clinical and prognostic value of immunogenetic
TRANSCRIPT

ARTICLE OPEN ACCESS
Clinical and Prognostic Value of ImmunogeneticCharacteristics in Anti-LGI1 EncephalitisSergio Muntildeiz-Castrillo MD Julie Haesebaert MD PhD Laure Thomas MD Alberto Vogrig MD
Anne-Laurie Pinto MSc Geraldine Picard MSc Charlotte Blanc MSc Le-Duy Do PhD
Bastien Joubert MD PhD Giulia Berzero MD Dimitri Psimaras MD Agusti Alentorn MD PhD
Veronique Rogemond PhD Valerie Dubois MD Aditya Ambati PhD Ryad Tamouza MD PhD
Emmanuel Mignot MD PhD and Jerome Honnorat MD PhD
Neurol Neuroimmunol Neuroinflamm 20218e974 doi101212NXI0000000000000974
Correspondence
Dr Honnorat
jeromehonnoratchu-lyonfr
AbstractObjectiveAntibodies against leucine-rich glioma-inactivated 1 (LGI1-Abs) characterize a limbic en-cephalitis (LE) strongly associated with HLA-DRB10701 although some patients lack LGI1-Abs in CSF or do not carry this allele Whether they represent a different subtype of disease orhave different prognoses is unclear
MethodsRetrospective analysis of clinical features IgG isotypes and outcome according to LGI1-AbCSF positivity and DRB10701 in a cohort of anti-LGI1 LE patients
ResultsPatients with LGI1-Abs detected in both CSF and serum (105134 78) were compared withthose who were CSF negative (29134 22) Both groups had similar clinical features andserum levels but CSF-positive patients had shorter diagnostic delay more frequently hypo-natremia inflammatory CSF and abnormal MRI (p lt 005) Human leukocyte antigen (HLA)genotyping was performed in 72134 (54) patients and 6372 (88) carried DRB10701Noncarriers (972 12) were younger more commonly women and had less frequentlypsychiatric and frontal symptoms (p lt 005) No difference in IgG isotypes according to CSFpositivity or HLA was found (p gt 005) HLA and IgG isotypes were not associated with pooroutcome (mRS gt2 at last follow-up) in univariate analyses CSF positivity was only identified asa poor outcome predictor in the multivariate analysis including the complete follow-upwhereas age and female sex also remained when just the first year was considered
ConclusionsLE without CSF LGI1-Abs is clinically indistinguishable and likely reflects just a lesser LGI1-Abproduction HLA association is sex and age biased and presents clinical particularities sug-gesting subtle differences in the immune response Long-term outcome depends mostly ondemographic characteristics and the intensity of the intrathecal synthesis
From the French Reference Center on Paraneoplastic Neurological Syndromes and Autoimmune Encephalitis (SM-C LT AV A-LP GP CB L-DD BJ VR J Honnorat)Hospices Civils de Lyon Hopital Neurologique Bron France SynatAc Team (SM-C LT AV A-LP GP CB L-DD BJ VR J Honnorat) Institut NeuroMyoGene INSERMU1217CNRS UMR 5310 Universite de Lyon Universite Claude Bernard Lyon 1 France Clinic Research and Epidemiology Department (J Haesebaert) Hospices Civils de Lyon Lyon FranceHESPER Team EA 7425 Medicine School Universite Claude Bernard Lyon 1 France Neurology Department 2-Mazarin (GB DP A Alentorn) Hopitaux Universitaires La PitieSalpetriere-Charles Foix APHP Brain and Spinal Cord Institute (GB DP A Alentorn) INSERMU1127CNRSUMR 7255 Universite Pierre-et-Marie-Curie Universites Sorbonnes ParisFrance HLA Laboratory (VD) French Blood Service EFS Auvergne-Rhone-Alpes Lyon France Stanford University Center for Sleep Sciences andMedicine (A Ambati EM) Palo AltoCA and Department of Psychiatry (RT) Hopitaux Universitaires Henri Mondor Creteil France Mondor Institute for Biomedical Research INSERM U955 Universite de Paris-Est-Creteil France
Go to NeurologyorgNN for full disclosures Funding information is provided at the end of the article
The Article Processing Charge was funded by Universite Claude Bernard Lyon 1
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial-NoDerivatives License 40 (CC BY-NC-ND) which permits downloadingand sharing the work provided it is properly cited The work cannot be changed in any way or used commercially without permission from the journal
Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology 1
Patients with limbic encephalitis (LE) and antibodies againstleucine-rich glioma-inactivated 1 (LGI1-Abs) are usually el-derlymenwho develop severe anterograde amnesia psychiatricsymptoms and seizures along with medial temporal lobe ab-normalities in brain MRI but intriguingly often without in-flammatory signs in CSF routine analysis1ndash5 Furthermorecontrary to other types of autoimmune encephalitis such asanti-NMDA receptor encephalitis6 serum testing is moresensitive than CSF for the detection of LGI1-Abs in our ex-perience which has also been reported by others37 The diseaseis also remarkably associated with the allele HLA-DRB10701which is found in nearly 90 of the patients8ndash11 However todate whether patients without detectable LGI1-Abs in the CSFand those not carrying DRB10701 show distinct particulari-ties is still unclear In addition despite the response to im-munotherapy in anti-LGI1 LE being satisfactory in mostpatients1ndash312 the cognitive recovery is usually incomplete anddiverse prognostic factors have been reported3111314 Never-theless the role of CSF positivity and human leukocyte antigen(HLA) on outcome has not been widely investigated1115
We therefore aimed to investigate whether clinical or immu-nologic differences exist among patients with anti-LGI1 LEaccording to CSF positivity for LGI1-Abs and HLA-DRB10701 carrier status In addition we studied the evo-lution of disability and the prognostic factors including theaforementioned biomarkers
MethodsPatients and Clinical DataAll consecutive patients diagnosed in our center from January2010 to November 2018 with LE and serum positive forLGI1-Abs were identified Serum LGI1-Abs were detectedwith a cell-based assay (CBA) as previously described5
Immunohistofluorescence (IHF) on rat brain sections wasused as screening technique in CSF and further confirmed byCBA only CSF samples positive for both techniques weretherefore considered as positive Demographic and clinicaldata were retrospectively collected from hospital charts in-cluding first clinical feature (table e-1 linkslwwcomNXIA430) disability at onset using the modified Rankin Scale(mRS) diagnostic delay CSF positivity for LGI1-Abs clinicalfeatures that developed during the course of the disease (tablee-1) presence of cancer intensive care unit (ICU) admissionpresence of hyponatremia inflammatory CSF (defined aslevels exceeding the upper limit of normal of our laboratory
reference values of protein content [gt05 mgdL] andorwhite cell count [gt2 cellsmL] andor oligoclonal bands)brain MRI (normal or unilateralbilateral medial temporalhypersignal) first-line treatment (corticosteroids IV immu-noglobulin [IVIG] and plasma exchange) second-linetreatment (rituximab and cyclophosphamide) chronic im-munotherapy (azathioprine and mycophenolate) dominantsequela at last follow-up and mRS at diagnosis and after 3 69 12 18 24 and 36 months Patients for whom only serumwas tested and those without clinical data were excluded fromthe study
Serum Levels of LGI1-AbsLevels of serum LGI1-Abs were measured using an ELISA on aCBA Culture medium was eliminated and cells were washedonce with phosphate-buffered saline (PBS 200 μLwell) Serawere next diluted (110) using a dilution medium composedof Dulbeccorsquos Modified Eagle Medium (DMEM) 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) nor-mal goat serum (NGS) 5 and bovine serum albumin (BSA)1 and then incubated for 30 minutes at 37degC (50 μLwell)Cells were washed once with PBS (200 μLwell) and fixed using4 paraformaldehyde for 15minutes at room temperature (100μLwell) Cells were washed once again with PBS (200 μLwell) and twice with 005PBS-Tween (200 μLwell) to belater incubated for 1 hourwith a secondary anti-human antibody(110000 dilution Peroxidase AffiniPure Goat Anti-HumanIgG Fcγ fragment specific Jackson ImmunoResearch Cam-bridge UK) coupled to peroxidase for 30 minutes at 37degC (50μLwell) Cells were washed using 005PBS-Tween twice andonce with PBS (200 μLwell) wells aspirated 339 559-tetra-methylbenzidine substrate solution (50 μLwell) added andincubated for 30 minutes The reaction was stopped using sul-furic acid (2 M 50 μLwell) The plate was immediately read at450 nm of wavelength using the SpectraMax Plus platform(Molecular Devices San Jose CA) All assays were performedin triplicate Within each test the mean of the 2 optic density(OD) values obtained was calculated for both transfected andnontransfected cells The difference between these labeled asDelta OD was then obtained For each sample the mean of theDelta OD from the 3 experiments was used for statisticalanalysis Twenty-five sera from patients negative for LGI1-Abswere used as controls for technical validation
IgG IsotypesIsotyping was performed using mouse anti-human antibodiesthat specifically recognize IgG1 (mouse anti-human IgG1CH2 domain Bio-Rad Hercules CA) IgG2 (purified mouse
GlossaryBSA = bovine serum albumin CBA = cell-based assay DMEM = Dulbeccorsquos Modified Eagle Medium FBDS = faciobrachialdystonic seizure HEPES = 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid HLA = human leukocyte antigen ICU =intensive care unit IHF = immunohistofluorescence IQR = interquartile range IVIG = IV immunoglobulin LE = limbicencephalitis LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 mRS = modified Rankin Scale NGS = normalgoat serum OD = optic density PBS = phosphate-buffered saline
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
anti-human IgG2 clone G18-21 [RUO] BD Biosciences SanJose CA) IgG3 (mouse anti-human IgG3 Bio-RAD) orIgG4 (purified mouse anti-human IgG4 clone G17-4 [RUO]BD Biosciences) Either 100 or 200 μL (according to whether96 or 24-well plate were used) of the IgG solution of interest(diluted 11000 for IgG1 and IgG3 and 1500 for IgG2 andIgG4) in DMEM-HEPES-NGS5-BSA1 was used and in-cubated for 1 hour at room temperature in the dark Afteraspiration cells were washed with DMEM-HEPES (100200μL) and once again with PBS (100200 μL) A secondary goatanti-mouse antibody (100200 μL) coupled to a fluoro-chrome (Alexa Fluor 555 ThermoFisher Scientific WalthamMA) diluted 11000 in DMEM-HEPES-NGS5-BSA1was added and then incubated for 1 hour at room temperaturein the dark After aspiration cells were washed with DMEM-HEPES (100200 μL) and with PBS (100200 μL) In ad-dition titration of IgG1 and IgG4 subclasses in serum andCSF was performed only in the double-positive samples anddetermined as the lowest dilution with positive signal by CBAAll the CBAs were read using a Zeiss Axiophot microscope(Zeiss Oberkochen Germany)
To validate the specificity of the secondary antibodies used forIgG isotyping a Western blot was performed with 1 μg ofevery purified IgG subclass (IgG1 HCA192 IgG2 HCA193IgG3 HCA194 IgG4 HCA195 Bio-Rad) load on each wellAfter migration transfer and saturation membranes wereseparately incubated with each anti-human IgG subtype (11000 dilution for anti-IgG1 and 3 1500 for anti-IgG2 and 4antibodies) Revelation was performed with goat anti-mouseIgG (120000 115-036-003 Jackson ImmunoResearchSuffolk United Kingdom)
HLA AnalysisHLA genotyping was performed in patients with availableDNA using next-generation sequencing on a MiSeq se-quencer system (Illumina San Diego CA) and is reported at a4-digit level resolution Controls (courtesy of EFS Auvergne-Rhone-Alpes) were 300 healthy subjects of Caucasian ethnicorigin genotyped for HLA A B C DR and DQ previouslyobtained using next-generation sequencing technology(Omixon Budapest Hungary)
Statistical AnalysisAn exploratory approach16 using χ2 and Fisher exact tests forcategorical variables and the Wilcoxon signed-rank test forquantitative data was used to compare patients according toCSF positivity for LGI1-Abs DRB10701 carrier status orIgG isotypes
To search for factors associated with good (defined as lastmRs le2) or poor prognosis (mRs gt2) a 2-step approach wasused first a univariate binary logistic regression (with con-tinuous variables categorized) and second a multivariateanalysis using a generalized linear mixed model for binarydistribution (SAS Glimmix procedure) This mixed modelassessed repeated measures of mRS for each patient we
declared the patient as random effect and the remaining factorsas fixed effect The dependent variable was goodpoor prog-nosis as defined above and the choice of independent variablesincluded was based on clinical criteria the demographic (agesex) and main clinical (amnesia faciobrachial dystonic seizures[FBDSs] other seizures psychiatric symptoms and frontalsyndrome) characteristics that are present at disease onsetCSF positivity for LGI1-Abs as a biomarker (HLA was ex-cluded due to the small sample size compared with the overallcohort) and diagnostic delay length of follow-up and treat-ment as possible confounder factors The probability to switchfrom good to poor outcome was modeled Statistical analyseswere conducted using SAS software version 94 (SAS InstituteCary NC) All p values were 2 tailed and p values lt005 wereconsidered statistically significant
Differences in HLA carrier frequencies between patients andcontrols were analyzed using the 2-tailed Fishers exact tests(SPSS software package version 250 IBM Corp ArmonkNY) Allele frequency comparisons were Bonferroni cor-rected using the number of alleles for each locus corrected p lt005 values were considered significant
Standard Protocol Approvals Registrationsand Patient ConsentsWritten informed consent was obtained from all patients forthe storage and use of biological samples and clinical in-formation for research purposes The Institutional ReviewBoard of the Universite Claude Bernard Lyon 1 and HospicesCivils de Lyon approved the study (ICARE NCT-04106596)
Data AvailabilityAny data not published within the article are available and willbe shared by request from any qualified investigator
ResultsCharacteristics of Patients According to LGI1-Ab CSF PositivityA total of 142 patients with LE and serum LGI1-Abs wereidentified Eight (8142 6) patients were excluded eitherbecause clinical data were lacking or because LGI1-Abs werenot assayed in CSF Among the remaining 134 patients positivefor LGI1-Abs in serum 105 (78) were also CSF positiveTwenty-nine (22) patients were considered to be CSF neg-ative 23 (79) were negative for both IHF and CBA 5 (17)were positive for IHF but negative for CBA and 1 subject (3)was negative for only CBA No significant difference in sex ageand clinical presentation was observed between the 2 groupsDiagnostic delay was longer in the CSF-negative (median 158days interquartile range [IQR] 61ndash295) vs the CSF-positive(median 98 days IQR 42ndash161 p = 001) group Patients withpositive CSF had more frequently hyponatremia (6110558 vs 1029 35 p = 002) inflammatory CSF findings(5899 59 vs 925 36 p = 004) and abnormal MRIs(72102 71 vs 1329 45 p = 001 table 1)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 3
Serum levels were determined by ELISA-CBA in 60 patientswith available samples 48 of these patients (80) had LGI1-Abs in both serum and CSF while 12 (20) had LGI1-Absonly in the serum No significant difference in serum levelswas found between CSF-positive and CSF-negative patients(p = 091 figure 1A)
HLA Association in Anti-LGI1 EncephalitisDNA was available in 72134 (54) patients 6872 (94) ofwhom were of Caucasian origin DRB10701 was carried by6372 (88) patients this was significantly more frequentthan in the control group (86300 29 corrected p lt 00001OR = 1742 95 CI 829ndash3658) Several alleles in linkage
disequilibrium with DRB10701 were also found more com-monly in patients A3001 (1072 14 vs 7300 2 in thecontrol group corrected p = 0009 OR = 675 95 CI247ndash1842) C0602 (2572 35 vs 36300 12 in thecontrol group corrected p lt 0001 OR = 390 95 CI215ndash709) and DQB10202 (5372 74 vs 78300 26 inthe control group corrected p lt 00001 OR = 794 95 CI443ndash1424) Another DRB1 allele DRB10402 was also sig-nificantly more frequent among patients (972 13) com-pared with controls (7300 2 corrected p = 003 OR = 5995 CI 22ndash167) however 79 (78) DRB10402 carrierswere also DRB10701 carriers Four alleles were found to besignificantly more common in controls than in patients but this
Table 1 Characteristics of the Patients According to LGI1-Ab CSF Positivity
Overall cohort (n = 134) Positive CSF (n = 105) Negative CSF (n = 29) p Valuea
Men n () 84 (63) 68 (65) 16 (55) 034
Median age y (IQR range) 67 (58ndash74 21ndash86) 66 (58ndash74 21ndash85) 68 (56ndash74 37ndash86) 061
Diagnostic delay d median (IQR range) 118 (46ndash182 4ndash854) 98 (42ndash161 4ndash854) 158 (61ndash295 31ndash545) 001
mRS score at onset gt2 n () 99 (74) 83 (79) 16 (55) 008
First symptom n () 042
Amnesia 48 (36) 38 (36) 10 (35)
Other seizures 38 (28) 31 (30) 7 (24)
FBDS 32 (24) 22 (21) 10 (35)
Psychiatric symptoms 16 (12) 14 (13) 2 (7)
Disease course n ()
Amnesia 116 (87) 92 (88) 24 (83) 049
Other seizures 98 (73) 81 (77) 17 (59) 011
FBDS 71 (53) 53 (51) 18 (62) 026
Psychiatric symptoms 83 (62) 67 (64) 16 (55) 039
Frontal syndrome 64 (48) 50 (48) 14 (48) 1
Sleep disorders 48 (36) 39 (37) 9 (31) 054
Apraxia 17 (13) 12 (11) 5 (17) 052
Aphasia 11 (8) 6 (6) 5 (17) 005
Dysautonomia 6 (5) 5 (5) 1 (4) 076
ICU admission n () 12 (9) 9 (9) 3 (10) 076
Status epilepticus n () 10 (8) 8 (8) 2 (7) 089
Hyponatremia n () 71 (53) 61 (58) 10 (35) 002
MRI (N = 131) MTL hyperintensity n () 85 (65) 72 (71) 13 (45) 001
Inflammatory CSF (N = 124) n () 67 (54) 58 (59) 9 (36) 004
Cancer n () 6 (5)b 5 (5) 1 (4) 076
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LE = limbic encephalitis LGI1 = leucine-rich glioma-inactivated 1 MTL = medial temporal lobea CSF positive vs CSF negativeb Includedmalignant thymoma (n = 2 diagnosed 91 and 6months before LE) lung adenocarcinoma (n = 1 4months after LE) kidney (n = 1 4months before)hepatic (n = 1 9 months after) and prostate (n = 1 2 months after) cancers
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
finding was likely a consequence of an overrepresentation ofDRB10701 and its linked alleles in the patients group (tablee-2 linkslwwcomNXIA430)
Clinical Characteristics Per DRB10701 StatusThe non-DRB10701 carriers were more frequently women(79 78 vs 1763 27 ofDRB10701 carriers p= 0005) andyounger (median age 46 years IQR 37ndash59 vs 66 IQR 58ndash74 for
DRB10701 carriers p = 0001) Only 3 patients with an asso-ciated cancer were analyzed for HLA genotyping 2 of them (witha kidney and a hepatic cancer)wereDRB10701 carriers whereas1 with a malignant thymoma was not There was no significantdifference according to HLA status for most of the variables an-alyzed however noncarriers presented less frequently with psy-chiatric symptoms (29 22 vs 4263 67 p = 0001) andfrontal syndrome (09 vs 3263 51 p = 0004 table 2)
Figure 1 Immunologic Characteristics of Anti-LGI1 Encephalitis
(A) Box plot showing LGI1-Abs serumlevels according to CSF positivity Nosignificant difference in serum levelsrepresented as Delta OD measuredby ELISA-CBA was found betweenCSF-positive (medianDelta OD= 037IQR 029ndash044) and CSF-negative(median Delta OD = 037 IQR019ndash048) patients (p = 091) Controlsera from patients without LGI1-Abswere used for technical validation (B)Venn diagram showing serum IgGisotypesmost sera (6089 67)werepositive for both IgG1 and IgG4 (C)Box plot representing IgG14 serumtiters IgG4 titers were higher thanIgG1 titers in 59 double-positivesamples analyzed (D) Venn diagramshowing CSF IgG isotypes IgG4 wasthe most detected isotype (374093) but 21 samples were also pos-itive for IgG1 (E) Box plot represent-ing IgG14 CSF titers IgG4 titers werehigher than IgG1 titers in the 29double-positive samples analyzedCBA = cell-based assay IQR = inter-quartile range LGI1-Abs = antibodiesagainst leucine-rich glioma-inacti-vated 1 protein OD = optic density
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 5
IgG Isotyping in Serum and CSFIgG isotypes were determined in 89 sera and 40 CSF 38samples were pairs (91 patients in total) Twenty sera (208923) with negative CSF for LGI1-Abs could not be isotyped inCSF due to nondetectable Abs HLA status was known for 6891 (75) patients and 6068 (88)wereDRB10701 carriers
The main serum isotypes detected were IgG1 (7789 87)and IgG4 (7289 81 figure 1B) However IgG4 titers weresignificantly higher (median 11280 IQR 11280ndash15120)than IgG1 titers (median 1640 IQR 1320ndash11280 p =00001) in 59 double-positive samples analyzed (figure 1C)In the CSF IgG4 (3740 93) was the most frequent iso-type followed by IgG1 (2440 60 figure 1D) When 21double-positive CSF samples were analyzed IgG4 titers were
significantly higher (median 180 IQR 140ndash1120) thanthose of IgG1 (median 140 IQR 115ndash180 p = 0008figure 1E)
There was no significant difference in serum isotypes orIgG14 titers according to CSF positivity nor in serum or CSFisotypes and IgG14 titers according to DRB10701 carrierstatus in addition there was no significant difference inclinical and paraclinical features according to the presenceabsence of IgG14 in serumCSF (data not shown)
The validating Western blot performed showed high speci-ficity for the anti-IgG1 anti-IgG3 and IgG4 used whereasanti-IgG2 presented slight cross-reactivity with all other IgGisotypes (data not shown)
Table 2 Characteristics of DRB10701 Carriers Compared With Noncarriers
DRB10701 carriers (n = 63) Noncarriers (n = 9) p Value
Men n () 46 (73) 2 (22) 0005
Median age y (IQR range) 66 (58ndash74 26ndash86) 46 (37ndash59 21ndash73) 0001
Diagnostic delay d median (IQR range) 41 (25ndash181 7ndash854) 121 (51ndash212 6ndash348) 027
First symptom n () 035
Amnesia 21 (33) 2 (22)
Other seizures 20 (32) 4 (44)
FBDS 11 (18) 3 (33)
Psychiatric symptoms 11 (18) 0 (0)
Disease course n ()
Amnesia 53 (84) 7 (78) 063
Other seizures 50 (79) 8 (89) 022
FBDS 34 (54) 4 (44) 072
Psychiatric symptoms 42 (67) 2 (22) 0001
Frontal syndrome 32 (51) 0 (0) 0004
Sleep disorders 24 (38) 4 (44) 072
Apraxia 9 (14) 1 (11) 1
Aphasia 6 (10) 0 (0) 1
Dysautonomia 3 (5) 1 (11) 042
ICU admission n () 5 (8) 0 (0) 038
Status epilepticus n () 1 (2) 2 (7) 070
Hyponatremia n () 36 (57) 4 (44) 049
MRI (N = 71) MTL hyperintensity n () 38 (61) 7 (78) 047
Inflammatory CSF (N = 67) n () 36 (62) 3 (33) 014
LGI-Abs in CSF n () 48 (76) 6 (67) 068
Cancer n () 2 (3) 1 (11) 033
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LGI1 = leucine-rich glioma-inactivated1 MTL = medial temporal lobe
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Patients with limbic encephalitis (LE) and antibodies againstleucine-rich glioma-inactivated 1 (LGI1-Abs) are usually el-derlymenwho develop severe anterograde amnesia psychiatricsymptoms and seizures along with medial temporal lobe ab-normalities in brain MRI but intriguingly often without in-flammatory signs in CSF routine analysis1ndash5 Furthermorecontrary to other types of autoimmune encephalitis such asanti-NMDA receptor encephalitis6 serum testing is moresensitive than CSF for the detection of LGI1-Abs in our ex-perience which has also been reported by others37 The diseaseis also remarkably associated with the allele HLA-DRB10701which is found in nearly 90 of the patients8ndash11 However todate whether patients without detectable LGI1-Abs in the CSFand those not carrying DRB10701 show distinct particulari-ties is still unclear In addition despite the response to im-munotherapy in anti-LGI1 LE being satisfactory in mostpatients1ndash312 the cognitive recovery is usually incomplete anddiverse prognostic factors have been reported3111314 Never-theless the role of CSF positivity and human leukocyte antigen(HLA) on outcome has not been widely investigated1115
We therefore aimed to investigate whether clinical or immu-nologic differences exist among patients with anti-LGI1 LEaccording to CSF positivity for LGI1-Abs and HLA-DRB10701 carrier status In addition we studied the evo-lution of disability and the prognostic factors including theaforementioned biomarkers
MethodsPatients and Clinical DataAll consecutive patients diagnosed in our center from January2010 to November 2018 with LE and serum positive forLGI1-Abs were identified Serum LGI1-Abs were detectedwith a cell-based assay (CBA) as previously described5
Immunohistofluorescence (IHF) on rat brain sections wasused as screening technique in CSF and further confirmed byCBA only CSF samples positive for both techniques weretherefore considered as positive Demographic and clinicaldata were retrospectively collected from hospital charts in-cluding first clinical feature (table e-1 linkslwwcomNXIA430) disability at onset using the modified Rankin Scale(mRS) diagnostic delay CSF positivity for LGI1-Abs clinicalfeatures that developed during the course of the disease (tablee-1) presence of cancer intensive care unit (ICU) admissionpresence of hyponatremia inflammatory CSF (defined aslevels exceeding the upper limit of normal of our laboratory
reference values of protein content [gt05 mgdL] andorwhite cell count [gt2 cellsmL] andor oligoclonal bands)brain MRI (normal or unilateralbilateral medial temporalhypersignal) first-line treatment (corticosteroids IV immu-noglobulin [IVIG] and plasma exchange) second-linetreatment (rituximab and cyclophosphamide) chronic im-munotherapy (azathioprine and mycophenolate) dominantsequela at last follow-up and mRS at diagnosis and after 3 69 12 18 24 and 36 months Patients for whom only serumwas tested and those without clinical data were excluded fromthe study
Serum Levels of LGI1-AbsLevels of serum LGI1-Abs were measured using an ELISA on aCBA Culture medium was eliminated and cells were washedonce with phosphate-buffered saline (PBS 200 μLwell) Serawere next diluted (110) using a dilution medium composedof Dulbeccorsquos Modified Eagle Medium (DMEM) 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES) nor-mal goat serum (NGS) 5 and bovine serum albumin (BSA)1 and then incubated for 30 minutes at 37degC (50 μLwell)Cells were washed once with PBS (200 μLwell) and fixed using4 paraformaldehyde for 15minutes at room temperature (100μLwell) Cells were washed once again with PBS (200 μLwell) and twice with 005PBS-Tween (200 μLwell) to belater incubated for 1 hourwith a secondary anti-human antibody(110000 dilution Peroxidase AffiniPure Goat Anti-HumanIgG Fcγ fragment specific Jackson ImmunoResearch Cam-bridge UK) coupled to peroxidase for 30 minutes at 37degC (50μLwell) Cells were washed using 005PBS-Tween twice andonce with PBS (200 μLwell) wells aspirated 339 559-tetra-methylbenzidine substrate solution (50 μLwell) added andincubated for 30 minutes The reaction was stopped using sul-furic acid (2 M 50 μLwell) The plate was immediately read at450 nm of wavelength using the SpectraMax Plus platform(Molecular Devices San Jose CA) All assays were performedin triplicate Within each test the mean of the 2 optic density(OD) values obtained was calculated for both transfected andnontransfected cells The difference between these labeled asDelta OD was then obtained For each sample the mean of theDelta OD from the 3 experiments was used for statisticalanalysis Twenty-five sera from patients negative for LGI1-Abswere used as controls for technical validation
IgG IsotypesIsotyping was performed using mouse anti-human antibodiesthat specifically recognize IgG1 (mouse anti-human IgG1CH2 domain Bio-Rad Hercules CA) IgG2 (purified mouse
GlossaryBSA = bovine serum albumin CBA = cell-based assay DMEM = Dulbeccorsquos Modified Eagle Medium FBDS = faciobrachialdystonic seizure HEPES = 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid HLA = human leukocyte antigen ICU =intensive care unit IHF = immunohistofluorescence IQR = interquartile range IVIG = IV immunoglobulin LE = limbicencephalitis LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 mRS = modified Rankin Scale NGS = normalgoat serum OD = optic density PBS = phosphate-buffered saline
2 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
anti-human IgG2 clone G18-21 [RUO] BD Biosciences SanJose CA) IgG3 (mouse anti-human IgG3 Bio-RAD) orIgG4 (purified mouse anti-human IgG4 clone G17-4 [RUO]BD Biosciences) Either 100 or 200 μL (according to whether96 or 24-well plate were used) of the IgG solution of interest(diluted 11000 for IgG1 and IgG3 and 1500 for IgG2 andIgG4) in DMEM-HEPES-NGS5-BSA1 was used and in-cubated for 1 hour at room temperature in the dark Afteraspiration cells were washed with DMEM-HEPES (100200μL) and once again with PBS (100200 μL) A secondary goatanti-mouse antibody (100200 μL) coupled to a fluoro-chrome (Alexa Fluor 555 ThermoFisher Scientific WalthamMA) diluted 11000 in DMEM-HEPES-NGS5-BSA1was added and then incubated for 1 hour at room temperaturein the dark After aspiration cells were washed with DMEM-HEPES (100200 μL) and with PBS (100200 μL) In ad-dition titration of IgG1 and IgG4 subclasses in serum andCSF was performed only in the double-positive samples anddetermined as the lowest dilution with positive signal by CBAAll the CBAs were read using a Zeiss Axiophot microscope(Zeiss Oberkochen Germany)
To validate the specificity of the secondary antibodies used forIgG isotyping a Western blot was performed with 1 μg ofevery purified IgG subclass (IgG1 HCA192 IgG2 HCA193IgG3 HCA194 IgG4 HCA195 Bio-Rad) load on each wellAfter migration transfer and saturation membranes wereseparately incubated with each anti-human IgG subtype (11000 dilution for anti-IgG1 and 3 1500 for anti-IgG2 and 4antibodies) Revelation was performed with goat anti-mouseIgG (120000 115-036-003 Jackson ImmunoResearchSuffolk United Kingdom)
HLA AnalysisHLA genotyping was performed in patients with availableDNA using next-generation sequencing on a MiSeq se-quencer system (Illumina San Diego CA) and is reported at a4-digit level resolution Controls (courtesy of EFS Auvergne-Rhone-Alpes) were 300 healthy subjects of Caucasian ethnicorigin genotyped for HLA A B C DR and DQ previouslyobtained using next-generation sequencing technology(Omixon Budapest Hungary)
Statistical AnalysisAn exploratory approach16 using χ2 and Fisher exact tests forcategorical variables and the Wilcoxon signed-rank test forquantitative data was used to compare patients according toCSF positivity for LGI1-Abs DRB10701 carrier status orIgG isotypes
To search for factors associated with good (defined as lastmRs le2) or poor prognosis (mRs gt2) a 2-step approach wasused first a univariate binary logistic regression (with con-tinuous variables categorized) and second a multivariateanalysis using a generalized linear mixed model for binarydistribution (SAS Glimmix procedure) This mixed modelassessed repeated measures of mRS for each patient we
declared the patient as random effect and the remaining factorsas fixed effect The dependent variable was goodpoor prog-nosis as defined above and the choice of independent variablesincluded was based on clinical criteria the demographic (agesex) and main clinical (amnesia faciobrachial dystonic seizures[FBDSs] other seizures psychiatric symptoms and frontalsyndrome) characteristics that are present at disease onsetCSF positivity for LGI1-Abs as a biomarker (HLA was ex-cluded due to the small sample size compared with the overallcohort) and diagnostic delay length of follow-up and treat-ment as possible confounder factors The probability to switchfrom good to poor outcome was modeled Statistical analyseswere conducted using SAS software version 94 (SAS InstituteCary NC) All p values were 2 tailed and p values lt005 wereconsidered statistically significant
Differences in HLA carrier frequencies between patients andcontrols were analyzed using the 2-tailed Fishers exact tests(SPSS software package version 250 IBM Corp ArmonkNY) Allele frequency comparisons were Bonferroni cor-rected using the number of alleles for each locus corrected p lt005 values were considered significant
Standard Protocol Approvals Registrationsand Patient ConsentsWritten informed consent was obtained from all patients forthe storage and use of biological samples and clinical in-formation for research purposes The Institutional ReviewBoard of the Universite Claude Bernard Lyon 1 and HospicesCivils de Lyon approved the study (ICARE NCT-04106596)
Data AvailabilityAny data not published within the article are available and willbe shared by request from any qualified investigator
ResultsCharacteristics of Patients According to LGI1-Ab CSF PositivityA total of 142 patients with LE and serum LGI1-Abs wereidentified Eight (8142 6) patients were excluded eitherbecause clinical data were lacking or because LGI1-Abs werenot assayed in CSF Among the remaining 134 patients positivefor LGI1-Abs in serum 105 (78) were also CSF positiveTwenty-nine (22) patients were considered to be CSF neg-ative 23 (79) were negative for both IHF and CBA 5 (17)were positive for IHF but negative for CBA and 1 subject (3)was negative for only CBA No significant difference in sex ageand clinical presentation was observed between the 2 groupsDiagnostic delay was longer in the CSF-negative (median 158days interquartile range [IQR] 61ndash295) vs the CSF-positive(median 98 days IQR 42ndash161 p = 001) group Patients withpositive CSF had more frequently hyponatremia (6110558 vs 1029 35 p = 002) inflammatory CSF findings(5899 59 vs 925 36 p = 004) and abnormal MRIs(72102 71 vs 1329 45 p = 001 table 1)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 3
Serum levels were determined by ELISA-CBA in 60 patientswith available samples 48 of these patients (80) had LGI1-Abs in both serum and CSF while 12 (20) had LGI1-Absonly in the serum No significant difference in serum levelswas found between CSF-positive and CSF-negative patients(p = 091 figure 1A)
HLA Association in Anti-LGI1 EncephalitisDNA was available in 72134 (54) patients 6872 (94) ofwhom were of Caucasian origin DRB10701 was carried by6372 (88) patients this was significantly more frequentthan in the control group (86300 29 corrected p lt 00001OR = 1742 95 CI 829ndash3658) Several alleles in linkage
disequilibrium with DRB10701 were also found more com-monly in patients A3001 (1072 14 vs 7300 2 in thecontrol group corrected p = 0009 OR = 675 95 CI247ndash1842) C0602 (2572 35 vs 36300 12 in thecontrol group corrected p lt 0001 OR = 390 95 CI215ndash709) and DQB10202 (5372 74 vs 78300 26 inthe control group corrected p lt 00001 OR = 794 95 CI443ndash1424) Another DRB1 allele DRB10402 was also sig-nificantly more frequent among patients (972 13) com-pared with controls (7300 2 corrected p = 003 OR = 5995 CI 22ndash167) however 79 (78) DRB10402 carrierswere also DRB10701 carriers Four alleles were found to besignificantly more common in controls than in patients but this
Table 1 Characteristics of the Patients According to LGI1-Ab CSF Positivity
Overall cohort (n = 134) Positive CSF (n = 105) Negative CSF (n = 29) p Valuea
Men n () 84 (63) 68 (65) 16 (55) 034
Median age y (IQR range) 67 (58ndash74 21ndash86) 66 (58ndash74 21ndash85) 68 (56ndash74 37ndash86) 061
Diagnostic delay d median (IQR range) 118 (46ndash182 4ndash854) 98 (42ndash161 4ndash854) 158 (61ndash295 31ndash545) 001
mRS score at onset gt2 n () 99 (74) 83 (79) 16 (55) 008
First symptom n () 042
Amnesia 48 (36) 38 (36) 10 (35)
Other seizures 38 (28) 31 (30) 7 (24)
FBDS 32 (24) 22 (21) 10 (35)
Psychiatric symptoms 16 (12) 14 (13) 2 (7)
Disease course n ()
Amnesia 116 (87) 92 (88) 24 (83) 049
Other seizures 98 (73) 81 (77) 17 (59) 011
FBDS 71 (53) 53 (51) 18 (62) 026
Psychiatric symptoms 83 (62) 67 (64) 16 (55) 039
Frontal syndrome 64 (48) 50 (48) 14 (48) 1
Sleep disorders 48 (36) 39 (37) 9 (31) 054
Apraxia 17 (13) 12 (11) 5 (17) 052
Aphasia 11 (8) 6 (6) 5 (17) 005
Dysautonomia 6 (5) 5 (5) 1 (4) 076
ICU admission n () 12 (9) 9 (9) 3 (10) 076
Status epilepticus n () 10 (8) 8 (8) 2 (7) 089
Hyponatremia n () 71 (53) 61 (58) 10 (35) 002
MRI (N = 131) MTL hyperintensity n () 85 (65) 72 (71) 13 (45) 001
Inflammatory CSF (N = 124) n () 67 (54) 58 (59) 9 (36) 004
Cancer n () 6 (5)b 5 (5) 1 (4) 076
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LE = limbic encephalitis LGI1 = leucine-rich glioma-inactivated 1 MTL = medial temporal lobea CSF positive vs CSF negativeb Includedmalignant thymoma (n = 2 diagnosed 91 and 6months before LE) lung adenocarcinoma (n = 1 4months after LE) kidney (n = 1 4months before)hepatic (n = 1 9 months after) and prostate (n = 1 2 months after) cancers
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
finding was likely a consequence of an overrepresentation ofDRB10701 and its linked alleles in the patients group (tablee-2 linkslwwcomNXIA430)
Clinical Characteristics Per DRB10701 StatusThe non-DRB10701 carriers were more frequently women(79 78 vs 1763 27 ofDRB10701 carriers p= 0005) andyounger (median age 46 years IQR 37ndash59 vs 66 IQR 58ndash74 for
DRB10701 carriers p = 0001) Only 3 patients with an asso-ciated cancer were analyzed for HLA genotyping 2 of them (witha kidney and a hepatic cancer)wereDRB10701 carriers whereas1 with a malignant thymoma was not There was no significantdifference according to HLA status for most of the variables an-alyzed however noncarriers presented less frequently with psy-chiatric symptoms (29 22 vs 4263 67 p = 0001) andfrontal syndrome (09 vs 3263 51 p = 0004 table 2)
Figure 1 Immunologic Characteristics of Anti-LGI1 Encephalitis
(A) Box plot showing LGI1-Abs serumlevels according to CSF positivity Nosignificant difference in serum levelsrepresented as Delta OD measuredby ELISA-CBA was found betweenCSF-positive (medianDelta OD= 037IQR 029ndash044) and CSF-negative(median Delta OD = 037 IQR019ndash048) patients (p = 091) Controlsera from patients without LGI1-Abswere used for technical validation (B)Venn diagram showing serum IgGisotypesmost sera (6089 67)werepositive for both IgG1 and IgG4 (C)Box plot representing IgG14 serumtiters IgG4 titers were higher thanIgG1 titers in 59 double-positivesamples analyzed (D) Venn diagramshowing CSF IgG isotypes IgG4 wasthe most detected isotype (374093) but 21 samples were also pos-itive for IgG1 (E) Box plot represent-ing IgG14 CSF titers IgG4 titers werehigher than IgG1 titers in the 29double-positive samples analyzedCBA = cell-based assay IQR = inter-quartile range LGI1-Abs = antibodiesagainst leucine-rich glioma-inacti-vated 1 protein OD = optic density
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 5
IgG Isotyping in Serum and CSFIgG isotypes were determined in 89 sera and 40 CSF 38samples were pairs (91 patients in total) Twenty sera (208923) with negative CSF for LGI1-Abs could not be isotyped inCSF due to nondetectable Abs HLA status was known for 6891 (75) patients and 6068 (88)wereDRB10701 carriers
The main serum isotypes detected were IgG1 (7789 87)and IgG4 (7289 81 figure 1B) However IgG4 titers weresignificantly higher (median 11280 IQR 11280ndash15120)than IgG1 titers (median 1640 IQR 1320ndash11280 p =00001) in 59 double-positive samples analyzed (figure 1C)In the CSF IgG4 (3740 93) was the most frequent iso-type followed by IgG1 (2440 60 figure 1D) When 21double-positive CSF samples were analyzed IgG4 titers were
significantly higher (median 180 IQR 140ndash1120) thanthose of IgG1 (median 140 IQR 115ndash180 p = 0008figure 1E)
There was no significant difference in serum isotypes orIgG14 titers according to CSF positivity nor in serum or CSFisotypes and IgG14 titers according to DRB10701 carrierstatus in addition there was no significant difference inclinical and paraclinical features according to the presenceabsence of IgG14 in serumCSF (data not shown)
The validating Western blot performed showed high speci-ficity for the anti-IgG1 anti-IgG3 and IgG4 used whereasanti-IgG2 presented slight cross-reactivity with all other IgGisotypes (data not shown)
Table 2 Characteristics of DRB10701 Carriers Compared With Noncarriers
DRB10701 carriers (n = 63) Noncarriers (n = 9) p Value
Men n () 46 (73) 2 (22) 0005
Median age y (IQR range) 66 (58ndash74 26ndash86) 46 (37ndash59 21ndash73) 0001
Diagnostic delay d median (IQR range) 41 (25ndash181 7ndash854) 121 (51ndash212 6ndash348) 027
First symptom n () 035
Amnesia 21 (33) 2 (22)
Other seizures 20 (32) 4 (44)
FBDS 11 (18) 3 (33)
Psychiatric symptoms 11 (18) 0 (0)
Disease course n ()
Amnesia 53 (84) 7 (78) 063
Other seizures 50 (79) 8 (89) 022
FBDS 34 (54) 4 (44) 072
Psychiatric symptoms 42 (67) 2 (22) 0001
Frontal syndrome 32 (51) 0 (0) 0004
Sleep disorders 24 (38) 4 (44) 072
Apraxia 9 (14) 1 (11) 1
Aphasia 6 (10) 0 (0) 1
Dysautonomia 3 (5) 1 (11) 042
ICU admission n () 5 (8) 0 (0) 038
Status epilepticus n () 1 (2) 2 (7) 070
Hyponatremia n () 36 (57) 4 (44) 049
MRI (N = 71) MTL hyperintensity n () 38 (61) 7 (78) 047
Inflammatory CSF (N = 67) n () 36 (62) 3 (33) 014
LGI-Abs in CSF n () 48 (76) 6 (67) 068
Cancer n () 2 (3) 1 (11) 033
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LGI1 = leucine-rich glioma-inactivated1 MTL = medial temporal lobe
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

anti-human IgG2 clone G18-21 [RUO] BD Biosciences SanJose CA) IgG3 (mouse anti-human IgG3 Bio-RAD) orIgG4 (purified mouse anti-human IgG4 clone G17-4 [RUO]BD Biosciences) Either 100 or 200 μL (according to whether96 or 24-well plate were used) of the IgG solution of interest(diluted 11000 for IgG1 and IgG3 and 1500 for IgG2 andIgG4) in DMEM-HEPES-NGS5-BSA1 was used and in-cubated for 1 hour at room temperature in the dark Afteraspiration cells were washed with DMEM-HEPES (100200μL) and once again with PBS (100200 μL) A secondary goatanti-mouse antibody (100200 μL) coupled to a fluoro-chrome (Alexa Fluor 555 ThermoFisher Scientific WalthamMA) diluted 11000 in DMEM-HEPES-NGS5-BSA1was added and then incubated for 1 hour at room temperaturein the dark After aspiration cells were washed with DMEM-HEPES (100200 μL) and with PBS (100200 μL) In ad-dition titration of IgG1 and IgG4 subclasses in serum andCSF was performed only in the double-positive samples anddetermined as the lowest dilution with positive signal by CBAAll the CBAs were read using a Zeiss Axiophot microscope(Zeiss Oberkochen Germany)
To validate the specificity of the secondary antibodies used forIgG isotyping a Western blot was performed with 1 μg ofevery purified IgG subclass (IgG1 HCA192 IgG2 HCA193IgG3 HCA194 IgG4 HCA195 Bio-Rad) load on each wellAfter migration transfer and saturation membranes wereseparately incubated with each anti-human IgG subtype (11000 dilution for anti-IgG1 and 3 1500 for anti-IgG2 and 4antibodies) Revelation was performed with goat anti-mouseIgG (120000 115-036-003 Jackson ImmunoResearchSuffolk United Kingdom)
HLA AnalysisHLA genotyping was performed in patients with availableDNA using next-generation sequencing on a MiSeq se-quencer system (Illumina San Diego CA) and is reported at a4-digit level resolution Controls (courtesy of EFS Auvergne-Rhone-Alpes) were 300 healthy subjects of Caucasian ethnicorigin genotyped for HLA A B C DR and DQ previouslyobtained using next-generation sequencing technology(Omixon Budapest Hungary)
Statistical AnalysisAn exploratory approach16 using χ2 and Fisher exact tests forcategorical variables and the Wilcoxon signed-rank test forquantitative data was used to compare patients according toCSF positivity for LGI1-Abs DRB10701 carrier status orIgG isotypes
To search for factors associated with good (defined as lastmRs le2) or poor prognosis (mRs gt2) a 2-step approach wasused first a univariate binary logistic regression (with con-tinuous variables categorized) and second a multivariateanalysis using a generalized linear mixed model for binarydistribution (SAS Glimmix procedure) This mixed modelassessed repeated measures of mRS for each patient we
declared the patient as random effect and the remaining factorsas fixed effect The dependent variable was goodpoor prog-nosis as defined above and the choice of independent variablesincluded was based on clinical criteria the demographic (agesex) and main clinical (amnesia faciobrachial dystonic seizures[FBDSs] other seizures psychiatric symptoms and frontalsyndrome) characteristics that are present at disease onsetCSF positivity for LGI1-Abs as a biomarker (HLA was ex-cluded due to the small sample size compared with the overallcohort) and diagnostic delay length of follow-up and treat-ment as possible confounder factors The probability to switchfrom good to poor outcome was modeled Statistical analyseswere conducted using SAS software version 94 (SAS InstituteCary NC) All p values were 2 tailed and p values lt005 wereconsidered statistically significant
Differences in HLA carrier frequencies between patients andcontrols were analyzed using the 2-tailed Fishers exact tests(SPSS software package version 250 IBM Corp ArmonkNY) Allele frequency comparisons were Bonferroni cor-rected using the number of alleles for each locus corrected p lt005 values were considered significant
Standard Protocol Approvals Registrationsand Patient ConsentsWritten informed consent was obtained from all patients forthe storage and use of biological samples and clinical in-formation for research purposes The Institutional ReviewBoard of the Universite Claude Bernard Lyon 1 and HospicesCivils de Lyon approved the study (ICARE NCT-04106596)
Data AvailabilityAny data not published within the article are available and willbe shared by request from any qualified investigator
ResultsCharacteristics of Patients According to LGI1-Ab CSF PositivityA total of 142 patients with LE and serum LGI1-Abs wereidentified Eight (8142 6) patients were excluded eitherbecause clinical data were lacking or because LGI1-Abs werenot assayed in CSF Among the remaining 134 patients positivefor LGI1-Abs in serum 105 (78) were also CSF positiveTwenty-nine (22) patients were considered to be CSF neg-ative 23 (79) were negative for both IHF and CBA 5 (17)were positive for IHF but negative for CBA and 1 subject (3)was negative for only CBA No significant difference in sex ageand clinical presentation was observed between the 2 groupsDiagnostic delay was longer in the CSF-negative (median 158days interquartile range [IQR] 61ndash295) vs the CSF-positive(median 98 days IQR 42ndash161 p = 001) group Patients withpositive CSF had more frequently hyponatremia (6110558 vs 1029 35 p = 002) inflammatory CSF findings(5899 59 vs 925 36 p = 004) and abnormal MRIs(72102 71 vs 1329 45 p = 001 table 1)
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 3
Serum levels were determined by ELISA-CBA in 60 patientswith available samples 48 of these patients (80) had LGI1-Abs in both serum and CSF while 12 (20) had LGI1-Absonly in the serum No significant difference in serum levelswas found between CSF-positive and CSF-negative patients(p = 091 figure 1A)
HLA Association in Anti-LGI1 EncephalitisDNA was available in 72134 (54) patients 6872 (94) ofwhom were of Caucasian origin DRB10701 was carried by6372 (88) patients this was significantly more frequentthan in the control group (86300 29 corrected p lt 00001OR = 1742 95 CI 829ndash3658) Several alleles in linkage
disequilibrium with DRB10701 were also found more com-monly in patients A3001 (1072 14 vs 7300 2 in thecontrol group corrected p = 0009 OR = 675 95 CI247ndash1842) C0602 (2572 35 vs 36300 12 in thecontrol group corrected p lt 0001 OR = 390 95 CI215ndash709) and DQB10202 (5372 74 vs 78300 26 inthe control group corrected p lt 00001 OR = 794 95 CI443ndash1424) Another DRB1 allele DRB10402 was also sig-nificantly more frequent among patients (972 13) com-pared with controls (7300 2 corrected p = 003 OR = 5995 CI 22ndash167) however 79 (78) DRB10402 carrierswere also DRB10701 carriers Four alleles were found to besignificantly more common in controls than in patients but this
Table 1 Characteristics of the Patients According to LGI1-Ab CSF Positivity
Overall cohort (n = 134) Positive CSF (n = 105) Negative CSF (n = 29) p Valuea
Men n () 84 (63) 68 (65) 16 (55) 034
Median age y (IQR range) 67 (58ndash74 21ndash86) 66 (58ndash74 21ndash85) 68 (56ndash74 37ndash86) 061
Diagnostic delay d median (IQR range) 118 (46ndash182 4ndash854) 98 (42ndash161 4ndash854) 158 (61ndash295 31ndash545) 001
mRS score at onset gt2 n () 99 (74) 83 (79) 16 (55) 008
First symptom n () 042
Amnesia 48 (36) 38 (36) 10 (35)
Other seizures 38 (28) 31 (30) 7 (24)
FBDS 32 (24) 22 (21) 10 (35)
Psychiatric symptoms 16 (12) 14 (13) 2 (7)
Disease course n ()
Amnesia 116 (87) 92 (88) 24 (83) 049
Other seizures 98 (73) 81 (77) 17 (59) 011
FBDS 71 (53) 53 (51) 18 (62) 026
Psychiatric symptoms 83 (62) 67 (64) 16 (55) 039
Frontal syndrome 64 (48) 50 (48) 14 (48) 1
Sleep disorders 48 (36) 39 (37) 9 (31) 054
Apraxia 17 (13) 12 (11) 5 (17) 052
Aphasia 11 (8) 6 (6) 5 (17) 005
Dysautonomia 6 (5) 5 (5) 1 (4) 076
ICU admission n () 12 (9) 9 (9) 3 (10) 076
Status epilepticus n () 10 (8) 8 (8) 2 (7) 089
Hyponatremia n () 71 (53) 61 (58) 10 (35) 002
MRI (N = 131) MTL hyperintensity n () 85 (65) 72 (71) 13 (45) 001
Inflammatory CSF (N = 124) n () 67 (54) 58 (59) 9 (36) 004
Cancer n () 6 (5)b 5 (5) 1 (4) 076
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LE = limbic encephalitis LGI1 = leucine-rich glioma-inactivated 1 MTL = medial temporal lobea CSF positive vs CSF negativeb Includedmalignant thymoma (n = 2 diagnosed 91 and 6months before LE) lung adenocarcinoma (n = 1 4months after LE) kidney (n = 1 4months before)hepatic (n = 1 9 months after) and prostate (n = 1 2 months after) cancers
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
finding was likely a consequence of an overrepresentation ofDRB10701 and its linked alleles in the patients group (tablee-2 linkslwwcomNXIA430)
Clinical Characteristics Per DRB10701 StatusThe non-DRB10701 carriers were more frequently women(79 78 vs 1763 27 ofDRB10701 carriers p= 0005) andyounger (median age 46 years IQR 37ndash59 vs 66 IQR 58ndash74 for
DRB10701 carriers p = 0001) Only 3 patients with an asso-ciated cancer were analyzed for HLA genotyping 2 of them (witha kidney and a hepatic cancer)wereDRB10701 carriers whereas1 with a malignant thymoma was not There was no significantdifference according to HLA status for most of the variables an-alyzed however noncarriers presented less frequently with psy-chiatric symptoms (29 22 vs 4263 67 p = 0001) andfrontal syndrome (09 vs 3263 51 p = 0004 table 2)
Figure 1 Immunologic Characteristics of Anti-LGI1 Encephalitis
(A) Box plot showing LGI1-Abs serumlevels according to CSF positivity Nosignificant difference in serum levelsrepresented as Delta OD measuredby ELISA-CBA was found betweenCSF-positive (medianDelta OD= 037IQR 029ndash044) and CSF-negative(median Delta OD = 037 IQR019ndash048) patients (p = 091) Controlsera from patients without LGI1-Abswere used for technical validation (B)Venn diagram showing serum IgGisotypesmost sera (6089 67)werepositive for both IgG1 and IgG4 (C)Box plot representing IgG14 serumtiters IgG4 titers were higher thanIgG1 titers in 59 double-positivesamples analyzed (D) Venn diagramshowing CSF IgG isotypes IgG4 wasthe most detected isotype (374093) but 21 samples were also pos-itive for IgG1 (E) Box plot represent-ing IgG14 CSF titers IgG4 titers werehigher than IgG1 titers in the 29double-positive samples analyzedCBA = cell-based assay IQR = inter-quartile range LGI1-Abs = antibodiesagainst leucine-rich glioma-inacti-vated 1 protein OD = optic density
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 5
IgG Isotyping in Serum and CSFIgG isotypes were determined in 89 sera and 40 CSF 38samples were pairs (91 patients in total) Twenty sera (208923) with negative CSF for LGI1-Abs could not be isotyped inCSF due to nondetectable Abs HLA status was known for 6891 (75) patients and 6068 (88)wereDRB10701 carriers
The main serum isotypes detected were IgG1 (7789 87)and IgG4 (7289 81 figure 1B) However IgG4 titers weresignificantly higher (median 11280 IQR 11280ndash15120)than IgG1 titers (median 1640 IQR 1320ndash11280 p =00001) in 59 double-positive samples analyzed (figure 1C)In the CSF IgG4 (3740 93) was the most frequent iso-type followed by IgG1 (2440 60 figure 1D) When 21double-positive CSF samples were analyzed IgG4 titers were
significantly higher (median 180 IQR 140ndash1120) thanthose of IgG1 (median 140 IQR 115ndash180 p = 0008figure 1E)
There was no significant difference in serum isotypes orIgG14 titers according to CSF positivity nor in serum or CSFisotypes and IgG14 titers according to DRB10701 carrierstatus in addition there was no significant difference inclinical and paraclinical features according to the presenceabsence of IgG14 in serumCSF (data not shown)
The validating Western blot performed showed high speci-ficity for the anti-IgG1 anti-IgG3 and IgG4 used whereasanti-IgG2 presented slight cross-reactivity with all other IgGisotypes (data not shown)
Table 2 Characteristics of DRB10701 Carriers Compared With Noncarriers
DRB10701 carriers (n = 63) Noncarriers (n = 9) p Value
Men n () 46 (73) 2 (22) 0005
Median age y (IQR range) 66 (58ndash74 26ndash86) 46 (37ndash59 21ndash73) 0001
Diagnostic delay d median (IQR range) 41 (25ndash181 7ndash854) 121 (51ndash212 6ndash348) 027
First symptom n () 035
Amnesia 21 (33) 2 (22)
Other seizures 20 (32) 4 (44)
FBDS 11 (18) 3 (33)
Psychiatric symptoms 11 (18) 0 (0)
Disease course n ()
Amnesia 53 (84) 7 (78) 063
Other seizures 50 (79) 8 (89) 022
FBDS 34 (54) 4 (44) 072
Psychiatric symptoms 42 (67) 2 (22) 0001
Frontal syndrome 32 (51) 0 (0) 0004
Sleep disorders 24 (38) 4 (44) 072
Apraxia 9 (14) 1 (11) 1
Aphasia 6 (10) 0 (0) 1
Dysautonomia 3 (5) 1 (11) 042
ICU admission n () 5 (8) 0 (0) 038
Status epilepticus n () 1 (2) 2 (7) 070
Hyponatremia n () 36 (57) 4 (44) 049
MRI (N = 71) MTL hyperintensity n () 38 (61) 7 (78) 047
Inflammatory CSF (N = 67) n () 36 (62) 3 (33) 014
LGI-Abs in CSF n () 48 (76) 6 (67) 068
Cancer n () 2 (3) 1 (11) 033
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LGI1 = leucine-rich glioma-inactivated1 MTL = medial temporal lobe
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
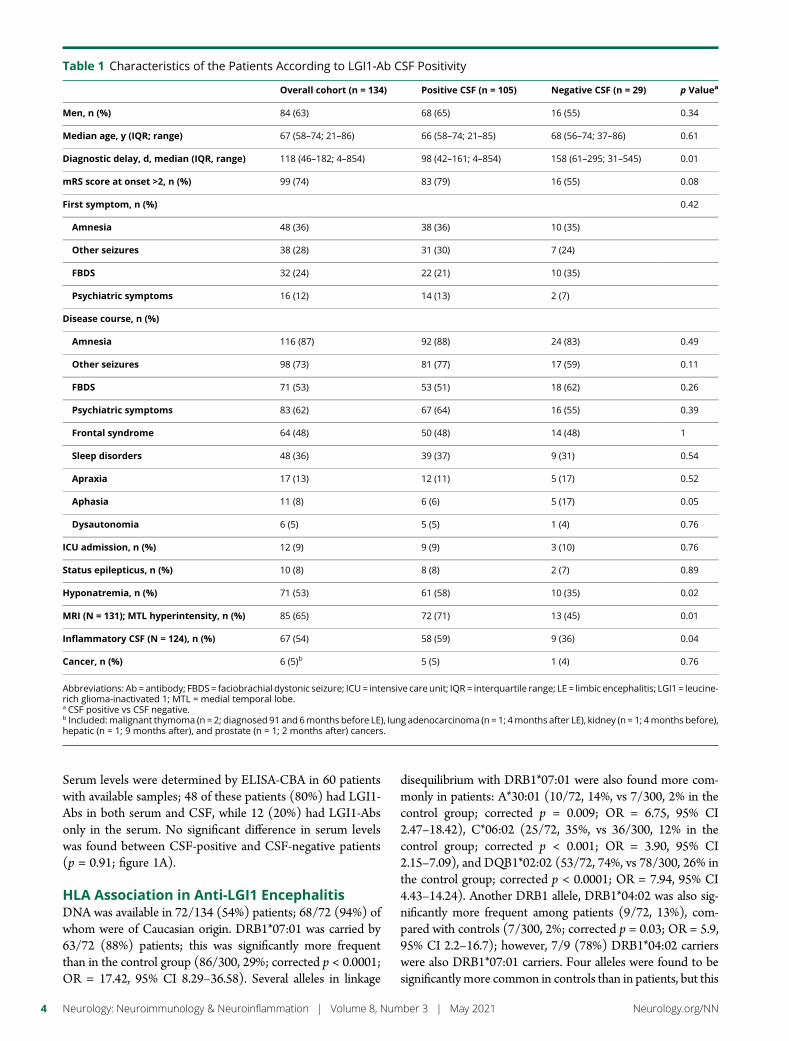
Serum levels were determined by ELISA-CBA in 60 patientswith available samples 48 of these patients (80) had LGI1-Abs in both serum and CSF while 12 (20) had LGI1-Absonly in the serum No significant difference in serum levelswas found between CSF-positive and CSF-negative patients(p = 091 figure 1A)
HLA Association in Anti-LGI1 EncephalitisDNA was available in 72134 (54) patients 6872 (94) ofwhom were of Caucasian origin DRB10701 was carried by6372 (88) patients this was significantly more frequentthan in the control group (86300 29 corrected p lt 00001OR = 1742 95 CI 829ndash3658) Several alleles in linkage
disequilibrium with DRB10701 were also found more com-monly in patients A3001 (1072 14 vs 7300 2 in thecontrol group corrected p = 0009 OR = 675 95 CI247ndash1842) C0602 (2572 35 vs 36300 12 in thecontrol group corrected p lt 0001 OR = 390 95 CI215ndash709) and DQB10202 (5372 74 vs 78300 26 inthe control group corrected p lt 00001 OR = 794 95 CI443ndash1424) Another DRB1 allele DRB10402 was also sig-nificantly more frequent among patients (972 13) com-pared with controls (7300 2 corrected p = 003 OR = 5995 CI 22ndash167) however 79 (78) DRB10402 carrierswere also DRB10701 carriers Four alleles were found to besignificantly more common in controls than in patients but this
Table 1 Characteristics of the Patients According to LGI1-Ab CSF Positivity
Overall cohort (n = 134) Positive CSF (n = 105) Negative CSF (n = 29) p Valuea
Men n () 84 (63) 68 (65) 16 (55) 034
Median age y (IQR range) 67 (58ndash74 21ndash86) 66 (58ndash74 21ndash85) 68 (56ndash74 37ndash86) 061
Diagnostic delay d median (IQR range) 118 (46ndash182 4ndash854) 98 (42ndash161 4ndash854) 158 (61ndash295 31ndash545) 001
mRS score at onset gt2 n () 99 (74) 83 (79) 16 (55) 008
First symptom n () 042
Amnesia 48 (36) 38 (36) 10 (35)
Other seizures 38 (28) 31 (30) 7 (24)
FBDS 32 (24) 22 (21) 10 (35)
Psychiatric symptoms 16 (12) 14 (13) 2 (7)
Disease course n ()
Amnesia 116 (87) 92 (88) 24 (83) 049
Other seizures 98 (73) 81 (77) 17 (59) 011
FBDS 71 (53) 53 (51) 18 (62) 026
Psychiatric symptoms 83 (62) 67 (64) 16 (55) 039
Frontal syndrome 64 (48) 50 (48) 14 (48) 1
Sleep disorders 48 (36) 39 (37) 9 (31) 054
Apraxia 17 (13) 12 (11) 5 (17) 052
Aphasia 11 (8) 6 (6) 5 (17) 005
Dysautonomia 6 (5) 5 (5) 1 (4) 076
ICU admission n () 12 (9) 9 (9) 3 (10) 076
Status epilepticus n () 10 (8) 8 (8) 2 (7) 089
Hyponatremia n () 71 (53) 61 (58) 10 (35) 002
MRI (N = 131) MTL hyperintensity n () 85 (65) 72 (71) 13 (45) 001
Inflammatory CSF (N = 124) n () 67 (54) 58 (59) 9 (36) 004
Cancer n () 6 (5)b 5 (5) 1 (4) 076
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LE = limbic encephalitis LGI1 = leucine-rich glioma-inactivated 1 MTL = medial temporal lobea CSF positive vs CSF negativeb Includedmalignant thymoma (n = 2 diagnosed 91 and 6months before LE) lung adenocarcinoma (n = 1 4months after LE) kidney (n = 1 4months before)hepatic (n = 1 9 months after) and prostate (n = 1 2 months after) cancers
4 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
finding was likely a consequence of an overrepresentation ofDRB10701 and its linked alleles in the patients group (tablee-2 linkslwwcomNXIA430)
Clinical Characteristics Per DRB10701 StatusThe non-DRB10701 carriers were more frequently women(79 78 vs 1763 27 ofDRB10701 carriers p= 0005) andyounger (median age 46 years IQR 37ndash59 vs 66 IQR 58ndash74 for
DRB10701 carriers p = 0001) Only 3 patients with an asso-ciated cancer were analyzed for HLA genotyping 2 of them (witha kidney and a hepatic cancer)wereDRB10701 carriers whereas1 with a malignant thymoma was not There was no significantdifference according to HLA status for most of the variables an-alyzed however noncarriers presented less frequently with psy-chiatric symptoms (29 22 vs 4263 67 p = 0001) andfrontal syndrome (09 vs 3263 51 p = 0004 table 2)
Figure 1 Immunologic Characteristics of Anti-LGI1 Encephalitis
(A) Box plot showing LGI1-Abs serumlevels according to CSF positivity Nosignificant difference in serum levelsrepresented as Delta OD measuredby ELISA-CBA was found betweenCSF-positive (medianDelta OD= 037IQR 029ndash044) and CSF-negative(median Delta OD = 037 IQR019ndash048) patients (p = 091) Controlsera from patients without LGI1-Abswere used for technical validation (B)Venn diagram showing serum IgGisotypesmost sera (6089 67)werepositive for both IgG1 and IgG4 (C)Box plot representing IgG14 serumtiters IgG4 titers were higher thanIgG1 titers in 59 double-positivesamples analyzed (D) Venn diagramshowing CSF IgG isotypes IgG4 wasthe most detected isotype (374093) but 21 samples were also pos-itive for IgG1 (E) Box plot represent-ing IgG14 CSF titers IgG4 titers werehigher than IgG1 titers in the 29double-positive samples analyzedCBA = cell-based assay IQR = inter-quartile range LGI1-Abs = antibodiesagainst leucine-rich glioma-inacti-vated 1 protein OD = optic density
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 5
IgG Isotyping in Serum and CSFIgG isotypes were determined in 89 sera and 40 CSF 38samples were pairs (91 patients in total) Twenty sera (208923) with negative CSF for LGI1-Abs could not be isotyped inCSF due to nondetectable Abs HLA status was known for 6891 (75) patients and 6068 (88)wereDRB10701 carriers
The main serum isotypes detected were IgG1 (7789 87)and IgG4 (7289 81 figure 1B) However IgG4 titers weresignificantly higher (median 11280 IQR 11280ndash15120)than IgG1 titers (median 1640 IQR 1320ndash11280 p =00001) in 59 double-positive samples analyzed (figure 1C)In the CSF IgG4 (3740 93) was the most frequent iso-type followed by IgG1 (2440 60 figure 1D) When 21double-positive CSF samples were analyzed IgG4 titers were
significantly higher (median 180 IQR 140ndash1120) thanthose of IgG1 (median 140 IQR 115ndash180 p = 0008figure 1E)
There was no significant difference in serum isotypes orIgG14 titers according to CSF positivity nor in serum or CSFisotypes and IgG14 titers according to DRB10701 carrierstatus in addition there was no significant difference inclinical and paraclinical features according to the presenceabsence of IgG14 in serumCSF (data not shown)
The validating Western blot performed showed high speci-ficity for the anti-IgG1 anti-IgG3 and IgG4 used whereasanti-IgG2 presented slight cross-reactivity with all other IgGisotypes (data not shown)
Table 2 Characteristics of DRB10701 Carriers Compared With Noncarriers
DRB10701 carriers (n = 63) Noncarriers (n = 9) p Value
Men n () 46 (73) 2 (22) 0005
Median age y (IQR range) 66 (58ndash74 26ndash86) 46 (37ndash59 21ndash73) 0001
Diagnostic delay d median (IQR range) 41 (25ndash181 7ndash854) 121 (51ndash212 6ndash348) 027
First symptom n () 035
Amnesia 21 (33) 2 (22)
Other seizures 20 (32) 4 (44)
FBDS 11 (18) 3 (33)
Psychiatric symptoms 11 (18) 0 (0)
Disease course n ()
Amnesia 53 (84) 7 (78) 063
Other seizures 50 (79) 8 (89) 022
FBDS 34 (54) 4 (44) 072
Psychiatric symptoms 42 (67) 2 (22) 0001
Frontal syndrome 32 (51) 0 (0) 0004
Sleep disorders 24 (38) 4 (44) 072
Apraxia 9 (14) 1 (11) 1
Aphasia 6 (10) 0 (0) 1
Dysautonomia 3 (5) 1 (11) 042
ICU admission n () 5 (8) 0 (0) 038
Status epilepticus n () 1 (2) 2 (7) 070
Hyponatremia n () 36 (57) 4 (44) 049
MRI (N = 71) MTL hyperintensity n () 38 (61) 7 (78) 047
Inflammatory CSF (N = 67) n () 36 (62) 3 (33) 014
LGI-Abs in CSF n () 48 (76) 6 (67) 068
Cancer n () 2 (3) 1 (11) 033
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LGI1 = leucine-rich glioma-inactivated1 MTL = medial temporal lobe
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm
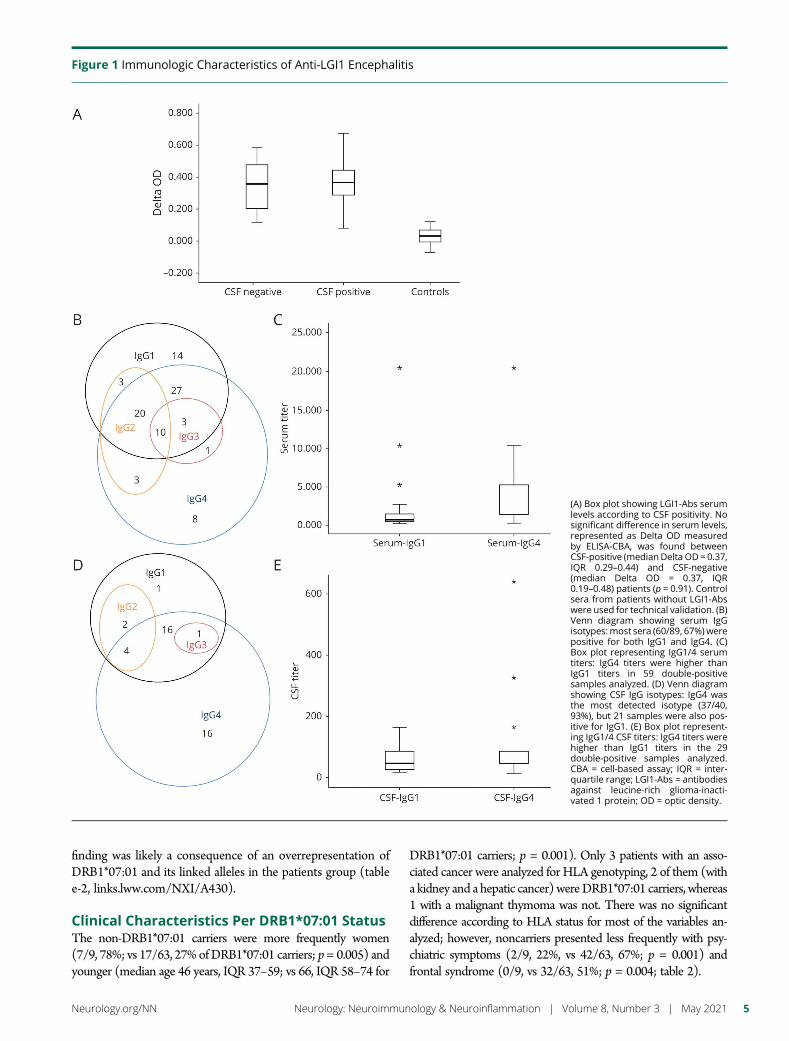
finding was likely a consequence of an overrepresentation ofDRB10701 and its linked alleles in the patients group (tablee-2 linkslwwcomNXIA430)
Clinical Characteristics Per DRB10701 StatusThe non-DRB10701 carriers were more frequently women(79 78 vs 1763 27 ofDRB10701 carriers p= 0005) andyounger (median age 46 years IQR 37ndash59 vs 66 IQR 58ndash74 for
DRB10701 carriers p = 0001) Only 3 patients with an asso-ciated cancer were analyzed for HLA genotyping 2 of them (witha kidney and a hepatic cancer)wereDRB10701 carriers whereas1 with a malignant thymoma was not There was no significantdifference according to HLA status for most of the variables an-alyzed however noncarriers presented less frequently with psy-chiatric symptoms (29 22 vs 4263 67 p = 0001) andfrontal syndrome (09 vs 3263 51 p = 0004 table 2)
Figure 1 Immunologic Characteristics of Anti-LGI1 Encephalitis
(A) Box plot showing LGI1-Abs serumlevels according to CSF positivity Nosignificant difference in serum levelsrepresented as Delta OD measuredby ELISA-CBA was found betweenCSF-positive (medianDelta OD= 037IQR 029ndash044) and CSF-negative(median Delta OD = 037 IQR019ndash048) patients (p = 091) Controlsera from patients without LGI1-Abswere used for technical validation (B)Venn diagram showing serum IgGisotypesmost sera (6089 67)werepositive for both IgG1 and IgG4 (C)Box plot representing IgG14 serumtiters IgG4 titers were higher thanIgG1 titers in 59 double-positivesamples analyzed (D) Venn diagramshowing CSF IgG isotypes IgG4 wasthe most detected isotype (374093) but 21 samples were also pos-itive for IgG1 (E) Box plot represent-ing IgG14 CSF titers IgG4 titers werehigher than IgG1 titers in the 29double-positive samples analyzedCBA = cell-based assay IQR = inter-quartile range LGI1-Abs = antibodiesagainst leucine-rich glioma-inacti-vated 1 protein OD = optic density
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 5
IgG Isotyping in Serum and CSFIgG isotypes were determined in 89 sera and 40 CSF 38samples were pairs (91 patients in total) Twenty sera (208923) with negative CSF for LGI1-Abs could not be isotyped inCSF due to nondetectable Abs HLA status was known for 6891 (75) patients and 6068 (88)wereDRB10701 carriers
The main serum isotypes detected were IgG1 (7789 87)and IgG4 (7289 81 figure 1B) However IgG4 titers weresignificantly higher (median 11280 IQR 11280ndash15120)than IgG1 titers (median 1640 IQR 1320ndash11280 p =00001) in 59 double-positive samples analyzed (figure 1C)In the CSF IgG4 (3740 93) was the most frequent iso-type followed by IgG1 (2440 60 figure 1D) When 21double-positive CSF samples were analyzed IgG4 titers were
significantly higher (median 180 IQR 140ndash1120) thanthose of IgG1 (median 140 IQR 115ndash180 p = 0008figure 1E)
There was no significant difference in serum isotypes orIgG14 titers according to CSF positivity nor in serum or CSFisotypes and IgG14 titers according to DRB10701 carrierstatus in addition there was no significant difference inclinical and paraclinical features according to the presenceabsence of IgG14 in serumCSF (data not shown)
The validating Western blot performed showed high speci-ficity for the anti-IgG1 anti-IgG3 and IgG4 used whereasanti-IgG2 presented slight cross-reactivity with all other IgGisotypes (data not shown)
Table 2 Characteristics of DRB10701 Carriers Compared With Noncarriers
DRB10701 carriers (n = 63) Noncarriers (n = 9) p Value
Men n () 46 (73) 2 (22) 0005
Median age y (IQR range) 66 (58ndash74 26ndash86) 46 (37ndash59 21ndash73) 0001
Diagnostic delay d median (IQR range) 41 (25ndash181 7ndash854) 121 (51ndash212 6ndash348) 027
First symptom n () 035
Amnesia 21 (33) 2 (22)
Other seizures 20 (32) 4 (44)
FBDS 11 (18) 3 (33)
Psychiatric symptoms 11 (18) 0 (0)
Disease course n ()
Amnesia 53 (84) 7 (78) 063
Other seizures 50 (79) 8 (89) 022
FBDS 34 (54) 4 (44) 072
Psychiatric symptoms 42 (67) 2 (22) 0001
Frontal syndrome 32 (51) 0 (0) 0004
Sleep disorders 24 (38) 4 (44) 072
Apraxia 9 (14) 1 (11) 1
Aphasia 6 (10) 0 (0) 1
Dysautonomia 3 (5) 1 (11) 042
ICU admission n () 5 (8) 0 (0) 038
Status epilepticus n () 1 (2) 2 (7) 070
Hyponatremia n () 36 (57) 4 (44) 049
MRI (N = 71) MTL hyperintensity n () 38 (61) 7 (78) 047
Inflammatory CSF (N = 67) n () 36 (62) 3 (33) 014
LGI-Abs in CSF n () 48 (76) 6 (67) 068
Cancer n () 2 (3) 1 (11) 033
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LGI1 = leucine-rich glioma-inactivated1 MTL = medial temporal lobe
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

IgG Isotyping in Serum and CSFIgG isotypes were determined in 89 sera and 40 CSF 38samples were pairs (91 patients in total) Twenty sera (208923) with negative CSF for LGI1-Abs could not be isotyped inCSF due to nondetectable Abs HLA status was known for 6891 (75) patients and 6068 (88)wereDRB10701 carriers
The main serum isotypes detected were IgG1 (7789 87)and IgG4 (7289 81 figure 1B) However IgG4 titers weresignificantly higher (median 11280 IQR 11280ndash15120)than IgG1 titers (median 1640 IQR 1320ndash11280 p =00001) in 59 double-positive samples analyzed (figure 1C)In the CSF IgG4 (3740 93) was the most frequent iso-type followed by IgG1 (2440 60 figure 1D) When 21double-positive CSF samples were analyzed IgG4 titers were
significantly higher (median 180 IQR 140ndash1120) thanthose of IgG1 (median 140 IQR 115ndash180 p = 0008figure 1E)
There was no significant difference in serum isotypes orIgG14 titers according to CSF positivity nor in serum or CSFisotypes and IgG14 titers according to DRB10701 carrierstatus in addition there was no significant difference inclinical and paraclinical features according to the presenceabsence of IgG14 in serumCSF (data not shown)
The validating Western blot performed showed high speci-ficity for the anti-IgG1 anti-IgG3 and IgG4 used whereasanti-IgG2 presented slight cross-reactivity with all other IgGisotypes (data not shown)
Table 2 Characteristics of DRB10701 Carriers Compared With Noncarriers
DRB10701 carriers (n = 63) Noncarriers (n = 9) p Value
Men n () 46 (73) 2 (22) 0005
Median age y (IQR range) 66 (58ndash74 26ndash86) 46 (37ndash59 21ndash73) 0001
Diagnostic delay d median (IQR range) 41 (25ndash181 7ndash854) 121 (51ndash212 6ndash348) 027
First symptom n () 035
Amnesia 21 (33) 2 (22)
Other seizures 20 (32) 4 (44)
FBDS 11 (18) 3 (33)
Psychiatric symptoms 11 (18) 0 (0)
Disease course n ()
Amnesia 53 (84) 7 (78) 063
Other seizures 50 (79) 8 (89) 022
FBDS 34 (54) 4 (44) 072
Psychiatric symptoms 42 (67) 2 (22) 0001
Frontal syndrome 32 (51) 0 (0) 0004
Sleep disorders 24 (38) 4 (44) 072
Apraxia 9 (14) 1 (11) 1
Aphasia 6 (10) 0 (0) 1
Dysautonomia 3 (5) 1 (11) 042
ICU admission n () 5 (8) 0 (0) 038
Status epilepticus n () 1 (2) 2 (7) 070
Hyponatremia n () 36 (57) 4 (44) 049
MRI (N = 71) MTL hyperintensity n () 38 (61) 7 (78) 047
Inflammatory CSF (N = 67) n () 36 (62) 3 (33) 014
LGI-Abs in CSF n () 48 (76) 6 (67) 068
Cancer n () 2 (3) 1 (11) 033
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure ICU = intensive care unit IQR = interquartile range LGI1 = leucine-rich glioma-inactivated1 MTL = medial temporal lobe
6 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

Treatment and PrognosisA total of 130134 (97) patients received immunotherapyamong them first-line treatments were used in all patients(130130 100) whereas second-line treatments were usedin 64130 (49) First-line treatments included corticoste-roids (109130 84) IVIG (110130 85) and plasmaexchange (8130 6) Second-line treatments were ritux-imab (4564 70) and cyclophosphamide (5064 78)Chronic immunotherapy was used in only 19 patients it waseither azathioprine (519 26) or mycophenolate (1419 74)
Median follow-up was 162 months (IQR 9ndash24 months) forthe entire cohort 18 months (IQR 9ndash36 months) for CSF-positive patients and 12 months (IQR 9ndash18 months) forCSF-negative patients At last follow-up the median mRSscore was 1 (IQR 1ndash2) for the total cohort or either of the 2
subgroups How disability (mRS) evolved over the first 12months in each subgroup and across the entire cohort isshown in figure 2 Among the 129 patients still alive at lastfollow-up the most frequent dominant sequela was memoryimpairment (78129 61) followed by psychiatric symp-toms (9129 7) other seizures (8129 6) and FBDS (3129 2) 31129 (24) patients did not report any sequela
Univariate analysis only identified 3 factors associated withpoor prognosis increasing age (p = 003) higher mRS atonset (p lt 0001) and status epilepticus (p = 002 table e-3linkslwwcomNXIA430) Multivariate analysis was basedon the variables described in the Methods section althoughonly second-line treatment was included as all treated patientsreceived first-line medications Multivariate analysis identifiedincreasing age (for an increase of 1 additional year OR = 10595 CI 102ndash107) female sex (OR = 259 95 CI
Figure 2 Evolution of Disability (mRS) With Long-term Follow-up
Data shown only for the first 12months of follow-up for the overall cohort (A n = 134) and for patients with CSF-positive (B n = 105) or CSF-negative (C n = 29)for LGI1-Abs Within every figure abscissa axis indicates for each month the number of patients with available data whereas ordinate axis represents thepercentage of patients with a certain mRS score LGI1-Abs = antibodies against leucine-rich glioma-inactivated 1 protein M =month mRS =modified RankinScale
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 7
158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

158ndash425) amnesia (OR = 331 95 CI 133ndash822) otherseizures (OR = 200 95 CI 106ndash379) and CSF-positivity(OR = 201 95 CI 103ndash391) as factors associated withpoor prognosis when a 12-month cutoff was applied onlyincreasing age (for an increase of 1 additional year OR = 10495 CI 102ndash107) female sex (OR = 227 95 CI130ndash398) and amnesia (OR = 355 95 CI 136ndash926)remained (table 3)
DiscussionThe absence of detectable Abs or of any overt inflammatoryabnormalities in the CSF of some patients with anti-LGI1 LEhas raised the question of how these cases could have signif-icant CNS pathology In addition it was unclear whetherthese patients were phenotypically or immunologically dif-ferent Herein we found no significant difference in clinicalpresentation between LGI1-Abs CSF-positive and -negativepatients Nevertheless patients with detectable LGI1-Abs inthe CSF had more frequently an inflammatory CSF hypo-natremia and MRI abnormalities suggesting a more intenseimmune response
Immunologic differences found in patients with LE with andwithout LGI1-Abs in the CSF seem to be more quantitativethan qualitative Recently LGI1-Abs producing B cells werefound in the CSF from patients without LGI1-Abs or otherabnormalities in the CSF demonstrating that even in thesepatients there is an intrathecal synthesis although it may benot strong enough to be detected by current techniques17 Inaddition we demonstrated herein that serum levels were notsignificantly different between patients with and without
LGI1-Abs in the CSF supporting the intrathecal origin ofCSF LGI1-Abs and arguing against a simple passive transferfrom the serum This is further reinforced by the recent reportof B-cell maturation occurring at least partially inside theCNS18
Previous studies have reported that LGI1-Abs were mainly ofIgG4 isotype1319ndash21 In the current series we confirmed thispredominance in both serum and CSF but we also found thatco-occurrence of other isotypes including IgG1 though atlower titers is very common The detection of IgG1 which incontrast to IgG4 can activate the complement and thereforecould produce irreversible structural damages has been pre-viously associated with poor prognosis and cognitive se-quelae20 although we and others did not find any associationbetween isotypes and outcome1521 We have also shown thatthe serum isotypes or IgG14 titers did not differ significantlybetween LGI1-Abs CSF-positive and -negative LE reinforc-ing the hypothesis of a similar autoimmune response in these2 subgroups that is only distinguishable by the amount ofLGI1-Abs intrathecally synthetized
Neurologic autoimmune diseases mediated by IgG4-Abs arestrongly associated with particular HLA class II haplotypes22
The present study confirms previous reports8911 indicatingthat DRB10701 is carried by nearly 90 of patients withLGI1-Abs LE Of interest we also found that DRB10701noncarriers were younger and more frequently women Re-cently a Chinese study reported lack of DRB10701 asso-ciation however more than 60 of their patients werewomen and the median age was nearly 40 years23 whichcould therefore support our results A higher frequency of theunusual sex and atypical age at onset among the noncarriers of
Table 3 Multivariate Analysis of Factors Associated With Poor Prognosis
Complete follow-up 12 mo follow-up
OR (95 CI) p Value OR (95 CI) p Value
Age (increase of 1 y) 105 (102ndash107) lt00001 104 (102ndash107) 00008
Female sex 259 (158ndash425) lt0001 227 (130ndash398) 0004
Diagnostic delay (increase of 1 d) 100 (099ndash100) 096 100 (099ndash100) 093
Length of follow-up (increase of 1 mo) 099 (097ndash101) 040 101 (099ndash104) 038
Amnesia 331 (133ndash822) 001 355 (136ndash926) 0009
Other seizures 200 (106ndash379) 003 192 (094ndash391) 007
FBDS 124 (076ndash204) 041 131 (076ndash228) 034
Psychiatric symptoms 139 (082ndash239) 022 134 (074ndash242) 033
Frontal syndrome 127 (078ndash206) 033 128 (074ndash219) 037
Second-line treatment 155 (078ndash206) 007 150 (088ndash256) 013
CSF LGI1-Abs 201 (103ndash391) 003 198 (095ndash409) 006
Abbreviations Ab = antibody FBDS = faciobrachial dystonic seizure LGI1 = leucine-rich glioma-inactivated 1
8 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

the associated HLA haplotype has been described in other au-toimmune diseases such as MS or ankylosing spondylitis2425
Despite sex bias on immune response being well describedmost of our knowledge about this phenomenon is based on theimmune stimulating effects of estrogens explaining the femalepredominance in the majority of the autoimmune diseases26
Conversely much less is known about the influence of sexon HLA although some evidence exists that estrogens mayalter HLA expression2728 and that sex also affects how HLAmodifies T-cell receptor repertoires29 Intriguingly anti-CASPR2 (contactin-associated protein-like 2) LE is similarlyto anti-LGI1 LE more common in elderly men and stronglyassociated with a particular HLA (DRB11101)30 Thus theinteraction between sex and HLA is far from elucidated espe-cially the underlying mechanisms of sex bias in some HLA classIIndashassociated diseases
We also found herein that anti-LGI1 LE patients not car-rying DRB10701 presented less frequently with psychiatricand frontal symptoms which has not been reported inprevious studies891115 while there was no association be-tween HLA status and outcome as it has been alreadydescribed1115 In IgLON5 encephalitis another IgG4-mediated CNS disorder tightly linked to HLA clinical pre-sentation and predominant IgG subclasses were differentaccording to DRB11001 carrier status likely reflecting anheterogeneous pathogenesis31 Conversely we demon-strated herein that CSF positivity and IgG isotypes did notsignificantly differ according to DRB10701 carrier status inLGI1-Abs LE Nevertheless other immune effectors such ascytokines may vary depending on the HLA involved32
explaining the differential clinical presentation Howeverlarger cohorts are necessary to further investigate the dif-ferential characteristics of patients according to their HLA
Anti-LGI1 LE is usually a nonparaneoplastic disorder althoughtumors mainly malignant thymoma have been described in fewpatients231314 Initially a lack of HLA association in paraneo-plastic cases was suggested9 however this finding was not fur-ther confirmed in a more recent study although it did notinclude malignant thymomas but other prevalent tumors no-tably basal carcinoma11 Herein 3 patients with cancer weregenotyped and the one with malignant thymoma did not carryDRB10701 We thus hypothesize that HLA may be useful indifferentiating the truly paraneoplastic associations from othersin anti-LGI1 LE Furthermore the strong HLA association innonparaneoplastic cases and its absence in paraneoplastic onesmight suggest different pathogenic pathways as previouslyreported in Lambert-Eatonmyasthenic syndrome33 and recentlydescribed in anti-CASPR2 diseases30 Because of the scarcity oftumors in anti-LGI1 LE international collaborative studies areneeded to collect large enough series and confirm these results
The overall outcome was initially described as favorable inanti-LGI1 LE1ndash312 but subsequent studies that performeddeeper evaluations found that at least three-quarters of caseshave cognitive sequelae334 close to the current cohort
Conversely long-term epilepsy was uncommon herein whichhas been already reported and likely reflects a better responseto immunotherapy compared with memory disturbances35 Inaddition because of the heterogeneity and retrospective na-ture of most studies several variables have been inconsistentlyassociated with a poor outcome such as the extension of MRIabnormalities3436 the development of hippocampal atro-phy14 the detection of IgG1-LGI1-Abs and higher LGI1-Absserum titers20 elevated IgG index and higher LGI1-Abs CSFtiters21 and CSF positivity for LGI1-Abs in the present seriesall of them likely reflecting the intensity of the immune re-sponse against the brain leading to structural damages andpermanent deficits Herein the worse outcome associatedwith increasing age is likely the result of a decrease in cognitivereserve34 whether older patients also develop a greater neu-ronal loss measured through neurodegenerative biomarkersin CSF3738 has not been investigated yet In addition im-mune responses in women are usually stronger than those inmen26 which could explain the association between femalesex and poor outcome that we found in the current study
The benefit of first-line immunotherapy mainly corticoste-roids is proven for FBDS and has been shown to prevent thedevelopment of cognitive dysfunction when usedpromptly3413343639 In contrast the role of second-linetreatments is less clear as regimens are not uniform studiesare retrospective and they are generally used in more se-verely affected patients142134 Herein we did not find apositive effect of second-line treatment on long-term prog-nosis and we could not analyze the role of first-line treat-ment as they were used in all patients Recently the firstrandomized trial with IVIG including a small sample of anti-LGI1 LE patients reported a significant response in seizurecontrol and a trend toward a better cognitive outcome15
Thus further prospective studies with a comprehensiveevaluation of cognitive dysfunction are needed to establishthe appropriate treatment for anti-LGI1 LE
The main limitations of the present study are its retrospectivenature the heterogeneity of the duration of follow-up theadopted classification of pleocytosis and the small sample sizeof the LGI1-Abs CSF-negative and DRB10701 noncarriergroups our results should therefore be confirmed in largercohorts Another limitation is the use of mRS for disabilityassessment which is not the most accurate scale for cognitiveevaluation although it has been widely used even in other typesof autoimmune encephalitis40 It is also worth mentioning thathigher sensitivity of CSF compared with serum has been alsoreported13 whether this finding represents a technical dis-crepancy (such as samples dilution or fixation processes) or adifference in the intrathecal synthesis has not been yet clarifiedFurthermore given this fact and the longer diagnostic delayobserved herein for CSF-negative patients it is highly recom-mended to send both kinds of samples to avoid underdiagnosis
In conclusion LGI1-Abs CSF-positive and -negative patientsare clinically similar while DRB10701 status is associated
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 9
with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

with particular demographic and clinical characteristics Po-tential therapeutic interventions should be investigated inlarge prospective cohorts as long-term outcome depends on acomplex interaction of demographic and immunologicfactors
AcknowledgmentThe authors thank NeuroBioTec Hospices Civils de LyonBRC (France AC-2013-1867 NFS96-900) for banking seraand CSF samples They thank Philip Robinson for help inmanuscript preparation (Direction de la Recherche CliniqueHospices Civils de Lyon)
Study FundingThis study is supported by FRM (Fondation pour la recher-che medicale) DQ20170336751 This work has been de-veloped within the BETPSY project which is supported by apublic grant overseen by the French National ResearchAgency (ANR) as part of the second ldquoInvestissementsdrsquoAvenirrdquo program (reference ANR-18-RHUS-0012) SMuntildeiz-Castrillo is supported by a research grant fromFundacion Alfonso Martın Escudero (Spain)
DisclosureThe authors report no conflict of interest Go to NeurologyorgNN for full disclosures
Publication HistoryReceived by Neurology Neuroimmunology amp NeuroinflammationSeptember 8 2020 Accepted in final form January 4 2021
References1 Lai M Huijbers MG Lancaster E et al Investigation of LGI1 as the antigen in limbic
encephalitis previously attributed to potassium channels a case series Lancet Neurol20109776ndash785
2 Irani SR Alexander S Waters P et al Antibodies to Kv1 potassium channel-complexproteins leucine-rich glioma inactivated 1 protein and contactin-associated protein-2in limbic encephalitis Morvanrsquos syndrome and acquired neuromyotonia Brain 20101332734ndash2748
3 van Sonderen A Thijs RD Coenders EC et al Anti-LGI1 encephalitis clinicalsyndrome and long-term follow-up Neurology 2016871449ndash1456
4 Irani SR Michell AW Lang B et al Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis Ann Neurol 201169892ndash900
5 Navarro V Kas A Apartis E et al Motor cortex and hippocampus are the two maincortical targets in LGI1-antibody encephalitis Brain 20161391079ndash1093
Appendix Authors
Name Location Contribution
SergioMuntildeiz-CastrilloMD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studymajor role in acquisitionand analysis of datastatistical analysis anddrafted and revised themanuscript for intellectualcontent
JulieHaesebaertMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Major role in statisticalanalysis analyzed thedata and revised themanuscript for intellectualcontent
LaureThomas MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of dataanalyzed the data andrevised the manuscript forintellectual content
AlbertoVogrig MD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Anne-LauriePinto MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Appendix (continued)
Name Location Contribution
GeraldinePicard MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
CharlotteBlanc MSc
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
Le-Duy DoPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
BastienJoubert MDPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
GiuliaBerzero MD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
DimitriPsimarasMD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
AgustiAlentornMD PhD
Hopitaux Universitaires LaPitie Salpetriere ampUniversites SorbonnesParis France
Acquisition of data andrevised the manuscript forintellectual content
VeroniqueRogemondPhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Acquisition of data andrevised the manuscript forintellectual content
ValerieDubois MD
EFS Auvergne-Rhone-Alpes Lyon France
Acquisition of data andrevised the manuscript forintellectual content
AdityaAmbati PhD
Stanford University PaloAlto CA
Analyzed the data andrevised the manuscript forintellectual content
RyadTamouzaMD PhD
Hopitaux UniversitairesHenri Mondor amp Universitede Paris-Est-Creteil France
Acquisition of data andrevised the manuscript forintellectual content
EmmanuelMignot MDPhD
Stanford University PaloAlto CA
Analyzed the data anddrafted and revised themanuscript for intellectualcontent
JeromeHonnoratMD PhD
Hospices Civils de Lyon ampUniversite Claude BernardLyon 1 France
Designed andconceptualized the studyacquisition and analyzedthe data drafted andrevised the manuscript forintellectual content andstudy supervision
10 Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 NeurologyorgNN
6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

6 Gresa-Arribas N Titulaer MJ Torrents A et al Antibody titres at diagnosis andduring follow-up of anti-NMDA receptor encephalitis a retrospective study LancetNeurol 201413167ndash177
7 Gadoth A Pittock SJ Dubey D et al Expanded phenotypes and outcomes among 256LGI1CASPR2-IgG-positive patients LGI1CASPR2-IgG + Patients Ann Neurol20178279ndash92
8 Kim T-J Lee S-T Moon J et al Anti-LGI1 encephalitis is associated with unique HLAsubtypes HLA Subtypes in Anti-LGI1 Encephalitis Ann Neurol 201781183ndash192
9 van Sonderen A Roelen DL Stoop JA et al Anti-LGI1 encephalitis is stronglyassociated with HLA-DR7 and HLA-DRB4 anti-LGI1 Encephalitis Ann Neurol201781193ndash198
10 Mueller SH Farber A Pruss H et al Genetic predisposition in anti-LGI1 and anti-NMDA receptor encephalitis GWAS Autoimmune Encephalitis Ann Neurol 201883863ndash869
11 Binks S Varley J Lee W et al Distinct HLA associations of LGI1 and CASPR2-antibody diseases Brain 20181412263ndash2271
12 Celicanin M Blaabjerg M Maersk-Moller C et al Autoimmune encephalitis associ-ated with voltage-gated potassium channels-complex and leucine-rich glioma-inactivated 1 antibodies a national cohort study Eur J Neurol 201724999ndash1005
13 Arintildeo H Armangue T Petit-Pedrol M et al Anti-LGI1ndashassociated cognitive im-pairment presentation and long-term outcome Neurology 201687759ndash765
14 Finke C Pruss H Heine J et al Evaluation of cognitive deficits and structural hip-pocampal damage in encephalitis with leucine-rich glioma-inactivated 1 antibodiesJAMA Neurol 20177450
15 Dubey D Britton J McKeon A et al Randomized placebo-controlled trial of in-travenous immunoglobulin in autoimmune LGI1CASPR2 epilepsy Ann Neurol202087313ndash323
16 Bender R Lange S Adjusting for multiple testing when and how J Clin Epidemiol200154343ndash349
17 Kornau H-C Kreye J Stumpf A et al Human cerebrospinal fluid monoclonal LGI1autoantibodies increase neuronal excitability Ann Neurol 202087405ndash418
18 Lehmann-Horn K Irani SR Wang S et al Intrathecal B-cell activation in LGI1antibody encephalitis Neurol Neuroimmunol Neuroinflamm 20207e669
19 Irani SR Pettingill P Kleopa KA et al Morvan syndrome clinical and serologicalobservations in 29 cases Ann Neurol 201272241ndash255
20 Thompson J Bi M Murchison AG et al The importance of early immunotherapy inpatients with faciobrachial dystonic seizures Brain J Neurol 2018141348ndash356
21 Gadoth A Zekeridou A Klein CJ et al Elevated LGI1-IgG CSF index predicts worseneurological outcome Ann Clin Transl Neurol 20185646ndash650
22 Muntildeiz-Castrillo S Vogrig A Honnorat J Associations between HLA and autoim-mune neurological diseases with autoantibodies Autoimmun Highlights 2020112doi 101186s13317-019-0124-6
23 Hu F Liu X Zhang L et al Novel findings of HLA association with anti-LGI1encephalitis HLA-DRB10301 and HLA-DQB10201 J Neuroimmunol 2020344577243 doi 101016jjneuroim2020577243
24 Hensiek AE Sawcer SJ Feakes R et al HLA-DR 15 is associated with female sex andyounger age at diagnosis in multiple sclerosis J Neurol Neurosurg Psychiatry 200272184ndash187
25 Yang M Xu M Pan X et al Epidemiological comparison of clinical manifestationsaccording to HLA-B27 carrier status of Chinese ankylosing spondylitis patientsTissue Antigens 201382338ndash343
26 Klein SL Flanagan KL Sex differences in immune responses Nat Rev Immunol 201616626ndash638
27 KaurM Schmeier SMacPherson CR et al Prioritizing genes of potential relevance todiseases affected by sex hormones an example of myasthenia gravis BMC Genomics20089481
28 Taneja V Sex hormones determine immune response Front Immunol 20189193129 Schneider-Hohendorf TGorlichD Savola P et al Sex bias inMHC I-associated shaping
of the adaptive immune system Proc Natl Acad Sci USA 20181152168ndash217330 Muntildeiz-Castrillo S Joubert B Elsensohn MH et al Anti-CASPR2 clinical phenotypes
correlate with HLA and immunological features J Neurol Neurosurg Psychiatry 2020911076ndash1084
31 Gaig C Ercilla G Daura X et al HLA and microtubule-associated protein tau H1haplotype associations in anti-IgLON5 disease Neurol Neuroimmunol Neuro-inflamm 20196e605
32 Ccedilebi M Durmus H Yılmaz V et al Relation ofHLA‐DRB1 to IgG4 autoantibody andcytokine production in muscle‐specific tyrosine kinase myasthenia gravis (MuSK‐MG) Clin Exp Immunol 2019197214ndash221
33 Wirtz PW Willcox N van der Slik AR et al HLA and smoking in prediction andprognosis of small cell lung cancer in autoimmune LambertndashEaton myasthenic syn-drome J Neuroimmunol 2005159230ndash237
34 Sola-Valls N Arintildeo H Escudero D et al Telemedicine assessment of long-termcognitive and functional status in anti-leucine-rich glioma-inactivated 1 encephalitisNeurol Neuroimmunol Neuroinflamm 20207e652
35 de Bruijn MAAM van Sonderen A van Coevorden-Hameete MH et al Evaluation ofseizure treatment in anti-LGI1 anti-NMDAR and anti-GABABR encephalitisNeurology 201992e2185ndashe2196
36 Shin YW Lee ST Shin JW et al VGKC-complexLGI1-antibody encephalitis clinicalmanifestations and response to immunotherapy J Neuroimmunol 201326575ndash81
37 Constantinescu R Krysl D Andren K et al Cerebrospinal fluid markers of neuronaland glial cell damage in patients with autoimmune neurologic syndromes with andwithout underlying malignancies J Neuroimmunol 201730625ndash30
38 Kortvelyessy P Pruss H Thurner L et al Biomarkers of neurodegeneration inautoimmune-mediated encephalitis Front Neurol 20189668
39 Irani SR Stagg CJ Schott JM et al Faciobrachial dystonic seizures the influence ofimmunotherapy on seizure control and prevention of cognitive impairment in abroadening phenotype Brain 20131363151ndash3162
40 Titulaer MJ McCracken L Gabilondo I et al Treatment and prognostic factors forlong-term outcome in patients with anti-NMDA receptor encephalitis an observa-tional cohort study Lancet Neurol 201312157ndash165
NeurologyorgNN Neurology Neuroimmunology amp Neuroinflammation | Volume 8 Number 3 | May 2021 11
DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm

DOI 101212NXI000000000000097420218 Neurol Neuroimmunol Neuroinflamm
Sergio Muntildeiz-Castrillo Julie Haesebaert Laure Thomas et al Encephalitis
Clinical and Prognostic Value of Immunogenetic Characteristics in Anti-LGI1
This information is current as of March 5 2021
ServicesUpdated Information amp
httpnnneurologyorgcontent83e974fullhtmlincluding high resolution figures can be found at
References httpnnneurologyorgcontent83e974fullhtmlref-list-1
This article cites 40 articles 5 of which you can access for free at
Subspecialty Collections
httpnnneurologyorgcgicollectionprognosisPrognosis
httpnnneurologyorgcgicollectionautoimmune_diseasesAutoimmune diseases
httpnnneurologyorgcgicollectionassociation_studies_in_geneticsAssociation studies in geneticsfollowing collection(s) This article along with others on similar topics appears in the
Permissions amp Licensing
httpnnneurologyorgmiscaboutxhtmlpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnnneurologyorgmiscaddirxhtmlreprintsusInformation about ordering reprints can be found online
Academy of Neurology All rights reserved Online ISSN 2332-7812Copyright copy 2021 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the AmericanPublished since April 2014 it is an open-access online-only continuous publication journal Copyright
is an official journal of the American Academy of NeurologyNeurol Neuroimmunol Neuroinflamm