clinicaloptions.com/hepatitis highlights from berlin 2011 march 30 - april 3, 2011 berlin, germany...
TRANSCRIPT

clinicaloptions.com/hepatitisHighlights From Berlin 2011
March 30 - April 3, 2011Berlin, Germany
Highlights From Berlin 2011CCO Independent Conference Coverage of the 46th Annual Meeting of the European Association for the Study of the Liver*
This program is supported by an educational grant from
*CCO is an independent medical education company that provides state-of-the-art medical information to healthcare professionals through conference coverage and other educational programs.
This program is supported by educational grants from

clinicaloptions.com/hepatitisHighlights From Berlin 2011
About These Slides
Our thanks to the presenters who gave permission to include their original data
Users are encouraged to use these slides in their own noncommercial presentations, but we ask that content and attribution not be changed. Users are asked to honor this intent
These slides may not be published or posted online without permission from Clinical Care Options (email [email protected])
DisclaimerThe materials published on the Clinical Care Options Web site reflect the views of the authors of the CCO material, not those of Clinical Care Options, LLC, the CME providers, or the companies providing educational grants. The materials may discuss uses and dosages for therapeutic products that have not been approved by the United States Food and Drug Administration. A qualified healthcare professional should be consulted before using any therapeutic product discussed. Readers should verify all information and data before treating patients or using any therapies described in these materials.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Faculty
Nezam H. Afdhal, MD, FRCPIAssociate Professor of MedicineHarvard Medical SchoolChief of HepatologyBeth Israel Deaconess Medical CenterBoston, Massachusetts
Paul Martin, MDProfessor of MedicineChief, Division of HepatologyCenter for Liver DiseaseUniversity of Miami School of MedicineMiami, Florida

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Disclosures
Nezam H. Afdhal, MD, FRCPI, has disclosed that he has received consulting fees and contracted research with GlaxoSmithKline, Merck, Pharmasset, Spring Bank, and Vertex.
Paul Martin, MD, has disclosed that he has received consulting fees from Bristol-Myers Squibb, Genentech, Merck, Salix, and Vertex; fees for non-CME services from Bristol-Myers Squibb and Vertex; and contracted research with Bristol-Myers Squibb, Gilead Sciences, Genentech, and Vertex.
Phase III Studies of Protease Inhibitors
clinicaloptions.com/hepatitisHighlights From Berlin 2011
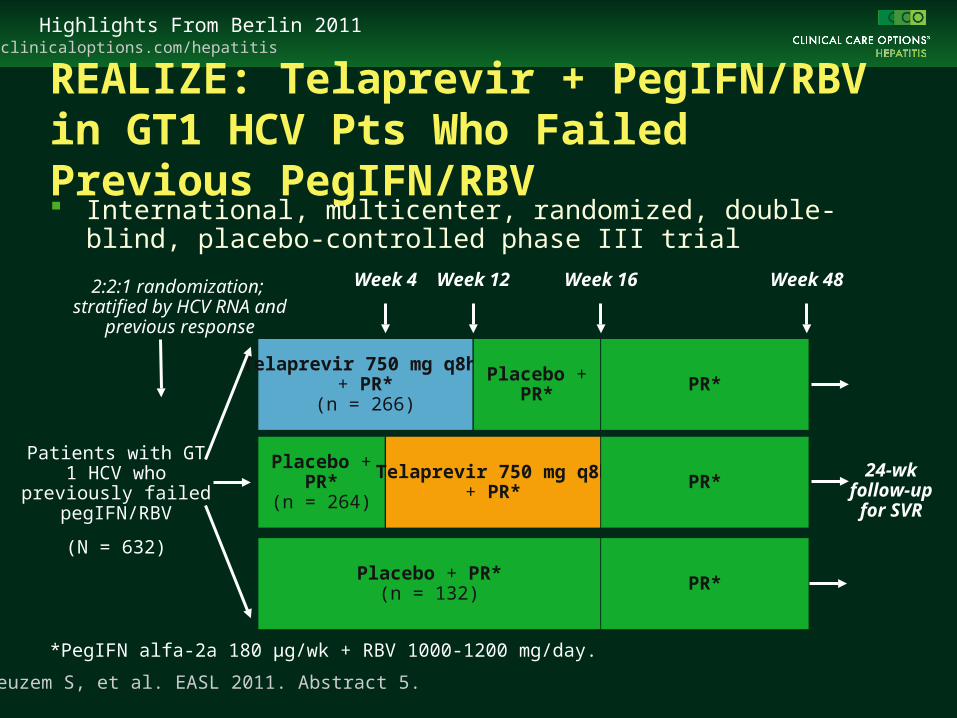
REALIZE: Telaprevir + PegIFN/RBV in GT1 HCV Pts Who Failed Previous PegIFN/RBV International, multicenter, randomized, double-blind, placebo-
controlled phase III trial
Zeuzem S, et al. EASL 2011. Abstract 5.
Patients with GT 1 HCV who previously failed pegIFN/RBV
(N = 632)
Telaprevir 750 mg q8h + PR*
(n = 266)
Placebo +PR*
(n = 264)
Placebo + PR*(n = 132)
Week 4
Telaprevir 750 mg q8h+ PR*
PR*
PR*
Week 12 Week 16 Week 482:2:1 randomization; stratified by HCV RNA and
previous response
*PegIFN alfa-2a 180 µg/wk + RBV 1000-1200 mg/day.
PR*
Placebo +PR*
24-wkfollow-up for SVR

clinicaloptions.com/hepatitisHighlights From Berlin 2011
REALIZE: SVR According to Previous Response
Zeuzem S, et al. EASL 2011. Abstract 5. Graphic used with permission.
100
80
60
40
20
0
SV
R (
%)
PreviousRelapsers
Previous Partial Responders
Previous NullResponders
*P < .001 vs PR48.LI, lead-in.
83* 88*
24
59*54*
15
33*29*
5
T12/PR48
LI-T12/PR48
PR48 T12/PR48
LI-T12/PR48
PR48 T12/PR48
LI-T12/PR48
PR48
n/N= 121/145 16/68 29/49 26/48 4/27 21/72 25/75 2/37124/141

clinicaloptions.com/hepatitisHighlights From Berlin 2011
REALIZE: SVR by Baseline Fibrosis Stage and Previous Response
Zeuzem S, et al. EASL 2011. Abstract 5.
SVR, % Pooled T12/PR48 PR48
Previous relapsers
No, minimal, or portal fibrosis 86 32
Bridging fibrosis 85 13
Cirrhosis 84 13
Previous partial responders
No, minimal, or portal fibrosis 72 18
Bridging fibrosis 56 0
Cirrhosis 34 20
Previous null responders
No, minimal, or portal fibrosis 41 6
Bridging fibrosis 39 0
Cirrhosis 14 10

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Subanalysis of ADVANCE: Role of IL28B in Response to Treatment With Telaprevir ADVANCE: phase III study of genotype 1, treatment-naive chronic hepatitis C
– T12PR: TVR + PR for 12 wks, then RGT with PR through Week 24 or 48
– T8PR: TVR + PR for 8 wks, placebo + PR for 4 wks, then RGT with PR through Week 24 or 48
– PR: placebo + PR or 12 wks, then PR through Week 48
42% (454 of 1088) of patients available for IL28B analysis; all patients in analysis were white
TVR increased SVR rates across IL28B genotypes, but CC still did better
CC patients tended to have better opportunity for RVR and shortened therapy
Jacobson I, et al. EASL 2011. Abstract 1369. Graphics used with permission.
SVR Rates in Patients Genotyped for IL28B
SV
R (
%)
T12PR T8PR PR
60
100
80
40
20
0n/N = 45/50 38/45 35/55
CC48/68 43/76 20/80
CT16/22 19/32 6/26
TT
90 84
6471
57
25
7359
23
SVR Rates in Patients With RVR
n/N = 39/42 30/32 9/9CC
36/41 34/47 2/2CT
10/13 14/16 0/0TT
93 94100
8872
100
7788

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Subanalysis of Phase III Boceprevir Trials: SVR in Advanced Fibrosis/CirrhosisSPRINT-2: GT1 treatment-naive
PR 4 wks, then BOC + PR 44 wks
PR 4 wks, then BOC + PR for 24 wks, then stop or PR + placebo 20 wks (RGT)
PR 4 wks, then PR + placebo 44 wks
RESPOND-2: GT1 relapsers and partial responders to pegIFN/RBV
PR 4 wks, then BOC + PR 44 wks
PR 4 wks, then BOC + PR for 32 wks, then stop or PR + placebo 12 wks (RGT)
PR 4 wks, then PR + placebo 44 wks
Bruno S, et al. EASL 2011. Abstract 7. Graphics used with permission. F3/4 F0/1/2
100
80
60
40
20
0
SV
R (
%)
F0/1/2
38
6767
384152
328319n= 313 243442
100
80
60
40
20
0
SV
R (
%)
F3/4
23
6668
13
44
68
61117n= 19 153231
Patients with F3/4 did better with full yr of therapy vs response-guided therapy
clinicaloptions.com/hepatitisHighlights From Berlin 2011
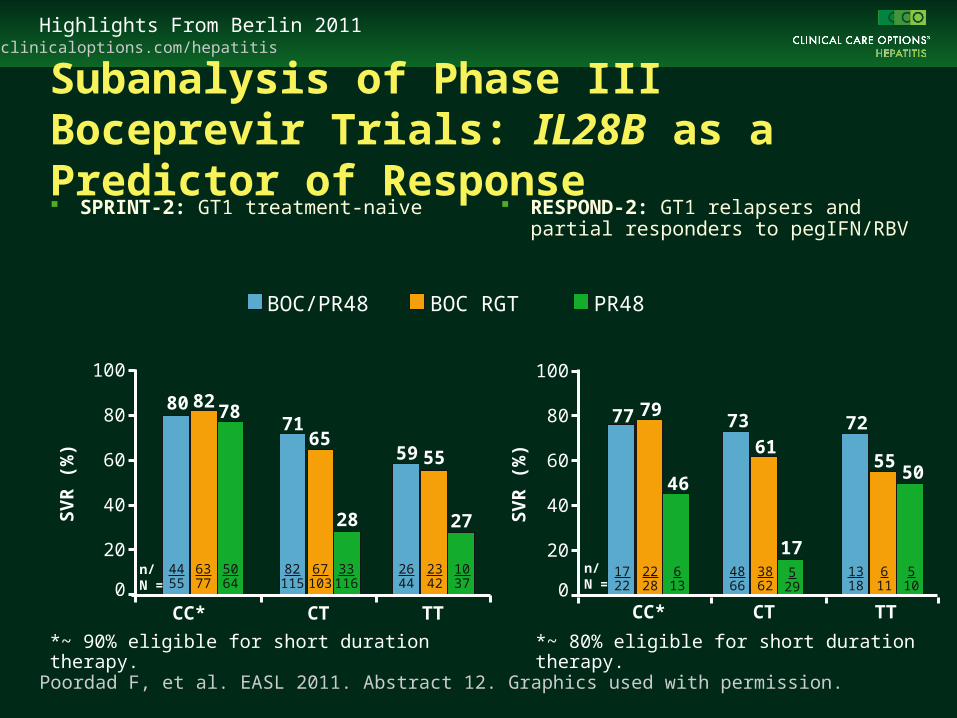
Subanalysis of Phase III Boceprevir Trials: IL28B as a Predictor of Response SPRINT-2: GT1 treatment-naive RESPOND-2: GT1 relapsers and
partial responders to pegIFN/RBV
Poordad F, et al. EASL 2011. Abstract 12. Graphics used with permission.
PR48BOC RGTBOC/PR48
100
80
60
40
20
0
SV
R (
%)
100
80
60
40
20
0
SV
R (
%)
CC* CT TT
6377
4455
67103
82115
2342
2644
82
6571
5559
5064
33116
1037
78
28 27
*~ 90% eligible for short duration therapy.
CC* CT TT
2228
1722
3862
4866
611
1318
7977
6173
613
529
510
46
17
55
72
50
80
*~ 80% eligible for short duration therapy.
n/N =
n/N =

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Poordad F, et al. EASL 2011. Abstract 12. Graphics used with permission.
100
80
60
40
20
0
Un
det
ecta
ble
HC
V R
NA
by
Wee
k 8*
(%
)
SPRINT-2 RESPOND-2
CCCT + TT
*Decision point for short vs long treatment duration with RGT.
89
52
82
51
118132
158304
4150
80156
Subanalysis of SPRINT-2 and RESPOND-2: IL28B as a Predictor of Response IL28B genotype a predictor of eligibility for shortened therapy

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Efficacy of Boceprevir When PegIFN alfa-2a Used as Backbone With RBV Randomized phase III trial with identical inclusion criteria to RESPOND-2 Previous nonresponders or relapsers randomized to
– 4-wk lead-in, then 44 wks placebo + pegIFN alfa-2a/RBV (n = 67), or
– 4-wk lead-in, then 44 wks BOC + pegIFN alfa-2a/RBV (n = 134)
Flamm S, et al. EASL 2011. Abstract 1366. Graphic used with permission.
SVR by Historical Response to Previous Treatment100
80
60
40
20
0
SV
R (
%)
PegIFN alfa-2a/RBV
BOC + pegIFN alfa-2a/RBV
Level observed in
RESPOND-2 trial using pegIFN alfa-2b
Previous Nonresponder Previous Relapser
5
47
28
70
21
64
Overall86/134 14/67 17/36 1/20 69/98 13/47n/N =
21
66
7
52
29
75
Novel HCV Agents in Treatment-Naive Patients

clinicaloptions.com/hepatitisHighlights From Berlin 2011
SILEN-C1: BI 201335 + PegIFN/RBV in GT1 Treatment-Naive Patients BI 201335: an inhibitor of HCV NS3-4A protease Placebo-controlled, double-blind phase IIb trial
Sulkowski M, et al. EASL 2011. Abstract 60.
*PegIFN alfa-2a 180 μg/wk + RBV 1000-1200 mg/day. †On Day 1, loading dose of BI 201335 given in all BI 201355 arms (double daily dose: 240 or 480 mg).
Treatment-naive patients infected with GT1 HCV
(N = 429) BI 201335 240 mg/day† + PR*(n = 143)
BI 201335 120 mg/day† + PR*(n = 69)
Week 24
BI 201335 240 mg/day† + PR* (n = 146)
Placebo + PR*(n = 71)
Randomized 1:2:2:1
Lead-in*(n = 146)
Lead-in*(n = 69)
Day 4
PR*
Stop treatment; follow-up only
PR*
PR*
Week 48
eRVR
No eRVR

clinicaloptions.com/hepatitisHighlights From Berlin 2011
SILEN-C1: BI 201335 + PegIFN/RBV in GT1 Treatment-Naive Patients Higher SVR rates in BI 201335
240 mg QD arms No benefit of extended treatment in
those with eRVR
Sulkowski M, et al. EASL 2011. Abstract 60. Graphics used with permission.
40/71 49/69 103/142 118/142
SVR
Pat
ien
ts (
%)
56
71 7383
100
80
60
40
20
0
P = .081
P = .021
P = .001
PegIFN/RBV 120 mg QD LI240 mg QD LI 240 mg QD 240 mg QD LI
240 mg QD
SVR in eRVR Patients Randomized to 24 or 48 Wks of PegIFN/RBV
40/49 53/57 46/48 53/59
24 Wks
8293 96
90100
80
60
40
20
0
P = .051
48 Wks
P = .743
Pat
ien
ts (
%)
LI, arm containing lead-in phase.
n/N = n/N =

clinicaloptions.com/hepatitisHighlights From Berlin 2011
SILEN-C1: BI 201335 + PegIFN/RBV in GT1 Treatment-Naive Patients
Sulkowski M, et al. EASL 2011. Abstract 60. Graphic used with permission.
Safety, % Control Arm
(n = 71)
240-mg BI 201335(n = 149)
240-mg BI 201335 With Lead-in
(n = 138)
120-mg BI 201335 With Lead-in
(n = 68)
Serious adverse event 4.2 12.8 15.9 11.8
Discontinuation due to adverse events 1.4 5.4 11.6 4.4
Rash 0 3.4 3.6 0
Photosensitivity 0 0.7 0 0
Jaundice 0 0.7 0 0
Adverse events*
Nausea 19.7 44.3 47.1 25.0
Diarrhea 18.3 26.8 31.9 13.2
Vomiting 5.6 22.8 18.1 20.6
Pruritus 16.9 37.6 34.8 32.4
Rash 16.9 26.8 28.3 20.6
• Moderate 2.8 14.1 8.0 2.9
• Severe 0 4.0 3.6 0
Jaundice† 1.4 24.2 18.8 5.9
*Events ≥ 10% relative to control.†No severe cases.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
ESSENTIAL: Alisporivir + PegIFN/RBV in GT1 Treatment-Naive Patients Alisporivir: oral inhibitor of cyclophilin that acts as host-targeted antiviral
– Modified form of cyclosporin A with enhanced cyclophilin binding but no immunosuppressive activity
– Targets host cyclophilin A required for HCV replication
Placebo-controlled, double-blind phase IIb trial
Flisiak R, et al. EASL 2011. Abstract 4.
Treatment-naive patients with
genotype 1 HCV
(N = 288)
Alisporivir* + PR†
(n = 72)
Alisporivir* + PR†
(n = 72)
Alisporivir* + PR†
(n = 71)
Week 48
Placebo + PR†
(n = 73)
Week 24
RGT: alisporivir + PR‡ 24-wk follow-up
*Alisporivir dosed at 600 mg BID for first wk, then 600 mg QD thereafter. †PegIFN alfa-2a 180 µg/wk + RBV 1000-1200 mg/ day. ‡Patients with RVR (ie, HCV RNA ≤ 10 IU/mL at Week 4) treated for 24 wks; patients without RVR treated for 48 wks.
clinicaloptions.com/hepatitisHighlights From Berlin 2011
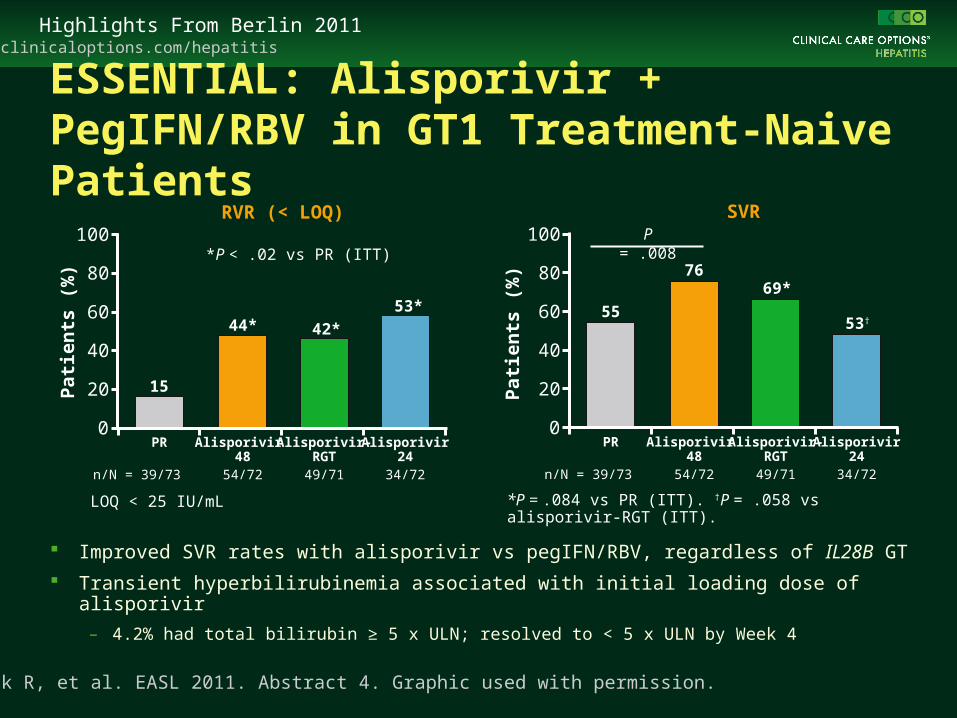
ESSENTIAL: Alisporivir + PegIFN/RBV in GT1 Treatment-Naive Patients
Improved SVR rates with alisporivir vs pegIFN/RBV, regardless of IL28B GT
Transient hyperbilirubinemia associated with initial loading dose of alisporivir
– 4.2% had total bilirubin ≥ 5 x ULN; resolved to < 5 x ULN by Week 4
Flisiak R, et al. EASL 2011. Abstract 4. Graphic used with permission.
100
80
60
40
20
0
Pat
ien
ts (
%)
LOQ < 25 IU/mL
15
44* 42*
53*
PR Alisporivir 48
Alisporivir-RGT
Alisporivir24
n/N = 39/73 54/72 49/71 34/72
100
80
60
40
20
0
Pat
ien
ts (
%)
55
7669*
53†
PR Alisporivir 48
Alisporivir-RGT
Alisporivir24
n/N = 39/73 54/72 49/71 34/72
P = .008RVR (< LOQ) SVR
*P = .084 vs PR (ITT). †P = .058 vs alisporivir-RGT (ITT).
*P < .02 vs PR (ITT)

clinicaloptions.com/hepatitisHighlights From Berlin 2011
BMS-790052: NS5A replication complex inhibitor
BMS-790052 dosed at 3, 10, or 60 mg QD or placebo, each with pegIFN/RBV for 48 wks
– High rates of SVR with BMS-790052 dosed at 10 or 60 mg QD
BMS-790052 in Tx-Naive GT1 Patients:12-Wk Posttx Analysis of Phase IIa Trial
Safety outcomes with BMS-790052 similar to pegIFN/RBV + placebo
– No incremental hematologic, dermatologic, or hepatic toxicities
Pol S, et al. EASL 2011. Abstract 1373. Graphic used with permission.
RVRSVR12
Su
bje
cts
(%
)*
100
80
60
40
20
05/12 5/12 11/12 11/12 1/12 3/1210/12 10/12
3 mg 10 mg
BMS-790052 (QD)
60 mg Placebo
*Intent to treat analysis.RVR, undetectable (< 10 IU/mL) HCV RNA at Week 4.
clinicaloptions.com/hepatitisHighlights From Berlin 2011
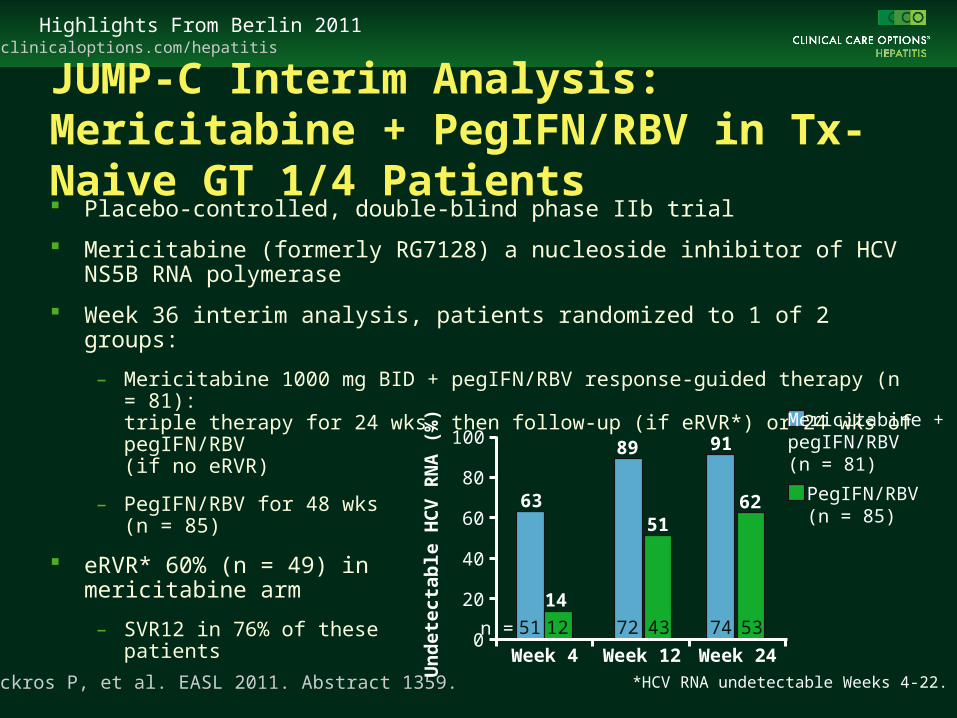
JUMP-C Interim Analysis: Mericitabine + PegIFN/RBV in Tx-Naive GT 1/4 Patients Placebo-controlled, double-blind phase IIb trial
Mericitabine (formerly RG7128) a nucleoside inhibitor of HCV NS5B RNA polymerase
Week 36 interim analysis, patients randomized to 1 of 2 groups:
– Mericitabine 1000 mg BID + pegIFN/RBV response-guided therapy (n = 81): triple therapy for 24 wks, then follow-up (if eRVR*) or 24 wks of pegIFN/RBV (if no eRVR)
– PegIFN/RBV for 48 wks (n = 85)
eRVR* 60% (n = 49) in mericitabine arm
– SVR12 in 76% of these patients
Pockros P, et al. EASL 2011. Abstract 1359. *HCV RNA undetectable Weeks 4-22.
63
89 91
14
5162
0
20
40
60
80
100
Week 4 Week 12 Week 24
Mericitabine + pegIFN/RBV(n = 81)
PegIFN/RBV(n = 85)
Un
det
ecta
ble
HC
V R
NA
(%
)
n = 51 72 4312 5374

clinicaloptions.com/hepatitisHighlights From Berlin 2011
ZENITH Week 12 Interim Analysis: VX-222 + Telaprevir ± PegIFN/RBV in GT1 Tx Naive Parallel-group, dose-ranging phase II study
*A fifth arm assessing VX-222 400 mg QD + telaprevir 1125 mg BID + RBV currently accruing.†PegIFN 180 µg/wk + weight-based RBV 1000-1200 mg/day.
Treatment-naive patients with
chronic GT1 HCV infection*
(N = 106)
VX-222 400 mg BID + Telaprevir 1125 mg BID(n = 29)
VX-222 100 mg BID + Telaprevir 1125 mg BID + PR†
(n = 29)
VX-222 400 mg BID + Telaprevir 1125 mg BID + PR†
(n = 30)
Week 12
VX-222 100 mg BID + Telaprevir 1125 mg BID(n = 18)
PR for 12 wks if HCV RNA detectable at Weeks 2 or 8†
Week 36‡Stratified by GT (1a/unknown vs 1b) Week 24
Di Bisceglie A, et al. EASL 2011. Abstract 1363.
Stop tx if HCV RNA undetectable at Weeks 2 and 8†
PR for 12 wks if HCV RNA
detectable at Weeks 2 or 8†
Stop tx ifHCV RNA
undetectable at Weeks 2 and 8†

clinicaloptions.com/hepatitisHighlights From Berlin 2011
No virologic breakthrough in quad-therapy arms
Virologic breakthrough common in VX-222/TVR dual-therapy arms (17% to 31%)
– Both dual regimens stopped prematurely per protocol
HC
V R
NA
Un
det
ecta
ble
(%
)
2217
0 0
24
59
1424
38
86
38
83
57
87
50
90
0
20
40
60
80
100
Week 2 Week 4 Weeks 2 & 8* Week 12
VX-222 100 mg + telaprevir (n = 18)
VX-222 400 mg + telaprevir (n = 29)
VX-222 100 mg + telaprevir + PR (n = 29)
VX-222 400 mg + telaprevir + PR (n = 30)
Di Bisceglie A, et al. EASL 2011. Abstract 1363.
ZENITH Week 12 Interim Analysis: VX-222 + Telaprevir ± PegIFN/RBV in GT1 Tx Naive
*Indicates patients eligible for shortened therapy.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
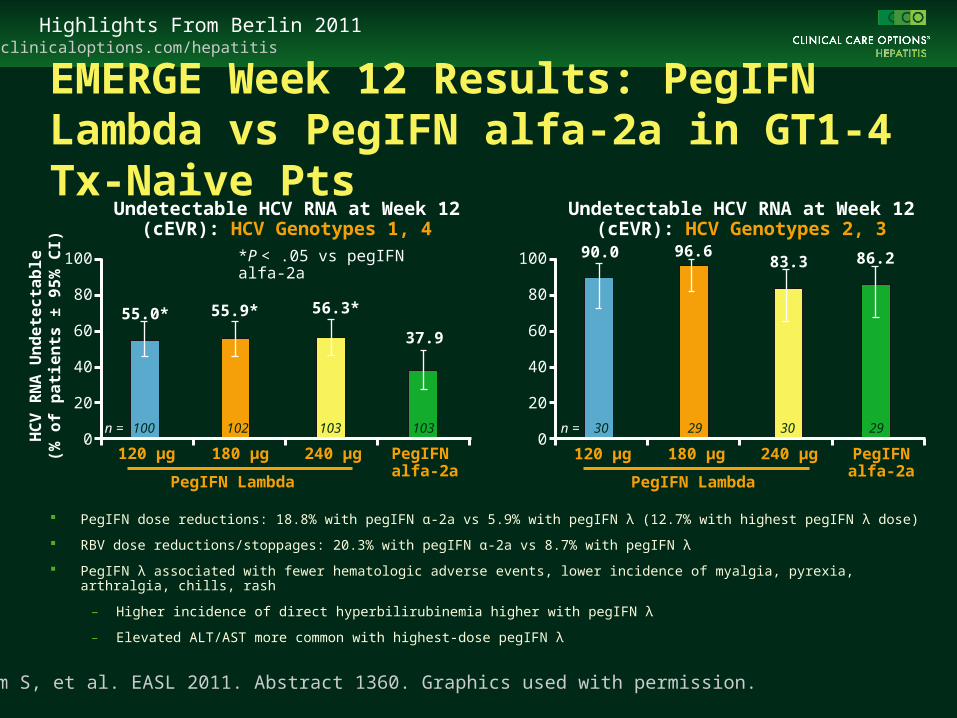
EMERGE Week 12 Results: PegIFN Lambda vs PegIFN alfa-2a in GT1-4 Tx-Naive Pts Phase IIb trial
Zeuzem S, et al. EASL 2011. Abstract 1360.
Interferon-naive pts
(N = 526)
PegIFN alfa-2a 180 μg/wk + RBV*(n = 133)
PegIFN lambda 120 μg/wk + RBV(n = 128)
PegIFN lambda 180 μg/wk + RBV(n = 131)
Week 24 genotypes 2,3Week 48 genotypes 1,4Genotyping at baseline
PegIFN lambda 240 μg/wk + RBV(n = 134)
*RBV dosed at 800 mg/day for genotype 2/3 and 1000-1200 mg/day for genotype 1/4 patients.
clinicaloptions.com/hepatitisHighlights From Berlin 2011
Zeuzem S, et al. EASL 2011. Abstract 1360. Graphics used with permission.
PegIFN dose reductions: 18.8% with pegIFN α-2a vs 5.9% with pegIFN λ (12.7% with highest pegIFN λ dose)
RBV dose reductions/stoppages: 20.3% with pegIFN α-2a vs 8.7% with pegIFN λ
PegIFN λ associated with fewer hematologic adverse events, lower incidence of myalgia, pyrexia, arthralgia, chills, rash
– Higher incidence of direct hyperbilirubinemia higher with pegIFN λ
– Elevated ALT/AST more common with highest-dose pegIFN λ
Undetectable HCV RNA at Week 12 (cEVR): HCV Genotypes 1, 4
55.0* 55.9* 56.3*
37.9
HC
V R
NA
Un
de
tec
tab
le(%
of
pa
tie
nts
± 9
5%
CI) 100
80
60
40
20
0120 µg 180 µg 240 µg PegIFN
alfa-2a
n = 100 102 103 103
*P < .05 vs pegIFN alfa-2a
Undetectable HCV RNA at Week 12 (cEVR): HCV Genotypes 2, 3
90.0 96.683.3 86.2100
80
60
40
20
0n = 30 29 30 29
PegIFN Lambda
120 µg 180 µg 240 µg PegIFNalfa-2a
PegIFN Lambda
EMERGE Week 12 Results: PegIFN Lambda vs PegIFN alfa-2a in GT1-4 Tx-Naive Pts

clinicaloptions.com/hepatitisHighlights From Berlin 2011
PROTON: PSI-7977 + PegIFN/RBV in GT2/3 or GT1 Treatment-Naive Patients PSI-7977: pyrimidine nucleotide
analog polymerase inhibitor
PROTON: phase IIb study of PSI-7977–based triple therapy in treatment-naive patients
– SVR12 in 96% of GT2/3 patients (N = 25) treated with PSI-7977 400 mg QD + pegIFN/RBV for 12 wks (ITT analysis)[1]
– 12-wk interim analysis in GT1 compares PSI-7977 at 200 mg QD or 400 mg QD vs placebo, all with pegIFN/RBV (ITT analysis)[2]
Extended RVR in 95% of GT1 patients receiving PSI-7977[2]
1. Lalezari J, et al. EASL 2011. Abstract 61. 2. Nelson D, et al. EASL 2011. Abstract 1372. Graphic used with permission.
100
80
60
40
20
0Week 2 Week 4 Week 12
HC
V R
NA
< L
OD
(%
)
PSI-7977 400 mg + pegIFN/RBV (n = 47)PSI-7977 200 mg + pegIFN/RBV (n = 48)Placebo + pegIFN/RBV (n = 26)
10092
62
9898
19
7177
NR

clinicaloptions.com/hepatitisHighlights From Berlin 2011
NUCLEAR: Phase I Study of 14 Days QD PSI-7977 + PSI-938 in Tx-Naive GT1 HCV PSI-938: purine nucleotide analog with complementary mechanism, activity to PSI-7977
Lawitz E, et al. EASL 2011. Abstract 1370. Graphic used with permission.
HCV RNA Change From Baseline*
Day 7 Day 14 Total
< LOD, n Median (Q1, Q3) < LOQ, n < LOD, n Median (Q1, Q3) < LOD, %
Cohort 1 2 -4.5 (-4.3, -4.7) 5 4 -5.2 (-4.8, -5.8) 50
Cohort 2 2 -4.6 (-4.2, -5.0) 8 8 -5.2 (-4.8, -5.5) 100
Cohort 3 4 -4.7 (-4.3, -4.8) 8 7 -5.0 (-4.6, -5.4) 88
Cohort 4 1 -4.4 (-4.2, -4.8) 8 5 -5.0 (-4.7, -5.3) 88†
HC
V R
NA
Ch
an
ge
Fro
m
Ba
se
lin
e (
log
10 I
U/m
L)
*Cumulative total of individuals whose HCV RNA reached < LOD as a result of the study treatment. †Includes 2 additional subjects whose HCV RNA reached < LOD on Day 16. LOD < 15 IU/mL. Median baseline HCV RNA 6.9 in cohort 1, 6.3 in cohort 2, 6.3 in cohort 3, 6.2 in cohort 4.
Cohort 1: PSI-938 Days 1-14
Cohort 2: PSI-938 Days 1-7 → PSI-938 + PSI-7977 Days 8-14
Cohort 3: PSI-7977 Days 1-7 → PSI-938 + PSI-7977 Days 8-14
Cohort 4: PSI-938 + PSI-7977 Days 1-14
0-1-2-3-4-5-6-7
20 144 6 8 10 12Days
PSI-938 dosed at 300 mg QD, PSI-7977 dosed at 400 mg QD.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
PILLAR: Impact of IL28B and IP-10 in GT1 Tx-Naive Patients Receiving TMC435 + PR Phase IIb study of TMC435 combined with pegIFN/RBV
In patients treated with placebo + pegIFN/RBV, IP-10 level and IL28B genotype predictive of response, most notably at Week 24
– Best responses in those with lower IP-10 levels, CC IL28B genotype
Aerssens J, et al. EASL 2011. Abstract 11. Graphic used with permission.
Virologic Response*: Placebo + PegIFN/RBV
100
80
60
40
20
0
IP-10
IL28
B
< 600 pg/mL600 pg/mL
Week 4 Week 24
TT
CT
CC
100
80
60
40
20
0
IP-10
IL28
B
< 600 pg/mL600 pg/mL
TT
CT
CCPat
ien
ts (
%)
20 5
17
0
50
77
40
100
*HCV RNA < 25 IU/mL.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
100
PILLAR: Impact of IL28B and IP-10 in GT1 Tx-Naive Patients Receiving TMC435 + PR High response rates with TMC435 + pegIFN/RBV regardless of
IP-10 level or IL28B genotype
Highest rates of response in difficult-to-treat patients (low IP-10, TT IL28B genotype) in those treated with TMC435 150 mg QD
Aerssens J, et al. EASL 2011. Abstract 11. Graphics used with permission.
Virologic Response*:TMC435 150 mg QD + PegIFN/RBV
Virologic Response*:TMC435 75 mg QD + PegIFN/RBV
Week 4
100
80
60
4020
0
IP-10
IL28
B
< 600 pg/mL600 pg/mL
TTCT
CCPat
ien
ts (
%)
N=1
86100
10010093
67
Week 24
100
80
60
4020
0
IP-10
IL28
B
< 600 pg/mL600 pg/mL
TTCT
CC
96100
100100
67
Week 4
100
80
60
4020
0
IP-10
IL28
B
< 600 pg/mL600 pg/mL
TT
CTCCP
atie
nts
(%
)
N=1
100
Week 24
100
80
60
4020
0
IP-10
IL28
B
< 600 pg/mL600 pg/mL
TTCT
CC
N=1
100 90100100
83
95
77
9596
100
100
*HCV RNA < 25 IU/mL
Novel HCV Agents in Treatment-Experienced Patients

clinicaloptions.com/hepatitisHighlights From Berlin 2011
BMS-790052 + BMS-650032 ± PegIFN/RBV for 24 Wks in GT1 Null Responders
In dual therapy arm, 2/2 GT1b vs 2/9 GT1a patients reached SVR12 and SVR24
No viral breakthrough with quadruple therapy
BMS-790052 and BMS-650032 alone or with pegIFN/RBV generally well tolerated
Lok A, et al. EASL 2011. Abstract 1356.
BMS-790052 60 mg QD + BMS-650032 600 mg BID
(n = 11)Phase IIa study: GT1 null responders*
with HCV RNA ≥ 105 IU/mL
(N = 21)
Follow-up 48 wksBMS-790052 60 mg QD +
BMS-650032 600 mg BID +PegIFN/RBV
(n = 10)
Week 24Stratified by HCV subgenotype
(1a vs 1b)
*< 2 log10 IU/mL decline in HCV RNA with ≥ 12 wks of pegIFN/RBV.
†1 patient not achieving SVR24 had HCV RNA < 25 IU/mL at EOT and undetectable on retesting at Day 35 of follow-up.
Undetectable HCV RNA, % (n)
BMS-790052 +BMS-650032
(n = 11)
BMS-790052 +BMS-650032 + PR
(n = 10)
RVR 64 (7) 60 (6)
SVR12 36 (4) 100 (10)
SVR24 36 (4) 90† (9)

clinicaloptions.com/hepatitisHighlights From Berlin 2011
SILEN-C2: BI 201335 + PegIFN/RBV in GT1 PegIFN/RBV Tx-Experienced Patients Phase IIb, double blind, placebo-controlled trial
Sulkowski M, et al. EASL 2011. Abstract 66.
GT1 previous nonresponders
(N = 288)
PR* + BI 201335 240 mg BID
PR* + BI 201335 240 mg QD†
Week 24
PR* + BI 201335 240 mg QD†‡
(n = 76)
Randomized 1:1:2
*PegIFN alfa-2a 180 μg/wk + RBV 1000-1200 mg/day. †Patients with eRVR at Week 24 rerandomized 1:1 to 24 or 48 total wks of pegIFN/RBV.
Lead-in*(n = 70)
Day 4
PR*
PR*
PR*
Week 48
Off-tx follow-upLead-in*(n = 142)

clinicaloptions.com/hepatitisHighlights From Berlin 2011
SILEN-C2: BI 201335 + PegIFN/RBV in GT1 PegIFN/RBV Tx-Experienced Patients
Sulkowski M, et al. EASL 2011. Abstract 66. Graphics used with permission.
SVR in eRVR Pts by Duration of PegIFN/RBV
Null response: < 1 log10 maximum HCV RNA reduction any time during treatment;partial response: > 1 log10 maximum HCV RNA reduction but never undetectable (with a sensitive assay).
100
80
60
40
20
0
Pat
ien
ts (
%)
Overall Partial Responders
Null Responders
39/142 22/70 16/54 10/24 12/57 11/38
2731 30
42
21
31/76 13/26 14/40
41
50
3529
240 mg QD 240 mg QD LI240 mg BID LI
240 mg QD LI 24 wks240 mg QD LI 48 wks100
80
60
40
20
0
Pat
ien
ts (
%)
Overall
12/30 21/29
40
P = .018
72
SVR According to Previous Response Category
n/N = n/N =

clinicaloptions.com/hepatitisHighlights From Berlin 2011
SILEN-C2: BI 201335 + PegIFN/RBV in GT1 PegIFN/RBV Tx-Experienced PatientsOutcome, % 240-mg QD
BI 201335(n = 76)
240-mg QDBI 201335
With Lead-in(n = 141)
240-mg BIDBI 201335
With Lead-in(n = 69)
Serious adverse event 14.5 14.2 27.5
Discontinuation due to adverse events 3.9 5.7 23.2
Rash 1.3 0 14.5
Photosensitivity 0 0 1.4
Jaundice 0 0.7 1.4
Adverse events*
Nausea 52.6 48.2 63.8
Diarrhea 31.6 31.9 39.1
Vomiting 22.4 17.0 31.9
Rash 27.6 34.0 42.0
• Severe 1.3 0.7 5.8
Jaundice† 21.1 19.0 41.4
Sulkowski M, et al. EASL 2011. Abstract 66. Graphic used with permission.*Events ≥ 10% relative to control. †No severe cases.
clinicaloptions.com/hepatitisHighlights From Berlin 2011
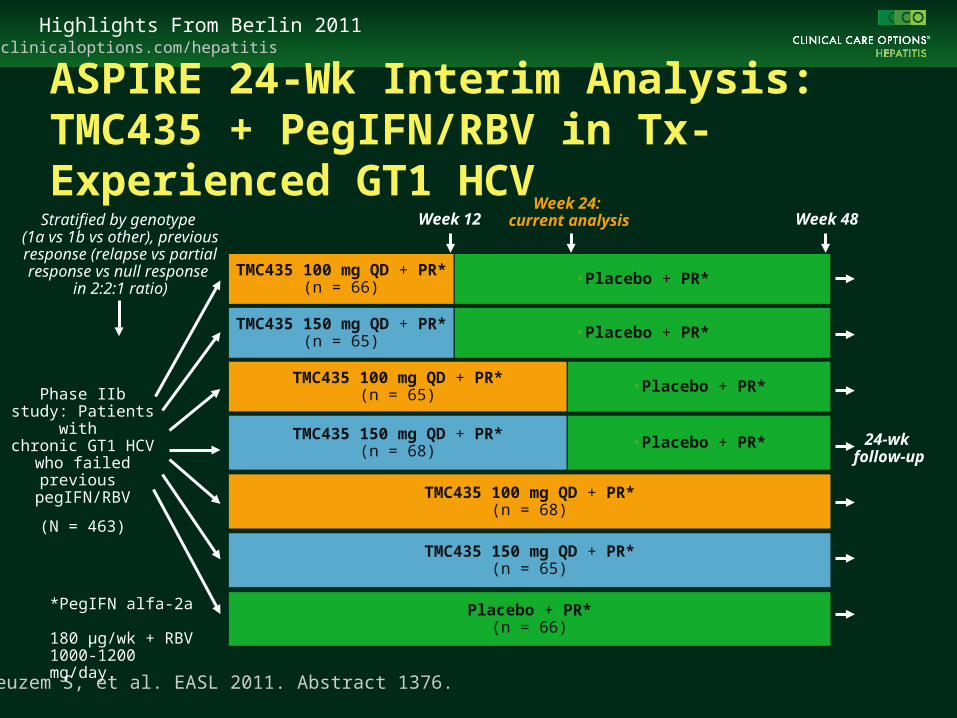
ASPIRE 24-Wk Interim Analysis: TMC435 + PegIFN/RBV in Tx-Experienced GT1 HCV
Zeuzem S, et al. EASL 2011. Abstract 1376.
*PegIFN alfa-2a 180 µg/wk + RBV 1000-1200 mg/day.
24-wk follow-up
Phase IIb study: Patients with
chronic GT1 HCV who failed previous
pegIFN/RBV
(N = 463)
TMC435 150 mg QD + PR*(n = 65)
TMC435 100 mg QD + PR*(n = 65)
TMC435 150 mg QD + PR*(n = 68)
Week 12
TMC435 100 mg QD + PR*(n = 66)
Week 48
TMC435 100 mg QD + PR*(n = 68)
TMC435 150 mg QD + PR*(n = 65)
Placebo + PR*(n = 66)
Week 24: current analysis
•Placebo + PR*
•Placebo + PR*
•Placebo + PR*
•Placebo + PR*
Stratified by genotype (1a vs 1b vs other), previous response (relapse vs partial response vs null response
in 2:2:1 ratio)

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Results of ASPIRE 24-Wk Interim Analysis in Previous Null Responders Significantly higher rates of undetectable HCV RNA with TMC435-containing
arms vs pegIFN/RBV alone
– Undetectable HCV RNA at Week 24 in 70% to 87% of previous null responders, 83% to 89% of previous partial responders, 92% to 96% of previous relapsers
Safety and tolerability of TMC435-based regimens comparable to pegIFN/RBV apart from increase in influenzalike symptoms and pruritus
Zeuzem S, et al. EASL 2011. Abstract 1376.
Rates of Undetectable HCV RNA in Previous Null Responders to PegIFN/RBV
10080
60
4020
0
Week 4
Pat
ien
ts (
%)
TMC 100 mgGroups(n = 47)
TMC 150 mgGroups(n = 51)
PR48(n = 16)
4036
100
8060
4020
0
Week 24
Pat
ien
ts (
%)
TMC 100 mg12 Wks(n = 14)
TMC 100 mg
24 & 48 WksCombined
(n = 28)
PR48(n = 9)
7470 7087
45
TMC 150 mg12 Wks(n = 17)
TMC 150 mg
24 & 48 WksCombined
(n = 31)
0

Hepatitis B

clinicaloptions.com/hepatitisHighlights From Berlin 2011
1285 HBsAg-positive individuals with 19,321 PYs follow-up
– 111 incident HCC cases
Persistent HBV DNA as Predictor for HCC
Liu J, et al. EASL 2011. Abstract 68. Graphic used with permission.
Factor HCC Incidence Rate per
100,000 PYs
Multivariable-Adjusted HR
for HCC*(95% CI)
P Value
HBeAg seroclearance†
No 1123.9 1.0
Yes 729.4 0.85 (0.53-1.36) .49
HBV DNA decreased to undetectable
No 669.2 1.0
Yes 94.3 0.28 (0.08-0.98) .04
HBsAg seroclearance
No 609.7 1.0
Yes 78.1 0.73 (0.09-6.25) .77
*Adjusted for age, sex, smoking, drinking, baseline HBV DNA, and baseline ALT.†HBeAg-positive patients only (N = 439).
0.12
0.10
0.08
0.06
0.04
0.02
0
Cu
mu
lati
ve H
CC
Inci
den
ce
0 2 4 6 8 10 12 14 16 18
Yrs
HBV DNA persistently detectable
HBV DNA seroclearance
1.5%
11.1%
clinicaloptions.com/hepatitisHighlights From Berlin 2011
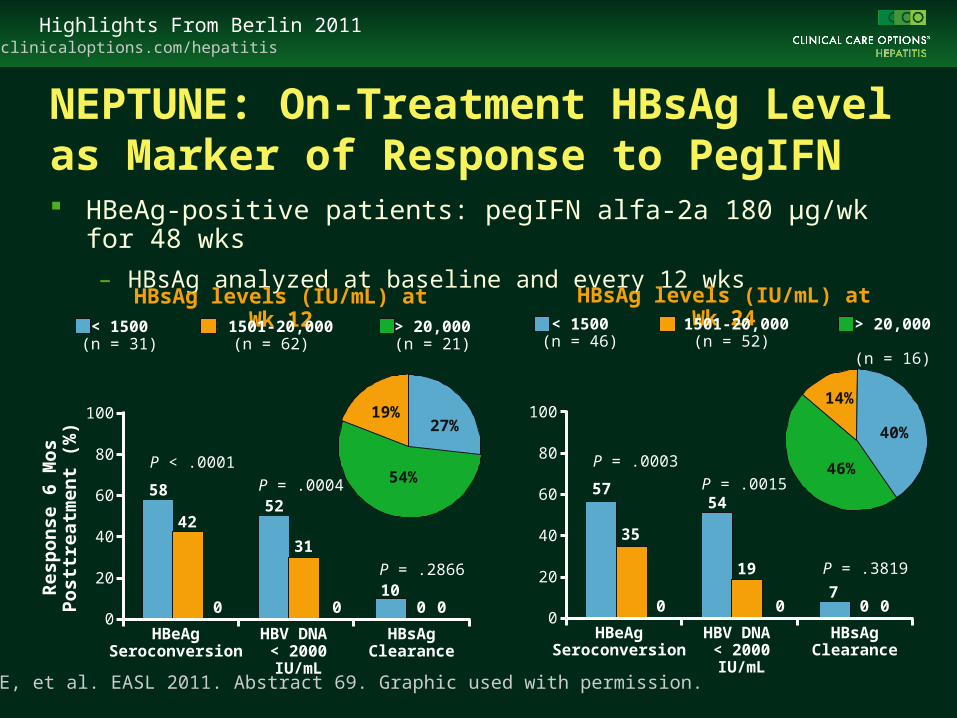
NEPTUNE: On-Treatment HBsAg Level as Marker of Response to PegIFN HBeAg-positive patients: pegIFN alfa-2a 180 µg/wk for 48 wks
– HBsAg analyzed at baseline and every 12 wks
Gane E, et al. EASL 2011. Abstract 69. Graphic used with permission.
HBsAg levels (IU/mL) at Wk 12
100
80
60
40
20
0
Res
po
nse
6 M
os
Po
sttr
eatm
ent
(%)
P < .0001
P = .0004
19%27%
54%
HBeAg Seroconversion
HBV DNA < 2000 IU/mL
HBsAg Clearance
< 1500(n = 31)
< 1501-20,000(n = 62)
> 20,000(n = 21)
P = .2866
58
42
0
52
31
0 0 010
HBsAg levels (IU/mL) at Wk 24
100
80
60
40
20
0
P = .0003
P = .0015
14%
40%
46%
HBeAg Seroconversion
HBV DNA < 2000 IU/mL
HBsAg Clearance
< 1500(n = 46)
< 1501-20,000 (n = 52)
> 20,000 (n = 16)
P = .3819
57
35
0
54
19
0 0 07

clinicaloptions.com/hepatitisHighlights From Berlin 2011
NEPTUNE: On-Treatment HBsAg as Marker of Response to PegIFN HBsAg < 20,000 IU/mL identified as key
marker of response
HBsAg > 20,000 IU/mL at Week 12 or 24 predicts lack of HBeAg seroconversion
– Negative predictive value: 100%
Combination of ALT level and HBsAg decline improves positive predictive value
Gane E, et al. EASL 2011. Abstract 69. Graphic used with permission.
100
80
60
40
20
0HB
eAg
Se
roco
nve
rsio
n
6 M
os
Po
sttr
eatm
ent
(%)
47
0 0
45
Week 12 Week 24
HBsAg (IU/mL)
(n = 93)
< 20,000
(n = 21)
> 20,000
(n = 98)
< 20,000
(n = 16)
> 20,000
100
80
60
40
20
0HB
eAg
Se
roco
nve
rsio
n
6 M
os
Po
sttr
eatm
ent
(%)
46
0 0
45
1-2 x ULN > 2 x ULN
HBsAg Levels at Week 12
< 1500 IU/mL 1500-20,000 IU/mL> 20,000 IU/mL
68
31
ALT

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Does IL28B GT Predict HBsAg Clearance? Primarily HBeAg-Negative Population HBsAg-positive patients treated
with IFN or pegIFN for 12-24 mos (N = 151)
– 127 HBeAg negative
– 24 HBeAg positive
– All white, HBV genotype D
Response defined as HBsAg loss and anti-HBs seroconversion
– Mean posttreatment follow-up: 24 mos (range: 12-52)
No significant association observed
Mangia A, et al. EASL 2011. Abstract 1331. Graphic used with permission.
P = .28
IL28B Genotype and HBsAg Clearance
100
80
60
40
20
0IL
28B
Dis
trib
uti
on
(%
)
HBsAg Clearance
No HBsAg Clearance
5044
6
35
47
18
CCCTTT

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Does IL28B GT Predict HBsAg Clearance? HBeAg-Positive Population HBeAg-positive patients treated with IFN (n =
14) or pegIFN alfa-2a or 2b ± LAM (n = 191)
– 65% Asian, 29% white
– HBV GT: 47% C, 20% B, 13% A, 13% D
IL28B genotyping at SNPs rs12980275 and rs12979860
– Only rs12980275 reported
– AA/AG/GG nomenclature with this SNP essentially equivalent to common CC/CT/TT nomenclature with rs12979860
Median follow-up: 173 wks (IQR: 108-356)
IL28B independently predicted HBeAg seroconversion and HBsAg seroclearance
Sonneveld MJ, et al. EASL 2011. Abstract 71.Graphics used with permission.
HR for AA vs AG/GG: 3.47 (1.04-13.48)
HR for AA vs AG/GG*: 2.14 (1.14-4.31)
*Adjusted for HBV genotype and baseline ALT and HBV DNA
100
80
60
40
20
0Cu
mu
lati
ve
Pro
ba
bil
ity
of
HB
eA
g S
ero
co
nv
ers
ion
0 48 96 144 192 240 288 336Wks
AA genotype
AG/GG genotype
P = .018
10
8
6
4
2
0
HB
sA
g S
ero
cle
ara
nc
e
0 48 96 144 192 240 288 336Wks
AA genotype
AG/GG genotype
P = .042

Advanced Liver Disease

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Rifaximin for Maintenance of Remission From Overt HE
1. Bass NM, et al. N Engl J Med. 2010;362:1071-1081. 2. Mullen K, et al. EASL 2011. Abstract 109.
Patients with recurrent HE (≥ 2 overt episodes
within 6 mos of screening) and Conn
score 0 or 1, currently in remission
(N = 299)
Rifaximin 550 mg BID*(n = 140)
Placebo*(n = 159)
Mo 6
*Concomitant lactulose permitted. †≥ 2 overt HE episodes within 12 mo of screening and Conn score ≤ 2.
Randomized-controlled trial[1] Open-label maintenance[2]
n = 82†
n = 70†
n = 170 new pts†Rifaximin 550 mg BID*
(n = 322)

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Rifaximin for Maintenance of Remission From Overt HE Rifaximin provided long-term
protection from HE recurrence Reduced rate of hospitalizations
in the long term with rifaximin
1. Bass NM, et al. N Engl J Med. 2010;362:1071-1081. 2. Mullen K, et al. EASL 2011. Abstract 109.Graphics used with permission.
HE
Bre
ak
thro
ug
h E
ve
nts
/PE
Y
2
1
0
1.6
0.6*
0.4*
0.2*0.3*
Long-term open-label F/U
Rifaximin RCT (n = 140)Placebo crossover (n = 82)Continuing rifaximin (n = 70)New rifaximin (n = 252)
Exposure (PEY)Events/PEY
461.59
500.62
1340.40
1470.24
3420.30
*P < .0001 vs placebo.PEY, person exposure yrs.
*Includes 140 patients in rifaximin group from RCT, 82 patients from placebo group in RCT who switched to open-label rifaximin maintenance, and 170 patients who newly entered the study during the open-label maintenance phase.†P = .0051 vs placebo‡P < .001 vs placebo.
RCT All RifaximinPatients*(n = 392)
Rifaximin(n = 140)
Placebo(n = 159)
PEY 50 46 510
Hospitalizations due to HE
n (%) 15 (11) 33 (21) 109 (23)
Events/PEY
0.30† 0.72 0.21‡
Placebo RCT (n = 159)
Patients Treated With Rifaximin

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Impact of Adrenal Dysfunction in Cirrhotic Patients With Ascites Corticotropin stimulation test performed in a series of 85 consecutive
cirrhotic patients with ascites
– Adrenal dysfunction: change in cortisol < 9 µg/dL and/or peak cortisol < 18 µg/dL
– Patients followed until liver transplantation or death (median: 198 days)
39% had adrenal dysfunction
Survival significantly poorer in pts with adrenal dysfunction (P = .02)
Predictors of mortality (multivariate analysis)
– Adrenal dysfunction: HR: 2.1 (95% CI: 1.1-4.0; P = .03)
– PRA > 4 ng/mL/hr: HR: 2.1 (95% CI: 1.1-4.0; P = .03)
– MELD score > 18: HR: 2.0 (95% CI: 1.1-3.5; P = .02)
Elia C, et al. EASL 2011. Abstract 106.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Does Moderate Hypothermia Prevent Brain Edema in Acute Liver Failure?* Prospective, randomized, controlled, multicenter trial
Patients with acute liver failure and imminent brain edema and planned intracranial pressure monitoring
– Standard medical therapy: n = 33
– Median core temperature: 36.7°C
– Standard medical therapy + 3 days moderate hypothermia: n = 21
– Median core temperature: 33.2°C
Similar rates of intracranial hypertension: 57% with MH vs 45% for control (P = .58)
Similar rates of mortality: 48% with MH vs 58% for control (NS)
Larsen, et al. EASL 2011. Abstract 56.
*Slide content based only on abstract data.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Radioembolization With 90Y-Resin Microspheres for Unresectable HCC Multicenter patient series: 82% male, 79% cirrhotic, mean age: 64.5 yrs
HCC etiology: HBV (13%), HCV (44%)
Previous procedures: surgical (n = 61), percutaneous ablation (n = 29), intra-arterial (n = 98)
Median survival
– 1 yr: 52.8%
– 2 yrs: 28.1%
– 3 yrs: 15.9%
Median survival according to BCLC stage (P < .001)
– BCLC stage A (n = 52): 24.4 mos
– BCLC stage B (n = 87): 16.9 mos
– BCLC stage C (n = 183): 10.0 mos
– BCLC stage D (n = 3): 5.2 mos
Sangro B, et al. EASL 2011. Abstract 80.
clinicaloptions.com/hepatitisHighlights From Berlin 2011
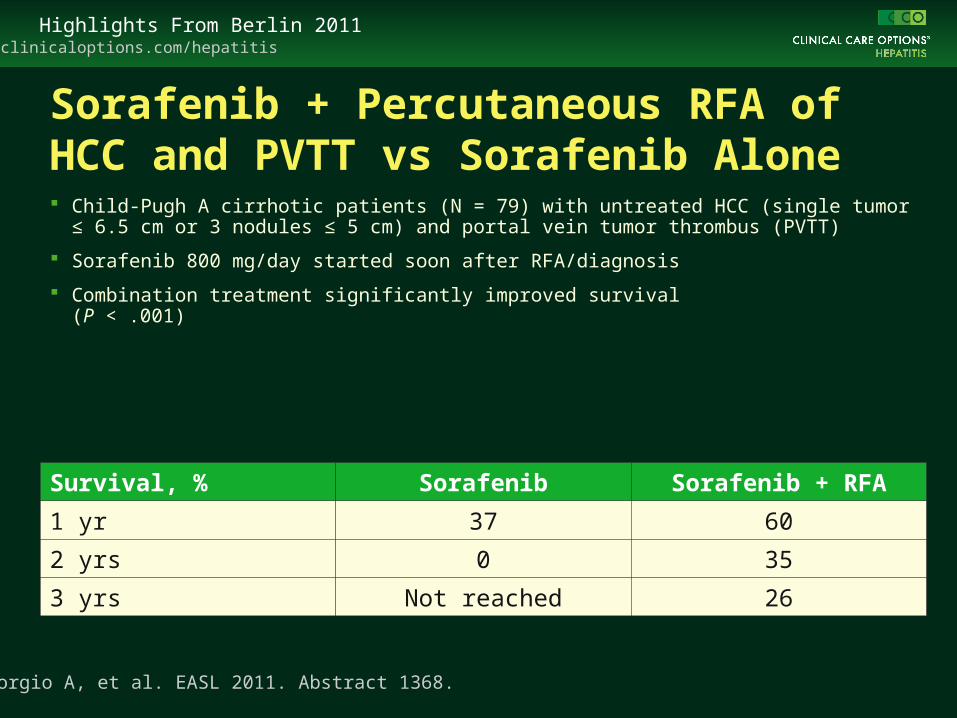
Sorafenib + Percutaneous RFA of HCC and PVTT vs Sorafenib Alone Child-Pugh A cirrhotic patients (N = 79) with untreated HCC (single tumor ≤ 6.5 cm or 3
nodules ≤ 5 cm) and portal vein tumor thrombus (PVTT)
Sorafenib 800 mg/day started soon after RFA/diagnosis
Combination treatment significantly improved survival (P < .001)
Giorgio A, et al. EASL 2011. Abstract 1368.
Survival, % Sorafenib Sorafenib + RFA
1 yr 37 60
2 yrs 0 35
3 yrs Not reached 26

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Resection of HCC Followed by Salvage Transplantation* 1998-2008: 114 transplantable patients with good liver function and
HCC within Milan criteria underwent resection
– Transplantation offered if recurrence of chronic liver disease
Recurrence occurred in 80% of resected cases
– Only 54% of patients went on to salvage transplantation
Risk factors for recurrence beyond Milan criteria (multivariate analysis)
– Poor differentiation, presence of vascular invasion, older than 60 yrs of age
Risk factors for missing opportunity of LT after recurrence (univariate analysis)
– Presence of F4, tumor size > 3 cm, R1 surgical margin
Fuks D, et al. EASL 2011. Abstract 57.
*Slide content based only on abstract data.

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Molecular Signature for Diagnosis, Prognosis of HCC* Whole-genome profiles of frozen samples analyzed (N = 110)
– HCC of various etiologies, HCA, FNH, cirrhosis, and normal liver tissues
– 96 genes analyzed as potential markers of
– Benign liver tumors according to their different pathologic and molecular subtypes, and
– HCC according to prognosis
5-gene predictor associated with overall survival in HCC
– HR: 2.6 (CI: 1.6-4.2; P < .001)
– More significantly associated with overall survival than previous G1-G6 or proliferative-transcriptomic classifications
Nault JC, et al. EASL 2011. Abstract 76.
*Slide content based only on abstract data.
clinicaloptions.com/hepatitisHighlights From Berlin 2011
IL28B as Predictor of Response to HCV Treatment in Recurrence After Transplant* Liver transplantation recipients with HCV recurrence who received ≥ 12 wks of
pegIFN/RBV (N = 132)
– IL28B SNPs rs8099917 and rs12979860 genotyped
– Recipients: peripheral lymphocytes or liver explants
– Donors: liver biopsies immediately after reperfusion of the graft
Patients with favorable donor and recipient IL28B genotypes had highest probability of SVR (79%; P = .001 vs other combinations)
Multivariate analysis: CC genotype of rs12979860 identified as baseline independent predictor of SVR (OR: 4.2; 95% CI: 1.4-12.3; P = .01)
SVR in 85% of recipients with CC genotype and HCV RNA < 6.5 log10 IU/mL vs 23% in patients with CT/TT genotype and HCV RNA > 6.5 log10 IU/mL (P < .001)
Crespo G, et al. EASL 2011. Abstract 30.
*Slide content based only on abstract data.
Nonviral Hepatitis
clinicaloptions.com/hepatitisHighlights From Berlin 2011
(N = 89)
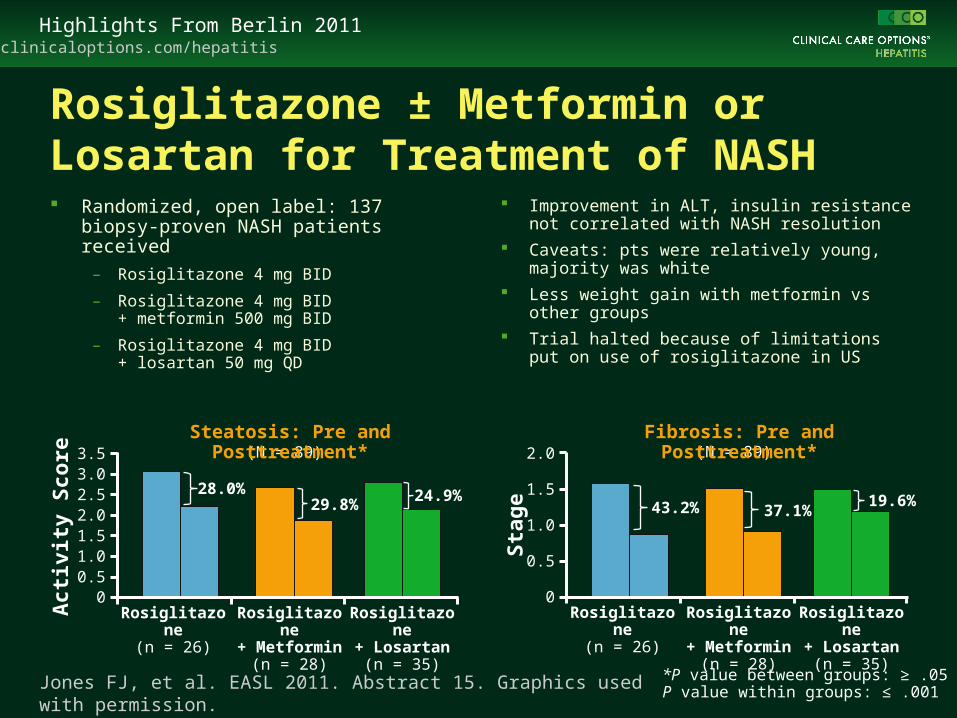
Rosiglitazone ± Metformin or Losartan for Treatment of NASH Randomized, open label: 137 biopsy-
proven NASH patients received
– Rosiglitazone 4 mg BID
– Rosiglitazone 4 mg BID + metformin 500 mg BID
– Rosiglitazone 4 mg BID + losartan 50 mg QD
Improvement in ALT, insulin resistance not correlated with NASH resolution
Caveats: pts were relatively young, majority was white
Less weight gain with metformin vs other groups
Trial halted because of limitations put on use of rosiglitazone in US
Jones FJ, et al. EASL 2011. Abstract 15. Graphics used with permission.
Steatosis: Pre and Posttreatment*
*P value between groups: ≥ .05P value within groups: ≤ .001
3.53.02.52.01.51.00.5
0Rosiglitazone
(n = 26)Rosiglitazone+ Metformin
(n = 28)
Rosiglitazone+ Losartan
(n = 35)
28.0%29.8%
24.9%
(N = 89)Fibrosis: Pre and Posttreatment*
2.0
1.5
1.0
0.5
0Rosiglitazone
(n = 26)Rosiglitazone+ Metformin
(n = 28)
Rosiglitazone+ Losartan
(n = 35)
43.2% 37.1%19.6%
Sta
ge
Act
ivit
y S
core

clinicaloptions.com/hepatitisHighlights From Berlin 2011
Mycophenolate Mofetil With Corticosteroids in Autoimmune Hepatitis Chart review: patients with AIH or AIH-overlap syndromes and past or
present use of MMF included (N = 661)
– Efficacy of MMF in pts with azathioprine nonresponse or intolerance
Pronk AMC, et al. EASL 2011. Abstract 23.
AIH Overlap syndrome
AZA Intolerant AZA NonrespondersOverall
Rem
issi
on
on
MM
F (
%)
100
80
60
40
20
0
47
67 63
13
57

Go Online for More CCO Coverage of EASL 2011!
Capsule Summaries of all the key data
Podium to Practice Expert Analysis panel discussion exploring the clinical implications of the most important data from the meeting
clinicaloptions.com/Berlin2011