clinical hematology wintrobe`s - szpiczak
TRANSCRIPT

Multiple Myeloma Angela Dispenzieri
Martha Q. Lacy
Phi l ip R. Greipp
Mul t ip le myeloma is a neoplast ic p lasma cel l dyscras ia (PCD) character ized by a c l in ica l
pentad: (a) anemia, (b) a monoc lonal protein in the serum or ur ine or both, (c ) abnormal
bone rad iographs and bone pain, (d) hyperca lcemia, and (e) renal insuff ic iency or fai lure.
W ith the except ion of monoclonal gammopathy of undetermined signi f icance (MGUS), i t is
the most common PCD, wi th an inc idence of about 4 .5 per 100,000 per year in the Uni ted
States. Sol i tary p lasmacytoma and plasma ce l l leukemia (PCL) are recognized as separate
ent i t ies and are much less prevalent . The under ly ing pathogenes is of the p lasma cel l
mal ignanc ies is not wel l unders tood but is an area of act ive invest igat ion. At present ,
according to the W HO (World Heal th Organizat ion) and REAL (Revised European-Amer ican
Lymphoma) c lass i f icat ion systems, there is only one category for mul t ip le myeloma (1).
Resul ts o f c l in ica l t r ia ls are confounded by th is underc lass i f icat ion. Emerg ing in formation
about the genet ic underpinning of the d isease, however, wi l l l ike ly change th is def ic iency.
The in teract ions among the plasma ce l ls, the i r ant ibody product , the local bone and bone
marrow envi ronment , and other organs are complex. There is no cure for mult ip le myeloma,
but there are many ef fect ive t reatments that pro long and improve the qual i ty of l i fe o f
pat ients wi th the d isease.
History
Earliest Diagnoses and Diagnostic Methods Samuel Sol ley repor ted the f i rst wel l -documented case of myeloma in Sarah Newbury in
1844 (mol l i t ies ossium) (2 ,3) . Several years la ter , W i l l iam MacIntyre described and recorded
the proper t ies of the disease we now cal l mul t ip le myeloma in Thomas Alexander McBean
(4) . Both Drs . MacIntyre and Bence Jones noted and described some of the pecul iar ur ine
proper t ies of th is same pat ient . On heat ing, the ur ine was found to “abound in animal
mat ter , ” which d isso lved on the addi t ion of n i t r ic ac id but reappeared af ter cool ing. These
ur inary prote ins became known as Bence Jones proteins (5). MacIntyre and Dal rymple
descr ibed the postmortem examinat ion of Mr. McBean's bones (4) . The former described the
af fec ted bones as sof tened and f ragi le , wi th thei r in ter iors replaced wi th a soft “ge la t in form”
b lood-red substance. Dal rymple suggested that the disease began in the cancel lous bone
and extended through the perios teum. The nucleated ce l ls , which formed the bu lk o f the
ge la t inous mater ia l , were heterogeneous in s ize and shape, but the majori ty were round to
ova l . Many of the larger and more i r regular ce l ls f requent ly contained two or three nuc le i (3) .
The term “mult ip le myeloma” was coined in 1873 by von Rust izky (6) , who independently
descr ibed a s imi lar pat ient to emphasize the mul t ip le bone tumors that were present .
In 1889, Professor Ot to Kahler (7) descr ibed a case involv ing a 46-year-o ld physic ian wi th
mult ip le myeloma and publ ished a major review of the disease. He descr ibed the ske le tal
pa in , albuminuria , pal lor , anemia, a precip i table ur inary prote in, and the f ind ings on
necroscopy and l inked these f ind ings as par t o f a c l in ical syndrome, which bears h is name
(mult ip le myeloma is a lso known as Kahler d isease) .
In 1898, W eber pred ic ted the usefu lness of roentgen x-rays in es tab l ish ing the diagnos is
(3 ,8) and la ter postula ted that the Bence Jones protein was produced in the bone marrow

(9) . W right (10) emphas ized that mult ip le myeloma arose spec i f ica l ly from p lasma cel ls o f
the marrow; Jacobson (11) recognized Bence Jones prote ins in the b loodstream; and
Walters (12) conc luded that the Bence Jones prote in was probably der ived f rom b lood
proteins through the act ion of the abnormal cel ls in the bone marrow. The technique of bone
marrow aspira t ion (13) fac i l i ta ted the d iagnosis o f mul t ip le myeloma.
Bayne-Jones and W ilson (14) ident i f ied two s imi lar but dist inc t groups of Bence Jones
proteins by immunizing rabbi ts wi th Bence Jones proteins der ived f rom pat ients . Prec ip i t in
tes ts on these Bence Jones preparat ions revealed two d is t inct groups: I and I I . Using the
Ouchter lony tes t , Korngold and L ipar i showed that ant isera to Bence Jones protein a lso
reacted wi th myeloma prote ins. The two classes of Bence Jones prote ins have been
designated κand λas a t r ibute to these two men. In 1962, Edelman and Gal ly (15) showed
that the l ight chains prepared f rom an IgG monoc lonal protein and the Bence Jones protein
f rom the same pat ient 's ur ine were ident ica l .
Serum elect rophoresis, descr ibed by Tise l ius in 1937 (16) , made i t poss ib le to separate
serum prote ins . Longsworth et al . (17) appl ied e lect rophoresis to the study of mult ip le
myeloma and descr ibed the ta l l , narrow-based “church sp i re” peak. The use of f i l ter paper
as a support for prote in e lec t rophores is permi t ted the separat ion of protein in to d is t inc t
zones that could be s ta ined wi th var ious dyes (18) . Because th is technique was s imple and
inexpensive, th is test became universal ly avai lable in c l in ical laborator ies. Paper
e lec t rophores is was supplanted by f i l ter paper in 1957 and most recent ly by h igh-resolut ion
e lec t rophores is on agarose ge l . Immunoelect rophoresis (19) and immunofixat ion or d i rec t
immunoelect rophoresis (20) made i t poss ib le to detect smal l monoc lonal l ight chains not
recognizable by elec t rophores is . The immunoglobul in free l ight -chain assay has been added
to the diagnost ic armamentarium to detect c i rcula t ing f ree l ight chains in the majori ty o f
pat ients hencetofor th des ignated nonsecretory (21) .
Kunkel (22) hypothes ized that monoclonal prote ins were the product of mal ignant p lasma
ce l ls and were the equiva lent of normal ant ibodies produced by normal p lasma cel ls . Before
1960, the term “gamma g lobul in” was used for any prote in that migrated in the gamma
mobi l i ty reg ion of the elec t rophoret ic pattern; however, in 1959, Heremans (23) proposed
the concept o f a fami ly of prote ins wi th ant ibody act iv i ty. In 1961, in a Harvey Lecture (24),
Waldenström d is t inguished between monoc lonal and polyc lonal hypergammaglobul inemia.
In 1928, Geschick ter and Copeland (25) repor ted on the largest case series of mul t ip le
myeloma—13 cases—and reviewed the 412 cases repor ted in the l i terature s ince 1848.
They documented a h igher incidence in men than women and an overal l surviva l of about 2
years . They emphas ized s ix features: (a) invo lvement o f the skele ta l t runk, (b) patho log ic
r ib f ractures, (c ) Bence Jones proteinur ia in 65% of cases, (d) backache wi th early
parapleg ia , (e) anemia in 77% of cases, and (f ) chronic renal disease. They d id not note
abnormal i t ies o f blood prote in or an increased erythrocyte
P.2373
sedimentat ion ra te (3) . In 1931, Magnus-Levy (26) descr ibed amylo idos is as a compl icat ion
of mul t ip le myeloma. Salmon, Durie , and Smi th developed methods to quant i ta te the to tal
body burden of tumor ce l ls (27) and to s tage pat ients (28) in 1970 and 1975, respect ively.
Earliest Treatments for Multiple Myeloma

In 1947 Snapper (29) repor ted that s t i lbamidine a long wi th a low-animal -protein d ie t
re l ieved myeloma pain in 14 of 15 pat ients . Subsequent s tud ies d id not conf i rm th is benef i t .
Urethane was bel ieved to be ef fect ive unt i l 1966 (30) . I t was f i rs t used in the treatment o f
mult ip le myeloma by Alwal l in 1947 (31,32) and then by Loge and Rundles in 1949 (31,32) .
Thei r ear ly observat ions were encouraging, and the use of urethane became widespread.
Toxic e f fects inc luded severe anorexia , nausea, and vomi t ing. Leukopenia,
thrombocytopenia, and hepat ic damage a lso occurred (33) . In 1966, however, Hol land et al .
(30) publ ished the resu l ts o f a randomized control led t r ia l o f urethane versus placebo in 83
pat ients wi th symptomatic mul t ip le myeloma. They found that there was no d i f ference in any
ob ject ive measurement of improvement between the two groups and that the median overa l l
surviva l was higher in the p lacebo group. Previous ly unt reated pat ients had a median
surviva l o f 12 or 5 months, depending on whether they received p lacebo or urethane,
respect ive ly.
In 1950, Thorn et a l . (34) repor ted the f i rst observat ions on the salu tary ef fects o f
adrenocor t icot rop ic hormones on myeloma (F ig . 99.1) . Dur ing that decade, i t was
recognized that the adrenocor t icot ropic hormones cor t isone and prednisone were usefu l
agents in pat ients wi th mul t ip le myeloma. Cort icostero ids decreased bone pain, improved
hyperca lcemia, increased hemoglobin va lues, and decreased abnormal serum and ur ine
g lobul in concentrat ions (33) . However, i t was not unt i l 1967 that h igh-dose cort icostero ids
were recognized as ef fec t ive ant ineoplast ic agents against mult ip le myeloma (35) .
Blokh in et a l . (36) reported benef i ts in three of s ix pat ients wi th mul t ip le myeloma who were
t reated wi th sarcolys in (a racemic mixture of the d - and l - isomers of phenyla lan ine mustard).
Subsequently, the d - and l - i somers were tes ted separate ly, and the ant imyeloma act iv i ty
was found to res ide in the l - isomer, melphalan. Bergsagel e t al . (37) repor ted s ign i f icant
improvement in 14 of 24 pat ients wi th mul t ip le myeloma wi th the use of melphalan; this
ac t iv i ty was qu ickly substant ia ted by others (38) . Simi lar e f fect iveness was noted wi th
cyc lophosphamide (39). Subsequently, in terferon-α , doxorubic in , carmust ine, thal idomide,
bor tezomib, and lenal idomide (40,41,42,43,44,45) have each been repor ted to have act iv i ty
as a s ing le agent in myeloma (F ig . 99.1) .
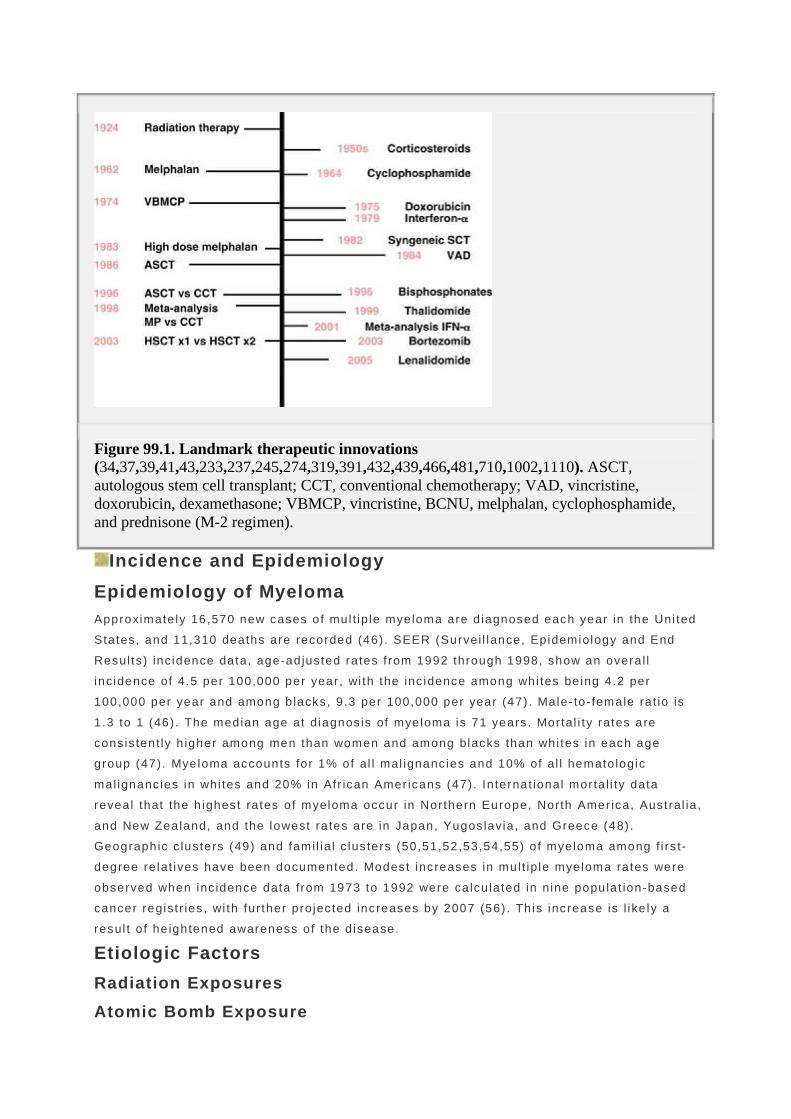
Figure 99.1. Landmark therapeutic innovations (34,37,39,41,43,233,237,245,274,319,391,432,439,466,481,710,1002,1110). ASCT, autologous stem cell transplant; CCT, conventional chemotherapy; VAD, vincristine, doxorubicin, dexamethasone; VBMCP, vincristine, BCNU, melphalan, cyclophosphamide, and prednisone (M-2 regimen).
Incidence and Epidemiology
Epidemiology of Myeloma Approximate ly 16,570 new cases of mul t ip le myeloma are d iagnosed each year in the Uni ted
States, and 11,310 deaths are recorded (46) . SEER (Surve i l lance, Epidemiology and End
Resul ts) incidence data, age-adjusted ra tes f rom 1992 through 1998, show an overa l l
incidence of 4.5 per 100,000 per year , wi th the inc idence among whi tes be ing 4.2 per
100,000 per year and among b lacks, 9 .3 per 100,000 per year (47) . Male- to- female ra t io is
1 .3 to 1 (46) . The median age at diagnos is of myeloma is 71 years . Mortal i ty rates are
cons is tent ly h igher among men than women and among blacks than whi tes in each age
group (47) . Myeloma accounts for 1% of al l mal ignanc ies and 10% of al l hemato logic
mal ignanc ies in whi tes and 20% in Afr ican Amer icans (47) . In ternat ional morta l i ty data
reveal that the h ighest ra tes of myeloma occur in Northern Europe, North Amer ica, Austral ia ,
and New Zealand, and the lowest ra tes are in Japan, Yugos lavia , and Greece (48) .
Geographic c lus ters (49) and fami l ia l c lus ters (50,51,52,53,54,55) o f myeloma among f i rs t-
degree re lat ives have been documented. Modest increases in mult ip le myeloma rates were
observed when inc idence data from 1973 to 1992 were ca lcu la ted in nine populat ion-based
cancer regist r ies , wi th fur ther projec ted increases by 2007 (56) . Th is increase is l ike ly a
resul t o f he ightened awareness of the d isease.
Etiologic Factors
Radiation Exposures
Atomic Bomb Exposure
Reports o f increased myeloma inc idence and morta l i ty among Japanese atomic bomb
survivors have suggested an assoc ia t ion between ion iz ing rad ia t ion and mult ip le myeloma.
Evaluat ions of cancer inc idence (57) and morta l i ty (58) among Japanese atomic bomb
survivors have demonstrated an increased r isk o f mul t ip le myeloma wi th increasing
rad ia t ion dose. However, wi th an addi t ional 12 years of fo l low-up f rom previous repor ts , the
f indings of an increased myeloma r isk assoc ia ted wi th a tomic bomb i r rad ia t ion were not
maintained (59) .
Radiation-Related Occupation An excess of myeloma deaths among U.S. rad io log is ts was repor ted in the 1960s (60) .
Myeloma r isk was considered to be two t imes h igher among radio logis ts exposed to low
doses of radia t ion than among phys ic ians not exposed to rad iat ion (61) . However, among
27,000 Chinese diagnost ic radiography workers, no excess inc idence of myeloma was
observed in a 30-year per iod (62). An analysis o f 115,000 workers f rom the combined roster
o f four d i f ferent nuclear p lants showed a pos i t ive assoc ia t ion between mul t ip le myeloma
and radia t ion exposure in o lder age groups (63) . No increases in mul t ip le myeloma
incidence and mortal i ty have been observed among Bri t ish (64) or New Zealand (65) mi l i tary
men who part ic ipated in a tmospheric nuc lear weapons tes t ing.
Diagnostic and Therapeutic X-rays Diagnost ic x- ray exposure has not been l inked wi th the development o f mul t ip le myeloma in
most ep idemiologic studies (66,67,68,69,70,71) . A large mul t icenter, populat ion-based
case-contro l study showed no evidence of excess r isk o f myeloma among indiv iduals who
reported exposure of 10 or more d iagnost ic rad iographs (72). One s tudy repor ted that the
overa l l r isk for mul t ip le myeloma was not high (RR, 1 .14) , but that there was evidence of
increas ing r isk wi th exposure to increasing numbers of rad iographic procedures (73).
P.2374
Of h is tor ic interest is the f ind ing of an associa t ion between myeloma and the use of
Thorot ras t (67) . Stud ies of the ef fec ts of therapeut ic i r radia t ion on myeloma r isk have
shown conf l ic t ing resu l ts, but a s tudy of 180,000 women t reated for cervica l cancer
demonstrated no overal l excess r isk o f develop ing myeloma (74) . Simi lar ly, a study of
14,000 pat ients suf fer ing f rom ankylos ing spondyl i t is and t reated wi th rad ia t ion revealed no
s ign i f icant increase in the r isk o f developing myeloma (75) .
Workplace Exposures
Agricultural Occupations and Exposures Severa l epidemio log ic s tud ies have evaluated the r isk o f myeloma among agricul tura l
workers , wi th pos i t ive assoc iat ions repor ted by many (76,77,78,79,80,81) but not a l l of the
s tud ies (82,83,84) . Khuder and Mutg i (85) found a rela t ive r isk o f 1 .23 in a meta-analys is o f
several s tud ies .
Metal Industries Workers in var ious metal occupat ions and industr ies have been repor ted to have an
increased myeloma r isk (86,87,88) .
Benzene

Benzene has been suggested as a poss ib le e t io log ic agent for mult ip le myeloma (89,90,91) .
A comprehensive review of publ ished l i terature found no evidence of a l ink between
benzene exposure and myeloma (92) . Subsequently, Sonoda and co l leagues (93) conducted
a meta-analys is o f case-contro l studies and showed no excess r isk for the development of
mult ip le myeloma. A meta-analysis by W ong and Raabe (94) o f more than 350,000
petroleum workers s imi lar ly showed no increased r isk .
Lifestyle Factors
Cigarette Smoking and Alcohol Consumption Mul t ip le s tud ies to date have found no et io logic ro le for c igaret te smoking or alcohol
consumption in the development o f mul t ip le myeloma (95,96,97,98).
Dietary Links Tavani e t a l . (99) suggested a die tary l ink for mult ip le myeloma and found a higher r isk
among people consuming large quant i t ies o f l iver (odds ra t io [OR], 2 .0) and but ter (OR, 2 .8) ,
and a lower r isk among people consuming large amounts of vegetables (OR, 0.4) . Cof fee
and a lcohol had no assoc iat ion wi th mul t ip le myeloma. No associa t ion of mult ip le myeloma
and consumpt ion of red meat has been found (99) . Brown and co l leagues (100) looked at
d ie t and nutr i t ion as r isk factors for mult ip le myeloma among blacks and whi tes in the
Uni ted States. Elevated r isks were assoc ia ted wi th obes i ty in comparison to people of
normal weight . Obes i ty was more f requent in b lack than in whi te contro ls. Reduced r isks
were associated wi th the f requent in take of c ruc i ferous vegetables, f ish, and vi tamin C
supplements . The authors conc luded that the greater use of v i tamin C supplements by
whi tes and the higher f requency of obesi ty among b lacks may expla in par t o f the higher
incidence of mult ip le myeloma among b lacks compared wi th whi tes in the United States.
Socioeconomic Status Some invest igators have repor ted that there is an inverse re la t ionship between the r isk o f
mult ip le myeloma and soc ioeconomic s tatus (101) and that th is inverse corre lat ion may
account for a substant ia l amount o f the black and whi te di f ferent ial of mul t ip le myeloma
incidence (102). Earl ier s tud ies d id not show a l ink between soc ioeconomic s tatus and
myeloma (103) .
Hair Dyes Personal use of ha ir dyes was evaluated as a r isk fac tor for myeloma (104) , including two
prospect ive s tudies (105,106). Thun et a l . (105) found that women us ing permanent ha i r
dyes are not general ly at increased r isk of fata l cancer . W omen wi th pro longed use of dark ,
par t icular ly b lack, hai r dyes may have increased r isk of fata l non-Hodgkin lymphoma and
mult ip le myeloma, but these women are a smal l f rac t ion of hai r -dye users. A subsequent
meta-analysis by Correa et al . (107) showed no increased r isk .
Precursor Medical Conditions
Monoclonal Gammopathy of Undetermined Significance MGUS is cons idered a potent ial precursor condit ion for mult ip le myeloma. In a long-term
s tudy of prognos is in MGUS, Kyle and col leagues (108) ident i f ied 1,384 pat ients in
southeastern Minnesota in whom MGUS was d iagnosed. Dur ing 11,009 person-years of
fo l low-up, 115 of the 1,384 MGUS pat ients progressed to mul t ip le myeloma, IgM lymphoma,

pr imary amyloidos is , macroglobul inemia, chronic lymphocyt ic leukemia, or p lasmacytoma.
The r isk o f progress ion of MGUS to mult ip le myeloma-re la ted disorders is thus ~1% per
year (109) . Among a group of 1 ,231 pat ients in I ta ly wi th MGUS and smolder ing mul t ip le
myeloma, cumulat ive t ransformat ion probabi l i t ies a t 10 and 15 years were 14 and 30%,
respect ive ly (110) . A h igher ra te of MGUS in Afr ican Amer icans accounts for par t o f the
increased incidence of myeloma in th is populat ion (111) .
Chronic Antigenic Stimulation Repeated or chronic ant igenic s t imulat ion of the immune system may lead to myeloma.
Severa l case-contro l led s tud ies have suggested that myeloma r isk is assoc iated wi th a past
h istory of in fec t ions, in f lammatory condi t ions, connect ive t issue d isorders, auto immune
i l lnesses, and al lergy-rela ted d isorders (96,112,113) . Increased r isks of myeloma have been
observed in pat ients wi th rheumato id ar thr i t is (54,114,115) . Other s tud ies of ind iv iduals wi th
these condit ions have shown no increased r isk o f mul t ip le myeloma (116,117,118,119) .
Viral Infections Pat ients wi th the human immunodef ic iency v i rus may have an increased l ike l ihood of
develop ing myeloma (120,121) . In addi t ion, myeloma and hepat i t is C may be assoc iated
(122,123,124) . The f inding of human herpes vi rus 8 has been suggested as a poss ible
e t io log ic agent (125) , but this has not been conf i rmed (126,127,128,129) .
Clinical Manifestations The symptoms of mul t ip le myeloma may be nonspeci f ic and inc lude fat igue, bone pain, easy
bru isabi l i ty and b leeding, recurrent in fect ions, mani festat ions of anemia, hyperca lcemia,
ly t ic bone les ions, hyperviscosi ty, thrombocytopenia, and hypogammaglobul inemia (F ig .
99.2). W eakness, infec t ion, b leeding, and weight loss are repor ted in as many as 82, 13, 13,
and 24% of pat ients , respect ive ly (130,131,132,133). Hyperca lcemia is present in 18 to 30%
of pat ients (130,131,132) . One th i rd to two thi rds of pat ients present wi th spontaneous bone
pain (130,131,132) . “Tumor fever” is present in <1% of present ing pat ients .
Anemia The most common c l in ica l feature of mul t ip le myeloma is anemia. A hemoglob in
concentrat ion of <120 g/L occurs in 40 to 73% of pat ients a t presentat ion (130,131,132) and
contr ibutes to the weakness and fa t igue observed in as many as 82% of pat ients
(130,131,132) . The anemia is normochromic , normocyt ic in most pat ients, but macrocytosis
may be observed as wel l . W hen there are high concentrat ions of serum immunoglobul in ,
rou leau format ion may be observed (Fig . 99.3) . The combinat ion of anemia and
hyperproteinemia leads to a marked increase of the erythrocyte sedimentat ion rate in >90%
of cases (134) .
P.2375

Figure 99.2. Signs and symptoms of 1,027 newly diagnosed myeloma patients seen at the Mayo Clinic from 1985 trhrough 1998.
The anemia is re lated par t ia l ly to d irect in f i l t ra t ion and rep lacement o f the bone marrow.
Hemoglobin concentrat ion is also correla ted d i rect ly wi th the percentage of myeloma ce l ls in
S phase (135) , suggest ing that the bone marrow cytok ine mi l ieu, permissive for myeloma
ce l l pro l i ferat ion, is not conduc ive to ef f ic ient erythropoies is . Cytok ines, l ike tumor necrosis
fac tor-α (TNF-α ) and in ter leukin-1 ( IL-1) , may inh ibi t erythropoiesis (136) . Fas l igand-
mediated erythroid apoptos is is a lso increased in pat ients wi th myeloma (137) . F ina l ly,
re lat ive erythropoiet in def ic iency from myeloma-induced renal insuf f ic iency a lso contr ibutes
to the observed anemia.
Monoclonal Proteins The M prote in (M component, myeloma prote in , or M sp ike) is a hal lmark of the disease;
97% of myeloma pat ients have ei ther an in tac t immunoglobul in or a f ree l ight chain that can
be detected by prote in elec t rophores is (Fig . 99.4), immunoelect rophores is, or
immunof ixat ion s tud ies of the serum or ur ine (130,132). Those cases wi thout a detectab le
monoclonal prote in have been referred to as nonsecretory myeloma, which had accounted
for ~1 to 3% of myeloma cases. W ith the immunoglobul in f ree l ight-chain assay, smal l
quant i t ies of f ree l ight -chain monoc lonal prote ins , previously not seen by o lder methods, are
detected in approximately two th i rds of the cases we had referred to as nonsecretory(21) .
His tor ica l ly, monoclonal proteins have had a va luable role in the f ie lds of immunology and
molecular bio logy, for d is t inguish ing MGUS f rom myeloma and for ca lculat ing myeloma
tumor burden and k inet ics (27,108,138). Pract ica l ly, both serum and urine M-prote in
concentrat ions are used to stage myeloma pat ients and to document the i r response to
t reatment .

Figure 99.3. Rouleaux.
Figure 99.4. A: Serum protein electrophoresis. B: Immunofixation pattern.
An M prote in represents overproduct ion of a homogeneous immunoglobul in or
immunoglobul in f ragment . In a series of 1 ,027 newly d iagnosed cases of myeloma, the

immunoglobul in type was IgG, IgA, IgD, and free l ight chain only (Bence Jones myeloma) in
52, 20, 2 , and 16% of cases, respect ive ly (132) . Fewer than 1% of myelomas are IgM; most
IgM monoc lonal proteins are assoc ia ted wi th diagnoses of MGUS, lymphoma, W aldenström
macroglobul inemia, or pr imary systemic amylo idos is (139) . Ninety- three percent o f pat ients
have a monoc lonal protein detected in thei r serum. About 90% of myeloma pat ients have
reduct ions in at least one of thei r un invo lved immunoglobul ins (139) . About 70% have a
monoclonal prote in—or fragment thereof—detected in the ur ine.
Bone Disease Approximate ly one th ird to two thi rds of pat ients present wi th bone pain (130,131,132,133).
There is an uncoupl ing of the t ight ly regulated balance between osteoclast ic and
osteoblast ic ac t iv i ty seen under normal c i rcumstances. Even before the development o f
bone lesions, enhanced osteoblast ic recru i tment wi th an increased generat ion of new
osteoc lasts is observed in early mul t ip le myeloma (140) . Regard less of the in i t iat ing s ignal ,
whether IL-1β , IL-6, and s IL-6R, TNF-α , MIP-1α , receptor ac t ivator o f NF-κB (RANK) l igand,
or parathyro id hormone–re lated prote in (PTHrP) (141) , the eventual outcome is bone
destruc t ion (142) .
Myeloma bone d isease is a major source of morbid i ty and may present as an area of
persistent pa in or as a vague migratory bone pain, o f ten in the lower back and pelv is . The
type, locat ion, and durat ion of the pa in has no character is t ic features. At t imes, pain and
tenderness may be sudden in onset , espec ial ly when assoc ia ted wi th a patho logic f rac ture,
and is most commonly prec ip i ta ted by movement . Persistent loca l ized pa in a lso may be
associated wi th a patho log ic f racture.
A myelomatous les ion may extend through the cor tex of a ver tebra l body and cause ei ther
nerve root or sp inal cord compress ion in <2% of pat ients (131) . Al ternat ive ly, the myeloma
can d is turb the mechanica l integri ty of a vertebra l body, resu l t ing in
P.2376
compress ion f rac ture wi th re t ropuls ion of ei ther plasmacytoma or bony f ragments in to the
sp inal canal , again causing neuro log ic def ic i ts .

Figure 99.5. Myeloma bone disease. A: Skull. B: Compression fracture. C: Myelomatous marrow involvmement by MRI. D: FDG-PET/CT, spine and rib involvement.
Approximate ly 75% of pat ients have punched-out ly t ic les ions, os teoporos is , or f rac tures on
convent ional rad iography. The ver tebrae, skul l , r ibs, sternum, proximal humeri , and femora
are invo lved most f requent ly (130,132,133) (Fig. 99.5). A smal l subset o f pat ients have de
novo os teosc lerot ic lesions (143) , and osteoscleros is is seen in a few pat ients a fter therapy
and may serve as a marker o f heal ing.
Because myelomatous bone les ions are character is t ica l ly ly t ic , convent ional radiography is
super ior to technet ium-99m bone scanning (144,145) . About twice as many myelomatous
bone lesions are detected by rad iographs as by bone scans; an except ion to this genera l
f inding is at the lumbar sp ine and the r ib cage, where the two methods are equal ly rel iab le

(145). There have been repor ts support ing the use of technet ium-99m sestamib i scans.
These scans are almost as sensi t ive as p la in rad iographs for bone d isease in unt reated
pat ients wi th act ive d isease (146) . They may be ab le to d is t inguish act ive myelomatous
bone lesions f rom inact ive les ions (146) and are qui te sens i t ive for bone marrow
invo lvement (147,148,149) . There is a h igh concordance between sc in t igraphic f ind ings and
c l in ical sta tus in pat ients undergoing chemotherapy or autologous s tem cel l t ransplantat ion
(150,151) . Fluorodeoxyglucose posi t ron emiss ion tomography (FDG-PET) a lso shows
promise in the s tag ing of myeloma, wi th sensi t iv i ty and spec i f ic i ty ra tes of 84 to 92% and 83
to 100%, respect ive ly (152) .
Computed tomography (CT) and magnetic resonance imaging (MRI) are more sens i t ive than
convent ional rad iography. Both reveal spec i f ic les ions in 40% of stage I myeloma pat ients
(153). The presence of lacunae >5 mm wi th trabecular d is rupt ion on CT appears to be
sens i t ive and speci f ic for myeloma. This in format ion may be usefu l in d is t inguishing
between seni le and myelomatous osteoporos is and compression f rac tures (154). Among
asymptomatic mul t ip le myeloma pat ients wi th normal radiographs, 50% have tumor-rela ted
abnormal i t ies on MRI of the lower sp ine (155).
P.2377
In pat ients wi th Dur ie Salmon s tage I myeloma, MRI can dist inguish pat ients at higher and
lower r isks of progress ion (156) . One th i rd of pat ients wi th an apparent ly so l i tary
p lasmacytoma of bone have evidence of other plasma cel l tumors on MRI (157) .
MRI is super ior to rad iographs for the detect ion of les ions in the pe lv is and the sp ine, but
overa l l i t is in fer ior to rad iographs for detect ing bone invo lvement in mul t ip le myeloma (79
vs . 87%, respect ively) (158) . On MRI, ver tebral f rac tures due to sp inal in f i l t ra t ion or
os teoporos is are seen in 48% of pat ients wi th symptomat ic myeloma, and spinal canal
narrowing wi th impingement occurs in 20% (155) . Nanni et al . (159) compared MRI to FDG-
PET/CT in 28 newly d iagnosed myeloma pat ients . In 25% of the pat ients , FDG-PET/CT
detected more lyt ic bone les ions, al l o f which were out o f the f ie ld of v iew of MRI; and in
25% of the pat ients, MRI detected an in f i l t ra t ive pat tern in the sp ine that was not d iscerned
on FDG-PET/CT.
MRI has been said to have predict ive value in pat ients newly d iagnosed wi th myeloma and
in pat ients who have received chemotherapy (160,161) . Three pat terns are descr ibed: focal
lesions, d i f fuse involvement , and an inhomogeneous pat tern of t iny les ions against a
background of normal marrow (var iegated) (161,162) . Not surpr is ingly, there are
corre lat ions among MRI pat terns of marrow involvement , bone marrow p lasmacytosis
(161,163,164) , and the c l in ica l s tage (162,164) . Af ter t reatment , resolu t ion of marrow
abnormal i ty or pers is tent abnormal i ty wi thout enhancement corresponds to a complete
response (160) . In one analysis, the best independent prognost icators o f surviva l were the
MRI f ind ings and C-react ive prote in leve ls . Even though pat ients wi th the d i f fuse pat tern
had more bone marrow plasmacytos is , h igher serum calc ium va lues, higher β2 -microglobul in
(β2 -M) va lues, and lower hemoglobin concentrat ion, these fac tors were not s ign i f icant on
mult ivar ia te analysis (165) . However, given the expense of MRI, i t cannot be recommended
for rout ine c l in ica l use in a l l pat ients .
Hypercalcemia

Hypercalcemia occurs in 18 to 30% of pat ients. About 13% have concentrat ions >11 mg/dl .
Rates of hypercalcemia at presentat ion have been decreasing in the last few decades,
perhaps because of the ear l ier d iagnosis o f pat ients (130,131,132,133) . Hypercalcemic
pat ients may compla in o f fa t igue, const ipat ion, nausea, or confusion. Calc ium can
precipi ta te in the k idneys and aggravate renal insuf f ic iency. Inorganic phosphate is rarely
decreased, except in cases of acqui red Fanconi syndrome (166).
Renal Insufficiency Approximate ly 25% of myeloma pat ients have a serum creat inine va lue >2 mg/dL a t
d iagnos is . Another 25% have mi ld ly elevated creat inine va lues
(130,131,132,133,167,168,169,170) . Pat ients wi th Bence Jones or IgD myeloma have the
h ighest rates of renal insuf f ic iency (168,170) . Free l ight-chain proteinur ia is a r isk fac tor for
renal fa i lure (171) . Contr ibut ing fac tors to the renal insuf f ic iency associa ted wi th myeloma
k idneys inc lude hypercalcemia, dehydrat ion, hyperur icemia, and the use of nephrotoxic
drugs (172). I f the renal insuf f ic iency reverses wi th therapy, as i t does in more than ha l f of
cases (172,173), survival is four fo ld to sevenfold h igher than in those in whom i t does not
reverse (167,174). Factors predic t ing for renal funct ion recovery include a serum creat inine
of <4 mg/dl , serum calc ium value >11.5 mg/d l , prote inuria <1 g per 24 hours , and adequate
rehydrat ion (167) . For those pat ients wi th mult ip le myeloma and severe renal fai lure who
survive the f i rs t 2 months on dia lys is , 40% have an ob ject ive response to chemotherapy and
a median survival of almost 2 years (175) .
The patho logic les ion of myeloma kidney consists o f monoclonal l ight chains in the tubules
in the form of dense, o f ten laminated, tubular casts. These casts conta in a lbumin and
Tamm-Horsfa l l prote in . Light chains are normal ly f i l tered by the g lomeru l i and reabsorbed
and catabol ized in the nephron 's proximal tubules. I t is postu la ted that these systems
become overwhelmed, and casts resu l t . When other causes contr ibut ing to renal
insuf f ic iency are exc luded, there is a good corre lat ion between the extent o f myeloma cast
format ion and the sever i ty o f renal insuf f ic iency (176,177) . Tubular a t rophy and
degenerat ion corre la te wel l wi th renal dysfunct ion (178) . The most common f ind ings on
autopsy include tubular a t rophy and f ibrosis (77%), tubular hya l ine casts (62%), tubular
ep i thel ia l g iant ce l l react ion (48%), and nephrocalc inos is (42%). Evidence of acute and
chronic pyelonephr i t is were observed in 20 and 23% of cases, respect ive ly. Plasma ce l l
in f i l t ra tes and amylo id may be observed in 10 and 5% of cases, respect ive ly (133) . Rarely,
myeloma may be assoc iated wi th the acqui red Fanconi syndrome (166,179) .
An important feature of myeloma kidney is that i t is pr imari ly a tubular ra ther than a
g lomeru lar disease (178). Glomerular funct ion is preserved ini t ia l ly , and there is a
predominance of immunoglobul in l ight -chain protein in the ur ine ins tead of the nonspeci f ic
protein loss observed in g lomeru lar disease. Th is feature helps predic t the renal les ion:
nonspec i f ic protein loss ( i .e . , most ly albumin) is more compatib le wi th pr imary systemic
amyloidos is , l ight -chain depos i t ion disease of the k idney, or prote inuria unrela ted to the
p lasma ce l l dyscrasia (176) ; a f ree l ight -chain predominance is cons is tent wi th myeloma
k idney.
Infection Pat ients wi th mult ip le myeloma are at h igh r isk for bacter ial in fec t ions and for dying of
overwhelming bacteremia. Overa l l , the inc idence of bacter ia l sepsis var ies between 0.8 and

1.4 in fec t ions per pat ient-year (180,181,182) . During the f i rs t 2 months after in i t ia t ing
chemotherapy the in fec t ion incidence is as h igh as 4.68 in fect ions per pat ient -year (182)
but decreases to 0.44 to 0 .49 per pat ient -year in those reaching a pla teau phase (181,182) .
Risk fac tors for in fect ion are serum creat in ine values ≥2 mg/d l (180,182) and decreased
leve ls of po lyclonal serum immunoglobul ins (181,182) .
Since the 1960s, Gram-negative baci l l i have become more common pathogens than
Streptococcus pneumoniae in pat ients wi th myeloma (183) . At d isease onset , infec t ions wi th
encapsulated organisms such as Streptococcus pneumoniae and Haemophi lus in f luenzae
are most common (183) . Af ter d iagnosis , the propor t ion of in fec t ions due to Gram-negative
baci l l i and Staphy lococcus aureus increases markedly, and are respons ible for >90% of
deaths f rom in fec t ion (183) . The mechanism of the immunodefic iency observed in these
pat ients is not unders tood complete ly.
Hemostasis in Myeloma Mul t ip le myeloma can be assoc ia ted wi th hemostat ic abnormal i t ies , more of ten bleeding
than thrombosis . Bleeding as a compl icat ion of myeloma may be present in as many as one
th i rd o f pat ients (184) and is rela ted to thrombocytopenia, uremia, hyperviscosi ty, and
in ter ference wi th the funct ion of coagulat ion fac tors .
Rare ly, myeloma proteins may a lso interact wi th coagulat ion prote ins. The immunoglobul in
may in terfere wi th f ibr in monomer aggregat ion (184,185) or serve as a spec i f ic inh ib i tor o f
thrombin (186), von W il lebrand factor , and fac tor VI I I (184) . Heparin l ike ant icoagulants have
been observed (187). Nonspeci f ic inhibi tors may a lso be present, but un l ike the speci f ic
inhib i tors , they do not corre late wi th c l in ica l ly observed bleeding tendenc ies (184) .
Depression of c lo t t ing fac tors I I , V, VI I , VI I I , X, and f ibr inogen has been descr ibed (184) .
The assoc ia t ion wi th thrombosis is less c lear because of coexis t ing fac tors such as o ld age
and immobi l i ty , which confound the interpretat ion of avai lab le data; however, the r isk o f
thrombosis may be increased in myeloma pat ients (184,188). Ind iv idual cases of aberrance
have been repor ted. Monoc lonal prote ins have been shown to be responsib le for the
development o f lupus ant icoagulants
P.2378
(189,190) , acqui red prote in S def ic iency (191,192) , acqui red act ivated prote in C resis tance
(193), and inhibi t ion of t issue p lasminogen act ivator (194).
Fewer than 7% of myeloma pat ients have a v iscos i ty >4 (130,132) . Symptoms of
hyperviscos i ty inc lude b leeding, par t icular ly f rom the oronasal areas, purpura, decrease in
v isual acui ty, re t inopathy, neuro log ic symptoms, dyspnea, expanded plasma volume, and
congest ive hear t fa i lure. Most pat ients become symptomat ic when the serum viscos i ty is 6
or 7 cent ipo ise (normal is ≤1.8 cent ipo ise) .
“Acute Terminal Phase of Plasma Cell Myeloma” and C ause
of Death Bergsagel and Pruzansk i (195) descr ibed the “acute terminal phase” o f pat ients wi th
myeloma, which they observed in about one th i rd o f thei r preterminal pat ients . They def ined
the syndrome as rap id ly progress ive d isease wi th an unexpla ined fever and pancytopenia
and a hyperce l lu lar marrow. Ext ramedul lary plasmacytomas are a lso not uncommon

preterminal ly (196). As the disease progresses, and at autopsy, cutaneous, v isceral , and
even meningeal invo lvement is poss ib le (196) . Bes ides “progress ive d isease,” the most
f requent causes of death are in fect ion in 24 to 52% and renal fai lure in ~20%
(133,172,195,196). Acute leukemia, myelodysplast ic syndromes, and hemorrhage are the
causes of death in a minor i ty of pat ients (133,195,196) . In one autopsy ser ies , 85% of
pat ients had evidence of e i ther bacter ial or fungal infec t ion, and myelomatous invo lvement
was found in the spleen, l iver , lymph nodes, and k idneys in 45, 28, 27, and 10% of pat ients ,
respect ive ly. Other, less f requent areas of myelomatous invo lvement were the lung, pleura,
adrenal g lands, pancreas, and tes t is (133).
Histopathology The bone marrow microenvi ronment is hospi table to mal ignant plasma ce l ls that c i rcula te
through the b lood. There is a complex in teract ion among the mal ignant c lone, i ts
surrounding s t romal ce l ls , and the remain ing immune ce l ls. The morpholog ic and
immunolog ic phenotypes of myeloma ce l ls can vary, and they of ten resemble normal plasma
ce l ls. P lasma cel ls are at least two to three t imes the s ize of peripheral lymphocytes and
are round to oval , wi th one or more eccentr ical ly p laced nuc le i (F ig . 99.6). The nuc leus,
which conta ins e i ther d i f fuse or c lumped chromatin , is d isplaced f rom the center by an
abundance of rough-surfaced endoplasmic ret icu lum—the s i te of spec ia l ized
immunoglobul in synthesis . In t ranuc lear and cytoplasmic inc lus ions are not uncommon (197).
There is a perinuclear c lear zone that is the s i te o f the Golg i apparatus, the machinery used
for immunoglobul in packaging and g lycosyla t ion for secret ion. Derangements of
immunoglobul in secret ion are responsible for an assor tment of cyto log ic aberrat ions,
includ ing f laming ce l ls, Mot t ce l ls , Russel l bodies, and Gaucher- l ike cel ls. F laming cel ls are
p lasma ce l ls that have intensely eosinophi l ic cytoplasm wi th a magenta or carmine color ing
of the i r marg ins, which is due to plugging of per iphera l secretory channels by precipi tated
immunoglobul in or immunoglobul in f ragments. These ce l ls are most commonly seen in IgA
myeloma. Thesaurocytes are large f laming cel ls wi th a pyknot ic nuc leus that is pushed to
the s ide. Mot t cel ls (grape ce l ls or morula forms) are plasma ce l ls f i l led wi th dense
spher ical immunoglobul in inc lusions; these inclus ions are co lor less, pink, or b lue. Other
inclus ions are Russel l bodies and the i r in tranuclear counterparts ( int ranuc lear dense
bodies) ; these appear cherry red and can be as large as severa l micrometers in d iameter.
Gaucher- l ike ce l ls are not uncommon in myeloma inf i l t ra tes; these ce l ls are macrophages
laden wi th sphingol ip ids re leased by the dying plasma cel ls (198) . None of these in terest ing
inclus ions are spec i f ic for mal ignancy, nor do they have prognost ic va lue.

Figure 99.6. Bone marrow. Myeloma cells on aspirate specimen.
In myeloma, there is o f ten d iscordance between the nucleus and cytop lasm, the former
appear ing immature and the la t ter h igh ly di f ferent ia ted. About 20% of myeloma cases have
p lasmablast ic morphology: a d i f fuse chromatin pat tern, nucleus >10 µm or nuc leo lus greater
than 2 µm, re lat ive ly less abundant cytop lasm, and a concentr ica l ly p laced nuc leus wi th
l i t t le or no hof (199,200). Both di f fuse and nodular in f i l t rat ion pat terns can be observed,
a l though the former is more common. A minor i ty o f pat ients have plasma ce l ls that have a
lymphoplasmacyt ic appearance. Myeloma cel ls are commonly present in cords around bone
marrow microvessels. There is a high correla t ion between the extent of bone marrow
angiogenes is , eva luated as microvessel area, and the pro l i ferat ing frac t ion of marrow
p lasma ce l ls in pat ients wi th mul t ip le myeloma (201,202) . Mi ld marrow f ibros is may be
observed in as many as 27% of cases; extens ive f ibrosis is rare (203,204). Less than 1% of
cases have an extensive id iopathic granulomatous react ion (197) . Growth pat terns may be
nodular, in f i l t rat ive, or both. In cases in which the marrow invo lvement is foca l ra ther than
d i f fuse, bone marrow spec imens f rom al ternate s i tes may vary.
The immunophenotype of myeloma ce l ls is complex. In general , myeloma ce l ls are CD45 - ,
CD38+ and CD138+ (205,206) . However, there is increasing evidence that a subset o f
myeloma ce l ls is CD45+ (206,207) , wi th an increas ing propor t ion of CD45+ myeloma ce l ls in
less advanced disease (208,209) . CD19 and CD20 are ear l ier B-cel l ant igens that are
var iably expressed on myeloma ce l ls; sur face immunoglobul in is seen in up to one th i rd of
pat ients . CD56 is s t rongly posi t ive in about 55 to 78% of myeloma cases (206,210,211) .
CD56-negat ive myeloma ce l ls tend to be present in more aggress ive d isease, such as end-
s tage myeloma or PCL (211,212) . Other sur face ant igens such as CD10 (CALLA), CD28,

CD117 (c-k i t ) , CD13, CD33, and CD20 are present on a minori ty o f pat ients ' myeloma ce l ls
(205,206,207,213,214) . Cost imulatory molecules involved in the act ivat ion of B and T
lymphocytes (CD28 and CD40) are seen in 40 and 70% of pat ients , respect ively (215,216) .
The label ing index of bone marrow p lasma ce l ls can be used to ident i fy plasma ce l l c lonal i ty
and ra te of d iv is ion. Th is assay has some va lue in d i f ferent ia t ing MGUS f rom myeloma and
indolent myeloma f rom act ive myeloma (217,218). Th is determinat ion can be done by 5-
bromo-2-deoxyur id ine immunof luorescence s ta in ing,
P.2379
thymid ine label ing, or f low cytometry. In general , myeloma is a low-growth- f ract ion tumor
wi th on ly a smal l percentage of cel ls in the S phase of the cel l cyc le at any g iven t ime.
No ind iv idual bone marrow f ind ing, however, is pathognomonic for a mal ignant plasma ce l l
process; the bone marrow d iagnos is o f myeloma re l ies on percentage of c lonal bone marrow
p lasma ce l ls, wi th 10% accepted as a cutof f . The c l in ical diagnos is , o f course, is made f rom
a synthes is of bone marrow f ind ings and other c l in ica l features.
Diagnosis The d iagnosis o f mul t ip le myeloma has not been subject to s tat ic norms. In 1973, the
Chronic Leukemia-Myeloma Task Force (219) set for th gu ide l ines for the d iagnos is of
myeloma (Table 99.1) . These cr i ter ia , which by today's s tandards are not s t r ingent enough,
have been replaced by a more modern def ini t ion (Table 99.2) (220) . In the las t 3 decades,
the terms and def ini t ions of MGUS, smolder ing myeloma, indolent myeloma, and
symptomat ic mul t ip le myeloma (130,221,222,223) have evolved and are now to be replaced
by the fo l lowing des ignat ions: MGUS, inact ive (smoldering) myeloma, and act ive (or
symptomat ic ) mul t ip le myeloma (220).
Th is in ternat ional ly accepted classi f icat ion schema is derived f rom more than 3 decades of
exper ience of t reat ing and s tudying mul t ip le myeloma pat ients . Because mult ip le myeloma
includes a spectrum of bio log ic features, physic ians should not feel compel led to s tart
t reatment as a resul t o f a s ingle threshold va lue. The d iagnosis o f act ive myeloma is not a
s t raight forward pathologic one; ra ther , i t is a c l in ica l d iagnosis that requi res thought ful
synthesis o f mul t ip le var iab les . Pat ients wi th Dur ie-Salmon stage I d isease, who also meet
the cr i ter ia for smolder ing or asymptomat ic myeloma, should be managed expectant ly.
Median progress ion- f ree survival in asymptomatic stage I pat ients, observed wi thout any
therapy, is 12 to >48 months (224,225,226,227) ; for s imi lar s tage I I pat ients , progress ion-
f ree survival is 12 months (224) . No survival advantage has been demonstrated by t reat ing
asymptomatic myeloma pat ients (223,225,226,228) .
Treatment for Multiple Myeloma Before star t ing therapy for mul t ip le myeloma, a dis t inc t ion must be made between
smolder ing (asymptomat ic ) myeloma and act ive myeloma (Table 99.2) . Approximately 20%
of pat ients wi th mul t ip le myeloma are recognized by chance wi thout s igni f icant symptoms;
such pat ients can be carefu l ly monitored wi thout inst i tu t ing therapy. Weber e t a l . ident i f ied
three r isk fac tors for progress ion: serum M protein >3 g/dl (30 g/L), IgA isotype, and Bence
Jones prote in excret ion >50 mg per day. Pat ients wi th two or more of these features
requi red t reatment a t a median of 17 months, whereas the absence of any adverse var iab les
was assoc iated wi th pro longed s tab i l i ty (median, 95 months) (p < .01) (229) . Cesana et al .

ident i f ied >10% bone marrow p lasmacytos is , Bence Jones proteinuria , and IgA isotype as
r isk fac tors for evo lu t ion. Other r isk fac tors for progression include ci rcu lat ing p lasma ce l ls
(230) and myeloma cel ls that produce h igh leve ls o f in ter leukin-1β (231) .
Table 99.1 Chronic Leukemia-Myeloma Task Force Definition of Multiple Myeloma (1973)
If M protein present in serum or urine, one or more of the following must be present: Marrow plasmacytosis >5% in absence of underlying reactive process Tissue biopsy demonstrating replacement and distortion of normal tissue by plasma cells More than 500 plasma cells/mm3 in peripheral blood Osteolytic lesion unexplained by other causes If M protein absent in serum and urine, there must be radiologic evidence of osteolytic lesions or palpable tumors and one or more of the following must be present: Marrow plasmacytosis of >20% from 2 sites in absence of a reactive process Tissue biopsy demonstrating replacement and distortion of normal tissue by plasma cells
Data from Proposed guidelines for protocol studies. I. Introduction. II. Plasma cell myeloma. 3. Chronic lymphocytic leukemia. IV. Chronic granulocytic leukemia. Cancer Chemother Rep 1973;4:141–173.
Table 99.2 Criteria for Diagnosis of MGUS, SMM, and MM, International Working Group
Monoclonal Gammopathy of Undetermined Significance Serum monoclonal protein (<30 g/L) Bone marrow <10% plasma cells No evidence of other B-cell proliferative disorders No related organ or tissue impairmenta,b Smoldering Myeloma (asymptomatic) Serum monoclonal protein (≥30 g/L) and/or Bone marrow clonal plasma cells ≥10% No related organ or tissue impairmenta Multiple Myeloma (active or symptomatic) Monoclonal protein present in serum and/or urine Clonal bone marrow plasma cells or plasmacytoma Related organ or tissue impairmenta
MGUS, monoclonal gammopathy of undetermined significance; MM, multiple myeloma; SMM, smoldering multiple myeloma. aThe absence of CRAB (calcium elevation [>1 mg/dl above upper limit of normal], renal dysfunction [creatinine >2 g/dl], anemia [hemoglobin 2 g/dl below lower limit

of normal], bone lesions [lytic lesions or osteoporosis with compression fracture] attributable to the plasma cell disorder). bThe existence of immunoglobulin light-chain amyloidosis or another paraneoplastic disorder attributable to the monoclonal gammopathy, such as a peripheral neuropathy, would be termed “monoclonal gammopathy associated with—.” Source:Criteria for the classification of monoclonal gammopathies, multiple myeloma and related disorders: a report of the International Myeloma Working Group. Br J Haematol 2003; 121:749–757
Once the dec is ion has been made to treat for symptomat ic disease, a long- term plan for
managing the d isease should be formulated before ins t i tut ing therapy. F igure 99.7A,B
out l ines a poss ib le t reatment algori thm. Because h igh-dose therapy wi th hematopoiet ic s tem
ce l l support has been accepted as an important treatment modal i ty for pat ients younger
than age 65, cumulat ive doses of a lkyla tor-based therapy should be avoided prior to the
co l lec t ion of hematopoiet ic s tem cel ls in pat ients considered candidates for high-dose
therapy.
Systemic Therapy
General Comments
Histor ica l ly, bi funct ional a lkyla t ing agents , such as melphalan and cyc lophosphamide, have
been the foundat ion of therapy for mul t ip le myeloma. Myeloma cel ls tend to pro l i ferate
s lowly, and alkyla tors , whose ef fec t iveness does not re ly heavi ly on cel l d iv is ion and DNA
rep l icat ion, are usefu l therapeut ic agents . Prior to 1999, the bi funct ional a lkyla tors ,
n i t rosoureas, doxorubic in , and g lucocort ico ids were the pr imary agents shown to have
s ing le-agent ac t iv i ty against mul t ip le myeloma in vivo (232) . These drugs, a long wi th
v incr is t ine, ei ther s ing ly or in combinat ion, had been the mainstay of chemotherapy for
myeloma f rom the early 1960s to the present (Fig . 99.1). Unt i l recent ly, the higher response
rates seen wi th reg imens that combine mul t ip le ac t ive agents as part o f in i t ia l therapy had
not resu l ted in improved overa l l surviva l ra tes (233) .
In terferon-α has been incorporated into induct ion and maintenance protocols wi th minimal
benef i t (40,234,235,236). Both autologous and a l logeneic s tem cel l t ransplantat ion have
become important therapeut ic opt ions s ince McElwain and Powles ' descrip t ion in 1983 (237)
o f the benef i t o f dose intensi f icat ion of melphalan
P.2380
in pat ients wi th mul t ip le myeloma. W ith the recogni t ion of thal idomide 's ac t iv i ty against
myeloma in 1999 (43) and the subsequent development o f bor tezomib (44) and lenal idomide
(45) , there is hope that the next 4 decades of myeloma t reatment wi l l be even more
promising than the las t.

Figure 99.7. Mayo stratification for myeloma and risk-adapted therapy. A: Risk stratification. B: Possible treatment algorithm for patients with newly diagnosed myeloma for patients not being treated on a clinical trial. Dex, dexamethasone; HR, high risk (see text);

lenalid, lenalidomide; MP, melphalan, prednisone; PR, partial response.
Before discussing induct ion, t ransplantat ion, maintenance, and sa lvage therapies, two
genera l concepts wi l l be reviewed: in terpretat ion of study response data, and the ef f icacy of
s ing le chemotherapeut ic agents commonly used to t reat myeloma. Figure 99.7 is an
a lgor i thm for t reat ing pat ients wi th newly d iagnosed myeloma. Table 99.3 serves as a
re ference for commonly c i ted reg imens.
Interpreting Study Response and Survival Data Four poin ts are emphas ized regarding the in terpretat ion and comparisons of the myeloma
t reatment l i terature. F i rst , def in i t ions of response vary (Table 99.4) . Second, def in i t ions of
eva luable pat ients may be d i f ferent. Th i rd, concurrent cort icostero id therapy, e i ther as par t
o f the reg imen or for o ther ind icat ions, may confound in terpretat ion of e f f icacy. Final ly,
pat ient populat ion r isk and prognos is may d i f fer substant ia l ly . Lead-t ime b ias and t reatment
o f MGUS or smolder ing myeloma can s ign i f icant ly d is tor t survival f igures, as can ef fec t ive
sa lvage regimens.
The measurement o f myeloma d isease burden, and therefore i ts response to therapy, is
complex, and invest igators have used di f ferent methods to def ine response (Table 99.4) .
The four most common response cr i ter ia are those of the Chronic Leukemia-Myeloma Task
Force (CLMTF) (219) , the Southwest Oncology Group (SW OG) (238,239), the Eastern
Cooperat ive Oncology Group (ECOG) (240) , and the Autologous Blood and Marrow
Transplant Regist ry and In ternat ional Bone Marrow Transplant Regis t ry ( IBMTR/ABMTR)
(241). These response cr i ter ia are re levant f rom a h is tor ica l prospect ive because they
should al l be supplanted by the new In ternat ional Response Consensus Cr i ter ia (242) .
Al though al l par t ia l ly take into account hemoglobin
P.2381
ca lc ium, bone changes, and bone marrow p lasmacytosis, the main dist inc t ion among them is
the ir cons iderat ion of the serum and ur ine M components. W ith the except ion of the old
SW OG cr i ter ia (238,239), a par t ia l response (PR) has been considered to be a 50%
reduct ion in serum M component and a >50 to 90% reduct ion in ur ine M component . In the
ear l ies t l i terature, response inc luded such factors as increas ing hemoglob in concentrat ion
or per formance sta tus, or decreasing b lood urea n i t rogen leve ls . Nei ther the CLMTF nor the
SW OG cr i ter ia or iginal ly had a complete response category, because i t was unusual for the
M prote in to d isappear complete ly. I t was not unt i l the advent o f h igh-dose melphalan that
invest igators such as Selby et a l . (243) and Gore et al . began (244) to def ine a complete
remiss ion category. Their def ini t ion, unl ike more modern def ini t ions, on ly included
d isappearance of M prote in as determined by e lec t rophoresis, which is less sensi t ive than
immunoelect rophoresis or immunofixat ion. Subsequent def in i t ions have requi red
immunof ixat ion negat iv i ty to qual i fy as complete remiss ion (241). Unt i l about 1990, a SW OG
object ive response was def ined as a 75% reduct ion in the tumor mass index (not serum M
protein), and improvement was def ined as a 50 to 74% reduct ion in the tumor mass index
(239). A new i terat ion of the SW OG response cr i ter ia uses the M component ( ra ther than
the tumor mass index) as the pr imary measurement o f the p lasma cel l burden. The f i rst
i terat ion of an in ternat ional consensus def in i t ion of myeloma response were the

IBMTR/ABMTR response cr i ter ia (241). Af ter near ly 8 years of use, severa l def ic ienc ies
were noted, and the Internat ional Myeloma W orking Group has recent ly issued a new
consensus def ini t ion cal led the In ternat ional Response Cri ter ia ( IRC), which inc ludes the
In tergroupe Français du Myélome ( IFM) very good part ia l response category (245) , the
ab i l i ty to measure response us ing the serum immunoglobul in f ree l ight chain, and a new
category of “s t r ingent
P.2382
complete response” that requi res documentat ion of the absence of c lonal i ty (242).
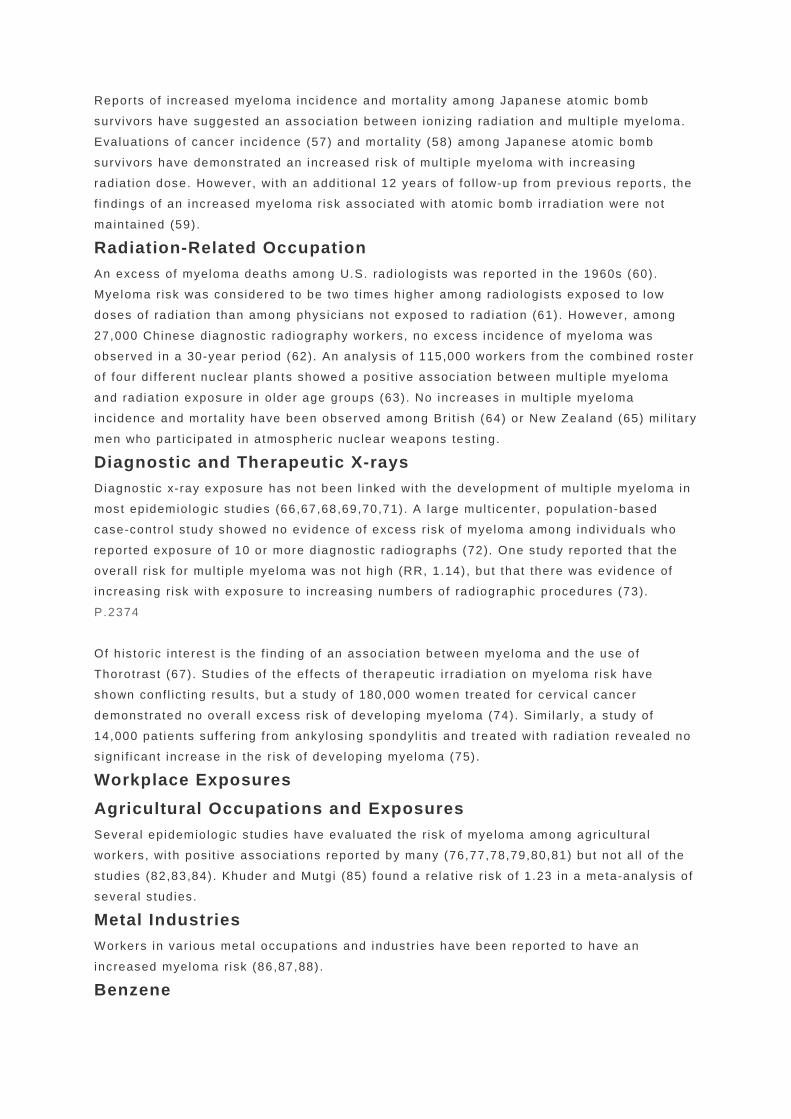
Table 99.3 Commonly Cited Regimens and Their Dosage Schedules
Regimen VCR Mel CTX BCNU ADR Gluco IMiD Bortez
MP — 9 mg/m2/d, d 1–4 q 4 wk or 0.15 mg/kg/d, d 1–7b
— — — P 100 mg/d, d 1–4 q 4 wk or P 60 mg/d, d 1–7b
— —
CPa — — 0.25 g/m2 per d, d 1–4 or 1 g/m2 IV
— — P 100 mg/d, d 1–4 or P 50 mg, qod
— —
ABCMc (251)
— 6 mg/m2/d, d 1–4
100 mg/m2/d, d 1–4
30 mg/m2 IV, d 1
30 mg/m2 IV, d 1
— — —
VBMCPd
0.03 mg/
0.25 mg/
10 mg/
0.5 mg/k
— P 1 mg/k
— —
(274) kg IV, d 1
kg, d 1–7
kg IV, d 1
g IV, d 1
g, d 1–7
VADd (391)
0.2 mg/m2/d CI, d 1–4
— — — 9 mg/m2/d CI, d1–4
D 40 mg/d, d 1–4, 9–12, 17–20
— —
C-VAMPa (395)
0.4 mg/d CI, d 1–4
— 500 mg IV, d 1, 8, 15
— 9 mg/m2/d CI, d 1–4
Methylpred 1 g/m2/d, d 1— 4
— —
Regimen
VCR
Mel CTX
Cisplatin (CDDP)
ADR
Gluco
IMiD
Bortez
DT-PACEd (672)
— — 400 mg/m2/ d× 4 d, CI
CI: CDDP 10 mg/m2/d × 4 d & Etop40 m/m2/d × 4 d both by CI
10 mg/m2/d× 4 d, CI
40 mg/d × 4 d
— —
Thal-dex
— — — — — 40 mg, d
Thal
—

(441) 1–4, 9–12, 17–20 or d 1, 8, 15, 22
50–100 mg/d
Len-dex (439)
— — — — — As above (441)
Len 25 mg/d, d 1–21, q 28 d
—
MPT (263,451)
— 0.25 mg/kg, d 1–4 q 6 wk
— — — P 2 mg/kg, d 1–4, q 6 wk
Thal 200 mg/d
—
Doxil/Borteza (677)
— — — — Pegylated dox 30 mg/m2, d 4
— — 1.3 mg/m2
, d 1, 4, 8, 11
VMPe (459)
— 9 mg/m2, d 1–4 q
— — — P 60 mg/m2, d 1–4 q 6 wk
— 1.3 mg/m2
, d 1,

6 wk
4, 8, 11, 22, 25, 29, & 32
IMiD, immune modulatory drug; ABCM, VBAP/VMCP without vincristine or prednisone; ADR, doxorubicin (Adriamycin); BCNU, carmustine; CDDP, cisplatin; CI, continuous infusion; CP, cyclophosphamide and prednisone; CTX, cyclophosphamide; C-VAMP, cyclophosphamide, vincristine, doxorubicin, and methylprednisolone; d, day; DT-PACE, dex, thalidomide, cisplatin, doxorubicin, cyclophosphamide, etoposide; gluco, corticosteroid; IV, intravenous; Mel, melphalan; MP, melphalan and prednisone; po, by mouth; MPT, MP and thalidomide; P, prednisone; q, every; qod, every other day; VAD, vincristine, doxorubicin, and dexamethasone; VAMP, vincristine, doxorubicin, and methylprednisolone; VBAP, vincristine, BCNU, doxorubicin, and prednisone; M-2, VBMCP; VCR, vincristine; VMCP, vincristine, melphalan, cyclophosphamide, and prednisone; Thal, thalidomide; Rev, lenalidomide; VMP, MP and bortezomib; wk, week. aRepeated at 3-wk intervals. bRepeated at 6-wk intervals. cAB and CM portions of regimen are given alternately every 3 wk. dRepeated every 5 wk. eRepeated every 6 wk for 4 cycles, and then repeated every 5 wk, with bortezomib schedule changing to weekly administration for 4 wk followed by 1 wk rest.
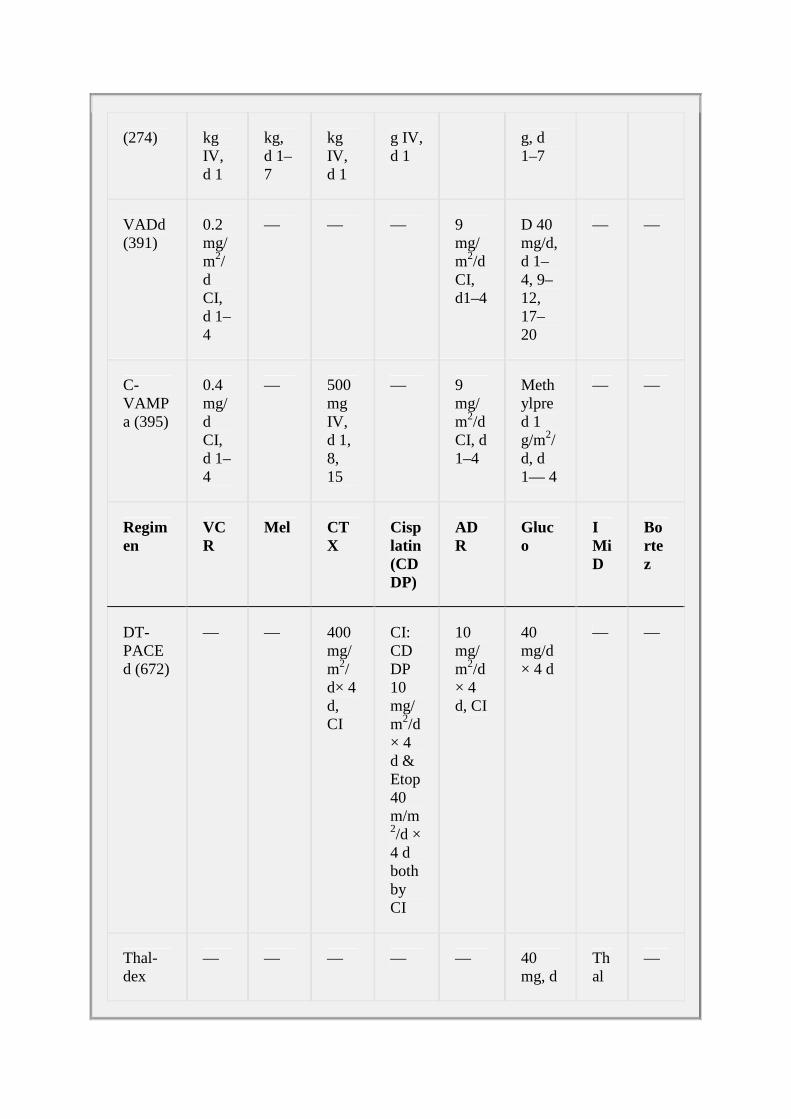
Table 99.4 Response Criteria
M protein Response Study % BMPC Serum Urine
Duration (wk)
Stringent CR (sCR)
IRC (242) <5a IF-b IF- 0
IRCc ≤5 IF- IF- 6
IBMTRc (241) <5 IF- IF- 6
Complete response
SWOG (239) <1a IF- IF- 8
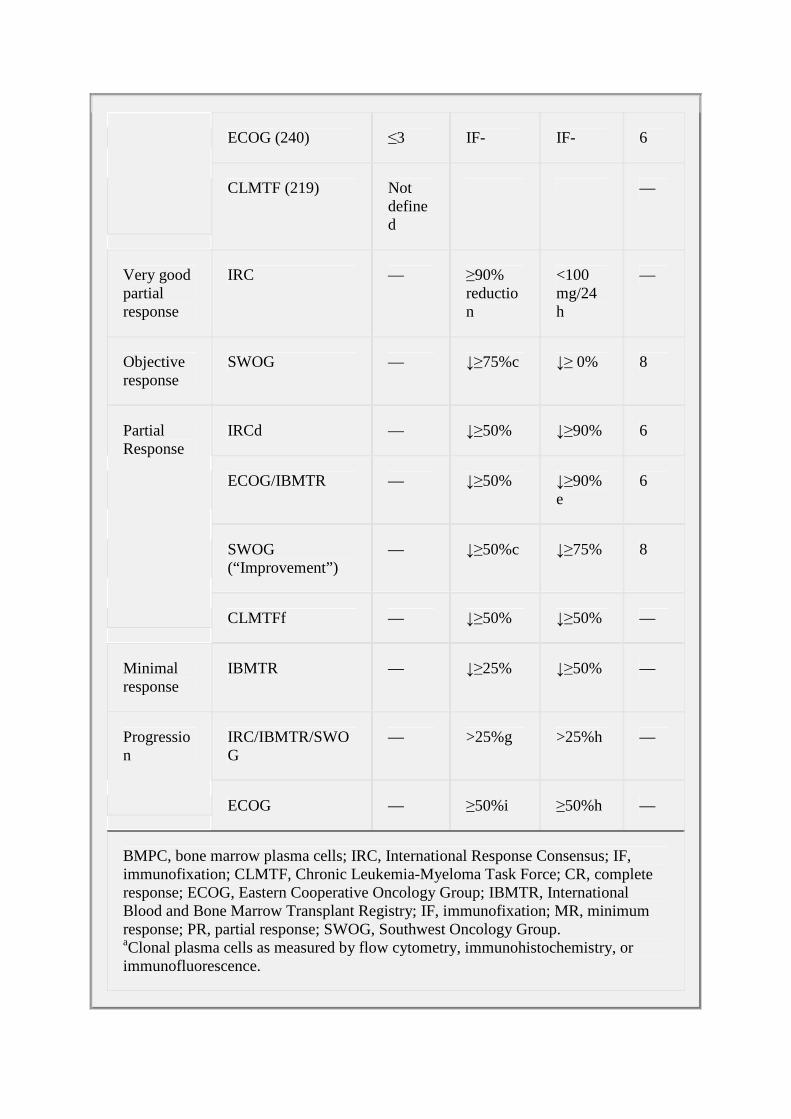
ECOG (240) ≤3 IF- IF- 6
CLMTF (219) Not defined
—
Very good partial response
IRC — ≥90% reduction
<100 mg/24 h
—
Objective response
SWOG — ↓≥75%c ↓≥ 0% 8
IRCd — ↓≥50% ↓≥90% 6
ECOG/IBMTR — ↓≥50% ↓≥90%e
6
SWOG (“Improvement”)
— ↓≥50%c ↓≥75% 8
Partial Response
CLMTFf — ↓≥50% ↓≥50% —
Minimal response
IBMTR — ↓≥25% ↓≥50% —
IRC/IBMTR/SWOG
— >25%g >25%h — Progression
ECOG — ≥50%i ≥50%h —
BMPC, bone marrow plasma cells; IRC, International Response Consensus; IF, immunofixation; CLMTF, Chronic Leukemia-Myeloma Task Force; CR, complete response; ECOG, Eastern Cooperative Oncology Group; IBMTR, International Blood and Bone Marrow Transplant Registry; IF, immunofixation; MR, minimum response; PR, partial response; SWOG, Southwest Oncology Group. aClonal plasma cells as measured by flow cytometry, immunohistochemistry, or immunofluorescence.

bAlso requires normalization of serum immunoglobulin free light chain ratio. cChange in synthetic index and not monoclonal protein concentration. dAllows for immunoglobulin free light-chain responses in patients whose serum and urine are not measurable. eOr <200 mg/24 hours. fResponse also takes into account reduction in size of plasmacytomas, >2 g/dl Hb rise, weight gain, correction of calcium, renal function, albumin. gAbsolute increase must be at least 5 g/L. hAbsolute increase must be >200 mg/24 hours. iFor ECOG, absolute increase must be at least 20 g/L.
The roving denominator a lso creates chal lenges in interpret ing therapeut ic studies . Of ten,
an in tent - to- t reat analys is is not used to describe response rates or surviva l , which
ar t i f ic ia l ly in f la tes these endpoints. Def ini t ions of eva luable pat ients may of ten include on ly
those pat ients who received an “adequate” t r ia l (3 or 6 months) o f therapy, thereby
exc lud ing pat ients wi th ear ly deaths or progress ion. In addi t ion, in a steroid-responsive
tumor such as myeloma, co incident use of prednisone or dexamethasone (246,247) as an
ant iemet ic or as therapy for hyperca lcemia may ser iously confound the resu l ts . F inal ly, the
s t r ik ing heterogenei ty of prognoses in myeloma pat ients cannot be exc luded as a major
confounding fac tor in interpret ing both Phase I I and Phase I I I t r ia ls . Severa l prognost ic
indicators have been ident i f ied, including stage, β2-M, label ing index, renal funct ion, serum
a lbumin, and chromosomal abnormal i t ies . Unfor tunately, the i r pred ic t ive va lue is l imi ted and
only skims the surface of myeloma bio logy and prognos is .
Efficacy of Single Chemotherapeutic Agents
Melphalan Bergsagel e t al . (37) demonstrated the benef i t of melphalan in 14 of 24 pat ients wi th
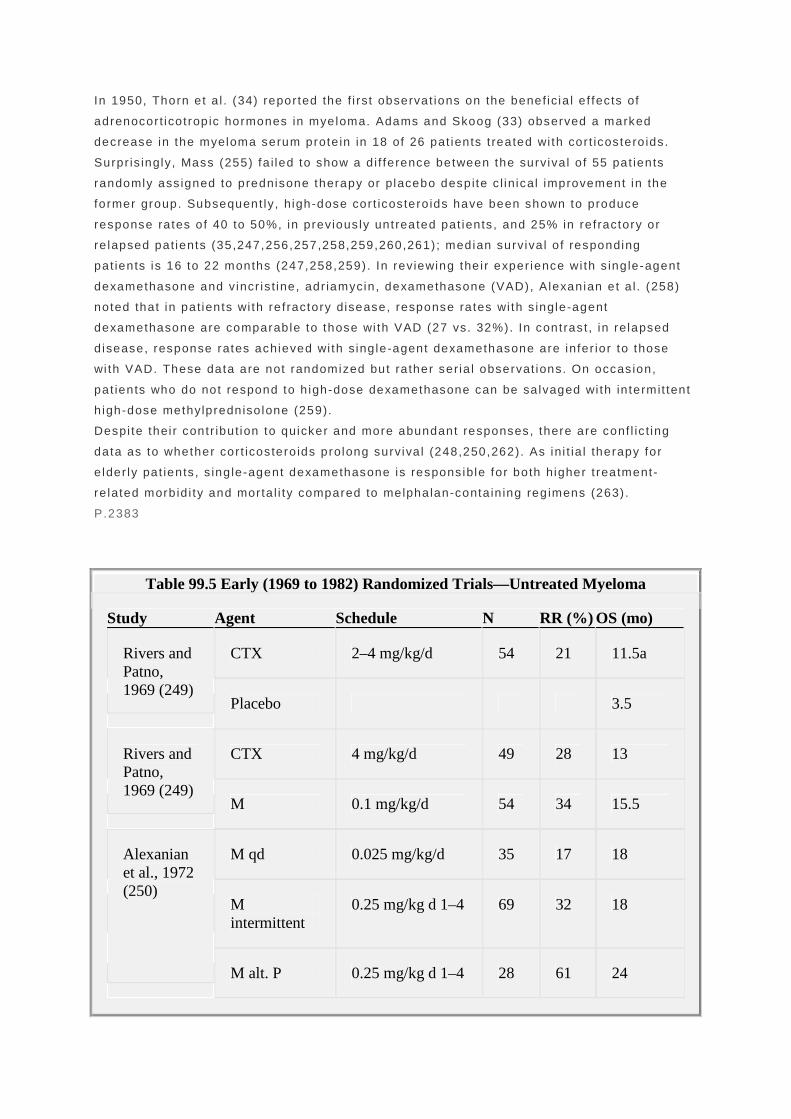
mult ip le myeloma. Others (Table 99.5) have substant ia ted that melphalan as a s ing le agent
resul ts in response rates of 20 to 34% and median overal l surviva l o f 15 to 27 months
(38,248,249,250,251).
Cyclophosphamide Korst e t a l . were the f i rst to report on the act iv i ty o f ora l cyclophosphamide. Twenty- four
percent o f mul t ip le myeloma pat ients achieved a part ia l response (50% M-prote in reduct ion),
and 48% had object ive improvement , that is , an improvement in the peripheral blood va lues,
bone marrow f ind ings, or serum b lood urea ni t rogen. Median surviva l was 24.5 months in a l l
207 pat ients and 32 months in the group that rece ived at least 2 months of
cyc lophosphamide therapy. The single-agent ac t iv i ty o f cyc lophosphamide (Table 99.5) has
been demonstrated in a p lacebo-contro l led t r ia l (249) , in mul t ip le s tud ies of previous ly
unt reated pat ients (252,253) , and in those who re lapsed or had re f rac tory d isease (254).
Glucocorticoids
In 1950, Thorn et a l . (34) repor ted the f i rst observat ions on the benef ic ia l e f fec ts of
adrenocor t icot rop ic hormones in myeloma. Adams and Skoog (33) observed a marked
decrease in the myeloma serum prote in in 18 of 26 pat ients t reated wi th cor t icostero ids .
Surpr is ingly, Mass (255) fa i led to show a d i f ference between the surviva l o f 55 pat ients
randomly ass igned to prednisone therapy or placebo despite c l in ical improvement in the
former group. Subsequent ly, high-dose cor t icostero ids have been shown to produce
response rates of 40 to 50%, in previous ly unt reated pat ients , and 25% in re f ractory or
re lapsed pat ients (35,247,256,257,258,259,260,261) ; median surviva l o f responding
pat ients is 16 to 22 months (247,258,259) . In reviewing the i r exper ience wi th s ing le-agent
dexamethasone and vincr is t ine, adr iamycin, dexamethasone (VAD), Alexanian et a l . (258)
noted that in pat ients wi th re f ractory disease, response rates wi th s ingle-agent
dexamethasone are comparable to those wi th VAD (27 vs. 32%). In contrast , in relapsed
d isease, response rates achieved wi th s ing le-agent dexamethasone are infer ior to those
wi th VAD. These data are not randomized but ra ther seria l observat ions. On occas ion,
pat ients who do not respond to h igh-dose dexamethasone can be sa lvaged wi th in termit tent
h igh-dose methylpredniso lone (259).
Despi te thei r contr ibut ion to quicker and more abundant responses, there are conf l ic t ing
data as to whether cor t icostero ids prolong surviva l (248,250,262) . As ini t ia l therapy for
e lder ly pat ients , s ing le-agent dexamethasone is respons ible for both higher t reatment-
re lated morb id i ty and morta l i ty compared to melphalan-conta in ing reg imens (263) .
P.2383
Table 99.5 Early (1969 to 1982) Randomized Trials—Untreated Myeloma
Study Agent Schedule N RR (%) OS (mo)
CTX 2–4 mg/kg/d 54 21 11.5a Rivers and Patno, 1969 (249)
Placebo 3.5
CTX 4 mg/kg/d 49 28 13 Rivers and Patno, 1969 (249)
M 0.1 mg/kg/d 54 34 15.5
M qd 0.025 mg/kg/d 35 17 18
M intermittent
0.25 mg/kg d 1–4 69 32 18
Alexanian et al., 1972 (250)
M alt. P 0.25 mg/kg d 1–4 28 61 24

& 1 mg/kg MWF
M concurr P 0.25 mg/kg d 1–4 & 2 mg/kg d 1–4
51 65 17
CTX 150 mg/d 114 NG 28b MRC, 1971 (252)
M 4 mg/d 105 NG 24b
MP M: 0.25 mg/kg & P: 2 mg/kg d 1–4
83 52a 21 Alexanian et al., 1972 (238)
MP & procarbazine
M: 0.2 mg/kg & P: 2 mg/kg d 1–4 & Pro: 3 mg/kg d 2–10
79 41 23
M qd 0.15 mg/kg ×7, maintenance 0.05 kg/d
53 20 27 (30,21)c
M qd & P M: as above & P: 1.25 mg/kg/d with taper 8 wk
70 39 NG (53,9)
Costa et al., 1973 (248)
M qd, P, & testosterone
M & P as above & testosterone: 10 g/kg/wk
56 43 NG (36,4)
MP M: 10 mg /d d 1–7; P: 40 mg/d d 1–7 q 3 wk
174 NG 32d,e
CTX IV 600 mg/m2 q 3 wk
179 24
MRC, 1980 (253)
MP See above 71 NG 6b,e

CMLP C: 250 mg/m2 po d 1–3; M: 5 mg/m2 d 1–3; L: 50 mg/m2 d 4; & P: 40 mg/m2 d 1–3 q 4 wk
61 NG 6
MP M: 0.15 mg/kg d 1–7; P: 0.8 mg/kg with taper
100 44f 27
Carmustine-P Carmustine: 150 mg/m2 IV; P: 0.8 mg/kg with taper
124 34 21
Cornwell et al., 1982 (276)
Lomustine-P Lomustine: 100 mg/m2 qd; P: 0.8 mg/kg with taper
137 30 21
Alt, alternating; C, cyclophosphamide; concurr., concurrently; CTX, cyclophosphamide; IV, intravenous; L, lomustine; M, melphalan; MRC, Medical Research Council Working Party on Leukaemia in Adults; NG, not given; OS, overall survival; P, prednisone; po, by mouth; qd, daily. aOverall survival is significant at p=.03. No corticosteroids allowed in trial. bSurvival estimated from survival curves. cPatients stratified for good and poor risk; median survival given as all patients (good risk, poor risk). Authors note that much quicker response observed with prednisone but worse survival with prednisone in poor-risk patients. dPatients were required to have BUN≤10 mM. Difference not significant (p=.16). eAll patients had BUN >10 mM. fResponse rate between melphalan and lomustine arms significant. Median survival is not different.
The mechanism of ac t ion of th is drug c lass is complex. Cort icosteroids suppress the
product ion of cytok ines that are important in myeloma growth, such as IL-6 and IL-1β , and
reduce nuc lear factor κB act iv i ty, resu l t ing in enhanced apoptos is (264,265,266,267) .
Vincristine Al though vincr is t ine has never been evaluated as a s ing le agent in newly d iagnosed
myeloma, i t has l i t t le ac t iv i ty as a s ing le agent in re f rac tory d isease. Twenty-one pat ients
were t reated wi th a 0.5-mg bolus of v incr ist ine fo l lowed by 0.25 to 0.5 mg/m 2 per day as a
cont inuous in fusion over 5 days on a 3-week schedule. Two pat ients had t rans ient
responses (1.2 and 2.2 months) (268) . F inal ly, the act iv i ty c redi ted to v incr is t ine as a
maintenance therapy is a lso ambiguous. Al though superior surviva l (35 vs . 27 months, p

= .003) was repor ted in pat ients treated wi th s ing le-agent melphalan and mainta ined on
b imonth ly v incr is t ine (1 mg/m2) and prednisone (0.6 mg/kg for 7 days) , the benef i t cou ld
easi ly be at t r ibuted to prednisone a lone (269) .
Alexanian et a l . (270,271) suggested that reg imens that inc luded vincr is t ine resul ted in
bet ter pat ient outcome than protocols that d id not inc lude this agent . The theory behind i ts
posi ted ut i l i ty was that af ter an in i t ia l k i l l o f myeloma ce l ls by a lkyla t ing agents , the
subsequent increase in the mi to t ic index made myeloma ce l ls more sensi t ive to v incr is t ine
(272). Reports by Lee et a l . , Salmon, and Case have been c i ted as conf i rmatory evidence
for ac t iv i ty o f v incr is t ine in myeloma (273,274,275) . However, several randomized control led
t r ia ls have not supported th is premise (276,277,278,279) (Table 99.6) . The most compel l ing
of these is the MRC IV Tr ia l in Myelomatosis , which randomized 530 newly d iagnosed
myeloma pat ients to month ly melphalan and prednisone, wi th or wi thout monthly v incr is t ine.
Median surviva l in both arms was 26 months (278) . Even though vincr is t ine has not been
shown to have signi f icant s ingle-agent in v ivo act iv i ty or to improve overa l l surviva l
(268,278,279,280), i t is inc luded in mul t ip le therapeut ic regimens.
Anthracyclines Doxorubic in is the most commonly used anthracyc l ine in the t reatment o f myeloma, but i t
has not been s tud ied as a s ingle agent in newly diagnosed myeloma pat ients . I ts ac t iv i ty as
a s ingle agent in re lapsed or re f rac tory d isease is modest, wi th response rates of about
10% (41,281) .
A Phase I I t r ia l o f mi toxantrone as a s ing le agent (12 mg/m 2 every 3 weeks) y ielded a
par t ia l response rate of 3% (1 of 35). An addi t ional four pat ients showed c l in ical
improvement las t ing 4 to 7 months (282) . Idarubic in is another anthracyc l ine that has been
P.2384
s tud ied in mult ip le myeloma. Response rates of 0 to 27% have been observed in re lapsed
and ref rac tory pat ients wi th s ing le-agent ora l regimens (30 mg/week in three div ided doses
g iven 3 of 5 weeks or 40 mg/m 2 every 3 weeks) (283,284) .
Etoposide In relapsed and ref rac tory d isease, s ingle-agent e toposide (200 to 250 mg/m 2 over 5 days)
has min imal ac t iv i ty; in 85 pat ients the response rate was <5% (285) . Bar log ie e t a l . (286)
t reated 14 pat ients wi th 200 mg/m 2 by cont inuous in fus ion, and 2 responded. In addi t ion,
there are 2 anecdotal repor ts of ac t iv i ty o f low-dose (25 to 50 mg/day) ora l etoposide
(287,288) .
Nitrosoureas The n i t rosoureas have sing le-agent ac t iv i ty in myeloma. In a randomized tr ia l o f 361
previously unt reated pat ients (Table 99.5), ob jec t ive response f requenc ies wi th carmust ine
(BCNU) (40%) and lomust ine (CCNU) (42%) were lower than that of melphalan (59%),
a l though the survival for a l l groups was not s ign i f icant ly di f ferent (276) .
Table 99.6 MP versus Combination Chemotherapy as Induction: Selected Randomized Trials

Study Regimen N RR (%)a
Overall Survival (mo)
P (RR) P (OS)
MP 125 40† 28 NS NS SWOG 727/1972 (238)
MP-Pcb 116 47 31
MP 187 29 36 NS NS SECSG 343/1984 (359)
BCP 186 37 36
MP 126 56 NG 0.047 NS CALGB 7161/1979 (353)
MCBP 124 68
MP 125 40b
28 NS NS NCI-C-MY1/1979 (583)
MCBP 239 39 31
MP 92 40 19 NS NS ECOG 4472/1982 (360)
BCP 96 50 25
MP 67 40 38 NS NS GATLA3-M-73/1980 & 198 (361,1087) CP-
MeCCNU 83 40 30
MP 145 33 42 NS NS GATLA3-M-77/1984 & 1988 (361,937) MPCV-
MeCCNU 115 44 44
Pavia MM-75/ MP 39 41 54 NS 0.039
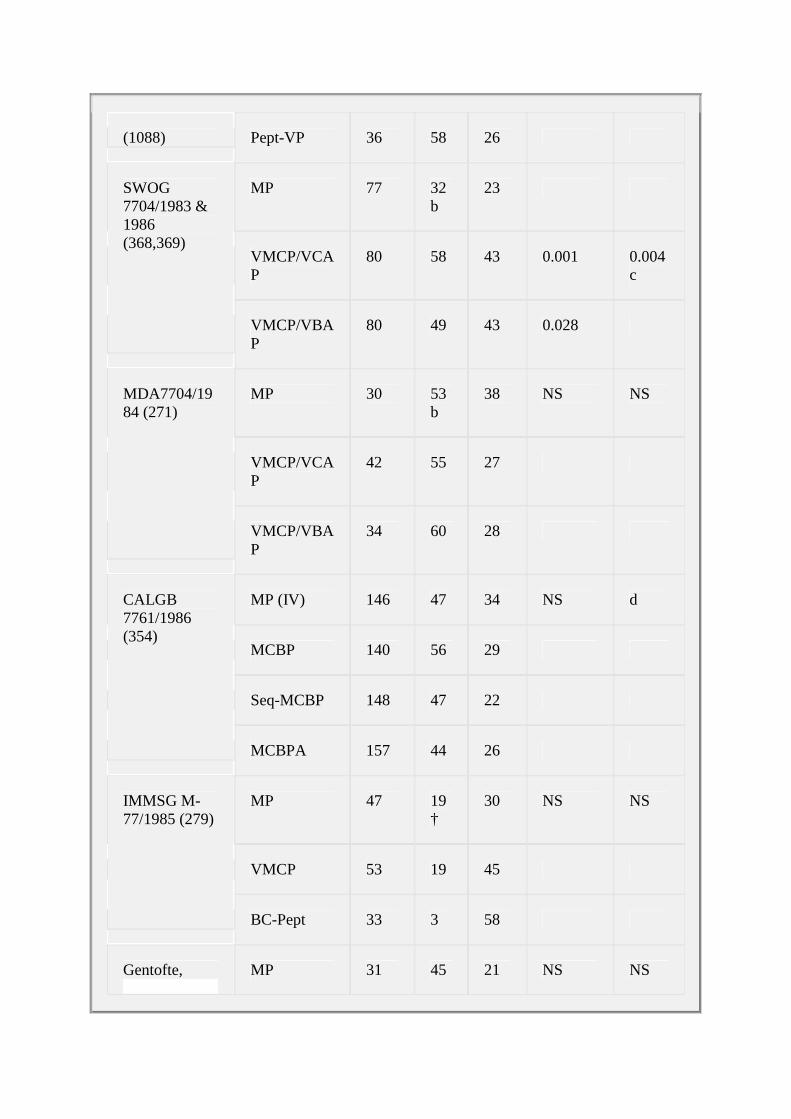
(1088) Pept-VP 36 58 26
MP 77 32b
23
VMCP/VCAP
80 58 43 0.001 0.004c
SWOG 7704/1983 & 1986 (368,369)
VMCP/VBAP
80 49 43 0.028
MP 30 53b
38 NS NS
VMCP/VCAP
42 55 27
MDA7704/1984 (271)
VMCP/VBAP
34 60 28
MP (IV) 146 47 34 NS d
MCBP 140 56 29
Seq-MCBP 148 47 22
CALGB 7761/1986 (354)
MCBPA 157 44 26
MP 47 19†
30 NS NS
VMCP 53 19 45
IMMSG M-77/1985 (279)
BC-Pept 33 3 58
Gentofte, MP 31 45 21 NS NS

VMP 32 73 30 Denmark/1985 (277)
VBMCP 33 58 21
MP 230 51 27 <0.0001 NS ECOG 2479/1997 (373)
VBMCP 235 72 29
MP 261 NG
26 NS NS MRC MYEL-4/1985 (278)
VMP 269 26
MP 66 54 41 < 0.02 NS Finnish MM80/1987 (363)
MOCCA 64 75 45
MP 48 48 29 NS NS Norwegian Trial 1986 & 1988 (364,385) VBMCP 44 54 33
MP 44 61 28 NS NS MGCS stage III/1989 (365)
VMCP/VBAP
42 52 24
MP 170 33b
60% 4 y OS
NS <0.02 MP
GMTG MM01/1988 & 1991 (371,384)
VMCP 150 33
MGCS stage MP 29 69 46 NS NS

II/1990 (370) VMCP 25 56 33
MP 55 58 26 NS NS MGCS stage III/1990 (370)
VMCP/VBAP
53 57 24
MP 146 64 37 0.02 NS IMMSG M-83/1991 (366)
VMCP/VBAP
158 77 32
MP 247 32 27 0.004 NS PEETHEMA 85/1993 (372)
VMCP/VBAP
241 45 32
MP 87 24 All 24
NS NS Pavia 1986/1994 (225)
Pept-VP 83 24
MP 74 64 31 NS 0.02 NMSG/1993 (367)
NOP 77 60 14
MP (IV)e 99 43 ~37 0.01 NS GMTG MM02/1995 (374)
VBAMDe 105 64
Meta-analysis Group (233)
MP vs. CCT 6,633
53 29 <0.00001
NS
A, doxorubicin; B, BCNU or carmustine; C, cyclophosphamide; CCT, combination chemotherapy; D, dexamethasone; IV, intravenous; M, melphalan; MeCCNU, methyl-CCNU; MOCCA, the additional C is for CCNU (lomustine); NG, not given;

NOP, mitoxantrone, vincristine, and prednisone; NS, not significant; P, prednisone; Pcb, procarbazine; Pept, peptichemo; V, vincristine. aExcept where stated, response is according to Myeloma Task Force criteria or modification. bSWOG response criteria. cSignificantly superior survival in combination chemotherapy arms compared to MP in the 174 stage III patients but not in the 74 stage I or II patients. dThe sequential arm was significantly worse than either the MP (p=.01) or the MCBP (p=.02) and marginally worse than MCBPA (p=.09). ePart of an interferon trial; stage III patients only. Data from Anonymous. Combination chemotherapy versus melphalan plus prednisone as treatment for multiple myeloma: an overview of 6,633 patients from 27 randomized trials. Myeloma Trialists' Collaborative Group. J Clin Oncol 1998;16:3832–3842.
Interferon Despi te the encouraging repor ts that da i ly human leukocyte in ter feron (3 to 9 MU/day) could
induce responses in as many of 60% of myeloma pat ients (40,234) subsequent s tud ies wi th
recombinant in ter feron-α y ie lded ra tes of 10 to 20% (236,289,290,291,292) . Toxic i ty was
not inconsequent ia l (292) . In v i t ro act iv i ty had good predic t ive va lue for in v ivo c l in ica l
response in 26 pat ients s tud ied (290). However, in ter feron has a s t imulatory e f fec t in about
one th i rd of myeloma samples tes ted in v i t ro (290) .
Thalidomide Thal idomide is the f i rst in the c lass of drugs cal led immune modulatory drugs ( IMiDs) .
Recognit ion of the ro le of increased
P.2385
angiogenes is in the pathogenesis and progress ion of myeloma (201), and evidence of
tha l idomide 's ant iangiogenic proper t ies (293,294) , led to c l in ica l t r ia ls in mult ip le myeloma
(43,295). The observed responses in pat ients wi thout h igh-grade angiogenesis suggest that
tha l idomide may act v ia o ther mechanisms as wel l (296). In v i t ro data suggest that the drug
and i ts metabol i tes may inh ib i t angiogenesis, but in addi t ion may modulate adhes ion
molecules of myeloma ce l ls and thei r surrounding s troma, modulate cytok ines, and af fec t
natura l k i l le r ce l ls. There is evidence that tha l idomide and i ts analogs induce apoptos is and
G1 growth arrest in myeloma ce l ls (296) .
The f i rs t publ ished report o f the ut i l i ty o f thal idomide in pat ients wi th re lapsed myeloma was
by Singhal e t a l . (43) . Eighty- four pat ients wi th re lapsed myeloma, 76 of whom had relapsed
af ter h igh-dose chemotherapy wi th s tem cel l support , were t reated wi th escalat ing doses of
tha l idomide. Pat ients were star ted on 200 mg each evening; the dose was escalated every 2
weeks i f to lerated to a f ina l maximal dose of 800 mg dai ly. Twenty- f ive percent o f pat ients
had at least a 50% reduct ion in the i r serum paraprotein . Pre l iminary evidence of response
was apparent wi th in 2 months in more than three quarters of the pat ients who d id respond.
Other invest igators have conf i rmed par t ia l response rates of 25 to 58%, with an addit ional 6

to 26% achieving a minimal response, median response durat ion of 9 to 12 months, 2-year
progress ion- f ree survival o f 10 to 20%, and 2-year overal l survival of 48%
(295,297,298,299,300,301,302,303,304,305) .
When tha l idomide is used as a s ingle agent in previous ly unt reated pat ients , response rates
of 25% may be achieved (306,307,308).
The ro le o f dose intens i ty in tha l idomide ef fec t iveness is unc lear (302,309) . In the or iginal
reports , the highest dose to lerated was admin is tered (43) . In h igh-r isk pat ients there was a
suggest ion that response rates were h igher and surviva l longer in pat ients receiv ing h igh
doses of thal idomide (≥600 mg/day) (310) . However, in some pat ients , responses may be
seen wi th doses as low as 50 to 100 mg/day (309) .
Toxic i t ies assoc ia ted wi th tha l idomide inc lude fe ta l malformations, const ipat ion, weakness
or fat igue, somnolence, skin problems, and sensory neuropathy in more than one thi rd o f
pat ients . There is a lso an increased r isk o f thrombosis in pat ients t reated wi th thal idomide,
which appears to be exacerbated by the use of concurrent combinat ion chemotherapy, wi th
ra tes as high as 28% (311,312,313) . Other l i fe-threaten ing compl icat ions have inc luded
Stevens-Johnson syndrome and hepat i t is (314,315) .
Thal idomide is now considered a standard therapy for mul t ip le myeloma, a l though U.S.
Food and Drug Admin is t ra t ion approval for th is ind icat ion is pending.
Lenalidomide (CC-5013; Revlimid) Lenal idomide is a smal l -molecule der ivat ive of tha l idomide and a member of the IMiD c lass.
Lenal idomide is more potent than tha l idomide in mediat ing di rec t cytokine-re lated and
immunomodulatory e ffects against human mul t ip le myeloma cel l l ines and pat ient -der ived
ce l ls in v i t ro. I t induces apoptos is of myeloma cel ls; overcomes cytokine and bone marrow
s t romal ce l l -mediated drug res is tance; has ant iangiogenic e ffec ts ; and s t imulates host
ant imyeloma T- and natura l k i l le r ce l l immuni ty (45,316) . In the or ig ina l Phase I s tudy, 30%
of pat ients responded to s ing le-agent therapy, wi th a 6-month median durat ion of response
(45) . At 50 mg/day the dose-l imit ing toxic i ty was myelosuppress ion. In the randomized
Phase I I t r ia l , two schedules were evaluated: 25 mg dai ly and 15 mg twice dai ly. In both
arms, drug was g iven only 21 out o f 28 days. Overa l l , ~17% of relapsed or re fractory
pat ients ach ieved a part ia l response, inc luding a 4% complete response rate, wi th a median
progress ion- f ree surviva l o f 4 .6 months for the pat ients receiv ing once-dai ly dosing (45,316).
An addi t ional 9% of pat ients achieved a minimal response. Aside f rom myelosuppression,
o ther grade 3–4 toxic i t ies included neuropathy and fa t igue in 3 and 7% of pat ients,
respect ive ly. In the open- label Phase I I t r ia l o f 222 pat ients , there was a 25% par t ia l
response rate, wi th a
P.2386
t ime to progress ion of 5 .1 months (317) . Lenal idomide has never been s tud ied as a s ingle
agent in newly d iagnosed myeloma.
CC-4047 (Actimid) CC-4047 is another IMiD wi th act iv i ty in MM (318) ; 54% of previous ly treated pat ients
respond to s ingle-agent therapy. Median progress ion- f ree survival was 9 months.
Bortezomib (Velcade)

Bortezomib is the f i rs t drug in i ts c lass of proteasome inh ib i tors . I t is a boronic ac id
d ipept ide that reversib ly and selec t ively inh ibi ts the proteasome, an in t race l lu lar complex
that degrades primar i ly ub iqu i t inated prote ins. The proteasome has a key ro le in prote in
degradat ion, cel l -cyc le regulat ion, and gene express ion. Tumor ce l ls, includ ing mul t ip le
myeloma ce l ls , are heavi ly dependent on proteasome-regulated proteins for the i r growth
and in teract ion wi th s tromal ce l ls . Inhibi t ion of the proteasome has emerged as an important
ant i tumor target, and bor tezomib has been shown in v i t ro and in v ivo to cause growth arrest ,
to induce apoptosis , and to inhib i t angiogenes is .
In myeloma pat ients, the same schedule (days 1, 4 , 8, and 11, every 21 days) o f two dose
leve ls , 1 .0 and 1.3 mg/m2 , has been s tud ied as second-l ine therapy as par t o f a randomized
Phase I I study. Pat ients had dexamethasone added to the bor tezomib ei ther because they
had progressed af ter two cyc les or they had not achieved a par t ia l response or bet ter a fter
four cyc les. Though no di rect comparisons were made, in the 1.3-mg/m2 arm there was a
t rend toward h igher s ingle-agent response rates (38 vs . 30%), less f requent dexamethasone
usage (46 vs . 57%), longer durat ion of response (417 days vs . 288 days), and longer t ime
to progress ion (333 vs . 212 days) , but h igher ser ious adverse events . Dose reduct ion was
necessary in a higher propor t ion of pat ients in the 1.3-mg/m 2 arm (35 vs . 11%).
Single-agent response rates in relapsed/ref rac tory myeloma range f rom 28 to 38%, wi th a
median durat ion of response of 8 months (319,320,321,322) . In the APEX t r ia l—the
randomized tr ia l comparing bor tezomib to dexamethasone—the response rates, progress ion-
f ree survival , and overal l survival at 1 year were s ign i f icant ly superior in the bor tezomib-
t reated pat ients compared to the dexamethasone-t reated pat ients (320) . Al though the
or iginal s tud ies using this drug inc luded only eight cyc les of therapy, 63 pat ients were
t reated on an extens ion s tudy wi thout s igni f icant ly more ser ious adverse events than were
seen in the parent s tud ies of e ight cycles alone (323) . In previous ly unt reated myeloma,
response rates were 40% (324) .
The most common adverse events associa ted wi th bortezomib are gast ro in tes t ina l
d isturbances, fa t igue, per ipheral neuropathy, and myelosuppress ion. Seventy- f ive percent
o f pat ients had serious (grade 3–4) adverse events , the most common of which were
thrombocytopenia, neutropenia, anemia, gast ro intes t ina l d is turbances, fa t igue, and
neuropathy (320) .
Arsenic Trioxide In v i t ro , arsenic t r ioxide (ATO) induces growth inh ibi t ion and apoptosis (325) . Generat ion of
react ive oxygen spec ies wi th subsequent accumulat ion of hydrogen peroxide enhances
ATO-induced apoptos is . Because glu ta thione is be l ieved to sa lvage f ree rad icals , methods
to reduce g luta th ione have been explored, the most popular of which is coadminist ra t ion of
ascorbic ac id. In v i t ro, th is approach has appeared to be more ef fec t ive against myeloma
ce l ls o f pat ients wi th ref rac tory d isease than those wi th newly d iagnosed d isease (326) .
As a s ingle agent in re f rac tory d isease, the overa l l part ia l response rate is 7 .1% (327) , wi th
a to ta l o f one thi rd ach ieving a 25% reduct ion in M prot in in one s tudy (328) .
Other Agents Bar log ie e t a l . (286) exp lored the ut i l i ty o f c ispla t in therapy for pat ients wi th myeloma.
Four teen pat ients were treated wi th 10 mg/m 2 for 7 days by cont inuous infus ion, and two

responded. The drug has been incorporated in to o ther reg imens for re lapsed d isease
(286,329,330) and induct ion therapy (331) .
Cytos ine arabinos ide (332) , ten ipos ide (333), topotecan (334) , deoxycoformyc in (335,336),
and pac l i taxe l (337,338) have been repor ted to produce response rates of 7 , 28, 16, 0 to 15,
and 15 to 29%, respect ive ly. Topotecan induces signi f icant toxic i ty, including ≥grade 3
granulocytopenia and thrombocytopenia in 93 and 53% of pat ients, respect ive ly (334) .
Pat ients t reated wi th pacl i taxe l were premedicated wi th 40 mg of dexamethasone every 21
days (337,338) , br ing ing in to quest ion whether the observed responses were at t r ibutable to
dexamethasone or pac l i taxe l .
Agents that do not appear to have any act iv i ty in myeloma include drugs that are interest ing
f rom a h is tor ica l perspect ive and drugs that have known act iv i ty in o ther d iseases. Agents
in the former category inc lude d iamid ines, such as st i lbamid ine; 1-
aminocyc lopentanecarboxyl ic ac id ; amsacr ine (339,340) , aclarub in (341) , ch lorozotocin
(342), hexamethylmelamine (343) , and azaser ine (38). Other agents wi thout ac t iv i ty against
myeloma inc lude methotrexate, 6-mercaptopur ine, 6- th ioguanine, 5- f luorouraci l ,
f luorodeoxyur id ine, hydroxyurea, mi tomyc in C (38) , v inb las t ine, v indes ine (247) , carboplat in
(344), bleomycin (281), ATRA (a l l - t rans - re t ino ic ac id) , f ludarabine (345) , 2-
ch lorodeoxyadenos ine (346) , f lavopi r idol (347), and imat inib (348) . Al though Durie e t a l .
(349) repor ted a 57% response rate wi th c lar i thromycin, subsequent repor ts d id not
corroborate this response rate, and the act iv i ty observed in the or ig ina l repor t was
at t r ibuted to concurrent cor t icosteroid therapy (350,351,352) .
Combination Chemotherapy for Induction
A combinat ion of mult ip le ac t ive agents in an ef for t to achieve synergy is a log ical corol lary.
The las t three decades of the 20th century were spent combining a lkylators , anthracyc l ines,
cor t icosteroids , and interferon. Th i r ty years of s tudy indicate that though these
combinat ions as in i t ia l therapy resul ted in h igher response rates, this d id not trans la te into
longer overa l l survival rates than s tandard melphalan and prednisone therapy (233) (Table
99.6) (F ig . 99.8) . Al though i t has been suggested that pat ients wi th more advanced disease
benef i t f rom combinat ion chemotherapy compared to melphalan (251,272,353,354,355) , that
hypothesis has not been proven (225,233). Now that IMiDs and proteasome inh ib i tors have
been shown to have act iv i ty, c l in ical invest igators have begun us ing these drugs in
combinat ion. For expediency, these regimens wi l l be separated in to f ive categor ies for
d iscussion: Alkyla tor-based wi thout anthracyc l ines, anthracyc l ine-contain ing reg imens,
anthracyc l ine-contain ing regimens wi th in tensi f ied doses of cor t icosteroids , reg imens
incorporat ing inter feron, and novel therapies (Tables 99.6,99.7,99.8) . As a general rule ,
pat ients who are be ing considered for s tem ce l l co l lec t ion and t ransplantat ion rece ive non–
a lkyla tor-containing induct ion reg imens, or i f a lkyla tor-conta ining reg imens are used, the
number o f cyc les is res t r ic ted to four pr ior to stem cel l mobi l izat ion. Cl in ica l research in
myeloma is moving at breakneck speed, and the current preferred induct ion therapies are
a l l in the “novel ” category (Tables 99.7 and 99.8). Descr ip t ions of older reg imens are
provided for two reasons: to g ive a histor ical backdrop; and to fami l iar ize the reader wi th
these reg imens. As “novel ” therapies move to f ront - l ine, these older “ induct ion” regimens
wi l l be important as sa lvage regimens. In t ime, we may be able to bet ter ascer ta in b io log ic
d i f ferences (356) between myeloma pat ients and d i rec t speci f ic types of therapy to thei r
b iology.

In the sett ing of induct ion pr ior to s tem cel l col lec t ion and t ransplantat ion, major quest ions
revo lve around “does i t mat ter” and is “best response” necessary before proceeding to stem
cel l co l lec t ion and t ransplantat ion. Unfor tunate ly, no completed prospect ive randomized t r ia l
has yet addressed this quest ion. Retrospect ive analyses have shown that pat ients
proceeding to stem cel l t ransplantat ion wi th deeper responses do bet ter (357) ; however,
does the bet ter outcome ref lec t on the therapies that brought the pat ient to the bet ter
response? Or does i t just re f lec t the fact that pat ients who
P.2387
have chemotherapy-sensi t ive d isease do bet ter? Is bio logy or therapy provid ing the better
outcomes in these ret rospect ive analyses?
Figure 99.8. Melphalan and prednisone (MP) versus combined chemotherapy (CCT) as induction. Results from 6,633 patients from 27 randomized trials. A: Overall survival. B: Response duration. (From Anonymous. Combination chemotherapy versus melphalan plus prednisone as treatment for multiple myeloma: an overview of 6,633 patients from 27 randomized trials. Myeloma Trialists' Collaborative Group. J Clin Oncol 1998;16:3832–3842. By permission of the American Society of Clinical Oncology.)
Melphalan ± Corticosteroids as Induction Therapy Since ear ly reports by Blokhin et a l . (36) and Bergsagel e t a l . (37) , various schedules of
melphalan have been t r ied, including cont inuous da i ly dose, 6 to 10 mg/day for 2 to 3 weeks,
fo l lowed by maintenance therapy of 0 .01 to 0 .03 mg/kg per day; in termi t tent total doses of
0 .25 mg/day g iven for 4 days every 4 to 8 weeks; or 0.15 mg/kg per day for 7 days every 6
weeks (250,358) . Several s tudies suggest that the intermi t tent schedule is super ior to
cont inuous da i ly dos ing (250,358)
Table 99.7 Induction for Patients Who Are Not Candidates for Hematopoietic Stem Cell Transplantation, Recent Publications

Author Regimen Phase N CR (%)
VGPR (%)
PR (%)
OR (%)
PFS (mo)
OS (mo)
Dex 3 127 1 0 41
42
12.2
33
Dex-IFN
3 121 1 0 42
43
15.2
32
MP 3 122 1 0 40
41
21.1
34
Facon (IFM 95-01) (263)
MD 3 118 3 0 67
70
22.9
40
Dex 3 235 — — — — — 25 Rajkumar, 2006 (446)
Thal-dex
3 235 — — — — — 25
Klueppenlberg, 2005 (1089)
LD-Thal-Dex-Z
2 45 0 30
68
98
2 y, 68%
Thal-dex
3 125/2
10
27
15
52
— — Ludwig, 2005 (450)
MP 3 125/2
3 12
20
35
— —
MP 3 3 5 26
34
17.5
30.3
Facon (IFM 99-06) (476)
MPT 3 0 14
37
33
84
29.5
NR
Palumbo, 2006 (436)
MP 3 126 2 10
36
48
~14
NR
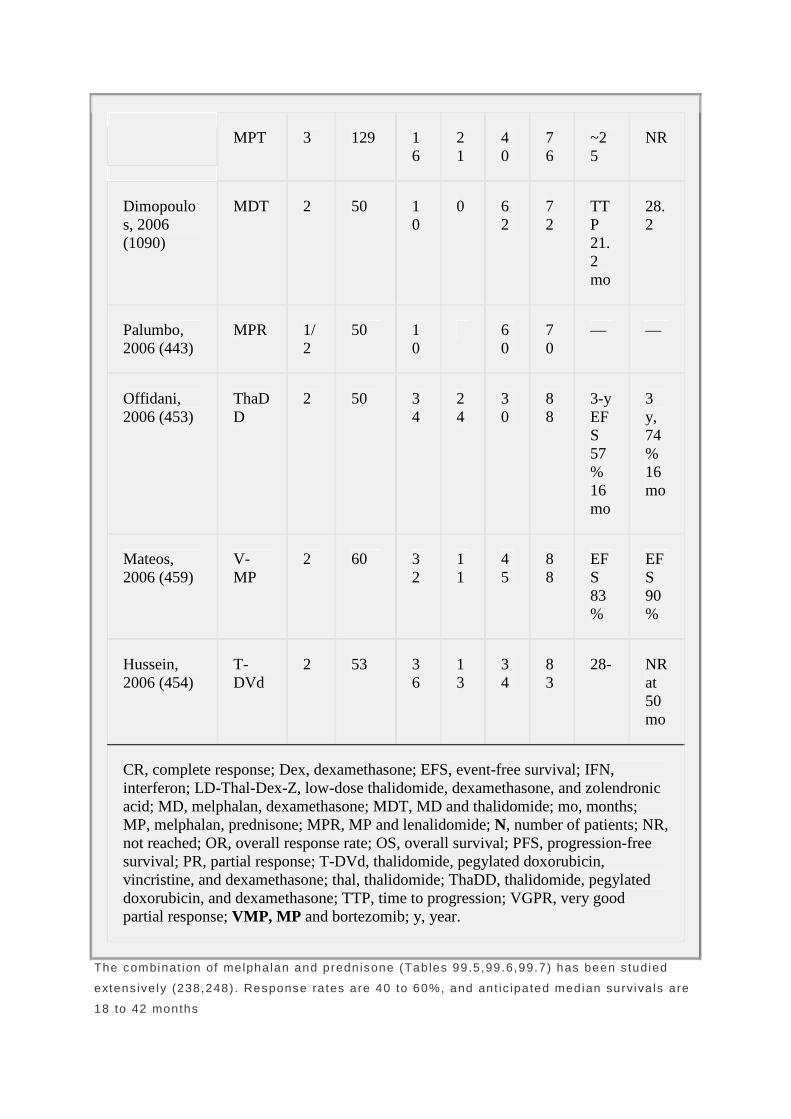
MPT 3 129 16
21
40
76
~25
NR
Dimopoulos, 2006 (1090)
MDT 2 50 10
0 62
72
TTP 21.2 mo
28.2
Palumbo, 2006 (443)
MPR 1/2
50 10
60
70
— —
Offidani, 2006 (453)
ThaDD
2 50 34
24
30
88
3-y EFS 57% 16 mo
3 y, 74% 16 mo
Mateos, 2006 (459)
V-MP
2 60 32
11
45
88
EFS 83%
EFS 90%
Hussein, 2006 (454)
T-DVd
2 53 36
13
34
83
28- NR at 50 mo
CR, complete response; Dex, dexamethasone; EFS, event-free survival; IFN, interferon; LD-Thal-Dex-Z, low-dose thalidomide, dexamethasone, and zolendronic acid; MD, melphalan, dexamethasone; MDT, MD and thalidomide; mo, months; MP, melphalan, prednisone; MPR, MP and lenalidomide; N, number of patients; NR, not reached; OR, overall response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; T-DVd, thalidomide, pegylated doxorubicin, vincristine, and dexamethasone; thal, thalidomide; ThaDD, thalidomide, pegylated doxorubicin, and dexamethasone; TTP, time to progression; VGPR, very good partial response; VMP, MP and bortezomib; y, year.
The combinat ion of melphalan and prednisone (Tables 99.5,99.6,99.7) has been s tudied
extens ive ly (238,248) . Response rates are 40 to 60%, and ant ic ipated median surviva ls are
18 to 42 months

(225,233,238,248,250,253,271,277,278,354,359,360,361,362,363,364,365,366,367,368,369,
370,371,372,373,374) . Because of the var iable gast ro intes t ina l t rac t absorpt ion of
melphalan, in t ravenous reg imens of 15 to 25 mg/m 2 every 4 weeks along wi th ora l
prednisone or dexamethasone have been t r ied and resul ted in response rates of 50 to 82%
(374,375) .
Table 99.8 Induction Regimens for Hematopoietic Stem Cell Transplantation– Eligible Patients
Reference Regimen Phase N CR (%)
VGPR (%)
PR (%)
OR (%)
Rajkumar, 2003 (307)
Thal 2 29 0 0 34 34
Rajkumar, 2001 (306)
Thal 2 16 0 0 37 37
Weber, 2003 (308)
Thal 2 28 0 0 36 36
Dex 3 104 0 0 41 41 Rajkumar, 2006 (441)
Thal-Dex 3 99 4 0 59 63
Rajkumar, 2002 (445)
Thal-Dex 2 50 0 0 64 64
Weber 2003 (308) Thal-Dex 2 40 16 0 56 72
Sidra, 2006 (668) CDT 2 15 0 27 60 87
Rajkumar 2005 (439)
Rev-Dex 2 34 6 32 53 91
Niesvizky, 2006 (465)
BiRD 2 40 25 18 53 95
Jagannath, 2005 Bortez 2 32 3 9 28 40
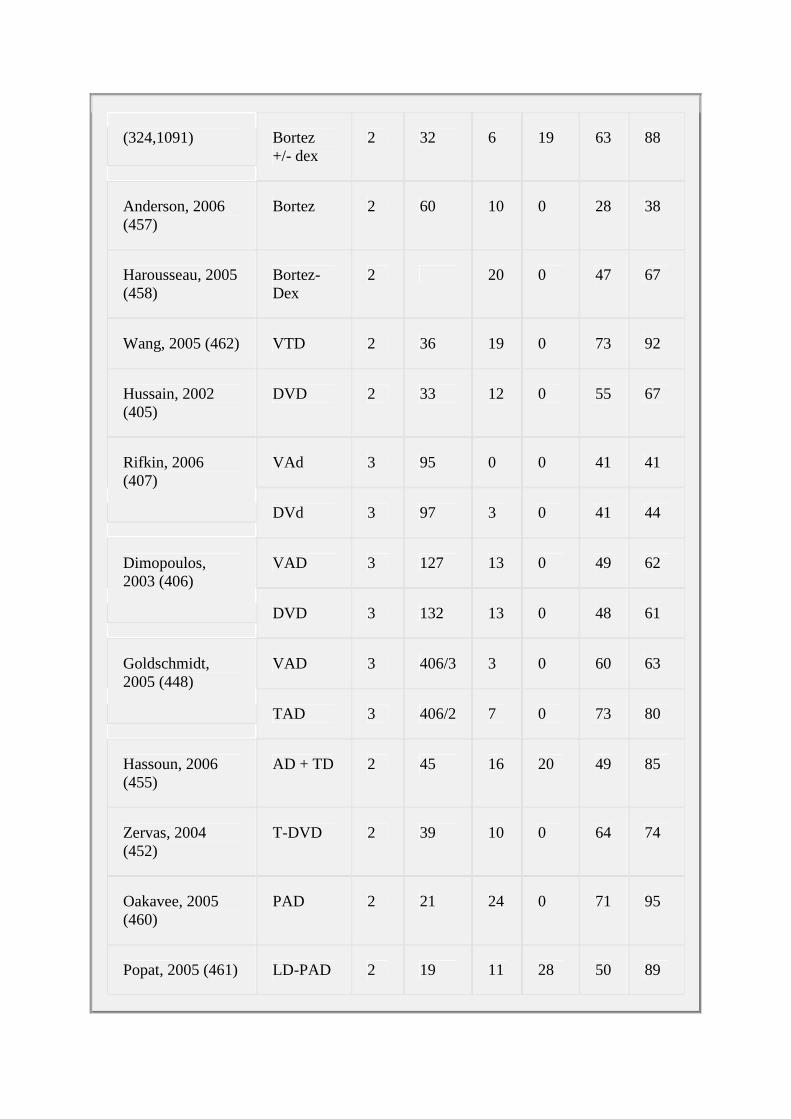
(324,1091) Bortez +/- dex
2 32 6 19 63 88
Anderson, 2006 (457)
Bortez 2 60 10 0 28 38
Harousseau, 2005 (458)
Bortez-Dex
2 20 0 47 67
Wang, 2005 (462) VTD 2 36 19 0 73 92
Hussain, 2002 (405)
DVD 2 33 12 0 55 67
VAd 3 95 0 0 41 41 Rifkin, 2006 (407)
DVd 3 97 3 0 41 44
VAD 3 127 13 0 49 62 Dimopoulos, 2003 (406)
DVD 3 132 13 0 48 61
VAD 3 406/3 3 0 60 63 Goldschmidt, 2005 (448)
TAD 3 406/2 7 0 73 80
Hassoun, 2006 (455)
AD + TD 2 45 16 20 49 85
Zervas, 2004 (452)
T-DVD 2 39 10 0 64 74
Oakavee, 2005 (460)
PAD 2 21 24 0 71 95
Popat, 2005 (461) LD-PAD 2 19 11 28 50 89

Badros, 2005 (463)
VDT-PACE
1/2 11 9 9 92 100
TT1 2 231 12 0 51 63 Barlogie, 2006 (1092)
TT2 no thal
3 323 10 0 30 40
Barlogie, 2006 (594)
TT2 +thal
3 345 19 0 41 60
See Table 99.7 for abbreviations.
P.2388
Not unt i l the report by McElwain and Powles (237) on the successfu l use of high-dose
melphalan (140 mg/m 2 int ravenously) had dose intens i ty been studied in myeloma. In
previously unt reated pat ients , Selby et al . (243) conf i rmed a 78% response rate, inc lud ing
27% of pat ients whose M component was no longer v is ible by prote in elect rophores is . Th is
dose in tensi ty wi thout s tem cel l salvage was assoc ia ted wi th pro longed, severe
thrombocytopenia and leukopenia ( las t ing a median of 24 and 28 days, respect ive ly) .
Treatment- re lated mortal i ty was 19%. The benef i t o f melphalan dose in tens i f icat ion was
conf i rmed by others who used at tenuated doses (50 to 70 mg/m 2 ) and repor ted response
rates of 50 to 85% (376,377,378) . These dose schedules are assoc iated wi th 8 and 6 days
of severe neutropenia and thrombocytopenia, respect ive ly (377). Doses of 25 to 30 mg/m 2
wi l l e f fec t responses in ~35 to 40% of re lapsed, re f rac tory pat ients (379,380) .
Cyclophosphamide ± Corticosteroids as Induction The rapy Since the or ig ina l repor t by Korst e t a l . (39) of the ut i l i ty o f cyclophosphamide in myeloma
pat ients , severa l s ingle-agent induct ion reg imens have been s tud ied. Despite documented
equiva lency for low-dose oral reg imens of cyc lophosphamide and melphalan (252),
induct ion therapies of melphalan and prednisone tend to be preferred over those of
cyc lophosphamide and prednisone. Most commonly, cyclophosphamide has been used in
mult idrug combinat ions for induct ion, for therapy in re lapse, and for s tem ce l l mobi l izat ion
ra ther than as a s ing le agent for induct ion, as has melphalan. For newly d iagnosed
myeloma, ora l da i ly dos ing of cyc lophosphamide (150 mg/day) (252,381,382) or in t ravenous
doses of 600 mg/m 2 every 3 weeks (253) , wi th or wi thout prednisone, has resul ted in a
response rate of ~25% and median surviva l o f 24 months.
Multidrug Combination Chemotherapy without Anthracy cline for
Induction

The 1970s and 1980s were a tes t ing ground for var ious combinat ions of alkylators ,
cor t icosteroids , and doxorubic in . Melphalan/cyclophosphamide/prednisone (270) ,
carmust ine/ cyclophosphamide/prednisone (359,60) ,
melphalan/cyc lophosphamide/armust ine/prednisone (MCBP) (270,353) , and
vincr is t ine/melphalan/cyc lophosphamide/prednisone (VMCP) (270) resul ted in response
rates of 47, 37 to 50, 49 to 68, and 62%, respect ive ly. Median survivals with these reg imens
were 25 to 36 months (270,353,359,360) . Lee and Case (274) int roduced the f ive-drug
reg imen of v incr is t ine/carmust ine/melphalan/cyc lophosphamide/prednisone (VBMCP or the
M-2 reg imen), which inc luded the same four drugs as MCBP p lus v incr is t ine; dose
in tensi t ies, however, were d i f ferent in these two reg imens. Response rate for VBMCP was
~85% in previous ly unt reated pat ients , wi th a median surviva l o f 38 months (274,383) . The
success of the VBMCP regimen supported the value of v incr ist ine. However, the MRC IV
t r ia l , which randomized 530 previous ly unt reated pat ients wi th myeloma to melphalan and
prednisone versus melphalan/vincr is t ine/prednisone, revealed no d i f ference in e i ther
response rate or overal l surviva l between the two arms (278). VMCP has not produced any
response or surviva l advantage over melphalan and prednisone (371,384). F ina l ly, the
MOCCA regimen, which is essent ial ly VBMCP wi th CCNU replac ing BCNU, resu l ts in
response rates s imi lar to those for VBMCP (75%), but again no surviva l benef i t in
comparison to melphalan and prednisone (363)
Al though subsequent randomized t r ia ls have substantia ted the superior response rates of
VBMCP over s tandard melphalan and prednisone (Table 99.6) , they have not demonstrated
super ior
P.2389
surviva l (277,364,373,385) . In fac t , the meta-analys is per formed by the Myeloma Tr ial is ts '
Col laborat ive Group (233) , invo lv ing 6,633 pat ients in 27 randomized t r ia ls , revealed a
super ior response rate (60.2 vs . 53.2%, p < .000001, two- ta i led) but no surviva l benef i t for
combinat ion chemotherapy over standard melphalan and prednisone (F ig . 99.8) . A pr ior
meta-analysis o f 18 publ ished t r ia ls (3 ,814 pat ients) a lso demonstrated no benef i t for
combinat ion chemotherapy in terms of survival . There might be a survival advantage in the
subgroup of pat ients wi th more aggress ive d isease (355) , but th is was not substant iated in
the larger meta-analys is (233).
Combination Chemotherapy with Anthracycline for Ind uction The use of a lkylator /doxorubic in-based combinat ion chemotherapy was s t imulated by a
report on the benef i ts o f a combinat ion of doxorubic in and BCNU in pat ients who had
become res is tant to melphalan (386) . Regimens such as MAP
(melphalan/doxorubic in/prednisone), CAP (cyclophosphamide/doxorubic in /prednisone),
VCAP (vincr ist ine and CAP), and VBAP (vincr is t ine/BCNU/ doxorubic in /prednisone) were
t r ied; by SW OG response cr i ter ia , objec t ive response rates were 41, 46, 64, and 61%,
respect ive ly (270,387) . Median surviva l ranged from 30 to 32 months; subsequent analys is
demonstrated a super ior median surviva l for the VBAP arm of 37 months (388).
Enthus iasm for a l ternat ing VMCP and VBAP (or VCAP) was generated by the SW OG study
of 237 pat ients randomized to melphalan and prednisone or the above regimens (Table
99.9) (368,369). Response rates were super ior in the a l ternat ing combinat ion chemotherapy
arms compared to the melphalan arm. Survival was a lso super ior in the combinat ion

chemotherapy arms (43 vs . 23 months for melphalan and prednisone, p = .004) (387).
However, a subsequent analys is wi th longer fo l low-up showed less separat ion of the
surviva l curves (median surviva l , 25 vs . 36 months) (388) . The survival benef i ts o f th is
in i t ia l study were not reproduc ib le by others (271,365,366,370,372,389,390) .
The Vth MRC myelomatos is t r ia l randomized pat ients to ABCM (VBAP/VMCP wi thout the
v incr is t ine or prednisone) or melphalan as a s ing le agent on the basis o f f ind ings emanat ing
f rom the IV MRC t r ia l , which demonstrated a lack of benef i t a t t r ibutable to the addit ion of
v incr is t ine. Median surviva l in the ABCM group was super ior to that o f the melphalan-only
arm (32 vs . 24 months, p = .0003) (251) . W hen corrected for adverse prognost ic fac tors
such as e levated β2 -M va lues, low hemoglobin va lues, renal insuff ic iency, performance
s ta tus, and s tage, the s ign i f icance of the survival d i f ference was p = .003 (280) .
Table 99.9 Risk of IMiD-Associated Thromboembolism
Reference N Regimen Prophylaxis TE (%)
134 TT2 No 14
87 TT2 + Thal No 34
35 TT2 + Thal LD coumadin 31
62 TT2 Enox 15
68 TT2 + Thal Enox 15
Zangari 2004 (437)
19 DVd-T No 58
26 DVd-T Late ASA 15 Baz, 2005 (438)
58 DVd-T ASA 19
Rajkumar 2005 (439)
34 Len-Dex ASA 0
65 MPT No 17 Palumbo, 2006 (436)
64 MPT Enox 3.1
Palumbo 2006 (443) 50 MPR ASA 2
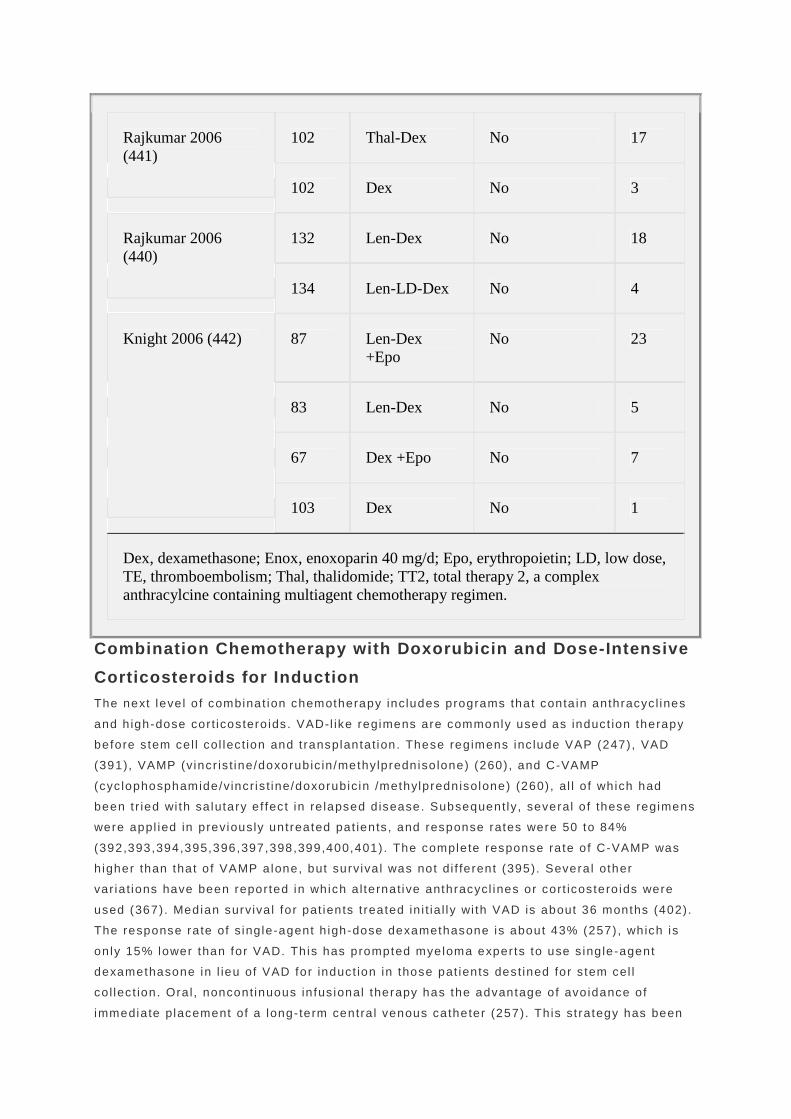
102 Thal-Dex No 17 Rajkumar 2006 (441)
102 Dex No 3
132 Len-Dex No 18 Rajkumar 2006 (440)
134 Len-LD-Dex No 4
87 Len-Dex +Epo
No 23
83 Len-Dex No 5
67 Dex +Epo No 7
Knight 2006 (442)
103 Dex No 1
Dex, dexamethasone; Enox, enoxoparin 40 mg/d; Epo, erythropoietin; LD, low dose, TE, thromboembolism; Thal, thalidomide; TT2, total therapy 2, a complex anthracylcine containing multiagent chemotherapy regimen.
Combination Chemotherapy with Doxorubicin and Dose- Intensive
Corticosteroids for Induction The next leve l o f combinat ion chemotherapy includes programs that conta in anthracyc l ines
and h igh-dose cor t icostero ids . VAD-l ike regimens are commonly used as induct ion therapy
before s tem cel l col lec t ion and t ransplantat ion. These reg imens inc lude VAP (247) , VAD
(391), VAMP (vincr is t ine/doxorubic in /methylpredniso lone) (260) , and C-VAMP
(cyc lophosphamide/vincr is t ine/doxorubic in /methylprednisolone) (260) , al l o f which had
been t r ied wi th sa lutary e f fec t in re lapsed d isease. Subsequently, several o f these regimens
were appl ied in previously unt reated pat ients , and response rates were 50 to 84%
(392,393,394,395,396,397,398,399,400,401) . The complete response rate of C-VAMP was
h igher than that o f VAMP alone, but surviva l was not di f ferent (395). Severa l other
var ia t ions have been repor ted in which a l ternat ive anthracycl ines or cort icostero ids were
used (367) . Median surviva l for pat ients t reated in i t ia l ly wi th VAD is about 36 months (402) .
The response rate of s ing le-agent h igh-dose dexamethasone is about 43% (257) , which is
on ly 15% lower than for VAD. This has prompted myeloma experts to use s ing le-agent
dexamethasone in l ieu of VAD for induct ion in those pat ients dest ined for s tem cel l
co l lec t ion. Ora l , noncont inuous in fus ional therapy has the advantage of avo idance of
immediate placement of a long- term centra l venous catheter (257). Th is st ra tegy has been

used successful ly, resu l t ing in adequate col lec t ions of per iphera l b lood stem cel ls wi thout
any apparent adverse ef fec ts on complete remission rates or progression- free survival in
several s ing le-arm s tud ies (403,404) . W ith the advent o f other ora l therapies, s ing le-agent
dexamethasone has been los ing favor as induct ion.
In another a t tempt to avo id the cont inuous in fus ion requi red to admin is ter VAD, several
invest igators have explored the use of the pegylated l iposomal doxorubic in . The
combinat ion of v incr is t ine, pegylated l iposomal doxorubic in , and dexamethasone (DVD) has
been studied. Response rates f rom s ingle ins t i tu t ions suggested that DVD was more
convenient and less toxic than VAD (405) . Two randomized t r ia ls comparing DVD to VAD—
using e i ther s tandard h igh-dose dexamethasone (406) or a t tenuated doses of
dexamethasone (407)—have been completed. Results were comparable between arms wi th
regard to response rates, 42% in the at tenuated-dexamethasone t r ia l (407) and 61% in the
s tandard-dose dexamethasone t r ia l (406). There was more alopecia in the non–l iposomal
doxorubic in arms and more pa lmar-p lantar erythrodysesthesia in the l iposomal doxorubic in
arms.
In a randomized t r ia l o f 151 pat ients compar ing the NOP reg imen (mi toxantrone, v incr ist ine,
and h igh-dose prednisone) to melphalan and prednisone, response rates were equiva lent
(~60%), but overal l surviva l was in fer ior in the NOP arm (14 vs . 31 months, p = .02) (367) .
Response rates of 80% have also been achieved using the CAD
(cyc lophosphamide/doxorubic in /dexamethasone) reg imen (408) . The addit ion of e topos ide
to C-VAD appears to contr ibute only toxic i ty (409) .
Combination Chemotherapy with Interferon for Induct ion In terferon-α ( INF) and dexamethasone have been combined as an induct ion reg imen in
pat ients wi th newly d iagnosed myeloma and a low tumor mass. A ret rospect ive comparison
showed that the response rate of th is regimen (57%) was s imi lar to the response rate (48%)
previously observed wi th dexamethasone alone (410) . A recent randomized t r ia l comparing
MP, melphalan/dexamethasone, dexamethasone, and dexamethasone/ IFN d id not
demonstrate any added benef i t by incorporat ing IFN into the t reatment reg imen (263) . Ahre
et al . (411) randomized 55 pat ients to melphalan and prednisone
P.2390
or in ter feron (3 to 6 MU dai ly) ; response rates in the melphalan and prednisone arm were
s ign i f icant ly h igher than in the in ter feron arm (44 vs . 14%, p < .001) .
In terferon has been combined wi th melphalan and prednisone
(412,413,414,415,416,417,418,419,420) ; VMCP (414,421,422,423); VMCP/VBAP (424) ,
prednisone, cyc lophosphamide, doxorubic in (Adr iamycin) , and carmust ine (BCNU) (PCAB)
(425,426) ; VAD (427) ; VBMCP (428) ; VBAP (429) ; and cyc lophosphamide (430) as par t o f
an induct ion reg imen. Resul ts have been mixed. Two meta-analyses have been per formed in
an at tempt to reconc i le these conf l ic t ing resu l ts (431,432) . The f i rs t , repor ted in 2000 by
Ludwig and Fr i tz (431) , used publ ished data and inc luded 17 induct ion t r ia ls
(412,413,414,415,416,417,418,419,420,422,423,424,425,426,427,429,430) wi th 2 ,333
evaluable pat ients ; the second, repor ted by The Myeloma Tr ia l is ts ' Col laborat ive Group in
2001 (432) , used pr imary data f rom 12 induct ion t r ia ls
(412,413,414,415,416,417,418,419,420,422,424,425,426,428,429,430,433) invo lv ing 2,469
pat ients . Overa l l , the resu l ts were s imi lar . In the f i rs t meta-analys is , the benef i ts

at t r ibutable to the addi t ion of in terferon to the induct ion reg imen included a 6.6% higher
response rate (p < .002) and a 4.8- and 3.1-month prolongat ion of relapse- f ree (p < .01)
and overal l survival (p < .01) , respect ive ly (431) . In the second meta-analys is , pat ients
receiv ing in terferon had a s l ight ly bet ter response rate (57.5 vs . 53.1%, p = .01) and
progress ion- f ree survival (30 vs. 25% at 3 years , p < .0003) , wi th a super ior median t ime to
progress ion of about 6 months. The surviva l advantage of 2 months, however, was not
s ign i f icant (p = .1) (432). F igure 99.9 demonstrates progress ion-f ree surviva l and overa l l
surviva l in pat ients receiv ing IFN as ei ther induct ion or maintenance versus those who
received none (432).
These meta-analyses suggest that incorporat ion of in terferon in to induct ion provides a
modest pro longat ion of response and possibly o f surviva l . The quest ion is whether these
s ign i f icant d i f ferences are c l in ica l ly re levant . W islo f f e t a l . (434) eva luated the qual i ty o f l i fe
o f 583 pat ients randomized to ei ther melphalan and prednisone or melphalan, prednisone,
and in ter feron as induct ion. Dur ing the f i rs t year o f t reatment wi th in ter feron, the pat ients
reported s igni f icant ly more fever, ch i l ls , dry sk in, fa t igue, pa in , nausea/vomi t ing, and
appet i te loss than the control pat ients . After the f i rs t year , however, the on ly symptom
reported more of ten was d izziness. Al though pat ients receiv ing inter feron had a 5- to 6-
month pro longat ion of the response and p lateau phase, there was no la te qual i ty-of - l i fe
benef i t observed to compensate for the ear ly impai rment. The authors quest ioned the
c l in ical va lue of the p lateau-phase prolongat ion and repor ted that only 60% of pat ients
cont inued to rece ive inter feron after 24 months, suggest ing that thei r data might
underest imate the potent ia l toxic i ty of the drug. A cost -ef fec t iveness est imat ion for
induct ion was also per formed. The authors conc luded that in ter feron admin is t ra t ion and
moni tor ing expenses amounted to $US 41,319.28 to save a year o f l i fe of myeloma pat ients ,
assuming a dosage of 12.1 MU/week (431).
A s tudy on pat ient preference also deserves mention. Ludwig et a l . (435) surveyed cancer
pat ients about “acceptable” toxic i ty o f an unident i f ied drug, which had the toxic i ty prof i le o f
in ter feron, re la t ive to i ts hypothet ical benef i t . About 50% of surveyed pat ients accepted the
toxic i ty o f an unident i f ied drug i f remiss ion or surviva l or both would be improved by at least
6 months. Of those pat ients who re jec ted the 6-month hypothet ica l benef i t , 25 to 50% were
wi l l ing to accept the toxic i t ies i f the benef i ts were ≥12 months.
Novel Therapies for Induction (Tables 99.7 and 99.8)
Complications Specific to Novel Therapies These new drugs can cause the compl icat ions seen wi th o ther agents , such as fa t igue,
myelosuppress ion, fevers , in fec t ions, and gastro in tes t ina l symptoms; however, there are
several s ide ef fec ts par t icu lar to these new agents—the most important o f which are
thrombosis and periphera l neuropathy.
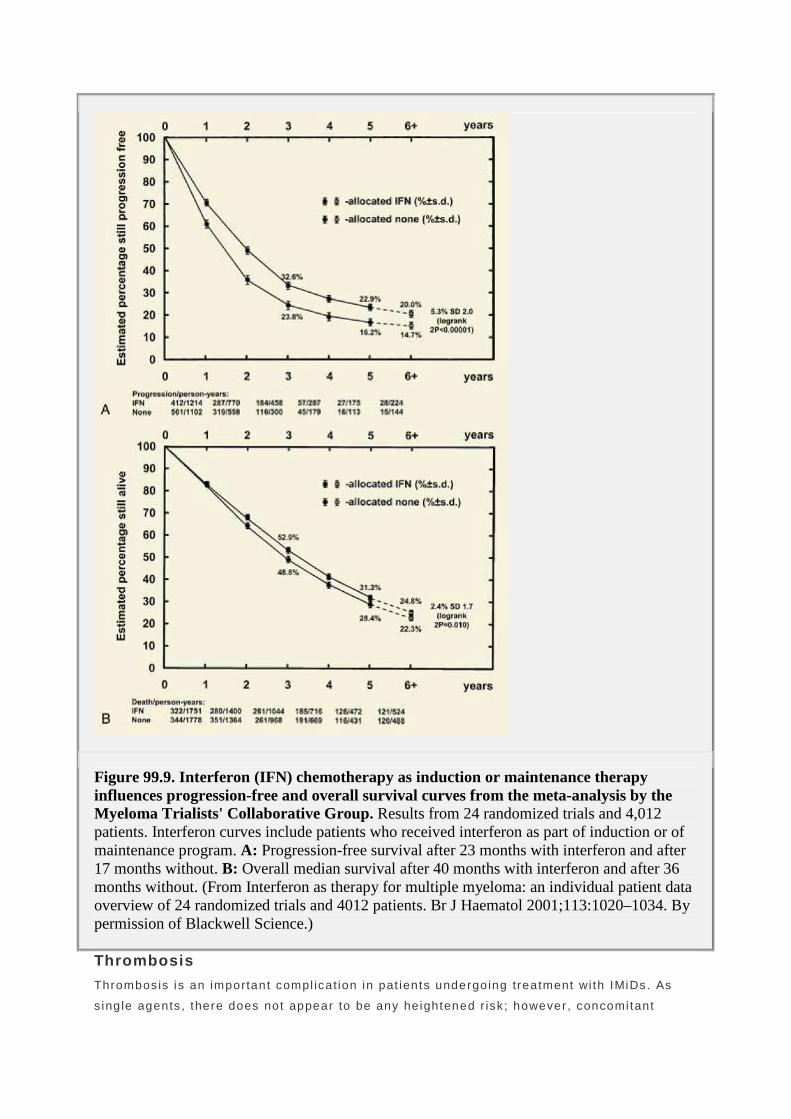
Figure 99.9. Interferon (IFN) chemotherapy as induction or maintenance therapy influences progression-free and overall survival curves from the meta-analysis by the Myeloma Trialists' Collaborative Group. Results from 24 randomized trials and 4,012 patients. Interferon curves include patients who received interferon as part of induction or of maintenance program. A: Progression-free survival after 23 months with interferon and after 17 months without. B: Overall median survival after 40 months with interferon and after 36 months without. (From Interferon as therapy for multiple myeloma: an individual patient data overview of 24 randomized trials and 4012 patients. Br J Haematol 2001;113:1020–1034. By permission of Blackwell Science.)
Thrombosis
Thrombosis is an important compl icat ion in pat ients undergoing treatment wi th IMiDs. As
s ing le agents , there does not appear to be any he ightened r isk ; however, concomi tant

chemotherapy (436)—especial ly anthracycl ines (437,438)—high-dose cort icosteroids
(439,440,441) , and erythropoiet in (442) appear to increase the r isk o f thrombosis to as h igh
as 58% (Table 99.9) . Prophylact ic low-molecular-weight hepar in (e .g . , enoxapar in 40 mg
dai ly) (436,437)or fu l l ant icoagulat ion wi th Coumadin abrogates that r isk. Low-dose
Coumadin is not protect ive. Dai ly asp i r in a lso appears to be protect ive (441,442,443) .
Peripheral Neuropathy
Thal idomide and bor tezomib are known to cause per iphera l neuropathy in more than a th i rd
o f pat ients . Pat ients treated wi th lenal idomide are a lso at r isk for neuropathy, but because
most s tudy pat ients receiv ing lenal idomide have been previous ly t reated, the raw rates are
unknown. The neuropathy associa ted wi th thal idomide is an i r revers ib le smal l - f iber
per iphera l neuropathy that appears to be both t ime- and dose-dependent.
The peripheral neuropathy assoc iated wi th bor tezomib has been bet ter character ized (444) .
I t comes in a l l forms: sensory, motor , and pa inful . In a recent review of 256 pat ients treated
in
P.2391
two Phase I I s tud ies, >80% of pat ients had basel ine peripheral neuropathy. Treatment-
emergent neuropathy was repor ted in 35% of pat ients . Grade 1 or 2 , 3 , and 4 neuropathy
occurred in 22, 13, and 0.4% of pat ients, respect ive ly. Grade 3 neuropathy was more l ikely
to occur in pat ients wi th a basel ine neuropathy. Seventy-one percent o f pat ients wi th
neuropathy ≥grade 3 and/or requi r ing discont inuat ion exper ienced resolut ion to basel ine or
improvement.
Thalidomide Combinations for Induction Therapy As a s ingle agent , response rates occur in about one th i rd of pat ients (306,307,308) . The
combinat ion of tha l idomide and dexamethasone resul ts in response rates of 63 to 72%
(308,445,446) . The tha l idomide/dexamethasone combinat ion has been compared to
dexamethasone a lone in two separate randomized t r ia ls (446). In the smal ler o f the two
t r ia ls (n = 207) , the overa l l response rate of tha l idomide/dexamethasone was s ign i f icant ly
h igher than that o f dexamethasone alone (63 vs. 41%); however, toxic i ty was greater using
the combinat ion, wi th grade 4–5 toxic i ty being 45 vs . 21%, p < .001 (441) . In the second,
larger t r ia l (n = 470 pat ients) , t ime to progress ion was signi f icant ly better in the
combinat ion arm (17.4 months, 95% CI : 8 .1 months—not reached vs . 6 .4 months, 95% CI :
5 .6 to 7.4 months) . Grade 3–4 adverse events were higher us ing the combinat ion therapy:
deep ve in thrombosis (DVT)/pu lmonary embol ism (PE) 15.4 versus 4.3%; cerebral ischemia
3.4 versus 1.3%; myocard ial in farc t ion 4.7 versus 1.3%, per iphera l neuropathy 3.8 versus
0.4% (446) . Th is combinat ion is commonly used as induct ion in the months before s tem cel l
co l lec t ion because of i ts h igh response rate and ease of admin is t rat ion, using only oral
medicat ions. The r isk o f thrombosis and other s ide ef fects make the combinat ion less
convenient than original ly thought . L imited use of thal idomide pre–stem cel l mobi l izat ion
does not impai r stem ce l l co l lect ion or engraf tment , al though pre l iminary data suggest that
there may be a de lay in p la te le t engraf tment wi th longer cont inuous use (447) .
Goldschmidt e t a l . (448) have repor ted prel iminary resul ts f rom the induct ion por t ion of the
HOVON 50/GMMG-HD3-Tr ia l , which is a Phase I I I s tudy of the ef fec t o f tha l idomide fo l lowed
by t ransplant in myeloma pat ients up to 65 years of age. Pat ients were randomized to e i ther

3 cycles of TAD ( thal idomide, 200 mg for HOVON/400 mg for GMMG; Adr iamyc in 9 mg/m 2 ,
days 1 to 4 ; dexamethasone 40 mg, days 1 to 4 , 9 to 12, 17 to 21) or VAD. The f i rs t group
of 406 pat ients (o f 1 ,050 inc luded) are evaluable for the compar ison of VAD versus TAD. A
t rend for a h igher toxic i ty was observed in the TAD arm compared wi th the VAD arm
(dropouts : 15 vs . 8%, p = .10) , though the overal l (80 vs . 63%, p < .001) and complete
response (7 vs . 3%, p = .1) rates were higher wi th TAD. However, prel iminar i ly there is no
d i f ference in overa l l or complete response af ter hematopoiet ic s tem ce l l t ransplantat ion
(HSCT). Cavo et a l . (449) per formed case match ing to compare pat ients treated wi th
tha l idomide/dexamethasone (TD) or VAD. L ike the HOVON/GMMG tr ia l , h igher induct ion
response rates were seen (76 vs . 52%). Toxic i ty prof i les were di f ferent , wi th more
myelosuppress ion in the VAD-t reated pat ients, but DVT was more common in the TD
pat ients . The number of pat ients who died and who did not make i t to t ransplant were also
comparable. Simi lar numbers of s tem ce l ls were co l lec ted in the TD arm compared to the
VAD arm, 7 .85 versus 10.5 ×106 CD34/kg (p = .4). Th is compar ison is confounded by the
fac ts that this was only a case-match compar ison ( ra ther than a randomizat ion) and that the
TD group received tha l idomide not only during induct ion but a lso dur ing transplantat ion and
post t ransplantat ion.
Though thal idomide/dexamethasone resul ts in h igher response rates compared to melphalan
and prednisone (450) , i t cannot be recommended as induct ion for e lder ly pat ients who are
not dest ined for periphera l blood s tem cel l col lec t ion because of the high toxic i ty ra tes .
Ludwig et al . randomized 350 elder ly pat ients to e i ther thal idomide/dexamethasone or
melphalan and prednisone. Pre l iminary data demonstrate a higher response rate using TD
(52 vs . 35%, p < .05) , but h igher ra tes of neuropathy (25 vs . 8%), psycholog ical toxic i ty (20
vs . 8%), skin toxic i ty (12 vs . 3%), and thrombotic events (8 vs . 3%). The only toxic i ty more
commonly seen in the MP arm was myelosuppress ion.
In contrast , combin ing melphalan, prednisone, and tha l idomide is qui te promis ing in e lder ly
pat ients who are not HSCT candidates, and, based on the resu l ts of two randomized tr ia ls
(436,451) , many would consider this program to be the new s tandard. Palumbo et al .
randomized pat ients to ei ther standard-dose oral melphalan and prednisone (MP) for 6
months or to melphalan and prednisone for 6 months wi th concurrent tha l idomide (MPT) that
is cont inued indef ini te ly (436). Overa l l response rates were s ign i f icant ly h igher wi th the
MPT than the MP (76.0 vs . 47.6%), as were the near-complete or complete response rates
(27.9 vs . 7 .2%) and the 2-year event- free surviva l ra tes (54 vs . 27%, p = .0006) . There was
a t rend toward improved 3-year overa l l surviva l in favor o f MPT (80 vs . 64%). Two cr i t ic isms
of this t r ia l are that 6 months of MP is shor t o f s tandard by about 6 months and that this
t r ia l addresses a maintenance quest ion as much as an induct ion quest ion.
The IFM 99-06 t r ia l bo ls ters the resu l ts o f the Palumbo t r ia l , though i t has not yet been
publ ished in pr in ted form (451) . In the IFM 99-06 s tudy, 436 pat ients were randomized to 1
year o f e i ther MPT or MP or to two sequential min i -autologous per iphera l b lood s tem cel l
t ransplants (MEL100). Higher response rates and longer progression- f ree surviva l (PFS)
were seen for the MPT compared to e i ther the MP or MEL100 groups, wi th respect ive PFS
t imes of 29.5, 17.2, and 19.0 months. W ith a median fo l low-up of 32 months, there is a
s ign i f icant surviva l advantage for the pat ients on the MPT arm, wi th respect ive overa l l
surviva l t imes not reached at 56, 30.3, and 38.6 months (451) . So far , no data have been

provided regard ing the percent o f pat ients in the nonthal idomide arm who received
tha l idomide regimens as salvage therapy.
Though both MPT-versus-MP t r ia ls demonstrated h igher response and surviva l endpoints for
MPT, they a lso had a cons is tent ly h igher toxic i ty prof i le for the three-drug combinat ion
compared to the two-drug combinat ion. In the Palumbo s tudy (436) , the respect ive
percentage of pat ients having grade 3–4 adverse events were as fo l lows: a t least 1 event ,
48 versus 25% (p = .0002) ; thrombosis /embol ism, 12 versus 2%; periphera l neuropathy, 10
versus 1%; in fec t ions, 10 versus 2%; and gastro in tes t ina l events , 6 versus 1%. There was
no s ign i f icant d i f ference in the toxic death ra te between the two arms (8 vs . 5%). The
authors poin t out that the f i rs t 65 pat ients rece ived no DVT prophylaxis , whi le the f inal 64
received enoxapar in ; 13 thromboembol ic events occurred in the f i rst group, but only 2
occurred in second group, and that was after d iscont inu ing the enoxaparin .
Dimopoulos et al . have explored a d i f ferent adminis t ra t ion schedule of tha l idomide a long
wi th melphalan. They treated 50 pat ients 75 years or o lder wi th melphalan, dexamethasone,
and thal idomide. A cycle was 5 weeks in durat ion, and the respect ive doses and schedules
of the three drugs were melphalan 8 mg/m2 days 1 to 4 ; dexamethasone 12 mg/m 2 days 1 to
4 and 14 to 18; and thal idomide 300 mg days 1 to 4 and 14 to 18. A planned course of
t reatment was three cyc les as above, but i f pat ients responded, the next n ine cyc les were
adminis tered wi thout the day 14–18 tha l idomide and dexamethasone. Us ing th is program,
62% of pat ients had a par t ia l response to therapy and 10% had a complete response.
Median t ime to progression was 21.2 months, deep venous thrombosis and peripheral
neuropathy each occurred in 9% of pat ients, and overa l l surviva l was 25 months.
Palumbo et a l . have t reated 50 e lder ly pat ients who were not deemed candidates for HSCT
wi th melphalan, prednisone, and lenal idomide (443) . Pat ients received aspi r in and
c iprof loxac in as prophylaxis . Pre l iminary reports demonstrated an overal l response rate of
70%, inc luding a 10% complete response rate. Th i r ty- f ive percent o f pat ients had grade 3–4
adverse events, includ ing one thromboembol ic event and two dermatologic events . The
major i ty o f adverse events cons is ted of myelosuppress ion.
P.2392
Zervas et a l . (452) treated 39 pat ients wi th thal idomide, v incr is t ine, pegyla ted l iposomal
doxorubic in, and dexamethasone and assessed response after four cyc les . Responses were
seen in 74%, inc luding 10% complete response. Grade 3–4 toxic i t ies included neutropenia
(15%), thrombosis (10%), const ipat ion (10%), rash (5%), and peripheral neuropathy (5%).
Two pat ients suf fered ear ly deaths secondary to in fec t ion. For ty-seven percent of pat ients
went on to s tem cel l co l lec t ion and t ransplantat ion.
Of f idani t reated 50 newly d iagnosed mul t ip le myeloma pat ients >65 years old wi th
tha l idomide (100 mg/day) , dexamethasone (40 mg on days 1 to 4 and 9 to 12), and
pegylated l iposomal doxorubic in (40 mg/m 2 on day 1) every 28 days for a to tal o f f ive to s ix
cyc les . The overa l l response rate was 88% (CR 34%, VGPR/nCR [near complete response]
24%, and PR 30%). Time to progress ion, event- f ree surviva l , and overa l l surviva l pro jec ted
at 3 years were 60, 57, and 74%, respect ive ly. Grade 3–4 infec t ions and thromboembol ic
acc idents were observed in 22 and 14% of pat ients , respect ively (453) .

Hussein et a l . (454) t reated 55 previously unt reated pat ients wi th DVd-T (pegylated
l iposomal doxorubic in, v incr is t ine, decreased-f requency dexamethasone, and tha l idomide)
for a maximum of e ight cyc les , fo l lowed by maintenance wi th maximum tolerated doses of
tha l idomide p lus a l ternate-day ora l prednisone. Though response rates were high (overa l l
93%, wi th CR of 36%), there was substant ial toxic i ty assoc iated wi th the program. Grade 3–
4 toxic i t ies included thromboembol ic events in 25%, per iphera l neuropathy in 22%,
neutropenia in 14%, pneumonia in 12%, palmar plantar erythrodysesthesia in 8%, and
thrombocytopenia in 5%. The median PFS was 28.2 months, and the overal l survival (OS)
was not reached at 50 months. Note that al though the pat ients of Of f idani e t al . (453) were
o lder and received lower doses of tha l idomide and no vincr is t ine, s imi lar response rates and
less toxic i ty were seen.
Hassoun et a l . (455) t reated 45 newly d iagnosed myeloma pat ients wi th doxorubic in and
dexamethasone for 2 or 3 months, fol lowed by tha l idomide and dexamethasone for 2 months
(AD-TD reg imen), wi th prophylact ic ant ibio t ics and dai ly aspi r in (81 mg/day) . Th i r ty-e ight
responded to therapy (84.4%), wi th seven complete responses (15.5%), n ine near-complete
responses (20.0%), and 22 par t ia l responses (48.9%). Pat ients to lerated the t reatment wel l ,
a l though f ive pat ients developed thromboembol ic compl icat ions (11%).
Baz et al . (456) t reated 16 pat ients wi th h igh-r isk , newly d iagnosed myeloma or
re lapsed/ref rac tory d isease wi th arsenic t r ioxide, ascorbic ac id, tha l idomide, and
dexamethasone. Four pat ients ach ieved a par t ia l response, and the PFS was 9.4 months.
Nineteen percent o f pat ients had thromboembol ic events.
Bortezomib as Induction Therapy Thi r ty-e ight to 40% of newly d iagnosed myeloma pat ients respond to s ing le-agent
bor tezomib (324,457) . The addi t ion of dexamethasone resul ts in an overa l l response rate of
67 to 88% (324,458) . A number o f combinat ions have been explored for induct ion.
Mateos et a l . (459) reported on thei r Phase I / I I resu l ts wi th VMP, bor tezomib, melphalan,
and prednisone, in 60 e lder ly pat ients not deemed to be HSCT candidates. Pat ients were
t reated wi th four 6-week cyc les fo l lowed by f ive 5-week cycles . The f ina l dose schedule was
bor tezomib (1 .3 mg/m 2 on days 1, 4 , 8 , 11, 22, 25, 29, and 32), melphalan (9 mg/m 2 on days
1 to 4) , and prednisone (60 mg/m 2 da i ly on days 1 to 4) . The authors exc luded the three
ear ly deaths and four o ther ear ly wi thdrawals f rom the i r response analys is and report the
fo l lowing response rates: overal l response rate 88% (32% CR, 11% VGPR, and 45% PR).
The 16-month event-f ree survival and overa l l surviva l were 83 and 90%, respect ive ly. The
most common adverse events were myelosuppression (>90%), infec t ion (75%), as thenia
(63%), gast ro in tes t inal toxic i ty (>55%), and per iphera l neuropathy (55%). The most common
grade 3–4 toxic i t ies were thrombocytopenia (51%)and neutropenia (43%), peripheral
neuropathy (17%), and diarrhea (16%). Pat ients who were >75 years of age were more
prone to the more ser ious nonhematologic s ide effects (459) .
Oakervee et a l . (460) have t reated 21 previous ly unt reated pat ients wi th PAD (bor tezomib,
doxorubic in, and dexamethasone). Pat ients rece ived four 21-day cycles of bor tezomib 1.3
mg/m 2 on days 1,4, 8, and 11; dexamethasone 40 mg on days 1 to 4 and 15 to 18; and
doxorubic in a t escalat ing doses of 4 .5 or 9 mg/m 2 /day as a cont inuous in t ravenous in fusion
over 4 days. Ninety- f ive percent o f pat ients ach ieved at least a par t ia l response, inc lud ing a
CR in 24% of pat ients. Fi f teen grade 3–4 adverse events occurred in 12 pat ients , wi th the
most common serious adverse events (SAE) includ ing in fec t ions (n = 7) and shing les (n = 3).

Grade 3–4 peripheral neuropathy, postura l hypotension, nausea and vomit ing, at r ia l
f ib r i l la t ion, and hyperglycemia each occurred in one pat ient . Al l but one pat ient proceeded
to stem cel l co l lec t ion and t ransplantat ion. Al though no cardiac toxic i ty was observed,
cardiac biomarker screening for subt le toxic i t ies were not per formed.
Popat e t a l . (461) t reated 19 pat ients wi th previous ly unt reated myeloma wi th four cycles of
LD-PAD (bor tezomib 1 mg/m 2 on days 1, 4 , 8 , and 11; doxorubic in 9 mg/m 2 by in t ravenous
in fus ion on days 1–4, and dexamethasone 40 mg on days 1 to 4 , 9 to 12, and 17 to 20 for
cyc le 1—subsequent courses on ly days 1 to 4) . Th is program d i f fers f rom that o f Oakervee
in that the dose of bor tezomib was reduced by about 25%. Eighteen pat ients were evaluable,
wi th an overa l l response rate of 89% (2 CR. 1 nCR, 4 VGPR, 9 PR). Al l pat ients
successful ly mobi l ized s tem cel ls . Toxic i ty in format ion was not provided.
Wang et a l . (462) t reated 36 previous ly unt reated pat ients wi th VTD ( tha l idomide 50 to 200
mg/day; bor tezomib 1.3 to 1 .9 mg/m 2 days 1, 4 , 8, and 11; and dexamethasone 20 mg on
days 1 to 4 , 9 to 12, and 17 to 20) . Al l pat ients received fu l l ant icoagulat ion. Overal l
response rate was 92%, includ ing a 19% CR rate. There did not appear to be any va lue
added wi th bor tezomib doses >1.3 mg/m2 .
In a Phase I / I I t r ia l , Badros et al . (463) combined escalat ing doses of bor tezomib wi th the
DT-PACE reg imen (dexamethasone, thal idomide, c isplat in , doxorubic in , cyc lophosphamide,
and etopos ide) . Four pat ients had no pr ior therapy, and seven had one prior cycle inc lud ing
DT (n = 4) and DT-PACE (n = 3) . Stem cel ls were col lec ted at a median of 13 days (range
12 to 15 days) in to the cyc le , y ie ld ing a median of 20.6 × 106 CD 34+ s tem cel ls /kg ( range
7.8 to 33.3 × 106 ) . A l l 11 pat ients responded, wi th two CR/nCRs. Grade 3–4 hematologic
toxic i ty, including neutropenic fever requi r ing hospi tal izat ion, was common. There were
three DVTs (despi te enoxapar in) , s ign i f icant ep isodes of hypotens ion, including syncope in
two, and two pat ients wi th grade 3 diarrhea.
Lenalidomide as Induction Therapy In previous ly unt reated pat ients wi th ac t ive myeloma, the combinat ion of lenal idomide and
dexamethasone wi th and wi thout c lar i thromycin y ie lds overa l l response rates of 91 to 95%,
wi th complete response/very good response rates of 32 to 38% (439,464). Rajkumar et a l .
(439) t reated 34 pat ients wi th lenal idomide 25 mg oral ly on days 1 to 21 and
dexamethasone 40 mg on days 1 to 4 , 9 to 12, and 17 to 20, both repeated every 28 days.
Aspir in was g iven as DVT prophylaxis . The overal l response rate was 91%, wi th 6%
achieving a complete response and 32% a very good par t ia l response. Grade 3–4
neutropenia occurred in 12% of pat ients . Forty-seven percent o f pat ients exper ienced grade
3 or h igher nonhemato log ic toxic i ty, most commonly fa t igue (15%). Six percent each had
grade 3–4 muscle weakness, anxie ty, pneumoni t is , or rash.
Niesvizky et al . (465) t reated 40 pat ients wi th c lar i thromycin, lenal idomide, and
dexamethasone. The rat ionale for the c lar i thromycin use is that i t a l ters the hepat ic
metabol ism of both drugs, resul t ing in h igher e ffect ive doses. The lenal idomide schedule
was as above, but dexamethasone was adminis tered only once week ly. Clar i thromycin was
g iven in doses of 500 mg twice dai ly. Aspir in was given as DVT prophylaxis . Pre l iminary
resul ts include a 95% response rate, inc lud ing 25% CR and 18% VGPR. For ty-e ight
P.2393
percent o f pat ients developed grade 3 or higher adverse events , inc luding 15% wi th

thromboembol ism, two of which were fa tal . Four of the seven thromboembol isms occurred in
pat ients who had d iscont inued aspi r in .
Risk fac tors for thromboembol ism in pat ients rece iv ing IMiDs include dexamethasone
in tensi ty, erythropoiet in , and other concomi tant chemotherapy (440,442)
Hematopoietic Stem Cell Transplantation
Autologous Transplant To overcome res is tance of the myeloma ce l ls to convent ional -dose chemotherapy, McElwain
and Powles (237) pioneered the use of high-dose melphalan to t reat mul t ip le myeloma and
p lasma ce l l leukemia. The t reatment was compl icated by pro longed myelosuppression.
Bar log ie e t a l . (466) subsequent ly used a regimen combining high-dose melphalan wi th
to tal -body i r rad ia t ion supported by auto logous bone marrow t ransplantat ion in mult ip le
myeloma pat ients re frac tory to VAD. Ten years later , At tal e t a l . publ ished the f i rs t
prospect ive randomized contro l led t r ia l demonstrat ing an improved overal l surviva l for
pat ients undergoing high-dose therapy wi th autologous s tem cel l support compared to
convent ional chemotherapy (245) .
Al though high-dose therapy fol lowed by auto logous s tem cel l t ransplantat ion (ASCT) is not
curat ive, i t improves event- f ree and overal l surviva l (Table 99.10) (245,467,468) Three of
the four “negat ive” s tud ies (469,470,471) are largely “ear ly” versus “de layed” t ransplant
t r ia ls , and the fourth “negat ive” study exc luded f rom randomizat ion those pat ients who did
not respond to induct ion therapy (472) . Response rates wi th ASCT are 75% to 90%, and
complete response rates are 20 to 40% (245,467,468,469,470,471,472) . Antedat ing these
randomized control led t r ia ls, his tor ical comparisons a lso showed conf l ic t ing resul ts . For
example, one histor ical compar ison study from Spain suggested that surviva l in good-r isk
pat ients rece iv ing on ly convent ional chemotherapy was s imi lar to that repor ted in se lected
ser ies of pat ients t reated wi th ASCT (473) . In contrast , the Nordic Myeloma Study Group
(474) prospect ive ly eva luated the ef fec t o f ASCT on survival in myeloma pat ients younger
than age 60 years and compared the surviva l ra tes of t ransplanted pat ients wi th those of
h istor ic controls derived f rom previous Nord ic populat ion-based s tud ies of convent ional -
dose chemotherapy. They found that survival was prolonged wi th the high-dose therapy—44
months for convent ional chemotherapy versus >60 months for pat ients t reated wi th ASCT.
Table 99.10 Conventional Chemotherpay (CCT) versus Single Autologous Hematopoietic Stem Cell Transplantation (ASCT); Randomized Trials

CR/VGPR (%) ORR (%) PFS (mo) OS (mo) SCT (%) N CCT ASCT CCT ASCT CCT ASCT CCT ASCT CCT ASC
T
IFM90 (245,475)
200
13
38a
57
81a
18
28a
44
57a
9 74
MRC7 (467)
401
8 44a
46
86a
19.6
31.6a
42
54a
15
75
MAG91 (469)
190
4 6 56
59
18.7
25.3a
47.6
47.8
22
75
MAG90 (470)
185
57
20
58
78
13
39 64
65 78
98
PEETHMA (472)
164
11
30a
83
82
33
42 61
66 18
90
S9321 (471)
516
17
15
90
93
7 y, 14%
7 y, 17%
7 y, 38%
7 y, 38%
34
82
MMSGb (468)
194
6 25a
66
72
16
28a
42
58+a
39
92
HOVON-24c (477)
303
13
28a
86
90
23
24a
50
55 — —
CR/VGPR, complete response or very good partial response; ORR, any response

greater than or equal to a partial response; PFS, progression-free survival; OS, overall survival; SCT, patients known to receive an autologous hematopoietic stem cell transplant. aSignificant. bTransplant arm is two low-dose (melphalan 100 mg/m2) autologous stem cell transplants. cOften included in “double-transplant” tables because both arms received melphalan 70 mg/m2 × 2 without stem cell support as induction therapy.
Figure 99.10. Conventional chemotherapy versus autologous hematopoietic stem cell transplantation, IFM 90 Trial. (With permission, from Attal M, Harousseau JL, Stoppa AM, et al. A prospective, randomized trial of autologous bone marrow transplantation and chemotherapy in multiple myeloma. Intergroupe Francais du Myelome. N Engl J Med 1996;335:91–97. Copyright © 1996 Massachusetts Medical Society. All rights reserved.)
As shown in Table 99.10, the Intergroupe Français du Myélome (245) publ ished the f i rs t
randomized tr ia l comparing high-dose chemotherapy fol lowed by auto logous bone marrow
t ransplantat ion wi th convent ional chemotherapy (F ig. 99.10). Two hundred pat ients wi th
previously unt reated mult ip le myeloma were randomized to receive ASCT or combinat ion
chemotherapy (CCT). The 5-year event- f ree surviva l (28 vs . 10%) and overa l l surviva l ra tes
(52 vs . 12%) were h igher in the t ransplantat ion group. An updated analys is wi th a median

fo l low-up of 7 years conf i rmed that h igh-dose chemotherapy improves event- f ree surviva l
(median, 28 vs . 18 months) as wel l as overa l l surviva l (median, 57 vs . 44 months) (475).
The Medica l Research Counc i l VI I t r ia l was the second publ ished s tudy addressing the
quest ion of CCT versus ASCT (467) . Th is tr ia l inc luded 401 randomized pat ients . The t r ia l
found that the complete response rates (8 vs . 44%), the median event- f ree surviva l (19 vs .
31 months) , and the overa l l surviva l (42 vs. 54 months)
P.2394
a l l s igni f icant ly favored the ASCT arm, even though only 75% of the pat ients ass igned to
the transplant group actua l ly rece ived i t and 15% of pat ients in CCT arm received salvage
ASCT.
Three t r ia ls addressed the “ear ly” versus “de layed” t ransplant s t ra tegy (469,470,471) . The
f i rst was the MAG90 t r ia l , in which Fermand et al . demonstrated that among the 185
pat ients randomized to ei ther ear ly or late ASCT, the overal l survival in both groups was 64
months, and the percentages of the respect ive groups actua l ly rece iv ing ASCT were 98 and
78%, respect ive ly (470) . Th is t r ia l was important because i t gave pat ients and physic ians
l icense to opt for t ransplants ei ther up- f ront or on a de layed bas is . Most chose to t ransplant
ear ly, because the t ime wi thout systemic therapy (TW iST) was longer in the ear ly than the
de layed ASCT group, potent ia l ly provid ing better qual i ty o f l i fe for the early- t ransplant
group. The MAG91 t r ia l (469) randomized 190 pat ients under the age of 56 years to CCT or
HSCT, but this t r ia l a lso examined the outcomes of ear ly versus la te t ransplants. Only
pat ients 55 to 65 years of age were included. Event- f ree surviva l (19 vs . 25 months) , but
not overa l l survival (47.6 vs . 47.8 months) , was bet ter in the ASCT arm. Despi te the 120-
month fo l low up, the overa l l surviva l s tat is t ics are confounded by the fac t that only 75% of
the “ASCT” arm received ASCT, and that 22% of the “CCT” arm received an HSCT. The
in tergroup t r ia l (S9321) randomized 510 pat ients age 70 or younger to CCT or HSCT (471) .
W ith a 76-month fo l low-up, 7-year overa l l surviva l was no d i f ferent between the arms;
however on ly 82% of the “ASCT” group received an ASCT and 34% of the “CCT” group
received an ASCT. Remarkably, 7 years af ter a myeloma d iagnosis, 38% of pat ients were
s t i l l a l ive.
The Spanish Cooperat ive Group prospect ive t r ia l was d issimi lar f rom the other randomized
t r ia ls in that on ly those pat ients who responded to therapy were randomized. At enro l lment,
216 pat ients were t reated ini t ia l ly wi th four cyc les of VBMCP and VBAD (vincr is t ine,
carmust ine, doxorubic in , and dexamethasone) (472) , and only 164 were randomized to
receive eight addi t ional courses of chemotherapy or intens i f icat ion wi th h igh-dose therapy
and s tem cel l t ransplantat ion. There was no di f ference between the groups wi th respect to
complete response rates, overal l response rates, progression-f ree survival , or overal l
surviva l . These data d i f fer f rom those of o ther t ransplant t r ia ls. I t is possib le that pat ients
wi th an excel lent response to the induct ion therapy g iven do not requi re consol idat ion wi th
ASCT; or that wi th longer fo l low-up, survival di f ferences wi l l emerge.
The MMSG97 t r ia l was un ique in that i t randomized pat ients aged 50 to 70 years of age to
e i ther melphalan and prednisone or two hal f -dose melphalan t ransplants (468) . Pat ients
receiv ing melphalan and prednisone only had sign i f icant ly worse outcomes. A s igni f icant
d i f ference between two low-dose ASCT and MP was not seen in the IFM 999-06 tr ia l (476).

The Hovon-24 t r ia l is commonly grouped in the “s ing le versus double” transplant category,
though i t is actual ly an “ in tens i f ied chemotherapy wi thout t ransplant” versus “ in tens i f ied
chemotherapy fo l lowed by h igh-dose chemotherapy and a s ing le ASCT” (477) . The most
recent analys is o f th is t r ia l demonstrates a s igni f icant ly higher complete response rate and
event- f ree survival in the h igh-dose t reatment arm. The d i f ferences in event- f ree survival ,
progress ion- f ree survival , and tota l t ime to progression were not seen unt i l the 4-year fol low
up had been reached. The authors repor t that the lack of d i f ference in overa l l surviva l is
l ike ly due to a “high propor t ion” o f pat ients f rom the contro l arm receiv ing HSCT at f i rs t
re lapse.
Table 99.11 Single versus Double Hematopoietic Stem Cell Transplantation, Randomized Trials
Event-Free Survival (mo) Overall Survival (%) Study N FU (mo) Single Double P Single Double P
IFM, 94 (481)
403
75 25 30 .03 48 58 .01
Bologna, 96 (482)
228
~48
21 31 .001
44% at 6 y
63% at 6 y
NS
MAG, 95 (1093)
193
27 41 events
43 events
NS 27 deaths
22 deaths
NS
Single versus Double Transplantation
As the evidence was mount ing that one course of dose-in tens i f ied chemotherapy wi th ASCT
was super ior to convent ional chemotherapy, invest igators began exper iment ing wi th two
consecut ive ASCTs. The concept o f double or tandem t ransplants was promulgated by Dr.
Bar log ie and co l leagues at the Universi ty of Arkansas (331,478,479,480) . These
invest igators repor ted high complete response rates and surviva l (331,478,479,480) . In the
f i rst repor t o f “ to ta l therapy 1, ” which included 231 pat ients wi th newly d iagnosed myeloma,
the overa l l survival wi th th is approach was 68 months (331) .
There have been prel iminary data f rom three randomized t r ia ls that indicate increased
response rates wi th tandem transplantat ion, but on ly two that demonstrate improvement in
event- f ree and overa l l surviva l (481,482,483) (Table 99.11) . In the largest and most mature
s tudy, that is , the IFM 94 s tudy, there was no di f ference in event- f ree or overa l l surviva l
between double and s ingle autologous s tem cel l t ransplants af ter 2 years of fo l low-up (484) ;
however, by 4 years and beyond, a surviva l benef i t was detected (481) . Though the
response rate was not s ign i f icant ly d i f ferent between the two groups (complete response
and very good par t ia l response 42% in the s ing le-t ransplant arm vs. 50% in the double-
t ransplant group, p = .15) , both event- free surviva l (25 vs. 30 months) and overal l surviva l
(48 vs . 58 months) were improved in the double- transplant arm. The respect ive 7-year

overa l l (21 vs . 42%) and event-f ree surviva l ra tes (10 vs . 20%) also s ign i f icant ly favored the
double-t ransplant group (F ig . 99.11). In this t r ia l , four fac tors were assoc ia ted wi th a longer
surviva l : low β2 -microg lobul in leve ls a t diagnos is (p < .01), young age (p < .05) , low lactate
dehydrogenase (LDH) at d iagnosis (p < .01) , and the t reatment arm to which the pat ient was
ass igned (p < .05) . W hen the authors d id an unplanned subgroup analysis , they found that
pat ients who benef i ted most f rom the tandem t ransplant were those who d id not achieve a
very good part ia l response or bet ter a fter thei r f i rs t t ransplant .
Cavo et a l . (482) have made s imi lar observat ions based on prel iminary data, includ ing the
benef i t o f a second t ransplant be ing l imi ted to those pat ients who do not ach ieve a very
good par t ia l response or bet ter a f ter the i r f i rs t t ransplant . Most pat ients under the age of 65
years should have enough s tem cel ls col lec ted for a t least two t ransplants.
Timing of Transplantation
As long as stem cel ls are co l lected early, in the context o f convent ional chemotherapy
versus as s ing le autologous s tem cel l t ransplant , t iming of t ransplant—ei ther as upfront
consol idat ion or salvage at relapse—does not inf luence overal l survival (469,470,471) .
P.2395
Because the t ime wi thout chemotherapy is longer in pat ients t ransplanted ear ly in thei r
course, many opt for early t ransplant . The s i tuat ion is less c lear when one int roduces the
concept of double t ransplants , as the relevant data are not yet ava i lable . Many phys ic ians
are act ing on the reasonable premise that t iming of double t ransplants does not mat ter, but
a l l three tandem t ransplant t r ia ls eva luated ear ly, “back to back” t ransplants . There are
emerg ing data—but no randomized t r ia ls—regarding the role a second t ransplant plays as
“sa lvage” therapy af ter re lapse f rom the f i rs t . A l l that can be conc luded f rom these
re t rospect ive analyses is that a second salvage ASCT is a feas ib le opt ion in some pat ients .
Figure 99.11. Single autologous versus double hematopoietic stem cell transplantation, IFM 94 trial. A: Event-free survival. B: Overall survival. (With permission, from Attal M,

Harousseau JL, Facon T, et al. Single versus double autologous stem-cell transplantation for multiple myeloma. N Engl J Med 2003;349: 2495–2502. Copyright ©2003 Massachusetts Medical Society. All rights reserved.)
The European Group for Blood and Marrow Transplantat ion Regist ry (EBMTR) analyzed
“p lanned” and “unplanned” second t ransplants among 7,444 pat ients spanning 9 years .
Though the surviva l was shorter a f ter the second t ransplant in the group that had the
“unplanned” and presumably de layed t ransplant , the overa l l survival o f both groups f rom the
t ime of the f i rst t ransplant was s imi lar : 60 months for the planned group and 51 months for
the unplanned group (485) .
Alvares et a l . studied retrospect ive ly the outcomes of 172 pat ients who re lapsed af ter a
s ing le autologous ASCT (486). Eighty- three had a second ASCT at relapse, 7 d ied, and
another 83 had al ternat ive therapies. The median event- f ree surviva l was simi lar in the two
groups at 1 .3 years versus 0.9 years (p = .73) , but there was a t rend toward longer overal l
surviva l in the second t ransplant group (2.9 vs . 1.7 years , p = .07) . The authors caut ioned
that the worse outcome in the la t ter group could potent ia l ly be accounted for by a poorer
per formance s tatus in the group not receiv ing a second t ransplant . Most notable , however,
was the d i f ference in overa l l surviva l between those pat ients who had less than an 18-
month re lapse- f ree surviva l a f ter thei r f i rst t ransplant relat ive to those who had a relapse-
f ree survival of 18 months or longer : The respect ive median overa l l surviva ls were <6
months in the former and near ly 3 years in the lat ter group (p < .00001).
El l ice et a l . (487) analyzed the outcomes of 26 pat ients who had a second t ransplant upon
re lapse after a s ing le t ransplant . From the date of re lapse, the overa l l surviva l o f pat ients
undergoing second t ransplant was 46.9 months, whereas that o f the pat ients rece iv ing
a l ternate sa lvage therapy was 28.3 months. The median overa l l surviva l and event- f ree
surviva l ca lcu la ted f rom the date of second ASCT were 38.1 and 14.8 months, respect ive ly.
Given the smal l numbers of pat ients , the di f ference between the two groups was not
cons idered to be s ta t ist ica l ly s igni f icant .
Mehta et al . repor ted on 42 pat ients a l lograf ted for myeloma af ter not responding to or a f ter
having had progress ion fo l lowing autologous s tem cel l t ransplantat ion (488) . They
compared those cases to 42 pa i r-matched contro ls that underwent sa lvage auto logous stem
cel l t ransplantat ion. The 3-year event- f ree surviva l was simi lar for both groups (20 vs . 25%),
but overa l l survival was s ign i f icant ly h igher a fter autologous t ransplantat ion (29 vs . 54%).
Al though the 3-year probabi l i ty of disease progression was lower af ter a l logeneic
t ransplantat ion (31 vs . 72%), the d i f ference could be at tr ibuted to the high 1-year t reatment-
re lated mortal i ty of 43% in the a l logeneic group. Lee et a l . (489) has shown that pat ients
re lapsing af ter two t ransplants may derive benef i t f rom a thi rd t ransplant as long as they
have favorable prognost ic fac tors.
Long-Term Survival in Myeloma Patients
High-dose chemotherapy wi th auto logous s tem cel l t ransplantat ion has improved outcomes
in pat ients wi th myeloma. Mere ly be ing e l ig ib le for t ransplant is i tse l f a favorable prognost ic
fac tor . In one s tudy, on ly 50% of pat ients who were of t ransplant-el ig ible age were actual ly
t ransplanted. The reasons for not t ransplant ing the other pat ients were poor medica l
condi t ion (25%) and unspeci f ied reasons (25%). Despi te the caveat o f selec t ion,

unprecedented long-term survivals are being seen in populat ions of t ransplanted pat ients .
Moreau et a l . (490) repor ted a 10-year surviva l of 9% percent in pat ients wi th β2 -
microglobul in o f >3 mg/L, compared to 41% for pat ients wi th β2 -microg lobul in o f ≤3 mg/L.
These same groups had median overa l l surviva ls o f 31 versus 73 months. More than one
th i rd o f the pat ients <55 years at diagnos is were a l ive at 10 years . In this re t rospect ive
analys is , the 10-year surviva l was 35% for pat ients who completed a second ASCT,
compared to 20% for those who had only one.
Though long- term surviva l was the focus of the previous paper, 20 to 30% 8-year survivors
have been descr ibed in o ther cohorts (471,491) .
Transplantation for Primary Refractory Myeloma In contrast to the exper ience wi th mal ignant lymphoma, s tem cel l t ransplantat ion appears to
be ef fec t ive for pat ients wi th pr imary res is tant d isease (492,493,494) . Pat ients wi th mul t ip le
myeloma, in whom f i rs t - l ine therapy such as VAD fa i ls , can be sens i t ive to h igh-dose
chemotherapy wi th s tem cel l reconst i tu t ion. Alexanian et a l . (492) repor ted a decrease of
75% in tumor burden in 56% of pat ients and a marked improvement in surviva l compared
wi th matched h is tor ica l controls. Kumar et a l . (494) also looked at s tem ce l l t ransplantat ion
in pr imary ref rac tory d isease and found that though there was a lower complete response
rate (20 vs . 35%) in the pr imary ref rac tory pat ients , the 1-year progress ion- f ree surviva l
was s imi lar to that o f pat ients wi th chemosens i t ive d isease.
Hematopoietic Stem Cell Collection Auto logous per iphera l b lood s tem cel l t ransplantat ion has replaced autologous bone marrow
t ransplantat ion because engraf tment is
P.2396
more rap id and there is less contaminat ion wi th myeloma ce l ls (495,496,497) .
Hematopoiet ic stem ce l ls should be col lected before the pat ient is exposed to alkyla t ing
agents (498,499) , because pro longed melphalan exposure leads to an impai red harvest of
per iphera l b lood s tem cel ls when s tem cel ls are mobi l ized wi th chemotherapy p lus growth
fac tors (500) or growth fac tors a lone (501) . Even af ter four to s ix cyc les of VMCP/VBAP,
which is a reg imen contain ing low doses of melphalan, suf f ic ient s tem cel ls could not be
co l lec ted for t ransplantat ion in ~10% of pat ients (245) . In contrast, successful stem ce l l
co l lec t ion is ach ieved in 95 to 100% of mul t ip le myeloma pat ients treated wi th VAD before
mobi l izat ion wi th h igh-dose cyc lophosphamide (474) . The absolute number o f CD34+
ce l ls/kg is the most re l iab le and pract ica l method for determin ing the adequacy of a s tem
cel l co l lec t ion.
There are many opt ions for mobi l iz ing regimens, f rom single-agent granulocyte colony-
s t imulat ing fac tor (G-CSF) (501) to pegylated G-CSF (502) , to an assor tment o f
chemotherapy-plus-growth fac tor reg imens (503,504,505,506,507). In general ,
chemotherapy mobi l izat ion resul ts in higher CD34 yie lds (503,508,509) . Chemotherapy
mobi l izat ion has been assoc iated wi th lower tumor contaminat ion of the stem cel l product
(503,509) , but no surviva l benef i t has been demonstrated (510) . The CXCR4-antagonis t
AMD3100 has not yet been approved by the U.S. Food and Drug Admin is t ra t ion, but i t has
a l ready shown eff icacy in c l in ica l t r ia ls (511) .

Autologous Hematopoietic Stem Cell Transplantation in Special
Populations
The morta l i ty rate from auto logous stem cel l t ransplantat ion is current ly <5%. Age >65
years a lone is not a contra ind icat ion for t ransplantat ion, al though there are no randomized
data proving or d isproving i ts ut i l i ty in th is age group. Such pat ients are candidates for
t ransplantat ion i f they have good funct ional sta tus and l imi ted comorb idi t ies (512,513) .
Pat ients wi th renal fa i lure, including dia lys is pat ients , can successfu l ly undergo HSCT wi th
melphalan 140 mg/m 2 , wi th s imi lar response rates and progression- f ree surviva l , and a
propor t ion wi l l even have reversal o f the i r renal fa i lure. Treatment- re la ted morb idi ty is
h igher (514) , and thei r overa l l surviva l is in fer ior to that o f thei r dialys is - independent
counterpar ts (515,516) .
Conditioning Therapy and Stem Cell Transplantation
In an effor t to improve auto logous stem cel l t ransplantat ion, var ious preparat ive reg imens
have been used. There has been only one prospect ive randomized contro l led t r ia l
comparing condi t ioning reg imens in pat ients wi th myeloma (517) . Moreau et al . (517)
randomized 282 pat ients to rece ive e i ther melphalan (140 mg/m 2 ) p lus to ta l -body i r radia t ion
or melphalan a lone (200 mg/m 2 ) . There was no d i f ference in response rates or event- f ree
surviva l . Survival at 45 months favored the melphalan-alone arm (65.8 vs. 45.5%, p = .05) .
Toxic i ty wi th melphalan a lone was s ign i f icant ly less . Most invest igators have now
d iscont inued the use of to ta l-body i r rad ia t ion and g ive on ly melphalan (200 mg/m2 ) as the
preparat ive reg imen.
Other reg imens inc lud ing var ious combinat ions of melphalan, busul fan, cyc lophosphamide,
idarubic in , e topos ide, and/or th io tepa have been used (518,519,520,521,522,523) , wi thout
any evidence of super ior i ty o f these regimens over melphalan 200 mg/m 2 , and severa l wi th
s ign i f icant ly more toxic i ty (519,520) and morb idi ty (518) . Innovat ive t r ia ls supplementing
melphalan wi th ske leta l targeted radia t ion [samarium 153-ethylenediaminetet ramethylene
phosphonate (524) and holmium 166-1,4,7,10- te t raazocyclodo-decane-1,4,7, 10-
te t ramethylenephosphonic acid (525) ] have been reported. Others have been s tudying
bor tezomib as a chemosensi t izer for the melphalan (526,527,528) .
Des ikan et a l . ret rospect ive ly compared the ef fect o f d i f ferent condit ion ing regimens used
for the second autologous t ransplant (529) . Outcomes of pat ients t reated wi th melphalan
200 mg/m 2 were bet ter than those condi t ioned wi th melphalan 200 mg/m 2 p lus
cyc lophosphamide 120 mg/m 2 , and melphalan 140 mg/m 2 p lus to ta l -body i r rad iat ion (1 ,125
cGy).
The Role of Purging Vir tua l ly a l l per iphera l b lood cel l products are contaminated wi th mal ignant ce l ls (530,531) .
I t is unclear whether the purging of tumor cel ls f rom the col lec t ion of hematopoiet ic s tem
ce l ls is benef ic ial . Purging marrow wi th cyc lophosphamide der ivat ives (532) or wi th
monoclonal ant ibodies (533,534,535) is feas ib le a l though assoc iated wi th prolonged
myelosuppress ion af ter transplantat ion. CD34+ se lec t ion of per iphera l blood progenitor cel ls
provided ef fec t ive hematopoiet ic support in a group of 55 pat ients wi th advanced mult ip le
myeloma af ter myeloablat ive chemotherapy (536) . However, one large Phase I I I randomized
t r ia l has shown no c l in ica l benef i t to using CD34+ -se lected auto logous per ipheral blood

stem cel ls (537) . Another randomized t r ia l showed an increased rate of infec t ion wi thout
improvement in overal l surviva l (538).
Ear ly work shows that f lowing hematopoiet ic ce l ls through pulsed elec t r ic f ie lds ef fec t ively
purges myeloma ce l ls wi thout sacri f ic ing funct ional s tem ce l ls (539) . This f inding has not
yet made i t in to the c l in ic .
Allogeneic Transplant Al logeneic t ransplantat ion e l iminates the problem of s tem cel l contaminat ion by tumor ce l ls
that is inevi tab le wi th auto logous s tem cel l t ransplantat ion. Fur ther , there is evidence of a
graf t -versus-myeloma effec t wi th a l lograft ing (540). Al logeneic s tem cel l t ransplantat ion
(a l logeneic SCT) can lead to complete response rates of 22 to 67%, including molecular
remiss ions in about one th i rd (495,541,542) , and pro longed d isease- f ree surviva l in
approximately one quar ter to one th i rd o f pat ients (471,495,543) (Table 99.12). The h igh
t reatment- related mortal i ty (10 to 63%) and sign i f icant toxic i ty f rom graf t -versus-host
d isease have l imi ted the ro le o f th is procedure in the treatment o f myeloma (495,544,545) .
Though there are no prospect ive randomized t r ia ls compar ing condi t ion ing regimens in
pat ients rece iv ing al logeneic t ransplants , one retrospect ive mul t icenter analysis o f 139
pat ients undergoing myeloablat ive condit ion ing showed bet ter outcomes in pat ients
receiv ing melphalan/ total -body i r rad ia t ion (TBI) compared to cyclophosphamide/TBI ,
includ ing higher CR rates (65 vs . 47%, p = .085) , lower relapse ra tes (37 vs . 81%, p
< .0001), and longer 5-year overa l l surviva l (44 vs. 28%, p = .06) (546).
A smal l s ing le-center study of 37 myeloma pat ients who underwent myeloablat ive a l logeneic
SCT, but that had a median fo l low-up of 108 months, repor ted that the pat ients ' 5-year
overa l l surviva l , progress ion- f ree survival , and event- f ree surviva l were 40, 54, and 24%,
respect ive ly (547) , despi te a 50% t reatment- rela ted morta l i ty and a median overal l surviva l
o f 28 months. At 10 years , about 30% of the pat ients were al ive. Outcomes were s imi lar for
the a l logeneic t reatment arm in the S9321 In tergroup s tudy (471) .
In another series , on ly 5 o f 80 pat ients were a l ive wi thout evidence of d isease at 4 to 7
years af ter an al logeneic bone marrow t ransplant for mult ip le myeloma (495) . I t must be
emphas ized that the major i ty of these pat ients had chemotherapy-resistant d isease before
t ransplantat ion. Outcomes for a l logeneic SCT have improved over t ime (548) . Of 690
a l logeneic , matched, s ibl ing donor transplants for mul t ip le myeloma repor ted to the
European Group for Blood and Marrow Transplantat ion reg is t ry, 334 were per formed
between 1983 and 1993 (a l l wi th bone marrow) and 356 between 1994 and 1998. The 3-year
overa l l surviva l was 35% for transplant rec ip ients during the ear l ier per iod and 55% for
rec ip ients of bone marrow t ransplants during the la ter per iod. The improvement in survival
s ince 1994 was the resu l t o f a s ign i f icant reduct ion in t ransplant- re lated mortal i ty , f rom 46
to 30% at 2 years (548).
P.2397
Table 99.12 Nonrandomized Comparisons of Autologous and Allogeneic Hematopoietic Stem Cell Transplantation for Multiple Myeloma

Study N TRM (%)
PFS (mo) P OS (mo) P
189 Auto
13 ~22 NS 34 .001 Bjorkstrand et al. (549)
189 Allo
41 ~12 18
24 Auto 12 16.7 NS 33.5 NS Varterasian et al. (550)
24 Allo 25 31 38.6
40 Auto 5 14 — >48 <.001 Couban et al. (551)
22 Allo 27 ~11 7
Auto 35 6 2 y, 30%
NS 2 y, 42%
NS Reynolds et al. (553)
Allo 21 19 2 y, 60%
2 y, 60%
50 Autoa
6 3 y, 67%
NS 3 y, 82%
NS Lokhorst et al. (552)
11 Alloa,b
18 3 y, 67%
3 y, 82%
2 y, 48%
.002 2 y, 74%
.006 166 Auto
13
4 y, 28%
NS 4 y, 41%
NS
Alyea et al. (554)
66 Allo b
24 2 y, 23%
2 y, 51%

4 y, 18%
4 y, 39%
1 y, 67%
NS 1 y, 86%
NS 70 Autoc
6
4 y, 18%
NS 4 y, 50%
NS
1 y, 58%
1 y, 64%
Arora et al. (555)
17 Allo 31
4 y, 32%
4 y, 64%
MS, median survial; NS, not significant; TRM, treatment-related mortality. aChemotherapy-sensitive patients only. bT-cell–depleted allogeneic stem cells. cCyclphosphamide and total-body irradiation conditioning.
Al logeneic t ransplants produce h igher ra tes of complete molecular responses. In a ser ies of
229 myeloma pat ients , al logeneic t ransplants resu l ted in a complete response of 38%,
compared wi th 22% af ter auto logous t ransplantat ion (p < .01) (541) . Among pat ients
achieving a c l in ica l complete response, 50% of the al logeneic t ransplant group had a
molecular complete response, compared wi th only 17% of those who had received an
autologous t ransplant (541) . The median re lapse- f ree survival for those who had a
molecular complete remission was 110 months, compared wi th 35 months for those who d id
not . Moreover, in those wi th a complete molecular remission, the re lapse ra te was only 16%
in the a l logeneic group and 41% in the auto logous group. Th is is s t rong evidence that
molecular complete responses are assoc ia ted wi th a longer re lapse- free surviva l .
There have been seven case-contro l or cohor t-control s tud ies compar ing auto logous to
a l logeneic s tem cel l t ransplants (Table 99.12) (549,550,551,552,553,554,555) . The largest
o f these was by Bjorkst rand et a l . (549) . In thei r re t rospect ive analys is o f data compi led by
the European Blood and Marrow Transplantat ion Group, there was in fer ior survival for
myeloma pat ients t reated wi th al logeneic bone marrow t ransplants compared to case-
matched controls t reated wi th auto logous t ransplants (18 vs . 36 months) (549). The s ix
smal ler s tud ies , which had rela t ive ly shor t fo l low-up, showed mixed resul ts wi th regard to
progress ion- f ree survival and overal l surviva l ; t ransplant- rela ted morta l i ty, however, was
cons is tent ly h igher in the a l logeneic groups (19 to 25%).
Only one repor t favored a l logeneic t ransplantat ion (555) . However, pat ients in the
a l logeneic group were bet ter-prognos is pat ients ; they were s ign i f icant ly younger and less

l i ke ly to have IgA myeloma. Though not reaching s tat is t ical s ign i f icance, there were more
autologous pat ients having the i r t ransplant as sa lvage (37 vs . 23%). In addi t ion,
cyc lophosphamide and to ta l-body i r rad ia t ion were used to condi t ion both the auto logous and
a l logeneic t ransplant pat ients . W ith fo l low-up t imes for the two groups of 24 and 43 months,
respect ive ly, the 1-year overa l l surviva l was 86 and 64%, and the 4-year OS was 50 and
64%.
Two of these studies have evaluated the ro le of T-ce l l deplet ion. Lokhors t e t al . (552)
compared auto logous s tem cel l t ransplants to T-ce l l–depleted a l logeneic s tem cel l
t ransplants . Myeloma pat ients were e l ig ib le i f they had chemotherapy-sens i t ive disease.
Genetic randomizat ion was used. Af ter 44 months ' median fo l low-up, overa l l surviva l had
not yet been reached in e i ther group (Table 99.12) . Transplant- re la ted mortal i ty in the
a l logeneic group was 18%, compared wi th 6% in the auto logous group. In thei r Phase
successor I I I s tudy (HOVON [Dutch-Belg ian Hemato-Oncology Cooperat ive Group] 24) , 53
newly d iagnosed myeloma pat ients wi th an HLA-ident ica l s ib l ing were a l located to a part ia l
T-ce l l–depleted a l logeneic SCT after induct ion therapy (556). The overa l l response rate was
89%, inc luding a 19% complete response. W ith a median fol low-up of 38 months, 33 (62%)
had d ied, 18 f rom t reatment- re lated mortal i ty . The median progression-f ree surviva l f rom
the a l logeneic SCT was 17 months, and median overa l l surviva l was 25 months. Only three
pat ients are in cont inu ing complete response. The authors conclude that the i r data do not
support T-ce l l–depleted myeloablat ive al logeneic SCT as par t o f f i rst - l ine therapy.
Alyea et al . a lso evaluated T-cel l–depleted a l lograf ts, fo l lowed by donor lymphocyte
in fus ions (Table 99.12) . Th is approach appeared to be of l imi ted benef i t , wi th a high
t reatment- related mortal i ty , in fer ior 2-year PFS and OS, but s imi lar 4-year PFS and OS
(554).
Bal len et al . reviewed the National Marrow Donor Program (NMDP) exper ience of
myeloablat ive al logeneic t ransplants (557) . There were 71 consecut ive cases f rom July
1989 to February 2000, wi th a median age of 44 years ( range 22 to 60 years) . Median t ime
to unre la ted donor t ransplant was 17 months. Thi r ty-n ine percent were T-ce l l–depleted. The
2-year survival rate was 27%, and at 5 years only 9% of pat ients were a l ive.
Nonmyeloablative Allogeneic Transplant
In another e f for t to reduce a l logeneic t ransplant-re lated mortal i ty , “nonmyeloablat ive, ”
“ reduced- in tensi ty” or “min i ” s tem ce l l t ransplant reg imens have been s tud ied in pat ients
wi th mul t ip le myeloma. The princ ip le behind th is approach is to harness the improved
complete response rate and re lapse- f ree morta l i ty seen in a s tandard fu l l a l logeneic
t ransplant whi le e l iminat ing the h igh t reatment- rela ted mortal i ty ra tes . The morta l i ty rate for
a l logeneic
P.2398
t ransplantat ion must be reduced before i t can assume a major ro le in the treatment of
mult ip le myeloma. Table 99.13 contains the resul ts f rom the f i rs t studies employing th is
reduced- intens i ty condi t ion ing approach. Many s tud ies inc luded relapsed or re fractory
pat ients , which was thought to account a t least in par t for the poor outcomes. I t a lso
became apparent that th is approach was less usefu l in pat ients who had signi f icant residual
tumor burden at the t ime of the nonmyeloablat ive t ransplant , which led to the concept o f a
p lanned autologous SCT fo l lowed a couple of months la ter by a reduced- in tens i ty a l logeneic
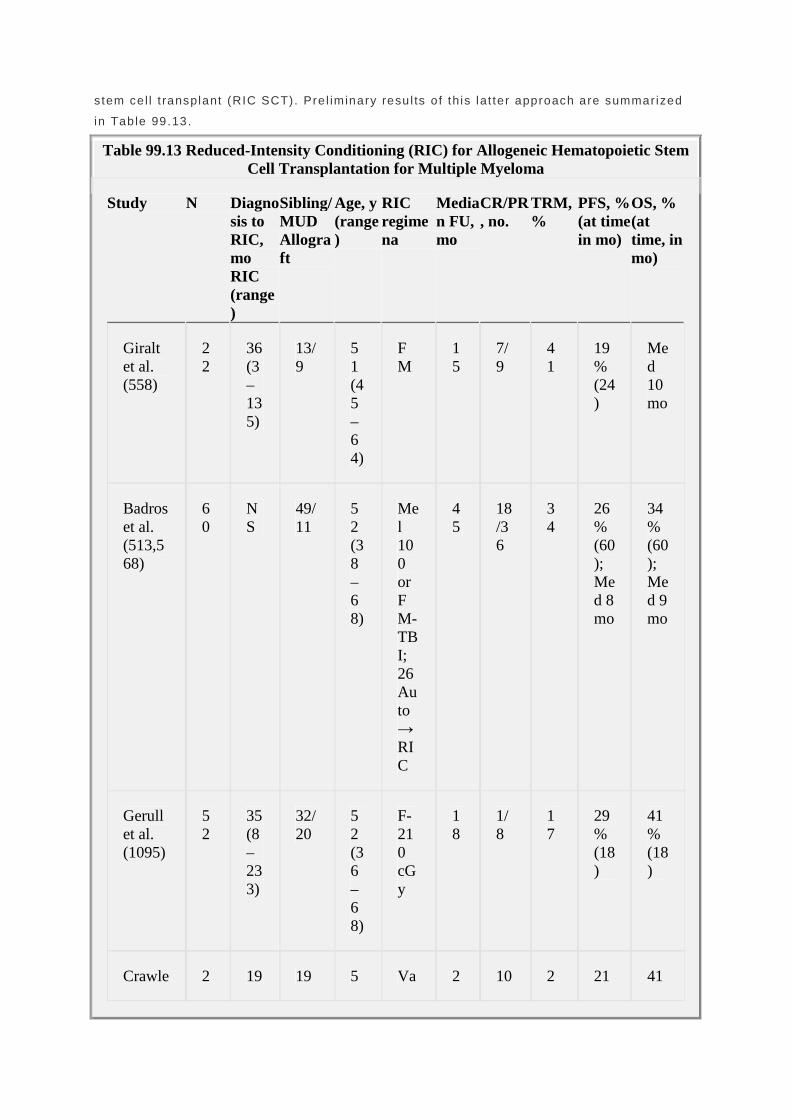
stem cel l t ransplant (RIC SCT). Pre l iminary resu l ts o f th is lat ter approach are summar ized
in Table 99.13.
Table 99.13 Reduced-Intensity Conditioning (RIC) for Allogeneic Hematopoietic Stem Cell Transplantation for Multiple Myeloma
Study N Diagnosis to RIC, mo RIC (range)
Sibling/ MUD Allograft
Age, y (range)
RIC regimena
Median FU, mo
CR/PR, no.
TRM, %
PFS, % (at time in mo)
OS, % (at time, in mo)
Giralt et al. (558)
22
36 (3–135)
13/9
51 (45–64)
FM
15
7/9
41
19% (24)
Med 10 mo
Badros et al. (513,568)
60
NS
49/11
52 (38–68)
Mel 100 or FM-TBI; 26 Auto → RIC
45
18/36
34
26% (60); Med 8 mo
34% (60); Med 9 mo
Gerull et al. (1095)
52
35 (8–233)
32/20
52 (36–68)
F-210 cGy
18
1/8
17
29% (18)
41% (18)
Crawle 2 19 19 5 Va 2 10 2 21 41

y et al. (560)
29
.2 (2–132)
2/37
2 (32–66)
ried
8 /53
2 % (36)
% (36)
Perez-Simon et al. (1096)
70
— — 54 (30–66)
FM; 15 Auto → RIC
19
18/40
24
Med 32 mo
Med 10 mo
Shimazaki et al. (1097)
45
— NS 53 (39–63)
F-based
25
9/24
9 18.8% (36)
38.5% (36)
Galimberti et al. (1098)
20
11 NS 51 (35–66)
Auto → RIC
35
NS
20
51% (24)d
58% (24)d
Maloney et al. (561)
54b
NS
54/0
52 (29–71)
Auto → RIC
22c
25/14
25
55% (24)c
78% (24)c
Kroger et al. (562,5
47
11.2 (4.
24/23
52 (3
Auto →
16
26/13
11
54% (36
70% (36

63,564)
7–57)
1–64)
RIC
) )
ATG, antithymocyte globulin; Bu, busulfan; CR, complete response; F, fludarabine; FC, fludarabine and cyclophosphamide; FM, fludarabine and melphalan; FU, follow-up; Mel, melphalan; MM, multiple myeloma; MMF, mycophenolate; MTX, methotrexate; MUD, matched unrelated donor; RIC, reduced-intensity conditioning; NS, not stated; OS, overall survival; PFS, progression-free survival; PR, partial response; TBI, total-body irradiation; TRM, treatment-related mortality. aAll studies used cyclosporine as part of the graft-versus-host prophylaxis program. bForty-eight percent with relapsed or refractory disease prior to autologous transplant. cTime measured from autologous stem cell transplantation. dTime measured from RIC.
The f i rs t publ ished report o f a RIC series came f rom Gira l t e t a l . , working at the M. D.
Anderson Cancer Center (Table 99.13) . They t reated 22 pat ients , who were predominant ly
re lapsed or ref rac tory, wi th a reduced- intens i ty program inc lud ing f ludarabine and
melphalan. W ith a median fol low-up of 15 months, the median overal l surviva l was 10
months, and 19% were progression- f ree at 24 months (558) . The same group compared
sa lvage auto logous ASCT to RIC SCT for pat ients fai l ing pr ior ASCT. W ith a median fo l low
up of 18 months for the autologous pat ients and 30 months for the al logeneic group, the
respect ive PFS were 6.8 and 7.3 months and the respect ive OS were 29 and 13 months
(559).
Invest igators f rom the Universi ty of Arkansas reported the resul ts o f RIC SCT in 31 poor-
r isk myeloma pat ients (513) . Twenty- f ive were HLA-compat ib le s ibl ings, and 6 of the
rec ip ient -donor pa i rs were unre la ted but matched (Table 99.13) . The condit ioning reg imen
cons is ted of melphalan 100 mg/m 2 for re la ted and melphalan 100 mg/m2 p lus to tal -body
i r radia t ion (250 cGy) p lus f ludarabine for unre la ted al lograf ts. Donor lymphocyte in fusions
were in i t ia l ly given on days 21, 42, and 112 to pat ients wi th no c l in ica l evidence of graf t-
versus-host d isease (GVHD); however, because of high ra tes of lymphocyte- induced GVHD,
donor lymphocyte infus ions were reserved for pat ients who needed to at tain ful l donor
ch imerism or who requi red eradicat ion of residual d isease. Al l but one pat ient had received
one or more than two pr ior auto logous t ransplants . Fi f ty- f ive percent o f the pat ients had
progress ive d isease at the t ime of the al lograf t . Acute GVHD developed in 18 pat ients . Ten
pat ients progressed to chronic GVHD—limi ted in 6 and extensive in 4 pat ients . Two pat ients
fa i led to engraf t even af ter a second a l logeneic per ipheral b lood s tem cel l in fusion. At a
median fol low-up of 6 months, 12 pat ients ach ieved complete remiss ion and another 7 a
near-complete remiss ion, whi le 3 achieved a par t ia l remission. There were 3 treatment-
re lated deaths dur ing the f i rs t 100 days and another 6 a fter 100 days, for an overa l l
t reatment- related mortal i ty o f 28%. Three pat ients died of progressive myeloma. Pat ients
who received t ransplants wi th progressive disease or who had received more than one pr ior

autograft had a sta t ist ical ly h igher morta l i ty ra te. The authors also compared the i r
nonmyeloablat ive t ransplant exper ience to thei r pr ior s tandard a l logeneic exper ience and
found that the nonmyeloablat ive group had a lower mortal i ty during the f i rs t year (p = .09) ,
most notab ly the subset who had received only one prior auto logous t ransplant (p = .05) .
Crawley et al . reported the outcome of 229 pat ients who received an al lograf t for myeloma
wi th reduced- in tensi ty condi t ion ing reg imens f rom 33 centers wi th in the European Group for
Blood and Marrow Transplantat ion (560) (Table 99.13). Ten percent o f pat ients had at least
two pr ior s tem cel l t ransplants, and 26% had never received an ASCT. Seventy-e ight
percent o f pat ients received matched sib l ing t ransplants . Sixteen percent had unre lated
donors . Only 20% received bone marrow s tem cel ls. Condit ion ing reg imens were
heterogeneous, but most were f ludarabine-based and T-ce l l–depleted wi th ant i thymocyte
g lobul in or alemtuzumab. Transplantat ion-rela ted morta l i ty a t 1 year was 22%. The 3-year
overa l l surviva l and progress ion- f ree survival rates were 41% and 21%, respect ive ly.
Adverse OS was associated wi th chemores is tant d isease (re la t ive r isk , 2 .9) , more than one
pr ior t ransplantat ion ( re la t ive r isk , 2 .0), and male pat ients wi th female donors ( rela t ive r isk ,
1 .45). Adverse PFS was associated wi th chemores is tance and alemtuzumab. Grades I I to IV
acute GVHD occurred in 31%. Chronic GVHD was assoc ia ted wi th bet ter OS and PFS and
were 84% and 46% for l imi ted, 58% and 30% for extens ive, and 29% and 12% in i ts absence,
suggest ing that a graft -versus-myeloma effect is important (F ig. 99.12) . The authors
conc luded that reduced-in tens i ty condi t ion ing is feasible , but heavi ly pret reated pat ients
and pat ients wi th progressive disease do not benef i t .
Maloney and co l leagues (561) repor ted resu l ts on 54 newly d iagnosed myeloma pat ients
who were t reated wi th a p lanned tandem auto logous/nonmyeloablat ive a l logeneic s tem cel l
t ransplantat ion (Table 99.13). Af ter induct ion wi th four cyc les of VAD chemotherapy,
fo l lowed by ASCT using melphalan 200 mg/m 2
P.2399
as condit ion ing, pat ients underwent a RIC SCT. The condit ion ing for the second t ransplant
was wi th to ta l -body i r radia t ion (200 cGy). Matched sib l ing donor periphera l blood s tem cel ls
were in fused immediate ly a f ter the to ta l -body i r rad ia t ion. Postgraf t ing immunosuppress ion
included mycophenolate and cyclosporine. Fi f ty- two of the 54 pat ients rece ived the p lanned
RIC SCT, wi th a median t ime between autologous and a l logeneic t ransplants o f 62 days.
The granulocyte and pla te le t nadi rs af ter the nonmyeloablat ive t ransplant were 760 and
95,000 cel ls /µ l , respect ive ly. Acute GVHD was seen in 38% of pat ients and was grade I I in
a l l but four cases. For ty-s ix percent o f pat ients developed chronic GVHD that requi red
therapy. Al l pat ients ach ieved donor engraf tment. F i f ty-seven percent o f pat ients not in
complete response af ter the f i rs t t ransplant ach ieved a complete response af ter the second
t ransplant. W ith a median fol low-up of surviv ing pat ients o f 18 months, 8 pat ients (15%) had
d ied of t ransplant- re lated compl icat ions, 2 o f progress ive myeloma, and 1 of lung cancer .

Figure 99.12. European Blood and Marrow Transplantation Registry data on the role of reduced intensity conditioning allogeneic transplantation regimens. A: Overall and progression-free survival. B: Overall survival relative to presence or absence of graft versus host disease. (With permission, ferom Crawley C, Lalancette M, Szydlo R, et al. Outcomes for reduced-intensity allogeneic transplantation for multiple myeloma: an analysis of prognostic factors from the Chronic Leukaemia Working Party of the EBMT. Blood 2005;105: 4532–4539. © the American Society of Hematology.)
Kroger e t a l . (562,563) have appl ied a s imi lar s t rategy, inc lud ing a planned s tandard-
in tensi ty autograft (melphalan 200 mg/m2 ) fo l lowed by a dose-reduced reg imen (f ludarabine
180 mg/m 2 , melphalan 100 mg/m 2 , and ant i thymocyte globul in 10 mg/kg on 3 days) before
a l lograf t ing (Table 99.13) . GVHD prophylaxis inc luded cyclospor ine and min i -methotrexate.
Nine pat ients rece ived al lograf ts f rom re la ted donors and 8 f rom unre la ted donors. Acute
GVHD stage I I to IV occurred in 6 pat ients (38%). Chronic GVHD developed in 40% of the
pat ients , but only 1 pat ient exper ienced extens ive chronic GVHD requi r ing fur ther
immunosuppress ive therapy. The 100-day morta l i ty ra te was 11%, and wi th a median fo l low-
up of 17 months af ter auto logous and 13 months af ter a l logeneic t ransplantat ion, 13
pat ients (76%) are al ive. The rate of complete remission wi th negat ive immunof ixat ion
increased f rom 18% after autograf t ing to 73% after al lograft ing, and 12 remain f ree of
re lapse or progression.
Th is same group has a lso repor ted on th is approach us ing matched unrela ted donors (564).
Twenty-one pat ients wi th advanced mul t ip le myeloma were condi t ioned wi th a reduced-
in tensi ty condi t ioning reg imen consist ing of f ludarabine (150 mg/m 2 ) , melphalan (100 to 140
mg/m 2 ) , and ant i thymocyte globul in (ATG; 10 mg/kg on 3 days) . Al l pat ients had received at
least one pr ior auto logous transplantat ion, in 9 cases as par t o f an auto logous-al logeneic
tandem protocol . Grade I I to IV acute GVHD was seen in 8 pat ients (38%), and severe
grade I I I / IV GVHD was observed in 4 pat ients (19%). Six pat ients (37%) developed chronic
GVHD, but on ly 2 pat ients (12%) exper ienced extensive chronic GVHD. The est imated
probabi l i ty o f nonre lapse morta l i ty a t 1 year was 26%. Af ter al lograf t ing, there was an
overa l l response rate of 90% (40% complete response and 50% part ia l response) . Af ter a

median fol low-up of 13 months, the 2-year est imated overal l and progress ion- f ree survival
ra tes were 74% (95% CI , 54 to 94%) and 53% (95% CI , 29 to 87%), respect ively. A shorter
progress ion- f ree survival was seen in pat ients who had al ready exper ienced relapse to pr ior
autografts (26 vs . 86%, p = .04) .
Table 99.14 Prospective Randomized Trials Comparing Tandem Autologous SCT to Tandem Autologous-HLA Identical Reduced-Intensity Allogeneic SCT
Study N Regimen Age, y (range)
Completed Both SCTs, %
Median FU, mo
Patients in CR, %.
TRM, %
PFS, %
OS, %
219a
Auto mel 200/220 ± IL-6 Ab
58 (28–65)
76 24
33 5 0 at 5 y
44 at 56 mo
Garban et al. (565,566)
65 Auto mel/Allo Bu/Flu/ATG
54 (38–65)
71 28
43 8 0 at 5 y
33 at 5 y
73 Auto mel 200/200
53 (33–64)
75 36
16 4 41 at 3 y
62 at 3 y
Bruno et al (567)
56 Auto mel 200/Allo TBI
54 (34–65)
100 36
46 11 75 at 3 y
84 at 3 y
FU, follow-up; OS, overall survivial; PFS, progression-free survivial; TRM, treatment-related mortality. aHigh-risk patients as defined by the presence of deletion 13 by FISH and β2-microglobulin of >3 mg/L.
Two randomized contro l led t r ia ls compared up- f ront sequent ia l auto logous SCT to
sequent ial autologous SCT, RIC a l logeneic SCT (565) (Table 99.14) .

The f i rs t of these was the IFM9903/9904 tr ia l , in which high-r isk pat ients, as def ined by a
β2 -microg lobul in >3 mg/L and delet ion 13 by FISH, were b io log ical ly randomized to e i ther a
p lanned ASCT fo l lowed by a RIC SCT (n = 65) or two dose- in tensi f ied tandem ASCTs
fo l lowed by t reatment wi th ant i - IL-6 monoc lonal ant ibodies (n = 219) (565,566) . On an
in tent - to- t reat analysis , outcomes of h igh-r isk myeloma pat ients were no d i f ferent between
the groups: median surviva l , 35 versus 41 months; and median event- free survival , 25
versus 30 months, respect ively. There was a t rend toward bet ter overa l l surviva l in the non–
al logeneic SCT arm, 47.2 versus 35 month, p = 0.07, when only pat ients who completed
the ir t reatment assignment were cons idered.
Bruno et a l . (567) have presented in abst rac t form the i r 3-year resul ts o f a prospect ive
randomized tr ia l of double auto logous t ransplants versus tandem auto-RIC. Outcomes were
s ign i f icant ly
P.2400
bet ter in the auto-RIC arm, wi th resu l ts far outs t r ipping those of o ther auto-RIC studies.
So the quest ion remains: W ho should rece ive reduced- in tensi ty condi t ioned SCT? The
answer is not c lear. Some invest igators , includ ing ourselves, have l imi ted the appl icat ion of
RIC SCT to pat ients wi th very h igh-r isk d isease. However, some avai lable data suggest that
pat ients def ined as h igh r isk by FISH delet ion 13 do not seem to do bet ter wi th RIC SCT
than pat ients receiv ing tandem auto logous HSCT (565,566) . Others have quest ioned
whether the RIC, which conta ined ant i thymocyte g lobul in , was too immunosuppress ive and
therefore abrogated a graf t -versus-myeloma ef fec t . Data f rom Lee et a l . show that pat ients
wi th metaphase cytogenet ic abnormal i t ies , which are in par t a surrogate for plasma ce l l
pro l i ferat ion, a lso do worse than the i r counterpar ts wi th normal cytogenet ics (568) . Pat ients
wi th cytogenet ic abnormal i t ies receiv ing RIC SCT had a 36% l ike l ihood of re lapse at 1 year ,
in contrast to 5% for pat ients who lacked cytogenet ic abnormal i t ies go ing in to RIC, even i f
they previous ly had cytogenet ic abnormal i t ies a t an ear l ier date (568).
Unt i l further re f inements are made and addi t ional conf i rmatory studies wi th longer fol low-up
are completed, the ro le o f nonmyeloablat ive a l logeneic stem cel l t ransplantat ion as in i t ia l
therapy in myeloma must be considered invest igat ional . See Table 99.13 for addi t ional
pre l iminary data.
Donor Lymphocyte Infusions A graft -versus-myeloma ef fec t has been noted after the administ ra t ion of donor per iphera l
b lood mononuclear ce l ls for relapse after a l logeneic t ransplantat ion (540,569) . Donor
lymphocyte in fus ion (DLI) has been used in three ways in myeloma pat ients . In i t ia l ly , i t was
used to t reat re lapsed or residual d isease after a fu l l myeloablat ive a l logeneic s tem cel l
t ransplant (540,569). Subsequent ly, i t was used to supply T ce l ls to pat ients who had
received an a l logeneic T-ce l l–depleted graft (570,571). Most recent ly, i t has been used in
RIC programs to t reat mixed ch imer ism, as wel l as for previous ly es tabl ished ind ic t ions
(572,573,574) .
In the largest DLI ser ies for relapsed myeloma (n = 54) (575) , 52% of pat ients responded to
donor lymphocyte in fus ions, 35% wi th a part ia l response and 17% wi th a complete response.
The most common s tar t ing T-cel l dose was 1 ×107 ce l ls /kg, wi th a range of 1 × 106 to 5 ×108
ce l ls/kg. Fi f ty- four pat ients rece ived a to ta l o f 95 DLI courses ( range, 1 to 7 courses) for a

median of 20 months (range 4 to 90 months). Retreatment was prompted by a lack of
response or lack of GVHD by 3 months. The major i ty o f pat ients rece ived some
chemotherapy before DLI . Progression- f ree and overa l l surviva l were 19 and 23 months,
respect ive ly. Rates of overa l l acute GVHD and of grade I I I to IV acute GVHD were 57 and
20%, respect ive ly. Rates of overa l l chron ic GVHD and of extens ive GVHD were 47 and 30%,
respect ive ly. Acute and chronic GVHD fo l lowing DLI were the s t rongest pred ic tors for
response (575) .
The best s tart ing dose for DLI has not yet been estab l ished. Ini t ia l repor ts suggested that a
T-ce l l dose of more than 1×108 cel ls /kg, response to re induct ion therapy, and
chemotherapy-sens i t ive d isease before a l logeneic t ransplantat ion (576) were predict ive of
best outcomes, but these data have not yet been conf i rmed by s tud ies wi th larger sample
s izes and fur ther fo l low-up (573,575,577) .
Von Donk et a l . reviewed the i r exper ience wi th donor lymphocyte in fusions given for
re lapsed (n = 48) or persis tent (n = 15) myeloma fo l lowing RIC SCT (574) . Acute and
chronic GVHD occurred in 38% and 43% of pat ients , respect ively. There were seven
t reatment- related deaths. Th i r ty-e ight percent o f pat ients responded, wi th ha l f achieving a
par t ia l response and hal f a complete response. Wi th a median fol low-up of 14 months,
overa l l surviva l a f ter DLI was 23.6 months (1 .0 to >50.7 months) : 23.6 months for
nonresponders and not yet reached for responders . In responders , progression-f ree surviva l
a f ter DLI was 27.8 months (1 .2 to >46.2 months). The only s igni f icant prognost ic factors for
response to DLI were the occurrence of acute and chronic GVHD.
Maintenance Therapy
Strateg ies for maintenance therapy can be d iv ided into two broad categories : (a) cont inued
induct ion therapy ad in f in i tum, and (b) addi t ion of a novel therapy af ter induct ion therapy.
The former s t ra tegy was prevalent unt i l recogni t ion of the r isk o f developing a lkylator-
induced myelodysplast ic syndromes and leukemia (578,579,580,581,582,583) . The la t ter
s t rategy has mainly used immune modulators , including prednisone, in ter feron, ce l lu lar
therapies, and, more recent ly, thal idomide and lenal idomide. To date, the benef i ts o f
maintenance therapy have been margina l a t best, but for severa l o f these agents , addi t ional
s tud ies are requi red. No benef i t has been observed wi th maintenance levamisole (271,369) ,
azath ioprine (584) , or bac i l lus Calmet te-Guérin (BCG) (387).
Maintenance Chemotherapy Through the 1970s and 1980s, severa l randomized s tudies estab l ished that alkyla tor-based
maintenance therapy does not produce a survival benef i t
(225,253,278,280,364,384,584,585,586) . In genera l , pat ients not receiv ing maintenance had
s imi lar to s l ight ly shor ter remiss ion durat ion than those receiv ing maintenance
(225,364,384,584,586,587) but had h igher ra tes of a second remiss ion (586,587) . Some
s tud ies showed a t rend toward longer surviva l in the former group (278,280,585) .
Induct ion therapy is commonly d iscont inued after p lateau is reached, def ined as no change
in M protein o f >25% for 4 to 6 months (225,278,588) . W ith a lkyla tor-based therapy, the
ab i l i ty to achieve a pla teau is as important as the degree of response achieved
(225,588,589,590,591,592) . No benef i t has been documented for treatment beyond 12
months (364) , a l though i t has been suggested—but not va l idated—that pro longed primary

chemotherapy may be benef ic ia l in pat ients ach ieving less than a par t ia l response, i .e . , a
minimal response or s tab le d isease (593) .
Alkylator-unmaintained remiss ions tend to last about 12 months (584). Pat ients who re lapse
of f alkyla tor-based chemotherapy have response rates of 25 to 80% wi th resumpt ion of the
or iginal reg imen (225,387,586,587) . Second response rates are lower in pat ients who
progress or relapse during maintenance than in those who relapse wi thout maintenance
therapy in the case of alkyla tor-based therapy (584,587) and IMiD-based therapy (594) . In a
s tudy of 115 newly d iagnosed pat ients t reated wi th VBMCP for ~1 year , an in i t ia l response
rate of 82% was achieved, wi th a median durat ion of response of 22 months. Af ter a f i rs t
re lapse, 26 of 38 pat ients (68%) responded again and had a median durat ion of response of
11 months. After a second relapse, 7 o f 16 pat ients (44%) responded, wi th a durat ion of
response of 3 .5 months (595) .
Corticosteroids as Maintenance Therapy Four s tud ies deal wi th cor t icostero ids as maintenance therapy. None just i f ies a
recommendation of prednisone as a s tandard maintenance reg imen for a l l pat ients .
The most recent s tudy (SW OG 9210) compared prednisone 10 mg every other day to
prednisone 50 mg every other day in pat ients who had responded (SW OG PR or bet ter) to 6
to 12 months of a VAD-based program, that is , a cor t icosteroid- in tens ive program. From the
t ime of randomizat ion to the two di f ferent al ternate-day prednisone schedules, the median
progress ion- f ree survival for the h igher-dose prednisone arm was 14 months, compared to 5
months for the lower dose (p = .003). Survival also was marginal ly bet ter , a t 37 and 26
months (p = .05) (596) . Al though the more dose-in tensive cor t icosteroid maintenance
s t rategy does provide a longer progress ion- f ree surviva l in cor t icosteroid-respons ive
pat ients , these data cannot be general ized. By compar ison, af ter a lkylator-based therapy
the median unmainta ined progression- f ree surviva l is 12 months in responding pat ients
(584).
P.2401
An ear l ier randomized s tudy, which compared dexamethasone maintenance to in ter feron
maintenance after induct ion wi th melphalan and dexamethasone, demonstrated equiva lence
to in fer ior i ty o f dexamethasone compared wi th inter feron. Pat ients rece ived maintenance
t reatment wi th in ter feron-α (3 MU 3 t imes a week) or dexamethasone (20 mg/m 2 oral ly da i ly
for 4 days repeated month ly) unt i l re lapse. Remission durat ion was ident ica l (10 months);
however, s igni f icant ly more pat ients responded upon re ins t i tut ion of the melphalan and
dexamethasone at d isease re lapse in the in ter feron group than in the dexamethasone group
(82 vs . 44%, p = .001) (597) .
The CALGB 7461 s tudy addressed this issue less di rec t ly. Pat ients were t reated ini t ia l ly
wi th a lkyla tor therapy and were randomized to observat ion or v incr ist ine and prednisone as
maintenance. Survival and response rates were s ign i f icant ly longer and h igher in the
v incr is t ine–prednisone maintenance group who had received up- front melphalan (median,
35.3 vs . 27.0 months; p = .003) but not in pat ients who had received up-f ront BCNU or
CCNU (269) .
F inal ly, SW OG 8624, which evaluated the in f luence of cor t icosteroid dose in tens i ty on
response and surviva l , ind i rec t ly provided data on cor t icostero id maintenance. Higher

object ive response rates and median survival were observed in pat ients who received
pro longed administ ra t ion of glucocort ico ids (prednisone 50 mg every other day) between
chemotherapy courses. Pat ients given VMCP/VBAP wi th and wi thout al ternate-day
prednisone had median overa l l surviva ls of 40 versus 31 months, respect ive ly (p = .02) . The
surviva l advantage may have been confounded by the complexi ty o f the study; di f ferent
t reatment p lans were ass igned after 12 months of induct ion therapy, determined by tumor
response (402) . Moreover , one could argue that the cor t icosteroid was a par t o f the
induct ion ra ther than the maintenance program.
Interferon as Maintenance Therapy
After Conventional Chemotherapy
The in i t ia l posi t ive f indings by Mandel l i et al . (598) in 1990 demonstrated a super ior
d isease- free and overa l l surviva l in chemotherapy-respons ive pat ients randomized to
maintenance inter feron-α . Subsequent studies have yie lded d ivergent resu l ts . Ludwig and
Fr i tz (431) analyzed 1,615 pat ients in 13 maintenance t r ia ls
(374,419,422,598,599,600,601,602,603,604,605,606,607,608) ; the Myeloma Tr ia l is ts '
Col laborat ive Group (432) used the ind iv idual data of 1 ,543 pat ients enrol led in 12
randomized tr ia ls (374,402,419,422,426,599,601,605,609,610,611). Results were s imi lar in
that the f i rs t group found a 4.4-month pro longat ion of re lapse- free surviva l (p < .01) and a
7.0-month increase in overa l l surviva l (p < .01) (431) . The lat ter group repor ted a 3-year
progress ion- f ree survival o f 27 versus 19 months (p < .00001) in favor o f the in terferon
maintenance group. Inter feron-α prolonged the overa l l surviva l by ~7 months (p = .04) (432)
(F ig . 99.10). Survival t ime f rom progress ion to death was s ign i f icant ly worse in the
in ter feron group than in the contro l group (odds rat io 1 .21, p = .007) . No analyzed fac tors
predic ted for the in terferon benef i t ( i .e . , pret reatment hemoglobin, calc ium, β2 -M, creat in ine,
sex, per formance s tatus, or immunoglobul in isotype). The level of response (complete
response, part ia l response, s tab le disease) or in ter feron dose in tensi ty (<12 vs . ≤12
MU/week) a lso d id not pred ic t for in ter feron ef fec t (432) . In 2000 the cost o f the 1-year
surviva l benef i t in pat ients t reated wi th inter feron as maintenance was $US 18,968,
assuming a dose of 11.6 MU/week (431) .
In Combination with Corticosteroids
Cort icostero ids have been added to maintenance in ter feron in an at tempt to intens i fy the
program. Smal l numbers of pat ients have been t reated wi th s tandard maintenance in ter feron
and e i ther dexamethasone (612) or prednisone (401,612) . In one smal l randomized s tudy,
the progress ion-f ree surviva l was longer in the cor t icostero id-p lus-inter feron arm than in the
in ter feron-only arm, a l though median surviva l was not di f ferent (401). The combinat ion can
a lso induce further par t ia l remiss ions in more than ha l f o f responding pat ients so t reated
(612) and may a lso pro long the durat ion of a second remiss ion (613) .
Interferon after High-Dose Chemotherapy with Stem Cell Support
Fewer data are avai lab le about the ut i l i ty o f in ter feron af ter autologous s tem cel l
t ransplantat ion. There is one smal l randomized t r ia l o f 85 pat ients (610) and a larger
re t rospect ive analys is o f regis t ry data by the European Group for Blood and Marrow
Transplantat ion (614) . The use of in ter feron in this sett ing cannot be recommended outs ide
of c l in ica l t r ia ls .

Cunningham et a l . (610) randomly ass igned 85 pat ients to in ter feron at 3 MU/m 2 three t imes
week ly or to observat ion. The median progression- f ree surviva l in the 43 pat ients
randomized to in ter feron-α was 46 months, compared wi th 27 months in the contro l pat ients
(p < .025) . Al though there was a s ign i f icant surviva l advantage at 54 months, a t which t ime
12% of pat ients in the inter feron group and 33% of pat ients in the no-in ter feron group had
d ied (p = .006), th is surviva l advantage was no longer evident a t a median fo l low-up of 77
months.
The data f rom the European Group for Blood and Marrow Transplantat ion reg is t ry included
473 pat ients who had received maintenance and 419 who had not . Unfor tunate ly, the two
groups were poor ly matched. The pat ients who did not receive in terferon had s igni f icant ly
more pr ior therapy, a higher s tage at diagnos is , and a longer t ime to t ransplantat ion. They
were a lso s ign i f icant ly o lder , and a h igher percentage had received to ta l -body i rradia t ion–
conta in ing condi t ion ing reg imens (614) . Al though these fac tors were “s tat is t ical ly corrected
for” in the survival analys is , the imbalance makes in terpretat ion of th is ret rospect ive
co l lec t ion of reg is t ry pat ients prob lemat ic . Prognost ic fac tors such as β2 -M, C-react ive
protein , cytogenet ics , and PCLI were not inc luded in the analys is . Overal l survival was
s ign i f icant ly bet ter in the pat ients who received inter feron (78 vs . 47 months, p = .007) .
Paradoxica l ly, there was a more prominent surviva l benef i t in those pat ients who achieved a
par t ia l response (97 vs . 46 months for in ter feron vs . no inter feron, p = .03) ra ther than a
complete response (64 vs . 51 months, p = .1) , and the par t ia l - response group had a better
overa l l surviva l than the complete-response group.
Thalidomide as Maintenance Therapy Severa l t r ia ls are evaluat ing the tolerabi l i ty o f tha l idomide as maintenance (615,616,617) ,
but very few Phase I I I data are evaluable at th is t ime, and therefore tha l idomide
maintenance cannot be recommended as standard therapy of f -s tudy. The two completed
t r ia ls that approach the quest ion are the IFM 99-02 (618) and Total Therapy 2 studies (594).
IFM 99-02 evaluates the va lue of maintenance tha l idomide versus no tha l idomide in low-r isk
myeloma pat ients who have undergone tandem ASCT. Though the 3-year event- f ree survival
(36 vs . 52%, p < .009) and the 4-year overal l surviva l (75 vs . 87%, p = .04) favored the
tha l idomide maintenance arm, there are severa l caveats to this t r ia l . The f i rs t is that median
fo l low-up is short at 39 months. The second is that on ly 65% of the pat ients on the no-
maintenance arm actua l ly received thal idomide at re lapse. The thi rd is that fewer of the no-
maintenance pat ients rece ived modern salvage therapy wi th lenal idomide or bor tezomib at
re lapse than d id the maintenance group (15 vs. 38%). W ith such a modest survival benef i t ,
i t is poss ib le that th is f ind ing wi l l not survive the tes t o f t ime.
The Tota l Therapy 2 t r ia l was a complex reg imen in which al l pat ients received in tensive
induct ion, tandem t ransplantat ion, and consol idat ive chemotherapy; pat ients were then
randomized to receive ei ther no thal idomide throughout or tha l idomide a long wi th a l l
therapies and cont inued as maintenance. Because of the intens i ty o f the program, i t is
d i f f icu l t to make sweeping genera l izat ions about the role that tha l idomide p layed as
maintenance therapy, but a few observat ions are worthy of note: Though response rates and
event- f ree survival ra tes were s ign i f icant ly
P.2402
bet ter in the group receiv ing tha l idomide, the overa l l surviva l ra tes were no di f ferent . Th is

t r ia l a lso i l lus t ra tes the danger o f concentrat ing too much on event-f ree and progression-
f ree endpoints in the context o f maintenance tr ia ls . Final ly, the quest ion that u l t imately
needs to be addressed is whether sa lvage therapy wi l l be as good as maintenance therapy.
Immunotherapy as Maintenance Therapy
Dendritic Cell-Based Vaccination
In an effor t to prolong durat ion of response and, hopeful ly, surviva l , id iotype- t reated
dendr i t ic cel l vacc ines are being explored as a therapeut ic modal i ty for myeloma pat ients .
B-cel l mal ignanc ies, includ ing mul t ip le myeloma, are un ique in the i r expression of
immunoglobul in (272). The immunoglobul in on mal ignant cel ls can be d is t inguished f rom
that on normal B cel ls or p lasma cel ls by v i r tue of speci f ic id io typ ic determinants . Dendr i t ic
ce l ls are the on ly known natura l cel ls that can present ant igen to naive T ce l ls (619).
Ant igen-pulsed dendr i t ic ce l ls can successful ly induce both humora l and cytotoxic ce l lu lar
immune responses.
Id iotyp ic vacc inat ions a lone have met wi th l imi ted success in human t r ia ls (620,621,622) .
However, vaccinat ion wi th pr imed dendr i t ic ce l ls appears to be a more potent way to induce
ant i tumor immuni ty than vaccinat ion wi th pept ide a lone (623,624,625) . Tr ia ls are now
explor ing the use of dendr i t ic cel l–based vacc inat ions in mul t ip le myeloma (626) .
Management of Relapsed or Refractory Disease
Relapsed and ref rac tory myelomas have dist inc t b iologies but are commonly grouped
together in d iscussions of chemotherapy regimens and tr ia ls. Di f ferent ia t ion between
re lapses occurr ing on therapy and of f therapy should be made, wi th the former having a
poorer prognosis. Simi lar ly, pr imary re f rac tory—the condi t ion in which the d isease has not
responded to in i t ia l therapy—and secondary re f rac tory (or resistant ) disease—should be
d ist inguished f rom each other. Final ly, wi th the growing l is t o f ac t ive agents now avai lable ,
the c lass of agents or the t reatment modal i ty to which the pat ient is ref rac tory should be
spec i f ied.
Before the in t roduct ion of h igh-dose chemotherapy wi th s tem cel l support , IMiDs, and
proteosome inhib i tors , t reatment gu ide l ines were more s t raight forward. I f the re lapse
occurred dur ing an unmaintained remiss ion, resumption of the pat ient 's or ig ina l therapy was
a good ru le (587) . F i f ty to 60% of pat ients responded to repeat t reatment i f re lapse occurred
af ter unmainta ined remiss ions (387,586,587,627) , wi th a median surviva l of about 10
months (587,628). The myeloma ce l l doubl ing t ime and durat ion of response tend to
decrease wi th each subsequent course of therapy (195,304,595). In the case of pr imary
re f rac tory d isease or acqui red res is tance on therapy, the mainstays of t reatment had been
c l in ical t r ia ls—anthracycl ine-based, cort icostero id-based, and a lkyla tor-based reg imens.
Table 99.15 Conventional Combinations for Relapsed, Refractory Disease
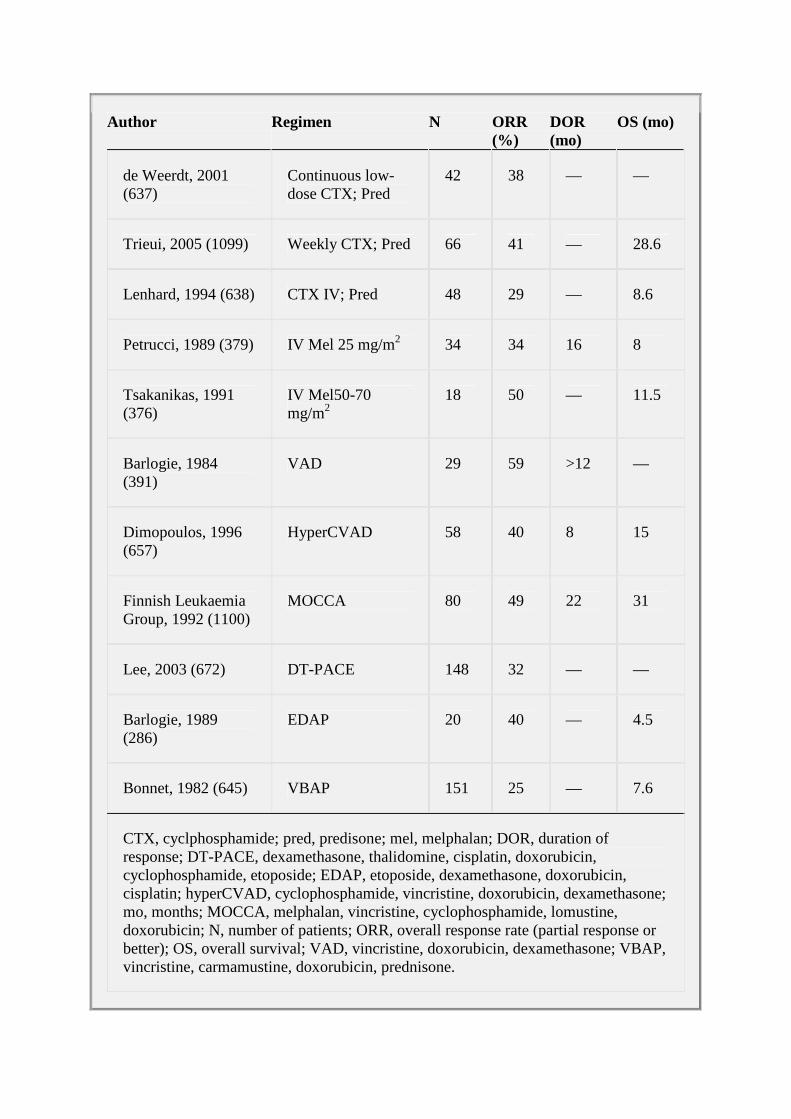
Author Regimen N ORR (%)
DOR (mo)
OS (mo)
de Weerdt, 2001 (637)
Continuous low-dose CTX; Pred
42 38 — —
Trieui, 2005 (1099) Weekly CTX; Pred 66 41 — 28.6
Lenhard, 1994 (638) CTX IV; Pred 48 29 — 8.6
Petrucci, 1989 (379) IV Mel 25 mg/m2 34 34 16 8
Tsakanikas, 1991 (376)
IV Mel50-70 mg/m2
18 50 — 11.5
Barlogie, 1984 (391)
VAD 29 59 >12 —
Dimopoulos, 1996 (657)
HyperCVAD 58 40 8 15
Finnish Leukaemia Group, 1992 (1100)
MOCCA 80 49 22 31
Lee, 2003 (672) DT-PACE 148 32 — —
Barlogie, 1989 (286)
EDAP 20 40 — 4.5
Bonnet, 1982 (645) VBAP 151 25 — 7.6
CTX, cyclphosphamide; pred, predisone; mel, melphalan; DOR, duration of response; DT-PACE, dexamethasone, thalidomine, cisplatin, doxorubicin, cyclophosphamide, etoposide; EDAP, etoposide, dexamethasone, doxorubicin, cisplatin; hyperCVAD, cyclophosphamide, vincristine, doxorubicin, dexamethasone; mo, months; MOCCA, melphalan, vincristine, cyclophosphamide, lomustine, doxorubicin; N, number of patients; ORR, overall response rate (partial response or better); OS, overall survival; VAD, vincristine, doxorubicin, dexamethasone; VBAP, vincristine, carmamustine, doxorubicin, prednisone.

The current landscape, however, is more compl icated. New combinat ions incorporat ing the
new and the o ld agents are be ing tested wor ldwide, leaving c l in ic ians wi th an assor tment o f
opt ions but l i t t le guidance on how to proceed. Does one use a ser ies of s ing le agents ,
adding addi t ional drugs as the s impler regimen fa i ls? And i f so, which agent does one use
f i rst? Or does one bet on synergy and star t wi th a mul t iagent program at f i rs t re lapse? So
far , there are no answers to these quest ions, and pat ient and physic ian preference guide
the dec is ion-making process ra ther than data. Moreover, as we review salvage therapies,
one must remember that response rates for o lder sa lvage regimens were based
predominant ly on a lkyla tors and cor t icostero ids sa lvaging a lkyla tor and cor t icosteroid
fa i lures. One would, for ins tance, expect the cyclophosphamide prednisone sa lvage rate to
be higher for thal idomide and dexamethasone fa i lures than melphalan and prednisone
fa i lures, a l though this hypothesis has not yet been examined in any formal s tudies .
Unt i l myeloma is a curable disease in a l l pat ients, c l in ica l t r ia ls wi l l p lay a cr i t ica l role in
the treatment o f these pat ients . They wi l l ass is t in def ining a better c lass i f icat ion system for
the d isease, c lar i fy which t reatments of fer the most value, and br ing new ef fec t ive agents
in to s tandard c l in ica l pract ice. The subject of chemotherapy for re lapsed or re fractory
d isease wi l l be d iv ided in to four sect ions: a lkylator-based reg imens, anthracycl ine-based
reg imens wi th or wi thout dose- in tensi f ied cor t icostero ids , novel therapies, and other
t reatment modal i t ies.
Alkylator-Based Regimens for Relapsed or Refractory Disease
(Table 99.15) There is c ross-resistance among the a lkyla tors , but th is is not absolute and may be
c i rcumvented by increasing dose in tensi ty. W ithout s ign i f icant dose in tens i f icat ion, 5 to 20%
of pat ients wi th melphalan-res is tant disease respond to cyc lophosphamide or BCNU as
s ing le agents or in combinat ion wi th prednisone (628,629,630,631,632,633,634) . Response
rates as high as 30 to 38% can be obta ined i f prednisone is administered wi th the
cyc lophosphamide (635,636,637) . Higher doses of cyc lophosphamide (e.g. , 600 mg/m2
in t ravenously for 4 consecut ive days) resu l t in response rates of 29 to 43% (254,638). Both
response durat ion and overa l l surviva l
P.2403
tend to be shor t , ~3 and 9 months, respect ive ly (254,638) . Consol idat ing the chemotherapy
in to a 1-day schedule rather than a 4-day schedule does not improve response rates but
does increase toxic i ty (639) . Simi lar ly, administ rat ion of 3 .6 g/m2 over 2 days wi th
prednisone appears to produce comparable responses (640) .
Dose intens i f icat ion of melphalan can also be qu i te e ffec t ive and is the bas is for high-dose
therapy wi th stem cel l support (237) . Selby et a l . (243) repor ted that 66% of pat ients wi th
res is tant d isease t reated wi th 140 mg/m 2 wi thout s tem cel l support responded, but median
response durat ion was on ly 6 months, a l l pat ients relaps ing wi thin a year. Median t imes to
leukocyte and p la tele t recovery were 42 and 37 days, respect ive ly, and the regimen-re la ted
toxic i ty was 13%. Doses of 50 to 70 mg/m2 resul t in a 50% response rate and leukocyte and
p la te le t recovery t ime of 20 and 16 days, respect ive ly (376,377) . Fur ther reduc ing the
in tensi ty to 30 mg/m2 every 2 months resul ts in response rates of 38% and a progress ion-
f ree survival of 10 months (380) .

VBMCP ( the M-2 reg imen) or MOCCA provides responses in 20 to 30% of re f ractory pat ients
(246,363,641) wi th a median surviva l o f about 11 months (246). Combinat ions of c isp la t in
wi th BCNU, cyclophosphamide, and prednisone have produced responses in heavi ly
pret reated pat ients (330); however, the addi t ion of c ispla t in and bleomycin to VBAP d id not
appear to produce bet ter outcomes than s tandard VBAP (286,329,330) .
Dimopoulos et al . (642) exp lored a combinat ion of high-dose cyclophosphamide (3 g/m 2 )
and etopos ide (900 mg/m 2 ) fo l lowed by granulocyte-macrophage colony-s t imulat ing fac tor .
Of the 52 pat ients wi th advanced and ref ractory mult ip le myeloma t reated, 42% responded.
Median t ime to granulocyte recovery was 19 days, and the median durat ion of remission
was 8 months.
Anthracycline-Based Regimens for Relapsed or Refrac tory
Disease Var ious permutat ions of doxorubic in-containing chemotherapy regimens—doxorubic in and
cyc lophosphamide (AC) (386); doxorubic in , BCNU, cyclophosphamide, and prednisone
(ABC-P) (643) ; CAP (644) ; VCAP (387) ; VBAP (645,646) ; and BAP (644) have been t r ied in
pat ients wi th re lapsed and ref rac tory d isease, resul t ing in response rates of 7 to 28%
(387,643,644,645). Response durat ion and surviva l tend to be shor t—<6 and 12 months,
respect ive ly. Responding pat ients tend to l ive 7 to 10 or even 22 months longer than
nonresponders (644,645,646) . Pat ients who have re lapsed d isease, ra ther than res is tant or
re f rac tory d isease, have h igher response rates ( i .e . , c lose to 30%).
Af ter s tudying high-dose cytos ine arabinos ide, c isp la t in , and etopos ide as s ing le agents ,
Bar log ie e t al . (331) did pre l iminary s tud ies wi th DAP (dexamethasone, cytos ine arab inos ide,
and c ispla t in) and la ter EDAP (etopos ide and DAP). In pat ients wi th ref rac tory disease,
response rates wi th these t reatments were 7, 14, 17, 0 , and 40%, respect ive ly. Median
surviva l in pat ients t reated wi th EDAP was 4.5 months. Th is regimen is myelosuppress ive,
wi th more than hal f of t reated pat ients requi r ing p la te le t t ransfus ions and 80% requi r ing
hospi ta l izat ion for neutropenic fever . In the f i rs t month, t reatment- re la ted morta l i ty was 15%.
In the complex Tota l Therapy 2 program, in which th is reg imen was used as par t o f
induct ion, the respect ive incrementa l objec t ive and complete response rates went f rom 55
and 9% to 65 and 15% af ter EDAP therapy (331).
Another approach to t reat ing relapsed or re f ractory myeloma is by augment ing anthracycl ine
and vincr ist ine wi th h igh-dose cor t icosteroids . Alexanian et al . (247) descr ibed VAP (bolus
v incr is t ine 1.5 mg on day 1, doxorubic in 35 mg/m 2 on day 1, and prednisone 45 mg/m 2 for 5
days repeated every 8 days for three cort icostero id pulses) ; response rates accord ing to
SW OG response and improvement cr i ter ia were 47%. Bar log ie et al . (391) publ ished thei r
exper ience wi th VAD, and numerous var iants have fol lowed. The overa l l response rate wi th
VAD in 29 pat ients who had ref rac tory or resistant disease was 59% accord ing to SW OG
cr i ter ia . In the 20 pat ients who had not rece ived pr ior doxorubic in , the response rate was
70%. VAD di f fered f rom VAP in that the former inc luded cont inuous- in fus ion v incr is t ine and
doxorubic in and a s ixfo ld cort icostero id dose intens i f icat ion (391) . The act iv i ty o f VAD has
been substant ia ted by others (647,648,649) . In fec t ion is the most important compl icat ion,
wi th 38% of pat ients having fever and 28%, a documented in fec t ious agent (391) . Ear ly
in t ravenous catheter removal may occur in ~16% of pat ients as a resul t o f thrombosis or
in fec t ion (258) .

Var iants o f VAD include reg imens that al ter the type or dose of cor t icostero id, schedule of
adminis t ra t ion, type of anthracycl ine used, as wel l as the addi t ion of o ther drugs. The
ef fec t iveness of VAMP (methylpredniso lone in p lace of dexamethasone) appears
comparable to VAD, wi th a response rate and overa l l surviva l o f 36% and 20 months,
respect ive ly, in pat ients wi th resis tant disease (260) . Browman et a l . (650) eva luated m-
VAD, in which a l l of the v incr is t ine and doxorubic in was g iven on day 1 over 2 hours and the
dexamethasone on days 1 to 4 and 15 to 18 on ly; the overal l response rate was 27% (95%
CI , 14 to 40%) wi th a median surviva l o f 7 .6 months. The authors expressed concern that
th is reg imen might be less ef fec t ive than s tandard VAD, but the conf idence interva ls o f the
response rate were large. In fac t , the same bolus schedule was used by Dimopoulos et a l .
(a lbe i t in newly d iagnosed pat ients) as one arm of a randomized t r ia l compar ing bo lus VAD
to DVD (VAD, but wi th l iposomal doxorubic in) . Outcomes were ident ical between the two
arms (406) .
Al ternat ive anthracycl ines have been t r ied, inc luding mitoxantrone (NOP or mitoxantrone,
v incr is t ine, and dexamethasone [MOD]) (651,652,653), which have resul ted in response
rates of 25 to 40% (651,653) epi rubic in (399,654) , and l iposomal doxorubic in (400). In one
randomized s tudy, pla teau durat ion was s ign i f icant ly longer in the VAD group than in the
MOD group, but there was no d i f ference in overal l survival (653) . Several invest igators have
added other drugs to the VAD base wi thout measurable benef i t . Concurrent in terferon
(427,655) adds nothing to response rate or overal l survival . In s ing le-arm s tud ies, there
does not appear to be any advantage to the addit ion of cyclophosphamide to VAD, VAMP, or
v incr is t ine, ep i rub ic in , and dexamethasone (VED) to y ie ld CVAD, hyperCVAD, C-VAMP, or
VECD (257,260,399,656,657) .
Novel Therapies for Relapsed or Refractory Disease
Thalidomide-Based Therapy for Relapsed or Refractory Disease
As has been ment ioned, s ing le-agent tha l idomide can induce a response in 25 to 58% of
re lapsed/ref rac tory pat ients (295,297,298,299,300,301,302,303,304) .There appears to be
synergy between thal idomide and dexamethasone (308,658). Response rates of 41 to 55%
(658,659,660,661) have been observed in pat ients wi th res is tant myeloma (Table 99.16) .
Doses of dexamethasone have ranged f rom 4 mg as a da i ly cont inuous dose (661) to 40 mg
on days 1 through 4 of each month (658,660). Dimopoulos et a l . (658) administered
dexamethasone for an addi t ional 8 days (days 9 to 12 and 17 to 20) in the f i rs t month only.
W ith these combinat ion reg imens, tha l idomide dose leve ls have ranged between 100 and
400 mg/day, wi thout any c lear dose–response effec t . Pat ients who are resis tant to
dexamethasone-based (658,659) or tha l idomide-based (662) reg imens may respond to the
combinat ion of these two agents . Coleman et a l . (663) described a 100% response rate for
re lapsed or ref rac tory d isease t reated wi th c lar i thromycin, low-dose tha l idomide, and
dexamethasone. These resul ts have yet to be substant ia ted by other invest igators, and
c lar i thromycin alone is not an effec t ive t reatment (350,351,352).
Invest igators have combined thal idomide wi th alkylators ei ther wi th
(664,665,666,667,668,669) or wi thout cor t icostero ids (670,671) , achieving overal l response
rates as high as 79%, inc lud ing complete response rates as h igh as 26%. Others have
added tha l idomide to anthracyc l ine-based therapies (452,454,672,673) .
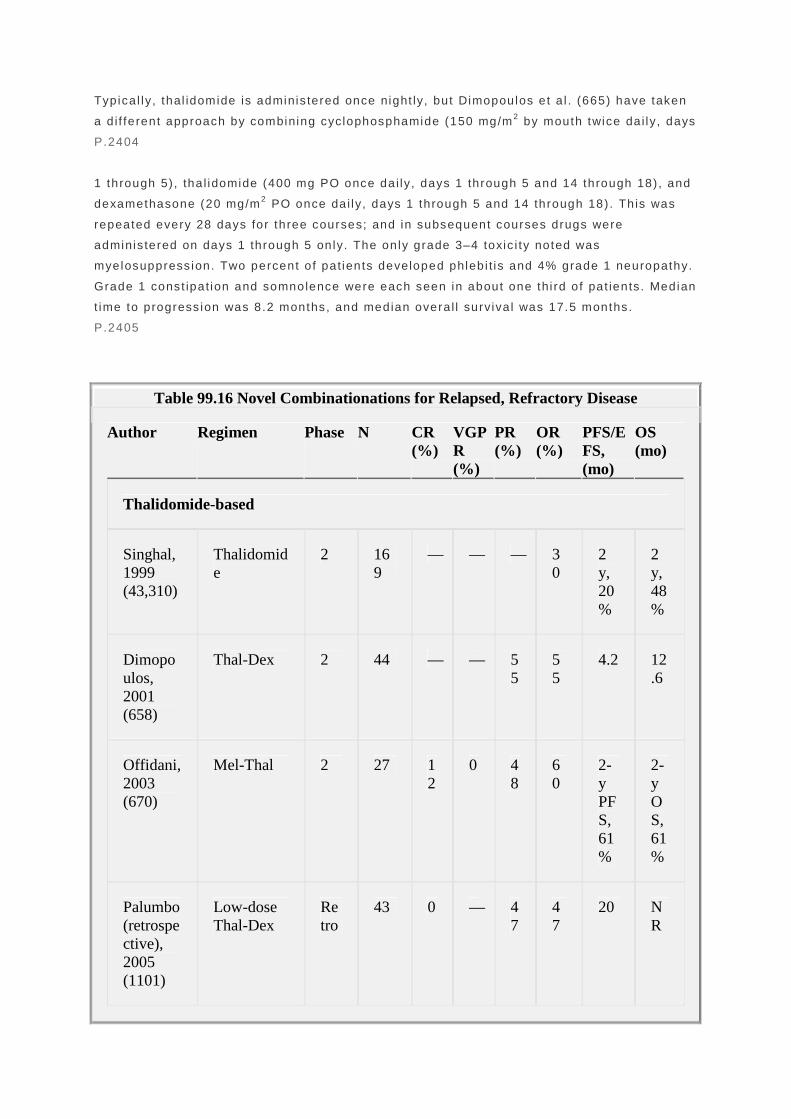
Typica l ly, thal idomide is adminis tered once night ly, but Dimopoulos et a l . (665) have taken
a d i f ferent approach by combining cyclophosphamide (150 mg/m 2 by mouth twice da i ly, days
P.2404
1 through 5) , tha l idomide (400 mg PO once dai ly, days 1 through 5 and 14 through 18) , and
dexamethasone (20 mg/m 2 PO once dai ly, days 1 through 5 and 14 through 18). Th is was
repeated every 28 days for three courses; and in subsequent courses drugs were
adminis tered on days 1 through 5 on ly. The only grade 3–4 toxic i ty noted was
myelosuppress ion. Two percent o f pat ients developed phleb i t is and 4% grade 1 neuropathy.
Grade 1 const ipat ion and somnolence were each seen in about one thi rd o f pat ients . Median
t ime to progress ion was 8.2 months, and median overa l l surviva l was 17.5 months.
P.2405
Table 99.16 Novel Combinationations for Relapsed, Refractory Disease
Author Regimen Phase N CR (%)
VGPR (%)
PR (%)
OR (%)
PFS/EFS, (mo)
OS (mo)
Thalidomide-based
Singhal, 1999 (43,310)
Thalidomide
2 169
— — — 30
2 y, 20%
2 y, 48%
Dimopoulos, 2001 (658)
Thal-Dex 2 44 — — 55
55
4.2 12.6
Offidani, 2003 (670)
Mel-Thal 2 27 12
0 48
60
2-y PFS, 61%
2-y OS, 61%
Palumbo (retrospective), 2005 (1101)
Low-dose Thal-Dex
Retro
43 0 — 47
47
20 NR

Hovenga, 2005 (671)
CTX Thal 2 38 11
0 64
75
30 20
Garcia-Sanz, 2004 (664)
CDT 2 71 2 0 53
55
2-y EFS, 57%
2-y OS, 66%
Dimopoulos, 2004 (665)
CDT 2 53 5 0 55
60
TTP 8.2
17.5
Kropff, 2003 (666)
CDT 2 60 3 0 65
68
11 19
Kyriakou, 2005 (667)
Low-dose CDT
2 52 17
0 62
79
— —
Sidra, 2006 (668)
CDT 2 47 0 19
63
83
— —
Palumbo, 2006 (669)
MPT IV 2 24 0 13
29
42
9 —
Zervas, 2004 (452)
T-DVD 2 39 10
10
64
84
— —
Hussein, 2006 (454)
T-DVd 2 49 20
24
31
75
15.5
39.9

Offidani, 2006 (673)
TDD 2 50 26
12
38
76
17 NR
Bortezomib-based
Richardson (SUMMIT), 2006 (321)
Bortezomib
2 193
4 6 18
28
7 17
Bortez-Dex (1.0 mg/m2)
2 27 0 19
19
37
TTP 10.9
26.7
Jagannath, 2004 (322)
Bortez-Dex (1.3 mg/m2)
2 26 0 4 46
50
TTP 7.0
NR
Bortezomib
3 315
6 7 25
38
6 1 y, 80%
Richardson, (APEX) 2005 (320)
Dex 3 312
1 1 16
18
— 1 y, 66%
Kropff, 2005 (1102)
Bortez-Dex 2 15 7 — 67
74
— —
Musto, 2006 (1103)
Bortezomib
2 21 10
0 33
43
— —
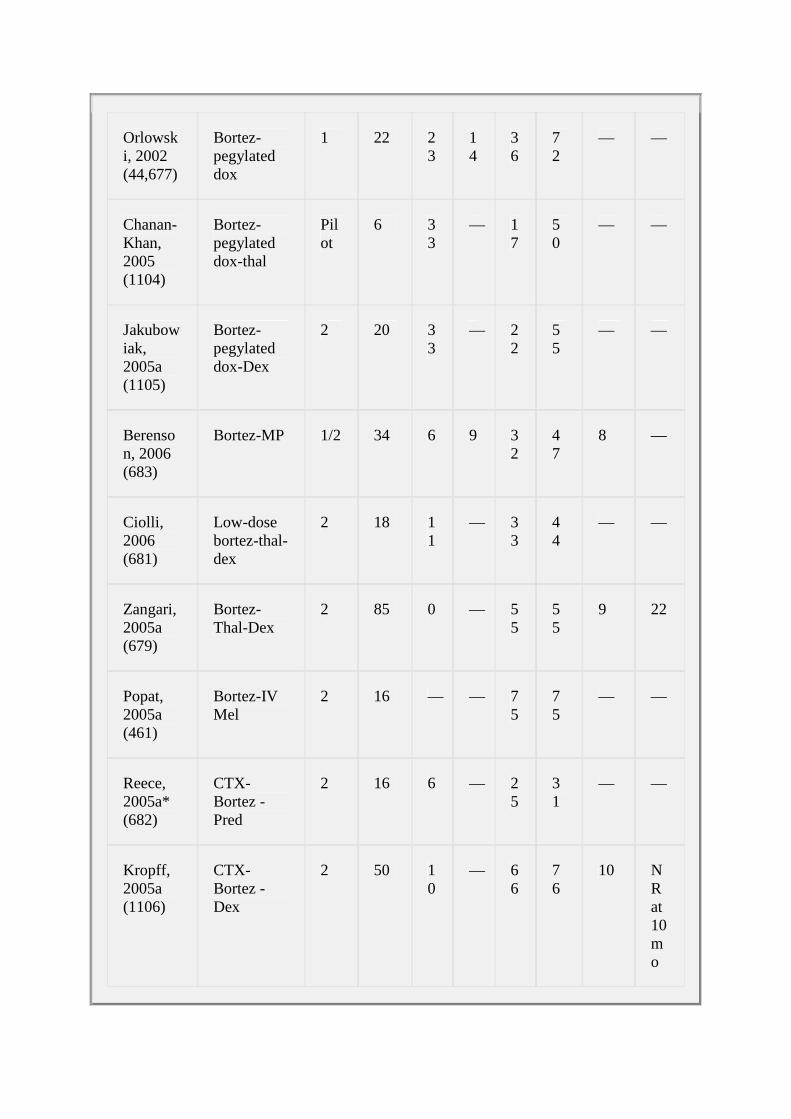
Orlowski, 2002 (44,677)
Bortez-pegylated dox
1 22 23
14
36
72
— —
Chanan-Khan, 2005 (1104)
Bortez-pegylated dox-thal
Pilot
6 33
— 17
50
— —
Jakubowiak, 2005a (1105)
Bortez-pegylated dox-Dex
2 20 33
— 22
55
— —
Berenson, 2006 (683)
Bortez-MP 1/2 34 6 9 32
47
8 —
Ciolli, 2006 (681)
Low-dose bortez-thal-dex
2 18 11
— 33
44
— —
Zangari, 2005a (679)
Bortez-Thal-Dex
2 85 0 — 55
55
9 22
Popat, 2005a (461)
Bortez-IV Mel
2 16 — — 75
75
— —
Reece, 2005a* (682)
CTX-Bortez - Pred
2 16 6 — 25
31
— —
Kropff, 2005a (1106)
CTX- Bortez -Dex
2 50 10
— 66
76
10 NR at 10 mo

Palumbo, 2005a (685)
Bortez-MP-Thal
1/2 20 10
10
35
55
— —
Terpos, 2005a (684)
Bortez-MD-Thal
2 25 8 — 48
56
— —
Teoh, 2006a (680)
Bortez-Thal-Dex
2 14 43
21
29
93
— —
Lenalidomide-based
Richardson, 2006 (316)
Lenalidomide
1 102
0 0 13
17
— —
Lenalidomide/dex
3 351/2
14
44
58
TTP 13.3
— Dimopoulos (MM-010), 2005a (688)
Dex 3 351/2
4 18
22
TTP 5.1
—
Lenalidomide/dex
3 177
59
TTP 11
— Weber (MM-090), 2006a (689)
Dex 3 177
21
TTP 4.7
24
Richardson, 2005a (317)
Lenalidomide
2 222
0 0 25
25
TTP 5.1
>15

Richardson, 2005 (693)
Bortez-Lenalid
1 19 5 5 42
53
— —
Gerecke, 2005a (692)
Lenalid-pegylated dox-Dex
1/2 6 100
— —
Baz, 2005a (691)
Pegylated dox-vincristine-Dex-Lenalid
1/2 45 13
11
35
59
— —
Other
Munshi, 2002 (327)
ATO 2 14 0 0 7 7 — —
Hussein, 2004 (328)
ATO 2 23 0 0 0 33b
— —
Abou-Jawde, 2006 (694)
ATO-Dex-AA
2 20 — — — 30
10.4
—
Berenson, 2006 (696)
MAC 2 65 2 0 23
26
7 19
Wu, 2005a (695)
ATO-Dex 2 20 0 0 13
13
— —
Berenson, 2006a (697)
ATO-Bortez-AA
1/2 22 9 0 9 18
— —

Baz, 2006a (456)
Dex/ATO/Thal/AA
2 16 0 0 25
25
9.4 —
AA, ascorbic acid; ATO, arsenic trioxide; Bortez, bortezomib; CDT, cyclophosphamide, dexamethasone, thalidomide (several different schedules); CR, complete response; Dex, dexamethasone; EFS, event-free survival; IFN, interferon; Lenalid, lenalidomide; MAC, melphalan, ATO, AA; MD, melphalan, dexamethasone; mo, months; MP, melphalan, prednisone; MPT IV, intravenous melphalan, prednisone, thalidomide; N, number of patients; NR, not reached; OR, overall response rate; OS, overall survival; PFS, progression-free survival; PR, partial response; Retro, retrospective analysis; TDD, thalidomide, pegylated doxorubicin, dexamethasone; T-DVD, thalidomide, pegylated doxorubicin, vincristine, dexamethasone; T-DVd, T-DVD, but low dose dexamethasone; Thal, thalidomide; TTP, time to progression; VGPR, very good partial response; y, years. aAbstract only. bMinimal response.
Most programs a lso include cort icostero ids . Two except ions are the protocols o f Hovenga et
a l . (671) and Of f idani (670) . Hovenga et al . (671) t reated 38 pat ients wi th cont inous low-
dose cyc lophosphamide (100 to 150 mg) and thal idomide (maximum dose of 400 mg).
Median doses of thal idomide and cyclophosphamide were 100 and 95 mg/day, respect ively.
Sixty- four percent of pat ients achieved a response (wi th 11% CR). W ith a median fol low-up
of 22 months, median PFS and OS were 30 and 20 months, respect ive ly. The most common
s ide ef fec ts were drowsiness, neurotoxic i ty, and const ipat ion wi th grade 3–4 rates in 20, 16,
and 13% of pat ients , respect ive ly. One pat ient developed a DVT. Two pat ients died af ter
grade 4 in fect ions. One pat ient developed secondary acute myeloid leukemia. Of f idani e t a l .
(670) t reated 27 pat ients wi th n ight ly thal idomide (100 to 600 mg) and melphalan 0.2
mg/kg/day for 4 days every 28 days unt i l maximum response or toxic i ty. Overa l l response
rate was 60%, includ ing 12% complete responses. At a median fo l low-up of 15 months, both
the 2-year PFS and OS were 61%. The main s ide ef fects were const ipat ion (82%),
somnolence (41%), fa t igue (22%), sensory per ipheral neuropathy (56%), deep venous
thrombosis (11%), and grade 3 leukopenia (30%). However, no severe in fec t ions occurred.
Moehler e t a l . added etoposide to tha l idomide, cyc lophosphamide, and dexamethasone and
reported a 68% response rate in relapsed and ref ractory pat ients (674); th is program was
associated wi th a 36% rate of severe infec t ions.
DT-PACE is a combinat ion of f ive drugs (Table 99.3) and is an in tegral par t of Tota l
Therapy 2 and 3, p i lo ted by Bar log ie and col leagues at the Univers i ty o f Arkansas. Lee et a l .
(672) descr ibed thei r exper ience using this combinat ion in 236 previously t reated pat ients
pr ior to s tem cel l col lect ion. Near ly two th i rds (n = 148) had shown progressive disease
af ter the i r pr ior therapy. Af ter two to four cyc les of DT-PACE, of the 229 evaluable pat ients ,
21 pat ients ach ieved a CR, 29 pat ients a nCR, and 44 pat ients a PR. Response was not
a f fec ted by chemosensi t iv i ty to preceding chemotherapy. The most common grade 3–4
toxic i t ies were myelosuppress ion (39%), neutropenic fever (9%), nausea and vomit ing (6%),

stomati t is (4%), and thromboembol ism (5%). Treatment- rela ted mortal i ty was 4%. Of note,
before rout ine thrombosis prophylaxis , thromboembol ic events occurred in 37% of cyc les
(one th ird o f which were l ine-associa ted thromboses) .
Of f idani e t a l . (673) t reated 50 previously unt reated pat ients wi th ThaDD, a combinat ion of
tha l idomide (100 mg dai ly) , pegyla ted l iposomal doxorubic in (40 mg/m2 on day 1 every 28
days) , and dexamethasone (40 mg PO on days 1 to 4 and 9 to 12) . Twenty-s ix percent o f
pat ients ach ieved a complete response, 6% a near-complete response, 6% a very good
par t ia l response, and 38% a par t ia l response, for an overa l l response rate of 76%. The
median event- f ree surviva l was 17 months, and the median overa l l surviva l has not been
reached. Grade 3 nonhemato log ic toxic i ty occurred in 12% of pat ients , thromboembol ic
d isease in 12%, and severe in fec t ion in 16%.
Hussein et a l . (454) t reated 55 pat ients wi th DVd-T (same as Of f idani , except that
dexamethasone was g iven on only 4 days per cycle) for a maximum of eight cycles , fo l lowed
by maintenance wi th maximum tolerated doses of thal idomide plus al ternate-day oral
prednisone. Though response rates were high (OR 75%, wi th 20% CR), there was
substant ia l toxic i ty assoc iated wi th the program. Grade 3–4 toxic i t ies included
thromboembol ic events in 25%, per iphera l neuropathy in 22%, neutropenia in 14%,
pneumonia in 12%, palmar/plantar erythrodysesthesia in 8%, and thrombocytopenia in 5%.
The median PFS was 15.5 months, and the OS was 39.9 months.
Bortezomib-Based
Therapies for Relapsed or Refractory Disease. Single-agent response rates in
re lapsed/ref rac tory myeloma range f rom 28 to 38%, wi th a median response durat ion of 8
months (319,320,321,322) (Table 99.16) . In v i t ro, there is s igni f icant synergy between
bor tezomib and both chemotherapy (675) and ioniz ing radia t ion (676) . Cl in ica l t r ia ls
exp lo i t ing th is synergy are beginn ing to emerge and are described in the fo l lowing.
Or lowks i e t a l . (44,677) treated 24 pat ients in thei r Phase I t r ia l of bor tezomib plus
l iposomal doxorubic in. Sixty-seven percent of thei r pat ients achieved a PR or bet ter , wi th a
CR rate of 21%. Grade 3 or 4 adverse events seen in a t least 10% of pat ients included
thrombocytopenia (43%), lymphopenia (40%), neutropenia (17%), fat igue (14%), pneumonia
(14%), per iphera l neuropathy (12%), febr i le neutropenia (10%), and d iarrhea (10%).
Zangar i e t a l . (678,679) have pre l iminari ly reported the i r exper ience wi th bor tezomib,
tha l idomide, and dexamethasone (VT + D). In a Phase I t r ia l wi th a 2 ×2 des ign, they
escalated bor tezomib and tha l idomide doses. I f no part ia l response was seen af ter three
cyc les of VT, dexamethasone was added (20 mg the day of and af ter bortezomib dosing) .
The overa l l response rate was 55%; EFS and OS were 9 and 22 months, respect ive ly.
Myelosuppress ion was the most common grade 3–4 toxic i ty. Per iphera l neuropathy
worsened above basel ine in 5 to 9% of these heavi ly pret reated pat ients . In another s tudy
presented in abst rac t form, addi t ion of bor tezomib to thal idomide and dexamethasone
increased the complete response rate f rom 7.7 to 42.9% (680) .
Cio l l i e t al . (681) exp lored the reg imen LD-VTD (Velcade/bor tezomib 1.0 mg/m 2 on days 1, 4,
8 , and 11 every 28 days; dexamethasone 24 mg on days 1, 2 , 4 , 5 , 8 , 9, 11, and 12; and
tha l idomide 100 mg each evening) for up to e ight cyc les . Pat ients rece ived therapeut ic
warfar in as DVT prophylaxis . The overal l response rate was 41%, wi th 11% of pat ients
achieving a CR. After a median fol low-up of 11 months, 6 pat ients had died.

Reece et a l . (682) have treated 16 pat ients wi th bor tezomib, cyc lophosphamide, and
prednisone as par t o f an ongoing Phase I s tudy. Pre l iminary in format ion suggests that there
is ac t iv i ty wi th th is program. So far , the overal l response rate is 31%, including one pat ient
wi th a near-complete response.
Berenson et a l . (683) have t reated 35 pat ients wi th relapsed, re f rac tory myeloma in a Phase
I / I I t r ia l combin ing bor tezomib and melphalan. Thei r maximum to lerated dose is a maximum
of eight 28-day cyc les of bor tezomib 1.0 mg/m2 o n days 1, 4 , 8, and 11, and melphalan 0.1
mg/kg on days 1 through 4. The overal l response rate was 47%, includ ing a combined
CR/VGPR rate of 15%. The authors emphasize that f ive of the s ix pat ients t reated had a
response to therapy. The main s ide ef fects were severe myelosuppress ion, fat igue, and
per iphera l neuropathy. Pat ients have suf fered f rom nausea, vomit ing, d iarrhea, const ipat ion,
fever , and rash.
Terpos et al . (684) have t reated 31 pat ients wi th re lapsed or ref rac tory myeloma wi th VMDT,
a combinat ion of bor tezomib (1 .0 mg/m 2 on days 1, 4 , 8 , and 11) , melphalan (0.15 mg/kg on
days 1 to 4) , dexamethasone (12 mg/m 2 on days 1 to 4 and 17 to 20, and tha l idomide (100
mg dai ly) . Pat ients were t reated for up to eight 28-day cycles . In thei r pre l iminary repor t on
25 of these pat ients , 56% achieved an ob ject ive response, inc luding 8% wi th a complete
response. Adverse events included fa t igue (56%), thrombocytopenia (12% grade 3/4) ,
neutropenia (8% grade 3/4) , anemia (8% grade 3), neuropathy (48% grade 1/2, no grade 3/4
observed) , infec t ions (36%, including two herpes zoster cases) , and hyponatremia (12%).
No pat ient exper ienced a DVT, whi le two pat ients died as a resu l t o f seps is .
In a Phase I s tudy, Palumbo et a l . (685) t reated 20 pat ients wi th VMPT, a combinat ion of
ora l melphalan (6 mg/m 2 on days 1 to 5), prednisone (60 mg/m2 on days 1 to 5) , and
tha l idomide (100 mg cont inuous ly) wi th dose escalat ions of bor tezomib (dose levels ranging
f rom 1 to 1.6 mg/m 2 admin is tered on days 1, 4 , 15, and 22 of each 5-week cyc le). A fu l l
course was def ined as s ix cyc les . Ten pat ients had a response, including two complete
responses, one near-complete response, and seven part ia l responses. Herpes zoster was a
common compl icat ion wi thout acyc lovir prophylaxis .
Other in terest ing combinat ions being explored inc lude samarium Sm153 lexidronam (a
bone-seeking rad ionuc l ide) and bortezomib (686) ; and the combinat ion of bor tezomib,
melphalan, and pegylated doxorubic in (687).
P.2406
Lenalidomide-Based Therapy for Relapsed or Refractory Disease
. Us ing lenal idomide as a s ingle agent , ~18 to 25% of re lapsed or re f rac tory pat ients
achieved a par t ia l response, and the median durat ion of response for responding pat ients
was 20 months (316,317) (Table 15). In a randomized Phase I I t r ia l of lenal idomide, the
addi t ion of dexamethasone (40 mg on days 1 to 4 and 15 to 18) for pat ients not responding
to 2 months of lenal idomide resul ted in part ia l response rates in an addit ional 22% of
pat ients (316) . The combinat ion of lenal idomide and dexamethasone has been studied in
two large Phase I I I t r ia ls (688,689) . The resul ts of the two t r ia ls were comparable, wi th 59%
of pat ients responding to the combinat ion, inc lud ing a 14% complete response rate. Th is
was s ign i f icant ly bet ter than what was observed wi th s ing le-agent dexamethasone (PR
22.5% and CR 2%). In addi t ion, both t ime to progress ion (11 to 13 months vs . ~5 months)

and overal l survival (not reached vs . 24 months) were super ior in the
lenal idomide/dexamethasone arm. A subgroup analysis was per formed to assess the effec t
o f pr ior therapy wi th thal idomide (690). Regardless of whether thal idomide had been used
previously, the lenal idomide/dexamethasone arm outper formed dexamethasone on al l
metr ics . However, there was a t rend toward bet ter lenal idomide/dexamethasone
per formance in pat ients who had not rece ived prior tha l idomide: CR (17.6 vs . 8.1%); and
TTP (13.6 vs . 8 .5 months) .
Baz et al . (691) have t reated 45 re lapsed, ref rac tory pat ients who were evaluable for
response wi th DVd-R (s tandard DVd plus lenal idomide 10 mg dai ly) for four to s ix cyc les ,
fo l lowed by lenal idomide and prednisone. Six had a CR (13%), 5 had a nCR (11%), and 16
had a PR (35%). Most common toxic i t ies were myelosuppression, in fec t ion, and
thromboembol ic events. W ith a median fo l low-up of 7 .3 months, 23 pat ients progressed and
16 died.
A number o f combinat ions are be ing explored, including lenal idomide, doxorubic in , and
dexamethasone (692) ; and lenal idomide, bor tezomib, and dexamethasone (693) . Both
combinat ions are showing evidence of ac t iv i ty.
Arsenic Trioxide Combinations for Relapsed or Refractory Disease
As a s ingle agent , arsenic t r ioxide (ATO) resu l ts in part ia l response rates of about 7%
(327); i f 25% reduct ion in the M-prote in concentrat ion is inc luded as “ response,” the rates
are as h igh as 33% (328) (Table 99.15). The combinat ion of dexamethasone, ATO, wi th and
wi thout ascorb ic ac id , resu l ted in response rates of 30 (694) and 13% (695) , respect ive ly.
Melphalan, ATO, and ascorbic ac id (MAC) provided a 26% response rate (696). Early
resul ts wi th other combinat ions are shown in Table 99.16 (456,697) .
Other Agents for Relapsed or Refractory Disease In terferon has been shown to modulate the mult idrug res is tance phenotype and to re induce
chemosensi t iv i ty in pat ients wi th chemores is tant mult ip le myeloma. In one s tudy,
nonresponding pat ients received the same chemotherapy to which they were res is tant ,
preceded by a 5-day course of in ter feron. An ob ject ive response was achieved in 4 of 14
pat ients (28.6%) (698) .
Severa l invest igators have combined in terferon wi th dexamethasone (402,699) or
methylpredniso lone (700) as therapy for pat ients wi th re lapsed or re f rac tory d isease. W ith
response rates of 29 to 66% (699,700) i t is d i f f icu l t to iso late the cort icosteroid and
in ter feron ef fec ts . There is no c lear evidence that the response rate or the survival t ime
improved compared wi th s imi lar treatments wi thout in terferon (655).
Because pat ients wi th mul t ip le myeloma ref rac tory to a lkylat ing agents f requent ly express
P-g lycoprote in , which is associated wi th the mult idrug res is tance phenotype, cyc losporine, a
mult idrug res is tance reversal agent , has been combined wi th VAD in pat ients wi th ref rac tory
or progress ive d isease. No benef i t was observed (701,702) . As a resul t of the f indings of a
Phase I / I I t r ia l in pat ients wi th myeloma (703) , PSC 833, a mul t idrug-res is tance glycoprote in
modulator , has been incorporated in to a smal l Phase I I I study of VAD versus VAD and PSC
833 in the re lapsed/ref rac tory sett ing (704). There was no d i f ference in response rate,
progress ion- f ree survival , or overa l l survival in the PSC 833 arm, though there was more
toxic i ty.

The human ant i -CD20 ant ibody has demonstrated some ef fec t in pat ients wi th myeloma.
About 20% of pat ients wi th myeloma have CD20 express ion on the i r plasma ce l ls . In one
s tudy, 1 o f 19 pat ients had a part ia l response to therapy; an addit ional 5 had s tab le disease
(705).
Because vascular endothel ia l growth factor has been shown to be involved in myeloma
pathogenes is (706), severa l invest igators have evaluated d i f ferent ant i -VEGF therapeut ic
s t rategies. Somlo et al . (707) have explored the ro le o f the ant i -VEGF ant ibody rhuMAB
bevacizumab versus bevac izumab and thal idomide in a randomized Phase I I t r ia l . Twelve
pat ients have been enro l led. Median t ime to progress ion for the 6 pat ients t reated wi th
bevacizumab a lone was 2 ( range 1 to 4) months. Progress ion- f ree survival for the 5
evaluable pat ients t reated wi th bevac izumab and thal idomide was 6 +, 7, 8 +, 10, and 30 +
months, wi th 2 pat ients st i l l on study and in response. Zangar i e t a l . have evaluated
SU5416, a smal l -molecule VEGF receptor-2 inhibi tor , in 27 pat ients wi th myeloma in a
mult icenter Phase I I s tudy (708) . Grade 3/4 toxic i t ies were rare ly observed; the most
f requent was thrombocytopenia (12%). There were three thromboembol ic ep isodes and f ive
cases of new-onset hyper tens ion. There were no ob ject ive responses, and overa l l median
surviva l was 42 weeks ( range, 3 to >92 weeks) . A decrease in median VEGF p lasma leve ls
was observed in pat ients wi th s tab le disease (n = 7) compared to pat ients wi th progressive
d isease (n = 5) .
The Hsp 90 chaperone inh ib i tor 17-AAG is showing promise in combinat ion wi th bor tezomib
in myeloma pat ients . In a Phase I t r ia l , Chanan-Khan et a l . t reated 20 pat ients (709) . Of the
12 bor tezomib-ref rac tory pat ients , one pat ient had a near-complete response and another
f ive had a 25% reduct ion in thei r serum M prote in.
Radiation Therapy As ear ly as the mid-1920s there was recogni t ion that externa l -beam radiat ion therapy could
promote immediate rel ief o f pa in , heal ing of patho log ic f rac tures, and resolut ion of
ext ramedul lary p lasmacytomas (25,710,711) . Unt i l the 1950s, radia t ion therapy was the only
e f fec t ive t reatment avai lab le for the management o f plasma ce l l tumors. W ith the advent o f
sys temic chemotherapy, indicat ions for i r rad ia t ion were pr imar i ly pa l l ia t ion of bone pain and
so l i tary p lasmacytomas. Concern for mainta ining bone marrow reserve a lso constrains the
use of radia t ion in pat ients wi th mul t ip le myeloma. Sykes et al . (712,713) showed that
rad ia t ion has long-term ef fec ts on the bone marrow; the major i ty o f pat ients rece iv ing
concentrated local doses of 3,500 cGy or more showed pers is tent loca l ized marrow aplasia .
One must admin is ter enough radia t ion to provide pa l l iat ion, wi thout jeopard iz ing
opportun i t ies for fur ther systemic therapy. In a ret rospect ive review, Norin (714) has found
that objec t ive improvement was lacking when the tumor dose was below a cumulat ive dose
(s ing le-dose equivalent ) o f 1 ,000 cGy. For pa l l ia t ion, the recommendat ion is therefore a
cumulat ive dose of 1 ,500 cGy, corresponding to a tumor dose of 3 ,400 cGy, in 10 to 15
f ract ions (714,715) . Leigh et a l . (716) recommended a to tal cumulat ive dose of 1 ,000 cGy in
these same pat ients. There is controversy as to whether the durat ion of response corre la tes
wi th the radia t ion dose in myeloma pat ients (716,717).
In contrast , the convent ional wisdom has been that pat ients wi th sol i tary p lasmacytoma of
bone should rece ive h igher doses in an at tempt a t cure. Al though the opt imal dose has not
been estab l ished by randomized control led tr ia ls, 4 ,000 to 5 ,000 cGy encompass ing a l l

disease wi th a marg in of normal t issue is recommended by most exper ts (718,719,720). A
recent s tudy of 203 pat ients wi th so l i tary plasmacytoma of bone has brought this pr inc iple
in to quest ion (721). These authors found that therapeut ic doses >3,000 cGy had no bear ing
on loca l control .
P.2407
Radiat ion can often spare pat ients f rom undergoing surgery (722) . In a recent ret rospect ive
analys is of 35 cases of pat ients wi th cervica l les ions and sp ina l ins tab i l i ty , i t was found that
19 of the 20 pat ients exper ienced resolut ion of pain , 15 of whom received rad ia t ion a lone.
Of the 10 pat ients wi th suf f ic ient fol low-up data, none showed c l in ical progress ion of
instabi l i ty .
Sequential Half-Body (Hemibody) Irradiation The f i rs t report of us ing whole-body i r rad ia t ion to t reat myeloma was by Medinger and
Craver (723) in 1942. Par t ia l or complete re l ie f o f pa in was noted in the majori ty o f pat ients .
Once ef fec t ive systemic chemotherapy came in to wide use, th is approach became less
popular unt i l 1971, when Bergsagel (724) postu lated that sequential hemibody rad ia t ion
could be a means of debulk ing tumor. He suggested that i f a dose of ~725 cGy were g iven
to the upper ha l f o f the body and 1,000 cGy to the lower ha l f , a theoret ical 3- log k i l l cou ld
be achieved and surviva l prolonged. Af ter a ser ies of re trospect ive s tudies
(606,725,726,727,728,729,730,731,732) and a randomized study (390,733) eva luat ing i ts
ro le in the ear l ier phases of myeloma, hemibody i r radia t ion has once again fal len out o f
favor . In pat ients who have end-s tage d isease, wi th poor pa in control , th is t reatment may
s t i l l be important.
The majori ty o f ser ies invo lv ing hemibody or sequential hemibody radia t ion are
re t rospect ive and inc lude pat ients who were ei ther res is tant to or relaps ing f rom a lkylator-
based therapy. Signi f icant rel ie f of bone pain occurred in 80 to 90% of pat ients
(606,725,726,727,728,729,730,731,732) , and the median durat ion of surviva l was 5 to 11
months (715,727) Object ive b iochemica l response occurred in 25 to 50% of pat ients
(606,727,734) . Pain rel ief typ ica l ly occurred 1 to 2 days after ins t i tu t ion of therapy, wi th a
maximal response in 1 to 2 weeks (725) . The most common s ide ef fec ts were moderate
myelosuppress ion, pneumoni t is , nausea, vomit ing, diarrhea, and s tomat i t is (715,725) . I f an
ora l lead shie ld was not used, mucos i t is a lso occurred (715) . Nadirs occurred wi thin 3
weeks (727), and whi te ce l l count and pla te le t count recovery occurred by about 6 weeks
(715,727) . Decrements in pulmonary funct ion occurred in about ha l f o f the t reated pat ients
(715). The most serious compl icat ion was radia t ion- induced pneumoni t is , which was seen in
14% of pat ients (727) . The opt ion of sequent ia l ha l f -body rad ia t ion therapy must be
ba lanced against unpredic tab le and varying degrees of pancytopenia and a l ternat ive
t reatment opt ions (734).
Bergsagel 's postu late (724) and prel iminary data f rom several smal l s tud ies (726,730,731)
led two cooperat ive group s tudies (SW OG 8229 and CALGB 8003) to incorporate systemic
rad ia t ion therapy as consol idat ion therapy (390,733) . Nei ther s tudy demonstrated a
meaningful advantage to pat ients rece iv ing ad juvant hemibody rad ia t ion (390,733) , and
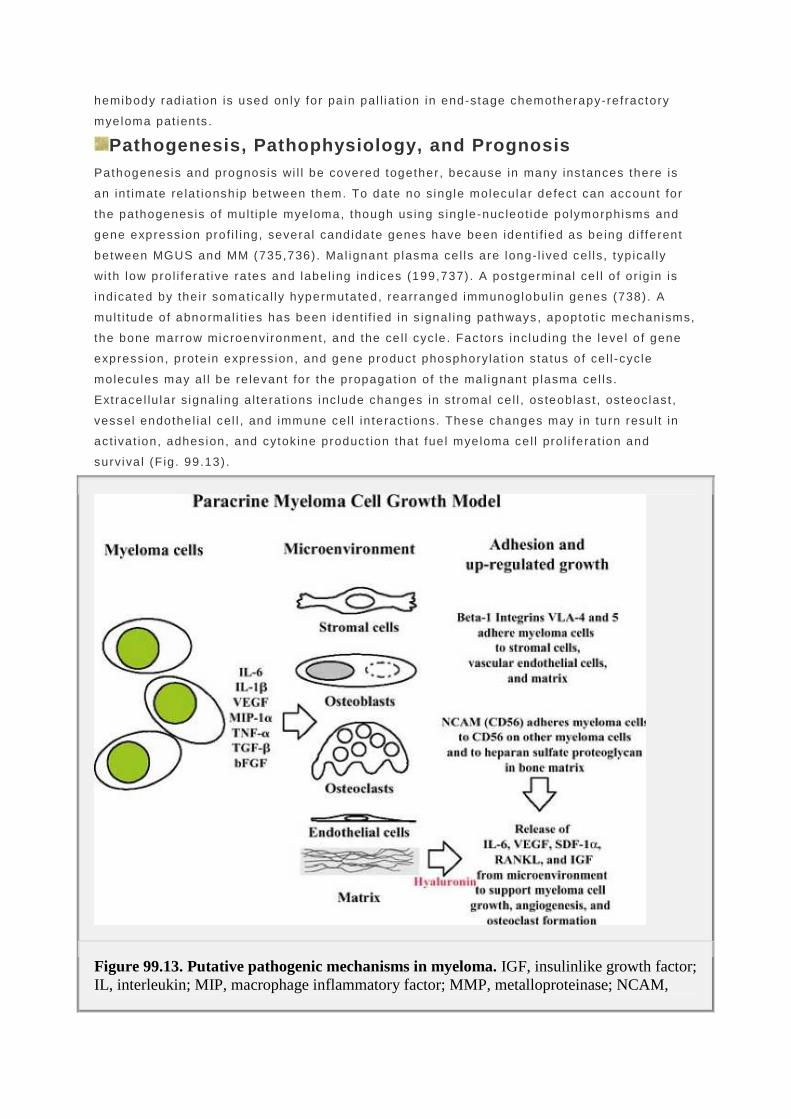
hemibody rad iat ion is used only for pa in pal l ia t ion in end-stage chemotherapy-ref ractory
myeloma pat ients .
Pathogenesis, Pathophysiology, and Prognosis Pathogenesis and prognos is wi l l be covered together, because in many ins tances there is
an in t imate re la t ionship between them. To date no single molecular defect can account for
the pathogenes is o f mult ip le myeloma, though us ing s ing le-nuc leot ide polymorphisms and
gene express ion prof i l ing, several candidate genes have been ident i f ied as be ing d i f ferent
between MGUS and MM (735,736) . Mal ignant plasma ce l ls are long-l ived ce l ls, typ ical ly
wi th low pro l i ferat ive ra tes and label ing ind ices (199,737) . A postgerminal ce l l o f or ig in is
indicated by the i r somat ica l ly hypermutated, rearranged immunoglobul in genes (738) . A
mult i tude of abnormal i t ies has been ident i f ied in s ignal ing pathways, apoptot ic mechanisms,
the bone marrow microenvi ronment , and the ce l l cyc le . Factors including the leve l o f gene
express ion, prote in express ion, and gene product phosphoryla t ion s ta tus of ce l l -cycle
molecules may al l be re levant for the propagat ion of the mal ignant p lasma ce l ls .
Ext race l lu lar s ignal ing a l terat ions inc lude changes in st romal ce l l , os teoblast , os teoclas t ,
vessel endothel ia l cel l , and immune ce l l in teract ions. These changes may in turn resu l t in
ac t ivat ion, adhes ion, and cytok ine product ion that fue l myeloma ce l l pro l i ferat ion and
surviva l (F ig . 99.13) .
Figure 99.13. Putative pathogenic mechanisms in myeloma. IGF, insulinlike growth factor; IL, interleukin; MIP, macrophage inflammatory factor; MMP, metalloproteinase; NCAM,

neural cell adhesion molecule; TNF, tumor necrosis factor; VEGF, vascular-derived endothelial growth factor; VLA, very late antigen.
Bone Marrow Microenvironment There is a synerg is t ic , patholog ic rela t ionship between myeloma ce l ls and the ce l ls
compr is ing the bone marrow microenvironment , inc luding f ibroblasts , os teoblasts, and
osteoc lasts . The s t romal cel ls in the marrow of myeloma pat ients produce h igh leve ls of
in ter leukin-6 ( IL-6) in v i t ro (739) . The IL-6 serves as a growth and survival fac tor for benign
and mal ignant plasma cel ls, which produce IL-1β (740,741) , VEGF, and macrophage
in f lammatory protein-1α (MIP-1α ) (742,743) . In turn, IL-1β and MIP-1α regulate and act ivate
osteoc lasts (740,744,745) .
A cel l adhesion molecule be longing to the immunoglobul in super family, CD56 (N-CAM), is
s t rongly expressed in most p lasma cel ls of myeloma pat ients (746) and is be l ieved to p lay a
ro le in myeloma homing and cel l adhesion to the marrow. Increased levels o f the adhes ion
molecules lymphocyte funct ion–associated ant igen (LFA)-3 (212) , LFA-1 (CD11a) (747) , and
very la te ant igen-4 (VLA-4) are expressed on the myeloma ce l ls in the major i ty o f pat ients .
VLA-4 may act to b ind myeloma ce l ls to f ibronect in in bone marrow (748) , which under
appropr ia te condi t ions can s ign i f icant ly increase IL-6 product ion by s t roma (749) . Cel l–ce l l
contact between marrow s t romal ce l ls and myeloma cel ls v ia VCAM-1 and α4β1 - in tegr in
enhances product ion of os teoc las t -s t imulat ing act iv i ty (750) . Hyaluronan, a
g lycosaminoglycan component of the bone marrow ext race l lu lar matr ix, appears to be a
surviva l and pro l i ferat ion factor for myeloma ce l ls (751) . Notch receptors are expressed in
ear ly hematopoiet ic s tem ce l ls , and Notch l igands are expressed on bone marrow s tem cel ls
(BMSCs). Myeloma cel ls expressing Notch receptors are act ivated by the BMSC Notch
l igand, protect ing the myeloma cel ls f rom drug- induced apoptos is . In addi t ion, th is
in teract ion also act ivates Notch s ignal ing in BMSCs, leading to secret ion of IL-6, VEGF, and
IGF-1 (752).Cel l -adhes ion drug resis tance (CAM-DR) is a wel l - recognized ent i ty (753) .
The endothel ia l microvascular environment has a lso been shown to be important in mult ip le
myeloma b io logy (201) . There
P.2408
is a high correla t ion between the extent of bone marrow angiogenes is , eva luated as
microvessel area, and the prol i ferat ing (S-phase) f rac t ion of marrow p lasma cel ls in pat ients
wi th mul t ip le myeloma and in those wi th MGUS (201,754,755) . VEGF plays an important role
in angiogenes is by act ing as a potent inducer o f vascular permeabi l i ty as wel l as serving as
a spec i f ic endothel ia l ce l l mi togen. Plasma cel ls in the bone marrow f rom mult ip le myeloma
pat ients express VEGF (756,757) , which can thereby interact wi th the Fl t -1 and KDR high-
af f in i ty VEGF receptors that are h igh ly expressed on bone marrow myelo id and monocyt ic
ce l ls surrounding the tumor (754) .
Invest igators are beginning to unders tand the complex in teract ions between osteoclasts ,
os teoblasts, and myeloma ce l ls . The receptor act ivator of NFκB (RANK), which is found on
osteoc lasts , in teracts wi th RANK l igand (RANKL) found on osteoblasts and bone marrow
s t romal ce l ls. These in teract ions contr ibute to bone destruc t ion (758) . Myeloma cel ls also
prevent d i f ferent ia t ion of os teoblasts through secret ion of the Wnt-s ignal antagonist DKK1

(759). MIP-1a is produced by myeloma cel ls and serves as an inducer o f os teoc las t
format ion (760) . In turn, os teoc las ts produce a number of fac tors that s t imulate myeloma
ce l ls, including IL-6 (141) .
Cytokines and Cell Signaling The search for a growth fac tor for myeloma ce l ls cu lminated in the ident i f icat ion of IL-6,
former ly known as B-cel l growth fac tor or hybridoma growth fac tor (761). IL-6 is among the
most important prol i ferat ion and surviva l fac tors in myeloma (762). Predominant ly produced
by bone marrow s tromal ce l ls—macrophages, f ibrob lasts , osteoblasts , osteoclas ts , and
monocytes (F ig. 99.13) (763)—it serves as a growth fac tor and as an ant iapoptot ic fac tor
(764,765,766,767). In the majori ty of cases, myeloma ce l ls and cel l l ines are capable of
producing IL-6 and the IL-6 receptor , resu l t ing in autocrine st imulat ion (764,765,766,767) .
IL-6 t ransmi ts messages in t race l lu lar ly through the s ignal - t ransduc ing prote in gp130, which
can act ivate two pathways: the JAK-STAT pathway (768) and the Ras-MAP k inase pathway
(769). Through the former pathway, which inc ludes JAK-2 and STAT3, the ant iapoptot ic
proteins Mcl -1 (768) and Bc l -XL (770) are up-regulated; through the la t ter pathway,
t ranscrip t ion fac tors such as ELK-1, AP-1, and NF-IL-6 (768) are up-regulated. NF-κB (771)
and IL-6 (772,773) may a lso mediate the observed increase in the ant iapoptot ic proteins
Bc l -2 (774,775), Mcl -1 (772) , and Bcl -XL (772,773,776,777) . The overal l e f fec t o f these
pathways is prevent ion of apoptosis and enhancement o f mul t ip le myeloma prol i ferat ion. In
addi t ion, the const i tu t ive act ivat ion of STAT3 may a lso be important in the pathogenesis o f
mult ip le myeloma, independent o f IL-6 (778) . Moreover , CD40 act ivat ion of myeloma cel ls
can a l ter the cel l sur face phenotype, t r iggering autocr ine IL-6 secret ion regulat ing myeloma
ce l l cyc le in a p53-dependent fashion (779) .
Other cytokines and growth fac tors produced by myeloma and st romal ce l ls that maintain
myeloma growth (780) inc lude IL-1β (781,782,783) , VEGF, insul in l ike growth fac tor ( IGF)
(784,785,786,787,788,789) , and tumor necros is fac tor-α (790,791). Aberrant expression of
IL-1β may be a cr i t ical s tep in the trans i t ion of MGUS to mul t ip le myeloma (740,783). IL-1β
up-regulates product ion of IL-6, changes expression of cel l adhesion molecules, and has
been shown to have osteoc last -ac t ivat ing fac tor ac t iv i ty. A l though IL-1β does not st imulate
myeloma ce l l prol i ferat ion d irect ly, by v i r tue of i ts e ffec t on s t romal ce l ls in the marrow i t
induces product ion of IL-6 (741) and IL-8 (792) . Myeloma ce l ls are capable of express ing
and secret ing VEGF and responding to the cytok ine in an autocr ine fash ion (742,743).
Moreover , s t romal and microvascular endothel ia l ce l l exposure to VEGF induces an
increase in IL-6 secret ion (742) , which then fur ther st imulates myeloma ce l ls . The prec ise
ro le that basic f ibroblast growth fac tor (bFGF), another potent angiogenic factor , p lays in
the growth of myeloma ce l ls is under ac t ive invest igat ion (793). Higher bFGF leve ls have
been found in more advanced s tages of mul t ip le myeloma (793) . IGF, which is bel ieved to
s ignal through the phosphat idyl inos i to l -3 ′-k inase (PI-3K) pathway (784) , is capable of
d i rec t ly s t imulat ing myeloma ce l l growth and enhancing myeloma cel l respons iveness to IL-
6 through mi togen-act ivated prote in k inase (787) and a lso inhibi t ing apoptos is by increasing
express ion of BAD (784).
Cell Cycle Regulatory s ignals underly ing prol i ferat ion of myeloma ce l ls inc lude increased cycl in D1
express ion, hypermethyla t ion of the cyc l in-dependent k inase (CDK) pathway regulatory

gene p16 (794), mutat ions of the ras oncogene (795,796) , loss of p53 (795,796) , and
poss ib ly overexpression of c-myc in progressive d isease (797) .
Approximate ly one–thi rd o f myeloma pat ients have up-regulat ion of cyc l in D1 by
immunohis tochemis t ry; the plasma ce l ls o f these same pat ients tend to have h igher
pro l i ferat ive ra tes (798) . The t (11;14) (q13;q32) translocat ion, which juxtaposes the
immunoglobul in heavy-chain promoter and the cyc l in D1 gene, is seen in ~25% of mul t ip le
myeloma pat ients (799,800,801,802,803) . Bergsagel et a l . have postula ted that ac t ivat ion of
one of the three cyc l in D genes is an in i t ia t ing event in myeloma (804) .
Both p15 and p16 are important cel l cycle inhib i tors that suppress cel l pro l i ferat ion through
inhib i t ion of CDK4 or CDK6 or both, thereby prevent ing the phosphoryla t ion of the
re t inoblastoma gene (RB) . A l though large de let ions of p15 and p16 are rare in myeloma (0
to 12% of cases) (805,806,807) , se lec t ive methyla t ion of these genes, a form of
t ranscrip t ional inact ivat ion, occurs in as many as 67 and 75% of cases, respect ive ly
(808,809,810) . Most data, including our own (811,812) suggest that hypermethyla t ion of p16
or p15 is assoc ia ted wi th d isease progression (811,812) .
K- and N- ras mutat ions have been descr ibed in 25 to 100% of newly d iagnosed mul t ip le
myeloma pat ients (796,813,814) , depending on the technique used for detect ion. A p53
tumor-suppressor gene delet ion is present in less than one th i rd of plasma cel ls f rom newly
d iagnosed myeloma pat ients (815), and mutat ions are even less common (816,817,818,819).
The c-myc protein and c-myc RNA are overexpressed in ~25% of mult ip le myeloma pat ients
(820,821) . Rearrangements of c -myc gene are present in ~15% of pat ients wi th mult ip le
myeloma or pr imary PCL (822) . Dysregulat ion of c -myc appears to be caused pr incipa l ly by
complex genomic rearrangements that occur dur ing la te s tages of mul t ip le myeloma
progress ion (797) .
Prognosis and Staging Surviva l o f mult ip le myeloma pat ients var ies f rom months to more than a decade (589,823).
There are no precise methods of ident i fy ing the subset o f newly d iagnosed pat ients who are
best served by s tandard-in tensi ty therapies, by maintenance therapies, by novel therapies,
or by more intens ive regimens such as hematopoiet ic stem ce l l t ransplantat ion. Prognost ic
fac tors are needed for pat ient counsel ing, therapeut ic dec is ion making, and c l in ical t r ia l
s t rat i f icat ion.
Stag ing is one form of prognost ic model ing. The Dur ie-Salmon system (Table 99.17) , which
unt i l recent ly was the most widely accepted mult ip le myeloma s tag ing system, separates
pat ients predominant ly by tumor burden and renal funct ion (28) . As the b io logy of myeloma
is bet ter understood, novel markers ref lec t ing myeloma cel l k inet ics , s ignal ing, genet ic
aberrat ions, and apoptosis have ecl ipsed the prognost ic s ign i f icance of tumor burden as a
predic tor o f surviva l .
A l though the Durie-Salmon system has some prognost ic u t i l i ty (28) , o ther b iolog ic var iab les
appear to be more va luable (388,824,825,826,827,828,829,830) . At the t ime of i ts incept ion,
the Dur ie-Salmon s taging system was an elegant system that incorporated information about
immunoglobul in product ion and hal f - l i fe, hemoglob in, ca lc ium, creat in ine, and extent o f
bone disease to der ive
P.2409

mathematica l ly the to ta l myeloma ce l l burden (28) . Quant i f icat ion of bone lesions used in
th is staging system, however, is not a lways rel iab le as a prognost ic factor (827) in that
pat ients c lass i f ied as s tage I I I so le ly on the basis o f bone lesion cr i ter ia do not have a
poorer prognosis.
Table 99.17 Durie-Salmon Staging System
Criterion Measured Myeloma Cell Mass (cells× 1012/m2)
Stage I
All of the following: Hemoglobin >100 g/L Serum calcium <12 mg/dl On radiograph, normal bone structure (scale 0)a or solitary bone plasmacytoma only Low M-component production rates IgG <50 g/L IgA <30 g/L Urine light-chain M component on electrophoresis <4 g/24 hours
<0.6 (low)
Stage II
Fitting neither stage I nor III 0.6–1.2 (intermediate)
Stage III
One or more of the following: Hemoglobin <85 g/L Serum calcium >12 mg/dl Advanced lytic bone lesions High M-component rates High M-component rates IgG >70 g/L IgA >50 g/L Urine light-chain M component on electrophoresis >12 g/24 h
>1.2 (high)
Subclassification

A: Serum creatinine <2 mg/dl B: Serum creatinine ≥2 mg/dl
aScale of bone lesions: normal bones, 0; osteoporosis, 1; lytic bone lesions, 2; and extensive skeletal destruction and major fractures, 3. From Durie BG, Salmon SE. A clinical staging system for multiple myeloma. Correlation of measured myeloma cell mass with presenting clinical features, response to treatment, and survival. Cancer 1975;36:842–854.By permission of the American Cancer Society.
Other variables , inc lud ing pat ient age, per formance s tatus, serum a lbumin, immunoglobul in
isotype, and bone marrow p lasma ce l l in f i l t ra t ion, have long been recognized to pred ic t
surviva l (831,832), and subsequent models have incorporated these fac tors
(253,589,830,833) (Table 99.18). Myeloma b io logy is better addressed by increased
concentrat ions of serum β2 -M, C-react ive protein , c i rcula t ing plasma ce l ls by per iphera l
b lood label ing index, o ther serum markers , bone marrow PCLI , and chromosomal
abnormal i t ies (388,824,825,828,829,830) . W hen designing a new s tag ing system, one must
choose between readi ly ava i lab le , inexpens ive markers , which f requent ly descr ibe the host
more than the int r ins ic propert ies of the myeloma, or more esoter ic , expens ive markers,
which ref lec t the int r insic bio logy of the indiv idual pat ient 's myeloma ce l ls . Each of these
systems has value, but the goal is to reach a consensus and to s tandard ize d iscuss ions and
comparisons among c l in ica l t r ia ls and outcomes. An internat ional consensus panel has
addressed this issue and developed the In ternat ional Stag ing System ( ISS) for mul t ip le
myeloma; i t incorporates serum a lbumin levels and β2 -microglobul in (491) . Though this
s tag ing system sat isf ies the former condit ion—it is inexpensive and readi ly ava i lab le—it
does not get to the hear t o f myeloma ce l l b io logy as genet ic changes do. Invest igators in
the myeloma communi ty have preferred severa l genet ic c lassi f icat ion systems; the next s tep
wi l l be to arr ive at a consensus system for th is as wel l . W ith these basic concepts in mind,
var ious prognost ic markers wi l l be d iscussed independent ly, and Tables 99.18 and 99.19
summarize severa l invest igators ' e f for ts to in t roduce more meaningfu l s tag ing systems.
Individual Prognostic Markers
β2-Microglobulin β2 -M concentrat ion is the s trongest and most re l iab le prognost ic fac tor for mul t ip le myeloma
that is rout ine ly ava i lable (Table 99.18) . I t depends not only on tumor burden but a lso on
renal funct ion. Elevated β2 -M va lues predict ear ly death (825,828,834) . Formulas to correct
the β2-M concentrat ions for the ef fec ts of renal insuf f ic iency have not improved i ts
predic t ive va lue (835) ; the β2 -M va lue is st i l l prognost ic in myeloma pat ients wi th normal
renal funct ion (824). β2 -M va lue a lso predicts h igh-dose therapy outcome ( i .e . , event- f ree
and overal l survival ) (245,837,838,839,840,841) . However, the Br i t ish Medica l Research

Counci l has shown that a f ter 2 years of survival , the ini t ia l β2 -M concentrat ion loses i ts
prognost ic va lue (836) .
C-Reactive Protein French invest igators f i rs t showed that C-react ive protein was usefu l as a un ivaria te and
mult ivar ia te (828) prognost ic marker in mul t ip le myeloma (Table 99.18) . These f ind ings
were substant ia ted in groups of pat ients f rom the Mayo Cl in ic (825) . C-react ive protein
va lues also predic t h igh-dose therapy outcome (803). However, C-react ive prote in
concentrat ion does not appear to be usefu l as a marker o f d isease s ta tus (842) .
Lactate Dehydrogenase Increased lac tate dehydrogenase va lues ident i fy a group of pat ients wi th poor prognos is
and aggressive d isease, sometimes a lymphomal ike d isease character ized by tumor masses
and ret roperi toneal adenopathy wi th a shor t c l in ica l course (843,844,845) . Only 7 to 11% of
pat ients wi th newly d iagnosed myeloma have an increased concentrat ion of LDH (132,845) .
Bone Marrow Plasma Cell Number and Morphology The quant i ty, growth patterns, and morpholog ic features of bone marrow p lasma cel ls have
been evaluated as prognost icators for pat ients with myeloma wi th var iab le resu l ts
(833,846,847,848,849) . Al though the est imat ion of percent bone marrow p lasmacytos is is
not a lways reproducible (846,847) , invest igators have repor ted prognost ic s ign i f icance
(833,849) . Bar t l e t a l . (833) constructed an int r icate s tudy of bone marrow character is t ics o f
myeloma pat ients (Table 99.18) . The archi tec tural pat tern of growth—inc lud ing in ters t i t ia l ,
in ters t i t ia l /sheets , in terst i t ia l /nodular , nodular , and packed—correla tes wi th survival
(833,849) , as does the plasma ce l l morphology (833). Accord ing to Bar t l e t al . (833),
myeloma ce l l h is to log ic features can be c lass i f ied in to s ix types: (a) Marschalko type—
predominant ly normal-appearing p lasma ce l ls wi th a mean s ize of 21 µm; (b) smal l cel l
type—smal l , round, and lymphoplasmacyto id wi th a mean size of 13 µm; (c) c leaved type—
notched, c leaved, or even convoluted nucle i o f var iab le s ize; (d) po lymorphous type—
marked ce l lu lar po lymorphism and mult inuclear i ty, wi th in terspersed giant p lasma cel ls and
cytoplasmic inc lusions; (e) asynchronous type—marked asynchronous maturat ion of the
nucleus and cytop lasm, large eccentr ic nuc lei , f requent nucleol i , and a pronounced
per inuc lear “hof ”; and ( f) b las t ic type—plasmablasts wi th large nuc le i , prominent centra l ly
located nucleol i wi th a moderate r im of basophi l ic cytoplasm, and a fain t per inuclear hof
(Table 99.18) . Nei ther o f these morpholog ic features—archi tec ture or p lasma cel l
phenotype—has been appl ied widely.
Other invest igators have demonstrated the powerfu l prognost ic s ign i f icance of immature or
p lasmablast ic plasma cel ls (199,200,826,845,850,851,852,853,854) . Plasmablast ic
morphology is assoc ia ted wi th a h igh PCLI , a higher leve l o f s IL-6R, and ras mutat ions
(826).
P.2410
Elect ron microscopy conf i rms that immature nuclear morphology and nuc lear cytoplasmic
asynchrony corre la te wi th one another and wi th poor prognos is (855) . Nuclear immaturi ty
and three cytoplasmic abnormal i t ies—scattered pat terns of mi tochondr ia, s ing le-sac
loopl ike s t ructures, and numerous in trami tochondr ial granules—have been associa ted wi th
poor outcome.

Table 99.18 Noncytogenetic Prognostic and Staging Systems in Newly Diagnosed Multiple Myeloma Patients (Standard-Intensity Chemotherapy Unless Stated
Otherwise)
Study No. of Patients
Risk or Stage Patients (%)
Features OS (mo)
Durie and Salmon, 1980 (28,1107)
150 IA IIA & IIB IIIA IIIB
11 27 50 13
Defined in Table 4.17
61 54 30 15
Low 22 BUN ≤8 mM and Hb >100 g/L
>48
Intermediate 56 Not meeting other criteria
~34
MRC, 1980 (253)
485
High 22 BUN >10 mM and Hb ≤75 g/L
~24
Low grade 71 Marschalko and small PCa
40
Intermediate grade
28 Cleaved, polymorphous asynchronous PC
20
Bartl et al., 1987 (833)
674
High grade 2 Plasmablastic PC
8
Low 30 PCLI <0.4% and β2-M <4 mg/L
48
Intermediate 25 PCLI ≥0.4% or β2-M ≥4 mg/L
29
Greipp et al., 1988 (824)
100
High 45 PCLI ≥0.4% and β2-M ≥4 mg/L
12

Low 50 β2-M and CRP <6 mg/L
54
Intermediate 35 β2-M or CRP ≥6 mg/L
27
Bataille et al., 1992 (828)
162
High 15 β2-M and CRP ≥6 mg/L
6
Low 14 PCLI <1% and β2-M <2.7 mg/L
71
Intermediate 54 PCLI ≥1% or β2-M ≥2.7 mg/L
40
Greipp et al., 1993 (825)
107
High 32 PCLI ≥1% and β2-M ≥2.7 mg/L
17
Ib 26 REb <6 or SM: ((a–d)=0
>80
II 52 6 ≤ RE ≤ 8.5 or SM: 0 > ((a–d)≤ 3
36
San Miguel et al., 1995 (830)
120
III 22 RE >8.5 or SM: ((a–d) ≥4
9
I 61 Hb ≥100 g/L and BMPC <70%
57
II 25 Hb <100 g/L or BMPC ≥70%
45
Finnish Leukaemia Group, 1999 (589)
324
III 14 Hb <100 g/L and BMPC ≥70%
25

I 13 β2-M <2.5 mg/L 53
II 43 β2-M ≥2.5 but <5.5 mg/L
41
III 33 β2-M ≥5.5 mg/L and alb >3 g/dl
24
Crowley et al., 2001 (388)
1,026
IV 11 β2-M ≥5.5 mg/L and alb <3 g/dl
16
I 29 β2-M <3.5 mg/L and alb ≥3.5 g/dl
62
II 38 Not stage I or III 45
International Staging System (491)
8,056
III 33 β2-M ≥3.5 mg/L 29
Alb, albumin; β2-M, β2-microglobulin; BMPC, bone marrow palsma cells; BUN, blood urea nitrogen; CRP, C-reactive protein; ECOG, Eastern Cooperative Oncology Group; MRC, Medical Research Council Working Party on Leukaemia in Adults; OS, overall survival; PC, plasma cells; PCLI, plasma cell labeling index; SWOG, Southwest Oncology Group. aSee text for details. The Bartl staging system is a plasma cell (PC) morphology–based staging system. bFrom risk equation (RE) and simplified model (SM): RE: (2.2 * %S phase PC) +(0.8 (β2-M) +(1.2 * ECOG) + (0.9 * age). SM: (a) S phase ≥ 3% (+2); (b) β2-M ≥ 6 µg/ml (+1); (c) ECOG ≥ 3 (+1); (d) age ≥ 69 (+1); absence of each (+0).
Plasma Cell Labeling Index The PCLI of bone marrow p lasma ce l ls is a reproducible and powerful prognost ic factor in
mult ip le myeloma (824,825,830,856) (Table 99.18) . The PCLI is determined f rom an
immunof luorescence sl ide-based assay (199) . Cel ls in DNA S phase of the ce l l cycle
incorporate bromodeoxyur idine, which can be recognized by us ing a monoc lonal ant ibody.
S-phase cel ls are then marked wi th a second ant ibody, and p lasma cel ls are recognized by
morphology and react iv i ty wi th ant ihuman immunoglobul in κ and λ l ight chains. An increased
PCLI pred ic ts a shor t remission and surviva l but does not predict response to therapy. Al l
la rge studies publ ished to date have conf i rmed the independent prognost ic va lue of the
PCLI for surviva l a f ter t reatment wi th convent ional chemotherapy (824,826,851,857) or
h igh-dose therapy (838) . Other methods for determining pro l i ferat ion inc lude Ki67

immunohis tochemica l s ta ining (858,859) , and determinat ion of S phase by f low cytometry
(830,860,861) . W itz ig et a l . (862,863) have also demonstrated the prognost ic va lue of the
per iphera l b lood label ing index.
Immunophenotype of Myeloma Cells As discussed previously, the phenotype of mal ignant p lasma cel ls is diverse
(205,206,207,210,211,213,214) and potent ial ly dynamic (864,865) . Invest igators have
demonstrated that sur face express ion of CD45, CD56, and CD117 por tends a better
prognos is (207,209) and expression of CD28 and CD44, a worse prognos is (207,866).
Pat ients wi th the t (11;14) t rans locat ion are more l ike ly to have sur face express ion of CD56,
and CD117. Pat ients wi th nonhyperd ip loid myeloma have increased express ion of both
CD20 and CD28 in the absence of react iv i ty for CD56 and CD117—al l poor prognost ic
f indings (207) .
Cytogenetics, Fluorescence in Situ Hybridization, a nd Other
Genetic Abnormalit ies The f i rs t cytogenet ic abnormal i t ies in myeloma were documented near ly 30 years ago (F ig.
99.14) . In the past decade i t has become increas ing apparent that cytogenet ic tes t ing is an
in tegral element of es tabl ish ing prognos is and a treatment plan for a l l newly d iagnosed
myeloma pat ients . Near ly a l l myeloma pat ients have abnormal chromosomes by
f luorescence in s i tu hybrid izat ion (FISH), includ ing dele t ions, aneuploidy, and
t rans locat ions (867,868), al though abnormal karyotypes are seen in only 18 to 30% of cases.
Th is apparent d iscrepancy is exp la ined by the general ly low pro l i ferat ive ra te of myeloma
ce l ls and the requi rement o f obta ining plasma ce l ls (and not just the rap idly d iv iding normal
myeloid
P.2411
precursors) in metaphase to generate convent ional cytogenet ics (869,870,871). Therefore,
any abnormal i ty in convent ional cytogenet ics ident i f ies a group wi th a higher pro l i ferat ive
ra te (872) and a par t icular ly poor prognos is . There is an excel lent correlat ion between
abnormal convent ional cytogenet ics and a h igh plasma ce l l prol i ferat ive ra te (873,874) . W ith
in terphase FISH, several chromosomal abnormal i t ies , such as immunoglobul in heavy-chain
t rans locat ions and delet ion of chromosome 13, are observed at equal f requenc ies among
the spectrum of p lasma pro l i ferat ive d isorders f rom MGUS to mul t ip le myeloma to PCL
(875,876) .
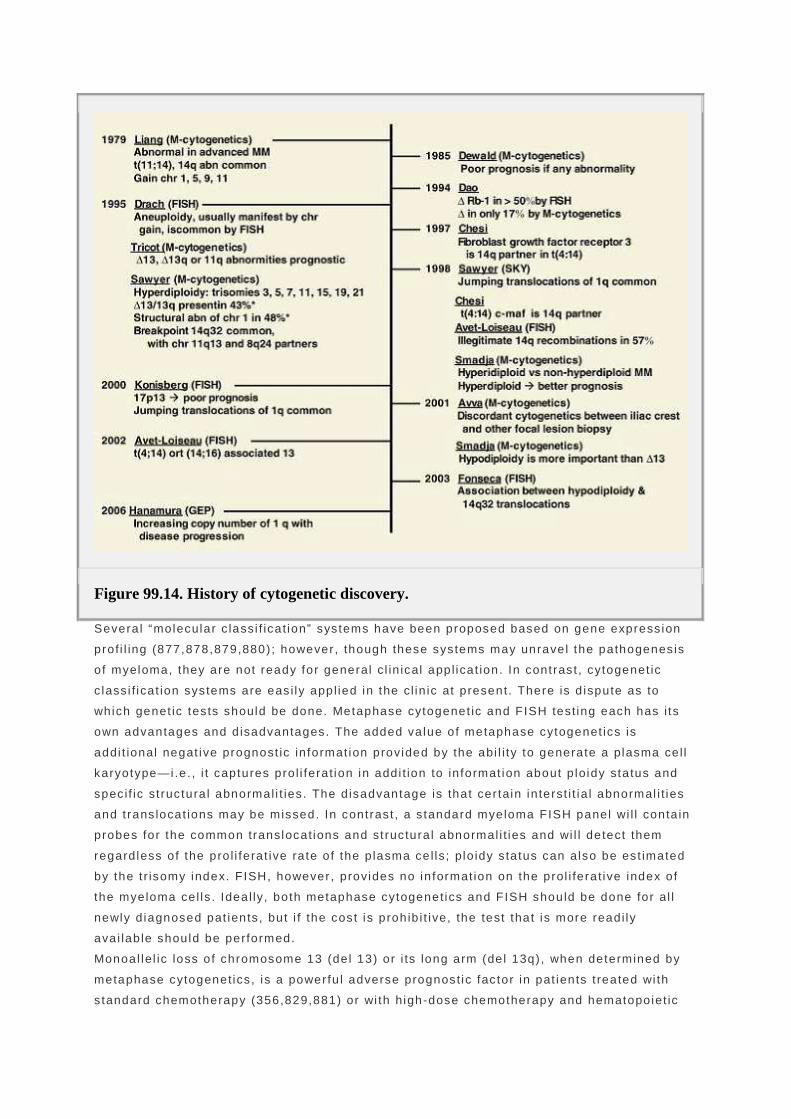
Figure 99.14. History of cytogenetic discovery.
Severa l “molecular c lassi f icat ion” systems have been proposed based on gene express ion
prof i l ing (877,878,879,880) ; however, though these systems may unravel the pathogenes is
o f myeloma, they are not ready for general c l in ical appl icat ion. In contrast , cytogenet ic
c lass i f icat ion systems are eas i ly appl ied in the c l in ic at present. There is d ispute as to
which genet ic tes ts should be done. Metaphase cytogenet ic and FISH test ing each has i ts
own advantages and d isadvantages. The added va lue of metaphase cytogenet ics is
addi t ional negat ive prognost ic in format ion provided by the abi l i ty to generate a plasma ce l l
karyotype—i.e. , i t captures pro l i ferat ion in addi t ion to in format ion about p loidy sta tus and
spec i f ic st ruc tura l abnormal i t ies. The d isadvantage is that cer tain in terst i t ia l abnormal i t ies
and t rans locat ions may be missed. In contrast , a s tandard myeloma FISH panel wi l l conta in
probes for the common translocat ions and st ruc tura l abnormal i t ies and wi l l detect them
regard less of the pro l i ferat ive ra te of the p lasma ce l ls; plo idy s ta tus can also be est imated
by the t r isomy index. FISH, however, provides no in format ion on the prol i ferat ive index of
the myeloma ce l ls . Ideal ly, both metaphase cytogenet ics and FISH should be done for al l
newly d iagnosed pat ients , but i f the cost is proh ib i t ive, the test that is more readi ly
ava i lab le should be performed.
Monoal lel ic loss of chromosome 13 (de l 13) or i ts long arm (de l 13q) , when determined by
metaphase cytogenet ics , is a powerfu l adverse prognost ic fac tor in pat ients t reated wi th
s tandard chemotherapy (356,829,881) or wi th high-dose chemotherapy and hematopoiet ic

stem cel l t ransplantat ion (331,480,803,882,883) (Table 99.18) . Approximate ly 50% of newly
d iagnosed mul t ip le myeloma pat ients have del 13 or de l 13q by FISH (874,876,884) . Our
group has shown that del 13q is assoc ia ted wi th spec i f ic bio logic features, inc lud ing a
h igher frequency of λ - type mul t ip le myeloma, s l ight female predominance, h igher PCLI , and
a h igher f requency of a serum M component o f <10 g/L (356) . Pat ients wi th the de let ion by
FISH have worse overa l l survival wi th s tandard chemotherapy (356,829,874) , h igh-dose
therapy (884,885), and in ter feron t reatment (356) . The absence of abnormal i t ies o f
chromosome 13 and 11 by convent ional cytogenet ics is associa ted wi th longer complete-
response durat ion, event- f ree survival , and overal l survival in pat ients t reated wi th high-
dose therapy (331) . The prognost ic s ign i f icance of del 13q by FISH is less than that for de l
13 by convent ional cytogenet ics , because the la t ter tes t incorporates both the chromosomal
abnormal i ty and a h igh ra te of plasma ce l l pro l i ferat ion, whereas the former captures on ly
the chromosomal abnormal i ty.
Hypodiploid myeloma has a worse prognos is than d ip lo id or hyperdiplo id myeloma. This has
been demonstrated by f low cytometr ic methods (881,886,887) and metaphase cytogenet ics
(883,888,889,890,891) . Controversy exis ts about whether the dele t ion 13q adds any
addi t ional prognost ic in format ion to a hypodiploid karyotype (888,891,892) .
Up to 75% of pat ients wi th mul t ip le myeloma have t ranslocat ions invo lv ing the heavy-chain
gene on chromosome 14. These t ranslocat ions inc lude i l legi t imate swi tch recombinat ions of
the variable regions of the immunoglobul in heavy-chain gene at 14q32. Par tners o f the
t rans locat ions into the IgH swi tch region on chromosome 14 include chromosomes 11, 4, 6 ,
and 16 (893) . The most common t rans locat ion in mul t ip le myeloma is t (11;14) (q13;q32)
(870,892) , which increases expression of cycl in D1 (802) , a protein involved in ce l l -cycle
progress ion. The prevalence of t (11;14) (q13;q32) is 20% in mult ip le myeloma
(870,892,894) . Previous publ icat ions had suggested that th is t rans locat ion was assoc ia ted
wi th an adverse outcome in mul t ip le myeloma (803,829) , but more recent data re fu te this
hypothesis (894) . The t (6 ;14) (p21;q32) is also associa ted wi th a neutra l prognos is (895) .
The t (4 ;14) (p16.3;q32) is present in 15% of mul t ip le myeloma pat ients
(896,897,898,899,900) . Th is t rans locat ion resul ts in the up-regulat ion of f ibrob last growth
fac tor receptor 3 (FGFR3) and in the hybr id t ranscrip t IgH/MMSET (896,897) . The t (14;16)
(q32;q23) is a lso seen in a smal l subset (~5%) of pat ients wi th mul t ip le myeloma (892,897) .
Both convey a very poor prognos is . In one s tudy there was a t ight assoc iat ion of de l 13
abnormal i t ies and h igh β2 -M va lues wi th the unfavorable t (4 ;14) and t(14;16) abnormal i t ies
(822).
P.2412
The f requency of h igh β2-M or de l 13 was one hal f that in pat ients wi th the t (11;14)
abnormal i ty. Th is suggests that the poor prognos is associa ted wi th del 13 may be because
of o ther nonrandom, assoc ia ted chromosomal abnormal i t ies. Fonseca et a l . (901) have
recent ly demonstrated that three d is t inc t s tag ing groups can be def ined by the presence of
t (14;16) (q32;q23) , t (4;14) (p16.3;q32) , dele t ion 17p13, and del 13q by FISH (Table 99.19) .
Table 99.19 Genetic-Based Prognostic and Staging Systems in Newly Diagnosed Multiple Myeloma Patients (Patients Treated with Standard-Intensity Chemotherapy
Unless Stated Otherwise)
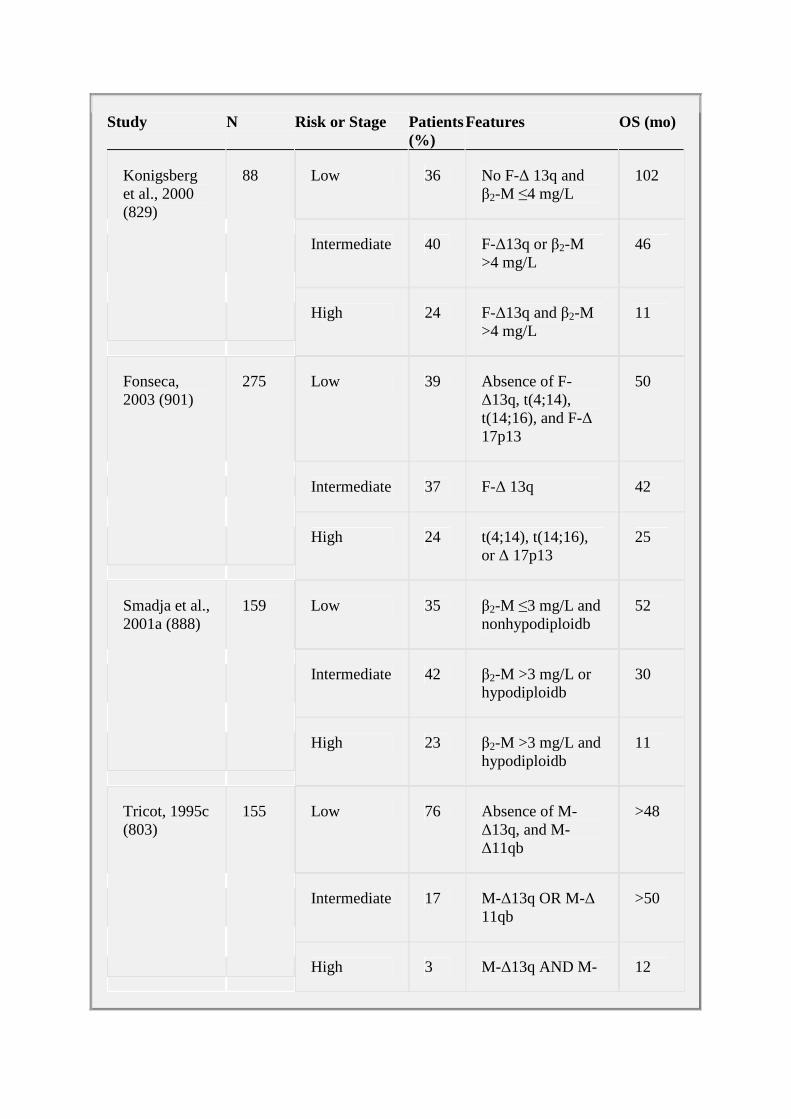
Study N Risk or Stage Patients (%)
Features OS (mo)
Low 36 No F-∆ 13q and β2-M ≤4 mg/L
102
Intermediate 40 F-∆13q or β2-M >4 mg/L
46
Konigsberg et al., 2000 (829)
88
High 24 F-∆13q and β2-M >4 mg/L
11
Low 39 Absence of F-∆13q, t(4;14), t(14;16), and F-∆ 17p13
50
Intermediate 37 F-∆ 13q 42
Fonseca, 2003 (901)
275
High 24 t(4;14), t(14;16), or ∆ 17p13
25
Low 35 β2-M ≤3 mg/L and nonhypodiploidb
52
Intermediate 42 β2-M >3 mg/L or hypodiploidb
30
Smadja et al., 2001a (888)
159
High 23 β2-M >3 mg/L and hypodiploidb
11
Low 76 Absence of M-∆13q, and M-∆11qb
>48
Intermediate 17 M-∆13q OR M-∆ 11qb
>50
Tricot, 1995c (803)
155
High 3 M-∆13q AND M- 12
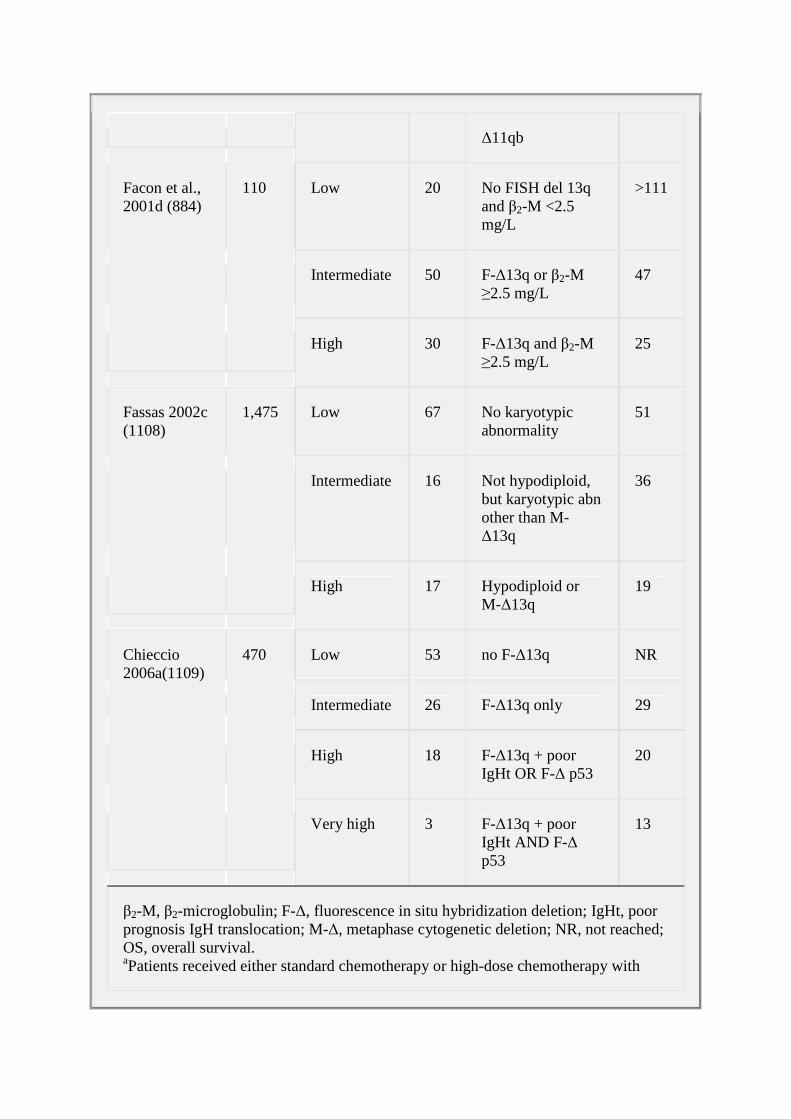
∆11qb
Low 20 No FISH del 13q and β2-M <2.5 mg/L
>111
Intermediate 50 F-∆13q or β2-M ≥2.5 mg/L
47
Facon et al., 2001d (884)
110
High 30 F-∆13q and β2-M ≥2.5 mg/L
25
Low 67 No karyotypic abnormality
51
Intermediate 16 Not hypodiploid, but karyotypic abn other than M-∆13q
36
Fassas 2002c (1108)
1,475
High 17 Hypodiploid or M-∆13q
19
Low 53 no F-∆13q NR
Intermediate 26 F-∆13q only 29
High 18 F-∆13q + poor IgHt OR F-∆ p53
20
Chieccio 2006a(1109)
470
Very high 3 F-∆13q + poor IgHt AND F-∆ p53
13
β2-M, β2-microglobulin; F-∆, fluorescence in situ hybridization deletion; IgHt, poor prognosis IgH translocation; M-∆, metaphase cytogenetic deletion; NR, not reached; OS, overall survival. aPatients received either standard chemotherapy or high-dose chemotherapy with

transplant. bMetaphase cytogenetics. cTandem transplant study, rather than conventional chemotherapy. dHigh-dose melphalan, single transplant, or tandem transplant.
Another new cytogenet ic prognost ic marker is the gain of 1q21 in myeloma. Abnormal i t ies o f
both the shor t and long arms of chromosome 1 have been noted s ince the f i rs t cytogenet ic
s tud ies of myeloma (869,903) (F ig . 99.14) . More recent ly, Hanamura et al . demonstrated
that the f requency of 1q21 ampl i f icat ions increases from monoc lonal gammopathy of
undetermined signi f icance (0%), to overt mul t ip le myeloma (43%), and f inal ly to re lapse
(72%). Ampl i f icat ions of 1q21 are concurrent wi th dysregulated express ion of c -MAF,
MMSET/FGFR3, or dele t ion 13 (902). Candidate genes for the molecular mechanism of
prognos is imparted by the 1q21 ampl icat ion include CDS1B, BCL-9, or RAB25, but this has
not been conf i rmed by others (736) .
Tr isomy is common by FISH and inc ludes chromosomes 3, 6 , 9 , 11, and 15 (904) . In another
s tudy, t r isomy of 3 , 7 , and 11 accounted for >50% of the hyperdiplo id cases (905) .
Tr isomies of chromosomes 6, 9, and 17 were assoc ia ted wi th pro longed surviva l (906).
Mutat ions of ras have been noted in 30 to 50% of MM pat ients , wi th increas ing prevalence
in the advanced stages of the disease (795,813) and shor ter surviva l (K-ras ) (796) .
Mutat ions of ras were f i rs t observed in fu lminant d isease (907) but have also been observed
in 27 to 39% of newly d iagnosed cases (795,796) . Pat ients wi th ras mutat ions had a median
surviva l o f 2 .1 years , versus 4 years for pat ients wi th wi ld- type ras (796) .
The inact ivat ing mutat ion of p53 , locus 17p13, is rare in f reshly exp lanted myeloma cel ls
but is common in human myeloma ce l l l ines and in pat ients wi th a terminal phase of
myeloma (907) . Such mutat ions have been observed in ~5% of cases of ear ly mul t ip le
myeloma, versus 20 to 40% of cases of PCL (816,817,818,819) . Delet ions of p53 as
detected by FISH are present in 9 to 33% of pat ients wi th newly d iagnosed myeloma
(815,908) and confer a poorer median survival (15.9 vs. >38 months) (815) .
Epigenet ic phenomena, such as methylat ion of the p16 (Met-p16 ) promoter reg ion, have
been associa ted wi th progress ion in the p lasma ce l l dyscras ias (794,909,910,911) . Met-p16
is uncommon in MGUS/smoldering mul t ip le myeloma, increases in f requency wi th advancing
s tages of the disease (811,911) , and is common in ext ramedul lary mul t ip le myeloma,
includ ing PCL.
Zhan et a l . (735,912) s tud ied the gene express ion of 74 myeloma pat ients by us ing h igh-
dens i ty o l igonucleot ide microarrays in terrogat ing about 6 ,800 genes. On h ierarch ical
c lus ter ing analys is , four d ist inc t subgroups of myeloma (MM1, MM2, MM3, and MM4) were
ident i f ied. The expression pat tern of MM1 was s imi lar to normal PCs and MGUS, whereas
MM4 was s imi lar to MM cel l l ines. Cl in ical var iables l inked to poor prognos is , includ ing
abnormal karyotype and h igh serum β2 -M leve ls , were most prevalent in MM4.
Overexpress ion of genes invo lved in DNA metabol ism and ce l l -cycle contro l were observed
in MM4. Novel candidate MM disease genes have been ident i f ied.
Angiogenesis Severa l s tud ies have demonstrated the prognost ic s ign i f icance of increased microvessel
dens i ty ( i .e. , angiogenesis) in mul t ip le myeloma (201) . The f i rst descr ip t ion was a
comprehens ive study of mult ip le myeloma and MGUS that showed a s t rong associa t ion wi th
d iagnos is and wi th an increased S-phase f rac t ion of p lasma cel ls measured by the PCLI
(201). Th is f inding was corroborated in a prospect ive c l in ica l t r ia l (913) . Median surviva ls
were 4.4 and 2 years in pat ients wi th low, intermediate, and high microvessel dens i ty,
respect ive ly. However, in this s tudy of only 74 pat ients there was no independent
prognost ic s ign i f icance for angiogenes is in a model that included PCLI , β2 -M, and the
percentage of marrow p lasma cel ls (913) . In another s tudy, angiogenes is fa i led to predict
surviva l (771) . I t is not known whether leve ls o f angiogenic
P.2413
cytokines such as VEGF, bFGF, or hepatocyte growth factor are assoc ia ted wi th poor
surviva l , a l though concentrat ions are reduced dur ing ef fect ive chemotherapy (793) .
Lymphocyte Subsets Low numbers of CD4 (helper T) ce l ls a t d iagnosis are assoc ia ted wi th worse prognos is
(914,915) ; the prognost ic importance of CD4 T ce l ls is present throughout the course of
d isease, inc lud ing af ter the complet ion of chemotherapy and at relapse (916) .
In the post t ransplantat ion set t ing, the number o f c i rcu la t ing lymphocytes appears to be an
important prognost ic fac tor . Porrata et a l . (917) demonstrated lower relapse ra tes and
pro longed survival for pat ients wi th h igher absolute lymphocyte counts a f ter auto logous
s tem cel l t ransplantat ion, suggest ing an ear ly graf t -versus-tumor ef fec t. The median overa l l
surviva l and progress ion- f ree survival for myeloma pat ients were s ign i f icant ly longer in
pat ients wi th an absolute lymphocyte count o f ≥500 ce l ls/µ l on day 15 than for pat ients wi th
an absolute lymphocyte count <500 ce l ls /µ l (33 vs . 12 months; 16 vs . 8 months) .
Researchers at the Univers i ty o f Arkansas made a s imi lar observat ion. In a t r ia l des igned to
eva luate the ro le of more intense condi t ion ing, lymphocyte recovery, evaluated as a
surrogate for immune recovery, was in fer ior in more in tensive ly t reated pat ients . Despi te
ident ical complete remiss ion rates, event- free surviva l and overa l l surviva l were
s ign i f icant ly decreased among pat ients rece iv ing more intens ive condi t ioning (529).
Other Prognostic Factors Other factors that have adverse prognost ic va lue include decreased sta in ing of bone
marrow p lasma ce l ls for ac id phosphatase (918) , increased ci rcu la t ing p lasma ce l ls as
measured by the per iphera l b lood label ing index (863) , apoptot ic index (218) , increased s IL-
6R (826,919) , serum neopterin (366), α1 -ant i t rypsin (920), C- terminal te lopept ide of type I
co l lagen (921,922) , serum bone sia loprotein (923) , B1 2 -b ind ing prote in (924) , soluble CD56
(925), so lub le Fc receptor (CD16) (926) , solub le syndecan or CD138 (927) , and serum IL-6
leve ls (920,928,929) . Al though IL-6 is known to have a major ro le in myeloma pathogenesis,

C-react ive prote in leve ls corre la te wel l wi th th is more expensive and less readi ly avai lab le
prognost ic tes t. There are mixed resul ts on the prognost ic va lue of serum thymid ine k inase
(930,931) .
Drug Resistance One form of drug res is tance is marked by mul t idrug res is tance-1 express ion on plasma ce l ls
as demonstrated by immunocytochemis t ry (932). The presence of th is P-glycoprotein in the
ce l l membrane of p lasma cel ls o f pat ients wi th mul t ip le myeloma is assoc ia ted wi th a poor
prognos is . Drug res is tance measured by immunocytochemica l detect ion of lung resistance
protein is highly corre la ted wi th fa i lure of response to melphalan and poor subsequent
surviva l (933) .
Significance of the Extent of Response after Therapy
Significance of Response after Standard-Intensity C hemotherapy Response is o f ten used as a measure of e ff icacy, and i t is of ten assumed that complete
remiss ions are a prerequis i te for cure. Indeed, pat ients t reated wi th s tandard- in tensi ty
chemotherapy wi th respons ive d isease tend to l ive a median of 18 months longer than do
pat ients wi th resistant disease (38,238,591) . However, tumor response may speak more to a
pat ient 's tumor bio logy than i t does to the therapy in quest ion. Most s tandard-in tens i ty
chemotherapy s tudies suggest that the degree of response does not corre la te wi th survival
(591,593,934,935,936) . Rather, the ab i l i ty to achieve a p la teau of a t least 6 months '
durat ion is as important, i f not more important , than the degree of response to therapy
(588,589,590) . The data f rom only three (251,368,369) o f 27
(233,277,354,359,362,363,366,385,937) randomized induct ion t r ia ls suggest that the
observed h igher response rate t rans lates in to longer overa l l surviva l (Table 99.6) .
The importance of response kinet ics is a lso a controvers ia l topic . Some data support the
premise that those wi th the most rap id responses to alkyla tor-based therapy have a shor ter
remiss ion durat ion and surviva l (586), whereas other data contradic t th is assumption (591) .
Significance of a Complete Response after High-Dose Therapy I t is unclear whether the achievement o f a complete response as def ined by the
d isappearance of the M protein by immunof ixat ion of the serum and ur ine af ter high-dose
therapy wi th hematopoiet ic s tem cel l support is of prognost ic va lue. Mul t ip le s tud ies have
produced incons is tent resu l ts (245,479,544,938,939,940,941) . Severa l o f these s tudies
(245,544,939) d id not use the more s t r ingent def in i t ion of “complete response”; they rel ied
on the absence of an M protein on an e lec trophoret ic pat tern ra ther than immunof ixat ion
negat iv i ty. These s tudies should be in terpreted wi th caut ion because they do not inc lude
several of the most powerful determinants o f prognos is—PCLI and cytogenet ics
(331,803,824,825,830) .
One of these is a re t rospect ive study of 344 pat ients wi th mul t ip le myeloma t reated wi th
h igh-dose chemotherapy fo l lowed by auto logous s tem cel l t ransplantat ion. Pat ients were not
t reated un i formly. The 5-year overal l surviva l was 48% in those who had no M prote in on
immunof ixat ion and 21% in those wi th a pers is tent M protein (940) . In another study,
Rawston et al . reported bet ter overa l l surviva l in pat ients ach ieving a complete response
e i ther by immunofixat ion or by f low cytometry (942). In yet another study, Davies and
co l leagues (941) reported a series of 96 pat ients who received h igh-dose therapy and were

assessed for the ef fec t of response on surviva l . Al though there was a trend toward
improved progression- f ree surviva l among pat ients wi th an immunof ixat ion-negat ive
complete response compared wi th pat ients wi th a part ia l response (49.4 vs . 41.1 months, p
= .26) , there was no improvement in overa l l surviva l . A lexanian et a l . (943) repor ted on a
ser ies of 68 pat ients t reated wi th dexamethasone-based induct ion therapy fo l lowed by ear ly
h igh-dose therapy; resu l ts were compared to those of 50 pat ients who were unable to
receive high-dose therapy because of socioeconomic reasons. Pat ients who achieved an
immunof ixat ion-negat ive complete response by ei ther means ( i .e. , h igh-dose or s tandard
chemotherapy) had super ior overa l l survival compared to pat ients who achieved a par t ia l
response or less . The impl icat ion of these data is that a complete response may be an
important surrogate marker o f long surviva l and less aggress ive myeloma b iology. In yet
another s tudy, Rajkumar et al . (944) repor ted a complete response in 33% of 126 mul t ip le
myeloma pat ients who underwent s tem cel l t ransplantat ion. There was no d i f ference in the
overa l l surviva l or progress ion- f ree survival between pat ients who achieved a complete
response and those who d id not; rather, overa l l surviva l was s ign i f icant ly in f luenced by the
leve l o f the PCLI (493) .
Special Cases of Myeloma
Nonsecretory Multiple Myeloma
Nonsecretory mul t ip le myeloma accounts for 1 to 5% of myeloma cases
(130,945,946,947,948,949) . W ith more sensi t ive tes t ing such as immunof ixat ion (950) and
f ree l ight -chain assays (21) , a major i ty o f these “nonsecretory” pat ients are found to be low
secretors or o l igosecretory. Immunoperoxidase or immunofluorescence s tud ies should be
per formed for al l pat ients in whom nonsecretory myeloma is suspected. More than 85% of
cases have a cytoplasmic monoclonal prote in ; in the remainder, no monoclonal prote in can
be detected in the cytop lasm (948,949,951) . Indiv iduals in this lat ter group are re ferred to
as “nonproducers . ” From a cl in ica l s tandpoint, both are termed “nonsecretory. ”
At presentat ion, hypercalcemia and anemia may be present. A reduct ion in background
immunoglobul ins is common (948,949) . There is minimal to no r isk o f myeloma k idney
(946,948) . Lyt ic bone d isease is present in most pat ients (945,946,947,948) . Median
P.2414
surviva l o f these pat ients is at least as good as for those wi th secretory myeloma
(945,947,948) . Response is di f f icul t to document, but wi th the new serum assays,
quant i ta t ion of f ree l ight chains is poss ib le in about two thi rds of these pat ients (21) .
Immunoglobulin D Myeloma IgD myeloma accounts for about 2% of a l l cases of myeloma (952) . The presence of a
monoclonal IgD in the serum usual ly ind icates myeloma, but three cases of IgD MGUS have
been documented (946). Pat ients wi th IgD myeloma general ly present wi th a smal l band or
no evident M sp ike on serum prote in elec t rophores is . Their c l in ica l presentat ion is s imi lar to
that o f pat ients wi th Bence Jones myeloma ( l ight-chain myeloma) in that both have a h igher
incidence of renal insuf f ic iency and coinc ident amylo idos is as wel l as a higher degree of
proteinur ia than in IgG or IgA myeloma (952) . IgD myeloma pat ients , however, appear to
have a h igher f requency of monoclonal λ l ight chains than κ l ight chains (952) . W ith an
incidence of 19 to 27%, ext ramedul lary involvement is more prevalent in pat ients wi th IgD

myeloma (953,954,955) . Surviva l wi th IgD myeloma has been repor ted to be in fer ior to that
wi th o ther forms of myeloma, wi th a median of 12 to 17 months (953,954,955). In the Mayo
Cl inic series , however, median surviva l was 31 months in pat ients diagnosed af ter 1980
(946,956) .
Immunoglobulin E Myeloma
IgE myeloma is a rare form of myeloma. A dispropor t ionate number of cases are PCL,
a l though the sample s ize is smal l , wi th only about 40 cases of IgE myeloma repor ted in the
l i terature (957,958) .
Plasma Cell Leukemia PCL is a rare form of plasma ce l l dyscras ia . Between 2 and 4% (904,959,960) o f mal ignant
p lasma ce l l dyscrasia cases are PCL. By def ini t ion, there are >20% plasma ce l ls in the
per iphera l b lood, wi th an absolute p lasma cel l count o f >2 × 109 /L . Some authors accept the
d iagnos is wi th on ly one of these cr i ter ia (946) . The presentat ion may be pr imary, de novo,
or secondary, evolv ing f rom an exis t ing case of myeloma as par t o f the terminal phase of
the d isease. About 60 to 70% of cases are pr imary (959) .
Al though there is overlap, the phenotype of p lasma cel ls f rom pat ients wi th pr imary PCL is
d i f ferent f rom those of myeloma pat ients . PCL plasma cel ls more f requent ly express the
CD20 ant igen (904) than those of mul t ip le myeloma (50 vs. 17%), and they of ten lack CD56
ant igen (210,904), which is present on the majori ty o f myeloma cel ls (904) . CD56 is
cons idered important in anchoring p lasma cel ls to bone marrow s t roma, and i ts absence is
associated wi th a poor prognosis (211,212) . CD28 is more f requent ly expressed on
mal ignant plasma ce l ls in secondary than in pr imary PCL, which is consistent wi th an
observat ion made in myeloma, i .e. , that acquis i t ion of the CD28 ant igen on p lasma ce l ls
appears to correla te wi th an increased pro l i ferat ive ra te and d isease progress ion (961) .
PCL p lasma cel ls have higher pro l i ferat ive ra tes (904)and more complex karyotypes than
myeloma p lasma cel ls (960) . By comparat ive genomic hybr idizat ion and by FISH techniques,
losses on 13q (962,963) and monosomy 13 (904) exis t in >80% of PCL pat ients (962,963) .
Losses on chromosome 16 also occur in ~80% of cases (963). Gains in 1q are present in
about ha l f o f the pat ients by FISH (904) , but in al l by comparat ive genomic hybrid izat ion
(963). In addi t ion, PCL pat ients have un ique losses of 2q and 6p (963) . Overexpress ion of
PRAD1/cycl in D1, which p lays an important role in contro l o f the cel l cycle , has a lso been
observed in PCL (964).
The c l in ical presentat ion of pr imary PCL is more aggress ive than that o f mult ip le myeloma,
wi th a h igher present ing tumor burden and h igher f requenc ies of ext ramedul lary invo lvement ,
anemia, thrombocytopenia, hyperca lcemia, renal impai rment (904,959,960,965), increased
leve ls o f serum lac tate dehydrogenase and β2 -M, and p lasma cel l pro l i ferat ive act iv i ty (904) .
The inc idence of ly t ic bone lesions is s l ight ly lower than that usual ly observed in mul t ip le
myeloma (904,966) .
Though the c l in ica l and laboratory features of pr imary and secondary PCL are s imi lar
(966,967) , the response to therapy and overa l l surviva l in pr imary and secondary PCL go
f rom poor to worse (959,960,966,967) . Higher response rates can be achieved wi th
mult iagent chemotherapy ra ther than s ing le-alkyla tor programs (47 to 66% vs. 8 to 13%)
(904,959,960,966). Regimens such as VMCP/VBAP, VAD, and combinat ion
cyc lophosphamide and etopos ide have resul ted in median survivals o f 18 to 20 months,

compared wi th 2 to 6 months when s ing le-agent therapy is used (904,959,960,966) .
Response and surviva l ra tes wi th secondary PCL remain low (966,967). When tha l idomide
and dexamethasone are used, responses are poss ible (968,969) (personal observat ion) ,
which is not surpr is ing g iven the high response rates observed in pat ients wi th h igh PCLIs
in our thal idomide t r ia l (970) . There are anecdota l reports o f ac t iv i ty of bor tezomib in these
pat ients (971,972,973) . Some pat ients der ive excel lent responses and 2- to 3-year d isease-
f ree survivals a f ter auto logous s tem cel l t ransplantat ion (974,975,976,977,978) . Saccaro et
a l . (979) repor ted on the cumulat ive outcomes of PCL pat ients undergoing hematopoiet ic
s tem ce l l t ransplantat ion repor ted in the l i terature. Median surviva l post–autologous HSCT
was 36 months, whereas i t was on ly 12 months after al logenic HSCT. Two authors have
independent ly noted the presence of an increased number of c i rcu la t ing large granular
lymphocytes af ter stem ce l l t ransplantat ion (974,980) ; d isappearance of these ce l ls in one
pat ient co inc ided wi th relapse (974) . The s igni f icance and impl icat ion of these observat ions
are yet to be determined.
Osteosclerotic Myeloma (POEMS Syndrome) Osteosclerot ic myeloma is a rare variant o f myeloma (≤3.3% of cases) (981) . There is a
s t raight os teosc lerot ic var iant that is s imi lar to mult ip le myeloma in that anemia, s ign i f icant
bone marrow p lasmacytos is , hyperca lcemia, and renal insuf f ic iency occur (143) . Surviva l in
these pat ients is comparable to that o f c lass ic mul t ip le myeloma pat ients. There is , however,
a more in terest ing form, which is known as Crow-Fukase syndrome, PEP (p lasma ce l l
dyscrasia , endocr inopathy, polyneuropathy) syndrome, Takatsuk i syndrome, and POEMS
syndrome (polyneuropathy, organomegaly, endocr inopathy, M prote in, and sk in changes)
(982,983,984,985). Th is var iant is associa ted wi th mul t ip le paraneoplast ic phenomena, and
i ts natural history is not s imi lar to that o f c lass ic mult ip le myeloma. The acronym POEMS
captures severa l o f the dominant features of the syndrome, but i t omi ts the sclerot ic bone
lesions, Cast leman disease, papi l ledema, per iphera l edema, asc i tes , polycythemia,
thrombocytos is , fa t igue, and c lubbing commonly observed in the d isorder. Not al l features
are requi red to make the d iagnosis ; a t a minimum, however, a pat ient must have: (a)
per iphera l neuropathy, (b) os teosc lerot ic myeloma ( i .e . , a c lonal plasma ce l l dyscras ia and
at least one sc lerot ic bone lesion) or Cast leman d isease, and (c) at least one of the other
previously ment ioned features (985) . The peak inc idence of POEMS syndrome is in the f i f th
and s ixth decades of l i fe, and there is a male predominance (983,985,986) .
Al though the precise mechanism of POEMS syndrome is unknown, VEGF appears to be a
dr iv ing fac tor in th is disorder (987,988,989) . Despi te the presence of os teosc lerot ic bone
lesions, which microscopical ly conta in c lonal plasma cel l in f i l t ra tes , bone marrow aspira te
and b iopsy of the i l iac crest typ ica l ly y ie ld on ly ~5% monoclonal lambda plasma ce l ls
(982,985,987) .
Treatment for th is disorder is far f rom s tandardized. Most agree that for an iso la ted
p lasmacytoma, i rradia t ion is the preferred t reatment (990,991,992,993) . Radiat ion therapy
produces substant ial improvement o f the neuropathy in more than hal f o f the pat ients
P.2415
who have a s ingle les ion or mult ip le les ions in a l imited area. I f there are widespread
lesions, chemotherapy and, potent ia l ly , per iphera l blood s tem cel l t ransplantat ion should be
cons idered (994). Responses of sys temic symptoms and sk in changes tend to precede those

of the neuropathy, wi th the former beginning to respond wi th in a month and the la t ter wi thin
3 to 6 months.
The most common causes of death are cardiorespi ratory fai lure, progressive inani t ion,
in fec t ion, capi l lary leak–l ike syndrome, and renal fa i lure (982,985). The neuropathy may be
unrelent ing and contr ibute to progress ive inani t ion and eventual card iorespi ratory fai lure
and pneumonia. St roke and myocard ia l in farct ion, which may or may not be rela ted to the
POEMS syndrome (985) , are a lso observed causes of death. Pat ients do not d ie o f c lass ic
myeloma ( i .e . , progressive bone marrow fai lure or hypercalcemia) .
Treatment of Complications and Supportive Care
Pharmacologic Therapy of Myeloma Bone Disease Myeloma bone d isease is a s igni f icant contr ibutor to morb idi ty, and there is expanding
in format ion about the re la t ionships between bone turnover and p lasma cel l growth and
surviva l (142,758,995,996,997) . Local ly ac t ing osteoc lastogenic and resorpt ive factors by
both osteoblasts and st romal ce l ls are dependent on a number o f in teract ions between them
and the myeloma ce l ls. Th is neoplast ic un i t releases in f lammatory and eros ive cytok ines,
such as IL-1β , IL-3, IL-6, IL-11, TNF-α , and a parathyro id hormone-rela ted prote in ,
hepatocyte growth fac tor, bas ic f ibrob last growth fac tor , meta l loproteases, and macrophage
in f lammatory protein-1α (142,997) .
The s tandard method of fo l lowing pat ients is wi th periodic (every 6 to 12 months) skele ta l
rad iographs; the use of more sophist icated imaging modal i t ies has been descr ibed in a
previous sect ion. Cross-l inked N-te lopept ides of type I co l lagen, which can be measured in
the serum or ur ine, appear to be a sens i t ive indicator o f bone turnover (922,998) , and
ur inary levels show a s trong pos i t ive correlat ion wi th the dynamic histomorphometr ic indices
of bone resorpt ion (999). Serum leve ls of bone metabol ism markers such as osteocalc in ,
MIP-1α , RANKL, and osteopetegr in have been s tud ied and shown to be aberrant ly
expressed in pat ients wi th ac t ive myeloma (142). Despi te carefu l moni tor ing, pat ients are at
r isk for skele ta l events . Bes ides t reat ing the under ly ing disease wi th chemotherapy,
b isphosphonates have been the mainstay of pharmacolog ic therapy of myelomatous bone
d isease. Other drugs, such as bone-seek ing radionuc l ides (524,686,1000) and inh ib i tors o f
the receptor ac t ivator o f nuclear fac tor κB (RANK) s ignal ing known as osteoproteger in
(1001), are be ing tes ted.
Month ly in t ravenous admin is t ra t ion of pamidronate has been shown to reduce the l ike l ihood
of a ske le tal event by a lmost 50% in pat ients wi th mul t ip le myeloma (1002).
Bisphosphonates inhib i t d issolu t ion of the hydroxyapat i te crys ta ls and down-regulate the
major os teoc las t funct ions. Af ter interna l izat ion, the n i t rogen-conta in ing b isphosphonates
in ter fere wi th the b iosynthet ic mevalonate pathway by inhib i t ing farnesyl diphosphonate
synthase, wi th the resu l t ing inabi l i ty o f os teoc lasts to form the ru ff led borders of the i r
membrane needed to act ivate bone resorpt ion. In th is s tudy, 392 pat ients wi th s tage I I I
myeloma and at least one lyt ic lesion received e i ther p lacebo or pamidronate, 90 mg
in t ravenously admin is tered as a 4-hour in fus ion month ly for 21 cyc les (F ig . 99.15B).
Skeletal events (patho log ic f rac ture, radia t ion or surgery, and spinal cord compress ion) and
hyperca lcemia were assessed monthly. At 12 months, there were fewer ske le tal - rela ted
events in the pamidronate group than in placebo-t reated pat ients (28 vs . 44%; p < .001)
(1002,1003). W ith longer fo l low-up of 21 months, the d i f ference between groups persisted

but narrowed s l ight ly, to 28% in the pamidronate group versus 51% in the p lacebo group (p
< .015) (1004). Th is prospect ive s tudy subsequent ly led the U.S. Food and Drug
Admin is t ra t ion (FDA) to approve the use of the drug in th is set t ing.
Figure 99.15. Bone risk in multiple myeloma. A: Natural history of bone events in patients with newly diagnosed myeloma (1945 to 2001) without bisphosphonate support. (With permission, from Melton LJ 3rd, Kyle RA, Achenbach SJ, et al. Fracture risk with multiple myeloma: a population-based study. J Bone Miner Res 2005;20:487–493.) B: Pamidronate versus placebo in newly diagnosed myeloma patients. (With permission, from Berenson JR, Lichtenstein A, Porter L, et al. Long-term pamidronate treatment of advanced multiple myeloma patients reduces skeletal events. Myeloma Aredia Study Group. J Clin Oncol 1998;16:593–602.)
Equivalency of pamidronate and zo ledronic ac id has been demonstrated in two randomized
c l in ical t r ia ls , a randomized Phase I I t r ia l (1004) and a randomized Phase I I I t r ia l (1005) . In
the Phase I I I t r ia l , pat ients wi th mul t ip le myeloma or breast cancer , who had lyt ic d isease,
were t reated wi th zo ledronic ac id (4 or 8 mg per dose) or pamidronate (90 mg) every 3 to 4

weeks. The infus ion t ime for zoledronic acid was increased f rom 5 to 15 minutes during the
t r ia l because of an increase in creat in ine occurr ing more f requent ly among pat ients
receiv ing the rap id in fus ion. Renal problems cont inued to occur more of ten among pat ients
randomized to 8 mg zo ledronic acidum, and the ir dose was subsequent ly reduced to 4 mg.
The sample s ize was based on showing noninfer ior i ty of zo ledronic ac id to pamidronate. A
to tal of 1 ,648 pat ients were enrol led; 510 had mul t ip le myeloma and the remainder had
metastat ic breast cancer. The por t ion of pat ients wi th any SRE af ter 13 months d id not
d i f fer among the three treatments and did not d i f fer between the breast cancer and mult ip le
myeloma pat ients . In February 2002, the FDA approved an expanded ind icat ion for
zo ledronic acid for the t reatment o f pat ients wi th bone metastases that inc luded i ts use in
mult ip le myeloma.
P.2416
Despi te the fac t that the longest fo l low-up of pat ient in these s tud ies was 24 months, the
recommendation of the Amer ican Soc iety of Cl in ica l Oncology was to cont inue these agents
indef in i te ly a t month ly interva ls (1006). The rat ionale for pract ice was not data-driven, but
based on severa l theoret ical benef i ts . The f i rs t was that pat ients have cont inued bone
d isease throughout the course of the i r d isease. The second was predicated on the in v i t ro
and in v ivo (mur ine) data that bisphosphonates exert ant i tumor act iv i ty (995) .
In the shor t term, the drugs were wel l to lerated—occas ional episodes of mi ld pyrexia , renal
funct ion impai rment , myalgias , and hypocalcemia occurred. However, by 2003, avascular
os teonecrosis o f the jaw (ONJ) had been descr ibed as a new compl icat ion associated wi th
the ir use (1007,1008,1009,1010,1011,1012,1013,1014,1015,1016,1017,1018).
Bisphosphonate-assoc ia ted ONJ has been descr ibed in various mal ignancies, including
mult ip le myeloma, breast cancer , and prostate cancer. A management a lgor i thm for ONJ
has recent ly been publ ished (1019). I t has been seen in both the mandible and the maxi l la
but is more frequent in the former. The et io logy of ONJ is unc lear , but i t is l ike ly
mult i fac tor ia l in or ig in. Al though most pat ients who develop ONJ have had recent dental or
ora l surg ical procedures (70%), the remainder develop spontaneous ONJ (1012). Proposed
mechanisms include that inhibi t ion of os teoc las t act iv i ty reduces bone turnover and
remodel ing and that bisphosphonates prevent re lease of bone-speci f ic fac tors that promote
bone format ion (1020). In addi t ion, bisphosphonates, par t icu lar ly zo ledronic ac id, may have
ant iangiogenic e f fects, and impai red b lood supply has been impl icated in the development
o f ONJ. F ina l ly, heal ing of an open bony oral wound is chal lenged by bacter ia l insu l t f rom
ora l microf lora.
Table 99.20 Mayo Clinic Consensus Statement for Bisphosphonate Use in Patients with Multiple Myeloma

Clinical Scenario Guideline
MM and lytic disease evident on plain radiographs
Intravenous bisphosphonates should be administered monthly.
No lytic disease evident on plain radiographs, but osteopenia or osteoporosis on bone mineral density studies
It is reasonable to start intravenous bisphosphonates in these patients.
Smoldering MM Not recommended outside context of a clinical trial.
Duration of bisphosphonate Patients should receive infusions of bisphosphonates monthly for 2 y. After 2 y: If the patient has achieved remission and is in stable plateau phase off treatment, the bisphosphonates can be discontinued. If the MM still requires active treatment, the frequency of bisphosphonate infusions can be decreased to every 3 mo.
Choice of bisphosphonate In patients with newly diagnosed MM, we favor use of pamidronate over zoledronic acid.
Dental evaluation and follow-up of patients taking bisphosphonates
Encourage patients to have comprehensive dental evaluation before receiving any bisphosphonate treatment. Undergo invasive dental procedures before starting bisphosphonate treatment. See a dentist at least annually and maximize preventive care; report oral/dental symptoms promptly. Manage new dental problems conservatively and avoid dental extractions unless absolutely necessary. See an oral and maxillofacial surgeon if surgery is required. Practice good dental hygiene. Encourage physicians to Withhold bisphosphonate treatment for at least 1 mo before the procedure and do not

resume until the patient has recovered from invasive dental procedures.
Source: Lacy MQ, Dispenzieri A, Gertz MA, et al. Mayo clinic consensus statement for the use of bisphosphonates in multiple myeloma. Mayo Clin Proc 2006;81:1047–1053.
The t rue inc idence of this compl icat ion is hard to es t imate. Durie and co l leagues (1015)
per formed a W eb-based survey of 1 ,203 pat ients wi th myeloma and breast cancer and found
an incidence of 6.8% in pat ients wi th MM and 4.4% in pat ients wi th breast cancer. The data
a lso suggested that the inc idence was higher in pat ients t reated wi th zoledronic acid than in
those treated wi th pamidronate (1015).
In another s tudy, Bamias et al . est imated inc idence rates in myeloma pat ients o f 9 .9%
(1014), and found that the t ime of exposure was st rongly associa ted wi th development o f
ONJ, and that ra tes were h igher in zo ledronic acid–treated pat ients. Pat ients who
developed ONJ received a median number of 35 in fus ions ( range, 13 to 68) , compared to 15
in fus ions ( range, 6 to 74) for pat ients wi th no ONJ. Median t ime of exposure to
b isphosphonates was 39.3 months for pat ients wi th ONJ (range, 11 to 86 months) ,
compared wi th 19 months (4 to 84.7) for pat ients wi th no osteonecros is . The l ike l ihood of
develop ing ONJ was 1% in the f i rs t year o f t reatment , increasing to 21% at 3 years of
t reatment for zo ledronic ac id–t reated pat ients, whereas in the non-zo ledronic ac id–t reated
pat ients the ra tes were 0 the f i rs t 2 years and 7% af ter 4 years of t reatment .
These observat ions prompted the Mayo Cl in ic Myeloma Group to prof fer a Consensus
Guidel ine Statement (Table 99.20) (1020). The recommendation is o f 2 years of monthly
therapy for pat ients wi th myelomatous bone disease, fo l lowed by e i ther cessat ion of therapy
in pat ients who are of f ac t ive t reatment for the i r myeloma, or cont inuat ion of
b isphosphonate therapy every 3 months for those who are rece iv ing ongoing therapy for
the ir myeloma. These recommendat ions are bo ls tered by two recent observat ions. The f i rs t
is the natural history o f myeloma bone
P.2417
d isease in the days before bisphosphonate use; the per iod wi th the h ighest ra tes of bone
d isease is the f i rs t 2 years (1021). The second is a repor t by the IFM group that
pamidronate use after tandem t ransplant for low-r isk pat ients does not provide any
s ign i f icant reduct ion in ske le tal events (618) .
Nonpharmacologic Treatment of Myeloma Bone Disease When lyt ic lesions are d iscovered in long bones, the r isk o f f racture has been demonstrated
to be very high i f pain is aggravated by funct ional use of that l imb or i f the les ion occupies

more than two th i rds of the diameter of that bone. Such lesions should be s tab i l ized by
in ternal f ixat ion (1022). Endostea l resorpt ion of one hal f the cort ica l width of the femur
weakens the bone by 70%. Surg ical t reatment should be cons idered for these lesions as
wel l (1023) . Once a bone has fractured, heal ing can occur , especial ly i f proper interna l
f ixat ion is performed and i f pat ients have an ant ic ipated survival of >6 months. Much of the
data regarding mal ignant bone disease are derived f rom pat ients wi th carcinoma rather than
mult ip le myeloma. In pat ients wi th carc inoma metastat ic to bone, modest postoperat ive
rad ia t ion doses (≤3,000 cGy) as adjuvant therapy are associa ted wi th better heal ing (1024),
but the ro le of ad juvant rad ia t ion therapy in mul t ip le myeloma pat ients is less c lear . Mul t ip le
myeloma is o ften chemotherapy-sensi t ive; adjuvant systemic chemotherapy in mul t ip le
myeloma pat ients may be more appropria te than ad juvant radia t ion therapy. In general ,
rad ia t ion therapy should be used for pa in rel ief in chemotherapy-ref rac tory d isease,
because i t re l ieves pain in 80 to 90% of pat ients wi th bony metastases (1025), long-term in
55 to 70% (1026).
Percutaneous vertebroplasty is occas ional ly an opt ion for pat ients wi th ver tebra l body
compress ion f rac ture. Pain re l ie f is genera l ly apparent wi th in 1 to 2 days af ter in jec t ion and
persists for a t least severa l months and up to severa l years (1027). Compl icat ions are
re lat ive ly rare, a l though some s tud ies repor ted a h igh incidence of c l in ica l ly ins ign i f icant
leakage of bone cement in to the paraver tebra l t issues. Compression of spinal nerve roots or
neura lgia as a resu l t o f the leakage of po lymer and pulmonary embol ism have also been
reported. Percutaneous kyphoplasty is a lso an opt ion (1028). To date, there are no
randomized tr ia ls to in form c l in ic ians as to which procedure is more ef fect ive.
Spinal Cord Compression In a paper publ ished in 1979, i t was est imated that near ly 10% of pat ients wi th myeloma
e i ther present wi th sp inal cord compress ion or that i t develops during the course of the
d isease (1029); wi th h igher awareness of myeloma and bet ter imaging technology, the
incidence is l ikely lower now. Cord compress ion, however, remains an important and
emergent subject . The usual s tandard t reatment is high-dose cort icostero ids and radia t ion
therapy (1030,1031,1032,1033). On rare occasions, surgica l decompress ion may be
cons idered. Because most myelomatous les ions ar ise f rom the ver tebral body, an anter ior
surgica l approach is genera l ly used, which may contr ibute addi t ional morbid i ty. One smal l
randomized tr ia l addressing the quest ion of rad iat ion versus laminectomy and radia t ion
showed no benef i t a t t r ibutable to laminectomy (1031); s imi lar ly, a larger re t rospect ive
ser ies found no benef i t (1030) . I f the def ic i t is a resul t o f compress ion by the p lasma cel l
tumor ( ra ther than a bone f ragment re t ropulsed by a pathologic compression f racture),
outcomes wi th rad ia t ion therapy are probably equal (or super ior) to surg ica l intervent ion in
a radiosensi t ive tumor such as myeloma (1030,1031).
High-dose cor t icosteroids may provide immediate pa in rel ie f and improvement in neurolog ic
funct ion (1032,1033). The opt imal cor t icostero id dose has not been establ ished, but
common dose schedules for metastat ic d isease inc lude dexamethasone in an ini t ia l bolus of
10 mg in t ravenously or 100 mg in t ravenously fol lowed by 4 mg oral ly 4 t imes da i ly (1034);
or a 100-mg in t ravenous bo lus fol lowed by 96 mg in 4 div ided doses for 3 days fo l lowed by
tapering doses (1032,1033).
Hypercalcemia

Pat ients wi th mult ip le myeloma are at r isk o f severe hypercalcemia that can prec ip i ta te
acute renal fa i lure, hyper tens ion, nausea, vomi t ing, pancreat i t is , card iac arrhythmia, coma,
and death. The ext racel lu lar vo lume deplet ion assoc iated wi th hypercalcemia should be
corrected by v igorous hydrat ion (727,1035) fol lowed by an ant i resorpt ive agent such as
in t ravenous b isphosphonate. Serum calc ium va lues usual ly dec l ine rap idly, reaching the
normal range wi thin 2 to 3 days in >80% of cases. I t occas ional ly goes be low normal at the
nadi r . Cor t icostero ids can a lso reduce serum calc ium concentrat ion in ~60% of pat ients wi th
hyperca lcemia (1036).
Gal l ium n i t ra te , mi thramycin, and ca lc i tonin are in terest ing f rom a his tor ica l perspect ive.
Since the advent o f b isphosphonates, they are not o ften used. Gal l ium n i t ra te therapy had
been shown to be superior to maximal ly approved doses of ca lc i tonin for acute control o f
cancer-re la ted hyperca lcemia (1037).
Hematologic Complications Including Anemia, Seconda ry
Leukemia, Hyperviscosity, and Cryoglobulinemia
Anemia
The anemia of mul t ip le myeloma can resul t f rom many fac tors . W hen the anemia is due
so le ly to myelomatous bone marrow in f i l t ra t ion, chemotherapy remedies the problem. Other
pat ients have a rela t ive erythropoiet in def ic iency re la ted to renal in jury due to the myeloma
or to age-rela ted changes. In these pat ients , as in any pat ient wi th renal insuf f ic iency,
modest doses of recombinant erythropoiet in are ef fect ive. For pat ients wi th chemotherapy-
induced anemia, recombinant erythropoiet in may be ef fec t ive at h igher doses (150 to 300
IU/kg three t imes week ly or 40,000 IU week ly) . Two p lacebo-contro l led t r ia ls in myeloma
pat ients demonstrate s ign i f icant ly improved hemoglobin levels and a reduced number of red
ce l l t ransfus ions in pat ients rece iv ing erythropoiet in (1038,1039). An inappropria te ly low
endogenous erythropoiet in concentrat ion is the most important fac tor predic t ing response
(1040)
Secondary Myelodysplasia and Acute Leukemia The most ominous cause of anemia in the sett ing of previous ly t reated mult ip le myeloma is
a secondary myelodysplast ic syndrome or acute leukemia. Kyle e t a l . (578) were among the
f i rst to recognize that cyto toxic agents can induce myelodysplasia and acute myelo id
leukemia (578,579,580,581) . The r isk o f a secondary myelodysplast ic syndrome or acute
leukemia is ~3% at 5 years and 10% at 8 to 9 years (1041,1042), wi th est imates as high as
25% at 10 years (1043), wi th mul t ip le o ther est imates somewhere in between (373,582,583).
Some authors have suggested that h igher cumulat ive doses of melphalan are impl icated as
a r isk for acute leukemia (1041). Others have shown no d i f ference in inc idence based on
the number o f courses of chemotherapy or the cumulat ive melphalan dose between pat ients
who d id and d id not develop acute leukemia (1042). In the F inn ish s tudy, the mean number
o f chemotherapy cyc les was 19.7 and 18.5 in pat ients wi th and wi thout secondary leukemia;
mean cumulat ive melphalan doses were 1,440 and 1,400 mg, respect ive ly (1042). Al though
cyc lophosphamide has been shown to be leukemogenic, data suggest that i t is less so than
melphalan (1041,1044,1045). Af ter secondary leukemia is d iagnosed, median surviva l tends
to be short—about 2 months (1042).
P.2418

The occurrence of concurrent acute leukemia in mult ip le myeloma suggests that there may
be a proc l iv i ty for acute leukemia to develop in pat ients wi th myeloma (1046,1047). After
s tem ce l l t ransplantat ion for myeloma, the r isk o f myelodysplast ic syndrome appears to be
re lated to pr ior chemotherapy ra ther than to the t ransplant i tsel f , a t least in one
re t rospect ive ser ies (1048).
Cryoglobulinemia
Approximate ly 5% of myeloma gammaglobul ins exhib i t revers ib le prec ip i ta t ion in the cold ,
so-ca l led cryoglobul ins , forming ei ther a f loccu lent precip i ta te or a ge l- l ike coagulum when
the serum is cooled (1049).
Hyperviscosity Plasmapheres is rel ieves the symptoms of hyperviscos i ty, but the benef i t o f th is t reatment in
the absence of concurrent chemotherapy is short- l ived (1050).
Renal Failure Normal c reat inine va lues are present in ~50% of mult ip le myeloma pat ients a t d iagnos is
(130,131,132,133,167,168,169,170) , and on ly 15 to 25% have a creat inine va lue >2 mg/d l
(132,173) . Pat ients in whom the renal fai lure is reversed have bet ter overa l l surviva l than
those wi thout improvement (171,174) . Factors that increase renal tubular cast format ion
include dehydrat ion, infec t ion, and hyperca lcemia. Mainta in ing a 24-hour f lu id in take of a t
least 3 L can improve renal funct ion (171) .
Because l ight chains wi th the lowest isoe lect r ic poin ts tend to be more nephrotoxic in
an imal models, avoidance of a low or ac idic ur inary pH is recommended. Ora l or
in t ravenous b icarbonate is useful in the sett ing of acute renal fa i lure (1051). The MRC 3rd
Myelomatos is Tr ia l randomized mult ip le myeloma pat ients wi th s ign i f icant renal fa i lure to
ora l sodium b icarbonate to neutra l ize ur ine pH (or not ), wi th a t rend toward bet ter surviva l
in the b icarbonate recipients (171) .
The use of p lasmapheres is in the sett ing of renal fa i lure remains controvers ial . There are
three randomized t r ia ls addressing this quest ion, wi th conf l ic t ing resul ts. One smal l
randomized s tudy of pat ients wi th ac t ive myeloma and progress ive renal fa i lure suggested
benef i t in a subset of pat ients (1052). Twenty-one pat ients were randomized to receive
e i ther forced d iures is and chemotherapy (10 pat ients) or forced diuresis , chemotherapy, and
p lasmapheres is (11 pat ients) . There was a t rend toward bet ter outcome in the
p lasmapheres is group, but the di f ference was not s tat is t ical ly s ign i f icant. I t is unclear
whether the lack of s ign i f icance is due to the smal l sample s ize or to an equiva lence of the
two therapeut ic st ra tegies. The s tudy d id demonstrate that the severi ty o f myeloma cast
format ion corre la ted di rec t ly wi th lack of improvement , regard less of t reatment st ra tegy.
Another randomized s tudy in myeloma pat ients wi th severe renal compromise compared
p lasma exchange (and hemodialys is when needed) wi th per i toneal d ia lysis (1053). Al l
pat ients rece ived chemotherapy and cor t icosteroids . Of the 29 pat ients in the s tudy, 24
received d ia lysis and 5 maintained serum creat in ine concentrat ions of >5 mg/dl wi thout
d ialys is . Th i rteen of the 15 pat ients in the p lasmapheres is (hemodia lysis group recovered
renal funct ion, reaching serum creat in ine va lues of ≤2.5 mg/d l in most cases, whereas on ly
2 pat ients in the per i toneal d ia lysis group had enough improvement to s top dialys is . The 1-

year surviva l ra tes were 66 and 28%, respect ive ly (p < .01) . The study's design was f lawed
in that one group received per i toneal d ia lysis and the other hemodialys is; the quest ion
about the ro le o f p lasmapheresis is not adequately sett led.
The largest and most recent tr ia l was a negat ive s tudy (1054). One hundred and four
pat ients wi th newly d iagnosed myeloma and a creat in ine of 2.3 mg/d l were randomized to
convent ional chemotherapy wi th or wi thout 5 to 7 sessions of plasma exchange over 10
days. The primary outcome was a composi te measure of death, dialys is dependence, or
g lomeru lar f i l t ra t ion ra te of <30 ml /min/1.73 m 2 . At 6 months the endpoint was reached in
58% of the p lasma exchange group and 69% of the contro l group. At 6 months, 7 of the 39
contro l pat ients (18%) and 5 of 58 p lasma exchange pat ients (9%) were on dialys is . At 6
months, 33% of each group had d ied. Cri t ic isms of this s tudy included the pat ient se lec t ion,
includ ing the absence of renal biopsy, the use of re lat ive ly inef fec t ive convent ional
chemotherapy, and smal l sample s ize. Pat ients were el ig ible i f the serum creat inine leve l
was at least 2 .3 mg/d l wi th an increase >0.6 mg/dl in the preceding 2 weeks despi te
correct ion of hypercalcemia, hypovolemia, and metabol ic acidos is . Th is impl ies that
inst i tu t ion of p lasma exchange was delayed and that there could have been other under ly ing
patho log ic renal lesions other than cast nephropathy, which would not be respons ive to
p lasma exchange. More than twice as many pat ients on the p lasma exchange group had
melphalan and prednisone as in the control group, which could have confounded the resul ts
because both overa l l response rates are lower and t ime to response is longer wi th
melphalan and prednisone than wi th VAD.
Infection Management In fec t ions are a major cause of morb id i ty in myeloma pat ients (1055,1056). Pneumonias and
ur inary t rac t in fect ions caused by Streptococcus pneumoniae, Haemophi lus in f luenzae, and
Escher ichia col i are most f requent (183,1057,1058,1059). The suscept ib i l i ty to in fec t ion
var ies wi th the phase of i l lness (182,1060). In one prospect ive s tudy, the overa l l ser ious
in fec t ion ra te was 0.92 in fec t ion per pat ient -year and was four t imes h igher dur ing per iods
of ac t ive d isease (1.90) than in p la teau-phase myeloma (0.49) (181). In a re t rospect ive
s tudy evaluat ing the sequential incidence of in fec t ion, the f i rs t 2 months of in i t ia l
chemotherapy emerged as a par t icular ly h igh-r isk per iod, wi th near ly ha l f o f the pat ients
exper ienc ing at least one cl in ica l ly s igni f icant in fec t ion (182) . In fec t ions la te in the course
of mul t ip le myeloma may be an inevi table resu l t of long-s tanding immunosuppress ion and
overwhelming tumor burden. Prevent ion of in fec t ion is a cr i t ica l goal for improving survival .
Prevent ion of in fect ions by use of vacc ines is an at t rac t ive st ra tegy. Unfortunate ly,
responses to vacc ines are poor among myeloma pat ients (191,1061,1062,1063). Pat ients
wi th myeloma were invest igated to assess whether immunologic r isk fac tors pred isposing to
ser ious in fec t ion could be ident i f ied (181) . Spec i f ic ant ibody t i ters to pneumococcal
capsular polysaccharides and te tanus and d iphther ia toxo ids were s igni f icant ly reduced
compared wi th the contro l populat ion. Low ant ipneumococcal and ant i -Escher ichia col i t i ters
corre lated wi th r isk o f ser ious in fec t ion. In addi t ion, among 41 immunized pat ients ,
responses to pneumococcus vacc ine and te tanus and d iphther ia toxo ids were poor. IgG
subc lass leve ls were s ign i f icant ly reduced, and a poor IgG response to pneumococcus
vaccine immunizat ion was associa ted wi th an increased r isk o f sept icemia. The predominant

s i te o f in fec t ion was the respi ratory t rac t. Decreased concentrat ions of the uninvolved
immunoglobul ins were s ign i f icant ly associa ted wi th a t least one serious infec t ion (181) .
The two most common prevent ion s t ra teg ies consis t of prophylaxis wi th ant ib io t ics (1064) or
in t ravenous immunoglobul in ( IVIg) (1064). A randomized, p lacebo-control led t r ia l o f
t r imethoprim-sul famethoxazole (TMP-SMX) demonstrated a s igni f icant decrease in severe
in fec t ions among newly d iagnosed myeloma pat ients randomized to TMP-SMX compared
wi th controls (1065). F i f ty-seven pat ients about to begin chemotherapy for mul t ip le myeloma
were randomly ass igned to prophylaxis for 2 months or to no prophylaxis (contro l) .
Ant ibio t ic prophylaxis cons is ted of TMP-SMX (160/800 mg ora l ly every 12 hours)
adminis tered for the f i rst 2 months of in i t ia l chemotherapy. Bacter ia l in fect ion occurred in
P.2419
11 contro l pat ients but in on ly 2 pat ients ass igned to rece ive TMP-SMX (p = .004) . Eight
severe infec t ions occurred in contro ls , compared wi th one in a TMP-SMX pat ient (p = .010).
Severe in fec t ions inc luded 5 cases of pneumonia (3 wi th seps is) , 2 ur inary t rac t infec t ions
wi th compl icat ing pneumonia or sepsis, 1 d ivert icu l i t is wi th per forat ion, and 1
s taphylococcal sca lded sk in syndrome. The rate of bacter ial in fec t ion was 2.43 per pat ient -
year for contro ls and 0.29 per pat ient -year for the TMP-SMX group (p = .001) . Toxic i ty (sk in
rash in 6 pat ients, nausea in 1 pat ient ) was not l i fe- threaten ing but requi red d iscont inuat ion
of TMP-SMX in 25% of pat ients . A randomized, double-bl ind p lacebo-contro l led t r ia l
demonstrated that IVIg s igni f icant ly reduced the number o f in fect ions in high-r isk pat ients
wi th p lateau-phase mult ip le myeloma (1064). Eighty- two such pat ients rece ived ei ther IVIg
(0 .4 g/kg per month) or an equal vo lume of p lacebo for 1 year . There were no episodes of
sept icemia or pneumonia in pat ients rece iv ing IVIg, compared wi th 10 in placebo pat ients (p
= .002) . There were 38 ser ious in fect ions in 470 pat ient -months for the p lacebo group,
compared wi th 19 in 449 pat ient -months for the IVIg group (p = .019). A poor ant ibody
response to pneumococcal vaccinat ion ( less than twofo ld increase) ident i f ied pat ients who
had maximum benef i t f rom IVIg. However, IVIg is expens ive and inconvenient and can be
associated wi th toxic i ty. Therefore, use of this agent is recommended only for pat ients wi th
a s igni f icant h is tory o f severe in fec t ions.
Differential Diagnosis The d iagnosis o f mul t ip le myeloma is made f rom a constel la t ion of f indings, inc lud ing
anemia, monoclonal prote ins , bone lesions, renal compl icat ions, hypercalcemia, and bone
marrow p lasmacytos is . Of ten the d iagnosis is stra ight forward, but other d isease ent i t ies
associated wi th hypergammaglobul inemia or monoc lonal bone marrow p lasma ce l ls must
a lso be cons idered. These inc lude react ive p lasmacytosis, MGUS, pr imary systemic
amyloidos is , W aldenström macroglobul inemia, l ight -chain deposi t ion d isease, acqui red
Fanconi syndrome, so l i tary p lasmacytoma, os teosclerot ic myeloma or POEMS syndrome,
and PCL.
Reactive Plasmacytosis and Polyclonal
Hypergammaglobulinemia React ive plasmacytosis and polyc lonal hypergammaglobul inemia must be d ist inguished f rom
a c lonal process. Pat ients wi th l iver d isease, chronic infec t ions including human

immunodef ic iency v i rus, connect ive t issue d iseases, o ther lymphopro l i ferat ive disorders ,
and carc inoma can have increased bone marrow p lasmacytos is (polyc lonal ) and
hypergammaglobul inemia (polyc lonal ) (24,119) . These condit ions should not be confused
wi th mul t ip le myeloma or MGUS, which are c lonal processes.
MGUS Two percent o f pat ients >50 years o ld have MGUS, which is a benign counterpar t or
precursor les ion of mul t ip le myeloma (108). I t is character ized by an M prote in in the serum
or ur ine, wi thout evidence of mul t ip le myeloma or other ser ious gammopathy-re lated
d isorder . MGUS pat ients do not have bone marrow suppression, ly t ic bone les ions,
hyperca lcemia, renal fa i lure, or suscept ib i l i ty to in fec t ion. Standard c l in ica l features do not
accurate ly predict which pat ients wi l l remain s tab le , and mul t ip le myeloma develops in ~1%
per year (108) . The cl in ica l d is t inc t ion between MGUS and asymptomatic mul t ip le myeloma
is derived f rom an arbi t rary def in i t ion (Table 99.2) , al though the under ly ing biologic
condi t ions may prove to be di f ferent .
The greatest chal lenges in di f ferent ia t ing MGUS f rom myeloma occur in pat ients who have
MGUS and (a) seni le osteoporos is , (b) renal insuf f ic iency f rom another cause, or (c )
hyperca lcemia due to hyperparathyro id ism. Approximate ly 50% of women >60 years have
osteoporos is , and a fract ion of these have vertebra l compress ion f ractures. CT scan of the
sp ine may help dist inguish between seni le os teoporos is and myelomatous bone d isease.
Simi lar ly, renal insuf f ic iency due to long-s tanding d iabetes, hyper tension, or nonsteroida l
drug use is not uncommon. In such cases, a pat ient may s t i l l have MGUS (or asymptomatic
myeloma, for that matter) and “end-organ damage.” The key is whether the damage is
a t t r ibutable to the p lasma prol i ferat ive d isorder or another cause. In some ins tances, renal
b iopsy may be requi red to c lar i fy this issue.
Primary Systemic Amyloidosis Primary systemic amylo idosis is a rare d isorder that is character ized by the depos i t ion of
amyloid f ibr i ls . These f ibr i ls are composed of immunoglobul in l ight -chain f ragments in a β -
p leated sheet conformation. I t should be suspected when a pat ient wi th a monoc lonal
protein in the serum or ur ine presents wi th nephrot ic - range prote inuria (pr imar i ly a lbumin)
wi th or wi thout renal insuf f ic iency, card iomyopathy, hepatomegaly, or per ipheral neuropathy.
Pat ients usual ly present wi th weight loss or fa t igue. Anemia is rare at presentat ion.
Symptoms rela ted to the af fec ted organ are a lso seen. A monoc lonal l ight chain is found in
the serum or ur ine in near ly 90% of pat ients wi th amylo idosis. Most o f the remaining
pat ients have monoclonal p lasma ce l ls detectable in the bone marrow; median percentage
of c lonal p lasma ce l ls in these pat ients is only 5%. A h is tologic d iagnosis is made by
demonstrat ing the amyloid f ibr i ls—green b i re f r ingence under polar ized l ight by us ing a
Congo red sta in , or 8- to 10-nm nonbranching f ibr i ls by elec t ron microscopy. The fat
aspi ra te is pos i t ive 70 to 80% of the t ime. The bone marrow demonstrates amylo id depos i ts
approximately hal f the t ime. Nearly 90% of pat ients wi th amylo id have a bone marrow or fa t
aspi ra te spec imen that is posi t ive for amylo id . In the remain ing 10%, a b iopsy spec imen of
the af fec ted organ is posi t ive.
Waldenström Macroglobulinemia

Waldenström macroglobul inemia should not be confused wi th IgM myeloma, which
compr ises on ly ~1% of myeloma cases (132) . Pat ients wi th Waldenström macroglobul inemia
may have anemia, hyperviscosi ty, B symptoms, bleeding, and neurologic symptoms.
Signi f icant lymphadenopathy or splenomegaly may a lso be present . Lyt ic bone disease is
markedly uncommon; i f i t is present , cons ider whether the pat ient has IgM myeloma. In
Waldenström macroglobul inemia, bone marrow biopsy typ ical ly reveals inf i l t ra t ion wi th
c lonal lymphoplasmacyt ic ce l ls (CD20-pos i t ive) . The natura l his tory and treatment opt ions
for Waldenström macroglobul inemia are d i f ferent f rom those of mul t ip le myeloma (1066).
Light-Chain Deposition Disease The nonamylo idogenic l ight -chain deposi t ion d iseases (LCDDs) are due to pathologic
protein depos i t ion in var ious t issues and organs. Unl ike the l ight -chain deposi ts observed in
pat ients wi th pr imary systemic amylo idos is , these in f i l t ra tes are not congophi l ic by l ight
microscopy, and by e lectron microscopy nonbranching f ibr i ls are not observed. Ins tead,
amorphous nodular depos i ts are seen.
LCDD may occur wi th or wi thout coexis t ing mul t ip le myeloma. Renal involvement is most
common, fo l lowed by card iac and hepat ic deposi ts . Cl in ica l ly, LCDD can be d i f ferent ia ted
f rom mul t ip le myeloma and primary systemic amylo idos is by the fo l lowing f indings. As in
pr imary systemic amyloidosis, ear ly in the d isease course the l ight -chain deposi ts have a
predi lec t ion for the renal g lomeru l i rather than the tubules. Th is resul ts in nonselect ive
proteinur ia , that is , a predominance of albuminuria , which is not
P.2420
usual in mul t ip le myeloma. I t is imposs ib le wi thout t issue b iopsy to dist inguish c l in ical ly the
cardiomyopathy and hepatopathy from primary systemic amyloidosis . In LCDD, the
under ly ing c lone is more commonly monoc lonal κ ra ther than λ .
The prognos is of pat ients who have this d isorder depends on whether there is under ly ing
mult ip le myeloma. In one re t rospect ive s tudy of 19 pat ients wi th LCDD, 5-year ac tuar ia l
pat ient surviva l and surviva l f ree of end-s tage renal d isease were 70 and 37%, respect ive ly
(1067).
Acquired Fanconi Syndrome Fanconi syndrome is a rare compl icat ion of p lasma cel l dyscrasias character ized by d i f fuse
fa i lure in reabsorpt ion at the level o f the proximal renal tubule and resul t ing in glycosuria ,
genera l ized aminoaciduria , and hypophosphatemia (179) . Fanconi f i rs t described the
syndrome in ch i ldren. Subsequent ly, acqui red forms were described in adul ts . Acqui red
Fanconi syndrome is usual ly assoc iated wi th MGUS. Overt hemato logic mal ignancies may
occur , such as mul t ip le myeloma, W aldenström macroglobul inemia, or other
lymphopro l i ferat ive d isorders. The prognos is is good in the absence of over t mal ignant
d isease. Cl in ica l manifestat ions include s lowly progressive renal fai lure and bone pain due
to os teomalacia . The d iagnos is of Fanconi syndrome can be made when a pat ient wi th a
monoclonal p lasma cel l d isorder presents wi th aminoac idur ia , phosphatur ia , and glycosuria .
Elect rolyte abnormal i t ies typ ica l ly inc lude hypokalemia, hypophosphatemia, and
hypouricemia. Bence Jones prote inur ia is usual ly present and is a lmost a lways of the κ type.
Rare pat ients have been repor ted wi th Fanconi syndrome associated wi th λ Bence Jones
proteinur ia .

Treatment cons is ts o f supplementat ion wi th phosphorus, ca lc ium, and vi tamin D.
Chemotherapy may benef i t pat ients wi th rapidly progressive renal fa i lure or symptomat ic
mal ignancy.
Solitary Plasmacytomas
Solitary Plasmacytoma of Bone (Intramedullary Plasmacytoma) Sol i tary plasmacytoma of bone is a rare form of plasma prol i ferat ive d isease. I ts t rue
incidence has not been descr ibed, but i t accounts for ~2 to 5% of mal ignant p lasma cel l
dyscrasias t reated at large referra l centers (223,1068,1069). In most ser ies , the def ini t ion
has requi red the fol lowing character is t ics : (a) histo log ic proof that the sol i tary lesion is a
p lasmacytoma; (b) no other bone lesions on metastat ic bone survey; (c ) <5% plasma cel ls
f rom a random bone marrow b iopsy s i te ; and (d) the absence of anemia, hypercalcemia, or
renal insuf f ic iency that had no at t r ibutab le cause. Some def in i t ions a l low for <10% bone
marrow p lasma ce l ls (718) , and others have rest r ic ted the quant i ty o f the serum or ur ine M
sp ike. Others have exc luded pat ients who developed d isseminated myeloma wi thin a year
a f ter d iagnosis o f the so l i tary plasmacytoma (1070). The In ternat ional Myeloma W ork ing
Group has adopted the above def in i t ion, but adds that i f MRI is done, i t should not
demonstrate any other areas of marrow invo lvement (220) .
There is a c lear male preponderance, and the median age is 55 years (718,1070,1071,1072).
Plasmacytomas most commonly ar ise f rom the axia l ske leton, par t icular ly the ver tebra l
bodies. Pain is the usual presentat ion. Spinal cord or nerve root compress ion may also be
present. I f the pat ient a lso has evidence of a periphera l neuropathy, and especia l ly i f the
bone lesion is sc lerot ic, one should cons ider the d iagnos is of POEMS. Monoclonal prote ins
are present in ~50% of pat ients (718,1070).
Careful s tag ing should be done in a l l pat ients , inc lud ing a complete b lood cel l count , protein
e lec t rophores is and immunofixat ion of the serum and ur ine, serum immunoglobul in f ree l ight
chains, a complete radiographic skele ta l survey, and random bone marrow aspi rat ion and
b iopsy. At a min imum, immunohis tochemica l s tains should be done on the bone marrow to
ident i fy a c lone apart f rom the so l i tary p lasmacytoma. MRI of the ent i re sp ine and pelv is
should also be done to determine whether the lesion is so l i tary. Us ing MRI, Moulopoulos et
a l . (157) found unexpected bone marrow involvement in 4 o f 12 pat ients wi th apparent ly
so l i tary p lasmacytomas of bone. FDG-PET may also provide useful in format ion.
From a h is tor ica l perspect ive, so l i tary plasmacytomas of bone were t reated surgica l ly wi th
or wi thout ad juvant rad iat ion (1073). Present-day, s ing le-modal i ty, def in i t ive rad ia t ion
therapy is the t reatment o f choice. Al though the opt imal dose has not been estab l ished by
randomized control led t r ia ls, 4 ,000 to 5 ,000 cGy encompassing a l l d isease wi th a marg in of
normal t issue is recommended by most exper ts on the basis o f re t rospect ive loca l re lapse
ra te data (718,719,720,1074). Th is pr inciple , however, has been chal lenged by recent data
that show no di f ference in local contro l as long as the therapeut ic dose is >3,000 cGy (721) .
Median 10-year d isease-f ree survival is ~25 to 40% (718,1075). Median t ime to fa i lure, that
is , local relapse, appearance of another p lasmacytoma, or d isseminated myeloma, is about
2 years (718,721,1075). Risk fac tors for evo lu t ion to myeloma include absence of a
monoclonal prote in at presentat ion (nonsecretory d isease), depress ion of immunoglobul in
va lues at presentat ion, pers is tence of the monoc lonal protein a f ter t reatment (1075),
abnormal immunoglobul in f ree l ight -chain ra t io at presentat ion (1076), tumor s ize of >5 cm,

and a nonver tebra l presentat ion (721).The persis tence of a monoc lonal protein a f ter
rad ia t ion therapy does not guarantee re lapse (223,718) , even af ter >10 years of fo l low-up
(1075). In rare ins tances, the maximum reduct ion of myeloma protein may take several
years af ter complet ion of the radia t ion therapy (223,718) . Median survival for a l l pat ients
present ing wi th so l i tary p lasmacytoma of bone—based on data f rom pat ients s taged before
rout ine use of MRI and bone marrow c lonal i ty s tud ies—was ~10 years
(718,721,1069,1075,1077). For those who progressed to myeloma, the median surviva l was
44 months after the s tar t o f chemotherapy (223). Adjuvant chemotherapy has not been
shown to produce a surviva l advantage and carr ies the r isk o f t reatment- re la ted
myelodysplast ic syndromes or acute leukemia; i t cannot be recommended.
W ith increasing ly sens i t ive d iagnost ic techniques, the incidence of so l i tary myeloma wi l l
decrease, but probably the relapse rate wi l l too.
Extramedullary Plasmacytoma Sol i tary ext ramedul lary plasmacytomas represent ~3% of a l l p lasma cel l neoplasms (1078).
They most commonly af fec t men in the ir ear ly 60s and occur in the upper respi ratory t rac t
(paranasal s inuses, nose, nasopharynx, and tons i ls ) . They a lso occur in lymph nodes, lung,
thyro id, gast ro in tes t inal t ract , l i ver , spleen, pancreas, tes tes, breast , or sk in (1079).
Amylo id invo lvement of the plasmacytoma occurs on occas ion. Al though ext ramedul lary
p lasmacytomas are not common in newly d iagnosed mult ip le myeloma, c lassic myeloma
must be exc luded by thorough staging. A monoc lonal protein in the serum and ur ine, ly t ic
bone lesions, anemia, renal insuff ic iency, and hyperca lcemia should be exc luded.
His to log ica l ly, an ext ramedul lary p lasmacytoma should be di f ferent ia ted f rom react ive
p lasmacytos is , p lasma ce l l granuloma, poorly di f ferent ia ted neoplasms, and immunoblast ic
lymphoma. Some ext ra-medul lary plasmacytomas may represent marginal zone B-ce l l
lymphomas that have undergone p lasmacyt ic di f ferent ia t ion (1080). Dimopoulos et a l .
(1078) compi led 128 ext ramedul lary p lasmacytoma pat ients f rom e ight publ ished ser ies
(1069,1079,1081,1082,1083,1084,1085,1086) and summarized thei r c l in ica l course. The
loca l fa i lure rate was 7%, mul t i focal ext ramedul lary re lapse occurred in 13%, and c lass ic
myeloma developed in 15%. Local radia t ion therapy is the t reatment o f choice, and ad juvant
chemotherapy is not recommended. The 10-year d isease- free surviva l is 70 to 80%. Ozsahin
et al . (1076) compi led 52 pat ients through a Rare Cancer Network study. There f ind ings
were s imi lar , wi th a 5-year progress ion rate of about 25% and a 5-year surviva l approaching
90%.
P.2421
References 1. Harr is NL, Jaf fe ES, Ste in H, et al . A revised European-Amer ican class i f icat ion of
lymphoid neoplasms: a proposal f rom the In ternat ional Lymphoma Study Group. Blood
1994;84:1361–1392.
2 . Dal rymple J . On the microscopica l character o f mol l i t ies oss ium. Dubl in Q J Med Sci
1846;2:85–95.
3 . Kyle RA. Mul t ip le myeloma: an odyssey of discovery. Br J Haematol 2000;111:1035–1044.

4. Clamp JR. Some aspects o f the f i rs t recorded case of mult ip le myeloma. Lancet
1967;2:1354–1356.
5 . Bence Jones H. Chemical patho logy. Lancet 1847;2:88–92.
6 . von Rust izky J . Mul t ip les myelom. Deutsche Z Chi rurg ie 1873;3:162–172.
7 . Kahler O. Zur Symptomato log i i des mul t ip lem Myleoms; Beobachtung von Albumosurie .
Prager Med W ochensch 1889;14:45.
8 . Weber FP. Genera l lymphadenomatosis o f bones, one form of ‘mul t ip le myeloma. ’ J
Pathol 1898;5:59–64.
9 . Weber FP, Hutch ison R, MacLeod JJR. Mul t ip le myeloma (myelomatos is) , wi th Bence
Jones prote id in the ur ine (myelopathic, albumosur ia o f Bradshaw, Kahler 's d isease) . Am J
Med Sc i 1903;126:644–665.
10. W right JH. A case of mul t ip le myeloma. Bul l Johns Hopk ins Hosp 1933;52:156.
11. Jacobson VC. A case of mul t ip le myelomata wi th chronic nephr i t is showing Bence Jones
protein in ur ine and blood serum. J Urol 1917;1:167–178.
12. W alters W . Bence Jones prote inuria : a report o f three cases wi th metabol ic s tud ies.
JAMA 1921;76:641–645.
13. Arink in MI . Die in t ravi ta le Untersuchungsmethodik des Knochenmarks. Fo l ia Haemato l
1929;38:233–240.
14. Bayne-Jones S, W ilson DW . Immunologica l react ions of Bence Jones prote ins . I I .
Di f ferences between Bence Jones proteins f rom var ious sources. Bul l Johns Hopkins Hosp
1922;33:119–125.
15. Edelman GM, Gal ly JA. The nature of Bence Jones proteins : chemica l s imi lar i t ies to
po lypept ide chains of myeloma g lobul ins and normal gamma-globul ins . J Exp Med
1962;116:207–227.
16. Tise l ius A. Elec t rophoresis o f serum globul in . I I . Elec t rophoret ic analys is o f normal and
immune sera. Biochem J 1937;31:1464–1477.
17. Longsworth LG, Shedlovsky T, MacInnes DA. Elect rophoret ic patterns of normal and
patho log ical human b lood serum and p lasma. J Exp Med 1939;70:399–413.
18. Kunkel HG, Tisel ius A. Elec t rophores is of prote ins on f i l ter paper. J Gen Phys iol
1951;35:89–118.
19. Grabar P, W i l l iams CA. Méthode permet tant l 'é tude conjuguée des propr iétés
é lec t rophorét iques et immunochimiques d 'un mélange de protéines. Appl icat ion au sérum
sanguin. Biochim Biophys Acta 1953;10:193–194.
20. W i lson AT. Di rec t immunoelect rophoresis. J Immunol 1964;92:431–434.
21. Drayson M, Tang LX, Drew R, e t al . Serum f ree l ight-chain measurements for ident i fy ing
and moni tor ing pat ients wi th nonsecretory mul t ip le myeloma. Blood 2001;97:2900–2902.
22. Kunkel HG. The ‘abnormal i ty ’ o f myeloma prote ins . Cancer Res 1968;28:1351–1353.
23. Heremans JF. Immunochemica l s tud ies on prote in pathology. The immunoglobul in
concept . Cl in Chim Acta 1959;4:639–646.
24. W aldenstrom J. Studies of condi t ions associated wi th d is turbed gammaglobul in
format ion (gammopathies) . Harvey Lect 1961;57:211–231.
25. Geschickter CF, Copeland MM. Mul t ip le myeloma. Arch Surg 1928;16:807–863.
26. Magnus-Levy A. Bence-Jones-Eiweiss und Amylo id . Z Kl in Med 1931;116:510.
27. Salmon SE, Smith BA. Immunoglobul in synthes is and to ta l body tumor cel l number in
IgG mul t ip le myeloma. J Cl in Invest 1970;49:1114–1121.
28. Dur ie BG, Salmon SE. A cl in ica l s taging system for mul t ip le myeloma. Correla t ion of
measured myeloma ce l l mass wi th present ing c l in ica l features, response to t reatment , and
surviva l . Cancer 1975;36:842–854.
29. Snapper I . St i lbamidine and pentamidine in mul t ip le myeloma. JAMA 1947;133:157–161.
30. Hol land JR, Hos ley H, Schar lau C, e t a l . A control led t r ia l of urethane t reatment in
mult ip le myeloma. Blood 1966;27:328–342.
31. Alwal l N. Urethane and s t i lbamid ine in mul t ip le myeloma; repor t on 2 cases. Lancet
1947;2:388–389.
32. Loge JP and Rundles RW . Urethane (ethylcarbamate) therapy in mul t ip le myeloma.
Blood 1949;4:201.
33. Adams W S, Skoog WA. The mangagement o f mult ip le myeloma. J Chronic Dis
1957;6:446.
34. Thorn GW , Forsham PH, Frawley RF, e t a l . The c l in ical usefu lness of ACTH and
cor t isone. N Engl J Med 1950;242:824.
35. Salmon SE, Shadduck RK, and Schi l l ing A. Intermi t tent h igh-dose prednisone (NSC-
10023) therapy for mul t ip le myeloma. Cancer Chemother Rep 1967;51:179–187.
36. Blokh in N, Larionov L, Perevodchikova N, et a l . Cl in ica l exper iences wi th sarcolys in in
neoplast ic d iseases. Ann N Y Acad Sc i 1958;68:1128–1132.
37. Bergsagel DE, Sprague CC, Aust in C, et al . Evaluat ion of new chemotherpeut ic agents
in the t reatment o f mul t ip le myeloma. IV. L-Phenyalanine mustard (NSC-8806). Cancer
Chemother Rep 1962;21:87–99.
38. Bergsagel DE, Gr i f f i th KM, Haut A, e t a l . The t reatment o f plasma ce l l myeloma. Adv
Cancer Res 1967;10:311–359.
39. Korst DR, Cl i f ford GO, Fowler W M, et a l . Mult ip le myeloma. I I . Analysis o f
cyc lophosphamide therapy in 165 pat ients . JAMA 1964;189.
40. Mel ls tedt H, Aahre A, Bjorkholm M, e t al . In ter feron therapy in myelomatos is . Lancet
1979;2:697.
41. Alber ts DS, Salmon SE. Adriamyc in (NSC-123127) in the t reatment o f a lkyla tor- res is tant
mult ip le myeloma: a pi lot s tudy. Cancer Chemother Rep 1975;59:345–350.
42. Salmon SE. Ni t rosoureas in mul t ip le myeloma. Cancer Treatment Rep 1976;60:789–794.
43. Singhal S, Mehta J , Des ikan R, e t al . Ant i tumor act iv i ty o f thal idomide in re f rac tory
mult ip le myeloma. N Engl J Med 1999;341:1565–1571.
44. Or lowsk i RZ, St inchcombe TE, Mi tchel l BS, et a l . Phase I t r ia l o f the proteasome
inhib i tor PS-341 in pat ients wi th re f ractory hemato log ic mal ignanc ies. J Cl in Oncol
2002;20:4420–4427.
45. Richardson PG, Schlossman RL, Wel ler E, e t a l . Immunomodulatory drug CC-5013
overcomes drug res is tance and is wel l to lerated in pat ients wi th relapsed mult ip le myeloma.
Blood 2002;100:3063–3067.
46. Jemal A, Siegel R, Ward E, et al . Cancer s ta t is t ics, 2006. CA Cancer J Cl in
2006;56:106–130.
47. Howe HL, W ingo PA, Thun MJ, e t a l . Annual report to the nat ion on the s ta tus of cancer
(1973 through 1998), featur ing cancers wi th recent increas ing t rends. J Nat l Cancer Inst
2001;93:824–842.
48. Cuzick J. Mul t ip le myeloma. Cancer Surv 1994;19–20:455–474.

49. Schwartz GG. Mul t ip le myeloma: c lusters , c lues, and dioxins . Cancer Epidemio l
Biomarkers Prev 1997;6:49–56.
50. Maldonado JE, Kyle RA. Famil ia l myeloma. Report o f e ight fami l ies and a s tudy of
serum prote ins in thei r re la t ives. Am J Med 1974;57:875–884.
51. Grosbois B, Jego P, At ta l M, e t a l . Famil ia l mul t ip le myeloma: repor t of f i f teen fami l ies.
Br J Haematol 1999;105:768–770.
52. Brown LM, L inet MS, Greenberg RS, et al . Mul t ip le myeloma and fami ly h is tory o f
cancer among blacks and whi tes in the U.S. Cancer . 1999;85:2385–2390.
53. Lynch HT, W atson P, Tarantolo S, et al . Phenotyp ic heterogenei ty in mult ip le myeloma
fami l ies. J Cl in Oncol 2005;23:685–693.
54. Landgren O, L inet MS, McMaster ML, e t a l . Famil ia l character ist ics o f auto immune and
hematologic disorders in 8 ,406 mul t ip le myeloma patients : a populat ion-based case-contro l
s tudy. In t J Cancer 2006;118:3095–3098.
55. Al t ier i A, Chen B, Bermejo JL, e t a l . Famil ia l r isks and temporal incidence t rends of
mult ip le myeloma. Eur J Cancer 2006;42:1661–1670.
56. Bray I , Brennan P and Boffe t ta P. Recent t rends and fu ture projec t ions of lymphoid
neoplasms—a Bayes ian age-per iod-cohort analysis . Cancer Causes Contro l 2001;12:813–
820.
57. Ichimaru M, Ish imaru T, Mikami M, e t a l . Mul t ip le myeloma among atomic bomb
survivors in Hi rosh ima and Nagasak i , 1950–76: re la t ionship to radia t ion dose absorbed by
marrow. J Nat l Cancer Ins t 1982;69:323–328.
58. Shimizu Y, Kato H, Schul l W J. Stud ies of the morta l i ty o f A-bomb survivors . 9 . Mortal i ty ,
1950–1985: Part 2 . Cancer mortal i ty based on the recent ly revised doses (DS86). Radiat
Res 1990;121:120–141.
59. Preston DL, Kusumi S, Tomonaga M, e t al . Cancer incidence in a tomic bomb survivors.
Par t I I I . Leukemia, lymphoma and mul t ip le myeloma, 1950–1987. Radiat Res 1994;137:S68–
S97.
60. Lewis EB. Leukemia, mul t ip le myeloma, and aplast ic anemia in American radiologists .
Sc ience 1963;142:1492.
61. Matanosk i GM, Sel tser R, Sar twel l PE, e t al . The current mortal i ty ra tes of rad io log is ts
and other phys ic ian specia l is ts : speci f ic causes of death. Am J Epidemiol 1975;101:199–
210.
62. W ang JX, Boice JD Jr , L i BX, e t al . Cancer among medica l d iagnost ic x- ray workers in
China. J Nat l Cancer Inst 1988;80:344–350.
63. W ing S, Richardson D, W olf S, e t a l . A case contro l study of mult ip le myeloma at four
nuclear fac i l i t ies . Ann Epidemio l 2000;10:144–153.
64. Mui rhead CR, Bingham D, Haylock RG, et a l . Fo l low up of morta l i ty and incidence of
cancer 1952-98 in men from the UK who par t ic ipated in the UK's a tmospher ic nuclear
weapon tes ts and exper imenta l programmes. Occup Environ Med 2003;60:165–172.
65. Pearce N, Pr ior I , Methven D, e t a l . Fol low up of New Zealand par t ic ipants in Br i t ish
atmospheric nuc lear weapons tes ts in the Paci f ic . Br Med J 1990;300: 1161–1166.
66. Fr iedman GD. Mul t ip le myeloma: rela t ion to propoxyphene and other drugs, rad ia t ion
and occupat ion. Int J Epidemiol 1986;15:424–426.
67. Andersson M, Storm HH. Cancer inc idence among Danish Thorot ras t -exposed pat ients .
J Nat l Cancer Ins t 1992;84:1318–1325.

68. Darby SC, Kendal l GM, Fel l TP, e t a l . A summary of mortal i ty and incidence of cancer in
men f rom the Uni ted Kingdom who par t ic ipated in the Uni ted Kingdom's atmospheric nuc lear
weapon tes ts and exper imenta l programmes. Br Med J (Cl in Res Ed) 1988;296:332–338.
69. Bof fe t ta P, Ste l lman SD, Garf inke l L . A case-contro l study of mult ip le myeloma nested in
the American Cancer Soc iety prospect ive s tudy. In t J Cancer 1989;43:554–559.
70. Cuzick J, De Stavola B. Mul t ip le myeloma—a case-contro l study. Br J Cancer
1988;57:516–520.
71. Davis FG, Boice JD Jr , Hrubec Z, e t al . Cancer mortal i ty in a rad ia t ion-exposed cohort
o f Massachuset ts tubercu los is pat ients . Cancer Res 1989;49:6130–6136.
72. Hatcher JL, Baris D, Olshan AF, et al . Diagnost ic rad ia t ion and the r isk o f mul t ip le
myeloma (United States). Cancer Causes Control 2001;12:755–761.
73. Boice JD, Jr , Mor in MM, Glass AG, et al . Diagnost ic x- ray procedures and r isk o f
leukemia, lymphoma, and mul t ip le myeloma. JAMA 1991;265:1290–1294.
74. Boice JD Jr , Day NE, Andersen A, e t a l . Second cancers fo l lowing radia t ion t reatment
for cervica l cancer . An in ternat ional col laborat ion among cancer regist r ies . J Nat l Cancer
Ins t 1985;74:955–975.
75. Darby SC, Dol l R, Gi l l SK, e t a l . Long term mortal i ty af ter a s ing le t reatment course wi th
X-rays in pat ients t reated for ankylos ing spondyl i t is . Br J Cancer 1987;55:179–190.
76. Semenciw RM, Morr ison HI , Riedel D, e t a l . Mul t ip le myeloma morta l i ty and agricu l tural
pract ices in the Pra i r ie provinces of Canada. J Occup Med 1993;35:557–561.
77. Pukkala E, Notkola V. Cancer inc idence among Finn ish farmers , 1979–93. Cancer
Causes Contro l 1997;8:25–33.
78. W iklund K, Dich J . Cancer r isks among male farmers in Sweden. Eur J Cancer Prev
1995;4:81–90.
79. Ronco G, Costa G, Lynge E. Cancer r isk among Danish and I tal ian farmers . Br J Ind
Med 1992;49:220–225.
P.2422
80. Kristensen P, Andersen A, I rgens LM, et al . Inc idence and r isk fac tors o f cancer among
men and women in Norwegian agr icul ture. Scand J Work Envi ron Heal th 1996;22:14–26.
81. Sonoda T, Ishida T, Mor i M, e t a l . A case-control study of mult ip le myeloma in Japan:
associat ion wi th occupat ional factors . As ian Pac J Cancer Prev 2005;6:33–36.
82. Cerhan JR, Cantor KP, W il l iamson K, e t a l . Cancer morta l i ty among Iowa farmers :
recent resu l ts , t ime t rends, and l i fes ty le fac tors (Uni ted States) . Cancer Causes Contro l
1998;9:311–319.
83. Nanni O, Fa lc in i F, Buiatt i E, e t a l . Mul t ip le myeloma and work in agricu l ture: resu l ts o f
a case-contro l s tudy in For l i , I ta ly. Cancer Causes Control 1998;9:277–283.
84. Pahwa P, McDuf f ie HH, Dosman JA, et al . Exposure to an imals and se lec ted r isk fac tors
among Canadian farm res idents wi th Hodgk in 's d isease, mul t ip le myeloma, or soft t issue
sarcoma. J Occup Envi ron Med 2003;45:857–868.
85. Khuder SA, Mutg i AB. Meta-analyses of mult ip le myeloma and farming. Am J Ind Med
1997;32:510–516.
86. Gal lagher RP, Thre l fa l l W J. Cancer mortal i ty in meta l workers. Can Med Assoc J
1983;129:1191–1194.

87. Fr i tsch i L , Siemiatyck i J . Lymphoma, myeloma and occupat ion: resu l ts o f a case-control
s tudy. In t J Cancer 1996;67:498–503.
88. McLaughl in JK, Malker HS, L inet MS, e t a l . Mul t ip le myeloma and occupat ion in Sweden.
Arch Envi ron Heal th 1988;43:7–10.
89. Rinsky RA, Smith AB, Hornung R, et al . Benzene and leukemia. An epidemio log ic r isk
assessment . N Engl J Med 1987;316:1044–1050.
90. Goldstein BD. Is exposure to benzene a cause of human mul t ip le myeloma? Ann N Y
Acad Sci 1990;609:225–230.
91. Decouf le P, Blat tner WA, Bla i r A. Morta l i ty among chemical workers exposed to benzene
and other agents. Envi ron Res 1983;30:16–25.
92. Bergsagel DE, Wong O, Bergsagel PL, e t a l . Benzene and mult ip le myeloma: appra isal
o f the scient i f ic evidence. Blood 1999;94:1174–1182.
93. Sonoda T, Nagata Y, Mor i M, e t a l . Meta-analys is o f mul t ip le myeloma and benzene
exposure. J Epidemiol 2001;11:249–254.
94. W ong O, Raabe GK. A cr i t ica l review of cancer epidemio logy in the petroleum industry,
wi th a meta-analysis o f a combined database of more than 350,000 workers . Regul Toxico l
Pharmacol 2000;32:78–98.
95. Thompson MA, Kyle RA, Mel ton LJ 3rd, e t a l . Ef fec t o f s tat ins , smoking and obes i ty on
progress ion of monoclonal gammopathy of undetermined sign i f icance: a case-control s tudy.
Haematologica 2004;89:626–628.
96. Gramenzi A, But t ino I , D 'Avanzo B, e t a l . Medical history and the r isk o f mul t ip le
myeloma. Br J Cancer 1991;63:769–772.
97. Brown LM, Everet t GD, Gibson R, et al . Smoking and r isk o f non-Hodgk in 's lymphoma
and mul t ip le myeloma. Cancer Causes Contro l 1992;3:49–55.
98. Brownson RC. Cigaret te smoking and r isk o f myeloma. J Nat l Cancer Ins t
1991;83:1036–1037.
99. Tavani A, La Vecchia C, Gal lus S, e t a l . Red meat in take and cancer r isk : a study in
I ta ly. In t J Cancer 2000;86:425–428.
100. Brown LM, Gr id ley G, Pot tern LM, et a l . Diet and nutr i t ion as r isk fac tors for mult ip le
myeloma among blacks and whi tes in the United States. Cancer Causes Control
2001;12:117–125.
101. Koessel SL, Theis MK, Vaughan TL, e t a l . Soc ioeconomic sta tus and the incidence of
mult ip le myeloma. Epidemiology 1996;7:4–8.
102. Baris D, Brown LM, Si lverman DT, e t a l . Soc ioeconomic s tatus and mult ip le myeloma
among US b lacks and whi tes . Am J Publ ic Heal th 2000;90:1277–1281.
103. Johnston JM, Gruf ferman S, Bourguet CC, e t al . Socioeconomic status and r isk o f
mult ip le myeloma. J Epidemiol Community Heal th 1985;39:175–178.
104. Brown LM, Everet t GD, Burmeis ter LF, e t a l . Hai r dye use and mult ip le myeloma in
whi te men. Am J Publ ic Heal th 1992;82:1673–1674.
105. Thun MJ, Al tekruse SF, Namboodi r i MM, et a l . Hai r dye use and r isk o f fa tal cancers in
U.S. women. J Nat l Cancer Ins t 1994;86:210–215.
106. Grodstein F, Hennekens CH, Cold i tz GA, e t a l . A prospect ive s tudy of permanent ha i r
dye use and hematopoiet ic cancer . J Nat l Cancer Inst 1994;86:1466–1470.

107. Correa A, Jackson L, Mohan A, e t a l . Use of ha ir dyes, hematopoiet ic neoplasms, and
lymphomas: a l i terature review. I I . Lymphomas and mul t ip le myeloma. Cancer Invest
2000;18:467–479.
108. Kyle RA, Therneau TM, Rajkumar SV, et al . A long- term s tudy of prognos is in
monoclonal gammopathy of undetermined signi f icance. N Engl J Med 2002;346:564–569.
109. Kyle RA. Diagnosis o f mul t ip le myeloma. Semin Oncol . 2002;29:2–4.
110. Cesana C, Klersy C, Barbarano L, et al . Prognost ic factors for mal ignant
t ransformat ion in monoclonal gammopathy of undetermined s igni f icance and smolder ing
mult ip le myeloma. J Cl in Oncol 2002;20:1625–1634.
111. Landgren O, Gr idley G, Turesson I , et al . Risk of monoc lonal gammopathy of
undetermined signi f icance (MGUS) and subsequent mul t ip le myeloma among Afr ican
American and whi te veterans in the Uni ted States. Blood 2006;107:904–906.
112. Gregersen H, Pedersen G, Svendsen N, e t al . Mul t ip le myeloma fo l lowing an ep isode
of communi ty-acqui red pneumococcal bacteraemia or mening i t is . Apmis 2001;109:797–800.
113. Bourguet CC, Logue EE. Ant igenic s t imulat ion and mul t ip le myeloma. A prospect ive
s tudy. Cancer 1993;72:2148–2154.
114. Katusic S, Beard CM, Kur land LT, e t a l . Occurrence of mal ignant neoplasms in the
Rochester , Minnesota, rheumato id ar thr i t is cohort . Am J Med 1985;78:50–55.
115. Isomaki HA, Hakul inen T, Joutsenlaht i U. Excess r isk o f lymphomas, leukemia and
myeloma in pat ients wi th rheumato id ar thr i t is . J Chronic Dis 1978;31:691–696.
116. Lewis DR, Pottern LM, Brown LM, et al . Mul t ip le myeloma among blacks and whi tes in
the Uni ted States: the role of chronic ant igenic s t imulat ion. Cancer Causes Control
1994;5:529–539.
117. Koepsel l TD, Dal ing JR, W eiss NS, e t al . Ant igenic st imulat ion and the occurrence of
mult ip le myeloma. Am J Epidemio l 1987;126:1051–1062.
118. L inet MS, Har low SD and McLaughl in JK. A case-contro l study of mul t ip le myeloma in
whi tes : chronic ant igenic s t imulat ion, occupat ion, and drug use. Cancer Res 1987;47:2978–
2981.
119. Dispenzier i A, Gertz MA, Therneau TM, et a l . Retrospect ive cohort study of 148
pat ients wi th polyc lonal gammopathy. Mayo Cl in Proc 2001;76:476–487.
120. Goedert JJ . The Epidemio logy of acquired immunodefic iency syndrome mal ignanc ies.
Semin Oncol 2000;27:390–401.
121. Gru l ich AE, W an X, Law MG, et al . Risk of cancer in people wi th AIDS. AIDS
1999;13:839–843.
122. Monte l la M, Cr ispo A, Fr igeri F, e t a l . HCV and tumors corre la ted wi th immune system:
a case-contro l s tudy in an area of hyperendemic i ty. Leuk Res 2001;25:775–781.
123. Gharagozloo S, Khoshnoodi J , Shokr i F. Hepat i t is C vi rus in fect ion in pat ients wi th
essent ial mixed cryoglobul inemia, mul t ip le myeloma and chronic lymphocyt ic leukemia.
Pathol Oncol Res 2001;7:135–139.
124. Yoshikawa M, Imazu H, Ueda S, e t a l . Prevalence of hepat i t is C vi rus in fec t ion in
pat ients wi th non-Hodgkin 's lymphoma and mul t ip le myeloma. A report f rom Japan. J Cl in
Gastroenterol 1997;25:713–714.
125. Ret t ig MB, Ma HJ, Vesc io RA, et al . Kapos i 's sarcoma-associa ted herpesvirus in fec t ion
of bone marrow dendr i t ic cel ls f rom mul t ip le myeloma pat ients . Sc ience 1997;276:1851–
1854.

126. Hjalgr im H, Frisch M, Melbye M. Inc idence rates of c lassica l Kapos i 's sarcoma and
mult ip le myeloma do not corre la te . Br J Cancer 1998;78:419–420.
127. Tar te K, Chang Y, Kle in B. Kaposi 's sarcoma-assoc ia ted herpesvi rus and mul t ip le
myeloma: lack of cr i ter ia for causal i ty. B lood 1999;93:3159–3163; d iscussion 3163–3154.
128. Cannon MJ, F landers W D, Pel le t t PE. Occurrence of pr imary cancers in assoc ia t ion
wi th mul t ip le myeloma and Kapos i 's sarcoma in the Uni ted States, 1973–1995. In t J Cancer
2000;85:453–456.
129. Tedeschi R, Kvarnung M, Knekt P, e t a l . A prospect ive seroepidemio log ical study of
human herpesvirus-8 in fec t ion and the r isk of mul t ip le myeloma. Br J Cancer 2001;84:122–
125.
130. Kyle RA. Mul t ip le myeloma: review of 869 cases. Mayo Cl inic Proc 1975;50:29–40.
131. Riccard i A, Gobbi PG, Ucci G, e t al . Changing c l in ical presentat ion of mul t ip le
myeloma. Eur J Cancer 1991;27:1401–1405.
132. Kyle RA, Gertz MA, W itz ig TE, e t a l . Review of 1027 pat ients wi th newly d iagnosed
mult ip le myeloma. Mayo Cl in Proc 2003;78:21–33.
133. Kapadia SB. Mul t ip le myeloma: a c l in icopatholog ic study of 62 consecut ive ly autopsied
cases. Medic ine (Bal t ) 1980;59:380–392.
134. Osserman EF. Plasma Cel l Myeloma. I I . Cl in ica l Aspects . N Engl J Med 1959;261:952–
960.
135. Fossa A, Brandhorst D, Myk lebust JH, e t al . Relat ion between S-phase f rac t ion of
myeloma ce l ls and anemia in pat ients wi th mul t ip le myeloma. Exp Hematol 1999;27:1621–
1626.
136. Musto P, Falcone A, D'Arena G, et al . Cl in ica l resul ts of recombinant erythropoiet in in
t ransfus ion-dependent pat ients wi th re f rac tory mul t ip le myeloma: role o f cytokines and
moni tor ing of erythropoies is . Eur J Haematol 1997;58:314–319.
137. Si lvest r is F, Caf for io P, Tucc i M, e t a l . Negat ive regulat ion of erythrob last maturat ion
by Fas-L(+)/TRAIL(+) h igh ly mal ignant plasma ce l ls : a major pathogenetic mechanism of
anemia in mul t ip le myeloma. Blood 2002;99:1305–1313.
138. Kyle RA, F inke ls tein S, Elveback LR, e t a l . Incidence of monoc lonal proteins in a
Minnesota communi ty with a c luster o f mul t ip le myeloma. Blood 1972; 40:719–724.
139. Kyle RA and Garton JP. The spectrum of IgM monoclonal gammopathy in 430 cases.
Mayo Cl in Proc 1987;62:719–731.
140. Bata i l le R, Chappard D, Marce l l i C, et al . Recru i tment o f new osteoblasts and
osteoc lasts is the earl iest c r i t ical event in the pathogenes is of human mul t ip le myeloma. J
Cl in Invest 1991;88:62–66.
141. Roodman GD. Role of the bone marrow microenvi ronment in mul t ip le myeloma. J Bone
Minera l Res 2002;17:1921–1925.
142. Si lvest r is F, Lombard i L , De Mat teo M, e t al . Myeloma bone disease: pathogenet ic
mechanisms and c l in ica l assessment . Leuk Res 2007;31:129.
143. Lacy MQ, Gertz MA, Hanson CA, e t al . Mul t ip le myeloma associa ted wi th d i f fuse
osteosclerot ic bone les ions: a c l in ical ent i ty d is t inc t f rom osteosclerot ic myeloma (POEMS
syndrome). Am J Hemato l 1997;56:288–293.
144. Kyle RA, Jowsey J , Kel ly PJ, e t al . Mul t ip le-myeloma bone d isease. The comparat ive
ef fec t o f sodium f luor ide and calc ium carbonate or p lacebo. J Engl J Med 1975;293:1334–
1338.

145. L indst rom E, Lindstrom FD. Skeletal scin t igraphy wi th technet ium d iphosphonate in
mult ip le myeloma—a comparison wi th skele ta l x- ray. Acta Med Scand 1980;208:289–291.
146. Catalano L, Pace L, Cal i fano C, e t a l . Detect ion of foca l myeloma lesions by
technet ium-99m-sestaMIBI sc int igraphy. Haemato log ica 1999;84:119–124.
147. Alexandrakis MG, Kyr iakou DS, Passam F, et a l . Value of Tc-99m sestamib i
scin t igraphy in the detect ion of bone les ions in mul t ip le myeloma: compar ison wi th Tc-99m
methylene diphosphonate. Ann Hemato l 2001;80:349–353.
148. Bal lear i E, Vi l la G, Garre S, e t a l . Technet ium-99m-sestamib i sc int igraphy in mult ip le
myeloma and rela ted gammopath ies: a useful too l for the ident i f icat ion and fo l low-up of
myeloma bone d isease. Haematologica 2001;86:78–84.
149. Font i R, Del Vecchio S, Zannet t i A, e t a l . Bone marrow uptake of 99mTc-MIBI in
pat ients wi th mul t ip le myeloma. Eur J Nuc l Med 2001;28:214–220.
150. Pace L, Cata lano L, Del Vecchio S, e t a l . Predic t ive va lue of technet ium-99m sestamib i
in pat ients wi th mul t ip le myeloma and potent ia l ro le in the fol low-up. Eur J Nuc l Med
2001;28:304–312.
151. Svaldi M, Tappa C, Gebert U, e t a l . Technet ium-99m-sestamib i sc in t igraphy: an
a l ternat ive approach for d iagnos is and fo l low-up of ac t ive myeloma les ions after h igh-dose
chemotherapy and auto logous s tem cel l t ransplantat ion. Ann Hemato l 2001;80:393–397.
P.2423
152. Schi r rmeis ter H, Bommer M, Buck K, e t a l . In i t ia l resu l ts in the assessment of mul t ip le
myeloma us ing (18)F-FDG PET. Eur J Nucl Med 2002;29:361–366.
153. Laroche M, Assoun J , Sixou L, et al . Comparison of MRI and computed tomography in
the various s tages of plasma ce l l d isorders : correla t ions wi th b iolog ica l and h is to log ical
f indings. Myelome-Mid i -Pyrenees Group. Cl in Exp Rheumatol 1996;14:171–176.
154. Lecouvet FE, Vande Berg BC, Malghem J, et a l . Magnetic resonance and computed
tomography imaging in mult ip le myeloma. Semin Musculoskelet Radio l 2001;5:43–55.
155. Per tu iset E, Bel la iche L, Lio te F, e t a l . Magnet ic resonance imaging of the spine in
p lasma ce l l dyscrasias . A review. Rev Rhum Engl Ed 1996;63:837–845.
156. Mar ie t te X, Zagdanski AM, Guermazi A, e t al . Prognost ic va lue of ver tebra l les ions
detected by magnet ic resonance imaging in pat ients wi th s tage I mul t ip le myeloma. Br J
Haematol 1999;104:723–729.
157. Moulopoulos LA, Dimopoulos MA, W eber D, e t al . Magnetic resonance imaging in the
s tag ing of so l i tary p lasmacytoma of bone. J Cl in Oncol 1993;11:1311–1315.
158. Lecouvet FE, Malghem J, Michaux L, e t a l . Skeletal survey in advanced mult ip le
myeloma: rad iographic versus MR imaging survey. Br J Haemato l 1999;106:35–39.
159. Nanni C, Zamagni E, Farsad M, e t al . Role of (18)F-FDG PET/CT in the assessment of
bone invo lvement in newly d iagnosed mult ip le myeloma: prel iminary resul ts . Eur J Nuc l Med
Mol Imaging. 2006;33:525–531.
160. Moulopoulos LA, Dimopoulos MA, Alexanian R, e t a l . Mul t ip le myeloma: MR pat terns of
response to treatment . Radio logy 1994;193:441–446.
161. Moulopoulos LA, Varma DG, Dimopoulos MA, e t a l . Mul t ip le myeloma: spina l MR
imaging in pat ients wi th unt reated newly d iagnosed disease. Radio logy 1992;185:833–840.
162. Stab ler A, Baur A, Bar t l R, e t a l . Contrast enhancement and quant i ta t ive s ignal
analys is in MR imaging of mul t ip le myeloma: assessment o f foca l and di f fuse growth
pat terns in marrow correla ted wi th b iopsies and surviva l ra tes . AJR Am J Roentgenol
1996;167:1029–1036.
163. Kusumoto S, J innai I , I toh K, et al . Magnetic resonance imaging pat terns in pat ients
wi th mul t ip le myeloma. Br J Haematol 1997;99:649–655.
164. Moulopoulos LA, Gika D, Anagnostopoulos A, e t a l . Prognost ic s igni f icance of
magnetic resonance imaging of bone marrow in previous ly unt reated pat ients wi th mul t ip le
myeloma. Ann Oncol 2005;16:1824–1828.
165. Lecouvet FE, Vande Berg BC, Michaux L, et a l . Stage I I I mul t ip le myeloma: c l in ical and
prognost ic va lue of spina l bone marrow MR imaging. Radiology 1998;209:653–660.
166. Maldonado JE, Velosa JA, Kyle RA, e t a l . Fanconi syndrome in adults. A mani fes tat ion
of a latent form of myeloma. Am J Med 1975;58:354–364.
167. Blade J , Fernandez-L lama P, Bosch F, et al . Renal fa i lure in mul t ip le myeloma:
present ing features and predic tors o f outcome in 94 pat ients from a s ingle ins t i tu t ion. Arch
In tern Med 1998;158:1889–1893.
168. Knudsen LM, Hippe E, Hjor th M, e t a l . Renal funct ion in newly d iagnosed mul t ip le
myeloma—-a demographic s tudy of 1353 pat ients. The Nordic Myeloma Study Group. Eur J
Haematol 1994;53:207–212.
169. Report on the second myelomatosis t r ia l a f ter f ive years of fo l low-up. Medical
Research Counc i l 's Working Party on Leukaemia in Adul ts . Br J Cancer 1980;42:813–822.
170. I r ish AB, W inear ls CG, L i t t lewood T. Presentat ion and surviva l o f pat ients wi th severe
renal fai lure and myeloma. Q J Med 1997;90:773–780.
171. Analys is and management o f renal fa i lure in four th MRC myelomatos is t r ia l . MRC
work ing par ty on leukaemia in adul ts . Br Med J (Cl in Res Ed) 1984; 288:1411–1416.
172. MacLennan IC, Cooper EH, Chapman CE, e t a l . Renal fa i lure in myelomatos is . Eur J
Haematol Suppl 1989;51:60–65.
173. Knudsen LM, Hjor th M, Hippe E. Renal fa i lure in mul t ip le myeloma: revers ib i l i ty and
impact on the prognos is . Nord ic Myeloma Study Group. Eur J Haematol 2000;65:175–181.
174. Bernste in SP, Humes HD. Reversible renal insuf f ic iency in mul t ip le myeloma. Arch
In tern Med 1982;142:2083–2086.
175. Torra R, Blade J , Cases A, e t a l . Pat ients wi th mul t ip le myeloma requi r ing long- term
d ialys is : present ing features, response to therapy, and outcome in a series of 20 cases. Br
J Haemato l 1995;91:854–859.
176. Hi l l GS, More l -Maroger L, Mery JP, et al . Renal les ions in mul t ip le myeloma: thei r
re lat ionship to assoc ia ted prote in abnormal i t ies . Am J Kidney Dis 1983;2:423–438.
177. Montseny JJ, Kle inknecht D, Meyr ier A, e t al . Long-term outcome according to renal
h isto logica l les ions in 118 pat ients wi th monoclonal gammopath ies . Nephro l Dia l Transplant
1998;13:1438–1445.
178. DeFronzo RA, Cooke CR, W right JR, et al . Renal funct ion in pat ients wi th mul t ip le
myeloma. Medicine (Balt) 1978;57:151–166.
179. Ma CX, Lacy MQ, Rompala JF, et al . Acqui red Fanconi syndrome is an indolent
d isorder in the absence of overt mul t ip le myeloma. Blood 2004;104:40–42.
180. Espersen F, Bi rgens HS, Hertz JB, e t al . Current patterns of bacter ial infec t ion in
myelomatos is . Scand J In fec t Dis 1984;16:169–173.

181. Hargreaves RM, Lea JR, Gr i f f i ths H, e t a l . Immunologica l fac tors and r isk o f in fect ion
in pla teau phase myeloma. J Cl in Pathol 1995;48:260–266.
182. Perr i RT, Hebbel RP, Oken MM. In f luence of t reatment and response s ta tus on
in fec t ion r isk in mul t ip le myeloma. Am J Med 1981;71:935–940.
183. Savage DG, Lindenbaum J, Garret t TJ. Biphas ic pat tern of bacter ial in fec t ion in
mult ip le myeloma. Ann In tern Med 1982;96:47–50.
184. Lackner H. Hemostat ic abnormal i t ies assoc ia ted wi th dysprote inemias. Semin Hemato l
1973;10:125–133.
185. Sai f MW , Al legra CJ, Greenberg B. Bleeding d iathesis in mul t ip le myeloma. J
Hematother Stem Cel l Res 2001;10:657–660.
186. Colwel l NS, Tol le fsen DM, Bl inder MA. Ident i f icat ion of a monoc lonal thrombin inh ib i tor
associated wi th mul t ip le myeloma and a severe bleeding d isorder . Br J Haemato l
1997;97:219–226.
187. Khoory MS, Nesheim ME, Bowie EJ, e t a l . Ci rculat ing heparan sul fate proteoglycan
ant icoagulant f rom a pat ient wi th a plasma ce l l d isorder . J Cl in Invest 1980;65:666–674.
188. Catovsky D, Ikoku NB, Pi tney W R, et a l . Thromboembol ic compl icat ions in
myelomatos is . Br Med J . 1970;3:438–439.
189. Shinagawa A, Koj ima H, Kobayashi T, e t a l . Lupus ant icoagulant- l ike act iv i ty observed
in a d imer ic lambda prote in produced by myeloma ce l ls . In t J Hematol 2001;73:526–531.
190. Yas in Z, Quick D, Th iagarajan P, e t a l . L ight-chain paraproteins wi th lupus
ant icoagulant ac t iv i ty. Am J Hemato l 1999;62:99–102.
191. Deitcher SR, Erban JK, L imentani SA. Acquired f ree prote in S def ic iency associa ted
wi th mul t ip le myeloma: a case repor t . Am J Hemato l 1996;51:319–323.
192. D'Angelo A, Mazzola G, Bergmann F, e t a l . Auto immune protein S def ic iency: a
d isorder predisposing to thrombosis . Haemato log ica 1995;80:114–121.
193. Zangari M, Saghaf i far F, Anaiss ie E, e t a l . Act ivated prote in C resis tance in the
absence of factor V Leiden mutat ion is a common f ind ing in mult ip le myeloma and is
associated wi th an increased r isk o f thrombotic compl icat ions. Blood Coagul F ibr ino lysis
2002;13:187–192.
194. Gargan PE, Plop l is VA, Scheu JD. A f ibr in speci f ic monoc lonal ant ibody which
in ter feres wi th the f ibr ino lyt ic e ffec t o f t issue plasminogen act ivator . Thromb Haemost
1988;59:426–431.
195. Bergsagel DE, Pruzansk i W . Treatment o f p lasma cel l myeloma wi th cytotoxic agents .
Arch In tern Med 1975;135:172–176.
196. McArthur JR, Athens JW , W int robe MM, et al . Melphalan and myeloma. Exper ience wi th
a low-dose cont inuous reg imen. Ann In tern Med 1970;72:665–670.
197. Larson RS, Sukpanichnant S, Greer JP, e t al . The spectrum of mult ip le myeloma:
d iagnost ic and b io log ical impl icat ions. Hum Pathol 1997;28:1336–1347.
198. Kapf f CT, Jandl JH. Blood al tas and sourcebook of hemato logy. 1991. Boston, Toronto,
London: L i t t le , Brown.
199. Gre ipp PR, Raymond NM, Kyle RA, e t a l . Mul t ip le myeloma: s ign i f icance of
p lasmablast ic subtype in morpholog ica l c lassi f icat ion. Blood 1985;65:305–310.
200. Bayrd ED. Bone marrow on sterna l asp i ra t ion in mul t ip le myeloma. Blood 1948;3:987–
1018.

201. Vacca A, Ribat t i D, Roncal i L , e t a l . Bone marrow angiogenes is and progress ion in
mult ip le myeloma. Br J Haematol 1994;87:503–508.
202. Rajkumar SV, Fonseca R, W itz ig TE, e t a l . Bone marrow angiogenes is in pat ients
achieving complete response af ter s tem cel l t ransplantat ion for mul t ip le myeloma. Leukemia
1999;13:469–472.
203. Abi ldgaard N, Bendix-Hansen K, Kr is tensen JE, et al . Bone marrow f ibrosis and
d isease act iv i ty in mult ip le myeloma monitored by the aminoterminal propept ide of
procol lagen I I I in serum. Br J Haemato l 1997;99:641–648.
204. Krzyzaniak RL, Buss DH, Cooper MR, et al . Marrow f ibros is and mul t ip le myeloma. Am
J Cl in Pathol 1988;89:63–68.
205. San Miguel JF, Garc ia-Sanz R, Gonzalez M, e t al . Immunophenotype and DNA cel l
content in mul t ip le myeloma. Bai l l ie res Cl in Haemato l 1995;8:735–759.
206. L in P, Owens R, Tr icot G, e t a l . F low cytometr ic immunophenotypic analysis o f 306
cases of mul t ip le myeloma. Am J Cl in Pathol 2004;121:482–488.
207. Mateo G, Castel lanos M, Rasi l lo A, e t a l . Genetic abnormal i t ies and pat terns of
ant igenic express ion in mult ip le myeloma. Cl in Cancer Res 2005;11:3661–3667.
208. Moreau P, Robi l lard N, Avet-Lo iseau H, e t a l . Pat ients wi th CD45 negat ive mul t ip le
myeloma receiv ing h igh-dose therapy have a shor ter surviva l than those wi th CD45 posi t ive
mult ip le myeloma. Haemato logica 2004;89:547–551.
209. Kumar S, Rajkumar SV, Kiml inger T, et al . CD45 express ion by bone marrow p lasma
ce l ls in mult ip le myeloma: c l in ical and b io log ical corre la t ions. Leukemia 2005;19:1466–1470.
210. Pel la t-Deceunynck C, Bar i l le S, Jego G, e t a l . The absence of CD56 (NCAM) on
mal ignant plasma ce l ls is a hal lmark of plasma ce l l leukemia and of a spec ia l subset o f
mult ip le myeloma. Leukemia 1998;12:1977–1982.
211. Van Riet I , De Waele M, Remels L, et al . Express ion of cytoadhesion molecules (CD56,
CD54, CD18 and CD29) by myeloma plasma ce l ls. Br J Haemato l 1991;79:421–427.
212. Barker HF, Hamil ton MS, Bal l J , e t a l . Express ion of adhes ion molecules LFA-3 and N-
CAM on normal and mal ignant human p lasma cel ls . Br J Haemato l 1992;81:331–335.
213. San Miguel JF, Gonzalez M, Gascon A, e t a l . Immunophenotyp ic heterogenei ty o f
mult ip le myeloma: in f luence on the bio logy and cl inica l course of the disease. Castel lano-
Leones (Spain) Cooperat ive Group for the Study of Monoclonal Gammopath ies . Br J
Haematol 1991;77:185–190.
214. Ocqueteau M, Orfao A, Garc ia-Sanz R, e t al . Express ion of the CD117 ant igen (c-Ki t )
on normal and myelomatous p lasma cel ls . Br J Haematol 1996;95:489–493.
215. Pel la t-Deceunynck C, Bar i l le S, Puthier D, et a l . Adhes ion molecules on human
myeloma ce l ls : s igni f icant changes in expression re la ted to mal ignancy, tumor spreading,
and immorta l izat ion. Cancer Res 1995;55:3647–3653.
216. Pope B, Brown RD, Gibson J , e t al . B7-2-posi t ive myeloma: incidence, c l in ica l
character is t ics , prognost ic s ign i f icance, and impl icat ions for tumor immunotherapy. Blood
2000;96:1274–1279.
217. Gre ipp PR, Kyle RA. Cl in ica l , morphologica l , and ce l l k inet ic di f ferences among
mult ip le myeloma, monoc lonal gammopathy of undetermined sign i f icance, and smoldering
mult ip le myeloma. Blood 1983;62:166–171.

218. W itzig TE, Timm M, Larson D, et al . Measurement o f apoptos is and pro l i ferat ion of
bone marrow p lasma cel ls in pat ients wi th p lasma cel l prol i ferat ive disorders . Br J Haemato l
1999;104:131–137.
219. Proposed guidel ines for protocol studies . I . In t roduct ion. I I . P lasma ce l l myeloma. 3 .
Chronic lymphocyt ic leukemia. IV. Chronic granulocyt ic leukemia. Cancer Chemother Rep
1973;4:141–173.
220. Cr i ter ia for the c lass i f icat ion of monoclonal gammopath ies , mul t ip le myeloma and
re lated d isorders : a repor t o f the Internat ional Myeloma W ork ing Group. Br J Haematol
2003;121:749–757.
221. Kyle RA, Gre ipp PR. 3 . The laboratory invest igat ion of monoclonal gammopathies .
Mayo Cl in Proc 1978;53:719–739.
222. Kyle RA, Gre ipp PR. Smolder ing mul t ip le myeloma. N Engl J Med 1980;302:1347–1349.
P.2424
223. Alexanian R. Local ized and indolent myeloma. Blood 1980;56:521–525.
224. Peest D, Leo R, Bloche S, et al . Low-dose recombinant in ter leuk in-2 therapy in
advanced mul t ip le myeloma. Br J Haemato l 1995;89:328–337.
225. Riccard i A, Ucci G, Luoni R, e t a l . Treatment o f mult ip le myeloma accord ing to the
extens ion of the disease: a prospect ive, randomised s tudy comparing a less wi th a more
aggress ive cystostat ic po l icy. Cooperat ive Group of Study and Treatment o f Mul t ip le
Myeloma. Br J Cancer 1994;70:1203–1210.
226. Hjorth M, Hel lquis t L , Holmberg E, e t al . In i t ia l versus deferred melphalan-prednisone
therapy for asymptomat ic mul t ip le myeloma stage I—a randomized study. Myeloma Group of
Western Sweden. Eur J Haematol 1993;50:95–102.
227. Facon T, Menard JF, Michaux JL, e t a l . Prognost ic factors in low tumour mass
asymptomatic mul t ip le myeloma: a repor t on 91 pat ients . The Groupe d 'Etudes et de
Recherche sur le Myelome (GERM). Am J Hemato l 1995;48:71–75.
228. Riccard i A, Mora O, Tine l l i C, e t a l . Long-term surviva l o f s tage I mult ip le myeloma
g iven chemotherapy jus t a f ter diagnos is or a t progress ion of the d isease: a mul t icentre
randomized s tudy. Cooperat ive Group of Study and Treatment o f Mul t ip le Myeloma. Br J
Cancer 2000;82:1254–1260.
229. W eber DM, Dimopoulos MA, Moulopoulos LA, e t a l . Prognost ic features of
asymptomatic mul t ip le myeloma. Br J Haemato l 1997;97:810–814.
230. W itzig TE, Kyle RA, O'Fal lon W M, et a l . Detect ion of peripheral blood p lasma ce l ls as
a pred ic tor o f d isease course in pat ients wi th smoulder ing mult ip le myeloma. Br J Haematol
1994;87:266–272.
231. Xiong Y, Donovan KA, Kl ine MP, e t a l . Ident i f icat ion of two groups of smoldering
mult ip le myeloma pat ients who are ei ther high or low producers of in ter leuk in-1. J In terferon
Cytok ine Res 2006;26:83–95.
232. Treatment o f myeloma. Comparison of melphalan, chlorambuci l , and azathioprine. Arch
In tern Med 1975;135:157–162.
233. Anonymous. Combinat ion chemotherapy versus melphalan p lus prednisone as
t reatment for mul t ip le myeloma: an overview of 6 ,633 pat ients f rom 27 randomized t r ia ls.
Myeloma Tr ia l is ts ' Col laborat ive Group. J Cl in Oncol 1998;16:3832–3842.

234. Gut terman JU, Blumenschein GR, Alexanian R, et al . Leukocyte in ter feron- induced
tumor regression in human metastat ic breast cancer , mul t ip le myeloma, and mal ignant
lymphoma. Ann In tern Med 1980;93:399–406.
235. Alexanian R, Gut terman J , Levy H. In ter feron t reatment for mul t ip le myeloma. Cl in
Haematol 1982;11:211–220.
236. Quesada JR, Hawkins M, Horn ing S, et al . Col laborat ive phase I - I I s tudy of
recombinant DNA-produced leukocyte in ter feron (c lone A) in metastat ic breast cancer ,
mal ignant lymphoma, and mul t ip le myeloma. Am J Med 1984;77:427–432.
237. McElwain T, Powles R. High-dose in t ravenous melphalan for p lasma-cel l leukaemia
and myeloma. Lancet 1983;2:822–824.
238. Alexanian R, Bonnet J , Gehan E, e t a l . Combinat ion chemotherapy for mul t ip le
myeloma. Cancer 1972;30:382–389.
239. McLaughl in P, Alexanian R. Myeloma prote in k inet ics fo l lowing chemotherapy. Blood
1982;60:851–855.
240. Oken MM, Kyle RA, Gre ipp PR, e t a l . Complete remiss ion induct ion wi th combined
VBMCP chemotherapy and in terferon ( rIFN alpha 2b) in pat ients wi th mul t ip le myeloma.
Leuk Lymphoma 1996;20:447–452.
241. Blade J , Samson D, Reece D, e t a l . Cr i ter ia for evaluat ing disease response and
progress ion in pat ients wi th mul t ip le myeloma treated by h igh-dose therapy and
haemopoiet ic s tem ce l l t ransplantat ion. Myeloma Subcommit tee of the EBMT. European
Group for Blood and Marrow Transplant . Br J Haemato l 1998;102:1115–1123.
242. Dur ie BG, Harousseau JL, Miguel JS, e t a l . In ternat ional un i form response cr i ter ia for
mult ip le myeloma. Leukemia 2006;20:1467–1473.
243. Selby PJ, McElwain TJ, Nandi AC, e t a l . Mul t ip le myeloma t reated wi th high dose
in t ravenous melphalan. Br J Haematol 1987;66:55–62.
244. Gore ME, Selby PJ, Viner C, e t al . In tens ive t reatment o f mul t ip le myeloma and cr i ter ia
for complete remission. Lancet 1989;2:879–882.
245. At ta l M, Harousseau JL, Stoppa AM, et al . A prospect ive, randomized t r ia l o f
autologous bone marrow t ransplantat ion and chemotherapy in mul t ip le myeloma.
In tergroupe Francais du Myelome [see comments] . N Engl J Med 1996;335:91–97.
246. Oken MM, Lenhard RE Jr , Tsia t is AA, et al . Contr ibut ion of prednisone to the
ef fec t iveness of hexamethylmelamine in mul t ip le myeloma. Cancer Treat Rep 1987;71:807–
811.
247. Alexanian R, Yap BS, Bodey GP. Prednisone pulse therapy for re f rac tory myeloma.
Blood 1983;62:572–577.
248. Costa G, Engle RL, Schi l l ing A, e t a l . Melphalan and prednisone: an ef fec t ive
combinat ion for the t reatment o f mul t ip le myeloma. Am J Med 1973; 54:589–599.
249. Rivers SL, Patno ME. Cyc lophosphamide vs melphalan in treatment o f plasma ce l l
myeloma. JAMA 1969;207:1328–1334.
250. Alexanian R, Haut A, Khan AU, e t a l . Treatment for mul t ip le myeloma. Combinat ion
chemotherapy wi th di f ferent melphalan dose reg imens. JAMA 1969; 208:1680–1685.
251. MacLennan IC, Chapman C, Dunn J , e t a l . Combined chemotherapy wi th ABCM versus
melphalan for t reatment o f myelomatosis. The Medica l Research Counc i l Working Party for
Leukaemia in Adults . Lancet 1992;339:200–205.

252. Myelomatosis : compar ison of melphalan and cyclophosphamide therapy. Br Med J.
1971;1:640–641.
253. Treatment comparisons in the thi rd MRC myelomatosis t r ia l . Medical Research
Counc i l 's Working Party on Leukaemia in Adults . Br J Cancer 1980; 42:823–830.
254. Lenhard RE Jr , Oken MM, Barnes JM, e t al . High-dose cyc lophosphamide. An ef fec t ive
t reatment for advanced ref rac tory mul t ip le myeloma. Cancer 1984; 53:1456–1460.
255. Mass RE. A comparison of the ef fec t o f prednisone and a p lacebo in the treatment o f
mult ip le myeloma. Cancer Chemother Rep 1962;16:257–259.
256. McIntyre OR, Pajak TF, Kyle RA, e t a l . Response rate and surviva l in myeloma pat ients
receiv ing prednisone alone. Med Pediat r Oncol 1985;13:239–243.
257. Alexanian R, Dimopoulos MA, Delasal le K, et a l . Pr imary dexamethasone t reatment o f
mult ip le myeloma. Blood 1992;80:887–890.
258. Alexanian R, Barlogie B, Dixon D. High-dose g lucocort ico id t reatment o f resis tant
myeloma. Ann Intern Med 1986;105:8–11.
259. Gertz MA, Garton JP, Gre ipp PR, e t a l . A phase I I s tudy of h igh-dose
methylpredniso lone in ref ractory or relapsed mul t ip le myeloma. Leukemia 1995;9:2115–2118.
260. Forgeson GV, Selby P, Lakhani S, et al . In fused vincr is t ine and adr iamycin wi th h igh
dose methylprednisolone (VAMP) in advanced previously t reated mult ip le myeloma pat ients .
Br J Cancer 1988;58:469–473.
261. Tip lady CW , Summerf ie ld GP. Cont inuous low-dose dexamethasone in re lapsed or
re f rac tory mul t ip le myeloma. [ let ter; comment ]. [see comments ] . Br J Haemato l
2000;111:381.
262. Palva IP, Ala-Har ja K, Almqvis t A, e t a l . Cor t icostero id is not benef ic ia l in mult ip le-
drug combinat ion chemotherapy for mul t ip le myeloma. Finnish Leukaemia Group. Eur J
Haematol 1993;51:98–101.
263. Facon T, Mary JY, Pegour ie B, e t al . Dexamethasone-based reg imens versus
melphalan-prednisone for e lder ly mul t ip le myeloma pat ients ine l ig ib le for h igh-dose therapy.
Blood 2006;107:1292–1298.
264. Feinman R, Koury J, Thames M, e t a l . Role of NF-kappaB in the rescue of mul t ip le
myeloma ce l ls from glucocort ico id- induced apoptos is by bcl -2 . Blood 1999;93:3044–3052.
265. Karadag A, Oyajobi BO, Apper ley JF, e t a l . Human myeloma cel ls promote the
product ion of inter leuk in 6 by pr imary human osteoblasts . Br J Haemato l 2000;108:383–390.
266. De Bosscher K, Vanden Berghe W , Vermeulen L, e t a l . Glucocor t icoids repress NF-
kappaB-dr iven genes by d isturbing the in teract ion of p65 wi th the basal t ranscr ipt ion
machinery, i r respect ive of coact ivator leve ls in the ce l l . Proc Natl Acad Sc i U S A.
2000;97:3919–3924.
267. Kawano M, Tanaka H, Ish ikawa H, et al . In ter leuk in-1 accelerates autocr ine growth of
myeloma ce l ls through inter leukin-6 in human myeloma. Blood 1989;73:2145–2148.
268. Jackson DV, Case LD, Pope EK, e t a l . S ingle agent v incr is t ine by in fus ion in re f rac tory
mult ip le myeloma. J Cl in Oncol 1985;3:1508–1512.
269. Cornwel l GG 3rd, Pajak TF, Kochwa S, e t a l . V incr is t ine and prednisone prolong the
surviva l o f pat ients receiv ing in t ravenous or ora l melphalan for mul t ip le myeloma: Cancer
and Leukemia Group B exper ience. J Cl in Oncol 1988;6:1481–1490.
270. Alexanian R, Salmon S, Bonnet J , e t al . Combinat ion therapy for mul t ip le myeloma.
Cancer 1977;40:2765–2771.

271. Alexanian R, Dreicer R. Chemotherapy for mul t ip le myeloma. Cancer 1984; 53:583–588.
272. Salmon SE. Immunoglobul in synthes is and tumor k inet ics o f mul t ip le myeloma. Semin
Hemato l 1973;10:135–144.
273. Lee BJ, Sahak ian G, Clarkson BD, et al . Proceedings: Combinat ion chemotherapy of
mult ip le myeloma wi th a lkeran, cytoxan, v incr is t ine, prednisone, and BCNU. Cancer
1974;33:533–538.
274. Case DC Jr , Lee DJ 3rd, Clarkson BD. Improved surviva l t imes in mult ip le myeloma
t reated wi th melphalan, prednisone, cyc lophosphamide, v incr is t ine and BCNU: M-2 protocol .
Am J Med 1977;63:897–903.
275. Salmon SE. Expansion of the growth f ract ion in mul t ip le myeloma wi th alkyla t ing
agents. Blood 1975;45:119–129.
276. Cornwel l GG 3rd, Pajak TF, Kochwa S, e t a l . Comparison of ora l melphalan, CCNU,
and BCNU wi th and wi thout v incr ist ine and prednisone in the t reatment o f mul t ip le myeloma.
Cancer and Leukemia Group B exper ience. Cancer 1982;50:1669–1675.
277. Hansen OP, Clausen NA, Drivsholm A, e t al . Phase I I I s tudy of in termi t tent 5-drug
reg imen (VBCMP) versus in termit tent 3-drug reg imen (VMP) versus intermi t tent melphalan
and prednisone (MP) in myelomatos is . Scand J Haematol 1985;35:518–524.
278. MacLennan IC, Cusick J. Object ive evaluat ion of the ro le o f v incr ist ine in induct ion and
maintenance therapy for myelomatos is . Medica l Research Counc i l W ork ing Party on
Leukaemia in Adults . Br J Cancer 1985;52:153–158.
279. Tr ibal to M, Amadori S, Cantonet t i M, e t al . Treatment of mul t ip le myeloma: a
randomized s tudy of three d i f ferent regimens. Leuk Res 1985;9:1043–1049.
280. MacLennan IC, Kel ly K, Crockson RA, et al . Resul ts o f the MRC myelomatos is t r ia ls for
pat ients entered since 1980. Hematol Oncol 1988;6:145–158.
281. Bennett JM, Si lber R, Ezdinl i E, e t a l . Phase I I s tudy of adriamyc in and b leomycin in
pat ients wi th mul t ip le myeloma. Cancer Treat Rep 1978;62:1367–1369.
282. Alber ts DS, Balcerzak SP, Bonnet JD, e t a l . Phase I I t r ia l o f mitoxantrone in mul t ip le
myeloma: a Southwest Oncology Group Study. Cancer Treat Rep 1985;69:1321–1323.
283. Sumpter K, Powles RL, Raje N, e t a l . Ora l idarubic in as a s ing le agent therapy in
pat ients wi th re lapsed or resistant mul t ip le myeloma. Leuk Lymphoma 1999;35:593–597.
284. Chises i T, Capnist G, de Domin ic is E, e t a l . A phase I I s tudy of idarubic in (4-
demethoxydaunorubic in) in advanced myeloma. Eur J Cancer Cl in Oncol 1988;24:681–684.
285. Gockerman JP, Barto lucc i AA, Nelson MO, et al . Phase I I evaluat ion of e topos ide in
re f rac tory mul t ip le myeloma: a Southeastern Cancer Study Group Tr ia l . Cancer Treat Rep
1986;70:801–802.
286. Barlogie B, Velasquez W S, Alexanian R, et a l . Etoposide, dexamethasone, cytarabine,
and c ispla t in in v incr ist ine, doxorubic in , and dexamethasone-refrac tory myeloma. J Cl in
Oncol 1989;7:1514–1517.
287. Tok iwa F, Utsunomiya A, Nakahara K, et al . [A case of re f ractory mult ip le myeloma
ef fec t ively t reated wi th long- term ora l e topos ide] . Gan To Kagaku Ryoho 1993;20:533–536.
288. Kato Y, Takeda H, Mihara H, e t al . Oral low-dose etoposide therapy for ref rac tory
mult ip le myeloma wi th ext ramedul lary invo lvement . In tern Med 1995; 34:1023–1026.
289. Costanzi JJ , Cooper MR, Scar f fe JH, e t a l . Phase I I study of recombinant alpha-2
in ter feron in resistant mul t ip le myeloma. J Cl in Oncol 1985;3:654–659.
P.2425

290. Brenning G, Ahre A and Ni lsson K. Corre la t ion between in v i t ro and in v ivo sens i t iv i ty
to human leucocyte in terferon in pat ients wi th mul t ip le myeloma. Scand J Haematol
1985;35:543–549.
291. Ahre A, Bjorkholm M, Mel ls tedt H, e t a l . Human leukocyte inter feron and intermi t tent
h igh-dose melphalan- prednisone admin is t rat ion in the t reatment o f mul t ip le myeloma: a
randomized c l in ical t r ia l f rom the Myeloma Group of Central Sweden. Cancer Treat Rep
1984;68:1331–1338.
292. Ohno R, Kimura K, Amaki I , et al . Treatment o f mult ip le myeloma wi th recombinant
human leukocyte A in ter feron. Cancer Treat Rep 1985;69:1433–1435.
293. D'Amato RJ, Loughnan MS, F lynn E, e t a l . Thal idomide is an inh ibi tor o f angiogenesis .
Proc Nat l Acad Sc i U S A 1994;91:4082–4085.
294. Kenyon BM, Browne F, D'Amato RJ. Ef fects o f thal idomide and related metabol i tes in a
mouse corneal model o f neovascular izat ion. Exp Eye Res 1997;64:971–978.
295. Rajkumar SV, Fonseca R, Dispenzier i A, e t a l . Thal idomide in the t reatment o f
re lapsed mul t ip le myeloma. Mayo Cl in Proc 2000;75:897–901.
296. Rajkumar SV. Current sta tus of thal idomide in the t reatment of cancer . Oncology
2001;(Ju ly) :867–874; .
297. Ber to l in i F, Mingrone W , Al ie t t i A, e t a l . Thal idomide in mul t ip le myeloma,
myelodysplast ic syndromes and h is t iocytosis. Analys is o f c l in ica l resu l ts and of surrogate
angiogenes is markers . Ann Oncol 2001;12:987–990.
298. Hus M, Dmoszynska A, Soroka-Woj taszko M, e t a l . Thal idomide t reatment o f resistant
or relapsed mult ip le myeloma pat ients . Haemato log ica 2001; 86:404–408.
299. Ju l iusson G, Cels ing F, Turesson I , e t a l . Frequent good par t ia l remissions f rom
tha l idomide inc luding best response ever in pat ients wi th advanced ref ractory and relapsed
myeloma. [see comments ] . Br J Haemato l 2000;109:89–96.
300. Knel ler A, Raanani P, Hardan I , et al . Therapy wi th thal idomide in ref ractory mul t ip le
myeloma pat ients—the reviva l of an old drug. Br J Haemato l 2000;108:391–393.
301. Blade J , Esteve J , Ros ino l L , e t a l . Thal idomide in re f rac tory and relaps ing mul t ip le
myeloma. Semin Oncol 2001;28:588–592.
302. Myers B, Crouch D, Dolan G. Thal idomide t reatment in advanced ref rac tory myeloma.
Br J Haematol 2000;111:986.
303. Tos i P, Ronconi S, Zamagni E, e t a l . Salvage therapy wi th thal idomide in mult ip le
myeloma pat ients relaps ing af ter auto logous periphera l b lood s tem cel l t ransplantat ion.
Haematologica 2001;86:409–413.
304. Kumar S, Gertz MA, Dispenzier i A, et al . Response rate, durabi l i ty o f response, and
surviva l a f ter thal idomide therapy for re lapsed mul t ip le myeloma.[comment ] . Mayo Cl in ic
Proc 2003;78:34–39.
305. Schey SA, Cavenagh J , Johnson R, e t a l . An UK myeloma forum phase I I s tudy of
tha l idomide; long term fol low-up and recommendat ions for treatment . Leuk Res
2003;27:909–914.
306. Rajkumar SV, Dispenzier i A, Fonseca R, et a l . Thal idomide for previously unt reated
indolent or smolder ing mul t ip le myeloma. Leukemia 2001;15:1274–1276.

307. Rajkumar SV, Gertz MA, Lacy MQ, et a l . Thal idomide as in i t ia l therapy for ear ly-stage
myeloma. Leukemia 2003;17:775–779.
308. W eber D, Rank in K, Gavino M, e t a l . Thal idomide alone or wi th dexamethasone for
previously unt reated mult ip le myeloma. J Cl in Oncol 2003;21:16–19.
309. Pini M, Barald i A, Pie t rasanta D, et al . Low-dose of tha l idomide in the t reatment o f
re f rac tory myeloma. Haemato log ica 2000;85:1111–1112.
310. Barlogie B, Des ikan R, Eddlemon P, e t a l . Extended surviva l in advanced and
ref rac tory mul t ip le myeloma af ter s ing le-agent tha l idomide: ident i f icat ion of prognost ic
fac tors in a phase 2 s tudy of 169 pat ients . Blood 2001;98:492–494.
311. Zangari M, Anaiss ie E, Barlogie B, et al . Increased r isk o f deep-ve in thrombosis in
pat ients wi th mul t ip le myeloma receiv ing thal idomide and chemotherapy. Blood
2001;98:1614–1615.
312. Osman K, Comenzo R and Rajkumar SV. Deep venous thrombosis and tha l idomide
therapy for mul t ip le myeloma. N Engl J Med 2001;344:1951–1952.
313. Camba L, Peccator i J , Pescaro l lo A, e t a l . Thal idomide and thrombosis in pat ients wi th
mult ip le myeloma. Haemato logica 2001;86:1108–1109.
314. Rajkumar SV, Gertz MA, W i tz ig TE. Li fe-threatening toxic ep idermal necro lysis wi th
tha l idomide therapy for myeloma. N Engl J Med 2000;343:972–973.
315. Fowler R and Imr ie K. Thal idomide-associa ted hepat i t is : a case repor t . Am J Hematol
2001;66:300–302.
316. Richardson PG, Blood E, Mi ts iades CS, e t al . A randomized phase 2 s tudy of
lenal idomide therapy for pat ients wi th re lapsed or re lapsed and ref rac tory mult ip le myeloma.
Blood 2006;108:3458.
317. Richardson P, Jagannath S, Hussein M, e t al . A mul t icenter, s ing le-arm, open- label
s tudy to eva luate the eff icacy and safety o f s ing le-agent lenal idomide in pat ients wi th
re lapsed and ref ractory mult ip le myeloma; prel in inary resul ts. ASH Annual Meet ing
Abstracts 2005;106:1565.
318. Schey SA, F ields P, Bar t le t t JB, e t a l . Phase I study of an immunomodulatory
tha l idomide analog, CC-4047, in relapsed or ref rac tory mul t ip le myeloma. J Cl in Oncol
2004;22:3269–3276.
319. Richardson PG, Barlogie B, Berenson J , e t al . A phase 2 s tudy of bortezomib in
re lapsed, re f rac tory myeloma. N Engl J Med 2003;348:2609–2617.
320. Richardson PG, Sonneveld P, Schuster MW, et a l . Bor tezomib or high-dose
dexamethasone for re lapsed mul t ip le myeloma. N Engl J Med 2005;352: 2487–2498.
321. Richardson PG, Barlogie B, Berenson J , e t al . Extended fol low-up of a phase I I t r ia l in
re lapsed, re f rac tory mul t ip le myeloma:: f inal t ime-to-event resul ts f rom the SUMMIT t r ia l .
Cancer 2006;106:1316–1319.
322. Jagannath S, Barlog ie B, Berenson J, e t a l . A phase 2 s tudy of two doses of
bor tezomib in re lapsed or re f rac tory myeloma. Br J Haemato l 2004;127:165–172.
323. Berenson JR, Jagannath S, Bar logie B, e t al . Safety of pro longed therapy wi th
bor tezomib in re lapsed or re f rac tory mul t ip le myeloma. Cancer 2005;104: 2141–2148.
324. Jagannath S, Durie BG, W olf J, et al . Bor tezomib therapy a lone and in combinat ion
wi th dexamethasone for previously unt reated symptomat ic mult ip le myeloma. Br J Haematol
2005;129:776–783.
325. Rousselot P, Labaume S, Maro l leau JP, e t al . Arsenic t r ioxide and melarsopro l induce
apoptos is in plasma ce l l l ines and in plasma ce l ls f rom myeloma pat ients. Cancer Res
1999;59:1041–1048.
326. Kalmadi SR, Hussein MA. The emerg ing ro le o f arsenic t r ioxide as an
immunomodulatory agent in the management o f mul t ip le myeloma. Acta Haemato l
2006;116:1–7.
327. Munshi NC, Tr icot G, Desikan R, e t a l . Cl in ica l ac t iv i ty o f arsenic tr ioxide for the
t reatment o f mult ip le myeloma. Leukemia 2002;16:1835–1837.
328. Hussein MA, Saleh M, Ravandi F, e t a l . Phase 2 study of arsenic t r ioxide in pat ients
wi th re lapsed or re f rac tory mult ip le myeloma. Br J Haemato l 2004;125:470–476.
329. Bonnet JD, Alexanian R, Salmon SE, e t a l . Addi t ion of c isp lat in and b leomycin to
v incr is t ine-carmust ine-doxorubic in-prednisone (VBAP) combinat ion in the t reatment o f
re lapsing or resistant mul t ip le myeloma: a Southwest Oncology Group s tudy. Cancer Treat
Rep 1984;68:481–485.
330. Broun GO Jr , Petruska PJ, Hi ramoto RN, e t a l . Cisp lat in, BCNU, cyc lophosphamide,
and prednisone in mul t ip le myeloma. Cancer Treat Rep 1982;66:237–242.
331. Barlogie B, Jagannath S, Des ikan KR, et al . Tota l therapy wi th tandem t ransplants for
newly d iagnosed mul t ip le myeloma. Blood 1999;93:55–65.
332. Kantarj ian H, Dre icer R, Bar log ie B, e t a l . High-dose cytos ine arabinos ide in mul t ip le
myeloma. Eur J Cancer Cl in Oncol 1984;20:227–231.
333. Ti re l l i U, Carbone A, Zagonei V, e t a l . Phase I I s tudy of tenipos ide (VM-26) in mul t ip le
myeloma. Am J Cl in Oncol 1985;8:329–331.
334. Kraut EH, Crowley JJ , W ade JL, e t a l . Evaluat ion of topotecan in resis tant and
re lapsing mul t ip le myeloma: a Southwest Oncology Group s tudy. J Cl in Oncol 1998;16:589–
592.
335. Grever MR, Crowley J , Salmon S, e t al . Phase I I invest igat ion of pentostat in in mul t ip le
myeloma: a Southwest Oncology Group s tudy. J Nat l Cancer Inst 1990;82:1778–1779.
336. Belch AR, Henderson JF, Brox LW . Treatment o f mul t ip le myeloma wi th
deoxycoformyc in. Cancer Chemother Pharmacol 1985;14:49–52.
337. Dimopoulos MA, Arbuck S, Huber M, e t al . Pr imary therapy of mult ip le myeloma wi th
pacl i taxe l ( taxo l ) . Ann Oncol 1994;5:757–759.
338. Mi l ler HJ, Leong T, Khandekar JD, e t al . Pacl i taxe l as the ini t ia l t reatment o f mul t ip le
myeloma: an Eastern Cooperat ive Oncology Group Study (E1A93). Am J Cl in Oncol
1998;21:553–556.
339. Ahmann FR, Meyskens FL Jr , Jones SE, e t a l . Phase I I evaluat ion of amsacrine (m-
AMSA) in sol id tumors, myeloma, and lymphoma: a Universi ty of Ar izona and Southwest
Oncology Group Study. Cancer Treat Rep 1983;67:697–700.
340. Gre ipp PR, Coleman M, Anderson K, et al . Phase I I t r ia l o f amsacr ine in pat ients wi th
mult ip le myeloma. Med-Pediat r -Oncol 1989;17:76–78.
341. Gockerman JP, Si lberman H, Bar to lucc i AA. Phase I I eva luat ion of aclarub ic in in
re f rac tory mul t ip le myeloma: a Southeastern Cancer Study Group Tr ia l . Cancer Treat Rep
1987;71:773–774.
342. Cornel l CJ Jr , Pajak TF, McIntyre OR. Chlorozotoc in: phase I I evaluat ion in pat ients
wi th myeloma. Cancer Treat Rep 1984;68:685–686.

343. Cohen HJ, Bar tolucc i AA. Hexamethylmelamine and prednisone in the t reatment o f
re f rac tory mul t ip le myeloma. Am J Cl in Oncol 1982;5:21–27.
344. Barlogie B, Crowley J , Salmon SE, e t a l . Phase I I s tudy of carboplat in (CBDCA) in
re f rac tory mul t ip le myeloma. A Southwest Oncology Group s tudy. Invest New Drugs
1994;12:53–55.
345. Kraut EH, Crowley JJ , Grever MR, et al . Phase I I s tudy of f ludarabine phosphate in
mult ip le myeloma. A Southwest Oncology Group s tudy. Invest New Drugs 1990;8:199–200.
346. Dimopoulos MA, Kantarj ian HM, Estey EH, et a l . 2-Chlorodeoxyadenos ine in the
t reatment o f mult ip le myeloma. Blood 1992;80:1626.
347. Dispenzier i A, Gertz MA, Lacy MQ, et al . Flavopi r idol in pat ients wi th relapsed or
re f rac tory mul t ip le myeloma: a phase 2 t r ia l wi th c l in ical and pharmacodynamic end-points .
Haematologica 2006;91:390–393.
348. Dispenzier i A, Gertz MA, Lacy MQ, et al . A phase I I t r ia l o f imatinib in pat ients wi th
re f rac tory/ re lapsed myeloma. Leuk Lymphoma 2006;47:39–42.
349. Dur ie BGM, Vi l larete L, Farvard A, e t a l . Clar i thromycin (Biaxin) as pr imary t reatemnt
for myeloma. Blood 1997;90:2578a.
350. Moreau P, Huynh A, Facon T, e t a l . Lack of e f f icacy of c lar i thromycin in advanced
mult ip le myeloma. In tergroupe Francais du Myelome (IFM) [ le t ter ] . Leukemia 1999;13:490–
491.
351. Stewart AK, Trudel S, Al -Berout i BM, et a l . Lack of response to short - term use of
c lar i thromycin (BIAXIN) in mul t ip le myeloma [ le t ter ] . Blood 1999;93:4441.
352. Morr is TC, Ranaghan L, Morr ison J , et al . Phase I I t r ia l o f c lar i thromycin and
pamidronate therapy in myeloma. Med Oncol 2001;18:79–84.
353. Har ley JB, Pajak TF, McIntyre OR, et al . Improved survival of increased-r isk myeloma
pat ients on combined t r ip le-a lkyla t ing-agent therapy: a s tudy of the CALGB. Blood
1979;54:13–22.
354. Cooper MR, McIntyre OR, Proper t KJ, e t a l . S ingle , sequent ia l , and mult ip le a lkyla t ing
agent therapy for mul t ip le myeloma: a CALGB Study. J Cl in Oncol 1986;4:1331–1339.
355. Gregory W M, Richards MA, Malpas JS. Combinat ion chemotherapy versus melphalan
and prednisolone in the treatment of mul t ip le myeloma: an overview of publ ished t r ia ls. J
Cl in Oncol 1992;10:334–342.
356. Fonseca R, Harr ington D, Oken MM, et a l . Bio log ical and prognost ic s ign i f icance of
in terphase f luorescence in s i tu hybridizat ion detect ion of chromosome 13 abnormal i t ies
(de l ta13) in mult ip le myeloma: an eastern cooperat ive oncology group study. Cancer Res
2002;62:715–720.
357. Alvares CL, Davies FE, Horton C, e t a l . Long- term outcomes of previously unt reated
myeloma pat ients : responses to induct ion chemotherapy and high-dose melphalan
incorporated wi thin a r isk st ra t i f icat ion model can help to d i rec t the use of novel t reatments .
Br J Haematol 2005;129:607–614.
358. George RP, Poth JL, Gordon D, e t a l . Mul t ip le myeloma—-intermi t tent combinat ion
chemotherapy compared to cont inuous therapy. Cancer 1972;29:1665–1670.
P.2426

359. Cohen HJ, Si lberman HR, Tornyos K, e t a l . Compar ison of two long-term chemotherapy
reg imens, wi th or wi thout agents to modi fy skele ta l repai r , in mul t ip le myeloma. Blood
1984;63:639–648.
360. Abramson N, Lur ie P, Miet lowsk i W L, e t a l . Phase I I I s tudy of in termi t tent carmust ine
(BCNU), cyclophosphamide, and prednisone versus in termi t tent melphalan and prednisone
in myeloma. Cancer Treat Rep 1982;66:1273–1277.
361. Pavlovsky S, Corrado C, Santarel l i MT, e t a l . An update of two randomized t r ia ls in
previously unt reated mult ip le myeloma compar ing melphalan and prednisone versus three-
and f ive-drug combinat ions: an Argent ine Group for the Treatment of Acute Leukemia Study.
J Cl in Oncol 1988;6:769–775.
362. Bergsagel DE. Treatment of plasma ce l l myeloma. Annu Rev Med 1979;30:431–443.
363. Palva IP, Ahrenberg P, Ala-Harja K, et al . Treatment of mul t ip le myeloma wi th an
in tensive 5-drug combinat ion or in termit tent melphalan and prednisone; a randomised
mult icentre t r ia l . F inn ish Leukaemia Group. Eur J Haematol 1987;38:50–54.
364. Ki ldahl -Andersen O, Bjark P, Bondevik A, e t a l . Mul t ip le myeloma in centra l and
nor thern Norway 1981–1982: a fo l low-up s tudy of a randomized c l in ical t r ia l of 5-drug
combinat ion therapy versus standard therapy. Eur J Haemato l 1988;41:47–51.
365. Osterborg A, Ahre A, Bjorkholm M, e t al . Al ternat ing combinat ion chemotherapy
(VMCP/VBAP) is not super ior to melphalan/prednisone in the t reatment o f mul t ip le myeloma
pat ients s tage I I I—a randomized s tudy f rom MGCS. Eur J Haematol 1989;43:54–62.
366. Boccadoro M, Marmont F, Tr iba l to M, e t al . Mul t ip le myeloma: VMCP/VBAP a l ternat ing
combinat ion chemotherapy is not superior to melphalan and prednisone even in h igh-r isk
pat ients . J Cl in Oncol 1991;9:444–448.
367. Keldsen N, Bjerrum OW , Dahl IM, e t a l . Mul t ip le myeloma t reated wi th mi toxantrone in
combinat ion wi th v incr is t ine and predniso lone (NOP reg imen) versus melphalan and
predniso lone: a phase I I I s tudy. Nord ic Myeloma Study Group (NMSG). Eur J Haemato l
1993;51:80–85.
368. Salmon SE, Haut A, Bonnet JD, e t al . Al ternat ing combinat ion chemotherapy and
levamiso le improves surviva l in mul t ip le myeloma: a Southwest Oncology Group Study. J
Cl in Oncol 1983;1:453–461.
369. Dur ie BG, Dixon DO, Carter S, et al . Improved surviva l durat ion wi th combinat ion
chemotherapy induct ion for mult ip le myeloma: a Southwest Oncology Group Study. J Cl in
Oncol 1986;4:1227–1237.
370. Hjorth M, Hel lquis t L , Holmberg E, e t al . In i t ia l t reatment in mul t ip le myeloma: no
advantage of mul t idrug chemotherapy over melphalan-prednisone. The Myeloma Group of
Western Sweden. Br J Haematol 1990;74: 185–191.
371. Peest D, Coldewey R, Deicher H. Overal l vs . tumor-re lated surviva l in mul t ip le
myeloma. German Myeloma Treatment Group. Eur J Cancer 1991;27:672.
372. Blade J , San Miguel JF, Alcala A, et al . Al ternat ing combinat ion VCMP/VBAP
chemotherapy versus melphalan/prednisone in the t reatment o f mul t ip le myeloma: a
randomized mul t icentr ic s tudy of 487 pat ients . J Cl in Oncol 1993;11:1165–1171.
373. Oken MM, Harr ington DP, Abramson N, et al . Compar ison of melphalan and prednisone
wi th v incr is t ine, carmust ine, melphalan, cyclophosphamide, and prednisone in the treatment
o f mul t ip le myeloma: resu l ts o f Eastern Cooperat ive Oncology Group Study E2479. Cancer
1997;79:1561–1567.

374. Peest D, Deicher H, Coldewey R, e t al . A comparison of po lychemotherapy and
melphalan/prednisone for pr imary remiss ion induct ion, and in terferon-alpha for maintenance
t reatment , in mul t ip le myeloma. A prospect ive t r ia l o f the German Myeloma Treatment
Group. Eur J Cancer 1995;2:146–151.
375. Schey SA, Kazmi M, I reland R, e t a l . The use of int ravenous in termediate dose
melphalan and dexamethasone as induct ion treatment in the management o f de novo
mult ip le myeloma. Eur J Haematol 1998;61:306–310.
376. Tsakanikas S, Papanastas iou K, Stamate lou M, et a l . In termediate dose of in travenous
melphalan in advanced mult ip le myeloma. Oncology 1991;48:369–371.
377. Lokhorst HM, Sonneveld P, W i jermans PW , et al . In termediate-dose melphalan ( IDM)
combined wi th G-CSF (f i lg rast im) is an effect ive and safe induct ion therapy for auto logous
s tem cel l t ransplantat ion in mul t ip le myeloma. Br J Haemato l 1996;92:44–48.
378. Barlogie B, Dicke KA, Alexanian R. High dose melphalan for re f rac tory myeloma—the
M.D. Anderson exper ience. Hematol Oncol 1988;6:167–172.
379. Petrucc i MT, Avvisat i G, Tr iba l to M, e t al . In termediate-dose (25 mg/m 2 ) in t ravenous
melphalan for pat ients wi th mul t ip le myeloma in re lapse or re f rac tory to s tandard treatment .
Eur J Haemato l 1989;42:233–237.
380. Palumbo A, Pi ler i A, Tr io lo S, e t al . Mul t icycl ic, dose- intens ive chemotherapy
supported by hemopoiet ic progeni tors in re frac tory myeloma pat ients. Bone Marrow
Transplant 1997;19:23–29.
381. Salokannel SJ, Palva IP, Timonen T, e t a l . Cyc lophosphamide in the t reatment o f
mult ip le myeloma. Blu t 1971;23:129–132.
382. Choi OS, Engl ish A, Hi l ton JH, e t al . Cyclophosphamide in the t reatment o f
myelomatos is . Can Med Assoc J 1967;97:1133–1139.
383. Case DC Jr , Sonneborn HL, Paul SD, e t al . Combinat ion chemotherapy for mul t ip le
myeloma wi th BCNU, cyclophosphamide, v incr is t ine, melphalan, and prednisone (M-2
protocol ) . Oncology 1985;42:137–140.
384. Peest D, Deicher H, Coldewey R, e t al . Induct ion and maintenance therapy in mul t ip le
myeloma: a mul t icenter tr ia l o f MP versus VCMP. Eur J Cancer Cl in Oncol 1988;24:1061–
1067.
385. Ki ldahl -Andersen O, Bjark P, Bondevik A, e t a l . Mul t ip le myeloma in centra l Norway
1981–1982: a randomized cl in ica l t r ia l o f 5-drug combinat ion therapy versus standard
therapy. Scand J Haemato l 1986;37:243–248.
386. Alber ts DS, Dur ie BG, Salmon SE. Doxorubic in/B.C.N.U. chemotherapy for mul t ip le
myeloma in re lapse. Lancet 1976;1:926–928.
387. Alexanian R, Salmon S, Gut terman J , et al . Chemoimmunotherapy for mul t ip le myeloma.
Cancer 1981;47:1923–1929.
388. Crowley J , Jacobson J , Alexanian R. Standard-dose therapy for mul t ip le myeloma: The
Southwest Oncology Group exper ience. Semin Hemato l 2001;38:203–208.
389. Dur ie BG, Stock-Novack D, Salmon SE, e t a l . Prognost ic value of pret reatment serum
beta 2 microg lobul in in myeloma: a Southwest Oncology Group Study. Blood 1990;75:823–
830.
390. Salmon SE, Tesh D, Crowley J , e t a l . Chemotherapy is super ior to sequentia l hemibody
i r radia t ion for remission consol idat ion in mul t ip le myeloma: a Southwest Oncology Group
s tudy. J Cl in Oncol 1990;8:1575–1584.
391. Barlogie B, Smi th L, Alexanian R. Ef fec t ive treatment of advanced mul t ip le myeloma
ref rac tory to a lkyla t ing agents . N Engl J Med 1984;310:1353–1356.
392. Alexanian R, Barlogie B, Tucker S. VAD-based reg imens as pr imary treatment for
mult ip le myeloma. Am J Hemato l 1990;33:86–89.
393. Samson D, Gaminara E, Newland A, e t a l . Infusion of v incr is t ine and doxorubic in wi th
ora l dexamethasone as f i rs t - l ine therapy for mult ip le myeloma. Lancet 1989;2:882–885.
394. At ta l M, Huguet F, Schla i fer D, e t a l . Intensive combined therapy for previously
unt reated aggress ive myeloma. Blood 1992;79:1130–1136.
395. Raje N, Powles R, Kulkarni S, e t a l . A compar ison of v incr ist ine and doxorubic in
in fus ional chemotherapy wi th methylpredniso lone (VAMP) wi th the addit ion of week ly
cyc lophosphamide (C-VAMP) as induct ion t reatment fo l lowed by autograf t ing in previous ly
unt reated myeloma. Br J Haematol 1997;97:153–160.
396. Kars A, Cel ik I , Kansu E, e t a l . Maintenance therapy wi th alpha- in terferon fo l lowing
f i rst - l ine VAD in mul t ip le myeloma. Eur J Haemato l 1997;59:100–104.
397. Anderson H, Scar f fe JH, Ranson M, e t al . VAD chemotherapy as remission induct ion
for mult ip le myeloma. Br J Cancer 1995;71:326–330.
398. Segeren CM, Sonneveld P, van der Hol t B, et a l . V incrist ine, doxorubic in and
dexamethasone (VAD) admin is tered as rapid int ravenous in fusion for f i rs t- l ine t reatment in
unt reated mult ip le myeloma. Br J Haemato l 1999;105:127–130.
399. Fossa A, Muer M, Kasper C, e t a l . Bo lus v incr is t ine and epi rub ic in wi th
cyc lophosphamide and dexamethasone (VECD) as induction and sa lvage t reatment in
mult ip le myeloma. Leukemia 1998;12:422–426.
400. Ts iara SN, Kapsal i E, Chr is tou L, et al . Admin is t ra t ion of a modif ied chemotherapeut ic
reg imen conta in ing v incr is t ine, l iposomal doxorubic in and dexamethasone to mul t ip le
myeloma pat ients : pre l iminary data. Eur J Haemato l 2000;65:118–122.
401. Salmon SE, Crowley JJ , Balcerzak SP, e t a l . In ter feron versus in ter feron p lus
prednisone remiss ion maintenance therapy for mul t iple myeloma: a Southwest Oncology
Group Study. J Cl in Oncol 1998;16:890–896.
402. Salmon SE, Crowley JJ , Grogan TM, et a l . Combinat ion chemotherapy, g lucocor t icoids ,
and in ter feron a l fa in the t reatment o f mul t ip le myeloma: a Southwest Oncology Group s tudy
[see comments ] . J Cl in Oncol 1994;12:2405–2414.
403. Anagnostopoulos A, Aleman A, W il l iams P, et a l . Auto logous s tem cel l t ransplantat ion
(ASCT) af ter nonmyelosuppress ive induct ion therapy wi th dexamethasone a lone is safe and
ef fec t ive for newly d iagnosed mult ip le myeloma (MM) pts who receive high dose
chemotherapy (HDC). Blood 2001;98:2858a.
404. Kumar S, Lacy MQ, Dispenzier i A, et al . Sing le agent dexamethasone for pre-s tem cel l
t ransplant induct ion therapy for mul t ip le myeloma. Bone Marrow Transplant 2004;34:485–
490.
405. Hussein MA, W ood L, Hsi E, e t a l . A Phase I I t r ia l o f pegyla ted l iposomal doxorubic in ,
v incr is t ine, and reduced-dose dexamethasone combinat ion therapy in newly d iagnosed
mult ip le myeloma pat ients . Cancer 2002;95:2160–2168.
406. Dimopoulos MA, Poul i A, Zervas K, et al . Prospect ive randomized comparison of
v incr is t ine, doxorubic in and dexamethasone (VAD) administered as in t ravenous bo lus
in jec t ion and VAD wi th l iposomal doxorubic in as f i rs t - l ine t reatment in mult ip le myeloma.
Ann Oncol 2003;14:1039–1044.

407. Ri fk in RM, Gregory SA, Mohrbacher A, et al . Pegylated l iposomal doxorubic in ,
v incr is t ine, and dexamethasone provide s igni f icant reduct ion in toxic i ty compared wi th
doxorubic in, v incr is t ine, and dexamethasone in pat ients wi th newly d iagnosed mult ip le
myeloma: a Phase I I I mul t icenter randomized t r ia l . Cancer 2006;106:848–858.
408. Szelenyi H, Kreuser ED, Kei lho lz U, e t a l . Cyc lophosphamide, adr iamyc in and
dexamethasone (CAD) is a highly e f fect ive therapy for pat ients wi th advanced mul t ip le
myeloma. Ann Oncol 2001;12:105–108.
409. Gi les FJ, W ickham NR, Rapoport BL, e t a l . Cyc lophosphamide, etopos ide, v incr is t ine,
adr iamycin, and dexamethasone (CEVAD) reg imen in ref ractory mult ip le myeloma: an
In ternat ional Oncology Study Group ( IOSG) phase I I protocol . Am J Hemato l 2000;63:125–
130.
410. Dimopoulos MA, Weber D, Delasal le KB, et a l . Combinat ion therapy wi th in ter feron-
dexamethasone for newly d iagnosed pat ients wi th mul t ip le myeloma. Cancer 1993;72:2589–
2592.
411. Ahre A, Bjorkholm M, Osterborg A, et al . High doses of natural alpha- inter feron (alpha-
IFN) in the t reatment o f mult ip le myeloma—a p i lot s tudy f rom the Myeloma Group of Centra l
Sweden (MGCS). Eur J Haematol 1988;41:123–130.
412. Corrado C, Pavlovsky S, Sas lasky J. Randomized t r ia l compar ing melphalan-
prednisone wi th or wi thout recombinant a lpha-2 in ter feron ( r -alpha2IFN) in mul t ip le
myeloma. Proc Am Soc Cl in Oncol 1989;8:258.
413. Garcia-Larana J , Steegmann J , Perez Oteyza J . Treatment o f mul t ip le myeloma wi th
melphalan-prednisone (MP) versus melphalan-prednisone and alpha-2b- in ter feron (MP-IFN).
Resul ts o f a Cooperat ive Spanish Group. Cong Int Soc Haemato l ISH 1992;24:301.
414. Vela-Ojeda J , Vazquez V, Garc ia Ruiz E. A randomized c l in ical t r ia l comparing
chemotherpy wi th or wi thout in ter feron a l fa-2b in newly d iagnosed pat ients wi th mult ip le
myeloma. IV In ternat ional Workshop on Mul t ip le Myeloma, Rochester , Minnesota, USA,
1993.
415. Montuoro A, De Rosa L, De Blas io A, e t a l . A lpha-2a- inter feron/melphalan/prednisone
versus melphalan/prednisone in previously unt reated pat ients wi th mult ip le myeloma. Br J
Haematol 1990;76:365–368.
416. In ter feron-a lpha 2b added to melphalan-prednisone for in i t ia l and maintenance therapy
in mult ip le myeloma. A randomized, control led tr ia l . The Nordic Myeloma Study Group. Ann
In tern Med 1996;124:212–-222.
P.2427
417. Osterborg A, Bjorkholm M, Bjoreman M, e t al . Natural in terferon-alpha in combinat ion
wi th melphalan/prednisone versus melphalan/prednisone in the t reatment o f mul t ip le
myeloma s tages I I and I I I : a randomized s tudy f rom the Myeloma Group of Centra l Sweden.
Blood 1993;81:1428–1434.
418. Cooper MR, Dear K, McIntyre OR, et al . A randomized c l in ical t r ia l compar ing
melphalan/prednisone wi th or wi thout in ter feron al fa-2b in newly d iagnosed pat ients wi th
mult ip le myeloma: a Cancer and Leukemia Group B s tudy. J Cl in Oncol 1993;11:155–160.
419. Capnis t G, Vespignani M, Spr iano M, e t al . Impact o f in ter feron at induct ion
chemotherapy and maintenance t reatment for mul t ip le myeloma. Pre l iminary resu l ts o f a

mult icenter s tudy by the I ta l ian non-Hodgkin 's Lymphoma Cooperat ive Study Group
(NHLCSG). Acta Oncol 1994;33:527–529.
420. Montuoro A, DeRosa L, Pescador L . In ter feron al fa-2b-MP versus MP a lone in
previously unt reated pat ients wi th mult ip le myeloma: prel iminary resul ts from a mult icenter
s tudy. 24th Congress of the In ternat ional Soc ie ty of Hemato logy, London, 1992.
421. Ludwig H, Cohen AM, Huber H, e t al . In terferon a l fa-2b wi th VMCP compared to VMCP
alone for induct ion and in ter feron al fa-2b compared to contro ls for remiss ion maintenance in
mult ip le myeloma: in ter im resul ts . Eur J Cancer 1991;27:S40–S45.
422. Ludwig H, Cohen AM, Pol l iack A, et al . In terferon-a lpha for induct ion and maintenance
in mult ip le myeloma: resu l ts o f two mul t icenter randomized t r ia ls and summary of o ther
s tud ies . Ann Oncol 1995;6:467–-476.
423. Scheithauer W , Corte lezzi A, Fr i tz E, e t al . Combined alpha-2C-in terferon/VMCP
polychemotherapy versus VMCP polychemotherapy as induct ion therapy in mul t ip le
myeloma: a prospect ive randomized tr ia l . J Bio l Response Mod. 1989;8:109–115.
424. Casassus P, Mahe B, Fain O. Double randomized compar ison of in ter feron-a ( IFN-a)
wi th VMCP/VBAP reg imen as the induct ion phase and of two doses of IFN-a lpha in p lateau
phase of unt reated mul t ip le myeloma: Resul ts of the KIF mult icenter t r ia l . VI Internat ional
Workshop on Mul t ip le Myeloma, Boston, 1997.
425. Joshua DE, Penny R, Mat thews JP, e t a l . Austra l ian Leukaemia Study Group Myeloma
I I : a randomized t r ia l o f in tens ive combinat ion chemotherapy wi th or wi thout in ter feron in
pat ients wi th myeloma. Br J Haematol 1997;97:38–45.
426. Avi les A, Ala t r is te S, Ta lavera A, e t al . Al ternat ing combinat ion chemotherapy and
in ter feron improves surviva l in poor prognos is mul t ip le myeloma. Cl in Oncol 1995;7:97–101.
427. Gertz MA, Kal ish LA, Kyle RA, e t a l . Phase I I I s tudy compar ing v incr is t ine, doxorubic in
(Adr iamycin) , and dexamethasone (VAD) chemotherapy wi th VAD p lus recombinant
in ter feron a l fa-2 in re f rac tory or relapsed mult ip le myeloma. An Eastern Cooperat ive
Oncology Group s tudy. Am J Cl in Oncol 1995;18:475–480.
428. Oken MM, Leong T, Lenhard RE Jr , e t al . The addi t ion of inter feron or h igh dose
cyc lophosphamide to s tandard chemotherapy in the t reatment o f pat ients wi th mul t ip le
myeloma: phase I I I Eastern Cooperat ive Oncology Group Cl inica l Tr ial EST 9486. Cancer
1999;86:957–968.
429. Galvez C, Pi re R, Bonamassa M. Mul t ip le myeloma: treatment wi th VABP wi th or
wi thout recombinant a l fa-2b in ter feron in mul t ip le myeloma. In : 18th Internat ional Congress
of Chemotherapy, Stockholm, Sweden, 1993.
430. Ai tchison R, W il l iams A, Schey S, e t a l . A randomised t r ia l o f cyclophosphamide wi th
and wi thout low dose a lpha- in terferon in the t reatment o f newly d iagnosed myeloma. Leuk
Lymphoma 1993;9:243–246.
431. Ludwig H, Fri tz E. In ter feron in mul t ip le myeloma—summary of t reatment resul ts and
c l in ical impl icat ions. Acta Oncol 2000;39:815–821.
432. In ter feron as therapy for mul t ip le myeloma: an indiv idual pat ient data overview of 24
randomized tr ia ls and 4012 pat ients . Br J Haemato l 2001;113:1020–1034.
433. Preis P, Schei thauer W , Fri tz E, e t a l . VMCP chemotherapy wi th or wi thout in terferon-
a lpha-2 in newly d iagnosed pat ients wi th mul t ip le myeloma. Onkologie 1989;12:27–29.
434. W islo f f F, Hjor th M, Kaasa S, e t a l . Ef fect o f in ter feron on the heal th-re lated qual i ty o f
l i fe o f mul t ip le myeloma pat ients : resu l ts o f a Nord ic randomized t r ia l compar ing melphalan-

prednisone to melphalan-prednisone +alpha-in terferon. The Nord ic Myeloma Study Group.
Br J Haematol 1996;94:324–332.
435. Ludwig H, Fri tz E, Neuda J , e t a l . Pat ient preferences for inter feron a l fa in mult ip le
myeloma. J Cl in Oncol 1997;15:1672–1679.
436. Palumbo A, Bringhen S, Caravi ta T, e t a l . Ora l melphalan and prednisone
chemotherapy plus tha l idomide compared wi th melphalan and prednisone a lone in e lder ly
pat ients wi th mul t ip le myeloma: randomised contro l led tr ia l . Lancet 2006;367:825–831.
437. Zangari M, Bar log ie B, Anaissie E, e t a l . Deep ve in thrombosis in pat ients wi th mul t ip le
myeloma t reated wi th tha l idomide and chemotherapy: ef fec ts o f prophylact ic and therapeut ic
ant icoagulat ion. Br J Haemato l 2004;126:715–721.
438. Baz R, L i L , Kot tke-Marchant K, e t a l . The role of aspi r in in the prevent ion of
thrombot ic compl icat ions of thal idomide and anthracycl ine-based chemotherapy for mult ip le
myeloma. Mayo Cl in Proc 2005;80:1568–1574.
439. Rajkumar SV, Hayman SR, Lacy MQ, et a l . Combinat ion therapy wi th lenal idomide plus
dexamethasone (Rev/Dex) for newly d iagnosed myeloma. Blood 2005;106:4050–4053.
440. Rajkumar SV, Blood E. Lenal idomide and venous thrombosis in mult ip le myeloma. N
Engl J Med 2006;354:2079–2080.
441. Rajkumar SV, Blood E, Vesole D, et al . Phase I I I c l in ical t r ia l o f tha l idomide p lus
dexamethasone compared wi th dexamethasone a lone in newly d iagnosed mult ip le myeloma:
a c l in ica l t r ia l coord inated by the Eastern Cooperat ive Oncology Group. J Cl in Oncol
2006;24:431–436.
442. Knight R, DeLap RJ, Zeld is JB. Lenal idomide and venous thrombosis in mul t ip le
myeloma. N Engl J Med 2006;354:2079–2080.
443. Palumbo A, Fa lco P, Benevolo G, e t al . Oral lenal idomide p lus melphalan and
prednisone (R-MP) for newly d iagnosed mul t ip le myeloma. J Cl in Oncol (Meet ing Abstr )
2006;24:7518.
444. Richardson PG, Br iemberg H, Jagannath S, e t al . Frequency, character ist ics, and
reversib i l i ty o f per ipheral neuropathy during t reatment o f advanced mul t ip le myeloma wi th
bor tezomib. J Cl in Oncol 2006;24:3113–3120.
445. Rajkumar SV, Hayman S, Gertz MA, e t al . Combinat ion therapy wi th tha l idomide p lus
dexamethasone for newly d iagnosed myeloma. J Cl in Oncol 2002;20:4319–4323.
446. Rajkumar SV, Hussein M, Catalano J , e t al . A mul t icenter, randomized, double-b l ind,
p lacebo-contro l led t r ia l of thal idomide plus dexamethasone versus dexamethasone alone as
in i t ia l therapy for newly d iagnosed mul t ip le myeloma. J Cl in Oncol (Meet ing Abstr )
2006;24:7517.
447. Ghobr ial I , Dispenzier i A, Bundy K, e t al . Pret ransplant induct ion wi th tha l idomide-
dexamethasone does not adverse ly a f fec t s tem ce l l col lec t ion in pat ients wi t mul t ip le
myeloma. Proc ASCO 2002;21:418a.
448. Goldschmidt H, Sonneveld P, Bre i tk reuz I , e t a l . HOVON 50/GMMG-HD3-Tr ia l : Phase
I I I s tudy on the ef fect o f tha l idomide combined with high dose melphalan in myeloma
pat ients up to 65 years . Blood 2005;106(11) :128a (abst r 424) .
449. Cavo M, Zamagni E, Tos i P, et al . Superior complete remission/very good par t ia l
remiss ion ra te wi th peri - t ransplant admin is t rat ion of tha l idomide-dexamethasone for newly
d iagnosed mul t ip le myeloma. Blood 2005:[5474].

450. Ludwig H, Drach J , Tothova E, e t a l . Thal idomide-dexamethasone versus melphalan-
predniso lone as f i rst l ine t reatment in e lder ly pat ients wi th mult ip le myeloma: an in ter im
analys is . Sess ion type: ora l session. 2005: [782] .
451. Facon T, Mary J , Harousseau J, e t a l . Super ior i ty o f melphalan-prednisone (MP) +
tha l idomide (THAL) over MP and auto logous s tem cel l t ransplantat ion in the treatment o f
newly d iagnosed elderly pat ients wi th mul t ip le myeloma. J Cl in Oncol (Meet ing Abstr )
2006;24:1.
452. Zervas K, Dimopoulos MA, Hatzichariss i E, e t al . Primary t reatment o f mul t ip le
myeloma wi th tha l idomide, v incr is t ine, l iposomal doxorubic in and dexamethasone (T-VAD
doxi l ) : a phase I I mul t icenter s tudy. Ann Oncol 2004;15:134–138.
453. Of f idani M, Corvat ta L , Piersantel l i MN, e t al . Thal idomide, dexamethasone and
pegylated l iposomal doxorubic in (ThaDD) for newly d iagnosed mult ip le myeloma pat ients
over 65 years . Blood 2006;108:2159.
454. Hussein MA, Baz R, Srkalovic G, e t al . Phase 2 s tudy of pegyla ted l iposomal
doxorubic in, v incr is t ine, decreased-f requency dexamethasone, and thal idomide in newly
d iagnosed and re lapsed-ref rac tory mul t ip le myeloma. Mayo Cl in Proc 2006;81:889–895.
455. Hassoun H, Reich L, Kl imek VM, et a l . Doxorubic in and dexamethasone fo l lowed by
tha l idomide and dexamethasone is an ef fec t ive wel l to lerated ini t ia l therapy for mul t ip le
myeloma. Br J Haematol 2006;132:155–161.
456. Baz RC, Kel ly M, Reed J , e t a l . Phase I I s tudy of dexamethasone, ascorbic ac id,
tha l idomide and arsenic t r ioxide (DATA) in high r isk previous ly unt reated (PU) and
re lapsed/ref rac tory (RR) mult ip le myeloma (MM). J Cl in Oncol (Meet ing Abstr )
2006;24:17535.
457. Anderson K, Richardson P, Chanan-Khan A, e t al . Sing le-agent bortezomib in
previously unt reated mult ip le myeloma (MM): Resul ts o f a phase I I mul t icenter s tudy. J Cl in
Oncol (Meet ing Abstr ) 2006;24:7504.
458. Harousseau JL, At ta l M, Coi teux V, e t al . Bor tezomib (VELCADE(r) ) p lus
dexamethasone as induct ion t reatment pr ior to auto logous s tem cel l t ransplantat ion in
pat ients wi th newly d iagnosed mul t ip le myeloma: prel iminary resu l ts o f an IFM Phase I I
s tudy. ASCO 2005:6653.
459. Mateos MV, Hernandez JM, Hernandez MT, e t al . Bor tezomib plus melphalan and
prednisone in elder ly untreated pat ients wi th mul t ip le myeloma: resu l ts o f a mul t icenter
phase I / I I s tudy. Blood 2006;108:2165–2172.
460. Oakervee HE, Popat R, Curry N, e t a l . PAD combinat ion therapy (PS-341/bortezomib,
doxorubic in and dexamethasone) for previous ly unt reated pat ients wi th mul t ip le myeloma.
Br J Haematol 2005;129:755–762.
461. Popat R, Oakervee HE, Curry N, e t al . Reduced dose PAD combinat ion therapy (PS-
341/bor tezomib, adriamyc in and dexamethasone) for previously unt reated pat ients wi th
mult ip le myeloma. ASH Annual Meet ing Abstr 2005;106:2554.
462. W ang M, Delasal le K, Gi ral t S, e t a l . Rapid contro l o f previous ly unt reated mult ip le
myeloma wi th bor tezomib- thal idomide-dexamethasone fo l lowed by ear ly in tens ive therapy.
Blood 2005:106:231a (abst r 784) .
463. Badros A, Rapoport A, Goloubeva O, e t al . Phase I t r ia l o f bor tezomib (V) in
combinat ion wi th “DT-PACE”: toxic i ty, s tem cel l co l lec t ion and engraf tment in newly
d iagnosed mul t ip le myeloma (MM) pat ients (Pts) . ASH Annual Meet ing Abstr 2005;106:2747.

464. Niesvizky R, Pekle K, Gelbshte in UY, e t a l . B iRD
(Biaxin(r ) /Revl imid(r )/Dexamethasone) combinat ion therapy (Rx) resu l ts in h igh complete
remiss ions (CR) and overa l l responses in myeloma (MM) wi th poor prognost ic features.
Blood 2005;106:190a (abst r 642) .
465. Niesvizky R, Jayabalan DS, Furs t JR, et al . Clar i thromycin, lenal idomide and
dexamethasone combinat ion therapy as pr imary treatment of mul t ip le myeloma. J Cl in Oncol
(Meet ing Abstr) 2006;24:7545.
466. Barlogie B, Hal l R, Zander A, e t a l . High-dose melphalan wi th auto logous bone marrow
t ransplantat ion for mul t ip le myeloma. Blood 1986;67: 1298–1301.
467. Chi ld JA, Morgan GJ, Davies FE, e t a l . High-dose chemotherapy wi th hematopoiet ic
s tem-cel l rescue for mul t ip le myeloma. N Engl J Med 2003; 348:1875–1883.
468. Palumbo A, Bringhen S, Petrucci MT, e t a l . In termediate-dose melphalan improves
surviva l o f myeloma pat ients aged 50 to 70: resul ts o f a randomized contro l led tr ia l . Blood
2004;104:3052–3057.
469. Fermand JP, Katsahian S, Div ine M, e t a l . High-dose therapy and auto logous b lood
s tem-cel l t ransplantat ion compared wi th convent ional t reatment in myeloma pat ients aged
55 to 65 years : long- term resul ts o f a randomized contro l t r ia l f rom the Group Myelome-
Autogref fe . J Cl in Oncol 2005;23:9227–9233.
470. Fermand JP, Ravaud P, Chevret S, et al . High-dose therapy and auto logous per iphera l
b lood s tem cel l t ransplantat ion in mul t ip le myeloma: up-f ront or rescue treatment? Resul ts
o f a mul t icenter sequentia l randomized c l in ical t r ia l . Blood 1998;92:3131–3136.
471. Barlogie B, Kyle RA, Anderson KC, e t a l . Standard chemotherapy compared wi th h igh-
dose chemoradiotherapy for mul t ip le myeloma: f ina l resu l ts o f phase I I I US In tergroup Tr ia l
S9321. J Cl in Oncol 2006;24:929–936.
P.2428
472. Blade J , Rosino l L , Sureda A, e t a l . High-dose therapy in tensi f icat ion compared wi th
cont inued standard chemotherapy in mul t ip le myeloma pat ients responding to the ini t ia l
chemotherapy: long- term resul ts from a prospect ive randomized t r ia l f rom the Spanish
cooperat ive group PETHEMA. Blood 2005;106:3755–3759.
473. Blade J , San Miguel JF, Fontani l las M, e t a l . Surviva l o f mul t ip le myeloma pat ients who
are potent ia l candidates for ear ly high-dose therapy in tens i f icat ion/ autot ransplantat ion and
who were convent ional ly t reated. J Cl in Oncol 1996;14:2167–2173.
474. Lenhof f S, Hjor th M, Holmberg E, e t a l . Impact on survival of high-dose therapy wi th
autologous s tem cel l support in pat ients younger than 60 years wi th newly d iagnosed
mult ip le myeloma: a populat ion-based s tudy. Nord ic Myeloma Study Group. Blood
2000;95:7–11.
475. Harousseau JL, At ta l M. The ro le o f stem cel l t ransplantat ion in mul t ip le myeloma.
Blood Rev 2002;16:245–253.
476. Facon T, Hul in C, Benboubker L , e t a l . Major superior i ty o f melphalan–prednisone (MP)
+ tha l idomide (THAL) over MP and autologous s tem cel l t ransplantat ion in the t reatment of
newly d iagnosed elderly pat ients wi th mul t ip le myeloma. Blood 2005:106;230a (abst r 780) .
477. Sonneveld P, van der Holt B, Vel lenga E, et a l . In tens ive versus double in tens ive
therapy in unt reated mult ip le myeloma: f inal analys is o f the HOVON 24 Tr ia l . ASH Annual
Meet ing Abstr 2005;106;715a (abst r 2545).
478. Vesole DH, Bar log ie B, Jagannath S, e t a l . High-dose therapy for ref ractory mul t ip le
myeloma: improved prognosis wi th bet ter support ive care and double t ransplants . Blood
1994;84:950–956.
479. Barlogie B, Jagannath S, Vesole DH, e t a l . Superior i ty o f tandem auto logous
t ransplantat ion over s tandard therapy for previous ly unt reated mult ip le myeloma. Blood
1997;89:789–793.
480. Desikan R, Barlog ie B, Sawyer J , e t a l . Resul ts o f h igh-dose therapy for 1000 pat ients
wi th mul t ip le myeloma: durable complete remissions and super ior survival in the absence of
chromosome 13 abnormal i t ies. Blood 2000; 95:4008–4010.
481. At ta l M, Harousseau JL, Facon T, et al . Sing le versus double autologous s tem-cel l
t ransplantat ion for mul t ip le myeloma. N Engl J Med 2003;349:2495–2502.
482. Cavo MA, Cel l in i C, Zamagni E, e t a l . Superior i ty of double over s ing le auto logous
s tem cel l t ransplantat ion as f i rs t - l ine therapy for mult ip le myeloma. Blood 2004;104:abstr
536.
483. Harousseau JL, Moreau P, Atta l M, e t al . Stem-cel l t ransplantat ion in mul t ip le myeloma.
Best Pract Res Cl in Haemato l 2005;18:603–618.
484. At ta l M, Harousseau JL, Facon T, et al . Double auto logous t ransplantat ion improves
surviva l o f mul t ip le myeloma pat ients : f inal analys is o f a prospect ive randomized s tudy of
the “In tergroupe Francophone du Myelome” (IFM 94) . Blood 2002;100;5a (abst r 7).
485. Morr is C, Iacobel l i S, Brand R, e t a l . Benef i t and t iming of second transplantat ions in
mult ip le myeloma: c l in ica l f indings and methodolog ical l imi ta t ions in a European Group for
Blood and Marrow Transplantat ion Regist ry s tudy. J Cl in Oncol 2004;22:1674–1681.
486. Alvares CL, Davies FE, Horton C, e t a l . The ro le o f second autograf ts in the
management o f myeloma at f i rst relapse. Haemato log ica 2006;91:141–142.
487. El ice F, Raimondi R, Tosetto A, e t a l . Prolonged overal l survival wi th second on-
demand auto logous t ransplant in mul t ip le myeloma. Am J Hemato l 2006;81:426–431.
488. Mehta J, Tr icot G, Jagannath S, e t a l . Salvage autologous or al logeneic t ransplantat ion
for mult ip le myeloma ref rac tory to or re lapsing after a f i rs t - l ine autograft? Bone Marrow
Transplant 1998;21:887–892.
489. Lee CK, Bar logie B, Zangari M, e t a l . Transplantat ion as sa lvage therapy for h igh-r isk
pat ients wi th myeloma in re lapse. Bone Marrow Transplant 2002;30:873–878.
490. Moreau P, Misbahi R, Mi lp ied N, et al . Long- term resul ts (12 years) o f high-dose
therapy in 127 pat ients wi th de novo mult ip le myeloma. Leukemia 2002;16:1838–1843.
491. Gre ipp PR, San Miguel J , Dur ie BG, et al . Internat ional staging system for mul t ip le
myeloma. J Cl in Oncol 2005;23:3412–3420.
492. Alexanian R, Dimopoulos MA, Delasal le KB, e t al . Myeloablat ive therapy for pr imary
res is tant mul t ip le myeloma. Stem Cel ls 1995;2:118–121.
493. Rajkumar SV, Fonseca R, Lacy MQ, et al . Auto logous stem cel l t ransplantat ion for
re lapsed and pr imary re frac tory myeloma. Bone Marrow Transplant 1999;23:1267–1272.
494. Kumar S, Lacy MQ, Dispenzier i A, et al . High-dose therapy and auto logous s tem cel l
t ransplantat ion for mul t ip le myeloma poorly responsive to in i t ia l therapy. Bone Marrow
Transplant 2004;34:161–167.

495. Bens inger W I, Buckner CD, Anasett i C, e t a l . A l logeneic marrow t ransplantat ion for
mult ip le myeloma: an analys is o f r isk fac tors on outcome. Blood 1996;88:2787–2793.
496. Harousseau JL, At ta l M, Div ine M, e t a l . Comparison of auto logous bone marrow
t ransplantat ion and per iphera l b lood s tem cel l t ransplantat ion af ter f i rs t remiss ion induct ion
t reatment in mul t ip le myeloma. Bone Marrow Transplant 1995;15:963–969.
497. Larsson K, Bjorks trand B, Ljungman P. Faster engraf tment but no reduct ion in
in fec t ious compl icat ions af ter peripheral blood s tem cel l t ransplantat ion compared to
autologous bone marrow t ransplantat ion. Support Care Cancer 1998;6:378–383.
498. Gertz MA, Lacy MQ, Inwards DJ, e t a l . Early harvest and la te t ransplantat ion as an
ef fec t ive therapeut ic st rategy in mul t ip le myeloma. Bone Marrow Transplant 1999;23:221–
226.
499. Tr icot G, Jagannath S, Vesole D, e t a l . Peripheral blood s tem cel l t ransplants for
mult ip le myeloma: ident i f icat ion of favorable variab les for rap id engraf tment in 225 pat ients .
Blood 1995;85:588–596.
500. Goldschmidt H, Hegenbart U, W al lmeier M, et a l . Factors inf luenc ing co l lec t ion of
per iphera l b lood progenitor ce l ls fol lowing h igh-dose cyclophosphamide and granulocyte
co lony-st imulat ing fac tor in pat ients wi th mul t ip le myeloma. Br J Haematol 1997;98:736–744.
501. Kroger N, Zel ler W , Hassan HT, e t a l . Successfu l mobi l izat ion of periphera l b lood s tem
cel ls in heavi ly pret reated myeloma pat ients wi th G-CSF a lone. Ann Hemato l 1998;76:257–
262.
502. Bruns I , Ste id l U, Kronenwet t R, et al . A s ing le dose of 6 or 12 mg of pegf i lgrast im for
per iphera l b lood progenitor ce l l mobi l izat ion resul ts in s imi lar y ie lds of CD34+ progeni tors
in pat ients wi th mul t ip le myeloma. Transfus ion 2006;46:180–185.
503. Gazi t t Y, Tian E, Bar logie B, e t a l . Di f ferent ia l mobi l izat ion of myeloma cel ls and
normal hematopoiet ic stem cel ls in mul t ip le myeloma af ter treatment wi th cyc lophosphamide
and granulocyte-macrophage co lony-s t imulat ing fac tor . Blood 1996;87:805–811.
504. Goldschmidt H, Hegenbart U, Haas R, e t a l . Mobi l izat ion of per ipheral b lood progeni tor
ce l ls wi th high-dose cyclophosphamide (4 or 7 g /m 2 ) and granulocyte co lony-s t imulat ing
fac tor in pat ients wi th mul t ip le myeloma. Bone Marrow Transplant 1996;17:691–697.
505. F i toussi O, Perreau V, Boi ron JM, e t a l . A compar ison of toxic i ty fo l lowing two d i f ferent
doses of cyclophosphamide for mobi l izat ion of per ipheral blood progenitor cel ls in 116
mult ip le myeloma pat ients . Bone Marrow Transplant 2001;27:837–842.
506. Corso A, Arca in i L , Caberlon S, et al . A combinat ion of dexamethasone,
cyc lophosphamide, e topos ide, and c isp la t in is less toxic and more effec t ive than high-dose
cyc lophosphamide for per ipheral stem ce l l mobi l izat ion in mul t ip le myeloma. Haemato log ica
2002;87:1041–1045.
507. Arora M, Burns LJ, Barker JN, e t a l . Randomized compar ison of granulocyte colony-
s t imulat ing fac tor versus granulocyte-macrophage colony-s t imulat ing fac tor plus intens ive
chemotherapy for per iphera l b lood s tem cel l mobi l izat ion and auto logous t ransplantat ion in
mult ip le myeloma. Biol Blood Marrow Transplant 2004;10:395–404.
508. Alegre A, Tomas JF, Mart inez-Chamorro C, e t al . Compar ison of per iphera l b lood
progenitor cel l mobi l izat ion in pat ients wi th mul t ip le myeloma: h igh-dose cyc lophosphamide
p lus GM-CSF vs G-CSF a lone. Bone Marrow Transplant 1997;20:211–217.

509. Cremer FW , Kiel K, W al lmeier M, e t al . Leukapheres is products in mul t ip le myeloma:
lower tumor load af ter mobi l izat ion wi th cyc lophosphamide p lus granulocyte co lony-
s t imulat ing fac tor (G-CSF) compared wi th G-CSF a lone. Exp Hemato l 1998;26:969–975.
510. Ding l i D, Nowakowsk i GS, Dispenzier i A, e t a l . Cyclophosphamide mobi l izat ion does
not improve outcome in pat ients rece iv ing s tem cel l t ransplantat ion for mul t ip le myeloma.
Cl in Lymphoma Myeloma 2006;6:384–388.
511. Devine SM, F lomenberg N, Vesole DH, e t a l . Rapid mobi l izat ion of CD34+ cel ls
fo l lowing administ ra t ion of the CXCR4 antagonis t AMD3100 to pat ients wi th mul t ip le
myeloma and non-Hodgkin 's lymphoma. J Cl in Oncol 2004;22:1095–1102.
512. Siegel DS, Desikan KR, Mehta J, et al . Age is not a prognost ic variab le wi th
autot ransplants for mul t ip le myeloma. Blood 1999;93:51–54.
513. Badros A, Bar log ie B, Morr is C, e t a l . High response rate in re f ractory and poor-r isk
mult ip le myeloma af ter al lo transplantat ion us ing a nonmyeloablat ive condi t ion ing reg imen
and donor lymphocyte infusions. [er ra tum appears in Blood 2001 Jul 15;98(2) :271; Blood
2001 Sep 15;98(6) :1653]. B lood 2001; 97:2574–2579.
514. San Miguel JF, Lahuerta JJ , Garcia-Sanz R, e t al . Are myeloma pat ients wi th renal
fa i lure candidates for auto logous s tem cel l t ransplantat ion? Hemato l J 2000;1:28–36.
515. Lee CK, Zangari M, Bar log ie B, e t a l . Dialysis-dependent renal fa i lure in pat ients wi th
myeloma can be reversed by high-dose myeloablat ive therapy and autot ransplant . Bone
Marrow Transplant 2004;33:823–828.
516. Knudsen LM, Nie lsen B, Gimsing P, e t a l . Auto logous s tem cel l t ransplantat ion in
mult ip le myeloma: outcome in pat ients wi th renal fa i lure. Eur J Haemato l 2005;75:27–33.
517. Moreau P, Facon T, At tal M, e t al . Compar ison of 200 mg/m(2) melphalan and 8 Gy
to tal body i r radia t ion p lus 140 mg/m(2) melphalan as condi t ioning reg imens for per iphera l
b lood s tem cel l t ransplantat ion in pat ients wi th newly d iagnosed mul t ip le myeloma: f inal
analys is of the In tergroupe Francophone du Myelome 9502 randomized t r ia l . Blood
2002;99:731–735.
518. Fenk R, Schneider P, Kropf f M, e t al . High-dose idarubic in , cyc lophosphamide and
melphalan as condi t ion ing for auto logous s tem cel l t ransplantat ion increases treatment-
re lated mortal i ty in pat ients wi th mul t ip le myeloma: resul ts o f a randomised s tudy. Br J
Haematol 2005;130:588–594.
519. Carr ion Gal indo R Sr, Serrano D, Perez-Corra l A, e t a l . High-dose chemotherapy and
autologous per iphera l b lood s tem cel l rescue (Auto-SCT) in mul t ip le myeloma (MM)
pat ients : busul fan + melphalan-140 (BuMel) versus (vs) melphalan-200 (Mel -200) as
condi t ion ing reg imens. J Cl in Oncol (Meet ing Abstr ) 2006;24:7612.
520. Hui jgens PC, Dekker-Van Roessel HM, Jonkhof f AR, et al . High-dose melphalan wi th
G-CSF-st imulated whole b lood rescue fol lowed by s tem cel l harvest ing and
busulphan/cyc lophosphamide wi th auto logous s tem cel l t ransplantat ion in mult ip le myeloma.
Bone Marrow Transplant 2001;27:925–931.
521. Schi l ler G, Nimer S, Vesc io R, e t al . Phase I- I I study of busul fan and
cyc lophosphamide condit ioning for t ransplantat ion in advanced mul t ip le myeloma. Bone
Marrow Transplant 1994;14:131–136.
522. Lahuerta JJ , Grande C, Blade J, et al . Myeloablat ive t reatments for mult ip le myeloma:
update of a comparat ive s tudy of d i f ferent reg imens used in pat ients f rom the Spanish
reg is t ry for t ransplantat ion in mult ip le myeloma. Leuk Lymphoma 2002;43:67–74.

523. Capria S, Petrucci MT, Pulsoni A, e t a l . High-dose idarubic in , busulphan and
melphalan for autologous stem cel l t ransplantat ion in mult ip le myeloma respons ive to DAV
chemotherapy: compar ison wi th a his tor ical contro l . Acta Haemato l 2006;115:9–14.
524. Dispenzier i A, W iseman GA, Lacy MQ, et a l . A Phase I s tudy of 153Sm-EDTMP wi th
f ixed h igh dose melphalan as a peripheral blood stem cel l condi t ion ing regimen in pat ients
wi th mul t ip le myeloma. Leukemia 2005;19:118–125.
P.2429
525. Gi ral t S, Bens inger W, Goodman M, e t a l . 166Ho-DOTMP plus melphalan fol lowed by
per iphera l b lood s tem cel l t ransplantat ion in pat ients wi th mul t ip le myeloma: resul ts o f two
phase 1/2 t r ia ls . Blood 2003;102:2684–2691.
526. Hol lmig K, Stover T, Ta lamo G, e t a l . Addi t ion of bor tezomib (Velcade(tm)) to high
dose melphalan (Vel -Mel ) as an ef fect ive condit ion ing reg imen wi th autologous s tem cel l
support in mul t ip le myeloma (MM). Blood 2004;104; 266a (abst r 929) .
527. Palumbo A, Avonto I , Bruno B, e t a l . In termediate-dose melphalan (100
mg/m 2 ) /bortezomib/thal idomide/dexamethasone and s tem cel l support in pat ients wi th
re f rac tory or re lapsed myeloma. Cl in Lymphoma Myeloma 2006;6:475–477.
528. Kaufman JL, W al ler EK, Torre C, e t a l . A randomized phase I t r ia l o f melphalan +
bor tezomib as condit ion ing for autologous t ransplant for myeloma. J Cl in Oncol (Meet ing
Abstr ) 2006;24:17550.
529. Desikan KR, Tr icot G, Dhodapkar M, e t a l . Melphalan plus total body i r radia t ion (MEL-
TBI) or cyclophosphamide (MEL-CY) as a condi t ion ing reg imen wi th second autot ransplant
in responding pat ients with myeloma is infer ior compared to h is tor ica l contro ls receiv ing
tandem t ransplants wi th melphalan alone. Bone Marrow Transplant 2000;25:483–487.
530. Gal imbert i S, Morabi to F, Guerr in i F, e t a l . Per iphera l b lood s tem cel l contaminat ion
evaluated by a h igh ly sens i t ive molecular method fa i ls to pred ic t outcome of
autot ransplanted mul t ip le myeloma pat ients . Br J Haematol 2003;120:405–412.
531. Gertz MA, W itz ig TE, Pineda AA, e t a l . Monoc lonal p lasma ce l ls in the blood s tem cel l
harvest f rom pat ients wi th mul t ip le myeloma are associated wi th shor tened relapse-f ree
surviva l a f ter transplantat ion. Bone Marrow Transplant 1997;19:337–342.
532. Reece DE, Barnett MJ, Connors JM, e t a l . Treatment of mul t ip le myeloma wi th
in tensive chemotherapy fo l lowed by autologous BMT us ing marrow purged wi th 4-
hydroperoxycyc lophosphamide. Bone Marrow Transplant 1993;11:139–146.
533. Seiden MV, Schlossman R, Andersen J, e t al . Monoc lonal ant ibody-purged bone
marrow t ransplantat ion therapy for mul t ip le myeloma. Leuk Lymphoma 1995;17:87–93.
534. Anderson KC, Andersen J , Soi f fer R, e t al . Monoc lonal ant ibody-purged bone marrow
t ransplantat ion therapy for mul t ip le myeloma. Blood 1993;82:2568–2576.
535. Tr icot G, Gazi t t Y, Leemhuis T, e t a l . Col lect ion, tumor contaminat ion, and engraf tment
k inet ics o f h ighly puri f ied hematopoiet ic progenitor ce l ls to support high dose therapy in
mult ip le myeloma. Blood 1998;91:4489–4495.
536. Schi l ler G, Vescio R, Freytes C, e t a l . Auto logous CD34-se lected b lood progeni tor ce l l
t ransplants for pat ients wi th advanced mul t ip le myeloma [see comments] . Bone Marrow
Transplant 1998;21:141–145.

537. Stewart AK, Vescio R, Schi l ler G, e t a l . Purging of auto logous periphera l -b lood s tem
cel ls us ing CD34 se lect ion does not improve overa l l or progression-f ree surviva l af ter h igh-
dose chemotherapy for mult ip le myeloma: resu l ts o f a mul t icenter randomized contro l led
t r ia l . J Cl in Oncol 2001;19:3771–3779.
538. Goldschmidt H, Bouko Y, Bourh is JH, e t al . CD34 + selec ted PBPCT resul ts in an
increased in fec t ive r isk wi thout pro longat ion of event f ree survival in newly d iagnosed
myeloma: a randomised s tudy f rom the EBMT (abstr ) . B lood 2000;96:558a.
539. Cra iu A, Sai to Y, Limon A, et al . F lowing ce l ls through pulsed e lec t r ic f ie lds ef f ic ient ly
purges s tem cel l preparat ions of contaminat ing myeloma ce l ls whi le preserving s tem cel l
funct ion. Blood 2005;105:2235–2238.
540. Tr icot G, Vesole DH, Jagannath S, e t a l . Graf t -versus-myeloma ef fec t : proof of
pr inc ip le. Blood 1996;87:1196–1198.
541. Mart ine l l i G, Terragna C, Zamagni E, et al . Molecular remiss ion af ter a l logeneic or
autologous t ransplantat ion of hematopoiet ic s tem cel ls for mul t ip le myeloma. J Cl in Oncol
2000;18:2273–2281.
542. Corrad in i P, Cavo M, Lokhors t H, e t a l . Molecular remission af ter myeloablat ive
a l logeneic s tem cel l t ransplantat ion pred ic ts a bet ter re lapse- f ree survival in pat ients wi th
mult ip le myeloma. Blood 2003;102:1927–1929.
543. Cavo M, Bandini G, Benni M, e t al . High-dose busul fan and cyc lophosphamide are an
ef fec t ive condi t ioning reg imen for a l logeneic bone marrow t ransplantat ion in chemosensi t ive
mult ip le myeloma. Bone Marrow Transplant 1998;22:27–32.
544. Gahrton G, Tura S, L jungman P, et al . Al logeneic bone marrow t ransplantat ion in
mult ip le myeloma. European Group for Bone Marrow Transplantat ion. N Engl J Med
1991;325:1267–1273.
545. Gahrton G, Tura S, L jungman P, et al . An update of prognost ic fac tors for al logeneic
bone marrow t ransplantat ion in mul t ip le myeloma us ing matched s ib l ing donors. European
Group for Blood and Marrow Transplantat ion. Stem Cel ls (Dayt) . 1995;13(suppl 2) :122–125.
546. Hunter HM, Peggs K, Powles R, et al . Analys is o f outcome fol lowing a l logeneic
haemopoiet ic s tem ce l l t ransplantat ion for myeloma using myeloablat ive condi t ion ing—
evidence for a super ior outcome us ing melphalan combined wi th total body i r rad iat ion. Br J
Haematol 2005;128:496–502.
547. Kennedy GA, But ler J , Morton J , e t a l . Myeloablat ive a l logeneic s tem cel l
t ransplantat ion for advanced s tage mult ip le myeloma: very long-term fo l low up of a s ingle
center exper ience. Cl in Lab Haemato l 2006;28:189–197.
548. Gahrton G, Svensson H, Cavo M, e t al . Progress in a l logenic bone marrow and
per iphera l b lood s tem cel l t ransplantat ion for mult ip le myeloma: a comparison between
t ransplants per formed 1983–93 and 1994–8 at European Group for Blood and Marrow
Transplantat ion centres. Br J Haematol 2001; 113:209–216.
549. Bjorks t rand BB, Ljungman P, Svensson H, et a l . A l logeneic bone marrow
t ransplantat ion versus auto logous stem cel l t ransplantat ion in mul t ip le myeloma: a
re t rospect ive case-matched s tudy f rom the European Group for Blood and Marrow
Transplantat ion. Blood 1996;88:4711–4718.
550. Var teras ian M, Janak i raman N, Karanes C, e t al . Transplantat ion in pat ients wi th
mult ip le myeloma: a mul t icenter comparat ive analys is o f peripheral blood s tem cel l and
a l logeneic t ransplant . Am J Cl in Oncol 1997;20:462–466.
551. Couban S, Stewart AK, Loach D, e t a l . Autologous and a l logeneic t ransplantat ion for
mult ip le myeloma at a s ing le centre . Bone Marrow Transplant 1997;19:783–789.
552. Lokhorst HM, Sonneveld P, Cornel issen JJ , e t al . Induct ion therapy wi th v incr is t ine,
adr iamycin, dexamethasone (VAD) and in termediate-dose melphalan ( IDM) fo l lowed by
autologous or al logeneic s tem cel l t ransplantat ion in newly d iagnosed mul t ip le myeloma.
Bone Marrow Transplant 1999;23:317–322.
553. Reynolds C, Ratanatharathorn V, Adams P, e t al . Al logeneic s tem cel l t ransplantat ion
reduces disease progress ion compared to auto logous t ransplantat ion in pat ients wi th
mult ip le myeloma. Bone Marrow Transplant 2001;27:801–807.
554. Alyea E, Wel ler E, Schlossman R, et al . Outcome af ter autologous and al logeneic s tem
cel l t ransplantat ion for pat ients wi th mult ip le myeloma: impact of graf t -versus-myeloma
ef fec t . Bone Marrow Transplant 2003;32:1145–1151.
555. Arora M, McGlave PB, Burns LJ, e t a l . Resul ts o f auto logous and al logeneic
hematopoiet ic cel l t ransplant therapy for mul t ip le myeloma. Bone Marrow Transplant
2005;35:1133–1140.
556. Lokhorst HM, Segeren CM, Verdonck LF, e t a l . Par t ia l ly T-ce l l -depleted al logeneic
s tem-cel l t ransplantat ion for f i rs t - l ine t reatment of mul t ip le myeloma: a prospect ive
evaluat ion of pat ients treated in the phase I I I s tudy HOVON 24 MM. J Cl in Oncol
2003;21:1728–1733.
557. Bal len KK, King R, Cars ton M, e t a l . Outcome of unrela ted t ransplants in pat ients wi th
mult ip le myeloma. Bone Marrow Transplant 2005;35:675–681.
558. Gi ral t S, Aleman A, Anagnostopoulos A, e t al . Fludarabine/melphalan condit ion ing for
a l logeneic t ransplantat ion in pat ients wi th mult ip le myeloma. Bone Marrow Transplant
2002;30:367–373.
559. Qazi lbash MH, Sal iba R, De Lima M, e t al . Second auto logous or a l logeneic
t ransplantat ion af ter the fa i lure of f i rs t autograf t in pat ients wi th mult ip le myeloma. Cancer
2006;106:1084–1089.
560. Crawley C, La lancet te M, Szydlo R, e t al . Outcomes for reduced- in tens i ty a l logeneic
t ransplantat ion for mul t ip le myeloma: an analys is of prognost ic fac tors f rom the Chronic
Leukaemia Working Party o f the EBMT. Blood 2005;105:4532–4539.
561. Maloney DG, Mol ina AJ, Sahebi F, e t a l . A l lograft ing wi th nonmyeloablat ive
condi t ion ing fo l lowing cytoreduct ive autograf ts for the t reatment o f pat ients wi th mult ip le
myeloma. Blood 2003;102:3447–3454.
562. Kroger N, Schwerdtfeger R, Kiehl M, e t al . Auto logous stem cel l t ransplantat ion
fo l lowed by a dose-reduced a l lograf t induces high complete remiss ion ra te in mul t ip le
myeloma. Blood 2002;100:755–760.
563. Kroger N. Auto logous-al logeneic tandem stem cel l t ransplantat ion in pat ients wi th
mult ip le myeloma. Leuk Lymphoma 2005;46:813–821.
564. Kroger N, Sayer HG, Schwerdtfeger R, e t a l . Unre la ted s tem cel l t ransplantat ion in
mult ip le myeloma af ter a reduced- in tensi ty condi t ioning wi th pret ransplantat ion
ant i thymocyte g lobul in is h igh ly ef fec t ive wi th low t ransplantat ion-re la ted morta l i ty . B lood
2002;100:3919–3924.
565. Garban F, At ta l M, Michal le t M, e t al . Prospect ive comparison of auto logous s tem cel l
t ransplantat ion fo l lowed by dose-reduced al lograft ( IFM99-03 t r ia l ) wi th tandem autologous
stem cel l t ransplantat ion ( IFM99-04 t r ia l ) in h igh-r isk de novo mul t ip le myeloma. Blood
2006;107:3474–3480.
566. Moreau P, Hul l in C, Garban F, e t a l . Tandem autologous stem cel l t ransplantat ion in
h igh-r isk de novo mul t ip le myeloma: f ina l resu l ts of the prospect ive and randomized IFM 99-
04 protocol . Blood 2006;107:397–403.
567. Bruno B, Rot ta M, Patr iarca F, e t a l . Double auto logous t ransplant versus tandem
autologus–non myeloablat ive a l logeneic t ransplant for newly d iagnosed mult ip le myeloma.
ASH Annual Meet ing Abstr . 2005;106:46.
568. Lee CK, Zangari M, Fassas A, e t a l . Clonal cytogenet ic changes and myeloma relapse
af ter reduced in tens i ty condi t ion ing a l logeneic t ransplantat ion. Bone Marrow Transplant
2006;37:511–515.
569. Lokhorst HM, Schattenberg A, Cornel issen JJ , et al . Donor leukocyte in fusions are
ef fec t ive in relapsed mult ip le myeloma af ter a l logeneic bone marrow t ransplantat ion. Blood
1997;90:4206–4211.
570. Alyea E, Wel ler E, Schlossman R, et al . T-ce l l–depleted a l logeneic bone marrow
t ransplantat ion fo l lowed by donor lymphocyte in fus ion in pat ients wi th mul t ip le myeloma:
induct ion of graf t -versus-myeloma effect . Blood 2001; 98:934–939.
571. Peggs KS, Mackinnon S, W il l iams CD, et a l . Reduced- intens i ty t ransplantat ion wi th in
v ivo T-ce l l deplet ion and adjuvant dose-escalat ing donor lymphocyte in fus ions for
chemotherapy-sens i t ive myeloma: l imi ted eff icacy of graf t -versus- tumor act iv i ty. B iol Blood
Marrow Transplant 2003;9:257–265.
572. Peggs KS, Thomson K, Hart DP, e t a l . Dose-escalated donor lymphocyte in fus ions
fo l lowing reduced in tensi ty t ransplantat ion: toxic i ty, ch imer ism, and disease responses.
Blood 2004;103:1548–1556.
573. Ayuk F, Shimoni A, Nagler A, e t a l . Ef f icacy and toxic i ty of low-dose escalat ing donor
lymphocyte in fusion g iven af ter reduced intens i ty condi t ioning a l lograf t for mult ip le myeloma.
Leukemia 2004;18:659–662.
574. van de Donk NW , Kroger N, Hegenbart U, et a l . Prognost ic factors for donor
lymphocyte in fus ions fol lowing non-myeloablat ive a l logeneic s tem cel l t ransplantat ion in
mult ip le myeloma. Bone Marrow Transplant 2006;37:1135–1141.
575. Lokhorst HM, W u K, Verdonck LF, e t a l . The occurrence of graf t -versus-host disease is
the major pred ic t ive fac tor for response to donor lymphocyte in fus ions in mult ip le myeloma.
Blood 2004;103:4362–4364.
576. Lokhorst HM, Schattenberg A, Cornel issen JJ , et al . Donor lymphocyte infus ions for
re lapsed mul t ip le myeloma af ter al logeneic s tem-cel l t ransplantat ion: pred ict ive factors for
response and long-term outcome. J Cl in Oncol 2000;18:3031–3037.
577. Peggs K, Mackinnon S. Graf t -versus-myeloma: are durable responses a c l in ica l real i ty
fo l lowing donor lymphocyte in fusion? Leukemia 2004;18: 1541–1542; author rep ly 1542–
1543.
578. Kyle RA, Pierre RV, Bayrd ED. Mul t ip le myeloma and acute myelomonocyt ic leukemia.
N Engl J Med 1970;283:1121–1125.
579. Nordenson N. Myelomatos is : a c l in ica l review of 310 cases. Acta Med Scand
1966;445(suppl ) :178–186.
P.2430

580. Osserman EF, Takatsuk i K and Tala l N. The pathogenes is of “amyloidosis. ” Semin
Hemato l 1964;1:3–85.
581. Edwards GA, Zawadzk i ZA. Ext raosseous les ions in p lasma cel l myeloma: a repor t o f
s ix cases. Am J Med 1967;43:194–205.
582. Gonzalez F, Truj i l lo JM, Alexanian R. Acute leukemia in mul t ip le myeloma. Ann In tern
Med 1977;86:440–443.
583. Bergsagel DE, Bai ley AJ, Langley GR, et a l . The chemotherapy on plasma-cel l
myeloma and the incidence of acute leukemia. N Engl J Med 1979;301:743–748.
584. Cohen HJ, Bar tolucc i AA, Forman WB, et al . Consol idat ion and maintenance therapy in
mult ip le myeloma: randomized compar ison of a new approach to therapy af ter in i t ia l
response to treatment . J Cl in Oncol 1986;4:888–899.
585. Remiss ion maintenance therapy for mul t ip le myeloma. Arch In tern Med 1975;135:147–
152.
586. Belch A, Shel ley W, Bergsagel D, et al . A randomized t r ia l o f maintenance versus no
maintenance melphalan and prednisone in responding mul t ip le myeloma pat ients . Br J
Cancer 1988;57:94–99.
587. Alexanian R, Gehan E, Haut A, e t a l . Unmainta ined remiss ions in mult ip le myeloma.
Blood 1978;51:1005–1011.
588. Corso A, Nozza A, Lazzar ino M, e t al . P la teau phase in mul t ip le myeloma: an end-point
o f convent ional -dose chemotherapy. Haematologica 1999;84:336–341.
589. Anonymous. Long-term survival in mul t ip le myeloma: a Finn ish Leukaemia Group s tudy.
Br J Haematol 1999;105:942–947.
590. Nagura E, Ich ikawa A, Kamiya O, e t a l . A randomized study comparing VMCP and
MMPP in the t reatment of mul t ip le myeloma. Cancer Chemother Pharmacol 1997;39:279–
285.
591. Blade J , Lopez-Gui l lermo A, Bosch F, e t a l . Impact o f response to t reatment on
surviva l in mul t ip le myeloma: resul ts in a series of 243 pat ients . Br J Haemato l
1994;88:117–121.
592. Dur ie BG, Jacobson J , Bar log ie B, e t a l . Magni tude of response wi th myeloma f ront l ine
therapy does not pred ic t outcome: importance of t ime to progression in southwest oncology
group chemotherapy t r ia ls . J Cl in Oncol 2004;22:1857–1863.
593. Oivanen TM, Kel lokumpu-Leht inen P, Koiv isto AM, et al . Response leve l and survival
a f ter convent ional chemotherapy for mult ip le myeloma: a Finn ish Leukaemia Group study.
Eur J Haemato l 1999;62:109–116.
594. Barlogie B, Tr icot G, Anaiss ie E, e t a l . Thal idomide and hematopoiet ic -ce l l
t ransplantat ion for mul t ip le myeloma. N Engl J Med 2006;354:1021–1030.
595. Paccagnel la A, Chiar ion-Si leni V, Soesan M, e t a l . Second and th i rd responses to the
same induct ion reg imen in re lapsing pat ients wi th mul t ip le myeloma. Cancer 1991;68:975–
980.
596. Berenson JR, Crowley JJ, Grogan TM, et a l . Maintenance therapy wi th a l ternate-day
prednisone improves surviva l in mul t ip le myeloma pat ients . Blood 2002;99:3163–3168.

597. Alexanian R, W eber D, Dimopoulos M, e t a l . Randomized t r ia l o f a lpha- inter feron or
dexamethasone as maintenance t reatment for mul t ip le myeloma. Am J Hemato l
2000;65:204–209.
598. Mandel l i F, Avvisat i G, Amadori S, e t a l . Maintenance t reatment wi th recombinant
in ter feron a l fa-2b in pat ients wi th mult ip le myeloma responding to convent ional induct ion
chemotherapy. N Engl J Med 1990;322:1430–1434.
599. Drayson MT, Chapman CE, Dunn JA, e t a l . MRC t r ia l o f a lpha2b- in ter feron
maintenance therapy in f i rs t p la teau phase of mult ip le myeloma. MRC W ork ing Party on
Leukaemia in Adults . Br J Haemato l 1998;101:195–202.
600. Salmon SE, Beckord J , Pugh RP, e t a l . a lpha- In ter feron for remission maintenance:
pre l iminary repor t on the Southwest Oncology Group Study. Semin Oncol 1991;18:33–36.
601. Browman GP, Bergsagel D, Sicher i D, e t a l . Randomized tr ia l of in ter feron
maintenance in mul t ip le myeloma: a s tudy of the Nat ional Cancer Ins t i tu te o f Canada
Cl inical Tr ials Group. J Cl in Oncol 1995;13:2354–2360.
602. Bergsagel D, Browman G, Sicher i D. Randomized t r ia l o f in ter feron-a lpha maintenance
in myeloma pat ients responding to melphalan and prednisone (MY-6) . VI In ternat ional
Workshop on Mul t ip le Myeloma, Boston, 1997.
603. Vela-Ojeda J , Garcia-Ruiz EM, Padi l la-Gonzalez Y. Alpha in ter feron ( IFN) for the
maintenance phase of pat ients (PTS) wi th mul t ip le myeloma (MM). The Mexican exper ience.
IV In ternat ional Workshop on Mul t ip le Myeloma, Boston, 1997.
604. W est in J , Cor telezzi A, Hjor th M, e t al . In terferon therapy during the p la teau phase of
mult ip le myeloma: an update of the Swedish s tudy. Eur J Cancer 1991;27:S45–S48.
605. Blade J , San Miguel JF, Escudero ML, e t a l . Maintenance t reatment wi th in ter feron
a lpha-2b in mult ip le myeloma: a prospect ive randomized s tudy f rom PETHEMA (Program for
the Study and Treatment o f Hemato logical Mal ignancies, Spanish Soc iety o f Hemato logy) .
Leukemia 1998;12:1144–1148.
606. McSweeney EN, Tobias JS, Blackman G, et a l . Double hemibody i r rad ia t ion (DHBI) in
the management o f re lapsed and primary chemores is tant mul t ip le myeloma. Cl in Oncol
1993;5:378–383.
607. Gro isbois B, Mary JY, Michaux JL. In ter feron maintenance therapy in mul t ip le myeloma
pat ients ach ieving p lateau phase af ter induct ion therapy: a mul t icenter randomized t r ia l . VI
In ternat ional W orkshop on Mul t ip le Myeloma, Boston, 1997 (abstr ) .
608. Powles R, Raje N, Cunningham D, e t al . Maintenance therapy for remission in myeloma
wi th In t ron A fo l lowing h igh-dose melphalan and e i ther an autologous bone marrow
t ransplantat ion or per iphera l s tem cel l rescue. Stem Cel ls 1995;13(suppl 2) :114–117.
609. W est in J . In ter feron therapy dur ing the p la teau phase of mul t ip le myeloma: an update
of a Swedish mul t icenter s tudy. Semin Oncol 1991;18:37–40.
610. Cunningham D, Powles R, Malpas J, et al . A randomized t r ia l o f maintenance
in ter feron fo l lowing h igh-dose chemotherapy in mul t ip le myeloma: long-term fol low-up
resul ts . Br J Haemato l 1998;102:495–502.
611. Pulsoni A, Avvisat i G, Teresa Petrucc i M, e t a l . The I ta l ian exper ience on inter feron as
maintenance t reatment in mul t ip le myeloma: ten years af ter [ le t ter ] . B lood 1998;92:2184–
2186.

612. Palumbo A, Boccadoro M, Gar ino LA, e t a l . Mul t ip le myeloma: in tensi f ied maintenance
therapy wi th recombinant inter feron-a lpha-2b p lus glucocor t ico ids . Eur J Haematol
1992;49:93–97.
613. Palumbo A, Boccadoro M, Gar ino LA, e t a l . In ter feron plus glucocor t ico ids as
in tensi f ied maintenance therapy prolongs tumor control in re lapsed myeloma. Acta
Haematologica 1993;90:71–76.
614. Bjorks t rand B, Svensson H, Goldschmidt H, e t al . Alpha- in terferon maintenance
t reatment is assoc ia ted wi th improved surviva l a f ter high-dose t reatment and auto logous
s tem cel l t ransplantat ion in pat ients wi th mul t ip le myeloma: a re t rospect ive regist ry s tudy
f rom the European Group for Blood and Marrow Transplantat ion (EBMT). Bone Marrow
Transplant 2001;27:511–515.
615. Br inker BT, W al ler EK, Leong T, e t a l . Maintenance therapy wi th thal idomide improves
overa l l surviva l a f ter auto logous hematopoiet ic progeni tor ce l l t ransplantat ion for mult ip le
myeloma. Cancer 2006;106:2171–2180.
616. Sahebi F, Spie lberger R, Kogut NM, et a l . Maintenance tha l idomide fo l lowing sing le
cyc le autologous per iphera l b lood s tem cel l t ransplant in pat ients wi th mul t ip le myeloma.
Bone Marrow Transplant 2006;37:825–829.
617. Stewart AK, Chen CI , Howson-Jan K, e t a l . Resul ts o f a mul t icenter randomized phase
I I t r ia l o f thal idomide and prednisone maintenance therapy for mul t ip le myeloma af ter
autologous s tem cel l t ransplant . Cl in Cancer Res 2004;10:8170–8176.
618. At ta l M, Harousseau J-L, Leyvraz S, et al . Maintenance therapy wi th tha l idomide
improves surviva l in mul t ip le myeloma pat ients. Blood 2006; 108:3289.
619. Banchereau J , Ste inman RM. Dendri t ic ce l ls and the control of immuni ty. Nature
1998;392:245–252.
620. Osterborg A, Henriksson L, Mel lstedt H. Id iotype immuni ty (natura l and vaccine-
induced) in ear ly s tage mult ip le myeloma. Acta Oncol 2000;39:797–800.
621. Cosc ia M, Mar ian i S, Bat tagl io S, e t al . Long-term fo l low-up of id iotype vaccinat ion in
human myeloma as a maintenance therapy af ter h igh-dose chemotherapy. Leukemia
2004;18:139–145.
622. Reichardt VL, Mi lazzo C, Brugger W , et a l . Id io type vacc inat ion of mul t ip le myeloma
pat ients using monocyte-der ived dendr i t ic cel ls . Haematologica 2003;88:1139–1149.
623. Hsu FJ, Benike C, Fagnoni F, e t a l . Vaccinat ion of pat ients wi th B-ce l l lymphoma using
autologous ant igen-pulsed dendr i t ic cel ls . Nat Med 1996;2:52–58.
624. Baner jee DK, Dhodapkar MV, Matayeva E, e t al . Expansion of FOXP3high regulatory T
ce l ls by human dendr i t ic ce l ls (DCs) in v i t ro and af ter in ject ion of cytokine-matured DCs in
myeloma pat ients . Blood 2006;108:2655–2661.
625. Mi lazzo C, Reichardt VL, Mul ler MR, et a l . Induct ion of myeloma-spec i f ic cytotoxic T
ce l ls us ing dendr i t ic cel ls t ransfected wi th tumor-der ived RNA. Blood 2003;101:977–982.
626. Reichardt VL, Brossar t P. Dendri t ic ce l ls in c l in ical t r ia ls for mul t ip le myeloma.
Methods Mol Med 2005;109:127–136.
627. Paccagnel la A, Carte i G, Fosser V, e t a l . Treatment o f mul t ip le myeloma wi th M-2
protocol and wi thout maintenance therapy. Eur J Cancer Cl in Oncol 1983;19:1345–1351.
628. Kyle RA, Gai lani S, Sel igman BR, e t a l . Mul t ip le myeloma res is tant to melphalan:
t reatment wi th cyclophosphamide, prednisone, and BCNU. Cancer Treat Rep 1979;63:1265–
1269.

629. Bergsagel DE, Sprague CC, Aust in C, e t a l . Evaluat ion of new chemotherpeut ic agents
in the t reatment o f mul t ip le myeloma. IV. L-Phenyalanine mustard (NSC-8806). Cancer
Chemother Rep 1972;21.
630. Kyle RA, Sel igman BR, W al lace HJ Jr , e t a l . Mut ip le myeloma res is tant to melphalan
(NSC-8806) t reated wi th cyc lophosphamide (NSC-26271), prednisone (NSC-10023), and
ch loroquine (NSC-187208). Cancer Chemother Rep—Part 1 1975;59:557–562.
631. Cohen HJ, Si lberman HR, Larsen W E, et al . Combinat ion chemotherapy wi th
in termi t tent 1-3-b is(2-chloroethyl )1- n i t rosourea (BCNU), cyclophosphamide, and
prednisone for mult ip le myeloma. Blood 1979;54:824–836.
632. Buzaid AC, Garewal HS, Greenberg BR. Management o f myelodysplast ic syndromes.
Am J Med 1986;80:1149–1157.
633. Blade J , Fel iu E, Rozman C, et al . Cross-res is tance to a lkylat ing agents in mul t ip le
myeloma. Cancer 1983;52:786–789.
634. Bergsagel DE, Cowan DH, Hasselback RH. Plasma ce l l myeloma: response of
melphalan-res is tant pat ients to h igh-dose in termit tent cyclophosphamide. Can Med Assoc J
1972;107:851–855.
635. Brandes LJ, Is raels LG. Treatment of advanced p lasma cel l myeloma wi th week ly
cyc lophosphamide and al ternate-day prednisone. Cancer Treat Rep 1982;66:1413–1415.
636. W i lson K, Shel ley W, Belch A, e t a l . W eekly cyc lophosphamide and a l ternate-day
prednisone: an ef fec t ive secondary therapy in mul t ip le myeloma. Cancer Treat Rep
1987;71:981–982.
637. de W eerdt O, van de Donk NW, Veth G, e t al . Cont inuous low-dose cyc lophosphamide-
prednisone is e f fec t ive and wel l to lerated in pat ients wi th advanced mul t ip le myeloma.
Netherlands J Med 2001;59:50–56.
638. Lenhard RE, Danie ls MJ, Oken MM, et a l . An aggressive high dose cyc lophosphamide
and prednisone regimen for advanced mul t ip le myeloma. Leuk Lymphoma 1994;13:485–489.
639. Lenhard RE Jr , Kal ish LA, Oken MM, et a l . Timed-sequent ial high-dose
cyc lophosphamide and vincr ist ine in the t reatment of mul t ip le myeloma. Cancer
1994;73:2113–2118.
640. Palumbo A, Boccadoro M, Bruno B, e t al . Cyc lophosphamide (3.6 g/m2) therapy wi th
G-CSF support for res is tant myeloma. Haematolog ica 1994;79: 513–518.
641. Cavo M, Gal ien i P, Tass i C, e t al . M-2 protocol for melphalan-resistant and re lapsing
mult ip le myeloma. Eur J Haematol 1988;40:168–173.
642. Dimopoulos MA, Delasal le KB, Champl in R, e t al . Cyclophosphamide and etopos ide
therapy wi th GM-CSF for VAD-resistant mult ip le myeloma. Br J Haematol 1993;83:240–244.
643. Presant CA and Klahr C. Adr iamycin, 1 ,3-b is (2-ch loroethyl ) 1 ni t rosourea (BCNU, NSC
No. 409962), cyclophosphamide plus prednisone (ABC-P) in melphalanresis tant mul t ip le
myeloma. Cancer 1978;42:1222–1227.
P.2431
644. Kyle RA, Pajak TF, Henderson ES, e t a l . Mul t ip le myeloma resis tant to melphalan:
t reatment wi th doxorubic in , cyc lophosphamide, carmust ine (BCNU), and prednisone. Cancer
Treat Rep 1982;66:451–456.

645. Bonnet J , Alexanian R, Salmon S, et al . Vincr is t ine, BCNU, doxorubic in, and
prednisone (VBAP) combinat ion in the t reatment o f relaps ing or resis tant mult ip le myeloma:
a Southwest Oncology Group s tudy. Cancer Treat Rep 1982;66:1267–1271.
646. Blade J , Rozman C, Montserrat E, e t a l . Treatment o f a lkyla t ing res is tant mult ip le
myeloma wi th v incr is t ine, BCNU, doxorubic in and prednisone (VBAP). Eur J Cancer Cl in
Oncol 1986;22:1193–1197.
647. Stenzinger W, Blomker A, Hiddemann W , et a l . Treatment o f re f rac tory mult ip le
myeloma wi th the v incr ist ine- adr iamycin-dexamethasone (VAD) regimen. Blu t 1990;61:55–
59.
648. Moncondui t M, Le Loet X, Bernard JF, et a l . Combinat ion chemotherapy wi th v incr is t ine,
doxorubic in, dexamethasone for re f rac tory or re laps ing mul t ip le myeloma. Br J Haematol
1986;63:599–601.
649. Anderson H, Scar f fe JH, Lambert M, e t a l . VAD chemotherapy—toxic i ty and ef f icacy—
in pat ients wi th mul t ip le myeloma and other lymphoid mal ignanc ies. Hemato l Oncol
1987;5:213–222.
650. Browman GP, Belch A, Ski l l ings J , e t a l . Modi f ied adriamyc in-vincr ist ine-
dexamethasone (m-VAD) in pr imary re f rac tory and relapsed plasma ce l l myeloma: an NCI
(Canada) p i lo t s tudy. The National Cancer Inst i tute o f Canada Cl in ical Tr ia ls Group. Br J
Haematol 1992;82:555–559.
651. Gimsing P, Bjerrum OW , Brandt E, et al . Refrac tory myelomatosis t reated wi th
mi toxantrone in combinat ion wi th v incr is t ine and prednisone (NOP-regimen): a phase I I
s tudy. The Nord ic Myeloma Study Group (NMSG). Br J Haemato l 1991;77:73–79.
652. W islo f f F, Gimsing P, Hedenus M, e t al . Bo lus therapy wi th mi toxantrone and
vincr is t ine in combinat ion wi th high-dose prednisone (NOP-bolus) in res istant mul t ip le
myeloma. Nord ic Myeloma Study Group (NMSG). Eur J Haemato l 1992;48:70–74.
653. Phi l l ips JK, Sher law-Johnson C, Pearce R, et a l . A randomized s tudy of MOD versus
VAD in the t reatment o f re lapsed and resistant mul t ip le myeloma. Leuk Lymphoma
1995;17:465–472.
654. Vincent M, Goss G, Sinof f C, e t a l . B i -week ly v incr is t ine, ep i rub ic in and
methylpredniso lone in a lkyla tor- re frac tory mult ip le myeloma. Cancer Chemother Pharmacol .
1994;34:356–360.
655. Alexanian R, Barlogie B, Gut terman J . Alpha- in ter feron combinat ion therapy of
res is tant myeloma. Am J Cl in Oncol 1991;14:188–192.
656. Adam Z, Elb l L , Vorl icek J , e t a l . Treatment o f ref rac tory mul t ip le myeloma wi th
v incr is t ine, adr iamycin, dexamethasone, and wi th repeated appl icat ion of cyc lophosphamide
(C- VAD). Acta Med Austr iaca 1994;21:111–115.
657. Dimopoulos MA, Weber D, Kantarj ian H, e t a l . HyperCVAD for VAD-res is tant mul t ip le
myeloma. Am J Hematol 1996;52:77–81.
658. Dimopoulos MA, Zervas K, Kouvatseas G, e t a l . Thal idomide and dexamethasone
combinat ion for re fractory mul t ip le myeloma. Ann Oncol 2001;12:991–995.
659. W eber DM, Gavino M, Delasal le K, et al . Thal idomide alone or wi th dexamethasone for
mult ip le myeloma. Blood 1999;94(suppl 1) :601a (abstr 2686).
660. Palumbo A, Giaccone L, Berto la A, e t a l . Low-dose tha l idomide p lus dexamethasone is
an ef fec t ive sa lvage therapy for advanced myeloma. Haemato log ica 2001;86:399–403.

661. Myers B, Gr imley C, Dolan G. Thal idomide and low-dose dexamethasone in myeloma
t reatment . [ let ter; comment ] . Br J Haematol 2001;114:245.
662. W eber DM, Rank in K, Gavino M, e t a l . Thal idomide wi th dexamethasone for resistant
mult ip le myeloma. Blood 2000;96(suppl 1) :168a (abstr 719) .
663. Coleman M, Leonard JP, Nahum K, e t al . Non-myelosuppressive therapy wi th BLT-D
(Biaxin , low dose tha l idomide and dexamethasone) is highly ac t ive in W aldenstrom's
macroglobul inemia and myeloma (abst ract ) . Blood 2000; 96:167a.
664. Garcia-Sanz R, Gonzalez-Porras JR, Hernandez JM, et a l . The ora l combinat ion of
tha l idomide, cyc lophosphamide and dexamethasone (ThaCyDex) is e f fec t ive in
re lapsed/ref rac tory mul t ip le myeloma. Leukemia 2004;18:856–863.
665. Dimopoulos MA, Hami los G, Zomas A, e t a l . Pu lsed cyclophosphamide, tha l idomide
and dexamethasone: an ora l regimen for previous ly t reated pat ients wi th mult ip le myeloma.
Hemato l J 2004;5:112–117.
666. Kropf f MH, Lang N, Bisping G, et al . Hyperf rac t ionated cyc lophosphamide in
combinat ion wi th pu lsed dexamethasone and tha l idomide (HyperCDT) in pr imary re f rac tory
or relapsed mult ip le myeloma. Br J Haemato l 2003;122: 607–616.
667. Kyr iakou C, Thomson K, D'Sa S, e t a l . Low-dose tha l idomide in combinat ion wi th oral
week ly cyclophosphamide and pulsed dexamethasone is a wel l to lerated and ef fec t ive
reg imen in pat ients wi th re lapsed and ref ractory mult ip le myeloma. Br J Haematol
2005;129:763–770.
668. Sidra G, W il l iams CD, Russel l NH, e t a l . Combinat ion chemotherapy wi th
cyc lophosphamide, tha l idomide and dexamethasone for pat ients wi th re frac tory, newly
d iagnosed or re lapsed myeloma. Haematolog ica 2006;91:862–863.
669. Palumbo A, Avonto I , Bruno B, e t a l . In t ravenous melphalan, tha l idomide and
prednisone in ref rac tory and re lapsed mul t ip le myeloma. Eur J Haemato l 2006;76:273–277.
670. Of f idani M, Marconi M, Corvat ta L , e t a l . Thal idomide plus ora l melphalan for advanced
mult ip le myeloma: a phase I I s tudy. Haemato log ica 2003;88:1432–1433.
671. Hovenga S, Daenen SM, de W olf JT, e t al . Combined thal idomide and
cyc lophosphamide t reatment for ref rac tory or relapsed mul t ip le myeloma pat ients : a
prospect ive phase I I s tudy. Ann Hematol 2005;84:311–316.
672. Lee CK, Bar logie B, Munshi N, e t a l . DTPACE: an ef fect ive, novel combinat ion
chemotherapy wi th thal idomide for previously t reated pat ients wi th myeloma. J Cl in Oncol
2003;21:2732–2739.
673. Of f idani M, Corvat ta L , Marconi M, e t a l . Low-dose tha l idomide wi th pegylated
l iposomal doxorubic in and h igh-dose dexamethasone for re lapsed/ re frac tory mul t ip le
myeloma: a prospect ive, mul t icenter, phase I I study. Haemato log ica 2006;91:133–136.
674. Moehler TM, Neben K, Benner A, e t al . Sa lvage therapy for mult ip le myeloma wi th
tha l idomide and CED chemotherapy. Blood 2001;98:3846–3848.
675. Ma MH, Yang HH, Parker K, e t a l . The proteasome inh ibi tor PS-341 markedly enhances
sens i t iv i ty of mult ip le myeloma tumor cel ls to chemotherapeut ic agents. Cl in Cancer Res
2003;9:1136–1144.
676. Goel A, Dispenzier i A, Geyer SM, et a l . Synerg is t ic act iv i ty of the proteasome inh ibi tor
PS-341 wi th non-myeloablat ive 153-Sm-EDTMP skeletal ly targeted rad iotherapy in an
or thotopic model of mult ip le myeloma. Blood 2006; 107:4063–4070.

677. Or lowski RZ, Voorhees PM, Garc ia RA, et al . Phase 1 t r ia l o f the proteasome inhibi tor
bor tezomib and pegylated l iposomal doxorubic in in pat ients wi th advanced hemato log ic
mal ignanc ies. Blood 2005;105:3058–3065.
678. Zangari M, Bar log ie B, Hol lmig K, et al . Marked act iv i ty o f ve lcade p lus thal idomide (V
+T) in advanced and ref rac tory mul t ip le myeloma (MM). ASH Annual Meet ing Abstr
2004;104:1480.
679. Pineda-Roman M, Zangar i M, van Rhee F, et a l . VTD combinat ion therapy wi th
bor tezomib- tha l idomide-dexamethasone is highly e f fec t ive in advanced and ref rac tory
mult ip le myeloma. Leukemia 2008;22:1419–1427.
680. Teoh G, Tan D, Hwang W , et al . Addit ion of bor tezomib to tha l idomide, dexamethasone
and zoledronic acid (VTD-Z regimen) s igni f icant ly improves complete remiss ion rates in
pat ients wi th re lapsed/ref ractory mul t ip le myeloma. J Cl in Oncol (Meet ing Abstr )
2006;24:17537.
681. Ciol l i S, Leoni F, Gig l i F , e t al . Low dose Velcade, thal idomide and dexamethasone
(LD-VTD): an ef fec t ive reg imen for relapsed and ref rac tory mul t ip le myeloma pat ients . Leuk
Lymphoma 2006;47:171–173.
682. Reece DE, Piza Rodr iguez G, Chen C, e t a l . Phase I- I I Tr ial o f bor tezomib p lus oral
cyc lophosphamide and prednisone in re lapsed and refractory mult ip le myeloma. J Cl in
Oncol 2008; in press.
683. Berenson JR, Yang HH, Sadler K, e t a l . Phase I / I I t r ia l assessing bortezomib and
melphalan combinat ion therapy for the t reatment o f pat ients wi th re lapsed or ref rac tory
mult ip le myeloma. J Cl in Oncol 2006;24:937–944.
684. Terpos E, Anagnostopoulos A, Kastr i t is E, e t a l . The combinat ion of bor tezomib,
melphalan, dexamethasone and in termi t tent tha l idomide (VMDT) is an ef fec t ive t reatment
for relapsed/ref rac tory myeloma: resu l ts of a Phase I I c l in ica l t r ia l . B lood 2005;106:110a
(abst r 363) .
685. Palumbo A, Ambrosin i MT, Pregno P, e t al . Ve lcadeT M p lus melphalan, prednisone, and
tha l idomide (V-MPT) for advanced mul t ip le myeloma. ASH Annual Meet ing abst rac ts . Blood
2005;106:717a (abstr 2553).
686. Yeh HS, Swi f t RA, Ferrett i D, e t a l . Phase I s tudy of bortezomib and 153Sm-lexidronam
combinat ion for re fractory and re lapsed mul t ip le myeloma. J Cl in Oncol (Meet ing Abstr )
2006;24:7614.
687. Chari A, Kaplan L, L inker C, e t al . Phase I / I I s tudy of bor tezomib in combinat ion wi th
l iposomal doxorubic in and melphalan in re lapsed or re fractory mult ip le myeloma. ASH
Annual Meet ing Abstr 2005;106:5182.
688. Dimopoulos MA, Spencer A, At tal M, e t al . Study of lenal idomide plus dexamethasone
versus dexamethasone alone in relapsed or re frac tory mul t ip le myeloma (MM): resul ts o f a
phase 3 study (MM-010). Blood 2005;106: abst r 6.
689. W eber DM, Chen C, Niesvizky R, et al . Lenal idomide p lus h igh-dose dexamethasone
provides improved overal l survival compared to high-dose dexamethasone a lone for
re lapsed or ref rac tory mul t ip le myeloma (MM): resu lts o f a North American phase I I I study
(MM-009). J Cl in Oncol (Meet ing Abstr ) 2006; 24:7521.
690. W ang M, Knight R, Dimopoulos M, e t al . Comparison of lenal idomide in combinat ion
wi th dexamethasone to dexamethasone a lone in pat ients who have received prior

tha l idomide in re lapsed or re fractory mult ip le myeloma. J Cl in Oncol (Meet ing Abstr )
2006;24:7522.
691. Baz R, Chouei r i TK, Jawde RA, e t a l . Doxi l (D) , v incr is t ine (V), reduced f requency
dexamethasone (d) and Revl imid ( R ) (DVd-R) Resul ts in a h igh response rate in pat ients wi th
re f rac tory mul t ip le myeloma (RMM). ASH Annual Meet ing Abstr Blood 2005;106:719a (abst r
2559).
692. Gerecke C, Knop S, Topp MS, et al . A mul t icenter phase I / I I Tr ial evaluat ing the safety
and ef f icacy of lenal idomide [Revl imida ( R ) , CC-5013] in combinat ion wi th doxorubic in and
dexamethasone (RAD) in pat ients wi th relapsed or ref rac tory mul t ip le myeloma. ASH Annual
Meet ing abst rac ts. Blood 2005; 106:367b (abst r 5136).
693. Richardson P, Schlossman R, Munshi N, e t a l . A phase 1 t r ia l o f lenal idomide
(REVLIMID ( R ) ) wi th bor tezomib (VELCADE ( R ) ) in re lapsed and ref rac tory mul t ip le myeloma.
ASH Annual Meet ing abst racts . Blood 2005;106:110a (abst r 365) .
694. Abou-Jawde RM, Reed J , Kel ly M, e t a l . Ef f icacy and safety resu l ts wi th the
combinat ion therapy of arsenic t r ioxide, dexamethasone, and ascorb ic ac id in mul t ip le
myeloma pat ients : a phase 2 t r ia l . Med Oncol 2006;23:263–272.
695. W u K, van Droogenbroeck J , Beksac M, e t al . Treatment wi th arsenic t r ioxide, ascorb ic
ac id and dexamethasone in advanced myeloma pat ients : pre l iminary f ind ings of a
mult icenter , phase I I s tudy. ASH Annual Meet ing abst rac ts. Blood 2005;106:367b (abst r
5135).
696. Berenson JR, Bocc ia R, Siegel D, e t a l . Ef f icacy and safety o f melphalan, arsenic
t r ioxide and ascorb ic ac id combinat ion therapy in pat ients wi th relapsed or re f rac tory
mult ip le myeloma: a prospect ive, mult icentre , phase I I , s ingle-arm s tudy. Br J Haematol
2006;135:174–183.
697. Berenson JR, Matous JV, Ferret t i D, et al . A phase I / I I s tudy of arsenic t r ioxide,
bor tezomib, and ascorb ic ac id in relapsed or re fractory mul t ip le myeloma. J Cl in Oncol
(Meet ing Abstr) 2006;24:7611.
698. Ia f fa io l i RV, Facchin i G, Tor tor ie l lo A, e t a l . Modulat ion of chemosens i t iv i ty by alpha
in ter feron in mul t ip le myeloma and non-Hodgk in 's lymphoma. J Exp Ther Oncol 1996;1:226–
230.
699. San Miguel JF, Moro M, Blade J , e t a l . Combinat ion of in ter feron and dexamethasone
in re f rac tory mul t ip le myeloma. Hematol Oncol 1990;8:185–189.
700. Ganjoo RK, Johnson PW , Evans ML, e t al . Recombinant in ter feron-a lpha 2b and h igh
dose methyl predniso lone in relapsed and resis tant mul t ip le myeloma. Hemato l Oncol
1993;11:179–186.
P.2432
701. Sonneveld P, Suc iu S, W ei jermans P, e t a l . Cyc losporin A combined wi th v incr is t ine,
doxorubic in and dexamethasone (VAD) compared wi th VAD a lone in pat ients wi th advanced
ref rac tory mul t ip le myeloma: an EORTC-HOVON randomized phase I I I s tudy (06914). Br J
Haematol 2001;115:895–902.
702. W eber D, Dimopoulos M, Sinic rope F, e t a l . VAD-cyc losporine therapy for VAD-
res is tant mul t ip le myeloma. Leuk Lymphoma 1995;19:159–163.
703. Sonneveld P, Mar ie JP, Huisman C, e t a l . Reversal of mult idrug resis tance by SDZ
PSC 833, combined wi th VAD (vincr is t ine, doxorubic in , dexamethasone) in re f ractory
mult ip le myeloma. A phase I study. Leukemia 1996;10:1741–1750.
704. Fr iedenberg W R, Rue M, Blood EA, e t a l . Phase I I I study of PSC-833 (va lspodar) in
combinat ion wi th v incr is t ine, doxorubic in , and dexamethasone (va lspodar/VAD) versus VAD
a lone in pat ients wi th recurr ing or re f rac tory mul t ip le myeloma (E1A95): a t r ia l of the
Eastern Cooperat ive Oncology Group. Cancer 2006;106:830–838.
705. Treon SP, Pi larski LM, Belch AR, et al . CD20-di rec ted serotherapy in pat ients wi th
mult ip le myeloma: b iologic considerat ions and therapeut ic appl icat ions. J Immunother
2002;25:72–81.
706. Kumar S, W itz ig TE, Timm M, et a l . Expression of VEGF and i ts receptors by myeloma
ce l ls. Leukemia 2003;17:2025–2031.
707. Somlo G, Bel lamy W, Z immerman TM, et a l . Phase I I randomized t r ia l of bevacizumab
versus bevacizumab and thal idomide for relapsed/ref rac tory mul t ip le myeloma. Blood
2005;106:abstr 2571.
708. Zangari M, Anaiss ie E, Stopeck A, e t al . Phase I I s tudy of SU5416, a smal l molecule
vascular endothel ia l growth fac tor tyros ine k inase receptor inh ibi tor, in pat ients wi th
re f rac tory mul t ip le myeloma. Cl in Cancer Res 2004;10:88–95.
709. Chanan-Khan A, Richardson P, Als ina M, e t a l . Phase 1 c l in ical t r ia l o f KOS-953 +
bor tezomib (BZ) in relapsed ref ractory mult ip le myeloma (MM). J Cl in Oncol (Meet ing Abstr)
2006;24:3066.
710. Stone W J. Mul t ip le myelomata. Am J Roentgenol 1924;12:543–545.
711. Jacox JW , Kahn EA. Mul t ip le myeloma wi th sp inal cord involvement . Am J Roentgenol
1933;30:201–205.
712. Sykes MP, Savel H, Chu FCH, et a l . Long-term ef fec ts o f therapeut ic i r rad iat ion upon
bone marrow. Cancer 1964;17:1144–1148.
713. Sykes MP, Chu FCH, Savel H, e t a l . The ef fec ts of varying dosages of i r radia t ion upon
s terna l-marrow regenerat ion. Radiology 1964;83:1084–1087.
714. Nor in T. Roentgen treatment of myeloma wi th spec ial cons iderat ion to the dosage.
Acta Radio l 1957;47:46–57.
715. Rostom AY, O'Cathai l SM, Folkes A. Systemic i r radia t ion in mul t ip le myeloma: a report
on nineteen cases. Br J Haematol 1984;58:423–431.
716. Leigh BR, Kur t ts TA, Mack CF, e t a l . Radiat ion therapy for the pa l l ia t ion of mul t ip le
myeloma. Int J Radiat Oncol Bio l Phys 1993;25:801–804.
717. Adamietz IA, Schober C, Schul te RW , et a l . Pa l l ia t ive rad io therapy in p lasma cel l
myeloma. Radiother Oncol 1991;20:111–116.
718. Frassica DA, Frassica FJ, Schray MF, e t al . So l i tary plasmacytoma of bone: Mayo
Cl inic exper ience. Int J Radiat Oncol Biol Phys 1989;16:43–48.
719. Mendenhal l CM, Thar TL, Mi l l ion RR. Sol i tary p lasmacytoma of bone and sof t t issue.
In t J Radiat Oncol Biol Phys 1980;6:1497–1501.
720. Mi l l W B. Radiat ion therapy in mul t ip le myeloma. Radio logy 1975;115:175–178.
721. Knobel D, Zouhai r A, Tsang RW , et a l . Prognost ic fac tors in so l i tary p lasmacytoma of
the bone: a mul t icenter Rare Cancer Network study. BMC Cancer 2006;6:118.
722. Rao G, Ha CS, Chakrabar t i I , e t a l . Mul t ip le myeloma of the cervica l sp ine: t reatment
s t rategies for pa in and sp ina l ins tab i l i ty . J Neurosurg Spine 2006;5:140–145.

723. Medinger FG, Craver LF. Total body i r rad ia t ion wi th review of cases. Am J Roentgenol
1942;48:651–671.
724. Bergsagel DE. Total body i r rad ia t ion for myelomatosis. Br Med J 1971;2:325.
725. Jaf fe JP, Bosch A, Raich PC. Sequential hemi-body rad io therapy in advanced mul t ip le
myeloma. Cancer 1979;43:124–128.
726. Bosch A, Fr ias Z. Radiotherapy in the t reatment o f mul t ip le myeloma. Int J Radiat
Oncol Bio l Phys 1988;15:1363–1369.
727. Singer FR, Ri tch PS, Lad TE, e t a l . Treatment o f hyperca lcemia of mal ignancy wi th
in t ravenous et idronate. A control led, mul t icenter s tudy. The Hypercalcemia Study Group.
Arch In tern Med 1991;151:471–476.
728. Thomas PJ, Daban A, Bontoux D. Double hemibody i rradia t ion in chemotherapy-
res is tant mul t ip le myeloma. Cancer Treat Rep 1984;68:1173–1175.
729. Tobias JS, Richards JD, Blackman GM, et a l . Hemibody i r rad ia t ion in mul t ip le myeloma.
Radiother Oncol 1985;3:11–16.
730. Troussard X, Roussel A, Reman O, e t a l . Hemibody i rradia t ion in stage I I I mult ip le
myeloma: resul ts o f 20 pat ients . Nouv Rev Fr Hemato l 1988;30:213–218.
731. Rowland CG, Garret t MJ, Crowley FA. Hal f body rad ia t ion in p lasma cel l myeloma. Cl in
Radiol 1983;34:507–510.
732. Qasim MM. Techniques and resul ts o f hal f body i r rad ia t ion (HBI) in metastat ic
carc inomas and myelomas. Cl in Oncol 1979;5:65–68.
733. McIntyre OR, Tef f t M, Proper t K, e t a l . Melphalan and prednisone p lus to tal bone
marrow i r rad ia t ion as in i t ia l t reatment for mul t ip le myeloma. In t J Radiat Oncol Bio l Phys
1988;15:1007–1012.
734. Jacobs P, le Roux I , K ing HS. Sequent ial hal f -body i r rad ia t ion as sa lvage therapy in
chemotherapy-res is tant mult ip le myeloma. Am J Cl in Oncol 1988;11:104–109.
735. Zhan F, Hard in J, Kordsmeier B, et al . Global gene express ion prof i l ing of mul t ip le
myeloma, monoclonal gammopathy of undetermined s igni f icance, and normal bone marrow
p lasma ce l ls. B lood 2002;99:1745-1757.
736. W alker BA, Leone PE, Jenner MW , et a l . Integrat ion of global SNP-based mapping and
express ion arrays reveals key regions, mechanisms, and genes important in the
pathogenes is of mult ip le myeloma. Blood 2006;108:1733–1743.
737. Drewinko B, Alexanian R, Boyer H, et al . The growth frac t ion of human myeloma cel ls .
B lood 1981;57:333–338.
738. Sahota SS, Leo R, Hambl in TJ, et al . Ig VH gene mutat ional pat terns indicate d i f ferent
tumor ce l l s ta tus in human myeloma and monoclonal gammopathy of undetermined
s ign i f icance. Blood 1996;87:746–755.
739. Mer ico F, Bergui L, Gregoret t i MG, et a l . Cytok ines invo lved in the progression of
mult ip le myeloma. Cl in Exp Immunol 1993;92:27–31.
740. Lust JA, Donovan KA. The role o f in ter leukin-1 beta in the pathogenes is o f mul t ip le
myeloma. Hemato l Oncol Cl in North Am 1999;13:1117–1125.
741. Carter A, Merchav S, Si lv ian-Draxler I , et al . The role o f in ter leukin-1 and tumour
necrosis fac tor-a lpha in human mul t ip le myeloma. Br J Haemato l 1990;74:424–431.
742. Dankbar B, Padro T, Leo R, e t al . Vascular endothel ia l growth fac tor and inter leuk in-6
in paracr ine tumor-s t romal ce l l in teract ions in mul t ip le myeloma. Blood 2000;95:2630–2636.

743. Podar K, Ta i YT, Davies FE, e t a l . Vascular endothel ia l growth factor t r iggers s ignal ing
cascades mediat ing mul t ip le myeloma cel l growth and migrat ion. Blood 2001;98:428–435.
744. Han JH, Choi SJ, Kur ihara N, e t a l . Macrophage in f lammatory prote in-1a lpha is an
osteoc lastogenic fac tor in myeloma that is independent o f receptor ac t ivator of nuclear
fac tor kappaB l igand. Blood 2001;97:3349–3353.
745. Roodman GD. Biology of os teoc las t act ivat ion in cancer . J Cl in Oncol 2001;19:3562–
3571.
746. Van Camp B, Dur ie BG, Spier C, e t al . Plasma cel ls in mul t ip le myeloma express a
natura l k i l le r ce l l - assoc ia ted ant igen: CD56 (NKH-1; Leu-19) . Blood 1990;76:377–382.
747. Ahsmann EJ, Lokhors t HM, Dekker AW , et al . Lymphocyte funct ion-associa ted ant igen-
1 express ion on plasma ce l ls correla tes wi th tumor growth in mul t ip le myeloma. Blood
1992;79:2068–2075.
748. Uchiyama H, Barut BA, Mohrbacher AF, e t al . Adhes ion of human myeloma-der ived ce l l
l ines to bone marrow s t romal ce l ls s t imulates in ter leukin-6 secret ion. Blood 1993;82:3712–
3720.
749. Hideshima T, Chauhan D, Podar K, e t a l . Novel therapies target ing the myeloma ce l l
and i ts bone marrow microenvi ronment . Semin Oncol 2001;28:607–612.
750. Mich igami T, Shimizu N, W il l iams PJ, e t a l . Cel l -cel l contact between marrow s t romal
ce l ls and myeloma cel ls v ia VCAM-1 and a lpha(4)beta(1)- in tegr in enhances product ion of
os teoc las t -s t imulat ing act iv i ty. B lood 2000;96:1953–1960.
751. Vincent T, Jourdan M, Sy MS, e t a l . Hyaluron ic ac id induces surviva l and prol i ferat ion
of human myeloma ce l ls through an in ter leuk in-6-mediated pathway invo lving the
phosphorylat ion of re t inoblastoma prote in . J Bio l Chem 2001;276:14728–14736.
752. Houde C, L i Y, Song L, e t a l . Overexpression of the NOTCH l igand JAG2 in mal ignant
p lasma ce l ls f rom mul t ip le myeloma pat ients and ce l l l ines. Blood 2004;104:3697–3704.
753. Landowsk i TH, Olashaw NE, Agrawal D, e t al . Cel l adhesion-mediated drug resis tance
(CAM-DR) is assoc iated wi th ac t ivat ion of NF-kappa B (RelB/p50) in myeloma ce l ls .
Oncogene 2003;22:2417–2421.
754. Bel lamy W T, Richter L , Frut iger Y, e t al . Express ion of vascular endothel ia l growth
fac tor and i ts receptors in hematopoiet ic mal ignancies. Cancer Res 1999;59:728–733.
755. Rajkumar SV, Greipp PR. Angiogenes is in mul t ip le myeloma. Br J Haemato l
2001;113:565.
756. Ribas C, Col leoni GW, Si lva MR, et al . Prognost ic s ign i f icance of vascular endothel ia l
growth fac tor immunoexpress ion in the context o f adverse s tandard prognost ic fac tors in
mult ip le myeloma. Eur J Haematol 2004;73:311–317.
757. Kiml inger T, Kl ine M, Kumar S, e t a l . Di f ferent ia l expression of vascular endothel ia l
growth fac tors and the i r receptors in mul t ip le myeloma. Haemato log ica 2006;91:1033–1040.
758. Yaccoby S, W ezeman MJ, Zangari M, e t al . Inh ib i tory e ffec ts o f osteoblasts and
increased bone formation on myeloma in novel cu l ture systems and a myelomatous mouse
model . Haemato log ica 2006;91:192–199.
759. Tian E, Zhan F, Walker R, et al . The ro le of the W nt-s ignal ing antagonist DKK1 in the
development o f osteolyt ic lesions in mul t ip le myeloma. N Engl J Med 2003;349:2483–2494.
760. Choi SJ, Oba Y, Gazi t t Y, e t al . Ant isense inh ibi t ion of macrophage in f lammatory
protein 1-alpha blocks bone destruc t ion in a model of myeloma bone d isease. J Cl in Invest
2001;108:1833–1841.
761. Nordan RP, Mock BA, Neckers LM, et a l . The role of plasmacytoma growth fac tor in the
in v i t ro responses of murine p lasmacytoma ce l ls. Ann N Y Acad Sc i 1989;557:200–205.
762. Xu FH, Sharma S, Gardner A, e t al . In ter leuk in-6-induced inh ibi t ion of mult ip le
myeloma ce l l apoptosis : support for the hypothesis that protect ion is mediated via inhibi t ion
of the JNK/SAPK pathway. Blood 1998;92:241–251.
763. Klein B, Zhang XG, Jourdan M, e t al . Paracr ine rather than autocrine regulat ion of
myeloma-cel l growth and d i f ferent ia t ion by inter leuk in-6. Blood 1989;73:517–526.
764. Frassani to MA, Cusmai A, Iodice G, et al . Autocr ine in ter leukin-6 product ion and h ighly
mal ignant mul t ip le myeloma: re la t ion wi th res is tance to drug- induced apoptos is . Blood
2001;97:483–489.
765. Klein B, Bata i l le R. Cytok ine network in human mult ip le myeloma. Hemato l Oncol Cl in
North Am 1992;6:273–284.
766. Klein B, Zhang XG, Lu ZY, e t a l . In ter leuk in-6 in human mult ip le myeloma. Blood
1995;85:863–872.
767. L ichtenste in A, Tu Y, Fady C, e t a l . In ter leuk in-6 inhib i ts apoptosis o f mal ignant
p lasma ce l ls. Cel l Immunol 1995;162:248–255.
768. Puth ier D, Batai l le R and Amiot M. IL-6 up-regulates mcl -1 in human myeloma ce l ls
through JAK/STAT rather than ras/MAP k inase pathway. Eur J Immunol 1999;29:3945–3950.
769. French JD, Tschumper RC, Jel inek DF. Dissect ion of the s ignal l ing requi rements of
in ter leukin-6-s t imulated myeloma ce l l growth. Acta Oncol 2000;39:777–781.
770. Cat le t t-Falcone R, Landowsk i TH, Oshi ro MM, et a l . Const i tu t ive act ivat ion of Stat3
s ignal ing confers res is tance to apoptosis in human U266 myeloma ce l ls . Immuni ty
1999;10:105–115.
771. Mi ts iades N, Mi ts iades CS, Poulaki V, e t a l . B iologic sequelae of nuc lear factor-kappaB
b lockade in mul t ip le myeloma: therapeut ic appl icat ions. Blood 2002; 99:4079–4086.
P.2433
772. Jourdan M, De Vos J , Mecht i N, e t a l . Regulat ion of Bc l -2- fami ly prote ins in myeloma
ce l ls by three myeloma surviva l factors : in ter leukin-6, in ter feron-a lpha and insu l in- l ike
growth fac tor 1 . Cel l Death Di f fer 2000;7:1244–1252.
773. Renner S, Weisz J , Kra jewski S, e t a l . Expression of BAX in plasma ce l l dyscras ias .
Cl in Cancer Res 2000;6:2371–2380.
774. Ladanyi M, W ang S, Niesvizky R, e t al . Proto-oncogene analys is in mult ip le myeloma.
Am J Pathol 1992;141:949–953.
775. Miguel -Garc ia A, Orero T, Matutes E, e t a l . bc l -2 express ion in p lasma cel ls f rom
neoplast ic gammopath ies and react ive p lasmacytos is : a comparat ive s tudy. Haematologica
1998;83:298–304.
776. Cheung W C, Van Ness B. The bone marrow s t romal microenvi ronment in f luences
myeloma therapeut ic response in v i t ro . Leukemia 2001;15:264–271.
777. Dalton W S, Jove R. Drug resistance in mul t ip le myeloma: approaches to c i rcumvent ion.
Semin Oncol 1999;26:23–27.
778. Rawat R, Rainey GJ, Thompson CD, et al . Const i tu t ive act ivat ion of STAT3 is
associated wi th the acquis i t ion of an in ter leukin 6- independent phenotype by murine
p lasmacytomas and hybridomas. Blood 2000;96:3514–3521.

779. Anderson K. Advances in the biology of mult ip le myeloma: therapeut ic appl icat ions.
Semin Oncol 1999;26:10–22.
780. Van Riet I , De Greef C, Aharch i F, e t al . Estab l ishment and character izat ion of a
human s t roma-dependent myeloma ce l l l ine (MM5.1) and i ts st roma-independent variant
(MM5.2) . Leukemia 1997;11:284–293.
781. L ichtenste in A, Berenson J , Norman D, e t a l . Product ion of cytokines by bone marrow
ce l ls obta ined f rom pat ients wi th mul t ip le myeloma. Blood 1989; 74:1266–1273.
782. Costes V, Por t ier M, Lu ZY, e t a l . In ter leukin-1 in mul t ip le myeloma: producer ce l ls and
the ir role in the contro l of IL-6 product ion. Br J Haematol 1998;103:1152–1160.
783. Lacy MQ, Donovan KA, Heimbach JK, et al . Compar ison of inter leuk in-1 beta
express ion by in s i tu hybr id izat ion in monoclonal gammopathy of undetermined s igni f icance
and mul t ip le myeloma. Blood 1999;93:300–305.
784. Ge NL and Rudikof f S. Insul in- l ike growth fac tor I is a dual e ffector of mul t ip le
myeloma ce l l growth. Blood 2000;96:2856–2861.
785. Asosingh K, Gunther t U, Bakkus MH, et a l . In v ivo induct ion of insul in- l ike growth
fac tor- I receptor and CD44v6 confers homing and adhes ion to mur ine mul t ip le myeloma
ce l ls. Cancer Res 2000;60:3096–3104.
786. Vanderkerken K, De Greef C, Asos ingh K, et a l . Select ive in i t ia l in v ivo homing pat tern
of 5T2 mult ip le myeloma cel ls in the C57BL/KalwRi j mouse. Br J Cancer 2000;82:953–959.
787. Je l inek DF, W itzig TE, Arendt BK. A ro le for insu l in- l ike growth fac tor in the regulat ion
of IL-6-respons ive human myeloma cel l l ine growth. J Immunol 1997;159:487–496.
788. Georg i i -Hemming P, W iklund HJ, L junggren O, e t al . Insu l in- l ike growth fac tor I is a
growth and surviva l fac tor in human mult ip le myeloma cel l l ines. Blood 1996;88:2250–2258.
789. Freund GG, Kulas DT, W ay BA, e t a l . Funct ional insu l in and insul in- l ike growth fac tor-1
receptors are preferent ial ly expressed in mul t ip le myeloma ce l l l ines as compared to B-
lymphoblasto id ce l l l ines. Cancer Res 1994; 54:3179–3185.
790. Hideshima T, Chauhan D, Schlossman R, e t a l . The role o f tumor necros is fac tor alpha
in the pathophys io logy of human mul t ip le myeloma: therapeut ic appl icat ions. Oncogene
2001;20:4519–4527.
791. Jourdan M, Tar te K, Legouffe E, e t a l . Tumor necros is fac tor is a surviva l and
pro l i ferat ion fac tor for human myeloma cel ls . Eur Cytok ine Netw 1999;10:65–70.
792. Kl ine M, Donovan K, W el l ik L , et al . Cytok ine and chemokine prof i les in mul t ip le
myeloma; s ign i f icance of s t romal in teract ion and corre lat ion of IL-8 product ion wi th d isease
progress ion. Leuk Res 2007;31:591–598.
793. Sezer O, Niemol ler K, Jakob C, e t a l . Relat ionship between bone marrow angiogenes is
and p lasma cel l in f i l t ra t ion and serum beta2-microglobul in leve ls in pat ients wi th mul t ip le
myeloma. Ann Hemato l . 2001;80:598–601.
794. Ng MH, Kan A, Chung YF, e t a l . Combined morphologica l and in terphase f luorescence
in s i tu hybridizat ion s tudy in mul t ip le myeloma of Chinese pat ients . Am J Pathol
1999;154:15–22.
795. Ner i A, Murphy JP, Cro L, e t a l . Ras oncogene mutat ion in mul t ip le myeloma. J Exp
Med 1989;170:1715–1725.
796. L iu P, Leong T, Quam L, et al . Act ivat ing mutat ions of N- and K-ras in mult ip le
myeloma show d i f ferent c l in ical associa t ions: analys is o f the Eastern Cooperat ive Oncology
Group Phase I I I t r ia l . Blood 1996;88:2699–2706.
797. Shou Y, Marte l l i ML, Gabrea A, e t a l . Diverse karyotyp ic abnormal i t ies o f the c-myc
locus assoc ia ted wi th c-myc dysregulat ion and tumor progress ion in mult ip le myeloma. Proc
Nat l Acad Sci U S A. 2000;97:228–233.
798. Lai R, Medei ros LJ, W i lson CS, e t a l . Expression of the ce l l -cycle-rela ted proteins E2F-
1, p53, mdm-2, p21waf-1, and Ki -67 in mul t ip le myeloma: corre la t ion wi th cyc l in-D1
immunoreact iv i ty. Mod Pathol 1998;11:642–647.
799. Ches i M, Bergsagel PL, Brents LA, et al . Dysregulat ion of cyc l in D1 by t rans locat ion
in to an IgH gamma swi tch region in two mult ip le myeloma cel l l ines. Blood 1996;88:674–681.
800. W eh HJ, Bart l R, Seeger D, e t al . Correla t ions between karyotype and cytolog ic
f indings in mul t ip le myeloma. Leukemia 1995;9:2119–2122.
801. Fonseca R, Hoyer JD, Aguayo P, e t a l . Cl in ica l s igni f icance of the t ranslocat ion
(11;14)(q13;q32) in mult ip le myeloma. Leuk Lymphoma 1999;35:599–605.
802. Hoyer JD, Hanson CA, Fonseca R, et al . The (11;14)(q13;q32) t ranslocat ion in mult ip le
myeloma. A morphologic and immunohis tochemica l s tudy. Am J Cl in Pathol 2000;113:831–
837.
803. Tr icot G, Bar log ie B, Jagannath S, e t a l . Poor prognos is in mul t ip le myeloma is
associated only wi th par t ia l or complete delet ions of chromosome 13 or abnormal i t ies
invo lv ing 11q and not wi th o ther karyotype abnormal i t ies. Blood 1995;86:4250–4256.
804. Bergsagel PL, Kuehl W M, Zhan F, e t a l . Cyc l in D dysregulat ion: an ear ly and un i fy ing
pathogenic event in mul t ip le myeloma. Blood 2005;106:296–303.
805. Tasaka T, Berenson J , Vescio R, e t a l . Analys is o f the p16INK4A, p15INK4B and
p18INK4C genes in mul t ip le myeloma. Br J Haemato l 1997;96:98–102.
806. Ogawa S, Hangaishi A, Miyawaki S, e t al . Loss of the cycl in-dependent k inase 4-
inhib i tor (p16; MTS1) gene is frequent in and h igh ly spec i f ic to lymphoid tumors in pr imary
human hematopoiet ic mal ignanc ies. Blood 1995;86: 1548–1556.
807. Zandecki M, Facon T, Preudhomme C, et al . The re t inoblastoma gene (RB-1) s ta tus in
mult ip le myeloma: a repor t on 35 cases. Leuk Lymphoma 1995; 18:497–503.
808. Urashima M, Teoh G, Ogata A, et al . Role of CDK4 and p16INK4A in in ter leukin-6-
mediated growth of mul t ip le myeloma. Leukemia 1997;11:1957–1963.
809. Gui l lerm G, Gyan E, W olowiec D, e t al . p16(INK4a) and p15( INK4b) gene methyla t ions
in plasma ce l ls f rom monoc lonal gammopathy of undetermined s ign i f icance. Blood
2001;98:244–246.
810. Ng MH, To KW , Lo KW , et a l . Frequent death-assoc ia ted protein k inase promoter
hypermethyla t ion in mul t ip le myeloma. Cl in Cancer Res 2001;7: 1724–1729.
811. McClure RF, Van Wier SA, Gre ipp PR, e t a l . Delet ion of the tumor suppressor gene
p16 in mul t ip le myeloma (MM) as determined by in terphase f luorescent in-s i tu hybrid izat ion
(FISH) and i ts rela t ion to methyla t ion of i ts promoter reg ion. Blood 2001;98:174b.
812. W inkler JM, Gonzalez-Paz N, McClure RF, et a l . Delet ion of the tumor suppressor gene
p16 in mul t ip le myeloma (MM) as determined by in terphase f luorescent in-s i tu hybrid izat ion
(FISH) and i ts rela t ion to methyla t ion of i ts promoter reg ion. Blood 2001;98:174b (abst r
4381).
813. Matozak i S, Nakagawa T, Nakao Y, e t a l . RAS gene mutat ions in mul t ip le myeloma and
re lated monoc lonal gammopathies . Kobe J Med Sc i 1991;37: 35–45.

814. Kalakonda N, Rothwel l DG, Scar f fe JH, e t al . Detect ion of N-Ras codon 61 mutat ions in
subpopulat ions of tumor ce l ls in mul t ip le myeloma at presentat ion. Blood 2001;98:1555–
1560.
815. Drach J , Ackermann J , Fr i tz E, et al . Presence of a p53 gene delet ion in pat ients wi th
mult ip le myeloma predic ts for shor t surviva l a f ter convent ional -dose chemotherapy. Blood
1998;92:802–809.
816. Corrad in i P, Inghi rami G, Asto l f i M, e t al . Inact ivat ion of tumor suppressor genes, p53
and Rb1, in p lasma cel l dyscrasias . Leukemia 1994;8:758–767.
817. Mazars GR, Por t ier M, Zhang XG, et a l . Mutat ions of the p53 gene in human myeloma
ce l l l ines. Oncogene 1992;7:1015–1018.
818. Ner i A, Baldini L , Trecca D, e t a l . p53 gene mutat ions in mul t ip le myeloma are
associated wi th advanced forms of mal ignancy. Blood 1993;81:128–135.
819. Preudhomme C, Facon T, Zandecki M, e t al . Rare occurrence of P53 gene mutat ions in
mult ip le myeloma. Br J Haematol 1992;81:440–443.
820. Selvanayagam P, Bl ick M, Narni F, e t a l . A l terat ion and abnormal express ion of the c-
myc oncogene in human mult ip le myeloma. Blood 1988;71:30–35.
821. Brown RD, Pope B, Luo XF, e t al . The oncoprotein phenotype of p lasma cel ls f rom
pat ients wi th mul t ip le myeloma. Leuk Lymphoma 1994;16:147–156.
822. Avet-Lo iseau H, Gerson F, Magrangeas F, et a l . Rearrangements of the c-myc
oncogene are present in 15% of pr imary human mul t ip le myeloma tumors. Blood
2001;98:3082–3086.
823. Kyle RA. Long-term survival in mult ip le myeloma. N Engl J Med 1983;308:314–316.
824. Gre ipp PR, Katzmann JA, O'Fal lon W M, et al . Value of beta 2-microglobul in leve l and
p lasma ce l l label ing indices as prognost ic fac tors in pat ients wi th newly d iagnosed myeloma.
Blood 1988;72:219–223.
825. Gre ipp PR, Lust JA, O'Fal lon W M, et a l . P lasma cel l label ing index and beta 2-
microglobul in pred ic t surviva l independent o f thymidine k inase and C-react ive prote in in
mult ip le myeloma. Blood 1993;81:3382–3387.
826. Gre ipp PR, Leong T, Bennett JM, e t a l . P lasmablast ic morphology—an independent
prognost ic fac tor wi th c l in ica l and laboratory corre la tes: Eastern Cooperat ive Oncology
Group (ECOG) Myeloma Tr ia l E9486 repor t by the ECOG Myeloma Laboratory Group. Blood
1998;91:2501–2507.
827. Rapoport BL, Falkson HC, Falkson G. Prognost ic fac tors a f fec t ing the surviva l o f
pat ients wi th mul t ip le myeloma. A ret rospect ive analysis o f 86 pat ients. S Afr Med J
1991;79:65–67.
828. Bata i l le R, Boccadoro M, Kle in B, e t al . C-react ive protein and beta-2 microg lobul in
produce a s imple and powerfu l myeloma s tag ing system. Blood 1992;80:733–737.
829. Konigsberg R, Zojer N, Ackermann J , e t a l . Predic t ive role o f in terphase cytogenet ics
for surviva l o f pat ients wi th mul t ip le myeloma. J Cl in Oncol 2000;18:804–812.
830. San Miguel JF, Garc ia-Sanz R, Gonzalez M, e t al . A new s taging system for mul t ip le
myeloma based on the number of S-phase p lasma ce l ls . B lood 1995;85:448–455.
831. Prognost ic features in the thi rd MRC myelomatosis t r ia l . Medical Research Counci l 's
Working Party on Leukaemia in Adul ts . Br J Cancer 1980;42:831–840.
832. Alexanian R, Balcerzak S, Bonnet JD, e t a l . Prognost ic fac tors in mult ip le myeloma.
Cancer 1975;36:1192–1201.

833. Bar t l R, Fr isch B, Fateh-Moghadam A, e t a l . His to log ic c lass i f icat ion and s taging of
mult ip le myeloma. A re t rospect ive and prospect ive s tudy of 674 cases. Am J Cl in Pathol
1987;87:342–355.
834. Bata i l le R, Cheval ier J , Ross i M, e t a l . Bone scin t igraphy in plasma-cel l myeloma. A
prospect ive s tudy of 70 pat ients . Radio logy 1982;145:801–804.
835. Ortega F, Gonzalez M, Moro MJ, e t a l . Prognost ic e ffec t of beta 2-microglobul in in
mult ip le myeloma. Med Cl in (Barc) 1992;99:645–648.
836. Cuzick J , De Stavola BL, Cooper EH, e t a l . Long- term prognost ic value of serum beta 2
microglobul in in myelomatos is . Br J Haemato l 1990;75: 506–510.
837. Bjorks t rand B, Goldstone AH, L jungman P, et a l . Prognost ic fac tors in auto logous stem
cel l t ransplantat ion for mul t ip le myeloma: an EBMT Regis try s tudy. European Group for
Bone Marrow Transplantat ion. Leuk Lymphoma 1994; 15:265–272.
P.2434
838. Rajkumar SV, Fonseca R, Lacy MQ, et al . Beta2-microg lobul in and bone marrow
p lasma ce l l invo lvement predic t complete responders among pat ients undergoing b lood ce l l
t ransplantat ion for myeloma. Bone Marrow Transplant 1999;23:1261–1266.
839. Majo l ino I , V ignet t i M, Melon i G, et al . Autologous t ransplantat ion in mult ip le myeloma:
a GITMO ret rospect ive analysis on 290 pat ients . Gruppo I tal iano Trapiant i d i Mido l lo Osseo.
Haematologica 1999;84:844–852.
840. Lemol i RM, Mart inel l i G, Zamagni E, e t a l . Engraftment, c l in ica l , and molecular fol low-
up of pat ients wi th mul t ip le myeloma who were re in fused wi th h igh ly puri f ied CD34 + ce l ls to
support s ingle or tandem high-dose chemotherapy. Blood 2000;95:2234–2239.
841. Tr icot G, Spencer T, Sawyer J , e t al . Predic t ing long- term (> or = 5 years) event- f ree
surviva l in mul t ip le myeloma pat ients fol lowing planned tandem autot ransplants. Br J
Haematol 2002;116:211–217.
842. Brown RD, Snowdon L, Uhr E, e t a l . C-react ive prote in (CRP) levels do not re f lect
d isease s tatus in pat ients wi th mult ip le myeloma. Leuk Lymphoma 1993;9:509–512.
843. Simonsson B, Brenning G, Kal lander C, e t al . Prognost ic va lue of serum lac t ic
dehydrogenase (S-LDH) in mult ip le myeloma. Eur J Cl in Invest 1987;17:336–339.
844. Barlogie B, Smal lwood L, Smith T, et al . High serum leve ls o f lact ic dehydrogenase
ident i fy a high-grade lymphoma-l ike myeloma. Ann Intern Med 1989;110:521–525.
845. Dimopoulos MA, Bar logie B, Smi th TL, et al . High serum lac tate dehydrogenase level
as a marker for drug res is tance and shor t survival in mul t ip le myeloma. Ann In tern Med
1991;115:931–935.
846. Cavo M, Baccarani M, Gobbi M, e t a l . Prognost ic value of bone marrow p lasma cel l
in f i l t ra t ion in s tage I mult ip le myeloma. Br J Haemato l 1983;55:683–690.
847. Rajkumar SV, Fonseca R, Dispenzier i A, e t a l . Methods for est imation of bone marrow
p lasma ce l l invo lvement in myeloma: pred ic t ive va lue for response and surviva l in pat ients
undergoing auto logous stem cel l t ransplantat ion. Am J Hemato l 2001;68:269–275.
848. Pasqualet t i P, Col lacciani A, Maccarone C, e t al . Prognost ic fac tors in mult ip le
myeloma: se lec t ion us ing Cox's propor t ional hazard model . B iomed Pharmacother
1996;50:29–35.
849. Bar t l R, Fr isch B. Cl in ica l s ign i f icance of bone marrow b iopsy and plasma cel l
morphology in MM and MGUS. Pathol Biol 1999;47:158–168.
850. Goasguen JE, Zandeck i M, Math io t C, e t a l . Mature p lasma cel ls as ind icator of bet ter
prognos is in mul t ip le myeloma. New methodology for the assessment o f p lasma cel l
morphology [see comments ]. Leuk Res 1999;23:1133–1140.
851. Rajkumar SV, Fonseca R, Lacy MQ, et al . Plasmablast ic morphology is an independent
predic tor o f poor surviva l a f ter auto logous s tem-cel l t ransplantat ion for mul t ip le myeloma. J
Cl in Oncol 1999;17:1551–1557.
852. Gr ignani G, Gobbi PG, Formisano R, e t a l . A prognost ic index for mul t ip le myeloma. Br
J Cancer 1996;73:1101–1107.
853. Carter A, Hocherman I , L inn S, e t a l . Prognost ic s ign i f icance of p lasma cel l
morphology in mul t ip le myeloma. Cancer 1987;60:1060–1065.
854. Paule B, Qui l lard J , Bisson M, e t al . Prognost ic s ign i f icance of p lasma cel l morphology
in mult ip le myeloma. Nouv Rev Fr Hemato l 1988;30:209–212.
855. Kurabayashi H, Kubota K, Shi rakura T, e t a l . Predic t ion of prognosis by e lec t ron
microscopic analys is o f myeloma ce l ls . Ann Hemato l 1996;73:169–173.
856. Rajkumar SV, Greipp PR. Prognost ic fac tors in mul t ip le myeloma. Hemato l Oncol Cl in
North Am 1999;13:1295–1314.
857. Boccadoro M, Marmont F, Tr iba l to M, e t al . Ear ly responder myeloma: k inet ic s tud ies
ident i fy a pat ient subgroup character ized by very poor prognosis . J Cl in Oncol 1989;7:119–
125.
858. Drach J , Gat t r inger C, Glassl H, e t al . The b io log ica l and cl in ica l s igni f icance of the KI-
67 growth f rac t ion in mult ip le myeloma. Hemato l Oncol 1992;10: 125–134.
859. Gi r ino M, Riccard i A, Luoni R, et al . Monoc lonal ant ibody Ki -67 as a marker o f
pro l i ferat ive act iv i ty in monoc lonal gammopath ies. Acta Haematol 1991;85:26–30.
860. Trendle MC, Leong T, Kyle RA, e t al . Prognost ic s ign i f icance of the S-phase f rac t ion of
l ight -chain-restr ic ted cytop lasmic immunoglobul in (cIg) pos i t ive plasma ce l ls in pat ients wi th
newly d iagnosed mul t ip le myeloma enrol led on Eastern Cooperat ive Oncology Group
t reatment tr ia l E9486. Am J Hemato l 1999;61:232–237.
861. Pope B, Brown R, Gibson J , e t al . The bone marrow p lasma cel l label ing index by f low
cytometry. Cytometry 1999;38:286–292.
862. W itzig TE, Dhodapkar MV, Kyle RA, et al . Quanti tat ion of c i rcu la t ing per iphera l b lood
p lasma ce l ls and the i r rela t ionship to disease act iv i ty in pat ients wi th mul t ip le myeloma.
Cancer 1993;72:108–113.
863. W itzig TE, Gertz MA, Lust JA, e t a l . Periphera l b lood monoc lonal plasma cel ls as a
predic tor o f surviva l in pat ients wi th mult ip le myeloma [see comments ] . Blood
1996;88:1780–1787.
864. Nadav L, Katz BZ, Baron S, et al . The generat ion and regulat ion of funct ional diversi ty
o f mal ignant p lasma ce l ls . Cancer Res 2006;66:8608–8616.
865. Yaccoby S. The phenotypic p last ic i ty of myeloma p lasma cel ls as expressed by
dedi f ferent ia t ion in to an immature, res i l ient , and apoptos is- res is tant phenotype. Cl in Cancer
Res 2005;11:7599–7606.
866. San Miguel JF, Gutierrez NC, Mateo G, e t a l . Convent ional diagnost ics in mul t ip le
myeloma. Eur J Cancer 2006;42:1510–1519.
867. Drach J , Anger ler J, Schuster J , e t a l . In terphase f luorescence in s i tu hybr id izat ion
ident i f ies chromosomal abnormal i t ies in plasma ce l ls f rom pat ients wi th monoc lonal
gammopathy of undetermined s igni f icance. Blood 1995;86:3915–3921.
868. Zandecki M, La i JL, Facon T. Mul t ip le myeloma: a lmost a l l pat ients are cytogenet ica l ly
abnormal . Br J Haemato l 1996;94:217–227.
869. Dewald GW , Kyle RA, Hicks GA, e t al . The cl in ica l s ign i f icance of cytogenet ic s tud ies
in 100 pat ients wi th mul t ip le myeloma, p lasma cel l leukemia, or amyloidosis . Blood
1985;66:380–390.
870. Sawyer JR, W aldron JA, Jagannath S, et al . Cytogenet ic f ind ings in 200 pat ients wi th
mult ip le myeloma. Cancer Genet Cytogenet 1995;82:41–49.
871. Smadja NV, Fruchar t C, Isnard F, et al . Chromosomal analys is in mul t ip le myeloma:
cytogenet ic evidence of two d i f ferent d iseases. Leukemia 1998; 12:960–969.
872. Rajkumar S, Fonseca R, Lacy M, e t a l . Abnormal cytogenet ics pred ic t poor surviva l
a f ter h igh-dose therapy and auto logous b lood cel l t ransplantat ion in mul t ip le myeloma. Bone
Marrow Transplant 1999;24:497–503.
873. Rajkumar SV, Fonseca R, Dewald GW , et al . Cytogenet ic abnormal i t ies corre la te wi th
the p lasma cel l label ing index and extent o f bone marrow invo lvement in myeloma. Cancer
Genet Cytogenet 1999;113:73–77.
874. Zojer N, Konigsberg R, Ackermann J , e t a l . Delet ion of 13q14 remains an independent
adverse prognost ic var iab le in mul t ip le myeloma despi te i ts f requent detect ion by in terphase
f luorescence in s i tu hybrid izat ion. Blood 2000;95:1925–1930.
875. Avet-Lo iseau H, L i JY, Mor ineau N, e t a l . Monosomy 13 is associa ted wi th the
t rans i t ion of monoc lonal gammopathy of undetermined s igni f icance to mul t ip le myeloma.
In tergroupe Francophone du Myelome. Blood 1999;94:2583–2589.
876. Fonseca R, Oken MM, Harr ington D, e t a l . Delet ions of chromosome 13 in mult ip le
myeloma ident i f ied by interphase FISH usual ly denote large delet ions of the q arm or
monosomy. Leukemia 2001;15:981–986.
877. Agnel l i L , Bicc ia to S, Mat t io l i M, e t al . Molecular c lass i f icat ion of mul t ip le myeloma: a
d ist inc t t ranscr ip t ional prof i le character izes pat ients expressing CCND1 and negat ive for
14q32 t rans locat ions. J Cl in Oncol 2005;23:7296–7306.
878. Bergsagel PL, Kuehl W M. Molecular pathogenesis and a consequent c lass i f icat ion of
mult ip le myeloma. J Cl in Oncol 2005;23:6333–6338.
879. Zhan F, Huang Y, Col la S, e t a l . The molecular c lass i f icat ion of mul t ip le myeloma.
Blood 2006;108:2020.
880. Fonseca R, Harr ington D, Blood E, et al . A molecular c lassi f icat ion of mul t ip le
myeloma (MM) based on cytogenet ic abnormal i t ies detected by interphase FISH, is powerfu l
in ident i fy ing d iscrete groups of pat ients wi th d iss imi lar prognos is . Blood 2001;98:733a.
881. Chng WJ, Santana-Davi la R, Van W ier SA, e t al . Prognost ic fac tors for hyperdip lo id-
myeloma: e ffec ts o f chromosome 13 de let ions and IgH t rans locat ions. Leukemia
2006;20:807–813.
882. Tr icot G, Sawyer JR, Jagannath S, e t a l . Unique ro le o f cytogenet ics in the prognos is
o f pat ients wi th myeloma receiv ing high-dose therapy and autot ransplants. J Cl in Oncol
1997;15:2659–2666.
883. Seong C, Delasal le K, Hayes K, e t al . Prognost ic value of cytogenet ics in mul t ip le
myeloma. Br J Haematol 1998;101:189–194.
884. Facon T, Avet-Lo iseau H, Gui l lerm G, e t a l . Chromosome 13 abnormal i t ies ident i f ied by
FISH analysis and serum beta2- microg lobul in produce a powerful myeloma s taging system
for pat ients rece iv ing high-dose therapy. Blood 2001;97:1566–1571.
885. W ore l N, Gre in ix H, Ackermann J, et al . Delet ion of chromosome 13q14 detected by
f luorescence in s i tu hybrid izat ion has prognost ic impact on surviva l a f ter h igh-dose therapy
in pat ients wi th mul t ip le myeloma. Ann Hemato l 2001;80:345–348.
886. Barlogie B, Alexanian R, Dixon D, e t a l . Prognost ic impl icat ions of tumor cel l DNA and
RNA content in mult ip le myeloma. Blood 1985;66:338–341.
887. Morgan RJ, J r , Gonchorof f NJ, Katzmann JA, e t a l . Detect ion of hypodiplo idy us ing
mult i -parameter f low cytometr ic analys is : a prognost ic ind icator in mul t ip le myeloma. Am J
Hemato l 1989;30:195–200.
888. Smadja NV, Bastard C, Brigaudeau C, e t a l . Hypodip loidy is a major prognost ic fac tor
in mult ip le myeloma. Blood 2001;98:2229–2238.
889. Gould J , Alexanian R, Goodacre A, e t a l . P lasma cel l karyotype in mul t ip le myeloma.
Blood 1988;71:453–-456.
890. Debes-Marun CS, Dewald GW , Bryant S, e t a l . Chromosome abnormal i t ies c lus ter ing
and i ts impl icat ions for pathogenesis and prognos is in myeloma. Leukemia 2003;17:427–436.
891. Shaughnessy J Jr , Tian E, Sawyer J , et al . Prognost ic impact o f cytogenet ic and
in terphase f luorescence in s i tu hybridizat ion-def ined chromosome 13 de let ion in mul t ip le
myeloma: ear ly resul ts of to ta l therapy I I . Br J Haemato l . 2003;120:44–52.
892. Fonseca R, Debes-Marun CS, Picken EB, e t a l . The recurrent IgH t rans locat ions are
h igh ly associa ted wi th nonhyperd ip loid var iant mul t ip le myeloma. Blood 2003;102:2562–
2567.
893. Ches i M, Kuehl W M, Bergsagel PL. Recurrent immunoglobul in gene t rans locat ions
ident i fy d is t inc t molecular subtypes of myeloma. Ann Oncol 2000; 11:131–135.
894. Fonseca R, Blood EA, Oken MM, et a l . Myeloma and the t(11;14)(Q13;Q32); evidence
for a b io log ical ly def ined un ique subset o f pat ients . Blood 2002;99:3735.
895. Shaughnessy J Jr , Gabrea A, Qi Y, e t al . Cyc l in D3 at 6p21 is dysregulated by
recurrent chromosomal translocat ions to immunoglobul in loc i in mul t ip le myeloma. Blood
2001;98:217–223.
896. Ches i M, Nardini E, Brents LA, et al . Frequent t rans locat ion t (4 ;14)(p16.3; q32.3) in
mult ip le myeloma is assoc ia ted wi th increased express ion and act ivat ing mutat ions of
f ibrob last growth fac tor receptor 3 . Nat Genet 1997;16:260–264.
897. Ches i M, Nardini E, L im RS, e t a l . The t (4;14) t ranslocat ion in myeloma dysregulates
both FGFR3 and a novel gene, MMSET, resu l t ing in IgH/MMSET hybr id t ranscr ip ts . Blood
1998;92:3025–3034.
898. Richelda R, Ronchet t i D, Bald in i L , et al . A novel chromosomal t rans locat ion t (4 ;
14)(p16.3; q32) in mul t ip le myeloma involves the f ibrob last growth- factor receptor 3 gene.
Blood 1997;90:4062–4070.
899. Avet-Lo iseau H, L i JY, Facon T, et al . High incidence of t rans locat ions
t (11;14)(q13;q32) and t (4 ;14)(p16;q32) in pat ients wi th plasma ce l l mal ignanc ies. Cancer
Res 1998;58:5640–5645.
900. Fonseca R, Conte G, Gre ipp PR. Laboratory correla tes in mul t ip le myeloma: how
usefu l for prognosis? Blood Rev 2001;15:97–102.

901. Fonseca R, Blood E, Rue M, e t a l . Cl in ical and biologic impl icat ions of recurrent
genomic aberrat ions in myeloma. Blood 2003;101:4569–4575.
P.2435
902. Hanamura I , Stewart JP, Huang Y, e t a l . Frequent ga in o f chromosome band 1q21 in
p lasma-cel l dyscras ias detected by f luorescence in s i tu hybridizat ion: inc idence increases
f rom MGUS to re lapsed myeloma and is re lated to prognosis and disease progression
fo l lowing tandem stem-cel l t ransplantat ion. Blood 2006;108:1724–1732.
903. L iang W , Hopper JE, Rowley JD. Karyotyp ic abnormal i t ies and cl in ical aspects of
pat ients wi th mul t ip le myeloma and rela ted paraproteinemic disorders. Cancer 1979;44:630–
644.
904. Garcia-Sanz R, Orfao A, Gonzalez M, e t a l . Pr imary p lasma cel l leukemia: c l in ical ,
immunophenotyp ic , DNA p loidy, and cytogenet ic character is t ics . Blood 1999;93:1032–1037.
905. Drach J , Schuster J, Nowotny H, et al . Mul t ip le myeloma: h igh incidence of
chromosomal aneuplo idy as detected by in terphase f luorescence in s i tu hybr id izat ion.
Cancer Res 1995;55:3854–3859.
906. Perez-Simon JA, Garc ia-Sanz R, Tabernero MD, et a l . Prognost ic value of numer ical
chromosome aberrat ions in mul t ip le myeloma: a FISH analysis o f 15 d i f ferent chromosomes.
Blood 1998;91:3366–3371.
907. Por t ier M, Moles JP, Mazars GR, et a l . p53 and RAS gene mutat ions in mul t ip le
myeloma. Oncogene 1992;7:2539–2543.
908. Avet-Lo iseau H, L i JY, Godon C, et al . P53 delet ion is not a frequent event in mul t ip le
myeloma. Br J Haematol 1999;106:717–719.
909. Arora T, Je l inek DF. Di f ferent ia l myeloma cel l respons iveness to in ter feron-a lpha
corre lates wi th di f ferent ia l induct ion of p19( INK4d) and cyc l in D2 expression. J Biol Chem
1998;273:11799–11805.
910. Lo YM, W ong IH, Zhang J, e t a l . Quant i ta t ive analysis o f aberrant p16 methyla t ion
us ing real - t ime quant i tat ive methyla t ion-spec i f ic po lymerase chain react ion. Cancer Res
1999;59:3899–3903.
911. Uchida T, Kinoshi ta T, Ohno T, e t a l . Hypermethyla t ion of p16INK4A gene promoter
dur ing the progression of p lasma cel l dyscras ia. Leukemia 2001;15:157–165.
912. Zhan F, Tian E, Bumm K, et al . Gene expression prof i l ing of human p lasma ce l l
d i f ferent ia t ion and class i f icat ion of mul t ip le myeloma based on simi lar i t ies to d is t inc t s tages
of la te-s tage B-ce l l development . Blood 2003;101:1128–1140.
913. Rajkumar SV, Leong T, Roche PC, e t a l . Prognost ic va lue of bone marrow
angiogenes is in mul t ip le myeloma. Cl in Cancer Res 2000;6:3111–3116.
914. San Miguel JF, Gonzalez M, Gascon A, e t a l . Lymphoid subsets and prognost ic fac tors
in mult ip le myeloma. Cooperat ive Group for the Study of Monoc lonal Gammopath ies. Br J
Haematol 1992;80:305–309.
915. Kay NE, Leong T, Bone N, e t a l . T-he lper phenotypes in the blood of myeloma pat ients
on ECOG phase I I I t r ia ls E9486/E3A93. Br J Haemato l 1998;100:459–463.
916. Kay NE, Leong TL, Bone N, e t a l . B lood levels o f immune ce l ls pred ict surviva l in
myeloma pat ients : resul ts o f an Eastern Cooperat ive Oncology Group phase 3 t r ia l for newly
d iagnosed mul t ip le myeloma pat ients . Blood 2001;98:23–28.

917. Porrata LF, Gertz MA, Inwards DJ, e t a l . Early lymphocyte recovery pred ic ts super ior
surviva l a f ter auto logous hematopoiet ic s tem ce l l t ransplantat ion in mul t ip le myeloma or
non-Hodgk in lymphoma. Blood 2001;98:579–585.
918. Saeed SM, Stock-Novack D, Pohlod R, e t a l . Prognost ic correlat ion of p lasma cel l acid
phosphatase and beta-g lucuronidase in mul t ip le myeloma: a Southwest Oncology Group
s tudy. Blood 1991;78:3281–3287.
919. Kyr tsonis MC, Dedouss is G, Zervas C, et al . Solub le in ter leukin-6 receptor (s IL-6R), a
new prognost ic fac tor in mult ip le myeloma. Br J Haematol 1996;93:398–400.
920. Mer l in i G, Perfe t t i V, Gobbi PG, e t a l . Acute phase prote ins and prognosis in mul t ip le
myeloma. Br J Haematol 1993;83:595–601.
921. Elomaa I , V i rkkunen P, Ris te l i L , e t a l . Serum concentrat ion of the cross- l inked
carboxyterminal te lopept ide of type I col lagen ( ICTP) is a useful prognost ic ind icator in
mult ip le myeloma. Br J Cancer 1992;66:337–341.
922. Fonseca R, Trendle MC, Leong T, et al . Prognost ic value of serum markers of bone
metabol ism in unt reated mult ip le myeloma pat ients . Br J Haemato l 2000;109:24–29.
923. W oitge HW , Pechers torfer M, Horn E, et al . Serum bone s ia loprote in as a marker o f
tumour burden and neoplast ic bone invo lvement and as a prognost ic fac tor in mul t ip le
myeloma. Br J Cancer 2001;84:344–351.
924. Arnal ich F, Zamorano AF, Mart inez-Hernandez P, et al . Addit ional pred ic t ive va lue of
serum unsaturated vi tamin B12 prote ins in mul t ip le myeloma. J Med 1990;21:277–286.
925. Kaiser U, Oldenburg M, Jaques G, e t a l . Solub le CD56 (NCAM): a new d i f ferent ia l -
d iagnost ic and prognost ic marker in mul t ip le myeloma. Ann Hematol 1996;73:121–126.
926. Math io t C, Mary JY, Tar tour E, e t al . Solub le CD16 (sCD16), a marker o f mal ignancy in
indiv iduals wi th monoclonal gammopathy of undetermined s ign i f icance (MGUS). Br J
Haematol 1996;95:660–665.
927. Seidel C, Sundan A, Hjorth M, e t al . Serum syndecan-1: a new independent prognost ic
marker in mul t ip le myeloma. Blood 2000;95:388–392.
928. Bata i l le R, Jourdan M, Zhang XG, et a l . Serum leve ls o f inter leuk in 6, a potent
myeloma ce l l growth factor , as a re f lec t o f d isease sever i ty in p lasma ce l l dyscrasias . J Cl in
Invest 1989;84:2008–2011.
929. Nachbaur DM, Herold M, Maneschg A, e t a l . Serum leve ls o f inter leukin-6 in mul t ip le
myeloma and other hemato logica l d isorders: corre la t ion wi th disease act iv i ty and other
prognost ic parameters. Ann Hemato l 1991;62:54–58.
930. Back H, Jagenburg R, Rodjer S, e t a l . Serum deoxythymid ine k inase: no he lp in the
d iagnos is and prognos is o f monoclonal gammopathy. Br J Haemato l 1993;84:746–748.
931. Brown RD, Joshua DE, Nelson M, e t a l . Serum thymid ine k inase as a prognost ic
indicator for pat ients wi th mul t ip le myeloma: resu l ts f rom the MRC (UK) V t r ia l . Br J
Haematol 1993;84:238–241.
932. Grogan TM, Spier CM, Salmon SE, et al . P-glycoprotein expression in human p lasma
ce l l myeloma: correla t ion wi th pr ior chemotherapy. Blood 1993; 81:490–495.
933. F i l ip i ts M, Drach J , Pohl G, e t a l . Expression of the lung resis tance protein predicts
poor outcome in pat ients wi th mul t ip le myeloma. Cl in Cancer Res 1999;5:2426–2430.
934. Palmer M, Belch A, Hanson J , e t a l . Reassessment of the re lat ionship between M-
protein decrement and surviva l in mul t ip le myeloma. Br J Cancer 1989;59:110–112.

935. Bald in i L , Radael l i F , Chiorbo l i O, et al . No corre lat ion between response and survival
in pat ients wi th mul t ip le myeloma t reated wi th v incr is t ine, melphalan, cyclophosphamide,
and prednisone. Cancer 1991;68:62–67.
936. Marmont F, Levis A, Falda M, e t a l . Lack of corre lat ion between object ive response
and death ra te in mul t ip le myeloma pat ients t reated wi th ora l melphalan and prednisone.
Ann Oncol 1991;2:191–195.
937. Pavlovsky S, Saslavsky J , Tezanos Pinto M, e t a l . A randomized t r ia l o f melphalan and
prednisone versus melphalan, prednisone, cyc lophosphamide, MeCCNU, and vincr is t ine in
unt reated mult ip le myeloma. J Cl in Oncol 1984;2:836–840.
938. Gahrton G, Tura S, L jungman P, et al . Prognost ic fac tors in a l logeneic bone marrow
t ransplantat ion for mul t ip le myeloma [see comments ] . J Cl in Oncol 1995;13:1312–1322.
939. Bjorks t rand B, Ljungman P, Bi rd JM, e t a l . Auto logous stem cel l t ransplantat ion in
mult ip le myeloma: resu l ts o f the European Group for Bone Marrow Transplantat ion. Stem
Cel ls 1995;2:140–146.
940. Lahuerta JJ , Mart inez-Lopez J , Serna JD, et a l . Remiss ion s ta tus def ined by
immunof ixat ion vs . e lect rophores is a fter auto logous transplantat ion has a major impact on
the outcome of mul t ip le myeloma pat ients . Br J Haematol 2000;109:438–446.
941. Davies FE, Forsyth PD, Rawstron AC, et al . The impact of at tain ing a min imal d isease
s ta te af ter h igh-dose melphalan and autologous t ransplantat ion for mult ip le myeloma. Br J
Haematol 2001;112:814–819.
942. Rawstron AC, Davies FE, DasGupta R, e t al . Flow cytometr ic d isease monitor ing in
mult ip le myeloma: the rela t ionship between normal and neoplast ic p lasma cel ls pred ic ts
outcome af ter t ransplantat ion. Blood 2002;100: 3095–3100.
943. Alexanian R, W eber D, Gi ral t S, e t a l . Impact o f complete remiss ion wi th in tens ive
therapy in pat ients wi th respons ive mul t ip le myeloma. Bone Marrow Transplant
2001;27:1037–1043.
944. Rajkumar SV, Fonseca R, Dispenzier i A, e t a l . Ef fec t o f complete response on outcome
fo l lowing autologous s tem cel l t ransplantat ion for myeloma. Bone Marrow Transplant
2000;26:979–983.
945. Dre icer R and Alexanian R. Nonsecretory mul t ip le myeloma. Am J Hemato l
1982;13:313–318.
946. Blade J , Kyle RA. Nonsecretory myeloma, immunoglobul in D myeloma, and plasma ce l l
leukemia. Hemato l Oncol Cl in North Am 1999;13:1259–1272.
947. Bourantas K. Nonsecretory mul t ip le myeloma. Eur J Haemato l 1996;56:109–111.
948. Cavo M, Gal ieni P, Gobbi M, e t al . Nonsecretory mul t ip le myeloma. Present ing f ind ings,
c l in ical course and prognosis. Acta Haemato l 1985;74:27–30.
949. Rubio-Fel ix D, Gi ra l t M, Gi ra ldo MP, e t a l . Nonsecretory mul t ip le myeloma. Cancer
1987;59:1847–1852.
950. Tormey W P. Low concentrat ion monoclonal and o l igoc lonal bands in serum and urine
us ing the Sebia Hydragel Prote in Elect rophoresis System [ le t ter ] . Cl in Chem Lab Med
1998;36:253–254.
951. Turesson I , Grubb A. Non-secretory or low-secretory myeloma wi th in t race l lu lar kappa
chains. Report o f s ix cases and review of the l i terature. Acta Med Scand 1978;204:445–451.
952. Blade J , Lust JA, Kyle RA. Immunoglobul in D mul t ip le myeloma: present ing features,
response to therapy, and survival in a ser ies of 53 cases. J Cl in Oncol 1994;12:2398–2404.

953. Shimamoto Y. IgD myeloma: c l in ica l character is t ics and a new s taging system based
on analys is of Japanese pat ients . Cancer Detect Prev 1995;19:426–435.
954. Jancelewicz Z, Takatsuki K, Sugai S, e t a l . IgD mult ip le myeloma. Review of 133 cases.
Arch In tern Med 1975;135:87–93.
955. F ibbe W E, Jansen J. Prognost ic factors in IgD myeloma: a s tudy of 21 cases. Scand J
Haematol 1984;33:471–475.
956. Blade J , Kyle RA. IgD monoc lonal gammopathy wi th long-term fol low-up. Br J Haemato l
1994;88:395–396.
957. Kairemo KJ, L indberg M, Prytz M. IgE myeloma: a case presentat ion and a review of
the l i terature. Scand J Cl in Lab Invest 1999;59:451–456.
958. Macro M, Andre I , Comby E, e t a l . IgE mul t ip le myeloma. Leuk Lymphoma
1999;32:597–603.
959. Kyle RA, Maldonado JE, Bayrd ED. Plasma ce l l leukemia. Report on 17 cases. Arch
In tern Med 1974;133:813–818.
960. Dimopoulos MA, Palumbo A, Delasal le KB, et a l . Pr imary p lasma cel l leukaemia. Br J
Haematol 1994;88:754–759.
961. Robi l lard N, Jego G, Pel la t -Deceunynck C, et a l . CD28, a marker assoc ia ted wi th
tumora l expansion in mul t ip le myeloma. Cl in Cancer Res 1998;4:1521–1526.
962. Avet-Lo iseau H, Andree-Ashley LE, Moore D 2nd, e t a l . Molecular cytogenet ic
abnormal i t ies in mul t ip le myeloma and p lasma cel l leukemia measured using comparat ive
genomic hybr id izat ion. Genes Chromosomes Cancer 1997;19: 124–133.
963. Gut ierrez NC, Hernandez JM, Garc ia JL, e t a l . Di f ferences in genet ic changes between
mult ip le myeloma and p lasma cel l leukemia demonstrated by comparat ive genomic
hybr idizat ion. Leukemia 2001;15:840–845.
964. Shimazak i C, Goto H, Arak i S, e t a l . Overexpress ion of PRAD1/cyc l in D1 in p lasma ce l l
leukemia wi th t (11;14)(q13;q32) . Int J Haemato l 1997;66: 111–115.
965. Pruzansk i W , Plat ts ME, Ogryzlo MA. Leukemic form of immunocyt ic dyscrasia (p lasma
ce l l leukemia) . A s tudy of ten cases and a review of the l i terature. Am J Med 1969;47:60–74.
P.2436
966. Noel P, Kyle RA. Plasma cel l leukemia: an evaluat ion of response to therapy. Am J
Med 1987;83:1062–1068.
967. Pasqualet t i P, Festucc ia V, Col lacc ian i A, et a l . P lasma cel l leukemia. A report on 11
pat ients and review of the l i terature. Panminerva Med 1996;38:179–184.
968. Ts iara S, Chaidos A, Kapsal i H, e t a l . Thal idomide admin is t ra t ion for the t reatment o f
res is tant p lasma cel l leukemia. Acta Haemato l 2003;109:153–155.
969. W ohrer S, Ackermann J , Baldia C, e t a l . Ef fec t ive t reatment of pr imary p lasma ce l l
leukemia wi th tha l idomide and dexamethasone—a case repor t . Hemato l J 2004;5:361–363.
970. Rajkumar SV, Dispenzier i A, Lacy MQ, et a l . Response rate and durabl i ty o f response
wi th thal idomide therapy for re lapsed mul t ip le myeloma (MM). Blood 2001:685abstr .
971. Espar is -Ogando A, Alegre A, Aguado B, e t al . Bortezomib is an eff ic ient agent in
p lasma ce l l leukemias. In t J Cancer 2005;114:665–667.
972. F innegan DP, Ket t le P, Drake M, e t a l . Bortezomib is e f fec t ive in pr imary plasma ce l l
leukemia. Leuk Lymphoma 2006;47:1670–1673.
973. Ataergin S, Arpaci F, Kaya A, et al . VAD combinat ion chemotherapy fo l lowed by
bor tezomib may be an effec t ive t reatment in secondary plasma ce l l leukemia. Am J Hematol
2006;81:987.
974. Panizo C, Ri fon J , Rodr iguez-W ilhe lmi P, et a l . Long- term surviva l in pr imary plasma
ce l l leukemia after therapy wi th VAD, autologous b lood s tem cel l t ransplantat ion and
in ter feron-alpha. Acta Haematol 1999;101:193–196.
975. Sica S, Chiusolo P, Salutar i P, e t a l . Long-las t ing complete remiss ion in p lasma ce l l
leukemia after aggress ive chemotherapy and CD34-se lected auto logous per iphera l b lood
progenitor cel l t ransplant : molecular fol low-up of minimal residual d isease. Bone Marrow
Transplant 1998;22:823–825.
976. Hovenga S, de W olf JT, Kl ip H, e t a l . Consol idat ion therapy wi th autologous stem cel l
t ransplantat ion in p lasma ce l l leukemia af ter VAD, h igh-dose cyc lophosphamide and EDAP
courses: a report o f three cases and a review of the l i terature. Bone Marrow Transplant
1997;20:901–904.
977. Yeh KH, Lin MT, Tang JL, e t a l . Long- term disease- f ree survival a f ter auto logous bone
marrow t ransplantat ion in a pr imary plasma ce l l leukaemia: detect ion of minimal residual
d isease in the t ransplant marrow by th i rd-complementar i ty-determining reg ion-spec i f ic
probes. Br J Haematol 1995;89: 914–916.
978. Yang CH, L in MT, Tsay W , et a l . Auto logous bone marrow t ransplantat ion for plasma
ce l l leukemia: report o f a case. Transplant Proc 1992;24:1531–1532.
979. Saccaro S, Fonseca R, Vei l lon DM, et a l . Pr imary p lasma cel l leukemia: repor t o f 17
new cases t reated wi th auto logous or a l logeneic s tem-cel l t ransplantat ion and review of the
l i terature. Am J Hematol 2005;78:288–294.
980. Sajeva MR, Greco MM, Cascavi l la N, e t a l . Ef fect ive auto logous periphera l b lood s tem
cel l t ransplantat ion in p lasma cel l leukemia fo l lowed by T- large granular lymphocyte
expans ion: a case report . Bone Marrow Transplant 1996;18:225–227.
981. Evison G, Evans KT. Sclerot ic bone depos i ts in mul t ip le myeloma [ let ter ] . Br J Radiol
1983;56:145.
982. Nakanish i T, Sobue I , Toyokura Y, e t a l . The Crow-Fukase syndrome: a s tudy of 102
cases in Japan. Neurology 1984;34:712–720.
983. Dr iedger H, Pruzanski W . Plasma cel l neoplas ia wi th per iphera l polyneuropathy. A
s tudy of f ive cases and a review of the l i terature. Medic ine 1980;59:301–310.
984. Bardwick PA, Zvai f ler NJ, Gi l l GN, et al . Plasma ce l l dyscras ia wi th po lyneuropathy,
organomegaly, endocrinopathy, M protein , and sk in changes: the POEMS syndrome. Report
on two cases and a review of the l i terature. Medic ine (Balt ) 1980;59:311–322.
985. Dispenzier i A, Kyle RA, Lacy MQ, et a l . POEMS syndrome: def in i t ions and long- term
outcome. Blood 2003;101:2496–2506.
986. Takatsuk i K, Sanada I . Plasma ce l l dyscrasia wi th po lyneuropathy and endocrine
d isorder : c l in ical and laboratory features of 109 repor ted cases. Jpn J Cl in Oncol
1983;13:543–555.
987. Soubr ier MJ, Dubost JJ , Sauvezie BJ. POEMS syndrome: a study of 25 cases and a
review of the l i terature. French Study Group on POEMS Syndrome. Am J Med 1994;97:543–
553.
988. Hashiguchi T, Ar imura K, Matsumuro K, et a l . Highly concentrated vascular endothel ia l
growth fac tor in pla te lets in Crow-Fukase syndrome. Musc le Nerve 2000;23:1051–1056.
989. W atanabe O, Ar imura K, Ki taj ima I , e t al . Great ly ra ised vascular endothel ia l growth
fac tor (VEGF) in POEMS syndrome [ le t ter ] . Lancet 1996;347:702.
990. Mor ley JB, Schwieger AC. The re la t ion between chronic polyneuropathy and
osteosclerot ic myeloma. J Neuro l Neurosurg Psychiatr 1967;30:432–442.
991. Davis L , Drachman D. Myeloma neuropathy. Arch Neurol 1972;27:507–511.
992. Phi l ips ED, el -Mahdi AM, Humphrey RL, e t al . The ef fec t o f the radia t ion t reatment on
the po lyneuropathy of mul t ip le myeloma. J Can Assoc Radio l 1972;23:103–106.
993. Iwashi ta H, Ohnish i A, Asada M, e t al . Po lyneuropathy, skin hyperpigmentat ion, edema,
and hyper t r ichos is in loca l ized osteosc lerot ic myeloma. Neuro logy 1977;27:675–681.
994. Dispenzier i A, Moreno-Aspita A, Suarez GA, e t al . Per iphera l b lood stem cel l
t ransplant (PBSCT) in s ixteen pat ients wi th POEMS syndrome, and a review of the l i terature.
Blood 2004:2004-2005–2046.
995. Abe M, Hiura K, W i lde J , et al . Osteoc lasts enhance myeloma ce l l growth and surviva l
v ia ce l l -cel l contact: a v ic ious cycle between bone destruc t ion and myeloma expans ion.
Blood 2004;104:2484–2491.
996. Stewart JP, Shaughnessy JD Jr . Role of os teoblast suppression in mul t ip le myeloma. J
Cel l Biochem. 2006;98:1–13.
997. Terpos E, Pol i tou M, Szydlo R, e t a l . Serum leve ls of macrophage in f lammatory
protein-1 alpha (MIP-1alpha) corre la te wi th the extent o f bone d isease and surviva l in
pat ients wi th mul t ip le myeloma. Br J Haematol 2003;123: 106–109.
998. Terpos E, Palermos J , Tsionos K, et al . Effec t of pamidronate adminis t rat ion on
markers of bone turnover and d isease act iv i ty in mult ip le myeloma. Eur J Haematol
2000;65:331–336.
999. Abi ldgaard N, Glerup H, Rungby J , e t a l . Biochemical markers of bone metabol ism
ref lec t os teoclast ic and osteoblast ic ac t iv i ty in mul t ip le myeloma. Eur J Haematol
2000;64:121–129.
1000. Iu l iano F, Abruzzese E, Mol ica S, e t a l . Samar ium(Sm)153 ethylene d iamine
te t ramethylene phosphonate (Sm-153-EDTMP) targeted radio therapy and zo ledronic ac id is
an ef fec t ive opt ion for elder ly wi th symptomatic re f rac tory mul t ip le myeloma. Blood
2003;102:446a–447a.
1001. Body JJ , Greipp P, Coleman RE, e t a l . A phase I s tudy of AMGN-0007, a recombinant
os teoprotegerin construct , in pat ients wi th mul t ip le myeloma or breast carc inoma rela ted
bone metastases. Cancer . 2003;97:887–892.
1002. Berenson JR, Lichtenstein A, Porter L , et al . Ef f icacy of pamidronate in reducing
ske leta l events in pat ients wi th advanced mult ip le myeloma. Myeloma Aredia Study Group.
N Engl J Med 1996;334:488–493.
1003. Berenson JR, Lichtenstein A, Porter L , et al . Long-term pamidronate t reatment o f
advanced mul t ip le myeloma pat ients reduces ske le ta l events . Myeloma Aredia Study Group.
J Cl in Oncol 1998;16:593–602.
1004. Berenson JR, Rosen LS, Howel l A, et al . Zo ledronic ac id reduces ske le tal - rela ted
events in pat ients wi th os teo lyt ic metastases. Cancer 2001;91: 1191–1200.
1005. Rosen LS, Gordon D, Antonio BS, e t a l . Zoledronic acid versus pamidronate in the
t reatment o f ske leta l metastases in pat ients wi th breast cancer or os teo lyt ic les ions of
mult ip le myeloma: a phase I I I , double-bl ind, comparat ive t r ia l . Cancer J 2001;7:377–387.

1006. Berenson JR, Hi l lner BE, Kyle RA, e t a l . Amer ican Soc iety of Cl in ica l Oncology
c l in ical pract ice gu ide l ines: the role o f bisphosphonates in mul t ip le myeloma. J Cl in Oncol
2002;20:3719–3736.
1007. Marx RE. Pamidronate (Aredia) and zo ledronate (Zometa) induced avascular necrosis
o f the jaws: a growing ep idemic . J Ora l Maxi l lo fac Surg 2003;61: 1115–1117.
1008. Carter GD, Goss AN. Bisphosphonates and avascular necrosis o f the jaws. Aust Dent
J . 2003;48:268.
1009. Lugassy G, Shaham R, Nemets A, et al . Severe osteomyel i t is o f the jaw in long- term
survivors of mul t ip le myeloma: a new c l in ica l ent i ty. Am J Med 2004;117:440–441.
1010. Mig l iorat i CA. Bisphosphanates and ora l cavi ty avascular bone necros is . J Cl in Oncol
2003;21:4253–4254.
1011. Tarassof f P, Csermak K. Avascular necrosis o f the jaws: r isk fac tors in metastat ic
cancer pat ients . J Oral Maxi l lo fac Surg 2003;61:1238–1239.
1012. Ruggiero SL, Mehrot ra B, Rosenberg TJ, e t a l . Osteonecrosis o f the jaws associa ted
wi th the use of bisphosphonates: a review of 63 cases. J Ora l Maxi l lo fac Surg 2004;62:527–
534.
1013. Bagan JV, Mur i l lo J , J imenez Y, e t al . Avascular jaw osteonecrosis in associa t ion wi th
cancer chemotherapy: ser ies of 10 cases. J Ora l Patho l Med 2005;34:120–123.
1014. Bamias A, Kastr i t is E, Bamia C, e t a l . Osteonecros is of the jaw in cancer af ter
t reatment wi th b isphosphonates: inc idence and r isk fac tors. J Cl in Oncol 2005;23:8580–
8587.
1015. Durie BG, Katz M, Crowley J . Osteonecrosis o f the jaw and b isphosphonates. N Engl
J Med 2005;353:99–102; d iscuss ion 199–102.
1016. Marx RE, Sawatar i Y, For t in M, e t al . Bisphosphonate- induced exposed bone
(osteonecrosis/os teopetros is) o f the jaws: r isk fac tors , recogni t ion, prevent ion, and
t reatment . J Oral Maxi l lo fac Surg 2005;63:1567–1575.
1017. Badros A, W eike l D, Salama A, e t a l . Osteonecros is of the jaw in mul t ip le myeloma
pat ients : c l in ica l features and r isk factors . J Cl in Oncol 2006;24:945–952.
1018. Kanat O, Ozet A, Arpaci F, et al . Bisphosphonate-assoc iated osteonecrosis o f the
jaws: Case repor ts and analysis o f 184 cases. J Cl in Oncol (Meet ing Abstr ) 2006;24:18595.
1019. Mig l iorat i CA, Casig l ia J, Epste in J , e t a l . Managing the care of pat ients wi th
b isphosphonate-associa ted osteonecrosis: an Amer ican Academy of Ora l Medic ine pos i t ion
paper. J Am Dent Assoc 2005;136:1658–1668.
1020. Lacy MQ, Dispenzier i A, Gertz MA, e t al . Mayo cl in ic consensus s tatement for the use
of bisphosphonates in mul t ip le myeloma. Mayo Cl in Proc 2006;81: 1047–1053.
1021. Mel ton LJ 3rd, Kyle RA, Achenbach SJ, e t a l . Fracture r isk wi th mult ip le myeloma: a
populat ion-based s tudy. J Bone Miner Res 2005;20:487–493.
1022. Mi re ls H. Metastat ic d isease in long bones. A proposed scoring system for d iagnos ing
impending patho log ic f rac tures Cl in Orthop 1989:256–264.
1023. McBroom RJ, Cheal EJ, Hayes W C. Strength reduct ions f rom metastat ic cor t ica l
defects in long bones. J Orthop Res 1988;6:369–378.
1024. Gainor BJ, Buchert P. Fracture heal ing in metastat ic bone disease. Cl in Orthop
1983:297–302.
1025. Al len KL, Johnson TW , Hibbs GG. Effec t ive bone pal l ia t ion as re la ted to var ious
t reatment reg imens. Cancer 1976;37:984–987.
1026. Tong D, Gi l l ick L , Hendrickson FR. The pal l ia t ion of symptomat ic osseous
metastases: f inal resul ts o f the s tudy by the Radiat ion Therapy Oncology Group. Cancer
1982;50:893–899.
1027. Levine SA, Per in LA, Hayes D, et al . An evidence-based evaluat ion of percutaneous
ver tebroplasty. Manag Care 2000;9:56–60, 63.
1028. Pf lugmacher R, Kandziora F, Schroeder RJ, e t a l . Percutaneous ba l loon kyphoplasty
in the t reatment o f pathologica l ver tebra l body f rac ture and deformi ty in mul t ip le myeloma: a
one-year fol low-up. Acta Radio l 2006;47:369–376.
1029. Benson W J, Scar f fe JH, Todd ID, e t al . Spina l -cord compression in myeloma. Br Med
J 1979;1:1541–1544.
1030. Gi lbert RW , Kim JH, Posner JB. Epidura l sp ina l cord compression from metastat ic
tumor: d iagnos is and t reatment . Ann Neuro l 1978;3:40–51.
1031. Young RF, Post EM, King GA. Treatment of spina l ep idura l metastases. Randomized
prospect ive compar ison of laminectomy and radio therapy. J Neurosurg 1980;53:741–748.
1032. Greenberg HS, Kim JH, Posner JB. Epidura l sp inal cord compress ion f rom metastat ic
tumor: resu l ts wi th a new t reatment protocol . Ann Neuro l 1980;8: 361–366.
P.2437
1033. Sorensen S, Helweg-Larsen S, Mour idsen H, e t a l . Ef fec t o f h igh-dose
dexamethasone in carcinomatous metastat ic spina l cord compression t reated wi th
rad io therapy: a randomised t r ia l . Eur J Cancer 1994;1:22–27.
1034. Vecht CJ, Haaxma-Reiche H, van Put ten WL, e t al . In i t ia l bolus of convent ional
versus high-dose dexamethasone in metastat ic sp ina l cord compression. Neurology
1989;39:1255–1257.
1035. Gucalp R, Ther iaul t R, Gi l l I , e t a l . Treatment o f cancer-assoc ia ted hyperca lcemia.
Double-bl ind comparison of rap id and s low in t ravenous in fusion reg imens of pamidronate
d isodium and sa l ine alone. Arch In tern Med 1994; 154:1935–1944.
1036. Mundy GR, W ilk inson R, Heath DA. Comparat ive s tudy of ava i lable medica l therapy
for hyperca lcemia of mal ignancy. Am J Med 1983;74:421–432.
1037. Warrel l RP, Jr, Is rae l R, Frisone M, e t a l . Gal l ium n i t ra te for acute t reatment o f
cancer-re la ted hyperca lcemia. A randomized, double-b l ind compar ison to ca lc i tonin . Ann
In tern Med 1988;108:669–674.
1038. Garton JP, Gertz MA, W itz ig TE, e t a l . Epoet in al fa for the t reatment o f the anemia of
mult ip le myeloma. A prospect ive, randomized, p lacebo-control led, double-b l ind t r ia l . Arch
In tern Med 1995;155:2069–2074.
1039. Dammacco F, Casto ldi G, Rodjer S. Ef f icacy of epoet in a l fa in the t reatment o f
anaemia of mult ip le myeloma. Br J Haematol 2001;113:172–179.
1040. Osterborg A, Boogaerts MA, Cimino R, e t al . Recombinant human erythropoiet in in
t ransfus ion-dependent anemic pat ients wi th mult ip le myeloma and non-Hodgkin 's
lymphoma—a randomized mul t icenter s tudy. The European Study Group of Erythropoiet in
(Epoet in Beta) Treatment in Mul t ip le Myeloma and Non-Hodgk in 's Lymphoma. Blood
1996;87:2675–2682.
1041. Cuzick J , Ersk ine S, Edelman D, e t a l . A compar ison of the incidence of the
myelodysplast ic syndrome and acute myeloid leukaemia fo l lowing melphalan and
cyc lophosphamide t reatment for myelomatosis. A repor t to the Medica l Research Counc i l 's
Working Party on Leukaemia in Adul ts . Br J Cancer 1987;55:523–529.
1042. Acute leukaemia and other secondary neoplasms in pat ients t reated wi th convent ional
chemotherapy for mult ip le myeloma: a Finnish Leukaemia Group s tudy. Eur J Haemato l
2000;65:123–127.
1043. Bergsagel DE. Chemotherapy of myeloma: drug combinat ions versus s ing le agents,
an overview, and comments on acute leukemia in myeloma. Hemato l Oncol 1988;6:159–166.
1044. West W O. Acute erythro id leukemia af ter cyc lophosphamide therapy for mul t ip le
myeloma: repor t o f two cases. South Med J 1976;69:1331–1332.
1045. Greene MH, Harr is EL, Gershenson DM, et a l . Melphalan may be a more potent
leukemogen than cyc lophosphamide. Ann Intern Med 1986;105:360–367.
1046. Cleary B, Binder RA, Kales AN, et al . Simultaneous presentat ion of acute
myelomonocyt ic leukemia and mult ip le myeloma. Cancer 1978;41:1381–1386.
1047. Rosner F and Grunwald H. Mul t ip le myeloma terminat ing in acute leukemia. Report o f
12 cases and review of the l i terature. Am J Med 1974;57:927–939.
1048. Govindara jan R, Jagannath S, F l ick JT, e t a l . Preceding s tandard therapy is the l ike ly
cause of MDS af ter autotransplants for mult ip le myeloma. Br J Haemato l 1996;95:349–353.
1049. W int robe M, Buel l M. Hyperprote inemia assoc iated wi th mul t ip le myeloma. Bul l Johns
Hopkins Hosp 1933;52:156.
1050. Siami GA, Siami FS. Plasmapheresis and paraproteinemia: c ryoprote in- induced
d iseases, monoclonal gammopathy, Waldenstrom's macroglobul inemia, hyperviscos i ty
syndrome, mul t ip le myeloma, l ight chain d isease, and amylo idos is . Ther Apher 1999;3:8–19.
1051. Smolens P, Venkatachalam M, Ste in JH. Myeloma k idney cast nephropathy in a ra t
model o f mul t ip le myeloma. Kidney Int 1983;24:192–204.
1052. Johnson WJ, Kyle RA, Pineda AA, e t al . Treatment o f renal fa i lure associated wi th
mult ip le myeloma. Plasmapheres is , hemodia lysis, and chemotherapy. Arch In tern Med
1990;150:863–869.
1053. Zucchel l i P, Pasqual i S, Cagnol i L , e t a l . Control led p lasma exchange t r ia l in acute
renal fai lure due to mul t ip le myeloma. Kidney In t 1988;33:1175–1180.
1054. Clark AD, Shet ty A, Soutar R. Renal fa i lure and mult ip le myeloma: pathogenes is and
t reatment o f renal fa i lure and management o f under ly ing myeloma. Blood Rev 1999;13:79–
90.
1055. Jacobson DR, Zol la-Pazner S. Immunosuppress ion and in fec t ion in mul t ip le myeloma.
Semin Oncol 1986;13:282–290.
1056. Paradis i F, Cor t i G, Cine l l i R. In fect ions in mult ip le myeloma. In fec t Dis Cl in North Am
2001;15:373–384.
1057. Meyers BR, Hi rschman SZ, Axel rod JA. Current patterns of in fec t ion in mul t ip le
myeloma. Am J Med 1972;52:87–92.
1058. Shaikh BS, Lombard RM, Appelbaum PC, et a l . Changing pat terns of infect ions in
pat ients wi th mul t ip le myeloma. Oncology 1982;39:78–82.
1059. Doughney KB, W il l iams DM, Penn RL. Mul t ip le myeloma: in fec t ious compl icat ions.
South Med J 1988;81:855–858.
1060. Rayner HC, Haynes AP, Thompson JR, et al . Perspect ives in mul t ip le myeloma:
surviva l , prognost ic fac tors and d isease compl icat ions in a s ing le centre between 1975 and
1988. Q J Med 1991;79:517–525.

1061. Lazarus HM, Lederman M, Lubin A, e t a l . Pneumococcal vaccinat ion: the response of
pat ients wi th mul t ip le myeloma. Am J Med 1980;69:419–423.
1062. Landesman SH, Schif fman G. Assessment o f the ant ibody response to pneumococcal
vaccine in h igh-r isk populat ions. Rev In fec t Dis 1981; 3(suppl ):S184–S197.
1063. But ler JC, Breiman RF, Campbel l JF, e t a l . Pneumococcal polysaccharide vacc ine
ef f icacy. An evaluat ion of current recommendations. JAMA 1993;270: 1826–1831.
1064. Chapel HM, Lee M, Hargreaves R, e t al . Randomised t r ia l o f in t ravenous
immunoglobul in as prophylaxis against in fec t ion in p la teau-phase mul t ip le myeloma. The UK
Group for Immunoglobul in Replacement Therapy in Mul t ip le Myeloma. Lancet
1994;343:1059–1063.
1065. Oken MM, Pomeroy C, W eisdor f D, e t a l . Prophylact ic ant ibio t ics for the prevent ion of
ear ly in fec t ion in mul t ip le myeloma. Am J Med 1996;100:624–628.
1066. Garc ia-Sanz R, Montoto S, Torrequebrada A, e t a l . Waldenstrom macroglobul inaemia:
present ing features and outcome in a ser ies wi th 217 cases. Br J Haemato l 2001;115:575–
582.
1067. Hei lman RL, Velosa JA, Hol ley KE, e t a l . Long- term fol low-up and response to
chemotherapy in pat ients wi th l ight - chain depos i t ion d isease. Am J Kidney Dis 1992;20:34–
41.
1068. Conkl in R, Alexanian R. Cl in ica l c lass i f icat ion of plasma ce l l myeloma. Arch Intern
Med 1975;135:139–143.
1069. Knowl ing MA, Harwood AR, Bergsagel DE. Compar ison of ext ramedul lary
p lasmacytomas wi th sol i tary and mul t ip le plasma ce l l tumors of bone. J Cl in Oncol
1983;1:255–262.
1070. Dimopoulos MA, Moulopoulos LA, Maniat is A, e t a l . Sol i tary p lasmacytoma of bone
and asymptomat ic mult ip le myeloma. Blood 2000;96:2037–2044.
1071. Woodruf f RK, Malpas JS, W hite FE. Sol i tary p lasmacytoma. I I : Sol i tary p lasmacytoma
of bone. Cancer 1979;43:2344–2347.
1072. Ozsahin M, Tsang RW , Poortmans P, e t a l . Outcomes and patterns of fa i lure in
so l i tary p lasmacytoma: a mul t icenter Rare Cancer Network s tudy of 258 pat ients . In t J
Radiat Oncol Biol Phys 2006;64:210–217.
1073. Bata i l le R, Sany J. Sol i tary myeloma: c l in ica l and prognost ic features of a review of
114 cases. Cancer 1981;48:845–851.
1074. Mi l l W B, And Gr i f f i th R. The ro le of rad ia t ion therapy in the management o f p lasma
ce l l tumors. Cancer 1980;45:647–652.
1075. Liebross RH, Ha CS, Cox JD, e t a l . Sol i tary bone plasmacytoma: outcome and
prognost ic fac tors fol lowing radio therapy. In t J Radiat Oncol Bio l Phys 1998;41:1063–1067.
1076. Ding l i D, Kyle RA, Rajkumar SV, e t a l . Immunoglobul in f ree l ight chains and sol i tary
p lasmacytoma of bone. Blood 2006;108:1979–1983.
1077. Bolek TW , Marcus RB, Mendenhal l NP. Sol i tary p lasmacytoma of bone and sof t t issue.
In t J Radiat Oncol Biol Phys 1996;36:329–333.
1078. Dimopoulos MA, Kiamouris C, Moulopoulos LA. Sol i tary plasmacytoma of bone and
ext ramedul lary p lasmacytoma. Hemato l Oncol Cl in North Am 1999;13:1249–1257.
1079. Gal ieni P, Cavo M, Pulsoni A, e t a l . Cl in ica l outcome of ext ramedul lary p lasmacytoma.
Haematologica 2000;85:47–51.
1080. Hussong JW , Perkins SL, Schnitzer B, e t a l . Ext ramedul lary p lasmacytoma. A form of
margina l zone cel l lymphoma? Am J Cl in Pathol 1999;111:111–116.
1081. Mayr NA, W en BC, Hussey DH, e t al . The ro le of radia t ion therapy in the t reatment of
so l i tary p lasmacytomas. Radiother Oncol 1990;17:293–303.
1082. Brinch L, Hannisdal E, Abrahamsen AF, e t a l . Ext ramedul lary plasmacytomas and
so l i tary p lasma cel l tumours of bone. Eur J Haemato l 1990;44: 132–135.
1083. Shih LY, Dunn P, Leung W M, et a l . Local ised plasmacytomas in Taiwan: compar ison
between ext ramedul lary p lasmacytoma and so l i tary p lasmacytoma of bone. Br J Cancer
1995;71:128–133.
1084. Woodruf f RK, Whi t t le JM, Malpas JS. Sol i tary p lasmacytoma. I : Ext ramedul lary soft
t issue plasmacytoma. Cancer 1979;43:2340–2343.
1085. Corwin J , L indberg RD. Sol i tary plasmacytoma of bone vs. ext ramedul lary
p lasmacytoma and the ir re lat ionship to mul t ip le myeloma. Cancer 1979;43: 1007–1013.
1086. Hol land J , Trenkner DA, Wasserman TH, et a l . P lasmacytoma. Treatment resul ts and
convers ion to myeloma. Cancer 1992;69:1513–1517.
1087. Cavagnaro F, Le in JM, Pavlovsky S, e t a l . Compar ison of two combinat ion
chemotherapy reg imens for mult ip le myeloma: methyl -CCNU, cyc lophosphamide, and
prednisone versus melphalan and prednisone. Cancer Treat Rep 1980;64:73–79.
1088. Riccardi A, Mer l in i G, Montecucco C, e t a l . Pept ichemio, v incr is t ine and prednisone
versus melphalan and prednisone as induct ion therapy in mult ip le myeloma. Eur J Cancer
Cl in Oncol 1986;22:787–791.
1089. Klueppelberg U, Shapi ra I , Smi th E, e t a l . Treatment o f newly d iagnosed, inner-c i ty
mult ip le myeloma pat ients wi th low-dose tha l idomide in combinat ion wi th dexamethasone
and zoledronate: a phase I I t r ia l . Blood 2005;11:5180.
1090. Dimopoulos MA, Anagnostopoulos A, Terpos E, e t a l . Pr imary t reatment wi th pu lsed
melphalan, dexamethasone and thal idomide for elder ly symptomat ic pat ients wi th mul t ip le
myeloma. Haemato logica 2006;91:252–254.
1091. Jagannath S, Dur ie BG, Wol f J , e t a l . Bor tezomib therapy a lone and in combinat ion
wi th dexamethasone for previously unt reated symptomat ic mult ip le myeloma. Session type:
ora l sess ion. Br J Haemato l 2005;129:776–783.
1092. Barlog ie B, Tr icot G, Rasmussen E, e t a l . Tota l therapy 2 wi thout tha l idomide in
comparison wi th to ta l therapy 1: role o f in tens i f ied induct ion and post t ransplantat ion
consol idat ion therapies. Blood 2006;107:2633–2638.
1093. Fermand JP, Maro l leau JP, Alber t i C, et al . In s ing le versus tandem high dose
therapy (HDT) supported wi th auto logous b lood stem cel l (ABSC) t ransplantat ion us ing
unselected or CD34 enr iched ABSC: prel iminary resul ts of a two by two des igned
randomized tr ia l in 230 young pat ients wi th mul t ip le myeloma (MM). Blood 2001;98:815a
(abst r 3387).
1094. Champl in R, Khour i I , Kornblau S, e t a l . A l logeneic hematopoiet ic transplantat ion as
adopt ive immunotherapy. Induct ion of graf t -versus-mal ignancy as pr imary therapy. Hemato l
Oncol Cl in North Am 1999;13:1041–1057.
1095. Geru l l S, Goerner M, Benner A, e t a l . Long- term outcome of nonmyeloablat ive
a l logeneic t ransplantat ion in pat ients wi th high-r isk mul t ip le myeloma. Bone Marrow
Transplant 2005;36:963–969.

1096. Perez-Simon JA, Sureda A, Fernandez-Avi les F, e t a l . Reduced-in tensi ty condi t ioning
a l logeneic t ransplantat ion is associa ted wi th a h igh incidence of ext ramedul lary relapses in
mult ip le myeloma pat ients . Leukemia 2006;20:542–545.
1097. Shimazaki C, Fu j i i H, Yoshida T, e t al . Reduced- in tensi ty condi t ioning al logeneic s tem
cel l t ransplantat ion for mul t ip le myeloma: resu l ts f rom the Japan Myeloma Study Group. In t
J Hemato l 2005;81:342–348.
1098. Gal imbert i S, Benedett i E, Morabi to F, e t a l . Prognost ic role o f min imal residual
d isease in mul t ip le myeloma pat ients a fter non-myeloablat ive al logeneic t ransplantat ion.
Leuk Res 2005;29:961–966.
P.2438
1099. Tr ieu Y, Trudel S, Pond GR, et a l . W eekly cyc lophosphamide and al ternate-day
prednisone: an ef fec t ive, convenient, and wel l - to lerated ora l t reatment for re lapsed mul t ip le
myeloma af ter autologous stem cel l t ransplantat ion. Mayo Cl in Proc 2005;80:1578–1582.
1100. Combinat ion chemotherapy MOCCA in res is tant and re laps ing mult ip le myeloma.
F innish Leukaemia Group. Eur J Haemato l 1992;48:37–40.
1101. Palumbo A, Fa lco P, Ambros ini MT, e t a l . Thal idomide p lus dexamethasone is an
ef fec t ive sa lvage reg imen for myeloma pat ients re lapsing af ter autologous t ransplant. Eur J
Haematol 2005;75:391–395.
1102. Kropf f MH, Bisp ing G, W enning D, et al . Bor tezomib in combinat ion wi th
dexamethasone for re lapsed mul t ip le myeloma. Leuk Res 2005;29:587–590.
1103. Musto P, Fa lcone A, Sanpaolo G, e t a l . Bor tezomib (Velcade) for progressive
myeloma af ter autologous stem cel l t ransplantat ion and thal idomide. Leuk Res
2006;30:283–285.
1104. Chanan-Khan A, Mi l ler KC. Velcade, doxi l and tha l idomide (VDT) is an ef fec t ive
sa lvage regimen for pat ients wi th relapsed and ref rac tory mul t ip le myeloma. Leuk
Lymphoma 2005;46:1103–1104.
1105. Jakubowiak AJ, Bracket t L , Kendal l T, e t a l . Combinat ion therapy with ve lcade, doxi l ,
and dexamethasone (VDD) for pat ients wi th relapsed/ref ractory mult ip le myeloma (MM).
ASH Annual Meet ing Abstr 2005;106:5179.
1106. Kropf f M, Bisping G, L ieb isch P, e t a l . Bor tezomib in combinat ion wi th h igh-dose
dexamethasone and cont inuous low-dose oral cyclophosphamide for re lapsed mul t ip le
myeloma. ASH Annual Meet ing Abstr 2005; 106:2549.
1107. Durie BG, Salmon SE, Moon TE. Pret reatment tumor mass, ce l l k inet ics , and
prognos is in mul t ip le myeloma. Blood 1980;55:364–372.
1108. Fassas AB, Spencer T, Sawyer J , e t al . Both hypodip loidy and delet ion of
chromosome 13 independently confer poor prognos is in mul t ip le myeloma. Br J Haemato l
2002;118:1041–1047.
1109. Chiecchio L, Protheroe RK, Ibrahim AH, et a l . Delet ion of chromosome 13 detected by
convent ional cytogenet ics is a cr i t ical prognost ic fac tor in myeloma. Leukemia
2006;20:1610–1617.
1110. Osserman EF, DiRe LB, DiRe J , e t a l . Ident ical twin marrow t ransplantat ion in
mult ip le myeloma. Acta Haematol 1982;68:215–223.