clinical application of pharmacogenomic testing in opioid ... · accepted standards of experimental...
TRANSCRIPT

Clinical Application of
Pharmacogenomic
Testing in Opioid Use
Disorder Management Earl Ettienne, LPD, MBA, RPh
Director of Graduate Programs and Industry Partnerships
Assistant Professor, Department of Clinical and
Administrative Sciences
Howard University College of Pharmacy
Adaku Ofoegbu, PharmD 2nd year PhD Student, Department of Clinical and Administrative Sciences
Howard University College of Pharmacy
1

Disclosure Statement Drs. Ettienne and Ofoegbu have no actual or
potential conflict of interest in relation to this
presentation
2

Planning Committee, Disclosures
AAAP aims to provide educational information that is balanced, independent, objective and free of bias
and based on evidence. In order to resolve any identified Conflicts of Interest, disclosure information from
all planners, faculty and anyone in the position to control content is provided during the planning process
to ensure resolution of any identified conflicts. This disclosure information is listed below:
The following developers and planning committee members have reported that they have no
commercial relationships relevant to the content of this webinar to disclose: AAAP CME/CPD
Committee Members Dean Krahn, MD, Kevin Sevarino, MD, PhD, Tim Fong, MD, Tom Kosten, MD, Joji
Suzuki, MD; and AAAP Staff Kathryn Cates-Wessel, Miriam Giles, and Justina Pereira.
All faculty have been advised that any recommendations involving clinical medicine must be based on evidence that is accepted within the profession of medicine as adequate justification for their indications and contraindications in the care
of patients. All scientific research referred to, reported, or used in the presentation must conform to the generally accepted standards of experimental design, data collection, and analysis. The content of this CME activity has been reviewed and the committee determined the presentation is balanced, independent, and free of any commercial bias. Speakers must inform the learners if their presentation will include discussion of unlabeled/investigational use of commercial products.
3

Target Audience
The overarching goal of PCSS-O is to offer
evidence-based trainings on the safe and
effective prescribing of opioid medications in
the treatment of pain and/or opioid addiction.
Our focus is to reach providers and/or
providers-in-training from diverse healthcare
professions including physicians, nurses,
dentists, physician assistants, pharmacists,
and program administrators.
4

Presentation Objectives
Review a basic history of the science behind
pharmacogenomics
Define pharmacogenomics and lay the foundation for its use in
the clinical setting
Discuss clinical applications for pharmacogenomics as it
pertains to opioid use disorder (OUD) management
Review a real-world example of clinical pharmacogenomics
implementation for OUD management
Consider the implications of clinical pharmacogenomics
testing on policy and regulatory affairs
5

Abbreviations Used in This Presentation
ASAM = American Society of Addiction
Medicine
ASIPP = American Society Of Interventional
Pain Physicians
CYP = cytochrome P450
DSM-V = Diagnostic and Statistical Manual of
Mental Disorders, 5th edition
EDDP = 2-ethylidene-1,5-dimethyl-3,3-
diphenylpyrrolidene
EM = extensive metabolizer (phenotype)
EMR = electronic medical record
HCP = health care provider
IM = intermediate metabolizer (phenotype)
MAT = medication-assisted treatment
NMDA = N-methyl-D-aspartate
OUD = opioid use disorder
PD = pharmacodynamics
PGx = pharmacogenomics
PK = pharmacokinetics
PM = poor metabolizer (phenotype)
SAMHSA = Substance Abuse and Mental Health
Services Administration
SNP = single nucleotide polymorphism
UGT = Uridine 5'-diphospho-
glucuronosyltransferase
UM = ultrarapid metabolizer (phenotype)
6

History of
Pharmacogenomics
7

Genomics History and the
Human Genome Project
8
https://unlockinglifescode.org/timeline

The Central Dogma of Molecular
Biology and Omics
DNA
• Genomics
mRNA
• Transcriptomics
Proteins (enzymes, receptors,
transporters, etc.)
• Proteomics
Metabolites
• Metabolomics
9
Transcription
Translation
Metabolism
The study of the structure, function, and
expression of all the genes in an organism
The study of the mRNA
within a cell or organism
The large-scale study of proteins,
including their structure and
function, within a cell/system,
organism
The study of global
metabolite profiles in a
system under a given set of
conditions

Types of Mutations
10
Source of Images:
National Library of
Medicine

Types of Mutations 11
Source of Images:
National Library of
Medicine

Pharmacogenomics
and its Clinical
Foundation
12

What is pharmacogenomics?
Pharmacology Genomics
the widespread
study of genes and
their functions
the science of
drug kinetics and
dynamics of
response
Clinical Pharmacogenomics Testing brings
the science of pharmacogenomics from the
bench to the bedside
13

Pharmacogenomics, Pharmacogenetics, Personalized Medicine, And Precision Medicine
Precision Medicine
Pharmacogenetics
Personalized medicine
Pharmacogenomics Improve
treatment
outcomes
14

Pharmacogenomics:
Targets of Interest
Pharmacodynamics
What the drug does to the body
• Drug receptors
• Drug transporters
• Enzymes
Pharmacokinetics
What the body does to the drug
• Proteins impacting drug absorption,
distribution, metabolism, or excretion, such
as the cytochrome P450 (CYP450) enzymes
15

Comparison of
Guideline-based vs.
Literature-based Pharmacogenomics
Information
Guideline-based
Literature-based
More challenging to interpret findings
Broader information on potentially
clinically-actionable variants
Allows HCP to use clinical judgment
Not all possible variants included
Provides evidence-based clinical
decision support
Lists clinically-actionable variants
(gene-drug)
• Clinical Pharmacogenetics
Implementation Consortium (CPIC)
Guidelines
(https://cpicpgx.org/genes-drugs/)
• Dutch Pharmacogenetics Working
Group (DPWG) Guidelines
• Canadian Pharmacogenomics
Network for Drug Safety (CPNDS)
• Pharmacogenomics Knowledge
Base (PharmGKB)
Sources of Information on
Clinical Pharmacogenomics
16

Cytochrome P450 Enzymes Commonly
Associated With Drug Metabolism
CYP1A2 CYP2B6 CYP2C8
CYP2C9* CYP2C19* CYP2D6*
CYP3A4 CYP3A5* CYP4F2*
17
*CYP enzymes that are included in the CPIC guidelines

CYP450 Enzyme Nomenclature:
Haplotype
CYP 3 A 4 * 1B Family Sub
Family Variant Allele Super
Family
18
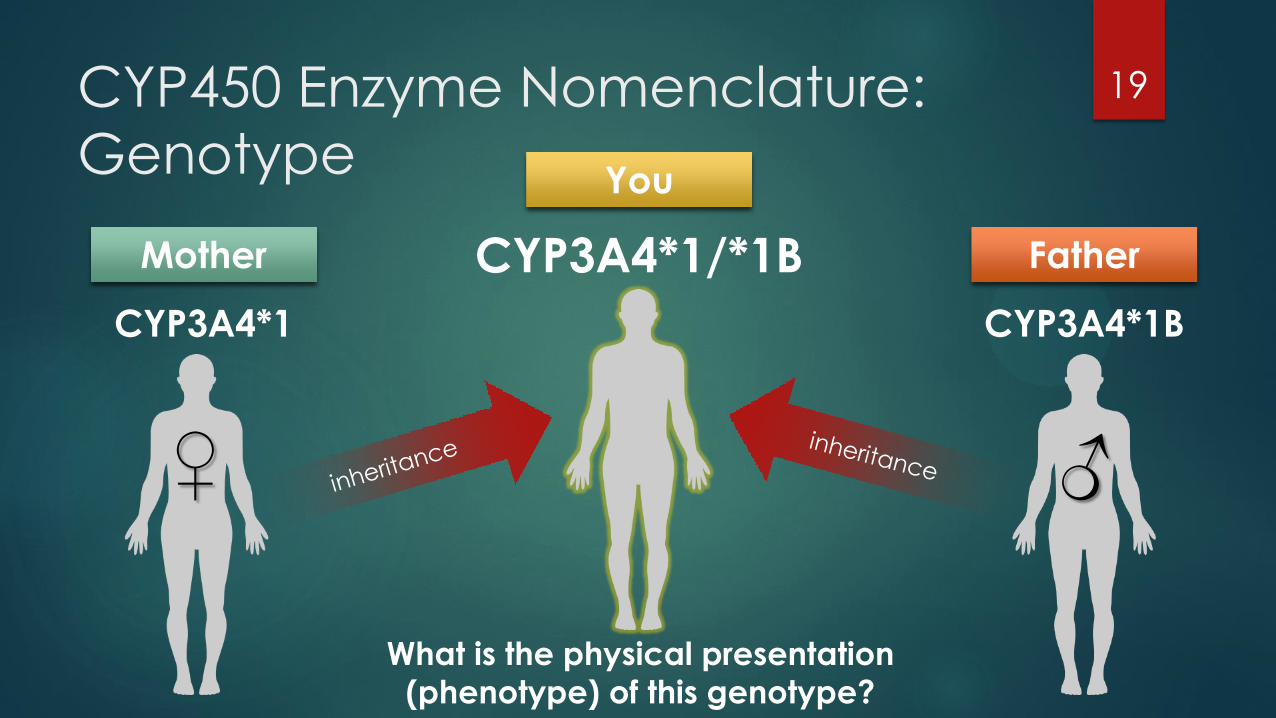
CYP450 Enzyme Nomenclature:
Genotype
19
CYP3A4*1
Mother
CYP3A4*1B
Father CYP3A4*1/*1B
You
♀ ♂
What is the physical presentation
(phenotype) of this genotype?

Cytochrome P450 Metabolizer
Phenotypes
MIN MAX
EM IM
PM UM
MIN MAX
EM IM
PM UM
MIN MAX
EM IM
PM UM
MIN MAX
EM IM
PM UM
Extensive
Metabolizer (EM) Ultrarapid
Metabolizer (UM)
Intermediate
Metabolizer (IM)
Poor Metabolizer (PM)
20
Normal
Rate
of
Metabolism

Pharmacogenetic Testing Process 21
A genetic sample is
collected either via buccal
swab or a blood sample
The clinician sends the sample
to a reference laboratory that
will sequence the DNA and
characterize the genetic
variations of the patient
The reference laboratory
sends a comprehensive
pharmacogenetic testing
report to the clinician for
the patient

Example of Pharmacogenetic
Testing Results
22
Genetic Test Genotype Phenotype Result Interpretation
CYP2C9 *1/*1 Extensive
metabolizer
Normal dosing anticipated; follow standard dosing
practices for CYP2C9 substrates
CYP2C19 *1/*9 Intermediate
metabolizer
Reduced metabolism of CYP2C19 substrates.
Decreased sensitivity to Plavix and other prodrugs
CYP2D6 *2B/*41 Intermediate
metabolizer
Higher serum concentrations of CYP2D6 substrate
medications expected at any treatment dose
CYP3A4 *1B/*1B Ultrarapid
metabolizer
Lower serum concentrations of CYP3A4 substrate
medications, including buprenorphine
CYP3A5 *1A/*6 Intermediate
metabolizer
Consider dose adjustments for CYP3A5 substrate
medications

Clinical Application of
Pharmacogenomic
Testing in Opioid Use
Disorder Management
23

Opioid Use Disorder (OUD)
According to the DSM-V, opioid
use disorder (OUD) is defined as
“a problematic pattern of
opioid use leading to clinically-
significant impairment or
distress” characterized by the
presence of at least two of the
following criteria over a 12-
month period.
24
Severe
(6 or more symptoms)
Moderate
(4 – 5 symptoms)
Mild
(2 – 3 symptoms)

OUD Diagnostic Criteria
1. Using larger amounts of opioids or over a longer period than was intended
2. Persistent desire to cut down or unsuccessful efforts to control use
3. Great deal of time spent obtaining, using, or recovering from use
4. Craving, or a strong desire or urge to use substance
5. Failure to fulfill major role obligations at work, school, or home due to recurrent opioid use
6. Continued use despite recurrent or persistent social or interpersonal problems caused or
exacerbated by opioid use
7. Giving up or reducing social, occupational, or recreational activities due to opioid use
8. Recurrent opioid use in physically hazardous situations
9. Continued opioid use despite physical or psychological problems caused or exacerbated
by its use
10. Tolerance (marked increase in amount; marked decrease in effect)
11. Withdrawal syndrome as manifested by cessation of opioids or use of opioids (or a closely
related substance) to relieve or avoid withdrawal symptoms.
25

Opioid Use Disorder (OUD)
Management
Several organizations involved in
OUD treatment recommend a
combination of pharmacological
measures, such as medication-
assisted treatment (MAT), and
psychosocial approaches, such
as recovery support groups, to
reduce both illicit opioid use and
harm related to opioid use while
improving quality of life
26
MAT options for OUD management
Buprenorphine/naloxone
Methadone
Injectable Naltrexone

Methadone Buprenorphine/
Naloxone
Naltrexone Naloxone
Standard
Dosing for
OUD
management
/Overdose
80-120 mg/day
PO; Start: 20-30
mg PO x1, then
5-10 mg q2-4h
prn
START: 2-8 mg SL
qd x1 day, then 8-
16 mg qd x1-2
days; 4 mg/1 mg-
24 mg/6 mg
buccally/SL qd
Start: 25 mg PO x1,
repeat in 1h if no
withdrawal; Alt:
100 mg PO qod,
150 mg PO q3
days
0.4-2 mg
SC/IM/IV q2-
3min prn; Alt:
0.005 mg/kg IV
x1, then 0.0025-
0.16 mg/kg/h IV
Pharmacokinetics
Metabolism CYP3A4,
CYP2B6,
CYP2C19,
CYP2C9,
CYP2D6
CYP3A4, UGT1A1,
UGT1A3, UGT2B7
Glucuronidation Glucuronidation
Metabolite(s) EDDP (inactive) Norbuprenorphine
(active)
6-β-naltrexol
(major) and others
Naloxone-3-
glucuronide
Pharmacodynamics
Mechanism of
Action
Full mu-opioid
agonist
NMDA receptor
antagonist
Partial mu-opioid
agonist
Kappa-opioid
receptor
antagonist
Full opioid
antagonist
Full opioid
antagonist
27

Buprenorphine Metabolism
28 Methadone Metabolism
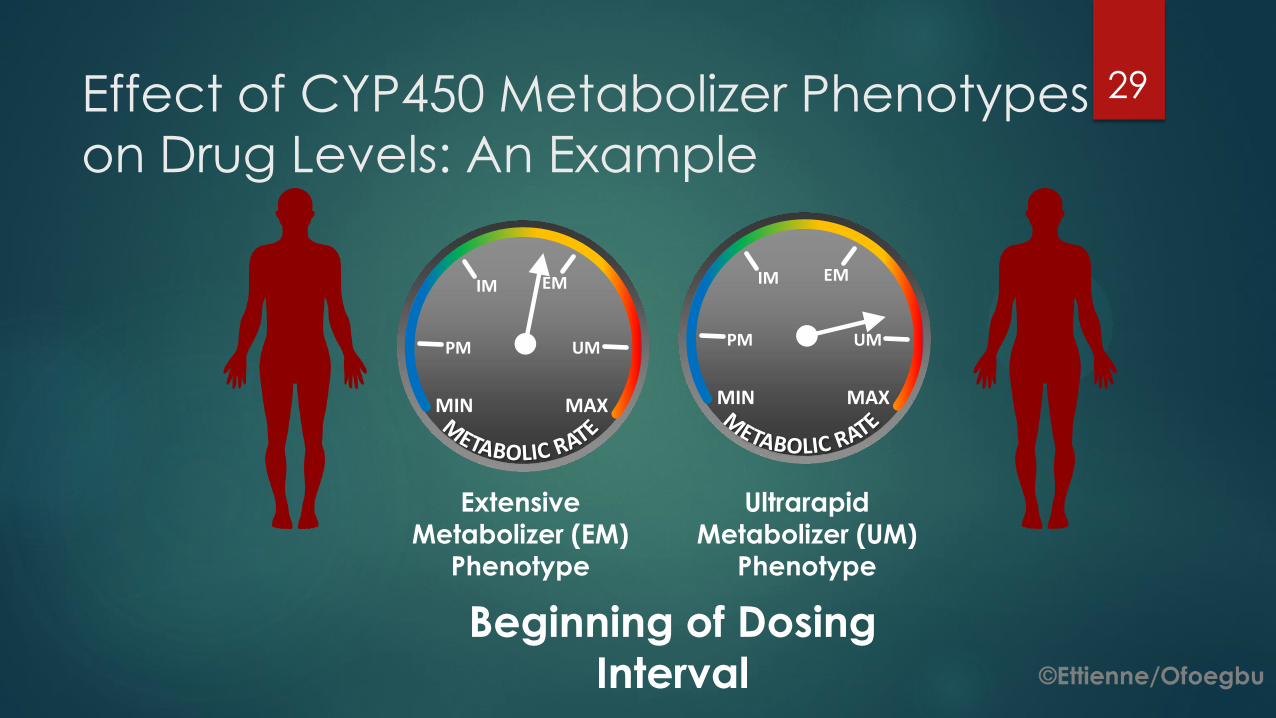
Effect of CYP450 Metabolizer Phenotypes
on Drug Levels: An Example
MIN MAX
EM IM
PM UM
MIN MAX
EM IM
PM UM
Extensive
Metabolizer (EM)
Phenotype
Ultrarapid
Metabolizer (UM)
Phenotype
Beginning of Dosing
Interval
29

Effect of CYP450 Metabolizer Phenotypes
on Drug Levels: An Example
MIN MAX
EM IM
PM UM
MIN MAX
EM IM
PM UM
Extensive
Metabolizer (EM)
Phenotype
Ultrarapid
Metabolizer (UM)
Phenotype
End of Dosing Interval
30

Opioid Analgesics and Their Metabolism
Opioid Analgesic Metabolism
Codeine CYP2D6
Morphine Glucuronidation
Hydrocodone CYP2B6, CYP2C19, CYP2D6, CYP3A4 (primary)
Hydromorphone UGT1A3, UGT2B7
Oxycodone CYP2D6, CYP3A4 (primary)
Oxymorphone Glucuronidation
Methadone CYP3A4, CYP2B6, CYP2C19, CYP2C9 (minor), CYP2D6 (minor)
Tramadol CYP2B6, CYP2D6, CYP3A4
Fentanyl CYP3A4
Buprenorphine CYP3A4, UGT1A1, UGT1A3, UGT2B7
Meperidine CYP2B6 (primary), CYP2C19, CYP3A4
Nalbuphine Unknown
Pentazocine Unknown
Tapentadol UGT substrate; CYP2C9, CYP2C19, CYP2D6
31

Opioids with FDA-Approved Labeling
Describing Abuse-Deterrent Properties
Brand Name Generic
Oxycontin® Oxycodone (extended release)
Targiniq ER® Naloxone/oxycodone (discontinued)
Embeda® Morphine (extended release)
Hysingla ER® Hydrocodone (extended release)
Morphabond ER® Morphine (extended release)
Xtampza ER® Oxycodone (extended release)
Troxyca® Naltrexone/oxycodone (extended release)
Arymo® Morphine (extended release)
Vantrela® Hydrocodone (extended release)
Roxybond® Oxycodone
32

A Real-World Example
of Clinical
Pharmacogenomics
Implementation
33

A Case Report of Clinical Pharmacogenetic
Testing in a Patient with OUD
Patient is an African-American male over the age of 50 and is
receiving buprenorphine as MAT for OUD management from a clinic
in the Washington DC/Maryland/Virginia area
Married, employed, stable home, history of Hepatitis C viral (HCV)
infection, HIV-negative
He consented to clinical pharmacogenetic testing within the regular
course of treatment
He received pharmacogenetic test results, which were used in the
clinical decision-making process
He is a Medicaid recipient
Between December 2015 and June 2016, the insurance company
mandated a maximum buprenorphine dose restriction to 24 mg/day
34

Patient 2D6 3A4 3A5 Ending Dose
(mg/day)
*5/*17
Intermediate
*1/*1B
Ultrarapid
*3A/*7
Poor 32 mg
35

Challenges with Undertreated
Patients with Opioid Use Disorder
Withdrawal symptoms
Criminal activity
Risk of exposure to HIV and Hepatitis C
Risk of death
Productivity
Overall health and wellbeing
36
OUD Management as
a Bio-Psycho-Social
Approach
37
Social
Biomedical Psychological

Policy and Regulatory Implications of
Clinical Pharmacogenomics Testing in Opioid Use Disorder Management
38

Key Stakeholder
Perspectives on
Policy-Relevant
Concerns
Surrounding
Pharmacogenomics Ettienne/Ofoegbu
39

Barriers to Implementation of
Clinical Pharmacogenomics Testing
HCP knowledge of
PGx
Dissemination of PGx test
results
Housing of PGx data (MD vs.
PharmD)
Clinical decision support
Integration of PGx data into
the EMR
Cost-effectiveness
of testing
Payor reimbursement
Preemptive v. reactive testing
Diversity of PGx testing algorithm
40

DNA
Sequencing
Costs (2001-
2015)
41

Pre-emptive vs. Reactive Clinical
Pharmacogenomics Testing
Have PGx test results readily
available
Bulk testing may reduce costs
Only order PGx testing for genes of
interest
More costly upfront
May order more than what is needed
Lag time due to lab analysis may delay availability of test
results
Pre-emptive Reactive
Pros:
Cons:
42
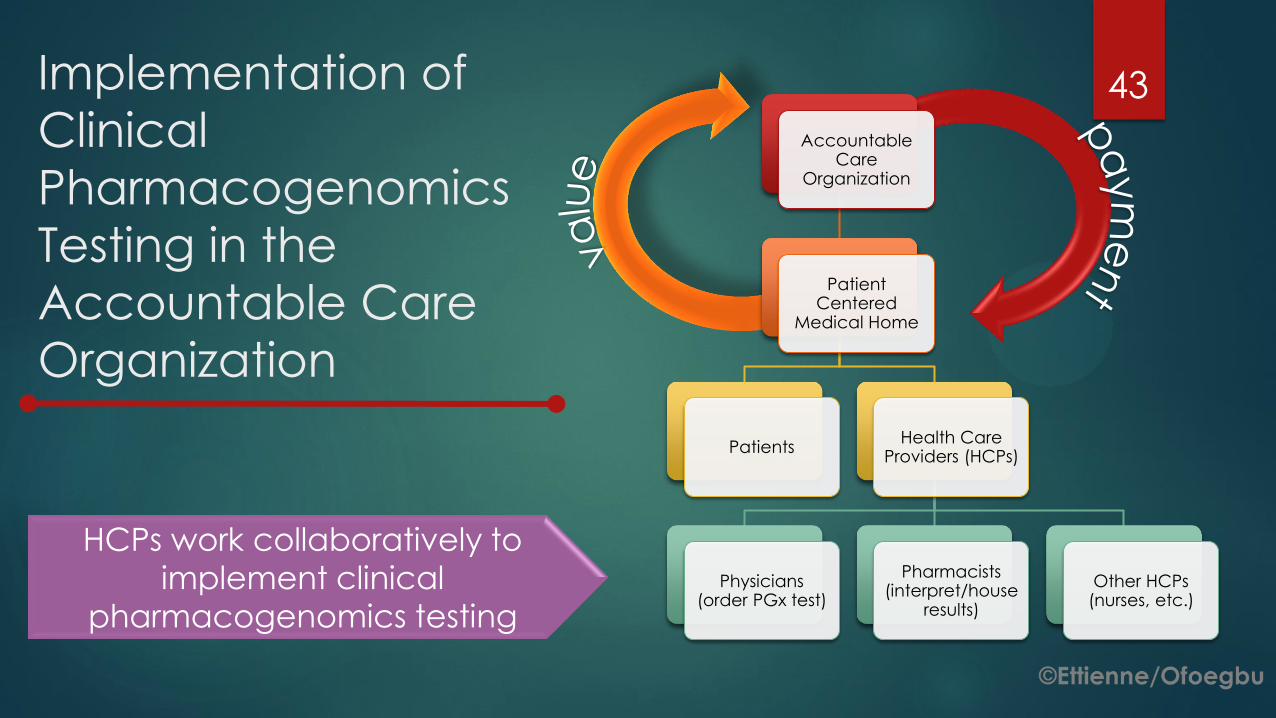
Implementation of
Clinical
Pharmacogenomics
Testing in the
Accountable Care
Organization
Accountable Care
Organization
Patient Centered
Medical Home
Patients Health Care
Providers (HCPs)
Physicians (order PGx test)
Pharmacists (interpret/house
results)
Other HCPs (nurses, etc.)
HCPs work collaboratively to
implement clinical
pharmacogenomics testing
43

FDA Response to Opioid Epidemic 44

FDA Opioid Action Plan
Expand use of advisory committees
Develop warnings and safety information for immediate-release (IR) opioid labeling
Strengthen postmarket requirements
Update Risk Evaluation and Mitigation Strategy (REMS) Program
Expand access to abuse-deterrent formulations (ADFs) to discourage abuse
Support better treatment
Reassess the risk-benefit approval framework for opioid use
Source: https://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm484714.htm
45

References 1. Johnston R. Review article. People Place and Policy Online. 2016;10(1):107-
110. http://dx.doi.org/10.1056/NEJMra1604339. doi: 10.3351/ppp.0010.0001.0008.
2. NLM. What kinds of gene mutations are possible? Genetics Home Reference Web site. https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations. Updated 2017. Accessed Sep 25, 2017.
3. NLM. What are single nucleotide polymorphisms (SNPs)? Genetics Home Reference Web site. https://ghr.nlm.nih.gov/primer/genomicresearch/snp. Updated 2017. Accessed Sep 25, 2017.
4. Horgan RP, Kenny LC. ‘Omic’ technologies: Genomics, transcriptomics, proteomics and metabolomics. The Obstetrician & Gynaecologist. 2011;13(3):189-195. http://onlinelibrary.wiley.com/doi/10.1576/toag.13.3.189.27672/abstract. doi: 10.1576/toag.13.3.189.27672.
5. Pirmohamed M. Pharmacogenetics and pharmacogenomics. British Journal of Clinical Pharmacology. 2001;52(4):345-7. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2014592/. doi: 10.1046/j.0306-5251.2001.01498.x.
6. NHGRI. National human genome research institute | talking glossary of genetic terms | personalized medicine. genome.gov Web site. https://www.genome.gov/glossary/index.cfm?id=150&textonly=true. Updated 2017. Accessed 9/24/, 2017.
7. NHGRI. NHGRI | DNA sequencing costs: Data from the NHGRI genome sequencing program (GSP). NHGRI Web site. https://www.genome.gov/sequencingcostsdata/. Updated 2016. Accessed September 27, 2017.
8. SurgeonGeneral.gov. Facing addiction in america: The surgeon general’s report on alcohol, drugs, and health, 2016 | SurgeonGeneral.gov. SurgeonGeneral.gov | Facing Addiction in America: The Surgeon General's Report on Alcohol, Drugs, and Health, 2016 Web site. https://www.surgeongeneral.gov/library/2016alcoholdrugshealth/index.html. Updated 2016. Accessed Sep 27, 2017.
46

References 9. Medication assisted treatment for opioid use disorders. Federal Register Web
site. https://www.federalregister.gov/documents/2016/07/08/2016-16120/medication-assisted-treatment-for-opioid-use-disorders. Updated 2016. Accessed Sep 20, 2017.
10. Medication and counseling treatment. SAMHSA.gov Web site. https://www.samhsa.gov/medication-assisted-treatment/treatment. Updated 2015. Accessed Sep 20, 2017.
11. Commissioner Oot. Press announcements - califf, FDA top officials call for sweeping review of agency opioids policies. FDA.gov Web site. https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm484765.htm. Updated 2016. Accessed Sep 20, 2017.
12. Califf RM, Woodcock J, Ostroff S. A proactive response to prescription opioid abuse. The New England journal of medicine. 2016;374(15):1480. http://www.ncbi.nlm.nih.gov/pubmed/26845291.
13. Human genome project timeline. Genome: Unlocking Life's Code Web site. https://unlockinglifescode.org/education-resource-profile/human-genome-project-timeline. Accessed Sep 20, 2017.
14. Research, Center for Drug Evaluation and. Information by drug class - FDA opioids action plan. FDA.gov Web site. https://www.fda.gov/Drugs/DrugSafety/InformationbyDrugClass/ucm484714.htm. Updated 2017. Accessed Sep
20, 2017.
15. PharmGKB. Gene-specific information tables for CYP2C9. https://www.pharmgkb.org/page/cyp2c9RefMaterials Web site. https://www.pharmgkb.org/page/cyp2c9RefMaterials. Updated 2017.
16. PharmGKB. Dosing guidelines | PharmGKB. https://www.pharmgkb.org/guidelines Web
site. https://www.pharmgkb.org/guidelines. Updated 2017. Accessed September 7, 2017.
47

References 17. Genetic contribution to variable human CYP3A-mediated
metabolism. http://www.sciencedirect.com/science/article/pii/S0169409X12002773. Accessed 3/18/, 2017.
18. What is pharmacogenomics? - genetics home reference. https://ghr.nlm.nih.gov/primer/genomicresearch/pharmacogenomics. Accessed 3/18/, 2017.
19. Lee JS, Cheong HS, Kim LH, et al. Screening of genetic polymorphisms of CYP3A4 and CYP3A5 genes. Korean J Physiol Pharmacol. 2013;17(6):479-484.
20. Journal of human genetics - table 3 for article: Analysis of CYP3A4 genetic polymorphisms in han chinese. http://www.nature.com/jhg/journal/v56/n6/fig_tab/jhg201130t3.html. Accessed 3/18/, 2017.
21. Allele and genotype frequencies of the polymorphic cytochrome P450 genes (CYP1A1, CYP3A4, CYP3A5, CYP2C9 and CYP2C19) in the jordanian population | SpringerLink. https://link.springer.com/article/10.1007/s11033-012-1807-5. Accessed 3/18/, 2017.
22. The pharmacogenomics journal - abstract of article: High frequency and founder effect of the CYP3A4[ast]20 loss-of-function allele in the spanish population classifies CYP3A4 as a polymorphic enzyme. http://www.nature.com/tpj/journal/v15/n3/abs/tpj201467a.html. Accessed 3/18/, 2017.
23. Pharmacogenomics and pharmacogenetics - springer. https://link.springer.com/chapter/10.1007/978-981-10-0875-7_7. Accessed 3/17/, 2017.
24. Buprenorphine package insert. Accessed 3/18/2017
48
National Library of Medicine Image References
1. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017
Sep 26. [Illustration] Missense mutation; [cited 2017 Sep 26]; [about 1 screen]. Available from:
https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
2. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017
Sep 26. [Illustration] Nonsense mutation; [cited 2017 Sep 26]; [about 1 screen]. Available from:
https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
3. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017
Sep 26. [Illustration] Insertion; [cited 2017 Sep 26]; [about 1 screen]. Available from: https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
4. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017
Sep 26. [Illustration] Deletion; [cited 2017 Sep 26]; [about 1 screen]. Available from:
https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
5. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017 Sep 26. [Illustration] Duplication; [cited 2017 Sep 26]; [about 1 screen]. Available from:
https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
6. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017
Sep 26. [Illustration] Frameshift mutation; [cited 2017 Sep 26]; [about 1 screen]. Available from:
https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
7. Illustration: National Library of Medicine (US). Genetics Home Reference [Internet]. Bethesda (MD): The Library; 2017
Sep 26. [Illustration] Repeat expansion; [cited 2017 Sep 26]; [about 1 screen]. Available from:
https://ghr.nlm.nih.gov/primer/mutationsanddisorders/possiblemutations
49

PCSS-O Colleague Support Program
and PCSS Discussion Forum • PCSS-O Colleague Support Program is designed to offer general information to health professionals
seeking guidance in their clinical practice in prescribing opioid medications.
• PCSS-O Mentors comprise a national network of trained providers with expertise in addiction
medicine/psychiatry and pain management.
• Our mentoring approach allows every mentor/mentee relationship to be unique and catered to
the specific needs of both parties.
• The mentoring program is available at no cost to providers.
• PCSS Discussion Forum: A resource that provides an “Expert of the Month” who will answer questions about educational content that has been presented through PCSS projects. To join, register here:
http://pcss.invisionzone.com/register
For more information on requesting or becoming a mentor visit:
www.pcss-o.org/colleague-support
50

PCSS-O is a collaborative effort led by American Academy of Addiction Psychiatry (AAAP) in partnership
with: Addiction Technology Transfer Center (ATTC), American Academy of Neurology (AAN), American
Academy of Pain Medicine (AAPM), American Academy of Pediatrics (AAP), American College of
Physicians (ACP), American Dental Association (ADA), American Medical Association (AMA), American
Osteopathic Academy of Addiction Medicine (AOAAM), American Psychiatric Association (APA),
American Society for Pain Management Nursing (ASPMN), International Nurses Society on Addictions (IntNSA), and Southeast Consortium for Substance Abuse Training (SECSAT).
For more information visit: www.pcss-o.org
For questions email: [email protected]
Twitter: @PCSSProjects
Funding for this initiative was made possible (in part) by grant no. 5H79TI025595-03 from SAMHSA. The views expressed in written conference materials or publications and by
speakers and moderators do not necessarily reflect the official policies of the Department of Health and Human Services; nor does mention of trade names, commercial practices,
or organizations imply endorsement by the U.S. Government.
51

Questions?
52