cleft lip and palate for orthodontist by almuzian
TRANSCRIPT

Cleft Lip & Palate
From Orthodontic Point of View
Table of ContentsTable of Contents......................................................................................................................2
Definition .................................................................................................................................6
Incidence...................................................................................................................................6
Syndromic and non-Syndromic clefting................................................................................8
Embryology of clefts of the lip and palate................................................................................8
Lip development ......................................................................................................................8
Abnormal lip Development.................................................................................................11
Development of the palate ....................................................................................................11
Theories of palatal shelf elevation. (Ferguson 1981)..............................................................12
Abnormal palate Development...........................................................................................13
Aetiology.................................................................................................................................14
Classifications.........................................................................................................................16
Descriptive method by Veau...............................................................................................16
Symbolic method using the “stripped Y” Kernahan 1971 ......................................................17
LAHSHAL classification developed by Kriens 1989..................................................................17
Preventive treatment..............................................................................................................17
CSAG Report (Clinical Standards Advisory Group) by Shaw 1995..........................................18
Indices and grading used in cleft cases...................................................................................20
Index of 5-year old children (Attack et al., 1997):...................................................................20
Grading ..........................................................................................................................20
GOSLON index (Great Ormond Street, London and Oslo Net) Yardstick (Mars et al., 1987)...22
I.Anteroposterior Assessment of labial segements.........................................................23
II.Vertical Assessment.....................................................................................................23
Mohammed Almuzian 2
III.Transverse Assessment...............................................................................................23
Ranking of GOLSON index.......................................................................................................24
Bergland index for secondary ABG outcomes.........................................................................24
Kindelan score ........................................................................................................................25
Problems Associated with Cleft Lip and Palate.......................................................................25
I.General difficulties ...............................................................................................................25
II.Dental disturbances in both repaired and unrepaired cleft cases ......................................25
III.Skeletal Features of unrepaired cleft lip and palate ...........................................................26
IV.Skeletal Features of repaired cleft lip and palate (Shaw 1990)...........................................27
Iatrogenic effect of surgery.....................................................................................................27
Ideal Cleft palate Team...........................................................................................................28
Summary of the whole Treatment .........................................................................................29
In details:................................................................................................................................31
Prenatal age............................................................................................................................31
At Birth ...................................................................................................................................32
Potential Complications and Clinical Pearls of NAM...............................................................35
SIX Months of age...................................................................................................................38
D.Dental roles:................................................................................................................39
6-12 Months of age.................................................................................................................40
A.Palatal Repair...............................................................................................................40
B.Sometime Lip and soft palate repair undertaken at 6 months at one time.................41
C.Dental roles:.................................................................................................................41
D.Pharygoplasty:.............................................................................................................41
Aetiological factors pf speech problems:-.......................................................................42
1-5 Years of age......................................................................................................................42
1.Lee records at 5 years stage ........................................................................................42
Mohammed Almuzian 3
2.Assessment using the 5-year-old index introduced by Attack 1997 ...........................42
3.Interceptive Orthodontic treatment ...........................................................................42
4.Dentist roles.................................................................................................................42
7-10 years of age.....................................................................................................................43
1.Lee’s records................................................................................................................43
2.GOSLON Yardstick (Mars 1987)....................................................................................43
3.Secondary alveolar bone grafting:...............................................................................43
The main aims secondary ABG........................................................................................45
Surgical technique of ABG...............................................................................................46
Postoperative instruction................................................................................................46
Postoperative assessment..............................................................................................47
The complications...........................................................................................................47
Influencing success.........................................................................................................48
Segmental Surgery at the same time of the secondary alveolar bone grafting, Harris 2008............................................................................................................................................48
Lesser Segment Alveolar Distraction ..................................................................................49
11-15 Years of age..................................................................................................................50
Pharyngoplasty...............................................................................................................50
Orthodontics..................................................................................................................50
18+ Years of age......................................................................................................................50
1.Lee’s Records ..............................................................................................................50
2.Orthognathic surgery...................................................................................................50
Secondary surgical correction for CLP patient........................................................................50
Specific Problems in Cleft Patients .....................................................................................50
Treatment Planning for CLP................................................................................................51
The Choice of Operation for CLP.........................................................................................52
Mohammed Almuzian 4
Airway Considerations for CLP during surgery........................................................................55
Postoperative considerations for CLP.................................................................................55
3.Secondary plastic procedures......................................................................................56
Terminology ...........................................................................................................................57
Maxillary and Nasal Impression .............................................................................................57
Mohammed Almuzian 5
Cleft Lip & Palate
From Orthodontic Point of View
Definition
Incomplete fusion of hard and /or soft tissue structures of the lip and
palate.
Incidence
A. Genetic risks
• One affected parent, risk of the first child 2%
• One affected child, risk of next child with is (4%).
• One affected parent and one affected child risk of next child
with is 10%
• Two affected parents, risk of first child 60%
B. Prevalence in the UK population
• UCLP 40%
• CP 30%
• BCLP 10%
• CL 10%
• Submucous cleft or soft palate cleft 10%
Mohammed Almuzian 6

C. CLP
Incidence of unilateral CL(P) varies with race:
1. In Negros is around 1 in every 2000 live birth.
2. In UK 1 in every 700 live births
3. In Caucasians it is about 1 in every 750 live births (Mitchell, 2000).
4. In oriental populations is around 1 in very 600 live births.
5. Left side is more affected than the right side (2:1).
6. More common in male 3:1
D. CP:
• Prevalence around 1:2000 live births.
• 55% Associated with syndromes such as Down, Treacher-
Collin, Pierre-Robin sequence.
• CP the incidence is higher in females overall (3:2).
E. Gender distribution:
• CLP has greater incidence in males 3:1
• CP the incidence is higher in females overall (3:2).
• There is a male predominance of submucus clefts.
• There is equal gender incidence of isolated soft palate clefts and
cleft lip alone
Mohammed Almuzian 7
Syndromic and non-Syndromic clefting
15% of cleft children have additional malformations especially BCLP and
CP to have additional malformations (400 syndrome) , example:
1. Van der Woude
• 1:28000
• Autosomal dominant.
• Lower lip pits
• +/or CL/P or CPO (2% of cleft cases).
• Hypodontia.
• No other anomalies.
2. Pierre Robin sequence. Triad of cleft palate, micrognathia,
macroglossia
3. Treacher Collins
Embryology of clefts of the lip and palate
Lip development
• Facial development begins at 4-6 weeks
• 5 facial prominences. Frontonasal process ‘’FNP’’ (unpaired), paired
maxillary process and paired mandibular process
Mohammed Almuzian 8

z
• By four weeks of development the two mandibular processes are the
first to unite and give rise
to the lower lip, lower
portion of the cheeks and
other mandibular
structures.
• By five weeks of
development, medial and
lateral nasal processes form
within the enlarged
frontonasal process to
surround an early
ectodermal thickening, the
nasal placode.
• The nasal placode gives
rise to highly specialized olfactory receptor cells and nerve fibre bundles
innervating the future nasal cavity.
• As the medial and lateral nasal processes enlarge, the nasal placodes
sink into the nasal pits, which demarcate the nostrils.
• Medial growth of the maxillary processes dominates subsequent
development of the face, resulting first in contact and then fusion with the
lateral nasal processes (6 weeks IU) to form:
1. Nasolacrimal duct
2. Cheek
Mohammed Almuzian 9
3. Alar base of the future nose.
• Further growth towards the midline pushes the lateral nasal processes
superiorly and allows fusion of the maxillary processes with the medial
nasal processes inferiorly, merging them together in the midline to form:
1. Central portion of the nose;
2. Upper lip philtrum;
3. Primary palate.
• Thus, the upper lip is formed from the maxillary processes laterally
and the medial nasal processes in the midline (Jiang et al, 2006).
• Posteriorly, from the medial sides of the maxillary process, the
secondary palate is formed via growth, elevation and subsequent fusion
between the paired palatine processes. These processes also fuse with the
nasal septum superiorly and the primary palate anteriorly, ultimately
separating the oral and nasal cavities. The essential features of the human
face have formed by eight weeks of development.
Mohammed Almuzian 10

Abnormal lip Development
Defective fusion at any of the sites highlighted in the above figures may
result in a facial cleft.
1. Cleft mandible
2. Lateral facial cleft
3. Oblique facial cleft
4. Cleft Lip (Unilateral or Bilateral)
5. Median cleft
Development of the palate
• 1° palate is made up of the medial nasal process. It contains the first
four teeth and contributes the philtrum of the upper lip.
• 2° palate apparent at 6 weeks as inferiorly lying outgrowths from the
maxillary process, lying lateral to the tongue.
Mohammed Almuzian 11

• At 8 weeks shelf elevation begins.
Theories of palatal shelf elevation. (Ferguson 1981)
• Extrinsic
1. Straightening of the cranial base.
2. Lifting of the head relative to the body.
3. Increased height of the oro-nasal cavity.
4. Tongue movement downward.
5. Increased mandibular prominence.
• Intrinsic
1. Increase in the osmotic pressure of the palatal shelves
2. Cellular reorganisation (increased density of epithelial/mesenchymal cells
on the palatal side of the shelf causing rotation),
Mohammed Almuzian 12

3. Contraction (muscle/non-muscle)
4. Vascular erectile force.
• Following elevation, at 9 weeks, further growth brings the medial edge of
each shelf into close contact. At this stage, mesenchyme from each shelf
is still separated by an epithelial seam of medial edge epithelium.
• Three mechanisms have been proposed to explain medial edge epithelium
breakdown:
1. Apoptosis (programmed cell death)
2. Epithelial to mesenchymal transformation, and
3. Migration of epithelium to the oral and nasal compartments.
• Regardless of the mechanism, breakdown of the epithelial seam results in
mesenchymal continuity and palatal fusion. As well as fusion between
secondary palatal shelves, an important step during palatogenesis is
fusion of the primary palate to the secondary palate.
Abnormal palate Development
• Clefts form when there is failure of process growth or fusion, this is due
to:
1. Primary defects leading to cleft palate include:
• Failure of shelf elevation
• Failure of shelf growth
• Failure of shelf fusion
Mohammed Almuzian 13
• Breakdown of shelf fusion
2. Secondary defects leading to cleft palate include:
• Growth disturbances in craniofacial structures
• Mechanical obstruction of palatal elevation.
Aetiology
In normal development, fusions of the embryological processes that
comprise the upper lip appear around 6 W.I.U life while fusion to form
the secondary palate occur around 8 W.I.U life. Any disruption affecting
the timing at which the fusion occurs will increase the incidence of cleft.
The etiological factors are:
A. Genetic: A gene coding for TGF has been implicated. These
include: homebox gene, SHH, MSX1, MSX2, BMP-2, FGF-8
B. Environmental
• IU position
• Social deprivation
• Smoking
• Alcohol
• Trauma.
• Radiation.
• Maternal hypoxia
Mohammed Almuzian 14

• Drugs like Steroids, Anticonvulsant drugs
• Infection like CMV, Rubella
• Endocrine like Diabetes
• Deficiency of nutritional supplements such as deficiency in folic acids
Bixler (1981) divided clefts into 3 aetiological domains
C. Syndromic . Represent 70% of clefting
D. Familial or hereditary .
E. Sporadically or Isolated or non-Familial . The patient is the first
person in a family with the defect. Most commonly:
• IU position
• Social deprivation
• Smoking
• Alcohol
• Trauma.
• Radiation.
• Maternal hypoxia
• Drugs like Steroids, Anticonvulsant drugs
• Infection like CMV, Rubella
Mohammed Almuzian 15

• Endocrine like Diabetes
• Deficiency of vitamin supplements such as deficiency in folic acids
Classifications
Descriptive method by Veau
This is most commonly used nowadays.
A. Cleft lip
• Notched lip
• Incomplete cleft lip
• Complete cleft lip
• Unilateral or bilateral
B. Cleft alveolus (primary palate)
C. Cleft palate
• Cleft uvula
• Soft palate only
• Submucous cleft
• Complete
• Incomplete
D. Combinations
Mohammed Almuzian 16
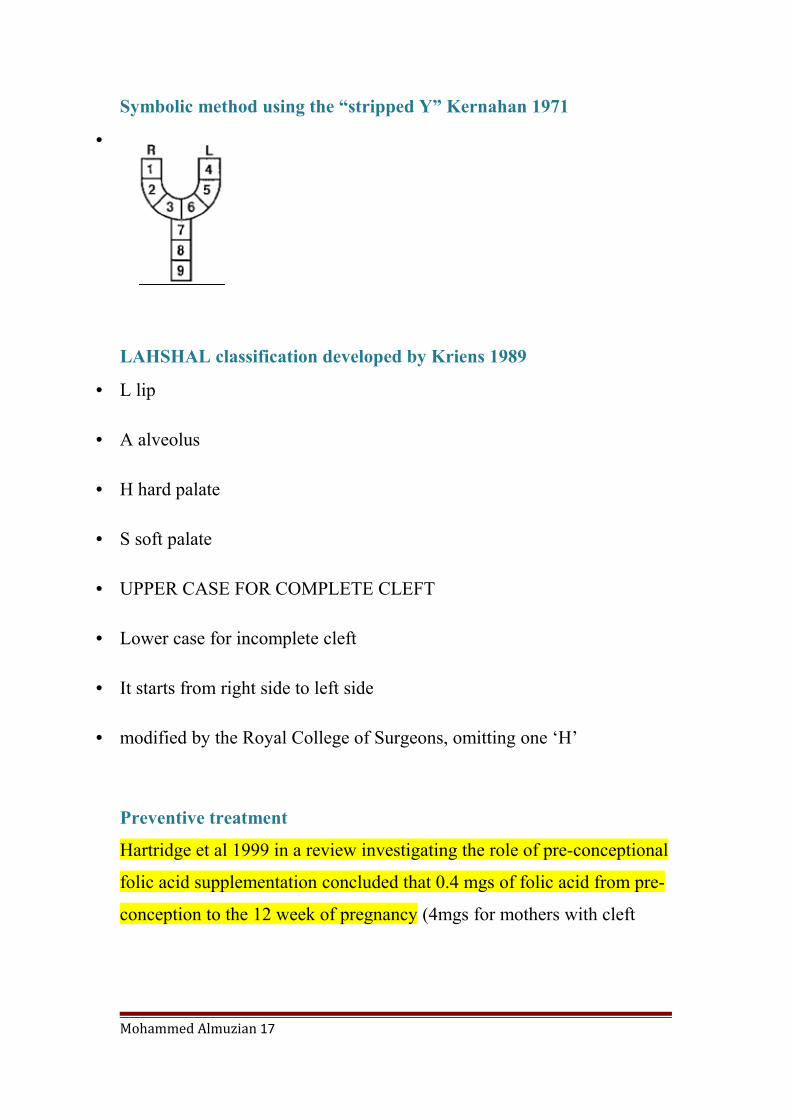
Symbolic method using the “stripped Y” Kernahan 1971
•
LAHSHAL classification developed by Kriens 1989
• L lip
• A alveolus
• H hard palate
• S soft palate
• UPPER CASE FOR COMPLETE CLEFT
• Lower case for incomplete cleft
• It starts from right side to left side
• modified by the Royal College of Surgeons, omitting one ‘H’
Preventive treatment
Hartridge et al 1999 in a review investigating the role of pre-conceptional
folic acid supplementation concluded that 0.4 mgs of folic acid from pre-
conception to the 12 week of pregnancy (4mgs for mothers with cleft
Mohammed Almuzian 17
children) although not proved conclusively can have significant
protective effects.
CSAG Report (Clinical Standards Advisory Group) by Shaw 1995
• First Mars 1987 show that UK is the worst.
• Professionals in the field of cleft work expressed concern regarding the
quality of treatment outcome for patients with cleft lip and palate in the
UK.
• This was based principally upon the outcome of two studies:
A. The GOSLON Yardstick (Great Ormond Street, London and Oslo)
was developed as a clinical tool that categorised dental arch
relationships into five discrete categories. Using this yardstick,
comparison between UK and Norwegian cleft centres demonstrated
significant shortcomings in outcomes associated with the UK
centre.
B. Eurocleft - a European, multicentre clinical audit of treatment
outcome for complete unilateral CLP. It found the two UK centres
that participated to be weakest on almost every aspect of care
• In 1995 the Department of Health in the UK charged the Clinical
Standards Advisory Group to investigate the quality of care within the
UK.
• All children in the UK with a unilateral complete cleft lip and palate aged
5 or 12 years of age in 1996-1997 were examined. Their speech, hearing,
facial appearance, dental malocclusion, dental health, quality of bone
Mohammed Almuzian 18
graft and skeletal base relationships were examined. (457 children non
syndromic with UCLP)
• Cleft care was provided in 57 centres.
• The study found that the average result in all these areas was poor.
Children from the UK centres were more likely to suffer mid-face
retrusion (70% of pt 12 years has class III) and poor dental relationships
than three of the European centres.
• Fewer than 60% of children in the UK had a successful bone graft in
comparison with 97% from one of the other European centres. It was
therefore clear that some patients were not receiving optimal care in the
UK.
The CSAG1 report 1998 made several recommendations, including:
I. Centres should be limited to 8-15 in the UK.
• England and Wales, 10 centres
• Northern Ireland operates as a single centre
• Scotland operates as one single centre known as CLEFTSiS
II. Each centre should provide a full range of cleft care.
III. Nationwide database.
IV. Results should be regularly audited.
V. Training should be provided for specialists in cleft care in high
volume centres only.
Mohammed Almuzian 19

VI. Each clinical team consists of specialist orthodontists, surgeons,
speech and language therapists, specialist nurses, geneticists,
paediatricians, ENT specialists, anaesthetists and psychologists. In
addition they have support staff responsible for data collection, audit
documentation and photography.
Indices and grading used in cleft cases
Index of 5-year old children (Attack et al., 1997):
• Index for dental relationships of 5 year old patients born with
unilateral cleft lip and palate.
• It divided the cases into 5 categories to be able to compare
treatment outcomes earlier and before surgical procedures and
orthodontic treatment.
• The categories used in the grading are:
1. Overjet
2. Inclination of ULS
3. Presence of Crossbite
4. Presence of Open bite
5. Maxillary arch shape and palatal vault anatomy
Grading
1. Grade I
• Positive overjet
Mohammed Almuzian 20

• Average inclined or retroclined incisors
• No crossbites
• No openbites
• Good maxillary arch shape and palatal vault anatomy.
Prognosis: Excellent outcomes
2. Grade 2
• Positive overjet
• Average inclined or proclined upper incisors
• Unilateral crossbite/crossbite tendency
• Open bite tendency around cleft site.
Prognosis: Good outcomes
3. Grade 3
• Edge-to-edge bite average inclined or proclined incisors;
• OR
• Reverse overjet with retroclined incisors
• Unilateral crossbite
• Open bite tendency around cleft site
Prognosis: Fair outcomes
4. Grade 4
Mohammed Almuzian 21
• Reverse overjet
• Average inclined or proclined incisors
• Unilateral crossbite, bilateral crossbite tendency
• Open bite tendency around cleft site .
Prognosis: Poor outcomes
5. Grade 5
• Reverse overjet
• proclined incisors
• Bilateral crossbite
• Open bite
• Very Poor maxillary arch form and palatal vault anatomy
Prognosis: Very poor outcomes
GOSLON index (Great Ormond Street, London and Oslo Net)
Yardstick (Mars et al., 1987)
• It was developed by Mars and used to compare UK results with the
rest of Eu, which actually instigate the CSAG
• It is a record of 10 year old patients
• It measures the severity of malocclusion, the difficulty of
correcting it and the outcomes of the child with a unilateral cleft lip and
palate of children in the early permanent dentition
Mohammed Almuzian 22
This depend on
I. Anteroposterior Assessment of labial segements
• The overjet is examined first. If there is a reverse overjet of 3-5
mm, this indicates that the case might belong to group 3.
• However, if there is already dentoalveolar compensation a higher
category should be considered.
• The anteroposterior relationships of the buccal segments are not of
importance in determining the grouping of a case.
II. Vertical Assessment
It helps in modification of the provisional category in borderline cases.
Deep bite is favorable and AOB is unfavorable
III. Transverse Assessment
It indicate a modification of the provisional category in borderline cases
Mohammed Almuzian 23

Ranking of GOLSON index
1. Groups 1 and 2 have occlusions that require either straightforward
orthodontic treatment or none at all.
2. Group 3 require complex orthodontic treatment to correct the Class III
malocclusion but a good result can be anticipated.
3. Group 4 are at the limits of orthodontic treatment, and if facial growth is
unfavorable, orthognathic surgery will be required.
4. Cases in group 5 require orthognathic surgery.
Bergland index for secondary ABG outcomes
Take periapical x-ray and assess the bone formation at interseptal area
around the ERUPTED canine to assess bone formation Bergland (1986).
1. Grade I: inter-alveolar bone at normal height
2. Grade II: inter-alveolar bone ¾ of normal height
3. Grade III: inter-alveolar bone less than ¼-¾ of normal height
4. Grade IV: no bone at inter-alveolar area. Failed outcomes.
Mohammed Almuzian 24

Kindelan score
After 4-6 months of ABG, take anterior occlusal radiograph and
assess the success using Kindelan score 1997.
It has an advantages that it can be applied even before the eruption
of the canine.
• The degree of bony fill in the cleft area was assessed using a 4-
point scale:
1. Grade 1 > 75% bony fill;
2. Grade 2 50-75% bony fill;
3. Grade 3 < 50% bony fill;
4. Grade 4 no complete bony bridge.
Problems Associated with Cleft Lip and Palate
I. General difficulties
1. Feeding
2. Speech
3. Hearing (which in turn can effect speech development) and middle
ear infections
4. Psychological problems
II. Dental disturbances in both repaired and unrepaired cleft cases
1. Hypodontia , 28% of UCLP and 60% BLCP
Mohammed Almuzian 25

2. Supernumeraries
3. Delayed eruption of teeth on cleft side
4. Increased incidence of impacted upper first molar in cleft side (4times
than non-clefts individuals) (Bjerklin et al., 1993)
5. Dilacerations
6. Hypoplasia
7. Microdontia
The above due to:
• Distortions of the development of the dental lamina which produce
tooth germs. In the patient with a cleft this process is disturbed and result
in dental problems.s
• Msx1 genes mutation.
III. Skeletal Features of unrepaired cleft lip and palate
It is called Embryological defects
1. Cleft Lip only, maxillary arch development is generally normal.
2. Clefts in to the alveolus (incomplete) only with or without lip,
increased incidence of cross bites (19%)
3. Complete bilateral, Premaxilla is anteriorly displaced beyond the tip of
the nasal septum. The lateral segments may have collapsed medially
producing bilateral crossbites.
Mohammed Almuzian 26
4. Complete unilateral, Major segment is rotated outward so the incisor
area appears prominent, the lesser (lateral) segment is more variable and
may be rotated outwards producing a wide cleft or there may be inward
displacement and segment overlap.
5. Isolated clefts of the palate, Excessive inter-tuberosity width may be
observed causing a scissor bite bilaterally
6. Mandibular growth reduced genetically
7. Increase MMP angle, Possibly due to
• Disrupted nasal respiration leading to oral respiration and a mouth open
posture, allowing buccal segments to over-erupt.
IV. Skeletal Features of repaired cleft lip and palate (Shaw 1990)
Embryological defects + Iatrogenic effect of surgery
Iatrogenic effect of surgery
Lip repair has minimal effect on facial growth.
1. AP disturbances. Palatal scar tissue around the tuberosity region hinders
maxillary translation.
2. Transverse disturbances. Scar tissue in the palate leads to a tendency for
buccal cross bites in the 1and 2 dentitions.
3. Vertical disturbances.
Mohammed Almuzian 27

• An ⇑ in LFH is often found. Possibly due to disrupted nasal respiration, ⇑
oral respiration and a mouth open posture, allowing buccal segments to
over-erupt.
Ideal Cleft palate Team
1. Cleft nurse
2. Plastic surgeon
3. Orthodontist
4. Maxillofacial surgeon
5. ENT surgeon
6. Speech therapist
7. Audiologist
8. Pediatrician
9. Psychologist
10.Geneticist
Mohammed Almuzian 28

Summary of the whole Treatment
In red are the roles of the orthodontist and GDP
Prenatal Ultrasound assessment, 70% of the cases are
detected on ultrasound scan at 16-18 weeks
At birth Parent counseling
Feeding
Pre-surgical orthopaedic appliance
6 months Primary surgical lip repair
Primary alveolar bone grafting (old regime)
Nasal repair
Tympanoplasty or grommet,
1 year Palate repair
Preventive dentistry/advice
2-7 years Revision of lip repair
Pharyngoplasty
Tympanoplasty or grommet,
Lee’s records
5 years Index Assessment
Interceptive orthodontic to:
Correct X bite
Mohammed Almuzian 29

Align the maxillary dentition (usually using
fixed appliances) in the growing child if the
appearance causes the child distress or the irregular
teeth are traumatizing soft tissues
Cleft orthodontists can be asked to provide
obturators to assist with speech prior to closure of
any residual fistulae at the time of alveolar bone
grafting
8-10 years Lee’s records
GOSOLN Index Assessment
Maxillary expansion prior to bone grafting,
extract supernumerary teeth and retained primary
teeth.
Bone grafting
OHI and optimal oral health
11-15 Lee’s records
Definitive alignment of the maxillary and
mandibular teeth using fixed appliances
Reverse facial mask
16-more Lee’s records
Orthognathic surgery
Decompensation and alignment for
orthognathic surgery using fixed appliances
Mohammed Almuzian 30
For patients with velo-pharyngeal
dysfunction, the poorly functioning soft palate is
raised with a palatal lift appliance and the velo-
pharyngeal space obturators to reduce hypernasal
speech, which assists the Speech and Language
Therapist in cases that are otherwise untreatable by
language therapy alone with/without surgery.
Electropalatography is a relatively new
technique where patients are provided with an
upper removable orthodontic appliance
incorporating numerous electrodes. When attached
to a PC, the patient can visualize tongue to hard
palate contact on various sounds and the Speech
and Language Therapist can direct therapy sessions
using this technique. Indeed portable EPG
hardware is now available such that the patient can
practice tongue positioning at home.
In details:
Prenatal age
• 70% of the cases are detected on ultrasound scan at 16-18 weeks when
looking for it.
• Cleft Lip and Palate Association (CLAPA) provide support for the
parents this stage.
Mohammed Almuzian 31
• Nurse to provide home visit for support
• Psychologist to provide support
At Birth
1. Parent counseling
Parents are usually in a shock after birth, therefore a counseling is
important to reassure them and facilitate the development of a bond
between the mother and the child. The parent reaction could be
depression, social avoidance, rejection and feelings of guilt
2. Feeding:
• Orthodontist should give counselling and advice on feeding.
• Acrylic plates are no longer used nowadays.
• In isolated CL the nipple will fill the gap so using large teats bottle
is enough.
• Soft feeding bottles with modified long teats which help to direct
the flow of the milk into the mouth are helpful. (Haberman feeder or
bottle or soft Plas bottle)
• Fortified milk
• Some babies are fed by nasogastric tube. One of the most common
reasons for a cleft baby being fed this way is due to Pierre Robin
sequence.
3. Airway
Mohammed Almuzian 32
• Many of these babies have severe airway problems and due to the
smallness of the lower jaw, the tongue remains in a very posterior
position, making oral feeding impossible for weeks or even months.
4. Pre-surgical orthopaedics:
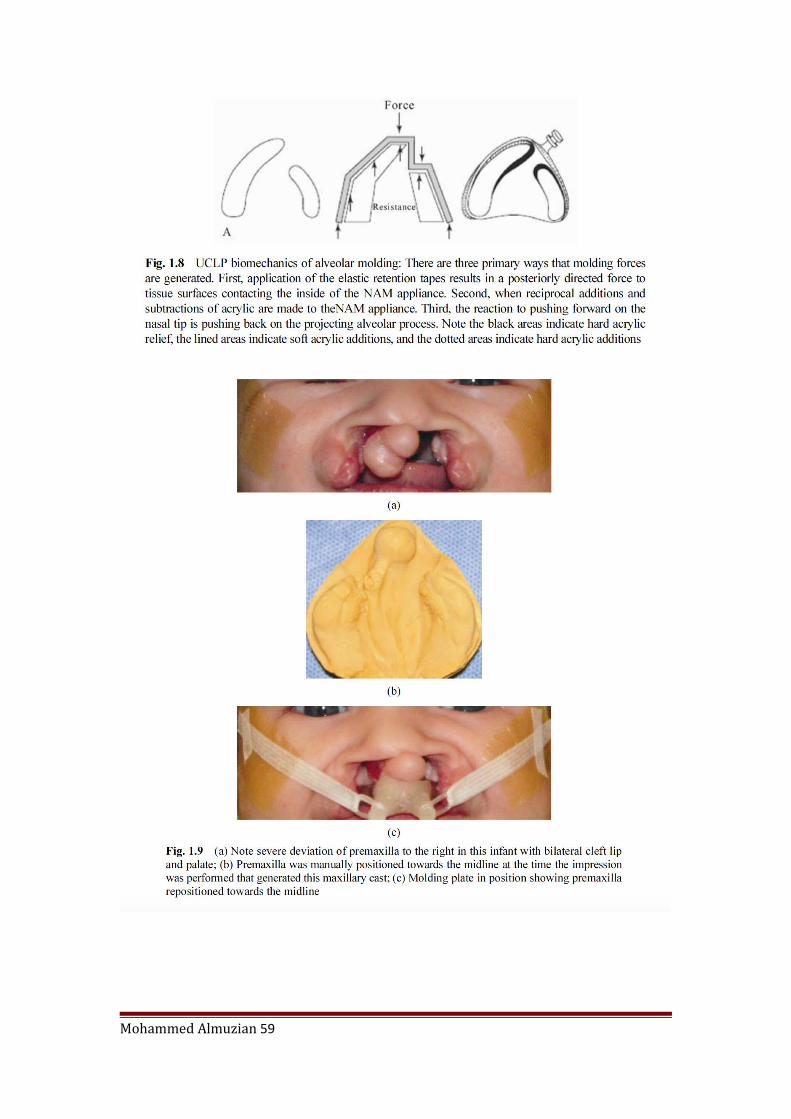
A. NASOALVEOLAR MOULDING: NAM inserted in the nostrile
• NAM uses an intraoral molding plate to gradually approximate the
displaced alveolar segments, which results in approximation of the cleft
lip segments as well as the medial and lateral aspects of the nose.
• Once the underlying alveolar segments are approximated, the
overlying lip and nasal soft tissues attain a degree of laxity that permits
reshaping and alignment with the introduction of the nasal stent.
• In addition, owing to the plasticity of the alar cartilage during
infancy, the achieved changes can become permanent
• It is indicated in:
1. Infant with complete unilateral cleft lip and palate (UCLP) and the
associated nasal deformity
2. Infants born with complete bilateral cleft lip and palate (BCLP)
often present with the premaxillary segment positioned outside the
oral cavity, a wide nasal tip and alar base, and a severely deficient
columella.
Mohammed Almuzian 33

if nasal moulding is required then it should be add after dentolaveolatr
moulding
Mohammed Almuzian 34
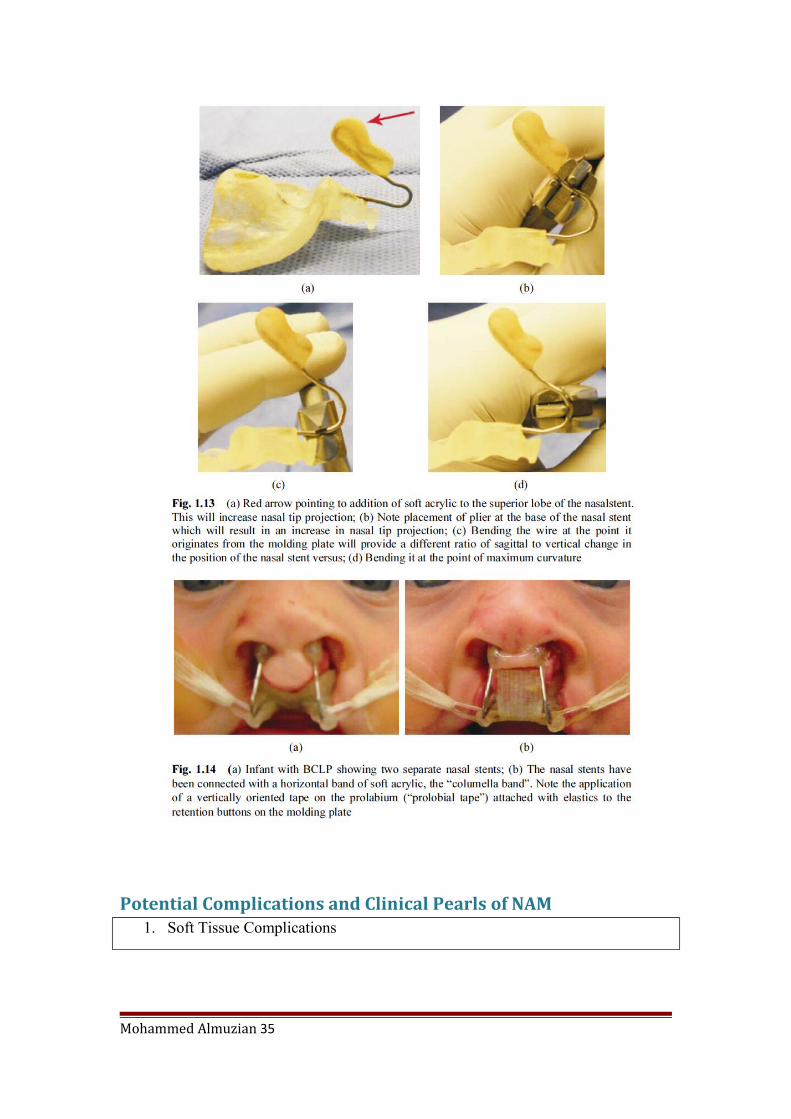
Potential Complications and Clinical Pearls of NAM1. Soft Tissue Complications
Mohammed Almuzian 35

• Mucosal irritatiom
• Nasal irritation
• Cheek irritation
2. Hard Tissue Complications
• severe reduction in
the width of an alveolar segment in the labiopalatal dimension which leads to an ectopic or premature eruption of the underlying primary teeth.
• Sometimes a neonatal
tooth is present on the cleft edge of the alveolar process. These “teeth” are ectopically located in a soft tissue sack that covers the bone on the alveolar gap and often must be surgically removed prior to the initiation
Mohammed Almuzian 36

of NAM therapy.
3. Compliance
• Various restraints can
be employed to prevent the child from removing the NAM ppliance from its mouth. (a) Mittens can be seen covering the hands; (
•
A. NASODENTAL MOULDING:
a. McNeil type plate
• Pioneered by McNeil.
• It is usually carried out immediately after birth.
• The types and their aims are:
• In unilateral clefts reduces displacement of the greater segment
and maintain the position of the lesser segment.
• In bilateral clefts to move the lateral segments outwards while the
prolabium is moved palatally and rotated downwards. Reduction of
premaxillary protrusion in bilateral clefts. Treatment comprises an intra
oral appliance carrying an active component (screws) to separate the
Mohammed Almuzian 37

lateral segments. Elastic strapping across the prolabium (upper lip) is
used to restrain the premaxillary growth.
b. lip taping
c. a pin-retained Latham
appliance (Latham lip
strapping)
B. OBTURATORS
• Passive obturating plates that assist feeding
• Active obturating plates
Recent evidences by Shaw et al in 1992 showed that:
• Low outcome if presurgical orthopaedic is used
• Dutch-cleft study by Anderson suggest that these devices offer
no benefit to outcome either in terms of the surgery or feeding
during this period.
SIX Months of age
A. Lip Repair
• Tennison technique or Randall technique (grives Fuller lip)
• Millard technique (gives best scar)
Mohammed Almuzian 38
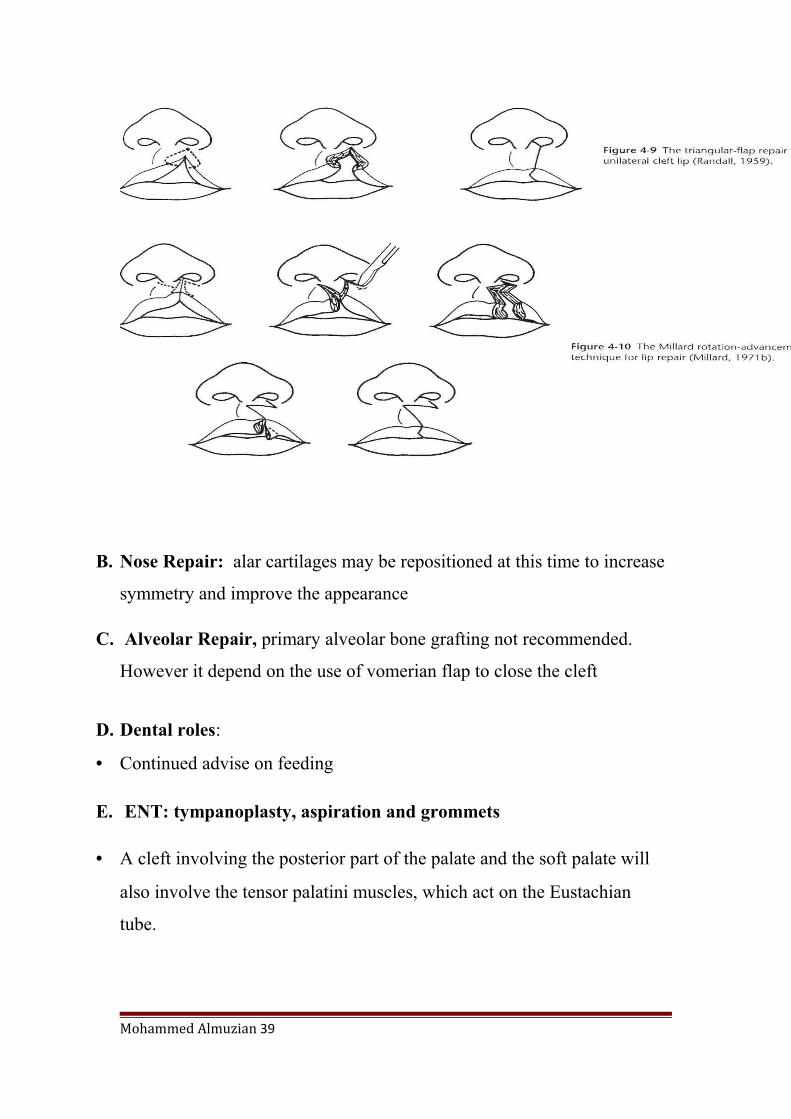
B. Nose Repair: alar cartilages may be repositioned at this time to increase
symmetry and improve the appearance
C. Alveolar Repair, primary alveolar bone grafting not recommended.
However it depend on the use of vomerian flap to close the cleft
D. Dental roles:
• Continued advise on feeding
E. ENT: tympanoplasty, aspiration and grommets
• A cleft involving the posterior part of the palate and the soft palate will
also involve the tensor palatini muscles, which act on the Eustachian
tube.
Mohammed Almuzian 39

• This predispose to problems in the middle ear ventilation (glue ear).
• Therefore, it is important that the cleft patient’s ears should be examined
at the time of lip surgery to ensure adequate middle ear drainage.
• About 98% of the cleft patients will have otitis media (Grant et al., 1988)
and will need tympanoplasty, aspiration (ventilation tubes inserted
through the tympanic membrane under general anaesthetic) and
grommets
6-12 Months of age
A. Palatal Repair
Soft palate repair
1. Z-plasty
2. Intra-velar veolplasty: radical dissection and reorientation
Hard Palate repair
1. V-Y closure technique
2. Von Langenbeck technique
3. Delair technique
4. Primary tongue flab technique
Some claim that it is better to delay the closure to 5-6 years to avoid scar
occurrence and subsequent growth retardation. But in this case the defect
Mohammed Almuzian 40

should be closed with obturators; otherwise the speech would be
dramatically influenced.
B. Sometime Lip and soft palate repair undertaken at 6 months at one
time
C. Dental roles:
• Continued advise on feeding,
• Diet analysis
• OHI
• Use of fluoride
• Restorative care
D. Pharygoplasty:
• In proportion of cases the repaired palate does not completely seal off the
nasopharynx during speech and nasal escape of air may occur, resulting
hypernasality.
• Nasopharyngoplasty is undertaken at the same time as the primary palatal
repair is performed.
• However, it is preferable to carry this procedure at the age of 4-5 years.
• Spreistersbach et al.25 quoted 50% of children with repaired cleft palate
develop normal speech spontaneously; 25% required speech and language
therapy and 25% required further palatal surgery.
Mohammed Almuzian 41

Aetiological factors pf speech problems:-
1. Velopharyngeal insufficiency,
2. Hearing problems
3. Dental and occlusal anomalies.
4. Developmental learning disability.
5. Psychosocial impact.
1-5 Years of age
1. Lee records at 5 years stage
2. Assessment using the 5-year-old index introduced by Attack 1997
3. Interceptive Orthodontic treatment
• Elimination of anterior crossbites
• Identify potential problems such as supernumaries.
• If second premolars are missing plan early loss of maxillary E’s to allow
spontaneous closure by the molars.
• In deep bite case consider a bite plane to allow posterior tooth eruption.
• Plan loss of deciduous teeth around the cleft early to improve quality of
mucosa prior to grafting
4. Dentist roles
• Diet analysis
Mohammed Almuzian 42

• OHI
• Use of fluoride
• Restorative care
5. Speech and hearing assessment. Consideration for pharygoplasty and
grommets.
6. Primary bone grafting is carried out within the first 2 years of life and is
less popular than secondary bone grafting. Primary bone grafting is
considered unfavorable and usually results in crossbite, malocclusion and
mal-union of the maxilla.
7-10 years of age
1. Lee’s records
2. GOSLON Yardstick (Mars 1987).
3. Secondary alveolar bone grafting:
Types of ABG
1. Primary bone grafting (at the time of lip repair at age of 3 months)
2. Early secondary bone grafting (between the ages of 2 and 5 years)
3. Secondary alveolar bone grafting (ABG) for patients with orofacial clefts
is usually carried out between the ages of 9 and 11 years;
4. Tertiary bone grafting in late adolescence (Rosenstein et al., 1982; eppley
and sadove, 2000)
• Alveolar bone grafting Introduced by Axhausen (1952).
Mohammed Almuzian 43
• Technique popularised by Boyne and Sands (1972, 1976).
• Pre graft records: Occlusal radiograph, study models and photos
• Orthodontic preparation for graft at approximately 8-11 years
before the eruption of the maxillary canine (Bergland 1986), ideally when
the canine root is ¼ to ½ formed. One exception is, if the lateral incisor
tooth is present, then earlier grafting may be considered.
• At this age, anteroposterior and transverse maxillary growth is
practically complete apart from the alveolar development of the erupting
permanent teeth. Hence grafting at this time does not affect mid face
growth but provides the all-important bone support for the erupting
canine.
• The viability of the result depend in the presence of unerupted teeth
otherwise the bone will resorbe again.
• Orthodontist might extract deciduous and supernumerary teeth to
provide sufficient attached gingiva.
• Treat caries and pathology
• The orthodontist is often required to expand the maxillary arch
prior to alveolar bone grafting, usually with a fixed expander such as a
tri- or quad-helix. This expansion help in:
1. Maximizes the size of the bony defect and creates access for the
surgeon to place the graft during surgery.
2. improves the maxillary arch form
Mohammed Almuzian 44

• Then the expander should be replaced with a stabilising
transpalatal arch with finger horizontal palatal extensions prior to surgery
to facilitate surgical access. Bilateral cleft cases require a stabilising arch
wire to secure the pre-maxilla, at least 19*25 SS.
• Transpalatal arches should remain for up to 3 months after surgery
for stabilisation.
• Care should be taken when aligning the incisors, as often the bone
covering the roots of the teeth is very thin. Often the aim then is to accept
the mesio-distal tip and rotations present in the upper incisors. Therefore
when placing the brackets it is wise to accept the inclination of these teeth
rather than try to upright them and moves the roots of the teeth out of the
bone and into the cleft space. After the bone graft the brackets can be
replaced and the roots moved into the correct position.
The main aims secondary ABG
1. Improve bony support for the alar base.
2. Improve nasal symmetry.
3. Eliminate any mucosal recesses liable to cause food
retention.
4. Elimination of oro-antral communication.
5. Aims to stabilize maxillary segments
6. Allow spontaneous eruption of teeth into the cleft area
7. Enable orthodontic tooth movement through the cleft site,
8. Facilitate any prosthetic restoration via implant
Mohammed Almuzian 45

Surgical technique of ABG
1. Incision
2. After closure of the nasal surface
3. Cancelous bone is harvested from donor sites, The best source of bone for
grafting for the alveolar cleft defect is the iliac crest, The rib, the cranium,
tibia and the mandible or artificial bone graft have also been used.
4. Cortical bone is not preferred because of the reduce vascularity and high
risk of necrosis.
5. Additional bone is placed under the ala and the nose on the cleft side to
provide nasal symmetry.
6. The covering flaps are then closed.
7. A protective palatal splint or orthodontic arch wire is sometimes used for
further stabilization,
8. Modified flaps may be needed to close residual palatal fistulae defects.
9. Success rate when graft placed prior to eruption of canine 90%. But drop
to 72% after or during eruption of canine.
10. Success of UCLP=BCLP if adequate stabilisation of premaxilla.
11.Then it is usually possible to proceed with orthodontic movement of teeth
in the grafted
Postoperative instruction
1. Preoperative intravenous antibiotics should be administered and then
postoperative prophylactic antibiotics given orally for 5 days.
Mohammed Almuzian 46
2. Maintain scrupulous oral hygiene.
3. The patient is given a semi- solid diet by mouth and chlorhexidine
gluconate mouthwashes.
4. Adequate analgesia for both oral and donor sites.
Postoperative assessment
1. General assessment After 6 weeks to check infection
2. After 4-6 months Kindealn score
3. Rarely, one year after ABG, Bergland index, Chelsea Index
(Witherow et al., 2002) comprises the Chelsea grade (position of bone)
and Chelsea scale (quality of bony bridge); whereas, the index proposed
by Long et al. (1995) assesses the percentage of bone covering the roots
of the teeth adjacent to the graft site.
The complications
1. Morbidity of donor area
2. Granuloma formation.
3. Failure
• A unilateral alveolar defect.
• Anterior oronasal fistula.
• Alar-base asymmetry
4. Around 15% of the canines will require exposure.
5. External root resorption
Mohammed Almuzian 47
Influencing success
1. Dental development – best results when carried out before canine
eruption (Bergland et al, 1986; Lee et al, 1995; Kalaaji et al, 1996;
Enemark et al, 1997)
2. Donor site: Iliac crest best (LaRossa et al, 1995) although not statistically
significant in CSAG study (Williams and Sandy, 2003). Chin is the good
as well but morbidity is high and the bone might be insufficient.
3. Pre-operative health of graft site
4. Post-operative care
5. Socioeconomic status and ethnic group
6. Surgical procedure + more experience = better results
7. Extraction of teeth at surgery (not statistically significant in CSAG
(Williams and Sandy, 2003)
8. Surgeon specialty (OMFS better than Plastic surgeon) not statistically
significant (Williams and Sandy, 2003)
9. Bone volume – weigh alveolar bone (Kamakura et al, 2003)
10.Complete closure of fistulae
Segmental Surgery at the same time of the secondary alveolar bone
grafting, Harris 2008
Segmental surgery is now rarely required at the time of alveolar bone
grafting, as orthodontic preparation or distraction osteogenesis will
usually align the segments. It should be avoided because:
Mohammed Almuzian 48
a) Fixation is problematic
b) Bone grafts do not unite with mobile segments.
However, the local dentoalveolar relationship may be improved by
combining the alveolar bone graft with an osteotomy to the lesser
segment or premaxilla. The lesser segment osteotomy is carried out at the
LeFort I level.
The most common indications are:
1. Vertical deficiency of the lesser segment.
2. The fistula is too large to close for bone grafting
3. Orthodontic expansion of the arch has not been possible as the lesser
segment may be trapped palatally.
4. Distraction osteogenesis is not available.
Lesser Segment Alveolar Distraction
• Segmental alveolar distraction may overcome the technical
difficulties of dividing and fixing small osteotomy segments.
• By slowly moving the lesser segment at one millimetre per day
towards the cleft, the size of the alveolar and dental gap is reduced.
• This decreases the size of both the graft and the flaps raised to
close the fistula. It may even eliminate the need for an autogenous bone
graft.
Mohammed Almuzian 49
Segmental distraction is only possible in young patients with erupted
teeth on which brackets and tubes can be applied to fit a rigid wire to
guide the distraction forward and around the arch form.
11-15 Years of age
Pharyngoplasty
• Pharygoplasty may be undertaken at 11-15 years to improve velo-
pharyngeal competence, if not already undertaken at an earlier age.
• VPI may become a greater problem in the adolescent as lymphoid
tissue shrinks effectively increasing the distance the scarred soft palate
needs to breach to create a seal.
Orthodontics
Conventional orthodontic treatment if the malocclusion is simple with or
without EOA
18+ Years of age
1. Lee’s Records
2. Orthognathic surgery
Secondary surgical correction for CLP patient
Specific Problems in Cleft Patients
1. Sever skeletal problem in all direction with malar hypoplasia.
2. Anterior open bites are common
Mohammed Almuzian 50

3. Posterior cross bites are common
4. Dental development may also be delayed in both arches but is most
evident in the cleft segment and may compromise the presurgical
orthodontics.
5. The repaired alveolar cleft is a potential site for fracture at the time of the
down-fracture.
6. If the maxillary alveolus has not been reconstructed, alignment of the
alveolus can be incorporated into the orthognathic procedure. However it
complicates the planning of the surgery and increases the potential
morbidity. Segmental osteotomies are less stable than one-piece
maxillary osteotomies.
7. Previous surgery produces scarring of the labial and buccal vestibule, the
palate and behind the maxillary tuberosities. This presents problems with
the surgical incisions, mobilisation and postoperative closure of the
surgical wound.
8. A pharyngeal flap may make advancement of the maxilla difficult and
will need to be divided. The patient has to be informed well in advance
about the possibility of VPI and speech problem that might developed
after the surgery.
Treatment Planning for CLP
The basic facial and orthognathic evaluation is the same as the non-cleft
case with important refinements.
1. Lip-incisor relationship. As in the non-cleft case, the lip to maxillary
incisor relationship is extremely important. The major surgical moves are
Mohammed Almuzian 51

predominantly in the maxilla and with a tight, previously scarred upper
lip, small skeletal moves have a pronounced effect on the incisor
exposure.
2. Asymmetries. Both dental and skeletal asymmetries are dominant
features, often with compensatory asymmetries in the mandible. This
should be considered
3. Pharyngeal obstruction can be caused by hypertrophied adenoidal tissue
or pharyngeal flaps. Nasal airway obstruction may arise from a deviated
nasal septum narrowing of the nares, hypertrophied turbinates, nasal
polyps and posterior choanal constriction from sub-periosteal bone and
asymmetrical vomer flaps. The management of these problems is an
essential part of the orthognathic procedure. Paradoxically the adenoid
mass may contribute to velopharyngeal function and its removal may
precipitate velopharyngeal inadequacy.
4. Preoperative speech assessment and counselling.
5. However, infection, bone and soft tissue necrosis, delayed healing, loss of
teeth and relapse all occur with greater frequency due to multiple
previous surgeries.
The Choice of Operation for CLP
Maxillary Hypoplasia
1. LeFort I osteotomy either one piece or two pieces maxilla for transverse
maxillary widening.
2. High LeFort I level osteotomy.
3. The modified LeFort II and Kufner LeFort III osteotomy
Mohammed Almuzian 52

4. SARPE
5. Rhinoplasty may be necessary.
6. Mismanagement of the soft tissues during closure of the labial vestibular
incision may cause shortening and thinning of the upper lip. The V-Y
closure of a maxillary vestibule incision may increase the vermilion show
in patients with a thin upper lip.
7. Maxillary advancement widens the alar base, increases the projection and
elevation of the nasal tip and the width of the nares. Various surgical
manoeuvres can be used to prevent these unwelcome side effects. These
include an alar base cinch suture, recontouring the bony piriform aperture
either by trimming and/or asymmetric bone grafting and alar base
resections.
Mid Face Distraction Osteogenesis
Indications:
• With gross maxillary hypoplasia and a severe degree of scarring, the
degree of advancement may be beyond the expected limits of stability of
a conventional osteotomy. Distraction of the maxilla is preferable to a
surgical compromise such as a mandibular setback.
• If the deformity is complex particularly in the upper mid face then a
higher level osteotomy with distraction often gives a better result than a
modified LeFort I with masking onlay bone grafts or modified LeFort II
and LeFort III osteotomies that are difficult to perform and can give
unsightly steps particularly over the radix of the nose.
Mohammed Almuzian 53
• There is usually a need for pre-surgical orthodontics.
• Due to risk of worsening VPI and due to previous surgical scarring, the
Large jaw discrepancies of 10mms and above may also require a
mandibular setback
• a modified maxillary Le fort 1 advancement or Converse Wake Procedure
(that move the maxilla without influencing the position of the palate) is
used with careful attention paid to the mobilisation of the maxilla.
• Use Horseshoe osteotomy as alternative
• Use Distraction osteogenesis as alternative
• Severe maxillary restriction may require Surgically assisted RME and 2
or 3 piece Le fort 1 osteotomies
• Any expansion gained should be permanently retained. (Proffit and White
1990)
Mandibular setback (BSSO, VSO)
Mandibular set back indicated in case of:
1. Mandibular prognathisism
2. When there is a maxillary surgical limitations such as severe palatal
scarring, borderline velopharyngeal insufficiency or a tight inferiorly
based pharyngoplasty flap.
3. During maxillary advancement and inferior positioning, the anterior
maxilla is differentially positioned more inferiorly. This will produce a
Mohammed Almuzian 54

posterior open bite deformity unless a mandibular ramus procedure is
undertaken simultaneously. Differential down grafting of the anterior
maxilla also results in a counter clockwise rotation of the mandible which
may make the chin retrogenic. This can be corrected by a simultaneous
augmentation genioplasty.
Airway Considerations for CLP during surgery
1. The surgeon can do the following whilst the maxilla is down fractured
• Contouring of the inner aspects of the nose
• Asymmetries in the piriform region
• The mucosa of the nostril floor can be repaired
• Septoplasty may be indicated
• Partial or complete inferior turbinectomies
• Antral and nasal polyps can be removed
2. Pharyngeal flaps raise additional concerns for the anaesthetist and
surgeon which may make intubation difficult and restrict the nasal
airway, so submental intubation might be indicated
Postoperative considerations for CLP
1. Speech therapy: The soft palate mechanism in non-cleft patients has
considerable reserve capacity and can adapt to an increase in length. The
repaired cleft soft palate does not have this capacity to adapt especially
Mohammed Almuzian 55
after major advances. The patient with borderline velopharyngeal
incompetence preoperatively is likely to develop worsening of their
speech postoperatively.
2. Relapse: As a prophylactic measure, extraoral elastic traction using a face
mask can be used in patients who are considered particularly at risk of
relapse either due to scarring or who have had large surgical moves
anteriorly and inferiorly.
3. Stability: The factors that increase stability include:
• High quality orthodontic preparation.
• Avoiding segmental procedures
• Overcorrection where possible.
• Compromise position must be planned and if necessary with
incorporatation of a mandibular setback.
• Alveolar bone grafting.
• Bone grafting for inferior repositioning of the maxilla.
• Internal rigid fixation for all moves.
3. Secondary plastic procedures
Such as nose and lip revision. These are best undertaken after growth,
since growth can detrimentally affect earlier revisions.
Mohammed Almuzian 56

Terminology
Velopharyngeal impairment is a generic term indicating that the patient
is unable to induce sufficient contact between the velum and the posterior
and lateral pharyngeal walls
Velopharyngeal insufficiency is a form of velopharyngeal impairment
caused by a soft palate whose functional length is insufficient.
Velopharyngeal incompetenceis a form of velopharyngeal impairment
caused by neuromuscular impairment .
Hypernasality is a resonance phenomenon that occurs when sound is
inappropriately generated in the nasal cavity.
Maxillary and Nasal Impression • Using an appropriately sized infant impression tray loaded with a heavy
body Polysiloxane impression material
• The clinician who performs the impression must remain constantly
attendant to the infant’s airway. A small dental instrument (e.g. intraoral
mirror handle) is used to prevent the tongue from occluding the airway
during the impression procedure.
• Good intraoral illumination facilitating direct visualization of the tongue
position and the posterior aspect of the pharynx is essential to prevent
airway obstruction by excess impression material or the tongue.
• A clinical assistant should be present to mix the impression material, load
the impression tray, and then help where needed.
Mohammed Almuzian 57

• The surgeon or a physician, qualified to take appropriate action in case of
an airway emergency, holds the swaddled infant upside down during the
maxillary impression
• After the impression material is set, the impression tray is removed and
the oral cavity is examined to ensure that there is no debris from the
impression remaining in the mouth.
• An impression of the nose including the left and right medial canthi is
performed with a light bodied material (Memosil 2, vinyl Polysiloxane,
Heraeus Kulzer, Germany)
• Recently, a computer-aided system for NAM appliance fabrication and
adjustment has been described, and appears promising
•
•
•
Mohammed Almuzian 58
Mohammed Almuzian 59