cme/moc chair's take: her2-targeted and other agents for
TRANSCRIPT

PeerView.com/GZH900
David H. Ilson, MD, PhDMemorial Sloan Kettering Cancer Center Weill Cornell Medical College New York, New York
Chair
Participate in interactive questions, download activity slides, and obtain your instant CME/MOC credit online.
This CME/MOC activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
CME/MOC
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer

PeerView.com/GZH900 2Go online to complete the post-test and evaluation for CME/MOC credit
Activity Information
Media: Enduring MaterialAccredited Activity Release Date: June 17, 2020Accredited Activity Expiration Date: June 16, 2021Time to Complete Activity: 30 minutes
Activity Description In this activity, an expert oncologist reviews the latest evidence and recent developments in gastric cancer care, including innovative targeted therapeutics, and offers strategies to optimally navigate patient care and integrate novel therapeutics into treatment plans.
Target Audience This activity has been designed to meet the educational needs of oncologists and other clinicians involved in the management of gastric cancer.
Educational Objectives Upon completion of this activity, participants should be better able to:• Describe the biologic rationale for therapeutic targeting of gastric cancer, such
as HER2 or PD-L1 overexpression• Summarize expert and guideline-based recommendations to accurately test
for biomarkers in gastric cancer that can guide appropriate treatment selection• Appraise the latest safety and efficacy data of established and emerging
therapeutics for gastric cancer, such as checkpoint inhibitors, novel cytotoxic agents, and HER2-directed antibody-drug conjugates
• Select appropriate validated or emerging therapeutic strategies for advanced gastric/GEJ cancers based on treatment history, patient preference, performance status, and biomarker status for patients who have progressed following first-line treatment
Providership, Credit, and SupportThis CME/MOC activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
This activity is supported by independent educational grants from AstraZeneca and Daiichi Sankyo, Inc.
Physician Continuing Medical EducationThis activity has been planned and implemented in accordance with the accreditation requirements and policies of the Accreditation Council for Continuing Medical Education (ACCME) through the joint providership of
Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education. The Medical Learning Institute, Inc. is accredited by the ACCME to provide continuing medical education for physicians.
The Medical Learning Institute, Inc. designates this enduring material for a maximum of 0.5 AMA PRA Category 1 CreditTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
MOC StatementSuccessful completion of this CME activity, which includes participation in the evaluation component, enables the participant to
earn up to 0.5 MOC points and patient safety MOC Credit in the American Board of Internal Medicine’s (ABIM) Maintenance of Certification (MOC) program. Participants will earn MOC points equivalent to the amount of CME credits claimed for the activity. It is the CME activity provider’s responsibility to submit participant completion information to ACCME for the purpose of granting ABIM MOC credit.
Participation information will be shared with ABIM through the ACCME’s Program and Activity Reporting System (PARS). Blinded individual or aggregated participant data may be shared with the funder of the activity.
Faculty DisclosuresChair David H. Ilson, MD, PhD Attending Physician Memorial Sloan Kettering Cancer Center Professor of Medicine, Weill Cornell Medical College New York, New York
David H. Ilson, MD, PhD, has a financial interest/relationship or affiliation in the form of: Consultant and/or Advisor for Astellas Pharma Inc.; AstraZeneca; Bayer Corporation; Bristol Myers Squibb; Eli Lilly and Company; F. Hoffmann-La Roche Ltd; Merck & Co., Inc.; Pieris Pharmaceuticals, Inc.; and Taiho Oncology, Inc. Grant/Research Support from Astellas Pharma Inc. and Taiho Oncology, Inc.
Planning Committee DisclosuresThe planners from Medical Learning Institute, Inc., the accredited provider, and PeerView Institute for Medical Education, the joint provider, do not have any financial relationships with an ACCME-defined commercial interest related to the content of this accredited activity during the past 12 months unless listed below.
Content/Peer Reviewer DisclosuresThe following Content/Peer Reviewers have nothing to disclose:
Amita B. Patel, MSN, RN, AOCNP, NP-CGina D. Cravey, BSN, RN, CHRC, CCRC
Disclosure of Unlabeled UseThis educational activity may contain discussions of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
DisclaimerParticipants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient's conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer's product information, and comparison with recommendations of other authorities.
Method of Participation There are no fees for participating in or receiving credit for this accredited activity. For information on applicability and acceptance of continuing education credit for this activity, please consult your professional licensing board.
A statement of credit will be issued only upon receipt of a completed activity evaluation form and will be emailed to you upon completion. You will receive your certificate from [email protected]. If you have questions regarding the receipt of your emailed certificate, please contact via email at [email protected].
In order to receive credit, participants must view the activity and complete the post-test and evaluation form. A score of 70% or higher is needed to obtain MOC credit. There are no prerequisites and there is no fee to participate in this activity or to receive MOC credit. Statements of Credit are awarded upon successful completion of the post-test and evaluation form.
About This CME/MOC ActivityPVI, PeerView Institute for Medical Education, and Medical Learning Institute, Inc. are responsible for the selection of this activity’s topics, the preparation of editorial content, and the distribution of this activity. Our activities may contain references to unapproved products or uses of these products in certain jurisdictions. The preparation of PeerView activities is supported by educational grants subject to written agreements that clearly stipulate and enforce the editorial independence of PVI and Medical Learning Institute, Inc.
The materials presented here are used with the permission of the authors and/or other sources. These materials do not necessarily reflect the views of PeerView or any of its partners, providers, and/or supporters.

PeerView.com/GZH900 3Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
Dr. Ilson: Hello and welcome to “Chairs Take: HER2-Targeted and Other Agents for Gastric Cancer.” I’m Dr. David Ilson from Memorial Sloan Kettering Cancer Center. During this presentation today, I will be providing a brief overview of recent developments on targeted therapies in gastric cancer, including the latest evidence presented at the 2020 ASCO Annual Meeting (ASCO 2020), and helping to interpret what these data mean to our patients.
• Third leading cause of cancer death globally
• Wide geographical variation – 50% of new cases occur
in developing countries • Worldwide: over 1 million new cases and
783,000 deaths (equating to 1 in every 12 deaths globally)
• In the United States, 27,600 new diagnoses and ~11,000 deaths annually
• Poor prognosis in metastatic disease (median OS 1 y)
Gastric Adenocarcinoma1
1. Bray F et al. CA Cancer J Clin. 2018;68:394-424.
32.1 17.1
12.7 11.3 10.4 10.1
8.7 8.2 8.1 7.9 7.8 7.2 6.4 6.2 5.6 5.4 5.4 4.9 4.7 4.7 3.0
4.0 3.8 2.6 4.0
2.8 3.1 2.9 3.5 4.0 4.1 6.3
3.7 5.1 6.4
5.0 6.0 6.9 7.5
13.2
60 40 20 0 20 40 60Age-Standardized (W) Incidence Rate per 100,000
Eastern Asia Eastern Europe South America
Western Asia Southern Europe
Melanesia Caribbean
Western Europe Central America
Micronesia/Polynesia South-Eastern Asia South Central Asia
Australia/New Zealand Northern Europe
Northern America Middle Africa
Southern Africa Western Africa Eastern Africa
Northern Africa
Korea, Republic of
Korea, Republic of
Stomach
Males Females
Gastric cancer is the third leading cause of cancer globally, and we can see from this slide that geographic incidence varies tremendously. We see the highest relative incidence in Eastern Asia, Eastern Europe, and South America, but we can see that in North America this is a relatively uncommon disease. Worldwide, over a million new cases will be diagnosed each year and 783,000 deaths. In the United States, we’ll see nearly 28,000 new diagnoses annually and about 11,000 deaths. Metastatic disease has a poor prognosis, with a median overall survival (OS) of only 1 year.
Oxali: EOX or
EOF
Cape: ECX or
EOX XP FLO FOLFIRI FUFIRI S-1 Cis DCF ECF
Pts 489 513 160 109 209 170 305 221 126
RR, % 44% 45% 41% 34% 39% 32% 54% 36% 45%
TTP, mo 6.7 6.5 5.6 5.5 5.3 5.0 6.0 5.6 7.4
OS, mo 10.9 10.4 10.5 10.7 9.5 9.0 13.0 9.2 8.9
1. Cunningham D et al. N Engl J Med. 2008;358:36-46. 2. Kang Y-K et al. Ann Oncol. 2009;20:666-673. 3. Al-Batran S-E et al. J Clin Oncol. 2008;26:1435-1442. 4. Dank M et al. Ann Oncol. 2008;19:1450-1457. 5. Koizumi W et al. Lancet Oncol. 2008;9:215-221. 6. Van Cutsem E et al. J Clin Oncol. 2006;24:4991-4997. 7. Webb A et al. J Clin Oncol. 1997;15:261-267.
Advanced Esophagogastric Cancer Chemotherapy: What Regimen to Use?1-7
So when we treat advanced esophageal gastric cancer, what’s the optimal chemotherapy regimen to use? I always include this slide in my talks because it reviews across the board phase 3 trials from two-drug and three-drug regimens. On the right side of the slide, you see the data for the triplet DCF and ECF regimens,
with response rates in the 35% to 45% range. However, two-drug regimens—particularly FOLFOX, FOLFIRI, and capecitabine/platinum-based regimens—also have response rates in a similar range. And if we look across the board at time to tumor progression, it’s virtually identical for these different regimens, and OS ranges from 9 to 10 months. Most patients are going to be best served with two-drug chemotherapy, both in terms of effectiveness and survival outcomes.
1. Yamada Y et al. Lancet Gastroenterol Hepatol. 2019;4:501-510.
Phase 3 JCOG1013 Study: Triplet Chemo With S-1 and Cisplatin Plus Docetaxel Versus Doublet Chemo With S-1 and Cisplatin1
Primary Endpoint: OS
No. at Risk (Censored) CS 371 (0) 319 (0) 228 (0) 143 (0) 83 (9) 57 (8) 35 (7) 18 (6) 10 (1) 6 (4) 4 (1) 6 (4)
DCS 370 (0) 321 (0) 221 (0) 143 (0) 85 (13) 55 (10) 31 (7) 12 (8) 4 (5) 3 (1) 0 (3) 0 (0)
Prop
ortio
n Su
rviv
ing
Time Since Randomization, mo
00.10.20.30.40.50.60.70.80.9
1
0 6 12 18 24 30 36 42 48 54 60 66
1.0
CS DCS
1-y OS, % (95% Cl) 61.5 (56.3-66.2) 59.7 (54.5-64.5)
Median OS, mo (95% Cl) 15.3 (14.2-16.2) 14.2 (12.9-15.9)
HR (95% Cl) 0.99 (0.85-1.16) P .47 ORR, % 56.0 59.3
– CS – DCS
And recently from Japan, we had a pivotal trial that looked at triplet chemotherapy with S-1, cisplatin, and docetaxel versus doublet chemotherapy with S-1 and cisplatin. OS was the primary endpoint. This trial treated over 700 patients with advanced gastric cancer, and you can see clearly that the primary endpoint, OS, was no different for two-drug versus three-drug chemotherapy. The hazard ratio on this trial was 0.99. To me, this is the most definitive evidence that two-drug therapy should be the standard of care, both to optimize not only effectiveness but also patient tolerance.
1. Adapted from Cancer Genome Atlas Network. Nature. 2014;513:202-209.
Molecular Classification Scheme for Gastric Adenocarcinoma1
50%
22%
20%
9% Tumor numbers
EBV (EBV-CIMP)
26
MSI (hypermutated)
64
GS
58
295
269
205
CIN (chrom instability)
147
Now we have molecular classification of gastric cancer to try and get us beyond conventional chemotherapy alone, looking at molecular targets that we can exploit for new drug development. This is the breakdown from The Cancer Genome Atlas, where

PeerView.com/GZH900 4Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
they studied 295 fresh frozen gastric and GEJ cancer biopsies. They identified four subgroups that could be classified based on genomic profiling. The most common, on the bottom, was chromosomally unstable tumors. This accounted for 50% of gastric cancers and nearly 95% of GEJ cancers. Then the other less common subtypes included genomically stable cancers. This corresponds to the more diffuse subtype of gastric cancer, and this subtype is relatively genomically bland with very few, if any, targetable mutations. Then we have a significant percentage of MSI-high or microsatellite-unstable tumors. In this series, it was 22%, but more realistically it ranges from 5% to 10%. And then lastly, about 9% to 10% of gastric cancers are associated with Epstein-Barr virus (EBV) infection.
Molecular Features of Subtypes of Gastric Adenocarcinoma1
Subtype EBV MSI GS CIN
Typical molecular features
• EBV+ • Profound hyper-
methylation • CDKN2A silencing • 80% PIK3CA mutation • PD-L1/2
overexpression
• DNA hyper-methylation
• Silencing of MLH1 • Elevated somatic
mutations (PIK3CA 42% and ERBB3 26%)
• PD-L1/2 overexpression
• Tumors lacking aneuploidy and elevated rates of mutation or hyper-methylation
• Somatic RHOA and CDH1 mutations
• CLDN18-ARHGAP6 or -ARHGAP26 fusion
• Marked aneuploidy • TP53 mutations • Recurrent
amplifications of receptor tyrosine kinases (HER2 24%)
Association with anatomy or traditional subtypes
Fundus and body Fundus, body, and antrum Mostly diffuse subtype
More common at the GEJ with intestinal
phenotype
1. Kankeu Fonkoua L, Yee NS. Biomedicines. 2018;6.
This shows the molecular features of the subtypes of gastric adenocarcinoma. The EBV subtype, again, which is about 9% to 10%, has common presence of PIK3CA mutations but also a high expression of PD-L1 and PD-L2. MSI-high patients have a high mutation burden because of silencing of MLH1, and they also have relatively high rates of expression of PD-L1 and PD-L2. Both MSI-high and EBV-associated gastric cancers may be better candidates for immune checkpoint inhibitor therapy. As I said earlier, genomically stable tumors, which are more diffuse type gastric cancers, generally have a paucity of mutations. And then lastly, the most common subtype, chromosomally unstable gastric cancers have a common presence of receptor-associated tyrosine kinase amplification and, most importantly, HER2, which is present in 24% of patients.
1. Kankeu Fonkoua L, Yee NS. Biomedicines. 2018;6.
TCGA: Four Genomic Subsets With Therapeutic Implications1
Nature 24: 2903; 2014
Genomically unstable (50% gastric, 95% GEJ): TP53 mutation, RTK amplification • RTK: HER2 only success • Failed trials targeting MET first
line in MET+, EGFR first/second/third line in unselected patients
MSI high (22%, GEJ <1%) • Immune checkpoint inhibitors • Approved for refractory
MSI- high cancers; may benefit first line (KN-62)
Genomically stable (20%) • Not clearly targetable
EBV (8%) • PIK3CA, immune checkpoint
inhibitors
What are the therapeutic implications of the molecular subtypes? Again, the MSI-high and EBV-associated cancers made be good candidates for immune checkpoint inhibitor therapy. The genomically unstable tumors, again with the receptor-associated tyrosine kinase amplification, may be candidates for targeted therapies. But to date HER2 is the only success. There have been failed trials targeting the MET pathway first-line, as well as EGFR not only in the first but in the second and third-line setting. And again, genomically stable tumors have not had clearly identifiable targets to develop new drugs to date.
HER2 Expression in Gastric/GEJ Cancer1-5
Incidence of HER2 Expression by IHC or FISH
All GC tumors ── 13%-23%
Histology Intestinal Diffuse
16%-34% 6%-7%
Primary tumor location GEJ Gastric
25%-34% 9%-20%
1. Bang YJ et al. Lancet. 2010;6736:61121-61132. 2. Gravalos C et al. Ann Oncol. 2008;19:1523-1529. 3. Yano T et al. J Clin Oncol. 2004;22(14 suppl): Abstract 4053. 4. Gravolos C et al. ASCO GI. Abstract 89. 5. Lordick F et al. Eur J Cancer Suppl. 2007;5(4): Abstract 3541.
So let’s shift the focus now to HER2-positive gastric cancer. HER2 expression in gastric and GEJ cancers is significant. Across the board, anywhere from 13% to 23% of these cancers are HER2-positive. We can see that intestinal cancers are more commonly HER2-positive, 15% to 34% compared with only 6% to 7% of diffuse gastric cancers. And again, GEJ cancers and esophageal adenocarcinomas have 25% to 35% rates of HER2 positivity compared with about 10% to 20% for more distal gastric cancers.
1.0
0.8
0.6
0.4
0.2
0.0 36 34 32 30 28 26 24 22 20 18 16 14 12 10 8 6 4 2 0
Time, mo
11.8 16.0
FC + T FC
Events
120 136
HR
0.65
95% CI
0.51-0.83
Median OS
16.0 11.8
0.1
0.3
0.5
0.7
0.9
Prob
abili
ty o
f Sur
viva
l
HER2+
HER2-
• Phase 3, randomized, multicenter international trial • Patients with advanced gastric or GEJ adenocarcinoma
1. Bang YJ et al. Lancet. 2010;376:687.
ToGA Trial (Trastuzumab): Clinical Benefit in High Expressors (IHC 3+, 2+/FISH+) in First-Line Setting1
HER2 is a key target in gastric cancer. Trastuzumab was validated as an active drug in HER2-positive gastric cancer from the ToGA trial. This randomized trial showed clinical benefit in first-line therapy for combining trastuzumab with chemotherapy compared with chemotherapy alone, but a particular survival improvement for high expressers that were either IHC 3+ or 2+ and FISH-positive. In this subgroup of patients, which was 75% of patients treated on the trial, we achieved a 5-month improvement in median OS with the addition of trastuzumab.

PeerView.com/GZH900 5Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
Benefit Limited to IHC 3+ or IHC 2+ FISH +1
1. Bang YJ et al. Lancet. 2010;376:687.
HR (95% Cl) Patients, n
Median OS, mo HR (95% Cl)
All preplanned exploratory analysisa
584 13.8 vs 11.1 0.74 (0.60-0.91)
IHC 0/FISH positive 61 10.6 vs 7.2 0.92 (0.48-1.76)
IHC 1+/FISH positive 70 8.7 vs 10.2 1.24 (0.70-2.20)
IHC 2+/FISH positive 159 12.3 vs 10.8 0.75 (0.51-1.11)
IHC 3+/FISH positive 256 17.9 vs 12.3 0.58 (0.41-0.81)
IHC 3+/FISH negative 15 17.5 vs 17.7 0.83 (0.20-3.38) Post-hoc exploratory analysisb
IHC 0 or 1+/FISH positive 131 10.0 vs 8.7 1.07 (0.70-1.62)
IHC 2+/FISH positive or IHC 3+ 446 16.0 vs 11.8 0.65 (0.51-0.83)
0.2 0.4 0.6 1 2 3 4 5
Favors trastuzumab plus chemotherapy Favors chemotherapy alone
And this next slide again highlights on a forest plot that the subsets that benefit from the addition of trastuzumab to chemotherapy include the IHC 3+ patients and the IHC 2+/FISH-positive. If we look at the bottom of the forest plot, we can see that if we’re only FISH-positive without IHC or IHC 1 that trastuzumab does not benefit, and we do see survival benefits again for the IHC 2+/FISH-positive or for the IHC 3+ plus subgroup of patients.
HER2-Targeted Agents: Esophagogastric Cancer Is Not Breast Cancer
First-Line Trials
• JACOB: capecitabine/cisplatin/trastuzumab ± pertuzumab (N = 780)1
– OS 17.5 vs 14.2 months; HR: 0.84; P = .056 • HELOISE: capecitabine/cisplatin + two dose levels of trastuzumab
(N = 400)2
• LOGiC: capecitabine/oxaliplatin + lapatinib (N = 545)3 – No difference in OS (12.2 vs 10.5 months; HR: 0.91)
1. Tabernero J et al. Lancet Oncol. 2018;19:1372-1384. 2. Shah M et al. J Clin Oncol. 2017;35:2558-2567. 3. Randolph Hecht J et al. J Clin Oncol. 2016;34:443-451.
So we know clearly from recent studies that esophagogastric cancer is not breast cancer. Drugs that are active in HER2-positive breast cancer in first and second line, unfortunately, are not similarly active in HER2-positive gastric cancer. One of the most disappointing trials was JACOB. This was a 780-patient, first-line trial looking at capecitabine/cisplatin alone, plus trastuzumab with or without the addition of pertuzumab, or dual-targeted therapy. Although there was a trend towards improved OS with dual-targeted therapy, at the end of the day this was not a statistically significant difference with a hazard ratio of 0.84.
Another negative trial was HELOISE. This looked at a dose escalation of trastuzumab in 400 patients and did not demonstrate a benefit for a higher dose of trastuzumab. And then lastly, the LOGiC trial looked at capecitabine/oxaliplatin with or without lapatinib, the tyrosine kinase inhibitor, in 545 patients. This was also a negative trial with no difference in OS for lapatinib.
Promising Phase 2: Pembrolizumab + Trastuzumab, FU/Capecitabine + Cis/Oxaliplatin1
N = 37 patients; most received cape/ox • 6-mo PFS: 75%;
median: 13 mo • Median OS:
27.3 mo • RR: 83%
1. Janjigian YY et al. Lancet Oncol. 2020;21:821- 831.
Ongoing phase 3 KEYNOTE-811 (NCT03615326)
No. at Risk 37 (0) 27 (1) 13 (8) 3 (13) 1 (14) 0 (15) 0 (15) (censored)
0
25
50
75
100
0 6 12 18 24 30 36
Prog
ress
ion-
Free
Sur
viva
l, %
6-month progression-free survival 75% (95% CI, 63%-91%) Median progression-free survival: 13.0 months (95% CI, 8.6-NR)
Time Since Start of Treatment, mo
No. at Risk 37 (0) 34 91) 20 (10) 12 (16) 8 (19) 2 (23) 0 (25)
(censored)
-120-100
-80-60-40-20
0204060
0 9 18 27 36 45 54 63 72 81 90 99 108 117
+
+ + +
+ + +
+
Complete response Partial response Stable disease Progression Escape lesion (off-target progression) Off treatment
Cha
nge
From
Bas
elin
e, %
Time Since Start of Treatment, wk
0
25
50
75
100
0 6 12 18 24 30 36
Ove
rall
Surv
ival
, %
12-month overall survival: 80% (95% CI, 68%-95%) Median overall survival: 27.3 months (95% CI, 18.8-NR)
Time Since Start of Treatment, mo
-120
-100
-80
-60
-40
-20
0
* * * *
* *
Max
imum
Cha
nge
From
B
asel
ine
in T
arge
t Les
ions
, %
We have seen recently very promising phase 2 data combining pembrolizumab, an immune checkpoint inhibitor, with trastuzumab and chemotherapy. This phase 2 trial administered either 5-FU or capecitabine with cisplatin or oxaliplatin, plus trastuzumab with the addition of pembrolizumab. Thirty-seven patients were treated on this phase 3 trial and most received capecitabine/oxaliplatin. The trial met the primary endpoint of improving 6-month progression-free survival (PFS), which was 75%. And overall, you can see that the median PFS was 13 months, with a rather striking median OS of 27 months.
And you can see from the spider plot and the waterfall plot that the vast majority of patients responded to this regimen, 83%. Based on these very promising data for adding pembrolizumab to trastuzumab and chemotherapy, there is an ongoing phase 3 trial, KEYNOTE-811, that is evaluating the addition of pembrolizumab to first-line chemotherapy with trastuzumab in HER2-positive esophagogastric cancer.
HER2-Targeted Agents: Esophagogastric Cancer Is Not Breast Cancer
First Line Trials
• JACOB: capecitabine/cisplatin/trastuzumab ± pertuzumab (N = 780)1
– OS 17.5 vs 14.2 months; HR: 0.84; P = .056 • HELOISE: capecitabine/cisplatin + two dose levels of trastuzumab
(N = 400)2
• LOGiC: capecitabine/oxaliplatin + lapatinib (N = 545)3 – No difference in OS (12.2 vs 10.5 months; HR: 0.91)
Second-Line Trials
• TyTAN: paclitaxel + lapatinib (N = 261)4
• GATSBY: paclitaxel vs T-DM1 (N = 412)5
• T-ACT: paclitaxel + trastuzumab (N = 89)6
1. Tabernero J et al. Lancet Oncol. 2018;19:1372-1384. 2. Shah M et al. J Clin Oncol. 2017;35:2558-2567. 3. Randolph Hecht J et al. J Clin Oncol. 2016;34:443-451. 4. Satoh T et al. J Clin Oncol. 2014;32:2039-2949. 5. Thuss-Patience P et al. Lancet Oncol. 2017;18:640-653. 6. Makiyama A et al. J Clin Oncol. 2020;38:1919-1927.
But again, esophagogastric cancer is not breast cancer. If we look at results from the second-line trials. Giving lapatinib second-line in the TyTAN trial—this was paclitaxel versus paclitaxel plus lapatinib, this did not show a survival benefit in 261 patients. And also the GATSBY trial, this looked at the promising drug T-DM1 versus paclitaxel in second-line treatment, and T-DM1 was no better than chemotherapy alone with paclitaxel in 412 patients.
And then lastly, recently published in the Journal of Clinical Oncology was the T-ACT trial. We always ask the question, “Does it

PeerView.com/GZH900 6Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
help patients to continue trastuzumab into second-line treatment after they’ve progressed on first-line trastuzumab?” This was a randomized phase 2 of paclitaxel with or without trastuzumab, and it did not show any survival benefit for continuing trastuzumab into second-line treatment.
Novel HER2-Directed Strategies
Antibody–drug conjugate • Trastuzumab deruxtecan (DS-8201a) • RC48-ADC: ongoing phase 2 trial (NCT03556345)
Monoclonal antibodies • Margetuximab (+ PD-1 inhibitor)
Bispecific antibodies • ZW25; targets two areas on HER2 (phase 2 in combination with SOC chemo
[NCT03929666], and phase 1/2 with chemo and PD-1 inhibitor [NCT04276493])
Combination with immunotherapy • With durvalumab, nivolumab, pembrolizumab (phase 3 KEYNOTE-811)
So are there novel HER2-targeted strategies? One of the most important approaches has been the advent of antibody–drug conjugates (ADCs), and we’ll talk at length about trastuzumab deruxtecan, or DS-8201, which is a clearly active agent in HER2-positive gastric cancer. And there are ongoing trials of other agents, including RC48-ADC, which is another ADC looking at a combination with an antimicrotubule agent.
Other monoclonal antibodies, like margetuximab, appear to be promising, in particular in combination with a PD-1 inhibitor. And now we have bispecific antibodies, including ZW25. This antibody targets two areas on HER2 and may potentially provide a more effective blockade. There are ongoing trials combining this agent with either chemotherapy or PD-1 inhibitors. And then, we mentioned already promising data for combining immunotherapy with trastuzumab, and we have the ongoing KEYNOTE-811 trial, which is first-line.
Trastuzumab deruxtecan designed with goal of improving critical attributes of an ADC
Payload with a different MOA
Payload with short systemic half-life
Bystander effect
Stable linker-payload
Tumor-selective cleavable linker
High drug-to-antibody ratio
High potency of payload
Trastuzumab Deruxtecan Structure and Mechanism of Action1
1. Iwata H et al. ASCO 2018. Abstract 2501.
7
Conjugation chemistry The linker is connected to cysteine residue of the antibody
Proprietary drug linker
Payload (DXd) Exatecan derivative
Drug linker Cysteine residue
So let’s focus our discussion specifically on trastuzumab deruxtecan and look at its structure and mechanism of action. This is a promising ADC, which combines an antiHER2-targeted monoclonal antibody connected with a cleavable tetra peptide linker to a chemotherapy payload, a topoisomerase I inhibitor.
This looks at a payload with a different mechanism of action, and it’s a high-potency payload. There is a very high drug-to-antibody ratio with this compound. Also interesting is once the antibody is internalized and the drug is released, it can have bystander effect. The chemotherapy payload can diffuse through cell membranes and affect neighboring cells.
• Results of preclinical experiments suggest bystander effect for trastuzumab deruxtecan (ie, kill neighboring tumor cells regardless of receptor expression)
Bystander Effect With Potential in HER2 Heterogeneous Tumors1
1. Ogitani Y et al. Cancer Sci. 2016;107:1039-1046.
HER2- cells MDA-MB-468
In Vivo Bystander Effect of Trastuzumab Deruxtecan vs T-DM1 After 14 Days of Treatment
Control T-DM1, 10 mg/kg Trastuzumab Deruxtecan, 3.0 mg/kg Co-culture of HER2+
and HER2- tumors in vivo HER2- cells still persist Both HER2+ and HER2- are affected
Tumor regression HER2- cells MDA-MB-468
HER2+ cells NCI-N87
So indeed, what we can see potentially with this agent is bystander effect. Not only would HER2-positive cells be affected, but, because the chemotherapy payload can diffuse out locally, it might potentially affect both HER2-positive and HER2-negative cancer cells in the same neighborhood.
a Subjects in part 1 were not required to have HER2+ (IHC 3+ or IHC 2+/ISH+) tumors. 1. Iwata H et al. ASCO 2018. Abstract 2501.
Trastuzumab Deruxtecan: Phase 1 Trial Design1
Part 2a, N = 100 T-DM1–treated HER2+ breast cancer
(IHC 3+ or ISH+) Doses: 5.4 or 6.4 mg/kg every 3 weeks
Part 2c, N = 40 HER2-low breast cancer
(IHC 2+/ISH-, IHC 1+/ISH-) Doses: 6.4 mg/kg every 3 weeks
Part 2d, N = 60 HER2-expressing or HER2-mutated solid tumors
(IHC 1+, IHC 2+, IHC 3+; or HER2 amplified or HER2 mutant) Doses: 6.4 mg/kg every 3 week
Part 2e (PK cohort), N = 20 HER2+ or HER2-low breast cancer
(IHC 1+, IHC 2+, IHC 3+, and/or ISH+) Doses: 6.4 mg/kg every 3 weeks
Part 2b, N = 40 Trastuzumab-treated HER2+ gastric cancer
(IHC 3+ or IHC 2+/ISH+) Doses: 5.4 or 6.4 mg/kg every 3 weeks
Dose expansion (part 2) Dose escalation (part 1)
HNSTD
Pharmacologically active level
Minimum effective level
Breast cancer or gastric/GEJ adenocarcinomaa
• Administered IV every 3 weeks
Dos
e
8.0 mg/kg
3.2 mg/kg
1.6 mg/kg
0.8 mg/kg
5.4 mg/kg
6 patients
6 patients 6.4 mg/kg
6 patients
3 patients
3 patients
3 patients
RD
RD
• HER2 status assessed on archival tissue in both parts 1 and 2
So a phase 1 trial development was undertaken for this agent and a recommended phase 2 dose of 6.4 mg/kg was established.
Total Evaluable Patients (n = 44)
ORR, n (%) (95% CI)
19 (43.2) (28.3-59.0)
DCR, n (%) (95% CI)
35 (79.5) (64.7-90.2)
Median DOR, mo (95% CI)
7.0 (4.4-16.6)
Median PFS, mo (95% CI)
5.6 (3.0-8.3)
Median OS, mo (95% CI)
12.8 (1.4-25.4)
1. Shitara K et al. Lancet Oncol. 2019;20:827-836.
Trastuzumab Deruxtecan Phase 1 Trial in Advanced HER2-Positive Gastric Cancer1
-100
-80
-60
-40
-20
0
20
40
60
80
Cha
nge
From
Bas
elin
e, %
N = 44
Generally well tolerated (grade 3/4) • Anemia: 30% • Platelets: 19% • Pneumonitis: 2%
• WBC: 16% • ANC: 21%
PeerView.com/GZH900 7Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
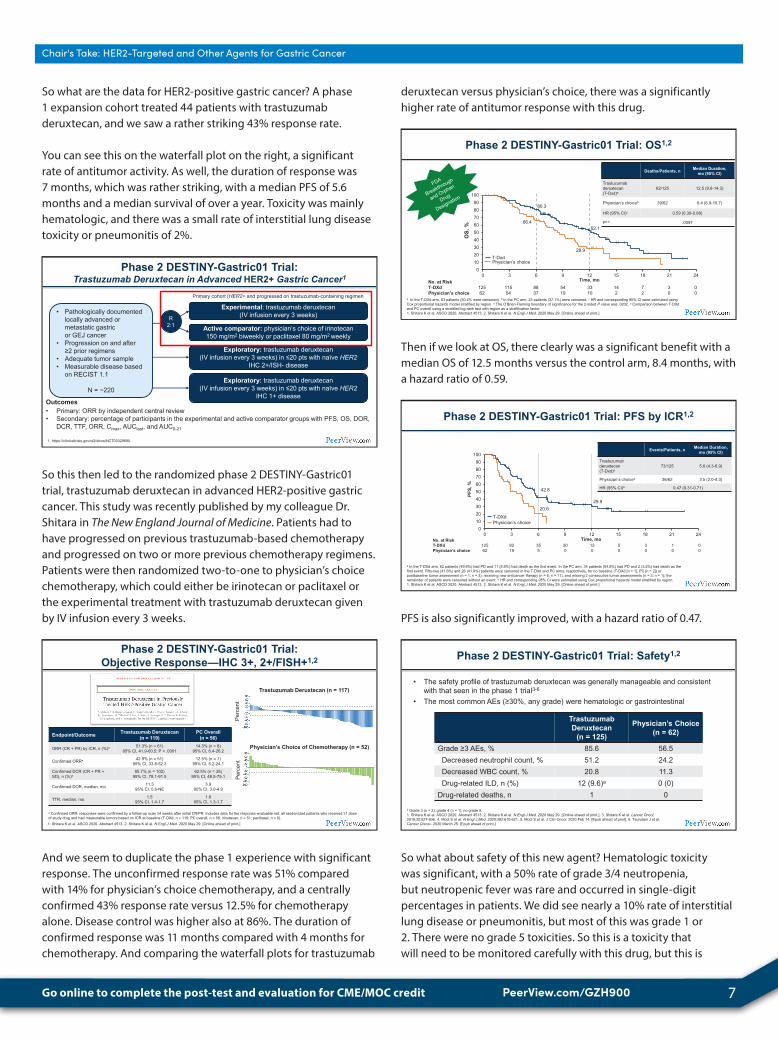
So what are the data for HER2-positive gastric cancer? A phase 1 expansion cohort treated 44 patients with trastuzumab deruxtecan, and we saw a rather striking 43% response rate.
You can see this on the waterfall plot on the right, a significant rate of antitumor activity. As well, the duration of response was 7 months, which was rather striking, with a median PFS of 5.6 months and a median survival of over a year. Toxicity was mainly hematologic, and there was a small rate of interstitial lung disease toxicity or pneumonitis of 2%.
Phase 2 DESTINY-Gastric01 Trial: Trastuzumab Deruxtecan in Advanced HER2+ Gastric Cancer1
Outcomes • Primary: ORR by independent central review • Secondary: percentage of participants in the experimental and active comparator groups with PFS, OS, DOR,
DCR, TTF, ORR, Cmax, AUClast, and AUC0-21
Active comparator: physician’s choice of irinotecan 150 mg/m2 biweekly or paclitaxel 80 mg/m2 weekly
• Pathologically documented locally advanced or metastatic gastric or GEJ cancer
• Progression on and after ≥2 prior regimens
• Adequate tumor sample • Measurable disease based
on RECIST 1.1
N = ~220
Experimental: trastuzumab deruxtecan (IV infusion every 3 weeks)
Exploratory: trastuzumab deruxtecan (IV infusion every 3 weeks) in ≤20 pts with naïve HER2
IHC 2+/ISH- disease
Exploratory: trastuzumab deruxtecan (IV infusion every 3 weeks) in ≤20 pts with naïve HER2
IHC 1+ disease
1. https://clinicaltrials.gov/ct2/show/NCT03329690.
R 2:1
Primary cohort (HER2+ and progressed on trastuzumab-containing regimen
So this then led to the randomized phase 2 DESTINY-Gastric01 trial, trastuzumab deruxtecan in advanced HER2-positive gastric cancer. This study was recently published by my colleague Dr. Shitara in The New England Journal of Medicine. Patients had to have progressed on previous trastuzumab-based chemotherapy and progressed on two or more previous chemotherapy regimens. Patients were then randomized two-to-one to physician’s choice chemotherapy, which could either be irinotecan or paclitaxel or the experimental treatment with trastuzumab deruxtecan given by IV infusion every 3 weeks.
Phase 2 DESTINY-Gastric01 Trial: Objective Response—IHC 3+, 2+/FISH+1,2
1. Shitara K et al. ASCO 2020. Abstract 4513. 2. Shitara K et al. N Engl J Med. 2020 May 29. [Online ahead of print.]
Endpoint/Outcome Trastuzumab Deruxtecan (n = 119)
PC Overall (n = 56)
ORR (CR + PR) by ICR, n (%)a 51.3% (n = 61) 95% CI, 41.9-60.5; P < .0001
14.3% (n = 8) 95% CI, 6.4-26.2
Confirmed ORRa 42.9% (n = 51) 95% CI, 33.8-52.3
12.5% (n = 7) 95% CI, 5.2-24.1
Confirmed DCR (CR + PR + SD), n (%)a
85.7% (n = 102) 95% CI, 78.1-91.5
62.5% (n = 35) 95% CI, 48.5-75.1
Confirmed DOR, median, mo 11.3 95% CI, 5.6-NE
3.9 95% CI, 3.0-4.9
TTR, median, mo 1.5 95% CI, 1.4-1.7
1.6 95% CI, 1.3-1.7
a Confirmed ORR: responses were confirmed by a follow-up scan ≥4 weeks after initial CR/PR. Includes data for the response-evaluable set: all randomized patients who received ≥1 dose of study drug and had measurable tumors based on ICR at baseline (T-DXd, n = 119; PC overall, n = 56; irinotecan, n = 51; paclitaxel, n = 5).
Trastuzumab Deruxtecan (n = 117)
Perc
ent
Physician’s Choice of Chemotherapy (n = 52)
Perc
ent
And we seem to duplicate the phase 1 experience with significant response. The unconfirmed response rate was 51% compared with 14% for physician’s choice chemotherapy, and a centrally confirmed 43% response rate versus 12.5% for chemotherapy alone. Disease control was higher also at 86%. The duration of confirmed response was 11 months compared with 4 months for chemotherapy. And comparing the waterfall plots for trastuzumab
deruxtecan versus physician’s choice, there was a significantly higher rate of antitumor response with this drug.
Phase 2 DESTINY-Gastric01 Trial: OS1,2
a In the T-DXd arm, 63 patients (50.4% were censored). b In the PC arm, 23 patients (37.1%) were censored. c HR and corresponding 95% CI were estimated using Cox proportional hazards model stratified by region. d The O’Brien-Fleming boundary of significance for the 2-sided P value was .0202. e Comparison between T-DXd and PC overall using a stratified log-rank test with region as a strafification factor. 1. Shitara K et al. ASCO 2020. Abstract 4513. 2. Shitara K et al. N Engl J Med. 2020 May 29. [Online ahead of print.]
No. at Risk T-DXd 125 115 88 54 33 14 7 3 0 Physician’s choice 62 54 37 19 10 2 2 0 0
T-Dxd Physician’s choice
80.3
52.1 66.4
28.9
0102030405060708090
100
0 3 6 9 12 15 18 21 24
OS,
%
Time, mo
Deaths/Patients, n Median Duration, mo (95% CI)
Trastuzumab deruxtecan (T-Dxd)a
62/125 12.5 (9.6-14.3)
Physician’s choiceb 39/62 8.4 (6.9-10.7)
HR (95% CI)c 0.59 (0.39-0.88)
Pd,e .0097
Then if we look at OS, there clearly was a significant benefit with a median OS of 12.5 months versus the control arm, 8.4 months, with a hazard ratio of 0.59.
Phase 2 DESTINY-Gastric01 Trial: PFS by ICR1,2
a In the T-DXd arm, 62 patients (49.6%) had PD and 11 (8.8%) had death as the first event. In the PC arm, 34 patients (54.8%) had PD and 2 (3.2%) had death as the first event. Fifty-two (41.6%) and 26 (41.9%) patients were censored in the T-DXd and PC arms, respectively, for no baseline (T-DXd [n = 1]; PC [n = 2]) or postbaseline tumor assessment (n = 1; n = 3), receiving new anticancer therapy (n = 6; n = 11), and missing 2 consecutive tumor assessments (n = 3; n = 1); the remainder of patients were censored without an event. b HR and corresponding 95% CI were estimated using Cox proportional hazards model stratified by region. 1. Shitara K et al. ASCO 2020. Abstract 4513. 2. Shitara K et al. N Engl J Med. 2020 May 29. [Online ahead of print.]
0102030405060708090
100
0 3 6 9 12 15 18 21 24No. at Risk T-DXd 125 82 35 20 12 5 3 1 0 Physician’s choice 62 19 5 0 0 0 0 0 0
Events/Patients, n Median Duration, mo (95% CI)
Trastuzumab deruxtecan (T-Dxd)a
73/125 5.6 (4.3-6.9)
Physician’s choicea 36/62 3.5 (2.0-4.3)
HR (95% CI)b 0.47 (0.31-0.71)
PFS,
%
Time, mo
20.6 29.9
42.8
T-DXd Physician’s choice
PFS is also significantly improved, with a hazard ratio of 0.47.
• The safety profile of trastuzumab deruxtecan was generally manageable and consistent with that seen in the phase 1 trial3-6
• The most common AEs (≥30%, any grade) were hematologic or gastrointestinal
a Grade 3 (n = 2); grade 4 (n = 1); no grade 5. 1. Shitara K et al. ASCO 2020. Abstract 4513. 2. Shitara K et al. N Engl J Med. 2020 May 29. [Online ahead of print.]. 3. Shitara K et al. Lancet Oncol. 2019;20:827-836. 4. Modi S et al. N Engl J Med. 2020;382:610-621. 5. Modi S et al. J Clin Oncol. 2020 Feb 14. [Epub ahead of print]. 6. Tsurutani J et al. Cancer Discov. 2020 March 25. [Epub ahead of print.]
Phase 2 DESTINY-Gastric01 Trial: Safety1,2
Trastuzumab Deruxtecan
(n = 125)
Physician’s Choice (n = 62)
Grade ≥3 AEs, % 85.6 56.5 Decreased neutrophil count, % 51.2 24.2 Decreased WBC count, % 20.8 11.3 Drug-related ILD, n (%) 12 (9.6)a 0 (0)
Drug-related deaths, n 1 0
So what about safety of this new agent? Hematologic toxicity was significant, with a 50% rate of grade 3/4 neutropenia, but neutropenic fever was rare and occurred in single-digit percentages in patients. We did see nearly a 10% rate of interstitial lung disease or pneumonitis, but most of this was grade 1 or 2. There were no grade 5 toxicities. So this is a toxicity that will need to be monitored carefully with this drug, but this is

PeerView.com/GZH900 8Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
counterbalanced by the high degree of efficacy and improvement in PFS and OS.
Phase 2 Trial: Trastuzumab Deruxtecan in HER2-Positive Gastric Cancer (DESTINY-Gastric02)1
1. https://clinicaltrials.gov/ct2/show/record/NCT04014075.
Outcomes • Primary: ORR • Secondary: PFS, OS, DOR
Trastuzumab deruxtecan (IV infusion every 3 weeks)
Disease progression or
withdrawal from treatment for other reasons
Patients must have HER2+ gastric or GEJ cancer that: • Cannot be removed surgically • Has moved to other parts
of the body • Worsened during or after
treatment that included trastuzumab
N = ~72
Recruiting
There is now an ongoing phase 2 trial to duplicate these results in a Western population, and we are now studying in a phase 2, single-arm study trastuzumab deruxtecan in HER2-positive gastric cancer in patients who have progressed on one prior therapy with a trastuzumab-containing chemotherapy. The primary endpoint is ORR, and this trial is actively recruiting in the United States.
Margetuximab1,2
Margetuximab had enhanced antibody-dependent cell-mediated cytotoxicity (ADCC) compared with trastuzumab
Target Cancer Cells
Immune Effect Cells
Fc-Optimized Antibody
Anti-gens (eg, HER2)
Fcg Receptors
Lysis Killing of Cancer Cells
The single-agent activity of margetuximab in HER2-positive gastroesophageal cancers was demonstrated with a confirmed PR rate of 10% (2 of 20)
FcγR CD16A genotype of V/F or F/F Phase 3 MAHOGANY: Combination Margetuximab, INCMGA00012, MGD013,
and Chemotherapy Phase 2/3 Trial in HER2+ Gastric/GEJ Cancer 1. Bang YJ et al. Ann Oncol. 2017;28:855-861. 2. https://clinicaltrials.gov/ct2/show/NCT04082364.
What about margetuximab? This is a novel antibody construct, which has an element targeting trastuzumab and also an element that may stimulate ADCC. We can see on the waterfall plot on the left that margetuximab had a single-agent activity of 10%, which might potentially be enhanced with the combination of checkpoint inhibitors. Based on this, there is an emerging phase 3 trial, which will look at margetuximab in combination with checkpoint inhibitor versus chemotherapy in HER2-positive gastric and GEJ cancers.
My Key Takeaways
HER2-targeted therapies have not been beneficial in patients with HER2-positive disease after progression on trastuzumab-containing regimens
Several novel strategies, including ADCs, monoclonal and bispecific antibodies, and immunotherapy combinations, are being investigated
Trastuzumab deruxtecan demonstrated statistically significant and clinically meaningful improvements in ORR and OS compared with standard chemotherapy in the phase 2 randomized DESTINY-Gastric01 trial
Positive results suggest ADCs may become a new treatment standard for patients who have been previously treated
So what are my key takeaways from HER2-targeted therapies? Beyond trastuzumab, it is clear that HER2-targeted therapies have not been beneficial in patients with HER2-positive disease after progression on first-line trastuzumab. Several novel strategies, including ADCs, monoclonal antibodies, and immunotherapy combinations are being investigated.
And I think the most promising and what could lead to potential regulatory approval is trastuzumab deruxtecan, which demonstrated substantial and clinically meaningful improvements in response rate and survival compared with standard chemotherapy in the phase 2 randomized DESTINY-Gastric01 trial. The positive results suggest that ADCs may become a new treatment standard for patients who have been previously treated.
RTOG 1010: HER2+, carboplatin/paclitaxel/RT surgery ± trastuzumab—esophageal and GEJ cancer1
PETRARCA (NCT02581462): FLOT ± trastuzumab + pertuzumab—gastric and GEJ cancer2
INNOVATION (EORTC) (NCT02205047): FU or cape/cisplatin + trastuzumab ± pertuzumab—gastric and GEJ cancer3
HER2-Targeted Treatments in Neoadjuvant Setting1-3
1. Safran H et al. ASCO 2020. Abstract 4500. 2. Hofheinz RD et al. ASCO 2020. Abstract 4502. 3. https://clinicaltrials.gov/ct2/show/NCT02205047.
So what about neoadjuvant therapy? I’m going to present now data from two neoadjuvant trials that were presented at ASCO 2020. One of the most anxiously awaited trials was RTOG 1010. This studied patients who were HER2-positive with esophageal and GEJ cancer. Patients were treated with standard chemoradiation followed by surgery, with carboplatin, paclitaxel, and radiation with or without the addition of trastuzumab.
Another important study presented, which was a smaller, randomized phase 2 trial, was PETRARCA that was in GEJ and gastric cancers looking at perioperative chemotherapy alone. This trial looked at the FLOT regimen with or without dual-targeted HER2 therapy, adding trastuzumab plus pertuzumab to perioperative chemotherapy in gastric and GEJ cancers.

PeerView.com/GZH900 9Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
Surgery • Newly diagnosed stage
T1N1-2, T2-3N0-2 adenocarcinoma of the esophagus involving the mid, distal, or esophagogastric junction and up to 5 cm of the stomach
• HER2+ disease as determined by IHC and FISH
N = 203 Surgery
Trastuzumab 6 mg/kg every 3 wk
for 13 treatments after surgery
5-8 wk after completion of
radiation R
CRTa + weekly trastuzumab 4 mg/kg
wk 1, then 2 mg/kg/weekly x 5 during CRT, then 6 mg/kg for 1 dose prior to surgery
CRTa
a CRT: chemotherapy (paclitaxel, 50 mg/m2 and carboplatin AUC = 2) weekly for 6 wk with radiation (RT: 3D-CRT or IMRT, 50.4 Gy in 28 fractions). 1. Safran H et al. ASCO 2020; Abstract 4500.
Phase 3 NRG Oncology/RTOG 1010 Trial1
Trastuzumab Plus Trimodality Treatment of HER2-Overexpressing Esophageal Adenocarcinoma1
So what were the results from the NRG Oncology RTOG 1010 trial? Again, this evaluated trastuzumab plus trimodality therapy in HER2-overexpressing esophageal and GEJ adenocarcinomas. Patients had to have either node-positive disease or a T2-3 disease that could be surgically resectable. HER2 status was confirmed centrally, and patients had to either be IHC 3+–positive or FISH-positive.
Two hundred and three patients were randomized one-to-one to standard chemoradiation followed by surgery, which again was carboplatin, paclitaxel, and radiation with or without the addition of trastuzumab. Both given during chemoradiation, and then as adjuvant therapy after surgery for 13 treatments every 3 weeks.
Phase 3 NRG Oncology/RTOG 1010 Trial: Outcomes1
1. Safran H et al. ASCO 2020. Abstract 4500.
0
25
50
75
100
0 6 12 18 24 30 36 42 48 54 60 66 720
25
50
75
100
0 6 12 18 24 30 36 42 48 54 60 66 72
No statistically significant increase in TRAEs was observed with the addition of trastuzumab, including no increase in cardiac events
DFS OS
No. at Risk CRT + trastuzumab 98 72 60 48 39 35 32 29 26 20 19 13 10 CRT 96 77 51 42 37 33 30 28 26 22 17 14 13
No. at Risk CRT + trastuzumab 98 87 79 67 55 51 46 40 37 26 23 16 12 CRT 96 87 78 69 61 52 46 44 39 31 24 17 15
HR (λCRT + Tras/CRT): 0.97 95% CI: 0.69-1.36
HR (λCRT + Tras/CRT): 1.01 95% CI: 0.69-1.47
Pts, N Failed, n Censored, n Median DFS (95% CI) CRT + trastuzumab 98 68 30 19.6 (13.5-26.2) CRT 96 67 29 14.2 (10.5-23.0)
Pts, N Failed, n Censored, n Median OS (95% CI) CRT + trastuzumab 98 54 44 38.5 (26.2-70.4) CRT 96 55 41 38.9 (29.0-64.5)
Censored P = .85 (two-sided log-rank)
Censored P = .95 (two-sided log-rank)
Time Since Randomization, mo Time Since Randomization, mo
DFS
, %
OS,
%
CRT + trastuzumab CRT CRT + trastuzumab CRT
Unfortunately, this was a negative trial. The primary endpoint was disease-free survival, and we can see that although there was a slight separation of the curves in the middle. At the end of the day, there was no statistically significant improvement in disease-free survival for adding trastuzumab to chemoradiation compared with chemoradiation alone, with a median disease-free survival of 19.6 months versus 14.2 months for chemoradiation, with a hazard ratio of 0.97.
OS also showed no benefit for the addition of trastuzumab, where here the hazard ratio was also near one, with a median OS for chemoradiation aloneof 38.9 months versus 38.5 months for the addition of trastuzumab. So what did we learn from this study? I think that moving forward trastuzumab alone will not be an adequate strategy to develop in the adjuvant or neoadjuvant treatment of esophageal gastric cancer. It’s simply not enough.
Surgery and Pathologic Complete Response (pCR)1
1. Safran H et al. ASCO 2020. Abstract 4500.
CRT + Trastuzumab
(n = 98)
CRT (n = 96) Chi-Squared P
Surgery Yes 82 (84%) 78 (81%) No (progression, mets, death) 5 (5%) 8 (8%) No (other) 11 (11%) 10 (10%) pCR .71 Yes 22 (27%) 23 (29%) No 60 (73%) 55 (71%)
What about surgery and pathologic outcome from the RTOG 1010 study? Similar numbers of patients went to surgery, whether or not they got trastuzumab, 84% versus 81%. There was also no difference in pathologic complete response rate with or without trastuzumab, which ranged from 27% to 29%.
• Esophagogastric adenocarcinoma
• cT2-4 cNany cM0 or Tany cN+ cM0
• HER2-positivity (centrally assessed)
• ECOG ≤2
R
FLOT x 4 resection FLOT x 4
FLOT x4 + trastuzumab + pertuzumab resection FLOT x 4 + trastuzumab +
pertuzumab trastuzumab + pertuzumab (9 cycles 3 weekly)
1. Hofheinz RD et al. ASCO 2020. Abstract 4502
Phase 2/3 PETRARCA Study Design1
Randomized, multicenter, investigator-initiated study
Stratification factors • ECOG (0 or 1 vs 2) • Location of primary (GE-junction vs stomach) • Age (<60 vs 60-69 vs ≥70 y)
So what about the PETRARCA trial? This was a study done in Germany, studying HER2-positive GEJ and gastric adenocarcinomas. Patients were randomized to receive standard perioperative FLOT chemotherapy before and after surgery, with or without the addition of dual-targeted HER2 therapy, combining trastuzumab with pertuzumab not only during chemotherapy, but also as additional adjuvant treatment for nine cycles after surgery.
Phase 2/3 PETRARCA: Histopathology and Primary Endpoint (pCR)1
1. Hofheinz RD et al. ASCO 2020. Abstract 4502
ypT-stage FLOT (n = 41)
FLOT + Trastuzumab/ Pertuzumab
(n = 40)
P
≤T1 11(27%) 17 (43%) T2 9 (22%) 8 (20%) T3 17 (41%) 14 (35%) T4 3 (7%) 0 (0%) N0 16 (39%) 27 (68%) pCR 5 (12%) 14 (35%) .02
Again, this was a small randomized phase 2 trial, and so we only treated 81 patients. It does appear, however, that there was

PeerView.com/GZH900 10Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
significant downstaging with more T1 patients. There were more node-negative patients receiving HER2-targeted therapy: 68% versus 39%. The pathologic complete response rate was increased from 12% to 35%. So there is a signal from this study that we may enhance response with dual-targeted HER2 therapy combined with the FLOT regimen.
Phase 2/3 PETRARCA: DFS and OS1
FLOT FLOT/Trastuzumab + Pertuzumab
mDFS, mo (22 mo median follow-up) 26 (13-NR) NR
HR: 0.576, P = 0.14
mOS, mo (22 mo median follow-up) NR NR
HR: 0.558; P =.24
1. Hofheinz RD et al. ASCO 2020. Abstract 4502
0
0.2
0.4
0.6
0.8
1
0 6 12 18 24 30 36 42
Surv
ival
Pro
babi
lity
Time, mo
0
0.2
0.4
0.6
0.8
1
0 6 12 18 24 30 36 42
Surv
ival
Pro
babi
lity
Time, mo
DFS OS
FLOT/T+P
FLOT
FLOT/T+P
FLOT
P = .1300 P = .2278
1.0 1.0
It’s difficult to interpret disease-free survival and OS, but the trends do suggest a benefit. Whether or not this is going to move forward in phase 3 is a bit complicated. Because we did see negative results for pertuzumab in the advanced disease study, but this trial does provide a signal that may indicate that further study of dual-targeted therapy is warranted, particularly given the lack of success for trastuzumab alone in the RTOG trial.
1. Lorenzen S et al. ASCO 2020. Abstract 4514. 2. https://clinicaltrials.gov/ct2/show/NCT03081143.
Anti-Angiogenesis in Gastric Cancer1,2
For pts with prior docetaxel use (71/110), median PFS was significantly longer and OS was numerically longer with FOLFIRI + ramucirumab than
with paclitaxel + ramucirumab
OS (ITT), mo OS (Docetaxel Pretreated), mo
FOLFIRI with ramucirumab 6.8 7.5 Paclitaxel with ramucirumab 7.6 6.5
• Ramucirumab + paclitaxel and single-agent ramucirumab (NCCN Category 1) • Recently amended to permit FOLFIRI + ramucirumab given increased use
of preoperative FLOT
Phase 2 Trial: FOLFIRI With Ramucirumab
So I’m going to mention briefly antiangiogenesis agents in gastric cancer. Ramucirumab plus paclitaxel and ramucirumab alone are approved as standard second-line treatments. These guidelines recently were amended to permit the use of FOLFIRI plus ramucirumab in the second line, given the increased usage of the FLOT regimen, which gives patients a taxane upfront.
We now have some supportive data for FOLFIRI with ramucirumab from a randomized phase 2 trial from Germany. This looked at FOLFIRI plus ramucirumab versus paclitaxel plus ramucirumab as second-line treatment in advanced esophageal gastric cancer. We see similar rates of OS with the two approaches, but more importantly almost 75% of the patients on this trial had prior docetaxel exposure.
There was an observation on this trial that the patients who had previous docetaxel exposure may have had an improved PFS, a better response rate, and a potentially numerically longer OS for the combination of FOLFIRI plus ramucirumab versus paclitaxel plus ramucirumab. So use of FOLFIRI plus ramucirumab might be a consideration in a patient who has received recent prior taxane-based chemotherapy.
Immunotherapy in Esophagogastric Cancer
1. Fuchs CS et al. JAMA Oncol. 2018;4:e180013. 2. Chen et al. Gastric Cancer. 2020;23:510-519. 3. Bang YJ et al. Ann Oncol. 2018;29:2052-2060. 4. Shitara K et al. Lancet. 2018;392:123-133. 5. Tabernero J et al. ASCO 2019. Abstract LBA4007. 6. Moehler MH et al. ASCO GI. Abstract 278.
Single-Agent Activity in Refractory Disease • KEYNOTE-0591: pembrolizumab; MSI high and PD-L1+ • ATTRACTION-22: nivolumab vs BSC • JAVELIN Gastric 3003: avelumab vs physician choice
Comparison With Second-Line Chemotherapy • KEYNOTE-0614: pembrolizumab vs paclitaxel; in PD-L1+
First-Line Use With or Without Chemotherapy
• KEYNOTE-0625: pembrolizumab in GEJ/gastric adenocarcinoma • JAVELIN Gastric 1006: maintenance first-line avelumab not superior to chemotherapy
What about immunotherapy? This gets a little bit more complicated, but I would argue that much of the results to date have been negative for checkpoint inhibitors in esophagogastric cancer. This slide overviews recent trial results. If we look at single-agent activity in refractory gastric cancer, the KEYNOTE-059 trial was a large, phase 2 expansion cohort trial of pembrolizumab in previously treated GEJ and gastric cancer. Patients who were PD-L1–positive had a response rate of about 10% to 12%, and a suggestion of median survival prolongation. Particularly striking were the results in MSI-high patients with a response rate exceeding 50% to 60%. Based on KEYNOTE-059, pembrolizumab ab was approved as a single agent in chemotherapy-refractory GEJ and gastric cancers if patients were MSI-high or PD-L1–positive.
The other positive study was ATTRACTION from Japan. This was a randomized phase 3 trial comparing nivolumab versus best supportive care in chemorefractory gastric cancer, with a response rate of about 11% and an 1-year survival of 20% for nivolumab. This drug is now approved in Japan irrespective of PD-L1 status. The JAVELIN Gastric 300 trial, however, was negative. This was a third-line trial of avelumab versus physician choice, and this did not show superiority for avelumab over third-line chemotherapy.
What about second-line chemotherapy? KEYNOTE-061 was a head-to-head comparison of pembrolizumab versus paclitaxel in PD-L1–positive adenocarcinoma. This was a negative trial; it did not show superiority for pembrolizumab over paclitaxel and also arguably used an inferior chemotherapy control arm. We should have really considered using paclitaxel plus ramucirumab and not paclitaxel alone. And then lastly, first-line trials. KEYNOTE-062—this was first-line checkpoint inhibitor therapy with or without chemotherapy. This also was a negative trial for the primary overall endpoints. We can debate the noninferiority question, but overall we’ll discuss essentially negative results for first-line use of pembrolizumab in

PeerView.com/GZH900 11Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
GEJ and gastric adenocarcinoma.And more recently, the JAVELIN trial Gastric 100 treated patients with first-line chemotherapy, and then they were randomized to maintenance avelumab or to continue chemotherapy. Avelumab was not superior to maintenance chemotherapy, so this was also a negative trial.
Phase 3 KEYNOTE-062: Pembrolizumab + Chemotherapy Versus Chemotherapy (CPS ≥1)1,a
a Data cutoff: March 26, 2019. 1. Tabernero J et al. ASCO 2019. Abstract LBA4007.
I want to focus a little bit now on KEYNOTE-062. This is the first-line pembrolizumab trial. These are the data results for pembrolizumab plus chemotherapy versus chemotherapy alone, again in all patients who were CPS-positive 1 or higher. You can see the negative outcome here; there was no difference in 12-month median OS. There was a slight trend of 5% at 2 years, but the hazard ratio was 0.85. So adding pembrolizumab to first-line chemotherapy is no better than chemotherapy alone.
Phase 3 KEYNOTE-062: Pembrolizumab + Chemotherapy Versus Chemotherapy (CPS ≥10)1,a
a Data cutoff: March 26, 2019. 1. Tabernero J et al. ASCO 2019. Abstract LBA4007.
A similar observation in patients who were CPS 10 or higher, pembrolizumab plus chemotherapy was no better than chemotherapy alone, with essentially no significant differences in 12-month median OS, and a 6% difference at 24 months. The take-home message is we should not combine pembrolizumab with chemotherapy first-line. It is not better than chemotherapy alone, even in PD-L1–positive patients.
Phase 3 KEYNOTE-062: Pembrolizumab in First-Line Gastric Cancer (CPS ≥1)1
0102030405060708090
100
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
12-month rate 47% 46%
Time, mo
OS,
%
24-month rate 27% 19% mOS, mo (95% CI)a
10.6 (7.7-13.8) 11.1 (9.2-12.8)
HR (99.2% CI) Pembrolizumab Chemotherapy
Events
79% 86%
0.91 (0.69-1.18)
NIa
1.2
256 201 162 139 120 107 94 83 59 38 23 12 4 0 0 250 230 192 144 114 94 75 49 38 21 15 6 2 2 0
No. at Risk Pembro Chemo
a HR (95% CI) = 0.91 (0.74-1.10); P = .162 for superiority of pembrolizumab vs chemotherapy. Data cutoff: March 26, 2019. 1. Tabernero J et al. ASCO 2019. Abstract LBA4007.
So what about the question of pembrolizumab versus chemotherapy? If we look at the PD-L1 or CPS 1 of patients, there was no difference in 12-month median OS of 47%, but the curves do start to separate later. The problem, however, is, as seen in the left side of the curve, the death rate with pembrolizumab alone was 10% or more higher during the first 12 months. More patients were dying of their cancer with pembrolizumab alone compared with chemotherapy.
Phase 3 KEYNOTE-062: Pembrolizumab Versus Chemotherapy (CPS ≥10)1
a Data cutoff: March 26, 2019. 1. Tabernero J et al. ASCO 2019. Abstract LBA4007.
92 71 62 56 52 50 45 40 32 22 13 9 4 0 0 90 82 70 53 42 33 28 20 16 8 7 3 0 0 0
12-month rate 57% 47%
OS,
%a
Time, mo No. at Risk
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42
10
20
30
40
50
60
70
80
90
100
0
24-month rate 39% 22%
HR (95% CI) Pembrolizumab Chemotherapy
Events
66% 83%
0.69 (0.49-0.97)
mOS, mo (95% CI) 17.4 (9.1-23.1) 10.8 (8.5-13.8)
The results were a little better in patients with CPS 10 and higher or PD-L1 10%. Again, there was no difference in 12-month median OS, but a more robust plateau later with a near 17% improvement in 24-month median OS. But again, if we look at the left side of the curve, there was a higher death rate in patients getting upfront pembrolizumab. And the late separation of the curves is not surprising, because we know that pembrolizumab helps a small subset of patients later and not earlier. These results do not change practice and use of pembrolizumab in patients who were PD-L1–positive in later line but not first-line treatment.

PeerView.com/GZH900 12Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
a PFS assessed per RECIST v1.1 by blinded independent central review (final analysis of PFS occurred at IA2); Data cutoff: Sept 28, 2018. 1. Tabernero J et al. ASCO 2019. Abstract LBA4007.
Phase 3 KEYNOTE-062: PFS Pembrolizumab Versus Chemotherapy1
CPS ≥10a
Pembrolizumab
Events HR (95% CI)
Chemotherapy 88% 89%
1.66 (1.37-2.01)
PFS,
%
256 91 61 44 30 24 17 8 5 4 3 0 0 0 0 250 199 125 70 43 27 14 7 5 2 1 1 0 0 0
12-month rate
mPFS, mo (95% CI) 2.0 (1.5-2.8) 6.4 (5.7-7.0)
14% 19%
0
10
20
30
40
50
60
70
80
90
100
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 Time, mo No. at Risk
0 3 6 9 12 15 18 21 24 27 30 33 36 39 42 0
10
20
30
40
50
60
70
80
90
100
Time, mo No. at Risk 92 40 30 24 17 15 10 6 5 4 3 0 0 0 0 90 68 43 20 13 8 5 3 2 0 0 0 0 0 0
12-month rate 21% 16%
mPFS, mo (95% CI) 2.9 (1.6-5.4) 6.1 (5.3-6.9)
Pembrolizumab
Events HR (95% CI)
Chemotherapy 80% 89%
1.10 (0.79-1.51)
PFS,
%
CPS ≥1a
The other concern is rapid progression on pembrolizumab. If we look at both the CPS 1 and 10 subgroups, this is PFS, and you can see that in both of these subgroups the majority of patients progress rapidly on pembrolizumab. PFS is arguably better with initial chemotherapy compared with pembrolizumab. The worry is, and again given the higher death rates, that you can’t salvage these patients with chemotherapy later.
KEYNOTE-061: Pembrolizumab in Second-Line Setting: Overall Survival by PD-L1 CPS1
a Primary endpoint. 1. Shitara K et al. Lancet. 2018;392:123-133.
0102030405060708090
100
0 6 12 18 24 30Time, mo
OS,
%
0102030405060708090
100
0 6 12 18 24 300
102030405060708090
100
0 6 12 18 24 30
OS,
%
OS,
%
CPS <1
mOS, mo (95% CI) 4.8 (3.9-6.1) 8.2 (6.8-10.6)
CPS ≥1a CPS ≥10
mOS, mo (95% CI) 9.1 (6.2-10.7) 8.3 (7.6-9.0)
mOS, mo (95% CI) 10.4 (5.9-17.3) 8.0 (5.1-9.9)
Time, mo Time, mo
HR (95% CI)
Pembrolizumab Paclitaxel
Events/Patients
87/99 86/96
1.20 (0.89-1.63)
HR (95% CI) Events/Patients
151/196 175/199
0.82 (0.66-1.03)
HR (95% CI) Events/Patients
34/53 46/55
0.64 (0.41-1.02)
99 41 23 14 2 0 96 61 29 13 5 0
No. at Risk 196 114 78 39 14 0 199 130 54 23 7 0
No. at Risk 53 34 24 13 6 0 55 33 13 7 4 0
No. at Risk Pembro Paclitaxel
So what about KEYNOTE-061? This is pembrolizumab in the second-line setting. Again, this was overall a negative trial. Certainly, if you’re PD-L1 or CPS-negative, median OS was inferior for pembrolizumab. For PD-L1 1% or CPS 1 of patients, again there was a trend towards a higher earlier death rate, but then the curves separate beyond 6 months. And for the CPS 10 or higher or PD-L1 10%, the separation is more robust later but again argues a late benefit for pembrolizumab. It is not superior within the first 6 to 8 months of treatment. It does indicate, however, that perhaps in the CPS 10 or higher of patients this drug is more active.
Abstract 4503: Long-term analysis found that second-line pembrolizumab prolonged OS among patients with PD-L1–positive GC and led to fewer drug-related AEs vs paclitaxel
Abstract 4512: A strong association found between TMB and response to pembrolizumab in patients with GC
Updates at ASCO 20201,2
1. Fuchs CS et al. ASCO 2020. Abstract 4503. 2. Fuchs CS et al. ASCO 2020. Abstract 4512.
So what about the updates for ASCO 2020? The KEYNOTE-061 trial was updated in abstract 4503 with long-term follow-up of second-line pembrolizumab; they pretty much came up with the same observations. We do see this late separation of the survival curves, particularly in patients who have the CPS 10-positive rate, and it did lead to fewer drug-related adverse events. I think more interesting from ASCO was the observation that there was an association between tumor mutational burden and benefit from pembrolizumab. However, high tumor mutational burden was only observed in a small minority of patients, and it’s not clear if this measure adds anything beyond measuring PD-L1 or CPS scores.
Novel Target: Zolbetuximab1-3
Ongoing Phase 3 Trials • SPOTLIGHT: FOLFOX ± zolbetuximab • GLOW: first-line zolbetuximab + CAPOX
• Phase 2 FAST trial: EOX + zolbetuximab (IMAB 362), a chimeric antibody specific to CLDN18.2
1. Al-Batran SE et al. ASCO 2016. Abstract LBA4001. 2. https://clinicaltrials.gov/ct2/show/NCT03504397. 3. Shah MA et al. ASCO 2020. Abstract TPS4648.
No. at Risk EOX 59 46 28 13 6 4 4 1 EOX + IMAB 362 57 52 38 30 26 14 7 1
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100 120
Time to Event, wk No. at Risk EOX 84 34 9 2 1 0 0 EOX + IMAB 362 77 40 18 11 9 3 0
0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1
0 20 40 60 80 100 120 140 160
Time to Event, wk
HR = 0.51 P = .0001
13.2 mo
8.4 mo
EOX (84) EOX + IMAB362 800/600 mg/m2 (77)
EOX (59) EOX + IMAB362 800/600 mg/m2 (57)
HR = 0.45 P < .0005
16.7 mo
9.0 mo
1.0
Surv
ival
Dis
trib
utio
n Fu
nctio
n
Surv
ival
Dis
trib
utio
n Fu
nctio
n
1.0
Then I want to mention another novel agent zolbetuximab, which is in ongoing phase 3 trials. Zolbetuximab is a chimeric antibody that targets the CLDN18.2 protein, which is a gap junction protein overexpressed in about 70% of gastric cancers. The FAST trial was a randomized, phase 2 trial of EOX chemotherapy with or without zolbetuximab in CLDN18.2-positive patients. In the total population, you saw about a 5-month improvement in OS adding zolbetuximab, and in the high expresses of CLDN18.2, which was about 30%, we saw a 7-month improvement in median survival. Based on these encouraging results, there are two ongoing phase 3 trials. The phase 3 trial SPOTLIGHT is FOLFOX plus or minus zolbetuximab. And then, there’s also an ongoing phase 3 trial, the GLOW trial, that is capecitabine/oxaliplatin with or without zolbetuximab.

PeerView.com/GZH900 13Go online to complete the post-test and evaluation for CME/MOC credit
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
My Key Takeaways: Novel Strategies With Targeted Therapies Set to Evolve the Standards of Treatment for Advanced Gastric Cancer
Trastuzumab alone + chemoradiotherapy and surgery did not improve any endpoint in esophageal and GEJ cancers • Combination targeted HER2 therapy will need to be studied • Dual-targeted HER2 strategy (PETRARCA) + immunotherapy, novel HER-targeted agents
Trastuzumab deruxtecan is significantly active (RR, PFS, OS) after prior trastuzumab based therapy
New combinations of chemotherapy with ramucirumab showed promise in the phase 2/3 RAMIRIS trial
While pembrolizumab is approved in the third-line setting, immune checkpoint inhibitors have shown modest activity in earlier settings
New combinations with immune checkpoint inhibitors may be promising
New targets and therapy strategies are ongoing and under investigation
So what are my key takeaways from this discussion today evaluating novel strategies with targeted therapies? Trastuzumab alone failed to improve any endpoint in esophageal and GEJ cancers when combined with chemoradiotherapy and surgery. Clearly, we need to do more than just trastuzumab alone. Combination targeted HER2 therapy will need to be studied, and we have some promising early results for dual-targeted HER2 therapy. There may be a potential role for including immunotherapy agents and novel HER2-targeted agents.
Trastuzumab deruxtecan is a significantly active new agent after prior trastuzumab-based therapy. New combinations of chemotherapy with ramucirumab have shown promise, particularly FOLFIRI plus ramucirumab in the setting of previous recent taxane exposure. While pembrolizumab is approved in the third-line setting, immune checkpoint inhibitors have shown modest activity in early-line setting and certainly have not achieved an indication to be combined with chemotherapy or replace chemotherapy in the first- or second-line. The exception, however, is MSI-high cancers in which checkpoint inhibitors have a high degree of response, PFS and OS, and we can consider earlier line use of these drugs in MSI-high cancers. New combinations with immune checkpoint inhibitors are promising, and new targets and therapy strategies are ongoing and under investigation. Thank you very much.
Narrator: This activity has been jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.

PeerView.com/GZH900The Oncology Topics You Want
From the Experts You Trust
CME/MOC
Chair's Take: HER2-Targeted and Other Agents for Gastric Cancer
Sign up for email alerts on new clinical advances and educational activities in your specialty: PeerView.com/signup
Copyright © 2000-2020, PeerView
This CME/MOC activity is jointly provided by Medical Learning Institute, Inc. and PVI, PeerView Institute for Medical Education.
This activity is supported by independent educational grants from AstraZeneca and Daiichi Sankyo, Inc.