closing the gap between oral hygiene and minimally
TRANSCRIPT

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 663
QUINTESSENCE INTERNATIONAL
Undoubtedly, after the advent of dentistry as
an academic discipline at the end of the 19th
century, the profession was influenced by a
mechanical era (with high-speed rotary cut-
ting instruments) and predominantly used a
surgical approach to remove caries. This
included radical removal of diseased por-
tions of the tooth, along with (material-driven)
geometric extensions to areas that were
assumed to be caries resistant; this concept
of extension for prevention was introduced
by Webb1 (and slightly modified by Black2
later on), and has influenced dentistry for
more than 120 years, even though this regi-
men was never scientifically based and was
misleading. Notwithstanding, already in
1922, it was recommended that restorative
treatment for these lesions should be con-
servative and that there is no need to remove
Closing the gap between oral hygiene and minimally invasive dentistry: A review on the resin infiltration technique of incipient (proximal) enamel lesionsAndrej M. Kielbassa, Dr Med Dent1/Jan Müller, Dr Med Dent2/
Christian R. Gernhardt, Dr Med Dent3
Dental caries on (proximal) tooth surfaces is still a problem in many industrialized coun-
tries. The objectives of this review were to present the scientific basis and the principles of
the resin infiltration concept, to discuss the inherent clinical applications, and to describe
how these backgrounds can be integrated into the concept of minimal intervention den-
tistry. Data were identified by searches of the Cochrane Registers, Medline, and Scopus.
Articles published in English and German through December 2008 were selected, and
most up-to-date or relevant references were chosen. Cross-referencing of significant arti-
cles identified additionally relevant articles written in other languages and those of histori-
cal value. A total of 23 in vitro studies (focusing on penetration depths or demineralization
prevention) were found, and 3 clinical studies (involving 122 subjects) could be retrieved;
these studies were not comparable. With an increased understanding of the caries
process, it is now recognized that demineralized but noncavitated enamel lesions can be
arrested or remineralized in many situations. The clinical research evidence on the resin
infiltration technique currently is of moderate extent to reach any decisive conclusions;
however, based on available laboratory and clinical studies, it seems convincing that resin
infiltration of enamel lesions should reduce (or even stop) the progress of white spot
lesions. Combining this ultraconservative restorative approach (which is considered
microinvasive) with a substantial caries remineralization program may provide therapeutic
benefits and significantly reduce both long-term restorative needs and costs, thus comple-
menting the concept of minimal intervention dentistry. (Quintessence Int 2009;40:663–681)
Key words: enamel, fluoride, minimal intervention dentistry, remineralization,
resin infiltration, subsurface caries lesion
1Professor and Head, Department of Operative Dentistry and
Periodontology, CharitéCentrum 3, University School of Dental
Medicine, Charité—Universitätsmedizin Berlin, Berlin, Germany.
2Assistant Medical Director, Department of Operative Dentistry
and Periodontology, CharitéCentrum 3, University School of
Dental Medicine, Charité—Universitätsmedizin Berlin, Berlin,
Germany.
3Associate Professor, Assistant Medical Director, Department of
Operative Dentistry and Periodontology, University School of
Dental Medicine, Martin-Luther-University Halle-Wittenberg,
Halle, Germany.
Correspondence: Dr Andrej M. Kielbassa, Abteilung für
Zahnerhaltungskunde und Parodontologie, CharitéCentrum 3
für Zahn-, Mund- und Kieferheilkunde, Aßmannshauser Straße
4-6, D-14197 Berlin, Germany. Fax: 49-30-450 562 932. Email:
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

664 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
sound tooth structure in the name of preven-
tion.3 Nowadays, such surgical techniques
are considered maximally invasive, destruc-
tive, and outmoded.4
In modern dentistry, it has been widely
accepted that no cavity design or restorative
material will cure caries. For sure, once there
is a cavitation on the enamel surface, surgi-
cal intervention will be justified; in these
situations, minimally invasive techniques
(restricted to the actual damage) reduce the
amount of destruction; biomimetic restora-
tive materials (imitating nature while adhe-
sively luted) allow for a satisfying clinical and
esthetic outcome (Fig 1), and, concomitantly,
the intervention will enable control of the
local microflora (by modifying the local envi-
ronment, and thus revealing that operative
and restorative dentistry is but a true part of
prevention). Nonetheless, minimally invasive
approach is late in the disease process and
destructive as well, and restorative materials
are neither a perfect nor an everlasting
replacement for original tooth structure.
Thus, in view of the mean lifetime of any
restoration type, the original anatomy,
strength, and esthetics are lost forever (even
with modern preparation concepts like slot,
tunnel, or minibox restorations), and this will
lead to the continuum of replacement den-
tistry,5,6 with repeatedly enlarged restorations
and increased damage of hard tissues.
Moreover, invasive and even minimally or
microinvasive restorative procedures might
be associated with postoperative sensitivity
or pathogenic pulpal reactions, sometimes
requiring highly destructive endodontic treat-
ment solutions.
However, a cavity is but a symptom of the
disease, because the term caries means
rather the process than simply a lesion
resulting from that process. Therefore, dis-
covering a frank cavity is not equivalent to
caries diagnosis, and caries diagnosis—if
defined as an intellectual course of collecting
and consolidating data obtained by clinical
Fig 1a to 1f (a) Initial bitewing radiograph revealing a proximal caries lesion at the distal aspect of the mandibular first molar.(b) Preoperative view with undermining caries visible distally. (c) Intraoperative view with rubber dam placement.(d) Etching of completed cavity preparation (matrix, wooden wedge, and G-ring to ensure tight proximation). (e) CompletedClass 2 restoration after finishing. (f) Clinical view 1 week after placement of restoration.
a cb
d fe
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 665
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
and radiographic examination along with the
use of objective diagnostic armamentarium,
biologic knowledge, and information gained
from anamnesis—will be much more than
detecting breakdown of surfaces.6 Indeed,
the concept of minimum intervention den-
tistry should be tantamount to preservative
dentistry, and should embody at least 5 gen-
eral principles7,8:
• Scientifically oriented caries diagnosis of
early lesions using adequate diagnostic
devices
• Disease control by reduction of cariogenic
bacteria/modification of the oral flora and
patient education
• Remineralization of the earliest lesions
• Minimum surgical intervention of cavitat-
ed lesions
• Repair in favor of replacement of defective
restorations
Proximal caries constitutes a large health
problem for high-risk patients; at the age of
21 years, up to 50% of patients show carious
or restored proximal surfaces,9 and lack of
compliance with preventive behavior by
these patients is still a major problem.10,11 In
recent decades, a much more tissue-
preserving approach to arrest and control
proximal or smooth-surface caries lesions
has been studied extensively; this concept
aims at occluding the highly porous struc-
tures of incipient enamel lesions by means of
low-viscosity resins, and has been called
penetration,12 plastification,12 (therapeutic)
sealing,13,14 infiltration,12,15 impregnation,12,16
noninvasive,17 or ultraconservative18 tech-
nique. In medicine, infiltration means the act
or process of infiltrating (as of liquids) into the
pores or cavities of a substance; thus, this
term seems most appropriate to describe the
treatment approach using low-viscosity resin
mixtures with high penetration capabilities
on subsurface enamel lesions.
The purpose of this article is to present the
scientific basis and the principles of the resin
infiltration technique, to discuss the inherent
clinical applications (which are considered
microinvasive), and to describe how these
backgrounds can be transferred into clinical
practice.
DATA SOURCES AND STUDY SELECTION
We searched The Cochrane Library, Medline,
and Scopus for relevant articles up to
December 2008. The search was supple-
mented by manual searching of reference
lists from each relevant article identified. The
main search terms were adhesive, demineral-
ization, artificial caries, enamel, sealant, sub-
surface lesion, and white spot lesion. Articles
published in English and German through
December 2008 were selected, and most
up-to-date or relevant references were cho-
sen. Cross-referencing of significant articles
identified additional relevant articles written in
other languages and those of historic value.
The research resulted in 23 experimental and
3 clinical articles.
Three fields of interest were identified—
reaction of resin with artificial enamel lesions,
13 studies; natural enamel lesions, 4 studies;
and sound enamel, 7 studies. Only original
experimental articles were considered (see
compilation of in vitro studies, Table 1), but
for completeness reasons, interim and case
reports or abstracts were not excluded from
this review.
INITIATION OF THECARIES PROCESS—SUBSURFACE WHITESPOT FORMATION
The roles of plaque and saliva in the initiation
and progression of dental caries are summa-
rized schematically in Fig 2. A central feature
is the generation of organic acids by acido-
genic plaque bacteria following the dietary
intake of carbohydrates such as sucrose.
Saliva performs 2 direct functions to combat
enamel dissolution by these acids: (1) The
continuous flow of saliva acts to clear the
acids from the mouth, and (2) a number of
diverse salivary constituents have “caries-
protective activity.” The latter constituents
can act on the acids themselves (via buffer-
ing or neutralization), on the bacteria (via inhi-
bition of the metabolic processes involved in
acid production), and on the enamel (by
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

QUINTESSENCE INTERNATIONAL
Kielbassa et a l
maintaining chemical supersaturation in the
adjacent plaque fluid). A key indirect function
of saliva is as a medium for the transfer of
potentially active therapeutic agents, such as
fluoride, to the site of action.
From a recent study, it seems that good
oral hygiene habits, established in early child-
hood, provide a foundation for a low experi-
ence of proximal caries in adolescents.11
Moreover, overweight and obese adoles-
cents had more proximal caries than normal-
weight individuals. Thus, the frequent con-
sumption of snack products during early
childhood appears to be a risk indicator for
caries at age 15.11
Demineralization and remineralization are
2 dynamic processes of dental caries in
which chemical composition plays a key role.
Type of Commercially available/
Evaluation
Pub. Ref. No. of Type ofdemineralization
Surface experimental Inhibition ofyear no. teeth enamel Gel Solution etch material Penetration demineralization
1989 110 15 Human x H3PO4 (37%; 60 s) Com. Resin tags Yes1992 87 48 Human x H3PO4 (36%; 60 s) Com. Yes (strong bond, Not studied
withstands thermocycling)
1997 65 20 Human x H3PO4 (37%; 20 s) Com. Not studied Yes2001 86 27 Human x H3PO4 (10%; 15 s) Com./Exp. Yes Yes2002 94 40 Human x H3PO4 (36%; 5 s) Com. Yes Not studied2003 109 15 Human x H3PO4 (37%; 60 s) Com. Not studied Yes2004 101 10 Human x H3PO4 (35%; 120 s) Com. Yes Not studied2005 95 27 Bovine x H3PO4 (20%; 5 s) Com. Yes Not studied2006 96 27 Bovine x H3PO4 (20%; 5 s) Com. Yes (best with Not studied
prolonged application time)
2006 106 27 Bovine x H3PO4 (20%; 5 s) Com. Yes Yes2006 107 27 Bovine x H3PO4 (20%; 5 s) Com. Yes Yes (not with
all resins)2007 97 27 Bovine x H3PO4 (20%; 5 s) Com. Yes (best with Not studied
high penetration coefficient)
2008 98 40 Bovine x H3PO4 (37%; 5 s) Com./Exp. Yes (best with Yeshigh penetration coefficient)
1975 12 24 Human Artificial/natural lesions H3PO4 (50%) Exp. Yes (if surface Not studiedetched)
1976 15 25 Human Natural lesions HCl (1 N; 5/10 s) Exp. Yes Not studied2007 93 30 Human Natural lesions HCl (15%; 120 s) Exp. Yes (best with Not studied
HCl etching)2008 108 40 Human Natural lesions HCl (15%; 120 s) Com./Exp. Yes (best with Not studied
high penetration coefficient)
1996 112 40 Human Sound enamel No information Com. Inhibition of demineralization2000 100 60 Human Sound enamel H3PO4 (35%; 60 s) Com. Full penetration of commercial
material with low viscosity2000 111 8 Bovine Sound enamel Citric acid (10%; 15 s) Exp. Inhibition of demineralization2003 109 10 Human Sound enamel H3PO4 (37%; 60 s) Com. Inhibition of demineralization2005 105 80 Bovine Sound enamel H3PO4 (35%; 60 s) Com./“Patch” Inhibition of demineralization2005 113 32 Human Sound enamel H3PO4 (35%; 30 s) Com. Inhibition of demineralization2005 115 40 Human Sound enamel H3PO4 (37%; 60 s) Com. Inhibition of demineralization
(H3PO4) Phosphoric acid; (HCl) hydrogen chloride.*Experimental design and main outcome of resin infiltration on artificially demineralized specimens and natural caries or sealants on sound enamel are given.
Table 1 Compilation of in vitro studies*
666 VOLUME 40 • NUMBER 8 • SPETEMBER 2009
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 667
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
The driving force for de- and remineralization
of tooth mineral is the degree of saturation
with respect to dental minerals in the adja-
cent liquid. The main inorganic anions are
chloride and inorganic phosphate, while
short-chain organic acids include lactic,
acetic, propionic, succinic, formic, pyruvic,
and butyric acids.19 The main cationic com-
ponents are ammonium, potassium, magne-
sium, and calcium. After repeated episodes
of prolonged exposure to acidic conditions
consistently below the critical pH (5.5) for
enamel dissolution, demineralization starts
as dissolution of apatites from the enamel
prisms. In the face of failure to remove
plaque from retentive tooth areas, with a diet
high in refined carbohydrates, the dynamic
equilibrium between demineralization and
remineralization will be tipped toward dem-
ineralization, and this will result in clinically
detectable white spot lesions.20
Without regular mechanical disturbance
of dental plaque,21 and with continuing de-
mineralization (and without the benefit of re-
mineralization), an initial subsurface lesion
will appear, and 2 zones of demineralization
can be histologically visualized now (Figs 3a
and 3b): the translucent zone (1% pore vol-
ume) at the advancing front, and the body of
the lesion (up to 25% pore volume).22
Dissolution may start at the prism cores,23
and mineral losses of up to 50% have been
observed at interprismatic areas and from
the prism peripheries.24 Moreover, 2 zones of
remineralization are present: the dark zone
(2% to 4% pore volume), and the surface
zone (< 5% pore volume) forming the
pseudointact surface overlying the lesion.22
The surface layer has a varying thickness of
some 40 µm and a mineral content of up to
82 vol%.25 These values are considerably
higher than with artificial lesions.26
TRADITIONAL TREATMENT OPTIONS
As long as the initial white spot lesion has an
intact surface (see Figs 3a and 3b), the most
effective means of caries control is an ade-
quately performed oral hygiene including the
complete removal of dental plaque using
mechanical means such as toothbrushing
and flossing.27 However, while flossing in par-
ticular seems to be a reasonable recommen-
dation for proximal surfaces, its preventive
effect has not been supported by evidence
up to now, neither with regard to gingival
health28 nor proximal caries,29 and only the
professional use on a supervised basis has
been identified to reduce caries risk (in chil-
dren).29,30 This way, arrest of the lesion may
be achieved, and remineralization becomes
possible; remineralization is the natural repair
process for noncavitated lesions (occurring
daily to repair the smallest demineraliza-
tions), and it relies on calcium and phos-
phate ions assisted by fluoride. However,
optimal conditions are mandatory to ensure
repair or healing by deposition of mineral on
existing damaged crystals or nucleation and
de novo crystal formation.20
Moreover, the additional use of antimicro-
bials (ie, chlorhexidine) should limit bacterial
growth and increase oral health.27 However,
caries-preventive properties of chlorhexidine
mouthrinses are limited, and most results are
inconclusive. A recent in situ study did not
Fig 2 Schematic diagram of the plaque-tooth interface (adapted andmodified from Duckwork and Gao19). Reprinted with permission fromS. Karger AG, Basel, Switzerland.
Pellicle
Saliva
Sugar
Acid
Enamel
Demineralization
Ions
Buffers
HCO3-
PI
PI
Ca2+
Ca2+CL-
K+
Dentalplaque
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

668 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
show any preventive effects of mouth rinsing
with 0.2% chlorhexidine, neither on acid
production of plaque samples nor enamel
demineralization.31 Moreover, chlorhexidine
obviously hampers fluoride accumulation
on tooth hard substances.32 Based on the
available literature, chlorhexidine rinses
(along with chlorhexidine gels and varnishes)
do not seem to be recommendable for caries
prevention.33
The use of topical fluorides to enhance
remineralization of demineralized proximal
enamel has been advocated.27 Application of
fluoride varnish every third month significantly
reduced the progression of proximal caries
lesions in premolars and molars. The most
obvious reduction of caries progression was
observed among children with moderate
caries risk, while children with high caries
activity (more than 9 new proximal lesions) did
not benefit from proximal caries reduction.34
However, in a recent study, caries prevention
of fluoride varnish treatment twice a year at 6-
month intervals was 69% in high-risk areas,
66% in medium-, and 20% in low-risk areas.35
Additionally, with fluoride mouth rinsing,
reduced caries incidence on proximal sur-
faces could be observed in adolescents with
low to moderate caries risk as well.36 All in all,
fluorides have been considered as an excel-
lent caries prevention strategy for proximal
surfaces in adolescents at the caries risk
ages of 13 to 16 years, and as a supplement
to oral home care and preventive efforts at
dental clinics.37 However, fluorides are not
able of completely preventing onset or pro-
gression of proximal caries in the long
term.9,38
There is some evidence that the use of
topical fluorides reduces the occurrence and
severity of white spot lesions, for example,
during orthodontic treatment; unfortunately,
Figs 3a and 3b (a) Proximal caries lesion with a smaller extent than the one treated in Fig 1. (b) Polarizingmicrograph of the slab from the same tooth (imbibed with quinoline), depicting a lesion not confined toenamel.
a b
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 669
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
it remains unclear which method or combi-
nation of methods to deliver the fluoride is
the most effective. Based on current best
practice in other areas of dentistry for which
there is evidence, it has been recommended
that patients with fixed brackets rinse daily
with a 0.05% sodium fluoride mouthrinse.39
These observations emphasize that the use
of fluorides is mainly a primary prevention
component, because fluoride aims to ham-
per demineralization and have a preventing
effect on developing lesions.
Indeed, studies on true remineralization of
proximal lesions are limited to only a few arti-
cles.40–42 It has been pointed out that even
with noncavitated proximal lesions, the caries
process may gradually progress to cavita-
tions if no preventive treatment is undertak-
en.43 Thus, because the enamel surface will
not be restored by salivary repair mecha-
nisms once a substantial loss of surface min-
erals has occurred (and surface discontinuity
is evident), plaque accumulation is regarded
as unavoidable in this situation. This might
explain why even small radiolucencies tend
to progress, albeit slowly.44
Therefore, close follow-ups should strong-
ly be recommended when considering a
preventive treatment regimen with small radi-
olucencies of proximal surfaces. The
process of caries development occurs over a
substantial length of time: Indeed, average
survival times of proximal lesions confined to
enamel of up to 8 years have been report-
ed.45 With regard to the treatment decision,
great variations in the thresholds of interven-
tion based upon lesion depth seen in radi-
ographic images among clinicians from vari-
ous countries have been observed. A con-
siderable number of professionals still tend
to practice invasive techniques; with lesions
confined to enamel, the decision to prepare
a cavity ranged from 19% in Norway46 to
nearly 50% in Mexico47 and Brazil,48,49 but
with even higher proportions in other coun-
tries.50,51 These values indicate an interven-
tionist attitude, which clearly could result in
overtreatment when remembering the slow
progression of enamel lesion development.
REMINERALIZATION OF (PROXIMAL) LESIONS
Due to the relative thickness and the consid-
erably high mineral contents, the pseudoin-
tact surface layer has been suspected to
inhibit remineralization. Therefore, the use of
acid etching52 and the acidulation of calcified
fluids53 have been investigated in vitro and
found to increase the surface porosity and to
facilitate remineralization.54 These proce-
dures obviously created a more pronounced
remineralization effect, thus indicating that
the surface of an incipient lesion constitutes
a barrier for remineralizing fluids; recently, an
effective reduction in the surface layer of nat-
ural enamel caries was achieved by etching
with a hydrochloric acid gel (15%; 90 to 120
seconds).55 Indeed, a 10-week remineraliza-
tion study using this acid-etch strategy
showed significant differences in lesion
depth, mineral content at the surface layer,
and integrated mineral loss between etched
and nonetched groups. However, addition of
fluoride accelerated the remineralization
process only in the beginning; in later stages,
the process leveled out and even reached a
plateau in all the groups, and it was conclud-
ed that full remineralization was not achieved
by etching, the addition of fluoride, or the
combination of treatments.56
Clinically, the degree of remineralization
seems to be limited, and this has been attrib-
uted to the presence of organic substances
attaching to the enamel surface and possibly
occluding the underlying pores in the caries
lesion.20,57,58 Moreover, the role of possible
remineralization inhibitors is not clearly
understood; the ability of albumin to bind and
to inhibit growth of calcium phosphate crys-
tals raises the question as to the possible role
of such molecules in the development of
caries lesions.59 Notwithstanding, mucins
have been shown to inhibit demineralization60
and to promote remineralization.61 In minimal
intervention dentistry (Fig 4), remineralization
or arrest of lesions should be utilized to a
maximum, because there is no real substitute
for natural tooth structure.
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

670 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
CLINICAL OBSERVATIONSON WHITE SPOT LESIONS
Concerning the fate of initial caries lesions
on smooth surfaces, the article by Backer
Dirks,62 showing that some 51% of early
white spot lesions might disappear after sev-
eral years, has been cited innumerable
times. A large part of the quoting articles
referred almost exclusively to remineraliza-
tion effects, and since that time, the profes-
sion has been increasingly attracted by the
concept of remineralization.63 Interestingly, in
a study similar to that of Backer Dirks62 only
13% of white spot lesions disappeared, while
50% showed no changes.64 In these 2
(uncontrolled) studies,62,64 the authors did
not clearly differentiate between active
(chalky, rough surface) and inactive (shiny,
hard surface) lesions, and lesion disappear-
ance has been attributed to either elimination
of caries challenge or remineralization.65
In a randomized clinical trial comparing
treatment with fluoride varnish and profes-
sional tooth cleaning for remineralization of
white spot lesions in caries-active adoles-
cents, there was a significant difference in
mean change in fluorescence between the 2
test groups; however, for lesion areas, no sig-
nificant differences could be observed.66 In
another study, adjunctive weekly brushing
with amine fluoride gel achieved no signifi-
cant enhancement of remineralization of
active white spot lesions monitored with the
Quantitative Light Fluorescence (QLF)
method, when compared to brushing alone
with amine fluoride dentifrice.67 This was cor-
roborated in another randomized clinical
study; here, long-existing white spot lesions
were observed over 6 months. The effective-
ness of dentifrices containing either sodium
fluoride (1,500 ppm) or amine fluoride (1,250
ppm) was not significantly different, and the
long-existing white spot lesions were stable
concerning fluorescence loss over the lesion
area. Moreover, fluorides did not seem to
have any effect on long-existing white spot
lesions.68
In a clinical study on postorthodontic de-
mineralized white spot lesions, demineralized
areas reduced by approximately half their
original size during the 6 months after treat-
ment.69 Again, the intervention using a low
fluoride test mouthrinse and dentifrice com-
bination compared with a nonactive control
combination failed to show any differences
or therapeutic effect; however, once formed,
many of these early lesions appear to be sur-
face demineralization, rather than a subsur-
face lesion with an intact surface zone,69 and
in these situations, abrasive effects are very
common. This would be in accordance with
other observations indicating that superficial
lesions seen after orthodontic treatment will
tend to disappear (“remineralize”) more rap-
idly and completely than deeper lesions on
removal of the cariogenic challenge.70
In his original work, Backer Dirks62 specu-
lated on either remineralization, abrasion, or
even both when trying to explain the clinically
observable disappearance of the smooth-
surface white spot lesions after several years.
When considering that white spot lesions on
smooth surfaces disappeared while proximal
caries obviously did not,62 and abrasion and
early recession are common in patients with
good oral care,71 the results of a previous
study seem to support the idea that tooth-
brushing on smooth surfaces might con-
tribute to abrasion of initial caries, in particular,
if vigorous toothbrushing is implemented as a
part of oral hygiene.26
Fig 4 Essential aspects of diagnosis and treatment planning. Resininfiltration fills the gap between oral hygiene and minimally invasivedentistry and can be integrated into the minimal intervention conceptof operative dentistry (adapted and modified from Mount and Ngo5).
Minimal intervention dentistry
Evaluation
SalivaMicrofloraDietSurface riskGeneral health
Diseasecontrol
Prevention Remineralization
Infiltration
Maximization of remineralization potentialDisruption of demineralization cyclesEducation and motivation
Maintain toothintegrityBiomimetic materialElimination cavitation
Treatmentneed
Adequate diseasecontrolCompromisedtooth integrityPatient agreement
Damagerepair
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 671
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
This would agree with scanning electron
microscopy (SEM) observations on demin-
eralized areas that formed beneath orthodon-
tic bands.70 Here, developmental white opaci-
ties had a higher luminance (ie, were whiter),
and the boundaries were more circular than
the postorthodontic caries lesions.72 Exam-
ination of definite white spot lesions revealed
characteristic patterns of initial tissue destruc-
tion. Focal holes and an accentuation of the
perikymata were observed affecting the
enamel surface zone (an area previously con-
sidered to remain relatively intact during the
development of a caries lesion).70 Another
SEM study on the fate of subsurface lesions
revealed a general tendency toward leveling
of the surface of the lesion indicating a loss of
porous tissue,73 probably by attrition/abrasion
due to functional wear and/or toothbrushing.74
These findings confirmed that removal of car-
iogenic challenge results in arrest of further
demineralization. However, the gradual regres-
sion of the lesion at the clinical level was
believed to be primarily a result of surface
abrasion.73,75
With proximal caries, it has been argued
that once a lesion is cavitated, it can no longer
be cleaned with flossing by the patient and,
hence, tends to progress,76,77 because the
constantly metabolically active biofilm cannot
be controlled. Therefore, from this threshold
an operative intervention is generally recom-
mended to prevent further lesion progression.
Unfortunately, the bitewing radiograph does
not give any direct information on the surface
integrity of proximal lesions. Clinical stud-
ies78–81 found comparably few cavitations in
R3 (radiolucency reaching the outer dentin on
bitewings) lesions (22% to 52%), while several
laboratory studies confirmed a considerably
earlier cavitation, with breakdown of surfaces
in up to 100% of R3 lesions (for review, see
Kielbassa et al44,82). Interestingly, gingival
bleeding has been shown to be related to sit-
uations with progressing proximal caries,83
and, according to the thoughts presented
here, possibly with breakdown of surfaces
(and higher accumulation of plaque). Caries
may be a multifactorial disease, but dental
plaque remains the only cause. Indeed, this
might be an explanation for the slow (but often
constant) progression of proximal lesions.43
Reliability of diagnosing precavitated
caries lesions for smooth (and proximal)
tooth surfaces has been shown to be poor.84
In this context, in clinical studies access to
the proximal space often is limited, thus lead-
ing to a possible underreporting of cavita-
tions. Moreover, a previous study reported a
sensitivity of only 76% for the clinical obser-
vation of R3 lesions with the naked eye after
tooth separation.85 Accordingly, it might be
speculated that clinical recording of small
cavities is extremely difficult during prepara-
tion procedures (Fig 5).
THE RESIN INFILTRATIONCONCEPT
Laboratory studies on penetrationdepthsFrom early histologic experiments, it is well
known that enamel lesions can be imbibed (in
water or quinoline; see Fig 3), because of the
increased microporosities of the different his-
tologic zones. Moreover, these tiny porous
openings and widened intercrystalline spaces
act as diffusion pathways for acids and dis-
solved minerals. With this in mind, it should be
possible to infiltrate incipient lesions with
other liquids, ie, with low-viscosity resins.
Thus, instead of removing the porous carious
tissue at a relatively late stage in the disease
process, attempts have been made to “fill” the
microporosities of lesions at a much earlier
stage of lesion development. This would not
only reduce the microporosities (and there-
fore the access of acid), but also afford some
mechanical support to the tissue.86
Early descriptive studies from the
1970s12,13 indicated that the adhesive encom-
passes the residual (in)organic materials of
the demineralized portions, thus transform-
ing the lesion into an acid-resistant unit.12
While artificial lesions can be infiltrated with a
comparable outcome, natural white spot
lesions have to be acid etched before infiltra-
tion.12,15,55 This obviously is due to the thick-
ness, and the low porosity/high mineral con-
tent of the surface layer (see above),25 and
due to organic substances found in natural
caries.59 However, it was found that a resin
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

672 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
infiltration depth of 60 µm was sufficient to
prevent further demineralization, even if the
surface coating had been dislodged.12
In a pioneering attempt at resin infiltrants,
well-defined requirements for potentially use-
ful materials were characterized. These mate-
rials should be:
• Hydrophilic
• Highly surface active and with low viscosity
• Bacteriostatic
• Nontoxic to oral tissues
• Polymerizable to a solid state
• Resistant against chemical and mechani-
cal challenges of the oral cavity
• Cosmetically acceptable15
Successful infiltration of materials into
lesions was demonstrated using resorcinol-
formaldehyde,15 which, however, was clinical-
ly unacceptable. Nevertheless, the results
showed that up to 60% of the lesion pore vol-
ume had been occluded following infiltration
and that this treatment was capable of reduc-
ing further acid demineralization.15
Acid conditioning of artificial subsurface
lesions with phosphoric acid revealed an
etching pattern similar to sound enamel.
Bonding to etched subsurface lesions
proved to be reliable, and was able to with-
stand thermocycling. Thus, it was concluded
that subsurface lesions are an acceptable
and suitable substrate for resin adhesion.87
However, the surface of natural white spot
lesions has been revealed to be more resist-
ant to phosphoric acid etching than adjacent
sound enamel.88
Further experiments revealed that viscosi-
ty, surface tension, and contact angle on
human enamel influence the penetration of
restorative resins into acid-etched enamel;
however, viscosity of the monomer mixture
was not shown to be a limiting factor for the
penetration of restorative resin monomers
into the pores of etched enamel surfaces,89
and depth of penetration decreased only
slightly with changing viscosity. Interestingly,
tag lengths (representing the penetration
depth) of up to 50 µm or more were observed
with composite as well as with non–composite
resins on (noncarious) phosphoric acid–
etched enamel.90–92 In a recent article, similar
penetration depths after surface conditioning
with hydrochloric acid were found in natural
lesions.93 Some commercially available adhe-
sives (sealants, bonding agents) have been
shown to be suitable for infiltration of artificial-
ly induced subsurface lesions, as well,94–96 but
significant differences could be revealed with
artificial lesions, when various resin infiltrants
Figs 5a and 5b Mesial surface of a maxillary premolar revealing a radio-lucency confined to the outer half of enamel (R1). The clinical situation(a) indicates a roughened surface and accentuated imbrication lines.SEM of the same lesion (b), depicting a breakdown of surface and micro-pores not considered remineralizable.
a
b
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 673
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
with differing penetration coefficients were
used.97 This has been corroborated with natu-
ral lesions recently,98 thus indicating that resin
infiltrants with high penetration coefficients99
are able to penetrate more deeply into sub-
surface lesions. In Fig 6, a typical example of
a resin infiltrated lesion is shown.
A previous SEM study on sealant penetra-
tion into etched fissures seems to confirm
these observations. Here, a low-viscosity
sealant penetrated fully and formed a resin-
infiltrated layer in enamel beyond the etched
depth. However, the high-viscosity sealants
used in that study did not penetrate enough
to ensure that the acid-etched enamel was
infiltrated sufficiently by the sealant to insure
good marginal seals.100
Another factor seems to be the degree of
microporosities. Penetration of an unfilled
resin into enamel was considerably influ-
enced by the degree of dental hard tissue
mineralization. Resin tags in demineralized
enamel were significantly longer (some 60
µm) than in other groups, and penetration
decreased significantly in remineralized areas
or after use of fluoride; however, this was still
significantly deeper than in control sites, and
remineralized enamel also allowed good pen-
etration of the unfilled bonding agent.101
Various modifications (additionally to acid
concentration and etching time) of the appli-
cation technique have been proposed to
improve the penetration depths in sound but
etched enamel. Ultrasonic treatment during
Figs 6a to 6c Light microscopic (a) aspects of a perpendicularly cut proximal surface of a molar showing a white spotlesion. Confocal laser scanning micrograph (b) of corresponding lesion confined to outer enamel, depicting the principle ofresin infiltration into subsurface lesions and revealing resin-infiltrated parts of the lesion (green, resin infiltrant labeled withfluorescent dye, fluorescein isothiocyanate [FITC]). SEM of the same lesion (c), confirming obturation of demineralized areas(note that at deeper lesion aspects, micropores have not been occluded).
a b c
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

674 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
etching procedure and drying of etched fis-
sures by means of acetone increased the
mechanical interlocking considerably.102 Re-
cently, it has been shown that conventional
phosphoric acid etching (if used alone) has
some limitations, and a deproteinization pre-
treatment using sodium hypochlorite (5.25%;
60 seconds) before etching revealed favor-
able results with regard to the retentive sur-
face.103 The additional use of alcohol has also
been advocated to dry the lesion areas,94 and
future studies should evaluate these addition-
al pretreatment regimens with regard to a
possibly increased penetration depth of resin
infiltrants. In Table 1, the respective studies
on penetration of subsurface lesions are
compiled.
Laboratory studies on preventionof lesion progressThe initiative to arrest caries by infiltration of
resins has been followed since the initial
studies mentioned above,12,13,15 and the
advent of dental adhesives with potentially
suitable properties has prompted a reexami-
nation of this concept in recent years.
In an early study resembling the infiltration
technique, the applied resin was aggressive-
ly air thinned to ensure oxygen inhibition
throughout the external surface film thick-
ness. In the absence of a polymerized outer
surface film, the infiltrated lesions showed a
reduced degree of demineralization, and an
experimental fluoride resin did not produce
statistically significant differences when com-
pared to a fluoride-free resin.104 Several
recent studies on artificial carieslike lesions
have demonstrated that commercially avail-
able adhesives having infiltrated the micro-
pores of the demineralized areas revealed a
considerable reduction of lesion progression
by either double application86,105,106 or extend-
ed penetration times (30 seconds compared
to 15 seconds).107 Using infiltrants with high
penetration coefficients facilitated inhibition
of lesion progression, thus showing that resin
infiltration sufficiently occludes the acids’ path-
ways and hampers demineralization.108 This
beneficial effect could be confirmed even
after thermocycling; when placed on acid-
etched surfaces, the resin adhered firmly to the
enamel with no evidence of demineralization
or enlargement of previously demineralized
areas underneath the sealants (see Table
1).109
A similar (but indeed different) approach
aimed at placing a physical barrier between
(carious) enamel and potentially cariogenic
biofilms. This concept has been retransmit-
ted from occlusal surfaces, where fissure
sealing has been performed successfully for
decades. Application of a thin layer of sealant
onto acid-etched artificial lesions has been
described as successfully improving the
resistance of subsurface lesions against
cariogenic challenge.110,111 Indeed, this was
not astonishing when regarding the already
known protective effects of fissure sealants;
a further concept has used an adhesive
patch as a barrier to block microorganisms
and their respective acids. This adhesive
patch also proved to be resistant against
acidic attacks.105
With “orthodontic” sealants, similar results
could be observed. Light-cured sealant treat-
ment after orthodontic appliance placement
significantly reduced or even prevented enam-
el demineralization.112,113 In another study,
demineralization in the sealant group was
reduced significantly, and teeth treated with
fluoride varnish exhibited 30% less demineral-
ization than the control teeth. Usually, sealants
are applied after acid etching, and removal of
surface coating after completion of orthodon-
tic therapy will leave resin tags in formerly
etched enamel; these areas have been shown
to be caries resistant as well.114 Therefore, par-
ticularly in patients who exhibit poor compli-
ance with oral hygiene and home fluoride use,
sealing has been recommended.115
In vivo studies proving the concept of resin infiltrationA recent SEM study on in vivo sealed (Clinpro
Sealant, 3M ESPE; with and without a pre-
ceding bonding) natural subsurface lesions
demonstrated an irregular resin network with
twisted and curved tags, while with the sound
enamel areas a regular etching pattern was
observed. Resin tag lengths were consider-
ably short and ranged from 4.2 to 5.5 µm. No
increased penetration depths could be
observed after the additional use of a low-
viscosity adhesive bonding agent (Single
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 675
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
Bond, 3M ESPE). No further pretreatment of
enamel was performed, and acid etching of
the surface zone was done with a phosphor-
ic acid gel.116 Penetration depths of the
sealant were somewhat higher in another
study using the same design; however, pre-
treatment with a bonding agent resulted in
decreased tag lengths.117 Nevertheless, in
both studies, a physical barrier was formed,
with protective function against exposure of
acids from bacterial origin, and cutting off
possibly remaining bacteria (within an
advanced lesion) from a nutritional supply of
fermentable carbohydrates.14
This was corroborated in a clinical study
on sealed (Gluma One Bond, Heraeus
Kulzer; or Concise Sealant, 3M ESPE; 18
months, 72 patients) proximal early active
lesions. As validated by subtraction radiogra-
phy, 43.5% of the sealed proximal lesions
had progressed during the 18-month study,
while 84.1% of the untreated controls (floss-
ing) showed increased demineralization
depths,118 thus indicating a reduced (and not
an arrested) progression rate for the proce-
dure. Interestingly, deeper test lesions
showed lower progression rates (33.0%)
when compared to untreated control sites,
thus reemphasizing the results already
known from fissure sealants119 to some
extent. From these observations, it might be
speculated whether lesion arrest over longer
periods after infiltration is due to reduced
microorganism viability or physical barrier
against acids from bacterial origin.120
A second clinical study on sealed (Concise
Sealant; 2 years, 50 patients) proximal sur-
faces17 (no data could be combined with the
latter trial,118 due to the diversity between the
studies) revealed that only 7% to 8% of the
sealed lesions showed progression, com-
pared to a 12% rate in the control group (flu-
oride varnish).17 This study did not use sub-
traction radiography for evaluation; thus, the
evaluated values are best compared to the
individual visual assessment values of the
study mentioned above; here, the correspon-
ding values were 9.7% for sealed lesions and
26.4% for the control group.118 In total, these
results show a tendency that would be com-
parable with the outcomes of a recent study
on occlusal fissure sealing; here, caries pro-
gression was highest in the control group,
and this was followed by the fluoride varnish
and the sealing group as well.121 However,
more clinical studies are clearly warranted.
Orthodontic treatment with fixed appli-
ances has been associated with white spot
lesions that often occur in otherwise well-
treated cases. The overall prevalence among
orthodontic patients is comparably high (up
to 44%),122 depending on the methods used
to assess and score decalcification, the pres-
ence of decalcification before treatment, and
the use of fluoride supplements during treat-
ment. A recent study revealed that the used
sealant (UltraSeal XT Plus, Ultradent) suc-
ceeded in preventing enamel from deminer-
alization. Unsealed teeth had a 3.8 times
greater number of white spot lesions than did
the teeth with sealants.123 However, it is inter-
esting to note that the sealant failed to protect
the entire enamel surface in 2 patients, obvi-
ously because of a failure of the sealant to
completely bond to the enamel surface,123
thus indicating that a thorough control of the
technique seems mandatory. Up to now, stud-
ies on infiltrant or sealant retention on (proxi-
mal) smooth surfaces with incipient lesions
are lacking. Nonetheless, a recent clinical
study on (proximal) adhesive patches showed
promising results since lesion progress was
predominantly arrested and remained stable
over a 2-year period, even after loss of the
patch. This indicated the postive effects of the
underlying bonding material.124
Advantages of the resin infiltrationconceptCaries-related clinical decision making
remains a centerpiece of clinical dentistry.
However, most dentistry still is re-dentistry
(with continued restorative procedures nec-
essary within the life span of the patient), and
the traditional core skills, along with the man-
ual dexterity and technical competence, have
less to offer to oral health than many clini-
cians have been accustomed to think. From
the foregoing review, it seems clear that the
resin infiltration technique bears several
advantages. These include:
• Mechanical stabilization of demineralized
enamel
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.
676 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
• Preservation of sound hard substance
(protection of both the same and the adja-
cent tooth)
• Permanent occlusion of superficial micro-
pores and cavities
• Obturation of porous, deeply demineral-
ized areas
• Arrest of lesion progress
• Minimized risk of secondary caries
• Delay of restorative intervention for longer
periods
• No risk of postoperative sensitivity and
pulpal inflammation
• Reduced risk of gingivitis and periodontitis
• Improved esthetic outcome when used as
a “masking” resin on demineralized labial
surfaces (white spot lesions, ie, with ortho-
dontic patients)
• High patient acceptance
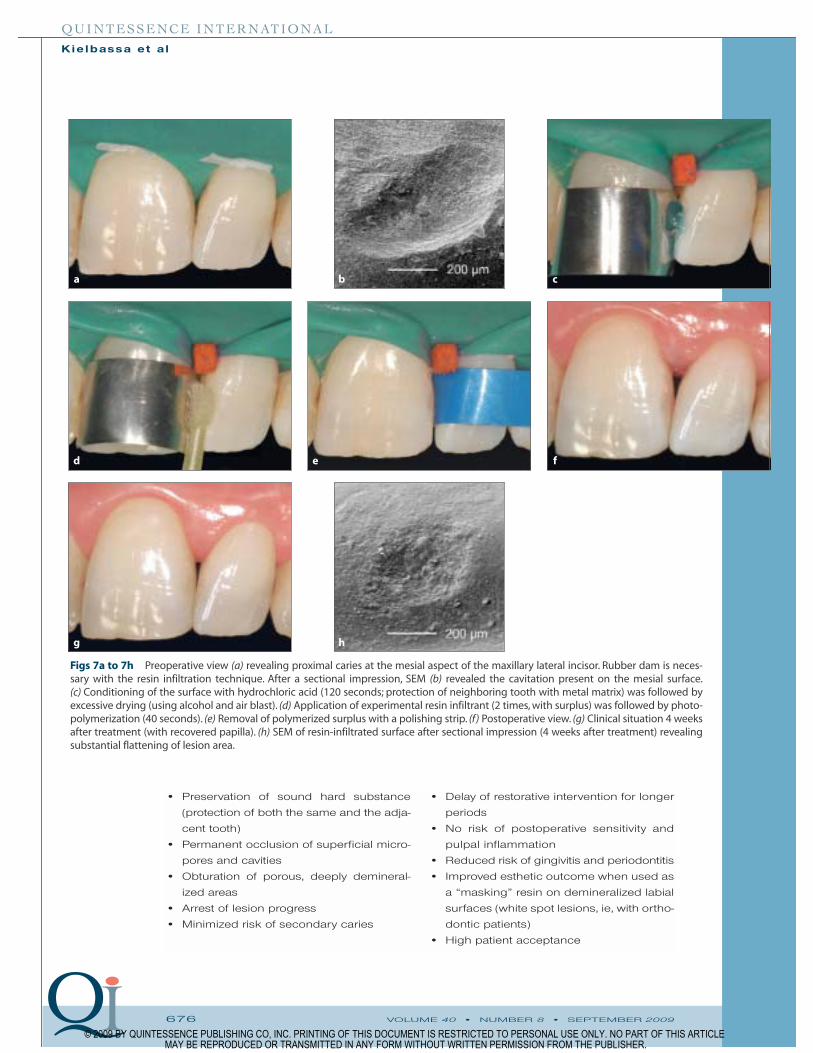
Figs 7a to 7h Preoperative view (a) revealing proximal caries at the mesial aspect of the maxillary lateral incisor. Rubber dam is neces-sary with the resin infiltration technique. After a sectional impression, SEM (b) revealed the cavitation present on the mesial surface.(c) Conditioning of the surface with hydrochloric acid (120 seconds; protection of neighboring tooth with metal matrix) was followed byexcessive drying (using alcohol and air blast). (d) Application of experimental resin infiltrant (2 times, with surplus) was followed by photo-polymerization (40 seconds). (e) Removal of polymerized surplus with a polishing strip. (f) Postoperative view. (g) Clinical situation 4 weeksafter treatment (with recovered papilla). (h) SEM of resin-infiltrated surface after sectional impression (4 weeks after treatment) revealingsubstantial flattening of lesion area.
a b c
g h
d e f
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 677
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
Therefore, regarding the impact on the
clinical decision process, a longitudinal clini-
cal risk assessment to discriminate between
progressive and remineralized lesions should
be established. Within the concept of minimal
intervention dentistry,7 the infiltration
approach seems suitable in case of early
treatment decision needs; at the same time,
even for later stages of the caries process
(in case remineralization with fluorides is not
considered a viable approach) this concept
should be an alternative to any type of cavity
preparation (see Figs 6 and 7), thus at least
postponing (if not avoiding) sacrifice of sound
structures. For protection reasons, and to
ensure dryness, use of rubber dam is recom-
mended with the resin infiltration technique.
Finally, resin infiltrants can be combined with
conventional resin restorations in case of
more complex treatment situations (Fig 8),4,18
and this should help to preserve dental hard
tissues.
CONCLUSIONS
With regard to the implications for practice,
resin infiltrants and some (un)filled resins obvi-
ously have a favorable penetration potential in
subsurface enamel lesions. In view of the
results presented in the current review, the
resin infiltration technique is a promising
microinvasive approach to preserve (deminer-
alized) enamel. With the use of adequate
materials with a sufficient resistance to
mechanical and chemical degradation, and
with a careful application technique, lesion
arrest seems achievable on a supervised
basis, thus closing the gap between oral hy-
giene and minimally invasive dentistry, and
providing a wait-and-see position to both the
clinician and the patient.
When reflecting on the implications for
research, the number of clinical trials was
found to be small. Therefore, more high-quality
research is needed to evaluate to what extent
there is a difference in the effectiveness of infil-
trated lesions and sites to be preserved by oral
hygiene/fluoride programs; the carry-over
effect of fluoride applications cannot be totally
ruled out, and randomized controlled trials with
a parallel group design seem mandatory.
Moreover, there is need to study the reasons for
lesion progress, in vitro and in vivo; mechanical,
chemical, and biologic behavior of materials
used as infiltrants, with variations of application
procedures (repeated application after different
time intervals, possible needs for reinfiltration
regimens within preventive-oriented recalls),
are considered fields of major interest.
ACKNOWLEDGMENTS
The authors are indebted to Dr Christian Hartwig for the
drawing of Fig 2 (reproduced with permission of S.Karger AG,
Basel, Switzerland). The assistance of Mrs Helga Grundt
(Department of Operative Dentistry and Periodontology,
CharitéCentrum 3, Berlin, Germany) with the scanning elec-
tron micrographs is greatly appreciated. Charité-
Universitätsmedizin Berlin holds US (US10/432,271) and
European (EP06021966.4) patent applications for an infiltra-
tion technique for dental caries lesions in which 2 of the
authors are appointed as inventors. Development of a resin
infiltrant has been furthered by a collaboration between
Charité, Berlin, and DMG, Hamburg, Germany,. SInce March
2009,a resin infiltrant called Icon has been marketed by DMG.
Figs 8a to 8c (a) Preoperative view of a 22-year-old patient after orthodontic therapy, with gross caries lesions and frank cavities onlabial surfaces. (b) Finished restorations (microfilled composite resin; 1 week after treatment) of cavitations; demineralized areas (of allteeth) were etched and resin infiltrated. (c) Postoperative view, 13 months after treatment.
a b c
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

678 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
REFERENCES
1. Osborne JW, Lopez Howell M, Marshall H. Webb and
extension for prevention: A literature review.Quintes-
sence Int 1999;30:399–403.
2. Black GV (ed).Operative Dentistry.Chicago:Med-Dent
Pub, 1924:142–143.
3. Friesell HE.The stage of dental caries. Dent Rec 1922;
42:58–59.
4. Mount GJ, Ngo H. Minimal intervention: Early lesions.
Quintessence Int 2000;31:535–546.
5. Mount GJ, Ngo H. Minimal intervention: A new con-
cept for operative dentistry. Quintessence Int 2000;
31:527–533.
6. Kielbassa AM. Current challenges in caries diagnosis.
Quintessence Int 2006;37:421.
7. Tyas MJ,Anusavice KJ,Frencken JE,Mount GJ.Minimal
intervention dentistry—A review. FDI Commission
Project 1–97. Int Dent J 2000;50:1–12.
8. Young DA, Featherstone JD, Roth JR, et al.Caries man-
agement by risk assessment: Implementation guide-
lines. J Calif Dent Assoc 2007;35:799–805.
9. Mejàre I, Källestål C, Stenlund H. Incidence and pro-
gression of approximal caries from 11 to 22 years of
age in Sweden: A prospective radiographic study.
Caries Res 1999;33:93–100.
10. Koivusilta L, Honkala S, Honkala E, Rimpela A. Tooth-
brushing as part of the adolescent lifestyle predicts
education level. J Dent Res 2003;82:361–366.
11. Alm A. On dental caries and caries-related factors in
children and teenagers.Swed Dent J Suppl 2008:7–63.
12. Davila JM, Buonocore MG, Greeley CB, Provenza DV.
Adhesive penetration in human artificial and natural
white spots. J Dent Res 1975;54:999–1008.
13. Davila JM, Sisca RF, Tinanoff N, Provenza DV. Plastic
sealing of proximal surfaces of teeth, a new technic.
J Baltimore Coll Dent Surg 1975;30:40–47.
14. Gomez SS, Onetto JE, Uribe SA, Emilson CG.
Therapeutic seal of approximal incipient noncavitat-
ed carious lesions: Technique and case reports.
Quintessence Int 2007;38:e99–e105.
15. Robinson C, Hallsworth AS, Weatherell JA, Kunzel W.
Arrest and control of carious lesions:A study based on
preliminary experiments with resorcinol-formal-
dehyde resin. J Dent Res 1976;55:812–818.
16. Rodda JC. Impregnation of caries-like lesions with
dental resins. N Z Dent J 1983;79:114–117.
17. Gomez SS, Basili CP, Emilson CG. A 2-year clinical eval-
uation of sealed noncavitated approximal posterior
carious lesions in adolescents. Clin Oral Investig 2005;
9:239–243.
18. Ardu S, Perroud R, Krejci I. Extended sealing of inter-
proximal caries lesions. Quintessence Int 2006;37:
423–427.
19. Duckworth RM,Gao XJ.Plaque as a reservoir for active
ingredients. Monogr Oral Sci 2006;19:132–149.
20. Hicks J, García-Godoy F, Flaitz C. Biological factors in
dental caries enamel structure and the caries process
in the dynamic process of demineralization and re-
mineralization (part 2). J Clin Pediatr Dent 2004;28:
119–124.
21. Holmen L, Mejàre I, Malmgren B, Thylstrup A. The
effect of regular professional plaque removal on den-
tal caries in vivo. A polarized light and scanning elec-
tron microscope study. Caries Res 1988;22:250–256.
22. Silverstone LM, Hicks MJ, Featherstone MJ. Dynamic
factors affecting lesion initiation and progression in
human dental enamel. II. Surface morphology of
sound enamel and carieslike lesions of enamel.
Quintessence Int 1988;19:773–785.
23. Robinson C, Shore RC, Brookes SJ, Strafford S, Wood
SR,Kirkham J.The chemistry of enamel caries.Crit Rev
Oral Biol Med 2000;11:481–495.
24. Arends J, Jongebloed W, Ogaard B, Rølla G. SEM and
microradiographic investigation of initial enamel
caries. Scand J Dent Res 1987;95:193–201.
25. Bergman G, Lind PO. A quantitative microradio-
graphic study of incipient enamel caries. J Dent Res
1966;45:1477–1484.
26. Kielbassa AM,Gillmann L,Zantner C,Meyer-Lueckel H,
Hellwig E,Schulte-Monting J.Profilometric and micro-
radiographic studies on the effects of toothpaste and
acidic gel abrasivity on sound and demineralized
bovine dental enamel. Caries Res 2005;39:380–386.
27. Hicks J, García-Godoy F, Flaitz C. Biological factors in
dental caries: Role of saliva and dental plaque in the
dynamic process of demineralization and remineral-
ization (part 1). J Clin Pediatr Dent 2003;28:47–52.
28. Berchier CE, Slot DE, Haps S, van der Weijden GA. The
efficacy of dental floss in addition to a toothbrush on
plaque and parameters of gingival inflammation: A
systematic review.Int J Dent Hygiene 2008;6:265–279.
29. Hujoel PP, Cunha-Cruz J, Banting DW, Loesche WJ.
Dental flossing and interproximal caries: A systematic
review. J Dent Res 2006;85:298–305.
30. Wright GZ, Banting DW, Feasby WH. Effect of inter-
dental flossing on the incidence of proximal caries in
children. J Dent Res 1977;56:574–578.
31. van Strijp AJ, Gerardu VA, Buijs MJ, van Loveren C, ten
Cate JM. Chlorhexidine efficacy in preventing lesion
formation in enamel and dentine: An in situ study.
Caries Res 2008;42:460–465.
32. Rieben AS, Zimny B, Noetzel J, Neumann K, Kielbassa
AM. Influence of chlorhexidine on fluoride uptake by
bovine dentin in vitro. Am J Dent 2008;21:351–355.
33. Autio-Gold J. The role of chlorhexidine in caries pre-
vention. Oper Dent 2008;33:710–716.
34. Modeer T, Twetman S, Bergstrand F. Three-year study
of the effect of fluoride varnish (Duraphat) on proxi-
mal caries progression in teenagers.Scand J Dent Res
1984;92:400–407.
35. Sköld UM, Petersson LG, Lith A, Birkhed D. Effect of
school-based fluoride varnish programmes on
approximal caries in adolescents from different caries
risk areas. Caries Res 2005;39:273–279.
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 679
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
36. Sköld UM,Birkhed D,Borg E,Petersson LG.Approximal
caries development in adolescents with low to mod-
erate caries risk after different 3-year school-based
supervised fluoride mouth rinsing programmes.
Caries Res 2005;39:529–535.
37. Sköld UM.On caries prevalence and school-based flu-
oride programmes in Swedish adolescents. Swed
Dent J Suppl 2005:11–75.
38. Gustafsson A, Svenson B, Edblad E, Jansson L.
Progression rate of approximal carious lesions in
Swedish teenagers and the correlation between
caries experience and radiographic behavior. An
analysis of the survival rate of approximal caries
lesions. Acta Odontol Scand 2000;58:195–200.
39. Benson PE,Parkin N,Millett DT,Dyer FE,Vine S,Shah A.
Fluorides for the prevention of white spots on teeth
during fixed brace treatment. Cochrane Database
Syst Rev 2004:CD003809.
40. Pitts NB. Regression of approximal carious lesions
diagnosed from serial standardized bitewing radi-
ographs. Caries Res 1986;20:85–90.
41. Pitts NB, Longbottom C. Temporary tooth separation
with special reference to the diagnosis and preven-
tive management of equivocal approximal carious
lesions. Quintessence Int 1987;18:563–573.
42. Altenburger MJ, Schirrmeister JF, Wrbas KT, Hellwig E.
Remineralization of artificial interproximal carious
lesions using a fluoride mouthrinse. Am J Dent
2007;20:385–389.
43. Amarante E, Raadal M, Espelid I. Impact of diagnostic
criteria on the prevalence of dental caries in
Norwegian children aged 5, 12 and 18 years.
Community Dent Oral Epidemiol 1998;26:87–94.
44. Kielbassa AM, Paris S, Lussi A, Meyer-Lueckel H.
Evaluation of cavitations in proximal caries lesions at
various magnification levels in vitro. J Dent 2006;34:
817–822.
45. Lith A, Lindstrand C, Grondahl HG. Caries develop-
ment in a young population managed by a restrictive
attitude to radiography and operative intervention: II.
A study at the surface level. Dentomaxillofac Radiol
2002;31:232–239.
46. Tveit AB, Espelid I, Skodje F. Restorative treatment
decisions on approximal caries in Norway. Int Dent J
1999;49:165–172.
47. Maupomé G, Sheiham A. Radiographic criteria
employed to diagnose and treat approximal caries by
final-year dental students in Mexico City. Community
Dent Oral Epidemiol 1997;25:242–246.
48. Traebert J,Marcenes W,Kreutz JV,Oliveira R,Piazza CH,
Peres MA. Brazilian dentists’ restorative treatment
decisions. Oral Health Prev Dent 2005;3:53–60.
49. Traebert J,Wesolowski CI, de Lacerda JT, Marcenes W.
Thresholds of restorative decision in dental caries
treatment among dentists from small Brazilian cities.
Oral Health Prev Dent 2007;5:131–135.
50. Doméjean-Orliaguet S, Tubert-Jeannin S, Riordan PJ,
Espelid I, Tveit AB. French dentists’ restorative treat-
ment decisions.Oral Health Prev Dent 2004;2:125–131.
51. Ghasemi H, Murtomaa H, Torabzadeh H, Vehkalahti
MM. Restorative treatment threshold reported by
Iranian dentists. Community Dent Health 2008;
25:185–190.
52. Flaitz CM, Hicks MJ.Role of the acid-etch technique in
remineralization of caries-like lesions of enamel: A
polarized light and scanning electron microscopic
study. ASDC J Dent Child 1994;61:21–28.
53. Flaitz CM, Hicks MJ. Remineralization of caries-like
lesions of enamel with acidulated calcifying fluids: A
polarized light microscopic study. Pediatr Dent 1996;
18:205–209.
54. Hicks MJ, Silverstone LM. Internal morphology of sur-
face zones from acid-etched caries-like lesions: A
scanning electron microscopic study. J Dent Res
1985;64:1296–1301.
55. Meyer-Lueckel H, Paris S, Kielbassa AM. Surface layer
erosion of natural caries lesions with phosphoric and
hydrochloric acid gels in preparation for resin infiltra-
tion. Caries Res 2007;41:223–230.
56. Al-Khateeb S, Exterkate R, Angmar-Mansson B, ten
Cate JM. Effect of acid-etching on remineralization of
enamel white spot lesions. Acta Odontol Scand
2000;58:31–36.
57. Silverstone LM. Effect of oral fluid and synthetic calci-
fying fluids in vitro on remineralization of enamel
lesion. Clin Prev Dent 1981;4:13–22.
58. Silverstone LM,Wefel JS,Zimmerman BF,Clarkson BH,
Featherstone MJ. Remineralization of natural and
artificial lesions in human dental enamel in vitro.
Effect of calcium concentration of the calcifying fluid.
Caries Res 1981;15:138–157.
59. Robinson C, Shore RC, Bonass WA, Brookes SJ, Boteva
E, Kirkham J. Identification of human serum albumin
in human caries lesions of enamel: The role of puta-
tive inhibitors of remineralisation. Caries Res 1998;32:
193–199.
60. Kielbassa AM, Oeschger U, Schulte-Monting J, Meyer-
Lueckel H. Microradiographic study on the effects of
salivary proteins on in vitro demineralization of
bovine enamel. J Oral Rehabil 2005;32:90–96.
61. Meyer-Lueckel H, Umland N, Hopfenmuller W,
Kielbassa AM. Effect of mucin alone and in combina-
tion with various dentifrices on in vitro remineraliza-
tion. Caries Res 2004;38:478–483.
62. Backer Dirks O.Posteruptive changes in dental enam-
el. J Dent Res 1966;45:503–511.
63. Hicks J, García-Godoy F, Flaitz C. Biological factors in
dental caries: Role of remineralization and fluoride in
the dynamic process of demineralization and rem-
ineralization (part 3). J Clin Pediatr Dent 2004;28:
203–214.
64. Pot TJ, Groeneveld A, Purdell-Lewis DJ.The origin and
behaviour of white spot enamel lesions. Ned Tijdschr
Tandheelkd 1977;85:6–18.
65. García-Godoy F, Summitt JB, Donly KJ. Caries progres-
sion of white spot lesions sealed with an unfilled
resin. J Clin Pediatr Dent 1997;21:141–143.
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

680 VOLUME 40 • NUMBER 8 • SEPTEMBER 2009
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
66. Tranaeus S, Al-Khateeb S, Bjorkman S, Twetman S,
Angmar-Mansson B.Application of quantitative light-
induced fluorescence to monitor incipient lesions in
caries-active children. A comparative study of rem-
ineralisation by fluoride varnish and professional
cleaning. Eur J Oral Sci 2001;109:71–75.
67. Karlsson L,Lindgren LE,Trollsas K,Angmar-Mansson B,
Tranaeus S. Effect of supplementary amine fluoride
gel in caries-active adolescents. A clinical QLF study.
Acta Odontol Scand 2007;65:284–291.
68. Zantner C,Martus P,Kielbassa AM.Clinical monitoring
of the effect of fluorides on long-existing white spot
lesions. Acta Odontol Scand 2006;64:115–122.
69. Willmot DR. White lesions after orthodontic treat-
ment: Does low fluoride make a difference? J Orthod
2004;31:235–242.
70. Melrose CA, Appleton J, Lovius BB. A scanning elec-
tron microscopic study of early enamel caries formed
in vivo beneath orthodontic bands. Br J Orthod
1996;23:43–47.
71. Adams D, Addy M, Absi E. Abrasive and chemical
effects of dentifrices. In: Embery G, Rølla G (eds).
Clinical and Biological Aspects of Dentifrices. Oxford:
Oxford Medical Publications, 1996:345–355.
72. Kanthathas K, Willmot DR, Benson PE. Differentiation
of developmental and post-orthodontic white
lesions using image analysis. Eur J Orthod 2005;
27:167–172.
73. Årtun J, Thylstrup A. Clinical and scanning electron
microscopic study of surface changes of incipient
caries lesions after debonding. Scand J Dent Res
1986;94:193–201.
74. Holmen L, Thylstrup A, Årtun J. Surface changes dur-
ing the arrest of active enamel carious lesions in vivo.
A scanning electron microscope study. Acta Odontol
Scand 1987;45:383–390.
75. Årtun J,Thylstrup A.A 3-year clinical and SEM study of
surface changes of carious enamel lesions after inac-
tivation. Am J Orthod Dentofacial Orthop 1989;
95:327–333.
76. Espelid I, Tveit AB. Clinical and radiographic assess-
ment of approximal carious lesions. Acta Odontol
Scand 1986;44:31–37.
77. Waggoner WF, Ashton JJ. Predictability of cavitation
based upon radiographic appearance:Comparison of
two film types. Quintessence Int 1989;20:55–60.
78. Bille J,Thylstrup A.Radiographic diagnosis and clinical
tissue changes in relation to treatment of approximal
carious lesions. Caries Res 1982;16:1–6.
79. Thylstrup A, Bille J, Qvist V. Radiographic and
observed tissue changes in approximal carious
lesions at the time of operative treatment. Caries Res
1986;20:75–84.
80. Pitts NB, Rimmer PA. An in vivo comparison of radi-
ographic and directly assessed clinical caries status of
posterior approximal surfaces in primary and perma-
nent teeth. Caries Res 1992;26:146–152.
81. Hintze H,Wenzel A,Danielsen B,Nyvad B.Reliability of
visual examination, fibre-optic transillumination, and
bite-wing radiography, and reproducibility of direct
visual examination following tooth separation for the
identification of cavitated carious lesions in contact-
ing approximal surfaces. Caries Res 1998;32:204–209.
82. Kielbassa AM, Meyer-Lueckel H, Lussi A. Proximal
caries: Diagnosis and treatment decision. In:
Heidemann D (ed). Deutscher Zahnärztekalender.
Cologne: Deutscher Zahnärzteverlag, 2002;62:37–58.
83. Ekstrand KR, Bruun G, Bruun M. Plaque and gingival
status as indicators for caries progression on approxi-
mal surfaces. Caries Res 1998;32:41–45.
84. Ismail AI. Clinical diagnosis of precavitated carious
lesions. Community Dent Oral Epidemiol 1997;25:
13–23.
85. Ratledge DK.A clinical and laboratory investigation of
the tunnel restoration [PhD thesis]. London:
University of London, 1999.
86. Robinson C,Brookes SJ,Kirkham J,Wood SR,Shore RC.
In vitro studies of the penetration of adhesive resins
into artificial caries-like lesions. Caries Res 2001;35:
136–141.
87. van Dorp CS, ten Cate JM. Bonding of fissure sealant
to etched demineralized enamel (lesions). Caries Res
1987;21:513–521.
88. Lee CQ, Shey Z, Cobb CM. Microscopic appearance of
enamel white-spot lesions after acid etching.
Quintessence Int 1995;26:279–284.
89. Asmussen E.Penetration of restorative resins into acid
etched enamel. I. Viscosity, surface tension and con-
tact angle of restorative resin monomers. Acta
Odontol Scand 1977;35:175–182.
90. Gwinnett AJ, Ripa LW. Penetration of pit and fissure
sealants into conditioned human enamel in vivo.Arch
Oral Biol 1973;18:435–439.
91. Silverstone LM. Fissure sealants. Laboratory studies.
Caries Res 1974;8:2–26.
92. Asmussen E.Penetration of restorative resins into acid
etched enamel. II. Dissolution of entrapped air in
restorative resin monomers. Acta Odontol Scand
1977;35:183–191.
93. Paris S, Meyer-Lueckel H, Kielbassa AM. Resin infiltra-
tion of natural caries lesions. J Dent Res 2007;86:
662–666.
94. Gray GB, Shellis P. Infiltration of resin into white spot
caries-like lesions of enamel: An in vitro study. Eur J
Prosthodont Restor Dent 2002;10:27–32.
95. Meyer-Lueckel H, Mueller J, Paris S, Hummel M,
Kielbassa AM. The penetration of various adhesives
into early enamel lesions in vitro [in German].Schweiz
Monatsschr Zahnmed 2005;115:316–323.
96. Meyer-Lueckel H,Paris S,Mueller J,Cölfen H,Kielbassa
AM. Influence of the application time on the penetra-
tion of different dental adhesives and a fissure sealant
into artificial subsurface lesions in bovine enamel.
Dent Mater 2006;22:22–28.
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.

VOLUME 40 • NUMBER 8 • SEPTEMBER 2009 681
QUINTESSENCE INTERNATIONAL
Kielbassa et a l
97. Paris S,Meyer-Lueckel H,Cölfen H,Kielbassa AM.Resin
infiltration of artificial enamel caries lesions with
experimental light curing resins. Dent Mater J 2007;
26:582–588.
98. Meyer-Lueckel H,Paris S. Improved resin infiltration of
natural caries lesions. J Dent Res 2008;87:1112–1116.
99. Paris S, Meyer-Lueckel H, Cölfen H, Kielbassa AM.
Penetration coefficients of commercially available
and experimental composites intended to infiltrate
enamel carious lesions. Dent Mater 2007;23:
742–748.
100. Irinoda Y, Matsumura Y, Kito H, et al. Effect of sealant
viscosity on the penetration of resin into etched
human enamel. Oper Dent 2000;25:274–282.
101. Schmidlin PR,Zehnder M,Pasqualetti T,Imfeld T,Besek
MJ.Penetration of a bonding agent into de- and rem-
ineralized enamel in vitro. J Adhes Dent 2004;6:
111–115.
102. Kersten S, Lutz F, Schupbach P. Fissure sealing:
Optimization of sealant penetration and sealing
properties. Am J Dent 2001;14:127–131.
103. Espinosa R,Valencia R,Uribe M,Ceja I,Saadia M.Enamel
deproteinization and its effect on acid etching: An in
vitro study. J Clin Pediatr Dent 2008;33:13–19.
104. Glasspoole EA, Erickson RL, Davidson CL. Protective
effects of resin impregnation on demineralization of
enamel. Am J Dent 1999;12:315–320.
105. Schmidlin PR, Zehnder M, Zimmermann MA,
Zimmermann J, Roos M, Roulet JF. Sealing smooth
enamel surfaces with a newly devised adhesive
patch: A radiochemical in vitro analysis. Dent Mater
2005;21:545–550.
106. Mueller J, Meyer-Lueckel H, Paris S, Hopfenmuller W,
Kielbassa AM. Inhibition of lesion progression by the
penetration of resins in vitro: Influence of the applica-
tion procedure. Oper Dent 2006;31:338–345.
107. Paris S, Meyer-Lueckel H, Mueller J, Hummel M,
Kielbassa AM. Progression of sealed initial bovine
enamel lesions under demineralizing conditions in
vitro. Caries Res 2006;40:124–129.
108. Meyer-Lueckel H, Paris S. Progression of artificial
enamel caries lesions after infiltration with experimen-
tal light curing resins. Caries Res 2008;42:117–124.
109. Bjarnason S, Dietz W, Hoyer I, Noren JG, Robertson A,
Kraft U.Bonded resin sealant on smooth surface den-
tal enamel—An in vitro study. Swed Dent J 2003;27:
167–174.
110. Goepferd SJ, Olberding P. The effect of sealing white
spot lesions on lesion progression in vitro. Pediatr
Dent 1989;11:14–16.
111. Tantbirojn D, Rozzi SM, Mitra SB, Kedrowski BL,
Douglas WH. In vitro inhibition of enamel demineral-
ization by a polymerizable amphiphilic film.Eur J Oral
Sci 2000;108:564–568.
112. Frazier MC, Southard TE, Doster PM. Prevention of
enamel demineralization during orthodontic treat-
ment: An in vitro study using pit and fissure sealants.
Am J Orthod Dentofacial Orthop 1996;110:459–465.
113. Buren JL,Staley RN,Wefel J,Qian F. Inhibition of enam-
el demineralization by an enamel sealant,Pro Seal:An
in-vitro study. Am J Orthod Dentofacial Orthop
2008;133:S88–94.
114. Davidson CL, Bekke-Hoekstra IS. The resistance of
superficially sealed enamel to wear and carious
attack in vitro. J Oral Rehabil 1980;7:299–305.
115. Hu W, Featherstone JD. Prevention of enamel dem-
ineralization: An in-vitro study using light-cured filled
sealant. Am J Orthod Dentofacial Orthop 2005;128:
592–600.
116. Gomez SS, Uribe S, Onetto JE, Emilson CG. SEM analy-
sis of sealant penetration in posterior approximal
enamel carious lesions in vivo. J Adhes Dent 2008;
10:151–156.
117. Gomez SS,Uribe SA,Onetto JE.SEM analysis of sealant
penetration in proximal incipient non-cavitated
caries lesion. J Dent Res 2003;82(Spec Iss B):1965.
118. Martignon S, Ekstrand KR, Ellwood R. Efficacy of seal-
ing proximal early active lesions:An 18-month clinical
study evaluated by conventional and subtraction
radiography. Caries Res 2006;40:382–388.
119. Hiiri A,Ahovuo-Saloranta A,Nordblad A,Makela M.Pit
and fissure sealants versus fluoride varnishes for pre-
venting dental decay in children and adolescents.
Cochrane Database Syst Rev 2006:CD003067.
120. Mertz-Fairhurst EJ, Curtis JW Jr, Ergle JW, Rueggeberg
FA, Adair SM. Ultraconservative and cariostatic sealed
restorations: Results at year 10. J Am Dent Assoc
1998;129:55–66.
121. Bravo M, Montero J, Bravo JJ, Baca P, Llodra JC. Sealant
and fluoride varnish in caries: A randomized trial.
J Dent Res 2005;84:1138–1143.
122. Årtun J, Brobakken BO. Prevalence of carious white
spots after orthodontic treatment with multibonded
appliances. Eur J Orthod 1986;8:229–234.
123. Benham AW, Campbell PM, Buschang PH.
Effectiveness of pit and fissure sealants in reducing
white spot lesions during orthodontic treatment. A
pilot study. Angle Orthod 2009;79:338–345.
124. Alkilzy M, Berndt C, Meller C, Schidlowski M, Splieth C.
Sealing of proximal surfaces with polyurethane tape:
A two-year clinical and radiographic feasibility study.
J Adhes Dent 2009;11:91–94.
© 2009 BY QUINTESSENCE PUBLISHING CO, INC. PRINTING OF THIS DOCUMENT IS RESTRICTED TO PERSONAL USE ONLY. NO PART OF THIS ARTICLE MAY BE REPRODUCED OR TRANSMITTED IN ANY FORM WITHOUT WRITTEN PERMISSION FROM THE PUBLISHER.