clinical anaesthesiology
DESCRIPTION
Clinical Anaesthesiology. Qiu Wei Fan Associate professor Department of Anaesthesiology Rui Jin Hospital Shanghai Second Medical University. Local Anaesthetic techniques. Features of local anaesthesia Methods of local anaesthesia Complications of local anaesthesia Regional block equipment - PowerPoint PPT PresentationTRANSCRIPT

Clinical Anaesthesiology
Qiu Wei FanAssociate professor
Department of AnaesthesiologyRui Jin Hospital
Shanghai Second Medical University

Local Anaesthetic techniques
Features of local anaesthesia Methods of local anaesthesia Complications of local
anaesthesia Regional block equipment Spinal, epidural, & caudal blocks Peripheral nerve blocks

Preoperative assessment and premedication Purpose
Establish rapport with the patient Obtain a history and perform a
physical examinations Order a special investigations Assess the risks of anaesthesia and
surgery and if necessary postpone or cancel the date of surgery
Instutite preoperative management Prescribe premedication and the
anaesthesia management
Preoperative assessment
and premedication
Routine preoperative anaesthetic evaluation
History Current problem Other known problems Medication history
Preoperative assessment and premedication Medication history
Allergies
Drug
intolerances
Present
therapy Prescription
Nonprescription
Nontherapeutic Alcohol
Tobacco
Illicit

Preoperative assessment and premedication
Previous anaesthetics, surgery, and obstetric deliverries
Family history Review of organ systems Last oral intake

Preoperative assessment and premedication Review of organ systems
General Respiratory Cardiovascular Renal Gastrointestinal Hematologic
Preoperative assessment and premedication Review of organ systems
Neurologic Endocrine Psychiatric Orthopedic Dermatologic

Preoperative assessment and premedication Physical examination
Vital signs Airway Heart Lungs Extremities Neurologic examination
Preoperative assessment and premedicationLaboratory evaluation Hematocrit or hemoglobin
concentrationAll menstruating womenAll patients over 60 years of ageAll patients who are likely to experience significant blood loss and may require transfusion
Serum glucose and creatinine (or blood urea nitrogen) concentration: all patients over 60 years of age
Electrocardiogram: all patients over 40 years of age
Chest radiogram: all patients over 60 years of age

ASA classification I A normal healthy patient other
than surgical pathology- without systemic disease.
II A patient with mild systemic disease – no functional limitations.
III A patient with moderate to severe systemic disturbance duo to medical or surgical disease- some functional limitation but not incapacitating.
ASA classification IV A patient with severe systemic
disturbance which poses a constant threat to life and is incapacitating.
V A moribund patient not expected to survive 24 hours with or without surgery.
E If the case is an emergency, the physical status is followed by the letter “E”-, “IIE”.
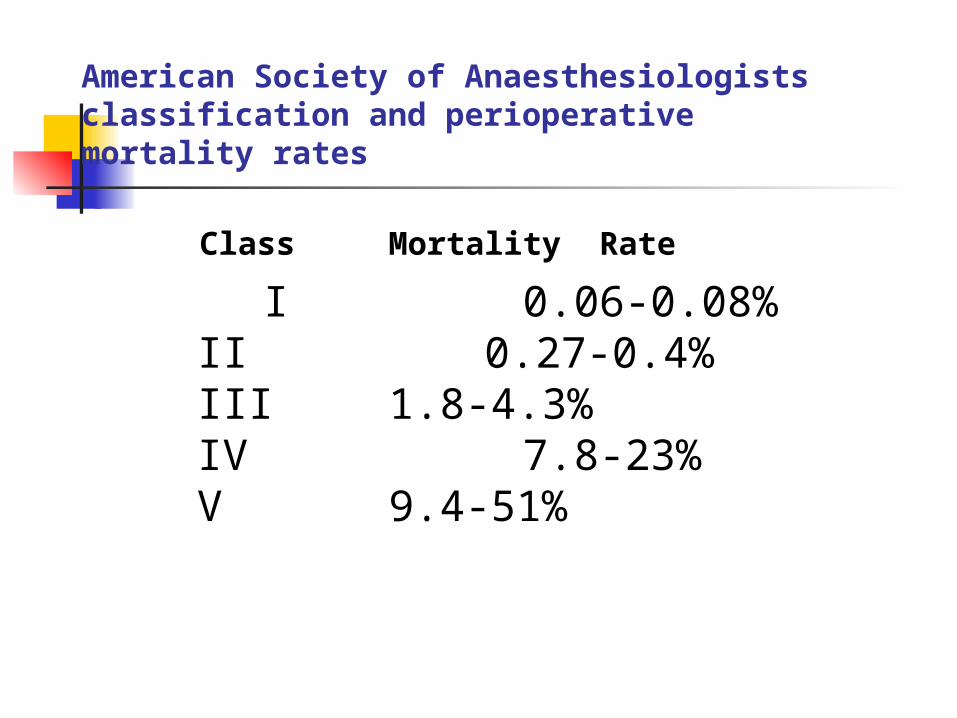
American Society of Anaesthesiologists classification and perioperative mortality rates
Class Mortality Rate I 0.06-0.08%
II 0.27-0.4%III 1.8-4.3%IV 7.8-23%V 9.4-51%

Documentation
Informed Consent The preoperative note The intraoperative
anaesthesia record The postoperative notes

Local Anaesthetic techniques Features of local anaesthesia
Preservation of consciousness The quality of early postoperative
analgesia Simplicity of administration Sympathetic blockade attenuation
of the stress response Minimal depression of ventilation
Local Anaesthetic techniques Methods of local anaesthesia
Surface anaesthesia Local infiltration Field block Regional blocks (Spinal,
epidural, & caudal blocks) Peripheral nerve blocks
Complications of local anaesthesia
Local anaesthetic toxicity( Systemic toxicity): Cardiovascular, Respiratory , Cerebral and Immunologic
Hypotension Motor blockade Pneumothorax Urinary retention Neurological complications Equipment problems
Local anaesthetic toxicity
Systemic toxicity Cardiovascular:
Cardiac dysrhythmia or circulatory collapse is often the presenting sign of local anaesthetic overdose during anaesthesia.
Local anaesthetic toxicity
Systemic toxicity Respiratory:
Lidocaine depresses hypoxic drive. Apnea can result from phrenic and intercostal nerve paralysis or depression of the medullary respiratory center.
Local anaesthetic toxicity
Systemic toxicity Cerebral:
Early symptoms are circumoral numbness, tongue paresthesia, and dizziness. Sensory complaints may include tinnitus and blurred vision.Excitatory signs often precede central nerve system depression.

Local anaesthetic toxicity
Systemic toxicity Immunologic:
True hypersensitivity reactions to local anaesthetic agents- as distinct from systemic toxicity due to excessive plasma concentration- are quite uncommon.

Regional block equipment
Spinal needles (26G) Pencil-point 24G needles Catheters Label syringes A short length of tubing Nerve stimulators Local anaesthetic drugs
Complications of local anaesthesia Hypotension
Sympathetic blockade Total spinal blockade Vasovagal attack Anaphylactoid reaction

Regional block
Subarachnoid block(SAB): Spinal anaesthesia
Extradural nerve block: Epidural anaesthesia may be performed in the sacral(caudal block), lumbar, thoracic or cervical regions.













蛛网膜下腔阻滞联合硬脊膜外腔阻滞

Regional BlockPhysiology:
Somatic BlackadeVisceral blackadeCardiovascularPulmonaryGastrointestinalLiverUrinary tractMetabolic & Endocrine

Physiology effects of SABDifferential nerve blockade
Sympathetic fibres block sensory block Motor block
Physiology effects of SABRespiratory system Roots of the phrenic nerves:
apnoea Thoracic level: loss of intercostal
muscle activity, decrease in vital capacity, reduction in cardiac output and pulmonary artery pressure, and increased ventilation/perfution imbalance, resulting in a decrease in arterial oxygen tension (PaO2)

Physiology effects of SABCardiovascular system
Denervation of the sympathetic outflow tracts (T1-L2): dilatation of resistance and capacitance vessels and results in hypotension
Bradycardia: vasovagal syndrome; block of the cardiac sympathetic fibres

Physiology effects of SABGastrointestinal system
Sympathetic denervation and unopposed parasympathetic action : a constricted gut with increased peristaltic activity (nausea, retching or vomiting)

Physiology effects of extradural block
The physiological effect of extradural blockade are similar to those following subarachnoid block.
Spinal anaesthesia :Indications Lower extremities Hip Perineum Lower abdomen Lumber spine
Type of surgery: Urology, Gynaecology, Obstetrics and any surgical procedure on the lower limbs or perineum.
Urologic endoscopic surgery, Rectal surgery, repair of hip fracture, obstetrics, orthopedic, Inguinal hernia repair, etc.

Spinal anaesthesia : Contraindications
Absolute:SepsisBacteremiaSkin infection at injection siteHypovolemiaCoagulopathyTherapeutic anticoagulationDemyelating central nerve system diseaseIncreased intracranial pressurePsychosis or dementiaLack of consent

Spinal anaesthesia : Contraindications
RelativePeripheral neuropathyMini-dose” heparinAspirin or other antiplatelet drugsPrior lumbar spine surgeryChronic back painCertain cardiac lesionsPsychologic or emotional instabilityUncooperative patients Prolonged surgerySurgery of uncertain durationSurgical team resistance to awake patients
Patient preparation Consent Physical examination Laboratory Tests Premedication

Equipment & Safety General Preparation:
Monitoring Administration of GA if
necessary Resuscitation equipment Regional equipment
Patient position Sitting position Lateral position Prone position
Technique : Needle Technique
Midline Technique Paramedian Technique
Factors influencing spinal anaesthesia
Agents: Procaine,
Tetracaine, Lidocaine,
Bupivacaine
Dosage
Vasoconstrictors
Specific Gravity:
Hyperbaric technique,
Hypobaric technique,
Isobaric technique
Posture
Intra-abdominal
Pressure
Spinal Curvature
Prior Surgery of Spine
Age
Obesity
Pregnancy
Spread of the agent
Redistribution

Spinal anaesthesia : Complications
Pain on injection Backache Headache Urinary Retention Meningitis and meningism Vascular injury Nerve injury: Cranial nerve palsy High spinal anaesthesia Transverse myelitis and cauda
equina syndrome
Epidural anaesthesia : Indications
Specific IndicationsHip and knee surgeryLow extremity RevascularizationObstetric deliveriesPostoperative management
Epidural anaesthesia :Contraindications
Epidural anaesthesia
shares the contraindications
discussed in the section on
spinal anaesthesia.
Applied Physiology for Epidural Anaesthesia
Segmental Blockade Differential Blockade

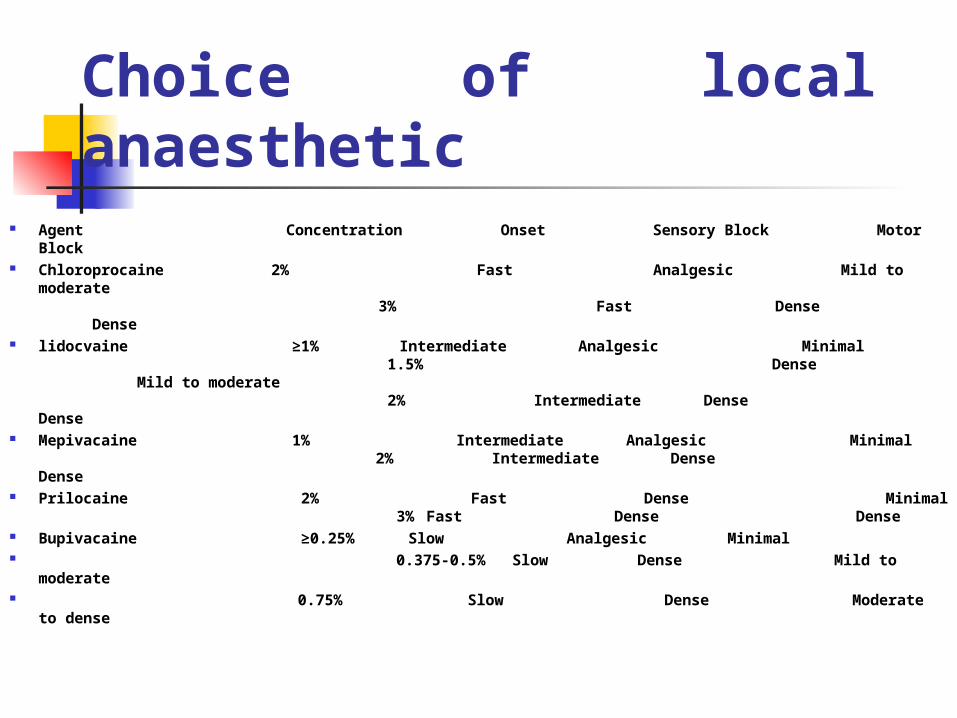
Table Agents for epidural anaesthesia
Agent Concentration Onset Sensory Block Motor Block Chloroprocaine 2% Fast Analgesic Mild to moderate
3% Fast Dense Dense lidocvaine ≥1% Intermediate Analgesic Minimal
1.5% Dense Mild to moderate 2% Intermediate Dense Dense
Mepivacaine 1% Intermediate Analgesic Minimal 2% Intermediate Dense Dense
Prilocaine 2% Fast Dense Minimal 3% Fast Dense Dense
Bupivacaine ≥0.25% Slow Analgesic Minimal 0.375-0.5% Slow Dense Mild to moderate
0.75% Slow Dense Moderate to dense

Technique of Epidural Anaesthesia
A) Safety B) Preparation of the patient
Informed consentPreoperative evaluationLaboratory assessmentPremedication
C ) Equipment: The epidural needle

Technical performance of a block
Identification of the epidural space:
Loss of resistance technique;
Hanging drop technique

Level selected Lumbar epidural anaesthesia:
Midline technique, paramedian technique
Thoracic epidural anaesthesia: Midline technique, paramedian technique
Cervical epidural anaesthesia: Midline technique
Strategies for injection of the anaesthetic agent
A test dose Incremental dosing
Choice of local anaesthetic
Agent Concentration Onset Sensory Block Motor Block
Chloroprocaine 2% Fast Analgesic Mild to moderate 3% Fast Dense Dense
lidocvaine ≥1% Intermediate Analgesic Minimal 1.5% Dense Mild to moderate 2% Intermediate Dense Dense
Mepivacaine 1% Intermediate Analgesic Minimal
2% Intermediate Dense Dense Prilocaine 2% Fast Dense Minimal
3% Fast Dense Dense Bupivacaine ≥0.25% Slow Analgesic Minimal 0.375-0.5% Slow Dense Mild to moderate 0.75% Slow Dense Moderate to dense
Factors that affect epidural anaesthesia
Dosage Patient Age Weight & Height Posture Vasoconstrictors pH adjustment of local
anaesthesia Failure of epidural block

Epidural anaesthesia Complications(Intraoperative)
Dural tap Total spinal anaesthesia Profound hypotension Apnoea Massive extradural block and
subdural block Intravenous toxitity Hypotension Shivering Nausea/ vomiting

Epidural anaesthesia Complications(Postoperative)
Headache Infection Extradural haematoma Neurological
complications
Caudal anaesthesia Indications
Obstetric patients, for vaginal deliveries
Surgery related to the sacral area (anorectal and vaginal procedures).

Caudal anaesthesia: Contraindications
The contraindications for
caudal anaesthesia are the
same as for any central block.

Caudal anaesthesia
Complications
The complications of caudal
block are essentially the same
as those associated with
epidural and spinal block.

Differences between subarachniod and extradural block
Dose of drug employed
Rate of onset
Intensity of block
Pattern of block
Subarachniod Extradural block
Small Large
Fast Slow
Complete anaesthesia Not complete
anaesthesia
Cord transection
Dermatomal
Peripheral nerve blocks
Upper limb blocks Brachial plexus block Axillary block Supraclavicular block Interscalene block
Peripheral nerve blocks
Lower limb blocks Sciatic nerve block Femoral nerve block Mid tarsal block

Question What are the complication of local
anaesthesia? What are the features of local
anaesthetic toxicity? What are the absolute
contraindications to subarachnoid block and extradural block?
Question
What are the major differences between subarachnoid block and extradural block?
How do you take the history from a patient?
What are the methods for identifying the epidural space?
Any Questions?
Thank you !