clinical treatment protocols of breast cancer phl 417 dr. mohamed m. sayed-ahmed
TRANSCRIPT

CLINICAL TREATMENT PROTOCOLS OF
BREAST CANCER
PHL 417
Dr. Mohamed M. sayed-Ahmed

BREAST CANCER
Breast cancer (BC) is the most common cancer and one of the leading causes of cancer-related death worldwide. About 1.2 million women worldwide are diagnosed with breast cancer (BC) every year.
According to the most recent National Cancer Registry (NCR) in Saudi Arabia, BC is at the top and the most frequent tumour among all the malignancies seen in Saudi females, accounting 26 %.
In Saudi Arabia, BC that developed before the age 40 accounted for 28 % of all female breast cancers compared with only 6.5% in USA.
Considering the growth and aging of population in Saudi Arabia, future burden of BC in Saudi Arabia is expected to increase by approximately 350 % by the year 2025 which could demonstrate enormous demands on health care resources. For all these reasons, BC represents a local and complex health problem in kingdom of Saudi Arabia.

Factors That Increase Risk of Breast Cancer
•Family History
•Lifestyle
•Personal History

Family History
If your mother, sister, or daughter has developed breast cancer before menopause, you are three times more likely to develop the disease.
If two or more close relatives (e.g., cousins, aunts, grandmothers) have/had breast cancer, you are at increased risk as well.
Recently, scientists have found that mutations in genes BRCA1 and BRCA2 increase one's susceptibility to breast cancer. A simple blood test can tell you if you have such a condition.
Personal HistoryIf you've had breast cancer, you have an
increased risk of getting it again. Also, if you've had benign breast disease (e.g., fibrocystic breast disease), you are at an increased risk.
The following also put you at greater risk:
• If you began menstruating early (before age 12)
• If you take birth control pills (though evidence
is not conclusive)
Life Style
• Several studies found a lower incidence of breast cancer among women who exercise regularly.
• Higher proportion of breast cancer among obese women.
• There is increased risk of breast cancer with increased alcohol use (i.e., 3 or more drinks per week); perhaps due to the fact that alcohol increases blood estrogen levels.
Additional Risk Factors
• If you never have children
• If you have children when you are 30 or older
• If you have menopause at 55 or older
• If you take Hormone Replacement Therapy (HRT)
• Higher estrogen levels are strongly linked with susceptibility to breast cancer.

Trouble Signs That Should Not Be Ignored
1. Finding a lump, hard knot or thickening
2. Unusual swelling, warmth, redness or darkening
3. Change in size or shape of your breast
4. Finding an itchy, scaly sore or rash on the nipple
5. Pulling in of the nipple or other parts of the breast
6. Nipple discharge that starts suddenly
7. Pain in one spot that does not vary with cycle

BREAST CANCER arises in the milk-producing glands of the breast tissue. Ductal carcinoma begins in the ducts, and lobular carcinoma has a pattern involving the lobules or glands.
Risk factors for the development of breast cancer, includes:
• family history of breast cancer in mother or sister (families in which there is a high breast cancer frequency have mutations affecting the tumor suppressor genes BRCA-1 and BRCA-2.
• early onset of menstruation and late menopause
• reproductive history: women who had no children or have children after age 30 and women who have never breastfed have increased risk
• history of abnormal breast biopsies
• hormone replacement therapy (HRT) that provides significant relief of menopausal symptoms, prevention of osteoporosis, and possibly protection from cardiovascular disease and stroke
DIAGNOSIS OF BREAST CANCER A- When a patient has no signs or symptoms:
• Screening involves the evaluation of women who have no symptoms or signs of a breast problem
• 1- Breast self examinations: • It is recommended that women get into the habit of doing monthly breast
self examinations to detect any lump at an early stage.
• 2- Mammography:
• Mammography is the study of the breast using x ray. The actual test is called a mammogram. There are two types of mammograms.
• A- A screening mammogram is ordered for women who have no problems with their breasts. It consists of two x-ray views of each breast.
• B- A diagnostic mammogram is for evaluation of new abnormalities or of patients with a past abnormality requiring follow-up (i.e. a woman with breast cancer treated with lumpectomy). Additional x rays from other angles or special views of certain areas are taken.

A mammogram of a normal breast
A mammogram showing an abnormal growth. A biopsy is needed to confirm whether this is indeed cancer.
B- When a patient has physical signs or symptoms:
such as the presence of a lump within the breast. Skin dimpling, nipple retraction, or bloody nipple discharge.
• 1- BIOPSY: Depending on the situation, different types of biopsy may be performed. The types include incisional and excisional, (complete removal) biopsies. In an incisional biopsy, the physician takes a sample of tissue, and in excisional biopsy, the mass is removed.
• 2- FINE NEEDLE ASPIRATION BIOPSY: In a fine needle
aspiration biopsy, a fine-gauge needle may be passed into the lesion and cells from the area suctioned into the needle can be quickly prepared for microscopic evaluation (cytology).
• 3- CORE NEEDLE BIOPSY:
• 4- Computed tomography: (CT scan, CAT scans), and magnetic resonance imaging (MRI) have only a very occasional use in the evaluation of breast lesions.

CLINICAL STAGING OF BREAST CANCER
Stage 1: Tumour is 2 cm and no cancer cells are found in the lymph nodes.
Stage 2: Tumour is between 2 to 5 cm, and the cancer has spread to the lymph nodes
Stage 3A: Tumor is larger than 5 cm and has spread to the lymph nodes, which have grown into each other.
Stage 3B: Tumour has spread to tissues near the breast, (local invasion), or to lymph nodes inside the chest wall, along the breastbone.
Stage 4: Tumour has spread to skin and lymph nodes beyond the axilla or to other organs of the body.
TREATMENT PROTOCOLS OF BREAST CANCER
Types of Treatment: Local and Systemic
Local Treatment: SurgeryRadiation Therapy
Systemic Treatment:Chemotherapy
Hormone TherapyBiological Therapy
CLINICAL TREATMENT PROTOCOLS OF BREAST CANCER
SURGERY
• Radical Mastectomy: surgical removal of the entire breast and axillary contents along with the muscles down to the chest wall.
• Modified Radical Mastectomy: Surgical removal of the entire breast and axillary contents, but the muscles of the chest wall are not.
• Lumpectomy: If the tumor is less than 4 cm (1.5 in) in size and located so that it can be removed without destroying a reasonable cosmetic appearance of the residual breast, just the primary tumor and a rim of normal tissue will be removed.

RADIOTHERAPY
• Like surgical therapy, radiation therapy is a local modality—it treats the tissue exposed to it and not the rest of the body. Radiation is usually given post-operatively after surgical wounds have healed. The pathologic stage of the primary tumor is now known and this aids in treatment planning.
Side effects of radiation therapy:
1- reddening of the skin 2- muscle stiffness 3- mild swelling 4- tenderness in the area 5- long term shrinking of the irradiated breast

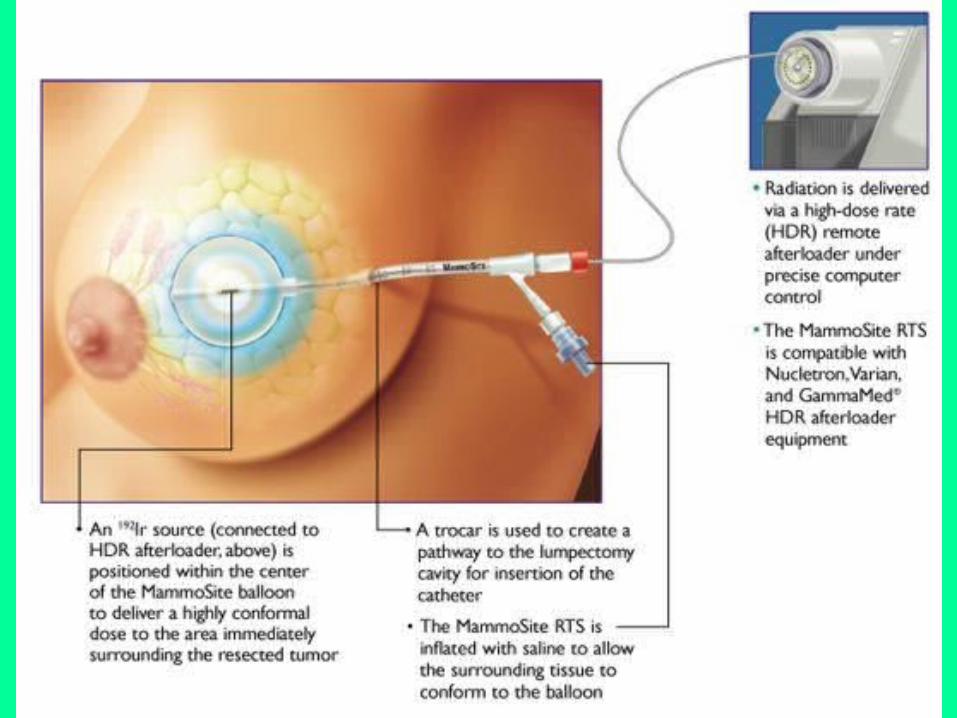
MammoSite 5-Day Targeted Radiation Therapy
• MammoSite Targeted Radiation Therapy works from the inside, meaning that a higher daily dose can be used for a shorter period of time – 5 days vs. 5-7 weeks for traditional external beam radiation therapy.
* The MammoSite® Radiation Therapy System received FDA clearance in 2002.

Advantages of MammoSite:1- Treatment with MammoSite 5-Day Targeted Radiation Therapy can help you get back to your normal life sooner – just 5 days vs. 5-7 weeks for traditional external beam radiation therapy.
2- MammoSite places the radiation source inside the lumpectomy cavity (the space left when a tumor is removed). This delivers radiation to the area where cancer is most likely to recur.
3- This therapy is given on an outpatient basis and No hospital stay is required.
MammoSite 5-Day Targeted Radiation Therapy
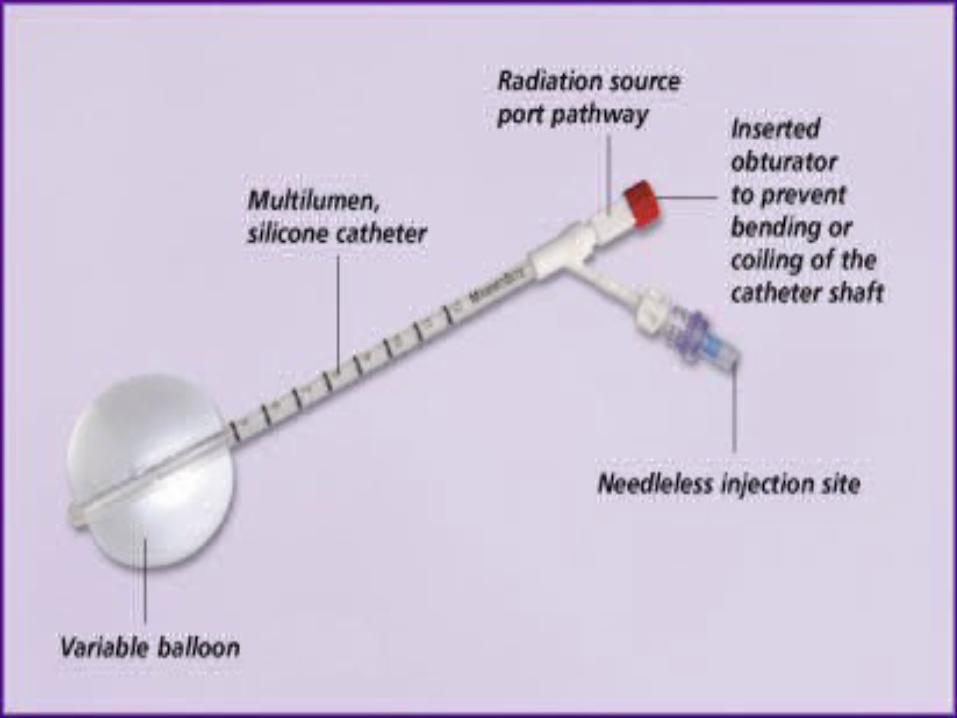

Balloon and lumpectomy

Chemotherapy
CMF
cyclophosphamide 600 mg/m2 PO d1-14
Methotrexate (MTX) 40 mg/m2 IV d1+8
5-Fluorouracil (5-FU) 600 mg/m2 IV d1+8
To be repeated every 4 weeks for 6 cycles
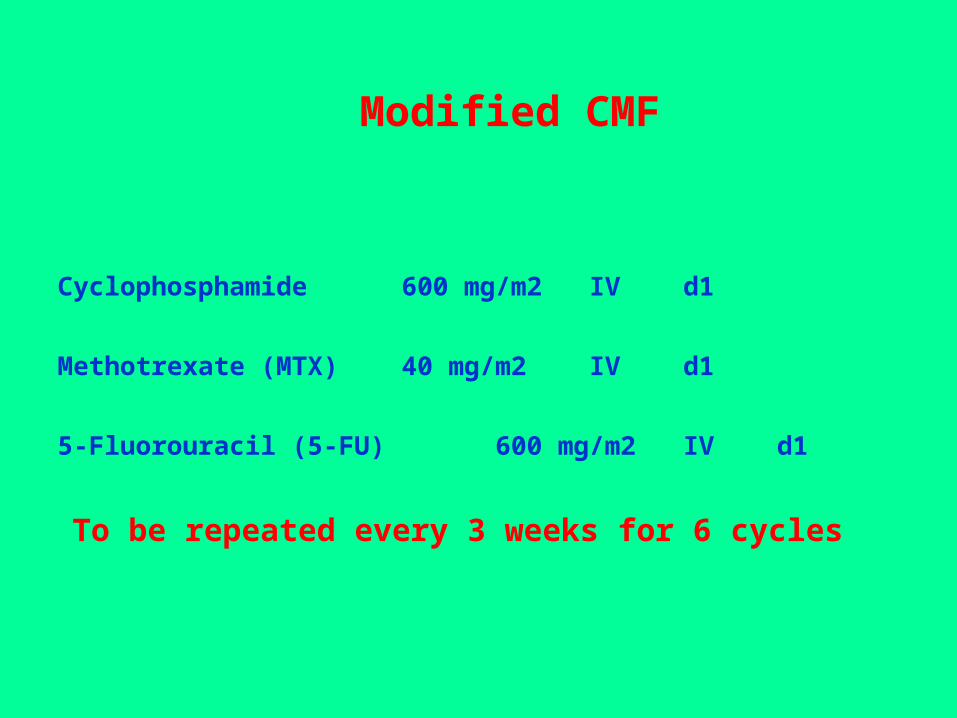
Modified CMF
Cyclophosphamide 600 mg/m2 IV d1
Methotrexate (MTX) 40 mg/m2 IV d1
5-Fluorouracil (5-FU) 600 mg/m2 IVd1
To be repeated every 3 weeks for 6 cycles

CAF
Cyclophosphamide 600 mg/m2 IV d1
Doxorubicin 60 mg/m2 IV d1
5-Fluorouracil (5-FU) 600 mg/m2 IVd1+8
To be repeated every 4 weeks ( 4 cycles adjuvant)

AC
Doxorubicin 60 mg/m2 IV d1
cyclophosphamide 600 mg/m2 IV d1+8
to be repeated every 3 weeks (4 cycles)
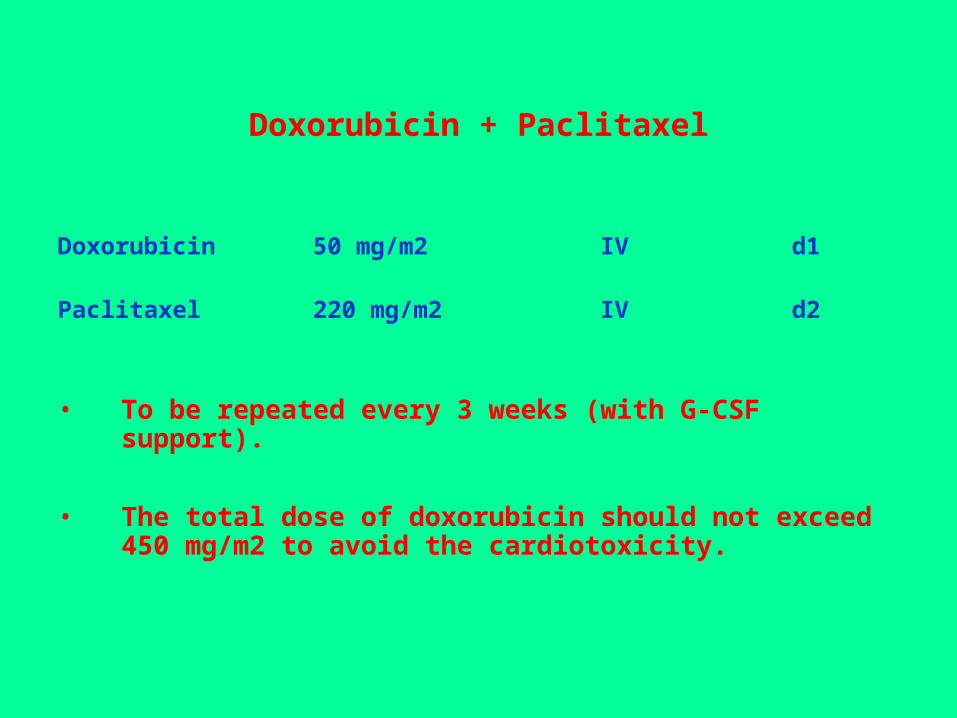
Doxorubicin + Paclitaxel
Doxorubicin 50 mg/m2 IV d1
Paclitaxel 220 mg/m2 IV d2
• To be repeated every 3 weeks (with G-CSF support).
• The total dose of doxorubicin should not exceed 450 mg/m2 to avoid the cardiotoxicity.

Modified AC: AC followed by Paclitaxel
Doxorubicin 60 mg/m2 IV d1
cyclophosphamide 600 mg/m2 IV d1+8
• to be repeated every 3 weeks (4 cycles), then
• Paclitaxel 175 mg/m2 IV(3h inf)d1

CEF
Cyclophosphamide 100 mg/m2 PO d1-14
Epirubicin 60 mg/m2 IV d1+8
5-Fluorouracil (5-FU) 500 mg/m2 IVd1+8
• To be repeated every 4 weeks for 6 cycles
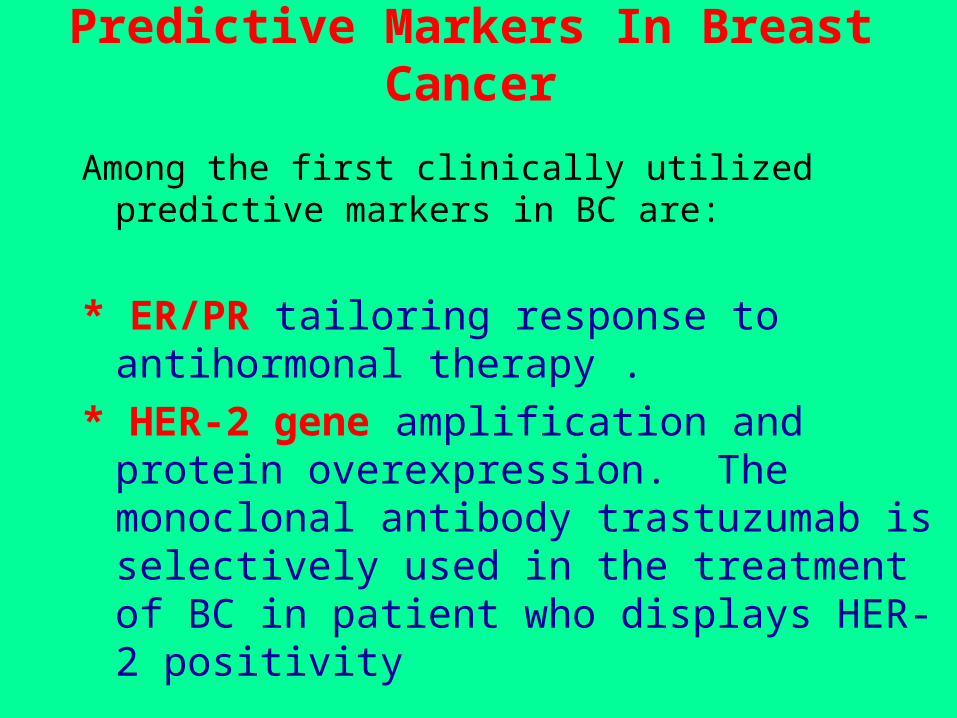
Predictive Markers In Breast Cancer
Among the first clinically utilized predictive markers in BC are:
* ER/PR tailoring response to antihormonal therapy .
* HER-2 gene amplification and protein overexpression. The monoclonal antibody trastuzumab is selectively used in the treatment of BC in patient who displays HER-2 positivity

Hormonal Therapy of Breast Cancer
• Patients with estrogen receptor positive tumors will typically receive a hormonal treatment after chemotherapy is completed. Typical hormonal treatments include:
A- ANTI-ESTROGEN
• It has been documented that one-third of all breast carcinomas are ESTROGEN-DEPENDENT and will regress after ESTROGEN DEPRIVATION. Thus reducing the level of estrogen remains a valuable target for treatment of breast carcinoma in both premenopausal and postmenopausal women. Reducing the effect of estrogen can be mediated by:
1- Agents that block Estrogen at receptor level: TAMOXIFEN
2- Agents that inhibit estrogen biosynthesis: AROMATASE INHIBITORS.
1- TAMOXIFEN (Nolvadex): (20 mg/d , PO, 5 years)
• As adjuvant therapy for patient with estrogen receptor positive irrespective of age and nodal status. As palliative therapy for postmenopausal patients with estrogen receptor positive advanced/metastatic tumours. Also, for the prevention of breast cancer in high risk women.
• TAMOXIFEN is an antineoplastic nonsteroidal selective estrogen receptor modulator (SERM). Tamoxifen competitively inhibits the binding of estradiol to estrogen receptors, thereby preventing the receptor from binding to the estrogen-response element on DNA. The result is a reduction in DNA synthesis and cellular response to estrogen. In addition, tamoxifen up-regulates the production of transforming growth factor B (TGFb), a factor that inhibits tumor cell growth, and down-regulates insulin-like growth factor 1 (IGF-1), a factor that stimulates breast cancer cell growth.

2 -AROMATASE INHIBITORS
• Aromatase inhibitors (AIs) act through
inhibition of the cytochrome P450,
AROMATASE, which catalyses the
conversion of androgen substrates to
estrogen, which are the main source of
estrogen in postmenopausal women.

1- ANASTROZOLE (Arimidex)
• A nonsteroidal inhibitor of estrogen synthesis that resembles paclitaxel in chemical structure.
• As a third-generation aromatase inhibitor, anastrozole selectively binds to and reversibly inhibits aromatase, a cytochrome P-450 enzyme complex found in many tissues including those of the premenopausal ovary, liver, and breast; aromatase catalyzes the aromatization of androstenedione and testosterone into estrone and estradiol, the final step in estrogen biosynthesis. In estrogen-dependent breast cancers, anastrozole may inhibit tumor growth.
2- LETROZOLE (Femara)
• A nonsteroidal inhibitor of estrogen synthesis that resembles paclitaxel in chemical structure.
• As a third-generation aromatase inhibitor, letrozole selectively and reversibly inhibits aromatase, a cytochrome P-450 enzyme complex found in many tissues including those of the premenopausal ovary, liver, and breast.
• Aromatase catalyzes the aromatization of androstenedione and testosterone into estrone and estradiol, the final step in estrogen biosynthesis.
• In estrogen-dependent breast cancers, anastrozole may inhibit tumor growth.
3- Exemestane (Aromasin)
• A synthetic androgen analogue. Exemestane binds irreversibly to
and inhibits the enzyme aromatase, thereby blocking the conversion
of cholesterol to pregnenolone and the peripheral aromatization of
androgenic precursors into estrogens.

CLINICAL PHARMACOLOGY OF THE NEW GENERATION OF AROMATASE INHIBITORS
CharacteristicsAnastrozole(Arimidex)
Letrozole(Femara)
Exemestane(Aromasin)
NatureNon-steroidalNon-steroidalsteroidal
Class of AIsType II, reversibleType II, reversibleType I, irreversible
Daily clinical dose
(mg/day)
12.525
Total monthly dose
(mg)
3075750
Time to steady-state
plasma levels (days)
7607
Half-life (hrs)417227
Time to maximal
Estradiol suppression
(days)
3-42-37
Intratumoural activity
reported
YESYESYES
FDA approvalYESYESYES
•B- Lutenizing hormone-releasing hormone (LHRH) agonists:
1- Leuprolide acetate
2 -Goserelin

Immunotherapy
TRASTUZUMAB (Herceptin)
TRASTUZUMAB is a recombinant humanized monoclonal
antibody directed against the human epidermal growth factor
receptor 2 (HER2).
After binding to HER2 on the tumor cell surface, trastuzumab induces an antibody-dependent cell-mediated cytotoxicity (ADCC) against tumor cells that overexpress HER2.
HER2 is overexpressed by many adenocarcinomas, particularly breast adenocarcinomas

• This therapy requires the obligation of HER-2 tumour typing following any surgical intervention of an invasive breast cancer.
• Trastuzumab must only be administered to female HER-2-positive patients, i.e., in whom the tumours overexpress the HER-2 protein or amplify the HER-2 gene.
• Monitoring of HER-2 in tumours is essential:
• The overexpression of HER-2 must be searched for using immunohistochemisty (IHC) in embedded tumour fragments, or using genic amplification in situ hybridisation (FISH1 or CISH2 technique).

Triple Negative Breast Cancer
* TNBC is a subtype of BC that lacks the expression of:
- Estrogen receptor (ER)
- Progesterone receptor (PR)
- Human epidermal growth factor receptor (HER-2).
* This uncommon subtype approximately representing 15 % of all BC cases with poor prognosis despite responding to conventional chemotherapy regimens

Characteristics of TNBC
1- Aggressive and early patterns of metastases.
2- Unique molecular characteristics.
3- BRCA-1 and BRCA-2 mutations.
4- Poor prognosis.
5- lack of targeted therapeutics.

Obstacles in Treatment of TNBC
1- ER and HER-2 are not expressed in TNBC.
2- As a result, therapies that decrease estrogen synthesis or block ER or HER-2 including aromatase inhibitors, estrogen receptor blockers, and trastuzumab are ineffective in its treatment.

* Poly (ADP-ribose) polymerase-1 (PARP-1), a nuclear enzyme, plays an important role in the repair of single-strand DNA breaks via the base excision repair pathway.
* PARP-1 represents an important novel target in cancer therapy.
Poly(ADP-ribose) polymerase (PARP-1) and TNBC

Earlier and recent studies confirmed that loss of BRCA-dependent DNA repair mechanisms combined with the PARP inhibitor, olaparib is associated with synthetic lethality and augmented cell death.
Preliminary results of a recent randomized phase II trial of chemotherapy (carboplatin plus gemcitabine) combined with the PARP inhibitor, in metastatic TNBC, showed significantly improved clinical benefit rate, progression free survival and overall survival compared with carboplatin plus gemcitabine alone.
PARP-1 Inhibitors and TNBC
Data from phase II study with the PARP inhibitor, olaparib, as a single agent to treat sporadic TNBC showed a limited and unimpressive result which further supports the use of combination PARP inhibitor plus chemotherapy in the treatment of patients with sporadic TNBC.
Results from a randomized, double-blind, multicenter study which investigated the efficacy of olaparib in combination with paclitaxel in the first or second line treatment of metastatic TNBC, yielded notable toxicity patterns in the form of grade 2 to 4 neutropenia which required dose modifications for both olaparib and paclitaxel.
PARP-1 Inhibitors and TNBC

In 2012, Patel et al., compared the actions of the PARP inhibitor, iniparib, with the more extensively characterized PARP inhibitors, olaparib and veliparib, and reported that iniparib failed to sensitize cells to cisplatin, gemcitabine, or paclitaxel and its effects are unlikely to reflect PARP inhibition and should not be used to guide decisions about other PARP inhibitors.
PARP-1 Inhibitors and TNBC