clinical research slipped capital femoral epiphysis with ... · endokrin berupa tumor kelenjar...
TRANSCRIPT

28The Journal of Indonesian Orthopaedic & Traumatology, Volume 1, Number 2, August 2018
ABSTRACT
Introduction: Slipped Capital Femoral Epiphysis (SCFE) is well associated with an underlying endocrine pathology. The clinical implication is multiplied: avoiding anesthesia complication in SCFE surgical treatment, assessing the need of prophylactic pinning at contralateral hip, and early detection of underlying disease. This case report will discuss the lessons learned from the management of endocrine-related SCFE with coexisting pituitary tumor, along with the long-term clinical outcome.
Methods: A 17-year-old male was diagnosed with unstable SCFE and underwent in situ pinning of the femoral head using 3 cannulated screws.
Results: Hormonal examination showed hypogonadism, hyperprolactinemia, and growth hormone deficiency. Brain scan displayed macroadenoma of pituitary gland. Five years later, the patient reported overall satisfaction of the treatment.
Conclusion: Clinical manifestation of delayed sexual maturation was the result of deficiency of the sex hormones and also related to the pathogenesis of SCFE. It is recommended to screen for endocrine disorders in SCFEs patients.
ABSTRAK
Pendahuluan: SCFE sangat erat kaitannya dengan kelainan endokrin. Perhatian klinisi pada kasus SCFE menjadi beberapa kali lipat karena perlu diperhatikan komplikasi anestesi intraoperatif, kebutuhan pinning profilaksis pada panggul kontralateral, dan deteksi dini kelainan. Laporan kasus ini akan membahas mengenai SCFE dengan kelainan endokrin berupa tumor kelenjar pituitary lengkap dengan follow up nya.
Metode: Seorang pria berusia 17 tahun yang didiagnosis SCFE tidak stabil telah menjalani prosedur in situ pinning kaput femoral menggunakan 3 buah cannulated screw.
Hasil: Pemeriksaan hormonal menunjukkan hipogonadisme, hiperprolaktinemia, dan kekurangan hormon pertumbuhan. Brain scan menunjukkan makro adenoma kelenjar pituitari. Lima tahun kemudian, pasien menyampaikan kepuasan terhadap prosedur yang telah dijalaninya.
Kesimpulan: Manifestasi klinis maturasi seksual yang terlambat adalah hasil dari defisiensj kelenjar hormon dan juga berkaitan dengan patogenesis SCFE. Disarankan melakukan pemeriksaan hormonal pada pasien SCFE
Slipped capital femoral epiphysis with coexisting pituitary tumor
Ifran Saleh,1,2 Andika Dwiputra Djaja,2 Elizabeth Yohmi,3 Maria Florencia Deslivia1
1 Department of Orthopaedic Surgery, St. Carolus Hospital, Jakarta2 Department of Orthopaedic and Traumatology, Dr. Cipto Mangunkusumo General Hospital - Faculty of Medicine Universitas
Indonesia, Jakarta3 Department of Pediatric, St. Carolus Hospital, Jakarta
Keywords: Slipped Capital Femoral Epiphysis, endocrine dysfunctions, management
Corresponding author : Andika Dwiputra Djaja, MD. [email protected]
Clinical Research

29Slipped capital femoral epiphysis with coexisting pituitary tumor
INTRODUCTION
Slipped capital femoral epiphysis (SCFE) is a common musculoskeletal problem in adolescents with reported incidence of 0,2-17,5 per 100,000 population.1,2 Even though the etiology remains to be elusive; it is well associated with an underlying endocrine pathology. Therefore, the highest incidence was found in obese adolescent male, followed by unusually tall and thin adolescent.3 Recognizing the relationship between SCFE and endocrinopathy is crucial to avoid the mistake of ignoring possible coexisting endocrine conditions in the SCFE patients and to devise the best treatment plan.
In principle, the treatment of SCFE involves surgical stabilization of the proximal femoral epiphysis. The overall complication rate is relatively high, alerting a meticulous clinical consideration upon recommending operative treatment. The complications after SCFE treatment include osteonecrosis of femoral head, chondrolysis, SCFE-induced impingement with associated articular cartilage damage and labral injury, fixation failure and deformity progression, growth arrest, and development of bilateral disease.4,5 On the other hand, the prevalence of bilaterality in proven endocrine-related SCFE varied from 70% to 100% 6,7, supporting the idea of prophylactic pinning on the contralateral hip. Therefore, the cost and benefit of performing prophylactic pinning for endocrine-related SCFE need to be assessed carefully.
Many researches related to SCFE and the underlying endocrine pathology. However, research is lacking in hormonal studies for SCFE patients and the possible complications of the SCFE surgery. We presented this case report to review the hormonal studies, complications and the follow up after the treatment.
In 2013, an adolescent male presented to our hospital with SCFE, he underwent in situ fixation, and was subsequently found to have concurrent brain tumor resulting in hormonal imbalance. The existence of endocrine disorder in relation to SCFE alerts special consideration. This case report will discuss the lessons learned from the management of this patient, along with the long-term clinical outcome.
Case Report
We reported a 17-year-old male patient reported pain
Figure 1. Red-circled structure is the separated part of epiphyseal plate of the right femoral head.
Figure 2. 3D reconstruction of CT images confirmed the existence of SCFE.
radiating from the right hip to the knee in the past 1 month. The pain worsened in the last 2 weeks. At the time of presentation, the patient was unable to walk. Passive flexion on the right hip resulted in external rotation
30
of the thigh. The patient’s height was 173 centimeter and weighed 69 kilograms (BMI = 23.05 kg/m2). MRI imaging displayed distraction of epiphyseal plate of the right femoral head, indicating fissure fracture (Figure 1). MSCT Scan confirmed the appearance of slipped epiphyseal plate of the right femoral head (Figure 2).
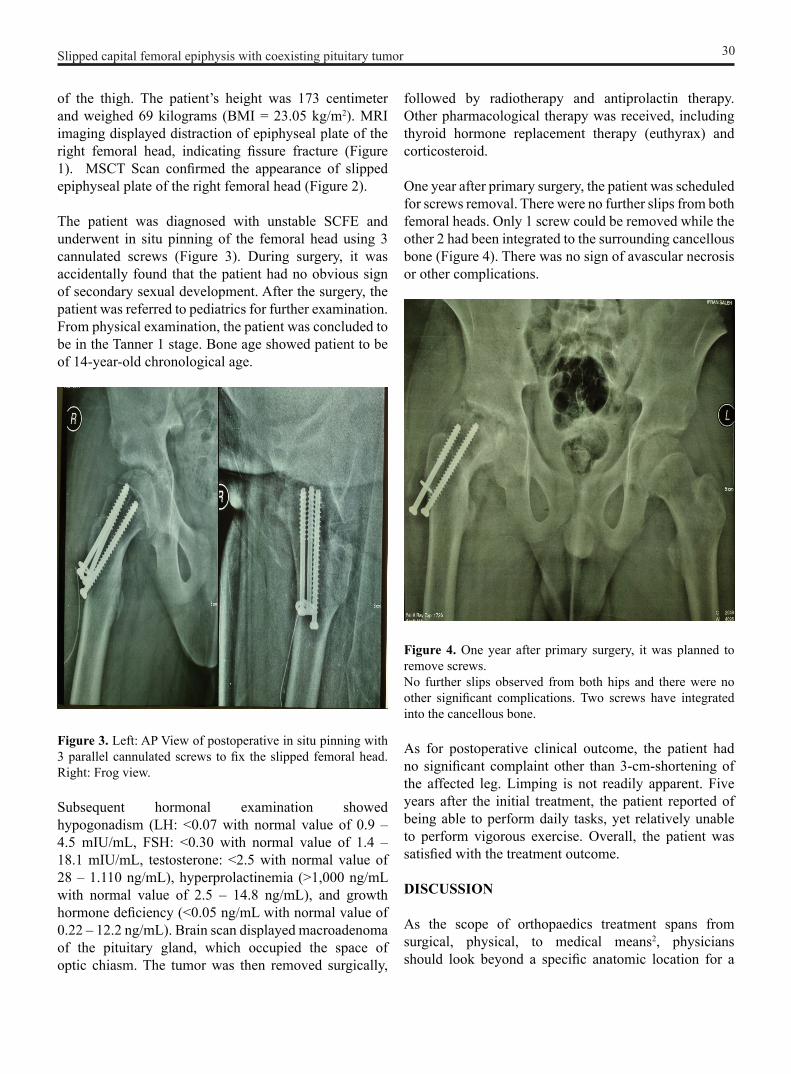
The patient was diagnosed with unstable SCFE and underwent in situ pinning of the femoral head using 3 cannulated screws (Figure 3). During surgery, it was accidentally found that the patient had no obvious sign of secondary sexual development. After the surgery, the patient was referred to pediatrics for further examination. From physical examination, the patient was concluded to be in the Tanner 1 stage. Bone age showed patient to be of 14-year-old chronological age.
Figure 3. Left: AP View of postoperative in situ pinning with 3 parallel cannulated screws to fix the slipped femoral head. Right: Frog view.
Subsequent hormonal examination showed hypogonadism (LH: <0.07 with normal value of 0.9 – 4.5 mIU/mL, FSH: <0.30 with normal value of 1.4 – 18.1 mIU/mL, testosterone: <2.5 with normal value of 28 – 1.110 ng/mL), hyperprolactinemia (>1,000 ng/mL with normal value of 2.5 – 14.8 ng/mL), and growth hormone deficiency (<0.05 ng/mL with normal value of 0.22 – 12.2 ng/mL). Brain scan displayed macroadenoma of the pituitary gland, which occupied the space of optic chiasm. The tumor was then removed surgically,
followed by radiotherapy and antiprolactin therapy. Other pharmacological therapy was received, including thyroid hormone replacement therapy (euthyrax) and corticosteroid.
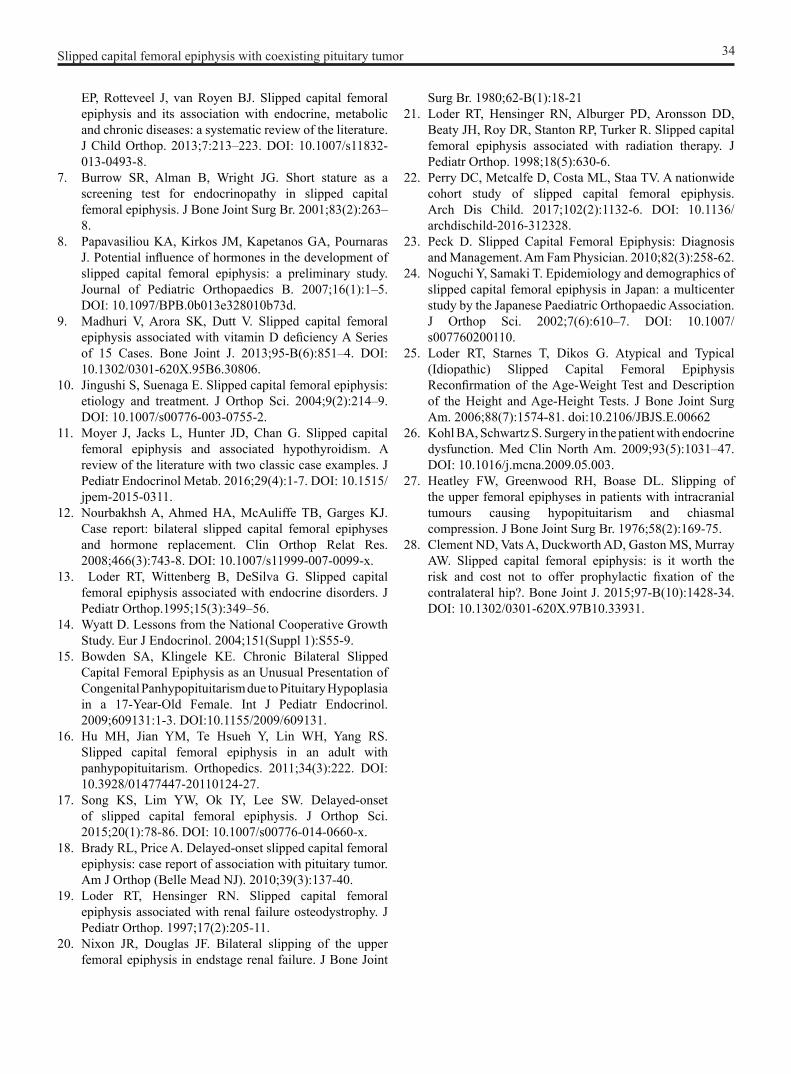
One year after primary surgery, the patient was scheduled for screws removal. There were no further slips from both femoral heads. Only 1 screw could be removed while the other 2 had been integrated to the surrounding cancellous bone (Figure 4). There was no sign of avascular necrosis or other complications.
Figure 4. One year after primary surgery, it was planned to remove screws. No further slips observed from both hips and there were no other significant complications. Two screws have integrated into the cancellous bone.
As for postoperative clinical outcome, the patient had no significant complaint other than 3-cm-shortening of the affected leg. Limping is not readily apparent. Five years after the initial treatment, the patient reported of being able to perform daily tasks, yet relatively unable to perform vigorous exercise. Overall, the patient was satisfied with the treatment outcome.
DISCUSSION
As the scope of orthopaedics treatment spans from surgical, physical, to medical means2, physicians should look beyond a specific anatomic location for a
Slipped capital femoral epiphysis with coexisting pituitary tumor

31
systemic underlying pathology. The SCFE case reported herein illustrated the importance of such observation in improving a patient’s quality of life. The patient was initially admitted for a pathognomonic sign of common adolescent hip condition, and later endocrine pathology rooting from an intracranial tumor was discovered and treated. Is it necessary to screen for endocrine abnormalities in SCFE patients? Can it be performed in a cost-effective manner?
Endocrine dysfunctions that were found to be associated with SCFE included, but not limited to, disorders in abnormalities in testosterone or estrogen levels8, 1,25-dihidroxyvitamin D9,10, hypothyroidism11,12, growth hormone deficiency13, growth hormone treatment8,14, panhypopituitarism and hypogonadism 15,16, pituitary gigantism17, and pituitary tumor18. Enormous endocrine changes also happen during puberty. Puberty reactivates gonadal axis, resulting in increment of levels of sex hormones. These hormones exert direct growth-stimulating effect on physis and indirect effect through growth hormone secretion from the pituitary gland6.
Clinical manifestation of delayed sexual maturation was the result of deficiency of the sex hormones, which,
in this patient, first triggered the cascade of hormonal investigations and the later finding of pituitary tumor.
Detecting endocrine disorders in SCFE
SCFE can be divided by its etiology: idiopathic and atypical, with the latter one associated with renal failure19,20, radiotherapy effects21,22, and endocrine disorders8,11-17. The difference between these 2 types of SCFE is important. The main concern is the underlying medical problems, which might complicate the process of anesthesia, and for deciding the need to perform prophylactic fixation on the contralateral hip.
Until now, there is no clear clinical practice guideline on purposefully investigating coexisting endocrine abnormalities in SCFE patients. The general consensus is that routine hormonal examination is not indicated in SCFE patients without any clinical evidence23. A number of studies reported that the proportion of SCFE patients with significant endocrine disorders is so minuscule that it does not require hormonal screening in all patients6,24,25.
The practice is considered as not cost-effective and thus, unfavorable in the era of Universal Health Coverage.
Reference Examination Definition RecommendationBurrow SR, et al (2001) [7] Height test Positive for endocrine-type
SCFE if the child’s height is
If positive, screen for a possible endocrine abnor-mality using measurement of thyroid-stimulating hor-mone and free thyroxine as a preliminary screen-ing test
≤10th percentile and nega-tive if >10th percentile of age.
Loder RT, et al (2006) [25] Age-weight test A patient of the same age is 8.4 times more likely to have an atypical slip if they are less than the 50th per-centile of weight.
NA
Current case (2018) Sexual maturation signs Lack of age-appropriate secondary sexual charac-teristics in patients with SCFE.
If positive, this should alert physicians to screen for specific hormones in-volved in gonadal axis.
Table 1. Summary of targeted examinations, which can be performed based on clinical markers alone, thus ensuring cost-effec-tiveness.
Slipped capital femoral epiphysis with coexisting pituitary tumor

32
On the other hand, previous literatures reported decreased T3, GH, FSH, LH, and testosterone8 among SCFE patients. In our case, the possibility of missing hypogonadism, and hence the pituitary tumor, would be catastrophic. It would delay the necessary treatment on the enlarging mass. Thus, what is the best practice recommended to detect any coexisting endocrine disorders, while remaining to be cost-effective? In SCFE cases, a targeted history-taking, and physical examination should be considered for early screening. Burrow et al7 found that short stature (below the tenth percentile of height) had a high sensitivity in detecting an underlying
endocrinopathy, thus the formulation is of age-height test. Another possible screening method is age-weight test, even though it has lower positive predictive value compared to age-height test.25 Hypothyroidism is known to be the most common endocrinopathy associated with SCFE, accounting for 95% of all cases,26 with short stature as one of the most obvious clinical signs. As for hypogonadism, screening of sexual maturation signs according to age could be a cost-effective early screening tool. Summary of targeted examination to screen for endocrine-related SCFEs is displayed in Table 1.
Slipped Capital Femoral Epiphysis
History of renal disease [19,20]
History of radiotherapy [21,22]
Rule out renal disease as etiology
Rule out side effect of radiotherapy as etiology
Yes
Yes
No
No
History of delayed sexual maturation [6] Yes
Confirmation of delayed sexual maturation with physical
examination
No
Height test ≤10th percentile [7,25]
Screen for hormones involved in gonadal axis [15,16]
Yes
Yes Screen for TSH and free thyroxine [26]
No
Idiopathic etiology
Slipped capital femoral epiphysis with coexisting pituitary tumor
Figure 5. Systematic investigation of atypical SCFE consists of focused history-taking and physical examination.

Based on literature review, we also proposed an algorithm (Figure 5) to exclude atypical SCFE through cost-efficient procedure. Considering the grave consequences of ignoring a possibly serious comorbidity in SCFE patients, adhering to a systematic investigation starting with history-taking and focused physical examination is beneficial to both patients and physicians. Focused physical examination here includes the examination of sexual maturation signs to exclude disorders in gonadal axis, and height test based on previous evidence.7 The algorithm was designed so as not to miss any possible disorders before concluding that the etiology of SCFE is idiopathic. It also factors in the possibility of more than one etiology in one single patient. Only when it is truly necessary, a costlier investigative effort, such as laboratory examination, is advised. Prospective studies should be conducted in the future to validate this recommendation.
Systematic investigation of atypical SCFE consists of focused history-taking and physical examination. The algorithm considers the possibility of one patient having more than one comorbidities. More costly procedures such as laboratory examination (blue boxes) are only performed based on sufficient evidence. The objective is to detect any possible comorbidity in SCFE case without carelessly resorting to unnecessary diagnostic tests and to advise best treatment plan for patient (e.g. anesthesia options, prophylactic pinning on contralateral hip, etc)The patient for our study was diagnosed with unstable SCFE and underwent in situ pinning of the femoral head using 3 cannulated screws, the patient also did not exhibit any abnormalities in the contralateral hip. The bone age at that time was according to a 12-year-old and the patient was supported by a complete hormonal therapy. During surgery, it was accidentally found that the patient had no obvious sign of secondary sexual development. After surgery, the patient was referred to pediatrics for further examination. From physical examination, the patient was concluded to be in the Tanner 1 stage. Bone age showed patient to be of 14-year-old chronological age. The screws removal was scheduled one year after the primary surgery. There were no further slips from both femoral heads. Only 1 screw could be removed while the other 2 had been integrated with the surrounding cancellous bone. Avascular necrosis or other complication for this patient was not presented. As for postoperative clinical outcome, the patient reported that there was no significant complaint other than 3-cm-shortening of the affected leg. Limping is not readily apparent. Five years after
the initial treatment, the patient reported of being able to perform daily tasks, yet relatively unable to perform vigorous exercise.
Clement ND (2015) recommended prophylactic pinning as a cost-effective procedure as it limits complications of further slip and poor functional outcome.28 However, that study was performed in subjects with a mean age of 12.3 years.28 In our case, the patient was 17-year-old, about the age of adulthood. The patient’s good compliance allowed for a regular follow-up, so we recommended only close observation. When sequential SCFE can be detected and treated early, close follow-up and not prophylactic pinning are supported by literature.29
When patients come with SCFEs, it is recommended to screen for endocrine disorders, as it will influence the surgery and to rule out other possible existing illness. In order to be cost-effective, it is recommended to perform targeted history-taking and physical examination. Prior evidence supports the examination for height, weight, and sexual maturation signs.
Acknowledgement
We would like to thank the patient who provided the informed consent for participation and publication, including the use of accompanying images. The authors declare that they have no conflicts of interest.
REFERENCES
1. Lehmann CL, Arons RR, Loder RT, Vitale MG. The epidemiology of slipped capital femoral epiphysis: an update. J Pediatr Orthop. 2006;26(3):286–90. DOI: 10.1097/01.bpo.0000217718.10728.70.
2. Loder RT, Skopelja EN. The Epidemiology and Demographics of Slipped Capital Femoral Epiphysis. ISRN Orthop. 2011;486512. DOI: 10.5402/2011/486512.
3. Salter RB. Disorders of Epiphyses and Epiphyseal Growth. Textbook of Disorders and Injuries of the Musculoskeletal System. 3rd Ed. 1999. Pennsylvania: Lippincott Williams & Wilkin.
4. Bitersohl B, Hosalkar HS, Zilkens C, Krauspe R. Current concepts in management of slipped capital femoral epiphysis. Hip International. 2015;25(2):104-14. DOI: 10.5301/hipint.5000189.
5. Roaten J, Spence DD. Complications related to the treatment of slipped capital femoral epiphysis. Orthop Clin North Am. 2016;47(2):405-13. DOI: 10.1016/j.ocl.2015.09.013.
6. Witbreuk M, van Kemenade FJ, van der Sluijs JA, Jansma
33Slipped capital femoral epiphysis with coexisting pituitary tumor
EP, Rotteveel J, van Royen BJ. Slipped capital femoral epiphysis and its association with endocrine, metabolic and chronic diseases: a systematic review of the literature. J Child Orthop. 2013;7:213–223. DOI: 10.1007/s11832-013-0493-8.
7. Burrow SR, Alman B, Wright JG. Short stature as a screening test for endocrinopathy in slipped capital femoral epiphysis. J Bone Joint Surg Br. 2001;83(2):263–8.
8. Papavasiliou KA, Kirkos JM, Kapetanos GA, Pournaras J. Potential influence of hormones in the development of slipped capital femoral epiphysis: a preliminary study. Journal of Pediatric Orthopaedics B. 2007;16(1):1–5. DOI: 10.1097/BPB.0b013e328010b73d.
9. Madhuri V, Arora SK, Dutt V. Slipped capital femoral epiphysis associated with vitamin D deficiency A Series of 15 Cases. Bone Joint J. 2013;95-B(6):851–4. DOI: 10.1302/0301-620X.95B6.30806.
10. Jingushi S, Suenaga E. Slipped capital femoral epiphysis: etiology and treatment. J Orthop Sci. 2004;9(2):214–9. DOI: 10.1007/s00776-003-0755-2.
11. Moyer J, Jacks L, Hunter JD, Chan G. Slipped capital femoral epiphysis and associated hypothyroidism. A review of the literature with two classic case examples. J Pediatr Endocrinol Metab. 2016;29(4):1-7. DOI: 10.1515/jpem-2015-0311.
12. Nourbakhsh A, Ahmed HA, McAuliffe TB, Garges KJ. Case report: bilateral slipped capital femoral epiphyses and hormone replacement. Clin Orthop Relat Res. 2008;466(3):743-8. DOI: 10.1007/s11999-007-0099-x.
13. Loder RT, Wittenberg B, DeSilva G. Slipped capital femoral epiphysis associated with endocrine disorders. J Pediatr Orthop.1995;15(3):349–56.
14. Wyatt D. Lessons from the National Cooperative Growth Study. Eur J Endocrinol. 2004;151(Suppl 1):S55-9.
15. Bowden SA, Klingele KE. Chronic Bilateral Slipped Capital Femoral Epiphysis as an Unusual Presentation of Congenital Panhypopituitarism due to Pituitary Hypoplasia in a 17-Year-Old Female. Int J Pediatr Endocrinol. 2009;609131:1-3. DOI:10.1155/2009/609131.
16. Hu MH, Jian YM, Te Hsueh Y, Lin WH, Yang RS. Slipped capital femoral epiphysis in an adult with panhypopituitarism. Orthopedics. 2011;34(3):222. DOI: 10.3928/01477447-20110124-27.
17. Song KS, Lim YW, Ok IY, Lee SW. Delayed-onset of slipped capital femoral epiphysis. J Orthop Sci. 2015;20(1):78-86. DOI: 10.1007/s00776-014-0660-x.
18. Brady RL, Price A. Delayed-onset slipped capital femoral epiphysis: case report of association with pituitary tumor. Am J Orthop (Belle Mead NJ). 2010;39(3):137-40.
19. Loder RT, Hensinger RN. Slipped capital femoral epiphysis associated with renal failure osteodystrophy. J Pediatr Orthop. 1997;17(2):205-11.
20. Nixon JR, Douglas JF. Bilateral slipping of the upper femoral epiphysis in endstage renal failure. J Bone Joint
Surg Br. 1980;62-B(1):18-2121. Loder RT, Hensinger RN, Alburger PD, Aronsson DD,
Beaty JH, Roy DR, Stanton RP, Turker R. Slipped capital femoral epiphysis associated with radiation therapy. J Pediatr Orthop. 1998;18(5):630-6.
22. Perry DC, Metcalfe D, Costa ML, Staa TV. A nationwide cohort study of slipped capital femoral epiphysis. Arch Dis Child. 2017;102(2):1132-6. DOI: 10.1136/archdischild-2016-312328.
23. Peck D. Slipped Capital Femoral Epiphysis: Diagnosis and Management. Am Fam Physician. 2010;82(3):258-62.
24. Noguchi Y, Samaki T. Epidemiology and demographics of slipped capital femoral epiphysis in Japan: a multicenter study by the Japanese Paediatric Orthopaedic Association. J Orthop Sci. 2002;7(6):610–7. DOI: 10.1007/s007760200110.
25. Loder RT, Starnes T, Dikos G. Atypical and Typical (Idiopathic) Slipped Capital Femoral Epiphysis Reconfirmation of the Age-Weight Test and Description of the Height and Age-Height Tests. J Bone Joint Surg Am. 2006;88(7):1574-81. doi:10.2106/JBJS.E.00662
26. Kohl BA, Schwartz S. Surgery in the patient with endocrine dysfunction. Med Clin North Am. 2009;93(5):1031–47. DOI: 10.1016/j.mcna.2009.05.003.
27. Heatley FW, Greenwood RH, Boase DL. Slipping of the upper femoral epiphyses in patients with intracranial tumours causing hypopituitarism and chiasmal compression. J Bone Joint Surg Br. 1976;58(2):169-75.
28. Clement ND, Vats A, Duckworth AD, Gaston MS, Murray AW. Slipped capital femoral epiphysis: is it worth the risk and cost not to offer prophylactic fixation of the contralateral hip?. Bone Joint J. 2015;97-B(10):1428-34. DOI: 10.1302/0301-620X.97B10.33931.
34Slipped capital femoral epiphysis with coexisting pituitary tumor