cleaning up your sample prep processes
TRANSCRIPT

Cleaning up your sample prep processes
Julia C. Drees, Ph.D., DABCC
Scientific Director—Chemistry
Kaiser Permanente Regional Laboratories
Berkeley and Richmond, CA
Financial disclosures
Nothing to disclose
Learning Objectives
After this presentation you will be able to: List strengths and weaknesses of common sample
preparation techniques used for clinical LC‐MS/MS
Develop a plan to select the best sample prep automation for your lab
Describe pitfalls and solutions encountered when using automated liquid handlers for clinical LC‐MS/MS sample preparation

Common Sample Prep Options
Dilution
Protein Crash or Ultrafiltration (PPT)
Liquid‐Liquid extraction (LLE)
Solid Phase extraction (SPE) – can be offline or online
Dilution
Usually for urine drug confirmations
Typically 10‐20x dilution
Add a filtration step for added robustness
Protein precipitation (PPT)
Avoid adding internal standard (IS) to precipitation solvent
Ideally a ratio of 3:1 precipitant:sample
Options to include phospholipid removal for improved clean‐up and robustness
Must optimize time and parameters for:
Mixing (vigorous; vortex or wide‐bore tip)
Centrifuging (need tight pellet) or vacuum/positive pressure (robust enough?)

Liquid‐Liquid Extraction (LLE)
Best for neutral analytes
Ideally 10:1 solvent:sample
Mixture of polar and nonpolar solvents
More polar → more junk
Phase separation with freeze/pour (manual)
Challenging to automate
Use round deep well 96‐well plates
Aggressively stress test for cross‐contamination
Supported liquid extraction (SLE) is easier to automate
Solid Phase Extraction (SPE)
Most chances for using scientific approach for optimization
Ion exchange SPE is most selective (charged analytes)
Wash aggressively
Ideally twice, 2D, using pH changes and organic solvents
Sacrificing recovery in favor of clean samples is OK
Elute with small volume for more concentrated samples and/or quicker dry times Adapted from Russell Grant, Ph.D. – MSACL Quant. MS Development
& Validation short course, with permission
Comparing extraction modes
Rank ordered 1=best, 4 = worst.
* = Ion exchange SPE mode etc.
Table from Russell Grant, Ph.D. – MSACL Quant. MS Development & Validation short course, with permission
Nature of analyte is
major decision
point

Extraction methods’ relative simplicity/robustness
SPE PPT LLE
Simpler More Robust
Best
Worst
Adapted from Judy Stone, Ph.D.
Regardless of extraction mode, do this: Add internal standard (IS) as FIRST step in extraction
Evaluate for ion suppression:
Qualitative (post‐column infusion with injection of multiple patient extracts) (Annesley, Clin Chem 2003; 49:1041‐4.)
Quantitative (no matrix & pre‐ & post‐ extraction spikes with matrix)
Getting pre‐ & post‐spikes correct is tricky!
Challenge with numerous patient samples EARLY in development
Don’t ignore outliers 1 failure in 10 samples translates to 10 repeats/day with a batch of 100 and
250 repeats/day with batches of 2,500!
How will you resolve MRM ratio failures, IS low recovery failures, interfering peaks, etc.?
Do precision first and don’t accept a 10‐15% CV as final
Understand that easier extractions (dilution, basic PPT) may look good in development but cause problems down the road
Adapted from Judy Stone, Ph.D.
Quantitative characterization of your extraction: recovery, efficiency, matrix effects Sample A: Neat sample (exhibits 100% recovery, no matrix effects)
Sample B: Unspiked patient/matrix sample, extracted then spiked during reconstitution (exhibits only matrix effects)
Sample C: Spiked patient/matrix sample, extracted (reduced recovery, exhibits matrix effects)
% Recovery = C/B * 100
% Matrix Effect = B/A * 100
% Process Efficiency = C/A * 100
Sample A can be averaged replicates; split patients to make samples B & C and do for multiple patients
Reproducibility between patients is more important than approaching 100%
Better: all patients exhibit 70‐80% matrix effect and 50‐60% recovery
Worse: some patients exhibit 90% recovery & matrix effect, others 60%
Matuszewski, Anal Chem 2003; 75(13):3019‐30.

Automation
Online extraction
Automated liquid handlers
Case histories in automation
Online SPE skips evaporation and reconstitution steps
Symbiosis product literature, Spark‐Holland
Online extraction ‐mechanics
Schebb, Anal.Methods 2011; 3: 420
6‐port switching valve

Considerations for feasibility of online extraction
Evaluate cycle times of extraction & LC run with care: Is throughput adequate? Are two extraction lines “multiplexed” to one LC?
Are more than one extraction + LC lines “multiplexed” to one MSMS?
Compatible with all MS vendors (customers in production)?
Vendor support for method development?
In‐house troubleshooting, repair?
Can’t start with primary patient sample tube Sample and IS still have to be mixed before the sample is
put onto the LC‐MSMS
Adapted from Judy Stone, Ph.D.
Considerations for Online Extraction‐ Analytical Issues
# of solvents, solvent types for wash & regeneration of SPE column (solvent select valves, miscibility, carryover)?
How to elute (strong solvent) from the extraction column and retain downstream on the analytical column (weaker solvent)?
How to do LC gradient development, SST, validate recovery & ion suppression (can you inject with bypass of the extraction column)?
Many labs do a protein crash before online extraction
Judy Stone, Ph.D., Mass Spec in the Clinical Lab 2013
Automated Liquid Handling

Adapted from Judy Stone, Ph.D.
Automated Liquid Handling
1, 2, 4, 8, &/or 96 pipetting channels
Tubes and 96 well plates
Can do tube to plate (starting with patient sample tube) AND extraction
Many accessories for extraction (shaker, heater, cooler, vacuum module, positive pressure, evaporator)
Barcode reading
Considerations for best value from ALH Disposable tips vs. washable (consumable cost vs.
carryover risk, speed of each?)
# of pipette channels (>$ = >throughput) 8 channel good for tube to plate transfer
96 channel good for “plate stamping”
Barcode reading Write files for worklist; interface to LIS/middleware?
Deck space—room for accessories? Gripper to move items around deck (stacking/unstacking)
Off‐deck storage with auto‐transfer to deck
Nearby service support
Application support/programming? Software is generally either user‐friendly OR powerful

Considerations for Automated Liquid Handling – Analytical Issues
Minimum and maximum pipettable volumes (and with what precision)?
Working with difficult liquids
Precise for organics? (Anti‐dripping solutions?)
Will acids damage components?
Can instrument be vented?
Liquid level sense & clot detection
Reagent delivery channel(s) ‐ how many solvents?
Effective on‐deck mixing is challenging
Cross‐contamination must be aggressively stress‐tested if using 96 well plates
Adapted from Judy Stone, Ph.D.
Automation choices Online extraction
Vendor “complete” solutions
Thermo‐Scientific/Cohesive Technologies
TLX Turbo‐Flow online SPE extraction
Spark‐Holland/Symbiosis – dual channel cartridge online SPE
Gerstel MPS Workstation with in‐tip dispersive SPE
User‐developed online SPE
Most LC‐MSMS vendors have packages/software ‐extraction pump(s), switching valves, installation, application notes
Automated Liquid Handling (ALH)
Many vendors and style options
Useful even just for tube to plate before online or off‐the‐deck extraction (e.g., positive pressure SPE)
*Most affordable option
Online Extraction vs. Automated Liquid Handling (ALH)Parameter Online ALH
Tech hands on time/sample Less More
LC sophistication required More Less
Flexibility Less More
Suited to many assays Less More
Suited to 1 high‐volume assay More Less
Sensitivity per L starting sampleǂ More Less
Risk of carryover More Less
Risk of cross contamination (96‐well plates) Less More
Throughput Less* More
Adapted from Judy Stone, Ph.D.
ǂIf limited sample available (e.g., pediatrics), online is better. ALH requires dead volume both in sample tube and after reconstitution*Multiplexed online extraction increases throughput

Automated Liquid Handling –Case Histories
Sample prep for 25‐OH Vitamin D analysis by LC‐MSMS
Thanks to my colleagues who helped troubleshoot these cases
Judy Stone, Ph.D.—Center for Advanced Laboratory Medicine, UCSD
Bret Martin – Applications Programmer, Hamilton Robotics
1. Transfer 50 µL IS from reservoir to plate (8 tips, pick up & dispense 12 times)
IS reservoir
2. Transfer serum from tubes to plate (8x12 tips) & mix w tips
Tube to Plate
3. Move plate to 2nd ALH (96 channel head)
4. Transfer serum + IS to PPT/phospholipid removal plate
5. Transfer precipitating reagent to extraction plate and mix with tips
7. Sealed plate on LC-MSMS
Plate Stamping
6. Vacuum to elute into collection plate below

Case 1 –The Touch‐OffTask
Pipet serum and internal standard (IS) to a 96‐well plate
Desired intra‐assay precision (within plate) = <5% CV
Development History
Original Protocol:
50 µL IS dispensed into plate
50 µL serum added, mix with tips
Intra‐assay precision 4‐6%
Revised Protocol:
2 precipitation reagents instead of 1 (more robust)
Total volume had to stay the same
IS volume must be decreased to 25 µL
Problem: %CV ↑ to 6‐9% when IS volume ↓ from 50 µL to 25 µL
Re‐measure bottom of plate dimensions w calipers & adjust height of dispense – not fixed
Lower height of dispense (with only 25 µL not touching off on bottom of plate?) – not fixed
Slow speed of dispense – not fixed
Pause after dispense – not fixed
Blow out of residual volume in tips – not fixed

Solution
Dispense serum 1st
Dispense IS 2nd ‐ touch off to serum (liquid) instead of questionable touch off to (dry) plate
Intra‐assay % CV decreased to 2‐4%
Trade offs
Touch off to serum requires new tip each well
Increased tip cost (from 8 to 96 tips)
Tube to plate time increased ~5 min/plate
Lesson learned – small changes can make a big difference in liquid handling precision
2. Transfer 50 25 µL IS from reservoir to plate (8 tips, pick up & dispense 12 times) (8x12 tips & mix)
IS reservoir
1. Transfer serum from tubes to plate (8x12 tips) & mix w tips
Switched order of tube to plate. Increased time and tip usage but superior precision.
Case 2 – Missing filtratesTask
Precipitate serum + IS in a hybrid (protein & phospholipid removal) filtration plate –transfer filtrate to collection plate (vacuum)
Major constraint
Don’t move plates off deck during the process to maintain viable work flow for 25 plates/day

Problem
First few plates look good
Then a few wells in every plate –no filtrate transferred to collection plate
All other wells in those plates have expected recovery
?
Investigation
Change of plate lot? – not fixed
Break through of filtration membrane or quick flow through in surrounding wells causing inadequate vacuum for problem wells? – unable to prove or disprove
Clogged membrane in problem wells –why OK before & not now?
Eureka!
Initial studies used frozen aliquots of pooled serum
Had recently switched to fresh patient samples
Vendor validated with frozen rat serum
Hypothesis
Frozen serum precipitate ≠ fresh serum precipitate
Difference size of particulate clogging filter?
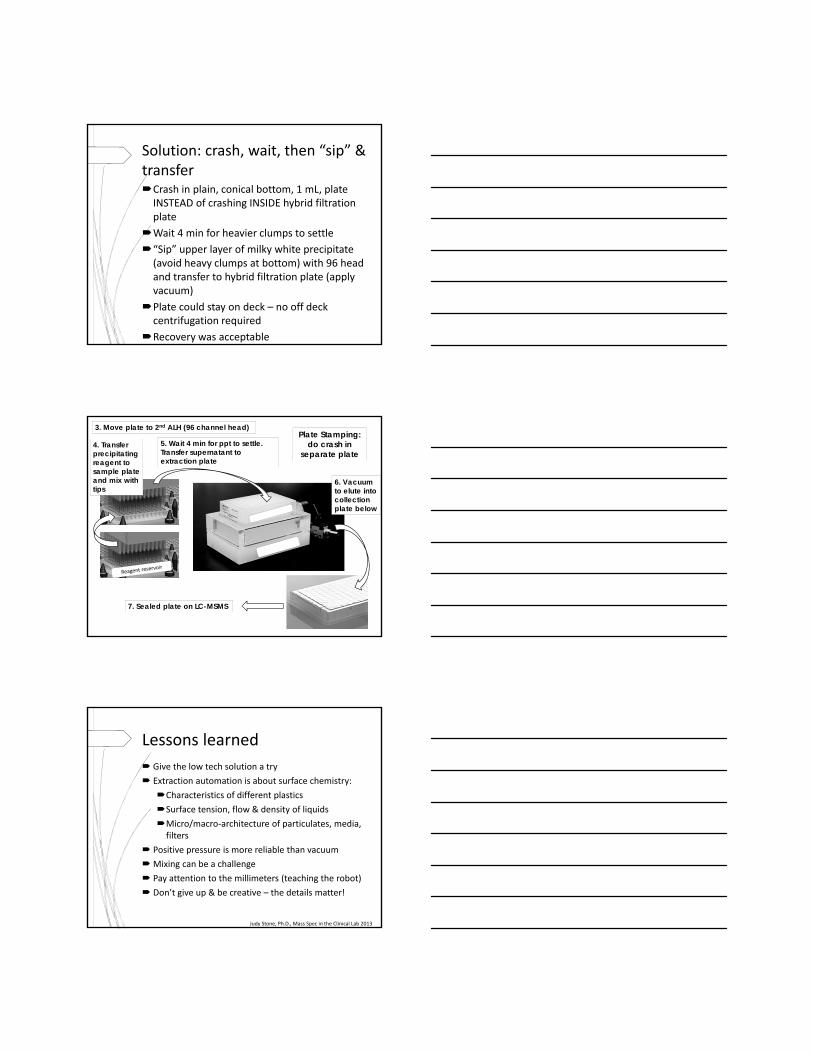
Solution: crash, wait, then “sip” & transferCrash in plain, conical bottom, 1 mL, plate INSTEAD of crashing INSIDE hybrid filtration plate
Wait 4 min for heavier clumps to settle
“Sip” upper layer of milky white precipitate (avoid heavy clumps at bottom) with 96 head and transfer to hybrid filtration plate (apply vacuum)
Plate could stay on deck – no off deck centrifugation required
Recovery was acceptable
3. Move plate to 2nd ALH (96 channel head)
5. Wait 4 min for ppt to settle. Transfer supernatant to extraction plate
4. Transfer precipitating reagent to sample plate and mix with tips
6. Vacuum to elute into collection plate below
7. Sealed plate on LC-MSMS
Plate Stamping: do crash in
separate plate
Lessons learned
Give the low tech solution a try
Extraction automation is about surface chemistry:
Characteristics of different plastics
Surface tension, flow & density of liquids
Micro/macro‐architecture of particulates, media, filters
Positive pressure is more reliable than vacuum
Mixing can be a challenge
Pay attention to the millimeters (teaching the robot)
Don’t give up & be creative – the details matter!
Judy Stone, Ph.D., Mass Spec in the Clinical Lab 2013

Case 3 – static cling of tips to pipette head (tips not shucked)
Solution
Purchase tips without plastic film wrapping of individual tip boxes
Only re‐use reagent tips a few times (static builds up with re‐use)
Static seemed to vary with humidity
Anti‐static devices were not too helpful
In conclusion
Attention to trivial detail & persistence was the key to success
Automation made possible extraction of 2,500 samples/day by two techs in 4‐5 hrs (LC‐MSMS ran for 20 hrs)
Long term (18 mos) precision across 3 instruments (6 streams): 4‐6% CV

Thanks for your attention