clipping and superficial temporal artery–m2 bypass for unruptured anterior communicating artery...
TRANSCRIPT
Surgical Neurolog
Aneurysm
Clipping and superficial temporal artery–M2 bypass for unruptured
anterior communicating artery aneurysm associated with atherosclerotic
internal carotid artery occlusion: report of 2 cases
Tomohiro Inoue, MD, Kazuo Tsutsumi, MD4, Shinobu Adachi, MD, Shota Tanaka, MD,
Kuniaki Saito, MD, Naoto Kunii, MDDepartment of Neurosurgery, Showa general hospital, 2-450 Tenjinn-cho Kodaira-shi, Tokyo, 187-8510, Japan
Received 6 January 2006; accepted 4 October 2006
www.surgicalneurology-online.com
Abstract Background: The management of the unruptured AcomA aneurysm associated with atherosclerotic
0090-3019/$ – see fro
doi:10.1016/j.surneu.2
Abbreviations: Ac
spinal fluid; ICA, int
MEP, motor-evoked
MRI, magnetic resona
SEP, somatosensory-e
computed tomograph
intelligence quotient;
4 Corresponding
E-mail address: k
occlusion of the unilateral internal carotid artery (ICA) raises several strategic dilemmas.
Methods: Two such patients with unruptured aneurysm on the AcomA, which supply cross-flow
toward the hemisphere with ICA occlusion, are presented.
Results: Both patients were treated with STA-M2 bypass followed by clipping of the unruptured
AcomA aneurysm in 1 stage through the transsylvian route. Both patients were doing well without
neurological deficit nor cognitive impairment at 1 year follow-up.
Conclusions: In the surgical treatment of unruptured AcomA aneurysm with atherosclerotic ICA
occlusion, preceding bypass would be ideal in case of intraoperative rupture as well as to reduce
perioperative ischemia if the bypass procedure itself could be performed with minimal risk. Enough
and atraumatic exposure of the sylvian fissure contributed to reduce brain retraction during the
clipping of AcomA aneurysm and, in addition, to ease the STA-M2 bypass.
D 2007 Elsevier Inc. All rights reserved.
Keywords: Cerebral revascularization; Cerebral aneurysm; Ischemic cerebrovascular disease
1. Introduction
The management of unruptured intracranial aneurysms
remains controversial. Especially when the patient is
harboring unruptured aneurysm and major trunk occlusion
simultaneously, the surgical risk would be higher and
strategic dilemmas would appear. We recently encountered
2 patients who harbored unruptured aneurysm with rela-
tively small size, however, on the AcomA that supplies
cross-flow toward the hemisphere with atherosclerotic ICA
nt matter D 2007 Elsevier Inc. All rights reserved.
006.10.031
omA, anterior communicating artery; CSF, cerebro-
ernal cerebral artery; MCA, middle cerebral artery;
potential; MRA, magnetic resonance angiography;
nce imaging; PIQ, performance intelligence quotient;
voked potential; SPECT, single photon emission
y; STA, superficial temporal artery; VIQ, verbal
WAIS-R, Wechsler Adult Intelligence Scale Revised.
author. Tel.: +81 424 61 0052; fax: +81 424 64 7912.
[email protected] (K. Tsutsumi).
occlusion. Both patients underwent successful surgical
repair with clipping in conjunction with STA-M2 bypass.
The details of the management are presented and discussed.
2. Case report
2.1. Case 1
A 59-year-old man presented to another hospital with the
complaint of recent and frequent dizziness. His medical
history included hypertension and hyperlipidemia. Magnetic
resonance imagings were performed, which revealed unrup-
tured AcomA aneurysm, left carotid ICA occlusion, and
multiple lacunar infarctions. He was referred to our
department for possible surgical intervention. Neurological
examination did not show any focal deficit, although WAIS-
R score was dull normal level showing VIQ 96, PIQ 57, and
full scale IQ 78. Cerebral angiography showed atheroscle-
rotic left internal carotid artery occlusion as well as
y 68 (2007) 226–232
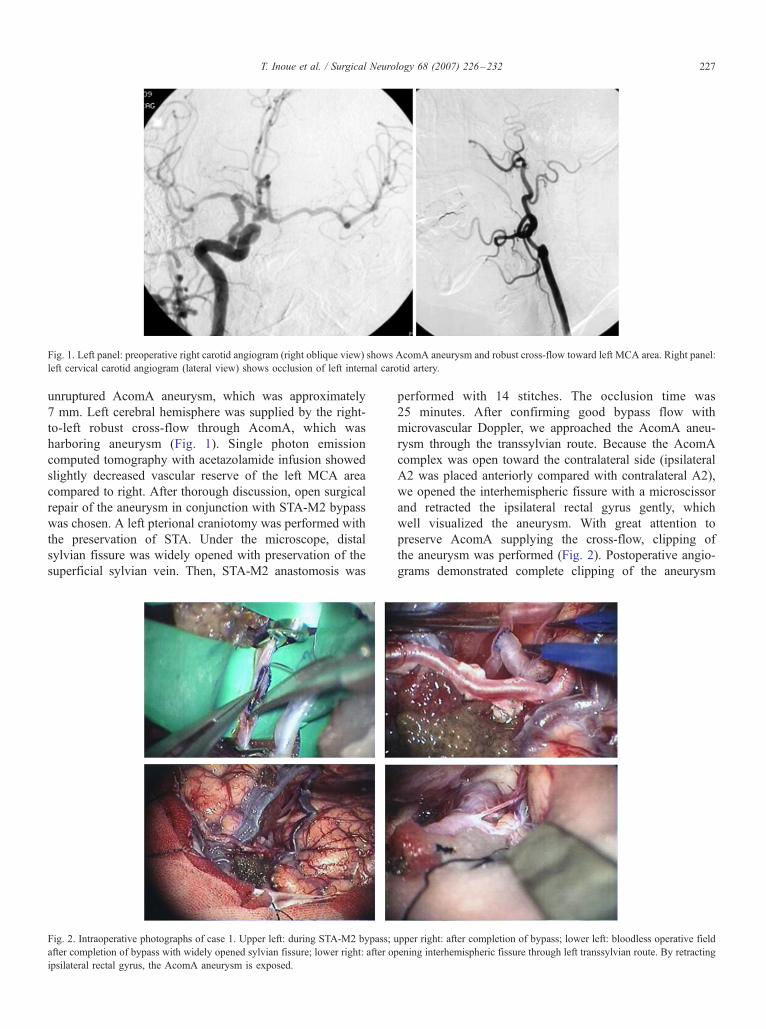
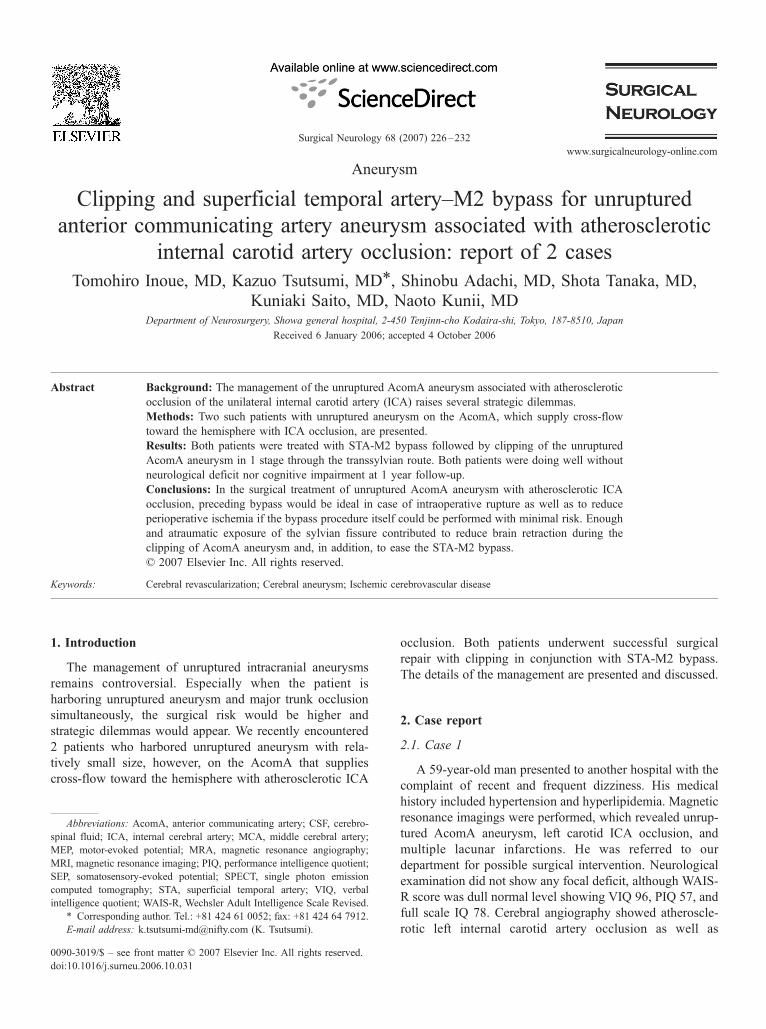
Fig. 1. Left panel: preoperative right carotid angiogram (right oblique view) shows AcomA aneurysm and robust cross-flow toward left MCA area. Right panel:
left cervical carotid angiogram (lateral view) shows occlusion of left internal carotid artery.
T. Inoue et al. / Surgical Neurology 68 (2007) 226–232 227
unruptured AcomA aneurysm, which was approximately
7 mm. Left cerebral hemisphere was supplied by the right-
to-left robust cross-flow through AcomA, which was
harboring aneurysm (Fig. 1). Single photon emission
computed tomography with acetazolamide infusion showed
slightly decreased vascular reserve of the left MCA area
compared to right. After thorough discussion, open surgical
repair of the aneurysm in conjunction with STA-M2 bypass
was chosen. A left pterional craniotomy was performed with
the preservation of STA. Under the microscope, distal
sylvian fissure was widely opened with preservation of the
superficial sylvian vein. Then, STA-M2 anastomosis was
Fig. 2. Intraoperative photographs of case 1. Upper left: during STA-M2 bypass; u
after completion of bypass with widely opened sylvian fissure; lower right: after op
ipsilateral rectal gyrus, the AcomA aneurysm is exposed.
performed with 14 stitches. The occlusion time was
25 minutes. After confirming good bypass flow with
microvascular Doppler, we approached the AcomA aneu-
rysm through the transsylvian route. Because the AcomA
complex was open toward the contralateral side (ipsilateral
A2 was placed anteriorly compared with contralateral A2),
we opened the interhemispheric fissure with a microscissor
and retracted the ipsilateral rectal gyrus gently, which
well visualized the aneurysm. With great attention to
preserve AcomA supplying the cross-flow, clipping of
the aneurysm was performed (Fig. 2). Postoperative angio-
grams demonstrated complete clipping of the aneurysm
pper right: after completion of bypass; lower left: bloodless operative field
ening interhemispheric fissure through left transsylvian route. By retracting
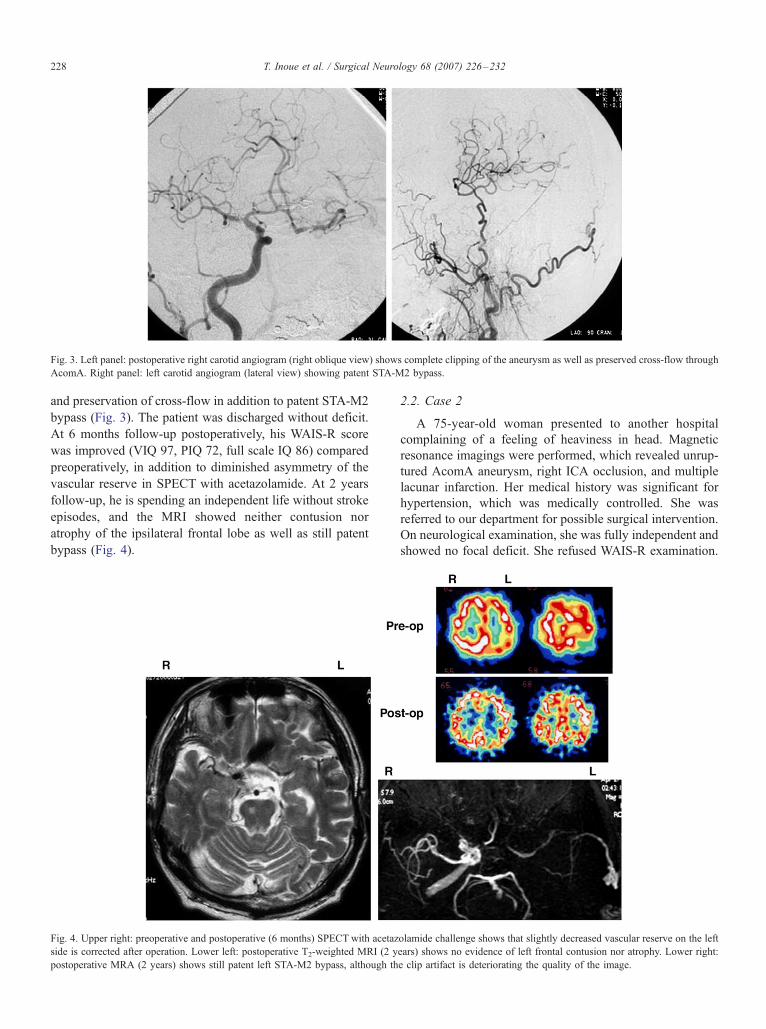
Fig. 3. Left panel: postoperative right carotid angiogram (right oblique view) shows complete clipping of the aneurysm as well as preserved cross-flow through
AcomA. Right panel: left carotid angiogram (lateral view) showing patent STA-M2 bypass.
T. Inoue et al. / Surgical Neurology 68 (2007) 226–232228
and preservation of cross-flow in addition to patent STA-M2
bypass (Fig. 3). The patient was discharged without deficit.
At 6 months follow-up postoperatively, his WAIS-R score
was improved (VIQ 97, PIQ 72, full scale IQ 86) compared
preoperatively, in addition to diminished asymmetry of the
vascular reserve in SPECT with acetazolamide. At 2 years
follow-up, he is spending an independent life without stroke
episodes, and the MRI showed neither contusion nor
atrophy of the ipsilateral frontal lobe as well as still patent
bypass (Fig. 4).
Fig. 4. Upper right: preoperative and postoperative (6 months) SPECT with acetaz
side is corrected after operation. Lower left: postoperative T2-weighted MRI (2 y
postoperative MRA (2 years) shows still patent left STA-M2 bypass, although th
2.2. Case 2
A 75-year-old woman presented to another hospital
complaining of a feeling of heaviness in head. Magnetic
resonance imagings were performed, which revealed unrup-
tured AcomA aneurysm, right ICA occlusion, and multiple
lacunar infarction. Her medical history was significant for
hypertension, which was medically controlled. She was
referred to our department for possible surgical intervention.
On neurological examination, she was fully independent and
showed no focal deficit. She refused WAIS-R examination.
olamide challenge shows that slightly decreased vascular reserve on the left
ears) shows no evidence of left frontal contusion nor atrophy. Lower right:
e clip artifact is deteriorating the quality of the image.

Fig. 5. Left panel: preoperative left carotid angiogram (left oblique view) shows AcomA aneurysm and robust cross-flow toward right MCA area. Right panel:
right cervical carotid angiogram (lateral view) shows occlusion of right internal carotid artery.
T. Inoue et al. / Surgical Neurology 68 (2007) 226–232 229
Cerebral angiography showed atherosclerotic right ICA
occlusion as well as AcomA aneurysm that was approxi-
mately 5 mm. Right cerebral hemisphere was supplied by the
left-to-right robust cross-flow through AcomA, which was
harboring aneurysm (Fig. 5). Single photon emission
computed tomography with acetazolamide infusion showed
slightly decreased vascular reserve of the right MCA area
compared to the left. After thorough discussion, open surgical
repair of the aneurysm in conjunction with STA-M2 bypass
was chosen. A right pterional craniotomywas performed, and
the details of the surgical procedure were almost the same as
Fig. 6. Intraoperative photographs of case 2. Upper left: during STA-M2 bypass. U
the aid of a retractor. Small continuous suction tube is located at the base. The tip
after opening interhemispheric fissure through transsylvian route. Only the nec
posteriorly. Lower right: final clipping view through the space posterior to ipsila
that illustrated in case 1. In this case, the AcomA complex
was open toward the contralateral side even more compared
with case 1 (ipsilateral A2 completely hid the aneurysm even
after opening up the interhemispheric fissure and retracting
the ipsilateral rectal gyrus). With great care not to injure the
ipsilateral Heubner artery, we opened the space posterior to
ipsilateral A2 and mobilized it anteriorly, which finally well
visualized the aneurysm. The clipping was completed with
the preservation of AcomA (Fig. 6). Postoperative angio-
grams demonstrated complete clipping of the aneurysm and
the preservation of cross-flow in addition to patent STA-M2
pper right: sylvian fissure is kept open by a prop (rolled Bensheet) without
of the suction tube is located deeper than the anastomosis site. Lower left:
k of the aneurysm is slightly visible even after retracting ipsilateral A2
teral A2.
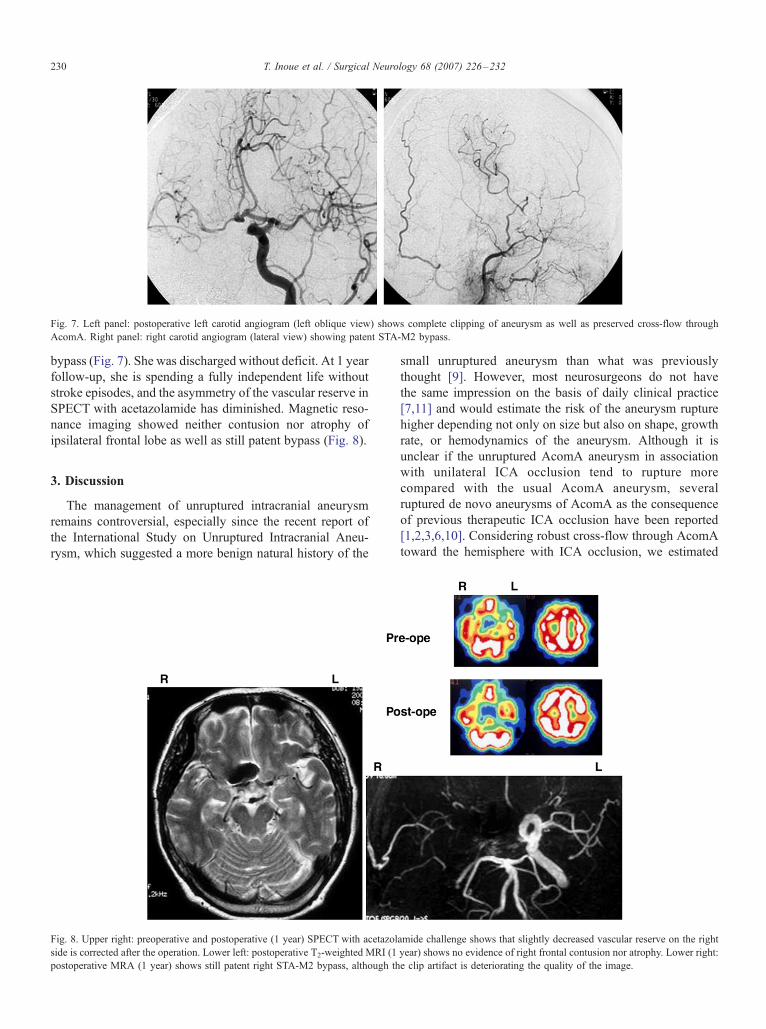
Fig. 7. Left panel: postoperative left carotid angiogram (left oblique view) shows complete clipping of aneurysm as well as preserved cross-flow through
AcomA. Right panel: right carotid angiogram (lateral view) showing patent STA-M2 bypass.
T. Inoue et al. / Surgical Neurology 68 (2007) 226–232230
bypass (Fig. 7). She was discharged without deficit. At 1 year
follow-up, she is spending a fully independent life without
stroke episodes, and the asymmetry of the vascular reserve in
SPECT with acetazolamide has diminished. Magnetic reso-
nance imaging showed neither contusion nor atrophy of
ipsilateral frontal lobe as well as still patent bypass (Fig. 8).
3. Discussion
The management of unruptured intracranial aneurysm
remains controversial, especially since the recent report of
the International Study on Unruptured Intracranial Aneu-
rysm, which suggested a more benign natural history of the
Fig. 8. Upper right: preoperative and postoperative (1 year) SPECT with acetazol
side is corrected after the operation. Lower left: postoperative T2-weighted MRI (1
postoperative MRA (1 year) shows still patent right STA-M2 bypass, although th
small unruptured aneurysm than what was previously
thought [9]. However, most neurosurgeons do not have
the same impression on the basis of daily clinical practice
[7,11] and would estimate the risk of the aneurysm rupture
higher depending not only on size but also on shape, growth
rate, or hemodynamics of the aneurysm. Although it is
unclear if the unruptured AcomA aneurysm in association
with unilateral ICA occlusion tend to rupture more
compared with the usual AcomA aneurysm, several
ruptured de novo aneurysms of AcomA as the consequence
of previous therapeutic ICA occlusion have been reported
[1,2,3,6,10]. Considering robust cross-flow through AcomA
toward the hemisphere with ICA occlusion, we estimated
amide challenge shows that slightly decreased vascular reserve on the right
year) shows no evidence of right frontal contusion nor atrophy. Lower right:
e clip artifact is deteriorating the quality of the image.

T. Inoue et al. / Surgical Neurology 68 (2007) 226–232 231
that the risk of rupture of the present 2 cases would be high
and decided on surgical intervention.
Surgical treatment of the unruptured aneurysm with
ischemic cerebrovascular disease could be related to
increased risk of postoperative morbidity and mortality due
to general atherosclerotic changes as well as special fragility
of the ischemic brain [8]. In addition, in the cases of AcomA
aneurysm on the robust cross-flow, the ischemic damage of
the hemisphere with ICA occlusion could be devastating in
case of intraoperative rupture necessitating temporary occlu-
sion of A1 or perioperative transient spasm of A1 andAcomA
related to surgical manipulation. For the purpose of insur-
ance, and in the presence of slightly decreased vascular
reserve, the preceding bypass could increase the perioper-
ative general ischemic tolerance against the negative factors
such as retraction during clipping, CSF aspiration, and
hemodynamic instability related to anesthesia effect if the
bypass procedure itself is smoothly performed with accept-
able occlusion time. Therefore, we conducted a preceding
STA-M2 bypass. The reason why we chose M2 as the
recipient is because we expected immediate more robust flow
through the bypass compared with choosing a cortical branch
with smaller caliber as the recipient. The high flow bypass
using radial artery graft, in the presence of multiple lacunar
infarction as well as decreased vascular reserve, was thought
to be not ideal just for the insurance of the inadvertent
temporary occlusion of AcomA or A1, considering the risk of
hyperperfusion as well as the complex nature of this
technique itself. If the preoperative hemodynamic compro-
mise is more severe with decreased cerebral blood flow at rest
as well as severely impaired vascular reserve, 2-staged
operation (bypass surgery in first stage and after improve-
ment of hemodynamic compromise, clipping surgery in
second stage) could be the choice.
From the technical standpoint to reduce perioperative
ischemic complications as well as to prevent cognitive
impairment related to surgery, we used several ideas in the
present cases. First, we continued antiplatelet medication
throughout the perioperative period to reduce general
ischemic risk. Great care was taken to maintain a bloodless
microscopic operative field compared with the usual crani-
otomy by rigid hemostasis, especially of the temporalis
muscle andmiddle meningeal artery, as well as by augmented
peripheral tacking suture of the dura to bone margin. Second,
we paid attention in keeping the blood pressure relatively
high intraoperatively to avoid hemodynamic ischemia
especially before the institution of the bypass. Although we
did not use intraoperative monitoring in the present 2 cases,
such as SEP or MEP, it would help to decide how high the
blood pressure should be controlled. Third, we made every
effort to ease the STA-M2 bypass. During STA-M2 bypass,
rolled Bensheet was inserted between the frontal lobe and the
temporal lobe as a dpropT to keep the sylvian fissure open
enough (Fig. 6) without the aid of a retractor, which is some-
what disturbing during a bypass procedure [5]. Continuous
suction of the CSF with a small soft tube located deeper than
the anastomosis site during recipient occlusion also contrib-
uted to a smooth anastomosis by preventing the overflow of
CSF to the anastomosis site [5]. Fourth, sharp and enough
dissection of the sylvian fissure and interhemispheric fissure
with a microscissor enabled visualization of AcomA aneu-
rysm with minimal and atraumatic retraction. In the present
2 cases, the need for STA-M2 bypass obliged us to approach
the AcomA aneurysm from the side wherein the ipsilateral
A2 is anteriorly located and hindering the visualization of
aneurysm. Opening up the intehemispheric fissure and
careful retraction of the ipsilateral rectal gyrus well compen-
sated the previously mentioned disadvantage [4]. Although
final view and retraction during the clipping procedure are
somewhat frontobasal rather than pure transsylvian, wide
dissection of the sylvian fissure alsomade the retraction of the
ipsilateral frontal lobe and rectal gyrus gentle, which might
have contributed to prevent cognitive impairment by surgical
manipulation. However, if the anatomical condition of the
AcomA aneurysm is not suitable for the approach from the
occlusion side completely, a 2-staged operation using
contralateral or interhemispheric approach should be consid-
ered after bypass surgery.
References
[1] Drapkin AJ, Rose WS.. Serial development of dde novoT aneurysms
after carotid ligation: case report. Surg Neurol 1992;38:302 -8.
[2] Dyste GN, Beck DW.. De novo aneurysm formation following carotid
ligation: case report and review of the literature. Neurosurgery
1989;24:88-92.
[3] Fujiwara Sh, Fujii K, Fukui M.. De novo aneurysm formation and
aneurysm growth following therapeutic carotid occlusion for intra-
cranial carotid artery (ICA) aneurysms. Acta Neurochir (Wien)
1993;120:20-5.
[4] Hino A, Fuse I, Echigo T, Oka H, Iwamoto Y, Fujimoto M.. Clipping
of upward projecting anterior communicating aneurysms via pterional
craniotomy: approach from the side of A2 of anterior displacement.
No Shinkei Geka 2006;34(2):149 -58.
[5] Kamiyama H.. Bypass with radial artery graft. No Shinkei Geka
1994;22(10):911 -24.
[6] Maiuri F, Spaziante R, Iaconetta G, Signorelli F, Cirillo S, Salle FD..
dDe novoT aneurysm formation: report of two cases. Clin Neurol
Neurosurg 1995;97:233-8.
[7] Morita A, Fujiwara S, Hashi K, Ohtsu H, Kirino T.. Risk of rupture
associated with intact cerebral aneurysms in the Japanese population:
a systematic review of the literature from Japan. J Neurosurg
2005;102:601-6.
[8] Nagashima M, Nemoto M, Hadeishi H, Suzuki A, Yasui N..
Unruptured aneurysm associated with ischaemic cerebrovascular
diseases. Surgical Indication. Acta Neurochir 1993;124:71-8.
[9] The International Study of Unruptured Intracranial Aneurysms
Investigators. Unruptured intracranial aneurysms—risk of rupture
and risks of surgical intervention. N Engl J Med 1998;339:1725-33.
[10] Timperman PE, Tomsick TA, Tew JM, van Loveren HR.. Aneurysm
formation after carotid occlusion. AJNR Am J Neuroradiol 1995;
16:329-31.
[11] Tsukahara T, Murakami N, Sakurai Y, Yonekura M, Takahashi T,
Inoue T, Yonekawa Y.. Treatment of unruptured cerebral aneurysms; a
multi-center study at Japanese national hospitals. Acta Neurochir
2005;94(Suppl):77 -85.