clinical relevance of blood-culture for anaerobes
DESCRIPTION
Clinical relevance of blood-culture for anaerobes. Elisabeth Nagy MD, PhD, DSc Institute of Clinical Microbiology, Faculty of Medicine, University of Szeged, Hungary 5th ESCMID School Santander, 10-16 June, 2006. Changing concept of sepsis. Earlier concept of sepsis : - PowerPoint PPT PresentationTRANSCRIPT

Clinical relevance of blood-culture Clinical relevance of blood-culture for anaerobesfor anaerobes
Elisabeth Nagy MD, PhD, DScElisabeth Nagy MD, PhD, DSc
Institute of Clinical Microbiology, Faculty of Medicine, Institute of Clinical Microbiology, Faculty of Medicine,
University of Szeged, HungaryUniversity of Szeged, Hungary
5th ESCMID School5th ESCMID SchoolSantander, 10-16 June, 2006Santander, 10-16 June, 2006
Changing concept of sepsisChanging concept of sepsis
Earlier concept of sepsis: - detectable primary focus of the infection + - positive blood cultures
Sepsis (new definition since 1992):- SIRS (systemic inflammatory response syndrome), which
is an acute physiological response to any insult- sepsis if SIRS is caused by infection- septic shock: hypotension, perfusion abnormalities- severe sepsis organ dysfunctions, hypotension- multiple organ dysfunction syndrome (MODS) requires rapid intervention for prevention of homeostasis

Infection SIRS Sepsis Sever sepsis
infection + SIRSinfec.+SIRS+hypoperfusion-cardiovascular (SHOCK)-renal-ARDS-icterus-CNS-lactacidaemia-metabolic acidosis
MODS
In sepsis a series of events occursIn sepsis a series of events occurs
- temperature <36 or >38oC- pulse rate > 90 bpm- respiratory rate >20/min or hyperventilation- WBC <4 000/mm3 or >12 000 mm3


Mortality in sepsisMortality in sepsis
SIRS 5-7%
Sepsis 10-15%
Sever sepsis 20-25%
Septic shock 40-60%

Types of bloodstream infectionsTypes of bloodstream infections
Bacteraemia / fungaemia Transient
mechanical or surgical manipulation of infected tissue tooth brushing or bowel movements
Intermittent typically seen with undrained abscesses localized infections such as pneumonia, urinary tract
infection CNS infection
Continuous intravascular infections such as infective endocarditis,
septic thrombophlebitis, mycotic aneurysm

Transient bacteraemia after tooth extraction Transient bacteraemia after tooth extraction involving anaerobesinvolving anaerobes
Important in patients with artificial valves or having vitium and for patients with no hart problems as case of distant infections
47 patients were involved Blood samples were taken after 10 minutes of the extraction. 35 patients had transient bacteraemia. 28 of them had poor or
medium oral hygiene
Blood culture results Number of patients
Only aerobes 2 Only anaerobes 15 Aerobes + anaerobes 18 All with positive blood culture 35
Szonthág, Méray, Nagy (1994)

Transient bacteraemia after tooth extraction Transient bacteraemia after tooth extraction involving anaerobesinvolving anaerobes
Two blood culture systems were comparedOxoid Signal systemBio-Merieux Vital system
Blood culture results Percentage of all patients
Negative in both systems 26%
Positive in both systems 42%
Positive only in Bio-Merieux system 28%
Positive only in Oxoid system 4%
No. of anaerobic isolates in Oxoid system : 27 isolates
No. Of anaerobic isolates in bio-Merieux system: 50 isolates

Bacteraemia after plate removal and tooth Bacteraemia after plate removal and tooth extraction extraction (Rajasou et al.: 2004)(Rajasou et al.: 2004)
6 of 10 patients had at least 10 minutes after extraction transient bacteraemia.
4 had only anaerobic bacteria and 2 aerobic and anaerobic bacteria
Altogether 14 different species were isolated 12 anaerobes and 2 aerobes
The mortality rate of anaerobic endocarditis is 21-43% (Brook 2002) bacteria involved most frequently are anaerobic cocci, P. acnes, B. fragilis

The best way to detect bloodstream infection The best way to detect bloodstream infection is to carry out blood culturesis to carry out blood cultures
Traditional systems

Automated blood culture systemsAutomated blood culture systems

Anaerobic infectionsAnaerobic infections
”Classical” infections caused by clostridia exogenous clinical diagnosis
”Modern” infections caused by non-spore-forming anaerobes endogenous mixed infection normal flora members are involved

The ”golden” era of anaerobesThe ”golden” era of anaerobes (1960-80) (1960-80)
Dr. Sydney Finegold at work in an anaerobic chamber in 1960s
Recognition of the role of non-spore forming anaerobes in severe infections
Understanding the role of anaerobes in the normal floraIncidence of anaerobes in bacteraemia: 5-15% (Finegold 1977, Brook 1989)
B. fragilis group : 60-75%Clostridium spp: 10-20%Peptostreptococcus spp: 10-15%Fusobacterium spp: 10-15%P. acnes: 2-5% ????

Decrease of the incidence of anaerobes in Decrease of the incidence of anaerobes in bloodstream infectionsbloodstream infections
Decreased enthusiasm about anaerobes world-wide, but especially in the USDue to the cost of the proceduresDue to time-consuming methods
Increased use of metronidazole (and other anti-anaerobic antibiotics) for prophylaxis
Potent antibiotics were developed for empiric treatment of infections involving anaerobes
Development in surgical procedure and more understanding about situation where anaerobes can be potential pathogens

Do we need anaerobic blood culturesDo we need anaerobic blood cultures ? CONS ? CONS
Low incidence of positivity Ortiz et al. 2000: Routine use of anaerobic blood cultures: are they
still indicated? During a 3-year period 0.4% of the patients with a positive blood culture
had true anaerobic bacteraemia All 7 patients with anaerobic bacteraemia had an obvious source of
anaerobic infection
Gené et al. 2005: Value of anaerobic blood cultures in paediatrics During 2 year period 9,165 paediatric blood samples were processed 497
(5.4%) overall positivity and 2 (0.02%) positive for anaerobe
Lee at al. 2000: The assessment of anaerobic blood culture in children During 4 year period 9886 paired blood cultures in children 618 aerobic isolates and 3 anaerobic isolates

Do we need anaerobic blood cultures ? CONSDo we need anaerobic blood cultures ? CONS
Chandler et al. 2000: Re-evaluation of anaerobic blood cultures in a veteran population 5-year retrospective study 22,175 anaerobic blood cultures, significant anaerobic bacterium was isolated
only in 0.14% in 92% of these patients anaerobic infection could be suspected selective rather than routine use of anaerobic blood culture in a veteran
population
Senda et al.: Anaerobic bacteraemia: the yield of positive anaerobic blood cultures: patient characteristics and potential risk factors During a two year period in Japan 34/6,215 university hospital patients and
35/838 community hospital patients had an anaerobic bacteraemia Because of the low positivity anaerobic blood cultures should be used
selectively

Do we need anaerobic blood cultures ? Do we need anaerobic blood cultures ? PROSPROS
Clinical significance and outcome of anaerobic bacteraemia (Salonen JH, Eerola E, Meurman O: CID 1998)
The study was carried out in Turku (Finland), University hospital which is a 1000-bed tertiary-care teaching hospital
Between 1991 and 1996 40 000 blood cultures were performed 5% overall positivity 81 patients 111 samples (4% of all positive blood cultures) yielded anaerobic
bacteria 0.18 cases / 1,000 admission 21 patients had >2 blood cultures positive for the same anaerobic bacterium 4 patients had multiple anaerobes in their blood cultures
Most common isolates: Bacteroides (57%) > Peptostreptococcus (11%) > Clostridium (10%)

Clinical significance and outcome of anaerobic Clinical significance and outcome of anaerobic
bacteraemiabacteraemia (Salonen JH, Eerola E, Meurman O: CID 1998)
Blood cultures positive for anaerobes 81 patients
Clinically significant bacteraemia57 patients
Clinically insignificant bacteraemia24 patients
Initial treatment effective28 patients (49%)
Initial treatment ineffective, changed to affective
18 patients (32%)
Initial treatment ineffective, not changed
11 patients (19%)
Died5 patients (18%)
Died3 patients (17%)
Died6 patients (55%)

Do we need anaerobic blood cultures ? Do we need anaerobic blood cultures ? PROSPROS
Several unusual case reports prove the importance of isolation anaerobes from blood: O’Donnell et al: Bacteroides fragilis bacteraemia and infected aortic aneurysm
presenting as fever of unknown origin: diagnostic delay without routine anaerobic blood cultures. (1999)
Ha G.Y. et al: Case of sepsis caused by Bifidobacterium longum. (1999) Matsukawa et al.: Multibacterial sepsis in an alcohol abuser with hepatic cirrhosis.
(2003) (B. thetaiotaomicron, F. mortiferum, S. constellatus) Elsaghier et al.: Bacteraemia due to Bacteroides fragilis with reduced
susceptibility to metronidazole (2003) Candoni et al.: Fusobacterium nucleatum: a rare cause of bacteraemia in
neutropenic patients with leukemia and lymphoma (2003) C. septicum positive blood culture is strongly associated with neutropenic colitis
and colonic malignancy (G.P Bodey 1991) Etc.

Use of molecular techniques to improve Use of molecular techniques to improve identification of anaerobic bacteria originating identification of anaerobic bacteria originating
from bloodfrom blood
Lau et al.: Anaerobic, non-sporulating, Gram-positive bacilli bacteraemia characterized by 16S rRNA gene sequencing. Journal of Medical Microbiology 2004. 165 blood culture isolates of anaerobic Gram-positive bacilli were tested 51 C. perfringens 75 P. acnes the remaining 39 isolates were subjected to 16S rRNA sequencing: Clostridium spp (17), Eggerthella spp (10), Lactobacillus spp (8),
Eubacterium tenue (2), Olsenella uli (1), Bifidobacterium pseudocatenulatum (1)
Out of these 39 isolates 36 was considered clinically significant.
conventional method

Clinically significant anaerobic bloodstream Clinically significant anaerobic bloodstream infections in our University Hospitalinfections in our University Hospital
Tercier-care hospital with 1314 beds
2004 2005 2006 (I-V months)
Total no. of blood culture sets 3320 5432 2560
No. of positive anaerobic bottles 49 72 33
No. of clinically relevant anaerobe isolate 24 25 20
No. of patients with anaerobic 19 (1)* 18 9 (1)*
bloodstream infection
Case/1000 hospital admission 0.06 0.1 0.08
*No. of patients with polymicrobial anaerobic bloodstream infection

Distribution of anaerobic species among Distribution of anaerobic species among positive patientspositive patients
2004 2005 2006
B. fragilis B. fragilis B. fragilis
B. ovatis B. capillosus B. capillosus
B. thetaiotaomicron F. nucleatum F. necrogenes
B. uniformis Pr. denticola Prevotella sp
B. urealyticus Pr. oralis C. perfringens
Pr. oralis A. meyeri Micromonas micros
F. nucleatum C. carnis Pst. assacharolyticus
C. perfringens C. innocuum P. acnes ???
A. meyeri C. perfringens
A. odontolyticus Clostridium sp
E. lentum L. acidophilus
Micromonas micros Pst. assacharolyticus
P. acnes ??? V. parvula
P. acnes ???

Propionibacterium spp Propionibacterium spp isolated from blood isolated from blood cultureculture
Real pathogen
? colonizer
? contaminant
(quantitative microbiology is needed to distinguish)

Primary infections of proven Primary infections of proven P. acnesP. acnes aetiology aetiology (in previously healthy individuals)(in previously healthy individuals)
Purulent folliculitis distinct from acne vulgaris (Maibach, 1967)
Acute meningitis (Schlessinger, 1977)
Acute osteomyelitis (Suter et al., 1992)
Primary infections of eyeendophthalmitis (acute / chronic) - canaliculitisconjunctivitis - peri-orbital
cellulitisblepharitis - abscesseskeratitis

Secondary or opportunistic infections caused Secondary or opportunistic infections caused by by P. acnesP. acnes
Rare (USA hospital: 94 proven infections in 10 years, Brook et al., 1991)
Predisposing conditions: foreign bodiesdiabetesprevious surgery invasive diagnostic procedure immunodeficiency or immunosupressionmalignancy
Most frequently observed infections: abscess formation,meningitis due to CNS shunt osteomyelitis, arthritis, endocarditis

Gram-negative anaerobic bacteria induce Gram-negative anaerobic bacteria induce cytokines cytokines (Szöke, Nagy, Mandy, Kocsis 1997)
Gram-negative anaerobic bacteria induce Gram-negative anaerobic bacteria induce cytokines cytokines (Szöke, Nagy, Mandy, Kocsis 1997)
Different Bacteroides species were isolated from infections
Human mononuclear cells and whole blood cultures were used for the induction
TNF release was detected by the WEHI 164 bioassay
IL-6 production was detected by the B-9 bioassay
Besides the whole cells of anaerobic bacteria, isolated LPS was also used in the induction experiments
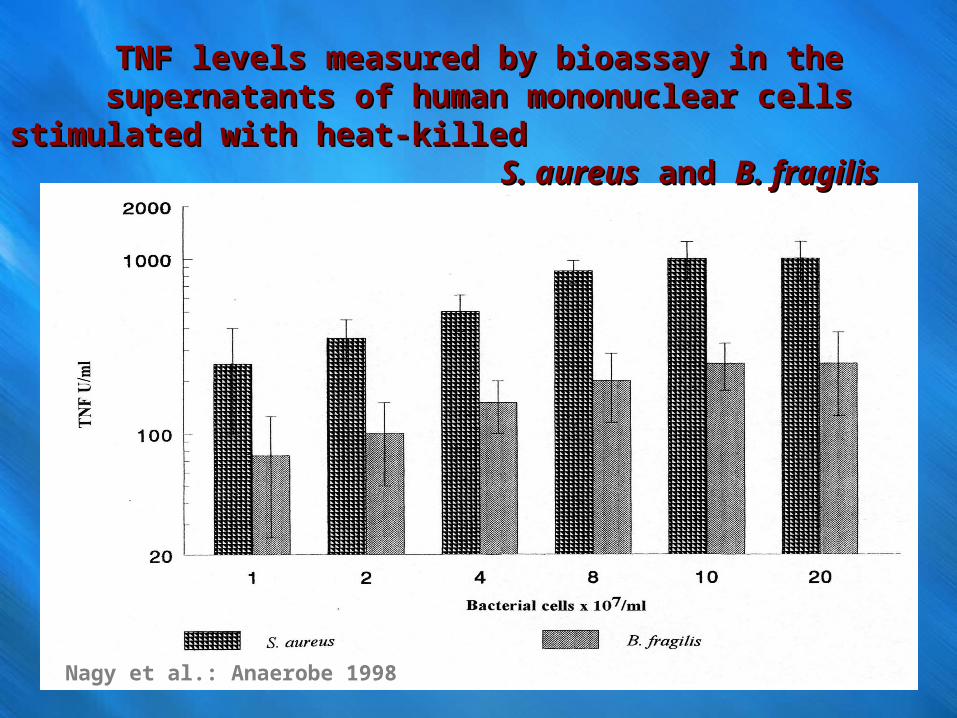
TNF levels measured by bioassay in the supernatants of human TNF levels measured by bioassay in the supernatants of human mononuclear cells stimulated with heat-killed mononuclear cells stimulated with heat-killed
S. aureusS. aureus and and B. fragilisB. fragilis
Nagy et al.: Anaerobe 1998

Induction of TNF and IL-6 by LPS of Induction of TNF and IL-6 by LPS of B. fragilisB. fragilis and and E. coliE. coli
Amount ofTNF (U/ml) IL-6 (pg/ml)
MN cells whole blood MN cells whole blood
B. fragilis LPS 1x102 5x102 1x105 1x105 E. coli LPS 2.5x102 7.5x102 1x106 1x106
B. fragilis was a clinical isolate obtained from an abscess
Anaerobes can easily be involved in the development of sepsis !!

Conclusions 1.Conclusions 1.
Risk factors for anaerobic bacteraemiaElderly ageHaematological malignancy with or without therapy, such
as febrile neutropenia, bone marrow transplant recipients Solid tumour as underlying diseaseUnderlying disease in the gastrointestinal tractPoor oral hygiene
Same facultative anaerobic bacteria grow better in the anaerobic bottle that in the aerobic one (earlier detection)

ConclusionsConclusions 2. 2.
Increasing number of publications proves the presence of anaerobic bacteraemia during FUO
Uncommon anaerobic infections may result in bacteraemia (diabetic foot ulcer, oral cancer, Lemmier’s syndrome, etc.)
Antibiotics used for empiric treatment of anaerobic mixed infections may fail to treat the patients due to antibiotic resistance in anaerobes (Bacteroides fragilis and related species)