clinical documentation guides - coding strategies
TRANSCRIPT
Brought to you by
Women’s Imaging ICD-10-CMClinical Documentation Guides
© Copyright 2015, Coding Strategies, Inc. | www.codingstrategies.comThe Resource for Physician and Outpatient Coding, Compliance & ICD-10-CM

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
WOMEN’S IMAGING ICD-10-CMCLINICAL DOCUMENTATION GUIDES
The Interventional Radiology Guide includes topics encountered in both vascular and non-vascular interventions. Some conditions covered in the IR package include circulatory disorders of the brain, DVT, traumatic brain injury, cholelithiasis, pleural effusion, and pneumothorax.
The MRI/CT package includes a broad range of conditions generally evaluated by these modalities, such as circulatory disorders of the brain, spinal disorders, traumatic brain injury, chest pain, and pneumothorax.
The Ultrasound package includes conditions frequently seen in ultrasound studies in the hospital, physician office, and freestanding facility setting. Among the conditions included in this package are ascites, DVT, diverticular disease, abdominal pain, limb pain, and thyroid disorders.
The Women’s Imaging package includes conditions encountered in bone density studies, mammography, breast ultrasound, and other breast studies and procedures. In addition to disorders of the breast and neoplasms of the breast, this package includes a guide that focuses on definition and documentation requirements of active cancer versus history of cancer.
OTHER CLINICAL DOCUMENTATION GUIDES
MRI AND CT ICD-10-CMCLINICAL DOCUMENTATION GUIDES
ULTRASOUND ICD-10-CMCLINICAL DOCUMENTATION GUIDES
INTERVENTIONAL RADIOLOGY ICD-10-CMCLINICAL DOCUMENTATION GUIDES

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
© Copyright 2014, Coding Strategies, Inc. | www.codingstrategies.comThe Resource for Physician and Outpatient Coding, Compliance & ICD-10-CM
Non-toxic Goiter Hypothyroidism Hyperthyroidism• Thyrotoxicosis
1. Select a condition and follow the arrows:
Physician Documentation Guide for Thyroid Disorders
Patient with Goiter, Thyroid Nodules, Hypo- & Hyperthyroidism
Diffuse• Simple
Single thyroidnodule• Colloid• Uninodular
Multinodular• Cystic
Congenital withdiffuse goiter
Congenital w/ogoiter
Other
With diffuse goiter• Exophthalmic• Graves’ Disease
With single thyroidnodule
With multinodulargoiter
From ectopic thyroid tissue
Factitia
Other
With thyrotoxicstorm or crisis
Without thyrotoxicstorm or crisis
2. Be descriptive:
How to use the ICD-10 Documentation Guides
Each documentation guide breaks down the clinical information that needs to be documented into columns and rows. Start with the first row and determine which clinical statement is appropriate for the patient. The additional information that needs to be documented for each condition continues on the following rows.
Some documentation guides are straightforward and follow a single column down the rows. This is the case with the guide for Thyroid Disorders below, once the determination is made that the patient has a non-toxic goiter, the additional information that needs to be documented is provided directly below the non-toxic goiter box.

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
© Copyright 2014, Coding Strategies, Inc. | www.codingstrategies.comThe Resource for Physician and Outpatient Coding, Compliance & ICD-10-CM
Physician Documentation Guide for Hypertension
Patient Diagnosed with Hypertension
1. Select type and follow the arrows:
Essential(default)
Secondary Hypertensive heart and/or kidney disease
Renovascular
Other renaldisorders
Endocrinedisorders
Other
Hypertensive heart disease
Hypertensive chronic kidney disease
Hypertensive heart and kidney disease
Heart Disease
With heart failure
Without heartfailure
Chronic Kidney Disease
With stage1-4 CKD
With stage 5 or ESRD
With heart failure
Without heart failure
AND
With stage 1-4 CKD
With stage 5 or ESRD
Document the type ofheart failure
Document the stage of chronic kidney disease
Document both the type of heart failure and the stage of kidney disease
Other documentation guides will be more complex. In these cases, the information in the sub-sequent rows must be further subdivided to provide the necessary level of detail. Below is the guide for Hypertension. As you can see, more information is necessary to document patients with hypertensive heart and/or kidney disease. Once the determination is made that the pa-tient has hypertensive heart or kidney disease, both the type of heart failure and the stage of kidney disease must be documented.

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
Documentation Guide for Disorders of the Breast and Other Abnormal Findings
Patient with Disorders of the Breast or Other Abnormal Findings:
Abnormal Findings Disorders of Breast
Presence of:
Personal history of breast cancer
Family history of breast cancer
1. Select condition and follow the arrows:
Mammographic microcalcifications
Mammographic calcifications
Inconclusive mammogram• Dense Breasts• Inconclusive mammogramOther inconclusive andabnormal findings
Solitary cyst of breast
Diffuse cystic mastopathy• Cystic breast• Fibrocystic disease of breast
Fibroadenosis of breast
Fibrosclerosis of breast
Mammary duct ectasia
Other benign mammary dysplasias
Inflammatory disorders of breast• Abscess areola/breast• Carbuncle of breast• Infective mastitis
Hypertrophy of breast
Lump
2. Be specific: 2. Select category:
4. Provide context:
Skip Step 3
and move to Step 4
Left Right
3. Laterality:

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
Physician Documentation Guide for Neoplasms
Location of Neoplasm – Specify precise location of neoplasm. See Breast documentation guides for examples.
Patient Diagnosed with Neoplasm
History of Cancer – treatment has ended and no evidence of cancer:• Primary site excised or
eradicated AND• Primary site no longer being
treated AND• No evidence of remaining
malignancy
Active Cancer – diseasethat is currently causing signsand symptoms and/or is undertreatment by any modality:• Surgery• Chemotherapy• Radiation• Hormonal Therapy• Alternative Medicine
All malignancies both primary and secondary should include sitespecific details – even if no longer active.
1. Select Status and follow the steps down the column:
Previous treatments • Radiation therapy • Chemotherapy
Primary Malignancy
Secondary Malignancy
In Situ
Benign Neoplasm
2. Select Previous Treatments: 2. Select Category:
3. Specify Location:
4. Reminder:
Skip Step 3
and move to Step 4

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
Physician Documentation Guide for Neoplasm of Breast
Patient Diagnosed with Neoplasm of Breast
Active Cancer – disease that iscurrently causing signs andsymptoms and/or is undertreatment by any modality:• Surgery• Chemotherapy• Radiation• Hormonal Therapy• Alternative Medicine
Primary Malignancy
Secondary Malignancy
In Situ
Benign Neoplasm
2. Provide context:
Previous treatments• Radiation therapy• Chemotherapy
History of Cancer– treatmenthas ended and no evidence ofcancer:
• Primary site excised oreradicated AND
• Primary site no longer beingtreated AND
• No evidence of remainingmalignancy
1. Select status and follow the steps down the column of the same color:
3. Select Gender:
Female
Male
Right
Left
4. Select Breast:
Nipple and Areola
Central Portion
Upper-Inner Quadrant
Lower-Inner Quadrant
Upper-Outer Quadrant
Lower-Outer Quadrant
Axillary Tail
Overlapping Sites
5. Select specific location:
All malignancies both primary and secondary should include site specific details – even if no longer active.
6. Reminder:
2. Select type:

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
Physician Documentation Guide for Osteopenia
Patient Diagnosed with Osteopenia
Left Right
Shoulder
Upper Arm
Forearm
Hand
Thigh
Lower Leg
Ankle/Foot
Other Site
Multiple Sites
1. Select side:
2. Select location:
© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
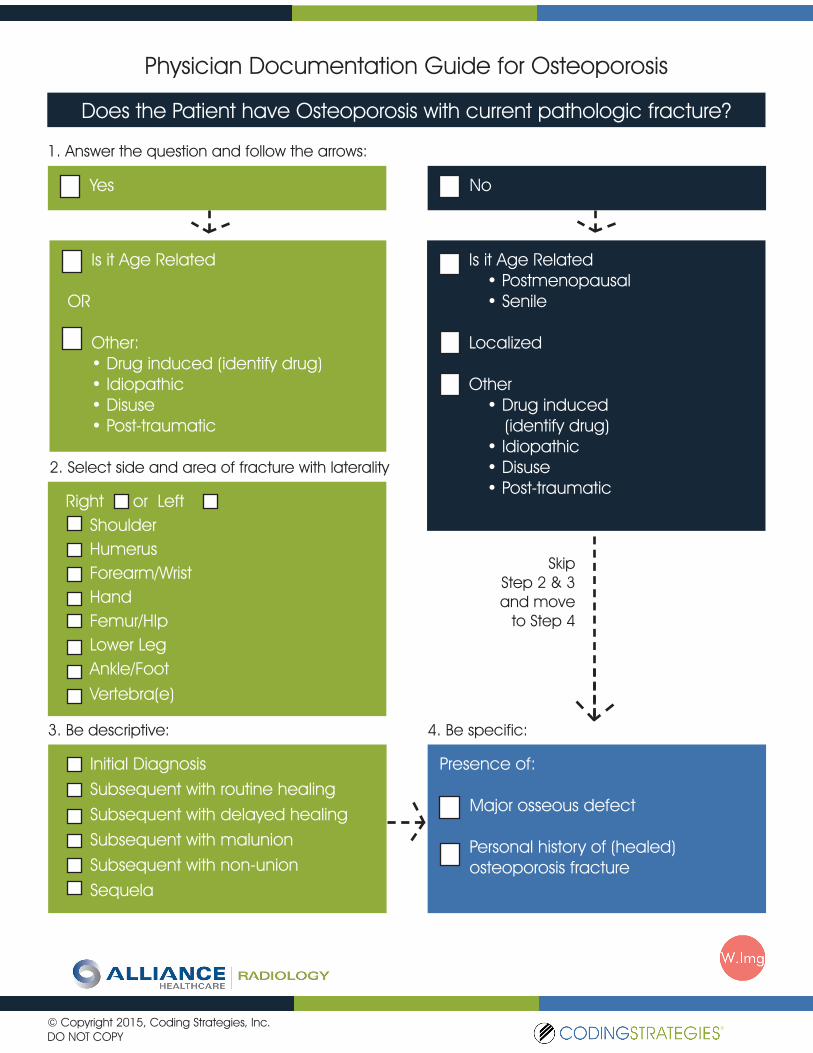
Physician Documentation Guide for Osteoporosis
Does the Patient have Osteoporosis with current pathologic fracture?
Yes No
1. Answer the question and follow the arrows:
Is it Age Related
OR
Other:• Drug induced (identify drug)• Idiopathic• Disuse• Post-traumatic
Right or LeftShoulderHumerusForearm/WristHandFemur/HIpLower LegAnkle/FootVertebra(e)
2. Select side and area of fracture with laterality
Initial DiagnosisSubsequent with routine healingSubsequent with delayed healingSubsequent with malunionSubsequent with non-unionSequela
3. Be descriptive:
Is it Age Related• Postmenopausal• Senile
Localized
Other• Drug induced
(identify drug)• Idiopathic• Disuse• Post-traumatic
Presence of:
Major osseous defect
Personal history of (healed) osteoporosis fracture
4. Be specific:
Skip Step 2 & 3 and move
to Step 4

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
Physician Documentation Guide for Episodes of Care Episodes of Care
1. Select a type and follow the arrows:
Initial Encounter (active treatment, may apply to multiple services and/or multiple dates of service)
Document as IE if:ED patient (seen in or referred from ED)
Surgical treatment including pre- & post-surgical imaging
New injury still being evaluated
2. Include the following:
Subsequent Encounter (routine care during the healing or recovery phase)
Document as SE if:Ordered as a “follow-up” or “check status” study
Presence of a cast, internal fixation device (beyond initial pre-/post- placement images)
Sequela (residual effect after the acute phase has terminated)
Document as a se-quela if the current complaint is related to prior accident/in-jury. Select from the following:
Scarring
Deformity
Post-traumatic arthritis
Pain and other conditions
Remember to include in the patient history details related to the accident/injury. e.g:
• Shoulder pain and bruising after fall from ladder
• Laceration forehead from MVA
For fractures subsequent encounters must document status as:
Routine healing
Delayed healing
Malunion
Non-union
Encounters for sequela require that the provider directly link the original injury to the identified residual effect or complication.
NOTE: Open fractures of the forearm, femur and lower leg are further defined by severity by using the Gustilo Classification. Please document class, if known.

© Copyright 2015, Coding Strategies, Inc.DO NOT COPY
NeoplasmDocument neoplasm
In other diseasesDocument disease
Physician Documentation Guide for Pathological Fractures
Pathological Fracture caused by/due to:
1. Select one
2. Choose the Location:
4. Encounter (Closed):
Not elsewhere classified
Initial
Subsequent routine healing
Subsequent delayed healing
Subsequent non-union
Subsequent malunion
Sequela
Shoulder
Humerus
Radius
Ulna
Hand
Pelvis
Femur
Tibia
Fibula
Ankle
Foot
Vertebra
Shoulder
Humerus
Radius
Ulna
Hand
Fingers
Pelvis
Femur
Tibia
Fibula
Ankle
Foot
Toes
Vertebra
Right Left
3. Select a side:

Coding Strategies® provides exceptional consulting & educational services designed to improve compliance & ensure appropriate reimbursement for the financial health of your business.
Coding Strategies®, dedicated to empowering healthcare professionals.
www.codingstrategies.com