clinical pathology correlate conference katrina cannon, md internal medicine
TRANSCRIPT
Clinical Pathology Correlate Conference
Katrina Cannon, MD
Internal Medicine

Case Presentation 50 yo African American female with 2 year hx
of intermittent dyspnea presented to ER with marked SOB and respiratory distress
Pulmonary clinic 6 months prior for dyspnea and abnormal CXR; recommended further evaluation including CT; not completed
Significant dyspnea ~ 2 weeks new heart palpitations
ER coursePhysical Exam
Gen: significant respiratory distress, cool but no diaphoresis, no pain
VS: HR 120-130 and BP 160/100 CV: distant heart sounds, no m/r Lungs: poor breath sounds, expiratory
wheezes and “tightness”Treatment: oxygen by facemask
Acute Respiratory FailureContinued SOB, appeared hypoxicABG: pH 7.15, PaCO2 51, PaO2 200 Decreasingly responsiveRapid Sequence Intubation
Sedation: versed, fentanyl Paralyzed: succinylcholine,vecuronium Intubation: ETT placed
ER coursePhysical Exam
VS: BP 80/60 Extremities: mottled, cool, hypoperfused
EKG/CXR/labs obtained

EKG
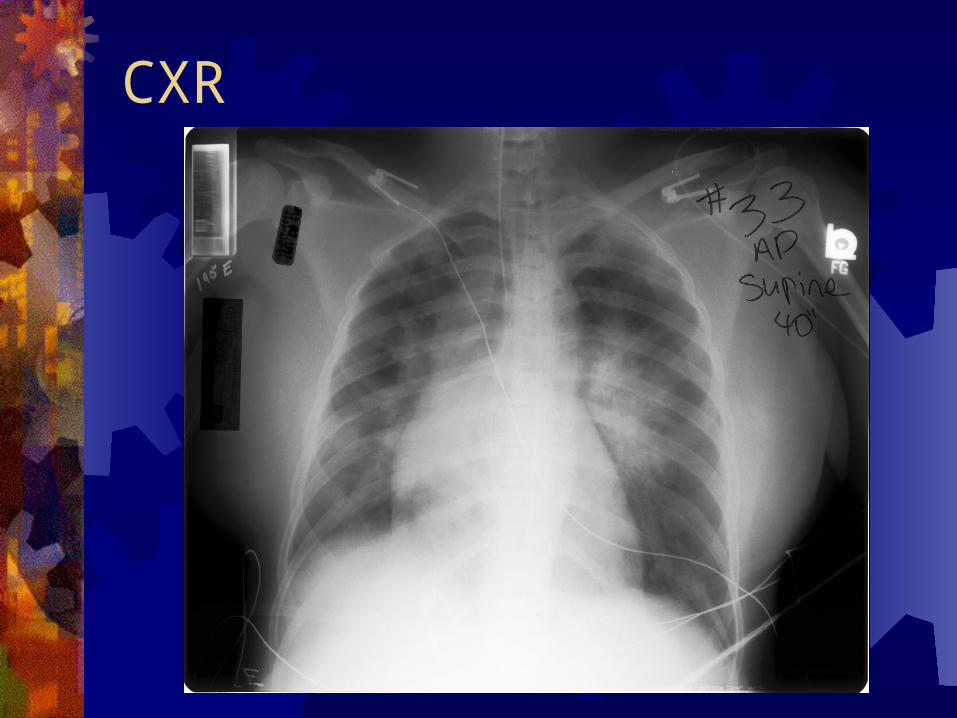
CXR

LabsGlucose 230Na 130, K 3.6, Cl 106, HCO3 22BUN 10, Cr 0.8WBC 8.7 (54% bands, 10% lymphs),
Hgb 9.5, Platelets 347,000CK 53, LDH 218, Trop T WNL

ER Course continues…Hypotension tx: IVF and DopamineCardiology Consult: abnormal EKG,
persistent hypotension and tachycardia ? possible AMI with cardiogenic shock
Cardioversion attempted-unsuccessfulEchocardiogram
EchocardiogramMild generalized hypokinesisMore focal wall motion in anterior apical
wallEF mildly reduced- difficult to assess
due to tachycardiaLVHNo acute valvular disordersSmall pericardial effusion

ER Course continues…Adenosine (transient AV block) revealed
underlying atrial rate of ~240Digoxin initiatedDopamine Neo-Synephrine startedBP responded, blood gas improved:
ABG pH 7.3 35/135 HCO3 17Transferred to ICU

ICU Course: Day 1Respiratory: ventilatorCardiovascular:
digoxin + procainamide HR 100-110 atrial tachycardia persisted
Diuresed with brisk responseNeo-Synephrine tapered off
PA CatheterPCWP = 13 (12-18)RA = 9 (2-6)PAP = 46/32 (25/10)CO = 5.4 (5.4 - 7.2)CI = 2.9 (2.9 - 3.9)PVR = 829 (<250 dyne) Initially on Neo-Synephrine (then off)
ICU CourseDay 2: extubated but continued O2
support for moderate dyspneaDay 3: EP consult for atrial tachycardia
Dx: automatic atrial tachycardia Tx: added Flecainide
Day 4: Sinus rhythm restored and maintained

Follow-up EKG

Follow-up Test ResultsEcho: LVH, recovery of LV function with
mildly depressed EF, no focal wall motion abnormalities
Cardiac biomarkers: negative
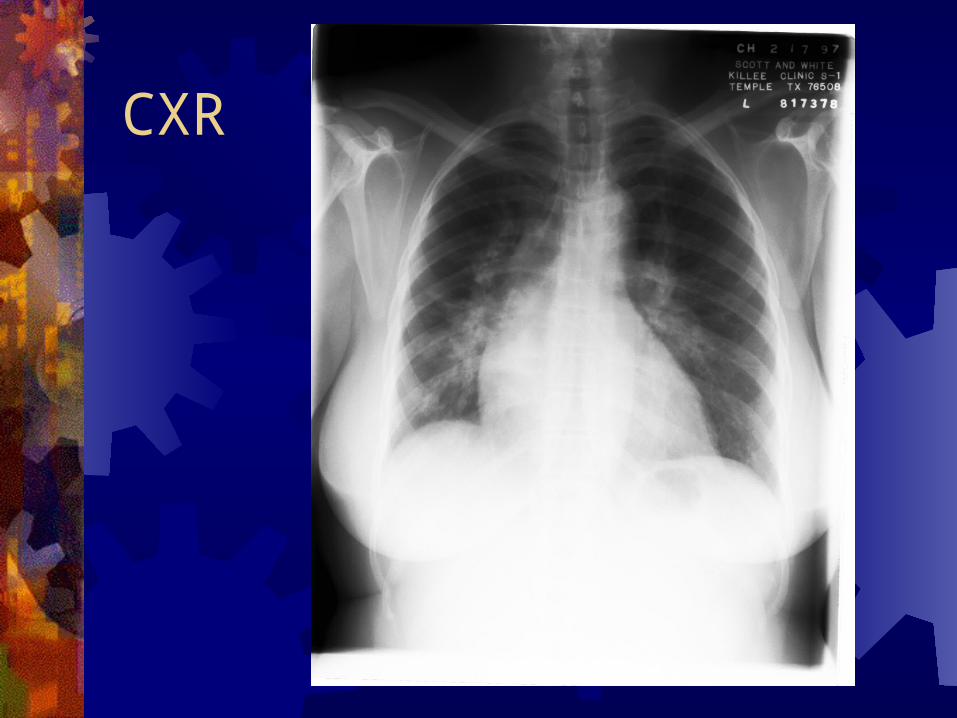
CXR
Transferred to FloorRespiratory: Pulmonary consult to
continue workup of dyspnea and abnormal CXR
Cardiovascular: continued on flecainide and digoxin, diuretic, + lisinopril (HTN)
Pulmonary Function TestsFVC = 1.39 L (42% predicted)FEV1 = 1.15 L (43% predicted)DLCO = 10.4 ml/min/mmHg (42% predicted) Interpretation:
Moderately severe restrictive change Severely reduced diffusing capacity Significant gas transfer disorder Mild airways obstruction
CT ScanBilateral interstitial infiltratesParticularly at the basesPerihilar adenopathy

Additional Laboratory Data Anemia: Hbg 9.5 11 with 2 PRBC Electrolytes/BUN/Cr: normalized Blood Cultures: negative Serum Protein Electrophoresis: normal ACE level: 40 (7-46) ABG: “normal”
Persistent hypoxia, wheezing and dyspnea on exertion

Day 5: BronchcoscopyStenotic lobar and segmental airway
involvement of entire tracheobronchial tree with compromised 50-60% of lumen diameter
Brush washings, transbronchial Bx, mucosal Bx and Cx obtained
Tx: steroids

Day 7: Hospital Discharge Improved clinically with less wheezing
and dyspneaDischarged: prednisone, lisinopril,
HCTZ, digoxin and flecainideF/U with Pulmonary and Cardiology
A Diagnostic Result was revealed.
Problem List: Dyspnea Respiratory
Acute Respiratory Failure Chronic Progressive Dyspnea Abnormal CXR/CT: interstitial infiltrates and perihilar
adenopthay Abnormal PFTs: restrictive lung disease with decreased
DLCO Cardiovascular
Tachyarrhythmia: automatic atrial tachycardia LVH Anemia Hypotension HTN
Respiratory: Dyspnea Acute Respiratory Failure ~tachyarrhythmia Chronic Dyspnea ~ 2 year history intermittent
and progressive SOB
CHRONIC DYSPNEA
Chronic Airway Disease: COPD, asthma Interstitial Lung Disease Chronic Cardiac Disease

Chronic Dyspnea Good Information: History, PE, labs, old and
recent CXR, CT, PFTs, and Bronchoscopy
Abnormal CXR/CT: bilateral interstitial infiltrates, particularly at the bases with perihilar adenopathy
Abnormal PFTs: restrictive lung disease with decreased diffusing capacity
Bronchoscopy: compromised lumen diameter
Interstitial Lung Disease
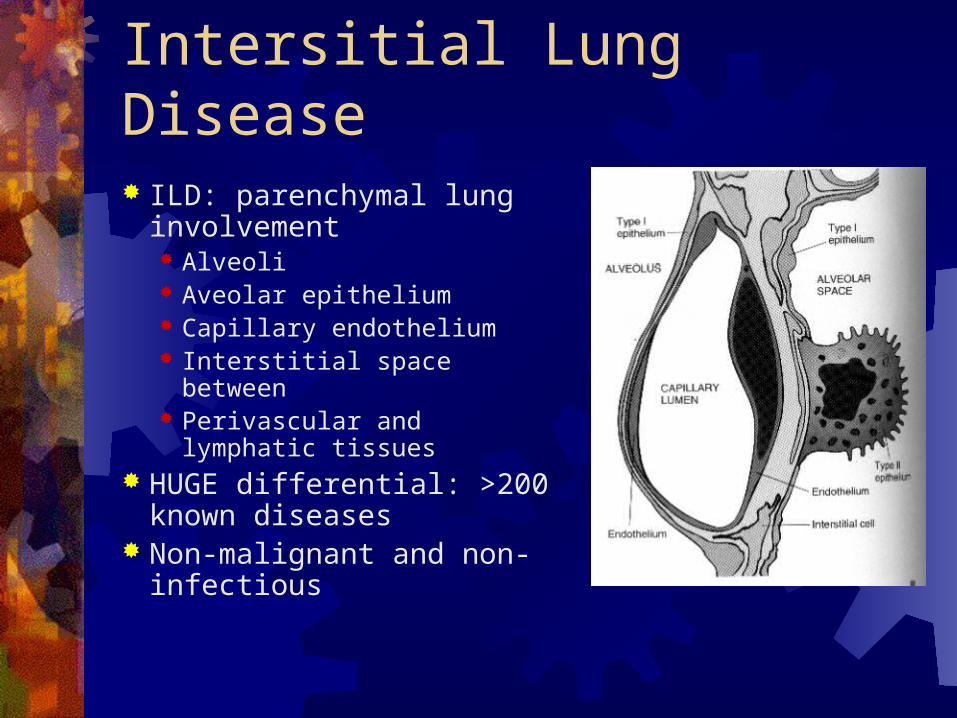
Intersitial Lung Disease ILD: parenchymal lung
involvement Alveoli Aveolar epithelium Capillary endothelium Interstitial space between Perivascular and lymphatic
tissues HUGE differential: >200
known diseases Non-malignant and non-
infectious

Diffuse Parenchymal Lung Disease
K n ow n C au se :D ru g s /Trea tm en t
E n viron m en ta l E xp osu reC o llag en V asc D isease
Id iop a th icP u lm on ary
F ib ros is
D esq u am ativeIn te rs tit ia l
P n eu m on ia
R esp ira to ryB ron ch io lit is
IL D
A cu teIn te rs tit ia l
P n eu m on ia
L ym p h ocyticIn te rs tit ia l
P n eu m on ia
N on -sp ec ificIn te rs tit ia l
P n eu m on ia(p rovis ion a l)
C ryp tog en icO rg an iz in gP n eu m on ia
(B O O P )
IIPo th er th an
IP F
Id iop a th icIn te rs tit ia l
P n eu m on ia
G ran u lom atou s :S arco id os is
P L C H is tiocytos is
P u lm on ary H em orrh ag eS yn d rom es
L A MA m ylo id os is

Primary Disease associated with Interstitial Lung Disease Sarcoidosis PLCH Vasculitides Hemorrhagic syndromes Amyloidosis Lymphangiolieomyomatosis (LAM) Lymphangitic Carcinomatosis Congenital/Hereditary Chronic Pulmonary Edema Alveolar Proteinosis Pulmonary Veno-occlusive Disease
ILD: History Timing: Chronic (months to years)
Idiopathic Pulmonary Fibrosis Sarcoidosis Pulmonary Langerhans Cell Histiocytosis (PLCH,
Histiocytosis X, Eosinophilic Granuloma)
Age (50) Sarcoid, PLCH, CVD, LAM, inherited ~20-40 IPF >50
History continued…Family History: negative
Neurofibromatosis Tuberous Sclerosis Hermansky-Pudlak syndrome
Occupational/Drug Exposure: none no amiodarone ACE induced cough Procainamide ~drug-induced SLE
History continued… Gender: LAM, tuberous sclerosis only in
premenopausal women
Race: African American Sarcoidosis 3-4 times more common in blacks,
lifetime risk 2.4% v. whites 0.85%
Smoking History: non-smoker +tob: PLCH, DIP, IPF, respiratory bronchiolitis -tob: sarcoidosis, hypersensitivity pneumonitis
Physical Exam Dyspnea, wheezing No cough, no hemoptysis, no chest pain
BOOP/COP Respiratory bronchiolitis Hypersensitivity pneumonitis Diffuse alveolar hemorrhage syndromes Granulomatous vasculitides Maligancy
No extrapulmonary findings
LabsNormal electrolytesNormal renal functionMild Anemia, stableABG: respiratory acidosis-resolved

Labs continued…ACE level 40 (7-46) upper limits of normal:
Increased 35-80% sarcoidosis But can be normal (sensitivity 57%) Less likely increased in chronic sarcoidosis Also increased Silicosis, TB, LIP
No ANCA: Wegner’s granulomatosisNo Anti-BM ab: Goodpasture’s
syndrome
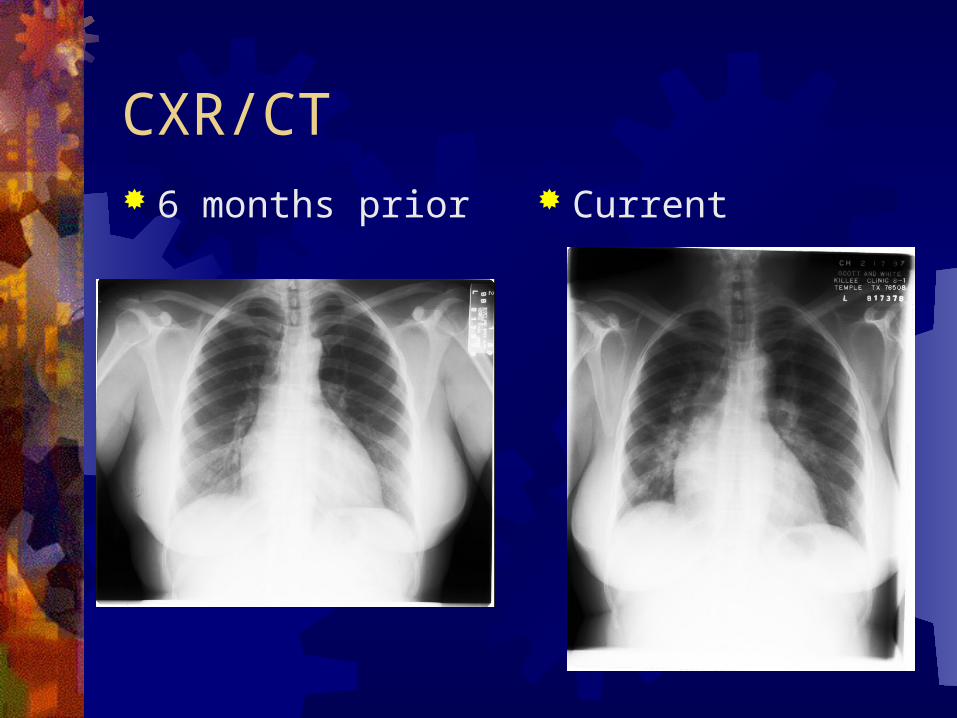
CXR/CT 6 months prior Current
ILD plus Perihilar Adenopathy Sarcoidosis Lymphoma Lymphangitic carcinomatosis Infectious: TB or Fungal Disease
(histoplasmosis) Lymphocytic interstitial pneumonia Amyloidosis Pneumoconioses (Beryllium, Silicosis) Bronchiogenic Carcinoma
Sarcoidosis Evidence For
Race: African American Age: <50 CXR/CT:Bilateral
Pulmonary infiltrates and perihilar adenopathy
PFTs: restrictive, DLCO Bronch: endobronchial
lesions CV: tachyarrhythmia
Evidence Against CXR/CT: Lower lung
zone Bronch: stenosis Lab: ACE ? No extrapulmonary
manifestations…

Sarcoidosis Stage I: bilateral hilar
adenopathy Stage II: bilateral hilar
adenopathy + interstitial infiltrates (upper > lower)
Stage III: interstitial disease with shrinking hilar nodes
Stage IV: advanced fibrosis

Sarcoidosis Evidence For
Race: African American Age: <50 CXR/CT:Bilateral
Pulmonary infiltrates and perihilar adenopathy
PFTs: restrictive, DLCO Bronch: endobronchial
lesions CV: tachyarrhythmia
Evidence Against CXR/CT: Lower lung
zone Bronch: stenosis Lab: ACE ? No extrapulmonary
manifestations…

Sarcoid and Cardiovascular Disease
Not uncommon: 5% clinically significant 25-30% postmortem
Granulomatous infiltration
Conduction disturbances Atrial Tachycardia*
Conclusion50 yo AAF with Chronic DyspneaPulmonary SarcoidosisFocal Atrial Tachycardia ~ CV sarcoidAcute Respiratory Failure:
CHF/Pulmonary EdemaCardiac: diuresis and antiarrhythmicsTx: Steroids

Dx: SarcoidosisClinical and Radiographic findings
supportive of SarcoidosisR/O infection:TB and fungal diseaseHistologic evidence of noncaseating
granulomas

Diagnostic ResultNoncaseating Granulomas
SARCOIDOSIS

The End
1. Proceed to the post test2. Download the post test3. Complete the post test4. Return the post test to Dr. S. Oliver
407i TAMUII

Post test question 1Sarcoidosis is most often diagnosed in
which of the following EXCEPT: Young adults (20-40 years old), Nonsmokers Hispanic-Americans Roughly equal in Caucasian men and
women

Post test question 2Sarcoidosis is usually treated initially
with which of the following:1. Steroids2. Methotrexate3. Thalidomide4. Cytoxin
References ACC/AHA/ESC Guidelines for the Management of Patients with
Supraventricular Arrhythmias; JACC Vol. 42. No. 8, 2003, Oct 15 2003: 1513-1516.
Braunwald, E; Essential Atlas of Heart Disease; Current Medicine 1997; Philadelphia, PA; pg 5.9.
Colucci, W; Braunwald, E; Atlas of Heart Failure: Cardiac Function and Dysfunction; 2nd Ed; Current Medicine 1999; Philadelphia, PA; pg 3.11.
Schwarz, M; King, T; Interstitial Lung Disease 4th Ed.; BC Decker Inc.; Hamilton London; 2003.
Uptodate: Approach to the Adult with Interstial Lung Disease, Evaluation of Diffuse Lung Disease by Plain Chest Radiography, Overview of Sarcoidosis, Atrial Tachycardias