cochrane database of systematic reviews (reviews) || injection therapy for subacute and chronic...
TRANSCRIPT

Injection therapy for subacute and chronic low-back pain
(Review)
Staal JB, de Bie R, de Vet HCW, Hildebrandt J, Nelemans P
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library
2011, Issue 2
http://www.thecochranelibrary.com
Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
2BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
10DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
12REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
15CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
39DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 epidural corticosteroids versus placebo injections, Outcome 1 Percentage improved over 1 to 3
months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 40
Analysis 1.2. Comparison 1 epidural corticosteroids versus placebo injections, Outcome 2 Percentage pain relief over 3 to 5
weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Analysis 2.1. Comparison 2 epidural corticosteroid injections versus other treatments, Outcome 1 General improvement at
2 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 41
Analysis 3.1. Comparison 3 Facet joint injections with corticosteroids versus placebo injections, Outcome 1 Self-rated
improvement at 1 month. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Analysis 3.2. Comparison 3 Facet joint injections with corticosteroids versus placebo injections, Outcome 2 Self rated
improvement at 6 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42
Analysis 4.1. Comparison 4 Facet joint injections with corticosteroids versus other injections, Outcome 1 Improvement in
pain severity at 1 month. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Analysis 4.2. Comparison 4 Facet joint injections with corticosteroids versus other injections, Outcome 2 Improvement in
pain severity at 3 months. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43
Analysis 5.1. Comparison 5 Facet joint injections with local anaesthetics versus other injections, Outcome 1 Pain reduction
post-treatment in positive group (VAS) (facet joint assumed to be the primary source of pain). . . . . . . 44
Analysis 6.1. Comparison 6 Local injections with corticosteroids versus placebo injections, Outcome 1 Self-reported
improvement at 2 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 44
Analysis 6.2. Comparison 6 Local injections with corticosteroids versus placebo injections, Outcome 2 Self-reported
improvement posttreatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Analysis 7.1. Comparison 7 Local injections with anaesthetics versus placebo injections, Outcome 1 Pain intensity at 2
weeks (VAS). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 45
Analysis 7.2. Comparison 7 Local injections with anaesthetics versus placebo injections, Outcome 2 Self-reported
improvement at 2 weeks. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 46
46ADDITIONAL TABLES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
48APPENDICES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
49WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
49HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
50CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
50DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
51INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iInjection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
[Intervention Review]
Injection therapy for subacute and chronic low-back pain
J Bart Staal1, Rob de Bie2, Henrica CW de Vet3, Jan Hildebrandt4, Patty Nelemans5
1Institute for Quality of Health Care (IQ health care), Radboud University Nijmegen Medical Center, Nijmegen, Netherlands.2Department of Epidemiology, Maastricht University, Maastricht, Netherlands. 3Department of Epidemiology and Biostatistics,
EMGO Institute for Health and Care Research, VU University Medical Center, Amsterdam, Netherlands. 4University Medicine Goet-
tingen, Goettingen, Germany. 5Epidemiology, University of Maastricht, Maastricht, Netherlands
Contact address: J Bart Staal, Institute for Quality of Health Care (IQ health care), Radboud University Nijmegen Medical Center,
PO Box 9101, Nijmegen, 6500 HB, Netherlands. [email protected].
Editorial group: Cochrane Back Group.
Publication status and date: Edited (no change to conclusions), published in Issue 2, 2011.
Review content assessed as up-to-date: 29 March 2007.
Citation: Staal JB, de Bie R, de Vet HCW, Hildebrandt J, Nelemans P. Injection therapy for subacute and chronic low-back pain.
Cochrane Database of Systematic Reviews 2008, Issue 3. Art. No.: CD001824. DOI: 10.1002/14651858.CD001824.pub3.
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
A B S T R A C T
Background
The effectiveness of injection therapy for low-back pain is still debatable. Heterogeneity of target tissue, pharmacological agent and
dosage generally found in randomized controlled trials (RCTs) points to the need for clinically valid comparisons in a literature synthesis.
Objectives
To determine if injection therapy is more effective than placebo or other treatments for patients with subacute or chronic low-back
pain.
Search methods
We updated the search of the earlier systematic review and searched the Cochrane Central Register of Controlled Trials, MEDLINE
and EMBASE databases from January 1999 to March 2007 for relevant trials reported in English, French, German, Dutch and Nordic
languages. We also screened references from trials identified.
Selection criteria
RCTs on the effects of injection therapy involving epidural, facet or local sites for subacute or chronic low-back pain were included.
Studies which compared the effects of intradiscal injections, prolotherapy or Ozone therapy with other treatments, were excluded unless
injection therapy with another pharmaceutical agent (no placebo treatment) was part of one of the treatment arms. Studies about
injections in sacroiliac joints and studies evaluating the effects of epidural steroids for radicular pain were also excluded.
Data collection and analysis
Two review authors independently assessed the quality of the trials. If study data were clinically and statistically too heterogeneous to
perform a meta-analysis, we used a best evidence synthesis to summarize the results. The evidence was classified into five levels (strong,
moderate, limited, conflicting or no evidence), taking into account the methodological quality of the studies.
1Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Main results
18 trials (1179 participants) were included in this updated review. The injection sites varied from epidural sites and facet joints (i.e.
intra-articular injections, peri-articular injections and nerve blocks) to local sites (i.e. tender- and trigger points). The drugs that were
studied consisted of corticosteroids, local anesthetics and a variety of other drugs. The methodological quality of the trials was limited
with 10 out of 18 trials rated as having a high methodological quality. Statistical pooling was not possible due to clinical heterogeneity
in the trials. Overall, the results indicated that there is no strong evidence for or against the use of any type of injection therapy.
Authors’ conclusions
There is insufficient evidence to support the use of injection therapy in subacute and chronic low-back pain. However, it cannot be
ruled out that specific subgroups of patients may respond to a specific type of injection therapy.
P L A I N L A N G U A G E S U M M A R Y
Injection therapy for subacute and chronic low-back pain
Injection therapy is one of many treatments available for patients with subacute (longer than six weeks) and chronic (longer than 12
weeks) low-back pain. Where the injection is given, what drug is used and why the injection is given can all vary.
The injection can be given into different parts of the spine (the space between the vertebrae, around the nerve roots, or into the disc),
ligaments, muscles or trigger points (spots in the muscles that when pressed firmly will produce pain). Drugs that reduce swelling
(corticosteroids, non-steroidal anti-inflammatory (NSAIDs)) and pain (morphine, anaesthetics) are used. Injection therapy can be used
for individuals with low-back pain with or without pain and other symptoms in the leg.
A number of electronic databases of healthcare articles were searched up to March 2007. This search identified 18 randomized controlled
trials (RCTs; 1179 participants) that looked at injections with a variety of drugs compared to a placebo drug or other drugs. The
injections were given into the epidural space (between the vertebrae of the back and outside the coverings that surround the spinal
cord), the facet joints (the joints of two vertebrae), or tender spots in the ligaments or muscles.
The review authors rated ten of the 18 RCTs as having a low risk of bias in the way the trials were conducted and reported. They
were unable to statistically pool the results because the injection sites, drugs used and outcomes measured were too varied. Only five of
the 18 trials reported significant results in favour of one of the treatment arms. The reviewer authors considered the likely treatment
benefits to be worth the potential harms in only two studies.
In nine out of the 18 studies, side effects such as headache, dizziness, transient local pain, tingling and numbness and nausea were
reported in small numbers of patients. The use of morphine was more frequently associated with itching, nausea and vomiting. Rare
but more serious complications of injection therapy have been mentioned in the literature, such as cauda equina syndrome, septic facet
joint arthritis, discitis, paraplegia, paraspinal abscesses. Although the absolute frequency of these complications may be rare, these risks
should be taken into consideration.
Based on these results, the review authors concluded that there is no strong evidence for or against the use of any type of injection
therapy for individuals with subacute or chronic low-back pain.
B A C K G R O U N D
Numerous treatments have been promoted as useful to reduce
the individual and socio-economic burden of low-back pain, but
many controversies still exist on the effectiveness of the available
treatment options (Weinstein 2004; Airaksinen 2006). Injection
therapy is one of the treatments for patients with subacute and
chronic low-back pain that needs careful evaluation with respect
2Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

to its effectiveness for short- and long-term pain relief. In order
to investigate the effects of injection therapy for low-back pain
in a systematic review, it should be realized that the content of
this treatment method, as studied in randomized controlled trials
(RCTs), may show a large degree of variation. The same holds for
daily clinical practice, which underlines the need to make clin-
ically valid comparisons of injection therapy interventions. The
first source of variation in the content of injection therapy is the
location of the injection and the tissue that is targeted for injec-
tion. The injection can be given into the facet joints, the epidu-
ral space, the spinal nerve root, the intervertebral disc, the lum-
bar sympathetic chain, sacro-iliac joints and also into local liga-
ments, muscles or trigger points (Airaksinen 2006). Second, the
pharmacological agent that is used for the injection varies from
different types of corticosteroids aimed at reducing inflammation
and anaesthetics aimed at pain relief, to a variety of other drugs,
all with potentially different dosages. Third, the indications for
the injection therapy may also be different. Injection therapy can
be applied in cases of acute, subacute or chronic low-back pain
with or without signs of nerve root compression. For obvious rea-
sons, the specific characteristics of the injection therapy with re-
spect to target tissue, pharmacological agent and dosage depends
on the presumed pathophysiological mechanisms leading to pain.
In some cases, injections are used for diagnostic purposes rather
than treatment. Injections into facet joints, for example, have been
presented as a diagnostic test for the so-called lumbar facet joint
syndrome (Mooney 1976; Mooney 1987). Furthermore, in some
RCTs, injection therapy is only one part of a multimodal treat-
ment package. These issues may challenge a valid assessment and
summation of the effects of injection therapy in patients with low-
back pain.
The present systematic review is an update of an earlier Cochrane
review on the effectiveness of injection therapy for subacute and
chronic low-back pain (Nelemans 2000). Many of the 21 studies
that were included in this prior systematic review were rated as
being of low methodological quality and in 11 of the 21 studies,
injection was compared with placebo. The authors concluded that
convincing evidence for the effectiveness of injection therapy was
still lacking and recommended large well-designed trials in this
field, preferably placebo-controlled (Nelemans 2000).
Since Nelemans 2000 et al was published, several new RCTs on
the effects of injections for low-back pain were published and the
method guidelines for systematic reviews in the field of low-back
pain were updated (van Tulder 2003). In order to reduce the clini-
cal heterogeneity identified in the earlier review, several more spe-
cific injection therapies have been covered in separate Cochrane
reviews. Therefore, the present systematic review does not include
the effects of intradiscal therapy (Niemisto 2003), prolotherapy
(i.e. injection of sclerosants) (Dagenais 2007) or epidural steroids
for radiculopathy due to disc herniation (registered as a title for
an upcoming Cochrane review). Although some overlap cannot
always be prevented since radiculopathy is not an exclusive diag-
nosis, we aim to exclude studies dealing specifically with epidu-
ral steroids for this particular study population from the present
update. Nelemans 2000 et al had included studies on epidural
steroids for radiculopathy in the earlier review. This update further
differs from the previous review with regard to the internal valid-
ity criteria that were used. We rated the studies according to the
eleven internal validity items recommended by van Tulder 2003
whereas Nelemans 2000 et al used a fifteen item list according to
ter Riet 1990 et al. In addition, we also added an assessment of
clinical relevance to the present review.
Because many studies in the review by Nelemans 2000 et al were
clinically heterogeneous, a major concern for the present update,
as stated before, was to come up with comparisons that made sense
from a clinical perspective. Therefore, we chose to classify studies
first according to the target tissue of the injection and second
according to the therapeutic agent that was used. If possible, these
strata were further subdivided into placebo-controlled trials and
those that compared injections with other treatments.
O B J E C T I V E S
The objective of this systematic review was to asses the effectiveness
of injection therapy for patients with subacute or chronic low-
back pain.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Only RCTs were included. Non-randomized studies were ex-
cluded.
Types of participants
Patients aged from 18 to 70 years were included if they had low-
back pain with symptoms persisting for at least one month. Suba-
cute low-back pain was defined as lasting for four weeks or longer
and chronic as lasting for 12 weeks or longer.
Types of interventions
The treatment had to include injection therapy for pain relief.
The injection therapy was studied at three different injection sites:
facet joints, epidural sites, and local sites. Studies that compared
the effects of epidural steroids for radicular pain, intradiscal in-
jections, prolotherapy or Ozone therapy with other treatments
3Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

were excluded unless injection therapy with another pharmaceuti-
cal agent (no placebo treatment) was part of one of the treatment
arms. Studies about injections into sacroiliac joints and studies in
which the drugs were administered by means of a catheter and not
directly by means of an injection were also excluded.
Additional treatments were allowed.
Types of outcome measures
Pain was considered to be the most important outcome measure.
In order to be included for the present review, studies should at
least have incorporated this outcome measure. This could be ex-
pressed as the percentage of patients with pain relief or as mean
improvement on a continuous scale. Other important outcome
measures were: a global measure of improvement (e.g. overall im-
provement, proportion of patients recovered, subjective improve-
ment of symptoms), back-specific disability (expressed on a back-
specific index, such as the Roland Disability Questionnaire or the
Oswestry Disability Index), generic health status or well-being,
disability for work, and patient satisfaction (Bombardier 2000;
van Tulder 2003). These outcomes were evaluated on both a short-
term (less than six weeks) and long-term basis (longer than six
weeks). Side effects were also considered.
Search methods for identification of studies
RCTs published in English, French, German, Dutch and Nordic
languages were included. The literature searches carried out by
Nelemans et al were updated and reiterated in the same databases
for the period from 1999 to March 2007 (Nelemans 2000). MED-
LINE and EMBASE searches were based on the search strategies
recommended by the Cochrane Back Review Group (van Tulder
2003). The Cochrane CENTRAL database was also screened for
relevant RCTs. In addition, citation tracking of the studies re-
trieved by the search was performed until no new studies were
found. See Appendix 1 for the PubMed and EMBASE search
strategies.
Data collection and analysis
Study selection and data extraction
For the 2007 update, two authors (JBS, RdB) independently se-
lected new studies, assessed the methodological quality, and ex-
tracted the data (using a standardized form). This was conducted
in the same way, described in the following sections, as in the pre-
viously published systematic review (Nelemans 2000). A consen-
sus method was used to solve disagreements about the selection
of RCTs, and a third author (PN) was consulted if disagreement
persisted. First, the two authors screened the titles, abstracts and
keywords of all references identified by the literature search to de-
termine if they met the inclusion criteria. Second, the full text of
the article was retrieved for studies for which it was unclear from
the screening procedure whether or not the study had to be in-
cluded.
Methodological quality assessment
The methodological quality of the RCTs was independently as-
sessed by two authors (JBS, RdB), using the methodological cri-
teria recommended by the Cochrane Back Review Group (van
Tulder 2003). A consensus method was used to resolve disagree-
ments and a third author was consulted if disagreements persisted
(PN). The items were scored as either positive (+), negative (-)
or unclear (?). The criteria used, and their operationalization are
listed in Table 1.
Clinical relevance
Two authors (JBS and RdB) independently assessed the clinical
relevance of the included studies according to several questions
which were recommended by the Cochrane Back Review Group
(van Tulder 2003). Each question was scored positive (+) if the
clinical relevance item was met, negative (-) if the item was not met
and unclear (?) if data were not available to answer the question.
We considered a 20% improvement in pain scores (Salaffi 2004)
and a 10% improvement in functioning outcomes (Bombardier
2000) to be clinically important. See Table 2 for the questions
used.
Analysis
The results of each RCT were plotted as point estimates with cor-
responding 95% confidence intervals (95% CI) as far as possi-
ble. The clinical homogeneity was evaluated by exploring the dif-
ferences between the RCTs, taking into consideration the study
population, the injection sites, the content of the injection ther-
apy with regard to medication and dosage, reference treatments,
timing of follow-up measurements and measurement instruments.
Furthermore, a distinction was made between studies that com-
pared injection with a placebo injection and studies that compared
two or more active agents (Nelemans 2000). Attempts were made
to statistically pool the data of homogeneous studies for the out-
come measures pain, overall improvement and disability for short
and long-term follow-up. If subgroups of studies were considered
to be clinically homogeneous, the statistical homogeneity was for-
mally tested. If studies were considered clinically heterogeneous
and/or studies did not report their results in a way that enabled us
to perform statistical pooling (for example, for continuous data,
means were presented but no standard deviations) we refrained
from following a formal meta-analytic approach. In stead of this,
we summarized the results according to a rating system with five
levels of evidence (best evidence synthesis), based on the quality
4Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

and the outcome of the studies (van Tulder 2003). The following
levels of evidence were distinguished:
• Strong evidence - Consistent findings among multiple
high quality RCTs;
• Moderate evidence - Consistent findings among multiple
low quality RCTs or one high quality RCT;
• Limited evidence - one low quality RCT;
• Conflicting evidence - inconsistent findings among
multiple trials;
• No evidence - no RCTs.
High quality studies were defined as RCT which fulfilled six or
more of the internal validity criteria. The results were considered
to be consistent if 75% of the studies showed results in the same
direction.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excluded
studies.
Study selection
The original 1998 search yielded 40 relevant papers (Nelemans
2000). After detailed reading, 19 studies were excluded because
they included acute patients (pain for less than one month), they
did not describe the duration of the reported symptoms, they ap-
peared to be non-randomized or the anesthetic agent was injected
into the wound during surgery (Nelemans 2000). From the re-
maining 19 studies that were covered by Nelemans 2000 et al,
nine studies were excluded from the present update due to the
modified inclusion criteria. As stated earlier, studies on the effects
of corticosteroids for radiculopathy will be summarized in an-
other Cochrane review. This means that four studies which inves-
tigated the effects of corticosteroids in patients with radiculopathy
in comparison with a placebo injection (Cuckler 1985; Mathews
1987; Bush 1991; Rogers 1992) were excluded. Furthermore, one
study dealt with intradiscal injection (Simmons 1992), one study
dealt with prolotherapy (Ongley 1987), both of which are covered
in another Cochrane review, and another study included patients
who had cervical symptoms and did not present separate results
for the lower back (Hameroff 1981). Two studies were excluded
because the drugs were administered by means of a catheter (Dallas
1987; Glynn 1988) and not directly by means of an injection. In
addition, the study population of one of them consisted of patients
with chronic pain with only a small subgroup of patients labeled
as having low-back pain (Glynn 1988). Consequently, from the
previous search by Nelemans 2000 et al, only 10 studies were in-
corporated into the present update.
The March 2007 literature search update resulted in the identifica-
tion of 11 new references from MEDLINE, eight references from
EMBASE and one reference from additional reference checking.
Four references were included in both the MEDLINE and EM-
BASE search results, leaving 16 references potentially relevant for
the purpose of the review. After careful reading of the papers, the
two reviewers (JBS and RdB) decided that eight studies had to
be excluded. Two of them compared two different needling tech-
niques (Stojanovic 2005) or injection sites (Pneumaticos 2006).
One study compared radiofrequency denervation with an injec-
tion of a small amount of lidocaine which was considered a sham
treatment (Oh 2004). Other studies dealt with patients with
radiculopathy (sciatic nerve pain) (Bonetti 2005), with acute pa-
tients (Tuzun 2003), patients with osteoporosis (Ofluoglu 2007),
or made use of epidural catheterization (Fredman 1999). One
study appeared not to be a RCT (Ney 2006). Together with 10
studies from the earlier review, we ended up with 18 studies that
were considered relevant for the purpose of this review.
Characteristics of included studies
The number of participants in the included studies varied from 16
to 206 patients. Only three studies included more than 100 partic-
ipants (Lilius 1990; Carette 1991; Aldrete 2003). The study popu-
lation in most of the included studies consisted of patients who had
low-back pain with or without sciatica. Two studies dealt only with
post-laminectomy patients (Rocco 1989; Aldrete 2003) and in one
of these studies, some of the patients also had radicular symptoms
(Aldrete 2003). In two other studies, populations were mixed: pa-
tients were included with low-back pain and/or sciatica whether
or not combined with neurological signs (Beliveau 1971; Mauro
2000). In some studies, participation was limited to patients who
responded positively to a facet block with an anesthetic (Carette
1991; Manchikanti 2001) or to patients with radiologically con-
firmed facet joint osteoarthritis (Fuchs 2005). The injection sites of
the studies included can be subdivided into epidural sites (Beliveau
1971; Breivik 1976; Rocco 1989; Serrao 1992; Aldrete 2003;
Lierz 2004; Takada 2005), facet joints (Lilius 1990; Carette 1991;
Marks 1992; Revel 1999; Mayer 2004; Fuchs 2005) and local sites
(Sonne 1985; Garvey 1989; Collee 1991; Mauro 2000). Facet in-
jections consisted of intra-articular injections (Lilius 1990; Carette
1991; Marks 1992; Revel 1999; Mayer 2004; Fuchs 2005), peri-ar-
ticular injections (Lilius 1990; Revel 1999) or nerve blocks (Marks
1992; Manchikanti 2001). Local injections sites varied from ten-
der- and trigger points (Garvey 1989; Collee 1991) to mus-
cles (Mauro 2000) and ligaments (Sonne 1985). The drugs that
were studied were mostly corticosteroids (i.e. methylprednisolone,
triamcinolone and prednisolone) (Beliveau 1971; Breivik 1976;
Sonne 1985; Garvey 1989; Lilius 1990; Rocco 1989; Carette
1991; Marks 1992; Aldrete 2003; Mayer 2004; Fuchs 2005) or
5Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

local anesthetics (i.e. procaine, lidocaine, bupivacaine, lignocaine
and ropivacaine) (Collee 1991;Revel 1999; Lierz 2004; Takada
2005). Other drugs that were studied were non-steroidal anti-
inflammatories (NSAIDs) (Aldrete 2003), sodium hyaluronate
(Fuchs 2005), Sarapin (i.e. a suspension of powdered pitcher plant
in alkaline solution) (Manchikanti 2001), Vitamin B12 (Mauro
2000), morphine (Rocco 1989) and Midazolam (Serrao 1992).
Eight studies appeared to be placebo-controlled (Beliveau 1971;
Breivik 1976; Sonne 1985; Garvey 1989; Lilius 1990; Carette
1991; Collee 1991; Mauro 2000) and 10 to be studies that
compared injections with other treatments (Rocco 1989; Marks
1992; Serrao 1992; Revel 1999; Manchikanti 2001; Aldrete 2003;
Lierz 2004; Mayer 2004; Fuchs 2005; Takada 2005). Among the
placebo-controlled studies, three used an anesthetic (i.e. procaine,
bupivacaine and lidocaine) as part of their reference injections
(Beliveau 1971; Breivik 1976; Garvey 1989). Nevertheless, we still
considered these studies placebo-controlled since the experimental
treatments in these studies consisted of corticosteroids with a sim-
ilar amount of anesthetic added to the solution as in the reference
treatment. Anesthetics in general have a relatively short duration
of action and from a pharmacological standpoint it seems unlikely
that they will result in lasting pain relief (Nelemans 2000).
In two studies the authors declared they had received their drugs
from commercial companies (Breivik 1976; Carette 1991). The
authors of three other studies explicitly reported that they had
no financial conflict of interest (Fuchs 2005; Lilius 1990; Aldrete
2003). The authors of the other studies provided no explicit in-
formation in their publication about funding or eventual conflicts
of interest.
Risk of bias in included studies
For the assessment of the methodological quality of the trials, we
combined the information from all papers reporting on the same
trial. The two reviewers disagreed on 72 of 198 items (36%) scored.
After discussing the results, they reached consensus on the scoring
of all items. Therefore, the assistance of a third reviewer was not
needed. Nine of the 18 studies included met six or more internal
validity criteria and were therefore considered to be at an acceptable
level of methodological quality (Breivik 1976; Garvey 1989; Rocco
1989; Carette 1991; Collee 1991; Marks 1992; Revel 1999; Lierz
2004; Takada 2005). The most prevalent shortcomings were: a
lack of clarity regarding the concealment of random treatment
allocation (N = 17), no reporting of co-interventions (N = 14)
and no reporting of an intention-to-treat analysis (N = 13). The
internal validity criteria that were most frequently met were: the
acceptability of the level of compliance of patients to the treatment
protocol (N = 18), the description and acceptability of the drop-
out rate (N = 14) and the similarity of the timing of the outcome
assessments (N = 13). See details in Figure 1.
6Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Figure 1. Summary of risks of bias
7Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Effects of interventions
Feasibility of statistical pooling
As stated in the method section, statistical pooling was only con-
sidered if subgroups of studies were clinically homogeneous and
the authors provided sufficient information on study character-
istics, outcome measures and study results. After reviewing the
study characteristics of the studies included, only two subgroups
of two studies seemed to be sufficiently clinically homogeneous to
perform statistical pooling. Beliveau 1971 et al and Breivik 1976
et al compared the effect of epidural corticosteroid injections to
placebo injections and looked at short-term results of pain re-
lief, measured on a subjective dichotomous scale. However, in the
study by Breivik 1976 et al, the patients who were allocated to a
particular treatment and who did not improve were also treated
with injections of the alternative group. The timing of the out-
come measurements in this study was not clear either. Therefore,
we thought these two studies were too heterogeneous to pool their
results. Carette 1991 et al and Lilius 1990 et al compared the ef-
fects of facet joint injections with corticosteroids to placebo injec-
tions (Lilius 1990; Carette 1991). However, the study by Carette
1991 et al used a dichotomous outcome for pain improvement,
whereas Lilius 1990 et al reported mean pain scores and no pro-
portions of patients with pain relief. Therefore, it was not possible
to pool the results of these two studies. Consequently, instead of
statistical pooling, we had to perform a best-evidence synthesis for
both subgroups of studies.
Effectiveness of injection therapy
1. Epidural injections
Epidural corticosteroids versus placebo injections
Two studies compared the short term effects of epidural corti-
costeroid injections to placebo injections (Beliveau 1971; Breivik
1976). One of them was rated as a high quality study (Breivik
1976) and the other one was rated as a low quality study (Beliveau
1971). These two studies did not show a significant result for pain
relief or other outcomes in favour of the corticosteroids group.
There is limited evidence that epidural corticosteroid injections
are not significantly different from placebo injections for general
improvement in the short term (1 trial; 48 patients). There is
moderate for pain relief and limited evidence for work disability
that epidural corticosteroid injections are not significantly differ-
ent from placebo injections in the short term (1 trial; 35 patients).
Back-specific disability, generic health status and patient satisfac-
tion were not measured.
Epidural corticosteroid injections versus other treatments
Three studies compared the effects of epidural corticosteroid injec-
tions to other treatments. The low quality study by Aldrete 2003
et al compared corticosteroids to NSAIDs (i.e. indomethacin) and
showed no significant differences in short-term pain progress and
physical activity in post-laminectomy patients. In the low quality
study by Serrao 1992 et al, corticosteroids were combined with
dextrose solution and compared to an intrathecal benzodiazepine
(i.e. Midazolam) combined with a dextrose solution. No signifi-
cant differences between the groups were reported for pain relief
at two weeks and two months, or general improvement at two
months. In a high quality study, Rocco 1989 et al compared cor-
ticosteroids to morphine and to a combination of corticosteroids
and morphine in post-laminectomy patients but found no signif-
icant differences in pain relief at one or six months.
There is limited evidence that the effect of epidural corticosteroid
injections are not significantly different from NSAIDs for pain
relief in the short term in post-laminectomy patients (1 trial; 206
patients), benzodiazepine for pain relief and general improvement
both in the short and intermediate term (1 trial; 28 patients), and
from morphine eventually combined with corticosteroids for pain
relief in the short and intermediate term in post-laminectomy pa-
tients (1 trial; 22 patients). Back-specific disability, generic health
status, disability for work and patient satisfaction were not mea-
sured.
Epidural injections with local anaesthetics versus other
treatments
In a high quality study, Lierz 2004 et al compared the effects of
epidural blocks with ropivacaine to epidural blocks with bupi-
vacaine. The purpose of these blocks with local anaesthesia was
to provide good analgesia to allow active physiotherapy. There
were no significant differences found between the groups in post-
treatment analgesia. In a low quality randomized cross-over study,
Takada 2005 et al also investigated the effects of epidural blocks
with ropivacaine of two different dosages and epidural blocks of
bupivacaine. No significant differences in pain scores were found
after the different epidural blockades.
There is moderate evidence (2 trials; 56 patients) that there is no
significant difference in the amount of analgesia provided between
epidural blocks with ropivacaine and epidural blocks with bupi-
vacaine. General improvement, back-specific disability, generic
health status, disability for work and patient satisfaction were not
measured.
2. Facet joint injections
8Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Facet joint injections with corticosteroids versus placebo
injections
One high quality study and one low quality study compared the
effects of facet joint injections with corticosteroids to placebo in-
jections. In their high quality study, Carette 1991 et al pre-se-
lected and only included patients who responded positively to a
facet joint injection with lidocaine (more than 50% reduction in
pain score). These patients were randomly allocated to either cor-
ticosteroids or placebo injections. No significant differences for
self-rated improvement, pain or functional status were found be-
tween the groups at one and three months. At six months, sig-
nificant differences were found with regard to self-rated improve-
ment, pain and functional status in favour of the corticosteroids
group (Carette 1991). In a low quality study, Lilius 1990 et al com-
pared corticosteroids injected intra-articularly to corticosteroids
injected peri-capsularly and to placebo injections. No significant
differences between the groups were reported for pain, disability
and work attendance at one hour, two weeks, six weeks and three
months (Lilius 1990).
There is moderate evidence (2 trials; 210 patients) that facet joint
injections with corticosteroids are not significantly different from
placebo injections for short term pain relief and improvement
of disability. There is conflicting evidence (2 trials; 210 patients)
whether facet joint injections with corticosteroids are more effec-
tive for intermediate term pain reduction and improvement of dis-
ability than placebo injections. There is limited evidence (1 trial;
109 patients) that there is no significant difference between the
effects of facet joint injections with corticosteroids and placebo
injection on work attendance. Generic health status and patient
satisfaction were not measured.
Facet joint injections with corticosteroids versus other
treatments
In four studies, the effects of corticosteroids injections into the
facet joints were compared with other treatments. In a low quality
study, Manchikanti 2001 et al compared the effects of multiple
medial branch blocks, consisting of corticosteroids combined with
local anaesthetics and Sarapin, to multiple medial branch blocks
consisting of only local anaesthetics and Sarapin. No significant
differences between the groups were found in pain relief, overall
health, physical, functional, and psychological status and return-
to-work at different follow-up moments throughout a 2.5-year
follow-up period. In a low quality study, Mayer 2004 et al made
a comparison between facet joint injections on one to three levels
bilaterally, with mixtures of local anaesthetics and corticosteroids
combined with a home stretching exercise program, and the home
stretching exercise program only. No significant post-treatment
differences between the groups were found for pain and disabil-
ity. In the high quality study by Marks 1992 et al, facet joint in-
jections with corticosteroids and lignocaine were compared with
facet nerve blocks using similar medication. The facet joint injec-
tions provided slightly better pain relief than facet nerve blocks,
although statistical significance was only reached at one month,
not immediately post-treatment, at two weeks or three months
(Marks 1992). In a low quality study, Fuchs 2005 et al compared
the effects of facet joint injections with sodium hyaluronate to
similar injections with corticosteroids. No significant differences
in pain relief, disability and quality of life between the groups were
found at different follow-up points over a 180-day period.
There is limited evidence (1 trial; 84 patients) that facet joint injec-
tions consisting of corticosteroids, local anaesthetics and Sarapin
are not more effective than similar injections, consisting of local
anaesthetics and Sarapin, in influencing pain relief, overall health,
physical, functional, psychological status and return-to-work at
short- and long- term follow-up. There is limited evidence (1 trial;
70 patients) that facet joint injections with mixtures of corticos-
teroids and local anaesthetics combined with a home stretching
exercise program are not more effective than a home stretching
exercise program alone in providing long term effects on pain and
disability. There is moderate evidence (1 trial; 86 patients) that
facet joint injections with corticosteroids and local anaesthetics are
not more effective in improving short- and long-term pain scores,
disability scores and work attendance than facet nerve blocks using
similar medication. There is limited evidence (1 trial; 60 patients)
that facet joint injections with sodium hyalorunate are not more
effective than similar injections with corticosteroids in providing
short- and long- term pain relief, better function and improved
quality of life. Patient satisfaction was not measured.
Facet joint injections with local anaesthetics versus other
treatments.
One high quality study by Revel 1999 et al, which was designed
from a diagnostic perspective, compared facet joint injections with
lidocaine to facet joint injections with saline. In both groups these
injections were followed by an injection with corticosteroids (i.e.
cortivazol) near the joints. The lidocaine group had significantly
higher pain relief post-treatment than the saline group (Revel
1999).
There is moderate evidence (1 trial; 80 patients) that facet joint in-
jections with lidocaine combined with peri-articular corticosteroid
injections are more effective for short-term pain relief than facet
joint injections with saline combined with peri-articular corticos-
teroid injections. General improvement, back-specific disability,
generic health status, disability for work and patient satisfaction
were not measured.
3. Local injections
Local injections with corticosteroids versus placebo
injections
9Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

In a high quality study, Garvey 1989 et al compared trigger point
injections with corticosteroids (i.e. Aristopan) to placebo injec-
tions, a dry needle stick (acupuncture) and a spray of ethylchlo-
ride and acupressure in patients with persistent non-radiating low-
back pain, who were able to localize a point of maximal tender-
ness. No significant differences between the groups in self-reported
improvements were found at two weeks. In a low quality study,
Sonne 1985 et al studied the effects of local iliolumbar ligament
injections with corticosteroids versus placebo and found no sig-
nificant differences in pain relief at two weeks. However, self-re-
ported improvement at two weeks was significantly higher in the
corticosteroid group than in the placebo group (Sonne 1985).
There is moderate evidence (1 trial; 63 patients) that trigger point
injections with corticosteroids are not significantly different from
placebo injections for self-reported improvements at short-term
follow-up. There is limited evidence (1 trial; 30 patients) that local
injections into the iliolumbar ligament are more effective than
placebo for self-reported improvement in the short term but not
for pain relief in the short term. Back-specific disability, generic
health status, disability for work and patient satisfaction were not
measured.
Local injections with anaesthetics versus placebo injections
The high quality study by Collee 1991 et al investigated the effects
of a single local injection of lignocaine into the point of maximal
tenderness over the medial part of the iliac crest versus a placebo
injection. At two weeks, the mean pain score was significantly
lower in the lignocaine groups compared to the placebo group. A
non-significant difference in favour of the lignocaine group was
also found for self-reported improvement (Collee 1991).
There is moderate evidence (1 trial; 41 patients) that an injection
with a local anaesthetic at the point of maximal tenderness over
the medial part of the iliac crest, in patients with iliac crest pain
syndrome is more effective for short-term pain relief than a placebo
injection. Back-specific disability, generic health status, disability
for work and patient satisfaction were not measured.
Intramuscular injections with Vitamin B12 versus placebo
injections
In a low quality study, Mauro 2000 et al compared the effects of
intramuscular Vitamin B12 injections to intramuscular placebo
injections and found significant effects for post-treatment pain
and disability in favour of the Vitamin B12 group.
There is limited evidence (1 trial; 60 patients) that intramuscu-
lar Vitamin B12 injections are more effective than intramuscu-
lar placebo injections for short-term pain relief and disability im-
provement. Generic health status, disability for work and patient
satisfaction were not measured.
Clinical relevance
There was disagreement between the two review authors with re-
gard to the scoring of 27 of 90 (30%) clinical relevance items
(Table 3). Consensus was reached on all scorings after discussion.
In only two studies, the review authors considered the likely treat-
ment benefits to be worth the potential harms (Revel 1999; Mauro
2000) and in only four studies, the size of the effect was considered
to be clinically important (Breivik 1976; Sonne 1985; Revel 1999;
Mauro 2000). According to the review authors, most of the studies
described the interventions and treatment settings well enough to
enable clinicians to replicate the treatment in clinical practice.
Side effects
In nine of the 18 studies, side effects such as headache, dizziness,
transient local pain, paresthesia and nausea were reported in small
numbers of patients (Table 2). The use of morphine was more
frequently associated with pruritis, nausea and vomiting (Rocco
1989).
D I S C U S S I O N
The overall methodological quality of the studies included in this
review was limited and only six of the 18 trials (Sonne 1985;
Collee 1991; Carette 1991; Marks 1992; Revel 1999; Mauro
2000) showed significant results for at least one outcome at a fol-
low-up time point in favour of one of the treatment arms. Four
of these six studies reported effects that could be considered to
be clinically important (Breivik 1976; Mauro 2000; Revel 1999;
Sonne 1985). We conclude there is no strong evidence to support
the use of any type of injection therapy (epidural, facet joint or
local sites) for subacute or chronic-low-back pain in patients with-
out radicular pain. In the earlier Cochrane review on this topic,
Nelemans 2000 et al also concluded that convincing evidence was
lacking on the effects of injection therapy for low-back pain, which
means that the general picture on the effectiveness of injection
therapy has not changed since then. The scientific basis for these
injections for low-back pain has not improved.
Nelemans 2000 et al proposed several recommendations for fu-
ture research. These recommendations involved the priority for
placebo-controlled trials instead of trials that compared injections
to other treatments, the need for methodologically sound RCTs,
and more of a focus on long-term effects of the treatment in-
stead of only short-term effects (Nelemans 2000). Among the 18
studies included in this review, seven new studies were covered
in the present update (Mauro 2000; Manchikanti 2001; Aldrete
2003; Lierz 2004; Fuchs 2005; Takada 2005 ). Of these seven new
studies, only Mauro 2000 et al compared intramuscular Vitamin
B12 with placebo injections, which resulted in a total of seven
10Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

placebo-controlled versus 12 studies that compared injections to
other treatments or to each other.
According to the methodological quality assessment, the new stud-
ies in this update had no higher methodological quality than the
studies of the earlier review. On the contrary, the mean number
of positive items was even lower (4.1 versus 6.3 positive scores;
Table 2; Table 3) in this group of studies compared to the studies
included in the earlier review. The most prevalent shortcomings,
which were a lack of clarity regarding the concealment of ran-
dom treatment allocation, no reporting of co-interventions and
no reporting of an intention-to-treat analysis, could easily have
been avoided and nowadays, researchers should be aware that
these are generally accepted principles of methodological qual-
ity for studying the effectiveness of treatments. Only four out of
the 18 studies included had outcome assessments performed at
six months post-randomization and beyond (Rocco 1989; Carette
1991; Manchikanti 2001; Fuchs 2005). The outcome assessments
of the other studies were either performed post-treatment or at
another short-term time interval. Of course, from a pharmaco-
logical standpoint, the agent under study may act upon the tar-
get tissue rather quickly, for example, by reducing inflammation.
However, it is advantageous that the favourable effects on pain
and disability will also stand at the longer term. Since the course
of sub-acute and chronic low-back pain can be described as con-
sisting of spontaneous remissions and exacerbations (Croft 1998)
short-term effects of injections do not necessarily reflect a success-
ful treatment result in clinical practice. Outcome measures which
were used in the studies included visual analogues scales for pain
relief and questions regarding self-perceived improvement or other
outcomes. Only six studies used well-known and validated ques-
tionnaires for measuring disability (Rocco 1989; Carette 1991;
Serrao 1992; Mauro 2000 ; Mayer 2004; Fuchs 2005).
For the purpose of this review, we subdivided the studies accord-
ing to injection sites (i.e. epidural, facet joint and local sites),
to pharmaceutical agents (i.e. corticosteroids, anaesthetics and
other agents) and according to the comparison that was made (i.e.
placebo-controlled versus comparison of two or more treatments).
By following this approach, our aim was to come up with groups
that were clinically comparable without ending up with groups
consisting of only one study. Despite the fact that this approach
seemed logical, there were still differences among the studies that
ended up in a group with regard to inclusion criteria, target tis-
sue (e.g. intra-articular facet joint injections, peri-capsular facet
joint injections and medial branch blocks), injection dosage, co-
interventions, reference treatments and outcome measures. This
should be kept in mind when reading the evidence statements in
the results section of this paper. Furthermore, it should be empha-
sized that we only separated trials on the basis of whether the com-
parator was a placebo injection or other treatment. Other aspects
of the studies, such as meticulous patient selection by diagnostic
injections or experience and skills of the treatment providers were
not assessed.
One of the main problems when studying the effects of injec-
tion therapy in low-back pain is the lack of diagnostic criteria for
determining the injection site. According to our view, it is ex-
tremely difficult to accurately diagnose and determine the local-
isation of tissues that cause the pain and other symptoms. Some
researchers have tackled this problem, for example, by only includ-
ing patients for facet joint injections who responded positively to
facet blocks with anaesthetics (Carette 1991; Manchikanti 2001)
or patients with radiologically confirmed facet joint osteoarthritis
(Fuchs 2005). From these three studies, only the study by Carette
1991 et al had positive results. They showed significant effects for
pain and the physical dimension of the Sickness Impact Profile
in favour of a methylprednisolone group compared to a placebo
group, even after six-month follow-up (Carette 1991).
The rationale behind the application of a particular pharmaceu-
tical agent among the included studies was variable. In 13 stud-
ies, the effects of corticosteroids were investigated. This may be a
reasonable choice since this agent aims to reduce inflammation.
In four studies, the main pharmaceutical agent under study was
anaesthetics (Collee 1991; Revel 1999; Lierz 2004; Takada 2005).
The reason for choosing an injection with anaesthetics is not al-
ways immediately clear. Due to the relatively short duration of
action of these pharmaceutical agents, they do not seem to be the
first choice for pain relief in sub-acute and chronic patients. Lierz
2004 et al and Takada 2005 et al compared the short- term anal-
gesic effects of epidural blocks with ropivacaine and bupivacaine
and found no significant differences between the groups. The au-
thors of both studies explained that epidural blocks may provide
analgesia to allow for exercise and active physiotherapy, thus facil-
itating more active therapies. Collee 1991 et al compared a local
injection of lignocaine versus saline into a tender point over the
medial part of the iliac crest. The study authors state that the in-
jection with lignocaine may somehow affect the ascending or sen-
sory input and its varying modulating systems. However, no sig-
nificant differences in improvement rates were found. The study
by Revel 1999 et al was carried out from a diagnostic perspective.
They compared facet joint injections with lidocaine to placebo
injections in order to determine several clinical criteria which were
predictive of significant relief of back pain after facet joint anaes-
thesia (Revel 1999). Other applied pharmaceutical agents were:
indomethacin (Aldrete 2003), sodium hyaluronate (Fuchs 2005),
Sarapin (Manchikanti 2001), morphine (Rocco 1989) and Vita-
min B12 (Mauro 2000). In the study by Mauro 2000 et al, daily
intramuscular injections for a two-week period with Vitamin B12
appeared to be effective for short-term pain and disability com-
pared to placebo injections.
Half of the included studies reported side effects in small numbers
of patients (see Characteristics of included studies table). These side
11Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

effects ranged from headache, dizziness and transient local pain
to nausea and vomiting. Although these are not life threatening
complications and have only been reported in a limited number
of patients, this does not mean that the application of injection
therapy in low-back pain is always without risk. Rare but more
serious complications of injection therapy have been mentioned in
the literature, such as, cauda equina syndrome (Bilir 2006), septic
facet joint arthritis (Weingarten 2006), discitis (Hooten 2006),
paraplegia (Houten 2002) and paraspinal abscesses (Cook 1999).
In another study, it was found that eight out of 128 consecutive
patients referred to a hospital with meningitis had a history of sin-
gle or repeated injections for low-back pain one to three weeks be-
fore their hospital admission (Gaul 2005). Although the absolute
frequency of these complications may be rare, these risks should be
taken into consideration, especially given the fact that convincing
evidence on the effects of injection therapy for low-back pain is
still lacking.
Seven out of the 18 trials included in this review reported signifi-
cant but short-lasting effects in favour of the intervention group,
with interventions varying from facet joint injections with cor-
ticosteroids (Carette 1991; Mayer 2004) and anaesthetics (Revel
1999), epidural injections with corticosteroids (Breivik 1976), lo-
cal injections with anaesthetics (Sonne 1985; Collee 1991) to
intramuscular injections with Vitamin B12 (Mauro 2000). The
overall picture of the results of this review reveals that there is
currently insufficient scientific evidence on the effects of injec-
tion therapy, regardless of type and dosage, for patients with sub-
acute and chronic low-back pain. It is discouraging that the aver-
age methodological quality of the trials published since the earlier
review has not improved while the validity criteria for effective-
ness research have become more familiar to back pain researchers.
Most studies dealt with heterogeneous groups of patients, which
on average, may mask potential treatment effects. Therefore, we
can not rule out that some type of injection therapy might be
effective for a particular subgroup of patients. Therefore, accu-
rate diagnostic criteria are needed. However, this remains merely a
theoretical consideration, which is not based on the results of the
present review.
A U T H O R S ’ C O N C L U S I O N S
Implications for practice
Based on the current state of the literature there is insufficient
evidence to support or refute the use of injection therapy, regardless
of type and dosage, for patients with subacute and chronic low-
back pain without radicular pain.
Implications for research
We can not rule out that some type of injection therapy is effective
for a particular subgroup of patients. More research is needed to
study the accuracy of diagnostic criteria to identify which, if any,
subgroups of patients are likely to respond to injection therapy
and if established, the effectiveness of injection therapy for these
subgroups. Corticosteroids seem to be the most logical therapeutic
agent, while anaesthetics seem only useful for diagnostic purposes.
If injection therapy turns out to be an effective treatment strategy
for a subgroup of low-back pain patients, it has to be embedded
in the current, widely supported active approach directed at reas-
surance and self management.
A C K N O W L E D G E M E N T S
The review team wishes to thank Professor Ferd Sturmans, The
Netherlands, for his contribution to the original review.
R E F E R E N C E S
References to studies included in this review
Aldrete 2003 {published data only}∗ Aldrete JA. Epidural injections of indomethacin for
postlaminectomy syndrome: a preliminary report. Anesth
Analg 2003;96(2):463–8.
Beliveau 1971 {published data only}
Beliveau P. A comparison between epidural anaesthesia with
and without corticosteroid in the treatment of sciatica.
Rheumatol Phys Med 1971;11(1):40–3.
Breivik 1976 {published data only}
Breivik HH, Hesla PE, Molnar I, Lind B. Treatment of
chronic low back pain and sciatica: comparison of caudal
epidural injections of bupivacaine and methylprednisolone
with bupivacaine followed by saline. Adv Pain Res Ther
1976;1:927–32.
Carette 1991 {published data only}∗ Carette S, Marcoux S, Truchon R, Grondin C, Gagnon J,
Allard Y, et al.A controlled trial of corticosteroid injections
into facet joints for chronic low back pain. N Eng J Med
1991;325(14):1002–7.
Collee 1991 {published data only}
Collee G, Dijkmans BA, Vandenbroucke JP, Cats A. Iliac
crest pain syndrome in low back pain. A double blind,
randomized study of local injection therapy. J Rheumatol
1991;18(7):1060–3.
Fuchs 2005 {published data only}
Fuchs S, Erbe T, Fischer HL, Tibesku CO. Intraarticular
12Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
hyaluronatica acid versus glucocorticoid injections for
nonradicular pain in the lumbar spine. J Vasc Interv Radiol
2005;16(11):1493–8.
Garvey 1989 {published data only}
Garvey TA, Marks MR, Wiesel SW. A prospective,
randomized, double-blind evaluation of trigger point
injection therapy for low back pain. Spine 1989;14(9):
962–4.
Lierz 2004 {published data only}
Lierz P, Gustorff B, Markow G, Felleiter P. Comparison
between bupivacaine 0.125% and ropivacaine 0.2% for
epidural administration to outpatients with chronic low
back pain. Eur J Anaesthesiol 2004;21(1):32–7.
Lilius 1990 {published data only}
Lilius G, Harilainen A, Laasonen EM, Myllynen P. Chronic
unilateral low-back pain. Predictors of outcome of facet
joint pain. Spine 1990;15(8):780–2.
Lillius G, Laasonen EM, Myllynen P, Harilainen A,
Gronlund G. Lumbar facet joint syndrome. A randomised
clinical trial. J Bone Joint Surg 1989;71:681–4.
Lillius G, Lassonen AM, Myllynen P, Harilainen A, Salo
L. The lumbar facet joint syndrome: significance of
inappropriate signs: a randomized, placebo-controlled trial.
French Journal of Orthopaedic Surgery 1989;3(4):479–86.
Manchikanti 2001 {published data only}
Manchikanti L, Pampati V, Bakhit C, Rivera JJ, Beyer CD,
Damron KS, et al.Effectiveness of lumbar facet joint nerve
blocks in chronic low back pain: a randomized clinical trial.
Pain Physician 2001;4(1):101–7.
Marks 1992 {published data only}
Marks RC, Houston T, Thulbourne T. Facet joint injection
and facet nerve block: a randomised comparison in 86
patients with chronic low back pain. Pain 1992;49(3):
325–8.
Mauro 2000 {published data only}
Mauro GL, Martorana U, Cataldo P, Brancato G, Letizia G.
Vitamin B12 in low back pain: a randomised, double-blind
placebo-controlled study. Eur Rev Med Pharmacol Sci 2000;
4(3):53–8.
Mayer 2004 {published data only}
Mayer TG, Gatchel RJ, Keeley J, McGeary D, Dersh J,
Anagnostis C. A randomized clinical trial of treatment for
lumbar segmental rigidity. Spine 2004;29(20):2199–2205.
Revel 1999 {published data only}
Revel M, Poiraudeau S, Auleley GR, Payan C, Nguyen
M, Chevrot A, et al.Capacity of the clinical picture to
characterize low back pain relieved by facet joint anesthesia.
Proposed criteria to identify patients with painful facet
joints. Spine 1998;23(18):1972–6.
Rocco 1989 {published data only}
Rocco AG, Frank E, Kaul AF, Lipson SJ, Gallo JP. Epidural
steroids, epidural morphine and epidural steroids combined
with morphine in the treatment of post-laminectomy
syndrome. Pain 1989;36(3):297–303.
Serrao 1992 {published data only}
Serrao JM, Marks RL, Morley SJ, Goodchild CS. Intrathecal
midazolam for the treatment of chronic mechanical low
back pain: a controlled comparison with epidural steroid in
a pilot study. Pain 1992;48(1):5–12.
Sonne 1985 {published data only}
Sonne M, Christensen K, Hansen SE, Jensen EM. Injection
of steroids and local anaesthetics as therapy for low back
pain. Scand J Rheumatol 1985;14(4):343–5.
Takada 2005 {published data only}
Takada MF, Fukusaki M, Terrao Y, Yamashita K, Inadomi
C, Sumikawa K. Comparative efficacy of ropivaciane
and bupivacaine for epidural block in outpatients with
degenerative spinal disease and low back pain. Pain Clinic
2005;17(3):275–81.
References to studies excluded from this review
Bonetti 2005 {published data only}
Bonetti M, Fontana M, Cotticelli B, Volta GD, Guidani M,
Leonardi M. Intraforaminal O2-O3 versus periradicular
steroidal infiltrations in lower back pain: Randomized
controlled study. AJNR Am J Neuroradiol 2005;26(5):
996–1000.
Bush 1991 {published data only}
Bush K, Hillier S. A controlled study of caudal epidural
injections of triamcinolone plus procaine for the
management of intractable sciatica. Spine 1991;16(5):
572–5.
Cuckler 1985 {published data only}
Cuckler JM, Bernini PA, Wiesel SW, Booth RE, Rothman
RH, Pickens GT. The use of epidural steroids in the
treatment of lumbar radicular pain. A prospective
randomized, double-blind study. J Bone Joint Surg Am
1985;67(1):63–6.
Dallas 1987 {published data only}
Dallas TL, Lin RL, Wu WH, Wolskee P. Epidural morphine
and methylprednisolone for low back pain. Anesthesiology
1987;67(3):408–11.
Fredman 1999 {published data only}
Fredman B, Zohar E, Ben Nun M, Iraqi R, Jedeikin R,
Gepstein R. The effect of repeated epidural sympathetic
nerve block on “failed back surgery syndrome” associated
chronic low back pain. J Clin Anesth 1999;11(1):46–51.
Glynn 1988 {published data only}∗ Glynn C, Dawson D, Sanders R. A double-blind
comparison between epidural morphine and epidural
clonidine in patients with chronic non-cancer pain. Pain
1988;34(2):123–8.
Hameroff 1981 {published data only}
Hameroff SR, Crago BR, Womble J, Kanel J. Comparison
of bupivacaine, etidocaine, and saline for trigger point
therapy. Anesth Analg 1981;60(10):752–5.
Mathews 1987 {published data only}
Mathews JA, Mills SB, Jenkins VM, Grimes SM, Morkel
MJ, Mathews W, et al.Back pain and sciatica: controlled
13Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
trials of manipulation, traction, sclerosant and epidural
injections. Br J Rheumatol 1987 26;6:416–23.
Ney 2006 {published data only}
Ney JP, Difazio M, Sichani A, Monacci W, Foster L,
Jabbari B. Treatment of chronic low back pain with
succesive injections of Botulinum Toxin A over 6 months:
a prospective trial of 60 patients. Clin J Pain 2006;22(4):
363–9.
Ofluoglu 2007 {published data only}
Ofluoglu D, Akyuz G, Unay O, Kayhan O. The effect of
calcitonin on beta-emdorphin levels in postmenopausla
osteoporotic patients with back pain. Clin Rheumatol 2007;
26(1):44–9.
Oh 2004 {published data only}
Oh WS, Shim JC. A randomized controlled trial of
radiofrequency denervation of the ramus communicans
nerve for chronic discogenic low back pain. Clin J Pain
2004;20(1):55–60.
Ongley 1987 {published data only}
Ongley MJ, Klein RG, Dorman TA, Eek BC, Hubert LJ. A
new approach to the treatment of chronic low back pain.
Lancet 1987;2(8551):143–6.
Pneumaticos 2006 {published data only}
Pneumaticos SG, Chatziioannou SN, Hipp JA, Moore WH,
Esses SI. Low back pain: prediction of short-term outcome
of facet joint injection with bone scintigraphy. Radiology
2006;238(2):693–8.
Rogers 1992 {published data only}
Rogers P, Nash T, Schiller D, Norman J. Epidural steroids
for sciatica. Pain Clin 1992;5(2):67–72.
Simmons 1992 {published data only}
Simmons JW, McMillin JN, Emery SF, Kimmich SJ.
Intradiscal steroids. A prospective double-blind clinical
trial. Spine 1992;17(6 Suppl):S172–5.
Stojanovic 2005 {published data only}
Stojanovic MP, Dey D, Hord ED, Zhou Y, Cohen SP.
A prospective crossover comparison study of the single-
needle and multiple-needle techniques for facet-joint medial
branch blocks. Reg Anesth Pain Med 2005;30(5):484–90.
Tuzun 2003 {published data only}
Tuzun F, Unalan H, Oner N, Ozguzel H, Kirazli Y,
Icagasioglu A, et al.Multicenter, randomized, double-
blinded, placebo-controlled trial of thiocolchicoside in acute
low back pain. Joint Bone Spine 2003;70(5):356–61.
Additional references
Airaksinen 2006
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-
Moffett J, Kovacs F, et al.Chapter 4. European guidelines
for the management of chronic nonspecific low back pain.
Eur Spine J 2006;15(Suppl 2):S192–300.
Bilir 2006
Bilir A, Gulec S. Cauda equina syndrome after epidural
steroid injection: a case report. J Manipulative Physiol Ther
2006;29(6):492.e1–3.
Bombardier 2000
Bombardier C. Outcome assessments in the evaluation
of treatment of spinal disorders: summary and general
recommendations. Spine 2000;25(24):3100–3.
Cook 1999
Cook NJ, Hanrahan P, Song S. Paraspinal abscess following
facet joint injection. Clin Rheumatol 1999;18(1):52–3.
Croft 1998
Croft PR, Macfarlane GJ, Papageorgiou AC, Thomas E,
Silman AJ. Outcome of low back pain in general practice: a
prospective study. BMJ 1998;316(7141):1356–9.
Dagenais 2007
Dagenais S, Yellans MJ, Del Mar C, Schoene ML.
Prolotherapy injections for chronic low back pain. Cochrane
Database of Systematic Reviews 2007, Issue 2. [DOI:
10.1002/14651858]
Gaul 2005
Gaul C, Neundorfer B, Winterholler M. Iatrogenis (para-)
spinal abscesses and meningitis following injection therapy
for low back pain. Pain 2005;116(3):407–10.
Hooten 2006
Hooten WM, Mizerak A, Carns PE, Huntoon MA. Discitis
after lumbar epidural corticosteroid injection: a case report
and analysis of the case report literature. Pain Med 2006;7
(1):46–51.
Houten 2002
Houten JK, Errico TJ. Paraplegia after lumbosacral nerve
root block: report of three cases. Spine J 2002;2(1):70–5.
Mooney 1976
Mooney V, Robertson J. The facet syndrome. Clin Orthoped
1976;115:149–56.
Mooney 1987
Mooney, V. Facet joint syndrome. In: Jayson MIV editor
(s). The lumbar spine: back pain. 3rd Edition. Edinburgh:
Chruchill Livingstone, 1987:370–82.
Niemisto 2003
Niemisto L, Kalso E, Malmivaara A, Seitsalo S, Hurri H.
Radiofrequency denervation for neck and back pain: a
systematic review of randomized controlled trials. Cochrane
Database of Systematic Reviews 2003, Issue 1. [DOI:
10.1002/14651858]
Salaffi 2004
Salaffi F, Stancati A, Silvestri CA, Ciapetti A, Grassi
W. Minimal clinically important changes in chronic
musculoskeletal pain intensity measured on a numerical
rating scale. Eur J Pain 2004;8(4):283–91.
ter Riet 1990
ter Riet G, Kleijnen J, Knipschild P. Acupuncture and
chronic pain: a criteria-based meta-analysis. J Clin
Epidemiology 1990;43:1191–9.
van Tulder 2003
van Tulder M, Furlan A, Bombardier C, Bouter L, Editorial
Board of the Cochrane Collaboration Back Review Group.
Updated method guidelines for systematic reviews in the
14Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Cochrane Collaboration Back Review Group. Spine 2003;
28(12):1290–9.
Weingarten 2006
Weingarten TN, Hooten WM, Huntoon MA. Septic facet
joint arthritis after a corticosteroid facet injection. Pain Med
2006;7(1):52–6.
Weinstein 2004
Weinstein J. Absent from work: nature versus nurture. Ann
Intern Med 2004;140(2):142–3.
References to other published versions of this review
Nelemans 2000
Nelemans PJ, de Bie RA, de Vet HCW, Sturmans F.
Injection therapy for subacute and chronic low back pain.
Cochrane Database of Systematic Reviews 2000, Issue 2.
[DOI: 10.1002/14651858]∗ Indicates the major publication for the study
15Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Aldrete 2003
Methods RCT; Randomization procedure not described.
Participants Pain care center, Florida, USA.
206 patients with recurrent LBP and radiculopathy after laminectomy, at least 6 months
post operation, lower back and extremity pain > 7 points on VAS scale (0 to 10). The
duration of pain was not specified. Exclusion criteria: pseudomeningocele, arachnoiditis
and/or recurrent pain from free disk fragments as confirmed by MRI study
Interventions (1) 2 epidural injections of indomethacin 1 mg.
(2) 2 epidural injections of indomethacin 2 mg.
(3) 2 epidural injections of methylprednisolone 80 mg.
In every case, the interval between the injections was 2 weeks and medication was diluted
in 3 ml of 0.5% bupivacaine
Outcomes Timing of outcomes: before and 2 weeks after randomization.
No significant differences were reported between the groups in pain progress and physical
activity at 2 weeks
Notes Side-effects: no instances of apparent dural puncture or high sensory or motor block
were noted, nor were other effects typical of NSAIDs therapy such as rash, epigastric
discomfort, or bruising
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Unclear risk unclear from text
Blinding?
All outcomes - care providers?
High risk no
Blinding?
All outcomes - outcome assessors
Unclear risk unclear from text
Incomplete outcome data addressed?
All outcomes - drop-outs?
High risk
16Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Aldrete 2003 (Continued)
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Unclear risk unclear from data given
Co-interventions avoided or similar? Unclear risk unclear from text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Beliveau 1971
Methods RCT; Patients were allocated alternately to treatment groups
Participants Department of Rheumatology and Physical medicine, UK.
48 patients with unilateral sciatica, thought to be caused by an intervertebral disc lesion,
with or without neurological signs, before or after other conservative treatments had
been tried. The duration of pain was not specified
Interventions (1) Epidural injection of 42 ml of procaine 0.5% in normal saline.
(2) Epidural injection of 40 ml of procaine 0.5% in normal saline to which 2 ml of
methylprednisolone 80 mg had been added.
In both groups injections were repeated in patients who had an improvement after the
first injection
Outcomes Timing of outcomes: before and 1 week after randomization.
(1) 16 of 24 patients improved at 1 week after the injection; (2) 18 of 24 patients
improved at 1 week after the injection; no other outcomes reported
Notes Side effects: Mild headache and dizziness occurred in about ten cases; the symptoms
were transient lasting up to 30 minutes after the injection. In two cases the theca was
penetrated by the needle during the injection and the procedure was stopped
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? High risk Patients were allocated alternately to treat-
ment groups
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
High risk
17Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Beliveau 1971 (Continued)
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
High risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
Low risk
Similarity of baseline characteristics? High risk
Co-interventions avoided or similar? High risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Breivik 1976
Methods RCT; Patients were allocated according to a list of random numbers
Participants Departments of Anesthesiology and Neurology, Akershus Central Hospital and outpa-
tient clinic, Norway
35 patients with incapacitating chronic low-back pain and sciatica unresponsive to con-
servative treatment for several months to several years. Diagnoses based on radiculogra-
phy: arachnoiditis (N=8), prolapsed disc (N=8), no abnormality (N=11), inconclusive
findings (N=5)
Interventions (1) Caudal epidural injection of 20 ml bupivacaine 0.25% with 80 mg depo-methyl-
prednisolone.
(2) Caudal epidural injection of 20 ml bupivacaine 0.25% followed by 100 ml saline.
Frequency: up to three injections at weekly intervals eventually followed by up three
injections of the alternative group
Outcomes Timing of outcomes: 2 to 5 weeks after randomization
Reported outcomes were pain relief, objective improvements (i.e. neural symptoms) and
work status.
Pain relief was obtained in 63% of the patients in the intervention group and 68% of
the patients in the reference group which was no statistically significant difference
Notes If there was no improvement 3 weeks after the last injection, up to three injections of
the alternative type were given. Side effects: not mentioned
Risk of bias
18Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Breivik 1976 (Continued)
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Patients were allocated according to a list
of random numbers
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Unclear risk data not provided
Co-interventions avoided or similar? Low risk
Compliance acceptable? Low risk
Timing outcome assessments similar? High risk
Carette 1991
Methods RCT; Randomization by random numbers generation, balancing after every 8 patients
Participants Centre Hospitalier de l’Université Laval, Quebec city, Canada.
101 patients with pain originating in the facet joints and who had a >50% reduction
(on a VAS score for pain) after injection with lidocaine were entered into the trial.
The mean duration of the current episode of pain was 18 (intervention group) and 24
months (control group). Exclusion criteria: back pain with a non mechanical origin,
previous injections in the facet joints or surgery, pregnancy, known allergy to anesthetic
or radiological contrast agents, presence of a blood coagulation disorder
Interventions (1) Facet joint injection of 20 mg (1 ml) of methylprednisolone acetate mixed with 1 ml
isotonic saline.
(2) Facet joint injection of 2 ml isotonic saline.
19Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Carette 1991 (Continued)
Outcomes Timing of outcomes: before and 1, 3 and 6 months after randomization and treatment.
At one and three months there were no significant differences in pain, functional status
and back flexion between the groups. At one month 42% of the patients in the methyl-
prednisolone group and 33% of the patients in the placebo group reported marked or
very marked improvement. At 6 months 46% of the patients in the methylprednisolone
group and 15% of the patients in the placebo group reported a significant marked or very
marked improvement. Significant differences at 6 months in favor of the methylpred-
nisolone group were also found for pain (VAS-score) and the physical dimension of the
Sickness Impact Profile. The differences were reduced when concurrent interventions in
the methylprednisolone group were taken into account
Notes Side effects: No adverse effects were reported, other than transient local pain at the
injection site
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Randomization by random numbers gen-
eration, balancing after every 8 patients
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Low risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear from text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
20Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Collee 1991
Methods RCT; Randomization procedure not described
Participants Department of Rheumatology, University Hospital Leiden, The Netherlands. Patients
recruited from a university based outpatient clinic (median duration of pain was 8 years)
and a large general practice in a rural area (median duration of pain was 18 days).
41 patients with iliac crest pain syndrome. Exclusion criteria were: diagnosis of sciatica,
ankylosing spondylitis, malignancy, infection, spondylolysthesis, severe degenerative disc
disease or fibromyalgia
Interventions Single local injection at the point of maximal tenderness over the medial part of the iliac
crest.
(1) Injection of 5 ml lignocaine 0.5%.
(2) Injection of 5 ml isotonic saline.
Outcomes Timing: at baseline and 10 minutes, 7 days, 14 days and 2 months after the injection.
At 14 days the mean pain score in the lignocaine group was significantly lower than in the
control group. In the lignocaine group 52% of patients improved at 14 days compared to
30% in the control group. This difference was not statistically significant. Among those
who improved with lignocaine, the beneficial effect continued for at least 2 months in
80% of the patients
Notes Side effects: 2 patients in the lignocaine group and 3 in the saline group complained of
a painful injection or increase of pain for some hours after the injection. Nausea some
hours after the injection occurred in 2 of the patients treated with lignocaine and in 1
patient treated with saline
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Low risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
Low risk
21Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Collee 1991 (Continued)
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear from text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Fuchs 2005
Methods RCT; block randomization, blocks of 6 patients generated by computer
Participants Private orthopedic practice, Goesfeld, Germany
60 patients with chronic non-radicular low-back pain (> 3 months) and with radiologic
confirmation of facet joint osteoarthritis
Interventions Injections into the facet joints at three levels of the lumber spine presumably most affected
by degenerative changes. Injections under CT guidance at weekly intervals. Each patient
received 6 injections.
(1) Injection of 10 mg sodium hyaluronate in 1 ml buffer solution.
(2) Injection of 10 mg glucocorticoids (triamcolone acetonide) in 1 ml crystalline sus-
pension
Outcomes Timing of outcomes: before and 7, 14, 21, 28, 90 and 180 days after randomization.
Both groups improved and had pain relief, better function and improved quality of life.
No statistically significant differences between the groups in outcomes were reported
Notes No adverse effects were reported after administration of both therapies
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk block randomization, blocks of 6 patients
generated by computer
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
High risk
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
Unclear risk unclear from text
22Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
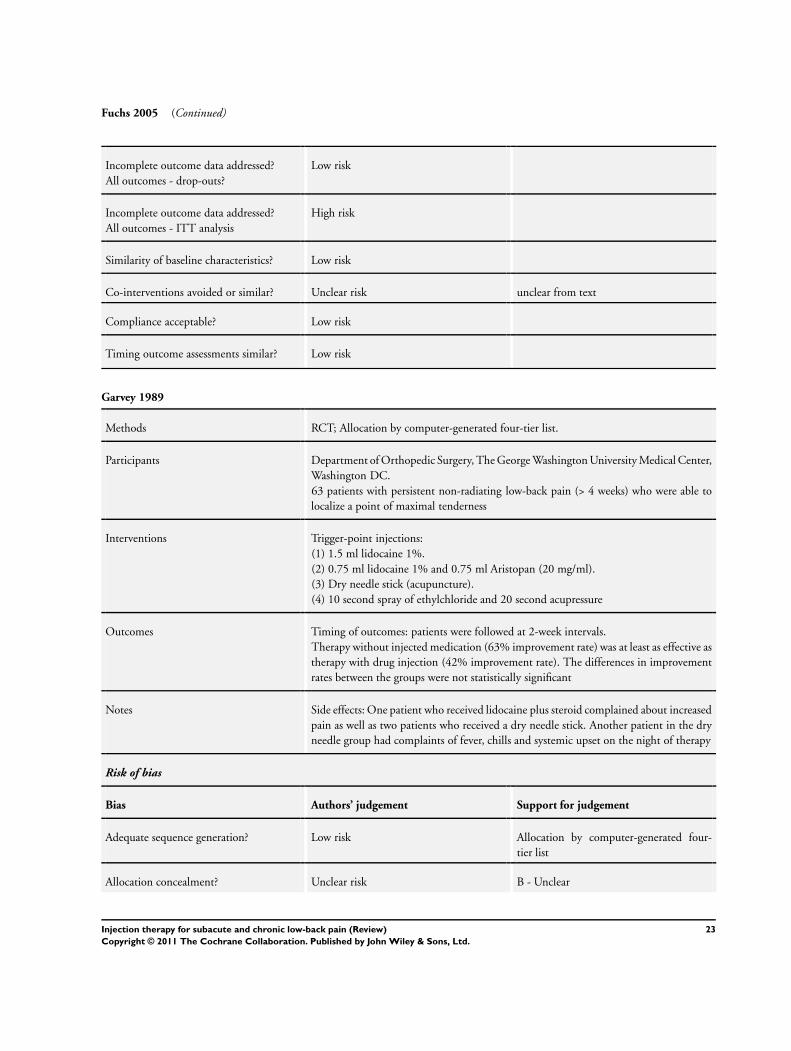
Fuchs 2005 (Continued)
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear from text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Garvey 1989
Methods RCT; Allocation by computer-generated four-tier list.
Participants Department of Orthopedic Surgery, The George Washington University Medical Center,
Washington DC.
63 patients with persistent non-radiating low-back pain (> 4 weeks) who were able to
localize a point of maximal tenderness
Interventions Trigger-point injections:
(1) 1.5 ml lidocaine 1%.
(2) 0.75 ml lidocaine 1% and 0.75 ml Aristopan (20 mg/ml).
(3) Dry needle stick (acupuncture).
(4) 10 second spray of ethylchloride and 20 second acupressure
Outcomes Timing of outcomes: patients were followed at 2-week intervals.
Therapy without injected medication (63% improvement rate) was at least as effective as
therapy with drug injection (42% improvement rate). The differences in improvement
rates between the groups were not statistically significant
Notes Side effects: One patient who received lidocaine plus steroid complained about increased
pain as well as two patients who received a dry needle stick. Another patient in the dry
needle group had complaints of fever, chills and systemic upset on the night of therapy
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Allocation by computer-generated four-
tier list
Allocation concealment? Unclear risk B - Unclear
23Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Garvey 1989 (Continued)
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Low risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
Low risk
Similarity of baseline characteristics? Unclear risk data not provided
Co-interventions avoided or similar? Low risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Unclear risk not clearly stated in text
Lierz 2004
Methods RCT; Randomization performed by computer, no further description of procedure
Participants Department of Anaesthesiology and Intensive Care, Hospital, Soest, Germany
40 patients with low-back pain for at least 6 months.
Interventions Eight single shot epidural blocks at an interval of 2 or 3 days. Active physiotherapy was
performed immediately after each session.
(1) 10 ml ropivacaine 0.2%.
(2) 10 ml bupivacaine 1.125%.
Outcomes Timing of outcomes: before and post-treatment.
Both groups showed no significant differences in analgesia post-treatment
Notes Side effects: no significant differences were reported in hemodynamic variables; there
were three cases of short episodes of headache, two in the ropivacaine group and one in
the bupivacaine group
Risk of bias
Bias Authors’ judgement Support for judgement
24Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
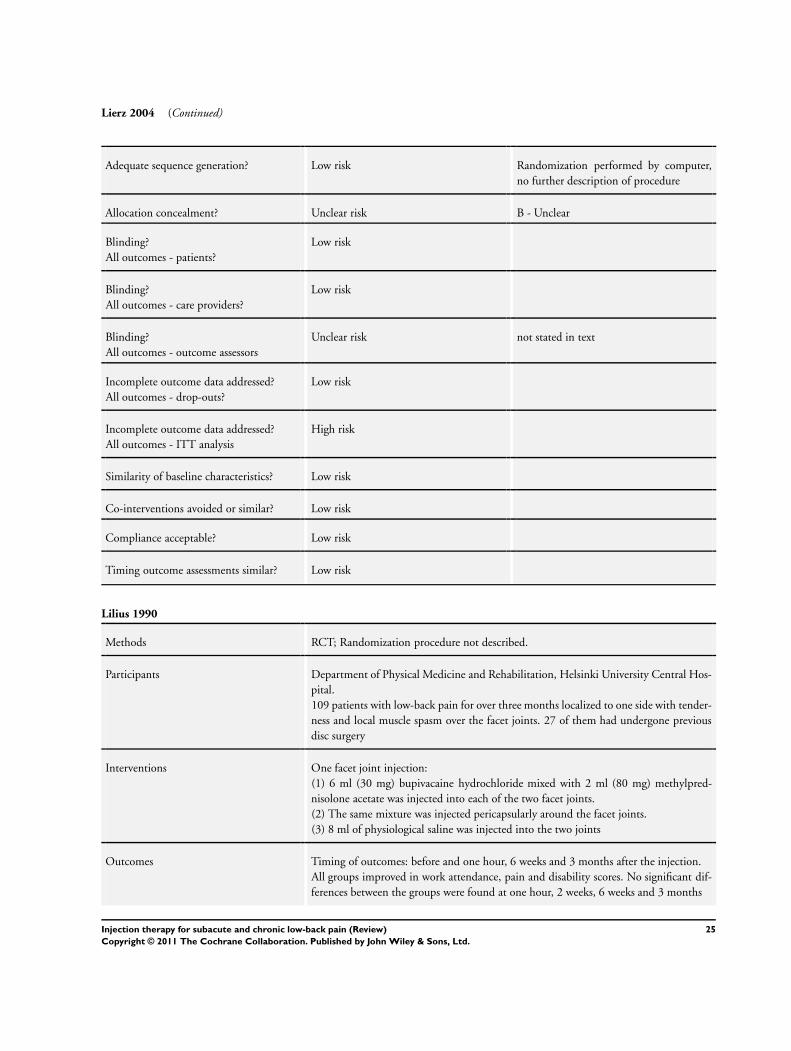
Lierz 2004 (Continued)
Adequate sequence generation? Low risk Randomization performed by computer,
no further description of procedure
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Low risk
Blinding?
All outcomes - outcome assessors
Unclear risk not stated in text
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Low risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Lilius 1990
Methods RCT; Randomization procedure not described.
Participants Department of Physical Medicine and Rehabilitation, Helsinki University Central Hos-
pital.
109 patients with low-back pain for over three months localized to one side with tender-
ness and local muscle spasm over the facet joints. 27 of them had undergone previous
disc surgery
Interventions One facet joint injection:
(1) 6 ml (30 mg) bupivacaine hydrochloride mixed with 2 ml (80 mg) methylpred-
nisolone acetate was injected into each of the two facet joints.
(2) The same mixture was injected pericapsularly around the facet joints.
(3) 8 ml of physiological saline was injected into the two joints
Outcomes Timing of outcomes: before and one hour, 6 weeks and 3 months after the injection.
All groups improved in work attendance, pain and disability scores. No significant dif-
ferences between the groups were found at one hour, 2 weeks, 6 weeks and 3 months
25Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Lilius 1990 (Continued)
Notes Side effects: 7 of the 109 patients reported side effects. The nature of the side effects was
not reported
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
High risk
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
High risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Unclear risk data not provided
Co-interventions avoided or similar? Unclear risk information not provided
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Manchikanti 2001
Methods RCT; Randomization procedure not described.
Participants Private pain management practice in a non-university setting, Paducah, Kentucky.
84 patients with low-back pain with or without lower extremity pain for more than
6 months who did not exhibit neurological deficits and who responded positively to
lidocaine blocks
Interventions (1) Multiple medial branch blocks with a local anesthetic (0.5% lidocaine or 0.25%
bupivacaine) and an equal volume of Sarapin.
(2) Multiple medial branch blocks with a mixture of a local anesthetic (0.5% lidocaine
or 0.25% bupivacaine), an equal volume of Sarapin and 1 mg of methyl prednisolone.
26Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Manchikanti 2001 (Continued)
The injections were given throughout the entire follow-up period
Outcomes Timing of outcomes: before the first injection and at different follow-up moments
throughout a 2.5 years period.
Both groups in improved in pain relief, overall health status, physical, functional and
psychological status and return to work over 2.5 years follow-up. No significant differ-
ences were reported between the groups
Notes Side effects: no complications were reported in any of the patients
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described.
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
High risk
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
Unclear risk unclear in text
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? High risk
Compliance acceptable? Low risk
Timing outcome assessments similar? High risk
27Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Marks 1992
Methods RCT; Random number system, concealment of assigned technique from referring clin-
icians and patients
Participants Pain or back clinic, Dundee, Scotland.
86 patients with lumbar or lumbosacral pain present most of the time for at least 6
months. Exclusion criteria were a radicular pattern in either lower limb, straight leg
raising limited at less than 60 degrees and no evidence of any progressive spinal disorder
of non-degenerative origin
Interventions (1) Facet joint injection with 0.5 ml DepoMedrol (20 mg methylprednisolone acetate)
followed by 1.5 ml lignocaine. (1%) at the lumbosacral level and at every other level 0.
5 ml DepoMedrol followed by 1.0 ml lignocaine.
(2) Facet nerve block of the medial articular branch of the posterior primary ramus from
L1 to L5
Outcomes Timing of outcomes: before and 30-60 minutes, 1 month and 3 months after infiltration.
The facet joints injections did slightly better in relieving pain than the facet nerve blocks.
This difference reached statistical significance only at 1 month but not immediately after
infiltration, at 2 weeks and at 3 months
Notes Side effects: no serious complications. Transient symptoms, such as headache, paresthesia
of one leg, nausea and worsening of pain occurred 15 times in the injection group and
18 times in the nerve block group
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Low risk Random number system
Allocation concealment? Low risk A - Adequate - concealment of assigned
technique from referring clinicians and pa-
tients
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Unclear risk unclear from text
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
28Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Marks 1992 (Continued)
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? High risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Mauro 2000
Methods RCT; Randomization procedure not described.
Participants Outpatient clinic of the department of Orthopedics of Palermo University Hospital,
Palermo, Italy
60 patients with lumbago or sciatic neuritis of mechanical origin without need for surgical
procedures. They had to present with a proven medical history for low-back pain (lasting
from 6 months to 5 years) and a pain intensity of at least 60 mm as evaluated on a visual
analogue scale
Interventions Intramuscular injections once daily for a 2 week period.
(1) 2 ml ampoules containing 1000 mg Vitamin B12 (Tricortin 1000).
(2) 2 ml placebo ampoules.
Outcomes Timing of outcomes: before and 2 weeks after randomization.
At the end of the treatment period there was a statistically significant difference in im-
provement in pain (visual analogue scale) and disability (Roland Disability Question-
naire) in favor of the Vitamin B12 group
Notes Consumption of paracetamol proved significantly higher in the placebo group compared
to the active treatment group. Side effects: No changes in vital signs, or adverse effects
were noted
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described.
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Unclear risk unclear from text
Blinding?
All outcomes - care providers?
Unclear risk unclear from text
29Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Mauro 2000 (Continued)
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
High risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear from text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Mayer 2004
Methods RCT; Assignment based on date of the month of their initial visit alternating with patients
allocated to the other group
Participants Department of Orthopedic Surgery, University of Texas, Southwestern Medical Center,
Dallas, Texas.
70 patients with chronic disabling work-related lumbar spine disorders who had lumbar
rigidity between 1 and 3 levels. The mean length of disability varied from 12 (intervention
group) to 16 months (control group)
Interventions (1) Facet joint injection on one to three levels bilaterally. Each point was injected with a
mixture of 1 ml 2% lidocaine, 1 ml 0.5% bupivacaine and 1 ml of a depot corticosteroid
preparation. In addition, a home stretching exercise program was instructed which was
supervised by physiotherapists on each subsequent visit of the patient (on average twice
a week).
(2) Patients in the control group only received the home stretching exercise program
Outcomes Timing of outcomes: before and post-treatment.
No significant differences were found in pain and disability between the groups. The
group which combined injections with home exercises had a significantly greater im-
provement in range of motion at 5 to 7 weeks compared to the control group
Notes Side effects were not reported by the study authors.
Risk of bias
Bias Authors’ judgement Support for judgement
30Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
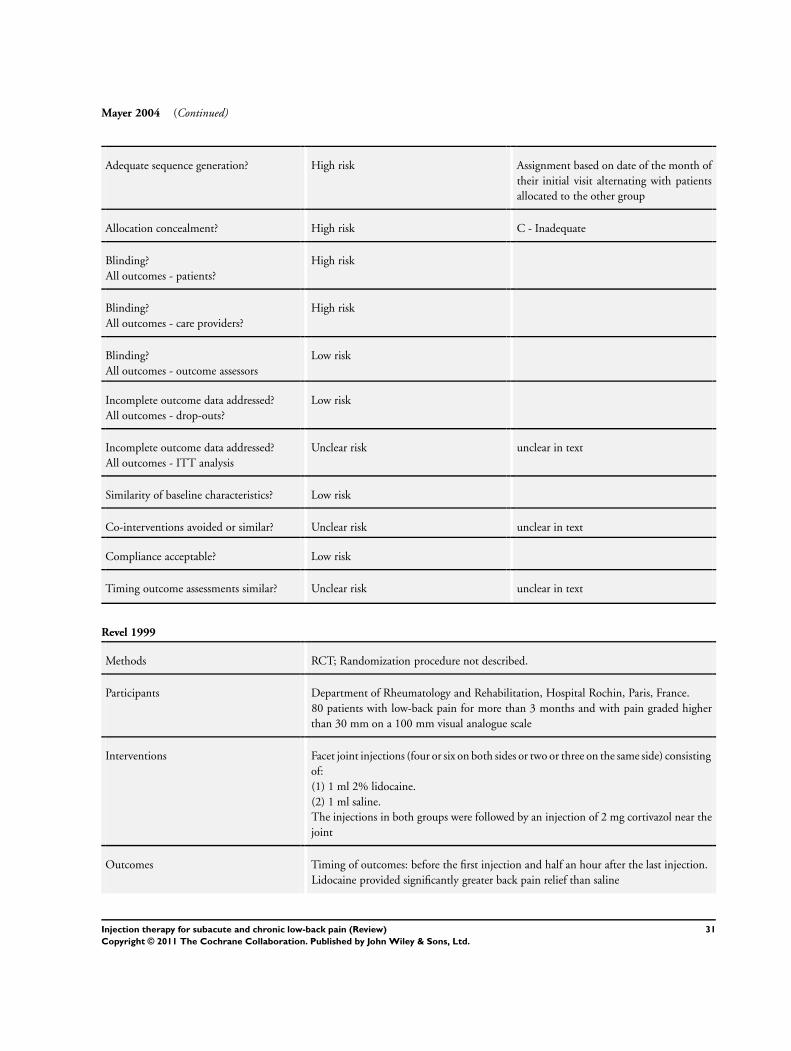
Mayer 2004 (Continued)
Adequate sequence generation? High risk Assignment based on date of the month of
their initial visit alternating with patients
allocated to the other group
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
High risk
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
Unclear risk unclear in text
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear in text
Compliance acceptable? Low risk
Timing outcome assessments similar? Unclear risk unclear in text
Revel 1999
Methods RCT; Randomization procedure not described.
Participants Department of Rheumatology and Rehabilitation, Hospital Rochin, Paris, France.
80 patients with low-back pain for more than 3 months and with pain graded higher
than 30 mm on a 100 mm visual analogue scale
Interventions Facet joint injections (four or six on both sides or two or three on the same side) consisting
of:
(1) 1 ml 2% lidocaine.
(2) 1 ml saline.
The injections in both groups were followed by an injection of 2 mg cortivazol near the
joint
Outcomes Timing of outcomes: before the first injection and half an hour after the last injection.
Lidocaine provided significantly greater back pain relief than saline
31Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Revel 1999 (Continued)
Notes The study was set up from a diagnostic perspective in order to determine clinical criteria
that could be used to identify patients with painful facet joints. Side effects were not
reported by the study authors
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Low risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
Low risk
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear in text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Rocco 1989
Methods RCT; randomization procedure not described.
Participants Pain Treatment Service, Brigham and Women’s hospital Boston.
22 patients who had undergone at least one prior laminectomy and who were still
symptomatic. The duration of pain at study entry was not specified
Interventions Epidural injections which were given at 1 month interval for 3 months:
(1) 1.9 ml (75 mg) triamcinolone diacetate plus 1 ml (50 mg) lidocaine.
(2) 8 ml (8 mg) morphine plus 1 ml (50 mg) lidocaine.
(3) 1.9 ml (75 mg) triamcinolone diacetate plus 8 ml (8 mg) morphine plus 1 ml (50
32Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rocco 1989 (Continued)
mg) lidocaine
Outcomes Timing of outcomes: before randomization, 1 month after randomization and 3 months
after the last injection (6 months after randomization).
No significant differences were reported with regard to pain relief at 1 and 6 months as
measured with a verbal ordinal scale and a visual analogue scale
Notes Side effects: more urinary retention was noted in the triamcinolone plus morphine group.
Nausea, vomiting and pruritis were noted more frequently in the patients given morphine
or triamcolone combined with morphine than in those given triamcolone alone
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk randomization procedure not described.
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
Low risk
Similarity of baseline characteristics? Unclear risk data not provided
Co-interventions avoided or similar? High risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
33Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
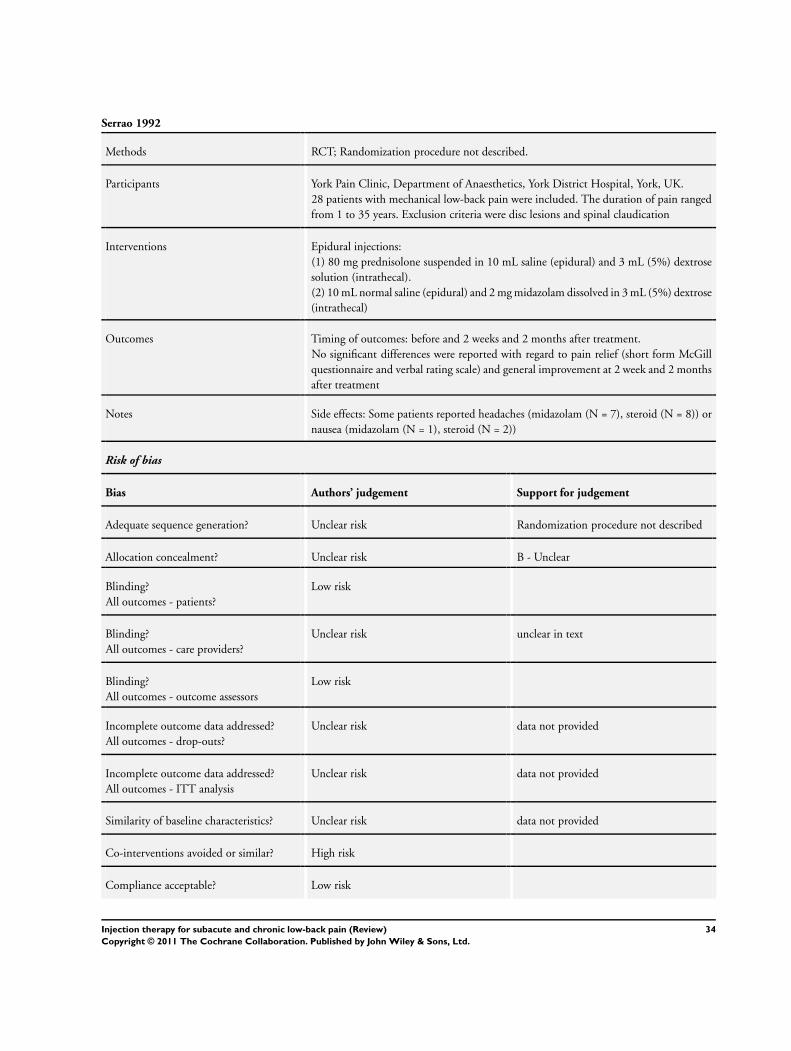
Serrao 1992
Methods RCT; Randomization procedure not described.
Participants York Pain Clinic, Department of Anaesthetics, York District Hospital, York, UK.
28 patients with mechanical low-back pain were included. The duration of pain ranged
from 1 to 35 years. Exclusion criteria were disc lesions and spinal claudication
Interventions Epidural injections:
(1) 80 mg prednisolone suspended in 10 mL saline (epidural) and 3 mL (5%) dextrose
solution (intrathecal).
(2) 10 mL normal saline (epidural) and 2 mg midazolam dissolved in 3 mL (5%) dextrose
(intrathecal)
Outcomes Timing of outcomes: before and 2 weeks and 2 months after treatment.
No significant differences were reported with regard to pain relief (short form McGill
questionnaire and verbal rating scale) and general improvement at 2 week and 2 months
after treatment
Notes Side effects: Some patients reported headaches (midazolam (N = 7), steroid (N = 8)) or
nausea (midazolam (N = 1), steroid (N = 2))
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk Randomization procedure not described
Allocation concealment? Unclear risk B - Unclear
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Unclear risk unclear in text
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Unclear risk data not provided
Incomplete outcome data addressed?
All outcomes - ITT analysis
Unclear risk data not provided
Similarity of baseline characteristics? Unclear risk data not provided
Co-interventions avoided or similar? High risk
Compliance acceptable? Low risk
34Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Serrao 1992 (Continued)
Timing outcome assessments similar? Low risk
Sonne 1985
Methods RCT; randomization procedure not described.
Participants Department of Rheumatology, Bispebjerg Hospital, Copenhagen, Denmark.
30 patients with low-back pain of longer than 1 month duration with the exception of
patients with herniated disc lesions, osteoporosis, arachnoiditis or ankylosing spondylitis
Interventions Local injections at the site of the iliolumbar ligament with a maximum of three injections
give at one week intervals.
(1) 5 mL lignocaine 1% mixed with 1 mL methylprednisolone.
(2) 5 mL isotonic saline.
Outcomes Timing of outcomes: before the study and at each visit and 2 weeks after completing the
study.
No significant differences between the groups in pain (visual analogue scale) and spinal
flexion at each visit and 2 weeks after completing the study. Self-reported improvement
was assessed 2 weeks after completing the study. 9 out of 15 patients in the methyl-
prednisolone group reported a good or excellent improvement compared to 3 out of 14
patients in the saline group which was a significant difference
Notes Side effects were not reported by the study authors.
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? Unclear risk randomization procedure not described.
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
Unclear risk unclear in text
Blinding?
All outcomes - care providers?
High risk
Blinding?
All outcomes - outcome assessors
Low risk
Incomplete outcome data addressed?
All outcomes - drop-outs?
Low risk
Incomplete outcome data addressed?
All outcomes - ITT analysis
High risk
35Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Sonne 1985 (Continued)
Similarity of baseline characteristics? Unclear risk data not provided
Co-interventions avoided or similar? High risk
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Takada 2005
Methods Randomized double blind cross-over study; Randomization procedure not described
Participants Department of Anesthesia, Nagasaki Rosai Hospital, Sasebo, Japan.
16 patients diagnosed as having degenerative spinal disease. The length of the history
of low-back pain ranged from 1 to 24 months. Patients who had a severe canal stenosis
with leg paresis or who had received spinal surgery were excluded from the study
Interventions Single epidural injection with:
(1) 8 ml ropivacaine 0.375%.
(2) 8 ml ropivacaine 0.2%.
(3) 8 ml bupivacaine 0.25%.
Test solutions were given in a randomized order at intervals of one week or more
Outcomes Timing of outcome: before and after epidural blockade.
No significant differences in pain scores (visual analogue scale) after epidural blockade
were found
Notes Side effects: one subject in the 0.375% ropivacaine trial was catheterized because of
bladder distension
Risk of bias
Bias Authors’ judgement Support for judgement
Adequate sequence generation? High risk Randomization procedure not described
Allocation concealment? High risk C - Inadequate
Blinding?
All outcomes - patients?
Low risk
Blinding?
All outcomes - care providers?
Low risk
Blinding?
All outcomes - outcome assessors
Low risk
36Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Takada 2005 (Continued)
Incomplete outcome data addressed?
All outcomes - drop-outs?
Unclear risk data not given
Incomplete outcome data addressed?
All outcomes - ITT analysis
Unclear risk data not given
Similarity of baseline characteristics? Low risk
Co-interventions avoided or similar? Unclear risk unclear in text
Compliance acceptable? Low risk
Timing outcome assessments similar? Low risk
Characteristics of excluded studies [ordered by study ID]
Study Reason for exclusion
Bonetti 2005 Study population consisted of patients with radiculopathy
Bush 1991 Study was about corticosteroid injections for radiculopathy versus placebo
Cuckler 1985 Study was about corticosteroid injections for radiculopathy versus placebo
Dallas 1987 The drugs were administered by means of a catheter and not directly by means of an injection
Fredman 1999 The drugs were administered by means of a catheter and not directly by means of an injection
Glynn 1988 The drugs were administered by means of a catheter and not directly by means of an injection
Hameroff 1981 Patients who had cervical symptoms were also included and no separate results for the lower back were presented
Mathews 1987 Study was about corticosteroid injections for radiculopathy versus placebo
Ney 2006 Study appeared not to be a RCT
Ofluoglu 2007 Study population consisted of patients with osteoporosis
Oh 2004 Radiofrequency denervation was compared with an injection of a small amount of lidocaine which was considered
a sham treatment
Ongley 1987 Study was about the effectiveness of prolotherapy
37Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

(Continued)
Pneumaticos 2006 Two different injection sites were compared and no comparison was made with regard to the type of injection
therapy
Rogers 1992 Study dealt with corticosteroid injections for radiculopathy versus placebo
Simmons 1992 Study was about the effectiveness of intradiscal injections
Stojanovic 2005 Two different needling techniques were compared and no comparison was made with regard to the type of
injection therapy
Tuzun 2003 Study population consisted of acute low-back pain patients
38Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
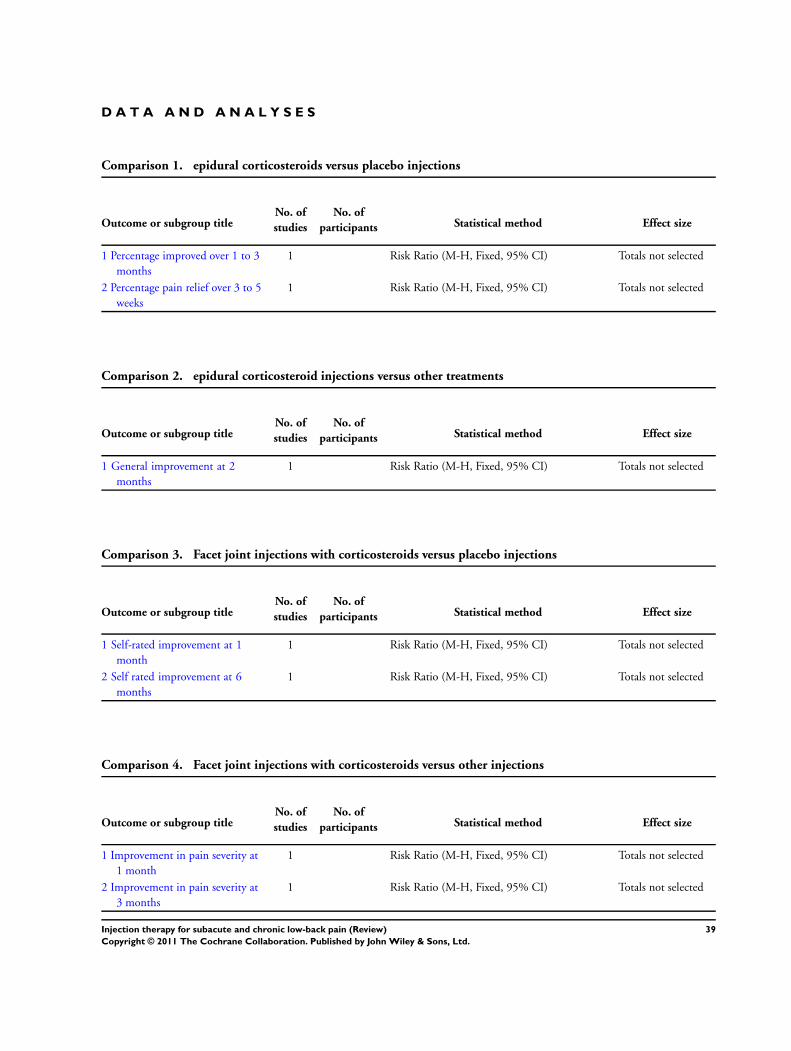
D A T A A N D A N A L Y S E S
Comparison 1. epidural corticosteroids versus placebo injections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Percentage improved over 1 to 3
months
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
2 Percentage pain relief over 3 to 5
weeks
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 2. epidural corticosteroid injections versus other treatments
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 General improvement at 2
months
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 3. Facet joint injections with corticosteroids versus placebo injections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Self-rated improvement at 1
month
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
2 Self rated improvement at 6
months
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 4. Facet joint injections with corticosteroids versus other injections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Improvement in pain severity at
1 month
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
2 Improvement in pain severity at
3 months
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
39Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
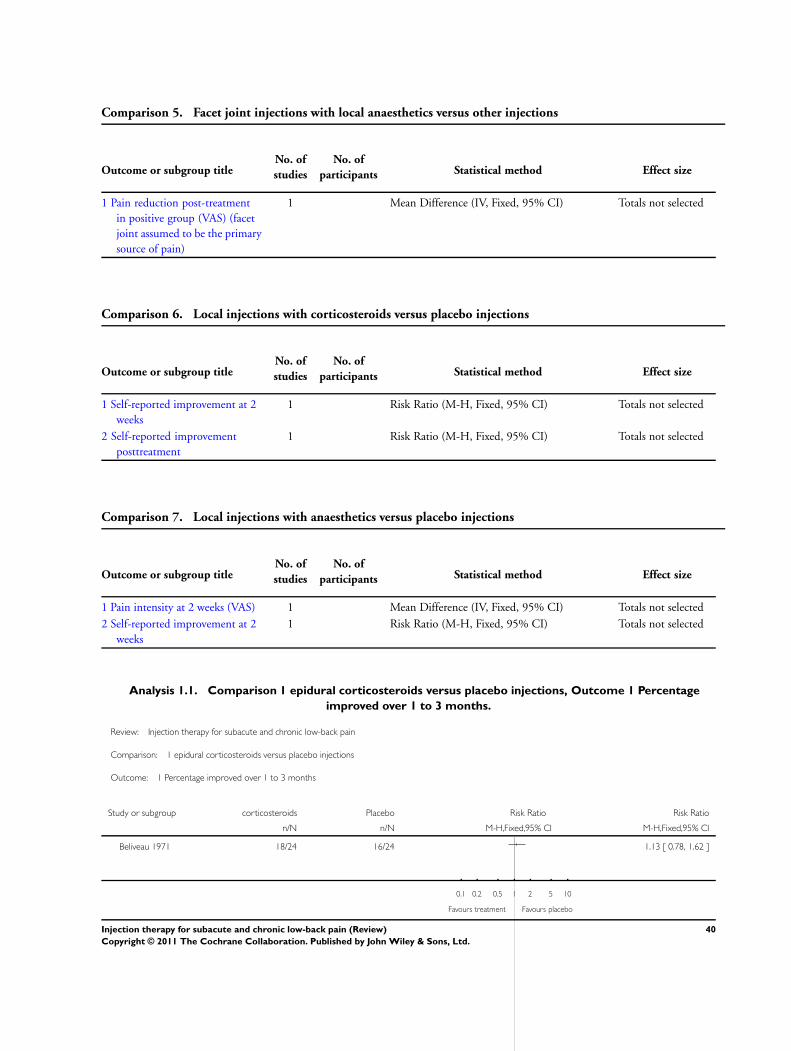
Comparison 5. Facet joint injections with local anaesthetics versus other injections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain reduction post-treatment
in positive group (VAS) (facet
joint assumed to be the primary
source of pain)
1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
Comparison 6. Local injections with corticosteroids versus placebo injections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Self-reported improvement at 2
weeks
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
2 Self-reported improvement
posttreatment
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Comparison 7. Local injections with anaesthetics versus placebo injections
Outcome or subgroup titleNo. of
studies
No. of
participants Statistical method Effect size
1 Pain intensity at 2 weeks (VAS) 1 Mean Difference (IV, Fixed, 95% CI) Totals not selected
2 Self-reported improvement at 2
weeks
1 Risk Ratio (M-H, Fixed, 95% CI) Totals not selected
Analysis 1.1. Comparison 1 epidural corticosteroids versus placebo injections, Outcome 1 Percentage
improved over 1 to 3 months.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 1 epidural corticosteroids versus placebo injections
Outcome: 1 Percentage improved over 1 to 3 months
Study or subgroup corticosteroids Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Beliveau 1971 18/24 16/24 1.13 [ 0.78, 1.62 ]
0.1 0.2 0.5 1 2 5 10
Favours treatment Favours placebo
40Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 1.2. Comparison 1 epidural corticosteroids versus placebo injections, Outcome 2 Percentage pain
relief over 3 to 5 weeks.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 1 epidural corticosteroids versus placebo injections
Outcome: 2 Percentage pain relief over 3 to 5 weeks
Study or subgroup Corticosteroids Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Breivik 1976 10/16 13/19 0.91 [ 0.56, 1.49 ]
0.1 0.2 0.5 1 2 5 10
Favours placebo Favours treatment
Analysis 2.1. Comparison 2 epidural corticosteroid injections versus other treatments, Outcome 1 General
improvement at 2 months.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 2 epidural corticosteroid injections versus other treatments
Outcome: 1 General improvement at 2 months
Study or subgroup Corticosteroids Midazolam Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Serrao 1992 5/14 7/14 0.71 [ 0.30, 1.72 ]
0.1 0.2 0.5 1 2 5 10
Favours Midazolam Favours treatment
41Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 3.1. Comparison 3 Facet joint injections with corticosteroids versus placebo injections, Outcome 1
Self-rated improvement at 1 month.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 3 Facet joint injections with corticosteroids versus placebo injections
Outcome: 1 Self-rated improvement at 1 month
Study or subgroup Favours placebo Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Carette 1991 20/49 16/48 1.22 [ 0.73, 2.07 ]
0.1 0.2 0.5 1 2 5 10
Favours placebo Favours treatment
Analysis 3.2. Comparison 3 Facet joint injections with corticosteroids versus placebo injections, Outcome 2
Self rated improvement at 6 months.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 3 Facet joint injections with corticosteroids versus placebo injections
Outcome: 2 Self rated improvement at 6 months
Study or subgroup Favours placebo Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Carette 1991 46/48 15/47 3.00 [ 1.97, 4.58 ]
0.1 0.2 0.5 1 2 5 10
Favours placebo Favours treatment
42Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 4.1. Comparison 4 Facet joint injections with corticosteroids versus other injections, Outcome 1
Improvement in pain severity at 1 month.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 4 Facet joint injections with corticosteroids versus other injections
Outcome: 1 Improvement in pain severity at 1 month
Study or subgroup Facet injection Facet nerve block Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Marks 1992 27/42 24/44 1.18 [ 0.83, 1.68 ]
0.1 0.2 0.5 1 2 5 10
Favours facet nerve block Favours treatment
Analysis 4.2. Comparison 4 Facet joint injections with corticosteroids versus other injections, Outcome 2
Improvement in pain severity at 3 months.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 4 Facet joint injections with corticosteroids versus other injections
Outcome: 2 Improvement in pain severity at 3 months
Study or subgroup Facet injection Facet nerve block Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Marks 1992 16/41 12/42 1.37 [ 0.74, 2.52 ]
0.1 0.2 0.5 1 2 5 10
Favours Facet nerve block Favours treatment
43Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.1. Comparison 5 Facet joint injections with local anaesthetics versus other injections, Outcome 1
Pain reduction post-treatment in positive group (VAS) (facet joint assumed to be the primary source of pain).
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 5 Facet joint injections with local anaesthetics versus other injections
Outcome: 1 Pain reduction post-treatment in positive group (VAS) (facet joint assumed to be the primary source of pain)
Study or subgroup Lidocaine PlaceboMean
DifferenceMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Revel 1999 42 35.36 (23.6) 38 11.87 (17.44) 23.49 [ 14.45, 32.53 ]
-50 -25 0 25 50
Favours placebo Favours treatment
Analysis 6.1. Comparison 6 Local injections with corticosteroids versus placebo injections, Outcome 1 Self-
reported improvement at 2 weeks.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 6 Local injections with corticosteroids versus placebo injections
Outcome: 1 Self-reported improvement at 2 weeks
Study or subgroup Corticosteroids Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Garvey 1989 4/14 5/13 0.74 [ 0.25, 2.18 ]
0.1 0.2 0.5 1 2 5 10
Favours placebo Favours treatment
44Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 6.2. Comparison 6 Local injections with corticosteroids versus placebo injections, Outcome 2 Self-
reported improvement posttreatment.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 6 Local injections with corticosteroids versus placebo injections
Outcome: 2 Self-reported improvement posttreatment
Study or subgroup Corticosteroids Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Sonne 1985 9/14 3/15 3.21 [ 1.09, 9.51 ]
0.1 0.2 0.5 1 2 5 10
Favours placebo Favours treatment
Analysis 7.1. Comparison 7 Local injections with anaesthetics versus placebo injections, Outcome 1 Pain
intensity at 2 weeks (VAS).
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 7 Local injections with anaesthetics versus placebo injections
Outcome: 1 Pain intensity at 2 weeks (VAS)
Study or subgroup anaesthetics PlaceboMean
DifferenceMean
Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Collee 1991 21 30.5 (26.1) 20 43.8 (27.5) -13.30 [ -29.73, 3.13 ]
-50 -25 0 25 50
Favours treatment Favours placebo
45Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
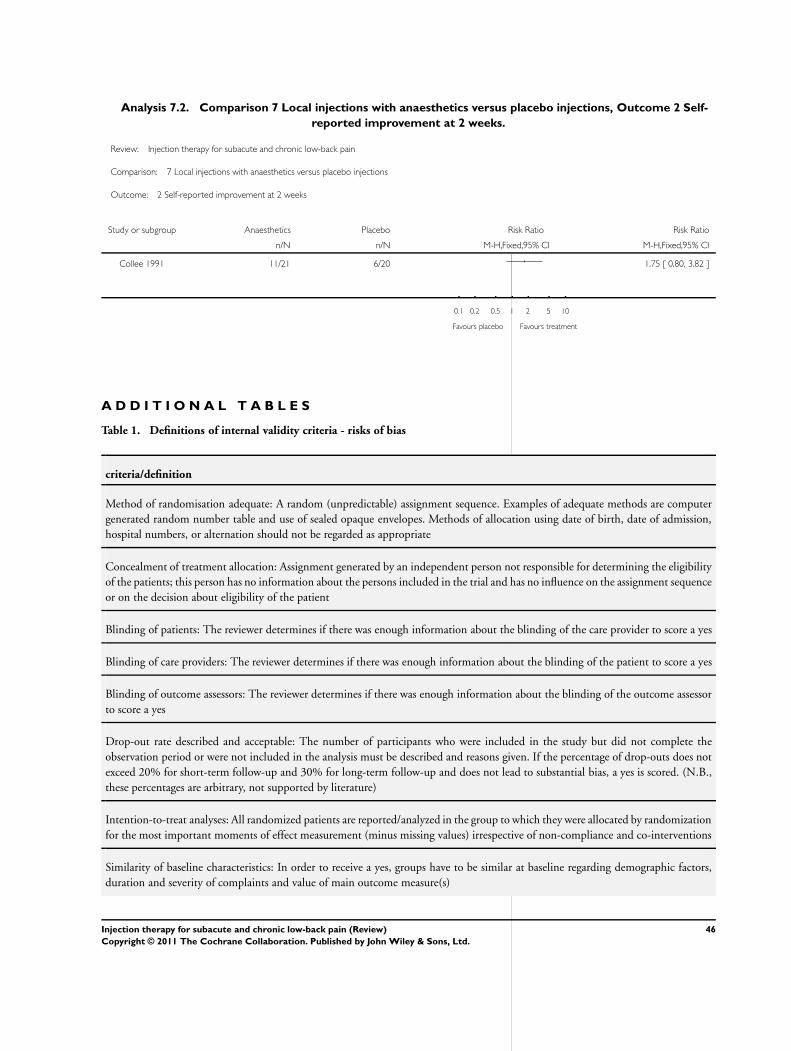
Analysis 7.2. Comparison 7 Local injections with anaesthetics versus placebo injections, Outcome 2 Self-
reported improvement at 2 weeks.
Review: Injection therapy for subacute and chronic low-back pain
Comparison: 7 Local injections with anaesthetics versus placebo injections
Outcome: 2 Self-reported improvement at 2 weeks
Study or subgroup Anaesthetics Placebo Risk Ratio Risk Ratio
n/N n/N M-H,Fixed,95% CI M-H,Fixed,95% CI
Collee 1991 11/21 6/20 1.75 [ 0.80, 3.82 ]
0.1 0.2 0.5 1 2 5 10
Favours placebo Favours treatment
A D D I T I O N A L T A B L E S
Table 1. Definitions of internal validity criteria - risks of bias
criteria/definition
Method of randomisation adequate: A random (unpredictable) assignment sequence. Examples of adequate methods are computer
generated random number table and use of sealed opaque envelopes. Methods of allocation using date of birth, date of admission,
hospital numbers, or alternation should not be regarded as appropriate
Concealment of treatment allocation: Assignment generated by an independent person not responsible for determining the eligibility
of the patients; this person has no information about the persons included in the trial and has no influence on the assignment sequence
or on the decision about eligibility of the patient
Blinding of patients: The reviewer determines if there was enough information about the blinding of the care provider to score a yes
Blinding of care providers: The reviewer determines if there was enough information about the blinding of the patient to score a yes
Blinding of outcome assessors: The reviewer determines if there was enough information about the blinding of the outcome assessor
to score a yes
Drop-out rate described and acceptable: The number of participants who were included in the study but did not complete the
observation period or were not included in the analysis must be described and reasons given. If the percentage of drop-outs does not
exceed 20% for short-term follow-up and 30% for long-term follow-up and does not lead to substantial bias, a yes is scored. (N.B.,
these percentages are arbitrary, not supported by literature)
Intention-to-treat analyses: All randomized patients are reported/analyzed in the group to which they were allocated by randomization
for the most important moments of effect measurement (minus missing values) irrespective of non-compliance and co-interventions
Similarity of baseline characteristics: In order to receive a yes, groups have to be similar at baseline regarding demographic factors,
duration and severity of complaints and value of main outcome measure(s)
46Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 1. Definitions of internal validity criteria - risks of bias (Continued)
Co-interventions avoided or similar: Co-interventions should either be avoided in the trial design or comparable between the index
and control groups
Compliance acceptable: The reviewer determines if the compliance to the interventions is acceptable, based on the reported intensity,
duration, number, and frequency of sessions for both the index intervention(s) and control intervention(s)
Timing outcome assessments similar: Timing of outcome assessment be identical for all intervention groups and for all important
outcome assessments
Table 2. Clinical Relevance questions
questions
A) Are the patients described in detail so that you can decide whether they are comparable to those that you see in your practice?
B) Are the interventions and treatment settings described well enough so that you can provide the same for your patients?
C) Were all clinically relevant outcomes measured and reported?
D) Is the size of the effect clinically important? We considered a 20 % improvement in pain scores (Salaffi 2004) and a 10%
improvement in functioning outcomes (Bombardier 2000) to be clinically important.
E) Are the likely treatment benefits worth the potential harms?
Table 3. Clinical relevance
reference A B C D E
Aldrete 2003 - + + - -
Beliveau 1971 ? + ? - -
Breivik 1976 + + + + ?
Carette 1991 + + + - -
Collee 1991 + + - - -
Fuchs 2005 + + + - -
Garvey 1989 - + - - -
Lierz 2004 ? + - - -
Lilius 1990 + + + - ?
Manchikanti 2001 - + + - -
47Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Table 3. Clinical relevance (Continued)
Marks 1992 + + - - -
Mauro 2000 + ? + + +
Mayer 2004 + + + - -
Revel 1999 + + - + +
Rocco 1989 - + - - -
Serrao 1992 + + + - -
Sonne 1985 - - + + -
Takada 2005 - + - - ?
A P P E N D I C E S
Appendix 1. Search Strategies
PubMed
Phase1: (randomized controlled trial[pt] OR controlled clinical trial[pt] OR randomized controlled trials[mh] OR random allo-
cation[mh] OR double-blind method[mh] OR single-blind method[mh] OR clinical trial[pt] OR clinical trials[mh] OR “clinical
trial”[tw]) OR ((single*[tw] OR doubl*[tw] OR trebl*[tw] OR tripl*[tw]) AND (mask*[tw] OR blind*[tw])) OR (“latin square”[tw])
OR placebos[mh] OR placebo*[tw] OR random*[tw] OR research design[mh:noexp] OR comparative study[mh] OR evaluation
studies[mh] OR follow-up studies[mh] OR prospective studies[mh] OR cross-over studies[mh] OR control*[tw] OR prospective*[tw]
OR volunteer*[tw] NOT (animal[mh] NOT human[mh])
Phase 2: (low back pain OR backache[tw] OR Lumbago[tw])
Phase 3: (injections) OR (injection) OR (chemonucleolysis) OR (rhizotomy) OR (facet denervation) OR (thermolesions)
Phase 4: 1 AND 2 AND 3
EMBASE
#1 clinical article
#2 clinical study
#3 clinical trial
#4 controlled study
#5 randomized controlled trial
#6 major clinical study
#7 double blind procedure
#8 multicentre study
#9 single blind procedure
#10 crossover procedure
#11 placebo
#12 (1 or 2 or 3 or 4 or 5 or 6 or 7 or 8 or 9 or 10 or 11)
#13 allocat$
#14 assign$
48Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

#15 blind$
#16 (clinic$ adj25 (study or trial))
#17 compar$
#18 control$
#19 cross?over
#20 factorial$
#21 follow?up
#22 placebo$
#23 prospectiv$
#24 random$
#25 ((singl$ or doubl$ or trebl$ or tripl$) adj25 (blind$ or mask$))
#26 trial
#27 (versus or vs)
#28 (13 or 14 or 15 or 16 or 17 or 18 or 19 or 20 or 21 or 22 or 23 or 24 or 25 or 26 or 27 or 28)
#29 (12 or 28)
#30 human
#31 nonhuman
#32 animal
#33 animal experiment
#34 (31 or 32 or 33)
#35 (30 and 34)
#36 (29 not 34)
#37 (29 and 35)
#38 (36 or 37)
#39 low back pain
#40 backache
#41 lumbago
#42 (#39 or #40 or #41)
#43 injection
#44 injections
#45 chemonucleolysis
#46 rhizotomy
#47 facet denervation
#48 thermolesion
#49 (#43 or #44 or #45 or #46 or #47 or #48)
#50 (#49 and #42 and #38)
W H A T ’ S N E W
Last assessed as up-to-date: 29 March 2007.
Date Event Description
19 January 2011 Amended Contact details updated.
49Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

H I S T O R Y
Protocol first published: Issue 3, 1996
Review first published: Issue 4, 1999
Date Event Description
23 November 2009 Amended Contact details updated.
12 May 2008 Amended converted to new review format
12 May 2008 New citation required but conclusions have not
changed
This review is an update of a previously withdrawn
review. In an attempt to increase clinical homogene-
ity, the withdrawn review was split, and the current
review no longer contains trials on the effects of in-
tradiscal therapy, prolotherapy, or epidural steroids for
radiculopathy due to disc herniation. These are topics
of current or future Cochrane reviews
As before, the review authors concluded that there was
insufficient evidence to support the use of injection
therapy in subacute and chronic low-back pain. How-
ever, it cannot be ruled out that specific subgroups of
patients may respond to a specific type of injection
therapy
12 May 2008 New search has been performed The search was updated and eight new RCTs were
included for the scope of the current review.
In the current review, the internal validity of the RCTs
was measured using the eleven criteria outlined in the
2003 Updated Cochrane Back Review Group method
guidelines. Half of the RCTs were rated as having a
low risk of bias
25 January 2006 New citation required but conclusions have not
changed
Review was withdrawn from publication because it was
out of date
C O N T R I B U T I O N S O F A U T H O R S
Bart Staal and Rob de Bie updated the searches for new trials, conducted the study selection, quality assessment, data extraction and
analysis of all new studies. Patty Nelemans and Rob de Bie conducted the study selection, quality assessment, data extraction and analysis
of all studies included in the original review. Bart Staal drafted the present manuscript. All authors critically revised and approved the
manuscript.
50Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D E C L A R A T I O N S O F I N T E R E S T
None declared
I N D E X T E R M SMedical Subject Headings (MeSH)
Anesthesia, Conduction; Anesthetics [∗administration & dosage]; Anti-Inflammatory Agents [∗administration & dosage]; Chronic
Disease; Glucocorticoids [∗administration & dosage]; Injections, Intra-Articular; Injections, Spinal [∗methods]; Low Back Pain [∗drug
therapy]; Randomized Controlled Trials as Topic; Steroids
MeSH check words
Humans
51Injection therapy for subacute and chronic low-back pain (Review)
Copyright © 2011 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.