clinical audit annual report - fraser health · corporate care standards discharge summaries –...
TRANSCRIPT

Prepared on behalf of HAMAC and the Regional Departments by Sharmen Lee, October 2014 Strategyst Healthcare Corporation
CLINICAL AUDIT ANNUAL REPORT
MEDICAL QUALITY OVERSIGHT AND IMPROVEMENT IN FRASER HEALTH
PROCEEDINGS AS DISCUSSED AND REPORTED TO THE FRASER HEALTH MEDICAL ADVISORY COMMITTEE
OCTOBER 2013 – JULY 2014

Page 1 of 210
Table of Contents
Opening messages 2 Executive Summary 3 Summary of Activities 10 Department Summaries Anesthesiology 21 Cardiology 25 Critical Care 40 Emergency Medicine 53 Family Practice 64 Geriatric Medicine 73 Hospitalists 92 Infection Prevention & Control 101 Laboratory Medicine & Pathology 107 Medicine 123 Medical Imaging 149 Mental Health & Substance Use 172 Obstetrics & Gynecology 181 Pediatrics 185 Surgery 186

OPENING MESSAGES Clinical Audit Annual Report
Page 2 of 210
QUALITY IS TRUST: Clinical Audit in FHA 2014
The Institute of Medicine (IOM) defines patient-centered care as "care that is respectful of and responsive to individual patient preferences, needs, and values, and ensuring that patient values guide all clinical decisions."
“How can you show that you are doing a good job” is a fundamental question of quality; this is where the process of clinical audit fits. This extensive report shows the enthusiastic uptake of documentation of quality by means of clinical audit and many other quality improvement tools by all of the clinical departments in Fraser Health. This is a remarkable and applaudable achievement in just three years.
Physicians in Fraser Health continue to participate in Regional Department Medical Quality committees that include Morbidity and Mortality rounds, Clinical Audit and many other quality activities.
There is still work to be done to improve the breadth and depth of quality processes amongst the physicians of FHA, but we are most definitely going in the right direction. These ongoing quality projects in FHA help ensure we keep getting better, and aspire for the best.
TRUST is a fundamental component of patient centered care:
The patient trusts the clinician is fully present and engaged
They both trust that all care team members will have all skills necessary to provide care
They both trust the system will support high quality care where and when needed
They both trust the medical system is committed to error free care
They both trust that transitions in care between locations and providers will be flawless.
Alice K Jacobs (past President American Heart Association) stated “ we must also remember that caring for patients is more than a career or even a profession. It defines us; it is part of who we are. This understanding transcends race and religion and geography. Those of us who are responsible for the lives of others, during health and during illness and when the end is near live by the dictum that we must care for all patients at all times. We cannot, however, believe that we are entitled to be trusted. We must reach out to others, for trust is earned, and it is fragile.”
For TRUST to be earned we must be able to demonstrate the quality of what we do.
Dr Peter Doris MD FRCSC Chair, HAMAC, Fraser Health
Dr Andrew Webb MD FRCP MFMLM VP Medicine, Fraser Health
Dr Jan Kornder MD FRCPC FACC PMD for Quality Improvement and Patient Safety, Fraser Health
Every patient should reasonably expect care that is free from error. We must also ensure care is patient-centered in all health care settings.

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 3 of 210
For the past 3 years, the Fraser Health Authority Medical Advisory Committee (HAMAC) and the Regional Departments have been implementing the four Board resolutions related to clinical audit, peer review and quality improvement. Two of the resolutions relate directly to clinical audit requesting HAMAC to:
ensure all regional departments develop a process of clinical audit by peer review that is
appropriate to the clinical function of the department and ensures continuing
improvement in the quality of medical care in the department.
ensure all members of the medical staff participate in regular clinical audit of their
clinical practice by peer review both within the process developed by regional
departments and as required by relevant accreditation processes, with a report of that
participation made available to the Board in the quarterly reporting by HAMAC.
This report, dated October 2014, provides an update on the activities undertaken by HAMAC and the regional departments to monitor and improve the medical quality of care provided by their 2,696 members.
Health Authority Medical Advisory Committee (HAMAC)
Appointed by the Board of the Directors, the Health Authority Medical Advisory Committee (HAMAC) undertakes several critical functions including: making recommendations to the Board of Directors with respect to the cancellation,
suspension, restriction, non-renewal, or maintenance of the appointments and privileges of all members of the medical staff to practice within the facilities and programs operated by the Fraser Health Authority.
providing advice to the Board of Directors and to the CEO on: the provision of medical care within the facilities and programs operated by the
Fraser Health Authority. the monitoring of the quality and effectiveness of medical care provided within the
facilities and programs operated by the Fraser Health Authority. the adequacy of medical staff resources. the continuing education of the members of the medical staff. planning goals for meeting the medical care needs of the population served by the
Fraser Health Authority. the availability and adequacy of resources to provide appropriate patient care in the
Fraser Health Authority.
HAMAC and its regional departments are the responsible for the medical quality oversight and improvement within the Fraser Health Authority.

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 4 of 210
Over the last year, HAMAC has met ten (10) times, and in addition to receiving the Department quality reports that are summarized in the subsequent sections, the following issues and concerns have been presented to HAMAC for information, discussion, advice, and when appropriate, approval:
Hand Hygiene- physician compliance; members of HAMAC to become Hand Hygiene Auditors; completion of the Hand Hygiene Course to become a requirement for renewal of Medical Staff appointments.
Nursing Sensitive Adverse Events –providing feedback on the improvement plan and identifying how physicians can best support the improvement work.
Perioperative Information Systems (PIMS) – a high quality initiative. Incomplete health records – managing notifications of incomplete records and
suspensions Conflict of Interest Policy Antimicrobial Stop Orders Policy Vehicular access to Surrey Memorial Hospital (SMH) during marathon Medical Imaging 24/7 Reporting Medication reconciliation and discharge prescription forms Medication Reconciliation at Transitions in Care Policy Influenza Control Policy Reports distribution and transcription turn-around times Physician Workload Manager – health informatics Proof of immunity to MMR/Pertussis as criteria for appointment Attendance of members at Medical Staff Association (MSA) meetings Physicians as “handlers” in Patient Safety Learning System (PSLS) Continuing Medical Education (CME) and health education – issue with
videoconferencing and accessibility of technology for case presentations across the region
Corporate Care Standards Discharge summaries – timely completion; discharge summary template – guideline
for recommended contents; Discharge summaries and patient transfer/repatriation Physician Partnership Agreement (formerly Statement of Expectations) Antimicrobial Stewardship – Carbapenem Utilization; updates Procedural Privileging – Medical Imaging context Provincial Privileging Project Orders on patients transferred to another site Quality of care issues for admitted patients in Emergency without a Most
Responsible Practitioner (MRP) Reporting by Departments on “preventable deaths” Patient Care Quality Office Case Management Approach Medical Imaging Department Review Emergency Room Physician staffing shortages SMH patient coverage plans Revisions to MRP (acute care) Policy

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 5 of 210
HAMAC has also discussed and identified improvements to consider with its own processes: Creation of a summary report to the medical staff members – items of importance
and interest to be summarized and forwarded to the members. Consideration to be given to establishing a Credentialing Committee as a standing
sub-committee of HAMAC to conduct (more) detailed reviews of credentialing recommendations.
Search and Selection – HAMAC to consider an approach for the management of vacancies within departments and to provide detailed guidelines for the Search and Selection process.
HAMAC Department Quality Goals Based upon a review of the topics, discussion and agenda items at HAMAC meetings over the past year, HAMAC has decided to set three quality goals for the coming year. The intention is for each Department/Division to address these quality goals as appropriate to their specialty. These goals are in addition to quality goals and initiatives that the Department/Division is undertaking.
Goal 1: 85% of all Discharge Summaries are dictated within 48 hours.
Goal 2: To increase the physician hand hygiene compliance rate by 15%.
Goal 3: To develop and implement trigger tools appropriate for each department to
enable discussion and learning from preventable deaths.
CLINICAL AUDITS
The following clinical audits have been completed or commenced prior to July 2014: Department of Anesthesiology
OR start times
OR hold times
Department of Cardiology
Clinical audit to determine the degree of concurrence of Electrocardiogram (ECG) Reader Interpretations.
Clinical audit of the medical care provided to patients presenting with Acute Coronary Syndrome (ACS)
Appropriateness and Effectiveness of the medical care provided to patients
receiving implantable cardiac electrical devices (pacemakers).

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 6 of 210
Appropriateness of Interventional Cardiology Procedures
The Appropriateness of Diagnostic Cardiac Catheterizations and Percutaneous
Coronary Interventions (PCI) at the Royal Columbian Hospital (RCH)
Department of Critical Care
Critical Care Physician Compliance with Rounding Checklist
Switching from routine daily chest X-rays (CXRs) to on-demand CXRs
Department of Emergency Medicine
Sepsis management
ST segment elevation myocardial infarction (STEMI) management
Stroke management
Department of Family Practice
Effectiveness of Family Practitioner and Hospitalists Discharge Practices
Utilization of standardized processes and documentation for admission, transfer,
and discharge of acute care patients by Family Practitioners
Department of Geriatric Medicine
Appropriateness and effectiveness of the medical care provided at the initial
assessment/new consult appointment to outpatients referred with a suspected
diagnosis of dementia
Department of Hospitalists
Utilization of the regional pre-printed orders for Geriatric Delirium (in acute care) by Hospitalists at the Royal Columbian (RCH) and Eagle Ridge Hospitals (ERH)
Clinical Audit of Hospitalist Care Processes Department of Medicine
Division of Endocrinology: Management of thyroid nodules
Division of Endocrinology: Diabetes in pregnancy outcomes
Department of Medicine, Division of Gastroenterology: Endoscopic Ultrasound
Chart Review
Division of General Internal Medicine: Concurrence of ECG reader interpretations
Division of General Internal Medicine: Clinical audit of the medical care provided to
patients presenting with Acute Coronary Syndrome (ACS)
Division of Infectious Diseases: Appropriateness and effectiveness of the medical
care provided by the Home IV Program to patients with diabetic foot infection.
Division of Nephrology: Clinical audit of primary reviews
Division of Neurology: Hot stroke rates and tissue plasminogen activator (tPA) use
for Stroke in Fraser Health Hospitals

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 7 of 210
Division of Neurology: Regional Stroke Scorecard
Division of Neurology: Audit of EEG Reporting Standards
Division of Neurology: Physician Teamwork
Division of Oncology: Completion of FHA MOST form on admission to SMH Oncology
Unit
Division of Respirology: Bronchoscopy reporting
Division of Respirology: Survey of physician “burnout” within the Division of Respirology
Eagle Ridge Hospital: Time to cardiac catheterization for ACS/NSTEMI patients at Eagle Ridge Hospital (ERH)
Department of Medical Imaging
Medical Imaging Examination Report Turn Around Time
Imaging Guided Lung Biopsy Yield and Results – Follow Up Audit
CT Pulmonary Angiography Diagnostic Yield
Critical Results Accreditation Standard Compliance Audit
XR and CT Utilization Trends in the Emergency Room (ER) Setting
Quality of Order Entry
Lower Mainland Standardization of Head CT Protocol
Thyroid Biopsy Yield
Recommendation Rates
Breast Imaging Reporting and Data System (BIRADS) Final Assessment Category –
Third Audit
Department of Mental Health and Substance Use
Division Tertiary Psychiatry: Polypharmacy and high dose antipsychotics
Division Tertiary and Geriatric Psychiatry: Anticholinergic load in patients admitted
to tertiary geriatric psychiatry units
Department of Surgery
Surgical safety checklist audit
Review of surgical site infections as identified by National Surgical Quality Improvement Program (NSQIP), RCH and ERH Orthopedics
Division of General Surgery: Breast cancer surgery
Division of Vascular Surgery: Effectiveness of complex endovascular aneurysm repair (EVAR) review policy
Division of Vascular Surgery: Effectiveness of Vollmar ring endarterectomy as an alternative to arterial bypass.
Division of Vascular Surgery Can a cardiac risk predictive index be used to determine need for High Acuity Monitoring in Vascular surgery.

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 8 of 210
PEER REVIEW AND CHART REVIEW
The following departments have implemented formal, continuous peer review or chart review programs. Department of Emergency Medicine
72 hour returns Department of Geriatric Medicine Department of Laboratory Medicine & Pathology
Anatomic Pathology quality management program Department of Medical Imaging
Peer Review Program Department of Mental Health and Substance Use Department of Surgery, NSQIP Department of Surgery, Division of Plastic Surgery
MORBIDITY & MORTALITY (M & M) REVIEW
Most M & M review is taking place at a local hospital level and appropriate medical quality committees have been established to ensure these activities are conducted in accordance with the requirements of Section 51 of the Evidence Act.
In accordance with the third HAMAC Quality Goal, over the coming year, departments will look to develop and implement trigger tools, such as the IHI Global Trigger Tool, to enable discussion and learning from preventable deaths.

EXECUTIVE SUMMARY Clinical Audit Annual Report
Page 9 of 210
PERFORMANCE REVIEW/CLINICAL PERFORMANCE APPRAISAL
Department of Cardiology
Cardiac Services BC Annual Cardiac Surgery Review
Cardiac Services BC Annual Interventional Cardiology Review
Trans-arterial Aortic Valve Implantation Program
Department of Emergency Medicine
Physician activity and utilization report
Department of Hospitalists Department of Medicine, Division of Gastroenterology
Colon Cancer Screening Program: Physician Quality Audit – Direct Observation of
Procedural Skills
Department of Mental Health and Substance Use Department of Obstetrics and Gynecology

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 10 of 210
Background At the February 22, 2011, meeting of the Board of Directors of the Fraser Health Authority, the Board passed four resolutions related to clinical audit, peer review and quality improvement. Of these resolutions two related directly to clinical audit requesting HAMAC to:
ensure that all regional departments develop a process of clinical audit by peer review
that is appropriate to the clinical function of the department and ensures continuing
improvement in the quality of medical care in the department.
ensure all members of the medical staff participate in regular clinical audit of their
clinical practice by peer review both within the process developed by regional
departments and as required by relevant accreditation processes, with a report of that
participation made available to the Board in the quarterly reporting by HAMAC.
Three years later, in this third annual report dated October 2014, an update on the implementation of these recommendations and the activities undertaken by HAMAC and the regional departments to monitor and improve the medical quality of care provided by their members is provided.
Fraser Health Authority Medical Advisory Committee (HAMAC) Chair: Dr. Peter Doris Vice-Chair: Dr. Anne Clarke
Purpose Appointed by the Board of the Directors, the Health Authority Medical Advisory Committee (HAMAC) undertakes several critical functions including: making recommendations to the Board of Directors with respect to the cancellation,
suspension, restriction, non-renewal, or maintenance of the appointments and privileges of all members of the medical staff to practice within the facilities and programs operated by the Fraser Health Authority.
providing advice to the Board of Directors and to the CEO on: the provision of medical care within the facilities and programs operated by the
Fraser Health Authority. the monitoring of the quality and effectiveness of medical care provided within the
facilities and programs operated by the Fraser Health Authority. the adequacy of medical staff resources. the continuing education of the members of the medical staff. planning goals for meeting the medical care needs of the population served by the
Fraser Health Authority. the availability and adequacy of resources to provide appropriate patient care in the
Fraser Health Authority.

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 11 of 210
Duties Medical Administration
the HAMAC recommends chairs and members of standing committees to the Board and HAMAC ensures these committees function effectively including recording minutes of meetings
the HAMAC makes recommendations to the Board of Directors on the development, maintenance and updating of medical staff rules, policies and procedures pertaining to medical care provided within facilities and programs operated by the Fraser Health Authority
the HAMAC advises on matters pertaining to clinical organization, medical technology, and other relevant medical administrative matters
Appointments and Privileges the HAMAC reviews recommendations from the HAMAC Credentials and Privileges
Committee concerning the appointment and review of medical staff members including the delineation of clinical and procedural privileges
the HAMAC makes recommendations to the Board of Directors concerning the appointment and review of medical staff
the HAMAC makes recommendations to the Board of Directors regarding disciplinary measures for violation of Bylaws, Rules or policies of the medical staff.
the HAMAC may require a member of the medical staff to appear before the committee whenever necessary to carry out its duties.
Quality of Care
the HAMAC receives, reviews and provides advice on reports from quality review bodies and committees concerning the evaluation of the clinical practice of members of the medical staff
the HAMAC reviews recommendations concerning the establishment and maintenance of professional standards in programs funded and operated by the Health Authority in compliance with all relevant legislation, Bylaws, Rules, and policies of the medical staff
the HAMAC submits regular reports to the Board of Directors and the CEO on the quality, effectiveness and availability of medical care provided, in relation to professional standards, in facilities and programs operated by the Health Authority
the HAMAC makes recommendations where appropriate concerning the quality of medical care in the Health Authority
the HAMAC makes recommendations where appropriate concerning the availability and adequacy of resources to provide appropriate patient care in the Health Authority

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 12 of 210
Medical Staff Resource Planning the HAMAC reviews reports regarding human resource requirements required to
meet the medical, dental, midwifery and nurse practitioner needs of the population served by the Fraser Health Authority and following the review provides advice to the Board of Directors and the CEO
Professional and Ethical Conduct of Members of the Medical Staff
the HAMAC reviews and reports on any concerns related to the professional and ethical conduct of physicians to the Board of Directors, and, where appropriate, reports those concerns to the appropriate regulatory College
Continuing Medical and Health Education
the HAMAC advises on and assists with the development of formally structured ongoing programs in continuing medical education and orientation and refresher training of medical staff
the HAMAC advises on and assists with programs in continuing education of other health care providers in the facilities and programs operated by the Health Authority
the HAMAC advises on, and makes recommendations concerning, the teaching and research role of the health authority
Physician Health and Wellbeing
the HAMAC advises on and assists with the development of formally structured ongoing programs in physician health and wellbeing
Composition The membership of HAMAC is described in the Medical Staff Rules, and includes representation from the following areas:
members of the medical staff who have been appointed to medical leadership positions within the Health Authority
members of the medical staff who have been elected by the medical staff of the Health Authority
the Chief Medical Health Officer of the Health Authority the Vice President Medicine of the Health Authority, who provides secretariat
services to the HAMAC the CEO of the Health Authority, who is a non-voting member other senior administrative or medical staff of the Health Authority as appropriate,
in a non-voting capacity The Chair and Vice-Chair of the HAMAC are appointed by the Board of Directors after considering the recommendation of the HAMAC, and are selected from among the members of the Active Medical Staff. The Chair or Vice-Chair of HAMAC provides a report to the Board of Directors and to the CEO on a regular basis. The Chair or Vice-Chair of HAMAC

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 13 of 210
attends meetings of the Board of Directors, and the appropriate committee of the Board, to participate in discussions pertaining to the purposes identified for the HAMAC.
Quality Agenda Health Authorities are responsible for ensuring the quality of care and services within their catchment area. The Board of Directors of the Health Authority is ultimately accountable for the quality of care in, and provision of, appropriate resources to the facilities and programs operated by the Health Authority. This includes having systems in place to monitor and report on the “quality agenda”. One important facet of the larger Fraser Health Authority (FHA) quality agenda is engagement of medical staff in quality management activity. It is important to recognize and understand how the interdependent relationships between the Board of Directors (of the HA), administration, medical staff, clinical staff and patients advances the quality agenda. The Medical Staff in Quality Agenda The FHA Medical Staff Organization exists as a means for the Board to apply its statutory authority to all members of the medical, dental, midwifery and allied health professions who are granted permits by the Board to practice their disciplines within FHA, and to maintain and support the rights and privileges of the Medical Staff as provided herein. The purpose of Medical Staff Organization is to:
ensure all members thereof are aligned with the FHA quality agenda - the provision of high quality patient care, and
provide advice to the Board in order to achieve the quality agenda and strategic directions of FHA.
HAMAC Representing the Medical Staff in the Quality Agenda The Medical Staff Organization fulfils this purpose through the (Health Authority) Medical Advisory Committee (HAMAC). On behalf of the medical staff and through representation from the Regional (Medical) Departments, acute care sites and Medical Staff Associations, HAMAC is responsible to meet the statutory obligations of the Medical Staff Organization. HAMAC is required to:
act in an advisory capacity to the FHA Board of Directors; be accountable for the quality of medical care provided in the programs and
facilities of FHA; assist in providing adequate and appropriate documentation for the purpose of
maintaining a health record for each patient; participate in relevant activities such as: quality improvement; risk assessment and
management; resource utilization; education and research; program development and evaluation; and
promote a high level of professional performance by medical staff.

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 14 of 210
Key Issues Addressed by HAMAC
Meeting date: October 9, 2013; November 13, 2013; December 11, 2013; January 8, 2014; February 12, 2014; March 12, 2014; April 9, 2014; May 14, 2014; June 11,2014; July 9, 2014.
In addition to receiving the Department quality reports that are summarized in the subsequent sections, the following issues and concerns have been presented to HAMAC for information, discussion, advice, and when appropriate, approval:
Hand Hygiene- physician compliance; members of HAMAC to become Hand Hygiene Auditors; completion of the Hand Hygiene Course to become a requirement for renewal of Medical Staff appointments.
Nursing Sensitive Adverse Events –providing feedback on the improvement plan and identifying how physicians can best support the improvement work.
Perioperative Information Systems (PIMS) – a high quality initiative. Incomplete health records – managing notifications of incomplete records and
suspensions Conflict of Interest Policy Antimicrobial Stop Orders Policy Vehicular access to SMH during marathon Medical Imaging 24/7 Reporting Medication reconciliation and discharge prescription forms Medication Reconciliation at Transitions in Care Policy Influenza Control Policy Reports distribution and transcription turn-around times Physician Workload Manager – health informatics Proof of immunity to MMR/Pertussis as criteria for appointment Attendance of members at MSA meetings Physicians as “handlers” in PSLS CME and health education – issue with videoconferencing and accessibility of
technology for case presentations across the region Corporate Care Standards Discharge summaries – timely completion; discharge summary template – guideline
for recommended contents; Discharge summaries and patient transfer/repatriation Physician Partnership Agreement (formerly Statement of Expectations) Antimicrobial Stewardship – Carbapenem Utilization; updates Procedural Privileging – Medical Imaging context Orders on patients transferred to another site Quality of care issues for admitted patients in Emergency without a MRP Reporting by Departments on “preventable deaths” Patient Care Quality Office Case Management Approach Medical Imaging Department Review Emergency Room Physician staffing shortages SMH patient coverage plans Revisions to MRP (acute care) Policy

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 15 of 210
HAMAC has also discussed and identified improvements to consider with its own processes: Creation of a summary report to the medical staff members – items of importance
and interest to be summarized and forwarded to the members. Consideration to be given to establishing a Credentialing Committee as a standing
sub-committee of HAMAC to conduct (more) detailed reviews of credentialing recommendations.
Search and Selection – HAMAC to consider an approach for the management of vacancies within departments and to provide detailed guidelines for the Search and Selection process.
HAMAC Department Quality Goals
Based upon a review of the topics, discussion and agenda items at HAMAC meetings over the past year, HAMAC has decided to set three quality goals for the coming year. The intention is for each Department/Division to address these quality goals as appropriate to their specialty. These goals are in addition to quality goals and initiatives that the Department/Division is undertaking.
Goal 1: 85% of all Discharge Summaries are dictated within 48 hours.
Goal 2: To increase the physician hand hygiene compliance rate by 15%.
Goal 3: To develop and implement trigger tools appropriate for each department to
enable discussion and learning from preventable deaths.
Department Quality Committees
The Department, Division, and local quality committee structures are the venue for engaging peers in discussion, and the foundation upon which medical quality improvement programs can be established. A significant undertaking for the regional departments has been determining quality committee structures that will enable quality activities to take place in a coordinated and planned approach, and to also ensure medical quality improvement activities are afforded protection under Section 51 of the Evidence Act.

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 16 of 210
All regional departments, with the exception of the newly established Department of Nurse Practitioners, have established a Regional Department Medical Quality Committee (RDMQC). Appointed by the Board on the recommendation of HAMAC, these standing medical committees are responsible for1:
evaluating, controlling and reporting on clinical practice in order to maintain and improve the safety and quality of patient care;
appraisal and control of quality of patient care;
professional practice evaluation and structured quality improvement of the care provided to patients by its members. This includes reviewing:
patient clinical outcomes
adverse clinical events arising from patient care
morbidity and mortality
mechanisms of care provision
providing advice to HAMAC with respect to patient care;
providing advice to Regional Department Heads and/or HAMAC with respect to the education of the Medical Staff and other health care professionals.
In addition to the RDMQC, some departments that have multiple divisions have established Regional Division Medical Quality Committees, and others have established medical quality committees at a site (local) level. This approach allows peers of sub-specialties within a division to have focused quality discussions and also aligns existing committees functioning at a local site level with regional department structures.
The accountability and reporting structure for the medical quality committees is illustrated in figure 1.
Figure 1 – Accountability and reporting structure.
1 Regional Department Medical Quality Committee Terms of Reference
Fraser Health Authority Board of Directors
Fraser Health Authority Medical Advisory Committee
Regional Department Medical Quality Committee
Division based Quality Committees Site based Quality Committees

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 17 of 210
Each regional department provides detailed reports to HAMAC outlining the medical quality improvement activities undertaken. Reporting occurs two times per year according to a predefined schedule (figure 2).
Figure 2 - Schedule of Reporting By Regional Departments to HAMAC Regional Department Month for Reporting
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec
Medical Imaging X X
Lab Medicine & Pathology X X
Medicine X X
Critical Care X X
Cardiology X X
Surgery X X
Anesthesiology X X
Obstetrics & Gynecology X X
Emergency Medicine X X
Mental Health & Addictions X X
Family Practice X X
Hospitalists X X
Pediatrics X X
Geriatric Medicine X X
Infection Prevention & Control & Public Health
X X
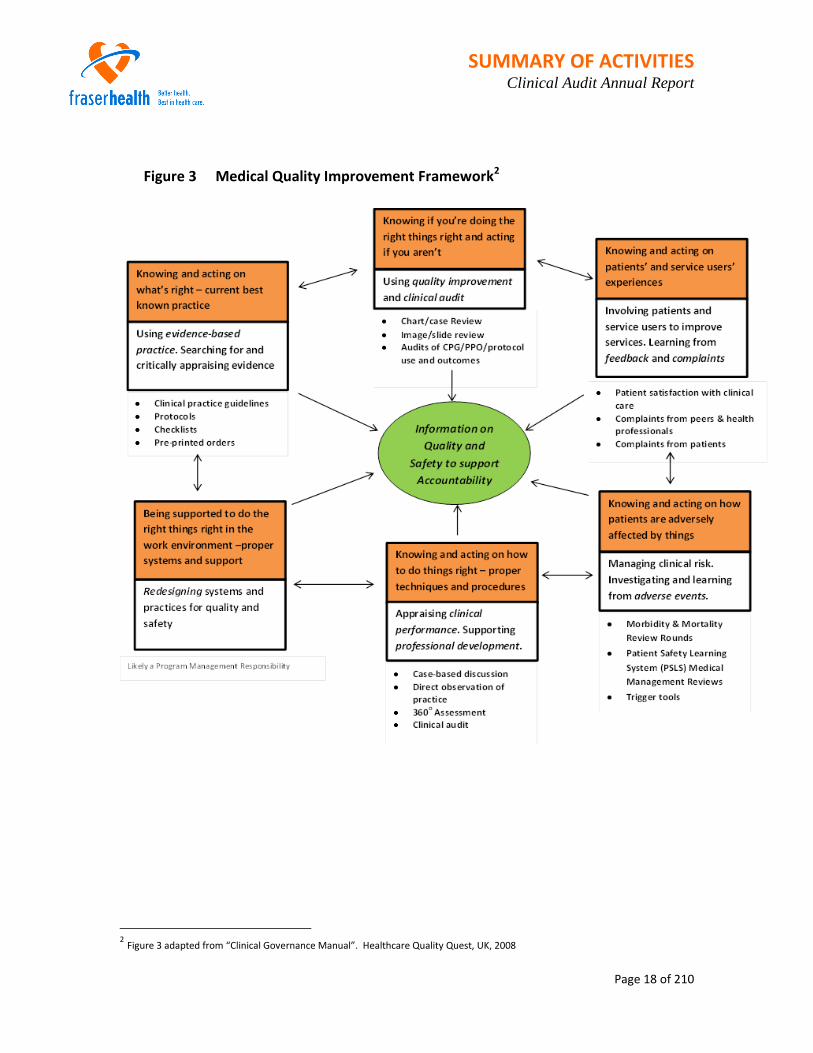
The Medical Quality Improvement Framework
The medical quality improvement framework (Figure 3) is used by Departments as an effective tool to guide discussions about medical quality improvement and to categorize activities undertaken. In summary, medical quality improvement activities focus on improving the medical management of the patient by answering key questions:
Do we know what the right things are to provide clinically effective care?
Are we doing the right things right?
Do we know what patients’ experiences have been with the medical aspects of their care?
Do we know what adversely affects patients?
Is the medical staff currently competent and supported through professional development?
How do we know?
SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 18 of 210
Figure 3 Medical Quality Improvement Framework2
2 Figure 3 adapted from “Clinical Governance Manual”. Healthcare Quality Quest, UK, 2008
SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 19 of 210
Clinical Audit – Defining, Identifying and Implementing
Clinical audit is a quality improvement process that seeks to improve patient care and outcomes through systematic review of care against explicit standards/criteria and the implementation of changes in practice if needed.3 Clinical audit has 3 key elements:
Measurement – measuring a specific element of clinical practice
Comparison – comparing results with the recognized standard/criteria
Evaluation – reflecting on the outcome of the audit and where indicated, changing practice accordingly
By conducting a clinical audit current clinical practice can be measured and compared objectively with established good practice, and if necessary, enable actions to be taken to improve care provision. As part of a comprehensive medical quality improvement program, clinical audit can:
provide evidence of current practice against regional department/provincial/national/ international guidelines or standards;
assess how closely local practice resembles recommended practice;
establish if you are actually doing what you think you are doing;
reinforce the implementation of evidence-based practice; and,
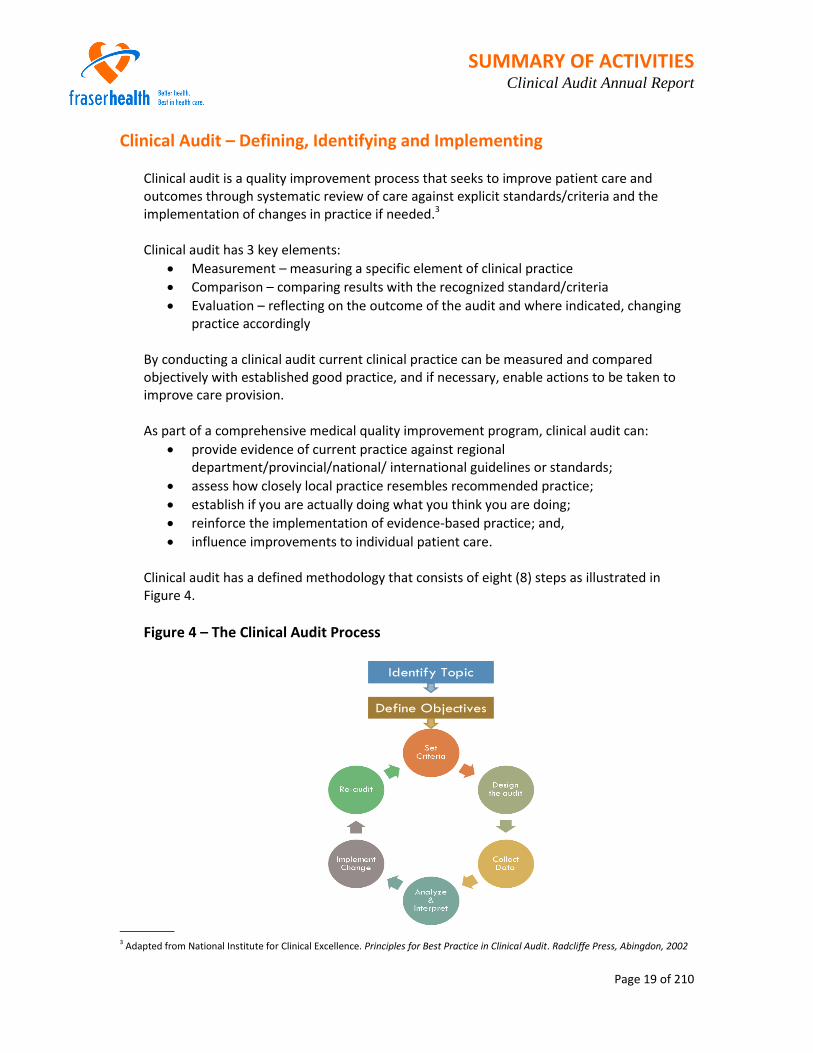
influence improvements to individual patient care. Clinical audit has a defined methodology that consists of eight (8) steps as illustrated in Figure 4.
Figure 4 – The Clinical Audit Process
3 Adapted from National Institute for Clinical Excellence. Principles for Best Practice in Clinical Audit. Radcliffe Press, Abingdon, 2002
Identify Topic
Define Objectives

SUMMARY OF ACTIVITIES Clinical Audit Annual Report
Page 20 of 210
The first two steps in the clinical audit process set the direction for all subsequent steps and activities. In identifying the topic and defining the audit objectives, it is crucial that the topic has value and relevance to the department/division members, and that the objectives focus on improving the medical quality of care. Departments and divisions have engaged in the discussion about clinical audit – what it is, why it is important, and identifying topics of interest. For those departments that have multiple divisions such as Medicine, clinical audits have been identified and implemented at a division level. Once the topic has been selected by the department/division, a physician champion or steering committee is established to continue the work of designing and implementing the audit. An update on clinical audit activities of each regional department/division is provided in the Department Summaries section of this report.
Morbidity and Mortality (M & M) Review – Policy, Procedures and Process
Morbidity and Mortality Review (M & M) is a well-established quality improvement process that answers the question “How could we have prevented this?” by reviewing patient cases and generating discussion. With this process, patient cases are selected for review using established “trigger tools” or screening criteria. The process for reviewing the patient case will vary but typically will involve presentation of the patient case to a group of peers who will discuss the case and generate recommendations to prevent recurrence. Provided the process of review is conducted in a supportive collegial environment, significant learning and improvements to patient care can result. Most M & M review is taking place at a local hospital level and appropriate medical quality committees have been established to ensure these activities are conducted in accordance with the requirements of Section 51 of the Evidence Act. In accordance with the third HAMAC Quality Goal, over the coming year, departments will look to develop and implement trigger tools, such as the IHI Global Trigger Tool, to enable discussion and learning from preventable deaths.

Department Summaries Clinical Audit Annual Report
Page 21 of 210
Anesthesiology Regional Department Head: Dr. John Ramsden
Regional Department Medical Quality Committee Activities The Department of Anesthesiology has established a Regional Department Medical Quality Committee with site based subcommittees.
Meeting Dates: February 18, 2013, March 18, 2013, June 17, 2013, September 16, 2013, November 2013
Clinical Audit
Operating Room (OR) start times are being gathered, and will be reported and broken down by hospital and contributing factor. OR hold times are being gathered, and will be reported and broken down by hospital and contributing factor. Clinical reports from sites currently using CPA are being designed and will be reported. Potential reports could include items such as “high glucose, not treated”, “insulin given, no labs”, “low glucose, not treated”, “red cells given, high hematocrit”, “red cells given, no hemoglobin or hematocrit”
Morbidity & Mortality Review Morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. 3 patient cases that had poor outcomes were selected for review. Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Surgical program to revisit provision of adequate on-call coverage for vascular surgery at SMH Communicated
2. Extended Post-Anesthesia Care Unit (PACU) at SMH be used for observation after major and/or emergent surgical cases
Complete

Department Summaries Clinical Audit Annual Report
Page 22 of 210
Learning Point / Recommendation
Status of Implementation
3. Patients with emergency tracheostomy for airway obstruction be sent to SMH EPACU for 24 hours for tracheostomy care.
Complete
4. Patients should receive adequate fluid resuscitation post contrast dye to avoid renal injury Communicated
5. Each elderly patient needs to be considered individually re suitability for each hospital Implemented
6. Pre Admission process needs to be improved - consult request needs to be emphasized In progress
7. FHA should track unexpected transfers out of community hospitals
In progress. Request sent to SIS
8. Hospitals should obtain means of assessing optimal fluid loading
In progress – Cardio Q vs. P pressure monitoring
9. Pulse pressure monitoring – optimal fluid loading – inherent part of Enhanced Recovery After Surgery (ERAS)
Looking at cost of systems
Evidence Based Practice/Medical Management Tools Obstructive Sleep Apnea Guidelines The Guideline has been finalized. In use at Abbotsford Regional Hospital and Cancer Centre (ARHCC), education completed at Chilliwack General Hospital (CGH) with rollout within weeks. The anticipated completion at all hospital will be the end of 2014. Significant education required for all hospitals in nursing. PATIENTS AT RISK: Care from discharge from PACU to discharge from hospital remains a significant problem. Resources at each hospital are significantly different. Planned monitoring equipment that may mitigate this risk at certain hospitals is unavailable due to funding and resource issues. Alternative strategies to prevent poor outcomes may result in increased costs secondary to extended PACU stays, and/or OR’s held up for lack of PACU space.

Department Summaries Clinical Audit Annual Report
Page 23 of 210
Quality Improvement Initiatives AIMS (Anesthesia information management system) Centricity Perioperative Management (CPA):
This system is a comprehensive Anesthesia Information Management System (AIMS) that follows a patient from first contact to discharge from the Acute Pain Service. Its core is the recording of intraoperative data from patient monitors, but it also includes a comprehensive pre- operative assessment package and post- operative monitoring package. The AIMS project is the highest priority item for anesthesia quality assurance
Implementation complete at ARHCC, SMH, and Jim Pattison Outpatient Care and Surgical Center (JPOCSC). SMH and JPOCSC anesthesiologists adjusting to change. Funding approved for software purchase to finish PAC and OR modules at all FHA hospitals. Planned implementation at all hospitals by the end of fiscal year 2015/16. Completed implementation will allow the accumulation of specific metrics needed to drive appropriate standardized anesthesia care in FHA. In conjunction with MPOG, (international database) allows the recognition of potentially inappropriate care models resulting in patient harm that may not be picked up locally because of insufficient incident rate. Currently exploring options with regards to MPOG and/or NACOR participation.
Operating Room Crisis Checklists:
Every anesthesia machine in FHA is being provided with a plasticized copy of the Safe Surgery OR crisis checklist to assist in the management of intraoperative crisis. They are currently being revised to take in to account FHA specific systems.
PAC redesign:
Phase one of pre admission clinic redesign using a LEAN model has now been completed at each hospital in FHA except for Delta Hospital (DH). We are now embarking on re visiting each location and assessing where we have been successful and where we have failed in achieving the stated goals. As part of the next phase of PAC redesign we are currently building the PAC module of CPA which will further standardize the gathering of information pre operatively on FHA patients and allow for better risk stratification and intra op management.

Department Summaries Clinical Audit Annual Report
Page 24 of 210
Supporting Professional Development
Regional Advanced Cardiovascular Life Support (ACLS) training specific to anesthesia providers implemented throughout FHA. Voluntary completion encouraged every 5 years.
An assessment was completed which showed that this project was determined to be of some value. Further courses are now being organized. Looking at ASA as another means of ACLS training.

Department Summaries Clinical Audit Annual Report
Page 25 of 210
Cardiology Regional Department Head: Dr. Gerald Simkus Medical Quality Committee Activities The Department of Cardiology has established a Regional Department Medical Quality Committee with five permanent subcommittees. The subcommittees are structured to encompass both division focused activities and hospital site locations.
Regional Department of Cardiology Medical Quality Committee Meeting dates: November 14, 2013 General Cardiology Quality Subcommittee, Abbotsford Regional Hospital and Cancer Centre General Cardiology Quality Subcommittee, Surrey Memorial Hospital Meeting dates: December 2 2013, January 6, 2014, January 20, 2014 Interventional Cardiology Quality Subcommittee, Royal Columbian Hospital General Cardiology Quality Subcommittee, Royal Columbian Hospital Cardiac Surgery Quality Subcommittee, Royal Columbian Hospital Meeting dates: October 24, 2013, November 28, 2013, January 23, 2014, February 27, 2014
Clinical Audits 1. Title: Clinical Audit to determine the degree of concurrence of ECG Reader Interpretations.
Division: General Cardiology and General Internal Medicine Phase:
Planning Designing Data Collection Analysis Reporting
Background: The Divisions of General Cardiology and General Internal Medicine are undertaking a collaborative clinical audit that will examine the degree of concurrence of ECG Reader interpretation between all ECG readers. The “ECG Peer Review Process” has been designed and agreed to by both Cardiologists and Internists and will be conducted in 2 phases.
Phase 1 – ECG peer review and education ECG Peer Review:
1. ECG selection:

Department Summaries Clinical Audit Annual Report
Page 26 of 210
20 abnormal ECGs from each ECG reader will be reviewed 2x per year for a total of 40 ECGs per reader per year.
ECGs will be selected from all sites (not just MUSE sites).
The ECGs for review will be "blinded" - all identifying information such as patient name and ECG reader name will be removed.
2. ECG Review
Each ECG will be reviewed by 1 member from the ECG Peer Reviewer pool. The pool will consist of 10 volunteer cardiologists who will over-read the ECG and record their determination as: "agree completely" or "agree mostly" or "disagree".
The "agree completely" and "agree mostly" will have no further action.
The "disagree" will proceed to review by the ECG Peer Review Committee.
The ECG Peer Review Committee will be Chaired by Dr. John Lemaitre and have as membership: Dr. Lemaitre; 1 cardiologist from SMH; 1 cardiologist from ARH; and 2 members from General Internal Medicine.
The entire Committee will over-read the ECGs brought forward as "disagrees" and record their determination as a Committee.
In reviewing the ECGs the Committee will also identify ECGs that have educational value and can be used as "seeded cases" for phase 2
3. Results Reporting:
The results of the ECG peer review process will be submitted: for cardiologists to Dr. Kornder; for internists to Dr. Shaw.
Drs. Kornder and Shaw will provide feedback to their respective members of individual performance and aggregate performance.
4. Addressing “outliers”
For those individuals identified as "outliers", it is proposed that a greater number of ECGs will be over-read. No definition of “outlier” is proposed at this time as the group recommends that the anonymized and aggregate results are reviewed first to see what overall performance of FHA ECG readers is.
5. Implementation
The Cardiology program will provide the cardiac technologists to support and operationalize the ECG peer review process.
Education: To support improved practice, ECG education will be provided on a regular and
continuous basis through virtual ECG meetings, circulating ECGs as "ECG of the Month" and/or having ECG rounds.
ECGs identified by the ECG Peer Review Committee as having educational value will be one source of ECGs for presentation.

Department Summaries Clinical Audit Annual Report
Page 27 of 210
Phase 2 – Enhanced ECG peer review
Once Phase 1 has been implemented successfully, an enhanced Phase 2 will be implemented.
Phase 2 would involve seeding "control" ECGs into the workflow of ECG readers. The control ECGs would be selected by the ECG Peer Review Committee.
2. Title: Clinical audit of the medical care provided to patients presenting with Acute Coronary
Syndrome (ACS) Division: General Cardiology and General Internal Medicine Phase:
Planning Designing Data Collection Analysis Reporting
Background: The Divisions of General Cardiology and General Internal Medicine are undertaking a collaborative clinical audit that will examine the medical care provided to patients presenting with Acute Coronary Syndrome (ACS).
Data collection strategy: A retrospective chart review will be conducted on 50 charts at each of the 8 sites as follows: For Cardiology: Surrey Memorial Hospital (SMH), Abbotsford Regional Hospital (ARH) and Royal Columbian Hospital (RCH) For Internal Medicine: Burnaby Hospital (BH), Ridge Meadows Hospital (RMH), Eagel Ridge Hospital (ERH), Delta Hospital (DH), Langley Memorial Hospital (LMH), Peace Arch Hosptial (PAH) Note: The sites of Mission Memorial Hospital (MMH), Fraser Canyon Hospital (FCH), and Chilliwack General Hospital (CGH) will not be included in this audit due to the low volume of patient cases. Each chart will be reviewed to determine the extent to which the following criteria are met:
History/Consult dictated and on chart within 24 hours
Medications within 24 hours of admission: ASA
Antiplatelets
Beta Blockers
RAAS Blockers
Statins Medications At Discharge: ASA
Antiplatelets
Beta Blockers
RAAS Blockers
Statins

Department Summaries Clinical Audit Annual Report
Page 28 of 210
Smoking Cessation discussion documented Cardiac Rehab referral discussion documented Discharge Summary in EMR within 24 hours of discharge Follow up plan documented and includes: Driving
Sex
Work
GP appointment
Specialist appointment
Readmission for any reason within: 30 days
6 months
3. Title: Appropriateness and Effectiveness of the medical care provided to patients receiving
implantable cardiac electrical devices (ICED).
Phase:
Planning Designing Data Collection Analysis Reporting Background:
A structured provincial evaluation of electrophysiology procedures and heart rhythm device implantation and management similar to the valuations for cardiac surgery and interventional cardiology has not yet been developed for electrophysiology and device implantation. A local assessment has been initiated:
Objectives: 1. Assess the extent to which patients are receiving appropriate care:
Was a pacemaker indicated? Were other alternatives more appropriate?
2. Assess the extent to which patients are receiving effective care: Did the patient receive the optimal type of pacemaker?
3. Determine where patients are receiving follow-up care. Case selection method: All patients who received an implantable cardiac electrical device (pacemakers) from November 1, 2013 – December 30, 2013 at Fraser Health facilities (Royal Columbian Hospital and JPOSC) through the ICED Program, will be included. It is anticipated that this will result in 200 patient cases being reviewed.

Department Summaries Clinical Audit Annual Report
Page 29 of 210
Methodology: This will be a prospective audit of patients having received implantable cardiac electrical devices (pacemakers) at Fraser Health facilities (Royal Columbian Hospital and JPOCSC) through the ICED Program. Sources of Information: Data will be collected through the review of patient referral information, records, and the BC Pacemaker Registry that includes:
Outpatient referrals: Referral package: referral form, consult notes/letters, medications list, ECGs, rhythm strips. Inpatient referrals: Pre-procedure consult notes for inpatients on 2S, Meditech information Post-procedure: Procedure notes Follow-up information obtained through the BC Pacemaker Registry
Case review and data collection: Cases will be reviewed, and data collected, by Dr. John Lemaitre. In the event that Dr.
Lemaitre requires a case to be reviewed by a second reviewer, Dr. Jorge Bonet will review the case
4. Title: Appropriateness of Interventional Cardiology Procedures
Division: Interventional Cardiology, Royal Columbian Hospital Phase:
Planning Designing Data Collection Analysis Reporting
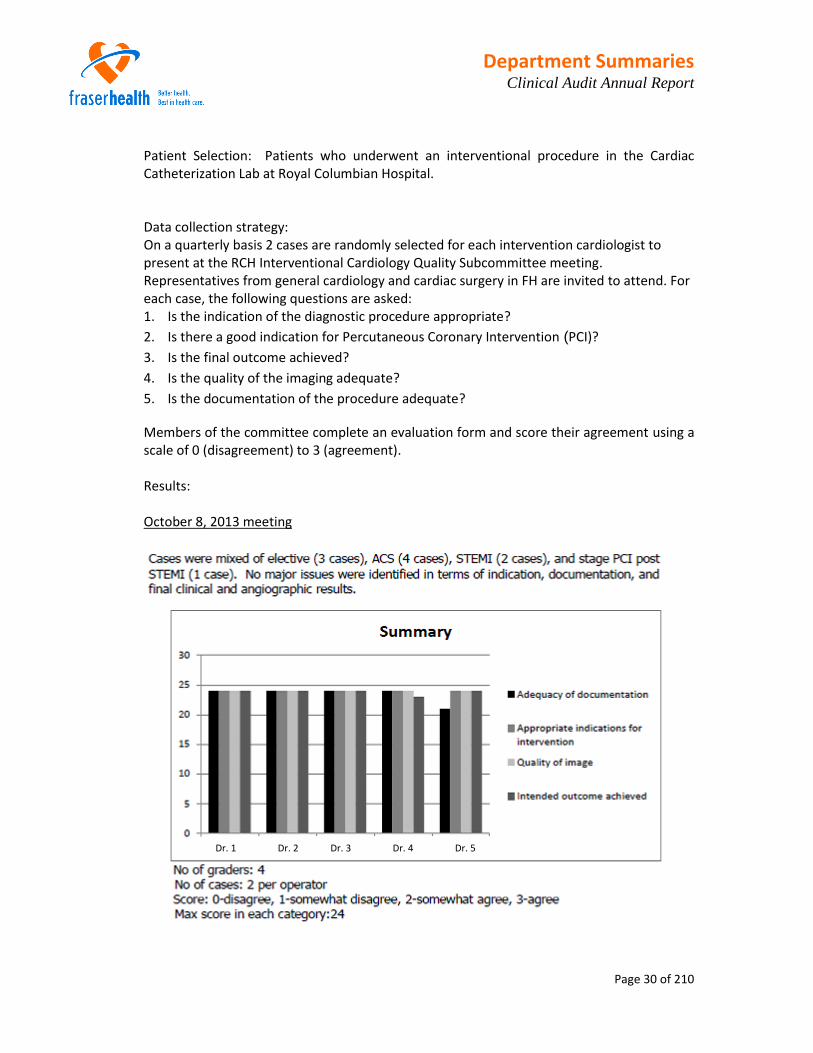
Background: On a quarterly basis the RCH Interventional Cardiology Quality Subcommittee undertakes case reviews to ensure that the best possible care and outcomes are delivered to cardiac patients and to ensure the adherence to clinical practice guidelines for patients who undergo procedures in RCH cardiac catheterization laboratories.
Objectives: The specific objectives for the case review include an independent evaluation of:
Adequacy of documentation
Appropriateness of indication for intervention
Quality of image
Intended outcome achieved
Department Summaries Clinical Audit Annual Report
Page 30 of 210
Patient Selection: Patients who underwent an interventional procedure in the Cardiac Catheterization Lab at Royal Columbian Hospital.
Data collection strategy: On a quarterly basis 2 cases are randomly selected for each intervention cardiologist to present at the RCH Interventional Cardiology Quality Subcommittee meeting. Representatives from general cardiology and cardiac surgery in FH are invited to attend. For each case, the following questions are asked: 1. Is the indication of the diagnostic procedure appropriate?
2. Is there a good indication for Percutaneous Coronary Intervention (PCI)?
3. Is the final outcome achieved?
4. Is the quality of the imaging adequate?
5. Is the documentation of the procedure adequate?
Members of the committee complete an evaluation form and score their agreement using a scale of 0 (disagreement) to 3 (agreement). Results: October 8, 2013 meeting
Dr. 1 Dr. 2 Dr. 3 Dr. 4 Dr. 5

Department Summaries Clinical Audit Annual Report
Page 31 of 210
November 30, 2013 meeting
February 25, 2014 meeting
Dr. 1 Dr. 2 Dr. 3 Dr. 4 Dr. 5

Department Summaries Clinical Audit Annual Report
Page 32 of 210
5. Title: The Appropriateness of Diagnostic Cardiac Catheterizations and Percutaneous
Coronary Interventions at the Royal Columbian Hospital: A Quality Assurance Project.
Lead: Dr Jahangir Charania
OBJECTIVE: To prove that patients undergoing diagnostic cardiac catheterization (DCC) at the Royal Columbian Hospital are appropriate for this procedure and that patients undergoing percutaneous coronary intervention (PCI) at the Royal Columbian Hospital are appropriate as defined by the American College of Cardiology (ACC). Hypothesis: Patients undergoing DCC and PCI at the Royal Columbian Hospital are appropriately having these procedures performed. A data request has been submitted to Cardiac Services BC

Department Summaries Clinical Audit Annual Report
Page 33 of 210
Morbidity & Mortality Review
Surrey Memorial Hospital At SMH during the period of October 2013, to February 2014, “Interesting Case” (morbidity and mortality) review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. 3-6 patient cases were reviewed per session. Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
No systematic issues were identified; however, wait times for cardiac procedures including surgery, and cardiac catheterization remain a concern.
Royal Columbian Hospital Multidisciplinary Mortality and Morbidity Review: Formal rounds for the purposes of evaluating and improving the quality of patient care provided are conducted monthly. Participation is approximately 15 members, including Cardiac Surgery, Interventional Cardiology, Clinical Cardiology, Cardiac Anesthesia, CSICU staff, and nursing staff. All adverse outcomes of the surgical and interventional programs as well as clinical outcomes are reviewed. 4-6 Case are reviewed per session Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
No systematic issues were identified. Weekly Clinical Rounds: Attendance is approximately 30, including clinical cardiology, interventional cardiology, cardiac surgery and medical imaging physicians nursing personnel and administration. Problem, complex and interesting cases are presented to the department for discussion of management and outcomes. This currently includes teleconferencing to Abbotsford Hospital. Extending teleconferencing to Surrey Hospital is under discussion. Six to 12 cases are presented each week. No systematic issues were identified
Abbotsford Regional Hospital
At ARH during the period of October 2013, to February 2014, “Interesting Case” (morbidity and mortality) review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. 3-6 patient cases were reviewed.

Department Summaries Clinical Audit Annual Report
Page 34 of 210
Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
No systematic issues were identified
Evidence Based Practice/Medical Management Tools There have been a number of treatment protocols/clinical practice guidelines (CPGs), covering most major clinical syndromes, that have been developed and standardized protocols implemented.
Regional Standardized Order Sets
Initiatives 2013-2014 Aim Extent of Implementation Developing standardized documentation tools, e.g., 24 hour record to support a future electronic medical record (EMR)
To ensure that there is standardized documentation within the cardiac program and that the work supports the future implementation of the EMR.
In development
Developing CPG – Pre- and Post-Procedure Care in the Cardiac Catheterization Laboratory
This CPG provides best practice recommendations and evidence based standards for the pre- and post-procedure care of patients who need the diagnostic or interventional services provided in a cardiac catheterization laboratory (CCL). The Royal Columbian Hospital (RCH) is the only facility in Fraser Health (FH) with a CCL. This CPG will provide an overview of the pre-procedure patient assessment and preparation, post-procedure care, as well as the identification and interventions related to possible CCL complications.
In development
Developing CPG – Inter-hospital Transport for Cardiac Patients.
The goal of this CPG is to clarify the role and responsibility of the transport nurse and provide a guideline for delivering care to this patient population. In order to improve communication there is a hand-over document that is to be used when transporting a STEACS patient.
In development

Department Summaries Clinical Audit Annual Report
Page 35 of 210
Initiatives 2013-2014 Aim Extent of Implementation Developing CPG – Care of patients needing cardioversion
This CPG will provide best practice recommendations and evidence based standards for patients having a cardioversion
In development
Developing CPG – Care of patients within the Cardiac Surgery Intensive Care Unit
This CPG will provide best practice recommendations and evidence based standards for the pre- and post-operative care of patients who need cardiac surgery. The RCH is the only facility in FH that provides this level of service and care.
In development
Developed Clinical Practice Guideline (CPG) – Care and Management of Patients Requiring Implantable Cardiac Electrical Devices (Permanent Pacemaker, Implantable Loop Recorder, Implantable Cardioverter Defibrillator, Cardiac Resynchronization Therapy)
This document provides a guideline for ICED patient pre-procedure assessment and preparation as well as post-procedure care. Applicable to: All Fraser Health (FH) acute in-patient units (referring sites) providing ICED pre-procedure care to patients awaiting procedure. The two (2) FH designated ICED implanting sites providing intra-procedure and immediate post-procedure care; Royal Columbian Hospital (RCH) and Jim Patterson Outpatient Care and Surgery Centre (JPOCSC), All FH acute in-patient units (referring sites) providing ICED post-procedure care to patients returning from the implanting site. Does not include: Neonatal/Pediatric populations
Fully implemented. Online access to the CPG is available through the Clinical Policy Office CDST library
Provided subject matter expertise to the development of the FH brochure led by the MOST Team “Making Informed Decisions about Cardio-Pulmonary Resuscitation (CPR)”
Made suggestions that more fully addressed the cardiac patient population
Fully implemented

Department Summaries Clinical Audit Annual Report
Page 36 of 210
Initiatives 2013-2014 Aim Extent of Implementation Implementing BC Ministry of Health 48/6 Model of Care
The 48/6 Model of Care for hospitalized adult patients in BC is an integrated care initiative which addresses 6 key care areas of functioning through patient screening and assessment (only where screening shows areas of concern) and which are then supported by the development (within 48 hours of the decision to admit) of an individualized Care Plan to address key areas of health for the senior.
Implemented in the cardiac program at ARH and SMH and by April 2014 at RCH as well.
Developed CPG – Cardiac Telemetry Monitoring (TM) in the Non-Critical Care Adult In-Patient Setting
A component of a multi-program multi-site partnership aimed at providing best practice recommendations and evidence based standards of care for the non-critical care adult in-patient who needs cardiac TM.
CPG go-live April 1st
, 2014 across all sites and all programs with TM. Online access to the CPG is available through the Clinical Policy Office CDST library
Provided subject matter expertise to the development of the FH Clinical Protocol – Intra-hospital Transport of High Acuity and Critical Care Patients
The purpose of the Protocol is to outline the minimum standard of care for intra-hospital transport for FH High Acuity and Critical Care patients.
Fully implemented. Online access to the CPG is available through the Clinical Policy Office CDST library
Developed Pre and Post CCL Pre-Printed Orders (PPOs)
Intended to support patient care and direct practitioners on how to bring evidence based practices (EBP) to patients.
Fully implemented
Developed PPOs for STEACS patient.
Intended to support patient care and direct practitioners on how to bring evidence based practices (EBP) to patients.
Fully implemented
Developed PPOs for Primary PCI Intended to support patient care and direct practitioners on how to bring evidence based practices (EBP) to patients.
Fully implemented
Developed PPOs for NSTEACS patient.
Intended to support patient care and direct practitioners on how to bring evidence based practices (EBP) to patients.
Fully implemented
Developed PPOs for Electrophysiology (EP) Patients
Intended to support patient care and direct practitioners on how to bring evidence based practices (EBP) to patients.
Fully implemented

Department Summaries Clinical Audit Annual Report
Page 37 of 210
Initiatives 2013-2014 Aim Extent of Implementation Reviewed/revised the Cardiac Surgery PPOs.
Intended to support patient care and direct practitioners on how to bring evidence based practices (EBP) to patients.
Fully implemented
Developed standardized patient discharge teaching
Intended to support standardized post-discharge patient care.
Fully implemented
Quality Improvement Initiatives 1. Fraser Health Authority Regional Acute Infarct Angioplasty Program Mortality Review.
Lead: Dr Gerald Simkus The Fraser Health Authority has had a regional acute infarct angioplasty program since 2003. The first three years of operation were published, describing procedure rates and overall mortality, which were comparable to other leading Canadian institutions. In order to further characterize the causes of mortality of patients with acute infarct angioplasty across the region, a review of all cases of mortality with patients with a diagnosis of ST segment elevation myocardial infarction has begun. Of the 3500 acute infarct patients identified in this time frame, approximately 200 cases will be reviewed, representing all patients 2010-2013 with a diagnosis of ST segment elevation patients who died. The goal of this review is to determine areas where system improvements could result in decreased mortality. While this is primarily a quality assurance exercise, it is anticipated that the results will be of interest more broadly. An expedited ethics approval has been received with a view to presentation of this data at the Canadian Cardiovascular Society Congress being held in Vancouver October 2014 with publication of the findings.
2. Causes Of Mortality And Morbidity After PCI In Fraser Health
Lead: Dr Albert Chan
HYPOTHESIS AND/OR STATEMENT OF INTENT Mortality and morbidity following percutaneous coronary interventions (PCI) could be related to multiple factors. We intend to perform a retrospective analysis of prospectively collected data to examine the frequencies and the causes of mortality and morbidity (blood product transfusion) in these patients in the contemporary interventional practice.

Department Summaries Clinical Audit Annual Report
Page 38 of 210
Outcomes after percutaneous coronary interventions (PCI) is considered as a surrogate markers for quality of care in interventional cardiology, and public reporting of outcomes is considered useful in determining the appropriateness and cost-effectiveness of procedures, and in helping general public to make informed decisions about health care choices. However, mortality and morbidity post-PCI are largely influenced by the severity of a patient’s illness and presentation, while those directly related to a PCI procedure is much less frequent. PCI-related death contributed to less than half of the overall post-PCI mortality in single-center study (1). Importantly, the reputations of an institution and a health care provider alike could be adversely affected by the disclosure of such data, leading to a tendency to avoid high-risk patients (e.g. ST-segment elevation myocardial infarction (STEMI), cardiogenic shock, post-cardiac arrest) who are most likely to benefit from PCI procedures. Mortality and morbidity after PCI procedures could be related to multiple factors, and these could be classified into PCI-related, cardiac-non-PCI-related, and non-cardiac-related categories. It is anticipated that the results will be available for presentation at the annual Canadian Cardiovascular Congress October 2014
3. Interventional Cardiology Checklist
A standard procedural surgical pause has been implemented in the cardiac catheterization lab. Formalization of a checklist pre-and post procedure is being developed.
Performance Review/Clinical Performance Appraisal
Cardiac Surgery
Cardiac Services BC Annual Cardiac Surgery Review For last 20 years, Cardiac Services British Columbia has conducted a comprehensive review of all cardiac surgery done in British Columbia. The cardiac surgery program at the Royal Columbian Hospital continues to have the highest acuity patients in British Columbia the risk adjusted outcomes are excellent and in line with other British Columbia Centers and there were no individual operator concerns. Previously a higher rate of blood transfusions peri-operatively was observed in 2008. The transfusion rate is now comparable to the other British Columbia centers. The most significant factor in this was a modification in peri-operatively practice patterns. A formal report from cardiac services BC quality committee to the Fraser Health Cardiac Sciences Quality committee is pending.

Department Summaries Clinical Audit Annual Report
Page 39 of 210
Interventional Cardiology
Cardiac Services BC (CSBC) Annual Interventional Cardiology Review
The annual provincial PCI meeting will be held in June 2014. This provides an in depth
review of outcomes across British Columbia. The previous database used had issues with
data quality and a new database has been in use for 1-2 years, with initial outcomes
analyses pending.
Trans-arterial Aortic Valve Implantation Program
Leads: Dr. Albert Chan, Dr. Daniel Wong
The provincial TAVI meeting was hosted by RCH in September 2013. The outcomes of RCH
group were presented by Dr. Albert Chan on behalf of the RCH team (Drs. D. Wong, T.
Latham, J. Charania). On average about 4 cases have been done each month. Thirty-day
mortality post-procedure was reported to be zero over the past 14 consecutive months. Re-
admission related to heart failure or valve-related problem was low (6.7%). Median hospital
stay was 5 days after the procedure. CSBC continues to oversee and restrict the funding and
scope of practice related to TAVI, and a provincial working group with RCH representation
will meet every 6 months to discuss these issues.
Participation in provincial VICOR group and planning first Provincial conference on Cardiac Revascularization. Leads: Dr. R Phillip and Dr. J Kornder CSBS has asked the Variation in Coronary Revascularization (VICOR) Group to look at overall cardiac revascularization in BC, and look for care pattern variation and explanations of variation to ensure that ALL patients get the correct revascularization.
Supporting Professional Development All members of the department are expected to participate in the Maintenance of Competence Program (MOCOMP) review. A survey is underway.

Department Summaries Clinical Audit Annual Report
Page 40 of 210
Critical Care Regional Department Head: Dr. Sean Keenan Regional Department Medical Quality Committee Activities Meeting Dates: April 18, 2013, May 16, 2013, June 18, 2013, September 25, 2013, October 30, 2013, December 17, 2013, January 28, 2014, February 18, 2014, March 11, 2014
Clinical Audits
1. Title: Critical Care Physician Compliance with Rounding Checklist Site: All sites with Intensive Care Units (ICUs)- (RCH, SMH, ARH, BH, RMH, PAH, LMH, CGH)
Phase:
Planning Designing Data Collection Analysis Reporting
Background: Care for the critically ill is complex and attention to detail very important. To ensure all aspects of care are considered on a regular basis, a checklist approach to daily patient rounds is proposed. This is comprised of care processes that have been demonstrated to improve patient outcomes including a daily review of sedation, ventilation plan, medication reconciliation, the need for invasive lines and a clear daily plan. In addition, it includes a review of family updates and barriers to patient transfer from the ICU. Objectives: Full compliance with the rounding checklist by all physicians working in the ICU Patient Selection: All ICU patients (at community hospitals may focus only on ventilated patients) Time period: Proposed to conduct ongoing audits … 1-2 months in duration. Data collection strategy: Prospective collection from rounding checklists Results: Each process included on the checklist is important to patient care and ensuring they are discussed on rounds will also ensure patients and their families are receiving best care and appropriate treatment, respectively.

Department Summaries Clinical Audit Annual Report
Page 41 of 210
0
20
40
60
80
100
A B C D E F
%
Physician
Rounding Checklist RCH Physician Compliance with
Rounding Checklist
0
10
20
30
40
50
60
70
80
90
100
SMH BH CGH
%
Compliance with Rounding Checklist
Audit 1
Audit 2
Audit 3
Audit 4

Department Summaries Clinical Audit Annual Report
Page 42 of 210
Actions: All sites are up and running, piloting their respective rounding checklists. Pilot collection of data for audit purpose is underway at most sites and some have submitted to Medical Quality Committee. The data is being reviewed at present. There are concerns that some sites are starting to slip on checklist use over the summer. Importance of refocusing on use of checklist and providing audits emphasized and accepted at September meeting. Physician participation rate: All physicians will participate.
2. Title: Switching from routine daily chest X-rays (CXRs) to on-demand CXRs
Site: Four larger ICUs (RCH, SMH, ARH and BH) Phase:
Planning Designing Data Collection Analysis Reporting Background: Traditionally CXRs have been done daily on ventilated patients in ICUs with the rationale that they allow early detection of potentially harmful events such as tube dislodgement, pneumothorax, etc. A number of studies have not demonstrated this to be true. Studies comparing CXRs on demand … ordered by physicians to address specific concerns … to daily morning CXRs have not shown any increased adverse events. More recently it has been recommended as part of the “Choose Wisely” campaign that we “Do not perform routine tests in the ICU, including routine daily CXRs”. As such, within FHA the move to on-demand CXRs has become a focus of the Medical Quality Committee. Objectives: To stop routine daily CXRs in our 4 larger ICUs (currently the 4 community sites do not do daily CXRs) and move to an on demand approach. Patient Selection: All ICU patients at RCH for our pilot study. Time period: Proposed to conduct ongoing audits in co-operation with the Department of Medical Imaging Data collection strategy: Approached RCH Department of Medical Imaging to obtain total number of CXRs conducted over past 6-12 months. This will be a crude approach to answering question as uptake during this period is expected to be gradual. In addition, will not be able to control for number of patients or those ventilated.

Department Summaries Clinical Audit Annual Report
Page 43 of 210
Results: We hope to see a reduction in total number of CXRs as a result in this change in practice that will avoid unnecessary movement of patients and associated risk of tube/line dislodgement and healthcare worker injury, reduction in radiation exposure (although this will be minor), and reduction in costs. Actions: Discussion initiated 6 months ago at Medical Quality Committee. Initial need to reassure physician representatives of safety and the fact that this has become a standard of care through review of literature and contact with local expert at Vancouver Coastal Health Authority. Through Program of Critical Care admission pre-printed orders are being changed to remove daily CXRs. The pilot project at RCH has relied upon discussions at Local Department Meeting and agreement that daily CXRs are not needed routinely. All Attending physicians have been encouraged to discontinue current order for daily CXRs and to reassess need for CXRs on the following daily as part of rounding process (item: review of daily blood work and CXR). While empirically there appears to have been a reduction in the number of CXRs we need to get more objective data and hope to partner with Medical Imaging to review data on CXRs over the last 6 months. Would plan to continue to follow these numbers over time to ensure ongoing compliance. Physician Participation Rate: All physicians will participate.
Morbidity & Mortality Review At the September 2012 Medical Quality Meeting the Committee recognized all 8 sites with ICUs as having their own formal Critical Care Morbidity and Mortality Review Committee chaired by the respective member for their hospital on the Medical Quality Committee. As such, all meetings will meet the criteria for Section 51 protection.
Abbotsford Regional Hospital and Cancer Centre
The Critical Care Department at ARHCC has been developing a process for conducting morbidity and mortality review rounds that will be piloted over the next several months. Patient cases will be selected for review using the following process and criteria.
Patient selection criteria:
Patient death in unit – expected and unexpected
Unexpected cardiac arrest
Unplanned extubation
Reintubation within 24-48 hours after planned extubation
Readmission to unit within 48 hours after discharge from unit
Acute respiratory distress syndrome (ARDS)
Complications of dialysis

Department Summaries Clinical Audit Annual Report
Page 44 of 210
Patients who meet at least one of the above criteria are recorded on the “Department of Critical Care ARH Morbidity and Mortality Identification Sheet” that is kept in an M & M Review binder in a secure location on the unit. Any member of the clinical team may record a patient in the binder. In unit deaths are classified as expected or unexpected, with an expected death defined as having occurred when the goals of the care have been changed to reflect impending patient death. On a quarterly basis, the Abbotsford Regional Hospital Department of Critical Care Morbidity & Mortality Review Committee will appoint a Reviewing Physician to conduct an initial review of the cases identified in the binder with the exception of deaths identified as expected. The Reviewing Physician will review the patients’ charts and prepare notes in preparation for presentation of the cases at the Abbotsford Regional Hospital Department of Critical Care Morbidity & Mortality Review Committee meeting. On a quarterly basis, a meeting of the Abbotsford Regional Hospital Department of Critical Care Morbidity & Mortality Review Committee will be convened. The Reviewing Physician will present each case for the purpose of:
discussing management decisions
discussing severity, causality and preventability of the event(s)
providing a learning opportunity
identifying opportunities to improve patient safety and quality of care.
In the case discussion, consideration will be given to whether any of the following contributed to the morbidity or mortality4:
Underlying disease
Treatments and procedures: including iatrogenic events (intrinsic to usual ICU procedures performed in accordance with standards of care) and nosocomial infections
Human error: including judgment, knowledge and technical skills
Equipment malfunction: including equipment failure and inadequate equipment
Work environment: communication problems, failure to provide or enforce policy/protocol, absence of policy/protocol, understaffing, poor task prioritization, inappropriate behaviour or action, lack of supervision, high-stress situation
Other: including lack of communication /coordination between ICU and other departments, patient’s condition (agitation, confusion), fatigue or burnout of caregivers
Unidentified and independent of the disease process or ICU procedures
The Department of Critical Care ARH Morbidity & Mortality Meeting Notes template will be used to record any recommendations arising from the review and to classify the event. The ARH M & M Committee met on March 2, 2014 for the purposes of evaluating and improving the quality of patient care provided. All deaths were reviewed and one case was selected for in-depth review. No recommendations were made, care was felt to be appropriate.
4 Ksouri et al. Impact of Morbidity and Mortality Conferences on Analysis of Mortality and Critical Events in Intensive Care Practice. American Journal of Critical Care, 2010;19:135-146

Department Summaries Clinical Audit Annual Report
Page 45 of 210
Expected Death Review
At the March 2, 2014
M&M rounds all patient deaths were review from November 1, 2013 to February 17, 2014. During this period 25 patients died (16.5% mortality rate). Of these 25, 18 occurred following family request to withdraw life support. 7 deaths occurred despite ongoing ICU care, 4 following cardiac arrests, 2 of massive GI bleeding and 1 of severe sepsis. At the M&M rounds the latter 7 deaths were reviewed. Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Need to ensure Critical Care involved earlier in patients deteriorating on the ward.
At present Patient Care Coordinators (PCCS) are called for Outreach patients. Critical Care physicians have asked to be made aware and attend these calls.
2. Improve medical imaging for severely morbidly obese patients.
Need to discuss with Medical imaging how patients with severe morbid obesity can be imaged in FHA.
Burnaby Hospital
In July 2012, the Critical Care Department at Burnaby Hospital commenced a morbidity and mortality review process. Patient cases will be selected for review using the following process and criteria. Patient selection criteria:
delay in care – medication, surgery, procedure
delay in patient transfer out for “higher level of care”
delay in patient transfer out to medical ward
complication of a procedure
iatrogenic complications
family dissatisfaction and/or complaint Patients who meet at least one of the above criteria are recorded in an M & M Review binder that is kept in a secure location on the unit. Any member of the clinical team may record a patient in the binder. Case will be reviewed by an assigned physician and presented at quarterly meetings.

Department Summaries Clinical Audit Annual Report
Page 46 of 210
The Burnaby Hospital M & M Committee met on February 13, 2014 for the purposes of evaluating and improving the quality of patient care provided. All cases that died in the ICU as well as other cases specifically identified by the ICU group from January 2013 to January 2014 were reviewed. These included both ICU and Internal Medicine cases. Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Delay in endoscopy for acute GI bleed Ongoing efforts to establish a GI Bleed Service.
2. Delay in referral to General Surgery and ICU.
Case identified for BH ER and Surgical M&M
3. Delay in CT imaging over holiday period Follow up with BH Medical imaging
4. Improve access to community advance directives
Follow-up by physician group and program team at BH
5. Ensure timely dictations on admission and
at time of death/discharge
ICU agree to follow this.
Royal Columbian Hospital
At present the Local Department Head is copied on all Death summaries and reviews these monthly. Those that appear to be of concern or interest are selected and the last attending physician is asked to provide a summary at the monthly business meeting for discussion. The first formal M&M round was completed in May, 2013. Between January and March 2013 there were a total of 530 admissions to Critical Care at RCH (235 to the ICU, 295 to the HAU). At total of 89 patients died (59 in the ICU and 30 in the HAU). The selection process for M&M review are less formal, patients to be identified either by the attending physician or LDH on review of death summary. One case was reviewed for the purposes of evaluating and improving the quality of patient care provided at the rounds:
Learning Point / Recommendation
Status of Implementation
1. Need to clarify appropriate response to patient found pulseless and no respiratory effort with a MOST designation for resuscitation.
Local Department Head to meet to discuss with Nurse Manager and consider bringing to RCH Multidisciplinary Healthcare Coordinating Committee (MHCC).

Department Summaries Clinical Audit Annual Report
Page 47 of 210
Surrey Memorial Hospital
At present, SMH conducts regular (monthly except summer) ICU rounds where selected cases are reviewed in a multidisciplinary setting. These rounds have been granted the status of an M&M review by the Critical Care Medical Quality Committee. In October, 2013 and January 23, 2014 the SMH Department of Critical Care conducted M&M rounds for the purposes of evaluating and improving the quality of patient care provided. Two cases were selected for review at the first round and one case at the second. Cases were selected as ones identified with concerning outcome, either unexplained death or significant morbidity Learning points and recommendations for improvement arising from the case reviewed, and the status of implementation is as follows:
Learning Point / Recommendation
Status of Implementation
1. Clostridium difficile (C diff) colitis can initially seem to respond to therapy but recur following an adequate course of therapy likely due to incomplete treatment.
Consider endoscopy to investigate recurrent sepsis in a patient with treated c diff.
2. Ischemic colitis when clinically probable requires laparotomy to exclude the diagnosis.
No specific further plans.
3. After nasogastric tube placement, any concerning appearance requires direct discussion with radiologist and follow-up.
Contact planned for further discussion with SMH Medical Imaging.
Chilliwack General Hospital During the period of May 2013 to December 2013 all deaths and transfers to higher level of care were reviewed in the ICU at CGH. Morbidity and mortality review rounds were conducted by the Chilliwack General Hospital M & M Committee for the purposes of evaluating and improving the quality of patient care provided on February 4, 2014. During the period reviewed 16 deaths occurred in the ICU, all patients had do not resuscitate orders and 5 had withdrawal of life support with 3 patients being on invasive mechanical ventilation and 4 on noninvasive ventilation.

Department Summaries Clinical Audit Annual Report
Page 48 of 210
8 patients were transferred to HLOC, 2 were ventilated. Issues of concern raised included: 1) Difficulty in getting tracheostomy done locally … exploring alternative to transfer 2) Weaning process was felt to be something that could improve … more attention to use of sedation and pain medications and use of daily spontaneous breathing trials. Peace Arch Hospital First meeting of M&M committee occurred October 16, 2013 for the purposes of evaluating and improving the quality of patient care provided. 1 case was reviewed in detail. Factors contributing to patient mortality were categorized under the cause and effect diagram illustrated below:
Learning points and recommendations for improvement arising from the case review included:
Physician issues Nurse issues
1) Early goal directive resuscitation measure for patient with septic shock 2) The benefit and risk of transferring unstable patient to higher level of care (HLOC) should be disused with HLOC intensivist 3) Proper documentation of patient clinical status daily in the progress notice
1) Proper sign out from ER nurse to ICU nurse 2) ICU order should be followed and not to go beyond the stated dose of sedative before informing MRP
Department Summaries Clinical Audit Annual Report
Page 49 of 210
Evidence Based Practice/Medical Management Tools 1. Rounding Tool/Checklist
A priority for the Department has been the development and implementation of a “rounding tool/checklist” that serves as a memory aid to the physician when conducting beside rounds. The use of this tool ensures consistent and comprehensive information regarding the patient’s care is reviewed and communicated during rounds. Rounding tools have been developed and implemented at all sites in Fraser Health. An audit of the rounding tool/checklist’s utilization has been planned periodically, ideally quarterly, at all sites but to date only 4 sites have reported … RCH, SMH, BH and CGH.
2. Handover Process
Critically ill patients are complex and transfer of care between physicians requires exchange of appropriate information to ensure care decisions are based on full understanding of patient. Handover needs to occur daily to the physician on call or first call for the night. In addition, at the 3 Tertiary sites and Burnaby Hospital with a closed ICU model, there is a weekly handover each Sunday. The processes used at each site has been reviewed and discussed at each meeting of the Medical Quality Committee.
Royal Columbian, Surrey Memorial, and Abbotsford Regional Hospitals
At present formal handover occurs reliably at the 3 Tertiary Sites with face-to-face handover, usually in form of bedside rounds on a daily basis late afternoon. In addition, weekly handover occurs Sunday afternoon from attending 2 physicians and the 2 ICU physicians beginning the next day. In addition, further handover occurs on the Monday morning for any new admissions overnight Sunday/Monday. Burnaby Hospital It has been agreed that all ventilated patients require phone or face-to-face handover. For non-ventilated, cardiac patients that are considered more routine a comprehensive daily note is considered adequate handover. Ridge Meadows, Langley Memorial, Chilliwack General and Peace Arch Hospitals The community sites have variable practices with Ridge Meadows Hospital refining a protected email update, but most sites using a more ad hoc method of contacting the on call physician about patients they are most concerned about. It has been agreed that all ventilated patients require phone or face-to-face handover. For non-ventilated, cardiac patients that are considered more routine a comprehensive daily note is considered adequate handover.

Department Summaries Clinical Audit Annual Report
Page 50 of 210
3. Follow-up of Higher Level of Care (HLOC) Transfers
At present Critical Care in Fraser Health is regionalized with published admission, discharge and transfer criteria for each site. At times, review of patients arriving at higher level of care sites by receiving sites raise concerns about pre-transfer care. While the PSLS should provide a means to address these concerns, it is not consistently used and is impersonal and at times slow to resolve concerns identified. A pilot study is almost completed at Surrey Memorial Hospital consisting of a short checklist for receiving physicians to fill out for all HLOC transfers. A lead CC physician will be responsible for following up on these and provide a means to provide feedback to the sending sites. This feedback will include:
1.) How the patient is doing at 3 days post-admission. The hope is to provide further patient outcome as well.
2.) Whether any concerns were raised by the admitting physician.
The lead physician will gather information to determine whether concerns were valid or not and, if so, provide feedback to sending physician and team. All this is to be accomplished in as positive a manner as possible. Gathering information on all transfers allows the occasional concern in care identified to be placed in context of all patients transferred, rather than focusing only on negative aspects of care. The process will also ensure that the sending ICUs and physicians receive information on their patients’ course in hospital and outcomes. Experience to date suggests that feedback is not occurring from receiving physicians at SMH to their colleague tasked with leading this initiative. The main barrier appears to be the heavy workload currently shared by the physicians at SMH. Formal review will occur in October, 2013 and more detailed information will be available to clearly determine barriers and potential ways to overcome them. Discussion underway with RCH group to consider similar pilot at RCH. No further progress has been made on this project … to be discussed at the next Medical Quality Committee meeting.
4. Antibiotic Stewardship
Over the past 3 Medical Quality Committee Meetings discussions regarding concerns of increasing incidence of Carbapenem-Resistant Enterobacteriaceae (CRE)/Carbapenemase-Producing Enterobactericeae (CPE) in FHA ICUs. This has highlighted the recognized need for more attention to measures to minimize nosocomial infections and transmission. Carbapenem use in FHA has been demonstrated to be significantly higher in FHA that VCHA within hospitals. To date actions include:
a) Contact with Microbiology regarding Antibiograms to better understand local flora and therefore need to use broader spectrum antibiotics.
b) Review antibiotic use at 4 larger ICUs, specifically comparing usage of carbapenems.

Department Summaries Clinical Audit Annual Report
Page 51 of 210
c) Representatives to share concerns with local departments on need to de-escalate antibiotic use appropriately and also importance of other preventive measures such as hand washing and universal contact precautions and use of PPE.
5. Simulation in Critical Care
One way of teaching and assessing critical care knowledge is through the use of simulation. While used almost universally now in Royal College training for Critical Care, it has not been more broadly adopted to provide CME for practicing ICU physicians. The goal is to develop a program in FHA using first RCH and later SMH as primary sites. The challenges will be to develop a program that is focused on physicians without simulation experience. Drs. Don Burke and Neil McLean have agreed to take this process forward.
To date actions include:
1) Identifying a Sim-man at RCH and plan to work with Department or Emergency Medicine to set up schedule of availability
2) Contact with Royal College by Dr. Don Burke regarding how to develop a recognized program in Simulation that allow MOCOMP points to be granted
3) Dr. Dave Sweet has previously forwarded some scenarios used at Vancouver General Hospital (VGH) that can be used
This project is still in its early stages of development but is expected to provide a major new way of ensuring ICU physicians within FHA are exposed to real-time education and feedback.
Quality Improvement Initiatives
1. 360 Assessment/Survey:
This process involves input from selected co-workers on evaluation of selected clinician qualities including leadership, clinical competence, etc. It has been used primarily within organizations with a hierarchical structure. Feedback is provided and those evaluated are expected to respond to this feedback. ICU physicians are independent contractors, not subject to the same need to respond as those within the administrative structure. While a 360 review is something that still could be used further thought needs to go into exactly what it would focus on … for example, clinical competence is not felt to be reliably assessed and focus would be more on qualities of team member and leader. We would need to have a clear plan on what would the expectations be from the physician evaluated. It may be that no specific expectations are expected other than acknowledgement that the review had been read. Still not clear whether to move forward on this.

Department Summaries Clinical Audit Annual Report
Page 52 of 210
2. Physician Burn Out Survey
There was generally a lot of interest in this. However, it was unclear exactly what to do with the results. It was expected that burn out would be appreciable but before proceeding with the survey discussion is required around whether changes would be suggested if burn out was found to be of concern.
Supporting Professional Development
Through our Physician Education Lead for Critical Care, Neil McLean, the following were arranged:
FHA Critical Care Journal Club, January 2014 In addition, there is ongoing access for all members for VGH monthly Critical Care Rounds. These can be attended in person, via video link at some sites and viewed over Web after the talk. There are regular, quarterly City-wide Journal Club for Critical Care that is attended by department members. A FHA member presented at the Journal Club on September 18
th
, 2013.

Department Summaries Clinical Audit Annual Report
Page 53 of 210
Emergency Medicine Regional Department Head: Dr. Anne Clarke Regional Department Medical Quality Committee Activities The Department of Emergency Medicine has established a Regional Department Medical Quality Committee that meets monthly. In addition, the twelve (12) acute sites hold regular monthly department meetings that include Morbidity & Mortality rounds.
Clinical Audits 1. Title: Sepsis Management
Site: All 12 acute care sites
Phase:
Planning Designing Data Collection Analysis Reporting
Background: Timely sepsis care decreases morbidity and mortality. Objectives: To maximize patient care – first antibiotics within one hour, first fluid bolus within 30 minutes, 2nd bolus of fluids within one hour. Target: meet the objectives 80% of the time Patient Selection: Patients with septic shock or severe sepsis Time period: Continuous ongoing audit Data collection strategy: Data is collected by a Registered Nurse (RN) auditor. Charts of all patients meeting the patient selection criteria are reviewed, or maximum of 30 charts per month. Results: We have seen a 50% decrease in the total number of sepsis cases since Period 7 and attribute this to more accurate screening at Triage.

Department Summaries Clinical Audit Annual Report
Page 54 of 210
First Antibiotics Within One Hour - by Period
0%
20%
40%
60%
80%
100%
P1 P2 P3 P4 P5 P6 P7 P8 P9 P10 P11
Com
plia
nce
2nd Bolus Administration - Compliance by Period
0%
20%
40%
60%
80%
100%
P1 P2 P3 P4 P5 P6 P7 P8 P9 P10 P11
Com
plia
nce

Department Summaries Clinical Audit Annual Report
Page 55 of 210
Actions: Analysis of data resulted in revising the Sepsis Pre-printed Orders (PPOs) to highlight needed action, ongoing education Physician participation rate: 100% 150 Lives in 150 Days [October 2013 - January 2014] The BC Sepsis Network launched a campaign in support of World Sepsis Day in October. The premise is for every five patients with severe sepsis and septic shock treated in accordance with a Sepsis Protocol one life is saved. If 750 patients across BC are treated, 150 lives will be saved in 150 days
Every Emergency Department (ED) in FH has signed up for this initiative (with the HDL as lead) and is submitting data to the Network. The goals for the Emergency Program are to: improve patient care and outcomes increase knowledge and awareness on sepsis care among all our physicians and nursing
staff increase the adoption and use of protocols and best practice in all our EDs track the positive impact of care delivered
Physician participation rate: 100%
Blood Culture Tests - Compliance by Period
0%
20%
40%
60%
80%
100%
P1 P2 P3 P4 P5 P6 P7 P8 P9 P10 P11
Com
plia
nce

Department Summaries Clinical Audit Annual Report
Page 56 of 210
2. Title: STEMI Management Site: All 12 acute care sites
Phase:
Planning Designing Data Collection Analysis Reporting
Background: Timely transfer for PCI decreases morbidity and mortality. Objectives: To optimize patient care by transferring patients to RCH for PCI within 30 minutes of arrival in the Emergency Room. Patient Selection: Patients with STEMI that were transferred to RCH Time period: Continuous ongoing audit Data collection strategy: Data is collected by a RN auditor. Charts of all patients meeting the patient selection criteria are reviewed each period. Results: Range of time from arrival to transfer to RCH at 12 sites is 75 to 160 minutes, exceeding target of 30 minutes.
0
10
20
30
40
50
60
70
Nu
mb
er
of
Cases/P
roto
co
ls
ARH BH LMH SMH
Sample of Sepsis Cases and Protocols Activated
Sepsis Cases Protocols Activated

Department Summaries Clinical Audit Annual Report
Page 57 of 210
Historically, the Emergency Program has been responsible for the first 30 minutes after the patient arrives in the ED. However, there are certain components over which the ED has no control, primarily the time between order entry for an ECG and the time the ECG is completed. This is dependent on resources available on site for timely ECGs. As a result, the Emergency Program seldom meets the target of 30 minutes in/out of the ED. The Program is in the process of changing targets and QPMS reporting of targets. The Program will accept responsibility for the procedures the ED can control and improve.
1. presentation to order entry for ECG (10 minutes) 2. ECG confirmation of STEMI to activation of Cardiac Catheterization Lab (10 minutes)
Physician participation rate: 100%

Department Summaries Clinical Audit Annual Report
Page 58 of 210
3. Title: Stroke Management
Phase:
Planning Designing Data Collection Analysis Reporting
Background: Timely access to thrombolytics for appropriate stroke patients may improve outcomes. Objectives:
To optimize patient care by streamlining the process for prompt assessment of
eligibility for tissue plasminogen activator (tPA) and administration within 3 hours of
symptom onset.
Triage to CT scan in 60 minutes or less
Patient Selection: Patients with hot stroke Time period: Continuous ongoing audit Data collection strategy: Data is collected by a RN auditor. Charts of all patients with hot stroke and eligible for TPA are reviewed each period.
Results:
1. FHA hot stroke number of cases (potential and confirmed)

Department Summaries Clinical Audit Annual Report
Page 59 of 210
2. Triage to CT time within 60 minutes
3. Triage to tPA time within 3 hours
Actions: hot stroke added to triage pick list inclusion/exclusion criteria at patient’s bedside for tPA
Stat CT scan process completed in partnership with EHS and Porters to CT scan
Physician participation rate: 100%

Department Summaries Clinical Audit Annual Report
Page 60 of 210
Chart Review Chart reviews are conducted for selected patients that return to the ER within 72 hours of initial visit and are admitted to hospital. Learning points are highlighted and recommendations made and introduced.
Morbidity & Mortality Review
During the period of April 2013 to March 2014 morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Cases are selected for regional review because they provide learning points and recommendations applicable to all sites and Emergency physicians. The cases presented originate through Patient Safety Reviews (PSRs), PSLS events, chart reviews and local site M&M Rounds.
Chart Reviews - Fiscal Year 2013/2014
33
35 35
31
26
24
32
15
17
21
1313
0
5
10
15
20
25
30
35
40
Period 1 Period 2 Period 3 Period 4 Period 5 Period 6 Period 7 Period 8 Period 9 Period 10 Period 11 Period 12
Nu
mb
er
of
Ch
art
s R
ev
iew
ed

Department Summaries Clinical Audit Annual Report
Page 61 of 210
Local M&M Rounds include the communication of learning points and recommendations from the regional review but also include cases based on individual physician experience and interest accompanied by learning points.
Medical Management Reviews During the period of April to November 2013 PSLS events were reviewed by the Local Department Head and with the physicians involved.
M&M Rounds: Cases Reviewed - All Sites and Regional - Fiscal Year 2013/2014
16
12
8
10
21
12
0
5
10
15
20
25
Period 7 Period 8 Period 9 Period 10 Period 11 Period 12
Nu
mb
er
of
Ca
se
s D
iscu
sse
d

Department Summaries Clinical Audit Annual Report
Page 62 of 210
Patient Safety Reviews (PSRs)
The Emergency Program conducted 3 PSRs between April and November 2013. All PSRs are reviewed with the Department Heads; the physicians involved in the PSR triggering event are included in the review. PSR Recommendation: Ensure CTAS 2 asthma patients are brought into the Emergency Department and not left in the waiting room. PSR Recommendation: Provide more comprehensive mental health assessment when there is no MHSU back-up on site at night. This is especially significant at small and medium sites. Status: A Suicide Assessment Tool was created to guide Emergency Physicians when no PLN
or Psychiatrist is on site.
Quality Improvement Initiatives
1. Revising and updating all discharge instructions to provide clear direction to patients after
they arrive home ‐ reviewed with patient, prior to discharge, to ensure understanding
2. Design and implementation of patient discharge package given to patient when discharged from the ER. Information includes name of attending physician, presenting complaint, discharge diagnosis, test results, recommended follow‐up.
given with discharge instructions specific to discharge diagnosis
Status: The Local Department Heads are trialing the new discharge package.
3. Priority triage for all pediatric patients: implemented at all sites to minimize pediatric waits
for care. Performance is reported on pediatric ER scorecard each period.
4. The Ministry of Health gave all Emergency Departments across BC a directive regarding the safe discharge of vulnerable patients. The Emergency Program created a checklist, based on the directive, to provide consistent, standardized and safe discharge of all vulnerable patients.
5. Hand Hygiene is one of the Key Performance Indicators for the Emergency Program. reported on QPMS displayed on Quality Boards in all Emergency Departments expect improved infection control in the ED

Department Summaries Clinical Audit Annual Report
Page 63 of 210
6. Continue to monitor numbers of patients who Register in the ED but leave without being seen (LWBS) by a physician or nurse. improvements in patient flow and reduced waiting time will reduce LWBS reported on QPMS
displayed on Quality Boards in all Emergency Departments
Nurse Sensitive Adverse Event (NSAE) The Canadian Institute of Health Information tracks four NSAEs: (1) in hospital fractures, (2) pressure ulcers, (3) hospital acquired pneumonia and (4) hospital acquired UTIs. The Emergency Program realized the biggest impact the EDs could make on improving patient care and reducing NSAEs would be on (3) hospital acquired pneumonia and (4) hospital acquired urinary tract infections (UTIs). These two indicators are currently the focus of our attention. Although the FH sites of focus are BH, RCH, RMH and SMH, the Emergency Program is making efforts to drastically reduce these two NSAEs at all sites. Data is being collected by FH.
Research Projects 1. Accuracy of Nurse Initiated Xray Orders of Extremity Injuries in the Emergency
Department 2. Effect of a DTU on Emergency Department Length of Stay and Inpatient Admissions 3. Canadian Assessment of Tomography for Childhood Head Injury (CATCH) Community ED
chart review 4. Breaking the Cycle of Recurrent Fracture: Prototyping a Fracture Liaison Service in BC
Performance Review/Clinical Performance Appraisal
1. Physician activity report for all ERPs number of CT scans and ultrasound per 100 patients seen per physician as
compared to peer group at site Patients seen per hour per ERP Length of Stay (LOS) <24 hour admission rate per Emergency Room Physician (ERP)
The Emergency Program is developing a process for peer audit reviews at each site. These reviews will be strictly for personal development.

Department Summaries Clinical Audit Annual Report
Page 64 of 210
Family Practice Regional Department Head: Dr. Peter Barnsdale Regional Department Medical Quality Committee Activities
Meeting dates: June 18, 2013, October 16, 2013
Clinical Audits 1. Title: Effectiveness of Family Practitioner and Hospitalist Discharge Practices
Site: Mission Memorial Hospital, Abbotsford Regional Hospital, Chilliwack General Hospital
Phase:
Planning Designing Data Collection Analysis Reporting
Background: Effective discharge practices can assist with the provision of optimal continuity of care for a patient leaving the hospital and returning to the care of a community practitioner. This clinical audit will focus on the issuance and content of a discharge letter.
Objectives: To assess the extent to which family practitioners’ practices for patient discharge are effective and consistent with accepted good practice.
Determine the extent to which a discharge letter is written
Determine the extent to which the discharge letter indicates:
o Admission reason
o Discharge diagnosis
o Medication changes
o Follow-up plan
Patient Selection: 10 patient cases, for each family practitioner (MRP), that were discharged from Mission Memorial Hospital, Abbotsford Regional Hospital, or Chilliwack General Hospital. Patient cases were identified by Health & Business Analytics.

Department Summaries Clinical Audit Annual Report
Page 65 of 210
Time period: Patient cases were identified from 2012. Data collection strategy: Retrospective review of 10 patient charts, per physician, to determine if a dictated discharge letter was present or not; and if present, if the letter contained: an admission reason; discharge diagnosis; medication changes; and follow-up plan. The following patient cases were excluded from this audit: labour and delivery, emergency room, dictation by resident or other physician. 1, 597 charts were reviewed of which 599 charts met the inclusion criteria. The audit involved reviewing the charts of 127 members of the Department of Family Practice. Mission Memorial Hospital:
Number of charts reviewed: 220 Number of charts included: 174 Number of Family Practitioners: 19
Abbotsford Regional Hospital: Number of charts reviewed: 740 Number of charts included: 394
Number of Family Practitioners: 53
Chilliwack General Hospital: Number of charts reviewed: 637 Number of charts included: 310
Number of Family Practitioners: 55
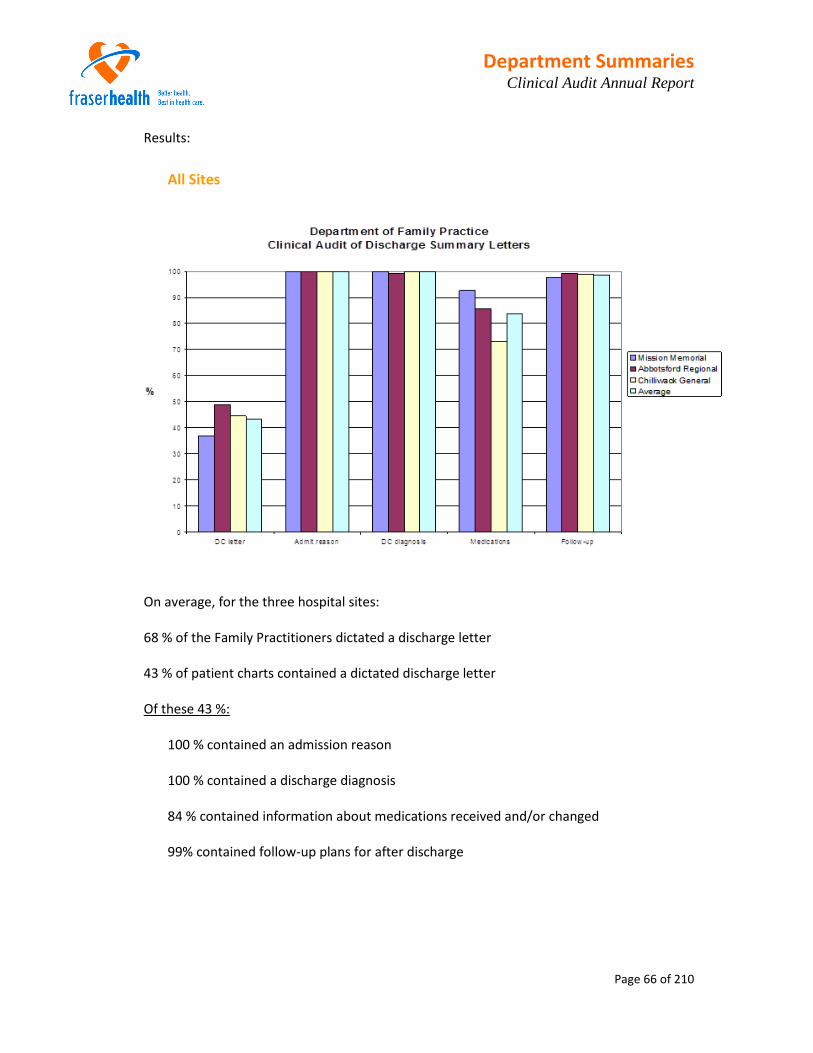
Department Summaries Clinical Audit Annual Report
Page 66 of 210
Results:
All Sites
On average, for the three hospital sites: 68 % of the Family Practitioners dictated a discharge letter 43 % of patient charts contained a dictated discharge letter Of these 43 %:
100 % contained an admission reason 100 % contained a discharge diagnosis 84 % contained information about medications received and/or changed
99% contained follow-up plans for after discharge

Department Summaries Clinical Audit Annual Report
Page 67 of 210
Mission Memorial Hospital:
53 % of the Family Practitioners dictated a discharge letter 37 % of patient charts contained a dictated discharge letter Of these 37 %:
100 % contained an admission reason 100 % contained a discharge diagnosis 93 % contained information about medications received and/or changed 98% contained follow-up plans for after discharge

Department Summaries Clinical Audit Annual Report
Page 68 of 210
Abbotsford Regional Hospital:
72 % of the Family Practitioners dictated a discharge letter 49 % of patient charts contained a dictated discharge letter Of these 49 %:
100 % contained an admission reason 99 % contained a discharge diagnosis 86 % contained information about medications received and/or changed 99% contained follow-up plans for after discharge

Department Summaries Clinical Audit Annual Report
Page 69 of 210
Chilliwack General Hospital:
69 % of the Family Practitioners dictated a discharge letter 44.5 % of patient charts contained a dictated discharge letter Of these 44.5 %:
100 % contained an admission reason 100 % contained a discharge diagnosis 73 % contained information about medications received and/or changed 99% contained follow-up plans for after discharge
Actions: The results of this baseline audit were shared with the Heads of Department (local) for the purposes of education and discussion of the importance of effective discharge practices for optimal continuity of patient care in the community. A follow-up clinical audit of discharge practices will be undertaken in the early spring. Physician participation rate: 100 %

Department Summaries Clinical Audit Annual Report
Page 70 of 210
2. Title: Utilization of standardized processes and documentation for admission, transfer, and
discharge of acute care patients by Family Practitioners Site: Mission Memorial Hospital, Abbotsford Regional Hospital, Chilliwack General Hospital
Phase:
Planning Designing Data Collection Analysis Reporting
Objectives: To assess the extent to which family practitioners’ practices for patient admission, transfer and discharge are effective and consistent with accepted good practice. 1. Admission practices
Determine the extent to which pre-printed orders (PPOs) are used at the time of admission
Determine which PPOs are used most frequently, by site
Determine the extent to which the PPO used at admission is appropriate for the diagnosis
Determine the extent to which the MOST form is used for patients over the age of 19 who are admitted
Determine the extent to which code status is recorded at admission
2. Transfer practices
For patients whose care has been transferred out to another physician or facility, the extent to which the patient transfer has been documented.
For patients returning to the hospital, the extent to which physician to physician communication has taken place, and been documented.
3. Discharge practices
Determine the extent to which a discharge letter is written
Determine the extent to which the discharge letter indicates:
o Admission reason
o Discharge diagnosis
o Medication changes
o Follow-up plan
Determine the length of time between patient’s discharge and the dictated date
Determine the length of time between the dictated and transcribed date
Determine the means of distribution of the discharge letter to the community general practitioner (e.g. EMR access, mailed letter, faxed letter, other)
Determine the length of time between the patient’s discharge and the community general practitioner receiving the discharge letter.

Department Summaries Clinical Audit Annual Report
Page 71 of 210
Patient Selection: This will be a prospective audit whereby patients are selected on the ward based upon the following criteria: Patient is currently an acute inpatient
Patient has been admitted by, and under the care of a Family Practitioner
Data collection strategy: For objective 1 (admission practices), data will be collected through the “in-person” review of patient charts on the in-patient ward in the following hospitals:
Fraser Canyon Hospital Mission Memorial Hospital Burnaby Hospital Chilliwack General Hospital Abbotsford Hospital Peace Arch Hospital Royal Columbian Hospital Ridge Meadows Hospital Delta Hospital Surrey Memorial Hospital Langley Memorial Hospital
Mission Memorial Hospital will be used as a pilot site to test the data collection protocol. The number of times that on-site data collection will occur for each hospital will be dependent on the number of Family Practitioners for that site. For objective 2 (transfer practices), a list of transferred out and returning patients will be used to select patient cases that will then be reviewed through the electronic medical record. For objective 3 (discharge practices), data will be collected through the review of the electronic medical records for the same patient cohort of objective 1, and follow-up with community general practitioner offices.

Department Summaries Clinical Audit Annual Report
Page 72 of 210
Quality Improvement Initiatives
Worked with Regional Department Head, Hospitalists to provide continuity of care at the Langley site during Hospitalist action and create a sustainable working model of care.
Supporting development of an inpatient resident and student training program overseen by Family Practice in Surrey. Working to minimize impact of recent Family Practice resignations in Surrey.
Regular quarterly meetings of Heads of Department (Local) to provide updates for FHA topics such as PPOs and 48/6, hear local issues and incorporate a quality agenda.
Looking at options to improve continuity of care through transitions and teams within hospital and between hospital and home.

Department Summaries Clinical Audit Annual Report
Page 73 of 210
Geriatric Medicine
Regional Department Head: Dr. M. Peter O’Connor
Regional Department Medical Quality Committee Activities Meeting Dates: 1st Wednesday bimonthly
Clinical Audit
Title: Appropriateness and Effectiveness of the medical care provided at the initial assessment/new consult appointment to outpatients referred with a suspected diagnosis of dementia.
Phase:
Planning Designing Data Collection Analysis Reporting Background: It is estimated that 1,500 new dementia cases are referred each year of which it is estimated
that 75% are on cholinesterase inhibitors. At the time of this clinical audit, patients with a suspected diagnosis of dementia were seen at 5 outpatient clinics within Fraser Health by 17 geriatricians. This clinical audit seeks to provide information on the appropriateness and effectiveness of the medical care provided at the initial assessment to patients referred with a suspected diagnosis of dementia.
Objectives:
1. Determine the extent to which the initial assessment is comprehensive and consistent with accepted good practice.
Baseline Mini Mental State Examination (MMSE) is established
Patient history is documented and includes: o Level of educational attainment o Bladder continence status
Physical examination is documented and includes: o Baseline body weight o Pulse rate o Patient’s motor strengths o Patient’s gait o Patient’s plantar response

Department Summaries Clinical Audit Annual Report
Page 74 of 210
Medications list is documented and reviewed o If patient is taking strongly anticholinergic medication (Beer’s List) this is
addressed in the notes. o If patient is taking inhaled medication for lung disease (Ventolin, Atrovent,
inhaled steroids, combination products such as Advair), the issue of worsening airways disease had been addressed in the notes.
Laboratory investigations are reviewed: o Serum TSH or T4 – abnormal results (elevated TSH or decreased T4) are noted o Serum B12 – abnormal result of <200 pmol/L are noted
2. Assess the extent to which physicians’ practices for patient support and safety are
consistent with recommended practice.
The presence or absence of a Power of Attorney is documented.
There is documentation of whether the patient drives or not.
3. Determine the % of patients with a new diagnosis of dementia that are prescribed cholinesterase inhibitors at the initial assessment or at a subsequent follow-up appointment.
Patient Selection: The patient population for this clinical audit was adult out-patients that received a first diagnostic workup by a dementia specialist (geriatrician) and who were started on a cholinesterase inhibitor [donepezil (Aricept), galantamine (Reminyl), or rivastigmine (Exelon)] at the initial appointment or at a subsequent follow-up appointment. Ten patients that met the selection criteria for each geriatrician were reviewed. Data collection strategy: This was a retrospective audit of geriatricians practices’ between December 1, 2012 and March 31, 2013. A list of patients that were seen at the 5 outpatient clinics for suspected memory problems was provided by Health and Business Analytics. Sharmen Lee reviewed the patient cases until 10 patient cases that met the inclusion criteria were identified for each of the 17 geriatricians. Data was abstracted by Sharmen Lee through the review of the consultation notes available in the electronic medical record.

Department Summaries Clinical Audit Annual Report
Page 75 of 210
Results:
Number of geriatricians included in the audit: 17 Number of patient cases reviewed: 798 Number of patient cases included in the audit: 150
Note: for 9 physicians, fewer than 10 patient cases met the inclusion criteria
Summary of Aggregate Data:
Average % of patients with item documented in consultation note
Baseline MMSE 98.8
Level of educational attainment 81.5
Bladder continence 58.6
Baseline weight 60.9
Pulse rate 87.3
Motor strength 62.3
Gait 70.0
Plantar response 38.4
Medications list 95.0
Serum TSH or T4 69.9
Serum B12 70.8
Presence of absence of Power of Attorney 60.9
Driving status 66.1

Department Summaries Clinical Audit Annual Report
Page 76 of 210
Summary of Data by Individual Practice:
The following anonymized data is presented to determine the practice patterns of the 17 geriatricians, as documented in the dictated consultation note.
Please note: These results reflect whether the item was documented in the consultation note available in the electronic medical record. The physical patient chart was not reviewed and may contain additional information that may have altered the results of this clinical audit.
1. Determine the extent to which the initial assessment is comprehensive and consistent with accepted good practice.
Baseline MMSE
98.8% of patients had a baseline MMSE documented in the consultation note.
98.8
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% Patients with Baseline MMSE Documented

Department Summaries Clinical Audit Annual Report
Page 77 of 210
Patient History - Level of Educational
81.5% of patients had their level of educational attainment documented in the consultation note.
81.5
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Education Level Documented

Department Summaries Clinical Audit Annual Report
Page 78 of 210
Patient History - Bladder Continence
58.6% of patients had their bladder continence documented in the consultation note.
58.6
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Bladder Continence Recorded

Department Summaries Clinical Audit Annual Report
Page 79 of 210
Physical Examination - Baseline Body Weight
60.9% of patients had their baseline body weight documented in the consultation note.
60.9
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Baseline Weight Documented

Department Summaries Clinical Audit Annual Report
Page 80 of 210
Physical Examination – Pulse Rate
87.3% of patients had their pulse rate documented in the consultation note.
87.3
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Pulse Rate Documented

Department Summaries Clinical Audit Annual Report
Page 81 of 210
Physical Examination – Motor Strength
62.3% of patients had their motor strength documented in the consultation note.
62.3
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Motor Strength Documented

Department Summaries Clinical Audit Annual Report
Page 82 of 210
Physical Examination – Gait
70.0% of patients had their gait documented in the consultation note.
70.0
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Gait Documented

Department Summaries Clinical Audit Annual Report
Page 83 of 210
Physical Examination – Plantar Response
38.4% of patients had their plantar response documented in the consultation note.
38.4
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Plantar Response Documented

Department Summaries Clinical Audit Annual Report
Page 84 of 210
Medications List
95.0% of patients had their medical list documented in the consultation note.
In reviewing the medications lists:
9 patients were taking inhaled medication for lung disease (Ventolin, Atrovent, inhaled steroids, combination products such as Advair). 2 of the 9 patients had the issue of worsening airways disease addressed in the consultation notes.
2 patients were taking strongly anticholinergic medication (Beer’s List) and this was addressed in the consultation notes.
95.0
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with a List of Medications Documented

Department Summaries Clinical Audit Annual Report
Page 85 of 210
Laboratory Investigations - Serum TSH or T4
69.9% of patients had their serum TSH or T4 documented as having being ordered or reviewed in the consultation note.
69.9
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with TSH/T4 Documented as Being Reviewed

Department Summaries Clinical Audit Annual Report
Page 86 of 210
Laboratory Investigations - Serum B12
70.8% of patients had their serum B12 documented as having being ordered or reviewed in the consultation note.
70.8
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with B12 Documented as Being Reviewed

Department Summaries Clinical Audit Annual Report
Page 87 of 210
2. Assess the extent to which physicians’ practices for patient support and safety are
consistent with recommended practice.
Power of Attorney
60.9% of patients had the presence or absence of a Power of Attorney documented in the consultation note.
60.9
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Presence or Absence of Power of Attorney Documented

Department Summaries Clinical Audit Annual Report
Page 88 of 210
Driving Status
66.1% of patients had their driving status documented in the consultation note.
66.1
0
10
20
30
40
50
60
70
80
90
100
%
Physician
% of Patients with Driving Status Documented
Department Summaries Clinical Audit Annual Report
Page 89 of 210
3. Determine the % of patients with a new diagnosis of dementia that are prescribed
cholinesterase inhibitors at the initial assessment or at a subsequent follow-up
appointment.
Due to the manner in which the patient cases were selected, it was not possible to determine the % of patients with a new diagnosis of dementia that were prescribed cholinesterase inhibitors at the initial assessment or at a subsequent follow-up appointment.
798 patient cases were reviewed to identify 150 that met the inclusion criteria of a new diagnosis of dementia that were prescribed cholinesterase inhibitors at the initial assessment or at a subsequent follow-up appointment.
Actions:
The results of this clinical audit were provided to the members of the Department of Geriatric Medicine for review and discussion. Individual physician practice profiles were unanimously requested and were sent individually to each Department member to allow for individual professional development.
A follow-up clinical audit is planned for the second half 2015.
Chart Review A mechanism and process for conducting chart review is currently under discussion.
Morbidity & Mortality Review A mechanism and process for conducting morbidity & mortality review is currently under discussion.

Department Summaries Clinical Audit Annual Report
Page 90 of 210
Medical Management Review During the period of May to December 2013, medical management reviews were conducted for the purposes of evaluating and improving the medical quality of care provided. PSLS reviews were conducted by the Older Adult Program Quality Committee. Learning points and recommendations for improvement arising from the case(s) reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Completion of MOST forms in a timely
fashion
Geriatricians to work with MRP’s to facilitate completion
2. Onset or recurrence of Clostridium
difficile post discharge
Information to discharged patients. Formal review of MD prescribing patterns ongoing (PPI/antibiotics) – RDMQC to consider further post‐review
During the period of December 2013 to June 2014, medical management reviews were conducted for the purposes of evaluating and improving the medical quality of care provided. PSLS reviews were conducted by the Older Adult Program Quality Committee. Learning points and recommendations for improvement arising from the PSLS case(s) reviewed, and the status of implementation are as follows:
Learning Point / Recommendation PSLS Clostridium difficile Cases Reviewed
Status of Implementation
1. PPI Use – 14/14 cases Notification of P&T Committee and Primary care
2. Clostridium difficile Protocol use – 0/14 cases
Follow-up with Medicine Program
3. De-escalation policy of broad spectrums and/or restrictions
Referral to Antimicrobial Stewardship
4. Case series included re-admitted patients Development of documentation/ information for discharged patients at risk

Department Summaries Clinical Audit Annual Report
Page 91 of 210
Evidence Based Practice/Medical Management Tools Pre-printed Orders (PPO) for Geriatric Delirium developed in conjunction with Hospitalist service. Now introduced FH‐wide as a single delirium PPO for Seniors on Form Imprint. Initial development of PPO indicated improved outcomes for delirium management, with reduced LOS, improved process of Medication review, improved delirium awareness by all staff, and reduction of delirium risk factors. A post‐implementation audit has been completed and shows the need for continued emphasis on maintenance phase.
Quality Improvement Initiatives
The hand-hygiene learning module has been completed by all primary Department members. The Department is working with Infection Control to pilot methodologies for physician-specific auditing.
Focused review of all fall patients.
Supporting Professional Development
Videoconferencing of UBC Division of Geriatric Weekly rounds to 4 sites within Fraser Health/Older Adult Program.
Physician Management Institute (PMI) courses have been offered to Department members, with uptake by three members.

Department Summaries Clinical Audit Annual Report
Page 92 of 210
Hospitalists Regional Department Head: Dr. Sayeeda Hudani Regional Department Medical Quality Committee Activities
The Department of Hospitalists is currently establishing a Regional Department Medical Quality Committee. In the interim, the Heads of Department (Local) have been meeting regularly with medical quality improvement a standing item on each agenda. Regional Department Meeting Dates: October 2, November 6 and December 18, 2013
Clinical Audits Title: Clinical Audit of Hospitalist Care Processes Phase:
Planning Designing Data Collection Analysis Reporting Objectives: 1. Assess the extent to which hospitalists' practices for patient admission are effective and
consistent with accepted good practice. determine the extent to which the Hospitalists General Admission Order PPO is used
by hospitalists determine the extent to which the MOST form is used
2. Assess the extent to which hospitalists' practices for patient discharge are effective and
consistent with accepted good practice. Determine the extent to which a discharge letter is written Determine the extent to which the discharge letter template has been utilized Determine the extent to which the discharge letter indicates: Most responsible diagnosis Co-morbidities Past medical/surgical history Operative interventions Other interventions Treatment/course in hospital Names of specialists associated with patient’s care Code status Allergies Medication on discharge Discharge disposition Post discharge follow-up

Department Summaries Clinical Audit Annual Report
Page 93 of 210
Patient Selection: 25 patient cases under the care of the Hospitalist Service, from three Fraser Health hospitals were included in the audit. Labour and delivery/newborn cases were excluded from the audit. Patient cases were identified by Health & Business Analytics. Time period: Patient cases were identified from 2012.
Data collection strategy: A retrospective review of 25 patient charts in Meditech, for each of the three hospitals, was undertaken to determine if PPOs, MOST forms, and dictated discharge letters were present. For the discharge letter, if present, data was collected to determine whether the letter contained the following:
Most responsible diagnosis Co-morbidities Past medical/surgical history Operative interventions Other interventions Treatment/course in hospital Names of specialists associated with patient’s care Code status Allergies Medication on discharge Discharge disposition Post discharge follow-up
The electronic chart review and data collection was completed by Karen Ostrom. Data analysis was completed by Sharmen Lee. 75 charts were reviewed of which 71 charts met the inclusion criteria.
Department Summaries Clinical Audit Annual Report
Page 94 of 210
Results: Admission and Discharge Practices:
Hospitalists General Admission Order PPO use by hospitalist service: The Hospitalists General Admission Order PPO is in use at the 3 hospitals. Utilization is fairly consistent between the 3 hospitals. Facility 101 68.0% Facility 102 57.1% Facility 103 56.0 % Average 60.6 % MOST form utilization
MOST forms were not been scanned into the electronic medical record. No data was therefore able to be collected.
Discharge Letters The practice of dictating a discharge summary letter is consistent high with two of the hospitals. Facility 101 56.0% Facility 102 100.0% Facility 103 96.0 % Average 83.1 % An additional practice of handwriting on a “Discharge Instructions and Return to Care” form was also noted at two of the facilities. It is notable that Facility 102 that dictated a discharge summary letter for all the patient cases reviewed (100%) did not utilize this other hand written form. Facility 101 68.0% Facility 102 0% Facility 103 40.0 % Average 38.0 %

Department Summaries Clinical Audit Annual Report
Page 95 of 210
Hospitalist Practices
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Gen Admission PPO DC Instructions & Return to Care Discharge letter
%
101
102
103
Average

Department Summaries Clinical Audit Annual Report
Page 96 of 210
Discharge letter contents: For those patient cases in which a discharge letter was dictated, on average only 41% of letters utilized the discharge letter template. There was consistent and high compliance with reporting in the areas of: Most responsible diagnosis Treatment and/or course in hospital Discharge disposition
Facility
101 102 103 Average
% % % %
Discharge template utilization 42.9 47.6 33.3 40.7
Most responsible diagnosis indicated 100.0 100.0 95.8 98.3
Co morbidities indicated 100.0 85.7 58.3 81.4
Past medical/surgical history indicated 71.4 66.7 70.8 69.5
Operative interventions indicated 14.3 9.5 20.8 15.3
Other interventions indicated 71.4 38.1 16.7 37.3
Treatment/course in hospital indicated 100.0 100.0 100.0 100.0
Names of specialists indicated 57.1 76.2 70.8 69.5
Code status indicated 28.6 38.1 50.0 40.7
Allergies indicated 42.9 61.9 29.2 44.1
Medications on discharge indicated 71.4 90.5 87.5 84.7
Discharge disposition indicated 92.9 95.2 100.0 96.6
Post discharge follow-up indicated 64.3 61.9 62.5 62.7

Department Summaries Clinical Audit Annual Report
Page 97 of 210
Actions: This preliminary audit was undertaken to provide initial data and to determine if the data collection methodology was effective and efficient, prior to implementation for all sites. As the electronic medical record does not contain all of the necessary documentation, the following changes to the methodology are recommended going forward: On-site data collection occurs on Hospitalist Service wards. Patient charts will be
reviewed on the ward and data collected will include: use of admission order sets, PPOs and MOST.
30 days post on-site data collection, the patients’ electronic medical records will be accessed to determine if a discharge summary letter has been dictated/transcribed, and to review the contents of the letter for comprehensiveness and completeness.
This secondary audit will be conducted in collaboration with the Department of Family Practice.
Discharge Letters
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
Templat
e
Diagn
osis
Com
orbiditie
s
Pas
t med
/sur
g hx
Ope
rativ
e inte
rven
tions
Oth
er in
terv
entio
ns
Tx/co
urse
in h
ospita
l
Nam
es o
f spe
cialists
Cod
e stat
us
Alle
rgies
Disch
arge
Med
s
Disch
arge
dispo
sitio
n
Follow-u
p
%
101
102
103
Average

Department Summaries Clinical Audit Annual Report
Page 98 of 210
Morbidity & Mortality Review
Inpatient Death Report template An Inpatient Death Report template has been developed and each site will be establishing a case review group and procedure to conduct the reviews. Further development is required with the processes of: collecting and formalizing data; ensuring each site has a process in place of getting charts; formalize template; how to use; what data to collect; and to formalize confidential reporting process
Evidence Based Practice/Medical Management Tools
Pre-Printed Orders New Regional PPOs for chronic obstructive pulmonary disease (COPD), Delirium, and Stroke are in place. Members of the Department are currently reviewing all Medicine PPOs, to ensure all are updated.
Quality Improvement Initiatives
Regional Department Scope of Practice The initiative is to guide the process of decision-making around disposition planning of all patients potentially earmarked for the Hospitalist service in Fraser Health. The preliminary work shows need for (few examples):
Care Pathways for C-spine injuries Improve bedline transfers Need for subspecialist coverage CME Events – i.e. chest tube management, hyponatremia, COPD management.
The current phase involves discussions on how to implement and who the stakeholders are that need to be involved in the implementation phase. The expected implementation phase anticipates a 6-9 month project.

Department Summaries Clinical Audit Annual Report
Page 99 of 210
Performance Review/Clinical Performance Appraisal
The Department has been working to develop peer audit reviews at each site. Some sites have a process in place.
Supporting Professional Development
Regional Hospitalist CME Events
October 24, 2013:
Keynote Speaker: Ethics Concepts Communication and Conflict Resolution for Hospitalists Case Presentations included:
Trauma, the Elderly and Delirium
COPD & Congestive Heart Failure (CHF)
One Practical Step Towards Reducing Rates of Hospital Acquired Infections (HAIs)
Sepsis: Clinical Cases Reviewed
June 21, 2014: Regional Department of Hospitalist Educational Symposium
Key Note Speakers (45 minute presentation, 15 minute question period)
1. Clinical Problem Solving Exercise - Dr Robert Sharpe 2. Update on Chronic Hepatitis C – Dr Edward Tam
Round-Table Presentations (20 minute presentation, 10 minute question period)
1. Diabetic Foot Infections - Dr Yasemin Arikan 2. Wound Healing, Problem Wounds & Dressing Options - Dr Rebecca Nelson 3. Chest Tube Insertion - Procedures – Dr Susan Kwan 4. What’s New in the Treatment of Overactive Bladder: Beyond Antimuscarinics - A
Paradigm Shift in Managing OAB – Dr Brian Yang 5. Heparin-Induced Thrombocytopenia – Dr Vicky Chan
Symposium Evaluation
32 Hospitalists attended the symposium. Feedback was generally very positive with the following recommendations being made for future educational events:
Topics relevant to hospitalist practice.
More “hands on” interactive, case based sessions – problem-based learning.
Shorter presentations, too much content on slides
More time for procedural practice, discussion/questions, more topics.

Department Summaries Clinical Audit Annual Report
Page 100 of 210
Regional Department of Hospitalists Communications: Launch of Webpage and e-Newsletter In November 2013, the department launched a Regional Department Hospitalists Webpage and e-Newsletter. The Hospitalist e-Newsletter will be a bi-weekly digest on Fridays. Each digest will include short, mobile-device friendly headlines with links directly to related documents on the new Hospitalists webpage. This method of communicating with all FH Hospitalists will reduce the weekly email interruptions while keeping you informed of current events of relevance to members of the Department. The webpage is on the public-facing FH Physicians Website so requires no log-in and can viewed at your leisure. The Regional Department Head will reserve direct e-mail communication with Members for matters for a sensitive nature. Regular e-Newsletter content will include:
Order Sets / Clinical Tools Updates General Member Information (references, manuals, guides etc.) Fraser Health Policy Updates Clinical Improvements / Videos / Apps Leader Development Opportunities Calendar Events Professional medical organization Links

Department Summaries Clinical Audit Annual Report
Page 101 of 210
Infection Prevention and Control and Public Health (IPC) Regional Department Head: Dr. Elizabeth Brodkin
Quality Improvement Initiatives
Actions taken to reduce Clostridium difficile infection (CDI) rates
Fraser Health facility-associated CDI rates from 2005/06 are shown in Figure 1. Our target is 6.0 cases per 10,000 patient days (based on the CNISP rate) and we surpassed that target in fiscal year 2013/14 with a rate of 4.1 cases per 10,000 patient days. Rates for fiscal year 2013/14 by site are shown in Figure 2. All nosocomial cases are now reviewed using a formal Review Tool that focuses on preventable risk factors, and the data are uploaded into the IPC surveillance system and shared with the IPC Committees at each site. Cases with poor outcomes (colectomy and death due to CDI) are entered into PSLS, and where indicated are the subject of a formal Patient Safety Review. In 2013/14 there was a large outbreak on the Older Adult unit at SMH, which led to a Patient Safety Review that resulted in a number of recommendations for the unit, site and program as well as nursing and physician practice. A current list of vulnerable units, where nosocomial CDI is most likely to occur, rank ordered by number of cases fiscal year to date is continuously monitored. This table is updated every fiscal period and distributed to site and program leadership. IPC continues to target vulnerable units with interventions and initiatives, including staff education, better isolation and cohorting of GI patients, changes to physical layout, hand hygiene and antimicrobial
stewardship.

Department Summaries Clinical Audit Annual Report
Page 102 of 210
Figure 1 FH CDI Case Counts and Rates by Fiscal Year 2005/06 through 2013/14
Figure 2 CDI Case Counts and Rates by Site 2013/14

Department Summaries Clinical Audit Annual Report
Page 103 of 210
Elimination of VRE) post elimination of screening / Vancomycin-resistant Enterococci (isolation requirements On November 5, 2012 Fraser Health eliminated the requirements both to screen high-risk patients for VRE, and to isolate those known to be colonized. This has freed up scarce isolation resources and eliminated over 10,000 VRE screening tests each year. A comprehensive surveillance plan has been put in place and all cases of VRE detected in clinical specimens are uploaded into the IPC surveillance system. Cases are categorized as colonizations or infections, the specimen site is recorded and each case is followed forward for 30 days. If death occurs a detailed chart review is carried out to determine if the death can be attributed to VRE infection.
Figure 3 VRE Colonizations and Infections in Clinical Specimens from November 2012
Figure 3 shows all VRE colonizations and infections detected in Fraser Health clinical specimens beginning with the cessation of screening on November 5, 2012. Unfortunately comparison with previous periods when screening and isolation did occur is not possible, due to differences in the counting and reporting of cases. There have been a total of 570 confirmed healthcare associated VRE cases since November 2012; 36% of these are colonizations and 64% are infections. Since the requirement to screen for VRE has been eliminated the number of colonizations has declined; this is to be expected. There is an apparent increase in the number of infections beginning in October 2013; however the surveillance protocol was changed at that time and IPC practitioners were asked to enter all

Department Summaries Clinical Audit Annual Report
Page 104 of 210
cases when the status changed from colonization to infection, or when the source of positive culture changed (e.g. from urine to blood), in addition to new infections. Recurrent positive blood cultures are also entered if they appear to be new infections. IPC will continue to monitor this apparent upward trend.
The majority of VRE detections since November 2012 have been in urine specimens (75%). Six percent of all VRE detections were found in blood cultures. See Figure 4.
Figure 4 VRE Specimen Source November 2012 through March 2014
VRE Specimen Source Total Cases (%)
Groin 4 (<1%)
Rectal/perineum 8 (1%)
Sputum/respiratory 8 (1%)
Surgical site wound 12 (2%)
Blood 35 (6%)
Skin & soft tissue wound 36 (6%)
Other (e.g. peritoneal fluid) 41 (7%)
Urine 426 (75%)
Grand Total 570 (100%)
Surveillance of linezolid use in Fraser Health was an additional measure put in place with the cessation of VRE screening. Linezolid is the primary treatment option for VRE infection and the purpose of this measure was to understand if Linezolid use is increasing, presumably as a result of an increasing number of VRE infections. Figure 5 indicates a consistent decline in the use of linezolid since November 2012.
Figure 5 Linezolid Use in FH
Date # DDD* Fiscal 2011/2012 2801.5
Nov 2012 to Feb 2013 918.0
Mar to May 2013 763.7
Jun to Aug 2013 531.5
Sep to Nov 2013 524.5
Dec 2013 to Feb 2014 441
*Defined Daily Dose (DDD) Linezolid 1200 mg

Department Summaries Clinical Audit Annual Report
Page 105 of 210
Carbapenemase-producing Enterobacteriaceae (CPE)
Bacteria resistant to carbapenem antibiotics through the production of carbapenemases have been emerging worldwide for over a decade. They have been seen in occasional Fraser Health clinical specimens since 2011, and are becoming more common, particularly at SMH and RCH. In fiscal 2013/14, 63 new cases of CPE were identified in Fraser Health. Forty-five (71%) of these cases were colonizations and 29% were infections. Although confirmation of transmission requires analysis of plasmids at the National Microbiology Laboratory in Winnipeg, in most cases it is possible to determine locally with reasonable certainty whether or not a new case is a result of transmission within a Fraser Health site. Of the 63 cases identified in Fraser Health in 2013/14, 41 (65%) were likely transmissions. Specimens collected from the ICU at SMH between June and October 2013 were all the same gene type; this and several other factors strongly suggested that transmission was happening within the unit. A similar pattern was noted on one of the medical units at RCH in January 2014, and an outbreak was formally declared on that unit. After 6 weeks with no transmissions the outbreak was declared over. Beginning in February 2014 another spike of cases was noted at SMH, likely focused around the HAU. Interventions have been put in place and there have been no new cases for several weeks.
Figure 6 CPE Cases at RCH, November 2013 through April 2014

Department Summaries Clinical Audit Annual Report
Page 106 of 210
Figure 7 CPE Cases at SMH, 2011 through 2014
Interventions that are necessary to interrupt transmission of CPE include:
Admission and point prevalence screening on the affected unit
Strict cohorting of patients, staff and equipment
Focus on compliance with hand hygiene and use of PPE
Enhanced cleaning of the unit
Daily chlorhexidine baths for all colonized patients
Focused communication that includes all programs and services operating on the affected unit
In order to detect patients colonized with carbapenemase-producing bacteria, and isolate them appropriately so they do not pose a risk to other patients, IPC has introduced a screening program for all new hospital admissions to Fraser Health sites. High-risk patients (i.e. those with a history of health care outside Canada) are placed on Contact Precautions on admission and screened via a rectal swab. Those subsequently found to be colonized are placed in private rooms with dedicated equipment. Screening is in place across Fraser Health sites, although difficulties have been encountered due to the limitations of Meditech.
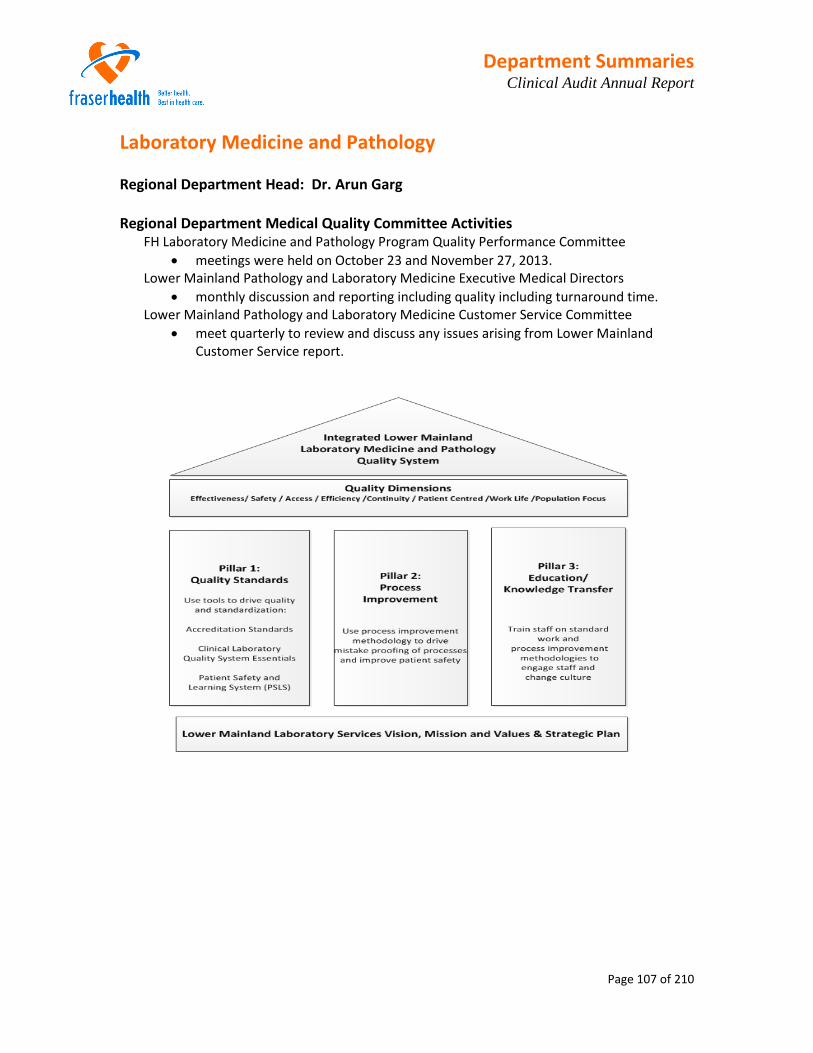
Department Summaries Clinical Audit Annual Report
Page 107 of 210
Laboratory Medicine and Pathology Regional Department Head: Dr. Arun Garg Regional Department Medical Quality Committee Activities
FH Laboratory Medicine and Pathology Program Quality Performance Committee meetings were held on October 23 and November 27, 2013.
Lower Mainland Pathology and Laboratory Medicine Executive Medical Directors monthly discussion and reporting including quality including turnaround time.
Lower Mainland Pathology and Laboratory Medicine Customer Service Committee meet quarterly to review and discuss any issues arising from Lower Mainland
Customer Service report.

Department Summaries Clinical Audit Annual Report
Page 108 of 210
Report for time period: April 2013 to December 2013
1. Key Performance Indicators (KPIs)
Turnaround Times (TAT) measures are used as key performance indicators for the Quality Dimension of Access.
Clinical Laboratory
The tests of potassium, troponin and hemoglobin have been designated as surrogate markers for all the tests done in the Chemistry and Hematology sections of the laboratory.
Metrics used for turnaround time are for patients in Emergency locations measured at the 50th Percentile from Order to Result.
Legend for Table below
On Target
Target over but within 20%
Target over and beyond 20%
Order to Result
How are we doing?
Hemoglobin Target = 30 minutes at
50th Percentile
Troponin Target = 60 minutes at
50th percentile Potassium
Target = 45 minutes at 50th percentile Overall Status Improving Trend Steady/Stable Trend Improving Trend FH- East
Abbotsford Regional Hospital
Chilliwack General Hospital
Fraser Canyon Hospital
Mission Memorial Hospital
FH - South Langley Memorial Hospital
Peace Arch Hospital
Delta Hospital
Surrey Memorial Hospital
FH - North Burnaby Hospital
Royal Columbia Hospital
Eagle Ridge Hospital
Ridge Meadows Hospital
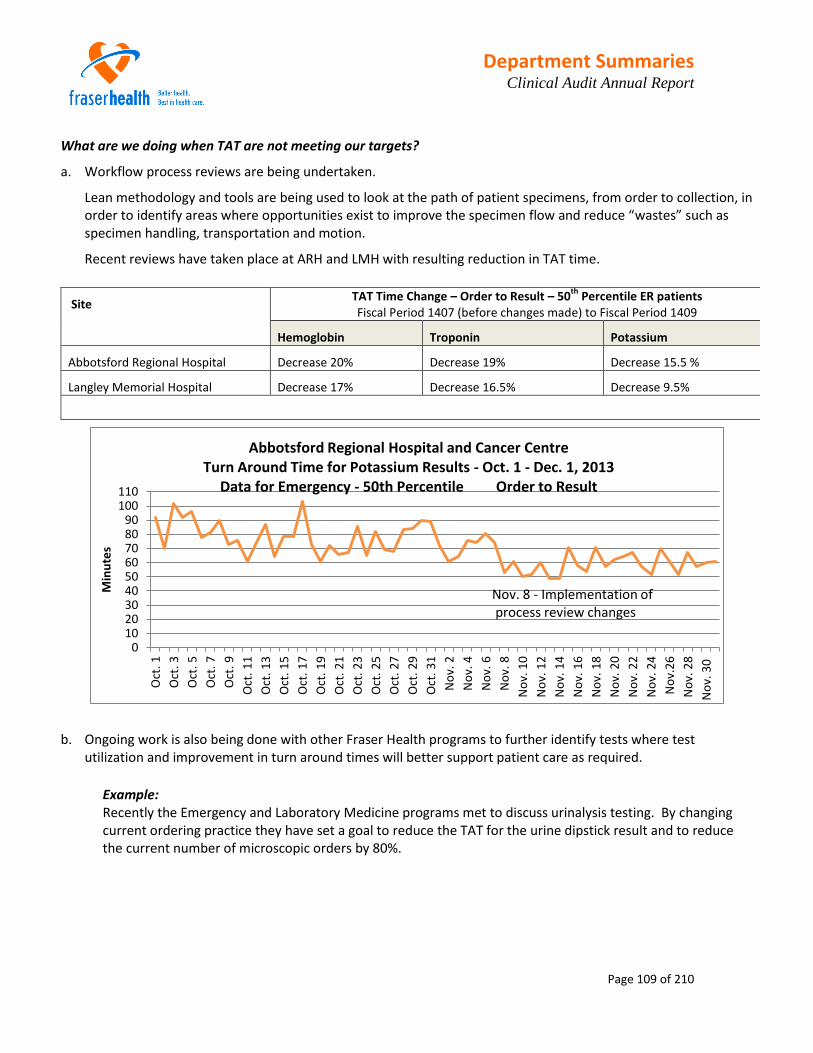
Department Summaries Clinical Audit Annual Report
Page 109 of 210
What are we doing when TAT are not meeting our targets?
a. Workflow process reviews are being undertaken.
Lean methodology and tools are being used to look at the path of patient specimens, from order to collection, in order to identify areas where opportunities exist to improve the specimen flow and reduce “wastes” such as specimen handling, transportation and motion.
Recent reviews have taken place at ARH and LMH with resulting reduction in TAT time.
Site TAT Time Change – Order to Result – 50
th Percentile ER patients
Fiscal Period 1407 (before changes made) to Fiscal Period 1409
Hemoglobin Troponin Potassium
Abbotsford Regional Hospital Decrease 20% Decrease 19% Decrease 15.5 %
Langley Memorial Hospital Decrease 17% Decrease 16.5% Decrease 9.5%
b. Ongoing work is also being done with other Fraser Health programs to further identify tests where test
utilization and improvement in turn around times will better support patient care as required.
Example: Recently the Emergency and Laboratory Medicine programs met to discuss urinalysis testing. By changing current ordering practice they have set a goal to reduce the TAT for the urine dipstick result and to reduce the current number of microscopic orders by 80%.
0102030405060708090
100110
Oct
. 1
Oct
. 3
Oct
. 5
Oct
. 7
Oct
. 9
Oct
. 11
Oct
. 13
Oct
. 15
Oct
. 17
Oct
. 19
Oct
. 21
Oct
. 23
Oct
. 25
Oct
. 27
Oct
. 29
Oct
. 31
No
v. 2
No
v. 4
No
v. 6
No
v. 8
No
v. 1
0
No
v. 1
2
No
v. 1
4
No
v. 1
6
No
v. 1
8
No
v. 2
0
No
v. 2
2
No
v. 2
4
No
v.2
6
No
v. 2
8
No
v. 3
0
Min
ute
s
Abbotsford Regional Hospital and Cancer Centre Turn Around Time for Potassium Results - Oct. 1 - Dec. 1, 2013
Data for Emergency - 50th Percentile Order to Result
Nov. 8 - Implementation of process review changes

Department Summaries Clinical Audit Annual Report
Page 110 of 210
Medical Microbiology
Note: At the beginning of July 2013 the integration of Burnaby Hospital Medical Microbiology to Royal Columbian Hospital Medical Microbiology took place. The movement of all microbiology services and staff was completed by the beginning of fiscal period 1405 (July 19 to August 15). This move was made to optimize staffing and technical resources for microbiology services within Fraser Health.
Anatomic Pathology - Quarterly Quality Review: July 1 to September 30, 2013
Turn Around Times (TAT) – total time from registration of case into Pathology Meditech program to time of sign out of the report by the Pathologist.
Cytogenetics RCH
Total number of specimens
CCMG guidelines for TAT in days
FHA average TAT in days
% failure rate
Amniotic Fluid
70
90% in 14 9 0
Amniotic Fluid – rapid aneuploidy detection by FISH
3 1 0
Bone Marrow – urgent including ALL, AML, CML
172
Preliminary 3-5
Final
14 Preliminary
3 Final
7 0
Bone Marrow – all other CLL, MM, MDS
21 15 0
Peripheral Blood
392 28 31 0
Tissues – products of conception 43 42 25 11.6
1517192123252729313335373941434547
13
01
13
02
13
03
13
04
13
05
13
06
13
07
13
08
13
09
13
10
13
11
13
12
13
13
14
01
14
02
14
03
14
04
14
05
14
06
14
07
14
08
14
09
Ho
urs
Fiscal Period
Order to Result Turn Around Time - 90th Percentile
C. difficile toxin B Gene
ARH
RCH
SMH

Department Summaries Clinical Audit Annual Report
Page 111 of 210
2. Occurrence Management indicators
PSLS event reporting and follow up is used as an indicator for the quality dimension of patient safety. PSLS events reported are handled daily at the site level with monitoring at the program level by the lead, quality and process improvement. Review of the monthly summary is done as a standing agenda item at the program Quality Performance Committee. Through this monitoring and regular discussion at the QPC opportunities for improvements are identified and process reviews initiated when appropriate.
Two formal quality reviews were undertaken and completed as the result of events reported as degree of harm 3. As well five process quality reviews were undertaken for events reported with no or minor harm but where an opportunity for improvement was recognized.
One such event involved newborn screening at RCH where a process review was undertaken with representatives from the MICY program and the laboratory:
In collaboration with the MICY program changes have been made in both nursery and laboratory processes to ensure that newborn screening on all babies is collected and sent for testing in a timely manner. The key step in this process change was to have the orders for newborn screening entered into the Meditech system (for T+1) when the baby is born, as is done for the orders for cord gases. Follow up meetings are taking place to ensure that the changes are working for all.
________________________________________________________________________________________
Approximately 75 - 80% of reported PSLS events are in the Pre-Analytic (before testing) area of the specimen workflow.
In the Pre-Analytic Events – approximately 25% of the reported total events reported deal with incorrectly or mislabeled patient samples.
Of these events 37 % were lab collected and 53% were collected by non-lab personnel. Continuing education in positive patient identification and proper specimen labeling is ongoing at the site level but we have not seen a
significant decrease in the number of this type of event reported yet.
0%
20%
40%
60%
80%
100%
Jan
-13
Feb-1
3
Mar-1
3
Apr-1
3
May-1
3
Jun
-13
Jul-1
3
Aug
-13
Sep
-13
Oct-1
3
Nov-1
3
De
c-1
3
PSLS Events Reported in Category Laboratory Divided by Where in Path of Work Event Occurred
%Pre/AnalyticalEvents/ Totalevents
% Analytical/TotalEvents
%Post Analytical/Total Events
Department Summaries Clinical Audit Annual Report
Page 112 of 210
Positive Patient Identification (PPID)
It’s good for patients: Better safety & ID verification
On December 11, 2013 the laboratory at Surrey Memorial Hospital became the first hospital in the province to use
positive patient identification (PPID) technology for blood collections.
PPID uses barcoding to positively match the patient and testing requests before blood collection, and allows the
printing out the needed specimen labels at the patient bedside.
This technology has the potential to significantly reduce, if not eliminate, laboratory responsible errors in patient
identification and specimen labeling.
PPID scanner and label printer

Department Summaries Clinical Audit Annual Report
Page 113 of 210
3. Activity
Blood Collections
ECGs
0
200,000
400,000
600,000
800,000
1,000,000
1,200,000
1,400,000
Inpatients Emergency Outpatients Total
All FH Sites - Total Number of Blood Collections Comparison by Fiscal Year FY2013 YTD
FY2014 YTD
02,0004,0006,0008,000
10,00012,00014,000
Total ECGs Done by Laboratory Medicine Staff
For Inpatient and Emergency Patients Comparison By Fiscal Year

Department Summaries Clinical Audit Annual Report
Page 114 of 210
Specimen Numbers
Anatomic Pathology Number of Specimens
Clinical Pathology Number of Specimens
Fiscal Year 2013 2014 Fiscal Year 2013 2014
Surgical 101,222 108,354 Chemistry 1,200,616 1,218,584
Cytology 5,629 5,725 Hematology 826,680 873,791
Fine Needle Aspiration 3,698 3,840 Coagulation 362,830 373,287
Cytogenetics 2,997 3,120 Chemistry Urinalysis 242,608 246,907
Bone Marrow 780 821 Blood Gases 135,856 144,594
Autopsy 525 505 Fluids, Body & CSF 7,337 8,018
SMH Referred In 423 411 Lab Special 359 1,171
RCH Referred In 9 12 Serology Virology 27,404 30,975
Total 117,296 124,802 Total 2,803,690 2,897,327
Transfusion Medicine
Number of Specimens
Medical Microbiology
Number of Specimens
Fiscal Year 2013 2014
Fiscal Year 2013 2014
Transfusion Medicine* 67,933 68,071
Urine Culture 142,097 129,345
Patient Order, Lot# Products 11,420 12,035
Blood Culture 84,214 92,077
Wound, tissue and fluid culture 28,613 29,648
Tissue Transplantation 456 551
Microbiology Culture 46,865 44,772
Tissue, Xenografts 35 45
Microbiology Tests 16,879 15,893
Total 79,845 80,704
ARO 40,242 36,321
Referred Out 25,018 25,241
Total 383,928 373,297 * Year to year comparison has revealed that the Jan 2014 HAMAC reported numbers were incorrect for this number
Total Specimens Fiscal 2013 (April 1, 2012 to March 31, 2013) 3,384,759
Total Specimens Fiscal 2014 (April 1, 2013 to March 31, 2014) 3,476,130 Increase in Number of Specimens from Fiscal 2013 to Fiscal 2014 2.70%

Department Summaries Clinical Audit Annual Report
Page 115 of 210
FHA MIS Procedure Trend
2008-09 2009-10 2010-11 2011-12 2012-13 2013-14 MIS Procedures
15,480,780 16,953,316 17,830,932 19,292,780 19,784,745 20,769,878
Year-over year change
1,472,536 877,616 1,461,848 491,965 985,133
% Change 10% 5% 8% 3% 5%
10,000,000
12,000,000
14,000,000
16,000,000
18,000,000
20,000,000
22,000,000
2008-09 2009-10 2010-11 2011-12 2012-13 2013-14
Nu
mb
er o
fPrc
ed
ure
s
MIS Procedure Trend - FHA Labs

Department Summaries Clinical Audit Annual Report
Page 116 of 210
Patient Safety and Learning System (PSLS) In Laboratory Medicine and Pathology all events reported in PSLS are monitored at the site level and at the program level with a monthly report generated and reviewed at the monthly Quality Performance Committee meeting. Events reported with degree of harm level 4 (severe harm had reached the patient) or 5 (event resulted in patient’s death) are investigated immediately upon notification being received. Investigations take place at the site level with support and actions by operations, medical and quality leadership as appropriate. Through these investigations if became apparent that within Fraser Health there were many patient events reported at critical level (PSLS levels 4 and 5); which upon further investigation, were found to be at a lower level of criticality. This misalignment of degree of harm assignment and patient safety outcomes was identified as an opportunity for continuous improvement and a review of all level 4 and 5 events reported from January 1, 2012 to February 7, 2014 was conducted. Data Analysis: Within FH Laboratories, from January 1, 2012 to February 7, 2014:
17 events were initially reported at level 4,
1 event was initially reported at level 5
Upon further investigation, these 18 events were re-classified as:
Event Categories Comments 4 Level 4 events (1) Transfusion Medicine event that went on to review
(1) Cross HA event that went on to review
(1) Clinical area issue, that led to the Laboratory Medicine program
developing the Critical Result Communication Policy and Procedure
(1) One event is still being investigated. The degree of harm is still
being determined.
Initial 4 then changed to 3 2 events 14 events were downgraded
after joint investigation with medical and clinical areas
Initial 4 then changed to 2 6 events Initial 4 then changed to 1 3 events Initial 4 then rejected 2 events Initial 5 then changed to 1 1 event
Types of Issues identified in these events:
Events Types of Issues 4 Level 4 events 3 Pre and Post Analytic
1 Transfusion Medicine (analysis) 14 Downgraded events 9 Pre and Post Analytic
2 Transfusion Medicine(blood products) 1 Microbiology 1 Hematology 1 Clinical issue

Department Summaries Clinical Audit Annual Report
Page 117 of 210
FH Sites where these events were reported:
Events Sites 4 Level 4 events 1 RCH
1 RCH with cross Health Authority process 1 ARHCC 1 BH
14 Downgraded events 5 ARHCC 3 SMH 2 RMH 1 CGH 1 LMH 1 PAH 1 RCH
Summary of Review Findings: Over the last two years, the experience in FH Laboratories had shown that after investigation with the reporting clinical areas, and discussion with medical and operations leaders, 14 of 18 PSLS events, that were originally reported as critical events (17 reported as level 4, one reported as level 5), were downgraded to a lower level of harm, or no harm, or the event was rejected. The one event that was originally reported at level 5 was determined to be unrelated to patient’s outcome. This event was changed to level 1. Review of these reported level 4 and 5 events also revealed that there were gaps in the notification of the laboratory personnel who would be responsible to investigate and follow up on the event.
Recommendations going forward: 1. Work with FH PSLS Coordinator to review and update notification lists of critical events to
Laboratory Medicine Operations team. 2. Share findings of review with the FH Laboratory Medicine Leadership team, and identify
potential systems issue.
3. Identify site specific potential opportunities for improvement; both within the laboratories, and working with site clinical areas to improve laboratory processes and communication
processes. 4. Work with FH regional Professional Practice Leaders to review reporting of Laboratory PSLS
events.
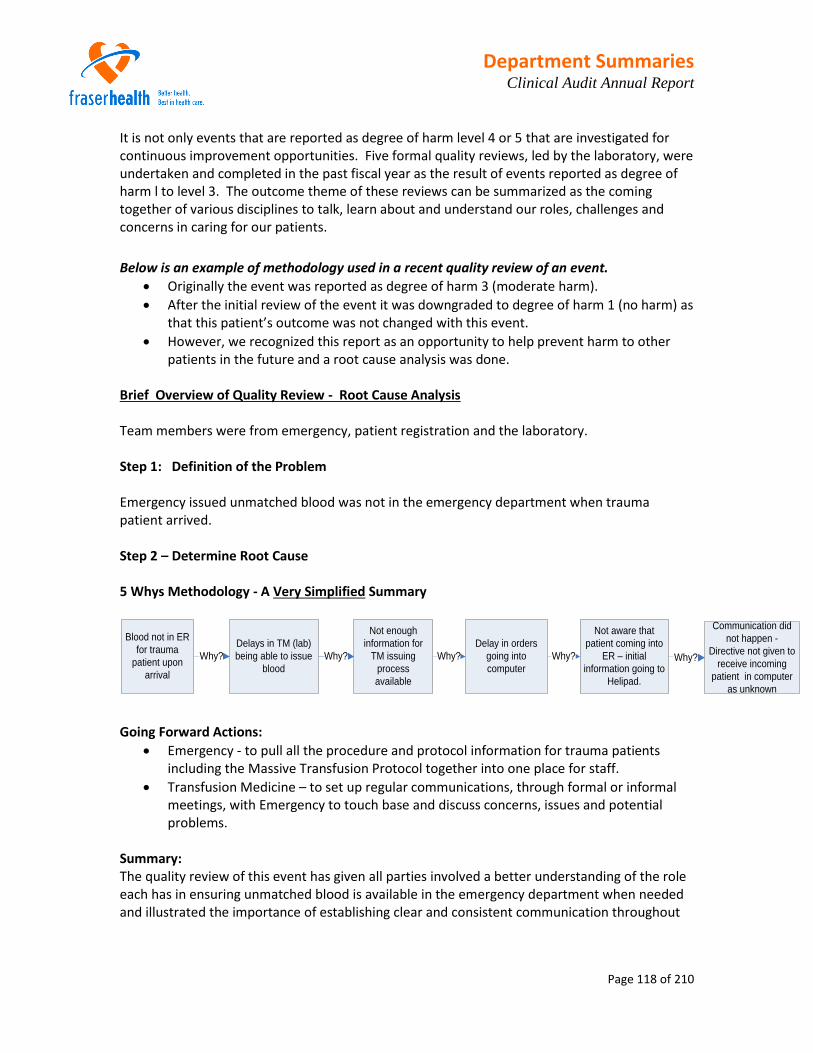
Department Summaries Clinical Audit Annual Report
Page 118 of 210
It is not only events that are reported as degree of harm level 4 or 5 that are investigated for continuous improvement opportunities. Five formal quality reviews, led by the laboratory, were undertaken and completed in the past fiscal year as the result of events reported as degree of harm l to level 3. The outcome theme of these reviews can be summarized as the coming together of various disciplines to talk, learn about and understand our roles, challenges and concerns in caring for our patients.
Below is an example of methodology used in a recent quality review of an event.
Originally the event was reported as degree of harm 3 (moderate harm).
After the initial review of the event it was downgraded to degree of harm 1 (no harm) as that this patient’s outcome was not changed with this event.
However, we recognized this report as an opportunity to help prevent harm to other patients in the future and a root cause analysis was done.
Brief Overview of Quality Review - Root Cause Analysis Team members were from emergency, patient registration and the laboratory. Step 1: Definition of the Problem Emergency issued unmatched blood was not in the emergency department when trauma patient arrived. Step 2 – Determine Root Cause 5 Whys Methodology - A Very Simplified Summary
Delays in TM (lab)
being able to issue
blood
Blood not in ER
for trauma
patient upon
arrival
Why?
Not enough
information for
TM issuing
process
available
Delay in orders
going into
computer
Not aware that
patient coming into
ER – initial
information going to
Helipad.
Communication did
not happen -
Directive not given to
receive incoming
patient in computer
as unknown
Why? Why? Why? Why?
Going Forward Actions: Emergency - to pull all the procedure and protocol information for trauma patients
including the Massive Transfusion Protocol together into one place for staff.
Transfusion Medicine – to set up regular communications, through formal or informal meetings, with Emergency to touch base and discuss concerns, issues and potential problems.
Summary: The quality review of this event has given all parties involved a better understanding of the role each has in ensuring unmatched blood is available in the emergency department when needed and illustrated the importance of establishing clear and consistent communication throughout

Department Summaries Clinical Audit Annual Report
Page 119 of 210
the process. Key to our success in providing the best quality care to our patients is the establishment of relationships, with open and timely communications.
PSLS Quality Initiative – Royal Columbian Laboratory Medicine and MICY Programs
• A collaborative and focused quality initiative to prevent Iatrogenic Injury. • PSLS written for all incidents and followed up same day. • Formal Training and Competence Assessment Program Developed for collectors to
improve specimen quality and patient safety and to reduce technical problems and TAT delays due to specimen quality.
• Test Order codes grouped to simplify and minimize amount of specimen collected, prevent missed tests and prevent recollections.
• Weekly meeting initially between Lab and Nursery decreased to monthly meetings as improvements made and sustained.
Outcome - Recollection of specimens for quality reasons decreased (day shift) by approximately 70%.
Patient Safety Initiative – Surrey Memorial Positive patient identification is essential to safe patient care in programs throughout our facilities. In PSLS errors in patient identification and specimen labelling account for approximately 25% events reported in PSLS Category Laboratory. 35% of these errors were for specimens collected by lab staff while 55% were for specimens collected by non-lab staff. The introduction, in December 2014, by the laboratory of positive patient identification device (PPID) technology at Surrey Memorial Hospital for patient identification and the generation of specimen labels, in the patient blood collection process, has resulted in no patient identification or specimen labelling errors to date when PPID is used. This is significant patient safety initiative in a site where there are approximately 215,000 inpatient venous blood collections per year. Our vision for the future would see this technology become the norm at all sites throughout all programs where positive patient identification is essential to safe and quality patient care. Accreditation The primary accreditation body for laboratories within British Columbia is the Diagnostic Accreditation Program (DAP). The DAP inspection assessment format involves 2 processes – the onsite technical inspection of each discipline area and the medical staff assessment. This accreditation cycle has one of continual learning and process improvement for both the DAP and Fraser Health as Fraser Health sites were among the first sites in British Columbia to participate in a newly design format with updated standards of which there are a total1963 mandatory requirements and 736 requirements divided among 20 sections. Throughout the DAP process our commitment as a region wide program with standardized policies, processes, and procedures along with strong leadership at all levels was recognized by and accepted by the DAP assessors. This cohesiveness helped stream line our DAP assessment process as much of the mandatory required evidence was the same for all sites.

Department Summaries Clinical Audit Annual Report
Page 120 of 210
Fraser Health sites have been in the DAP inspection and assessment cycle since February 2012 when our first five sites had their onsite technical inspection. In February 2014 the technical inspection of all our sites were completed. Our first medical assessment did not take place until November 2013. Our sites have achieved an average of 98.5% compliance with the mandatory standards. To date 6 sites have achieved full accreditation status, 3 sites are waiting for the medical staff assessment to be done and 4 sites are waiting for a provincial review of the standard requirements for a Medical Peer Review program. Resource Utilization Initiative
Urinalysis Testing – Emergency Program and Laboratory Medicine
In early December 2013 the Emergency and Laboratory Medicine programs met to discuss urinalysis testing. During the meeting the following became apparent:
the combined order of UA (urine dipstick) and UMIC (microscopic) on urine samples is ordered before the ER physician has seen the patient and
the expected protocol is to have the UA ordered and reported before the physician sees the patient.
Change in practice proposed:
Urine microscopic to be ordered by physician after patient assessment as an “add on” test to urinalysis.
Goals Working together the Emergency and Laboratory Medicine program have set the goals to:
reduce the current number of urine microscopic orders by 80% through ordering practice change
reduce the turnaround time for the urine dipstick result - target TAT is 30 minutes – through:
o decrease in number of urine microscopics to be done o increased staff education and awareness of TAT target o regional implementation of auto verification for urinalysis dipstick reporting
Outcome to Date:
Average Number of Microscopic Orders per Day (24 Hours)
Site Before Change in practice Data from Nov 10, 2013 to Nov. 27 2013
After Change in practice Data from Jan 13, 2014 to April 8, 2014
% Decrease In Microscopic
Orders
Urine Dipstick TAT – target 30
minutes % Time Target Is Being Met
Abbotsford 16.7 4.5 73 82
Burnaby 16.7 5.1 70 97
Chilliwack 15.3 3.0 80 88
Delta 10.0 2.3 77 97

Department Summaries Clinical Audit Annual Report
Page 121 of 210
Eagle Ridge 14.3 5.1 65 84
Fraser Canyon 0.6 0.4 36 89
Langley Memorial
14.8 3.9 73 81
Mission Memorial
6.2 1.2 81 93
Peace Arch 21.3 4.2 80 90
Ridge Meadows 13.3 5.0 63 95
Royal Columbian 19.4 11.4 41 98
Surrey Memorial 37.8 13.5 64 83
FH Totals 186.4 Orders/Day
59.4 Orders/Day 78% Decrease Graph next page shows TAT changes after Microscopic Order Practice change made
Urine Dipstick TAT Percentage of Time 30 Minute TAT Target is Being Met
Trend Based on Collection Dates 2014-Jan-13 to 2014-Apr-08
ARH
ARH
ARH ARH
BH
BH BH
BH
CGH
CGH
CGH
CGH
DH DH DH
DH
FCH
FCH
FCH
FCH
LMH
LMH LMH
LMH
PAH
PAH PAH
PAH
RCH RCH
RCH
RCH RMH
RMH
RMH RMH
SMH
SMH
SMH
SMH
75
80
85
90
95
100
1 2 3 4

Department Summaries Clinical Audit Annual Report
Page 122 of 210
Transfusion Medicine –Education Initiative
Dr. Morrison, Dr. Sigurdson and our colleagues from Vancouver Coastal and the Provincial Blood Coordinating Office have developed an on-line educational module on Transfusion Medicine for Physicians. This education module is located on the CCRS learning site – search with the word Physician. It is available to anyone (not just physicians) who would like to participate in free continuing education that uses brief case studies with accompanying references and resources to test practice knowledge in Transfusion Medicine.
Department Summaries Clinical Audit Annual Report
Page 123 of 210
Medicine Regional Department Head: Dr. Anne McNamara Regional Department Medical Quality Committee Activities
The Department of Medicine has established a Regional Department Medical Quality Committee with fifteen permanent subcommittees. The subcommittees are structured to encompass both division focused activities and hospital site locations as follows:
Regional Division of Gastroenterology Medical Quality Committee Regional Division of Infectious Diseases Medical Quality Committee Regional Division of Neurology Medical Quality Committee Regional Division of Rehab Medicine & Physiatry Medical Quality Committee Regional Division of Endocrinology Medical Quality Committee Regional Division of General Internal Medicine Medical Quality Committee Regional Division of Nephrology Medical Quality Committee Regional Division of Oncology Medical Quality Committee Regional Division of Respirology Medical Quality Committee Abbotsford Regional Hospital, Department of Medicine, Medical Quality Committee Delta Hospital, Department of Medicine, Medical Quality Committee Eagle Ridge Hospital, Department of Medicine, Medical Quality Committee Burnaby Hospital, Department of Medicine, Medical Quality Committee Royal Columbia Hospital – Clinical Teaching Unit, Department of Medicine, Medical Quality Committee Surrey Memorial Hospital – Short Stay Unit, Department of Medicine, Medical Quality Committee
Regional Division of Endocrinology Clinical Audit 1. Title: Diabetes in Pregnancy Outcomes
Phase: Planning Designing Data Collection Analysis Reporting
Clinical audit objective: To examine maternal and neonatal outcomes in pregnant women with diabetes to
determine if there is inter-hospital variation within Fraser Health.

Department Summaries Clinical Audit Annual Report
Page 124 of 210
Patient outcomes to be examined include: Maternal: C section delivery Pre-eclampsia Ethnicity Insulin use Hypoglycemia
Neonatal: Macrosomia Hypocalcemia hypoglycemia Jaundice Prematurity Shoulder dysocia
Patient population: Babies born in a Fraser Health hospital between January 1, - December 31, 2012 to moms with a diagnosis of gestational diabetes. Data collection strategy: The BC Perinatal database will be used as the source of data for this clinical audit. Specific data elements within the database have been identified and communicated to Health and Business Analytics to abstract.
2. Title: Management of Thyroid Nodules
Phase: Planning Designing Data Collection Analysis Reporting
Background: The Division of Endocrinology has selected the management of thyroid nodules as the medical quality initiative for clinical audit. The Division is currently creating consensus guidelines for the region with the participation of Medical Imaging, Surgery and Pathology. Once the clinical practice guidelines have been established, an education session will be held within the division. A clinical audit will be undertaken to determine the degree of compliance to the use of the clinical practice guidelines for the management of thyroid nodules.

Department Summaries Clinical Audit Annual Report
Page 125 of 210
Morbidity and Mortality Review
The Division held M & M rounds for the purposes of evaluating and improving the quality of patient care provided. Two cases were reviewed with the learning points and recommendations as follows: 1. Hypoglycemia in pregnancy has a wide differential diagnosis - an investigative strategy
was devised. 2. Insulin tolerance tests should be performed where there is acute care support.
Evidence Based Practice/Medical Management Tools
The division continues to develop the Acute Care Subcutaneous Insulin Pre-printed orders. There was a pilot phase at RCH in Feb 2014. The goal of these orders is to standardize insulin orders across the region, encourage the use of regularly scheduled insulin, thereby improving glycemic management of inpatients, reduce medication errors and ultimately reduce patient morbidity/mortality.
Preliminary work has been completed on regional Diabetic Ketoacidosis (DKA)pre-printed orders but this process will not be advanced until the Subcutaneous Insulin order set is finalized.
Quality Improvement Initiatives The Division, along with Laboratory medicine, is interested in examining whether the Subcutaneous Insulin orders will have any impact on hyperglycemia and hypoglycemia rates in hospital. Glucometer data from the pilot project, analyzed by ward, will be reviewed pre and post-implementation.
Laboratory medicine and Endocrinology are working to improve reporting of FT4 in pregnancy with trimester-specific reference ranges

Department Summaries Clinical Audit Annual Report
Page 126 of 210
Division of Gastroenterology Clinical Audit
Colonoscopy Audits:
The colon cancer screening program for asymptomatic stool FIT positive patients over age of 50 includes a mandatory Colonoscopy audit similar to the one FH gastroenterologists have used. No further FH Gastroenterology Division colonoscopy audit will be planned in the near future as the BCCA Colon Cancer Screening program will capture all the items and will be ongoing.
As part of the Colon Cancer screening program, there will also be a new item for Physician Quality Audit - Direct Observation of Procedural Skills (DOPS). At least one FH gastroenterologist and 2 general surgeons have been selected to be trained as DOPS assessors. All colonoscopists participating in the Colon Cancer Screening program will be assessed over the next 1-2 years.
Endoscopic Ultrasound Chart Review:
There is a single Endoscopic Ultrasound (EUS) service at RCH. It is performed by a single gastroenterologist. A prospective chart review of all consecutive EUS cases performed in 2013 was conducted. The following outcomes were found.
N= 262 cases Average wait time = 30. 2 days Most rectal cancer staging pre-op surgery or radiation done in < 2 weeks Most solid mass lesions in organs for biopsy done in < 3 weeks
Referrals for suspected tumors or cancers (228/262) = 87.0% of referrals Fine Needle Aspirations (FNA) done on 110 cases. FNA of solid lesions for potential tumor = 69 Nondiagnostic “acellular” specimens = 0; 67/69 obtained tissue “cellularity” in FNA attempts 97%; suspicious or confirmed carcinoma/solid tumor = 38; benign cellular results = 29; # Cases referred back for repeat EUS FNA = 0
10 pancreas cyst fluid aspirations suggestive of a mucinous pancreas cystic tumor Endoscopic mucosal resection (EMR) done on 12 cases for subepithelial lesions Pseudocyst drainage and stenting = 2. Both successful and without complications
Overall Immediate EUS complications: Perforations = 0 Bleeding = 0 Post-biopsy pancreatitis = 0 Sedation complications = 0
Conclusion: The majority of EUS referrals are for potential cancers/tumors. The EUS FNA rates of 97% cellularity are consistent with the highest rates reported in the literature. The complication rate was very low. The EUS service is being performed for appropriate indications, and at acceptable standards.

Department Summaries Clinical Audit Annual Report
Page 127 of 210
Morbidity & Mortality Review The Division held M & M review rounds for the purposes of evaluating and improving the quality of patient care provided. Six cases were reviewed with the learning points and recommendations as follows: 1. Patients admitted in non-tertiary care referral centers with gastric and esophageal
varices should undergo definitive endoscopic treatment prior to discharge (i.e. Gastric variceal gluing, or esophageal banding) as they are at high risk of rebleeding.
2. Patients with colorectal cancer should undergo tattoo inking during colonoscopy using the entire vial of ink to aid surgeon with laparoscopic resection as it can be challenging to locate small volumes of ink during surgery.
3. There can be post-sphincterotomy bleeding in up to 1% of procedures. Referrals from non-ERCPist to ERCPist should ensure anti-platelet agents, anticoagulants, and coagulopathy be managed prior to ERCP if a sphincterotomy is anticipated.
4. In cases of obscure GI bleeding, a CT angiogram or RBC scan might locate the bleeding source when upper and lower endoscopy are negative. These scans should be available at RCH, SMH and ARH. If CT angiogram is positive, RCH interventional radiology is the only FH site capable of doing Angioembolization should this be needed. Occasionally a CT angio will show that the bleeding is within reach of a repeat endoscopy. If RCH interventional radiology angioemboliztion is needed, a Patient Transfer Network conference call among referring RCH radiology GI, RCH GI, plus admitting service (ICU or ER or CTU) may be needed to get patients to RCH for a procedure that will require an admitting service.
5. In cases where a colonoscopy is done with poor bowel preparation, a repeat colonoscopy may be needed in the appropriate situation to ensure there are no missed lesions.
6. Patients with previous cholecystectomy for gallbladder stones, and recent ERCP sphincterotomy but ongoing biliary colic pain with normal liver enzymes and U/S can still have non-cleared biliary stones. A MRCP or EUS is the next approach in these patients to evaluate the bile duct.
Evidence Based Practice/Medical Management Tools
Patient Transfer Network (PTN) is assisting with ON CALL Gastroenterology / Endoscopy referrals. There is not a gastroenterologist in every FH site, and not every FH site with a Gastroenterologist has complete daytime or after hours coverage. An algorithm has been presented to the Physician Advisory Group of lead Gastroenterologist/General Surgeons at each site and has been approved. It will help referring physicians and PTN to understand who to call if urgent Gastroenterology or Urgent Endoscopy is needed during the daytime and afterhours.

Department Summaries Clinical Audit Annual Report
Page 128 of 210
Quality Improvement Initiatives Members of the division are participating on the Fraser Health GI Council that discusses
endoscopy quality and planning. GI Division is working on increasing the accessibility of out-of-hours emergency
endoscopy services. Surrey Memorial Hospital GI physicians have established a formal 24/7 on-call service.
Supporting Professional Development
GI rounds are conducted at the RCH site. Some FH Gastroenterologists attend the St. Paul’s Hospital weekly GI/General Surgery rounds
Division of General Internal Medicine Clinical Audit 1. Title: Concurrence of ECG Reader Interpretations.
Divisions: General Internal Medicine and General Cardiology Phase:
Planning Designing Data Collection Analysis Reporting
Background: The Divisions of General Internal Medicine and General Cardiology are undertaking a collaborative clinical audit that will examine the degree of concurrence of ECG Reader interpretation between all ECG readers. The “ECG Peer Review Process” has been designed and agreed to by both Cardiologists and Internists and will be conducted in 2 phases.
Objective:
To determine the degree of concurrence of ECG Reader Interpretations Phase 1 – ECG peer review and education ECG Peer Review: 1. ECG selection:
20 abnormal ECGs from each ECG reader will be reviewed 2x per year for a total of 40 ECGs per reader per year.
ECGs will be selected from all sites (not just MUSE sites).

Department Summaries Clinical Audit Annual Report
Page 129 of 210
The ECGs for review will be "blinded" - all identifying information such as patient name and ECG reader name will be removed.
2. ECG Review
Each ECG will be reviewed by 1 member from the ECG Peer Reviewer pool. The pool will consist of 10 volunteer cardiologists who will over-read the ECG and record their determination as: "agree completely" or "agree mostly" or "disagree".
The "agree completely" and "agree mostly" will have no further action.
The "disagree" will proceed to review by the ECG Peer Review Committee.
The ECG Peer Review Committee will be Chaired by Dr. John Lemaitre and have as membership: Dr. Lemaitre; 1 cardiologist from SMH; 1 cardiologist from ARH; and 2 members from General Internal Medicine.
The entire Committee will over-read the ECGs brought forward as "disagrees" and record their determination as a Committee.
In reviewing the ECGs the Committee will also identify ECGs that have educational value and can be used as "seeded cases" for phase 2
3. Results Reporting:
The results of the ECG peer review process will be submitted: for cardiologists to Dr. Kornder; for internists to Dr. Shaw.
Drs. Kornder and Shaw will provide feedback to their respective members of individual performance and aggregate performance.
4. Addressing “outliers”
For those individuals identified as "outliers", it is proposed that a greater number of ECGs will be over-read. No definition of “outlier” is proposed at this time as the group recommends that the anonymized and aggregate results are reviewed first to see what overall performance of FHA ECG readers is.
5. Implementation
The Cardiology program will provide the cardiac technologists to support and operationalize the ECG peer review process.
Education: To support improved practice, ECG education will be provided on a regular and
continuous basis through virtual ECG meetings, circulating ECGs as "ECG of the Month" and/or having ECG rounds.
ECGs identified by the ECG Peer Review Committee as having educational value will be one source of ECGs for presentation.
Phase 2 – Enhanced ECG peer review Once Phase 1 has been implemented successfully, an enhanced Phase 2 will be
implemented. Phase 2 would involve seeding "control" ECGs into the workflow of ECG readers. The control ECGs would be selected by the ECG Peer Review Committee.

Department Summaries Clinical Audit Annual Report
Page 130 of 210
2. Title: Clinical audit of the medical care provided to patients presenting with Acute Coronary
Syndrome (ACS)
Phase: Planning Designing Data Collection Analysis Reporting
Background: The Divisions of General Internal Medicine and General Cardiology are undertaking a collaborative clinical audit that will examine the medical care provided to patients presenting with Acute Coronary Syndrome (ACS).
Data collection strategy: A retrospective chart review will be conducted on 50 charts at each of the 8 sites as follows: For Cardiology: SMH, ARH and RCH For Internal Medicine: BH. RMH. ERH. DH, LMH, PADH Note: The sites of MMH, Hope, and Chilliwack will not be included in this audit due to the low volume of patient cases. Each chart will be reviewed to determine the extent to which the following criteria are met:
History/Consult dictated and on chart within 24 hours
Medications within 24 hours of admission: ASA
Antiplatelets
Beta Blockers
RAAS Blockers
Statins Medications At Discharge: ASA
Antiplatelets
Beta Blockers
RAAS Blockers
Statins Smoking Cessation discussion documented Cardiac Rehab referral discussion documented Discharge Summary in EMR within 24 hours of discharge Follow up plan documented and includes: Driving
Sex
Work
GP appointment
Specialist appointment
Readmission for any reason within: 30 days
6 months

Department Summaries Clinical Audit Annual Report
Page 131 of 210
Division of Infectious Diseases Clinical Audit
Title: Appropriateness and Effectiveness of the medical care provided by the Home IV Program to Patients with Diabetic Foot Infection. Division: Infectious Diseases Phase:
Planning Designing Data Collection Analysis Reporting The audit objectives and design are currently under review.
Division of Nephrology Clinical Audits
Title: Clinical Audit of Primary Reviews Phase:
Planning Designing Data Collection Analysis Reporting Background: Provincial Standards have been identified for a number of patient parameters. Patient care has also been hampered by the lack of patient information being transferred to other services or among the group. Objectives: To ensure that an annual review of every renal patient was complete by the primary nephrologist. To ensure that specific standards were met in the reviews such as vascular access, MOST completion, medication reconciliation, transplant assessment Patient Selection: All hemodialysis patients in FHA Time period: Jan –July 2013 Data collection strategy: Prospective, ongoing Results: Primary review completion ranged from 80 – 100% among all nephrologists in FHA. Actions: Results circulated to physician group. Aim is for 100% completion. Physician participation rate: 100%

Department Summaries Clinical Audit Annual Report
Page 132 of 210
Evidence Based Practice/Medical Management Tools
Foot Care Screen Tool: Dr. Yao Dr. Yao shared the foot care tool. Results were discussed and group decided that a quick look from a nephrologist would be successful. In the long term, this could also be a cost saving method. Currently this is an Abbotsford project for PD and HD. Action Item: An education session would be set up with a podiatrist; Dr. Yao will share the information with the group.
MOST Presentation: Alexandra Kruthaup-Harper via t-con reviewed the forms with the group. Dr. Karim also presented to the group in the room in detail. Group discussion regarding Do Not Resuscitate (DNR) orders, C1, fine print to be moved up on the form. Action Item: Dr. Karim and Alex will come back to the group with a clear algorithm
Renal Chart Order: Chart Order presented. Allergies and Orders to be placed in physician order slot Action Item: Dr. Torng will communicate this information with MQSC
Dialysis Chart Redesign: The group us working on the optimal format of the chart to establish consistency, accuracy and ease of communication across the FHA Renal Program.
BCPRA KCC & PD Referral Algorithm: The province Wide Evidence Based algorithm was discussed and will be instituted in FHA.
Physician to Physician Communication: The group will be working on options to set up a structured methodology in communicating patient issues
Post Parathyroidectomy Pre-printed orders: Orders were discussed and decision to trail was made Potassium Algorithm
A new algorithm was reviewed and a survey was circulated. Revisions were made and the new algorithm will be trialed
Quality Improvement Initiatives
Medinet Mail Presentation: The FHA Renal Program is exploring different avenues to communicate via e-mail in a secure fashion in order to promote safe and efficient patient care.
Annual Reviews: Physicians are conducting annual reviews that will now be placed in the chart to facilitate information for all members of the health care team.
RELAY proposal: The FHA Renal program is exploring a partnership with family physicians in Surrey to optimize the care of patients with chronic kidney disease
Format of Primary Reviews: A standard format for primary reviews was established for consistency and to ensure that crucial information was included.
AVF Referral Trigger for PD Patients: There has been a decrease in AVF referral. The delay has been from referral to VAC. The decline may result in the inappropriate reallocation of OR time at JPOCSC. Early discussion with the Patient regarding fistula is encouraged. Dr. Wong is leading this.
Empiric Antibiotics for Suspected Line Sepsis: Lowest appropriate dose - the antibiotic form will be laminated to the new rover computer at SMH.

Department Summaries Clinical Audit Annual Report
Page 133 of 210
Fluconazole: Dosage for resistant organisms was discussed - there is a concern for about under dosing. Suggest 200mg every second day.
Engagement with the Transition Nurses: TN progress - all agreed that they are doing well, especially with chronic patients. It takes approximately 5 weeks for a patient to see the TN from start time. SMH have a direct in person contact with their TN and other sites have preferred written. TN timeline targets needs to be established. Circulation of TN cell phone numbers to nephrologists
Supporting Professional Development The group is partnering with the Ethics group in FHA with ongoing educational sessions and integrating these skills into everyday clinical practice.
Division of Neurology Clinical Audit
1. Title: Hot stroke rates and tPA use for Stroke in Fraser Health Hospitals
Phase: Planning Designing Data Collection Analysis Reporting
Background: Need to determine just how prevalent the use of tPA is in the Hyperacute Management of Ischemic Stroke for planning purposes and for auditing as part of the Provincial Stroke Management Objectives: To assess the extent and use of tPA in all Fraser Health Emergencies for Stroke Management Patient Selection: Patients receiving tPA for Stroke in Fraser Health Emergencies Time period: Ongoing from 2012 Data collection strategy: Prospective Results: Ongoing assessments Actions: Start of a Hyperacute Stroke Team for Fraser Health in the near future Physician participation rate: Stroke Team Members:

Department Summaries Clinical Audit Annual Report
Page 134 of 210
2. Title: Regional Stroke Scorecard Phase:
Planning Designing Data Collection Analysis Reporting Background: To provide Fraser Health with a more complete audit of Stroke Data for a better understanding of weaknesses in the provision of Stroke Services in the Fraser Health Objectives: A more complete audit of stroke parameters in all Fraser Health Hospitals, including emergency visit, admission, rehab and acute treatment outcomes data Patient Selection: All patients coming into Fraser Health Hospitals with diagnosis of stroke Time period: Launch early 2014 Data collection strategy: Prospective see excel spreadsheet included for design Results: Ongoing assessments Actions: Ongoing assessment of stroke services, impact of improving care including stroke cohorts, stroke unit starting at SMH, hyperacute stroke service starting at RCH Physician participation rate: All FH neurologists
3. Title: Audit of EEG Reporting Standards
Phase: Planning Designing Data Collection Analysis Reporting
Site: Fraser Health EEG Labs
Background: To ensure Fraser Health EEG Labs maintain Canadian Standards for EEG Reporting

Department Summaries Clinical Audit Annual Report
Page 135 of 210
4. Title: Physician Teamwork
Phase: Planning Designing Data Collection Analysis Reporting
Site: Abbotsford Regional Hospital
Background: The Division is piloting a questionnaire that will allow health care teams to provide individual confidential feedback to neurologists on issues related to teamwork and safety.
The “Modified Safety Attitudes Questionnaire” is based upon the JB Sexton article “The
Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research.” (BMC Health Serv. Res. 6, 44 (2006).) The neurologists at ARH will pilot the initial teamwork assessment tool. Objectives: Using a modified safety attitudes questionnaire tool, physicians will be able to obtain feedback from peers/health care team members regarding key aspects of safe and effective teamwork. Time period: December 2013 – February 2014 Data collection strategy: The questionnaire was distributed to peers/health care team members to provide confidential, anonymized feedback to the individual physicians. A companion self-assessment questionnaire was provided to the individual physician for completion. Results: For each individual physician, a confidential, anonymized report was provided reflecting the aggregate responses from peers/health care team members. Actions: Participants are reviewing and reflecting on their self-reported and observer-reported responses and will present to the Neurology Quality Committee at a future meeting. Physician participation rate: All neurologists Abbotsford as pilot

Department Summaries Clinical Audit Annual Report
Page 136 of 210
Quality Improvement Initiatives
The Division of Neurology has elected to make a quality practice improvement piece included in every division meeting. This will be a short presentation of a relevant topic to improve clinical practice in Neurology, and is meant mainly for the new Neurologists on staff to provide “pearls” that they can use in their practice. These items will be kept in an archive for future reference. The first piece was given June 2013, on the availability of genetic tests for neurological conditions in BC, and info on the requisition forms for BC doctors through the BC Children’s Hospital.
Supporting Professional Development
Fraser Valley Stroke Symposium: Stroke Management in Fraser Health “Acute to Rehab”, April 5, 2014
Division of Oncology Clinical Audit
Title: Completion of FHA MOST form on admission to SMH Oncology Unit Phase:
Planning Designing Data Collection Analysis Reporting Background: FHA implemented the MOST policy in October of 2012. This policy has significant implications for treatment of the oncology population during admission for acute care. Objectives: To determine SMH based division compliance with the new FHA policy, and timeliness of form completion in order to ensure appropriate patient care from time of patient admission. Patient Selection: All patients admitted to the SMH Unit 51 Oncology Ward between March and May 2013 Time period: March – May, 2013 Data collection strategy: retrospective Results: 84% of patients had MOST form completed as of day of admission.

Department Summaries Clinical Audit Annual Report
Page 137 of 210
Actions: Results communicated and discussed at Division Medical Quality Committee meeting August 2013. We agreed upon continued reinforcement to unit coordinators, nurses and physicians that completion of MOST form is expected at time of admission. The department has committed to the FHA policy and has encouraged unit clerks or nursing staff to page the admitting oncologist if a MOST form has not been completed at the time of admission. Physician participation rate: 100%
Morbidity & Mortality Review
The Division held M & M review rounds for the purposes of evaluating and improving the quality of patient care provided. Five cases were reviewed with the learning points and recommendations as follows: 1. Patients on chemo may be at risk for thromboembolism. Venous thromboembolism
(VTE) prophylaxis implemented for in-patients, no routine prophylaxis for out-patients recommended.
2. Improved communication is needed between Medical and Radiation Oncologists for patients receiving dual modality treatment with concurrent chemoradiation.
3. Precautions for chemotherapy and radiation therapy related toxicities need to be emphasized during new patient education - implemented
4. Physicians need to closely watch for potential bleeding complications in patients receiving anticoagulation - implemented.
Evidence Based Practice/Medical Management Tools
Pre-printed Orders (PPO) Project: All outpatient units at FH will adopt the BC Cancer Agency (BCCA) PPOs. The next phase of this project will cover FH Inpatient units
A formal review of chemotherapy treatment units within Burnaby, Royal Columbian, and Ridge Meadows Hospitals was conducted in early 2013. A formal report was submitted to FHA leadership, and the report has been distributed within the Division, reviewed at the Quality Committee meeting August 2013. The division supports the use of BCCA pre-printed orders (available at BC Cancer Agency) and protocols at the FHA hospital sites.

Department Summaries Clinical Audit Annual Report
Page 138 of 210
Quality Improvement Initiatives
Chemotherapy induced diarrhea (CID) is the second most common high risk emergency complication of chemotherapy in oncology patients. Rapid appropriate triage, blood work, complete bowel rest, anti-diarrheal medications, and antibiotic treatment is vital to prevention of morbidity and mortality. Previous audits of CID presentations to FHA Emergency Departments revealed delays in recognition and in evidence-based treatment of this oncology emergency. Root cause analysis determined the need for a “just in time” triage algorithm, protocol, PPOs and education.
Purpose: To create a regional CID protocol, PPOs, and educational module for FHA Emergency Departments, available in electronic format on Form Imprint.
Outcome goal – to initiate and maintain evidence based treatment of CID and increase awareness of CID.
Method: An interdisciplinary team worked with the FHA Policy office to develop a draft regional protocol, obtain review with intent for sign-off from all stakeholders, involving all regional educators, and mount learning modules on the CCRS web based system.
Results: Draft created as of March 2014
Supporting Professional Development
Monthly Department of Oncology Education Rounds, RCPSC accredited (videolinked
to BCCA Abbotsford Centre, Burnaby Hospital, Royal Columbian Hospital)
Monthly Regional Journal Club Rounds, RCPSC accredited (also videolinked)
Weekly or Monthly Tumour Site Specific Regional Interdiscplinary Rounds/Journal
Club, some RCPSC accredited (Breast, GI, Gyne, Lymphoma, Head and Neck) These
rounds are case-based, with regular review of evidence and published articles.
Regional involvement of other disciplines e.g. surgery and pathology. Some rounds
are BCCA provincial, by videolink.
Weekly BCCA provincial Medical Oncology Education Rounds (videolinked)
Monthly Regional Radiation Program Rounds
Weekly FVCC Radiation Case Conferences
Department Summaries Clinical Audit Annual Report
Page 139 of 210
Division of Respirology
Clinical Audit 1. Title: Bronchoscopy reporting
Phase: Planning Designing Data Collection Analysis Reporting
Background: The division has decided to focus on the performance and dictated reporting of bronchscopy, incorporating "procedural pause" and other elements of good practice. The clinical audit involves two phases:
Phase 1: All Respirologists will review the “Essential Bronchoscopist” online tutorial to develop standardized reporting content.
Phase 2: An audit will be undertaken to review the content of Physicians’ reports.
2. Title: Survey of physician “burnout” within the Division of Respirology
Phase: Planning Designing Data Collection Analysis Reporting
Background:
Burnouti—a pathologic response to stress manifested by the triad of emotional exhaustion, depersonalization, and diminished sense of personal accomplishment—is common among healthcare professionals. Studies have demonstrated that physician burnout has been associated with increased medical errors and suboptimal patient care due to related concerns such as difficulty making decisions, and communicating effectively; decreased patient satisfaction; and longer post-discharge recovery times. The personal impact of physician burnout can also lead to increased retention and turnover challenges, reduced productivity, lower morale, and issues with physicians’ mental and physical healthii.
Objectives:
Recognizing the significance of physician burnout, the Division of Respirology undertook a confidential Physician Burnout Survey to determine the degree to which the division, as a whole, is at risk of burnout.
Data collection strategy:
The Maslach Burnout Inventory (MBI) was the tool used for physicians to self-assess their risk of burnout. The MBI explores three components: exhaustion, depersonalization and personal achievement. The MBI tool makes specific statements in each of these three

Department Summaries Clinical Audit Annual Report
Page 140 of 210
component areas and asks the responder to rate their frequency to the statements on a 7 point Likert scale. The tool was developed into an online confidential survey that was sent to each of the 20 members of the Division of Respirology. Members were asked to complete the online survey between November 20 and December 20, 2014. The online survey tool collected the confidential responses and provided a report of the anonymized aggregate results.
Results and Interpretation:
Participant response rate: 55% (11 of the 20 physicians)
SUMMARY RESULTS Section A: Burnoutiii: This section testifies to fatigue at the very idea of work, chronic fatigue, trouble sleeping, physical problems. For the MBI, exhaustion is a key component.
Total score of 17 or less: Low-level burnout Total score between 18 – 29: Moderate burnout Total over 30: High level burnout
Average score for Division: 12.37 Low-level burnout
Section B: Depersonalizationiii: This section examines “depersonalization” or loss of empathy. The notion of detachment is excessive leading to cynicism with negative attitudes with regard to patients or colleagues, feelings of guilt, avoidance of social contacts and withdrawing into oneself.
Total score of 5 or less: Low-level burnout Total score between 6 – 11: Moderate burnout Total over 12: High level burnout
Average score for Division: 7.08 Moderate burnout
Section C: Personal Achievementiii: This section focuses on the reduction of personal achievement. The individual assesses himself negatively, feels s/he is unable to move the situation forward. This component represents the demotivating effects of a difficult, repetitive situation leading to failure despite efforts. The person begins to doubt her/his genuine abilities to accomplish things.
Total score of 33 or less: High-level burnout Total score between 34 – 39: Moderate burnout Total over 40: Low level burnout
Average score for Division: 40.35 Low-level burnout

Department Summaries Clinical Audit Annual Report
Page 141 of 210
DETAILED RESULTS
Section A: Burnout Never
A few
times
per
year
Once a
Month
A few
times
per
month
Once a
week
A few
times
per
week
Everyday
Total
Responses
I feel
emotionally
drained by my
work.
0 (0%) 2 (18%) 2 (18%) 5 (45%) 1 (9%) 1 (9%) 0 (0%) 11
Working with
people all day
long requires a
great deal of
effort
2 (18%) 1 (9%) 2 (18%) 1 (9%) 0 (0%) 5 (45%) 0 (0%) 11
I feel like my work
is breaking me
down
4 (36%) 2 (18%) 2 (18%) 2 (18%) 1 (9%) 0 (0%) 0 (0%) 11
I feel frustrated
by my work.
2 (18%) 4 (36%) 3 (27%) 1 (9%) 0 (0%) 1 (9%) 0 (0%) 11
I feel I work too
hard at my job.
2 (18%) 3 (27%) 1 (9%) 3 (27%) 0 (0%) 2 (18%) 0 (0%) 11
It stresses me
too much to
work in direct
contact with
people.
7 (64%) 3 (27%) 0 (0%) 0 (0%) 1 (9%) 0 (0%) 0 (0%) 11
I feel like I am at
the end of my
rope
6 (55%) 3 (27%) 1 (9%) 1 (9%) 0 (0%) 0 (0%) 0 (0%) 11

Department Summaries Clinical Audit Annual Report
Page 142 of 210
Section B: Depersonalization Never A few
times
per year
Once a
Month
A few
times
per
month
Once a
week
A few
times
per
week
Everyday Total
Responses
I feel I look after
certain
patients/clients
impersonally, as if
they are objects
4 (36%) 4 (36%) 1 (9%) 1 (9%) 1 (9%) 0 (0%) 0 (0%) 11
I feel tired when I
get up in the
morning and have
to face another
day at work.
3 (27%) 4 (36%) 2 (18%) 1 (9%) 0 (0%) 1 (9%) 0 (0%) 11
I have the
impression that
my
patients/clients
make me
responsible for
some of their
problems.
3 (27%) 4 (36%) 1 (9%) 3 (27%) 0 (0%) 0 (0%) 0 (0%) 11
I am at the end of
my patience at end
of my work day
3 (27%) 4 (36%) 1 (9%) 2 (18%) 1 (9%) 0 (0%) 0 (0%) 11
I really don't care
about what
happens to some
of my
patients/clients.
9 (82%) 1 (9%) 1 (9%) 0 (0%) 0 (0%) 0 (0%) 0 (0%) 11
I have become
more insensitive to
people since I've
been working.
7 (64%) 2 (18%) 1 (9%) 1 (9%) 0 (0%) 0 (0%) 0 (0%) 11
I'm afraid this job
is making me
uncaring.
7 (64%) 2 (18%) 0 (0%) 2 (18%) 0 (0%) 0 (0%) 0 (0%) 11
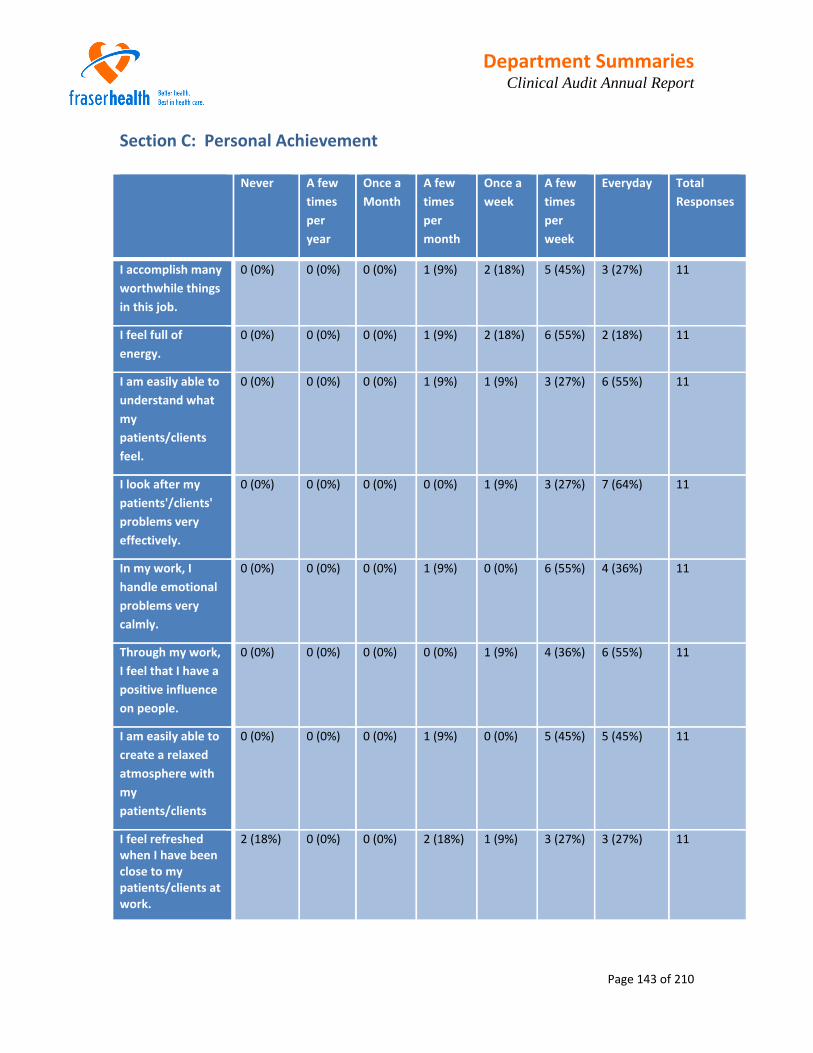
Department Summaries Clinical Audit Annual Report
Page 143 of 210
Section C: Personal Achievement Never A few
times
per
year
Once a
Month
A few
times
per
month
Once a
week
A few
times
per
week
Everyday Total
Responses
I accomplish many
worthwhile things
in this job.
0 (0%) 0 (0%) 0 (0%) 1 (9%) 2 (18%) 5 (45%) 3 (27%) 11
I feel full of
energy.
0 (0%) 0 (0%) 0 (0%) 1 (9%) 2 (18%) 6 (55%) 2 (18%) 11
I am easily able to
understand what
my
patients/clients
feel.
0 (0%) 0 (0%) 0 (0%) 1 (9%) 1 (9%) 3 (27%) 6 (55%) 11
I look after my
patients'/clients'
problems very
effectively.
0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (9%) 3 (27%) 7 (64%) 11
In my work, I
handle emotional
problems very
calmly.
0 (0%) 0 (0%) 0 (0%) 1 (9%) 0 (0%) 6 (55%) 4 (36%) 11
Through my work,
I feel that I have a
positive influence
on people.
0 (0%) 0 (0%) 0 (0%) 0 (0%) 1 (9%) 4 (36%) 6 (55%) 11
I am easily able to
create a relaxed
atmosphere with
my
patients/clients
0 (0%) 0 (0%) 0 (0%) 1 (9%) 0 (0%) 5 (45%) 5 (45%) 11
I feel refreshed when I have been close to my patients/clients at work.
2 (18%) 0 (0%) 0 (0%) 2 (18%) 1 (9%) 3 (27%) 3 (27%) 11

Department Summaries Clinical Audit Annual Report
Page 144 of 210
Evidence Based Practice/Medical Management Tools The work-up of patients with pleural effusions within FHA frequently includes a referral to Medical Imaging for an ultrasound guided thoracentesis. Studies and the FHA experience has shown that this approach often causes a to 2 day extension of the LOS of inpatients. Appropriate tests on the pleural fluid seldom performed on these cases. The efficient and highest quality approach for these patients is a same-day ultrasound guided thoracentesis at the bedside.
Recommendations:
1. Respirologists should see these patients on a priority basis and perform ultrasound guided thoracentesis at the bedside.
2. FHA is requested to ensure appropriate access to portable ultrasound machines to allow this procedure to be done at each site.
3. The Respirology Division is willing to Lead the development of a standardized Meditech order entry for all routine pleural fluid tests to allow for rapid order entry by clerical and lab staff, and
4. There should be a standard “kit” easily available at any site where thoracentesis is performed (in Radiology or at bedside). The “kit” should include the appropriate containers for the required pleural fluid tests and should be readily available for use by the respirologists and others. The very successful kit currently deployed at RMH could easily be used as a model.
Quality Improvement Initiatives The Respiratory therapists (RRT) assisting with the technical procedure of Endobronchial Ultrasound Transbronchial Needle Aspiration Biopsy (EBUS-TBNA) work as a team with the respirologist. A quality issue has arisen because of frequent changes in RRT staffing for EBUS procedures. Evidence shows that a small number specifically designated RRTs only should perform these tasks and should do so on a long term (several years) basis. Failure to do this results in inexperienced RRTs assisting, and increases the chance of errors, reduces the quality of specimens.
Recommendation: Managers should be required to appoint a minimal number of RRTs as principal assistants in the endoscopy suites when EBUS-TBNA procedures are being performed. In order to become technically proficient, the same RT should work with the EBUS team for several years without being rotated to other duties.
Scheduling of fibreoptic bronchoscopy should not be a barrier to the rapid evaluation of patients with lung cancer.
Recommendation: Patients with suspected lung cancer should receive priority access to bronchoscopy. An arbitrary limit to the number of diagnostic procedures for those patients should be eliminated. Respirologists are willing to work with Operational staff on scheduling systems.

Department Summaries Clinical Audit Annual Report
Page 145 of 210
Supporting Professional Development Royal Columbian Hospital Grand Rounds and Surrey Memorial Hospital group 2x/month case based rounds.
Eagle Ridge Hospital
Clinical Audit
Title: Time to cardiac catheterization for ACS/NSTEMI patients at Eagle Ridge hospital Phase:
Planning Designing Data Collection Analysis Reporting Background: The time to cardiac catheterization for an ACS/NSTEMI can be variable depending on patient stability, presence or absence of chest pain, troponin elevation, ECG changes, cardiac suite staffing, wait list etc. With the limited bed availability at ERH Monitored Care Unit (MCU), bed management is of utmost importance and the time to cardiac catheterization for ACS/NSTEMI patients must be optimized Objectives: To improve/optimize the wait for cardiac catheterization of admitted ACS/NSTEMI patients at ERH Patient Selection:
Inclusion criteria: 1. Age greater than 35 2. Admitted for ACS/NSTEMI with positive troponin +/- ECG changes
Exclusion criteria: 1. Unstable or stable angina with no troponin elevation 2. ACS/STEMI 3. Patients with ACS managed medically with no plans for cardiac catheterization
Time period: 6 months Data collection strategy: Prospective real time data collection recording the time to cardiac catheterization for ACS/NSTEMI patients at Eagle Ridge hospital

Department Summaries Clinical Audit Annual Report
Page 146 of 210
Morbidity and Mortality Rounds M & M review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. A total of 4 cases were reviewed of patients admitted for severe hyponatremia (Na< 120). For each chart, the diagnostic workup and treatment were reviewed.
Medical Management Review One review was performed triggered by a patient complaint. Learning point: Better patient education on management plan at time of discharge
Evidence Based Practice/Medical Management Tools New ACS protocols formulated by Fraser Health will be implemented at ERH.
Supporting Professional Development Monthly Internal Medicine Grand rounds via teleconference.
Surrey Memorial Hospital Short Stay Unit (SMH SSU)
Morbidity and Mortality Review
During the period of September 2013 to February 2014 M & M review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Three cases were reviewed. Learning points included: 1. Cardiac Involvement in Mixed Connective Tissue disease is more common than with
other connective tissue diseases. Recommendation: monitor ECG and Troponin in patients with undifferentiated CTD and cardiac or respiratory symptoms.
2. Complicated UTI includes pregnant patients, recurrent UTI’s, and Diabetics. Recommendation: use broader coverage of antibiotics in complicated UTIs and to consider early Infectious Disease consultation in this patient group.
3. Ensure dosing of IV acyclovir is weight based and there is pre-hydration
4. Recognize and manage acyclovir induced renal failure.
5. Recognize and manage post-infectious inflammatory conditions in viral meningitis.

Department Summaries Clinical Audit Annual Report
Page 147 of 210
Quality Improvement Initiatives
Initiation of Computerized Physician Order Entry (CPOE) internal medicine consultation to determine its effect on consult volume
SSMU audit of VTE Prophylaxis to determine initiation of automatic VTE orders at 48hrs
Development of SSMU specific DKA/HONK protocol
Supporting Professional Development Physicians mandated to receive Physician Workload Manager (PWM) training on
Meditech by June 01, 2014 in order to provide a continuous consult list and provide shared rounding lists on the new Neurology and Nephrology wards and SSMU
Royal Columbian Hospital Clinical Teaching Unit
Morbidity and Mortality Review
The CTU conducted morbidity and mortality review rounds for the purposes of evaluating and improving the quality of care provided. During the period July 26, 2013 – December 13, 2013, 13 cases were reviewed. Learning points included: 1. Regardless of the original reason for admission to CTU, a thorough History and
Examination needs to be done on all patients. 2. An effective communication style is necessary when discussing code status 3. The appropriate type and speed of Na correction is imperative in patients with
hyponatremia, including use of DDAVP. 4. When patients’ medications are changed during admission, we need to ensure the
patient has resources to pay, and that Special Authority forms are filled out and follow up occurs.
5. Consider use the LACE index to quantify readmission risk. 6. Need to involve the appropriate services when caring for patients with substance abuse. 7. Ensure adequate IV access when patients are transferred during the first 24 hours from
ICU or HAU areas to CTU, regardless of timing. 8. Clear discussion with patients and families is needed to ensure understanding of
reasons for and risks of not discontinuing medications prior to procedures. 9. VTE prophylaxis needs to be considered on all CTU admissions.

Department Summaries Clinical Audit Annual Report
Page 148 of 210
In January 2014, 13 cases were reviewed. Learning points included: 1. Need to improve communication between CTU, nephrology, psychiatry, medical RNs &
Psychiatry RNs. Take ownership for catheters you have placed even if someone else has suggested to D/C its use. Need to carefully review patients transferred to psychiatry as managing of lines/tubes is not within their scope of practice. Write in the order to remove all lines/tubes when transferring patients to psychiatry.
2. Anorexia Nervosa is a specialized medical condition that is best managed by a specialized multidisciplinary care team. It is often necessary on all fronts to set limits and establish treatment protocols to optimize success. A lack of expertise and appropriate monitoring can lead to undesired outcomes.
3. Anemia is important marker of disease in patients with MDS, and associated with increased CV risk such as cardiac remodeling, CHF, CAD, MI, Arrhythmia, & CV mortality. Studies suggest significant difference in overall survival in patients with Hemoglobin < 110 (male) and < 90 (female). Transfusion dependency an independently poor prognostic indicator of survival.
4. CAP in COPD is associated with high morbidity & mortality rates (5-15%) despite treatment. Comorbidities with COPD have been associated with a higher 30 & 90 d mortality rate (30 vs 21%). Treat patients aggressively. The use of 2 antibiotics in these patients decrease mortality.
5. Check doses carefully, especially when patients are sick or have comorbid disease states that may affect dosing (renal / hepatic insufficiency & pregnancy). Weigh benefit vs risk in all patients but particularly when potentially devastating outcomes such as preterm labour are a consideration.
6. Follow clinical status closely. When patients don’t respond to therapy as expected, go back to basics and reevaluate the patient with a broad differential. Establish code status early with the patient and family to ensure you advocate for patient safety (monitored in the appropriate setting). Pts transferred out of high acuity units should be watched closely particularly for early signs of rapid decompensation.

Department Summaries Clinical Audit Annual Report
Page 149 of 210
Medical Imaging Regional Department Head: Dr. Spencer Lister (to May 2014)
Regional Department Medical Quality Committee Activities
Meeting Dates: May 27,2013, June 24, 2013, September 9, 2013, October 15, 2013, December 16, 2013, January 15, 2014, February 19, 2014, March 10, 2014, April 14, 2014, May 12, 2014
Clinical Audit
1. Title: Medical Imaging Examination Report Turn Around Time
Summary:
Regular monthly reporting of medical imaging report turnaround time is now implemented. Reports are posted every month on the Department sharepoint site, and are accessible to all FH physicians and staff. Mean and 90th percentile statistics are reported for every modality and site, for every step in the report production process. The data is used to celebrate and learn from success and to identify opportunities for improvement. Examples of Success:

Department Summaries Clinical Audit Annual Report
Page 150 of 210
Once speech recognition is fully implemented (June2014), additional gains are expected.
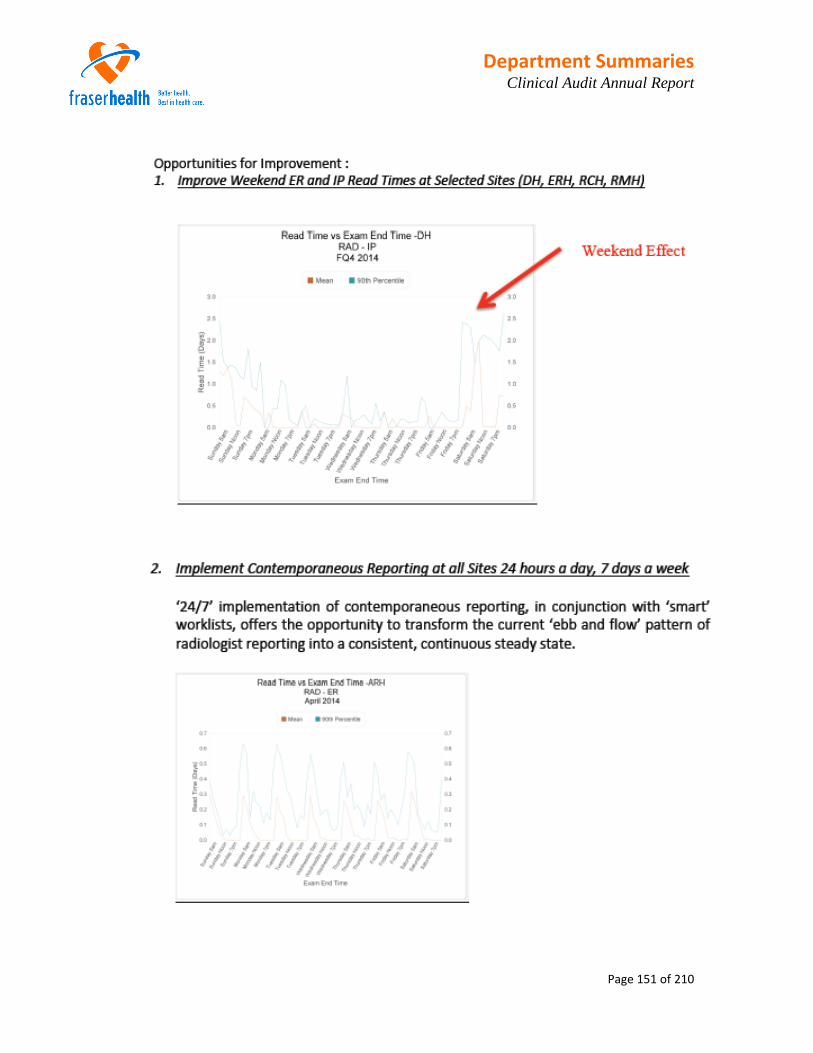
Department Summaries Clinical Audit Annual Report
Page 151 of 210

Department Summaries Clinical Audit Annual Report
Page 152 of 210
Background: Medical Imaging examination and report turnaround time has been identified by referring physicians and staff from other departments and programs as a factor which impacts access and flow in the acute care setting.
Objectives: 1. To measure the average turnaround time each month for each step in the medical
imaging report production process. 2. To deliver granular data to sites and department members demonstrating how
individual sites, modalities and physicians contribute to report turnaround time 3. To increase awareness of site, modality and individual contributions to report
turnaround time, thereby enabling front line staff and physicians to change performance
Patient Selection: All patients, all examinations
952,942 Examinations in 2011:
267,197 IP 212,170 ER 473,575 OP

Department Summaries Clinical Audit Annual Report
Page 153 of 210
1,006,107 Examinations in 2012
280,624 IP 223,811 ER 501,672 OP
935,236 Examinations in 2013 (YTD)
267,719 IP 214,841 ER 452,676 OP
Time period: January 1, 2011 – November 30, 2013
Data collection strategy: A Meditech report is generated for each month which includes the following data fields:
Site
Dictating Physician
Modality
Meditech Procedure Mnemonic
Patient Registration Status (IP, OP or ER)
6 Time Stamps
Each month’s Meditech report data is then imported into a 64 bit database (Filemaker 12) with an integrated presentation layer. Data is presented in various ways to illustrate different forms of variation in the report production process (examples: by site, by registration status, by modality, by time of day, by day of week) Results: Reporting of data commenced in March 2012. A change in performance followed which was sustained, with continued improvement. In the inpatient population (fig 6):
Mean dictation time for inpatient exams decreased from 15 hours (2011) to 11 hours (2012), to 10 hours (2013) a 33% decrease across a projected annual exam volume of 292,000 exams.
36,589 fewer days waiting in the inpatient setting for an examination to be dictated in 2012 compared to 2011.
12,205 fewer days waiting in the inpatient setting for an examination to be dictated in 2013 compared to 2012
This improvement occurred in the setting of a 9% increase in projected IP exam volume in 2013 compared to 2011.

Department Summaries Clinical Audit Annual Report
Page 154 of 210
In the emergency room patient population (fig 6):
Mean dictation time for emergency patient exams decreased from 14 hours (2011) to 13 hours (2012), to 12 hours (2013) a 17% decrease across a projected annual exam volume of 226,425 exams.
10,042 fewer days waiting in the ER setting for an examination to be dictated in 2012 compared to 2011.
10,220 fewer days waiting in the ER setting for an examination to be dictated in 2013 compared to 2012
This improvement occurred in the setting of a 7% increase in projected ER exam volume in 2013 compared to2011.

Department Summaries Clinical Audit Annual Report
Page 155 of 210
In the transcription time component (fig 7):
Transition to a speech text dictation system is expected to result in substantial gains in overall report turnaround time.
The transition period has presented project challenges as well as challenges with retention of medical transcription staff which has resulted in significant increases in transcription turnaround time (fig7)
Where speech text dictation has been implemented, transcription turnaround times have dropped 98.5% in a 1 month period (134 hours November 2013 with non-speech text users vs 2 hours November 2013 with speech text users). Continued improvement is expected as this marked change has occurred in the setting of new users and project challenges.
Actions: A dedicated desktop server has been resourced to maintain, automate and further build on this audit and reporting activity. The Fraser Health Business Analytics team is developing an interactive online tool to further enhance and build on this work.
Continue with regular publishing and discussion of monthly turnaround time reports with all stakeholders.

Department Summaries Clinical Audit Annual Report
Page 156 of 210
Incorporate statistics on outpatient population to the report (where data exists). Comment: A similar approach could be applied to any department or program wishing to analyze a process in which Meditech time s tamps are recorded.
2. Title: Imaging Guided Lung Biopsy Yield and Results – Follow Up Audit
Phase: Planning Designing Data Collection Analysis Reporting
Background: Variation in lung biopsy method and biopsy yield has been observed. An audit performed in 2012 identified a need to adjust audit methodology to compare biopsy results with biopsy method. Objectives: To quantify variation in lung biopsy yield and method across all sites. Patient Selection and Time Period: A clinical audit of all CT guided lung biopsy procedures from June 1, 2012 to May 31, 2013 was performed. Data collection strategy: Data was obtained by reviewing biopsy reports in PACS and Meditech charts. All cases with mortality within 30 days of biopsy underwent chart review to determine whether the biopsy was a cause of death. Results: 355 procedures were performed. The FNA rate has decreased compared to the previous audit and is now at approximately 8% (92% core biopsy). Analysis of yield and procedure related mortality is underway. Actions: Presented to RDMQC in February 2014 for review and recommendations. RDMQC recommendations:
All sites to aim for 50% core biopsy rate
Radiologists performing core biopsies of lung should follow recommended technique.

Department Summaries Clinical Audit Annual Report
Page 157 of 210
3. Title: CT Pulmonary Angiography Diagnostic Yield
Phase: Planning Designing Data Collection Analysis Reporting
Background: A clinical decision rule using Well’s criteria and highly sensitive D-dimer (ELISA) has been previously demonstrated to safely improve CT Pulmonary Angiography yield. Yields in the 15-20% range have been safely achieved at some institutions. Objectives: To measure CT pulmonary angiography yield across all sites in the ER patient population.4 Patient Selection and Time Period: A clinical audit of CT angiograms from January 1, 2012 to June 30, 2013 was performed. 40 examinations from each site were randomly selected. Data collection strategy: Data was obtained by reviewing examination reports in PACS. Exams were scored using an audit database. Results: 400 procedures were reviewed (10 sites x 40 exams per site)

Department Summaries Clinical Audit Annual Report
Page 158 of 210
Discussion: The results of this audit and prior published work suggest:
An opportunity exists to improve CTPA yield across most sites
Clinical decision rules and D-dimer can be used to safely increase CTPA yield
Actions:
Presentation to VCH Board January 22, 2014 (Lower Mainland Program Quality and Utilization Initiative
Presentation to RDMQC in February 2014 for review and recommendation
Sharing of results with ER program and physicians
Sharing of results with Medical Imaging program and physicians
Follow-up Actions since February 2014:
Development of an online tool on RCH ER website which generates a validation code (derived from Wells score) when ordering a CT Pulmonary Angiogram: http://www.rchemerg.com/var/storage/wells.php

Department Summaries Clinical Audit Annual Report
Page 159 of 210
Added a field to CTPA order entry page in Meditech to capture validation code, enable retrospective analysis of code use and to inform future utilization management / appropriateness efforts.
More information: http://www.rchemer.com/academics/academic-projects-at-ERH-and-RCH/FHA-study-assessment-of-CTA-usage-to-diagnose-pulmonary-embolism
4. Critical Results Accreditation Standard Compliance Audit
Phase: Planning Designing Data Collection Analysis Reporting
Background: Failure to communicate critical medical imaging results is an established cause of harm to patients. In the United States, failure to communicate is a factor in approximately 80% of successful personal injury litigation involving radiologists and medical imaging facilities.1
The Diagnostic Accreditation Program (operated by the CPSBC) sets out mandatory accreditation criteria for a diagnostic facility’s critical result communication policy. The term ‘critical result’ in this context refers to:
Findings that suggest a need for an immediate or urgent intervention
Findings that are discrepant with a preceding interpretation of the same examination and where failure to act may adversely affect patient health
Findings that may be seriously adverse to the patient’s health and are unexpected by the treating or referring physician
Objectives: To assess current critical result communication practice against the DAP mandatory accreditation standard. Patient Selection and Time Period: All non-contrast CT head examinations were reviewed from a single day in January (January 15, 2014) Data collection strategy: Examination reports were assessed for the presence or absence of a critical result. Examination reports with a critical result were further characterized with regard to:
‘level of urgency’ of the result using a colour code system (‘red’, ‘orange’, ‘yellow’ as described in an effective critical result policy at another facility)2
Critical result communication compliance with the DAP 2010 accreditation standard (final report notes confirmed receipt of critical result communication including name of person receiving result, date and time of communication and mode of communication; i.e. “Dr Surgeon notified of these findings by Dr Radiologist at 0930h April 2, 2014 on the telephone.”)

Department Summaries Clinical Audit Annual Report
Page 160 of 210
Results: 141 non contrast CT Head examinations were performed on January 15, 2014. The report for each of these examinations was reviewed. 20 reports (14%) contained a critical result, 121did not. Of the 20 reports containing a critical result, 1 was ‘level red’ (acute subdural hemorrhage), 14 were ‘level orange’, and 5 were ‘level yellow’. Of the 20 reports containing a critical result, 1 report was compliant with the DAP critical result communication accreditation standard, 19 were not (no documented communication).
Actions: These results were reviewed with RDMQC members. RDMQC members agreed the current FH critical result policy is not compliant with the 2010 DAP Accreditation Standard, and requires revision. The opportunity to lead critical result communication policy redevelopment was extended to RDMQC members. Members noted that communication of critical results may be occurring even though communication may not be documented in the report. Members supported a request that all radiologists document critical result communication in final reports. Members supported inclusion of referring physician contact information in the speech text report window to facilitate improved critical result communication.
5. XR and CT Utilization Trends in the ER Setting
Phase: Planning Designing Data Collection Analysis Reporting
Background: Strategies to decrease inappropriate utilization of imaging enable safer care by reducing population dose of ionizing radiation. Strategies to decrease inappropriate utilization allow scare medical imaging human and financial resources to be used more effectively. Objectives: To establish a baseline understanding of the trends in XR and CT utilization across FH in the ER setting.

Department Summaries Clinical Audit Annual Report
Page 161 of 210
Patient Selection and Time Period: All ER CT and XR exams were included in the analysis from January 2011 to August 2013. Data collection strategy: A graphic report was prepared using the department exam database. Snapshots of ER activity from period 7 11/12 vs period 7 13/14 were obtained to compare changes in imaging activity to changes in ER visit volume and to assess for any changes in CTAS scores in ERs. The ‘XR:CT Ratio’ was reported. Results: The utilization ratio of XR to CT has been decreasing across FH sites over the last 2.5 years. This change is due to an increase in CT demand. XR demand has been stable. This trend is seen in most sites with the exception of RCH (which also has the lowest ratio of XR:CT utilization). CTAS case mix was stable over a 2 year period at most sites (except SMH). Increases in ER visits did not account for the increase in utilization.

Department Summaries Clinical Audit Annual Report
Page 162 of 210

Department Summaries Clinical Audit Annual Report
Page 163 of 210
Actions:
Presented to FH CIEC
Presented to FH Health Technology Assessment Committee
Discussion amongst Medical Imaging Department Heads
Presentation to VCH Board January 22, 2014 (Lower Mainland Program Quality and Utilization Initiative)
6. Title: Quality of Order Entry
Phase: Planning Designing Data Collection Analysis Reporting
Background: Awareness of pertinent clinical history and the reasons for ordering medical imaging examinations enables radiologists to provide more accurate reports. ‘Reasons for Examination’ and ‘Pertinent History’ fields must be completed every time an imaging examination is ordered in Meditech. Entry of at least one character is required in each field. Objectives: To determine how often the ‘Reasons for Examination’ and ‘Pertinent History’ fields are left ‘blank’ (single character). To develop an initial understanding of the characteristics of the data in these fields, to inform future analysis and quality improvement approaches. Patient Selection and Time Period: All August 2013 ER and IP exams. Data collection strategy: Department database reports were developed to report the frequency of ‘blank’ (single character) ‘Reasons for Examination’ and ‘Pertinent History’ fields. Results: ‘Reasons for Examination’ fields were rarely blank. ‘Pertinent History’ fields were often blank. Substantial variation was demonstrated across sites (table 3,4) and units (not shown). Variation was more closely linked to the order entry person rather than the ordering physician (not shown).

Department Summaries Clinical Audit Annual Report
Page 164 of 210

Department Summaries Clinical Audit Annual Report
Page 165 of 210
Discussion: Further assessment of this issue presents challenges:
Free text order entry fields are difficult to quantify
‘non-blank’ fields are not necessarily useful
More thought is needed on ways to analyze and improve the quality of order entry. The distinction between ‘pertinent history’ and ‘reasons for exam’ may not be apparent to some users. In some cases the information is redundant.
7. Title: Lower Mainland Standardization of Head CT Protocol
Phase: Planning Designing Data Collection Analysis Reporting
Background: Regular review of CT Head Radiation Dose was initiated by the Lower Mainland Medical Imaging Program as required under Radiation Safety Code 35. The results of the review demonstrated substantial variation in CT head radiation dose across Fraser Health sites. A standards, dose optimized CT head protocol was developed by the Regional CT Medical Practice Lead and the Lower Mainland Program Physicist. Objective: Reduction of radiation dose to as low as reasonably achievable. Patient Selection and Time Period: All sites Data collection strategy: Feedback is being collected from 5 exams per site on image quality after protocol adjustment.
8. Title: Thyroid Biopsy Yield
Phase: Planning Designing Data Collection Analysis Reporting
Background: Significant variation in thyroid FNA yield is believed to exist between Fraser East sites and other sites. The magnitude of variation and causes of variation are unknown. Objectives: To compare thyroid FNA yield across sites and amongst different operators.

Department Summaries Clinical Audit Annual Report
Page 166 of 210
9. Title: Recommendation Rates
Phase: Planning Designing Data Collection Analysis Reporting
Background: Medical imaging demand is driven by requests from non-radiologist care providers. Sometimes these requests are a response to a radiologist’s recommendation to perform additional imaging tests. These recommendations are contained in reports and contribute to medical imaging demand. Some institutions have set recommendation rate “benchmarks”, and regularly measure this parameter of department, site and individual performance as a component of their quality improvement programs.
Objectives: 1. To develop an initial understanding of ‘recommendation rates’ in Fraser Health across
sites, modalities and amongst individual radiologists. 2. To understand the degree to which radiologist recommendations contribute to medical
imaging demand in Fraser Health. 3. To determine where variation exists. 4. To promote discussion on the reasons (or lack thereof) for observed variation. 5. To develop strategies to reduce unexplained variation in recommendation rates in an
effort to reduce inappropriate utilization of scarce medical imaging resources.
Patient Selection and Time Period: A sample of 10 contrast CT abdomen and pelvis examinations were randomly selected for every radiologist in Fraser Health from the 2013 calendar year. Data collection strategy: The report for each sampled examination was assessed for the presence or absence of a recommendation for additional imaging. Results: 948 reports were reviewed (94 Radiologists had a sample of 10 exams, 1 Radiologist had a sample of 7 exams, 1 Radiologist had a sample of 1 exam) 28% of examinations included a recommendation for additional imaging, 72% did not. Some of the recommendations seemed subjectively appropriate to the radiologist auditor. Some recommendations could not be characterized as appropriate (recommending follow-up imaging without a reason). Some of the recommendations fell into categories for which consensus guidelines exist, but may not have been followed.

Department Summaries Clinical Audit Annual Report
Page 167 of 210
Discussion: Subgroup analysis of the positive recommendation group may be informative and used to guide future quality of care / appropriate utilization initiatives. Actions: Regional department members supported subgroup analysis. Confidential sharing of each radiologist’s individual results did not receive support at the RDMQC.
10. Title: Breast Imaging Reporting and Data System (BIRADS) Final Assessment Category –
Third Audit
Phase: Planning Designing Data Collection Analysis Reporting
Background: The use of BIRADS final assessment categories in breast imaging reports is an established and accepted standard of practice amongst radiologists. The FH Division of General Surgery requested through the Division Head that Members of the MI Regional Department include a BIRADs Final Assessment Category in every diagnostic breast imaging report. Use of BIRADS Final Assessment Categories in reports is useful to our surgical colleagues. Use of BIRADs Final Assessment Categories reduces ambiguity in follow up recommendations. Use of BIRADs Final Assessment Categories facilitates audit of reports for

Department Summaries Clinical Audit Annual Report
Page 168 of 210
incomplete follow up (BIRADs 0), as well as correlation with outcomes and refinement of reporting processes. A clinical audit of all breast imaging (excluding MR) examinations from a single day in December 2011 was performed previously. This initial audit demonstrated that 60% of reports did not include a BIRADS Final Assessment Category. Objectives: 1. To document and report on the use of BIRADs Final Assessment Categories in breast
imaging reports across sites, and amongst individual radiologists. 2. To promote greater awareness of performance at the site and individual radiologist
level. 3. To increase the frequency of BORADS Final Assessment Category use in breast imaging
reports. Patient Selection and Time Period: September to October 2013. 5 randomly selected breast imaging reports per radiologist. Data collection strategy: Data was obtained by reviewing examination reports in PACS. Exams were scored using an audit database. Results: Results were distributed to all radiologists using a standard reporting letter which included an introduction letter, and FAQ and a report page summarizing aggregate results and reporting the individual’s results along with the accession numbers of the 5 randomly selected exams which were audited.

Department Summaries Clinical Audit Annual Report
Page 169 of 210
Discussion:
The frequency of BIRADs final assessment categories in mammography reports has increased from 40% to 76% across Fraser Health since the first ‘single day’ audit conducted in 2011.
The frequency of BIRADs final assessment categories in breast ultrasound reports has increased from 38% to 54% across Fraser Health since the first audit conducted in 2013.
The frequency of BIRADs final assessment categories in breast MRI reports has increased from 40% to 100% across Fraser Health since the first audit conducted in 2013.
Morbidity & Mortality Review
During the period of May 2013 to May 2014 morbidity and mortality reviews were conducted for the purpose of evaluating and improving the quality of patient care provided. 8 patient cases were selected for review with the resulting learnings and recommendations:
Critical results must be communicated. The Critical Result Communication policy
has since been redeveloped and a critical result communication audit has taken
place.
Quality Improvement Initiatives
Title: Contemporaneous 24/7 Reporting of Medical Imaging Examinations –Update
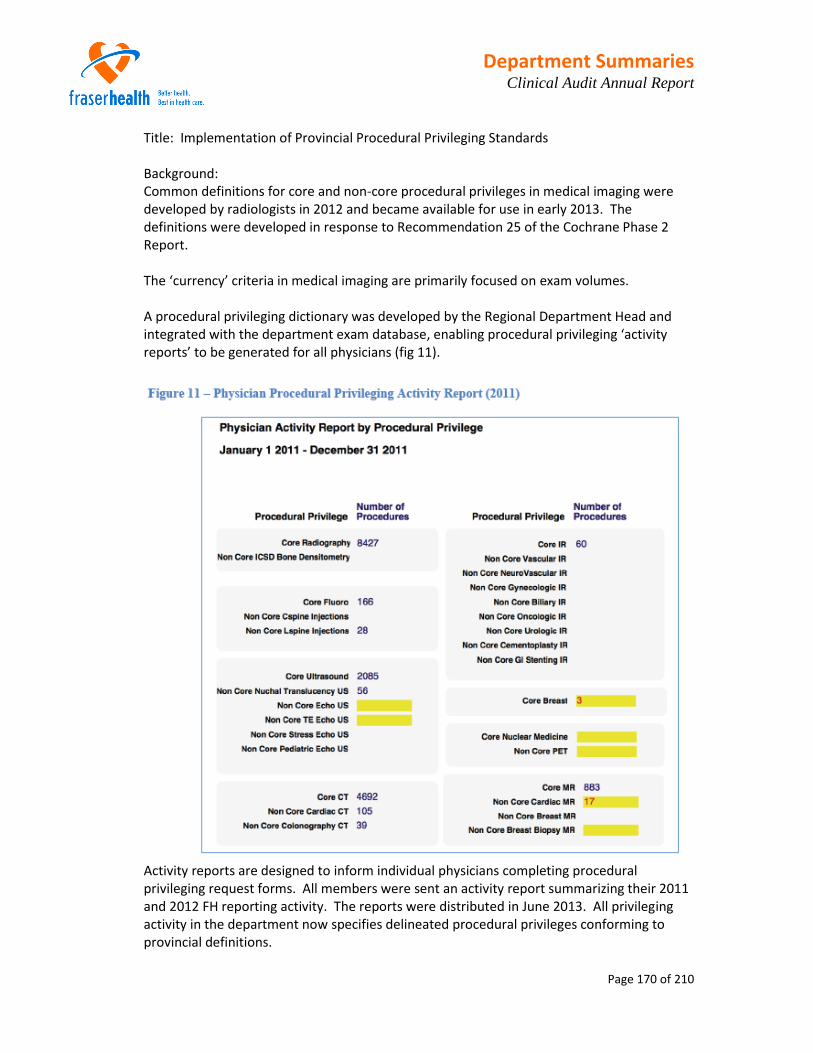
Department Summaries Clinical Audit Annual Report
Page 170 of 210
Title: Implementation of Provincial Procedural Privileging Standards Background: Common definitions for core and non-core procedural privileges in medical imaging were developed by radiologists in 2012 and became available for use in early 2013. The definitions were developed in response to Recommendation 25 of the Cochrane Phase 2 Report. The ‘currency’ criteria in medical imaging are primarily focused on exam volumes. A procedural privileging dictionary was developed by the Regional Department Head and integrated with the department exam database, enabling procedural privileging ‘activity reports’ to be generated for all physicians (fig 11).
Activity reports are designed to inform individual physicians completing procedural privileging request forms. All members were sent an activity report summarizing their 2011 and 2012 FH reporting activity. The reports were distributed in June 2013. All privileging activity in the department now specifies delineated procedural privileges conforming to provincial definitions.

Department Summaries Clinical Audit Annual Report
Page 171 of 210
Peer Review
Title: Peer Review Program Background: A peer review program was initiated in January 2012. Objectives: To enable colleagues to provide each other with confidential feedback regarding report
content. To improve patient care. Patient selection: 2% of the previous week’s reported CT examinations are randomly selected for inclusion in the peer review system. Cases are randomly assigned to radiologists. The reviewer assigns a score regarding level of agreement with the report content for each reviewed case. The original interpreting physician receives these comments by hospital mail. Reviewer identify is withheld. Discrepancies which are determined to be clinically significant by the reviewer are fast-tracked. Time period: January 2012 to May 2014 Data collection strategy: The cases are presented to each reviewer through a username/password protected website on the corporate network. A web form is completed by the reviewing radiologist. Results:

Department Summaries Clinical Audit Annual Report
Page 172 of 210
Mental Health and Substance Use (MHSU) Regional Department Head: Dr. Terry Isomura
Regional Department Medical Quality Committee Activities
Meeting Dates: September 23, 2013, November 4, 2013, January 6, 2014, March 3, 2014
Division of Tertiary Psychiatry Medical Quality Committee Meeting Dates: October 10, 2013, January 9, 2014
Division of Geriatric Psychiatry Medical Quality Committee
Meeting Dates: October 24, 2013, January 23, 2014 Division of Child, Youth and Young Adult Psychiatry Medical Quality Committee
Meeting Dates: February 7, 2014 Surrey Memorial Hospital, Department of Psychiatry, Medical Quality Committee
Meeting Dates: March 28, 2014 Peace Arch Hospital, Department of Psychiatry, Medical Quality Committee
Meeting Dates: December 12, 2013 Abbotsford Regional Hospital, Department of Psychiatry, Medical Quality Committee
Meeting Dates: March 21, 2014 Chilliwack General Hospital, Department of Psychiatry, Medical Quality Committee
Meeting Dates: December 13, 2013
Clinical Audit 1. Title: Polypharmacy and high dose antipsychotics
Division: Tertiary Psychiatry Phase:
Planning Designing Data Collection Analysis Reporting
Background: Although there is little evidence to support the use of polypharmacy and high dose antipsychotics, both practices are widespread and believed to be associated with increased side effects

Department Summaries Clinical Audit Annual Report
Page 173 of 210
Objectives: To determine the prevalence of this practice and understand the reasons for it. This builds on and extends an audit completed last year.
Patient Selection: All patients in Fraser health adult Tertiary Psychiatric facilities. Time period: TBC Data collection strategy: chart review of current patients – Feb 2014
Physician participation rate: all physicians in the division have agreed to take part
2. Title: Anticholinergic load in patients admitted to tertiary geriatric psychiatry units.
Division: Tertiary and Geriatric psychiatry
Phase: Planning Designing Data Collection Analysis Reporting
Background: Recognized that anticholinergic side effects of medication are common and can have cumulative negative effect on the geriatric population. Objectives: To determine the total anticholinergic “load” in a sample population and relation to behavior/outcome with a view to plan a larger study. Patient Selection: Patients in a Fraser health older adult Tertiary facility – Oceanside who have been admitted for more than one month. Time period: Data collection Dec 4, compared to admission data Data collection strategy: chart review and PharmaNet search.
Physician participation rate: all physicians in the division have agreed to take part

Department Summaries Clinical Audit Annual Report
Page 174 of 210
Chart Review
Ridge Meadows Hospital, Department of Psychiatry conducted a review on readmissions to the inpatient unit. Readmission rates were high when compared to other sites. Almost all of the admissions were related to substance use issues and lack of adherence to the treatment recommendations.
RCH Department of Psychiatry – Main learning point from this case review was reporting to MCFD when a child is involved.
PAH Department of Psychiatry – Lessons were drawn regarding consent, transference and the ongoing need for renewed treatment goals and proper documentation.
CGH Department of Psychiatry – Lessons were drawn regarding communication with GP for assessment of medical needs and vital signs documentation.
Morbidity & Mortality Review
At the Regional Departmental Quality Committee in October it was agreed that each Division and Department would review any level 4 and 5 events, as well as any trends in less serious events at their quality meetings.
Division of Geriatric Psychiatry
During the period of August 2013 to March 2014 morbidity and mortality reviews were conducted for the purpose of evaluating and improving the quality of patient care provided. 2 patient cases were selected for review with the resulting learnings and recommendations: no recommendations.
Division of Adult Psychiatry
During the period of August 2013 to March 2014 morbidity and mortality reviews were conducted for the purpose of evaluating and improving the quality of patient care provided. 9 patient cases from SMH were selected for review with the resulting learnings and recommendations:
Physician reminder with relation to requirement for written order for restraints.
Physicians to be reminded to complete physician orders in chart and to sign all relevant documents. Routine Chart Audits (CNE) of ED presentations will occur effective 2014.
Review protocols with Coast Foundation/Timbergrove with relation to process for advising tenants of eviction. Ensure case manager aware and participates and supports the client during an eviction process.

Department Summaries Clinical Audit Annual Report
Page 175 of 210
Recommend review of New Therapeutic Leave Policy/Procedure to determine if concerns raised in this PSLS event are addressed.
Recommending level 3 therapeutic leaves from PHAU/PICU’s are discussed regarding efficacy and procedure if granted to check for contraband.
Tracking tool: Constipation Management Sheet to be implemented at Care Facility with immediate effect.
Consultation with relation to placement options should occur when clients are not succeeding in their living environments.
Contracted facility staff to be advised that they cannot leave an Emergency Department with one of their clients until the patient has been seen by an ERP.
Format of regular meetings at facility will be improved via introduction of a standardized checklist to include details of care such as GP visits, Dental, Bowel Checklist, Metabolic recording. Quarterly review notes to be forwarded to GP.
Improve Communication with Probation Services by establishing regular meetings with Probation Services and by educating probation services about MHSU.
Develop a system to ensure Communication Binder is updated and kept current.
Facility MOC or MHC Case Manager to call ahead to the MHSU Zone PCC at SMH to alert them to a CRP transfer. MHSU PCC to track these patients.
Consultation with relation to placement options should occur when clients are not succeeding in their living environments.
2 patient cases from RMH were selected for review with the resulting learnings and recommendations: no recommendations
Division of Tertiary Psychiatry
During the period of August 2013 to March 2014 morbidity and mortality reviews were conducted for the purpose of evaluating and improving the quality of patient care provided. 3 patient cases were selected for review with the resulting learnings and recommendations:
Improved response time (Emergency response was 35 minutes)
Increase staffing presence during higher risk times; including observation.
Training suction machine and swallowing are included in staff orientation. Care plan development training.
Development of OT referral form completed
All small plastic containers cream/milk to be removed from the unit. All garbage containers to be kept in safe location.
Collateral must be obtained from Forensic and Pre-trial facilities for patients who present at the ED’s after a recent discharge from these facilities.
Patient Discharge Planning processes to be improved, to include patient discharge instructions which contain specific information on discharge destination and clinical follow-up.

Department Summaries Clinical Audit Annual Report
Page 176 of 210
Division of Child, Youth and Young Adults
During the period of August 2013 to March 2014 morbidity and mortality reviews were conducted for the purpose of evaluating and improving the quality of patient care provided. 2 patient cases were selected for review with the resulting learnings and recommendations:
When youth do not engage and there is a plan to refer to another service, clinician to ensure transition of care is completed by contacting service provider referred to or with the youth/family, and documenting in client chart
Risk assessment and follow up with transitioning clients must be done in a timely manner. Develop method for flagging Coordinator of high suicide risk clients that do not go through the intake process but are transitioned between MHC, teams, CYMH to Adult MH.
Evidence Based Practice/Medical Management Tools
The EPI, PTOP & ACT Programs are developing an antipsychotic algorithm for the use of Clozapine based on the guidelines developed by Dr. Ofer Agid, Centre for Addiction & Mental Health (CAMH), Toronto. Dr. Agid presented to EPI, PTOP and ACT physicians on November 15, 2013.
Prescribing Observatory for Mental Health – POMH-UK The vast majority of patients who come under specialized mental health care within the Fraser Health Authority will be prescribed some form of psychopharmacologic agent as part of their treatment program. These treatments will often be required on a long-term basis. Most patients being treated with psychopharmacologic agents require various forms of monitoring to reduce harmful side effects. The choice of specific psychopharmacologic drugs should be based on a knowledge of the evidence base supporting their use in specific clinical situations. Proper prescribing and monitoring of psychopharmacologic agents is a significant quality issue within the mental health and substance use portfolio. At present, we have a less than optimal understanding of how psychiatric prescribing and monitoring practices within our health authority as a whole align with evidence-based standards. In line with our goals of striving for optimal practice, quality assurance and improvement in the area of psychiatric prescribing and monitoring, the MHSU Executive has decided to become a member of the Prescribing Observatory for Mental Health – UK (POMH-UK) Quality Improvement Programmes, an organization with voluntary member NHS Mental Health Trusts, whose goal is quality improvement in the area of psychiatric medication prescribing, monitoring and treatment.

Department Summaries Clinical Audit Annual Report
Page 177 of 210
Suicide Risk Management – Clinical Policy & Suicide Risk Management – Clinical Practice Guideline On April 1st 2014, the Suicide Risk Management CPG and Clinical Policy will be implemented for all MHSU staff/physicians as part of their regular practice. Practice Changes:
All individuals will be screened for warning signs and key suicide risk factors upon initial contact with any mental health and substance use service
If the screening process identifies a potential heightened risk for suicide, and after the individual’s immediate safety is ensured, then a complete in-depth assessment will be completed within 24 hours. Novel assessment factors include assessment confidence and changeability.
Anyone at heightened risk for suicide will have a care plan that includes environmental safety guards and therapeutic interventions. Recommended therapeutic interventions include a safety plan, combination of universal Interventions and some specialized interventions if available. “No-harm contracts” are not supported.
Monitoring frequency should be determined by the identified degree of risk and the clinical complexity of the individual.
Staff and Physicians will document useful and appropriate client information in the health record, according to organizational and professional standards and guidelines.
Performance Review/Clinical Performance Appraisal
To improve physician performance and quality of patient care, the Department of MHSU is designing and implementing a specific Physician Practice Professional Development Process for MHSU physicians in Fraser Health. This process will provide a structured format to guide the discussions between department/division/site leaders and individual members of the department for the purposes of practice improvement and personal development. The process includes: • Self-evaluation completed by the physician • Physician practice profile –quantitative information about the physician’s patient case
load over the past year • Feedback from Peers – online 360o tool to collect anonymous multi-source feedback • Development of a personal development plan and discussion with a trusted advisor. Pilot and Evaluation A pilot of the consisting of the 3 parts: self-evaluation, physician practice profile and 3600
multisource online feedback tool will be conducted with 20-25 participating physicians May 20 – June 20, 2014.

Department Summaries Clinical Audit Annual Report
Page 178 of 210
Following the pilot, a formal evaluation of the performance review tool and process will take place.
Implementation A tentative date for the implementation of the performance review tool across the
Department has been set for late Fall 2014.
Supporting Professional Development
September 20, 2013 - Sponsored and organized 7th Pacific Psychopharmacology Conference
September 23, 2013 - Guest Speaker, Prof Tim Kendall, Director, NCCMH, Royal College of Psychiatrists: Critical review of evidence for community mental health services to regional department heads and RCH rounds.
Eighty physicians attended the Regional Physicians Update on February 20, 2014. Agenda topics included: Update on the Mental Health Act, Suicide Risk Assessment Clinical Practice Guideline, Learnings from PTOP: Clozapine and Myocarditis, and Opioid Overdose: harmful benzodiazepine prescribing. Each Division Head presented an update on their division and Dr. Terry Isomura updated the physicians on the Physician Professional Development Tool being implemented for physicians in the MHSU Program.
Tertiary Division rounds
Date Topic Presenter
Sept. 25, 2013 Dialectical Behaviour Therapy Gail Howell-Jones
Oct. 23, 2013 Pharmacy Student presentation Charles Yu
Nov. 27, 2013 Recovery Centered Clinical System (RCCS) case study
Maryam Daftariar
Adult Division rounds Consult Liaison Lecture Series Date Topic Presenter
Oct. 3, 2013 Updates in the treatment of Bipolar Disorder Dr. David Bond
Jan. 15, 2014 QTc Prolongation, TdP, Psychotropics Dr. Megan Roberts

Department Summaries Clinical Audit Annual Report
Page 179 of 210
RCH CME (with videoconference to PAH & SMH) Date Topic Presenter
Sept. 24, 2013 Guidelines for Psychosis Dr. Tim Kendall
Oct. 8, 2013 OCD Dr. E. Stewart
Nov. 12, 2013 Resident Grand Rounds Simon Woo
Dec. 10, 2013 He, She, They: Gender Dysphoria in the Psychiatry Office
Brynn Fredricksen
Jan. 14, 2014 Near Death & Related Experiences from a Psychiatry Perspective
Dr. Tony Benning
Feb. 11, 2014 The Paradox of Diagnostic Certainty: A case study Dr. Ambrose Cheng
Mar. 11, 2014 Psychotherapy in Psychiatric Training George Hadjipavlou
RCH Rounds Date Topic Presenter
Dec. 4, 2013 Geriatric Psychiatry - Alzheimer's Treatment Dr. Salina Chan
Feb. 4, 2014 Psychotherapy – Motivational Interviewing Mark Goheen
Feb. 19, 2014 Reproductive Psychiatry–Perinatal Bipolar Disorder Dr. Tricia Bowering
March 4, 2014 Psychotherapy Rounds – CBT and Insomnia Dr. Julius Elefante
Burnaby Mental Health & Addiction Services Continuing Education Date Topic Presenter
Sept. 20, 2013 Responding to HIV and other challenges in Vancouver’s Downtown Eastside
Dr. Evan Wood
Oct. 18, 2013 Violent Behaviour and Psychopathy: A Case Study Dr. J. Ronsley & Constable R. Kalman
Nov. 15, 2013 DSM 5-Development, Organization & Focus on some changes
Dr. Ian Forbes`
Jan. 17, 2014 M&M's: Metabolic Syndrome and Mental Illness Dr. Natasha Afzal
Feb. 21, 2014 Violence Triage Dr. Kelly Watt
Mar. 21, 2014 Addiction Medicine 101 Dr. Nader Sharifi
Surrey Memorial Hospital – Grand Grounds Date Topic Presenter
Oct. 4, 2013 Marijuana Morning Sickness Dr. Nader Sharifi
Oct. 18, 2013 How to Manage DDMHS patient in ER Dr. R. Friedlander
Nov. 22, 2013 Use of Long Acting Injectibles in Psychiatry Dr. R. Williams
Jan. 17, 2014 "I always just assumed it was somehow my fault": Introducing a New Specialist Provincial Psychiatric Genetic Counselling Service
Dr. Angela Inglis
Feb. 21, 2014 "Should We Be Anxious About DSM-5 Changes in Anxiety Disorder Criteria?"
Dr Kevin Kjernisted
Mar. 21, 2014 “Jill’s Story: A Case Study on Mood Across the Female Reproductive Life Cycle”
Dr. Shaila Misri

Department Summaries Clinical Audit Annual Report
Page 180 of 210
Surrey Memorial Hospital - Department of Psychiatry – Journal Club Date Topic Presenter
Sept. 6, 2013 Nabilone Decreases Marijuana Withdrawal and a Laboratory Measure of Marijuana Relapse
Dr. L. Patterson
Nov. 1, 2013 Managing Challenging Behaviour in Alzheimer’s Dementia
Dr. Vincent Choong
Dec. 6, 2013 Childhood Trauma & Psychosis Selective Mutism
Dr. D. Yew Dr. K. Dhaliwal
Feb. 7, 2014 Effects of Cannabis Use on Outcomes of Psychotic Disorders: Systematic Review
Dr. I. Hussain
Mar. 7, 2014 A 16-year prospective study of prodromal features prior to BPI onset in well Amish children
Dr. S. Chow
Apr. 4, 2014 Cognitive therapy for people with schizophrenia spectrum disorders not taking antipsychotic drugs: a single-blind randomized controlled trial
Dr. M. Casagrande
Surrey Memorial Hospital – Psychiatry Resident Education – Pharmacology Rounds
Aug. 9, 2013 Introduction to psycho Pharmacology – From Circuits to Symptoms via Synapses
Dr. M. Selvaraj
Sept. 13, 2013 Antidepressants Dr. M. Selvaraj
Oct. 11, 2013 Antipsychosis Dr. M. Selvaraj
Nov. 8, 2013 Mood Stabilizers Dr. M. Selvaraj
Jan. 10, 2014 Psychiatric Drug–Drug Interactions – A Refresher! Sue Corrigan
Feb. 14, 2014 Insomnia and Sedative Hypnotics Sue Corrigan
Mar. 14, 2014 Food – Cause or Cure for Mental Illness Dr. M. Selvaraj
Accreditation October 29-30, 2013 an external review of the Fraser Psychiatry Residency Stream was conducted by Dr. Paul Dagg. Report and recommendations reviewed.

Department Summaries Clinical Audit Annual Report
Page 181 of 210
Obstetrics & Gynecology Regional Department Head: Dr. Peter Beresford Medical Quality Committee Activities
Currently, medical quality improvement activities are reported to the Maternal Infant Child and Youth (MICY) Program Quality and Performance Committee and conducted through the activities of the Perinatal & Neonatal Quality Review Committee and Local Multi-disciplinary Review Committees (LMRC). Over the past year, attention has been focused to determining a quality committee structure for the Department of Obstetrics and Gynecology that will be effective and efficient, and build upon the culture of multi-disciplinary review and quality improvement. A Regional Department Medical Quality Committee (RDMQC) for the Department has recently been established. Terms of Reference for the RDMQC were presented at the September 11, 2013 HAMAC meeting, for approval. In addition to implementing a program of professional practice evaluation and structured quality improvement for the Department, the RDMQC will regularly receive and review reports from the Perinatal & Neonatal Quality Review Committee and Local Multi-disciplinary Review Committees.
MICY Quality Performance Committee (QPC) Meeting dates: October 9, 2012, November 13, 2012, January 8, 2013, February 17, 2013, April 30, 2013, May 14, 2013, June 11, 2013
Perinatal & Neonatal Quality Review Committee Meeting dates: October 24, 2012, November 28, 2012 , January 23, 2013, February 27, 2013, March 27, 2013, April 24, 2013, May 22, 2013, June 25, 2013
Local Multi-disciplinary Review Committee Meeting recurrence varies at each site. LMRC reports received and approved for this time period include:
Royal Columbian Hospital - 5 reports Surrey Memorial Hospital - 1 report Abbotsford Regional Hospital - 1 report Langley Memorial Hospital - 2 reports Burnaby Hospital Neonatal Intensive Care Unit - 2 reports Ridge Meadows Hospital - 4 reports

Department Summaries Clinical Audit Annual Report
Page 182 of 210
Morbidity & Mortality Review
During the period of October 1, 2012 to June 30, 2013 morbidity and mortality review rounds were conducted by the Local Multi-disciplinary Review Committees for the purposes of evaluating and improving the quality of patient care provided. 50 patient cases were selected for review using the Perinatal Trigger Tool; as identified by PSLS events; or based upon specific criteria that may include i) Stillbirth or intrauterine death, ii) neonatal pH < 7.0 or base excess > -12, iii) Apgars of <4 at 1 min & <6 at 5 min, iv) significant maternal morbidity. 77 recommendations for improvement arose from the cases reviewed.
Medical Management Review
Since October 1, 2012, there have been 11 reviews that were conducted for the purposes of evaluating and improving the quality of care provided.
Patient Safety Reviews: 8 Commissioned Patient Safety Reviews occurred 63 recommendations for improvement arouse from the PSR cases reviewed
External Medical Reviews: 2 patient cases were externally reviewed, of which 1 case review is still in process 5 recommendations for improvement have been received
Patient Care Quality Office Review Board: 1 case was reviewed 2 recommendations for improvement have been received
Evidence Based Practice/Medical Management Tools
Members of the Department have been involved in the development, review and/or implementation of the following clinical practice guidelines and pre-printed order sets: Regional nausea and vomiting of pregnancy PPO Epidural protocol and PPO Preterm labour protocol and PPO Algorithm for Perinatal patients presenting in Emergency Department Diversion policy Term newborn PPO Late preterm and SGA PPO

Department Summaries Clinical Audit Annual Report
Page 183 of 210
2 Postpartum PPOs – vaginal birth, post-op C/S PPROM protocol NST and ultrasound surveillance guideline Antepartum admission PPO Induction of labour policy 3 Hypertension PPOs – antepartum, postpartum, and antihypertensive treatment of
severe hypertension in pregnancy 2 Diabetes PPOs – antepartum/intrapartum and postpartum
Quality Improvement Initiatives
Leadership Safety Walkabouts (LSW) took place at all sites and units within the MICY Program during Canadian Patient Safety Week, from October 29, to November 2, 2012. The MICY Program Senior Leaders appreciated the opportunity to meet with front line staff and physicians to engage in discussions related to patient safety. Unit specific feedback reports were sent to each unit manager and Head of Department (local) for their prospective areas and action plans were developed around items identified. LSW summary reports for Perinatal, NICU and Pediatrics were reviewed at the January and February 2013, MICY QPC meetings. The 3 top regional themes identified as program priorities were: Perinatal
Regional action regarding timely, straightforward transfer process, and clarity on Levels of Service (LOS) for all sites: BC Bedline & BC Women’s and Children’s Hospital processes for transfer to Higher Levels of Care are complex and time-consuming, and BC Women’s and Children’s Hospital may expect Fraser Health community sites to care for inappropriate patients.
Staffing mix and staffing levels: some sites have significantly different resources and staff/patient ratios than others. No after hours unit clerk support is having a significant impact on busy Labour & Delivery units where all admission processes must be completed by nurses. PP only nurses and novice nurses on the units are making it difficult to manage emergencies and very busy shifts. Unfunded nursery spaces are causing staff shortages on maternity units.
Delays to care: Delays to OR/anesthesia/ analgesia for maternity patients, delays to assessment and intervention as obstetrics and pediatrics medical staff are not in-house or not adequate at busy sites.

Department Summaries Clinical Audit Annual Report
Page 184 of 210
Pediatrics & Neonatal Intensive Care Unit (NICU)
Communication and transitions in care: (Pediatrics & NICU) Incomplete or erroneous information at transfer, inconsistent staff consultation regarding new equipment and processes, inconsistent approval of overtime.
Environment, equipment, & cleaning: (Pediatrics & NICU) Availability, appropriateness, and functioning of equipment, and timely repair or replacement of equipment is problematic in many areas. Discussion regarding cumbersome process in new lower mainland service model. Crowded physical space, insufficient isolation space, and clutter and equipment wires are a problem in many units. Cleaning is a concern as cleaners are often rushed and not cleaning all surfaces.
Lab interface with NICU and Pediatrics: Injuries to neonates during blood draws, incorrect reports, side rails and isolettes not always secured, clotted samples, delays in Lab response or reporting in urgent / emergent situations.
Performance Review/Clinical Performance Appraisal
4 physicians have undergone a performance review. 4 physicians have had modifications to their scope of practice. 1 physician has had their obstetrical privileges suspended
Supporting Professional Development
Medical staff participate in the MoreOB program.

Department Summaries Clinical Audit Annual Report
Page 185 of 210
Pediatrics Regional Department Head: Dr. Mark Sorial Medical Quality Committee Activities
The Regional Department of Pediatrics is in the process of establishing a Regional Department Medical Quality Committee. Currently medical quality improvement activities are reported to the MICY Program Quality and Performance Committee and undertaken by the Child & Youth Quality Committee, and site-based committees. A goal for the coming year will be to determine a committee structure for the department that will be effective and efficient.
Medical Management Review
A Patient Safety Review was undertaken in the past year. Recommendations arising from this review include: Early consultation/referral to pediatrics for complicated surgical cases Better hand-over Better documentation of clinical progress More education in certain clinical domains
Evidence Based Practice/Medical Management Tools
Members of the Department have been involved in the development, review and/or implementation of the following clinical practice guidelines and pre-printed order sets:
Diabetic Ketoacidosis (DKA) Conscious sedation Pre-printed orders for Neonates Asthma and Diabetes clinics - standardization of care Participating in Child Health BC initiatives to improve quality and safety and to develop a
Tiers of Service document which will help ensure proper and safe care at the appropriate site.
Quality Improvement Initiatives
Tiers of service, ensuring that hospitals are delivering the appropriate level of care based on what they can and cannot do
Working with BC Children’s Hospital on subspecialty clinics and co-branding Plans are underway for an observation unit at Chilliwack General Hospital modeled on
the successful Ridge Meadows Hospital unit Improving access to Mental Health services

Department Summaries Clinical Audit Annual Report
Page 186 of 210
Surgery Regional Department Head: Dr. Jean Lauzon Regional Department Medical Quality Committee Activities The Department of Surgery has established a Regional Department Medical Quality Committee. Within Fraser Health there are several surgical committees that meet. Most of these committees are site based, and at the larger institutions, these committees are also based upon sub-specialties (divisions). Meeting Dates: September 26, 2013, October 17, 2013, November 21, 2013, February 20,
2014
Division Meeting Activities Several divisions within the Department of Surgery hold meetings at which quality
improvement is an item for discussion. General Surgery: January 31, 2013, September 26, 2013, December 3, 2013 Neurosurgery: February 21, 2013, January 16, 2014, February 6, 2014 Ophthalmology: March 11, 2013, June 10, 2013, September 9, 2013, December 9, 2013,
March 10, 2014 Oral & Maxillofacial Surgery: April 2, 2013 Plastic Surgery: Journal Club: January 16, 2013. Division: January 17, 2013, May 28, 2013,
September 24, 2013, October 29, 2013, January 28, 2014 Urology: September 10, 2013, February 25, 2014 Vascular Surgery: May 7, 2013, October 1, 2013, January 29, 2014
Local Site Medical Quality Committee Activities Listed below are those site medical quality committees for which meeting dates are known:
Burnaby Hospital: May 15, 2013 Delta Hospital: January 28, 2013, March 11, 2013, June 19, 2013, September 9, 2013,
October 16, 2013, November 20, 2013, January 27, 2014 Eagle Ridge Hospital: April 3, 2013; May 15, 2013; June 5, 2013; September 11, 2013,
November 13, 2013, January 15, 2014, February 12, 2014 Langley Memorial Hospital: April 4, 2013, 4th Thursday of every month, excluding December Ridge Meadows Hospital: January 30, 2013 Royal Columbian Hospital/Eagle Ridge Hospital – Orthopedic Surgery: February 7, 2013,
May 30, 2013

Department Summaries Clinical Audit Annual Report
Page 187 of 210
Regional Department of Surgery Initiatives Clinical Audits
1. Title: Surgical Safety Checklist Audit
Sites: All surgical sites within Fraser Health Phase:
Planning Designing Data Collection Analysis Reporting Background: The FHA Surgical Safety Checklist is based on the WHO checklist. All FH operating rooms have the Checklist mounted on the wall. Surgeons and operating room personnel are expected to conduct all 3 phases for each operation:
• Pre-induction, • Pre-incision, and • Debriefing.
Combined with the surgical pause and site marking, the checklist has been shown to reduce medical errors and improve engagement and morale of the nursing staff. Over the past 2 years FH has been auditing the use of the checklist. Improvement to the auditing procedure and tool were implemented in July 2013 and will be used for future audits. This revised audit tool collects information regarding the team performance of the Surgical Safety Checklist within the surgical suites of Fraser Health.
Objective: To assess the use of the Surgical Safety Checklist, teamwork, and to identify areas to further improve checklist implementation and improve surgical safety. Time period: Data collection using the revised audit tool will commence in the fall 2013. Once implemented, this will be an ongoing, routine audit. Data collection strategy:
20 audits per month, per surgical site, will be completed.
The auditor will ideally be a person who is not part of the OR team. This will provide less biased reporting and the opportunity for coaching and feedback to the team.
Copies of the audit will be sent to FH administrative assistant for stats collection and reporting. Copies will also be kept on site for review with the Surgical Manager, Chiefs of Surgery and Anesthesia as well as surgical teams.
Department Summaries Clinical Audit Annual Report
Page 188 of 210
Morbidity & Mortality Review
At its meeting of March 26, 2013, morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Learning points and recommendations for improvement arising from the cases reviewed follows:
a. If an anesthetic block is to be performed at a site distant to the proposed incision, the site of the block is to be initialed by the anesthesiologist during the Briefing.
b. If a regional anesthetic is to be performed prior to the Briefing (outside the operating room) then the relevant components of the Briefing must be completed prior to the procedure by those present.
c. The Briefing portion of the Surgical Safety Checklist will be done before any anesthetic procedures are performed in the operating room.
Quality Improvement Initiatives
National Surgical Quality Improvement Program (NSQIP): Fraser Health’s 11 surgical sites participate in the American College of Surgeons National Surgical Quality Improvement Program (NSQIP). NSQIP is a data-driven, risk adjusted, outcomes based surgical quality improvement program that allows participating sites to view their performance in comparison to other North American hospitals. Fraser Health participating sites provide NSQIP with specific patient clinical information, and NSQIP provides results to sites on mortality, morbidity and complication rates from which quality can be monitored and improvement opportunities identified and implemented. Each surgical site has a physician champion that is supported by a surgical case reviewer (SCR). Working together, the physician champion and SCR provide data and reports to the local surgical group to facilitate discussions about quality and to identify improvement initiatives. At many of the sites, the physician champion will also have confidential discussions with individual surgeons on their performance in comparison to peers using the NSQIP data.
The latest semi-annual report (SAR) shows that we still “need improvement with surgical site infections (SSI)’s, UTI’s and Post-op Pneumonia. However, some sites/divisions are achieving exemplary status on several parameters, including the 3 mentioned above.
We have arranged a meeting with the Surgical Champions from each site on Mar 13, 2014, to determine why we have not been able to improve these results, and what needs to be done to change this.

Department Summaries Clinical Audit Annual Report
Page 189 of 210
Evidence Based Practice/Medical Management Tools A significant new initiative that is being implemented region wide is the Enhanced Recovery After Surgery (ERAS) protocols. These protocols have been shown to significantly decrease length of stay as well as morbidity & mortality rates. The ERAS protocols will be Division specific and standardized region wide.
The development of Division Specific PPO’s is well under way. The pre-admission components of ERAS will be addressed through the Pre-admission clinic. The intra-operative components will be addressed by the Department of Anesthesia. We are developing teams at each site that will help implement/sustain the ERAS protocol. An auditing tool is required to confirm all the steps in the ERAS protocol are being followed. This is currently being discussed at the Provincial level.
Department Summaries Clinical Audit Annual Report
Page 190 of 210
Division of General Surgery
Clinical Audits
1. Title: Breast cancer surgery
Site: All FHA sites
Planning Designing Data Collection Analysis Reporting
Background: Breast cancer is the most common malignancy in women, and is managed by multi-disciplinary teams. Many organizations have developed quality indicators for breast cancer care. Breast cancer surgery is performed by most general surgeons at all sites in the Fraser Health Authority. A working group from the Division of General Surgery was established to review the quality of breast cancer surgical care at all sites across the region.
Objectives:
For patients with a diagnosis of breast cancer, assessing the quality of surgical care provided through the measurement of selected indicators of breast cancer surgical quality.
Measure 1: The % of patients undergoing breast cancer surgery who obtained the diagnosis of breast cancer pre-operatively by a core biopsy.
Measure 2: The % of patient with a diagnosis of invasive breast cancer that underwent a Sentinel Lymph Node procedure.
Measure 3: The % of surgical specimens that have the orientation marked.
Patient Selection: For each general surgeon, 10 patient cases that met the following inclusion criteria were randomly selected. Patient cases were identified by James Gurling, Business Analytics Leader, Surgery Information Systems. Inclusion criteria: Females over 30 years old at the date of surgery with a diagnosis code of “30YMCC” (Breast Cancer – Regular) and ORM primary procedure code one of:
BREAST BIOPSY/LUMPECTOMY BREAST BIOPSY/LUMPECTOMY - FINE WIRE BREAST BIOPSY/LUMPECTOMY W AXILLARY DISSECTION MASTECTOMY - MODIFIED RADICAL MASTECTOMY - PARTIAL MASTECTOMY PARTIAL-AXILLARY DISSECTION MASTECTOMY SIMPLE MASTECTOMY SIMPLE-AXILLARY DISSECTION
Department Summaries Clinical Audit Annual Report
Page 191 of 210
MASTECTOMY SUBCUTANEOUS MASTECTOMY TOTAL MASTECTOMY TOTAL - BILATERAL SENTINEL NODE BIOPSY
Time period: The clinical audit included surgical procedures performed between April 1, 2012 and March 31, 2013. The clinical audit was conducted by Sharmen Lee during the month of November 2013.
Data collection strategy: This was a retrospective audit of general surgeons practices’ in performing breast cancer surgery between April 1, 2012 and March 31, 2013. Data was collected by Sharmen Lee through the review of diagnostic pathology reports, medical imaging reports and operative reports. 10 cases were randomly selected, per surgeon, for inclusion in the audit by Surgery Information Systems. For surgeons performing fewer than 10 cases, all cases were included in the audit. Methodology for random selection of 10 cases per surgeon: 1. Obtain relevant data for all candidate cases meeting inclusion criteria 2. For each record, assign a random number using the RAND() function in Excel 3. For each surgeon, select the 10 records with smallest random numbers for inclusion.
For each measure, data was recorded as follows:
Pre-operative diagnosis: Core biopsy, or excisional fine wire guided biopsy, or fine needle aspirate. Lymph node: Sentinel lymph node biopsy, or axillary lymph node dissection, or no lymph node procedure Specimen orientation: yes or no Patient identifying information was not collected as part of the quality indicator data set.

Department Summaries Clinical Audit Annual Report
Page 192 of 210
Quality Improvement Initiatives
Development of Regional Clinical Plan for General Surgery Development of new PPOs based on ERAS for RCH Regional planning for PPOs and adoption of ERAS Colonoscopy audits planned at all sites.
Division of Ophthalmology
The Division has been engaged in discussions related to identifying, selecting and implementing medical quality improvement activities. The Division has decided to focus on two quality activities for the coming year: Morbidity and Mortality review Surgical Safety Checklist – Ambulatory Cataract Surgery
Morbidity & Mortality Review
The Division will be focusing their efforts in establishing regional Morbidity & Mortality (M & M) review rounds under the leadership of Dr. H. Dhaliwal. M & M review for Ophthalmology will be conducted on a regional basis under the jurisdiction of the Regional Division of Ophthalmology. Over the next several months, work will focus on establishing: case selection criteria the process for identification of cases that meet the selection criteria the processes for case review: case preparation, case presentation, frequency of
meetings, roles of individuals involved, etc.
Quality Improvement Initiatives
Surgical Safety Checklist – Ambulatory Cataract Surgery
VIHA has adapted the WHO Surgical Safety Checklist for use in Ambulatory Cataract Surgery. Over the coming year the Division will review and discuss whether the implementation of this checklist within Fraser Health is something they would recommend. If the recommendation by the Division is forthcoming, discussions with the Surgical Program will follow to determine the feasibility of its implementation within Fraser Health.

Department Summaries Clinical Audit Annual Report
Page 193 of 210
Division of Neurosurgery
Morbidity & Mortality Review
At its meeting of January 16, 2014, morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided.
3 cases involving aspects of complex brain tumor management were discussed including cases involving a deep insular glioma, skull base tumor and posterior fossa tumor. Additional related cases were discussed.
Morbidity and complication avoidance were discussed as well as strategies for complication avoidance.
Learning points and recommendations:
Exploration of more advanced image guidance, specifically fluorescence guided tumor resection should be trialed for implementation as a means to provide more accurate intraoperative tumor identification with goals of more complete tumor resection, improved surgical and avoidance of complication. This may represent a relatively cost effective means of achieving these improvements.
Complex brain tumor surgery that fits within the scope and capability of FHA neurosurgery should be conducted under optimal conditions. This would include:
o Ideally, scheduled/planned operating time during the regular slate o Peri-operative/intra-operative management may be most optimally
conducted under the care of a core nucleus of anesthetists with interest/experience in the perioperative management of complex neurosurgical cases including complex brain tumor surgery.
Division of Vascular Surgery Clinical Audit
1. Title: Effectiveness of Complex Endovascular Aneurysm Repair (EVAR) review policy
Sites: All surgical sites within Fraser Health Phase:
Planning Designing Data Collection Analysis Reporting
Background: Complex EVAR is an expensive aspect of the care of high risk patients. Objectives: Length of stay, Mortality, myocardial infarction (MI) rate and renal function

Department Summaries Clinical Audit Annual Report
Page 194 of 210
Patient Selection: Reviewed retrospectively all patients who had been approved for complex EVAR during the first 6 month 2013 Time period: 8 months Data collection strategy: Retrospective Results: N=8 2/8 underwent surgery this year to date 6/8 have not progressed to surgery
Patient Age LOS MI Renal failure Mortality 1 67 12 Yes Yes No 2 74 7 Yes No No
Comment: Only 25% of patients approved for complex EVAR have actually had their procedure. Electronic chart review indicates that the risk work up and assessment is lengthy placing these patients at potential risk of rupture prior to surgery.
Actions:
Need to revise the flow pathway to expedite care.
Need to monitor outcomes on prospective basis. Patients to be entered into VQI data basis on intention to treat basis so that we can compare the outcomes against any consequence of delay in care.
Physician participation rate: Patients selection is by all members of the division of vascular surgery.
2. Title: Effectiveness of Vollmar ring endarterectomy as an alternative to arterial bypass.
Sites: All surgical sites within Fraser Health Phase:
Planning Designing Data Collection Analysis Reporting
Background: Vollmar ring endarterectomy offers an alternative to conventional by pass where stenting is inappropriate. Potential advantages are avoidance of prosthetic material, preservation of normal anatomy, and shorter hospital stay. This is a new technique that is not widely performed hence the importance of documenting results.

Department Summaries Clinical Audit Annual Report
Page 195 of 210
Patient Selection: Prospective data collection of all patients undergoing a Vollmar Ring endarterectomy Data collection strategy: prospective Results: N =12 6 iliac and 6 SFA. Excluded are 4 patients converted to bypass for technical reasons. Iliac = 6
Patient LOS MI Mortality Infection Primary Patency
1 21 N N N Y 2 2 N N N Y 3 3 N N N Y 4 5 N N N Y 5 2 N N N Y 6 3 N N N Y
SFA = 6
Patient LOS MI Mortality Infection Primary Patency
1 6 N N N Y 2 1 N N N Y 3 3 N N N Y 4 3 N N N Y 5 4 N N N Y 6 1 N N N Y
Comment: Vollmar ring endarterectomy is an alternative to bypass in selected patients and hence these results must be compared to Aortofemoral and fem-pop bypass surgery. In the first group of iliac reconstructions, the patient presented with a septic fem-fem x-over graft. As this was the first case a laparotomy was performed as a precaution for possible rupture during the procedure as the entire right iliac require endarterectomy. The prolong stay reflects the cautious approach to this first patient. If this LOS is excluded, all subsequent iliac reconstruction were done with an Average LOS of 3 days. For SFA reconstruction Average LOS = 3 days. The initial results are encouraging with shorter LOS. No mortality or MI and 100% primary patency. Where Vollmar ring proved technically impossible in 4 cases, conversion to conventional bypass was made. Actions:
Continue to monitor results as use becomes more wide spread.

Department Summaries Clinical Audit Annual Report
Page 196 of 210
Physician participation rate: Results reflect a single surgeon’s outcome of a new procedure. Other members of the Division are waiting training.
3. Title: Can a cardiac risk predictive index be used to determine need for High Acuity
Monitoring in Vascular surgery.
Background: The last NSQIP report documented a higher than expected Myocardial infarct rate post surgery in vascular patients at RCH. This was not evident at ARH. Access to a monitored bed in Higher Acuity is more readily available at ARH ,. This study looks at the possible influence on cardiac outcome if aortic patients are routinely monitored in a High Acuity unit post surgery.
The VSG-CRI is a predictive score for specific vascular surgical operations. See attached Article “ The vascular Study Group of New England Cardiac Risk index ( VSG-CRI) predicts cardiac complications more accurately than the Revised Cardiac Risk Index in vascular Surgery Patients” JVS Vol 52, # 3. Cardiac complication is defined as a myocardial infarct, new atrial fibrillation or Congestive Heart Failure. For Open AAA repair VSG-CRI looks at:-age; Prior CABG or stent; CCF; COPD; Renal function; use of B blockers and prior vascular surgery. For EVAR repair VSG-CRI looks at :- CCF; Cardiac Stress test; Use of Plavix and AAA size. Patient selection: This retrospective study is confined to patients with Abdominal Aortic Aneurysms as the Division has in place stringent selection criteria so that patient selection should be similar at the 2 sites.. The study compares VSG-CRI cardiac risk predictive scores and cardiac event in 2 cohorts of sequential patients who were all monitored post operative in a High Acuity unit and had routine troponin, ECG and chest x-rays as part of their post op protocol. A third Cohort of patients turned down for AAA repair is presented for documentation of level of risk of patients refused surgery.
The decision for open vs EVAR surgery was mainly an anatomical one based upon the CT. Patients were managed according to the EVAR 2 trial and were refused open or EVAR surgery if life expectancy was estimated to be less than 2 years.
Data collection Strategy: Retrospective

Department Summaries Clinical Audit Annual Report
Page 197 of 210
Results: Open AAA Patient VSG-CRI EVENT LOS 1 15.1 % Y 22 2 13.8 % N 7 3 8.5 % N 7 4 47.8 % N 8 5 35.4 % Y 8 6 8.5 % N 6 7 13.8 % Y 8 8 30.8 % N 7 9 21.9 % Y 6 10 17.0 % N 7 Average 21.3 % 4/10 8.6
EVAR 11 2.5 % N 1 12 24.0 % N 2 13 1.2 % N 3 14 1.2 % N 1 15 24.0 % N 1 16 24.0 % N 2 17 2.5 % N 2 18 6.8 % N 4 19 3.4 % N 1 20 4.6% N 7 Average 9.42 % 0/10 2.4 days Cancelled due to clinical risk assessment Patient VSG-CRI open VSG-CRI EVAR 21 46 % 26.5% 22 55.2 % 61 % 23 15.2 % 3.1 % ( patient refused) 24 46 % 9.1 % 25 40 % 24 % 26 23.7 % 10% 27 17.8 % 2.5% 28 38.9 % 6.8 % 29 35.4 % 26.5 % 30 46.3 % 3.9% Average 36.5 17.3 During this time period an additional 5 patients were refused surgery due to the finding of a malignancy, 1 for dementia and 2 ruptured while waiting and were hence excluded from analysis

Department Summaries Clinical Audit Annual Report
Page 198 of 210
Comment:
Allocation to open or EVAR was based upon anatomic characteristics and not by not risk clinical assessment. Patients assessed as having high risk were excluded from both forms of surgery. The assumption therefore is that open and EVAR groups have similar risk profiles.
VSG-CRI predicts a higher risk for open vs EVAR ( 21.3% vs 9.42 %)
In keeping with the prediction of VSG-CRI open surgery carried a higher risk of a cardiac event (40 % vs 0%) Please note that only 1 of 4 events was a MI. It is thought that timely intervention in the other 3 events may have prevented a MI occurring.
Open surgery had higher LOS ( 8.6 vs 2.4 days)
In this small study; a VSG-CRI less than 10% was associated with 0% post operative cardiac events while the 8 open surgical patients with a score higher than 10 had 4 (50%) significant cardiac events.
Based upon VSG-CRI there were patients turned down for repair who may have had a lower risk than clinically predicted.
Conclusion and Recommendations:
VSG-CRI be part of pre-operative assessment for vascular patients. Risk predictions are available for Open AA, EVAR, Carotid endarterectomy and leg bypass.
Patients having open AAA surgery with a VSG-CRI greater than 10% should be routinely monitored in High Acuity with a post operative protocol to include troponin measurements, ECG and CXR. This group of patients have a 50% rate of a significant cardiac event occurring post operatively. Early timely intervention may be important in preventing MI occurring in patients with atrial fibrillation or fluid overload causing CCF.
The majority of EVAR patients can be safely managed outside of a High Acuity Unit.
Due to the shorter LOS ( 2.4 vs 8.6 days) and lower cardiac risk ( 0 vs 40%), where anatomically suitable EVAR is preferred to open AAA repair.
Morbidity & Mortality Review
At its meeting of May 7, 2013, morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Learning points and recommendations for improvement arising from the cases reviewed are as follows: Perclose devices are to be used with caution in complex cases Care should be done to ensure that the puncture is infra inguinal and that the artery is
not calcified. In the decision to use a Perclose device consideration needs to be given to planning
rescue intervention should the device fail. If a total common iliac occlusion is to have angioplasty following use of a subintimal
dissection techniques, suitable cover stents must be available in the OR to deal with any rupture.

Department Summaries Clinical Audit Annual Report
Page 199 of 210
Dr Toppin at RCH and Dr Lewis at ARH review site M&M. All unexpected death or major iatrogenic complications are referred to Dr. Lewis for chart review and action. Any discussion occurs at monthly division meetings.
Evidence Based Practice/Medical Management Tools The division has implanted standardized selection
criteria for EVAR repair
Complex EVAR
TEVAR All Complex EVAR and TEVAR are subject to Divisional review Standardized post op EVAR orders available.
Quality Improvement Initiatives
There are 4 main Quality issues that the division has been trying to get implemented. VQI database The Division lacks the ability to analyze outcomes and hence justify or reject changes in the direction of care. Vascular surgery has changed from a relatively low tech field to a very technology dependent expensive specialty. Some of the advances are valid, others are not. We cannot establish performance goals or compare ourselves to benchmarks without a valid data base. NSQIP is not such a base. The international standard is VQI which is the most widely used data base in the world. It allows for real time prospective data collection of all vascular patients and comparison to peer hospitals. The Division has championed this as a way for the FHA to gain accurate data and control of all aspects of vascular surgery to enhance patient care and evaluate resource allocation. The system has been approved. Funding is lacking.. Vascular Lab for functional studies of arterial flow. This is essential in predicting limb loss, and assessing need for intervention. Diabetic foot clinic. The FHA has a high amputation rate in diabetics due to a systemic lack of preventative care. Nurse Assistant on the vascular wards to facilitate flow pathways. All 4 of these programs have been applied for. VQI and the Vascular Lab are approved but await funding. The requests for a diabetic foot clinic and Nurse assistants are still being considered by the FHA.
Department Summaries Clinical Audit Annual Report
Page 200 of 210
Supporting Professional Development
The division discusses complex cases at regularly scheduled monthly meeting except for during summer.
Division of Plastic Surgery
Chart Review
A chart review was completed in the late spring of 2013. All cases where alloderm was used in breast reconstruction were reviewed. The indications and outcomes of surgery were reviewed. The rates of infection, reoperation and loss of implant were specifically addressed. UTI, Mortality, Pneumonia, Thrombolembolism were not present and not the focus of the review. Best practice, information sharing and intradisciplinary exchange will help to minimize morbidity in this patient population. The chart review was coordinated with the UBC breast reconstruction surgeon in an effort to share and learn as much as possible
Local Quality Committees Royal Columbian Hospital and Eagle Ridge Hospital
Clinical Audit
Title: Review of surgical site infections as identified by NSQIP Division: Department of Orthopaedics Site: Royal Columbian Hospital and Eagle Ridge Hospital Phase:
Planning Designing Data Collection Analysis Reporting Background: As a department, we are trying to use the NSQIP data to help improve our quality of care. Seventeen patients were identified to have surgical site infections and these patients were reviewed. A chart review was performed and various perioperative factors were identified that may have predisposed to the surgical site infections.

Department Summaries Clinical Audit Annual Report
Page 201 of 210
Patient Selection: The patients were identified by the NSQIP clinical reviewers as having surgical site infections according to the NSQIP definition. Time period: The patients identified were in the date range from September 2011 to December 2012. Data collection strategy: A chart review was performed on the identified patients. The factors looked at were as follows:
1. Operative procedure 2. BMI 3. Date of birth 4. Sex 5. Whether the patient was a study patient 6. Whether the patient was transferred to the treating facility 7. Wait time for surgery 8. Days postoperatively until surgical site infection diagnosed 9. Surgical priority status 10. Surgeon 11. Length of surgical procedure 12. Use of intraoperative fluoroscopy 13. Prep solution 14. Splint application 15. Dressing used 16. Drain 17. Fracture type 18. Preoperative antibiotics 19. Timing of preoperative antibiotics and intra-operative re-dosing 20. Tourniquet use 21. Postoperative antibiotics 22. Patient temperature intra-operatively as well as in the PACU 23. Use of body warmer 24. Patient glucose 25. Length of hospital stay 26. Assessment of infection depth
Results: Although many of these patients had surgical site infections, some patients had been referred for an osteomyelitis. Therefore, this would not have been a true postoperative surgical site infection as it was a preexisting condition. There appears to be some inaccuracies with the NSQIP data which need to be further investigated. As well, the participating surgeons indicated that they knew of other patients with infections that had not been identified by NSQIP so it was unclear if this review was complete or just a sample of the cases.

Department Summaries Clinical Audit Annual Report
Page 202 of 210
Therefore, several issues have been identified with the NSQIP data. Firstly, it is unclear how the surgical site infection diagnoses are being made when the data is being collected. Although there are NSQIP criteria, the data does not appear to always accurately identify the patients with true surgical site infections. Follow-up Action: Dr. Lemke will meet with the NSQIP staff to obtain more information on how the data is collected and reported. It also came to the attention of the involved surgeons that many of the GP’s and ER physicians start patients on antibiotics without obtaining cultures. Some of these patients have redness due to reaction to the sutures or staples. Occasionally these patients have stitch abscesses that cause sterile drainage. These are not true surgical site infections. Therefore, emergency physicians and family physicians should be more cautious in terms of starting antibiotics prior to notifying the treating surgeon as once the antibiotics have been started and the patient is seen several days later it is very difficult to determine whether a true surgical site infection was present. Follow-up Action: Dr. Perey will communicate with the Head of Emergency and the Hospitalists to highlight this issue for them. As well, we had received some feedback that antibiotic timing preoperatively was not always within one hour of the surgical procedure and that post-op hypothermia may be a contributing factor to infection. On review of our data, most (14/17) patients received their antibiotic less than 60 minutes prior to starting their surgery, which is in keeping with the AAOS guidelines. We were unable to comment on the significance of patient temperature and its correlation with surgical site infections due to insufficient pre and intra-op data. Our review showed that most (15/17) patients’ temperatures in the PACU were within the normal range. The sample size was too small to make any definitive conclusions on these two factors. Our final conclusion is that NSQIP data is important and the goal of achieving improved quality assurance should be pursued. Within our healthcare system, ways of optimizing data collection would help to more accurately report these problems and may help to decrease patent morbidity with respect to surgical site infections.
Morbidity & Mortality Review
Orthopedic Surgery morbidity and mortality review rounds were conducted on October 25, 2012 and February 7, 2013 for the purposes of evaluating and improving the quality of patient care provided. Themes for the M & M rounds included hip fracture collapse after gamma nail fixation, and subdural hemorrhage. 3 patient cases were selected for review and discussion.

Department Summaries Clinical Audit Annual Report
Page 203 of 210
Ridge Meadows Hospital
Morbidity & Mortality Review
Morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Criteria for case review included: Project 800 – Wound Complications Field 1 – Dehiscence Field 2 – Evisceration Field 3 – Infection Project 820 – Surgical Complications, Other Field 1 – Anastomotic Leak Field 2 – Return OR 14 days Field 3 – Transfusion Intra/Postop >=4 Filed 4 – Transferred to Other Acute Institution Field 5 – Expired - within 14 days of surgery
- any admission with surgeons as MRP (no surgery) Field 6 – Perf/Bleed Post Endo Project 821 – Non-Surgical Complications Field 1 – DVT Field 2 – Acute MI Field 3 – Other Serious Comp Field 4 – Pneumonia Field 5 – PE Field 6 – Stroke Field 7 – TPN > 14 days Field 8 – DIC Field 9 – Intra-abdominal Abscess 26 patient cases were selected for review using the pre-established patient selection criteria. Of these 26 cases, 9 were identified for further review and discussion.

Department Summaries Clinical Audit Annual Report
Page 204 of 210
Chilliwack General Hospital
Morbidity & Mortality Review
Morbidity and mortality review rounds were conducted by the Chilliwack General Hospital Surgical Audit Committee for the purposes of evaluating and improving the quality of patient care provided. 1 patient case was reviewed. Learning points and recommendations for improvement arising from the cases reviewed follows:
1. Surgery for pheochromocytomas should be performed in tertiary care centres with experience in the condition and the necessary supports for the patient and condition.
2. Patient with significant disease or co-morbidities should be seen in the pre-operative assessment clinic well in advance of surgery to allow adequate pre-operative assessment and management.
Eagle Ridge Hospital
Morbidity & Mortality Review
During the period of March 2013 to September 2013 morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided.
Five patient cases were selected for review using the following process and criteria: - Return to operating room - Transfer to higher level care - Deaths in OR - Unexpected complications
Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Confirmation on Pediatric Policy with potential for overnight stay after OR and update staff on this policy
Done
2. Process of missing instrument piece and protocol for xray in the OR prior to patient leaving OR. Reminder to staff
Done

Department Summaries Clinical Audit Annual Report
Page 205 of 210
During the period of October 2013 – February 2014 morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Eight patient cases were selected for review using the following process and criteria: - Return to operating room - Transfer to higher level care - Deaths in OR - Unexpected complications Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Confirmation of policy regarding unexplained occurrence postoperatively in daycare (e.g. corneal abrasion). Education for recovery nurses
Done
Medical Management Review
During the period of October 2013 – February 2014, 2 medical management reviews was/were conducted for the purposes of evaluating and improving the medical quality of care provided. Learning points and recommendations for improvement arising from the case(s) reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Delayed discharge of daycare patients and importance of informing MRP. Review procedure/plans of communication with recovery nurses.
Done
2. Assessment of RN experience and mandate of MCU
Ongoing review
3. OSA policy and impact on patient beds FH Policy ongoing with implementation per hospital. ERH will be done later. Anesthesia to follow-up with Division regarding FH policy and current guidelines

Department Summaries Clinical Audit Annual Report
Page 206 of 210
Delta Hospital
Morbidity & Mortality Review During the period of September 2013 to February 2014 morbidity and mortality review rounds were conducted for the purposes of evaluating and improving the quality of patient care provided. Eight patient cases were selected for review by physician self-reporting and NSQIP identified cases. Learning points and recommendations for improvement arising from the cases reviewed, and the status of implementation are as follows:
Learning Point / Recommendation
Status of Implementation
1. Chlorhexidine preparation reduces risk of a surgical site infection.
Chlrohexidine wipes now being given to a wide range of patients preoperatively
2. Use of antibiotics preoperatively will reduce surgical site infections
Continuing to enforce need for preoperative antibiotics.
Langley Memorial Hospital
NSQIP Quality Improvement Activities UTI: Current overall NSQIP rate = 1.3% Current overall LMH rate = 2.3% Current LMH 2013 rate = 1.5% June (0%), July (0.6%), and August (0.6%) have shown sustainment of 2 or less UTI’s / month for 3 months now, and for 6 of 8 months this year. Our overall rate continues to decline (down another 0.1% since June 2013) and our yearly rate continues to decline also (down 0.2% since June 2013). Our 2011 rate was 3.3%, 2012 was 2.4% and so far in 2013 we are at 1.5%. Our UTI work and practice changes have been mostly sustained, with some review for staff of when to catheterize and when to do an in and out is needed to maintain our gains in this area. A document is being prepared and edited by our local Urologists to reflect these practices. This document will be used as an educational tool for ward nurses.
SSI: Current overall NSQIP rate = 1.7% Current overall LMH rate = 1.7% Current LMH 2013 rate = 1.6%

Department Summaries Clinical Audit Annual Report
Page 207 of 210
Reflecting on our work as a team, the antibiotic prophylaxis guidelines went in to place in June of 2013, the Chlorhexidine scrubs were started on the unit in June of 2013 with PDSA cycles ongoing in to July 2013 until the practice was solidified. Audits in August 2013 showed the practice of Chlorhexidine scrubs for non-elective inpatients was imbedded in the staff practice. Audits in July 2013 showed good compliance and timing with antibiotics, and some areas where consistency was lacking were addressed. We will need to see if we continue to have reduced numbers in the coming months to fully assess the impact of the changes we made starting in June 2013.
Normothermia assessment is ongoing and we will be undertaking inservicing on BAIR huggers for ward staff in order to allow for consistent pre-warming of all surgical patients. We will be auditing postop temperatures in PACU in the coming weeks. Physician participation rate: The QI activities chosen by the NSQIP team in consultation with the surgeons are specifically those germane to all surgeons and all surgical patients. The results and activities have been shared with the entire surgical department and surgeons and anesthesiologists are actively engaged and participating.
Case Reviews
Selected cases were reviewed for the purposes of evaluating and improving the quality of patient care provided. Learnings and recommendations included the following:
Issue: Potential for loss of limb
Staff Safety Ideas: Education of nurses to manage acute emergency of compression d/t cast. Better support from MRP
Issue: Anticoagulation
Staff Safety Ideas: The prescribers should be aware of the contraindications. Nurses should be educated and anesthiologists should be consulted before any new anticoagulants are started while the patient is on epidural.
Staff Safety Ideas: No pre-op heparin orders for C-section patients to be given by nursing staff. Could the gynecologist please ask anesthesia to give heparin when the anesthesia physician is comfortable with patient status?
Supporting Professional Development August 2013 - Sepsis Workshop # 5 for new staff/refresher for existing staff, Large number of ESNs orientating; New orientation program designed, Working on iERAS protocol with Surgical team, Elective Pre-Op Arthroplasty Teaching content updated

Department Summaries Clinical Audit Annual Report
Page 208 of 210
September 2013 - Roll out of NEW report sheet for end of shift communication, Continued/enhanced Infection control refreshers, End of Life in-services (Palliative care for acute care), Updated New Hire Orientation LPNs. NGs, RN with and without surgical experience, transition of RN rotation E8-D12 October 2013 - VernaCare inservice, Move towards NSQIP SSI actions, Refreshers on CVCs on unit.

Department Summaries Clinical Audit Annual Report
Page 209 of 210
i M. Catherine Sargent, MD. “Physician Burnout and Patient Safety”. American Association of Orthopedic Surgeons. AAOS Now December 2012 Issue http://www.aaos.org/news/aaosnow/dec12/research4.asp
ii Alan H. Rosenstein, MD. “Physician Stress and Burnout: Prevalence, Cause, and Effect.” American
Association of Orthopedic Surgeons. AAOS Now August 2012 Issue http://www.aaos.org/news/aaosnow/aug12/managing4.asp
iii
Burnout Self-Test: Maslach Burnout Inventory (MBI)