clinical advisory subcommittee of the emergency … advisory subcommittee of the emergency medical...
TRANSCRIPT

Clinical Advisory Subcommittee of the Emergency Medical Care Committee
Meeting Agenda 11:00 A.M., Tuesday May 13.2014 Health Agency Second Floor Large Conference Room 2180 Johnson Avenue San Luis Obispo Members Chair: Dr. Mark Eckert, County Medical Society Sue Fortier, RN, MICNs TBD, Fire Service Paramedics Joe Piedalue, Ambulance Paramedics Paul Quinlan, Fire Service EMTs Dr. Jana Reed, Non-Base Station ED Physicians Chad Robertson, ad hoc Dr. Joe Robinson, Base Station ED Physicians Dr. Stefan Teitge, County Medical Society
Staff STAFF LIAISON: Kathy Collins, RN, SCS Coordinator Steve Lieberman, EMS Division Director Dr. Tom Ronay, Medical Director Vicci Stone, EMS Specialist Tracy Eby, Administrative Assistant
Marigrace Waage, Ambulance EMTs TBD, Non-Base Station Hospital ED Nurses John Prickett, Lead Field Training Officer
AGENDA ITEM LEAD
Call to Order Introductions Dr. Eckert
Public Comment
Discussion Discussion on field use and need:
Dopamine – policy change to make “optional” for non-transporting ALS agencies
V-fib with ROSC to STEMI Centers -discussion
Trauma o Spinal Immobilization – draft policy o Trauma polices-
General Trauma Head/Neck/Facial Trauma Chest/Abdomen Trauma Extremity Trauma Traumatic Arrest Triage criteria (staff summary)
Saline shortage
Intranasal Narcan
Dr. Ronay- staff
Adjourn Announcements Dr. Eckert
Adjourn Declaration of Future Agenda Items
Updating/reformatting polices
Dr. Eckert
Next Meeting – May 13, 2014 11:00 a.m. – 12:30 p.m. 2
nd floor Conference Room, Health Agency

Policy No XXX
[Type text]
San Luis Obispo County
Emergency Medical Services Agency
Spinal Motion Restriction (SMR) ADULT PEDIATRIC
BLS PROCEDURES
o UNIVERSAL ALGORITHM
o Scene Safety / PPE
o ABCs
o Administer Oxygen Per Policy 580
o PURPOSE
o Full spinal immobilization/motion restriction (SMR) is to
protect the patient from further injury when an unstable
spinal fracture exists
o Routine use of full SMR should be avoided and reserved for
patients with confirmatory physical findings or high suspicion
of spinal fracture.
o Full SMR may cause airway or respiratory compromise. Lead
to skin breakdown and may cause significant pain
o INDICATIONS
o ASSOCIATED RISK FACTORS
Age > 65 years
Patients meeting STEP 3 MIO trauma criteria
Axial loading to head - i.e. diving accidents
Numbness or tingling in extremities
o FULL SMR IS NOT REQUIRED FOR:
Awake patients not under the influence of alcohol or
drugs with whom one can communicate effectively
That deny neck pain
Are neurologically intact
And do not have distracting injuries
o CONSIDER FULL SMR
BLUNT TRAUMA with any of the following
ALOC
Spinal tenderness – Mid-line for patients
<65 yrs or any neck pain for patients > 65yrs
Neurologic deficit or complaint
Anatomic deformity of the spine
SAME AS ADULT

Effective Date: November 1, 2012 Next Review Date: November 2015 ____________________________________________ Thomas Ronay, MD, EMS Medical Director
Evidence of alcohol or drugs
Distracting injury(s)
Inability to communicate
PENETRATING INJURY to head, neck or torso with:
Neurologic deficit or complaint
If in doubt “immobilize”
o SPECIAL CONSIDERATIONS
o Acute or chronic difficulty in breathing – consider elevation or
positioning patient/board
o Anatomic variations may require padding to place spine in a
neutral position
o Pediatric -
Utilize car seat if appropriate
Pad shoulders and head for anatomic alignment
o Pregnancy – tilt board to left to facilitate blood flow and aid in
respiratory comfort
Optional Scope
None
ALS Prior to Base Hospital Contact
o REMOVAL Of C-SPINE IMOBILIZATION
o My be done BY ALS for patients that have been placed in full
SMR but meet the criteria to NOT place in full SMR
SAME AS ADULT
Base Hospital Orders Only
o None
DOCUMENTATION
o Neurologic status before and after spinal immobilization
o When full SMR is NOT done and/or a paramedic removes spinal
precautions - PCR documentation must include all of the exclusion
criteria
o Awake and cooperative without influence of drugs/alcohol
o Deny neck pain
o Neurologically intact
o No distracting injuries

Effective Date: November 1, 2012 Next Review Date: November 2015 ____________________________________________ Thomas Ronay, MD, EMS Medical Director
o

Policy No XXX
San Luis Obispo County
Emergency Medical Services Agency
General Trauma ADULT PEDIATRIC
BLS PROCEDURES
o UNIVERSAL ALGORITHM
o Do not delay transport with non-essential treatment of the
non-entrapped/transport ready critical trauma patient.
o Attempt to limit on scene time to 10 min or less when Trauma
Triage Criteria are met
CONSIDERATIONS
o Assess for injuries that meet trauma triage guidelines Policy #
153
o Step 1 - Physiologic findings
Hemodynamic compromise (BP<90 mmHg)
Respiratory compromise - <10 or >29
Mental status – GCS <13 (AVPU??)
o Step 2 – Anatomic Injuries
Penetrating - number of wounds and type of
weapon
o Step 3 – Mechanism of Injury (MOI)
Vehicle collision
Estimated speed
Type of vehicle
Type of impact (i.e. head-on, roll-
over, auto-ped, etc.)
Damage (passenger space, steering
wheel, windshield, etc.)
Protective devices ( helmet, seatbelt,
airbag, child seat, etc)
Patient complaints/injuries ( seat belt
marks, etc)
Falls
Precipitating factors/cause
(mechanical vs syncope)
Height and direction
Landing surface
Patient complaints/injuries
o Step 4 – Special Considerations
Modifying factors
Age
Pregnancy
CONSIDERATIONS - same as adults except for age specific
findings
o Assess for injuries that meet trauma triage guidelines
Policy # 153
o Step I – Physiologic findings
Pediatric hemodynamic compromise –
poor perfusion - capillary refill > 2 sec.
Respiratory rate >60 or < 20 in
infants < 1yr.
Mental status – GCS <13
o Assess for Steps 2-4 – Same as Adult
Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
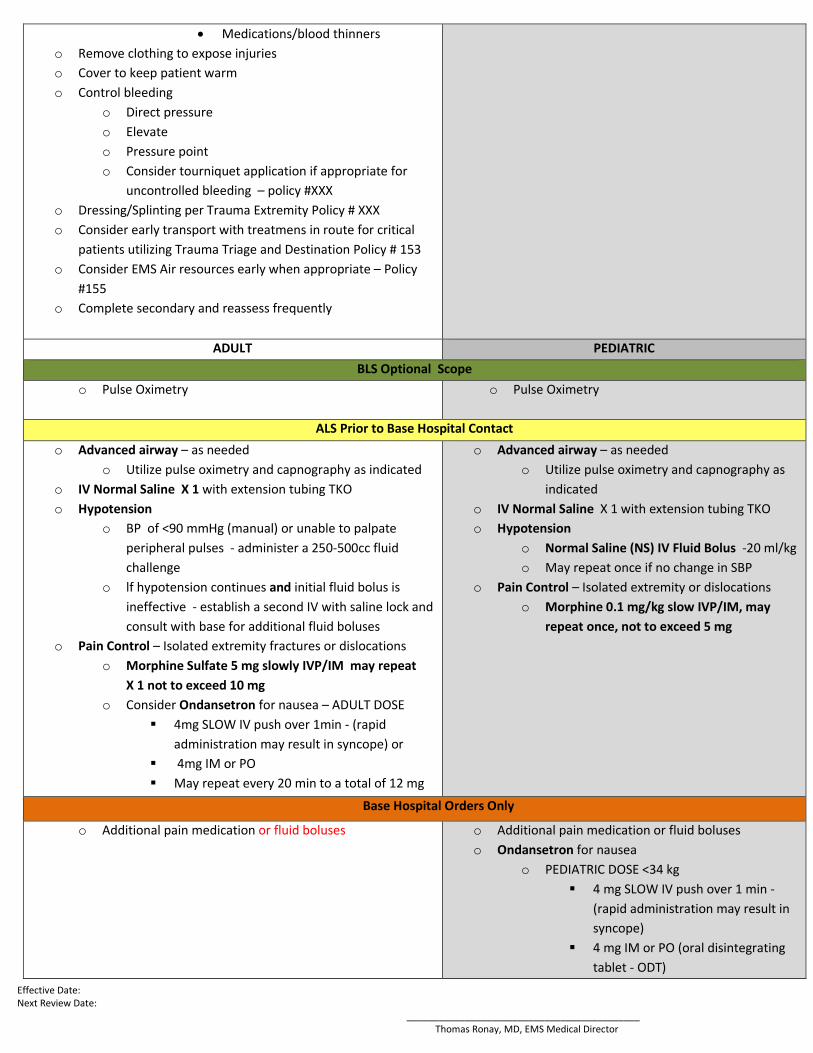
Medications/blood thinners
o Remove clothing to expose injuries
o Cover to keep patient warm
o Control bleeding
o Direct pressure
o Elevate
o Pressure point
o Consider tourniquet application if appropriate for
uncontrolled bleeding – policy #XXX
o Dressing/Splinting per Trauma Extremity Policy # XXX
o Consider early transport with treatmens in route for critical
patients utilizing Trauma Triage and Destination Policy # 153
o Consider EMS Air resources early when appropriate – Policy
#155
o Complete secondary and reassess frequently
ADULT PEDIATRIC
BLS Optional Scope
o Pulse Oximetry o Pulse Oximetry
ALS Prior to Base Hospital Contact
o Advanced airway – as needed
o Utilize pulse oximetry and capnography as indicated
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o BP of <90 mmHg (manual) or unable to palpate
peripheral pulses - administer a 250-500cc fluid
challenge
o lf hypotension continues and initial fluid bolus is
ineffective - establish a second IV with saline lock and
consult with base for additional fluid boluses
o Pain Control – Isolated extremity fractures or dislocations
o Morphine Sulfate 5 mg slowly IVP/IM may repeat
X 1 not to exceed 10 mg
o Consider Ondansetron for nausea – ADULT DOSE
4mg SLOW IV push over 1min - (rapid
administration may result in syncope) or
4mg IM or PO
May repeat every 20 min to a total of 12 mg
o Advanced airway – as needed
o Utilize pulse oximetry and capnography as
indicated
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o Normal Saline (NS) IV Fluid Bolus -20 ml/kg
o May repeat once if no change in SBP
o Pain Control – Isolated extremity or dislocations
o Morphine 0.1 mg/kg slow IVP/IM, may
repeat once, not to exceed 5 mg
Base Hospital Orders Only
o Additional pain medication or fluid boluses o Additional pain medication or fluid boluses
o Ondansetron for nausea
o PEDIATRIC DOSE <34 kg
4 mg SLOW IV push over 1 min -
(rapid administration may result in
syncope)
4 mg IM or PO (oral disintegrating
tablet - ODT)
Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
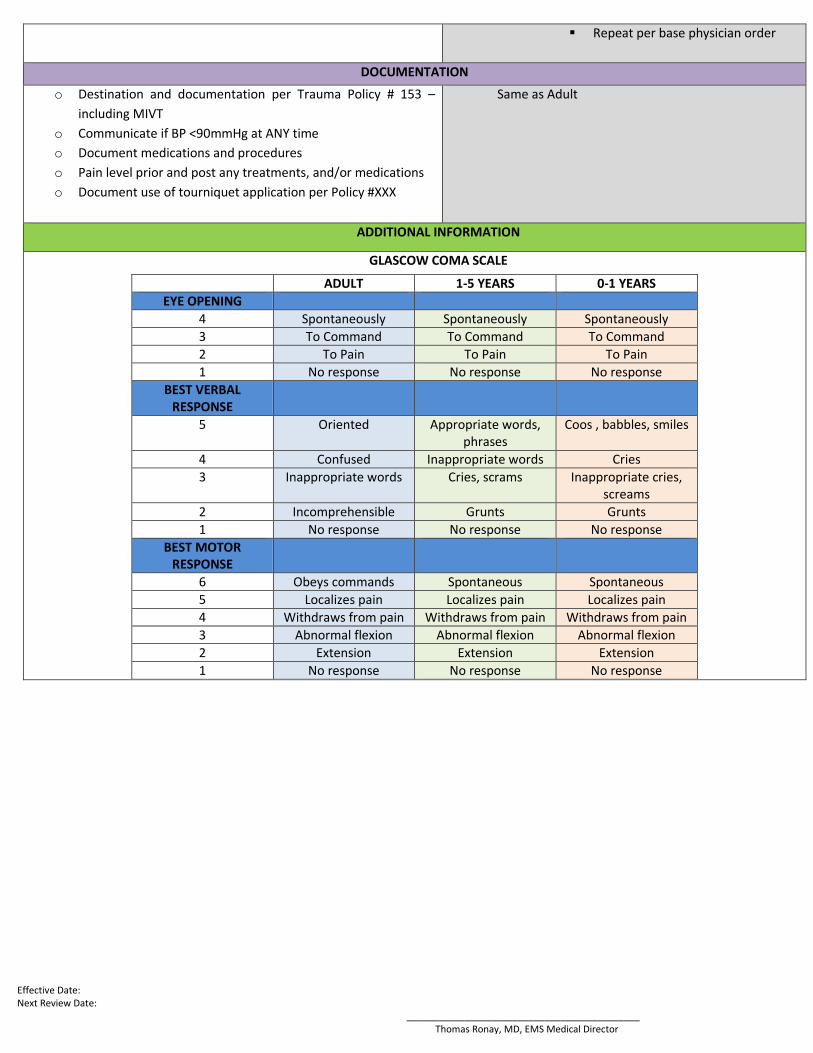
Repeat per base physician order
DOCUMENTATION
o Destination and documentation per Trauma Policy # 153 –
including MIVT
o Communicate if BP <90mmHg at ANY time
o Document medications and procedures
o Pain level prior and post any treatments, and/or medications
o Document use of tourniquet application per Policy #XXX
Same as Adult
ADDITIONAL INFORMATION
GLASCOW COMA SCALE
ADULT 1-5 YEARS 0-1 YEARS
EYE OPENING
4 Spontaneously Spontaneously Spontaneously
3 To Command To Command To Command
2 To Pain To Pain To Pain
1 No response No response No response
BEST VERBAL RESPONSE
5 Oriented Appropriate words, phrases
Coos , babbles, smiles
4 Confused Inappropriate words Cries
3 Inappropriate words Cries, scrams Inappropriate cries, screams
2 Incomprehensible Grunts Grunts
1 No response No response No response
BEST MOTOR RESPONSE
6 Obeys commands Spontaneous Spontaneous
5 Localizes pain Localizes pain Localizes pain
4 Withdraws from pain Withdraws from pain Withdraws from pain
3 Abnormal flexion Abnormal flexion Abnormal flexion
2 Extension Extension Extension
1 No response No response No response

Policy No XXX
San Luis Obispo County
Emergency Medical Services Agency
Head, Neck and Facial Trauma ADULT PEDIATRIC
BLS PROCEDURES
o UNIVERSAL ALGORITHM
o GENERAL TRAUMA ALGORITHM
CONSIDERATIONS
o Remove clothing to expose injuries
o Cover to keep patient warm
o Monitor and maintain airway
o Be prepared to suction
o Avoid hyperventilation (adults 10-12 breaths per
minute)
o Control bleeding
o Direct pressure
o Elevate
o Pressure point
o Eye Injuries
o Trauma/foreign body
Cover both eyes with dressings
Do not remove foreign body or impaled
object – stabilize with bulky dressings
o Chemical Contamination
Flush continuously with NS for at least
15 min or until arrival at the hospital
o Avulsed Teeth
o Place in saline gauze and transport with patient
SAME AS ADULT
CONSIDERATIONS
o Avoid hyperventilation
o Use small tidal volumes
ADULT PEDIATRIC
BLS Optional Scope
o Pulse Oximetry
o Pulse Oximetry

Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
ALS Prior to Base Hospital Contact
o Advanced airway as indicated while maintaining spinal
immobilization
o Monitor airway for obstruction (suction as
necessary)
o Utilize plus oximetry
o Utilize end-tidal CO2
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o BP of <90 mmHg (manual) or unable to palpate
peripheral pulses - administer a 250-500cc fluid
challenge
o lf hypotension continues and initial fluid bolus is
ineffective -establish a second IV with saline
lock and consult with base for additional fluid
boluses
o Pain Control – Isolated extremity or dislocations
o Morphine Sulfate 5 mg slowly IVP/IM - may
repeat X1 not to exceed 10 mg
o Consider Ondansetron for nausea – ADULT DOSE
4mg SLOW IV push over 1min - (rapid
administration may result in syncope) or
4mg IM or PO
May repeat every 20 min to a total of 12
mg
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o Normal Saline (NS) IV Fluid Bolus -20 ml/kg
o May repeat once if no change in SBP
o Pain Control – Isolated extremity or dislocations
o Morphine 0.1 mg/kg slow IVP/IM, may repeat
once, not to exceed 5 mg
Base Hospital Orders Only
o Additional pain medication or fluid boluses o Additional pain medication or fluid boluses
o Ondansetron for nausea
o PEDIATRIC DOSE <34 kg
4 mg SLOW IV push over 1 min - (rapid
administration may result in syncope)
4 mg IM or PO (oral disintegrating
tablet - ODT)
Repeat per base physician order
DOCUMENTATION
o Destination and documentation per Trauma Policy # 153
– including MIVT
o Pain level prior and post treatments and/or medications
o Document use of tourniquet application per Policy #XXX
Same as Adult
ADDITIONAL INFORMATION

Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
GLASCOW COMA SCALE
ADULT 1-5 YEARS 0-1 YEARS
EYE OPENING
4 Spontaneously Spontaneously Spontaneously
3 To Command To Command To Command
2 To Pain To Pain To Pain
1 No response No response No response
BEST VERBAL RESPONSE
5 Oriented Appropriate words, phrases
Coos , babbles, smiles
4 Confused Inappropriate words Cries
3 Inappropriate words Cries, scrams Inappropriate cries, screams
2 Incomprehensible Grunts Grunts
1 No response No response No response
BEST MOTOR RESPONSE
6 Obeys commands Spontaneous Spontaneous
5 Localizes pain Localizes pain Localizes pain
4 Withdraws from pain Withdraws from pain Withdraws from pain
3 Abnormal flexion Abnormal flexion Abnormal flexion
2 Extension Extension Extension
1 No response No response No response

Policy No XXX
San Luis Obispo County
Emergency Medical Services Agency
Chest and Abdomen Trauma ADULT PEDIATRIC
BLS PROCEDURES
o UNIVERSAL ALGORITHM
o Scene Safety/PPE
o Do not delay transport with non-essential
treatment of the non-entrapped/transport ready
critical trauma patient.
o Attempt to limit on scene time to 10 min or less
when Trauma Triage Criteria are met
o CONSIDERATIONS
o Remove clothing to expose injuries
o Cover to keep patient warm
o Control bleeding
o Communicate if BP <90 mmHg at ANY time
o Evaluate and communicate mechanism of injury
o Evaluate for seatbelt signs or other points of
impact
o IMPALDED OBJECTS
o Immobilize the object to prevent further
movement
o CHEST
o Open Wounds – With air leak - cover with
Vaseline impregnated dressing and tape on 3
sides or use chest seal device seal
o Flail Chest – support fail segment and monitor
respirations – support if necessary
o ABDOMINAL
o Eviscerations – cover with moist saline dressing
o PREGNANCY
o If > 20 weeks pregnant place in left lateral
position for transport ( if in spinal immobilization
tilt spine board to left)
SAME AS ADULT
ADULT PEDIATRIC
Optional Scope
o Pulse Oximetry
Pulse Oximetry

Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
ALS Prior to Base Hospital Contact
o Advanced airway if indicated
o Utilize pulse oximetry and capnography
o Needle thoracotomy for suspected tension
pneumothorax
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o BP of <90 mmHg (manual) or unable to
palpate peripheral pulses - administer a
250-500cc fluid challenge
o lf hypotension continues and initial fluid
bolus is ineffective - establish a second IV
with saline lock and consult with base for
additional fluid boluses
o Pain Control – Isolated extremity or dislocations or
Burns without multisystem trauma
o Morphine Sulfate 5 mg slowly IVP/IM –
may repeat X1 not to exceed 10 mg
o Consider Ondansetron for nausea – ADULT
DOSE
4mg SLOW IV push over 1min -
(rapid administration may result in
syncope) or
4mg IM or PO
o May repeat every 20 min to a total of 12 mg
o Advanced airway if indicated
o Utilize pulse oximetry and capnography
o Needle thoracotomy for suspected tension
pneumothorax
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o Normal Saline (NS) IV Fluid Bolus -20
ml/kg
o May repeat once if no change in SBP
o Pain Control – Isolated extremity or dislocations or
burns without multisystem trauma
o Morphine 0.1 mg/kg slow IVP/IM, may
repeat once, not to exceed 5 mg
Base Hospital Orders Only
o Pain control not covered above
o Additional fluid boluses
o Pain control not covered above
o Additional fluid boluses
DOCUMENTATION
Policy No XXX
San Luis Obispo County
Emergency Medical Services Agency
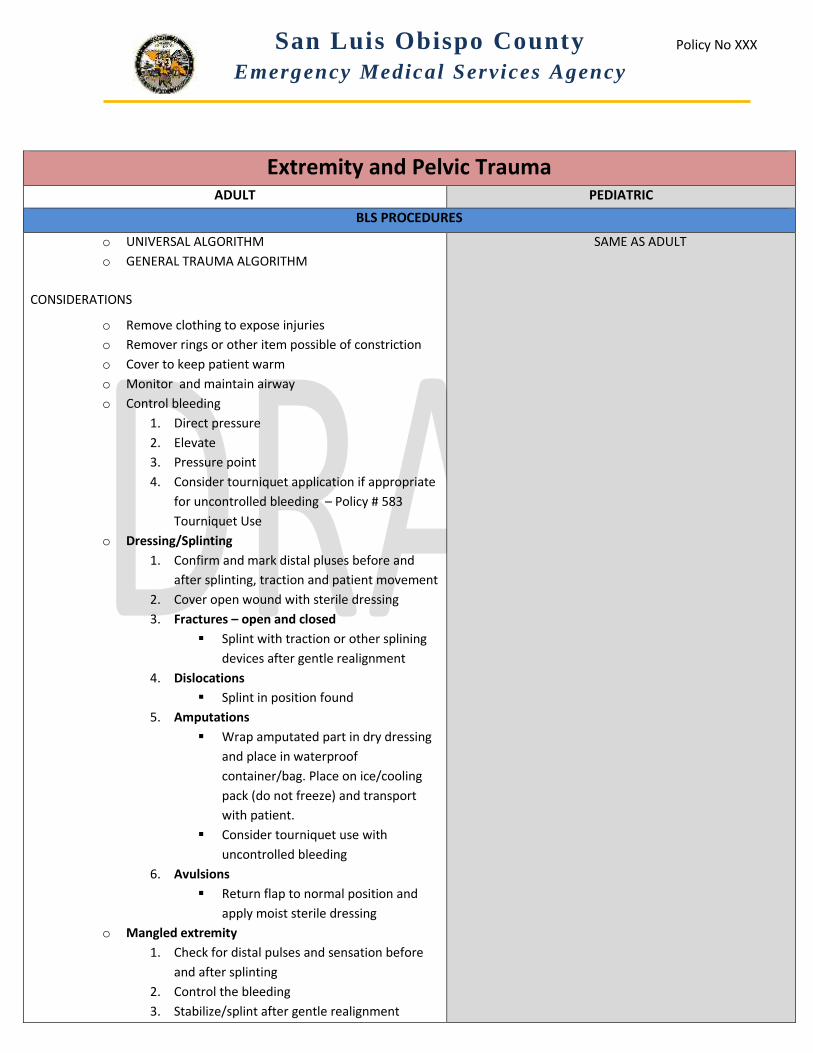
Extremity and Pelvic Trauma ADULT PEDIATRIC
BLS PROCEDURES
o UNIVERSAL ALGORITHM
o GENERAL TRAUMA ALGORITHM
CONSIDERATIONS
o Remove clothing to expose injuries
o Remover rings or other item possible of constriction
o Cover to keep patient warm
o Monitor and maintain airway
o Control bleeding
1. Direct pressure
2. Elevate
3. Pressure point
4. Consider tourniquet application if appropriate
for uncontrolled bleeding – Policy # 583
Tourniquet Use
o Dressing/Splinting
1. Confirm and mark distal pluses before and
after splinting, traction and patient movement
2. Cover open wound with sterile dressing
3. Fractures – open and closed
Splint with traction or other splining
devices after gentle realignment
4. Dislocations
Splint in position found
5. Amputations
Wrap amputated part in dry dressing
and place in waterproof
container/bag. Place on ice/cooling
pack (do not freeze) and transport
with patient.
Consider tourniquet use with
uncontrolled bleeding
6. Avulsions
Return flap to normal position and
apply moist sterile dressing
o Mangled extremity
1. Check for distal pulses and sensation before
and after splinting
2. Control the bleeding
3. Stabilize/splint after gentle realignment
SAME AS ADULT

Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
4. Cover with dry dressing
ADULT PEDIATRIC
BLS Optional Scope
o Pulse Oximetry o Pulse Oximetry
ALS Prior to Base Hospital Contact
o Dressing/Splinting
o Dislocation
Splint in position found
With signs of neurovascular compromise
attempt to place in anatomic position with
gentle traction
o Pelvic instability
Adult patients with mechanism of injury and
complaint of severe pelvic pain with a BP<90
mmHg – consider applying binder (sheet or
commercial device)
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o BP of <90 mmHg (manual) or unable to palpate
peripheral pulses - administer a 250-500cc fluid
challenge
o lf hypotension continues and initial fluid bolus is
ineffective - establish a second IV with saline lock and
consult with base for additional fluid boluses
o Pain Control – Isolated extremity or dislocations
o Morphine Sulfate 5 mg slowly IVP/IM – may repeat
X1 not to exceed 10 mg
o Consider Ondansetron for nausea – ADULT DOSE
4mg SLOW IV push over 1min - (rapid
administration may result in syncope) or
4mg IM or PO
May repeat every 20 min to a total of 12 mg
o IV Normal Saline X 1 with extension tubing TKO
o Hypotension
o Normal Saline (NS) IV Fluid Bolus -20
ml/kg
o May repeat once if no change in SBP
o Pain Control – Isolated extremity or dislocations
o Morphine 0.1 mg/kg slow IVP/IM, may
repeat once, not to exceed 5 mg
Base Hospital Orders Only
o Additional pain medication or fluid boluses o Additional pain medication or fluid boluses
o Ondansetron for nausea
o PEDIATRIC DOSE <34 kg
4 mg SLOW IV push over 1 min -
(rapid administration may result
in syncope)
4 mg IM or PO (oral
disintegrating tablet - ODT)
Repeat per base physician order
DOCUMENTATION

Effective Date: Next Review Date: ____________________________________________ Thomas Ronay, MD, EMS Medical Director
o Destination and documentation per Trauma Policy # 153 –
including MIVT
o Pain level prior and post pain reduction treatments and
medications
o Document use of tourniquet application per Policy #583
Same as Adult
Policy No XXX
Review: 2016 ____________________________________________ Thomas Ronay, MD, EMS Medical Director
San Luis Obispo County
Emergency Medical Services Agency
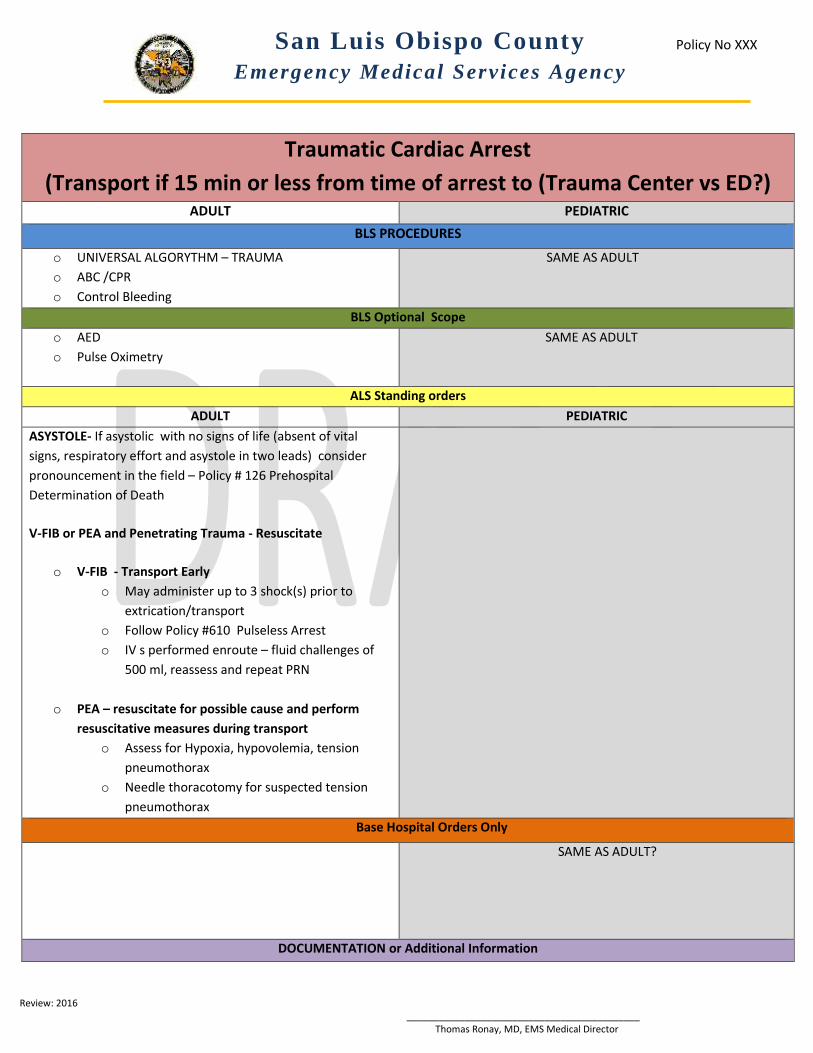
Traumatic Cardiac Arrest
(Transport if 15 min or less from time of arrest to (Trauma Center vs ED?) ADULT PEDIATRIC
BLS PROCEDURES
o UNIVERSAL ALGORYTHM – TRAUMA
o ABC /CPR
o Control Bleeding
SAME AS ADULT
BLS Optional Scope
o AED
o Pulse Oximetry
SAME AS ADULT
ALS Standing orders
ADULT PEDIATRIC
ASYSTOLE- If asystolic with no signs of life (absent of vital
signs, respiratory effort and asystole in two leads) consider
pronouncement in the field – Policy # 126 Prehospital
Determination of Death
V-FIB or PEA and Penetrating Trauma - Resuscitate
o V-FIB - Transport Early
o May administer up to 3 shock(s) prior to
extrication/transport
o Follow Policy #610 Pulseless Arrest
o IV s performed enroute – fluid challenges of
500 ml, reassess and repeat PRN
o PEA – resuscitate for possible cause and perform
resuscitative measures during transport
o Assess for Hypoxia, hypovolemia, tension
pneumothorax
o Needle thoracotomy for suspected tension
pneumothorax
Base Hospital Orders Only
SAME AS ADULT?
DOCUMENTATION or Additional Information

Effective Date: January 1, 2014 Review: 2016 ____________________________________________ Thomas Ronay, MD, EMS Medical Director
CONSIDERATIONS
o Cardiac etiology in older patients with low probable
mechanism of injury
o Unsafe scene may warrant transport despite low
potential for survival
o Consider minimal disturbance of potential crime scene
SAME AS ADULT

K:\PublicData\COMMITTEES\Clinical Advisory Subcommittee\2014\May.13.2014\Staff Report Summary_Policy 153 trauma triage 4.3 ops 05022014 SL.docx
Public Health Department
Emergency Medical Services Agency 2156 Sierra Way, San Luis Obispo, CA 93401
805-788-2511 ▪ FAX 805-788-2517
www.sloemsa.org
Policy 153 Trauma Triage
MEETING DATE Clinical Advisory Committee
STAFF CONTACT Kathy Collins, Specialty Care Systems Coordinator, 788-2514
SUBJECT Policy 153 Trauma Triage and Destination
SUMMARY The current triage guidelines in SLO county are not in line with triage guidelines of neighboring counties or the CDC recommendations. Specifically the following falls out occur in Step 2 Mechanism of Injury for patients with” significant injures”:
Two proximal long bone fractures
Crushed, degloved, mangled or pulseless extremity
Amputation proximal to the wrist or ankle
Pelvic instability/fractures
When the State EMS Authority approved the SLO Trauma Plan it was with the direction that a QI process would review the criteria that were not in line with the CDC recommendations. The Trauma Center and the EMS Agency reviewed trauma consults in 2013 with “two or more proximal long bone fractures” and identified 8 patients with two more proximal long bone fractures. Of these patients, 6 were associated with other injuries, 4 were transferred to higher level of care, and 3 did not meet any other triage criteria but had serious injuries.
REVIEWED BY Trauma Advisory Committee EMS Staff Thomas Ronay, MD, SLO County Medical Director Steve Lieberman, EMS Division Director Sierra Vista Trauma Advisory
RECOMMENDED ACTION(S)
A high association of serious injury for patients with two proximal long bone fractures was demonstrated though a review of the SLO data, and noting it is also national and regional standard in other programs - staff is recommending “two proximal long bone fractures” be moved to Step 2 for patients that are “significantly injured” and that the other anatomic injures continued to be monitored over the coming years.
ATTACHMENT(S) Policy 153 trauma triage and destination matrix
SAN LUIS OBISPO COUNTY HEALTH AGENCY
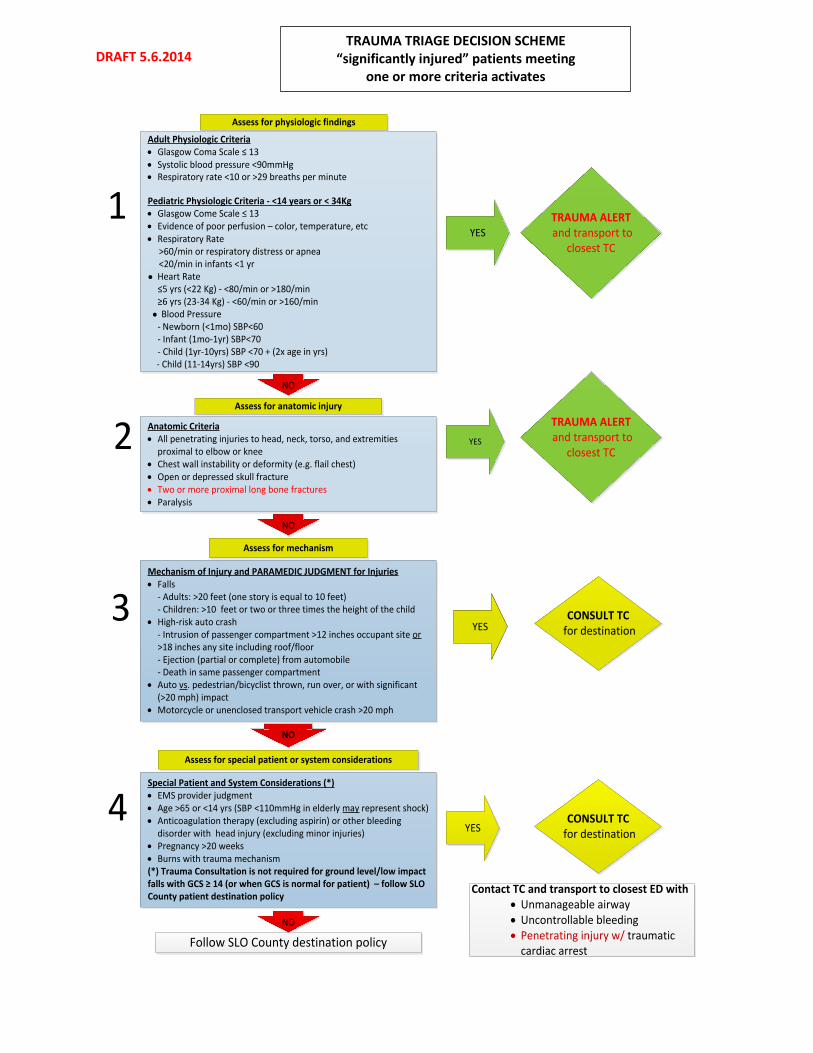
DRAFT 5.6.2014 TRAUMA TRIAGE DECISION SCHEME
“significantly injured” patients meeting one or more criteria activates
Adult Physiologic Criteria · Glasgow Coma Scale ≤ 13 · Systolic blood pressure <90mmHg · Respiratory rate <10 or >29 breaths per minute Pediatric Physiologic Criteria - <14 years or < 34Kg · Glasgow Come Scale ≤ 13· Evidence of poor perfusion – color, temperature, etc · Respiratory Rate >60/min or respiratory distress or apnea <20/min in infants <1 yr ● Heart Rate
≤5 yrs (<22 Kg) - <80/min or >180/min≥6 yrs (23-34 Kg) - <60/min or >160/min
● Blood Pressure- Newborn (<1mo) SBP<60 - Infant (1mo-1yr) SBP<70- Child (1yr-10yrs) SBP <70 + (2x age in yrs)
- Child (11-14yrs) SBP <90
Anatomic Criteria· All penetrating injuries to head, neck, torso, and extremities
proximal to elbow or knee · Chest wall instability or deformity (e.g. flail chest)· Open or depressed skull fracture· Two or more proximal long bone fractures· Paralysis
Special Patient and System Considerations (*)· EMS provider judgment· Age >65 or <14 yrs (SBP <110mmHg in elderly may represent shock)· Anticoagulation therapy (excluding aspirin) or other bleeding
disorder with head injury (excluding minor injuries) · Pregnancy >20 weeks· Burns with trauma mechanism(*) Trauma Consultation is not required for ground level/low impact falls with GCS ≥ 14 (or when GCS is normal for patient) – follow SLO County patient destination policy
Mechanism of Injury and PARAMEDIC JUDGMENT for Injuries· Falls
- Adults: >20 feet (one story is equal to 10 feet)- Children: >10 feet or two or three times the height of the child
· High-risk auto crash - Intrusion of passenger compartment >12 inches occupant site or
>18 inches any site including roof/floor - Ejection (partial or complete) from automobile - Death in same passenger compartment· Auto vs. pedestrian/bicyclist thrown, run over, or with significant
(>20 mph) impact· Motorcycle or unenclosed transport vehicle crash >20 mph
TRAUMA ALERT and transport to
closest TC
Assess for mechanism
Follow SLO County destination policy
Contact TC and transport to closest ED with· Unmanageable airway· Uncontrollable bleeding· Penetrating injury w/ traumatic
cardiac arrest
Assess for anatomic injury
Assess for special patient or system considerations
CONSULT TC for destination
YES
YES
YES
YES
NO
NO
NO
NO
2
3
4
TRAUMA ALERT and transport to
closest TC
Assess for physiologic findings
1
CONSULT TC for destination