of randomization (2 points),
appropriateness of blinding (2 points), and description of dropouts
and withdrawals (1 point). Differences in scoring were resolved by
consensus. A third author (V.W.) was consulted when necessary.
Consensus was reached for all trials. Studies were divided into low
and high quality, based on the median quality score to examine
the effect of the quality on the difference between active treatment
and placebo groups.
The median methodological quality was 2, with a range from 2 to
5. Two trials scored full points for randomization, one scored full
points for double blinding, and three did not report withdrawals
and dropouts.
R E S U L T S
A total of 170 subjects were allocated to placebo groups receiv-
ing sham-TENS and 251 subjects received active TENS (153 for
conventional mode, 98 for acupuncture-like TENS).
There was no significant heterogeneity for any comparisons, indi-
cating that the difference between treated and control groups was
consistent across trials. For all of the outcome measures assessed,
no significant difference was found between the active treatment
and placebo control groups. Three studies measured pain using
a visual analogue scale (VAS) at the end of treatment, with a to-
tal of 171 subjects (89 active TENS, 82 placebo). There was a
trend towards greater pain reduction with the active TENS appli-
cation compared to the placebo, however, this difference was not
statistically significant (SMD: -0.207 [95% CI: -0.508 - 0,095]).
When converted to the original units of the VAS, this represents
a difference of 4mm on a 100mm scale. The relative difference
in percentage change from baseline for each trial with pain as an
outcome ranged from 11% to 38% (Table 01).
For the subgroup analysis regarding high versus low quality appli-
cations, there was no difference in the effect on pain or function.
There was also no difference in pain and function between high
and low frequency applications for the time points reported. Due
to the small number of trials, the remaining pre-planned subgroup
analyses ( treatment duration, type of TENS application) were not
conducted.
D I S C U S S I O N
The results of this meta-analysis suggest that TENS does not have
a clinically important benefit on pain in patients with chronic LBP.
A difference of 4mm on a 100mm VAS was obtained. Furthermore
no evidence of effect on other outcomes. There is poor evidence
to include TENS alone as an intervention for chronic LBP. De-
spite several RCTs of TENS, no consistent benefit was shown on
clinically relevant outcomes (Deyo, 90a; Gemignani, 91, Jarzem,
97, Marchand, 93,Moore, 97). Sub-group analyses revealed no
significant differences between low and high quality studies and
high vs low frequency.
These results are in concordance with previous systematic reviews
for chronic LBP (Reeve, 96,Van Tulder, 99). These results are
also in agreement with the Philadelphia Panel (2001) and BMJ
evidence-based clinical practice guidelines (EBCPGs) which do
not recommend TENS for chronic LBP, but in conflict with the
QTF (Quebec Task Force) CPGs which recommended TENS
4Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

for pain relief. However, the QTF did not differentiate between
electroanalgesia and TENS and was not based on a systematic
review.
Various methodological biases were potentially introduced in the
individual trials. A misclassification bias related to the LBP condi-
tion studied is present with the lack of precise medical and phys-
iotherapy diagnoses observed (Binkley, 93,Delitto, 93,Delitto A
95,Delitto A 95,Magistro, 93, Marras, 95,Zimny, 95). Selection
bias could have occurred with the presence of heterogeneity of
clinical characteristics such age, prevalent versus incident cases,
stages of the disease, level of pain and presence or absence of neu-
rological deficits. However, differences in disease duration were
minimized by excluding studies with a mix of acute and chronic
conditions or mixed diagnoses other than sciatalgia.
The quality of the included papers was acceptable but low (median
2).There was no difference in effect between high versus low qual-
ity studies. Randomization was rarely adequate (i.e. performed
using computerized random number lists). Insufficient informa-
tion was noted in several RCTs about the treatment assignment
procedure. Inappropriate blinding could also lead to information
bias. Blinding is an issue with physical rehabilitation interven-
tions. Complete blinding is difficult to achieve because of visual
and other sensory differences between the active treatment and the
placebo as well as through unintended communication between
the patient and evaluator (Deyo, 90a). A valid placebo for TENS
is difficult to achieve since TENS involves cutaneous stimulation.
It has been suggested that the effect of TENS is due to a placebo
effect since placebo TENS has been shown to relieve pain relative
to a control group receiving no therapy (Jensen, 85).Few investi-
gators reported adequate information regarding withdrawals and
loss to follow-up and failed to indicate if they were considered in
the data analysis.
Characteristics of the device parameters and of the therapeutic
application could also affect the treatment effect size. There is a
marked heterogeneity among included studies. In some articles
these parameters are not even reported (Gemignani, 91,Jarzem,
97). A theoretical framework for the application of TENS similar
to the one proposed by Morin et al. should be considered (Morin,
96).
Specific therapeutic application of TENS is of key importance. For
example, Guieu et al. (Guieu, 91) observed positive results when
using mechanical vibrations simultaneously with TENS. Vibra-
tory stimulation has been recommended as part of the TENS ap-
plication, especially for chronic pain relief (Guieu, 91,Lundeberg,
84b,Tardy-Gervet, 93). None of the trials included in our review
included or mentioned vibratory stimulation. There is a need for
strict and rigorous RCTs of TENS using combined vibratory stim-
ulation.
The neuro-regulatory peripheral and central effects (Coderre,
93,Han, 91,Janko, 80,Willer, 88) of the TENS are thought to
be more effective with higher intensity applications (Langley, 84
,Morin, 96) such as with the acupuncture-like application. This ef-
fect was not captured by our sub-analyses involving acupuncture-
like application compared to placebo. According to Levin, both
conventional and acupuncture-like TENS excite afferent fibers
in the A-alpha-beta range (Levin, 93). The plausible effect is ex-
plained by the activation of intrinsic pain-suppressive systems
(Cheng, 80,Sjolund, 85) and the concomitant release of opiate and
non-opiate neuro-regulators (Han, 91,Han and Terenius„Peets,
85,Sjolund, 79). This effect was not captured by our sub-analyses
involving acupuncture-like application compared to placebo. This
observation may be due to the fact that the effectiveness of the
TENS application, especially for LBP is also influenced by a
number of risk factors (Andersson) including biological (Biering-
Sorenson, 86), psychosocial (Bigos, 91,Bongers, 93, Strong, 94,
Venning, 87), occupational (Hagberg, 92,Hope, 99,Riihimäki,
89, Svensson, 83,Winkel, 94) health indicators. Unfortunately, it
was not possible to examine these risk factors.
The development and use of a theoretical framework to rationalize
TENS and also to provide uniformity in reporting the character-
istics of the device and the therapeutic application in clinical set-
tings and in scientific reports are imperative (Morin, 96,Rothstein,
95). The large variability in methodological quality reflects the
need for standardization of reporting and conducting clinical trials
in physiotherapy. Standardized measurement of outcomes is also
recommended to facilitate scientific advances in clinical care for
LBP (Deyo, 98,Delitto A. 94). More information on responsive-
ness and the minimally important change in scores is needed for
most of the instruments for LBP management (Deyo, 98, Strat-
ford, 94Stratford, 96). Little is known about valid and sensitive
outcome measures in LBP (Van Tulder, 99) and more psychomet-
ric studies are needed. These recommendations will contribute to
evidence-based practice (Helewa, 00).
The effectiveness of conservative treatment of LBP is a complex
issue (Van Tulder, 99, Erhard, 94). Physical rehabilitation is de-
fined as a combination of physical agents. Rehabilitation special-
ists often use concomitant treatment interventions in their daily
practice (Gam, 95). Each individual modality is usually an adjunct
therapy. Certain modalities such as thermotherapy and TENS are
used for pain relief or as a treatment preparation before the main
intervention. The use of single and specific interventions does not
reflect the complexity of the global approach adopted by rehabili-
tation specialists in real life clinical situations for the treatment of
chronic LBP.
The therapeutic application in daily practice of several concur-
rent rehabilitation interventions is based on empirical experience
(Gam, 95, Delitto, 93, Jette, 97) and the measurement of their
effects is complex (Delitto A. 94,Duckworth, 99). The practice
of rehabilitation requires a better theoretical basis (Delitto A. 94,
DeRosa, 92,Rothstein, 95, Morin, 96, Fritz, 98) and well-designed
controlled research (Schlapbach, 91).
5Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

In summary, this meta-analysis suggests that TENS is not effective
in reducing pain, improving functional status, increasing ROM
or activity in patients with chronic LBP. There is poor evidence to
include TENS alone as an intervention for chronic LBP. However,
there is no evidence regarding the effects in diagnostic subgroups
of LBP. Furthermore no evidence was found regarding the effects
of vibratory stimulation.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
The evidence from RCT’s does not support the use of TENS alone
in the treatment of chronic low back pain.
Implications for research
Further studies are needed to evaluate the efficacy of TENS com-
bined with vibratory stimulation in the treatment of low back
pain. These studies should report standardized, clinically relevant
outcome measures with special attention to the findings of this
meta-analysis regarding treatment application (Ex. low vs. high
frequency, type of applications or combined applications, treat-
ment duration, and site of application).
N O T E S
As of Issue 1, 2001, this current review by Milne et al replaces the
original review by Gadsby et al entitled, “ TENS and acupuncture-
like TENS for chronic low back pain” which was first published
Issue 2, 1997 and officially withdrawn Dec. 1999.
Any further questions may be directed to the Back Review Group
Coordinator @ [email protected]
P O T E N T I A L C O N F L I C T O F
I N T E R E S T
None known
A C K N O W L E D G E M E N T S
The authors wish to thank Jessie McGowan for her consultation
on the search strategy, Dr. Ghoname & Jarzem for providing data.
Thanks to Dr. Claire Bombardier and Andrea Furlan for assistance
obtaining unpublished data, and to Mathieu Nadeau for assisting
with data extraction.
S O U R C E S O F S U P P O R T
External sources of support
• CIGNA Foundation provided an educational grant USA
• Lucie Brosseau is an Ontario Ministry of Health & Long-Term
Care Career Scientist CANADA
Internal sources of support
• No sources of support supplied
R E F E R E N C E S
References to studies included in this review
Deyo, 90a {published data only}∗Deyo RA, Walsh NE, Martin DC, Schoenfield LS, Ramamurthy S.
A Controlled Trial of Transcutaneous Electrical Stimulation (TENS)
and Exercise for Chronic Low Back Pain. New England Journal of
Medicine, June 7, 1990;322(23):1627-1634.
Gemignani, 91 {published data only}∗Gemigniani G. Transcutaneous Electrical Nerve Stimulation in
Ankylosing Spondylitis: a Double-Blind Study. Arth Rheum 1991;34
(6):788-789.
Jarzem, 97 {published and unpublished data}∗Jarzem P, Harvey EJ, Arcaro N, Kazarowski J. Transcutaneous
Electrical Nerve Stimulation for Non-Acute Low Back Pain: A
Randomized Double-Blind Study of Conventional, Nu-Wavefor,
Acupuncture-Type and Sham Therapies. A Randomized Double-
Blind Study of Conventional, Nu-Wavefor, Acupuncture-Type and
Sham Therapies. American Academy of Orthopaedic Surgeons, 1997
Annual Meeting.
Marchand, 93 {published data only}∗Marchand S, Charest J, Li J, Chenard JR, Lavignolle B, Laurencelle
L. Is TENS Purely a Placebo Effect? - A Controlled Study on Chronic
Low Back Pain. Pain 1993;54:99-106.
Moore, 97 {published data only}∗Moore SR, Shurman J. Combined Neuromuscular Electrical Stim-
ulation and Transcutaneous Electrical Nerve Stimulation for Treat-
ment of Chronic Back Pain: A Double-Blind, Repeated Measures
Comparison. Arch Phys Med Rheabil 1997;78:55-60.
References to studies excluded from this review
Biedermann, 87
Biedermann HJ, McGhie A, Monga TN, Shanks GL. Perceived and
actual control in EMG treatment of back pain. Behaviour Research &
Therapy 1987;25(2):137-147.
Cheng, 87
. Cheng RSS, 1987 ???.
6Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Ghoname, 99
Ghoname EA, Craig WF, White PF, Ahmed HE, Hamza MA, Hen-
derson BN, Gajraj NM, Huber PJ, Gatchel RJ. Percutaneous Elec-
trical Nerve Stimulation for Low Back Pain. JAMA, March 3, 1999;
281(9):818-823.
Hackett, 88
Hackett GI, Seddon D, Kaminski D. Electroacupuncture compared
with paracetamol for acute low back pain. Practitioner 1988,Feb 22;
232(1443):163-164.
Hamza, 99
Hamza M, Ghoname E, White P, Craig W, Ahmed H, Gajraj N,
Vakharia A. Effect of the duration of Electrical Stimulation on the
Analgesic Response in Patients with Low Back Pain. Anesthesiology1999;91(6):1622-7.
Herman, 94
Herman E, Williams R, Stratford P, Fargas-Babjak A, Trott M. A Ran-
domized Controlled Trial of Transcutaneous Electrical Nerve Stimu-
lation (CODETRON) to determine its Benefits in a Rehabilitation
Program for Acute Occupational Low Back Pain. SPINE 1994;19
(5):561-568.
Jeans, 79
Jeans ME. Relief of Chronic Pain by Brief, Intense Transcutaneous
Electrical Stimulation - A Double-Blind Study. Advances in Pain Re-search and Therapy 1979;3:601-606.
Laitinen, 76
Laitinen J. Acupuncture and transcutaneous electric stimulation in
the treatment of chronic sacrolumbalgia and ischialgia. American
Journal of Chinese Medicine 1976 Summer;4(2):169-175.
Lehmann, 83
Lehmann TR, Russell DW, Spratt KF. The impact of patients with
nonorganic physical findings on a controlled trial of transcutaneous
electrical nerve stimulation and electroacupuncture. Spine 1983 Sep;
8(6):625-634.
Lundeberg, 84
Lundeberg T. A Comparative Study of the Pain Alleviating Effect
of Vibratory Stimulation, Transcutaneous Electrical Nerve Stimula-
tion, Electroacupuncture and Placebo. American Journal of Chinese
Medicine 1984;12:72-79.
Macdonald, 95
Macdonald AJR, Coates TW. The discovery of transcutaneous spinal
electroanalgesia and its relief of chronic pain. Physiotherapy 1995 Nov;
81(11):653-661.
Melzack, 80
Melzack R, Jeans ME, Stratford JG, Monks RC. Ice Massage and
Transcutaneous Electrical Stimulation: Comparison of Treatment for
Low-Back Pain. Pain 1980;9:209-217.
Melzack, 83
Melzack R, Vetere P, Finch L. Transcutaneous Electrical Nerve Stim-
ulation for Low Back Pain - A Comparison of TENS for Pain and
Range of Motion. Physical Therapy April 1983;63(4):489-493.
Schuster, 80
Schuster GD, Infante MC. Pain relief after low back surgery: the
efficacy of transcutaneous electrical nerve stimulation. Pain 1980 Jun;
8(3):299-302.
Sternbach, 76
Sternbach RA, Ignelzi RJ, Deems LM, Timmermans G. Transcuta-
neous Electrical Analgesia: A Follow-Up Analysis. Pain 1976;2:35-
41.
Stonnington, 76
Stonnington HH, Stillwell GK, Ebersold MJ, Thorsteinsson G, Laws
ER. Transcutaneous Electrical Stimulation for Chronic Pain Relief:
A Pilot Study. Minnesota Medicine 1976:A Pilot Study. Minnesota
Medicine 1976; 681-683.
Thorsteinsson, 78
Thorsteinsson G, Stonnington HH, Stillwell GK, Elveback LR. The
Placebo Effect of Transcutaneous Electrical Stimulation. Pain 1978;
5:31-41.
Additional references
Andersson, 97
Andersson GBJ: The epidemiology of spinal disorders. In: J.W. Fry-
moyer (Ed.), The adult spine:principles and practice. Second edition.
Raven Press, Ltd. 93-141.
APTA, 93
APTA Anthology: American Physical Therapy Association Anthol-
ogy: Electrical Stimulation: Management of Pain, Volume 2. Man-
agement of Pain, Volume 2. APTA, 1993.
Barr, 99
Barr JO. Transcutaneous Electrical Nerve Stimulation for pain man-
agement. In: Clinical electrotherapy, 3rd edition, Nelson RM, Hayes
KW, Currier DP eds, Appleton & Lange, 1999. Clinical electrother-
apy, 3rd edition, Nelson RM, Hayes KW, Currier DP eds, Appleton
& Lange, 1999. 291-354.
Biering-Sorenson, 86
Biering-Sorenson F, Thomsen C. Medical, social and occupational
history as risk indicators for low-back trouble in a general population.
Spine 1986;11(7):720-5.
Bigos, 91
Bigos SJ, Battie MC, Sprengler DM. A prospective study of work
perceptions and psychosocial factors affecting the report of back pain
injury. Spine 1991;16:1-6.
Binkley, 93
Binkley J, Finch E, Hall J, Black T, Gowland C. Diagnostic classifi-
cation of patients with low back pain: report on a survey of physical
therapy experts…. Physical Therapy 1993;73:138-55.
BMJ, 99
BMJ:. Issue 2 [British Medicine Journal Clinical Evidence: A Com-
pendium of the Best Available Evidence for Effective Health Care].
Bongers, 93
Bongers PM, deWinter CR, Konpier MAJ, Hildebrandt VH. Psy-
chosocial factors at work and musculoskeletal disease. Scandinavian
Journal of Work and Environmental Health 1993;19:297-312.
Bowman, 91
Bowman JM. The meaning of chronic Low Back Pain. 381-384,
1991.
Chapman, 91
Chapman C. E.: Can the use of physical modalities for pain control
be rationalized by the research evidence?. 704-712, 1991.
7Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
Cheng, 80
Cheng R, Pomeranz B. Electroacupuncture analgesia could be medi-
ated by at least two pain-relieving mechanisms: endorphin and non-
endorphin systems. 1957-1962, 1980.
Clark, 99
Clark HD, Wells GA, Huet C, McAlister FA, Salmi LR, Ferguson
D, Laupacis A. Assessing the quality of randomized trials: reliability
of the Jadad scale. Control Clin Trials. 1999;20(5):448-52.
Cochrane Library
Clarke M, Oxman AD, editors. Formulating the problem. Cochrane
Reviewers’ Handbook 4.0 [updated July 1999]; Section 4. In: Review
Manager (RevMan) [Computer program]. Version 4.0. Edition. Ox-
ford, England: The Cochrane Collaboration, 1999.
Coderre, 93
Coderre TJ, Katz J, Vaccarino AL, Melzack R. Contribution of cen-
tral neuroplasticity to pathological pain: review of clinical and exper-
imental evidence. Pain 1993;52:259-85.
Coste, 89
Coste J, Paolaggi JB. Revue critique de l’épidémiologie des lombal-
gies. Rev Epidemiol Santé Publique 1989;37:37:371-383.
Delitto 98
Delitto A. (1998). Clinicians and researchers who treat and study
patients with low back pain: are you listening?. 705-7.
Delitto A 95
Delitto A, Snyder-Mackler L. The diagnostic process: examples in
orthopaedic physical therapy. Physical Therapy 1995;75:203-11.
Delitto A. 94
Delitto A. Are measure of function and disability important in low
back care?. Physical Therapy 1994;74:452-62.
Delitto, 93
Delitto A, Cibulka MT, Erhard RE, Bowling RW, Tenhula JA. Ev-
idence for use of an extension-mobilization category in acute low
back syndrome: a prescriptive validation pilot study. Physical Therapy
1993;73:216-28.
DeRosa, 92
DeRosa CP, Porterfield JA. A physical therapy model for the treat-
ment of low back pain. Physical Therapy 1992;72:261-9.
Deyo, 87a
Deyo RA, Tsui-Wu YJ. Descriptive epidemiology of low-back pain
and its related medical care in the United States. Spine 1987a;12:
264-268.
Deyo, 87b
Deyo RA, Tsui-Wu YJ. Functional disability due to low-back pain.
Arthritis Rheumatism 1987b;30:1247-1253.
Deyo, 90b
Deyo RA, Wash NE, Schoenfeld LS, Ramamurthy S. Can trials of
physical treatments be blinded: the example of transcutaneous elec-
trical nerve stimulation for chronic pain. 6-10, 1990.
Deyo, 98
Deyo R, Battie M, Beurskens A, Bombardier C, Croft P, Koes B,
Malmivaara A, Roland M, Von Korff M, Waddell G. Outcome Mea-
sures for Low Back Pain Research. Spine 1998;23(18):2003-2013.
Duckworth, 99
Duckworth M. Outcome measurement selection and typology. Phys-
iotherapy 1999;85:21-6.
Erhard, 94
Erhard RE, Delitto A, Cibulka MT. Relative effectiveness of an exten-
sion program and a combined program of manipulation and flexion
and extension exercises in patients with acute low back syndrome.
Physical Therapy 1994;74:1093-100.
Fields
Fields HL, Basbaum AI. Endogenous pain control mechanisms. In
Well PD, Melsack R Eds. Textbook of pain. Edinburg, Scotland:
Churchill Livingstone, 198. Pg. Churchill Livingstone, 198. Pg. 142-
152.
Fritz, 98
Fritz H. Three-dimensional biomechanical model for simulating the
response of the human body to vibration stress. Med Biol Eng Comput.
1998;36(6):686-92.
Gam, 95
Gam AN, Johannsen F. Ultrasound therapy in musculoskeletal dis-
orders: a meta-analysis. Pain 1995;63:85-91.
Guieu, 91
Guieu R, Tardy-Gervet MF, Roll JP. Analgesic effects of vibration
and transcutaneous electrical nerve stimulation applied separately
and simultaneously to patients with chronic pain. 113-119, 1991.
Hagberg, 92
Hagberg M. Exposure variables in ergonomics epidemiology. Amer-
ican Journal of Industrial Medicine 1992;21:91-100.
Han and Terenius,
Han JS, TereniusL. Neurochemical basis of acupuncture analgesia.
193-220.
Han, 91
Han JS, Chen XH, Sun SL. Effect of low- and high frequency TENS
on metenkephalin-Arg-Phe and dynorphin: an immunoreactivity in
human lumbar CSF. 295-298, 1991.
Haynes, 94
Haynes RB, Wilczynski N, McKibbon KA, Walker CJ, Sinclair JC.
Developing optimal search strategies for detecting clinically sound
studies in MEDLINE. Journal of the American Medical InformaticsAssociation 1994;1(6):447-58.
Helewa, 00
Helewa A, Walker J. Saunders, editor.Critical Evaluation of research
in physical Rehabilitation. Walker J. Saunders, editor.Critical Eval-
uation of research in physical Rehabilitation. Philadelphia:2000.
Henneken, 87
Henneken, Buring CH. Epidemiology in Medicine. Boston: Little
Brown & Company, 1987.
Hope, 99
Hope P, Forshaw M. Assessment in psychological distress. Physiother-
apy 1999;85:563-70.
Jadad, 96
Jadad A, Moore A, Carrol Dea. Assessing the quality of randomized
trials: Is blinding necessary?. Controlled Clinical Trials 1996;17:1-12.
Janko, 80
Janko M, Trontelj JV. Transcuteneous electrical nerve stimulation: a
microneurographic and perceptual study. 219-230, 1980.
8Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Jensen, 85
Jensen JE, Conn RR, Hazelrigg G, Hewett JE. The use of transcuta-
neous neural stimulation and isokinetic testing in arthroscopic knee
surgery. American Journal of Sports Medicine 1985;13:27-33.
Jette 86
Jette DU: Effect of Different Forms of TENS on experimental pain.
187-192, 1986.
Jette, 97
Jette AM, Delitto A. Physical therapy treatment choices for muscu-
loskeletal impairments. Physical Therapy 1997;77:145-54.
Langley, 84
Langley GB, Sheppeard H, Johnson M. The analgesic effects of tran-
scutaneous electrical nerve stimulation and placebo in chronic pain
patients: A double blind non-crossover comparison. Rheumatol Int1984;4:119-123.
Levin, 93
Levin MF, Hui-Chan CWY. Conventional and acupuncture-like
transcutaneous electrical nerve stimulation excites similar afferent
fibers. Arch Physical Medicine and Rehabilitation 1993;74:54-60.
Lundeberg, 84b
Lundeberg T. Long-term results of vibratory stimulation as pain re-
lieving for chronic pain. 13-23, 1984.
Magistro, 93
Magistro C, Delitto A, Guccione AA, Jette A, Sahrmann S. Diagnosis
in physical therapy. PT–Magazine of Physical Therapy 1993;1:58-65.
Marras, 95
Marras WS, Parnianpour M, Ferguson SA, Kim JY, Crowell RR, Bose
S, Simon SR. The classification of anatomic- and symptom-based
low back disorders using motion measure models. Spine 1995 Dec
1;20(23):2531-46.
Mayer, 84
Mayer DJ, Watkins LR. Multiple endogenous opiate and non-opiate
analgesia systems. In: Kruger L, Liebeskind JC Eds. Advances in pain
research and therapy. New York, Raven Press 2, 1984. Kruger L,
Liebeskind JC Eds. Advances in pain research and therapy. New York,
Raven Press 2, 1984. 253-276.
Melzack and Wall, 82
Melzack R, Wall P.
Melzack, 65
Melzack R, Wall PD. Pain Mechanisms: a new theory. Science 1965;
150:971-9.
Melzack, 75
Melzack R. Prolonged relief of pain by brief, intense transcutaneous
somatic stimulation. 357-373, 1975.
Morin, 96
M Morin, L Brosseau, C Quirion-DeGrardi. A theoretical framework
on low level laser therapy (classes I, II and III) application for the
treatment of OA and RA. Proceedings of the Canadian PhysiotherapyAssociation National Congress 1996;1.
Ottenbacher, 95
Ottenbacher KJ. Why Rehabilitation Research Does Not Work (As
Well as we think it should). Arch Phys Med Rehabil 1995;76:123-129.
PEDro
PEDro: Physiotherapy Evidence Database. 2000 up-date. Aus-
tralian Physiotherapy Association, Cochrane Collaboration Re-
habilitation and related Field, School of Physiotherapy of the
University of Sydney (Australia) (http://ptwww.cchs.usyd.edu.
//ptwww.cchs.usyd.edu.au/pedro).
Peets, 85
Peets JM, Pomeranz B. Acupuncture-like transcutaneous electrical
nerve stimulation is influenced by spinal cord endorphins but not
serotonin: an intrathecal pharmacological study. In: Fields HL, Dub-
ner R, Cervero F Eds. Advances in Pain research and therapy. New
York, Raven 9, 1985. Pg. Fields HL, Dubner R, Cervero F Eds. Ad-
vances in Pain research and therapy. New York, Raven 9, 1985. Pg.
519-525.
Petitti 94
Petitti D. Meta-analysis, decision analysis, and cost-effectiveness analy-sis: methods for quantitative synthesis in medicine. New York: Oxford
University Press, 1994.
Quebec Task Force
Québec Task Force. Treatment of activity-related spinal disorders.
Treatment of activity-related spinal disorders.
Reeve, 96
Reeve J, Menon D, Corabian P: Transutaneous electrical nerve stim-
ulation (TENS): a technology assessment. 299-324, 1996.
Riihimäki, 89
Riihimäki H, Tola S, Videman T, Hanniken K. Low-back pain and
occupation: a cross-sectional questionnaire study of men in machine
operating, dynamic physical work. Spine 1989;14:204-9.
Rothstein, 95
Rothstein JM, Delitto A, Scalzitti DA. Understanding AHCPR clin-
ical practice guideline no 14: acute low back problems in adults.
PT—Magazine of Physical Therapy 1995;3:1-24.
Schlapbach, 91
Schlapbach, P, Gerber, NJ. In: Basel and Karger, editor(s). Physiother-apy: Controlled trials and facts. 1991.
Sjolund, 79
Sjolund BH, Eriksson MB. The influence of naloxone on analgesia
produced by peripheral conditioning stimulation. 295-301, 1979.
Sjolund, 85
Sjolund BH. Peripheral nerve stimulation suppression of C-fibre-
evoked flexion reflex in rats. 612-616, 1985.
Skovron, 92
Skovron ML. Epidemiology of low back pain. Baillieres Clinical
Rheumatologia 1992;6:559-573.
Stratford 99
Stratford PW. Who will decide the efficacy of physiotherapeutic in-
terventions?. 235-238, 1999.
Stratford, 93
Stratford P, Solomon P, Binkley J, Finch E, Gill C. Sensitivity of
Sickness Impact Profile items to measure change over time in a low-
back pain patient group. Spine 1993;18:1723-7.
Stratford, 94
Stratford PW, Binkley J, Solomon P, Gill C, Finch E. Assessing change
over time in patients with low back pain. Physical Therapy 1994;74:
528-33.
9Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Stratford, 96
Stratford PW, Binkley J, Solomon P, et al. Defining the minimum
level of detectable change for the Roland-Morris Questionnaire ….
Physical Therapy 1996;76:359-68.
Strong, 94
Strong J, Ashton R, Stewart A. Chronic low back pain: toward an
integrated psychosocial assessment model. Journal of Consultation and
Clinical Psychology 1994;62(5):1058-63.
Svensson, 83
Svensson HO, Andersson GBJ. Low back pain in 40 – to 47 – year
– old men: work history and work environment factors. Spine 1983;
6:272-6.
Takeda and Wessel,94
Takeda W, Wessel J. Acupuncture for the treatment of osteoarthritic
knee pain. Bull-Cancer-Paris 1994;7:118-22. [MedLine: 95244631].
Tardy-Gervet, 93
Tardy-Gervet MF, Guieu R, Ribot-Ciscar E, Roll JP. Les vibrations
mécaniques transcutanées : effets antalgiques et mécanismes antinoci-
ceptifs. Rev Neurol 1993;149(3):177-185.
Van der Heijden, 95
Van der Heijden GJMG, Beukskens AJHM, Koes BW, et al. The
efficacy of traction for back and neck pain: a systematic, blinded
review of randomized clinical trial methods. Physical Therapy 1995;
75(93):103.
Van Tulder, 99
Van Tulder MW, Koes BW, Assendelft WJJ, Bouter LM: The Effec-
tiveness of Conservative Treatment of Acute, Chronic Low Back Pain.
The Effectiveness of Conservative Treatment of Acute and Chronic
Low Back Pain. Amsterdam, EMGO Institute, 1999.
Venning, 87
Venning PJ, Walter SW, Stitt LW. Personal and job-related factors as
determinants of incidence of back injuries among nursing personal.
Journal of Occupational Medicine 29: 820-825. Journal of Occupa-tional Medicine 1987;29:820-5.
Willer, 88
Willer JC. Relieving effect of TENS on painful muscle contraction
produced by an impairment of reciprocal innervation: an electro-
physiological analysis. 271-274, 1988.
Winkel, 94
Winkel J, Mathiassen SE. Assessment of physical work load in epi-
demiologic studies: Concepts, issues and operational considerations.
Ergonomics 1994;37:979-88.
Zimny, 95
Zimny NJ, Goodman CC, Orest M, Delitto A, Snyder-Mackler
L. Physical therapy diagnosis… “The diagnostic process: examples
on orthopaedic physical therapy”. Physical Therapy 1995;75(March):
635-8.
∗Indicates the major publication for the study
T A B L E S
Characteristics of included studies
Study Deyo, 90a
Methods Randomized, double blind, parallel group
Sample size: total: 145, group 1: 36, group 2: 37, group 3: 36, group 4: 36
Treatment duration: 4 weeks
Follow up at 3 and 6 months
Participants Inclusion: low back pain > 3 months, with or without abnormal imaging or laboratory studies
Exclusion: history of cancer, use of corticosteriods / anticoagulant, maximal pain above T12, age > 70 yr or
< 18 yr, cardiac pace maker, known heart disease, severe coexisting disease, previous unevaluated neurologic
deficit, who can not be followed up, previous use of TENS, on disability compensation
Mean age: total: 51.4, group 1: 53.7, group 2: 53, group 3: 48.1, group 4: 50.6
Symptom duration: 4.1 yr
% females: total: 58, group 1: 58, group 2: 59, group 3: 58, group 4: 59
Patients completing: total: 125 at 4 weeks, 122 at 3 months, group 1: 31, group 2: 34, group 3: 31, group
4: 29
Compliance: 14%, 20 dropped out
%post surgery: total: 10, group 1: 19, group 2: 3, group 3: 10, group 4: 10
Disease: for most subjects there is no definitive diagnosis for low back pain
Interventions Group 1: TENS
Group 2: TENS + exercise ( 12 sequential exercises: 3 relaxation followed by 9 for flexibility for spine, hip,
lower extremities)
10Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Group 3: no exercise + sham TENS
Group 4: sham TENS + exercise
TENS device characteristics: Epix 982 units
Amplitude: conventional: 30, acupuncture like: 100
Pulse width: NA
Pulse frequency: conventional: 80-100, acupuncture like: 2-4
Stimulation mode: conventional high frequency, acupuncture like low frequency
Mode of stimulation: modulated-pulse-rate for all
Electrodes placement: over the area of most severe pain; in sciatica on leg and back
Total number of electrodes: 4; each 5.5 cm in diameter
Treated time per session: 45 mn
Schedule of treatment: 3 times / day
Total number of treatment sessions: 4 weeks
Concurrent treatments: hot packs, written and oral advice for lifting, standing, resting positions
Outcomes Functional status
Pain
Physical measures
Use of services
Wish to continue TENS therapy
Notes Quality: 5 (2,2,1)
Allocation concealment A
Study Gemignani, 91
Methods Double blind, placebo controlled, parallel group, single intervention
Sample size: total: 20
Treatment duration: 3 weeks
Participants Inclusion: Ankylosing Spondylitis (New York criteria), lumbar pain and sitffness > 1 month, NSAID not
sufficient for treatment
Interventions Group A: TENS
Group B: placebo
TENS device characteristics: Agopik A86
Amplitude: NA
Pulse with: NA
Pulse frequency: 5
Stimulation mode: NA
Single / Dual channel: NA
Size of the head: NA
Electrodes placement: on the skin, lower back, standard acupuncture points
Total number of electrodes: 4
Time per session: 20 min
Schedule of treatment: 3 weeks
Total number sessions: 10
Concurrent treatments: paracetamol 1 in group A, 5 in group B ; other NSAIDs were discontinued 1 week
before trial
Outcomes Pain
Stiffness
Analgesic pill count
Notes Quality: 2 (1,1,0)
Allocation concealment D
11Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of included studies (Continued )
Study Jarzem, 97
Methods Randomized, double blind, parallel group.
Sample size: total: 324; group 1: 83; group 2: 84; group 3: 78; group 4: 79.
Treatment duration: 28 days
Participants Inclusion: LBP
Mean age (SE): group 1: 47.3 (1.8); group 2: 45.4 (1.4); group 3: 43.1 (1.6); group 4: 44.4 (1.6).
Mean pain duration, yrs (SE): group 1: 10.1 (1.1); group 2: 9.0 (1.1); group 3: 9.4 (1.1); group 4: 12.2 (1.3).
% female : group 1: 51.8; group 2: 48.8; group 3: 43.6; group 4: 54.4.
Work missed, wks (SE): group 1: 16.5 (5.2); group 2: 22.1 (5.2); group 3: 13.5 (6.3); group 4: 30.3 (9.8)
Interventions Group 1: Sham-TENS
Group 2: TENS, conventional mode (ND)
Group 3: TENS, Acupuncture mode (ND)
Group 4: TENS, New-Wave mode (ND)
Outcomes McGill Activity (0-100)
McGill Work (0-100)
Disability (Roland)
ROM (Flexion / extension / SLR)
Isolift
Zung depression scale
Notes Quality: 2 (2,0,0)
Allocation concealment A
Study Marchand, 93
Methods Randomized, placebo controlled, single intervention
Sample size: total 42, group 1: 14, group 2: 12, group 3: 16
Treatment duration: 10 weeks
Follow-up: 6 months
Participants Inclusion: chronic pain > 6 months, complete medical work up, no relief from other appropiate therapy
Exclusion: Scoliosis > 15*, root compression and surgical indication, collapse of > 3 lumbar level, spondy-
lolisthesis > 1 cm, obesity > 20%, important psychological problems
Mean age: total: 36 (18-60), group 1: 35.46+/- 7.84, group 2: 35.08+/- 7.38, group 3: 37.25+/- 8.18
Symptom duration: total: 9 yr, group 1: 10.73+/- 7.08 yr, group 2: 8.83+/- 6.21, group 3: 6.51+/- 6.22
Males / Females: total: 20 / 22, group 1: 6/8, group 2: 6/6, group3: 8/8
Diseases: somatogenic pain, AS, RA, scoliosis < 15*, pyramidal syndrome
Interventions Group 1: TENS
Group 2: placebo TENS
Group 3: control, no treatment
TENS device characteristics: TENS 7720
Amplitude: low
Pulse with: 125 ms
Pulse frequency: 100
Stimulation mode: medtronic adjustable
Single / Dual channel: 2 channel
Size of the head: NA
Electrodes placement: dermatome of pain
Total number of electrodes: NA
Time per session: 30 mn
Schedule of treatment: 10 weeks
Total number session: 2 / week
Outcomes Pain intensity
12Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Pain unpleasantness
Notes Quality: 2 (1,1,0)
Allocation concealment B
Study Moore, 97
Methods Randomized, double blind, placebo-controlled trial, parallel group
Sample size: total : 28
Treatment duration : 2 days
Participants Inclusion: low back pain > 6 months, LBP unresponsive to previous treatments
Exclusion: cardiac pace maker, serious psychological disorder, previous TENS or NMES
Total mean age: 51.67 yr (26-80)
Mean symptom duration: 3.83 yr (2-10)
Males / Females: 8 / 16
Patients completing: 24, 4 men dropped out
Diseases: bulging disc 9, postlaminectomy 7, spinal stenosis 5, spondylothesis 1
Interventions Group 1: placebo, modified TENS unit, sham stimulation
Group 2: TENS
Group 3: NMES
Group 4: Combined NMES / TENS
TENS device characteristics: Amplitude: 0-60, Pulse with: 100
Pulse frequency: 100
Stimulation mode: conventional
Electrode placement: over the back where pain was most intense
Total number of electrodes: 4
NMES: 5 sec on, 15 sec off, pulse width: 200ms, frequency: 70 Hz, Amplitude: 0-100 mA
Treated time per session: 5 consecutives hours / day for 2 consecutive days with 2 days hiatus
Outcomes Present pain intensity scale
VAS-R
Pain relief
Notes Quality: 3 (1,1,1)
Allocation concealment B
Characteristics of excluded studies
Study Reason for exclusion
Biedermann, 87 Inappropriate control groups
Cheng, 87 Not compared to placebo (acupuncture)
Ghoname, 99 No control group (percutaneous stimulation)
Hackett, 88 Electroacupuncture, not TENS
Hamza, 99 No appropriate control group (TENS vs. percutaneous stimulation)
Herman, 94 No appropriate control group (TENS + exercise vs. exercise)
Jeans, 79 Only 6 patients with LBP
Laitinen, 76 No appropriate control group (TENS vs. acupuncture)
Lehmann, 83 inpatients
Lundeberg, 84 Only myalgia patients
13Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Characteristics of excluded studies (Continued )
Macdonald, 95 Superficial acupuncture
Melzack, 80 No appropriate control group (TENS vs. ice massage)
Melzack, 83 No appropriate control group (TENS vs. massage)
Schuster, 80 inpatients
Sternbach, 76 Not randomized
Stonnington, 76 No appropriate control group (TENS vs.)
Thorsteinsson, 78 Could not separate LBP patients from other diagnoses.
A D D I T I O N A L T A B L E S
Table 01. Clinical Relevance
Study
Treatment
Group
Oucome,
Scale # of pt.’s
Baseline
Mean
End of Study
Mean
Absolute
Difference
Absolute
Difference%
Deyo 90 TENS Pain, VAS 65 39.9 21.7 -4.30 -11%
Placebo 60 37.9 24.0
Gemignagi 91 TENS Pain, VAS 10 57.1 35.6 -15.80 -38%
Placebo 10 47.6 41.9
Marchand 93 TENS Pain, VAS 14 33 13.3 -12.10 -37%
Placebo 12 32 24.4
G R A P H S
Comparison 01. TENS vs Placebo, end of treatment (2 days)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Pain, continuous, patient-
assessed
Weighted Mean Difference (Fixed) 95% CI Subtotals only
Comparison 02. TENS vs Placebo, end of treatment (approx 1 month)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Pain, continuous, patient-
assessed
Weighted Mean Difference (Fixed) 95% CI Subtotals only
02 Pain Improvement, VAS
(0-100)
1 125 Weighted Mean Difference (Fixed) 95% CI 5.20 [-6.55, 16.95]
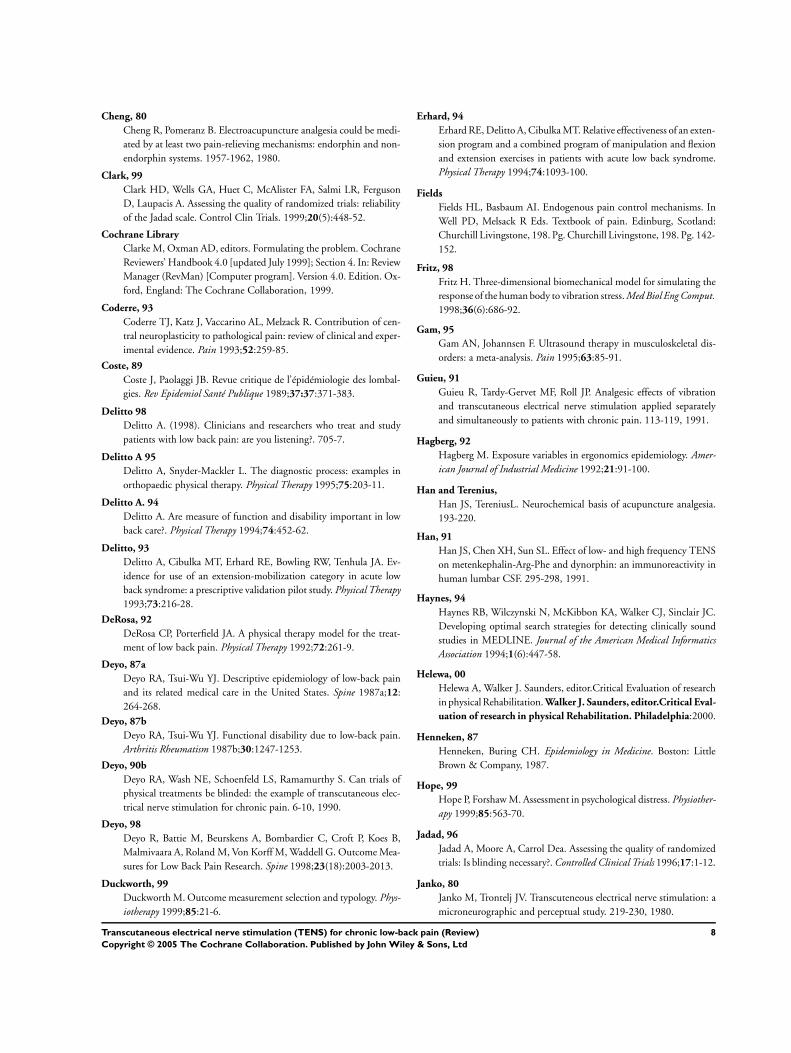
03 Pain frequency (1 - 5, 1 = never,
5 = all the time)
1 125 Weighted Mean Difference (Fixed) 95% CI -0.10 [-0.50, 0.30]
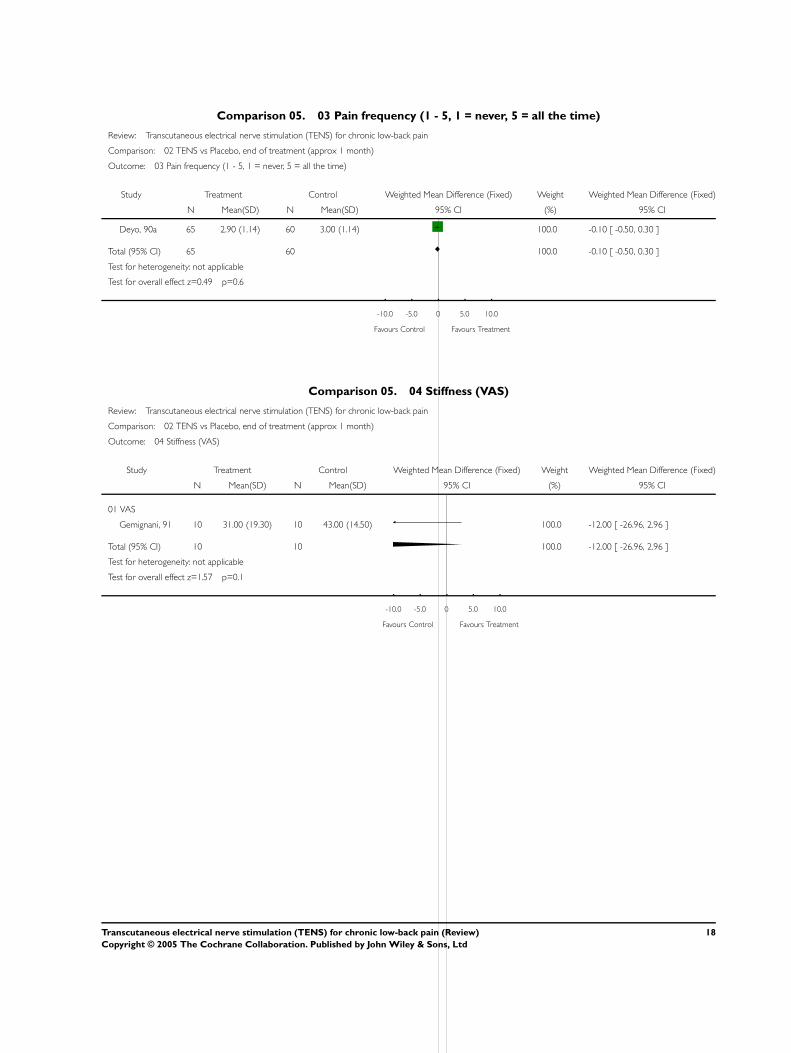
04 Stiffness (VAS) 1 20 Weighted Mean Difference (Fixed) 95% CI -12.00 [-26.96,
2.96]
05 Flexion ROM 3 417 Weighted Mean Difference (Fixed) 95% CI 0.10 [-0.27, 0.46]
06 Extension (degrees) 1 167 Weighted Mean Difference (Fixed) 95% CI 1.80 [-0.28, 3.88]
07 Function (Change from
baseline)
2 292 Weighted Mean Difference (Fixed) 95% CI -0.18 [-1.39, 1.03]
08 Self-Rated Activity Level 2 292 Weighted Mean Difference (Fixed) 95% CI 0.00 [-0.20, 0.20]
14Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

09 Use of services 2 250 Weighted Mean Difference (Fixed) 95% CI -0.08 [-0.22, 0.06]
10 Patient Satisfaction 1 128 Odds Ratio (Fixed) 95% CI 0.71 [0.35, 1.45]
11 McGill Work 1 167 Weighted Mean Difference (Fixed) 95% CI -1.00 [-3.23, 1.23]
12 Lasegue’s SLR (degrees) 1 125 Weighted Mean Difference (Fixed) 95% CI 0.00 [-2.70, 2.70]
13 SLR (degrees) 2 334 Weighted Mean Difference (Fixed) 95% CI 0.80 [-2.84, 4.44]
Comparison 03. TENS vs Placebo, Follow up (3 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Pain, continuous, patient-
assessed
Weighted Mean Difference (Fixed) 95% CI Subtotals only
Comparison 04. TENS vs Placebo, Follow up (6 months)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Pain, continuous, patient-
assessed
Weighted Mean Difference (Fixed) 95% CI Subtotals only
Comparison 05. TENS- High Quality vs. Low Quality, End of Treatment (1 month)
Outcome titleNo. of
studies
No. of
participants Statistical method Effect size
01 Pain, continuous, patient
assessed
3 171 Weighted Mean Difference (Fixed) 95% CI -4.32 [-10.36, 1.72]
02 Disability 2 292 Weighted Mean Difference (Fixed) 95% CI -0.18 [-1.39, 1.03]
I N D E X T E R M S
Medical Subject Headings (MeSH)
Chronic Disease; Low Back Pain [∗therapy]; Randomized Controlled Trials; ∗Transcutaneous Electric Nerve Stimulation
MeSH check words
Humans
C O V E R S H E E T
Title Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Authors Milne S, Welch V, Brosseau L, Saginur M, Shea B, Tugwell P, Wells G
Contribution of author(s) Sarah Milne, Michael Saginur, Bev Shea, Vivian Welch selected trials and extracted data.
Sarah Milne, Lucie Brosseau and Vivian Welch are responsible for the results and interpre-
tation of data.
George Wells provided statistical consultation.
Peter Tugwell was involved in the clinical interpretation of results.
Issue protocol first published 1998/1
Review first published 2001/2
Date of most recent amendment 23 February 2005
Date of most recent
SUBSTANTIVE amendment
03 August 2000
15Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

What’s New Information not supplied by author
Date new studies sought but
none found
Information not supplied by author
Date new studies found but not
yet included/excluded
Information not supplied by author
Date new studies found and
included/excluded
30 June 2000
Date authors’ conclusions
section amended
Information not supplied by author
DOI 10.1002/14651858.CD003008
Cochrane Library number CD003008
Editorial group Cochrane Back Group
Editorial group code HM-BACK
G R A P H S A N D O T H E R T A B L E S
Comparison 05. 01 Pain, continuous, patient-assessed
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 01 TENS vs Placebo, end of treatment (2 days)
Outcome: 01 Pain, continuous, patient-assessed
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 relief
Moore, 97 24 40.58 (27.55) 24 44.81 (30.67) 100.0 -4.23 [ -20.72, 12.26 ]
Subtotal (95% CI) 24 24 100.0 -4.23 [ -20.72, 12.26 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.50 p=0.6
02 mean reduction in intensity, VAS
Moore, 97 24 -5.55 (5.78) 24 -5.83 (7.48) 100.0 0.28 [ -3.50, 4.06 ]
Subtotal (95% CI) 24 24 100.0 0.28 [ -3.50, 4.06 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.15 p=0.9
04 McGill Pain Questionnaire: Present Pain Intensity *
Moore, 97 24 2.27 (1.13) 24 2.42 (1.15) 100.0 -0.15 [ -0.80, 0.50 ]
Subtotal (95% CI) 24 24 100.0 -0.15 [ -0.80, 0.50 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.46 p=0.6
-10.0 -5.0 0 5.0 10.0
Favours Treatment Favours Control
16Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 01 Pain, continuous, patient-assessed
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 01 Pain, continuous, patient-assessed
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 VAS (0-100)
Deyo, 90a 65 21.70 (20.66) 60 24.00 (20.66) 69.5 -2.30 [ -9.55, 4.95 ]
Gemignani, 91 10 35.60 (20.50) 10 41.90 (16.30) 13.9 -6.30 [ -22.53, 9.93 ]
Marchand, 93 14 13.30 (8.30) 12 24.40 (25.00) 16.7 -11.10 [ -25.90, 3.70 ]
Subtotal (95% CI) 89 82 100.0 -4.32 [ -10.36, 1.72 ]
Test for heterogeneity chi-square=1.16 df=2 p=0.56 I =0.0%
Test for overall effect z=1.40 p=0.2
02 Unpleasantness
Marchand, 93 14 11.11 (8.35) 12 22.20 (23.00) 100.0 -11.09 [ -24.82, 2.64 ]
Subtotal (95% CI) 14 12 100.0 -11.09 [ -24.82, 2.64 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.58 p=0.1
03 Self-rated improvent (1-6)
Deyo, 90a 65 2.90 (1.04) 60 2.90 (1.04) 100.0 0.00 [ -0.36, 0.36 ]
Subtotal (95% CI) 65 60 100.0 0.00 [ -0.36, 0.36 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.00 p=1
-10.0 -5.0 0 5.0 10.0
Favours Treatment Favours Control
Comparison 05. 02 Pain Improvement, VAS (0-100)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 02 Pain Improvement, VAS (0-100)
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Deyo, 90a 65 47.00 (33.49) 60 41.80 (33.49) 100.0 5.20 [ -6.55, 16.95 ]
Total (95% CI) 65 60 100.0 5.20 [ -6.55, 16.95 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.87 p=0.4
-10.0 -5.0 0 5.0 10.0
Favours Treatment Favours Control
17Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd
Comparison 05. 03 Pain frequency (1 - 5, 1 = never, 5 = all the time)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 03 Pain frequency (1 - 5, 1 = never, 5 = all the time)
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Deyo, 90a 65 2.90 (1.14) 60 3.00 (1.14) 100.0 -0.10 [ -0.50, 0.30 ]
Total (95% CI) 65 60 100.0 -0.10 [ -0.50, 0.30 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.49 p=0.6
-10.0 -5.0 0 5.0 10.0
Favours Control Favours Treatment
Comparison 05. 04 Stiffness (VAS)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 04 Stiffness (VAS)
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 VAS
Gemignani, 91 10 31.00 (19.30) 10 43.00 (14.50) 100.0 -12.00 [ -26.96, 2.96 ]
Total (95% CI) 10 10 100.0 -12.00 [ -26.96, 2.96 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.57 p=0.1
-10.0 -5.0 0 5.0 10.0
Favours Control Favours Treatment
18Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 05 Flexion ROM
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 05 Flexion ROM
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 finger-to-floor
Deyo, 90a 65 8.70 (7.27) 60 8.70 (7.27) 2.0 0.00 [ -2.55, 2.55 ]
Subtotal (95% CI) 65 60 2.0 0.00 [ -2.55, 2.55 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.00 p=1
02 Schober test (cm)
Deyo, 90a 65 4.20 (1.05) 60 4.10 (1.05) 97.6 0.10 [ -0.27, 0.47 ]
Subtotal (95% CI) 65 60 97.6 0.10 [ -0.27, 0.47 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.53 p=0.6
03 degrees
Jarzem, 97 84 3.00 (19.20) 83 3.30 (19.10) 0.4 -0.30 [ -6.11, 5.51 ]
Subtotal (95% CI) 84 83 0.4 -0.30 [ -6.11, 5.51 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.10 p=0.9
Total (95% CI) 214 203 100.0 0.10 [ -0.27, 0.46 ]
Test for heterogeneity chi-square=0.02 df=2 p=0.99 I =0.0%
Test for overall effect z=0.52 p=0.6
-10.0 -5.0 0 5.0 10.0
Favours Control Favours Treatment
Comparison 05. 06 Extension (degrees)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 06 Extension (degrees)
Study TENS Placebo Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Jarzem, 97 84 2.40 (7.30) 83 0.60 (6.40) 100.0 1.80 [ -0.28, 3.88 ]
Total (95% CI) 84 83 100.0 1.80 [ -0.28, 3.88 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.69 p=0.09
-10.0 -5.0 0 5.0 10.0
19Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 07 Function (Change from baseline)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 07 Function (Change from baseline)
Study treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Scales (SIP % Roland Disability)
Deyo, 90a 65 -5.70 (4.99) 60 -6.20 (4.99) 47.6 0.50 [ -1.25, 2.25 ]
Jarzem, 97 84 -1.40 (5.50) 83 -0.60 (5.50) 52.4 -0.80 [ -2.47, 0.87 ]
Total (95% CI) 149 143 100.0 -0.18 [ -1.39, 1.03 ]
Test for heterogeneity chi-square=1.11 df=1 p=0.29 I =9.9%
Test for overall effect z=0.29 p=0.8
-10.0 -5.0 0 5.0 10.0
Favours Treatment Favours Control
Comparison 05. 08 Self-Rated Activity Level
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 08 Self-Rated Activity Level
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
03 Scale (SIP Activity Level, McGill Activity)
Deyo, 90a 65 1.70 (0.57) 60 1.70 (0.57) 99.9 0.00 [ -0.20, 0.20 ]
Jarzem, 97 84 5.80 (22.90) 83 2.20 (21.00) 0.1 3.60 [ -3.06, 10.26 ]
Total (95% CI) 149 143 100.0 0.00 [ -0.20, 0.20 ]
Test for heterogeneity chi-square=1.12 df=1 p=0.29 I =10.8%
Test for overall effect z=0.03 p=1
-10.0 -5.0 0 5.0 10.0
Favours Control Favours Treatment
20Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 09 Use of services
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 09 Use of services
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 days in hospital
x Deyo, 90a 65 0.00 (0.00) 60 0.00 (0.00) 0.0 Not estimable
Subtotal (95% CI) 65 60 0.0 Not estimable
Test for heterogeneity: not applicable
Test for overall effect: not applicable
02 visits to other providers
Deyo, 90a 65 0.22 (0.40) 60 0.30 (0.40) 100.0 -0.08 [ -0.22, 0.06 ]
Subtotal (95% CI) 65 60 100.0 -0.08 [ -0.22, 0.06 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.12 p=0.3
Total (95% CI) 130 120 100.0 -0.08 [ -0.22, 0.06 ]
Test for heterogeneity: not applicable
Test for overall effect z=1.12 p=0.3
-10.0 -5.0 0 5.0 10.0
Favours Control Favours Treatment
Comparison 05. 10 Patient Satisfaction
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 10 Patient Satisfaction
Study Treatment Control Odds Ratio (Fixed) Weight Odds Ratio (Fixed)
n/N n/N 95% CI (%) 95% CI
Deyo, 90a 34/60 44/68 100.0 0.71 [ 0.35, 1.45 ]
Total (95% CI) 60 68 100.0 0.71 [ 0.35, 1.45 ]
Total events: 34 (Treatment), 44 (Control)
Test for heterogeneity: not applicable
Test for overall effect z=0.93 p=0.4
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours control
21Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 11 McGill Work
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 11 McGill Work
Study Tens Placebo Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Jarzem, 97 84 -0.90 (8.20) 83 0.10 (6.40) 100.0 -1.00 [ -3.23, 1.23 ]
Total (95% CI) 84 83 100.0 -1.00 [ -3.23, 1.23 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.88 p=0.4
-10.0 -5.0 0 5.0 10.0
Comparison 05. 12 Lasegue’s SLR (degrees)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 12 Lasegue’s SLR (degrees)
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
Deyo, 90a 65 84.00 (7.69) 60 84.00 (7.69) 100.0 0.00 [ -2.70, 2.70 ]
Total (95% CI) 65 60 100.0 0.00 [ -2.70, 2.70 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.00 p=1
-10.0 -5.0 0 5.0 10.0
Favours Control Favours Treatment
22Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 13 SLR (degrees)
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 02 TENS vs Placebo, end of treatment (approx 1 month)
Outcome: 13 SLR (degrees)
Study TENS Placebo Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 Right leg
Jarzem, 97 84 -0.30 (17.40) 83 -1.50 (16.40) 50.4 1.20 [ -3.93, 6.33 ]
Subtotal (95% CI) 84 83 50.4 1.20 [ -3.93, 6.33 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.46 p=0.6
02 Left leg
Jarzem, 97 84 -0.90 (19.20) 83 -1.30 (14.60) 49.6 0.40 [ -4.77, 5.57 ]
Subtotal (95% CI) 84 83 49.6 0.40 [ -4.77, 5.57 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.15 p=0.9
Total (95% CI) 168 166 100.0 0.80 [ -2.84, 4.44 ]
Test for heterogeneity chi-square=0.05 df=1 p=0.83 I =0.0%
Test for overall effect z=0.43 p=0.7
-10.0 -5.0 0 5.0 10.0
Comparison 05. 01 Pain, continuous, patient-assessed
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 03 TENS vs Placebo, Follow up (3 months)
Outcome: 01 Pain, continuous, patient-assessed
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 VAS (0-100)
Marchand, 93 14 21.40 (26.70) 12 25.70 (24.70) 100.0 -4.30 [ -24.07, 15.47 ]
Subtotal (95% CI) 14 12 100.0 -4.30 [ -24.07, 15.47 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.43 p=0.7
02 Unpleasantness
Marchand, 93 14 20.00 (26.70) 12 21.40 (24.70) 100.0 -1.40 [ -21.17, 18.37 ]
Subtotal (95% CI) 14 12 100.0 -1.40 [ -21.17, 18.37 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.14 p=0.9
-10.0 -5.0 0 5.0 10.0
Favours Treatment Favours Control
23Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 01 Pain, continuous, patient-assessed
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 04 TENS vs Placebo, Follow up (6 months)
Outcome: 01 Pain, continuous, patient-assessed
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 VAS (0-100)
Marchand, 93 14 15.70 (24.00) 12 24.20 (22.30) 100.0 -8.50 [ -26.31, 9.31 ]
Subtotal (95% CI) 14 12 100.0 -8.50 [ -26.31, 9.31 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.94 p=0.3
02 Unpleasantness
Marchand, 93 14 14.30 (24.00) 12 22.10 (22.30) 100.0 -7.80 [ -25.61, 10.01 ]
Subtotal (95% CI) 14 12 100.0 -7.80 [ -25.61, 10.01 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.86 p=0.4
-10.0 -5.0 0 5.0 10.0
Favours Treatment Favours Control
Comparison 05. 01 Pain, continuous, patient assessed
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 05 TENS- High Quality vs. Low Quality, End of Treatment (1 month)
Outcome: 01 Pain, continuous, patient assessed
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 High Quality (>2, median quality)
Deyo, 90a 65 21.70 (20.66) 60 24.00 (20.66) 69.5 -2.30 [ -9.55, 4.95 ]
Subtotal (95% CI) 65 60 69.5 -2.30 [ -9.55, 4.95 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.62 p=0.5
02 Low Quality (2 or less)
Gemignani, 91 10 35.60 (20.50) 10 41.90 (16.30) 13.9 -6.30 [ -22.53, 9.93 ]
Marchand, 93 14 13.30 (8.30) 12 24.40 (25.00) 16.7 -11.10 [ -25.90, 3.70 ]
Subtotal (95% CI) 24 22 30.5 -8.92 [ -19.86, 2.01 ]
Test for heterogeneity chi-square=0.18 df=1 p=0.67 I =0.0%
Test for overall effect z=1.60 p=0.1
Total (95% CI) 89 82 100.0 -4.32 [ -10.36, 1.72 ]
Test for heterogeneity chi-square=1.16 df=2 p=0.56 I =0.0%
Test for overall effect z=1.40 p=0.2
-10.0 -5.0 0 5.0 10.0
Favours treatment Favours control
24Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd

Comparison 05. 02 Disability
Review: Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain
Comparison: 05 TENS- High Quality vs. Low Quality, End of Treatment (1 month)
Outcome: 02 Disability
Study Treatment Control Weighted Mean Difference (Fixed) Weight Weighted Mean Difference (Fixed)
N Mean(SD) N Mean(SD) 95% CI (%) 95% CI
01 High Quality (>2, median quality)
Deyo, 90a 65 -5.70 (4.99) 60 -6.20 (4.99) 47.6 0.50 [ -1.25, 2.25 ]
Subtotal (95% CI) 65 60 47.6 0.50 [ -1.25, 2.25 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.56 p=0.6
02 Low Quality (2 or less)
Jarzem, 97 84 -1.40 (5.50) 83 -0.60 (5.50) 52.4 -0.80 [ -2.47, 0.87 ]
Subtotal (95% CI) 84 83 52.4 -0.80 [ -2.47, 0.87 ]
Test for heterogeneity: not applicable
Test for overall effect z=0.94 p=0.3
Total (95% CI) 149 143 100.0 -0.18 [ -1.39, 1.03 ]
Test for heterogeneity chi-square=1.11 df=1 p=0.29 I =9.9%
Test for overall effect z=0.29 p=0.8
-10.0 -5.0 0 5.0 10.0
Favours treatment Favours control
25Transcutaneous electrical nerve stimulation (TENS) for chronic low-back pain (Review)
Copyright © 2005 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd