clinical management of continuous-flow left ventricular ... et al... · effects of the device in...
TRANSCRIPT

CaMLRSMMSD
FDURCU
http://www.jhltonline.org
1d
linical management of continuous-flow left ventricularssist devices in advanced heart failureark S. Slaughter, MD,a* Francis D. Pagani, MD,b* Joseph G. Rogers, MD,c*eslie W. Miller, MD,d* Benjamin Sun, MD,e* Stuart D. Russell, MD,f*andall C. Starling, MD, M.P.H.,g* Leway Chen, MD,h Andrew J. Boyle, MD,i
uzanne Chillcott, RN,j Robert M. Adamson, MD,j Margaret S. Blood, RN,k
argarita T. Camacho, MD,l Katherine A. Idrissi, RN, MSN,m
ichael Petty, RN, PhD,i Michael Sobieski, RN, CCP,a
usan Wright, RN, BSN, CCRN,b Timothy J. Myers, BS, CRA,n andavid J. Farrar, PhD,o for the HeartMate II Clinical Investigators
rom the aUniversity of Louisville, Louisville, Kentucky; bUniversity of Michigan, Ann Arbor, Michigan; cDuke University,urham, North Carolina; dGeorgetown University, Washington Hospital, Washington, District of Columbia; eOhio Stateniversity, Columbus, Ohio; fJohns Hopkins Hospital, Baltimore, Maryland; gCleveland Clinic, Cleveland, Ohio; hUniversity ofochester, Rochester, New York; iUniversity of Minnesota, Minneapolis, Minnesota; jSharp Memorial Hospital, San Diego,alifornia; kUniversity of Alabama, Birmingham, Alabama; lBeth Israel Medical Center, Newark, New Jersey; mColumbia
niversity, New York, New York; nHouston, Texas; and oThoratec Corporation, Pleasanton, California.Continuous-flow left ventricular assist devices (LVAD) have emerged as the standard of care foradvanced heart failure patients requiring long-term mechanical circulatory support. Evidence-basedclinical management of LVAD-supported patients is becoming increasingly important for optimizingoutcomes. In this state-of-art review, we propose key elements in managing patients supported with thenew continuous-flow LVADs. Although most of the presented information is largely based on inves-tigator experience during the 1,300-patient HeartMate II clinical trial, many of the discussed principlescan be applied to other emerging devices as well. Patient selection, pre-operative preparation, and thetiming of LVAD implant are some of the most important elements critical to successful circulatorysupport and are principles universal to all devices. In addition, proper nutrition management andavoidance of infectious complications can significantly affect morbidity and mortality during LVADsupport. Optimizing intraoperative and peri-operative care, and the monitoring and treatment of otherorgan system dysfunction as it relates to LVAD support, are discussed. A multidisciplinary heart failureteam must be organized and charged with providing comprehensive care from initial referral untilsupport is terminated. Preparing for hospital discharge requires detailed education for the patient andfamily or friends, with provisions for emergencies and routine care. Implantation techniques, trouble-shooting device problems, and algorithms for outpatient management, including the diagnosis andtreatment of related problems associated with the HeartMate II, are discussed as an example of aspecific continuous-flow LVAD. Ongoing trials with other continuous-flow devices may produceadditional information in the future for improving clinical management of patients with these devices.J Heart Lung Transplant 2010;29:S1–S39 © 2010 Published by Elsevier Inc.
KEY WORDS:patient selection;patient and devicemanagement;LVAD;mechanical circulatorysupport;assisted circulation;bridge totransplantation;destination therapy
Conflict of Interest: See Disclosure Statement on page S36.Reprint requests: Dr David J. Farrar, Thoratec Corporation, 6035 Stoneridge Dr, Pleasanton, CA 94588. Fax: 925-847-8574.E-mail address: [email protected]
*Drs. Slaughter, Pagani, Rogers, Miller, Sun, Russell, and Starling contributed equally to this article.053-2498/10/$ -see front matter © 2010 Published by Elsevier Inc.oi:10.1016/j.healun.2010.01.011

T
V
Ifl
Mapctdspsldna
urHt
S2 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
able of Contents
I. Introduction and Overview of Continous-flow LeftVentricular Assist Systems .....................................S2
I.A. Continuous-Flow LVASs...........................S3
II. Patient Selection and Preoperative Considerations ........S4II.A. Patient Selection for LVAD Support: Illness
Assment for Operative Risk ......................S4II.B. Patient Mortality Risk for Undergoing LVAD
Implantation ...............................................S5II.B.1. Overall Risk Factors for Operative
Mortality......................................S6II.B.2. Obesity Paradox..........................S7II.B.3. Assessment of Right Ventricular
Function ......................................S7II.C. Preoperative Assessment and Optimization.....S8
III. Intraoperative Considerations................................S12III.A. Managing Valvular Heart Disease ..........S13
III.A.1. Aortic Valve Pathology ............S13III.A.2. Mitral Valve Pathology ............S14III.A.3. Tricuspid Valve Pathology.......S14
III.B. Preclotting Considerations .......................S14III.C. Pump Placement.......................................S15III.D. Percutaneous Lead Placement .................S16III.E. Cardiopulmonary Bypass.........................S16III.F. De-airing and Transitioning from CPB...S17III.G. Coagulopathy and Bleeding.....................S18III.H. Intraoperative Management of RV Dysfunc-
tion............................................................S19III.I. Intraoperative Echocardiography.............S19III.J. Replacing a HeartMate XVE LVAD with a
Continuous-Flow LVAD .........................S20III.K. Exchanging a HeartMate II LVAD with a
HeartMate II LVAD ................................S20
IV. Post-operative Patient Management......................S20IV.A. RV Function.............................................S21IV.B. Anti-coagulation.......................................S21
IV.B.1. Titrating Anti-coagulation ........S21IV.B.2. Thromboelastography ...............S22
IV.C. Blood Pressure Monitoring and Manage-ment..........................................................S22
IV.D. Patient Education .....................................S22IV.D.1. System Operation......................S23IV.D.2. Self-Care Infection Prophylaxis
and Percutaneous Lead Immobili-zation.........................................S23
IV.D.3. Maintaining Volume Status/Hydra-tion.................................................S23
V. Post-operative Device Management .....................S23V.A. Monitoring Device Function ...................S23
V.A.1. Flow/Power ...............................S24V.A.2. Pulsatility Index ........................S24V.A.3. Selecting Optimum Pump Speed..S24
VI. Diagnosing and Managing Post-operative Complica-tions........................................................................S25
VII. Outpatient Management ........................................S27 m
VII.A. Preparing for Hospital Discharge............S27VII.B. Outpatient Medical Therapy....................S28VII.C. Outpatient Device Management ..............S31
VII.C.1. Percutaneous Lead Care and ExitSite Wound Management .........S31
VII.D. Handling Emergencies .............................S32VII.E. Outpatient Follow-Up ..............................S32
III. Troubleshooting .....................................................S32VIII.A. Pump Thrombus.......................................S32VIII.B. Pump Stops ..............................................S35VIII.C. Suction Events .........................................S35VIII.D. Obstruction ...............................................S35
IX. Results from Completed Clinical Trials ...............S36
. Introduction and overview of continuous-ow left ventricular assist systems
Key Points
Continuous-flow left ventricular assist systems arenew-generation devices with a number of major advan-tages over previous pulsatile technology:
● Continuous-flow, rotary blood pumps eliminate theneed for a blood pumping chamber and volumecompensation.
● A lighter, smaller pump is better suited for patientswith a smaller body size.
● Simple designs include only 1 internal moving part,the rotor, and no internal valves. This affords mark-edly enhanced device durability.
● They are silent in operation.● The potential benefits of the smaller percutaneous
lead include a reduced infection risk and greaterpatient comfort.
echanical circulatory support (MCS) for patients withdvanced heart failure has evolved considerably during theast 30 years and is now standard therapy at many medicalenters worldwide. Left ventricular assist systems (LVASs)hat use continuous-flow rotary blood pumps have beeneveloped during the past decade in response to the need formaller and more durable devices.1–9 Although the earlierulsatile LVAS designs provided adequate cardiac outputupport, their large size and limited durability hinderedong-term success. Continuous-flow left ventricular assistevices (LVADs) are small and durable, which offers aumber of advantages that aid in minimizing complicationsssociated with LVAD support.
Recent clinical studies of patients supported by contin-ous-flow LVADs indicate that there are fewer device-elated complications and outcomes are improved.1,7,8
owever, complications persist during LVAD support dueo pre-existing effects of advanced heart failure, the require-
ent for extensive surgery to implant the device, and the
euvb
bchbcDtpopSy
izsafosnato
fmdfXmcmm
I
Cpppc1sCccstscr
ef
tccapsbaustgcc
flochtuiAale
Fdtt
S3Slaughter et al. Management of Continuous-Flow LVADs
ffects of the device in compromised patients. The contin-ed improvement in survival rate and quality of life for thisery ill population of patients requires consistent evidence-ased clinical management throughout LVAD support.
This supplement is devoted to comprehensive informationased on a large experience during the last decade with thelinical management of continuous-flow LVADs in advancedeart failure patients. Most of the information presented isased on the authors’ experiences during the 1,300-patientlinical trial on the HeartMate II LVAS that led to Food andrug Administration (FDA) approval for bridge to transplan-
ation (BTT) and destination therapy (DT) approvals and onublished data from this trial. However, because all continu-us-flow LVASs are similar in basic features, some of therinciples of clinical management are relevant to all devices.pecific differences between various LVAS designs are be-ond the scope of this article.
Topics that are generic to most continuous-flow devicesnclude patient selection, pre-operative assessment and optimi-ation, intraoperative considerations related to medical issuesuch as valvular heart disease and hemostasis, and post-oper-tive patient management, including right ventricular (RV)unction, blood pressure monitoring, patient education, andutpatient management and medical therapy. Topics that arepecific to the HeartMate II device include implantation tech-iques, anti-coagulation, post-operative device management,nd troubleshooting. As additional experience is gained withhe HeartMate II and other continuous-flow pumps, these rec-mmendations may change.
We recommend that readers also refer to the directionsor use, guidelines for care, and other published docu-ents that are specific to each device or generic to all
evices. For example, the 2-volume practice guidelinesor destination therapy10,11 were written for the HeartMateVE pulsatile-flow LVAD but contain applicable infor-ation for all long-term implantable LVADs, including
andidate selection, team organization, nutrition manage-ent, infection control, intraoperative and peri-operativeanagement, and discharge planning.
.A. Continuous-flow LVASs
ontinuous-flow LVASs use new-generation rotary bloodumps that are designed to provide extended circulatory sup-ort. They consist of an internal LVAD blood pump with aercutaneous lead that connects the pump to an external systemontroller and a power source (batteries or line power; Figure). Continuous-flow rotary designs significantly reduce LVADize and weight compared with implantable pulsatile pumps.ontinuous-flow LVADs are also silent during operation andreate minimal motion and vibration. These features makeontinuous-flow devices more suitable for use in patients withmaller body size. Additional benefits over pulsatile LVADechnology include greater durability (no internal valves, and aingle internal moving part, the pump rotor), greater patientomfort and enhanced quality of life, and a reduced infection
isk. The enhanced durability and reliability of this new-gen- cration LVAD should lead to more patients being supportedor extended durations.
All continuous-flow LVADs share important func-ional characteristics, the most important of which is theontinuous unloading of the LV throughout the cardiacycle. This type of support diminishes or eliminates therterial pulse, making the routine assessment of bloodressure more challenging and much less reliable. Sub-tantial clinical experience has confirmed that the humanody can be adequately supported with a diminished orbsent pulse with a continuous-flow LVAD. However,sers of these systems should have a thorough under-tanding of the fundamental differences between pulsa-ile-flow and continuous-flow pumps. Table 1 provides aeneral comparison of the 2 types of LVADs now inlinical use, and Table 2 compares the pulsatile-flow andontinuous-flow LVADs that are presently in clinical use.
Continuous-flow LVASs use centrifugal-flow or axial-ow blood pumps. The fundamental design characteristicf both types of pump is that they have a single movingomponent, the impeller. Conversely, pulsatile LVADsave multiple moving components that are all susceptibleo wear and failure. The rotating impellers of the contin-ous-flow LVAD have 1 of 3 types of bearing: (1) bloodmmersed, (2) hydrodynamic, or (3) magnetic levitation.ll 3 types have nominal or absent friction, heat gener-
tion, or wear, making these devices very durable duringong-term support. There have been numerous reports ofxtended support with these devices and with promising
igure 1 The HeartMate II continuous-flow left ventricular assistevice receives blood from the left ventricular apex and returns it tohe ascending aorta. The pump is connected with a percutaneous leado an external controller and batteries worn by the patient.
linical results.1,7,8,12–16

Ic
Pdatow
Da
Ia
CtdLdb
iiovsHpmwtRmcl
clih(r1pdtpbc
S4 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
I. Patient selection and preoperativeonsiderations
Key Points● The highest risk of death after LVAD implant is
before hospital discharge. Thus, patient selectionand the timing of implant are two of the majordeterminants of success.
● Key selection criteria include assessment of the pa-tient’s severity of illness and ability to successfullyundergo the implant procedure.
● The trend at many centers is toward earlier use of aLVAD to avoid progressive end-organ dysfunction.
● Pre-implant optimization of comorbid conditions is veryimportant in minimizing the incidence and severity ofpost-operative adverse events and for enhancing survival.The most influential pre-implant measures are:y Improving nutritional status.y Lowering pulmonary vascular resistance to opti-
mize right-heart function and to reduce right atrialpressure and secondary hepatic congestion.
y Aggressively managing volume to minimize rightventricular workload and hepatic congestion.
y Optimizing coagulation.y Optimizing renal, hepatic, pulmonary, and neuro-
logic function.y Treating any infection or providing prophylactic
anti-biotic therapy.
● The patient’s support system, psychosocial status,compliance with care, and ability to operate and carefor external system components all warrant consid-erations in the patient-selection process.
atient selection and the timing of implant remain primaryeterminants of success for LVAD therapy. Patients aressessed for (1) appropriateness for LVAD support based onhe degree of illness, (2) ability to successfully undergo theperative procedure, and (3) ability to be discharged to home
Table 1 Comparison of Pulsatile and Continuous Flow Ventric
Attribute Pulsatile-flow VAD
Size Large; intracorporeal devices limitextracorporeal devices especiallypatients or for biventricular sup
Blood flow capacity Up to 10 liters/minType of pump Sac or diaphragmImplantation Extracorporeal or intracorporeal ty
diaphragmatic intraperitoneal oMain hemodynamic
characteristicIntermittent unloading of ventricl
pressure; asynchronous with heaPhysiologic flow variables Pre-load dependantMechanical flow variables Automatic or fixed rate and stroke
ith adequate family/caregiver support for long-term success. t
uring LVAD candidate assessment, risk factors for poor survivalre identified and treated, when possible, to minimize their effect.
I.A. Patient selection for LVAD support: illnessssessment for operative risk
andidates for LVAD support will present with comorbidi-ies that vary in severity, depending on the extent anduration of heart failure. The acceptance of candidates forVAD support and the timing of device implant need to beetermined by careful consideration of potential risks andenefits.
Many issues affecting successful outcomes after LVADmplant are related to patient illness and timing. For example,mplanting the LVAD before irreversible end-organ failure hasccurred, or delaying implant until comorbidities can be re-ersed or controlled, increases the likelihood of post-implanturvival. The Heart Failure Survival Score17 and the Seattleeart Failure Model18 can be used to estimate a heart failureatient’s expected survival during the next 1 to 2 years onedical management and identify patients at high risk of deathho might benefit from LVAD support. A recent study used
he Seattle Heart Failure model to analyze patients in theandomized Evaluation of Mechanical Assistance in Treat-ent of Chronic Heart Failure (REMATCH) trial and con-
luded that patients could be stratified into high, medium, andow risk for LVAD support.19
The Interagency Registry for Mechanically Assisted Cir-ulatory Support (INTERMACS) registry,20–22 which fol-ows all long-term mechanical circulatory support systemsn the United States, has defined patient profiles that canelp identify risks associated with the timing of implantTable 3). The current 6-month survival data for patientseceiving pulsatile LVADs indicates that patients in profile, cardiogenic shock, have the lowest survival, and those inrofile 3, stable on inotropes, have the best survival.20 Theseata indicate that patients with cardiogenic shock may beoo sick for permanent LVAD support. Thus, for theseatients, consideration should be given for immediate sta-ilization with biventricular support, using temporary per-utaneous or surgically placed systems or other appropriate
sist Devices
Continuous-flow VAD
arge patients;d for smaller
Smaller; accommodates most patients,excluding infants
Up to 10 liters/minCentrifugal or axial flow by rotating impeller
b-ritoneal
Extracorporeal, intracardiac, pericardial,sub-diaphragmatic
atile arterial Continuous unloading of ventricle
Pre-load and after-load dependante capacity Set speed of the impeller rotation
ular As
ed to lsuite
port
pes: sur prepee; pulsrt
volum
reatments, to optimize their condition, if possible, before

pipicOe
aa
dn
Ii
OL
S5Slaughter et al. Management of Continuous-Flow LVADs
ermanent LVAD implant. These data also support thencreasing practice of implanting a LVAD earlier in therogression of heart failure. Most patients who are stable onnotropes in INTERMACS category 3 would be appropriateandidates who would likely benefit from LVAD therapy.utcomes from INTERMACS levels 4 and higher are under
valuation for appropriateness of support.Many of the patients considered for long-term LVAD ther-
py have important comorbidities that may limit functionality
Table 2 Pulsatile-Flow and Continuous-Flow Long-term Left VUnited States Food and Drug Administration Approvals and Ong
ManufacturerType of pummechanism
Pulsatile-flow devicesHeartMate XVE Thoratec Corp,
Pleasanton, CAElectric; pu
Thoratec PVAD Thoratec Corp,Pleasanton, CA
Pneumaticpump
Thoratec IVAD Thoratec Corp.,Pleasanton, CA
Pneumaticpump
Excor Berlin Heart, Berlin,Germany
Pneumaticpump
MEDOS VAD MEDOS MedizintechnikAG, Stolberg, Germany
Pneumaticpump
CardioWest TAH Syncardia SystemsInc., Tucson, AZ
Pneumaticpump
Continuous-flow devicesAxial-flow pumps
HeartMate II Thoratec Corp,Pleasanton, CA
Axial-flow pblood-imbearings
Jarvik 2000 Jarvik Heart Inc., NewYork, NY
Axial-flow pblood-imbearings
Heart Assist 5 Micromed CardiovascularInc., Houston, TX
Axial-flow pblood-imbearings
Incor Berlin Heart, Berlin,Germany
Axial-flow pmagnetic
Synergy CircuLite Inc, SaddleBrook, NJ
Axial-flow pblood-imbearings
Centrifugal pumpsHVAD HeartWare Inc, Miami
Lakes, FLCentrifugal
with hydbearing
DuraHeart Terumo Heart Inc, GrandRapids, MI
Centrifugalwith maglevitation
Levacor VAD World Heart Inc., SaltLake City, UT
Centrifugalwith maglevitation
EVAHEART LVAS EVAHEART USA,Pittsburgh, PA
Centrifugal
BiVAD, biventricular assist device; BTT, bridge to transplant; CE Mark,and Drug Administration; IDE, investigational device exemption; LVAD,Medical Device Agency (Japan); TAH, total artificial heart; UniVAD, univ
nd survival. Patients with multiple or severe non-cardiac con- s
itions that significantly limit quality or duration of life mayot be suitable candidates for LVAD implantation.
I.B. Patient mortality risk for undergoing LVADmplantation
nce a patient’s heart failure status indicates candidacy forVAD support, his or her ability to survive the implant
lar Assist Devices in Clinical Use and Status of European andlinical Trials
Type of support EU approvals FDA approvals
late LVAD CE Mark BTT DT
e BiVAD or UniVAD CE Mark PC BTT
e BiVAD or UniVAD CE Mark PC BTT
e BiVAD or UniVAD CE Mark
e BiVAD or UniVAD CE Mark
e TAH CE Mark BTT
ith LVAD CE Mark BTT DT
ith LVAD CE Mark IDE trial ongoingfor BTT
ith LVAD CE Mark IDE trial ongoingfor BTT
ithg
LVAD CE Mark
ith LVAD CE Mark trialongoing
micLVAD CE Mark IDE trial ongoing
for BTT
LVAD CE Mark IDE trial ongoingfor BTT
LVAD IDE trial ongoingfor BTT
LVAD Trial in Japancomplete; PMDApending
IDE trial for BTT
ity mark in European Economic Area; DT, destination therapy; FDA, Foodtricular assist device; PC, post-cardiotomy; PMDA, Pharmaceutical andlar assist device.
entricuoing C
ping
sher p
sac-typ
sac-typ
sac-typ
sac-typ
sac-typ
ump wmersed
ump wmersed
ump wmersed
ump wbearinump w
mersed
pumprodyna
pumpnetic
pumpnetic
pump
conformleft venentricu
urgery should be assessed. Whenever possible, LVAD im-

pecicficfcc
IAtssiagtfotl
bpsttriseon
ff
srwp8�whhTrgtmttmli
tw2t
S6 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
lant surgery should be elective and not emergent. This isspecially true for the DT indication because most patientsan be stabilized and their risks assessed and reduced beforemplant. Implantation of a long-term LVAD should not beonsidered for patients with irreversible major end-organailure, uncertain neurologic status, severe hemodynamicnstability, major coagulopathy, prolonged need for me-hanical ventilation, sepsis, or right-heart failure. Otheractors that may preclude implant include a “high-risk”lassification, unresolved psychosocial issues, and non-ompliance concerns.
I.B.1. Overall risk factors for operative mortalitynumber of investigators have developed operative mor-
ality outcome models based on a patient’s pre-operativetatus.23–26 Numerous factors influence outcome, but noingle factor or specific combination of factors have beendentified as definitive predictors of death. Most risk factorsre additive. Thus, composite risk scores can be used touide patient selection and treatment for pre-operative op-imization. Risk assessment for medical and surgical issuesor BTT and DT are nearly identical. Accurate assessmentf right-heart function is crucial for DT candidates becauseransplantation is not an option, and those who requireong-term inotropic therapy for RV support do poorly.
An analysis of the HeartMate XVE LVAD DT Registryy Lietz and Miller27 demonstrated that death before hos-ital discharge in patients receiving an implant as DT wastrongly influenced by worsening nutritional status, hema-ologic abnormalities, end-organ and right-heart dysfunc-ion, and the lack of inotropic use, factors that are alsoelevant to BTT. These pre-operative clinical characteristicsdentified patients who were at high risk for not survivingurgery. Pre-operative risk factors associated with the high-st risk of death were severe functional impairment, markersf global cardiac dysfunction, end-organ damage, and mal-utrition.
Lietz and Miller27 analyzed pre-operative clinical datarom 222 patients who received the HeartMate XVE LVAD
Table 3 INTERMACS Patient Profiles and Timeframe for Initiat
Profile # Description
1 “Crashing and burning”—critical cardiogenic shock2 “Progressive decline”—inotrope dependence with3 “Stable but inotrope dependent”—describes clinic
of intravenous inotropes (patients stable on teminotropes are within this profile).
4 “Recurrent advanced heart failure”—“recurrent” ra5 “Exertion intolerant”—describes patients who are
intolerant.6 “Exertion limited”—describes a patient who is abl
results within a few minutes of any meaningful7 “Advanced NYHA III”—describes patients who are
of comfortable activity, despite history of previo
IMTERMACS, Interagency Registry for Mechanically Assisted CirculAssociation.
or DT. They established a risk scoring system to estimate
urvival after implant. The multivariate analysis produced 9isk factors for 90-day mortality, which were assigned aeighted score (Table 4). The cumulative scores for eachatient were then used to determine the risk category: 0 to, low risk; 9 to 16, medium risk; 17 to 19, high risk; and19 was very high risk. The survival to hospital dischargeas 87.5%, 70.5%, 26%, and 13.7% for the low-, medium-,igh-, and very high-risk groups, respectively. Examples ofow a patient’s risk score is determined are provided inable 5. This risk score stratified patients based on operative
isk and identified the highest-risk patients (the “futile”roup) with an extremely low likelihood for survival. Pa-ients who initially present as high-risk or very high-risk areost likely to benefit from a period of optimization therapy
o attempt to lower their risk score (eg, coagulation, nutri-ion, renal function, right atrial pressure) and then becomeore suitable candidates for LVAD support. Patients with a
ow risk should be considered for prompt elective LVADmplant before their condition worsens.
We must point out that a limitation of this risk model ishat it was developed initially in only DT patients implantedith the pulsatile HeartMate XVE LVAD from 2002 to005. The risk model has not yet been validated with con-inuous-flow devices implanted for DT.
chanical Circulatory Support
Time to MCS
Within hoursing deterioration. Within a few days
ility on mild-to-moderate dosescirculatory support without
Within a few weeks
an “refractory” decompensation. Within weeks to monthstable at rest but are exercise Variable
some mild activity but fatiguel exertion.
Variable
lly stable with a reasonable levelompensation that is not recent.
Not a candidate for MCS
upport; MCS, mechanical circulatory support; NYHA, New York Heart
Table 4 Risk Factors for 90-Day Mortality and theWeighted Scores
Risk factor Score
Platelet count �148 � 103/�l 7Serum albumin �3.3 g/dl 5International normalization ratio �1.1 4Vasodilator therapy 4Mean pulmonary artery pressures �25 mm Hg 3Aspartate aminotransferase �45 U/ml 2Hematocrit �34% 2Blood urea nitrogen �51 mg/dl 2No intravenous inotropes 2
ing Me
.continual stabporary
ther thcomfor
e to dophysicaclinicaus dec
atory S

IOH�rrBcttobto
�db�namg
atehpamnb
IRLsfi
spedaHnatsrspom
oXR4attsii6pit
ructsas
S7Slaughter et al. Management of Continuous-Flow LVADs
I.B.2. Obesity paradoxbesity is common in patients with heart failure. In theeartMate II BTT and DT trials, a body mass index (BMI)40 kg/m2 was an exclusion criterion for study purposes. A
ecent report, however, showed that obesity had no delete-ious effects on outcome in LVAD patients and that a lowMI was associated with higher risk.28 Obesity is not aontraindication to using a continuous-flow LVAD, andhese devices can provide sufficient cardiac output supporto meet the metabolic demands of obese patients. Goodutcomes in obese patients will likely depend on the capa-ility of a LVAD to maintain adequate hemodynamics andhe freedom from comorbidities, such as infection, that mayccur more frequently in these patients.
Conversely, studies have shown that cachexia (a BMI22 kg/m2) is associated with a high risk for peri-operative
eath, often due to infection.28,29 Hence, nutrition needs toe improved before LVAD implant (a pre-albumin level15 mg/dl). It is equally important to maintain adequate
utrition after the implant surgery. Data from Lockard etl30 has shown that patients with a pre-albumin level of �15g/dl at 2 weeks after LVAD implant had a significantly
reater risk of dying in the hospital.In some cases, LVADs have been used in obese patients
s BTT eligibility, with the goal that during LVAD support,he obese patients will lose sufficient weight to becomeligible for transplant. In general, however, few patientsave achieved sufficient weight loss to qualify for trans-lantation. Providing hemodynamic support with a LVADs a means for weight loss should be undertaken with aultidisciplinary team approach that includes physicians,
urses, dieticians, exercise physiologists, and potentially,ariatric surgeons.
I.B.3. Assessment of RV functionV failure is a leading cause of morbidity and death afterVAD implant due to the inability of the RV to pumpufficient blood through the pulmonary circuit to adequately
Table 5 Examples of Destination Therapy Risk Scoring in Two
Risk factor [score]
Patient 1
Value
Platelet count �148 � 103/�l [7] 170Serum albumin �3.3 g/dL [5] 3.1INR �1.1 [4] 1.3Vasodilator therapy [4] YesMean PAP �25 mm Hg [3] 28AST �45 U/ml [2] 42Hematocrit �34% [2] 32Blood urea nitrogen �51 mg/dL [2] 55No intravenous inotropes [2] Inotropes used
Total scoreOperative risk category
AST, aspartate aminotransferase; INR, international normalization ra
ll the left heart. It is a major contributing factor to other f
erious adverse events such as bleeding, renal failure, androlonged hospitalization. RV function is a major consid-ration for both volume-displacement and continuous-flowevices. LV unloading with a LVAD should decrease RVfter-load by reducing pulmonary artery pressures (PAPs).31
owever, mechanical support may increase systemic ve-ous return to a myopathic right heart that is unable toccommodate the additional volume. Furthermore, reduc-ion in LV pressure can cause the interventricular septum tohift leftward, potentially causing disadvantageous geomet-ic changes in the RV that reduce septal contribution to RVtroke volume and exacerbate tricuspid regurgitation.31 Im-ortantly, RV failure after implant can be anticipated pre-peratively and improved with various therapies that opti-ize RV function.Historically, various studies have reported a wide range
f use of RVADs or biventricular support. In the HeartMateVE LVAS BTT study, 11% of 280 patients received anVAD.32 In the paracorporeal Thoratec VAD BTT study,8% of 213 patients received planned biventricular support,nd 17% more were converted to biventricular support withhe later addition of an RVAD.33 In the HeartMate II BTTrial, right-heart failure was defined as the need for RVADupport, or inotropic support for at least 14 days after themplant, or inotropic support starting after 14 days. Thencidence of right-heart failure in the BTT trial was 20%:% required RVAD support, 7% required extended inotro-ic support for more than 14 days, and 7% required use ofnotropes after 14 days of support.34 In the HeartMate II DTrial, there was a 4% use of RVADs.1
RV failure patients had increased length of stay andeduced survival compared with patients without RV fail-re. Thus, the incidence of RV failure in patients with theontinuous-flow HeartMate II is comparable to or betterhan previous pulsatile devices, but RV failure remains aignificant factor for morbidity and mortality. Perhaps thebility to adjust pump speed in real time, as guided byurface echocardiography to define RV and LV size and
ts
Patient 2
Score Value Score
0 220 05 4.2 04 1.3 44 Yes 43 24 00 40 02 36 02 53 20 No inotropes 2
20 12Very high Medium
P, pulmonary artery pressure.
Patien
tio; PA
unction, has contributed significantly to the ability to man-

at
fas�aIupcrbppa
bpappwmmac
Wps
cdCbiHHRi
ppwrtrjiwa
flp
tviv
I
PtAutbr
NonaimcoLwtrp
fagtan
S8 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
ge patients on the new continuous-flow pumps and tohereby reduce RVAD use.
Two recent studies have reported predictive modelsor RV failure after LVAD implant.35,36 One model usedweighted scale that included the need for vasopressor
upport, bilirubin �2.0 mg/dl, aspartate aminotransferase80 IU, and creatinine �2.3 mg/dl to predict the prob-
bility of RV failure and the need for RVAD support.36
n another study, a predictive algorithm for RVAD needsed the cardiac index, RV stroke work index, severere-operative RV dysfunction, creatinine level, previousardiac surgery, and systolic blood pressure.35 Patients atisk for post-operative RV failure should not necessarilye eliminated from LVAD support. However, the im-lanting team should promptly treat RV failure usingharmacotherapeutics and mechanical RV support, asppropriate or needed.
Low pre-operative RV stroke work index (RVSWI) haseen demonstrated to predict prolonged inotropic use afterulsatile LVAD implant, supporting the role of RVSWI aspredictor of RV dysfunction.37 In 1 study, inotropic sup-
ort �14 days post-operatively was required in 38% ofatients with a RVSWI �600 mm Hg � ml/m2 comparedith 29% of patients with a RVSWI 600 to 900 mm Hg �L/m2, and only 3% with a RVSWI �900 mm Hg �L/m2.38 RVSWI provides a quantitative measure of the
bility of the RV to generate pressure and flow and isalculated using this formula:
RVSWI (mm Hg � ml ⁄ m2)
� {[mean PAP (mm Hg) � mean CVP (mm Hg)]
� SV (ml)} ⁄ BSA (m2)
ith BSA as body surface area, CVP, as central venousressure; PAP as pulmonary artery pressure, and SV astroke volume.
An analysis of 484 patients in the HeartMate II BTTlinical trial demonstrated the following independent pre-ictors of RV failure: pre-operative ventilatory support,VP/pulmonary capillary wedge pressure ratio �0.63, andlood urea nitrogen �39 mg/dl.34 Univariate predictors alsoncluded a RVSWI �300 mm Hg � ml/m2, CVP �15 mmg, elevated BUN, and elevated white blood cell count. TheeartMate II trial found no difference in the incidence ofV failure in the heart failure patients with non-ischemic vs
schemic etiology.Other signs of poor RV function can be found with
re-implant echocardiography. Close attention should beaid to RV size, with particular caution extended to patientsho have a dilated, poorly contracting RV. Severe tricuspid
egurgitation also can be associated with early post-opera-ive RV failure. Some have advocated repair of the tricuspidegurgitation at the time of LVAD implant if its severity isudged to be more than moderate, either pre-operatively orntraoperatively by echocardiogram. Note that in patientsith RV dysfunction, setting the pump speed to achieve
ppropriate flow may be more challenging with continuous-
ow devices than with volume displacement (ie, pulsatile)umps.
Parameters to consider for evaluating right-heart func-ion are listed in Table 6. Issues related to the presence ofalvular heart disease are discussed in Section III. Morenformation on the management of RV dysfunction is pro-ided in Sections II.F., III.H., and IV.A.
I.C. Pre-operative assessment and optimization
re-operative optimization is targeted toward minimizinghe frequency and severity of adverse events after implant.
complete system assessment should begin immediatelypon referral for LVAD support. Table 7 outlines variousests and assessments that should be done in all patientsefore implant. Table 8 lists pre-operative goals in terms ofelevant metabolic markers.
utrition. Holdy et al29 report that “comprehensive pre-perative evaluation of the LVAD patient should include autrition assessment and formalized plan to initiate anddvance nutrition support while addressing the metabolicmbalances associated with heart failure.” Careful attentionust be paid to the nutritional status of any LVAD therapy
andidate before implant. Poor nutritional status is oftenverlooked and is a potentially modifiable risk factor inVAD candidates. Malnutrition is very common in patientsith advanced heart failure. If not improved, it increases
he risk of infection, decreases the body’s ability toecover after surgery, and is generally associated withoor outcomes.
Prospective LVAD patient assessment should be per-ormed by a team consisting of a dietitian, a pharmacist, andheart failure physician. Nutrition optimization should be-
in on initial presentation and continue throughout the en-ire peri-operative period. Patients with severe cachexia whore stable without worsening organ function should undergoutrition optimization before implant, if possible, generally
Table 6 Evaluating Right-Heart Function
Parameter Desirable valuea
RVSWI �300 mm Hg � ml/m2
Central venous pressure �15 mm HgTricuspid regurgitation Minimal to moderatePulmonary vascular resistance �4 Woods unitsTranspulmonary gradient �15 mm HgRV size
RVEDV �200 mlRVESV �177 ml
Need for pre-op ventilator support None
PVR, pulmonary vascular resistance; RV, right ventricle; RVEDV,right ventricular end-diastolic volume; RVESV, right ventricular end-systolic volume; RVSWI, right ventricular stroke work index.
aThese are conservative desired values indicating the least risk,and are not absolute cutoffs; pulmonary vascular resistance andtranspulmonary gradient will typically be reduced during left
ventricular assist device support.
wtawcc
s
em�d�tiswc
fpetppaamuat
Htbdlc
ultures,
S9Slaughter et al. Management of Continuous-Flow LVADs
ith an enteral feeding tube, even if surgery is delayed. Duringhis time, however, these patients must be carefully monitorednd the LVAD should be implanted promptly if their conditionorsens, even if complete nutrition optimization has not been
ompleted. A detailed pre-operative nutrition assessment forman be found in Appendix A.
General guidelines for nutrition management in LVAD-upported patients have been previously published.29 Mark-
Table 7 General Preoperative Assessment
Laboratory testsa
CBC with differential and platelet countComplete chemistry panelUric acidThyroid profileLactate dehydrogenasePT/PTT, INRPRA (if potential transplant candidate)Pregnancy test (HCG) for womenIron, transferrin, ferritinGlycosylated hemoglobinHeparin antibody only if clinically suspected, such as a platelet
count �150,000 or recent decrease of �20%Serotonin release assay (if heparin antibody-positive)Albumin, pre-albuminUrinalysis, culture, and sensitivity
AAA, abdominal aortic aneurysm; ABI, ankle-brachial index; AP, ancomputed tomography; EGD, esophagogastroduodenoscopy; FFP, fresh froratio; PRA, plasma renin activity; PRBC, packed red blood cells; PT, phormone; US, ultrasonography.
aIn addition to these tests, some centers check protein C, protein Smay be used to guide postoperative management. Other non-routine teenterovirus, nasal swab for Staphylococcus infection, peripheral blood c
Table 8 Minimal Pre-implantation Goals
Parameter Desired value
RenalBlood urea nitrogen �40 mg/dlSerum creatinine �2.5 mg/dlEstimated GFR �50 ml/kg/min
HematologyINR �1.2Hemoglobin �10 g/dlPlatelets �150,000/mm
NutritionalPre-albumin �15 mg/dlAlbumin �3 g/dlTransferrin �250 mg/dl
HepaticTotal bilirubin �2.5 mg/dLALT, AST �2 times normal
HemodynamicRight atrial pressure �15 mm HgPCWP �24 mm Hg
ALT, alanine aminotransferase; AST, aspartate aminotransferase;GFR, glomerular filtration rate; INR, international normalized ratio;PCWP, pulmonary capillary wedge pressure.
u
rs of severe malnutrition include a BMI �20 kg/m2, albu-in �3.2 mg/dl, pre-albumin �15 mg/dl, total cholesterol130 mg/dl, lymphocyte count �100, and purified protein
erivative skin test anergy. For patients with a pre-albumin15 mg/dl, enteral feedings are often helpful pre-opera-
ively and should be continued after implant until the patients taking adequate nutrition. Several recent reports have alsohown that patients with a pre-albumin �15 mg/dl at 2eeks after implant are at high risk of dying before dis-
harge.30
Diets should be liberal and include oral supplements,ood from home, and between-meal snacks. When possible,atients should take multivitamins, iron supplements, andrythropoietin. The pre-albumin level should be checkedwice weekly and should exceed 15 mg/dl before implant, ifossible. A nocturnal tube feeding may be useful in someatients to allow for more daytime activity, such as physicalnd occupational therapy. Heart failure patients often havepoor appetite due to poor perfusion, congestion, hepato-egaly, and inactivity and may benefit from appetite stim-
lants. Depression is also common in heart failure patientsnd may contribute to poor nutrition, but it can be effec-ively treated with antidepressants.
emodynamics. Pre-operative comorbidities are generallyhe result of acute or chronic low perfusion or congestion, oroth. Optimizing hemodynamics, especially increasing car-iac output, if possible, with inotropic and intra-aortic bal-oon pump support can improve a patient’s pre-operativeondition.
A pulmonary artery catheter 24 hours before implant is
dies Other
st X-ray (AP and lateral) Dental evaluation withpanorex imageotid Doppler if history of CAD or
50 years oldst/abdominal CT if previous chestr abdominal surgery
I if claudication history or diabetesominal US for AAA screen if �60ears old or presence of PADor colonoscopy within past 2 years
sterior; CAD, coronary artery disease; CBC, complete blood count; CT,sma; HCG, human chorionic gonadotropin; INR, international normalizedbin time; PTT, partial thromboplastin time; TSH, thyroid-stimulating
nti-cardiolipin antibodies to identify coagulation abnormalities thatmay be performed are rectal swab for vancomycin-resistantand plasma levels of free hemoglobin.
Stu
CheCar
�Che
oABAbd
yEGD
teropozen plarothrom
, and asts that
seful in most patients to assess the cardiac index and

vitwsHsIadvwp
gcsrRspphmioc
tgfszptppropri
RagcemGmUafwtd
stifshmplc
pioimclHhpr
GqhffdBb
Hptmiabfshuc
fLtvp
ii(ns
S10 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
olume status as well as to guide diuretic, vasodilator, andnotropic support. One of the main objectives is to reducehe CVP to 15 mm Hg or less. This will aid in reducing RVorkload and minimizing hepatic congestion and the pos-
ible need for an RVAD. When the CVP exceeds 20 mmg, ultrafiltration and inotrope and vasodilator therapy
hould be used; also consider temporary RVAD support.ncreasing the cardiac index with vasodilators, inotropes,nd using an intra-aortic balloon pump will improve con-itions for all organ systems. Because pre-operative use ofasopressor medications has been shown to be associatedith poor outcomes, these agents should be avoided whenossible.
Patients who present in cardiogenic shock may not beood candidates for an implantable LVAD. However, theirondition can be optimized with temporary support with ahort-term device as a bridge to decision.39–41 Paracorpo-eal biventricular support may be considered for BTT.42
ecent reports indicate that the planned use of biventricularupport with LVAD and temporary RVAD or with bilateralaracorporeal VADs vs delayed RVAD after LVAD im-lant improves outcomes in selected patients with right-eart failure or pulmonary hypertension, or both.43 Imple-entation of early mechanical support has been shown to
mprove the hemodynamic profile and end-organ functionf patients in cardiogenic shock sufficiently to allow suc-essful long-term LVAD support.
Medications that can lower pulmonary vascular resis-ance (PVR) and the improve cardiac index before sur-ery may be beneficial in reducing the incidence of RVailure after implant.44,45 Medications that have beenhown to reduce PVR include angiotensin-converting en-yme (ACE) inhibitors, hydralazine, nitroglycerin, nitro-russide, nitric oxide, sildenafil, prostaglandins, and ino-ropes (milrinone and dobutamine). Patients with highre-operative pulmonary pressures and normal right atrialressure (and thus high RVSWI) are actually at lowerisk of post-operative RV failure because findings dem-nstrate that the RV is capable of generating sufficientressure. Conversely, low PAP (mean �25 mm Hg) ofteneflects significant RV failure and is associated withncreased mortality.
enal function. Renal dysfunction is another predictor ofdverse outcomes in LVAD-supported patients.23,46–48 Ineneral, indicators associated with poor outcomes are areatinine level �2.5 mg/dl and BUN �40 mg/dl, or anstimated glomerular filtration rate (GFR) of �0.5 ml/kg/in (calculated using the new formula for estimatedFR),49 because serum creatinine can seriously underesti-ate the severity of renal impairment, or chronic dialysis.rine output as low as 20 to 30 ml/hour for 6 to 8 hours is
lso an identified risk factor for poor post-operative renalunction and death.25 Patients in the HeartMate II BTT trialere excluded if their creatinine level was �3.5 mg/dl or if
hey needed chronic dialysis; 11% of patients had some
egree of renal dysfunction after implant.7 pOptimizing renal function pre-operatively entails mea-ures to increase renal perfusion and reduce CVP. Diureticherapy may either improve or worsen renal function, depend-ng on the patient’s overall volume status and baseline renalunction. However, normalization of volume status is a criticaltep in reducing secondary pulmonary hypertension and right-eart dysfunction.50 Intravenous drips of loop diuretics may beore effective than an intravenous bolus administration in
atients who demonstrate diuretic resistance. Intra-aortic bal-oon pump support can improve renal function by increasingardiac output and renal perfusion pressure.
Renal dysfunction generally improves after LVAD im-lant if decreased GFR is due to low cardiac output beforemplant. In the HeartMate II BTT trial, patients with pre-perative BUN and creatinine values above normal hadmprovement after 6 months of support, from 37 mg/dl to 23g/dL for BUN, and from 1.8 mg/dl to 1.4 mg/dl for
reatinine.51 Evidence of renal dysfunction is not an abso-ute contraindication to use of a continuous-flow LVAD.owever, renal function may not improve in patients whoave sustained acute or chronic renal injury from poorerfusion or, more commonly, in patients with underlyingenal disease such as diabetes or chronic hypertension.
astrointestinal. Because the continuous-flow LVAD re-uires systemic anti-coagulation, its use in patients with aistory of gastrointestinal (GI) bleeding should be care-ully considered. Active GI blood loss should be assessedor 3 to 4 weeks before LVAD implant. Of 331 patientsischarged from the hospital on HeartMate II support forTT, 31 (9.4%) required blood transfusions due to GIleeding.52
epatic function. Hepatic dysfunction is associated withoor outcomes after LVAD implant.53 Hepatic dysfunctionhat is secondary to right-heart failure may improve withechanical support (LVAD or BiVAD), whereas cirrhosis
s predictive of poor outcome. Liver dysfunction is associ-ted with greater need for intraoperative and peri-operativelood transfusion, which can result in worsened right-heartunction and the need for RVAD support. Many centerscreen patients with clinical evidence of significant right-eart failure or serologic evidence of hepatic dysfunctionsing hepatic ultrasound imaging or liver biopsy to rule outirrhosis.
As with renal function, there is evidence that hepaticunction improves after implantation of a continuous-flowVAD.54,55 In the HeartMate II BTT trial, alanine amino-
ransferase, aspartate aminotransferase, and total bilirubinalues in patients with abnormal baseline parameters im-roved to normal over 6 months.51
Specific management strategies should be initiated tomprove hepatic function before a LVAD is implanted inndividuals with abnormal values for prothrombin timePT), partial thromboplastin time (PTT), and internationalormalized ratio (INR). Right heart pressure and PVRhould be decreased using combinations of drugs to reduce
re-load and after-load or ultrafiltration, or both. Consider-
atw
ocompaa
Ht(oaoa
CgmpIa
fatmpcfpcdrae
agiphivwaihdiae
Peetdf
PsTerfcmesOphf
Icifssf
ctbecspotfticfsi
tTo
Ntmcd
S11Slaughter et al. Management of Continuous-Flow LVADs
tion of an intra-aortic balloon pump or a temporary percu-aneous assist device to improve systemic blood flow is alsoarranted.Supplemental vitamin K may be beneficial in repletion
f vitamin K-dependent coagulation factors in chroni-ally malnourished patients, those treated with warfarin,r in individuals with baseline hepatic insufficiency. Ad-inistering vitamin K to normalize INR levels and stop-
ing all anti-coagulant and anti-platelet agents well indvance of surgery are critical to minimizing peri-oper-tive bleeding.
ematology. Thrombocytopenia and a low hematocrit arewo hematology parameters associated with poor outcomesTable 2). Patients should be thoroughly assessed for etiol-gy and to correct any abnormalities before implant. Inddition, type and cross-matches must be performed pre-peratively to prepare blood products for transfusion duringnd immediately after the operation.
oagulation. Similar to the assessment of a patient under-oing any major surgical procedure, attempts should beade to correct or improve clotting abnormalities in
rospective LVAD patients. At a minimum, the PT/PTT,NR, platelet count, and antibodies to heparin should bessessed.
Pre-operative abnormal coagulation is common in heartailure patients due to hepatic dysfunction and the use ofnti-coagulant or anti-platelet medications. When possible,hese medications should be stopped before implant. Vita-in K may be given to reverse the effects of warfarin. For
atients who are at high risk of pre-operative thrombosis, aontinuous infusion of heparin should be given as the ef-ects of warfarin are reversed. Infusion of fresh frozenlasma may also be used to improve coagulation defects. Aontroversial issue at present relates to the use of clopi-ogrel during the peri-operative period in patients who haveecently received a drug-eluting stent. Little data are avail-ble to guide this decision, thus the risks and benefits forach patient must be weighed.
Heparin-induced thrombocytopenia (HIT) is a clottingbnormality that warrants consideration for patients under-oing LVAD implant.56 Although not monitored routinelyn all patients, HIT should be assessed pre-operatively inatients with platelet counts �150,000 or in those have whoad a recent drop of �20%. Clinical manifestations of HITnclude a significant decrease in platelet count—even if thealue is within the normal range—or any thrombotic eventhile receiving heparin. Laboratory evaluation should includecoagulation profile and heparin antibody assay. It may also
nclude the thromboelastogram. Alternative anti-coagulants toeparin (eg, argatroban and bivalirudin) have been used anec-otally in LVAD-supported patients with HIT. Routine screen-ng of all patients can be misleading, as can regular laboratoryssays. The serotonin release assay is the most reliable test for
stablishing the diagnosis of HIT.57,58 beripheral vascular disease. Many LVAD clinical trials havexcluded patients with significant peripheral vascular dis-ase. Abdominal ultrasound imaging and determination ofhe ankle-brachial index may be warranted to evaluate theegree of disease in susceptible patients being consideredor LVAD support.
ulmonary function. Patients with severe obstructive or re-trictive pulmonary disease are not eligible for LVAD therapy.here are no absolute pulmonary function criteria for LVADxclusion, and severe cardiac dysfunction may preclude accu-ate assessment of pulmonary function.50 When pulmonaryunction testing can be performed reliably, and the forced vitalapacity, forced expiratory volume at 1 second, and carbononoxide diffusing capacity are all less than 50% predicted,
xclusion from LVAD implant should be considered. Thecreening scale for assessing post-implant survival devised byz et al24 determined that pre-implant mechanical ventilationresented the highest risk for a poor outcome. Other studiesave also determined that mechanical ventilation is a riskactor for RV failure.59
nfection. Limiting device-related infections remains cru-ial to improving long-term morbidity and survival withmplantable LVADs. “Adherence to evidence-based in-ection control and prevention guidelines, meticulousurgical technique, and optimal post-operative surgicalite care form the foundation for LVAD-associated in-ection prevention.”60
Patients with active systemic infection should not beonsidered for LVAD support because infection is one ofhe leading causes of morbidity and death. Implant shoulde delayed for patients with localized infections that can beffectively treated, if clinically feasible. Always exerciseaution in patients who are at increased risk of infection,uch as patients with established or suspected infections,rolonged intubation, cutaneous lesions at surgical sites, orther comorbidities, including multisystem organ dysfunc-ion, immunosuppression, poorly controlled diabetes, renalailure, malnutrition, or debilitation. Correcting as many ofhese factors as possible before device implant can min-mize the risk of infection and optimize long-term out-omes. Another consideration is checking an immuneunction assay and quantitative immunoglobulins to as-ess overall immunity and relative risk of opportunisticnfections.
Strict adherence to the basic principles of infection con-rol should be a primary goal of LVAD patient management.able 9 outlines measures to minimize the risk that a peri-perative infection will develop.
eurologic, psychosocial, and psychiatric considerations. Pa-ients with neurologic or psychiatric disease that compro-ises their ability to use and care for external system
omponents, or to ambulate and exercise, are poor can-idates for LVAD support.61 All patients with an audible
ruit or peripheral arterial disease, diabetes, or age �60 years,
scpoa
caPncacpsrai
I
S12 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
hould undergo a carotid ultrasound study to rule out signifi-ant stenosis or the presence of unstable plaque. Patients withrevious stroke also warrant computed tomography (CT) scanr magnetic resonance imaging (MRI) to establish a pre-oper-tive baseline study.
Psychiatric disorders, drug abuse, and other psychoso-ial issues must be investigated to assess the patient’sbility to understand and comply with care instructions.atients with known recent drug abuse and/or a history ofon-compliance may not be suitable. Adequate family/aregiver support, housing, and community infrastructurere additional determining factors for potential LVADandidates. Although not an absolute requirement, LVADatients should have family or friends nearby to provideupportive care when necessary. Patients must have aeliable means of transportation for follow-up visits andconvenient, reliable telephone service to call for med-
Table 9 Preoperative Infection Control Guidelines
Area Activity
Patient Selection ● Exercrisk,mg/d
All indwelling catheters ● Rotatcultu�36
Remote infections ● Asses● Exerc
urina
Placement and maintenance of central venouscatheters and monitoring catheters
● Pract● Educ● Use m● Use 2● Assur
unde● Cons
veno● Use a
to de
Administration of peri-op anti-biotic prophylaxiscustomized per institution’s flora andsusceptibility pattern
● Vancalter
● Rifam● Fluco● Gram
susce● Adjus
Patient preparation ● Scrubbefor
● Clip t
Prophylaxis against Staphylococcus aureus ● Nasaadmithen
BMI, body mass index; IV, intravenous; LVAD, left ventricular assist
cal help in an emergency.
II. Intraoperative considerations
Key Points● Moderate to severe aortic insufficiency and mitral
stenosis must be corrected during LVAD implant.● Inflow cannulas must be directed posteriorly toward
the mitral valve. Obstruction may result if the can-nula is directed or angled toward the septum or freewall or due to changes in position as the LV chambersize is reduced over time.
● Proper placement of the percutaneous lead is ofutmost importance for long-term prevention of in-fection and damage to wires. Tunnel the percutane-ous lead to maximize the amount of velour that isinside the body. It may be positioned in a gentle loop
hnique
tion with patients with conditions that increase infections obesity (BMI �40 kg/m2), malnutrition (pre-albumin �15C �10,000, or fever.
site every 72 to 96 hours. If patient is febrile, draw bloodl catheters should be new or replaced with new access sitebefore LVAD surgery.
al hygiene.tion with patients who have remote infections, such as sinus,t, bowel, or skin.
d promote good hand washing.se who insert and maintain catheters.l sterile barrier.orhexidine preparation for skin asepsis.dressings are occlusive and that moisture does not collect
ransparent dressings.plying a chlorhexidine-impregnated sponge at the centraleter site to maintain anti-sepsis at the insertion site.crobial- or anti-septic-impregnated central venous cathetersthe risk of catheter infections.
(15 mg/kg IV) 1 hr pre-op, then every 12 hrs � 48 hrs, oragent effective against gram-positive bacteria.00 mg IV) 1 to 2 hrs pre-op, then every 24 hrs � 48 hrs.(400 mg IV) pre-op, then every 24 hrs � 48 hrs.
ive coverage tailored to patient flora and/or institutionalty.s for renal and hepatic failure.
nt with anti-septic soap such as chlorhexidine the nightery and again the morning of surgery.gical area as close to the operative time as possible.
re for S aureus should be performed pre-op. If positive,mupirocin 2% nasal ointment the evening before surgery anddaily for 5 days.
WBC, white blood cell.
or tec
ise causuch al), WB
e theres. Alhours
s dentise caury trac
ice anate tho
axima% chle thatr the tider apus cathnti-micrease
omycinnativepin (6nazole-negatptibilit dose
patiee surghe sur
l cultunistertwice
device;

Teuce
I
TiaBrcv
IIcva
AdTcn
AtLsbvhe
apbfiFs
S13Slaughter et al. Management of Continuous-Flow LVADs
or arc, leaving some internal slack for accidentaltugs in the peri-operative period.
● Certain LVAD implant steps can be taken before initia-tion of cardiopulmonary bypass (CPB) to minimize CPBtime: (1) tunnel the percutaneous lead, and (2) anastomo-sis of the outflow graft to the ascending aorta.
● Before the patient is taken off CPB, air removalshould be conducted at low LVAD speeds. Thepatient should be weaned off CPB or at minimalCPB support (approximately �1 liter/min) beforeincreasing rpm speeds to permit complete filling ofthe LV (�10 mm Hg) and to prevent aspiration ofair around the inflow conduit.
● Initiate the pump at low speeds and make increasesslowly.
● Use care to protect and preserve RV function, espe-cially by not overstressing the RV. If RV dysfunctionoccurs, resulting in poor LVAD inflow, temporaryright-heart bypass can be used to provide blood flow tothe LVAD while transitioning from CPB. For moreprofound RV failure, a temporary RVAD should beconsidered and implemented expeditiously.
● Intraoperative echocardiography is essential foridentifying valvular pathology, intracardiac thrombi,and an atrial septal defect or patent foramen ovale(PFO). A PFO should be closed at the time of im-plant. Intracardiac thrombus identified in the leftatria or ventricle should be removed before LVADimplant. Echocardiography is critical for assessingLV chamber size, cannula position, septal shifting,and aortic valve opening—factors used to determineoptimal pump position and speed setting.
his section addresses some general intraoperative consid-rations that are relevant to the implantation of any contin-ous-flow LVAD and a number of recommendations spe-ific to the HeartMate II LVAS that are based on clinical
Table 10 Valve Issues
Issue Possible solution and comments
Aortic insufficiency Aortic insufficiency that is greater thabe partially over-sewn or the valveexpected post-operative aortic insufhigh left ventricular filling pressurespressures, reassessment of the degrweaning of cardiopulmonary bypass
Mitral regurgitation Generally does not require repair.Mitral stenosis Mitral stenosis to a moderate degree o
bioprosthetic valve.Tricuspid insufficiency Moderate to severe tricuspid insufficienc
This is especially important for patienperformed using annuloplasty repair (
Mechanical prostheticvalves
A mechanical prosthesis in the aorticclosure. The mitral valve generally d
xperience after completion of the clinical trials. d
II.A. Managing valvular heart disease
able 10 lists valvular conditions that should be consideredntraoperatively; and, where appropriate, potential solutionsre presented. Outcomes in patients in the HeartMate IITT trial with concurrent valvular procedures showed higher
isk with aortic procedures vs no effect on survival with tri-uspid or mitral procedures.62 Aortic, mitral, and tricuspidalve issues are described in detail the subsequent sections.
II.A.1. Aortic valve pathologyn the HeartMate II BTT trial, 12 of 281 patients underwentoncurrent aortic valve procedures, consisting of 8 aorticalve replacements and 4 with an over-sewn aortic valve orortic patch.62
ortic stenosis. Existing stenosis of the aortic valve usuallyoes not require correction before implanting the LVAD.he LVAD will decompress the LV and provide most of theardiac output. Therefore, aortic stenosis is generally insig-ificant with regard to pump performance.
ortic insufficiency. With continuous-flow devices, the pa-ient usually has minimal or no pulse pressure. The nativeV, although contracting, may not generate enough pres-ure to open the aortic valve. Aortic insufficiency (AI) maye present in both diastole and systole, resulting in rapidentricular filling and high pump flows. Thus, AI tends toave a significant effect on pump performance and thestimated flow rates.
The clinical effect of AI is related to the duration ofnticipated LVAD support. For very long-term LVAD sup-ort, for example, AI may represent a significant lesionecause AI is likely to progress over time. Commissuralusion of the aortic valve leaflets has been reported with anncreasing prevalence of AI during HeartMate II support.63
unction of the aortic valve should be monitored throughoutupport, especially in patients being considered for myocar-
derate degree must be corrected. The aortic valve leaflets canreplaced with a bioprosthetic valve. Note: The amount ofy may be underestimated pre-operatively in the presence ofe setting of substantially lower left ventricular fillingortic insufficiency must be performed immediately afterull pump support.
ter must be corrected with mitral valve replacement with a
ld be considered for repair to optimize right ventricular function.pulmonary hypertension. Tricuspid valve repair can be
or DeVega technique).n must be replaced with a bioprosthetic valve or patcht require replacement; consider greater anti-coagulation.
n a mocan beficienc. In th
ee of awith f
r grea
y shouts witha ringpositiooes no
ial recovery and device explant. On the other hand, for

pdg
savsortm
psss
watistcqmtogNpr
cpmqpipsfiv
Pwnmctts
mtto
I
MtUflEsamb
Miu5(meplvtpdwtr
Ecoctpt
I
Tpswefi
I
SeocIttm
S14 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
atients being supported for BTT with an expected shorturation, AI may be a less significant problem. Most sur-eons do not recommend treating mild AI.
AI may appear minimal before implant but become moreevere as the LVAD unloads the LV and ejects blood into thescending aorta, increasing the pressure differential across thealve. Studies have demonstrated that AI can become moreignificant over the duration of LVAD support, but is usuallynly mild to moderate.63,64 When AI is severe, the amount ofegurgitant flow may be reduced by lowering the pump speedo reduce the transvalvular pressure gradient,65 although this
ay not improve systemic perfusion.Moderate to severe AI warrants surgical repair or re-
lacement. There are two approaches. The first is partialtitching of the aortic valve leaflets, in which some surgeonsew the leading edges of the cusps together (the “Parktitch”) to eliminate most of the AI.66
The second is complete over-sewing of the outflow tract,hich can be done with a couple of approaches.67,68 One
pproach is to leave the leaflets intact and place a patch: sizehe opening with an aortic valve sizer, and put in a Hemash-eld (Boston Scientific, Natick, MA) circular patch usingtandard aortic valve suturing techniques. Care should beaken to make sure that the edges of the patch are below theoronary ostia. If a mechanical valve is in place, it is alsouick and easy to sew a patch to the sewing cuff of theechanical valve, thereby covering it and excluding it from
he blood flow. Another approach, which is an inexpensiveption, is to use the excess end of the HeartMate II outflowraft and trim it to appropriate size using a valve sizer.ote: A patient with an over-sewn aortic valve is com-letely dependent on the LVAD, and even short-term dis-uption of device function could be fatal.
If aortic valve replacement is necessary, use of a me-hanical valve is not recommended because of the increasedotential for thromboembolic complications. Thrombusay form sub-valvularly due to infrequent opening, inade-
uate strut washing, and stasis. Tissue valves are thereforereferred. Pump speed may need to be reduced to allowntermittent opening of the valve as long as adequate sup-ort can be provided. There have been reports of LVAD-upported patients with a bioprosthetic aortic valve in whombrosis or endothelialization of the bioprosthetic valve de-eloped and resulted in its functional closure.68–70
re-existing aortic mechanical valves. Although patientsere excluded from the HeartMate II BTT trial if they wereot converted to a bioprosthetic valve, a pre-existing aorticechanical valve is not considered an absolute contraindi-
ation to LVAD support. There is ongoing debate whethero leave the mechanical valve in place or replace it with aissue valve. The individual patient’s indications for LVADupport may dictate the course of action.
If a patient requires long-term LVAD support, then aechanical valve should be replaced with a tissue valve or
he outflow tract over-sewn as previously described becausehere may be a greater chance for thromboembolic events
ver an extended period. pII.A.2. Mitral valve pathology
itral valve stenosis. Mitral stenosis needs to be corrected atime of LVAD implant to maximize ventricular filling.62
nlike aortic valve stenosis, mitral stenosis will limit pumpow while maintaining a high left atrial pressure (LAP).levated LAP could cause persistent pulmonary hyperten-ion and RV dysfunction. Currently, valve replacement withtissue valve would be most appropriate. However, thereay be specific situations where a mitral valvuloplasty may
e indicated.
itral insufficiency. There is general consensus that mitralnsufficiency, in most cases, does not require repair in contin-ous-flow LVAD patients. In the HeartMate II BTT trial, onlyof 281 patients had concurrent mitral valve repair procedures
plus 4 in conjunction with other cardiac procedures).62 Mostitral insufficiency in end-stage heart failure is from annular
nlargement secondary to LV dilation. Once the LV is decom-ressed with the LVAD, the mitral regurgitation (MR) willikely improve. Although some have suggested that mitralalve repair can improve post-operative LVAD and LV func-ion, no surgical procedure usually is required for MR inatients being supported by a LVAD. Also, MR can be re-uced by increasing the speed of the pump when appropriate,hich may improve unloading of the ventricle. In cases where
he pump is removed after myocardial recovery, significantesidual mitral insufficiency should be repaired.
xisting prosthetic valves. Functioning bioprosthetic or me-hanical mitral prostheses generally do not require removalr replacement, although greater anti-coagulation should beonsidered to avoid thromboembolic risk. If anti-coagula-ion is discontinued or reduced due to bleeding events,atients are at an increased risk of valve thrombosis andhromboembolism.
II.A.3. Tricuspid valve pathology
ricuspid insufficiency. Because of the importance of im-roving early right-heart function, there is consensus thatevere tricuspid insufficiency should be repaired or treatedith valvular replacement, which would have an early ben-
ficial effect. Mild to moderate tricuspid regurgitation and aunctional valve would probably improve with a reductionn RV afterload that typically occurs during LVAD support.
II.B. Pre-clotting considerations
ome device conduits require pre-clotting. To avoid unnec-ssary bleeding from the LVAD conduits, the porous graftn the inflow and the outflow conduits must be thoroughlyovered with an adherent material. Users of the HeartMateI should meticulously follow the pre-clotting instructions inhe instructions for use. The inflow cannula assembly andhe outflow graft both need to be pre-clotted correctly andeticulously (Figure 2). Care must be taken to ensure that
re-clotting material is inserted along the graft down into

tcmflslcsut
(tme
I
DaHofmt
●
●
●
●
atlcfigsiistlaw
i
1
234
5
p
t
Fg ws th
S15Slaughter et al. Management of Continuous-Flow LVADs
he space between the graft and the metal junction of theonnector to the LVAD. Inserting material into this spaceay be accomplished more easily if the material remainsuid for a time after application; for example, albuminolution, followed by autoclaving, or cryoprecipitate, fol-owed by thrombin. If a react-in-place sealant is used, spe-ial care must be taken to deliver the sealant into thesepaces before the reaction is complete. The instructions forse for these materials should be closely followed to ensurehat the material adheres well to the porous materials.
Note: Hemostatic matrix materials such as SurgifloEthicon, Somerville, NJ) or FLOSEAL (Baxter Interna-ional, Inc., Deerfield, IL) should not be used because theseaterials do not produce a layer with sufficient strength to
nsure that the graft is sealed.
II.C. Pump placement
evices should be placed in the intended anatomic locations designed. As an example, we describe placement of theeartMate II, but similar recommendations also apply tother devices. The HeartMate II LVAD pump was designedor preperitoneal placement; that is, below the left rectususcle, above the posterior rectus sheath (Figure 3). Keys
o proper placement include:
The inflow cannula must point posteriorly toward the mitralvalve. It should not be pointing or angled toward the septumor free wall because this may cause partial occlusion of theinflow cannula, which may lead to poor flow into the LVADand possible hemolysis or thromboembolic complications.The placement of the inflow cannula should accommo-date anticipated reductions in LV chamber size that canoccur over time.The position of the inflow cannula should be assessed
igure 2 (Left) Inflow cannula pre-clotting must ensure coatingraft. (Right) Scanning electron microscopy after explantation sho
before and after chest closure. s
The outflow graft should be pulled tight when estimatinglength for attachment to the ascending aorta in an end-to-side fashion.
During placement of the silastic cuff on the LV apex, properttention must be given to the heavy green ligature that is usedo secure the inflow cannula. The green ligature should beoosened and hanging freely before the cuff is attached. Theuff should be rotated so that the open portion of the ligature isacing upward and is easily accessible after the inflow conduits in position. A hemostat or Rommel should be placed on thereen ligature to isolate it from the other suture that is used forecuring the cuff to the epicardium. Once the inflow cannula isn place, the green ligature is tied tightly around the cuff andnflow cannula to secure its position. Do not cross the ligatureuch that the ligature will cut the silastic cuff when it is it isightened. It may also be necessary to place an additionaligature between the green ligature and the felt portion of thepical sewing ring to reduce bleeding from the holes throughhich the green ligature passes.The sequence of surgical steps for positioning the pump
ncludes:
. Create a sternotomy with a 4- to 6-cm extension in theupper midline.
. Incise the left anterior rectus fascia.
. Elevate the left rectus muscle.
. With the heart beating, select the location on the dome ofthe diaphragm for the inflow cannula.
. Set the pump below the left rectus muscle, anterior to theposterior rectus sheath. No opening is made in thediaphragm.
A detailed description for the entire surgical implantrocedure has been published by Thoratec.71
Preperitoneal placement of the HeartMate II requireshe dissection of a pump pocket that is significantly
een the convolutions and at the junction of the hardware and theat the pre-clotting material has not completely covered the graft.
betw
maller than with the HeartMate XVE. In most patients in

tpa
I
PitsptspcpoTge
t
1
2
Ispcslw
Stmm
I
Ib
(below
S16 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
he BTT trial, the pump was placed in the preperitonealosition, although there are anecdotal reports of intra-bdominal placement.
II.D. Percutaneous lead placement
roper placement and externalization of the percutaneous leads of utmost importance to minimize infection and damage tohe percutaneous lead. Planning for the percutaneous lead exitite location should begin well before the operation. Whenossible, the site should be selected with the patient standing;his will help expose anatomic factors and limitations. Siteelection might also involve patient input, with a discussion ofatient habits and preferences such as waistband or clothingonsiderations. In general, the distance between the pumpocket and exit site is maximized to allow the greatest portionf the velour covering to be within the subcutaneous tissue.he percutaneous lead should exit the pump housing with aentle curve. Sharp bends or kinks may result in damage to thelectrical wires or data cables within the lead (Figure 4).
There are two main techniques for tunneling the percu-aneous lead:
. The percutaneous lead is tunneled in a U-shape, whichincreases the amount of velour covering within the subcu-taneous tissue (Figure 5A). The tunneling instrument bentinto a U-shape allows the lead to be brought downwardtoward the naval, and then back upward to the exit site
Figure 3 Preperitoneal placement of the HeartMate II pump
at the midclavicular line below the right subcostal margin. I
. The percutaneous lead is positioned in a gentle loopnear the midline leaving some internal slack for acci-dental tugs and to avoid tight bends (Figure 5B). AVicryl (Ethicon. Somerville, NJ) suture is placedaround the percutaneous lead and through the perito-neum to secure the loop into position. This methodmaximizes the length of velour covering within thesubcutaneous tunnel and is a preferred method bysome of the most experienced surgeons.
The exit site can be prepared with the circular skin knife.f a circular skin knife is not used, then the size of the exitite created by a punch or incision should be as small asossible. A small exit site minimizes exposure of the sub-utaneous tissue and reduces tension on the skin. Therehould be approximately 1 to 2 cm of the velour-coveredead outside of the skin exit. The lead must be stabilizedith one of several external stabilizing methods.As is emphasized in the post-operative management in
ection IV, immobilizing the percutaneous lead is impera-ive. Immobilization reduces exit site trauma, which pro-otes wound healing and tissue ingrowth, and this mini-izes the risk of infection.
II.E. Cardiopulmonary bypass
ssues surrounding CPB during LVAD implantation haveeen covered in detail previously and should be reviewed.10
the left rectus muscle and above the posterior rectus sheath).
n addition, information related to the transition from CPB

tIafspta
Ctgsp
Lp
I
BaT
otacoaftttrC
aiLhvHincb
FT avoid
S17Slaughter et al. Management of Continuous-Flow LVADs
o the HeartMate II implantation is contained in SectionII.F, which follows. In general, adjusting inotropic andfterload-reducing drugs before CPB can maximize RVunction and reduce PVR while optimizing systemic perfu-ion pressure. Prolonged CPB can have deleterious effects,articularly coagulopathy and inflammatory responses con-ributing to systemic hypotension, pulmonary hypertension,nd resultant right-sided circulatory failure.72
Certain LVAD implantation steps can be taken beforePB is initiated to minimize bypass times. These include
unneling the percutaneous lead, completing the outflowraft anastomosis, and positioning the pump, if the patient istable. Generally, CPB is used during apical coring andlacement of the inflow cannula within the ventricle.
Although a few experienced surgeons have implantedVADs using off-pump techniques, the safety of these ap-roaches have not been validated for widespread use.73–75
II.F. De-airing and transitioning from CPB
efore the LVAD is activated, all air should be removednd the left heart should be readily filling with blood.
igure 4 The percutaneous lead must be tunneled without sharphe insert shows a bend radius that is too sharp, which should be
ransesophageal echocardiography should be used through- c
ut the de-airing and LVAD startup procedures to identifyhe presence of air in the LV or aorta. For the HeartMate II,ir is removed from the LV and pump through the Luer lockonnection on the outflow cap. Air is expelled from theutflow graft by partially releasing the cross-clamp andllowing backflow from the aorta. Once all air is removedrom the LV pump and the outflow graft, the graft is at-ached to the pump. Before attachment, however, thehreads of the graft and pump should be examined and anyhrombus should be removed. When necessary, the hearthythm is cardioverted and blood volume is shifted from thePB circuit to the patient’s circulation.
De-airing is continued during startup of the LVAD withcross-clamp on the outflow graft, and a needle is placed
nto the highest portion of the outflow graft. Elevating theV apex can aid in the removal of air from the heart;owever, this should not be done after the LVAD is acti-ated because there is a risk of air entrainment. With theeartMate II set at the lowest speed setting (6,000 rpm),
nitiate pumping while continuing de-airing through theeedle. CPB flow is decreased, followed by removal of theross-clamp from the graft. With an adequate volume oflood moving through the LV and LVAD, there should be
The large illustration shows an acceptable bend radius of the lead.ed.
bends.
ontinuous blood flow through the needle vent.

tiw
Tcos�taoapbb
Lteeeitw
●
●
●
●
Nhttca
I
PefbtLcaimab
●
●
●
Fta
S18 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
A temporary ultrasonic flow probe may be used to de-ermine LVAD flow at the lower speed (flow �3 liters/mins not estimated). Most surgeons do not use a LV vent andill vent through the outflow graft.Initiate the pump at low speeds; increase speeds slowly.
he use of higher speeds (eg, about 8,000 rpm) beforeompletely filling the LV and coming off CPB is not rec-mmended because it can lead to entrainment of air. CPBupport should be stopped and the LV should be full (LAP10 mm Hg) before a higher pump speed is used. Flooding
he chest with carbon dioxide, blood, or saline during de-iring reduces air entrainment. Transesophageal echocardi-graphy should be used to assess for air in the LV or aorta,nd for LV size and septal position to determine initialump speeds. Where cardiac function is adequate, CPB cane completely discontinued to allow thorough de-airingefore the device is activated.
Some centers have found that direct measurements ofAP are useful in setting pump speeds and assuring that
here is adequate RV output. Only centers with routinexperience in placing and using direct LA monitoring cath-ters should attempt this. If an LA catheter is placed, usextreme caution to avoid sucking air into the LA through thensertion site and to avoid flushing air into the LA directlyhrough the LA catheter. There is also a risk that tamponadeill develop after the catheter is removed.A straightforward method for de-airing is:
Before connecting the outflow graft to the pump, allowblood to fill the pump from the LV, temporarily releasethe cross-clamp on the outflow graft to fill the graft withblood from the aorta, and then attach the screw ringconnector on the graft to the outflow of the pump.
igure 5 (A) The percutaneous lead is tunneled with a U-shapeissue. (B) A gentle loop, with care to avoid tight bends, is creatmount of velour covering exposure to the subcutaneous tissue.
Insert a needle in the outflow graft at the highest point.
Look for air on the echocardiogram.If no air is observed, remove the clamp from the outflowgraft (de-air through outflow graft).
ote: Assure that the porous areas of inflow conduits thatave not been pre-clotted are completely covered withhe pre-clotting material and the pump is sealed properlyo avoid entraining air into the pump through the inflowonduit. See Section III.A.3 for pre-clotting consider-tions.
II.G. Coagulopathy and bleeding
ost-operative bleeding is one of the most frequent adversevents after LVAD implant. It can contribute to right-heartailure, infection, and a number of adverse effects related tolood transfusion. Owing to the comorbid conditions andreatments related to heart failure, patients undergoingVAD implant are highly susceptible to developing seriousoagulopathy. It is important to withhold any anti-platelet ornti-coagulant medication for 4 to 7 days before the LVADs implanted and attempt to normalize INR before surgery toinimize the risk of bleeding requiring reoperation. There
re a number of intraoperative measures that can minimizeleeding:
Minimize CPB time to reduce the coagulopathic effect ofextracorporeal circulation.Minimize dissection and practice meticulous surgicaltechnique for hemostasis.Normothermia should be maintained by keeping the roomtemperature as high as tolerable, and CPB temperature
rease the amount of velour covering exposed to the subcutaneoushe percutaneous lead before it is tunneled, which maximizes the
to inced in t
should be adjusted to normal body temperature.

●
●
●
●
●
●
●
Id
Mraio�TaascpdiRcMoosh�
trtbpnL
�RCTtItd
gdoistLi
I
IdfltaBdspHs
orirCwuflrt
Fcas
S19Slaughter et al. Management of Continuous-Flow LVADs
When the apical cuff is attached in an area of friablemyocardium, felt reinforcement is recommended.Dissection of the pump pocket should be minimal, withcareful cauterization of potential bleeding sites.Use autologous blood transfusion and ensure that ade-quate blood products for transfusion are readily availableduring the implant procedure.Platelets should be transfused in patients with thrombo-cytopenia; some centers preemptively transfuse platelets.Whole blood and plasma may be used to prime the CPBsystem in patients who are anemic or who have persistentelevation of liver enzymes or an elevated INR.Aminocaproic acid may be given after CPB is complete.Some centers use a thromboelastogram for intraoperativemanagement of coagulation factors.
II.H. Intraoperative management of RVysfunction
anagement of RV dysfunction should focus on preventionather than treatment. The tricuspid valve should be evalu-ted and repaired, if necessary. If RV dysfunction is due toschemia, consider revascularization. Avoid RV volumeverload and maintain CVP �16 to 18 mm Hg. If CVP is10 mm Hg, some volume may be given to improve flow.he use of carbon dioxide in the operative field may reduceir embolism, which is believed to contribute to intraoper-tive RV dysfunction. Normal ventilation and oxygenationhould be maintained to avoid pulmonary vasoconstrictionaused by acidosis or hypoxia. Milrinone, epinephrine, iso-roterenol, or vasopressin can be used with moderate RVysfunction. The need for or use of vasopressor agents mayncrease the risk of significant RV failure and need for anVAD. Inhaled nitric oxide can reduce PVR, and someenters have found that inhaled Flolan (GlaxoSmithKline,iddlesex, UK) is effective and less expensive than nitric
xide.76–79 Pacing can be used if the heart rate is notptimal. High pump speeds that cause leftward septal shifthould be avoided. Leaving the sternum open for 24 hoursas been reported to help reduce CVP in patients with CVP16 mm Hg but there is an increased risk of infection.If RV failure results in poor flow to the LVAD, short-
erm intraoperative right-heart bypass can be established toeduce the load on the RV and deliver oxygenated blood tohe LVAD.80 This can be done by returning part of thelood from the CPB circuit through a cannula inserted in theulmonary artery or LA through the right superior pulmo-ary vein. This technique allows adequate filling of theVAD without requiring excessive right-heart work.
If in spite of these interventions if the cardiac index is2.0 liters/min/m2 and the CVP �20 mm Hg, a temporaryVAD should be considered before leaving the OR. AentriMag (Levitronix, Waltham, MA) or a paracorporealhoratec VAD (Thoratec Corp., Pleasanton, CA), are two of
he most commonly used devices for temporary RV support.n assessing the need of an RVAD, the proper function ofhe LVAD must be confirmed. Use the echocardiogram to
etermine if the LV is being unloaded or not and to help puide positioning of the inflow cannula, which should beirected toward the mitral valve and not toward the septumr lateral wall. The HeartMate II pump speed should be setn a range that provides a sufficient level of cardiac outputupport (i.e., usually 8,600 to 9,800 rpm). High pump speedhat causes leftward septal shift or collapse of the LV andA should be avoided. Finally, the outflow graft should be
nspected to ensure that there is no obstruction or kinking.
II.I. Intraoperative echocardiography
ntraoperative echocardiography is a standard procedureuring LVAD implant for assessing LV, RV, and valvularunction, for detecting the presence of a PFO,81–84 and forocating intracardiac thrombi. Detecting and removing in-raventricular thrombi before pump insertion is critical tovoiding thrombi entry into the pump when it is started.ecause detection of intraventricular thrombi with echocar-iography is not completely reliable, visual inspectionhould be performed. Intraoperative echocardiography alsolays a critical role in determining optimal pump speed.ow to use echocardiography as a guide for setting pump
peed is described in Section V.A.3.Some centers visually inspect the atrial septum to rule
ut PFO because of a significant incidence of false-negativeesults in pre-bypass examinations (including bubble stud-es). If direct inspection is not done, it may be necessary toepeat the bubble study after implant and weaning fromPB. With the left heart decompressed and the right heartorking and loaded, a previously undetected PFO may benmasked and significant shunting may be seen by color-ow Doppler and bubble study (Figure 6). It is important toepair a PFO to prevent right-to-left shunting and, poten-ially, hypoxemia after implant.
igure 6 This transesophageal echocardiogram shows signifi-ant flow by color Doppler across a patent foramen ovale (PFO)fter the left ventricle was decompressed by left ventricular assistystem support. The PFO was not apparent in the pre-bypass
eriod due to the previously high left atrial pressure.
Ic
Tttlit
●
●
●
●
●
●
●
●
(tIHrHss
IH
TidTpapads
1
1
1
1
ro
I
S20 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
II.J. Replacing a HeartMate XVE LVAD with aontinuous-flow LVAD
he pulsatile-flow HeartMate XVE LVAD can be replaced athe end of its pump life with a continuous-flow LVAD. De-ailed information on exchange techniques has been pub-ished.85–88 In this section, we describe a procedure for replac-ng the device with a HeartMate II LVAD, although similarechniques could be used for any continuous-flow LVAD:
A redo sternotomy approach is recommended.The patient is placed on CPB. Alternative cannulation strategiesmay be used, such as femoral or axillary cannulation.The apical sewing cuff from the HeartMate XVE is usu-ally retained.The inflow cannula of the HeartMate XVE is removed.The inflow cannula from the HeartMate II LVAD isplaced through the old silastic cuff.The HeartMate II outflow graft is beveled and anasto-mosed back to the aorta, or alternatively, end-to-end to aremnant of the HeartMate XVE outflow graft (see below).The new HeartMate II percutaneous lead is externalizedthrough a new sub-cutaneous tunnel and exit site, whichcan be to the left upper quadrant to avoid possible con-tamination from the old site.Pump pocket drains may be required for the residualspace left by the HeartMate XVE. This pocket shouldeventually close. Sometimes removing part or the entireold fibrous capsule from the HeartMate XVE will dimin-ish the potential space difference.
The outflow graft on the HeartMate II device is smaller16 mm) than the HeartMate XVE aortic graft (20 mm), buthey can be sewn together end-to-end. The HeartMateI grafts should be beveled to accommodate the largereartMate XVE graft. This technique will also work if
emoving the HeartMate XVE graft and attaching theeartMate II back to the aorta. Alternatively, a linear down-
ize of the aortotomy can be used. De-airing issues areimilar to those described in Section III.F.
II.K. Exchanging a HeartMate II LVAD with aeartMate II LVAD
he HeartMate II LVAD may require exchange due tonfection of the percutaneous lead or pump, irreparableamage to the percutaneous lead, or pump thrombosis.87
he connections from the inflow and outflow conduits to theump have been designed to allow exchange of the pumpnd percutaneous lead only. The exchange can be accom-lished without entry into the chest cavity, and the inflownd outflow conduits are left in place unless there is evi-ence that these components should also be exchanged,uch as obstruction due to thrombosis. For this procedure:
1. Establish femoral-femoral or axillary-femoral cannula-tion for CPB.
2. Make a left subcostal “chevron” incision over the area
of the pump.3. Expose and dissect free the connections of the inflowand outflow conduits and a portion of the outflow graft.A sufficient area of the graft is exposed for cross-clamping when the device is removed. The screw ringconnectors on either side of the pump must be acces-sible to facilitate detachment and removal.
4. Place the patient into the Trendelenburg position andinitiate CPB.
5. Cross-clamp the outflow graft and detach the screw ringconnectors.
6. Divide the percutaneous lead and remove the pump.7. Place the new pump in the same position and attached
with the screw ring connectors.8. Externalize the new percutaneous lead in a new sub-
cutaneous track.9. De-air the pump with a needle in the outflow graft.0. Turn on the pump on at a low speed setting (about
8,000 rpm or less) while the de-airing needle and cross-clamp are in place.
1. After all air has been removed and confirmed withechocardiography, remove the needle from the graftand remove the cross-clamp.
2. Slowly wean off CPB while gradually increasing the pumpspeed to about 9,000 rpm, depending on patient conditions.
3. Irrigate the entire surgical area with an antibiotic solu-tion and close all incisions in standard fashion.
HeartMate II exchange can be easily accomplished withapid recovery from the exchange surgery.87 Routine post-perative care is provided.
V. Post-operative patient management
Key Points● A patient’s RV function can be affected by pump
speed. Avoid setting the pump speed too high or toolow.
● To avoid severe post-operative bleeding, anti-coagula-tion should be completely reversed after CPB. Routineuse of heparin is not indicated immediately after theLVAD is implanted. Patients are usually anti-coagu-lated with warfarin and anti-platelet agents (aspirin)when they are able to take oral medications.
● Mean arterial blood pressure should be maintainedbetween 70 and 80 mm Hg and should not exceed 90mm Hg. In the early post-operative period, an arterialcatheter is used to monitor blood pressure. After thecatheter is discontinued, the most accurate non-invasivemethod is with Doppler and a sphygmomanometer.
● A proper balance of LV pressure and pump speed isdesirable. This is typically accomplished with apulse pressure of 10 to 20 mm Hg and the aorticvalve opening approximately once every 3 beats.Echocardiography may be used to confirm idealpulse pressure and aortic valve opening frequency.

TpmflRbe
I
Gfs
●
●
●
●
●
●
I
Actiaeitw2vmftl2H
ISAurscbie
s
S21Slaughter et al. Management of Continuous-Flow LVADs
The presence of a dicrotic notch in the arterial linealso signifies aortic valve opening.
● Self-care should stress rigorous adherence to aseptictechnique for exit site care and immobilization of thepercutaneous lead.
he post-operative management of continuous-flow LVADatients in most instances is quite similar to the manage-ent of all patients after major cardiac surgery. Continuous-ow LVAD patients have special considerations related toV function and volumes, anti-coagulation and bleeding,lood pressure monitoring and management, and patientducation, which are described the subsequent sections.
V.A. RV function
eneral considerations for evaluating and managing RVunction and setting the pump speed in the post-operativeetting include the following:
Avoid setting the pump speed so high that it causes asignificant leftward septal shift and abnormal RV geom-etry, which can adversely affect RV function. High pumpspeeds also can collapse the LV and obstruct flow throughthe LVAD inlet cannula draining the LV. See SectionV.A.3 regarding proper pump speed settings.Because of the potential for large volume shifts in theearly post-operative period, echocardiography should beperformed routinely because these volume changes alonemay cause changes in RV and LV function.How often the aortic valve needs to open is debated. Acommon practice aims to adjust pump speed so that theaortic valve opens every second or third beat. This frequencyreduces the risk of aortic valve thrombosis and at the sametime ensures that the LV is reasonably loaded and not nearcollapse. In some patients, however, the aortic valve will notopen even at low pump speed due to poor LV function.There are insufficient data to make firm conclusions aboutthe long-term effects of this phenomenon. Although long-term mechanical circulatory support with the aortic valveremaining closed without apparent negative clinical effecthas been reported, there are also reports of aortic valvefusion63,89,90 and anecdotal reports of aortic valve thrombusdeveloping on the non-coronary cusp.
Table 11 Postoperative Anti-coagulation Guidelines for the H
Timing Action
Before leaving OR Completely reverse the anti-coaguImmediate post-op period Generally, no action. Patients wit
fibrillation, history of LVA or LADay 2 to 5 Once there is no evidence of blee
with a target range for the INRDuration of support Maintain on aspirin and warfarin,
INR, international normalized ratio; IV, intravenous; LA, left atrium; Lroom.
If a patient is clinically decompensating (signs of poorforward flow or right-heart failure), consider a repeatechocardiogram and reevaluate pump speed and also forpossible tamponade.When the pump speed is set, the RV should be assessed tosee if it becomes dilated and hypocontractile at high or lowspeeds. Use extreme care when increasing pump speed toassess RV dysfunction, because once the RV begins to showsigns of failure it can be very difficult to reverse.A sign of poor LV unloading in some patients is the amountof MR. If the patient has severe MR, consider increasing thepump speed and evaluating inflow and outflow position.
V.B. Anti-coagulation
nti-coagulation therapy is required during support withontinuous-flow LVADs to avoid thrombotic complica-ions. However, results from the HeartMate II BTT trialndicate that anti-coagulation requirements for this therapyre less than was initially believed. Early in the BTT trialxperience, anti-coagulation therapy was aggressive andncluded the optional post-operative use of intravenous dex-ran, followed by intravenous heparin as a transition to oralarfarin and anti-platelet therapy. The target INR range was.5 to 3.5.91,92 However, results from the clinical trial re-ealed that the incidence of thrombotic events is very low—uch lower than bleeding—which remains one of the most
requent adverse events.1,7,8 Other studies have confirmedhis observation, which has resulted in reduced anti-coagu-ation therapy at the most experienced centers.52,93–95 The009 revised proposals for anti-thrombotic therapy duringeartMate II support are presented in Table 11.
V.B.1. Titrating anti-coagulationtarting anti-coagulation too early is a common mistake.dequate hemostasis should be achieved before anti-coag-lation is initiated. Modification of the anti-coagulationegimen may be required in the face of changing clinicalituations. If LVAD flow remains low (�3.0 liters/min),onsider increasing anti-coagulation. If there is a risk ofleeding, consider decreasing the warfarin dose and increas-ng or maintaining anti-platelet medications. Anti-plateletffect may be confirmed with laboratory studies.
In most cases, the use of intravenous heparin as a tran-ition to long-term warfarin therapy in the early post-oper-
te II Based on Results From the Clinical Trial
r indications for anti-coagulation therapy, such as atrialbus, or low LVAD flow should be treated with anti-coagulants.
nd the chest tubes have been removed, begin warfarin therapyto 2.5. Also begin aspirin at a dose of 81 to 325 mg daily.
ventricular aneurysm; LVAD, left ventricular assist device; OR, operating
eartMa
lation.h othethrom
ding aof 1.5
VA, left

aeohhapwLtu
cHtcIa2wapuaa
bihttt
stobbtfugpTTwero
ISmcocfs
I
TLctwostTvppac
flatbpaaepmmad
avjioaaspI
vwieio
dbm
I
Et
S22 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
tive period is not necessary. In a recent study by Slaughtert al96 of 418 patients, 300 (72%) who had sub-therapeuticr no heparin therapy before warfarin was begun did notave an increased risk of thromboembolic events; therefore,eparin may not be needed in most cases. However, therere some clinical conditions of higher thrombotic risk whereost-operative heparin may be indicated in the transition toarfarin therapy, such as small patients who have lowVAD flow rates, a small ventricle, previous stroke or
ransient ischemic attack, chronic atrial fibrillation, or doc-mented LA or LV thrombus.
In a recent study by Boyle et al52 of long term anti-oagulation therapy in 331 outpatients supported by theeartMate II, the risk for thromboembolism was also shown
o be much lower than that of bleeding. This study con-luded, “the risk of thrombotic events increases with anNR � 1.5 while the risk of hemorrhagic events is presentt all INR ranges and is particularly increased with INRs �.5.” Therefore, current recommendations are to adjust thearfarin dose to achieve a target INR of 1.5 to 2.5. In
ddition to warfarin, patients should also be given anti-latelet therapy, such as aspirin (81 to 325 mg daily). These of dipyridamole was optional in the trial and variedmong centers; thus, it is no longer part of the standardnti-coagulation and anti-platelet algorithm.
Anti-coagulation and anti-platelet therapy may need toe adjusted for some clinical conditions. Some types ofnfection, especially bacteremia, are associated with aigher incidence of stroke due to increased endothelial ac-ivation and platelet aggregation.97 Therefore, increased an-i-platelet therapy may be warranted during systemic bac-erial infections.
GI bleeding is a complication of continuous-flow pumpupport that may be severe and require that anti-coagulationherapy be reduced or discontinued.98–101 Two hypothesesf the cause of GI bleeding during LVAD support that areeing studied are acquired von Willebrand syndrome causedy increased shear stress,102–104 and reduced pulsatility ofhe continuous-flow device.101 There are anecdotal reportsrom some centers that have decreased the speed of contin-ous-flow LVADs with the hypothesis this would create areater pulse pressure and reduce shear stress through theump and might potentially reduce the risk of GI bleeding.hese practices have not been studied in a series of patients.here are also anecdotal cases where patients have beenithout warfarin and/or asprin for extended durations after
pisodes of persistent GI bleeding. The risks and benefits ofemoving warfarin or antiplatelet therapy should be thor-ughly assessed and discussed with the patient.
V.B.2. Thromboelastographyome experienced centers are using thromboelastography toanage and adjust anti-coagulation therapy, but its use in
ontinuous-flow LVAD patients is insufficient to make rec-mmendations. Teams should be well trained to ensureonsistent results. The thromboelastogram is initially per-ormed daily to assess anti-platelet needs until stable and
atisfactory levels are achieved. bV.C. Blood pressure monitoring and management
he major hemodynamic effects of a continuous-flowVAD are increases in diastolic pressure and flow.105 Be-ause these devices pump continuously throughout the en-ire cardiac cycle, aortic flow is also present during diastolehen normal pulsatile flow is absent. When the pump speedf a continuous-flow LVAD is increased, the diastolic pres-ure rises, the systolic pressure remains fairly constant, andhe pulse pressure (systolic � diastolic) is greatly reduced.he pulse pressure is influenced by LV contractility, intra-ascular volume, pre-load and after-load pressure, and byump speed. Therefore, assessment of the arterial bloodressure values and waveform gives valuable informationbout the physiologic interaction between the LVAS and theardiovascular system.
Owing to the reduced pulse pressure during continuous-ow LVAD support, it is often difficult to palpate a pulsend measure blood pressure accurately by the usual auscul-atory or automated methods. When listening with a manuallood pressure cuff, the start of the Korotkoff sound is aressure value that is estimated to be in the range of the systolicnd diastolic pressures. In the early post-operative period, anrterial catheter is necessary to monitor blood pressure prop-rly. After the arterial catheter is removed, the arterial bloodressure is most reliably assessed using Doppler and a sphyg-omanometer. Pressure values obtained using the Dopplerethod may be measured at any point during the cardiac cycle
nd should not necessarily be considered the actual systolic,iastolic, or mean pressure values.
Arterial blood pressure should be controlled with vaso-ctive and inotropic medications and intravascular fluidolume management. The pump speed should not be ad-usted to achieve a desired arterial blood pressure. The goals to maintain the mean arterial blood pressure in the rangef 70 to 80 mm Hg. It should not exceed 90 mm Hg. Unlikepulsatile LVAD, the amount of cardiac output support bycontinuous-flow pump is affected by the after-load, or
ystemic vascular resistance. Maintaining the mean arterialressure in the desired range will optimize cardiac support.t may also reduce stroke due to hypertension.
It is desirable to have some arterial pulsatility and aorticalve opening during support.106 A flat arterial blood pressureaveform with a low pulse pressure indicates that LV function
s extremely poor or that the set pump speed is close toxceeding the available pre-load (LV volume). When pulsatil-ty is absent, ventricular suction and collapse are more likely toccur. See Section V.A.3 on proper pump speed setting.
Pulse oximetry, if obtainable, may be unreliable due toiminished pulse pressure. Instead, some centers use cere-ral oximetry for assessing hemodynamic conditions whenore invasive monitoring is not available.
V.D. Patient education
ffective education requires a collaborative, multidisciplinaryeam approach that extends to the LVAD patient, family mem-
er(s), and companion(s) in care. Training on proper self-care
attatfd
IAceLisbaaLrsctdspip
IpTpmoidlraaidtssmsfp
IIbadca
caip
V
CivtdHdpastd
V
Cfl
S23Slaughter et al. Management of Continuous-Flow LVADs
nd system operation, with an emphasis on meticulous care ofhe percutaneous lead and exit site, should begin pre-opera-ively. Training continues throughout hospitalization. Eventu-lly, the patient’s demonstration of understanding and compe-ency may be a requirement for discharge. The fundamentaleatures of an effective patient education program have beenescribed previously.10,11,107,108 Also, refer to Section VII.
V.D.1. System operationthorough understanding of LVAS operation and system
omponent features for any specific device type is necessary tonsure patient safety, particularly in the outpatient setting. TheVAS patient and his or her family member(s) or compan-
on(s) must be able to competently perform routine activities ofelf-care as well as LVAS care and operation. They must alsoe prepared to respond appropriately to alarm symbols andudible tones. Of particular importance, the device must havedequate power at all times. In the case of the HeartMate IIVAS, a power base unit/power module or batteries serve as a
outine power supply. Loss of power will cause the pump totop. Pump cessation may have serious consequences, espe-ially in those patients who are device-dependent or in whomhe outflow tract has been over-sewn. Owing to this criticalependence on a continuous power supply, patient traininghould focus on the proper procedures for switching betweenower sources and for estimating available charge levels dur-ng battery-powered operation. Troubleshooting pump stop-age is covered in Section VIII.B.
V.D.2. Self-care infection prophylaxis andercutaneous lead immobilizationhe best measure for infection prophylaxis is to protect theercutaneous lead from movement at the exit site.60 Move-ent of the percutaneous lead will disrupt the sub-cutane-
us tissue ingrowth in the velour lining of the lead, resultingn infection. This tissue ingrowth is delicate and is easilyamaged with minor trauma. The lead should be immobi-ized in the operating room with a stabilization belt orestraint device that should be worn continuously. Patientsnd their caregivers should always take precautions to avoidny unnecessary exit site movement, especially sudden pull-ng on the lead. A patient’s ability to accomplish this goal inay-to-day life can greatly depend on the effectiveness ofhe education to which he or she has access. Thus, educationhould routinely emphasize to the patient that proper exitite care is critical to long-term survival. The importance ofeticulous aseptic techniques for exit site care must also be
tressed and periodically demonstrated. See Section VII.C.1or more information on outpatient device management andercutaneous lead and exit site care.
V.D.3. Maintaining volume status and hydrationt is common for LVAD patients to become dehydratedecause they continue to limit their oral intake and maintainsalt-restricted diet. To help monitor volume status after
ischarge, patient self-care routines should include dailyharting of weight and paying attention to symptoms such
s orthostatic hypotension. Patients should be prompted to tall if their weight fluctuates more than 1.3 kg (3 lb) during24-hour period. Consider repeating echocardiogram stud-
es during outpatient visits to determine if the patient’sump is set at the proper speed.
. Post-operative device management
Key Points● Continuous-flow LVADs do not contain valves. If the
pump stops, there may be back flow that can havesevere consequences (similar to aortic insufficiency).Avoid power interruption or inadvertent power leaddisconnection that would lead to loss of support.
● Continuous-flow pumps can generate large negativepressures at the pump inlet, which may result in septalshift or ventricular collapse. Consequently, pump-speed optimization and device monitoring presentunique challenges compared with pulsatile devices.
● Avoid setting the pump speed too high, which canresult in ventricular collapse or inlet obstruction andinitiate arrhythmias.
● The system-provided parameters of speed, power,pulsatility index, and estimated flow in conjunctionwith echocardiography serve as the primary indica-tors of proper device function. The patient’s clinicalstatus should always be assessed when device func-tion is evaluated.
● The range of safe operating speed is determined bymeans of a ramped speed study with echocardiogra-phy. Changes in ventricular shape and function andthe patient’s physiologic response to changing pumpspeeds will determine the appropriate speed setting.
● The flow rate displayed on most systems is an esti-mate that should be used for trending and not as aprecise measurement of cardiac output.
ontinuous-flow LVADs present unique challenges in mon-toring and optimizing support compared with pulsatile de-ices. Because each device has specific system characteris-ics, it is not possible to cover all possible scenarios forevice management for all devices. We will focus on theeartMate II, although some properties are generic to otherevices as well. This section first describes how the system-rovided parameters of speed, power, pulsatility index (PI),nd estimated flow are used to assess the adequacy ofupport; it concludes with troubleshooting tips. Note: Theerm pulsatility index is shortened to “Pulse Index” forisplay on the HeartMate II system monitor screen.
.A. Monitoring device function
ontinuous-flow LVADs do not contain valves. As a result,ow can become retrograde if the pump is turned off or in
he presence of high afterload pressure and low pump speed.

AtiCwl
aeLpclia
VFrsvipo
aetsepar
mslodIo
tm05
VWcfltIitlcdiawit
VOLohihaspsf
Fo
FHt
S24 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
nother distinctive feature of continuous-flow LVADs isheir ability to generate large negative pressures at the pumpnlet, which may result in septal shift or ventricular collapse.onsequently, speed optimization and device monitoringith continuous-flow LVADs present some unique chal-
enges compared with pulsatile devices.The system-provided parameters of speed, power, PI,
nd estimated flow for the HeartMate II, in conjunction withchocardiography, serve as the primary indicators of properVAS function. It is important to view each of these devicearameters in the larger context of the patient’s overallondition. Once baseline values representing a satisfactoryevel of patient support are established, the degree of changen a parameter usually has more clinical significance than itsbsolute value.
.A.1. Flow and powerlow estimate and power at a given speed are closelyelated. Power is directly measured by the HeartMate IIystem controller, and the reported flow is an estimatedalue determined from power and pump speed. An increasen power is converted into an increase in flow through theump and will be displayed as such on the system monitorr display module.
An increase in power not related to increased flow, suchs thrombus on the rotor, will cause an erroneously highstimated flow reading. Power values under normal condi-ions of operation will run within an expected range for eachet speed (Figure 7). If the power values are outside of thexpected range, the display of estimated flow will be re-laced with “���” or “���” when the calculated flow isbove or below the expected physiologic limits at the cur-ent set speed, respectively.
The minimum value for the flow estimator is 3.0 liters/in. Gradual increases in power, without a change in the set
peed, an increase in volume status, or a decrease in after-oad, may indicate the formation of thrombus on the bearingr rotor. Conversely, an occlusion of the flow path willecrease flow and cause a corresponding decrease in power.n either situation, an independent assessment of pumputput should be performed.
igure 7 The minimum and maximum expected power values
pver the range of speed settings for the HeartMate II.The average values of power, flow, and pulsatile index inhe HeartMate II BTT trial are shown in Figure 8. At 6onths of support, the average estimated flow was 5.6 �
.9 liters/min, pump power was 6.8 � 1.2 W, the PI was
.0 � 0.9, and the pump speed was 9,450 � 490 rpm.
.A.2. Pulsatility indexhen the LV contracts, the increase in ventricular pressure
auses an increase in pump flow. The magnitude of theseow pulses is measured and averaged for a 15-second in-
erval to produce the displayed PI value (appears as Pulsendex on monitor). In general, the magnitude of the PI values inversely related to the amount of assistance provided byhe pump. As the level of pump support increases, there isess ventricular filling, less pressure development, and aorresponding decrease in the measured PI. A significantrop in the PI without an increase in pump speed mayndicate a decrease in circulating blood volume. Conversely,n increase in left ventricular contractility, as may occurith an increase in volume status, myocardial recovery, and
notropic medications, or during exercise, will cause the PIo increase.
.A.3. Selecting optimum pump speedptimal pump speed is achieved when the cardiac index andV size are within normal range and there is no rightwardr leftward shift of the septum. In addition, it is desirable toave some pulsatility with intermittent aortic valve open-ng.7,93 A ramped speed study using echocardiography andemodynamic assessment provides the most direct method toscertain what speed provides the desired level of cardiacupport for each patient.109 Throughout the procedure, LV size,osition of the septum, blood pressure, and aortic valve openinghould be monitored to determine the appropriate combination ofactors that define the optimum operating point.
Ideally, a ramped speed study with echocardiography is
igure 8 Flow, speed, power, and pulsatility index (PI) during theeartMate II bridge-to-transplant trial are shown. Data presented are
he mean values with the standard deviation (range bars).
erformed in the operating room after the patient is stable

arfaabpiomcb
sna
tmr
e
1
2
3
Vc
Pfsteb
S25Slaughter et al. Management of Continuous-Flow LVADs
nd before the transesophageal echocardiography probe isemoved. A transthoracic echocardiogram may be per-ormed in the intensive care unit when the patient is stablend before invasive monitoring catheters are removed, andgain before hospital discharge. Additional studies shoulde performed when there are symptoms of inadequate sup-ort. Some experienced centers prefer to set the pump speedn the operating room using hemodynamic and echocardi-graphy parameters and to leave the speed setting constantost of the time throughout support unless there are indi-
ations of inadequate support, at which point the setting wille reassessed.
Note: The range of speed that is used for the remainder ofupport is optimally determined when the patient’s hemody-amic condition is stable (ie, volume is normal and vasoactivend inotropic agents are not supporting the patient).
The proper speed setting of the HeartMate II is in a rangehat is well above the minimum setting and well below theaximum setting. The usual speed range is 8,600 to 9,800
pm; only rarely is the setting outside of this range.To set the pump speed in patients who are stable and
uvolemic, the following protocol can be used:
. Determine the low-end of the speed range. Starting fromthe current fixed speed, lower the speed gradually until theaortic valve opens with each heart beat and there are nosigns of heart failure. Note: Some patients with very poorLV function may not have aortic valve opening. If the aorticvalve is not opening and a PA catheter is in place, thelowest speed setting can be determined when the cardiacindex is about 2.5 liters/min/m2 and/or the pulmonarywedge pressure begins to increase. Without a PA catheter,the low speed setting can be established when the LV sizeincreases and there is rightward shift of the septum. If anarterial pressure catheter is present, observe and record thepressure values and calculate the pulse pressure. Record theLV dimensions. Allow the patient to stabilize at each speedsetting and do not allow the fixed speed to decrease below8,000 rpm. It is possible that even at 8,000 rpm the aorticvalve will not open.
. Determine the high-end of the speed range. Startingfrom the low-end fixed speed as determined above, in-crease the pump speed gradually until the parasternalshort-axis or apical 4-chamber views show flattening ofthe septum (Figure 9). The LV diastolic dimensionshould decrease near the low-end of the normal range. Inpatients whose aortic valve was opening at the low-endspeed, the aortic valve will most likely remain closed,and the pulse pressure should be in the range of 10 to 15mm Hg. The cardiac index should increase and the pul-monary wedge pressure will decrease. The high-endspeed is usually below 9,600 rpm.
. An appropriate fixed speed setting usually will fallmidway between the low-end and high-end speedrange. The selected speed may be adjusted from themidpoint based on clinical judgment, taking into consid-eration the desire for periodic aortic valve opening and apalpable pulse. To accommodate normal shifts in volume
and hemodynamic status, the fixed speed should gener- aally be set at least 400 rpm below the maximum speed asdetermined above. If premature ventricular contractionsor ventricular tachycardia occurs with increased pumpspeed, the speed is too high and should be reduced.
I. Diagnosing and managing post-operativeomplications
Key Points● Perform physical examinations and laboratory test-
ing regularly throughout LVAD support.● Teach patients and family member(s)/caregiver(s)
how to identify and respond to signs and symptomsof the most common problems.
● Echocardiography is very useful in diagnosing prob-lems with the patient-pump interface. Echocardiog-raphy can assess:y Adequacy of pump speed and support by deter-
mining ventricular size.y Valvular function.y Inflow and outflow abnormalities.
● Left and right-heart catheterization may be neces-sary in some clinical circumstances such as sus-pected pump thrombosis or kinked conduit.
● Computed tomography may be useful in confirmingproblems with the pump.
● Bleeding complications:y Consider lowering anti-coagulation and anti-
platelet medication.
● TIA/stroke:y To avoid hemorrhagic stroke, do not aggressively
anti-coagulate.y Maintain pump flow �3.0 liters/min.
● Infection:y Educate patients and family member(s)/caregiv-
er(s) on percutaneous lead and exit site care, em-phasizing rigid adherence to aseptic techniquesfor dressing changes and lead immobilization.
● Arrhythmias:y Strong consideration on placing an implantable
cardioverter defibrillator for those that meet therequirements.
y To avoid suction-induced arrhythmias, do not setpump speeds too high.
hysical examination and laboratory testing should be per-ormed regularly throughout LVAD support. Patientshould be educated on identifying signs and symptoms ofhe most common problems and know how to respond toach. Subtle symptoms, such as low energy and fever, cane signs of impending serious problems and should be
ssessed promptly. In addition to routine examinations,
Fo
S26 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
igure 9 Echocardiography is shown for (left) parasternal long-axis and (right) apical four-chamber views at HeartMate II pump speed
f (top to bottom) 9,000, 10,000, 11,000, and 12,000 rpm.
sp
●
●
●
●
Nps
aL
V
Tslccfyheicdotp
tacacpersLnp
V
Ptapeo
S27Slaughter et al. Management of Continuous-Flow LVADs
ome specialized tests are particularly useful in diagnosingroblems associated with LVAD support, such as:
Echocardiography. Echocardiography is very useful forassessing post-operative complications because it allowsvisualization of the cardiac chambers and blood flow atthe LVAD inlet and outlet. Echocardiography is essentialfor evaluating cardiac valve function. Transthoracic echo-cardiography is often adequate for assessing inlet andoutlet velocities. If transthoracic echocardiography is in-sufficient to provide adequate assessment, consider trans-esophageal echocardiography. Occasionally, cardiaccatheterization or CT may be helpful for diagnosing bothinflow and outflow obstruction.Left-Heart Catheterization. Some patients on LVADsupport may have progression of coronary artery disease,with either acute or sub-acute coronary syndromes. It isappropriate to treat these patients the same as non-LVADpatients, and it is safe to perform coronary arteriograms.Because the outflow graft is attached to the ascendingaorta, guiding wires and catheters could potentially enterthe graft. A pigtail catheter can be placed in the LV in thesame manner as for a left ventriculogram, but passingthe catheter into the pump must be avoided. Panning overthe inflow and outflow cannula permits visual assessmentfor graft kinking and flow obstruction.Right-Heart Catheterization. Because the flow shown onthe HeartMate II system monitor is an estimate of flowthrough the LVAD and does not necessarily reflect thetotal cardiac output, a right-heart catheterization can beperformed for a more precise estimate of right-heartand left-heart function. Thermodilution or Fick meth-ods for obtaining cardiac outputs should be accurate inmost cases.Computed Tomography. CT can be used to assess theoutflow and inflow graft for kinking, twisting, or throm-bus (Figure 10). It does not allow visualization of thetitanium portions of the pump or inlet cannula.
ote: Magnetic resonance imaging (MRI) should never beerformed on a patient with an implanted LVAD due to thetrong magnetic fields.
Table 12 lists potential complications and suggested man-gement approaches related to support with the HeartMate IIVAS.
II. Outpatient management
Key Points● Successful long-term LVAD support depends on
comprehensive care from a multidisciplinary team,including the patient and his or her familymember(s)/caregiver(s).
p
● Effective patient education and support are key com-ponents of successful outpatient support.
● The target INR for patients receiving the Heart-Mate II is 1.5 to 2.5 with warfarin therapy, andaspirin at 81 to 325 mg daily for anti-platelettherapy.
● Stabilize the INR before discharge from the hos-pital.
● Over-anti-coagulation should be avoided.● Hypertension must be controlled to avoid decreased
LVAD support and cardiac output as well as to avoidcerebrovascular events.
● Before discharge, thoroughly assess the patient’smedical readiness.
● Immobilizing the percutaneous lead to prevent exitsite trauma reduces infection risk. Care of the per-cutaneous lead and exit site must be a priority forsuccessful outpatient care.
he outcomes of patients discharged from the hospital whileupported by the continuous-flow LVADs have been excel-ent.1 Successful long-term LVAD support depends onomprehensive care from a multidisciplinary team, in-luding the patient and his or her family/caregiver(s), orriends.110–113 Parents often become the primary caregiver forounger patients. Responsibility for patient care shifts from theeart failure team to the patient and his or her family/caregiv-r(s) when the patient is discharged from the hospital. Educat-ng the patient and his or her family and companion(s) oraregiver(s) begins when the decision is made to implant theevice. After implant, patients should be taught some aspectf outpatient care during each hospital day; consequently,here is a high level of confidence at discharge that theatient will not experience avoidable complications.
Managing LVAD outpatients with different types of sys-ems is similar in many ways. However, users must beware of the key points specific to each device to minimizeomplications and to optimize survival. Users are encour-ged to take advantage of the manuals, documents, andlinical support pieces developed by the manufacturers to sup-ort outpatient success. A 2-volume document developed fromxperience with pulsatile devices as DT are still useful as aeference for continuous-flow devices.10,11 Also, readershould refer to material by Maclver et al111 for management ofVAD patients in the community. These documents provide aumber of checklists, forms, and protocols to aid in dischargelanning and proper outpatient management.
II.A. Preparing for hospital discharge
reparing patients for hospital discharge begins during pa-ient selection, when a prospective patient’s support systemnd outpatient living environment are assessed. Before im-lant, the patient and his or her family members(s)/caregiv-r(s) must be informed of the requirements for successfulutpatient support. In addition to the patient’s spouse, life
artner, or companion, his or her children, neighbors, and
ftimltpeae
HtmLadpaht
cie
Ptsetsds
Dritoitpo
CaTpScn
V
AttuHtdaH3eatsosRacvp
H
Fa
S28 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
riends should be enlisted to participate in care and moni-oring efforts.111 Creating a broad network of involvedndividuals maximizes support for the patient and can
inimize the burden of the primary caregiver duringong-term LVAD support such a for DT patients. Beforehe LVAD is implanted, it may be worthwhile to have theatient and his or her family member(s)/caregiver(s) ex-cute a “behavioral contract” that lists caregiver tasksnd specifically identifies the responsible party(ies) forach expectation or need.
eart failure teams. Although a VAD coordinator is usuallyhe person charged with training patients and their familyembers/caregivers, and for assuring follow-up throughoutVAD support, all heart failure team members have valu-ble contributions to make when preparing the patient forischarge.114 When appropriate, the patient’s primary carehysician should be involved, and communication amongll team members should be coordinated. For example, theeart failure team must communicate the same information
igure 10 Computed tomography scan with contrast is used tossess inflow and outflow grafts. LV, left ventricle.
o the patient and the patient’s support group to avoid any w
ontradictions regarding care and emergency measures. Fornexperienced users, discharge planning meetings with thentire team can facilitate a smooth transition for the patient.
atient education. Effective education for the patient andhose who will be caregiver(s) is the key to outpatientuccess. Accordingly, all team members must learn thessentials of LVAD patient care, as well as system opera-ion, maintenance, troubleshooting, and emergency re-ponse. Competency evaluation must be performed andocumented before discharge, and the need for retraininghould be assessed periodically.
ischarge readiness. Before discharge, the patient’s medicaleadiness must be thoroughly assessed. One of the mostmportant tasks before discharge is stabilizing the INR andhe dose of anti-coagulants. Fluid balance may be a keyutpatient concern for many patients and should be normal-zed before discharge. Physical, occupational, and respira-ory therapy rehabilitation should be complete, and theatient must be physically capable of managing much of hisr her own care.
ommunity services. Community preparation varies greatlymong users and should be individualized accordingly.115
raining of emergency medical services personnel onroper LVAS emergency measures should be considered.pecific written instructions or an emergency identificationard with contact numbers to the VAD center for emergencyotification should be with the patient at all times.
II.B. Outpatient medical therapy
nti-coagulation. Proposals for post-operative anti-coagula-ion therapy are discussed in Section IV.B. and carry intohe outpatient phase of support. Adjusted warfarin doses aresed to achieve a target INR in most cases of 1.5 to 2.5 foreartMate II recipients. Aspirin (81 to 325 mg daily) is
ypically used for anti-platelet therapy. This therapy is in-ividually adjusted to minimize the risk of ischemic strokend major bleeding.52 Of 331 patients discharged witheartMate II support, the total thrombotic event rate was.3%, compared with a much higher rate of hemorrhagicvents of 22%, suggesting that some patients have been overnti-coagulated.52 Results from the clinical trial show thathe current recommended anti-coagulation therapy is con-iderably less than it was when the trial was started. Of theutpatients who had non-surgical bleeding events, the GIystem was identified as the most frequent site of bleeding.egular testing of the coagulation and hematology profilesre recommended. Because hemolysis may potentially oc-ur, the lactate dehydrogenase and plasma free hemoglobinalues should be determined when occult bleeding isresent.
ypertension. Cardiovascular medical therapy is prescribed
ith consideration to avoid hypertension while maintaining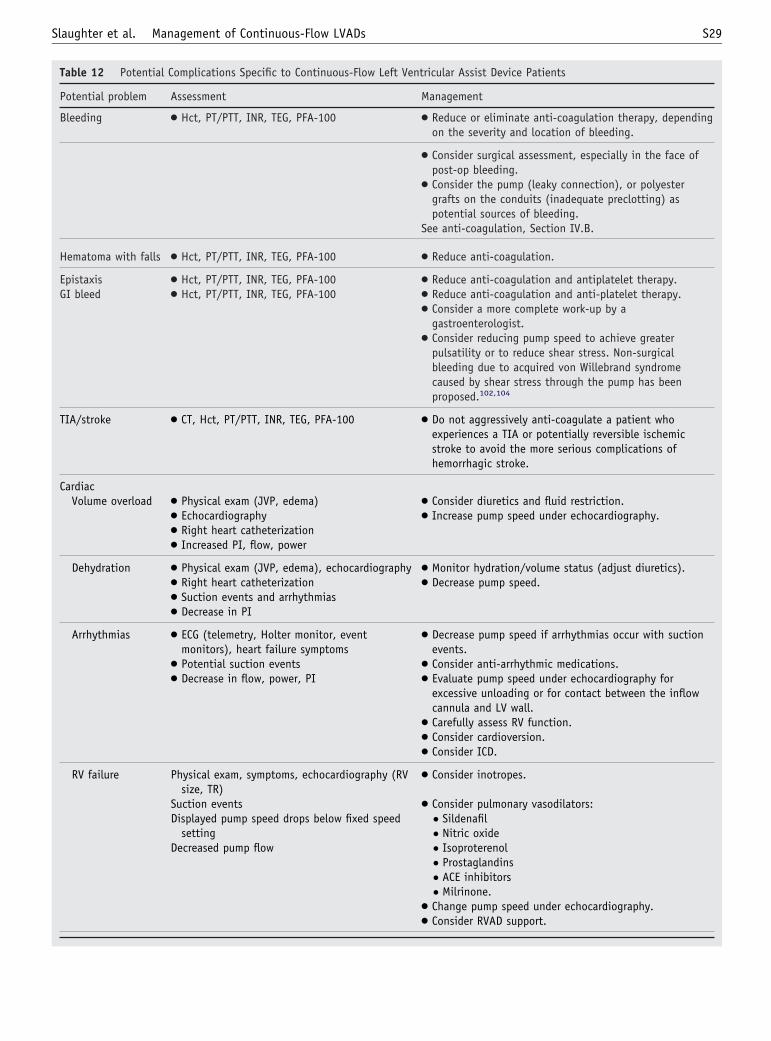
S29Slaughter et al. Management of Continuous-Flow LVADs
Table 12 Potential Complications Specific to Continuous-Flow Left Ventricular Assist Device Patients
Potential problem Assessment Management
Bleeding ● Hct, PT/PTT, INR, TEG, PFA-100 ● Reduce or eliminate anti-coagulation therapy, dependingon the severity and location of bleeding.
● Consider surgical assessment, especially in the face ofpost-op bleeding.
● Consider the pump (leaky connection), or polyestergrafts on the conduits (inadequate preclotting) aspotential sources of bleeding.
See anti-coagulation, Section IV.B.
Hematoma with falls ● Hct, PT/PTT, INR, TEG, PFA-100 ● Reduce anti-coagulation.
Epistaxis ● Hct, PT/PTT, INR, TEG, PFA-100 ● Reduce anti-coagulation and antiplatelet therapy.GI bleed ● Hct, PT/PTT, INR, TEG, PFA-100 ● Reduce anti-coagulation and anti-platelet therapy.
● Consider a more complete work-up by agastroenterologist.
● Consider reducing pump speed to achieve greaterpulsatility or to reduce shear stress. Non-surgicalbleeding due to acquired von Willebrand syndromecaused by shear stress through the pump has beenproposed.102,104
TIA/stroke ● CT, Hct, PT/PTT, INR, TEG, PFA-100 ● Do not aggressively anti-coagulate a patient whoexperiences a TIA or potentially reversible ischemicstroke to avoid the more serious complications ofhemorrhagic stroke.
CardiacVolume overload ● Physical exam (JVP, edema) ● Consider diuretics and fluid restriction.
● Echocardiography ● Increase pump speed under echocardiography.● Right heart catheterization● Increased PI, flow, power
Dehydration ● Physical exam (JVP, edema), echocardiography ● Monitor hydration/volume status (adjust diuretics).● Right heart catheterization ● Decrease pump speed.● Suction events and arrhythmias● Decrease in PI
Arrhythmias ● ECG (telemetry, Holter monitor, eventmonitors), heart failure symptoms
● Decrease pump speed if arrhythmias occur with suctionevents.
● Potential suction events ● Consider anti-arrhythmic medications.● Decrease in flow, power, PI ● Evaluate pump speed under echocardiography for
excessive unloading or for contact between the inflowcannula and LV wall.
● Carefully assess RV function.● Consider cardioversion.● Consider ICD.
RV failure Physical exam, symptoms, echocardiography (RVsize, TR)
● Consider inotropes.
Suction events ● Consider pulmonary vasodilators:Displayed pump speed drops below fixed speed
setting● Sildenafil● Nitric oxide
Decreased pump flow ● Isoproterenol● Prostaglandins● ACE inhibitors● Milrinone.
● Change pump speed under echocardiography.● Consider RVAD support.

S30 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
Table 12 Continued
Potential problem Assessment Management
Tamponade ● Physical exam, symptoms, echocardiography,chest X-ray, CT scan
● Return to OR for re-exploration.
● Suction events ● Consider pericardiocentesis.● Sudden and unexpected decrease in chest tube
output● Decreased pump flow
Hypotension ● Symptoms, BP monitoring ● Adjust vasoactive medications.● Increase in pump flow and power ● Consider volume expansion.● Decrease in PI
Hypertension ● BP monitoring, assess volume status ● Decrease afterload with medications.● Decrease in pump flow and power ● Consider diuretics for volume overload.● Increase in PI
Recurrence ofheart failuresymptoms
● Physical exam, symptoms; other testing asappropriate
● Evaluate pump speed settings.
● Decrease in pump flow and PI ● Evaluate RV function.● Pulmonary dysfunction, edema and hypoxemia ● Treat pulmonary symptoms.
Aorticinsufficiency
● Physical exam, symptoms ● Repair/replace as needed (see Section III.A).
● Echo● Fluoroscopy● Decreased perfusion● Dilated LV with high pump flow
InfectionPercutaneous lead ● Exam ● Administer anti-biotics.
● Culture and sensitivity ● Improve percutaneous lead exit site care andimmobilization.
● Consider wound VAC for significant wound healingissues.
● See details in Outpatient Management Section.
Pocket ● Exam ● Administer anti-biotics.● X-ray ● Explore pump pocket and drain abscess fluid.● Ultrasound ● Place PMMA beads (typically containing vancomycin
and/or tobramycin) into pump pocket.● CT scan ● Irrigate and débride pump pocket.● Tap pocket ● Consider pocket revision, though a new access may be
required.● Cultures
OtherPercutaneous lead
site tearing● Exam ● Patient education: Warn patient to avoid tugging or
twisting percutaneous lead or allowing the controller tofall or drop.
● Use a stabilization belt or abdominal binder to securethe system controller (driver) and immobilizepercutaneous lead.
Percutaneous leadinsulationtearing
● Visual exam ● Patient education: Warn patient to avoid tugging ortwisting percutaneous lead or allowing the controller tofall or drop.
● Contact Thoratec.

flmoicci
Ors
V
EaHb(a
ptscfmm
stcettt
VmPtipwfattf
gccpfdpfss
●
S31Slaughter et al. Management of Continuous-Flow LVADs
uid balance and glycemic control. Hypertension is nor-ally controlled with �-blockers, with careful monitoring
f RV function; or with ACE inhibitors, with careful mon-toring of renal function. Because hypertension may de-rease LVAD support and total cardiac output and causeerebral events, frequent assessment of blood pressure ismperative.
ther therapy. When indicated, antibiotics, statins, and thy-oid medications should be prescribed. A prescribed diethould be followed and adjusted as necessary.
II.C. Outpatient device management
ach continuous-flow LVAD system has specific peripher-ls and components for outpatient use. As an example, aeartMate II patient receives a complete primary set and aackup set of external system components before dischargeTable 13). The patient may also receive a stabilization beltnd the accessories listed in Table 13.
Table 12 Continued
Potential problem Assessment
Hemolysis ● LDH test
● Plasma-free hemoglobin
● Consider decreasing speed
ACE, angiotensin-converting enzyme; AV, arteriovenous; BP, blood prHct, hematocrit; INR, international normalized ratio; JVP, jugular venoroom; PI, pulsatility index; PFA-100, Platelet Function Analyzer (PFAprothrombin time; PTT, partial thromboplastin time; RV, right ventricle;ischemic attack; TR, tricuspid regurgitation; VAC, vacuum assisted closu
Table 13 Required HeartMate II Equipment for HospitalDischarge
Component Required Backup Optional
System controller ✓ ✓ . . .Batteries (2 sets) ✓ ✓ . . .Battery clips ✓ . . . Backup optionalEmergency power pack ✓ . . . . . .Display module ✓ . . . . . .Power base unit or
power module withcable
✓ . . . . . .
Universal batterycharger
✓ . . . . . .
System controllerbattery module
. . . ✓ . . .
Stabilization belt ✓ . . . Backup optionalModular belt ✓ . . . Backup optionalShower bag ✓ . . . Backup optionalHolster vest ✓ . . . Backup optionalConsolidated bag ✓ . . . Backup optionalPatient handbook ✓ . . . . . .
Before discharge, the backup system controller must berogrammed with the same parameters as the primary con-roller. Patients must keep the backup controller, chargedpare batteries, battery clips with cables, and emergency IDard with them at all times. Before discharge and duringollow-up training, the critical nature of the backup equip-ent and the proper use and safe maintenance of all equip-ent should be emphasized.Patients and their caregivers must be able to recognize
ystem alerts and alarms and know the appropriate measureso be taken for each. This is a significant part of patient/aregiver education. Patients and family members/caregiv-rs are trained to handle alarms and taught when to contacthe physician or VAD coordinator. Patients are taught howo record all alarm conditions and any related circumstanceshat may aid in troubleshooting.
II.C.1. Percutaneous lead care and exit site woundanagementercutaneous lead infection and damage to the wires within
he lead are potentially serious adverse events that are lead-ng reasons for hospital re-admission. The incidence ofercutaneous lead infections in the HeartMate II DT trialas 0.48 events/patient-year, and lead damage was the most
requent cause of pump replacement.1 Many of these eventsre preventable through meticulous protection and care ofhe percutaneous lead. Updates in the design of the percu-aneous lead are expected to improve its durability in theuture.
Outpatient prevention of percutaneous lead infection be-ins in the early post-operative period when the patients andaregivers become involved in self-care. Established proto-ols for inpatient and outpatient percutaneous lead care haveroven to be effective for pulsatile devices and should beollowed.10,60,107,108 Infection prevention has been ad-ressed throughout this document because it is a serious andreventable adverse event that requires meticulous attentionrom the time of LVAD implant and for the remainder ofupport.60 Some key points for outpatient support that de-erves emphasis are:
Immobilization of the percutaneous lead at the exit site isvital to prevent disruption of subcutaneous tissue in-
Management
● Evaluate potential sources: inflow/outflow occlusions,pump issues, etc (see Section V).
● Consider temporarily reducing pump speed (most casesare transient).
CT, computed tomography; ECG, electrocardiogram; GI, gastrointestinal;ure; LDH, lactate dehydrogenase test; LV, left ventricle; OR, operatingDade Behring Inc, Deerfield, IL); PMMA, polymethylmethacrylate; PT,right ventricular assist device; TEG, thromboelastogram; TIA, transient
essure;us press)-100 (RVAD,re.
growth.

●
●
●
●
ctntp
tvtthsbattbio
V
Priahpgpoei
V
Ophmppi
●
●
●
●
●
●
●
●
V
Apciuds
irOtant
sTgia
V
CH(
S32 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
All caregivers must perform exit site care with meticuloussterile technique (some centers use clean technique whenthe patient is at home and the site is well healed).The observation of erythema or increased drainage shouldbe immediately reported and prompt an investigation forcause.Cleansing of the exit site must be gentle and non-trau-matic.Various immobilization methods may need to be evalu-ated by the patient for optimal comfort and effectiveness.
Various methods of immobilization are used by differententers. Stabilization belts have been very effective in pro-ecting the exit site and percutaneous lead. Alternative tech-iques for percutaneous lead stabilization have been devisedo accommodate patient preferences or for patients withoor compliance.
When signs of infection develop, the method of percu-aneous lead stabilization should be re-evaluated and re-ised, if necessary. If there is serous or purulent drainage,he frequency of dressing changes should be increased untilhe infection is resolved. For worsening infections, considerospitalization for more intensive therapy. Surgical revi-ion, wound vacuum-assisted closure therapy, antimicrobialeads, and pump exchange may be necessary. Prolongednti-biotic use in the absence of infection should be avoidedo decrease the chance of developing infection from resis-ant organisms. However, some patients need chronic anti-iotic suppression therapy if their infection cannot be elim-nated. Note: Refer to Chinn et al60 for detailed clinicalutlines on handling percutaneous lead infection.
II.D. Handling emergencies
atients and their caregivers must be able to recognize andespond to emergency conditions and should refer to train-ng documents on how to handle emergencies.107 For ex-mple, HeartMate II patients must be able to respond to “redeart,” or low-flow alarms immediately, followed by appro-riate notification of the VAD coordinator. A list of emer-ency contacts must remain with the patient at all times. Theatient should be encouraged to contact his or her physicianr VAD coordinator for all conditions that may be consid-red serious. Because emergencies are rare, frequent retrain-ng is advisable.
II.E. Outpatient follow-up
ngoing follow-up is a key part of effective care for out-atients supported by continuous-flow LVADs. A compre-ensive, multidisciplinary team approach to outpatient careay have an important effect on long-term survival. A
roactive approach to outpatient care can help to identifyroblems earlier with more effective treatment. The follow-ng aspects of outpatient follow-up warrant consideration:
The frequency of follow-up clinic visits varies amongpatients, depending on medical issues, concerns for self-
care, and the distance a patient is from the implant center. rPatients usually return to the clinic weekly until the heartfailure team determines that less frequent visits are pru-dent. As a patient’s condition improves and there are nomedical concerns, outpatient visits can be decreased fur-ther.Follow-up by telephone calls may be useful in maintain-ing a constant communication with patients, especiallythose who do not live near the implant center.Anti-coagulation therapy must be carefully monitored toavoid large variations in the INR.Outpatients should be assessed whenever significantchanges in pump flow, PI, or power are observed andafter any alarm condition. Teaching patients to record thisinformation every day on a chart may assist them inknowing what their “normals” are.Changes in exercise tolerance, weight, appearance of thepercutaneous lead exit site, or other symptoms should beconsidered as potentially serious adverse events, and athorough evaluation should be promptly performed.Outpatients must have access to the heart failure team atall times. The patient should have contact information foremergencies or for questions and technical support.Serial echocardiograms with a ramped speed study duringroutine clinic visits may be useful to reassess the pumpspeed setting and to evaluate the potential of myocardialrecovery.
III. Troubleshooting
s has been described, each LVAS provides a number ofarameters that can be used to monitor patient and pumponditions specific to each device. The authors’ experiencen the clinical trial with the HeartMate II LVAS has beensed to write this chapter specifically for patients with thatevice. These parameters and their significance in trouble-hooting are listed in Table 14.
Pump operating parameters are not surrogates for mon-toring the patient’s clinical status. The changes in all pa-ameters should be considered when assessing a situation.wing to variability between patients, trends observed in
he system parameters are usually more valuable than thebsolute values presented. Abrupt changes in the parametersot associated with normal physiologic changes can be usedo identify conditions that warrant further evaluation.
The use of these parameters in troubleshooting severalelected complications is presented subsequently and inable 15. Typical methods for assessing situations areiven, along with the corresponding device behavior. It ismportant to monitor pump readings and interpret changess they may relate to patient complications.
III.A. Pump thrombus
linically relevant pump thrombus was rare during theeartMate II clinical trial, occurring in 5 of 133 DT patients
4%)1 and in 4 of 281 BTT patients (1.4%), 2 of whom
equired pump replacement and 2 died.8 The source of the
tpl
t
spip
S33Slaughter et al. Management of Continuous-Flow LVADs
hrombus may have grown from smaller deposits within theump or could have been ingested from the left atrium oreft ventricle.
Thrombus within the pump can affect all 4 parameters of
Table 14 Significance of Displayed HeartMate II Pump Param
ParameterHow parameter isgenerated Significance of c
Pump rotorspeed
Direct measurementthrough motor
● System operateunder normal c
● Large speed ch● Suction even
9,000 rpm).● At the end o
setting.● Failure of th
event indica
Power Direct measure of currentand voltage applied tomotor
● Varies directly● Increased flo● An increase
pump power● Changes in p● Flow obstruc● Flow obstruc
result in inc● Abrupt change
the pump:● Note that ab
trial with no● Contact Thor● Gradual pow
on the beari
Pulsatilityindex
Calculated from pumppower normalized bymean power
● PI corresponds● PI fluctuates● Under norma
natural hear● PI decreases:
● Decrease in● Inflow/outfl
and consequ● Abnormal po
bearings).
Flow Estimation based onpump speed and power
● Under normaconditions o
● Estimation a● Imprecise at● Flow estimat
as an absolu● Increases wi
increased pu● Abnormal pow
can result in o● May introduc
conditions.● Even in abno
flow.
LV, left ventricle; LVAD, left ventricular assist device; PI, pulsatility
he HeartMate II LVAS: speed, power, flow, and PI. A g
ufficiently large thrombus can obstruct the flow through theump. A large thrombus in contact with the rotor or bear-ngs can increase the drag on the rotor and increase theower requirement. Such increases in power have been
fixed speed that matches displayed setting of about 100 rpmons.in fixed speed mode indicate an abnormal condition:precipitate decrease in speed to lower speed limit (default:
tion event, speed gradually increases to the fixed speed
m to maintain the fixed speed setting without a suctioner pump or controller issues.
ump speed and flow under normal conditions:lts in increased power.
rease in pump speed will result in an increase or decrease inctively.ogic demand can affect power.ithout contact with the LVAD rotor results in reduced power.the form of a thrombus with contact with the rotor can
power.wer should be evaluated for potential ingested thrombus into
ower changes up to 2 W have been reported in the clinicalse events.chnical support.
ease (over hours or days) may signal deposition or thrombusrotor (see Sections V.A.1 and VIII.A.).
gnitude of flow pulse through the pump:changes in volume status and the natural heart’s contractility.itions, PI increases with increased pressure developed by theh can result from increased LV pre-load or contractility.
status.truction, which reduces relative magnitude of the flow pulsehe power pulse.evation (eg, from deposition or thrombus on the rotor or
itions, reflects actual pump flow changes due to patiente operation.normal pump operation.
ates less than about 3 liters/min.ould be used for trending changes in conditions rather thansurement of flow.77
reased pressure differential across the pump and witheed.ation (eg, from deposition or thrombus on rotor or bearings)mation of flow:lse-negative when using flow estimate to rule out low-flow
ituations, flow estimate is unlikely to under-predict actual
RV, right ventricle.
eters
hanges
s at aonditiangest will
f a suc
e systetes oth
with pw resuor dec, respehysioltion wtion inreaseds in po
rupt padveratec teer incrngs or
to mawithl condt, whic
volumeow obsently twer el
l condr devicssumesflow rion shte meath decmp sper elevverestie a fa
rmal s
index;
radual, taking hours or days as opposed to abrupt changes,

S34 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
Table 15 Potential Device Complications
Problem LVAS response Assessment Management
Inflow obstructionwithout contactwith LVAD rotor
● Decreased pump power ● HF symptoms ● Ensure patient is hydrated.● Decreased PI ● Hemolysis ● Consider reducing pump speed in presence
of inlet obstruction against myocardium orseptum.
● Decreased flow ● Inflow position ● Provide supportive therapy to optimizeright heart function.
● Suction events ● Chest X-ray, echocardiography ● Consider re-exploring chest to relievetamponade or adjust pump position andanchor pump.
● Angiography● CT angiography● Evaluate right heart function● Tamponade● Ramped speed study for LV size
change with speed change● Diastolic arterial blood pressure
change with speed change
Outflow obstructionwithout contactwith LVAD rotor
● Decreased pump power ● HF symptoms ● Consider re-exploring chest.● Decreased PI ● Hemolysis● Decreased flow ● Outflow position● Suction events ● Echocardiography, chest X-ray,
and angiography to determineflow through the outflow graft;assess for graft kink
● Ramped speed study● LV size change with speed
change● Diastolic arterial blood pressure
change with speed change
LV suck down orsuction event
● Pump speed automaticallydecreases below set speedto low speed limit andramps back up to setspeed
● Echocardiography and chestX-ray (inflow position, LV size)
● Ensure patient is hydrated.
● Decreased pump flow ● Evaluate RV function ● Decrease pump speed.● Arrhythmias
Percutaneous leador motor failure
● Pump runs rough/vibrates ● HF symptoms ● Contact Thoratec to determine if lead repairis feasible; if not, replace pump.
● not maintaining set pumpspeed; damagedcontrollers
● Arterial blood pressuredecreases with increased pulsepressure
● If controllers are damaged, operate theLVAS on batteries rather than PBU/PMpower.
● PI �10
Thrombus in pumpin contact withrotor
● High power and estimatedflow, or flow blanking
● HF symptoms ● Consider pump replacement.
● Decreased PI ● Hemolysis ● Consider thrombolytic therapy with caution.Continuous IV heparin may preventprogression of thrombus.
● Sound of pump(w/stethoscope) changes
● Arterial blood pressuredecreases with increased pulsepressure
● Angiography andechocardiography to confirmlack of pump inflow
HF, heart failure; IV, intravenous; LV, left ventricle; LVAD, left ventricular assist device; LVAS, left ventricular assist system; PI, pulsatility index; PBU,power base unit; PM, power module; RV, right ventricle.

wcptd
esqflicpa
hiih
cmfip“eav
V
BwpposdT5eIe
vrpipprob
itop
attcep
tRorspsSts
IpscWbvhadafis
V
Tsivtbasso
ilbrl1dfl
V
F
S35Slaughter et al. Management of Continuous-Flow LVADs
hich may indicate an ingested thrombus. With the in-reased power, PI is reduced because the pulsatile com-onent of power becomes relatively small compared withhe steady component of power required to overcome therag.
If the flow obstruction is substantial, the pressure differ-nce across the pump will be increased by the obstruction,o the relative influence of the pressure pulse and conse-uently the PI is diminished. In such situations, the pumpow is also limited. The normal unloading of the LV with
ncreasing pump speed, therefore, is not observed. Thus, theombination of decreased PI and increased arterial pulseressure from the increased preload can be an indication ofpump blockage.Thrombus should also be suspected with the presence of
emolysis, for example, if the lactate dehydrogenase levelncreases to �1,500 or 3 times the previous level, or if theres any hemoglobinuria or significantly elevated plasma freeemoglobin.
In an extreme case, although rare, the drag on the rotoran become high enough that the motor can no longeraintain the pump speed and the speed will fall below thexed speed setting. In cases where thrombus increasesump power, the flow display may be replaced with���” if it is outside the expected operating range. How-ver, it also may be overestimated and displayed flow couldppear in the normal range even though the pump flow isery low.
III.B. Pump stops
ecause not all pump stops may be associated with a hard-are malfunction, it is important to understand why stop-age occurs. A pump stop condition can be created if theump stop command is entered on the system monitor. Lossf power to the pump (eg, disconnecting both power leadsimultaneously) will cause the pump to stop and so willisconnecting the percutaneous lead from the controller.wo of the 281 patients in the HeartMate II BTT trial andof 133 (4%) in the initial DT study died after loss of
xternal power due to incorrect replacement of batteries.1,8
t is imperative that only 1 battery be replaced at a time, asxplained in the instructions for use.
Unlike a positive-displacement LVAD that containsalves, if a continuous-flow LVAD stops, there will beegurgitant flow from the aorta to the LV. Under normalhysiologic pressures, this regurgitant flow will be approx-mately 1 to 2 liters/min for the HeartMate II. Just as theump in the stopped condition will limit the backflow, theump provides substantial resistance to forward flow. As aesult, if the pump is stopped and the LV outflow tract isccluded, the ability of the device to support the patient wille very limited.
If the pump stops, an audible alarm will sound. If the stops a result of complete loss of power, there will be a con-inuous audible alarm and no indicator lights will illuminaten the system controller. If the controller is still receiving
ower, a pump stop will be accompanied by an audible clarm and a “red heart” alarm will illuminate on the con-roller. The pump stop condition will also be indicated onhe system monitor or display module screen if they areonnected to the power base unit or power module; how-ver, the pump speed and flow will not be displayed and theower will be zero.
If the pump is stopped and all connections to the con-roller are intact, pressing the Test Select button or Alarmeset switch will restart the pump. At a fixed speed settingf 8,000 rpm or higher, if the power to the pump is inter-upted and the pump stops, when power is restored theystem controller will automatically restart the pump at thereviously set speed. However, if the fixed speed setting islower than 8,000 rpm, the user must press and hold theilence Alarm or Test Select button for 2 seconds to restarthe pump. Pressing the Test Select and Alarm Reset buttonsimultaneously will start the controller in the backup mode.
When the system monitor is connected to the HeartMateI LVAS, pump operation can be verified by the display ofump speed and power information on the system monitorcreen. If the monitor is not connected, it is possible toonfirm pump operation through the system controller.hen the pump is running properly, the green power sym-
ol on the controller will be illuminated and there will be noisual or audible alarms. If the pump is not running, the redeart symbol will be illuminated and a continuous audiblelarm will sound. If all power to the controller has beenisconnected, no lights will be illuminated and a continuousudible alarm will sound. An alternative approach for con-rming that the pump is running is to listen for pumpsounds with a stethoscope over the pump location.
III.C. Suction events
he system parameters can also be used to troubleshootuction events. Suction events occur when the pump speeds set higher than appropriate in relation to the availableolume in the LV. Such events are typically precipitated byhe patient becoming hypovolemic, but can also be causedy anything that reduces the return of blood to the LV, suchs RV failure, cardiac tamponade, or pulmonary hyperten-ion. Poor cannula positioning can also increase the propen-ity for a suction event because the LV wall or septum maybstruct the inflow cannula.
When the system detects a suction event, the pump speeds automatically reduced below the fixed speed setting to theow speed limit setting in the controller (user adjustable,etween 8,000 and 10,000 rpm and is usually set 400 to 800pm below the fixed speed setting). When suction is noonger present, the speed gradually increases (at a rate of00 rpm per second) back to the original speed setting. Thisrop in speed is also associated with a reduction in pumpow and is reflected in the displayed flow estimate.
III.D. Obstruction
low path obstruction can occur if the inflow or outflow
annula is blocked or kinked. A kink in the grafts or a
bdflarb
pnp
ftuCa
I
TtatH2ilKcDHaLthcotapRL2Ir8
D
T
sscgc
CfiNpHfDrrHr
A
b2
R
S36 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
lockage of the inflow cannula results in a higher pressureifference across the pump and, consequently, lower pumpow. Because such flow restrictions do not influence thection of the pump rotor, the flow estimator will reflect theeduction in flow. If the HeartMate II estimated flow iselow about 3 liters/min the flow display will be “���.”
With decrease in flow, there is also a decrease in pumpower. A flow obstruction will limit pump flow, so theormal unloading of the LV associated with increasingump speed will be diminished or absent.
The location of a flow obstruction cannot be determinedrom the pump parameters because the pump only respondso the differential pressure across the pump, and changespstream or downstream of the pump have identical effects.T, angiography, or echocardiography may be useful inssessing the location of a flow obstruction.
X. Results from completed clinical trials
he first continuous-flow LVAD to complete FDA clinicalrials for BTT and for DT is the HeartMate II. Other devicesre in ongoing trials and results will be published after thoserials are completed. The BTT clinical trial for theeartMate II resulted in FDA market approval in April008. Of the 489 patients in the BTT trial, the results in thenitial 133 patients were published,7 and an 18 month fol-ow-up analysis has been completed in 281 patients.8 Theaplan-Meier survival at 12 months was 68% in the initial
ohort7 and 73% after inclusion of additional patients.8 TheT trial, with a randomized comparison between theeartMate II and the HeartMate XVE, was also completed,
nd details on the first cohort of patients who received aVAD from March 2005 to May 2007 were published in
he New England Journal of Medicine.1 The HeartMate IIad a highly significantly increased percentage of patientsompared with the XVE who reached the primary end pointf survival at 2 years free of disabling stroke and reopera-ion for pump replacement. The actuarial survival of 68%nd 58% at 1 and 2 years was significantly improved com-ared with the 55% and 24% for the HeartMate XVE.esults of additional cohorts of DT patients who receivedVADs later in the trial will be published as they reach-year end-points. Since FDA approval for BTT, HeartMateI patients have been tracked by INTERMACS and initialesults in over 500 patients show a six month survival of8%.20
isclosure Statement
his supplement was supported by Thoratec.The authors disclose the following: Dr Slaughter, grant
upport from Thoratec and HeartWare; Dr Pagani, grantupport from Terumo, HeartWare, and Thoratec; Dr Rogers,onsulting fees and grant support from Thoratec; Dr Miller,rant support and paid speaking from Thoratec; Dr Sun,
onsulting fees from Thoratec, ABIOMED, HeartWare,ardioMEMS, and Sunshine Heart; Dr Russell, consultingees and grant support from Thoratec; Dr Starling, consult-ng fees from Medtronic and Wellpoint, grant support fromovartis, Thoratec, Medtronic, NIH, and XDx, other sup-ort from XDx; Dr Chen, Clinical Event Committee,eartWare; Dr Boyle, consulting fees and paid speaking
rom Thoratec; Ms Chilcott, paid speaking from Thoratec;r Adamson, consulting fees and paid speaking from Tho-
atec; Dr Petty, paid speaking and grant support from Tho-atec; Mr Myers, consulting fees from Thoratec andeartWare; and Dr Farrar, employee and stock holder, Tho-
atec.
ppendix. Supplementary data
Supplementary data associated with this article cane found, in the online version, at doi:10.1016/j.healun.010.01.011.
eferences
1. Slaughter MS, Rogers JG, Milano CA, et al. Advanced heart failuretreated with continuous-flow left ventricular assist device. N EnglJ Med 2009;361:2241-51.
2. Goldstein D, Zucker M, Pagani FD, Frazier OH. Rotary ventricularassist devices. In: Kirklin JK, Frazier OH, editor. ISHLT monographseries: mechanical circulatory support. New York: Elsevier; 2006. p.77-104.
3. Lahpor J. State of the art: implantable ventricular assist devices. CurrOpin Organ Transplant 2009:16.
4. John R. Current axial-flow devices—the HeartMate II and Jarvik2000 left ventricular assist devices. Semin Thorac Cardiovasc Surg2008;20:264-72.
5. Simon MA, Watson J, Baldwin JT, Wagner WR, Borovetz HS.Current and future considerations in the use of mechanical circulatorysupport devices. Annu Rev Biomed Eng 2008;10:59-84.
6. Kirklin JK, Holman WL. Mechanical circulatory support therapy asa bridge to transplant or recovery (new advances). Curr Opin Cardiol2006;21:120-6.
7. Miller LW, Pagani FD, Russell SD, et al. Use of a continuous-flowdevice in patients awaiting heart transplantation. N Engl J Med2007;357:885-96.
8. Pagani FD, Miller LW, Russell SD, et al. Extended mechanicalcirculatory support with a continuous-flow rotary left ventricularassist device. J Am Coll Cardiol 2009;54:312-21.
9. Fang JC. Rise of the machines—left ventricular assist devices aspermanent therapy for advanced heart failure. N Engl J Med 2009;361:1-3.
10. Advanced practice guidelines for HeartMate destination therapy. Vol1. Pleasanton, CA: Thoratec Corporation; 2004.
11. Advanced practice guidelines for HeartMate destination therapy. Vol2. Pleasanton, CA: Thoratec Corporation; 2004.
12. Westaby S, Siegenthaler M, Beyersdorf F, et al. Destination therapywith a rotary blood pump and novel power delivery. Eur J Cardio-thorac Surg 2009 [in press, doi:10.1016/j.ejcts.2009.03.071].
13. Morshuis M, El-Banayosy A, Arusoglu L, et al. European experience ofDuraHeart magnetically levitated centrifugal left ventricular assist sys-tem. Eur J Cardiothorac Surg 2009;35:1020-7; discussion 1027-8.
14. Loforte A, Montalto A, Ranocchi F, et al. HeartMate II axial-flow leftventricular assist system: management, clinical review and personalexperience. J Cardiovasc Med (Hagerstown) 2009;10:765-71.
15. Lahpor J, Khaghani A, Hetzer R, et al. European results with a
continuous-flow ventricular assist device for advanced heart-failure
S37Slaughter et al. Management of Continuous-Flow LVADs
patients. Eur J Cardiothorac Surg 2009[in press, doi:10.1016/j.ejcts.2009.05.043].
16. Strueber M, Birks E, Jansz P, O’Driscoll G, Wiesenthaler, G. Clinicalresults of the international HeartWare LVAS bridge to transplanttrial. J Heart Lung Transplant 2009;28:S255.
17. Aaronson KD, Schwartz JS, Chen TM, Wong KL, Goin JE, ManciniDM. Development and prospective validation of a clinical index topredict survival in ambulatory patients referred for cardiac transplantevaluation. Circulation 1997;95:2660-7.
18. Levy WC, Mozaffarian D, Linker DT, et al. The Seattle heart failuremodel: prediction of survival in heart failure. Circulation 2006;113:1424-33.
19. Levy WC, Mozaffarian D, Linker DT, Farrar DJ, Miller LW. Can theSeattle heart failure model be used to risk-stratify heart failure pa-tients for potential left ventricular assist device therapy? J Heart LungTransplant 2009;28:231-6.
20. Kirklin JK, Naftel DC, Kormos RL, et al. Second INTERMACSannual report: More than 1,000 primary left ventricular assist deviceimplants. J Heart Lung Transplant 2010;29:1-10.
21. Holman WL, Pae WE, Teutenberg JJ, et al. INTERMACS: intervalanalysis of registry data. J Am Coll Surg 2009;208:755-61; discus-sion 61-2.
22. Stevenson LW, Pagani FD, Young JB, et al. INTERMACS profiles ofadvanced heart failure: the current picture. J Heart Lung Transplant2009;28:535-41.
23. Farrar DJ. Preoperative predictors of survival in patients with Thor-atec ventricular assist devices as a bridge to heart transplantation.Thoratec Ventricular Assist Device Principal Investigators. J HeartLung Transplant 1994;13:93-100; discussion 101.
24. Oz MC, Goldstein DJ, Pepino P, et al. Screening scale predictspatients successfully receiving long-term implantable left ventricularassist devices. Circulation 1995;92:II169-73.
25. Rao V, Oz MC, Flannery MA, Catanese KA, Argenziano M, Naka Y.Revised screening scale to predict survival after insertion of a leftventricular assist device. J Thorac Cardiovasc Surg 2003;125:855-62.
26. Lin CY, Tsai FC, Tian YC, et al. Evaluation of outcome scoringsystems for patients on extracorporeal membrane oxygenation. AnnThorac Surg 2007;84:1256-62.
27. Lietz K, Long JW, Kfoury AG, et al. Outcomes of left ventricularassist device implantation as destination therapy in the post-REMATCH era: implications for patient selection. Circulation 2007;116:497-505.
28. Mano A, Fujita K, Uenomachi K, et al. Body mass index is a usefulpredictor of prognosis after left ventricular assist system implanta-tion. J Heart Lung Transplant 2009;28:428-33.
29. Holdy K, Dembitsky W, Eaton LL, et al. Nutrition assessment andmanagement of left ventricular assist device patients. J Heart LungTransplant 2005;24:1690-6.
30. Lockard KL, Degore L, Schwarm P, et al. Lack of improvement inprealbumin at two weeks predicts a poor outcome after mechanicalcirculatory support. J Heart Lung Transplant 2009;28:S66.
31. Farrar DJ, Compton PG, Hershon JJ, Fonger JD, Hill, J.D. Right heartinteraction with the mechanically assisted left heart. World J Surg1985;9:89-102.
32. Frazier OH, Rose EA, Oz MC, et al. Multicenter clinical evaluationof the HeartMate vented electric left ventricular assist system inpatients awaiting heart transplantation. J Thorac Cardiovasc Surg2001;122:1186-95.
33. Farrar DJ, Hill JD, Pennington DG, et al. Preoperative and postop-erative comparison of patients with univentricular and biventricularsupport with the Thoratec ventricular assist device as a bridge tocardiac transplantation. J Thorac Cardiovasc Surg 1997;113:202-9.
34. Kormos RL, Teuteberg JJ, Pagani FD, et al. Right ventricular failurein patients with the HeartMate II continuous flow left ventricularassist device: incidence, risk factors, and impact on outcomes. J Tho-rac Cardiovasc Surg 2010[in press].
35. Fitzpatrick JR 3rd, Frederick JR, Hsu VM, et al. Risk score derivedfrom pre-operative data analysis predicts the need for biventricularmechanical circulatory support. J Heart Lung Transplant 2008;27:
1286-92.36. Matthews JC, Koelling TM, Pagani FD, Aaronson KD. The rightventricular failure risk score a pre-operative tool for assessing the riskof right ventricular failure in left ventricular assist device candidates.J Am Coll Cardiol 2008;51:2163-72.
37. Ochiai Y, McCarthy PM, Smedira NG, et al. Predictors of severeright ventricular failure after implantable left ventricular assist deviceinsertion: analysis of 245 patients. Circulation 2002;106:I198-202.
38. Schenk S, McCarthy PM, Blackstone EH, et al. Duration of inotropicsupport after left ventricular assist device implantation: risk factorsand impact on outcome. J Thorac Cardiovasc Surg 2006;131:447-54.
39. Loforte A, Potapov E, Krabatsch T, et al. Levitronix CentriMag toBerlin Heart Excor: a “bridge to bridge” solution in refractory car-diogenic shock. ASAIO J 2009;55:465-8.
40. Haj-Yahia S, Birks EJ, Amrani M, et al. Bridging patients aftersalvage from bridge to decision directly to transplant by means ofprolonged support with the CentriMag short-term centrifugal pump.J Thorac Cardiovasc Surg 2009;138:227-30.
41. Gregoric ID, Jacob LP, La Francesca S, et al. The TandemHeart as abridge to a long-term axial-flow left ventricular assist device (bridgeto bridge). Tex Heart Inst J 2008;35:125-9.
42. Farrar DJ. The Thoratec ventricular assist device: a paracorporealpump for treating acute and chronic heart failure. Semin ThoracCardiovasc Surg 2000;12:243-50.
43. Fitzpatrick JR 3rd, Frederick JR, Hiesinger W, et al. Early plannedinstitution of biventricular mechanical circulatory support results inimproved outcomes compared with delayed conversion of a leftventricular assist device to a biventricular assist device. J ThoracCardiovasc Surg 2009;137:971-7.
44. Galie N, Ghofrani HA, Torbicki A, et al. Sildenafil citrate therapy forpulmonary arterial hypertension. N Engl J Med 2005;353:2148-57.
45. Klodell CT Jr, Morey TE, Lobato EB, et al. Effect of sildenafil onpulmonary artery pressure, systemic pressure, and nitric oxide utili-zation in patients with left ventricular assist devices. Ann ThoracSurg 2007;83:68-71; discussion
46. Sandner SE, Zimpfer D, Zrunek P, et al. Renal function and outcomeafter continuous flow left ventricular assist device implantation. AnnThorac Surg 2009;87:1072-8.
47. Ma L, Fujino Y, Matsumiya G, Sawa Y, Mashimo T. Renal functionwith left ventricular assist devices: the poorer the preoperative renalfunction, the longer the recovery. Med Sci Monit 2008;14:CR621-7.
48. Butler J, Geisberg C, Howser R, et al. Relationship between renalfunction and left ventricular assist device use. Ann Thorac Surg2006;81:1745-51.
49. Levey AS, Stevens LA, Schmid CH, et al. A new equation to estimateglomerular filtration rate. Ann Intern Med 2009;150:604-12.
50. Aaronson KD, Patel H, Pagani FD. Patient selection for left ventric-ular assist device therapy. Ann Thorac Surg 2003;75:S29-35.
51. Russell SD, Rogers JG, Milano CA, et al. Renal and hepatic functionimprove in advanced heart failure patients during continuous-flowsupport with the HeartMate II left ventricular assist device. Circula-tion 2009;120:2352-7.
52. Boyle AJ, Russell SD, Teuteberg JJ, et al. Low thromboembolismand pump thrombosis with the HeartMate II left ventricular assistdevice: analysis of outpatient anti-coagulation. J Heart Lung Trans-plant 2009;28:881-7.
53. Reinhartz O, Farrar DJ, Hershon JH, Avery GJ Jr, Haeusslein EA,Hill JD. Importance of preoperative liver function as a predictor ofsurvival in patients supported with Thoratec ventricular assist devicesas a bridge to transplantation. J Thorac Cardiovasc Surg 1998;116:633-40.
54. Radovancevic B, Vrtovec B, de Kort E, Radovancevic R, GregoricID, Frazier OH. End-organ function in patients on long-term circu-latory support with continuous- or pulsatile-flow assist devices.J Heart Lung Transplant 2007;26:815-8.
55. Letsou GV, Myers TJ, Gregoric ID, et al. Continuous axial-flow leftventricular assist device (Jarvik 2000) maintains kidney and liverperfusion for up to 6 months. Ann Thorac Surg 2003;76:1167-70.
56. Warkentin TE, Greinacher A, Koster A. Heparin-induced thrombo-cytopenia in patients with ventricular assist devices: are new preven-
tion strategies required? Ann Thorac Surg 2009;87:1633-40.
S38 The Journal of Heart and Lung Transplantation, Vol 29, No 4S, April 2010
57. Morel-Kopp MC, Aboud M, Tan CW, Kulathilake C, Ward C. Wholeblood impedance aggregometry detects heparin-induced thrombo-cytopenia antibodies. Thromb Res 2010[in press, doi:10.1016/j.thromres.2009.12.001].
58. Levy JH, Winkler AM. Heparin-induced thrombocytopenia and car-diac surgery. Curr Opin Anaesthesiol 201023:74-9.
59. Kormos RL, Teuteberg JJ, Siegenthaler MP, et al. Pre-VAD implantrisk factors influence the onset of adverse events (AEs) while onVAD. J Heart Lung Transplant 2009;28:S153.
60. Chinn R, Dembitsky W, Eaton L, et al. Multicenter experience:prevention and management of left ventricular assist device infec-tions. ASAIO J 2005;51:461-70.
61. Tylus-Earl N, Chillcott S. Mental health and medical challenges.Management of a depressed patient with a left ventricular assistsystem in an inpatient psychiatric setting. J Psychosoc Nurs MentHealth Serv 2009;47:43-9; quiz 51.
62. Pal JD, Klodell CT, John R, et al. Low operative mortality withimplantation of a continuous-flow left ventricular assist device andimpact of concurrent cardiac procedures. Circulation 2009;120:S215-9.
63. Mudd JO, Cuda JD, Halushka M, Soderlund KA, Conte JV, RussellSD. Fusion of aortic valve commissures in patients supported by acontinuous axial flow left ventricular assist device. J Heart LungTransplant 2008;27:1269-74.
64. Matthews JC, Aaronson KD, Jain R, Pagani FD, Kolias, T.J. Aorticinsuffciency—trends over time in LVAD supported patient. J HeartLung Transplant 2009;28:S306.
65. Haghi D, Suselbeck T, Saur J. Aortic regurgitation during left ven-tricular assist device support. J Heart Lung Transplant 2007;26:1220-1.
66. Park SJ, Liao KK, Segurola R, Madhu KP, Miller LW. Managementof aortic insufficiency in patients with left ventricular assist devices:a simple coaptation stitch method (Park’s stitch). J Thorac Cardio-vasc Surg 2004;127:264-6.
67. Stringham JC, Bull DA, Karwande SV. Patch closure of the aorticanulus in a recipient of a ventricular assist device. J Thorac Cardio-vasc Surg 2000;119:1293-4.
68. Rao V, Slater JP, Edwards NM, Naka Y, Oz MC. Surgical manage-ment of valvular disease in patients requiring left ventricular assistdevice support. Ann Thorac Surg 2001;71:1448-53.
69. Feldman CM, Silver MA, Sobieski MA, Slaughter MS. Managementof aortic insufficiency with continuous flow left ventricular assistdevices: bioprosthetic valve replacement. J Heart Lung Transplant2006;25:1410-2.
70. Butany J, Leong SW, Rao V, et al. Early changes in bioprostheticheart valves following ventricular assist device implantation. IntJ Cardiol 2007;117:e20-3.
71. HeartMate II LVAS: Instructions for use. Pleasanton, CA: ThoratecCorporation; 2008.
72. Chen JM, Rose EA. Management of perioperative right-sided circu-latory failure. In: Goldstein DJ, Oz M, eds. Cardiac assist devices.Armonk, NY: Futura Publishing Co Inc; 2000. p 83-101.
73. Nakashima K, Kirsch ME, Vermes E, Rosanval O, Loisance D.Off-pump replacement of the INCOR implantable axial-flow pump.J Heart Lung Transplant 2009;28:199-201.
74. Frazier OH, Gregoric ID, Cohn WE. Initial experience with non-thoracic, extraperitoneal, off-pump insertion of the Jarvik 2000 Heartin patients with previous median sternotomy. J Heart Lung Trans-plant 2006;25:499-503.
75. Sun BC, Firstenberg MS, Louis LB, et al. Placement of long-termimplantable ventricular assist devices without the use of cardiopul-monary bypass. J Heart Lung Transplant 2008;27:718-21.
76. Augoustides JG, Ochroch EA. Inhaled selective pulmonary vasodi-lators. Int Anesthesiol Clin 2005;43:101-14.
77. Augoustides JG, Ochroch EA. Pro: inhaled prostaglandin as a pul-monary vasodilator instead of nitric oxide. J Cardiothorac VascAnesth 2005;19:400-2.
78. De Wet CJ, Affleck DG, Jacobsohn E, et al. Inhaled prostacyclin is
safe, effective, and affordable in patients with pulmonary hyperten-sion, right heart dysfunction, and refractory hypoxemia aftercardiothoracic surgery. J Thorac Cardiovasc Surg 2004;127:1058-67.
79. Dickstein ML. Con: inhaled prostaglandin as a pulmonary vasodilatorinstead of nitric oxide. J Cardiothorac Vasc Anesth 2005;19:403-5.
80. Tector AJ, Kress DC, Downey FX, Schmahl TM, Dasse KA, PoirierVL. Transition from cardiopulmonary bypass to the HeartMate leftventricular assist device. Ann Thorac Surg 1998;65:643-6.
81. Stainback RF, Croitoru M, Hernandez A, Myers TJ, Wadia Y, FrazierOH. Echocardiographic evaluation of the Jarvik 2000 axial-flowLVAD. Tex Heart Inst J 2005;32:263-70.
82. Catena E, Milazzo F. Echocardiography and cardiac assist devices.Minerva Cardioangiol 2007;55:247-65.
83. Chumnanvej S, Wood MJ, MacGillivray TE, Melo MF. Perioperativeechocardiographic examination for ventricular assist device implan-tation. Anesth Analg 2007;105:583-601.
84. Augoustides JG. Perioperative echocardiographic assessment of leftventricular assist device implantation: additional causes of inflowcannula obstruction. Anesth Analg 2008;106:673-4; author reply 4.
85. Gregoric ID. Exchange techniques for implantable ventricular assistdevices. ASAIO J 2008;54:14-9.
86. Gregoric ID, Bruckner BA, Jacob L, et al. Clinical experience withsternotomy versus subcostal approach for exchange of the HeartMateXVE to the HeartMate II ventricular assist device. Ann Thorac Surg2008;85:1646-9.
87. La Francesca S, Smith R, Gregoric ID, et al. Replacement of amalfunctioning HeartMate II left ventricular assist device in a 14-year-old after a sudden fall. J Heart Lung Transplant 2006;25:862-4.
88. Lodge AJ. Clinical experience with sternotomy versus subcostalapproach for exchange of the HeartMate XVE to the HeartMate IIventricular assist device. Invited commentary. Ann Thorac Surg2008;85:1650.
89. Letsou GV, Connelly JH, Delgado RM 3rd, et al. Is native aorticvalve commissural fusion in patients with long-term left ventricularassist devices associated with clinically important aortic insuffi-ciency? J Heart Lung Transplant 2006;25:395-9.
90. Banchs JE, Dawn B, Abdel-Latif A, et al. Acquired aortic cusp fusionafter chronic left ventricular assist device support. J Am Soc Echo-cardiogr 2006;19:1401 e1-3.
91. Amir O, Bracey AW, Smart FW, Delgado RM 3rd, Shah N, Kar B.A successful anticoagulation protocol for the first HeartMate II im-plantation in the United States. Tex Heart Inst J 2005;32:399-401.
92. Frazier OH, Delgado RM 3rd, Kar B, Patel V, Gregoric ID, Myers TJ.First clinical use of the redesigned HeartMate II left ventricular assistsystem in the United States: a case report. Tex Heart Inst J 2004;31:157-9.
93. John R, Kamdar F, Liao K, et al. Low thromboembolic risk forpatients with the HeartMate II left ventricular assist device. J ThoracCardiovasc Surg 2008;136:1318-23.
94. Struber M, Sander K, Lahpor J, et al. HeartMate II left ventricularassist device; early European experience. Eur J Cardiothorac Surg2008;34:289-94.
95. John R, Kamdar F, Liao K, Colvin-Adams M, Boyle A, Joyce L.Improved survival and decreasing incidence of adverse events withthe HeartMate II left ventricular assist device as bridge-to-transplanttherapy. Ann Thorac Surg 2008;86:1227-34; discussion 34-5.
96. Slaughter MS, Naka Y, John R, et al. Postoperative heparin may notbe required in transitioning patients with HeartMate II LVAD to longterm warfarin therapy. J Heart Lung Transplant 2010[in press].
97. Basra SS, Attallab AA, Wagle R, Loyalka R, Kar, B. Infections inpatients on continuous flow LVAD: epidemiology and role in causa-tion of cerebrovascular accidents. J Heart Lung Transplant 2009;28:S285.
98. Tulchinsky M. Lower gastrointestinal bleeding diagnosed by redblood cell scintigraphy in a patient with a left ventricular assistdevice. Clin Nucl Med 2008;33:856-8.
99. Daas AY, Small MB, Pinkas H, Brady PG. Safety of conventionaland wireless capsule endoscopy in patients supported with nonpul-satile axial flow Heart-Mate II left ventricular assist device. Gas-
trointest Endosc 2008;68:379-82.
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
1
S39Slaughter et al. Management of Continuous-Flow LVADs
00. Garatti A, Bruschi G, Girelli C, Vitali E. Small intestine capsuleendoscopy in magnetic suspended axial left ventricular assist devicepatient. Interact Cardiovasc Thorac Surg 2006;5:1-4.
01. Letsou GV, Shah N, Gregoric ID, Myers TJ, Delgado R, Frazier OH.Gastrointestinal bleeding from arteriovenous malformations in pa-tients supported by the Jarvik 2000 axial-flow left ventricular assistdevice. J Heart Lung Transplant 2005;24:105-9.
02. Malehsa D, Meyer AL, Bara C, Strüber M. Acquired von Willebrandsyndrome after exchange of the HeartMate XVE to the HeartMate IIventricular assist device. Eur J Cardiothorac Surg 2009;35:1091-3.
03. Klovaite J, Gustafsson F, Mortensen SA, Sander K, Nielsen LB.Severely impaired von Willebrand factor-dependent platelet aggre-gation in patients with a continuous-flow left ventricular assist device(HeartMate II). J Am Coll Cardiol 2009;53:2162-7.
04. Geisen U, Heilmann C, Beyersdorf F, et al. Non-surgical bleedingin patients with ventricular assist devices could be explained byacquired von Willebrand disease. Eur J Cardiothorac Surg 2008;33:679-84.
05. Myers TJ, Bolmers M, Gregoric ID, Kar B, Frazier OH. Assessmentof arterial blood pressure during support with an axial flow leftventricular assist device. J Heart Lung Transplant 2009;28:423-7.
06. Frazier OH, Myers TJ, Gregoric ID, et al. Initial clinical experiencewith the Jarvik 2000 implantable axial-flow left ventricular assist
system. Circulation 2002;105:2855-60.07. HeartMate II left ventricular assist system: patient handbook. Pleas-anton, CA: Thoratec Corp; 2005.
08. HeartMate II left ventricular assist system (LVAS) community livingguide. Pleasanton, CA: Thoratec Corp; 2009.
09. Myers TJ, Frazier OH, Mesina HS, Radovancevic B, Gregoric ID.Hemodynamics and patient safety during pump-off studies of anaxial-flow left ventricular assist device. J Heart Lung Transplant2006;25:379-83.
10. Ueno A, Tomizawa Y. Cardiac rehabilitation and artificial heartdevices. J Artif Organs 2009;12:90-7.
11. MacIver J, Ross HJ, Delgado DH, et al. Community support ofpatients with a left ventricular assist device: The Toronto GeneralHospital experience. Can J Cardiol 2009;25:e377-81.
12. Oosterom A, de Jonge N, Kirkels JH, et al. End-stage heart failureand mechanical circulatory support: feasibility of discharge fromhospital. Neth Heart J 2007;15:45-50.
13. Drews TN, Loebe M, Jurmann MJ, Weng Y, Wendelmuth C, HetzerR. Outpatients on mechanical circulatory support. Ann Thorac Surg2003;75:780-5; discussion 5.
14. El-Menyar AA. Multidisciplinary approach for circulatory support inpatients with advanced heart failure. Expert Rev Cardiovasc Ther2009;7:259-62.
15. Seemuth SC, Richenbacher WE. Education of the ventricular assist
device patient’s community services. ASAIO J 2001;47:596-601.