clinical handover - bcpft.nhs.uk
TRANSCRIPT

Version 2.0 August 2016
Clinical Handover
Target Audience
Who Should Read This Policy
All staff responsible for Clinical Handover

Clinical Handover Policy
Version 2.0 August 2016
2
Ref. Contents Page
1.0 Introduction 4
2.0 Purpose 4
3.0 Objectives 4
4.0 Clinical Handover Process 4
4.1 Standard of Handover 5
5.0 Procedures connected to this Policy 8
6.0 Links to Relevant Legislation 8
6.1 Links to Relevant National Standards 9
6.2 Links to other Key Policies 10
6.3 References 11
7.0 Roles and Responsibilities for this Policy 12
8.0 Training 13
9.0 Equality Impact Assessment 13
10.0 Data Protection and Freedom of Information 14
11.0 Monitoring this Policy is Working in Practice 14
Appendices
1.0 Example of a Patient Information Handover Sheet 15

Clinical Handover Policy
Version 2.0 August 2016
3
Explanation of terms used in this policy Clinical Handover - A semi-structured exchange of information and awareness of the clinically
relevant issues including the transfer of key issues, tasks and changes in management plan from one care professional/ care team to another. The handover process can take place in different ways
and at different times during the day, not just in scheduled meetings
Patient - The term is used to describe any person who uses services managed by the Black Country
Partnership NHS Foundation Trust
Shift – Recurring periods in which different groups of workers do the same jobs in relay
Risks - Information which may identify that a patient’s condition may change or need review in the
period of the shift
Clinician - A health professional with responsibility for patient care
Key Tasks - Important actions which must be undertaken within the period of responsibility for care
Situation, Background, Assessment and Recommendation (SBAR) – A structured method for communicating critical information that requires immediate attention and action contributing to
effective escalation and increased patient safety
Out-of-hours - The out of hours is the time period between 17:00 hours to 09:00 hours Monday to Friday and for the entire duration of weekends and bank holidays

Clinical Handover Policy
Version 2.0 August 2016
4
1.0 Introduction Handover is described as ‘The transfer of professional responsibility and accountability for some or all aspects of care for a patient, or group of patients, to another person or professional group on a temporary or permanent basis’ (National Patient Safety Agency). The fundamental intention of any handover is to achieve the efficient transfer of high quality clinical information at times of transition of responsibility for patients’ care. Shift work relies on effective continuity of information transfer which underpins all aspects of seamless continuity of care. The standardisation of handover contents and processes can improve patient safety by ensuring consistency in the exchange of information critical to safe and effective care. This can lead to increased service satisfaction for the patient as every member of staff working with a patient can begin where the last left off, aiding the recovery process. Handover of care is one of the most important procedures in healthcare, if carried out improperly it can be a major contributory factor to subsequent error and harm to patients. Lapses in information during handover can lead to mistakes being made, including delayed decisions relating to care, repeated investigations, incorrect diagnoses and incorrect treatment. How the information is transmitted and recorded in the handover process has a major impact on the way it is retained and therefore acted on subsequently. The importance of handover processes and recording is escalating with the requirement for shorter hours for doctors and an increase in shift patterns of working. Black Country Partnership NHS Foundation Trust recognises this and aims to ensure that the risks involved in the process of transferring clinical responsibility are minimised.
Trust staff deliver care in a variety of settings, shift patterns and clinical specialties and the complexity of the provision of care puts extra emphasis on the quality of information shared when one team or clinician hands over responsibility of care to the next. The information contained within this document contains the minimum standard expected within the scope of the policy.
2.0 Purpose The aim of this policy is to provide direction and guidance for staff on the delivery of a safe and robust handover that preserves confidentiality and ensures that all important information is conveyed relevant to the optimum care of all patients. 3.0 Objectives The principle objectives of this policy are to:
Ensure that all services have robust arrangements to ensure effective handover of patient clinical information
Ensure clinical handover is effective, timely and factual to maximise patient safety across the organisation
Ensure all relevant information is transferred at clinical handovers Ensure all verbal clinical handovers are evidenced with written information
4.0 Clinical Handover Process Handover must include clinically relevant information including the transfer of key issues and concerns, tasks to be completed and changes to management plans.

Clinical Handover Policy
Version 2.0 August 2016
5
To ensure that safe appropriate clinical handover of patient care occurs and their care continues with minimal interruption and risks:
Shifts need to be coordinated
Adequate time must be allowed in rotas for members of the team to meet, share information, and clarify responsibility for ongoing care and outstanding tasks
Handover should have clear leadership
4.1 Standard of Handover 4.1.1 Who is Required to Attend Handover? There should be an understanding of who is required to attend handover. Senior input is essential if handover is to be effective and all grades of staff should ideally be involved. Professionals may require their own meetings but all should be engaged in the clinical handover regardless of profession. Multidisciplinary handover is to be encouraged when practical; however, the information requirements for medical, nursing and other allied health professionals may be different and this should be respected; it may be appropriate to have different arrangements for different staff groups. Clinical handover should include the relevant group of patients receiving direct care. The nurse in charge of the incoming shift must receive handover for all patients in their sphere of responsibility during the duration of the shift. 4.1.2 Handover Leadership There should be clear identification of who is leading the handover. This may be the most senior person of the incoming shift or the designated nurse-in-charge for the shift. Tasks should be appropriately delegated, in terms of allocating tasks to those with the skills to undertake them most effectively in the patient’s best interests, and to ensure the best use of the available team member’s time with consideration given to overall workload and other demands on the team. There should be clarity as to who is responsible for ensuring key tasks are completed and how this is co-ordinated. For nursing teams this may require reporting back to the nurse-in-charge during the shift. 4.1.3 Designated Time for Handover Handover should occur:
At the change of shift
When transfer of care from one team to another team
At patient’s transfer to another hospital
On a patient’s discharge
When a patient’s presentation and needs change Start time of the handover should be as soon as the incoming staff come into the work area, in order to ensure that all staff are fully briefed on care received and care required, to allow for continued safe and effective care delivery. Time should be factored in to working patterns to allow sufficient time for effective handover between incoming and outgoing workers. Shift end times must be noted and recorded and all reasonable attempts made to ensure staff are able to leave on time having fulfilled their obligation at handover. Steps should be taken to protect handover time as far as possible and while immediate engagement with clinical matters may on occasion be necessary it is important to maintain the essential nature of effective handover. Unnecessary interruptions should be avoided where possible.

Clinical Handover Policy
Version 2.0 August 2016
6
4.1.4 Handover Structure There should be an effective structure for what and how the information at handover is communicated, recorded and retained. When conducting the clinical handover all clinicians are expected to read from the patients’ care record to promote communication of factual, timely and comprehensive information relevant to a patient’s care. No jargon or acronyms may be used in the clinical handover process. All information must be transferred both verbally and in written format. Staff teams receiving handover should use a standardised handover sheet/ book (within their team) to document key information and clinical risks that are relevant to patient care. It is important that each area has a mechanism of recording that handover has occurred and that the agreed items are being handed over effectively between incoming and outgoing shifts. A record should be maintained of all patients discussed at handover and a list of who attended. Due to the patient specific information contained on handover sheets/ book it is vital that confidentiality is maintained and therefore the sheets/ book must be filed away in a secure place. Where possible handover should take place in an appropriate private place where the details cannot be overheard by any unauthorised person in order to maintain patient confidentiality, as well as dignity and respect. 4.1.4.1 SBAR Communication Tool ‘Situation, Background, Assessment and Recommendation’ (SBAR) tool is an example of a communication tool that can be used for handover (see Appendix 1). SBAR is especially useful to support handover during patient transfers between settings. SBAR can be used very effectively to escalate a clinical problem that requires immediate attention, or to facilitate efficient handover of information relevant to patient care between clinicians or other teams. The written documentation should be recorded using permanent ink and be readable when photocopied or scanned. It should be written clearly, legibly and in such a manner that they cannot be erased. It should also be accurately dated, timed and signed. If a handover book is used the SBAR format can still be utilised to record information. The example found in Appendix 1 can be adapted to suit different services. Please see 4.1.5 for examples of information to be exchanged which could be used as headings on the SBAR. 4.1.4.2 Safe Wards SBAR communication tool can be adapted to include positive words and bad news mitigation. This information can also be added to other handover sheets/ books. 4.1.4.2.1 Positive Words When giving handover staff should say something positive about what each patient has been doing during the shift, or draw attention to some positive quality they have,

Clinical Handover Policy
Version 2.0 August 2016
7
or if this is not possible something positive about the way in which staff supported the patient (positive appreciation). In addition, if any difficult or disruptive behaviour is reported, a possible psychological understanding of the patient's behaviour must be offered. For further information see Safewards – Positive Words. 4.1.4.2.2 Bad News Mitigation Be aware of occasions and events that might generate angry or upset reactions. In each handover discuss as a team the issue of bad news and share knowledge about patients in order to predict who might receive unwelcome news and how support is going to be offered. Either work with the multidisciplinary team in the ward round to express the bad news sympathetically, or intercept the patient after it has happened. For further information see Safewards – Bad News Mitigation. 4.1.5 Sufficient and Relevant Information Sufficient and relevant information should be exchanged to ensure patient safety and effective clinical care. This policy cannot be prescriptive about the specific issues to be handed over in each area so each division is encouraged to agree its own key issues for handover. This is not an exhaustive list, but is intended as a guide:
Patient presentation - mental and physical wellbeing
Observations levels (or frequency of contact in the case of community teams) - Section 17 Leave escorted/ unescorted (or how many visits are offered per week in the case of community teams)
Mental Health Act status - Informal/ detained under Mental Health Act
Mental Capacity issues or DOLS
Risk, both nature and level (for example risk of falls, absconsion, harm to self, suicide, neglect, risk of harm to others)
Medication - changes to medication/ omissions/ allergies
Physical health investigations i.e. CT Scan, X-ray
Blood investigations, for example, Clozapine/ lithium levels, blood sugars, drug screen
Physical health - BP (blood pressure), TPR (temperature, pulse and respiration), resuscitation status, blood sugar monitoring, nutrition and hydration
End of Life Care
Safeguarding alerts/ issues (children/ adults)
DATIX incidents
Changes/ updates to care plans
New admissions/ discharge/ referrals
Multidisciplinary Meeting (MDM) feedback
Equality diversity and human rights considerations (including effective communication needs, cultural sensitivities)
Outstanding tasks
Untoward occurrences
Operational issues affecting the care of the client
Activities i.e. social events/ visitors (see 4.1.4.2)

Clinical Handover Policy
Version 2.0 August 2016
8
Handover is of little value unless action is taken where needed. All team members including bank and agency staff should be aware of their responsibilities and need to ensure that:
Tasks are prioritised to enable completion in a timely, effective and safe manner
Plans for further care are put in place and clarified with all relevant parties
Unstable patients are reviewed as often as required
If busy, additional handovers are considered in order to further support the team, re-prioritise workload and identify new “at risk” patients
Any patient who is considered at risk of deterioration has an adequate care plan to prevent or manage this as effectively as possible and that it is acted on accordingly
5.0 Procedures connected to this Policy
Standard Operating Procedure 1 (SOP 1) - Medical Handover for CYPF Specialist Mental Health Services (CAMHS and CAFS)
6.0 Links to Relevant Legislation
Data Protection Act 1998 Data Protection Act came into force in March 2001, replacing the 1984 Act, to control the way information is handled and to give legal rights to people who have information stored about them. It sets out strict rules for people who use or store data about living people and gives rights to those people whose data has been collected. The law applies to data held on computers or any sort of storage system, including paper records. On 6 April 2010, the Information Commissioner’s Office was given new powers to issue monetary penalties requiring organisations to pay up to £500,000 for serious breaches of the Data Protection Act. Freedom of Information Act 2000 This Act provides public access to information held by public authorities. It does this in two ways, public authorities are obliged to publish certain information about their activities and members of the public are entitled to request information from public authorities. The main principle behind freedom of information legislation is that people have a right to know about the activities of public authorities, unless there is a good reason for them not to. This is sometimes described as a presumption or assumption in favour of disclosure. The Act does not give people access to their own personal data (information about themselves) such as their health records. If a member of the public wants to see information that a public authority holds about them, they should make a subject access request under the Data Protection Act 1998. Health and Social Care Act 2008 The Care Act represents the most significant reform of social care in more than 60 years, putting service users and stakeholders in control of their care and support. The primary focus of the Health and Social Care Act 2008 was to create a new regulator whose purpose was to provide registration and inspection of health and adult social care services together for the first time, with the aim of ensuring safety and quality of care for service users. Thus the Care Quality Commission (CQC) was

Clinical Handover Policy
Version 2.0 August 2016
9
established, with enhanced powers to regulate primary care services, including hospitals, GP practices, Dental practices and Care Homes. Equality Act 2010 Equality Act came into force on 1 October 2010 and brought together over 116 separate pieces of legislation into one single Act to provide a legal framework to protect the rights of individuals and advance equality of opportunity for all. The Act simplifies, strengthens and harmonizes the current legislation to provide a new discrimination law which protects individuals from unfair treatment and promotes a fair and more equal society.
6.1 Links to Relevant National Standards
SBAR - Situation - Background - Assessment - Recommendation 2008 SBAR was initially developed by the US Navy and adapted for use in the healthcare environment by staff at Kaiser Permanente in Colorado, USA. SBAR is a nationally recognised tool to improve communication between all members of staff. It is an easy to remember mechanism that can be used to frame communications or conversations, facilitating a structured way of communicating information that requires a response from the receiver. It enables staff to clarify what information should be communicated between members of the team, and how. It can help to develop teamwork and foster a culture of patient safety. The SBAR process consists of 4 x standardised stages or prompts that help staff to anticipate the information needed by colleagues and formulate important communications with the right level of detail: S = Situation (a concise statement of the problem) B = Background (pertinent and brief information related to the situation) A = Assessment (analysis and consideration of options - what you found / think) R = Recommendation (action requested/recommended - what you want) CQC Regulation 12: Safe Care and Treatment The intention of this regulation is to prevent people from receiving unsafe care and treatment and prevent avoidable harm or risk of harm. Providers must assess the risks to people's health and safety during any care or treatment and make sure that staff have the qualifications, competence, skills and experience to keep people safe. Providers must make sure that the premises and any equipment used is safe and where applicable, available in sufficient quantities. Medicines must be supplied in sufficient quantities, managed safely and administered appropriately to make sure people are safe. Providers must prevent and control the spread of infection. Where the responsibility for care and treatment is shared, care planning must be timely to maintain people's health, safety and welfare. CQC understands that there may be inherent risks in carrying out care and treatment, and they will not consider it to be unsafe if providers can demonstrate that they have taken all reasonable steps to ensure the health and safety of people using their services and to manage risks that may arise during care and treatment.

Clinical Handover Policy
Version 2.0 August 2016
10
Nursing and Midwifery Council (NMC) - Code of Conduct - Preserve Safety Staff should make sure that patient and public safety is protected. They should work within the limits of their competence, exercising ‘duty of candour ‘and raising concerns immediately whenever they come across a situation that puts the patients or public safety at risk. They should take necessary actions to deal with any concerns where appropriate. Nursing and Midwifery Council (NMC) - Code of Conduct – Practice effectively Staff should assess needs and deliver or advise on treatment or give help (including help and rehabilitative care) without too much delay and to the best of their abilities, on the basis of the best evidence available and best practice. Staff should communicate effectively, keeping clear and accurate records and sharing skills, knowledge and experience where appropriate. Staff should also reflect and act on any experience they receive to improve their practice. Nursing and Midwifery Council (NMC) - Record Keeping Good record keeping is an integral part of nursing and midwifery practice and is essential to the provision of safe and effective care. Good record keeping whether as an individual team or organisational level, has many important functions:
Providing documentary evidence of service delivered
Promoting better communication and sharing of information between members of the multidisciplinary team
Help to identify risk and enabling early detection of complications
Making continuity of care easier and improve accountability
You should beware of, and develop, your ability to communicate effectively within teams. The way you record information and communicate is crucial. Other people will rely on your records at key communication points, especially during handover, referral and in shared care
6.2 Links to other Key Policies
Clinical Record Keeping Standards Policy The aim of this policy is to provide direction and guidance to staff on how to meet the standards required for the recording of information within health care records. Discharge and Transfer of Care Policy The purpose of this policy is to ensure that discharge or transfer from services managed by the Black Country Partnership NHS Foundation Trust is effective, consistent and organised around the needs of individual service users and carers. Incident Reporting Policy The purpose of this policy is to make clear the system used for reporting incidents involving patients, staff and others undertaking activities on behalf of the Trust. Risk Management Policy The purpose of the Risk Management Policy is to provide an effective framework through which the Trust can safely and effectively manage risks. This policy does not cover individual patient clinical risk assessments which may be identified as part of a patients care plan. These individual clinical risk assessments for example, falls risk assessments, suicide risk assessments etc. will be conducted in line with the relevant clinical policy and process for the risk identified.

Clinical Handover Policy
Version 2.0 August 2016
11
Clinical Risk Management Policy This policy is intended to guide practitioners who work with service users to manage the risk of harm. It sets out the principles and standards required that should underpin best practice across all health settings, and describes the tools that are used to structure the often complex clinical risk management process. Clinical Observations and Engagement Policy The purpose of this policy is to make clear the standards expected of clinical staff for the observation and engagement of patients, and to provide them with direction and guidance for making decisions about observation levels including reviews, carrying out observations, correct completion of documentation and their training requirements. Dignity and Respect Policy The purpose of this policy is to identify best practice for maintaining a culture of dignity and respect for patients, carers, staff and members of the public in compliance with the Caring Counts Strategy 2013/2016. The strategic approach outlined in Caring Counts ensures integration of the 6Cs in the delivery of fundamental care through a process of cultural challenges and sustainable change. Information Sharing Policy This policy provides clarity and guidance for staff to comply with the many different rules in relation to the release of patient information for requests to access any other types of information, please refer to the Trust’s Freedom of Information Policy.
6.3 References
Nursing and Midwifery Council - Code of Conduct
Nursing and Midwifery Council - Record keeping
Essence of Care Benchmarking Standards
NHS Institute of Innovation and Improvement Productive Wards Series - Shift Handover Module
Australian Commission on Safety and Quality in Health Care (2010) The OSSIE Guide to Clinical Handover Improvement
BMA (2004) Safe handover: safe patients Guidance on clinical handover for clinicians and managers
Royal College of Nursing (2008) Improving the safe transfer of care: A quality improvement initiative

Clinical Handover Policy
Version 2.0 August 2016
12
7.0 Roles and Responsibilities for this Policy
Title Role Key Responsibilities
Clinical Staff Adherence - Ensure they are familiar with the policy and be responsible for adhering to the procedures referred to within the policy - Ensure that any deviation or errors arising from clinical handover are dealt with in the correct manner, according to the
Incident Reporting Policy of the Trust - Ensure the necessary documentation is available for clinical handover
Service Managers and Ward Managers
Operational - Ensure they are familiar with this policy and be responsible for adhering to the procedures referred to - Ensure staff attend training applicable to their role and implement the guidance across their areas of responsibility - Ensure staff work to the standards set out in this policy - Ensure all incidents relating to clinical handover are reported
Nurse in Charge Operational - prioritise and delegate tasks - Ensure staff are competent to complete the delegated task and update care plans and risk assessments, where
appropriate, when actions are completed
Deputy Modern Matrons, Senior Nurses and Lead Nurses
Operational Leads
- Ensure support is given to the service managers and ward managers to implement this policy - Ensure support and guidance regarding resources is available to enable this policy to be implemented
Group Directors and Group Managers
Implementation - Ensure that all managers are aware of the policy and promote good practice - Provide support and guidance regarding resources to enable this policy to be implemented - Ensure staff implement safe systems of work in accordance with the procedures referred to in the policy
Nursing Board Responsible - Oversee the implementation of a systematic and consistent approach to the practice of clinical handover - Provide exception and progress reports to Quality and Safety Steering Group
Group Quality and Safety Groups
Monitor - Ensure the practice of clinical handover is monitored including any risks identified within their Group. Membership is representative of the Group as a whole multi-disciplinary in nature, with a mix of representatives from each of the service areas, professional leads, practice development professionals and representatives from clinical sub-groups
- Ensure all incidents in relation to clinical handover are reported via DATIX, the trust’s incident reporting procedure - Ensure a report of all incidents is discussed at monthly meetings of Group Quality and Safety Steering Groups - Receive the results and recommendations of all completed clinical audits relating to clinical handover and be responsible
for monitoring action plans to implement changes to current practice until completion
Quality and Safety Steering Group
Scrutiny and Performance
- Ensure that the practice of clinical handover is managed efficiently and effectively in accordance with the Board’s Assurance Framework and strategic priorities
Clinical Directors Trust Leads - Identify and manage any risks in relation to standards of clinical handover within their group - Lead discussions on the practice of clinical handover at Group Quality and Safety Steering meetings - Oversee the completion of audits in respect of clinical handover - Monitor the implementation of subsequent action plans to improve the quality of clinical handover of care as required - Provide updates on the use of clinical handover within their Group to the Quality and Safety Steering Group

Clinical Handover Policy
Version 2.0 August 2016
13
Title Role Key Responsibilities
Trust Board Strategic - Strategic overview and final responsibility for overseeing the practice of clinical handover within service areas across the Trust in accordance with its objective to provide high quality safe care
Executive Director of Nursing, AHPs and Governance
Executive Lead - Ensure the Trust’s management and practice of clinical handover is discharged appropriately and has lead responsibility for the implementation of this policy
- Identify and implement strategies to minimise any risks in relation to the standards for clinical handover - Ensure any serious concerns regarding the implementation of this policy are brought to the attention of the Board
8.0 Training
What aspect(s)
of this policy will require staff
training?
Which staff groups require this
training?
Is this training covered in the Trust’s Mandatory and Risk
Management Training Needs Analysis document?
If no, how will the training be delivered?
Who will deliver the training?
How often will staff require
training
Who will ensure and monitor that staff have
this training?
SBAR Training All staff responsible
for Clinical Handover
No, staff will receive specific
training in relation to this policy where it is identified in
their individual training needs
analysis as part of their development for their
particular role and responsibilities
Internally Practice Development
Nurse
As required Nursing Board
Solution Focussed
Therapy Training
Mental Health
Urgent Care Staff
No, staff will receive specific
training in relation to this policy where it is identified in
their individual training needs analysis as part of their
development for their
particular role and responsibilities
Internally MH Group Training
Team coordinated by Consultant Clinical
Psychologist
One off Mental Health Quality and
Safety Group
9.0 Equality Impact Assessment Black Country Partnership NHS Foundation Trust is committed to ensuring that the way we provide services and the way we recruit and treat staff reflects individual needs, promotes equality and does not discriminate unfairly against any particular individual or group. The Equality Impact Assessment for this policy has been completed and is readily available on the Intranet. If you require this in a different format e.g. larger print, Braille, different languages or audio tape, please contact the Equality & Diversity Team on Ext. 8067 or email [email protected]

Clinical Handover Policy
Version 2.0 August 2016
14
10.0 Data Protection and Freedom of Information This statement reflects legal requirements incorporated within the Data Protection Act and Freedom of Information Act that apply to staff who work within the public sector. All staff have a responsibility to ensure that they do not disclose information about the Trust’s activities in respect of service users in its care to unauthorised individuals. This responsibility applies whether you are currently employed or after your employment ends and in certain aspects of your personal life e.g. use of social networking sites etc. The Trust seeks to ensure a high level of transparency in all its business activities but reserves the right not to disclose information where relevant legislation applies.
11.0 Monitoring this Policy is Working in Practice
What key elements will be monitored?
(measurable policy objectives)
Where described in
policy?
How will they be monitored?
(method + sample size)
Who will undertake this
monitoring?
How Frequently?
Group/Committee that will receive and
review results
Group/Committee to ensure actions
are completed
Evidence this has
happened
Handover requirements between all care settings, to
include both giving and receiving of information
4.0 Process/ Appendix 2
A detailed review of practice will be audited -
The audit will include compliance with the key
elements of this policy. Any
deviation from the policy and/or recommendations
arising from the audit will result in an action plan
Head of Nursing Annually Group Quality and Safety Steering
Groups/ Nursing Board
Nursing Board Minutes of Meetings/
Action plans signed off
How handover is recorded 4.0 Process/ Appendix 2
A detailed review of practice will be audited
Head of Nursing Annually Group Quality and Safety Steering
Groups/ Nursing Board
Nursing Board Minutes of Meetings/
Action plans signed off
Out of hours handover
process
4.0 Process/
Appendix 2
A detailed review of
practice will be audited
Head of Nursing Annually Group Quality and
Safety Steering Groups/ Nursing
Board
Nursing Board Minutes of
Meetings/ Action plans
signed off

Clinical Handover Policy
Version 2.0 August 2016
15
Appendix 1
Example of a Patient Information Handover Sheet
Staff members present
S Situation
Name: Age
Sex: Age: Room No:
Status (Informal/Detained under Mental Health Act):
Diagnosis:
B Background
New admission/ Referral: Patient presentation - mental and physical wellbeing:
Allergies:
Communication needs:
Physical health monitoring - BP (blood pressure), TPR (temperature, pulse and respiration), resuscitation status, blood sugar monitoring:
Observations levels:
Section 17 Leave escorted/unescorted:
A Assessment
Medication changes to prescribed treatment plan, depot injection: Risks Assessment i.e. absconds, self-harm: MDM feedback/ Feedback from other professionals: Physical health Investigations:
Bloods investigations Clozapine/Lithium Levels: Changes / updates to care plans:
R Recommend
Special Needs:
Activities:
Nutrition/ Hydration:
VAP Safeguarding Issues:
Clinical Handover Policy
Version 2.0 August 2016
16
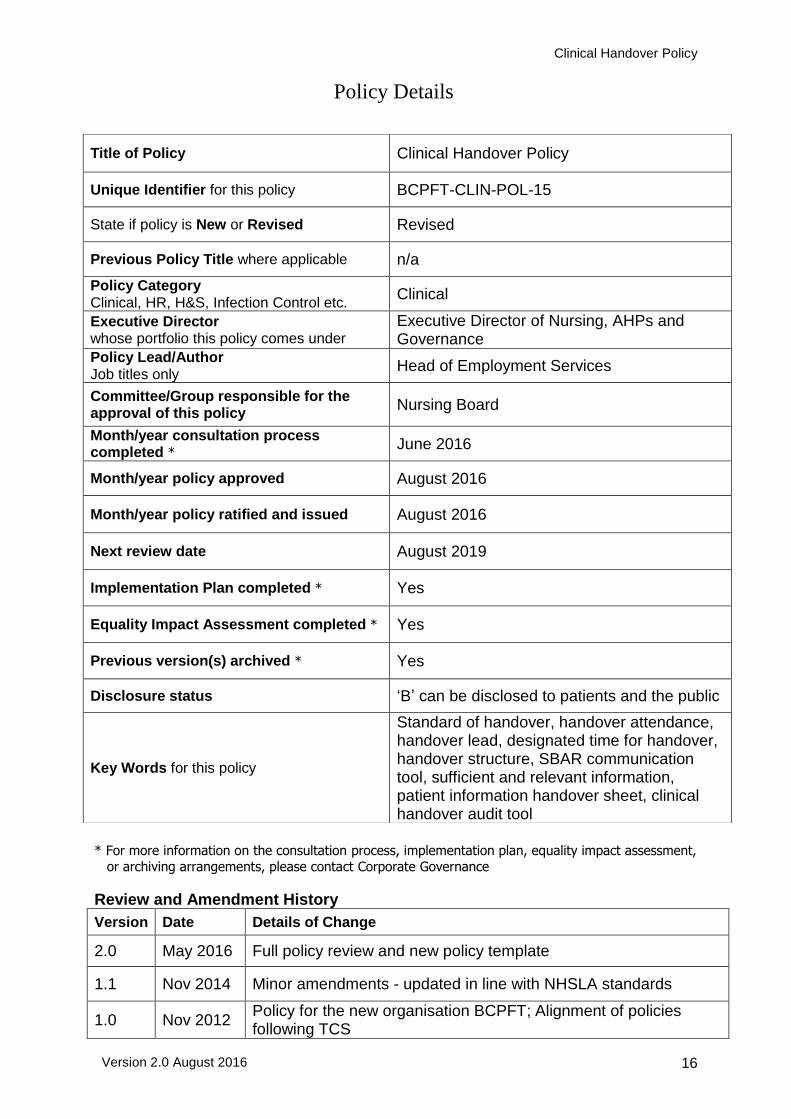
Policy Details
* For more information on the consultation process, implementation plan, equality impact assessment,
or archiving arrangements, please contact Corporate Governance
Review and Amendment History
Version Date Details of Change
2.0 May 2016 Full policy review and new policy template
1.1 Nov 2014 Minor amendments - updated in line with NHSLA standards
1.0 Nov 2012 Policy for the new organisation BCPFT; Alignment of policies following TCS
Title of Policy Clinical Handover Policy
Unique Identifier for this policy BCPFT-CLIN-POL-15
State if policy is New or Revised Revised
Previous Policy Title where applicable n/a
Policy Category Clinical, HR, H&S, Infection Control etc.
Clinical
Executive Director whose portfolio this policy comes under
Executive Director of Nursing, AHPs and Governance
Policy Lead/Author Job titles only
Head of Employment Services
Committee/Group responsible for the approval of this policy
Nursing Board
Month/year consultation process completed *
June 2016
Month/year policy approved August 2016
Month/year policy ratified and issued August 2016
Next review date August 2019
Implementation Plan completed * Yes
Equality Impact Assessment completed * Yes
Previous version(s) archived * Yes
Disclosure status ‘B’ can be disclosed to patients and the public
Key Words for this policy
Standard of handover, handover attendance, handover lead, designated time for handover, handover structure, SBAR communication tool, sufficient and relevant information, patient information handover sheet, clinical handover audit tool